
Submitted:
10 August 2023
Posted:
11 August 2023
You are already at the latest version
Abstract
Podiatric surgeons routinely use electrosurgical devices to cut and coagulate tissue during surgical procedures. Although advances in technology have made electrosurgery increasingly safer for patients and personnel, its use is still poorly understood by those using it and the hazards associated with its use still exist presently. Human error, direct or indirect transfer of electricity to a conductive device, or device malfunction can cause serious adverse events, including burns, electrical shocks, and or fires. Here, we report a rare case of a 43-year-old man who suffered severe burns during hallux valgus surgery. The surgeon and the nursing staff did not notice any injuries during the surgical intervention. This case highlights the need to implement tools to help health professionals improve patient safety during surgery. Based on the case herein reported, a specific checklist was implemented to prevent adverse events related to electrosurgery in our podiatric unit to reduce the risk of electrosurgical complications.
Keywords:
electrosurgical injury
; monopolar diathermy
; burns
; electrosurgical safety
1. Introduction
Electrosurgery is the most used energy source in orthopaedic and podiatric surgery. Since its introduction into surgical practice, surgeons have increasingly used electrosurgery. Despite the technical improvement in terms of the safety of the equipment used, human error, direct or indirect transfer of electricity to conductive devices, or device malfunction can cause adverse events. The exact incidence of electrosurgical complications is not known exactly. Injuries related to diathermy have probably been under-reported, and most complications are treated without knowing the cause. It is estimated that approximately two-thirds of thermal injuries may not be detected during the procedure [1,2,3,4].
The physical principle of electrosurgery is based on generating high-frequency alternating energy from low-frequency electrical current. This energy achieves the cutting and coagulation effects in the tissues in which it is applied, derived from the thermal energy that is generated. There are two commonly used electrosurgical modalities depending on the number of electric poles at the site, monopolar and bipolar diathermy. Both electro-surgical devices require two poles to complete an electric current. The main difference between the two types of current is the distance between the poles that determines the power used. In unipolar mode, the tip of the device is the active pole, while the second pole is the return electrode or grounding plate. In monopolar mode, a continuous current is necessary to produce vaporisation of cellular water around the electrode. Efficient cutting requires the electrode to move slowly but continuously through the tissue, while with bipolar current, both poles are part of the tip of the instrument. Monopolar diathermy devices have a high-power output needed to overcome the long distance between the poles because the human body is a relatively poor conductor of electric current. Bipolar devices have a lower power between one third and one tenth than unipolar systems, so the energy generated is insufficient to cut the tissue and can only desiccate it [5,6].
In orthopaedic surgery, monopolar mode is the most widely used modality due to its most appropriate current to use in mixed mode, providing good dissection with varying degrees of coagulation. However, monopolar electrosurgery requires considerable knowledge, understanding, and vigilance of the operator to avoid the hazards of unintentional thermal injuries [5,6,7]. We report a rare case of electrosurgical burns of partial thickness burns on three toes during hallux valgus surgery. This unusual clinical case serves to highlight the importance of implementing protocols to prevent injuries related to the use of electrosurgery. On purpose of the herein reported case, a specific checklist was implemented to prevent adverse events related to monopolar diathermy in our podiatric unit.
2. Detailed Case Description
A 43-year-old man presented in surgical service of the Podiatric Clinic Area of the Universidad de Sevilla. He presented a painful matarso-phalangeal joint (MPJ) with loss of flexor capacity in the hallux and slight hyperesthesia in the tips of the hallux and in the second and third toes of the left foot. According to his surgical history, in 2021 he underwent an operation to correct hallux valgus deformity by chevron capital osteotomy and proximal Akin procedure (Figure 1). The patient reports that a year later he had to be operated on again due to pain at the level of the first MPJ to remove the osteosynthesis material. The second surgery was performed outpatiently with epidural anaesthesia through a medial incision at the level of the MPJ (Figure 2).
The patient was reviewed to perform the first cure five days after surgery, and the nurse noticed that the skin was red and the blisters fade under pressure with pain in the ball of the first, second, and third toes compatible with partial thickness burns (Figure 3a). After consulting with the surgeon, he is unaware of the circumstances that caused the injuries, and the nursing staff was urged to take care of the cures for both the surgical wound and the burns. The injuries were initially treated by the patient at home with applications of povidone iodine antiseptic solution. After two weeks, the skin staples were removed in the medial incision made in the MPJ, and redness of the blisters was observed to fade under pressure (Figure 3b). After three weeks, rupture and desiccation of the blisters with epidermal necrosis areas in the burns could be observed that required surgical excision and local application of silver sulfadiazine (Figure 4a,b). Complete healing was achieved at 7 weeks.
Our radiographic examination showed signs of severe joint destruction compatible with resection arthroplasty at the level of the MPJ with significant shortening of the first toe (Figure 5). The patient was treated conservatively with orthopaedic insoles.
3. Discussion
In orthopaedic surgery, monopolar electrosurgery mode is the most widely used modality due to its most appropriate current to be used in mixed mode, providing good dissection with varying degrees of coagulation [5,6]. Several are drawbacks of monopolar electrosurgery, it requires considerable knowledge, understanding, and vigilance of the operator to avoid the hazards of unintentional thermal injuries. Accidental burns usually occur due to inadvertent contact with active or heated electrodes; direct or capacitive coupling; insulation defects in instruments or connections, and improper placement of the return electrode [5,6,7].
The Adverse events related to electrosurgery have been mainly reported as thermal injuries. An American College of Surgeons survey showed that 18% of laparoscopic surgeons experienced a complication attributed to electrosurgery, and 70% of burns originating during laparoscopic surgery are estimated to be unidentified [3]. In a review (January 1994 to December 2013) conducted using the FDA database on Surgical Energy-Based Device Injuries, 178 deaths and 3,553 injuries were reported. Most injuries caused by electrosurgery were commonly referred to as burns by direct application (32%), by dispersive electrode burns due to ground failure (29%) and burns due to insulation failure (14%). Almost half of the reported complications (45%) occurred with monopolar electrosurgical devices [1]. Inadvertent burns may occur in several ways during electrosurgery use. The reported burn injuries were most often caused by an improper application of a neutral electrode or by involuntary contact of the active electrode with tissue [8,9]. Thermal injuries due to device insulation failure of the device, direct coupling, or capacitative coupling are exceptional [10,11].
Capacitive coupling is a condition that occurs when electrical current is transferred from a conductor through intact insulation to adjacent conductive materials. Direct coupling occurs when another metal object such as a probe or retractor is touched by the active electrode. When the active electrode encounters another metal instrument, energy can be transferred from the active electrode to the instrument. In monopolar electrosurgery, direct coupling is often intentionally utilized to coagulate small bleeders using hemostatic forceps, held in contact with the active electrode. However, when the active electrode comes into unintended contact with another electrode or non-insulated conductive instrument, current from the active electrode flows through the adjacent instrument through the pathway of least resistance, and potentially damages adjacent structures or tissues not within the visual field that are in direct contact with the secondary instrument.
Adverse events by direct coupling have been widely described in the literature as a complication associated with laparoscopic surgery [4,7]. In orthopedic surgery, most of the reported cases occurred during arthroscopic surgery procedures, with much more rare cases reported in open surgery [12,13]. In the present case, it is likely that the injuries were caused by direct coupling when the active electrode inadvertently encountered a non-insulated metallic instrument such as an orthopedic retractor. The current could have been carried through the instrument, causing burns to the tissue in which this contact. Injuries could also have occurred if the metal retractor encountered a hemostat that was energized to coagulate a bleeding vessel.
The literature review shows that in 82% of the cases injuries from energy-based surgical devices were identified intraoperatively, inpatient postoperatively in 9%, and after discharge in 9% [1]. As in the present case, the injuries were undetected and not recognized until the following five days when a partial thickness burns were observed on the skin between one or three inches away from the medial incision (MPJ), appearing far away from the region where the electrosurgery was performed. These burn sites could be an area where the retractor rested on the skin.
To avoid accidents due to direct coupling as reported in this case, the exact location of the active electrode must be always controlled when it is being energized. Special care should be taken whenever the active electrode is energized near another metal object, especially retractors. Given that the surgical approach was made through a medial incision, it is likely that the plantar location retractor was the one that repeatedly encountered the active electrode, causing burns in the plantar area of the toes.
Because metal is a conductor far superior to tissue, it is possible that current density can increase around the metal implant if it is located between the active and dispersive electrodes. To date, no case reports have been reported on alternate site burns related to orthopaedic implants. The most commonly used metal implants in orthopaedic surgery are made of titanium. The electrical conductivity of titanium is very low because the availability of 2 free electrons in a 3d orbital makes titanium conduct electricity, but it is always at a low intensity. Due to this circumstance, it is unlikely that in the present case the removal of the osteosynthesis material (screws) could be related to the origin of the burns. However, remote thermal injury caused by aberrant intraoperative current grounding through titanium plating implants has been reported [14]. When metallic implants cannot be removed before use of electrosurgery, the best way to avoid this risk is to reduce the distance between the electrodes or, if necessary, use a bipolar device.
The available evidence shows scarce training about diathermy in trainees with a dearth of awareness among surgeons about diathermy resulting in failure to adhere to what is considered best practice [15,16,17]. The role of all the personnel involved in electro surgery is critical in the implementation of precautions to prevent electrosurgical injuries. Staff training, along with regular safety inspections, and the implementation of a standardized process are key to minimizing such risks and injuries associated with the use of electrosurgical devices use.
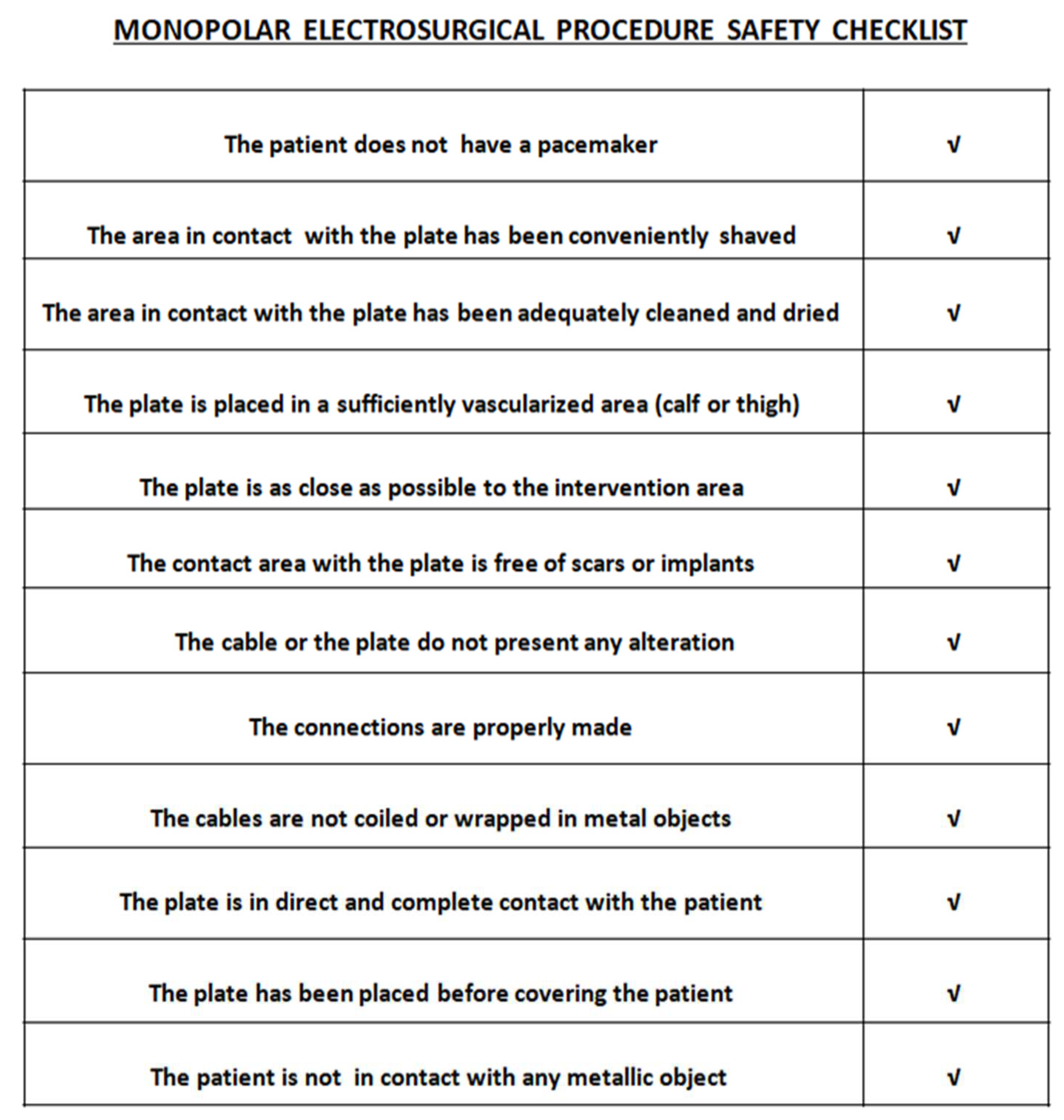
The incidence of error in surgery such as those reported here should be reduced, and surgeons and perioperative nurses should standardize processes and preoperatively assess risks, including electrosurgical injuries. The Surgical Safety Checklist is a useful tool developed by the World Health Alliance for Patient Safety, to help health professionals improve patient safety during surgery [18]. Numerous specialties have incorporated checklists in their strategies for the safety of surgical interventions [19]. However, nowadays it is necessary to continue to reduce the incidence of error in surgery. Guideline for Electrosurgical Safety provides guidance to perioperative personnel on the safe use of electrosurgical units [20]. Regarding the case presented, and to adapt and implement a tool based on clinical practise guidelines related to electrosurgical safety, we have developed a specific checklist model to improve safety related to possible adverse effects associated with the use of monopolar diathermy in our podiatry unit (Figure 6).
Author Contributions
A.C-F.: Conceptualization, data acquisition, visualization and writing original draft. F. M-G., A.L-C , M.D. J-C and VE.C-J.: data acquisition. A.C-F. and A.L-C..: supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Written informed consent was obtained from the patient to publish this paper. The confidentiality of patients’ data was respected.
Data Availability Statement
All data generated during this study are included in this article. Further enquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Overbey, D.M.; Townsend, N.T.; Chapman, B.C.; Bennett, D.T.; Foley, L.S.; Rau, A.S. : Yi, J.A.; Jones, E.L.; Stiegmann, G.V.; Robinson, T.N. Surgical Energy-Based Device Injuries and Fatalities Reported to the Food and Drug Administration. J. Am. Coll. Surg. 2015, 221, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Choudhry, A.J.; Haddad, N.N.; Khasawneh, M.A.; Cullinane, D.C.; Zielinski, M.D. Surgical Fires and Operative Burns: Lessons Learned From a 33-Year Review of Medical Litigation. Am. J. Surg. 2017, 213, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Tucker, R.D. Laparoscopic electrosurgical injuries: Survey results and their implications. Surg. Laparosc. Endosc. 1995, 5, 311–317. [Google Scholar] [PubMed]
- Perantinides, P.G.; Tsarouhas, A.P.; Katzman, V.S. The medicolegal risks of thermal injury during laparoscopic monopolar electrosurgery. J. Healthc. Risk Manag. 1998, 18, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Vilos, G.A.; Rajakumar, C. Electrosurgical generators and monopolar and bipolar electrosurgery. J. Minim. Invasive Gynecol. 2013, 20, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Crossley, B. Exploring Differences between Bipolar and Monopolar Modes on Electrosurgical Units. Biomed. Instrum. Technol. 2019, 53, 152–153. [Google Scholar] [CrossRef] [PubMed]
- Alkatout, I.; Schollmeyer, T.; Hawaldar, N.A.; Sharma, N.; Mettler, L. Principles and safety measures of electrosurgery in laparoscopy. JSLS 2012, 16, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Saaiq, M.; Zaib, S.; Ahmad, S. Electrocautery burns: Experience with three cases and review of literature. Ann. Burns Fire Disasters 2012, 25, 203–206. [Google Scholar] [PubMed]
- Bae, H.S.; Lee, M.Y.; Park, J.U. Intraoperative burn from a grounding pad of electrosurgical device during breast surgery: A CARE-compliant case report. Medicine (Baltimore) 2018, 97, e8370. [Google Scholar] [CrossRef]
- Robinson, T.N.; Barnes, K.S.; Govekar, H.R.; Stiegmann, G.V.; Dunn, C.L.; McGreevy, F.T. Antenna coupling--a novel mechanism of radiofrequency electrosurgery complication: Practical implications. Ann. Surg. 2012, 256, 213–218. [Google Scholar] [CrossRef]
- Townsend, N.T.; Jones, E.L.; Paniccia, A.; Vandervelde, J.; McHenry, J.R.; Robinson, T.N. Antenna coupling explains unintended thermal injury caused by common operating room monitoring devices. Surg. Laparosc. Endosc. Percutan Tech. 2015, 25, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Sanders, S.M.; Krowka, S.; Giacobbe, A.; Bisson, LJ. Third-degree burn from a grounding pad during arthroscopy. Arthroscopy 2009, 25, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- Van Eck, C.F.; Van Meel, T.A.C.; Van den Bekerom, M.P.J.; Zijl, J.A.C.; Kooistra, B. Heat-Related Complications from Radiofrequency and Electrocautery Devices Used in Arthroscopic Surgery: A Systematic Review. Arthrosc. Sports Med. Rehabil. 2021, 3, e605–e613. [Google Scholar] [CrossRef] [PubMed]
- Mundinger, G.S.; Rozen, S.M.; Carson, B.; Greenberg, RS.; Redett, RJ. Case report: Full-thickness forehead burn over indwelling titanium hardware resulting from an aberrant intraoperative electrocautery circuit. Eplasty 2007, 8, e1. [Google Scholar] [PubMed]
- Assiotis, A.; Christofi, T.; Raptis DA, Engledow, A. ; Imber, C.; Huang, A. Diathermy training and usage trends among surgical trainees--will we get our fingers burnt? Surgeon 2009, 7, 132–136. [Google Scholar] [CrossRef] [PubMed]
- McQuail, P.M.; McCartney, B.S.; Baker, J.F.; Kenny, P. Diathermy awareness among surgeons-An analysis in Ireland. Ann. Med. Surg. (Lond) 2016, 12, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Siddaiah-Subramanya, M.; Tiang, K.W.; Nyandowe, M. ; Complications, Implications, and Prevention of Electrosurgical Injuries: Corner Stone of Diathermy Use for Junior Surgical Trainees Surg. J. (N Y) 2017, 3, e148–e153. [Google Scholar] [CrossRef] [PubMed]
- WHO Guidelines for Safe Surgery 2009, Safe Surgery Saves Lives; World Health Organization: Geneva, Switzerland, 2009.
- García-París, J.; Coheña-Jiménez, M.; Montaño-Jiménez, P.; Córdoba-Fernández, A. Implementation of the WHO "Safe Surgery Saves Lives" checklist in a podiatric surgery unit in Spain: A single-center retrospective observational study. Patient Saf. Surg. 2015, 9, 29. [Google Scholar] [CrossRef] [PubMed]
- Link, T. Guidelines in Practice: Electrosurgical Safety. AORN J. 2021, 114, 60–72. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Radiological aspect of foot before of second procedure.

Figure 2.
Postoperative appearance of the medial incision prior to staple removal.

Figure 3.
Appearance of the foot at five days (a) and two weeks postoperatively (b).
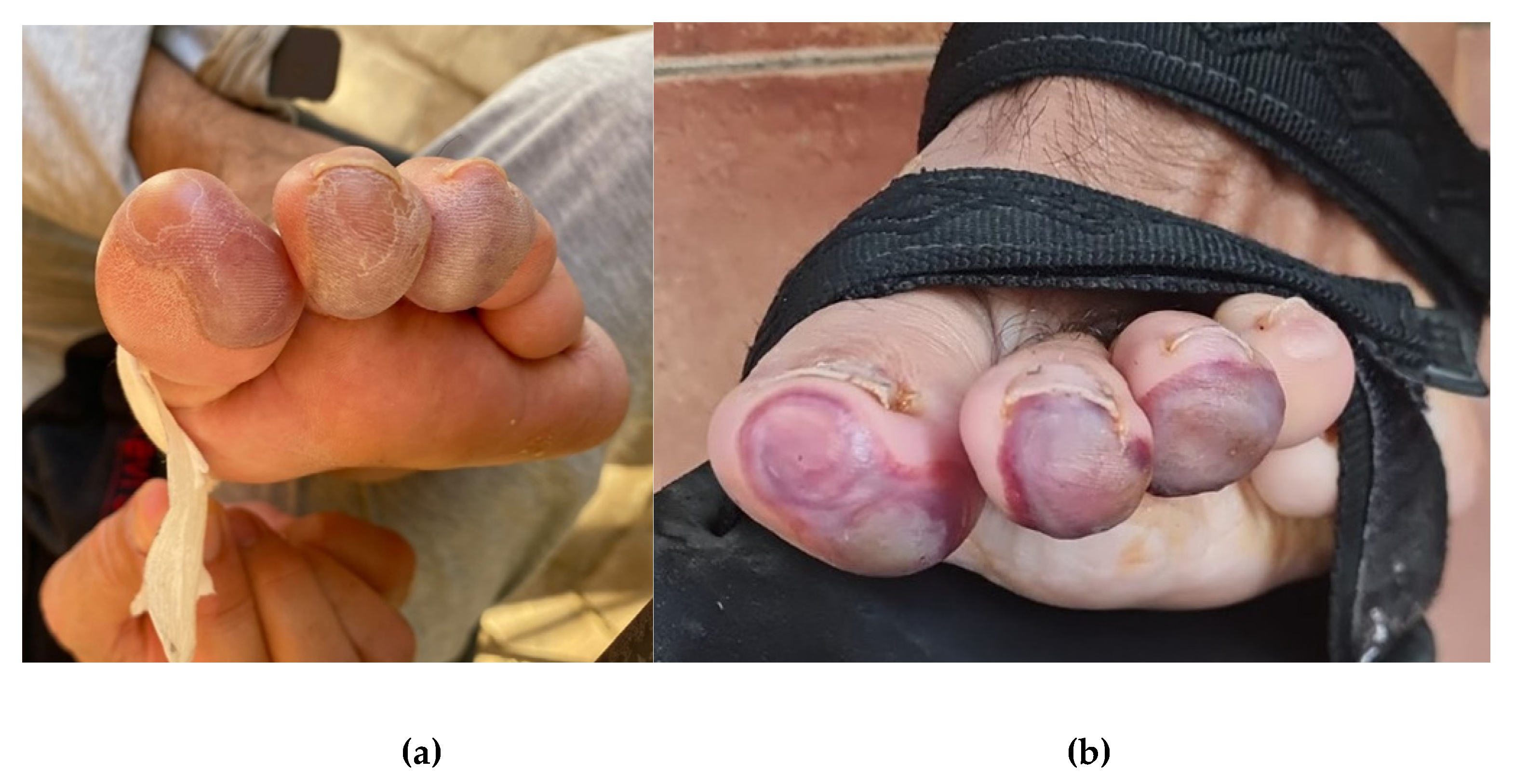
Figure 4.
Rupture and desiccation of the blisters with areas of epidermal necrosis can be observed in the burst injuries after three weeks (a). Aspect after surgical excision of epidermal necrosis areas (b).
Figure 4.
Rupture and desiccation of the blisters with areas of epidermal necrosis can be observed in the burst injuries after three weeks (a). Aspect after surgical excision of epidermal necrosis areas (b).
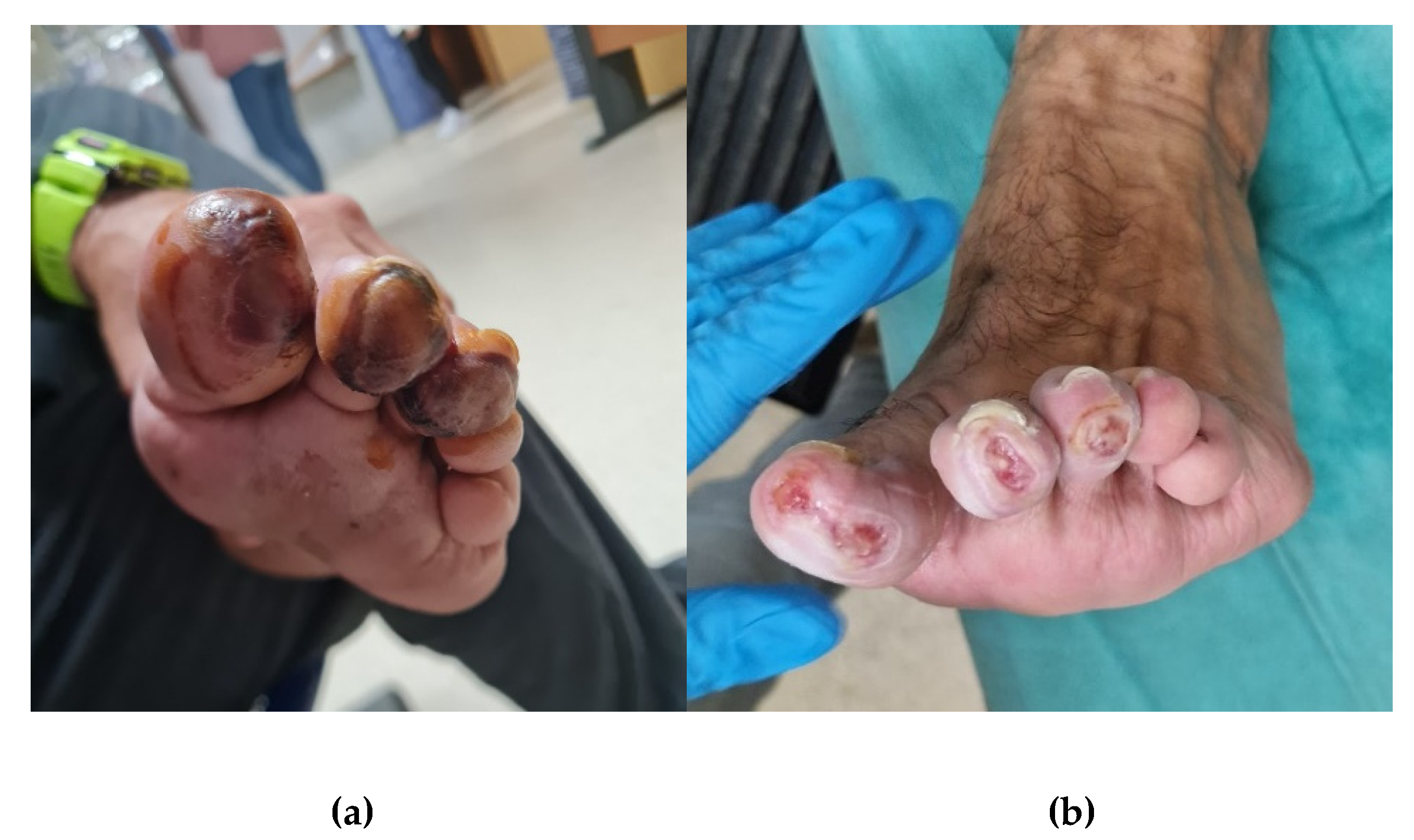
Figure 5.
Postoperative radiography after second surgery. Signs of severe joint destruction compatible with resection arthroplasty.
Figure 5.
Postoperative radiography after second surgery. Signs of severe joint destruction compatible with resection arthroplasty.

Figure 6.
Electrosurgical safety checklist model. Items to evaluate before the use of monopolar diathermy.
Figure 6.
Electrosurgical safety checklist model. Items to evaluate before the use of monopolar diathermy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



