
Submitted:
11 August 2023
Posted:
14 August 2023
You are already at the latest version
Abstract
Spinal deformity refers to a range of disorders that are defined by anomalous curvature of the spine and may be classified as scoliosis, lordosis, or kyphosis. Among these, scoliosis stands out as the most common type of spinal deformity in human beings, and it can be distinguished by abnormal lateral spine curvature accompanied by axial rotation. Accurate identification of spinal deformity is crucial for a person's diagnosis, and numerous assessment methods have been developed by researchers. Therefore, the present study aims to systematically review recent works on spinal deformity as-assessment for scoliosis diagnosis, utilizing image processing techniques. To gather relevant studies, a search strategy was conducted on three electronic databases (Scopus, ScienceDirect, and PubMed) between 2012 and 2022, using specific keywords and focusing on scoliosis cases. A total of 17 papers fully satisfied the established criteria and were extensively evaluated. Despite variations in methodological designs across the studies, all reviewed articles obtained quality ratings higher than satisfactory. Various diagnostic approaches have been employed, including artificial intelligence mechanisms, image processing, and scoliosis diagnosis systems. These approaches have the potential to save time and, more significantly, can reduce the incidence of human error. While all assessment methods have potential in scoliosis diagnosis, they possess several limitations that can be ameliorated in forthcoming studies. Therefore, the findings of this study may serve as guidelines for the development of a more accurate spinal deformity assessment method that can aid medical personnel in the real diagnosis of scoliosis.
Keywords:
spine deformity
; scoliosis diagnostic
; image processing
; medical images
1. Introduction
Three types of spinal deformities-scoliosis, lordosis, and kyphosis- are a set of disorders that are characterized by anomalous spine curvature. A spine is deemed to be in good health where it is perfectly straight in frontal plane whereas it has lordosis in lumbar region and kyphosis in thoracis in sagittal plane. The most prevalent kind of deformity is scoliosis, which is a complicated three-dimensional curvature that unable to view from a single angle [1]. Scoliosis can be categorized into many types hence the most common scoliosis is adolescent idiopathic scoliosis which it can occurs and affecting approximately 2% to 4% of adolescents [2]. Spinal deformity evaluation is a vital stage in deciding treatment since a good diagnosis of scoliosis can result in a better plan of care for the scoliotic patients. Treatment developed for scoliosis followed by diagnosis which depends on the severity of the diseases on the person [3,4,5] such as bracing, surgery, and changes in daily lifestyle.
Scoliosis can be confirmed through clinical examination and specific radiological exam by a key metric that is currently used by the clinicians which is Cobb angle. Clinicians used a protractor to draw two lines that are perpendicular to each other where each line must lie at the most tilted vertebrae [6]. This process was undertaken to calculate the Cobb angle between the superior endplate of the upper extremity curvature and the inferior endplate of the lower extremity of the vertebrae [7]. Even though this measurement is the golden principle for identifying scoliosis, however the measurement’s accuracy can be questionable as it is manually measured by the clinicians which might lead to human error. The measurement also can vary from a clinician to another clinician due to their eye observation of the most curved vertebrae [8,9]. Ferguson angle is an alternative measurement that identifies the three markers of a scoliotic curve: the geometric centers of the upper, apical, and lower vertebrae[1]. Both metrics required medical professionals to manually choose the vertebrae, which might result in bias based on the medical professionals that lead to inaccurate diagnosis. Scoliosis can classify into these two common systems which are angle degrees of the spine’s curve or Lenke Classification but there are many ways can be used to classify this [10]. Ref. [9] stated that the person has no scoliosis if the Cobb angle less than 10 degrees, the person has mild scoliosis if Cobb angle between 10 to 45 degrees and the person has severe scoliosis if the Cobb angle has greater than 45 degrees.
Modern three-dimensional medical imaging offers emerging opportunities and potential in assessing spinal deformities. These opportunities offered by emerging imaging diagnostic equipment, such as computers and software applications, can avoid or lessen the shortcomings highlighted in the past and meeting the demands of the medical community. The current diagnosis of scoliosis can be established by radiographic examination [11] and four imaging modalities that relevant to the diagnosis are; plane radiography (X-rays), computed tomography (CT), magnetic resonance imaging (MRI), and back surface topography (ST) [1]. While CT and MRI could provide detailed images of the spine in three dimensions, radiography can only provide a basic view of the spine in two potential projections—anterior-posterior and lateral. ST is a photogrammetric technique that involves reconstructing the object' forms, sizes, and relative placements. Hence, each modalities have their pros and cons which these can affect the performance of the diagnosis.
In this regard, several researchers have attempting to create novel methods that might enhance the way spinal deformity is currently assessed such as raster stereography, artificial intelligence (AI) scoliosis detection method and many more. Hence, the aim of this systematic review paper is to provide a summary on current and latest spine deformity assessment for scoliosis diagnostic using image processing techniques. It aims to find gaps and valuable perceptions of spine deformity assessment methods that can be helpful for future works.
2. Materials and Methods
The 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standard [12] were followed for this systematic review.
2.1. Eligibility Criteria
This study started with the PICO (Population, Intervention, Comparison, Outcome) strategy as follows: The population interested in this study was on human that encounter spinal deformity diseases especially scoliosis and the intervention of the interest was the assessment method to diagnose the scoliosis utilizing image processing techniques. The outcome of the interest was the effectiveness and how successful of the method in diagnosing scoliosis. Thus, using the PICO technique, relevant studies based on the evaluation method that used image in diagnosing scoliosis may be discovered, allowing for a thorough comprehension of the most recent literature on this subject.
2.2. Search Strategry
Articles search was performed through the electronic databases and was restricted to ten years of publication. Three databases were used to obtain the articles which is Scopus (2012 – 2022), ScienceDirect (2012 – 2022), and PubMed (2012-2022). The following search keywords were used: "spinal deformity", "assessment", "diagnostic," "treatment", and "image" to identify research addressing the assessment and diagnosis of spine deformity using imaging techniques. The Boolean operator “AND” was used in searching the papers. All papers were procured and meticulously reviewed to guarantee that the findings of the database search were significant and connected to other papers. Final articles underwent a rigorous screening process before being selected to ensure that our findings were confined within the research parameters. The literature search via electronic databases included only complete English textual articles. In the titles and abstracts screening process, articles were searched with an emphasis on research methods to assess and diagnose scoliosis deformity. The articles were evaluated using following criteria: (1) Cobb and Ferguson angle, (2) assessment method to diagnose scoliosis using image. The study did not impose any limitations on the subject’s age, gender, BMI, or medical history. Articles authored by the same individual were eliminated to prevent duplication.
2.3. Selection of the Studies
The results of the search were assessed by the two reviewers (N.N.A. and K.S.B.) based on the inclusion criteria. Final articles after screening were obtained and segregated from the duplicate articles in various databases. Titles and abstract of the articles were read thoroughly and a selection was made in accordance with the criteria. A comprehensive analysis of the articles was conducted in instances which during the screening process, the articles disclosed inadequate information in the titles and abstract. The articles that were rejected were rescreened to prevent any unnoticed information.
2.4. Risk-of-Bias Assessment
There is no standardized or validated method to evaluate the credibility of the identified articles. In this paper, the articles were assessed using a systematic quality method to analyze and review them. This method can be instrumental in obtaining the most pertinent and significant information from the articles. Questions were adapted from Kavita et al. [13] and Wen et al. [14] to evaluate the credibility of the articles and several questions were excluded as it failed to justify spine deformity assessment and diagnosis. Some of the questions underwent modifications based on imaging processing method. Each of the questions was valued a score of “2” if it fulfilled the questions whereas a score of “1” if it has lack on detailed information. A score of “0” or “no” was given if there was no information provided and “NA” for questions that are not applicable. The questions are as follows below:
- Has the objective of the study been articulated with clarity?
- Does the study design have a clear and detailed outline?
- Are the subject/data’s characteristics and details presented distinctly?
- Does method used to assess the spinal deformity is clearly defined and described?
- Is it the study involving imaging method to diagnose spine deformity?
- Is parameter measured used in the method clearly described?
- Does it use the appropriate numerical methods in data analysis and clearly verified or validated?
- Is it study has clear outcome?
- Is it the study stated the limitations?
- Does the study have a clear conclusion?
3. Results
3.1. Primary Search Results.
The authors conducted full-text review due to the limited nature of the information provided. Seventeen articles were selected after a meticulous screening procedure and Figure 1 provides the selection procedure of the systematic review of the articles. A total of 1384 articles were obtained following the screening process and 97 of these articles were identified as duplicates and eliminated. Titles and abstract of the articles were reviewed to evaluate the relevancy of the article studies and 983 articles were then eliminated. An additional screening was performed by reading full text of the articles to ascertain the goals of the studies based on the parameters and criteria that were assessed. There were 17 articles retrieved for further review that related and met the criteria after eliminating another 49 articles.
3.2. Analyzed Data Quality.
The quality score of the 17 reviewed articles is presented in Table 1. The reviewed articles exhibit quality scores in the range of 70% to 95%. Those articles’ scores of above 85% are considered good as they satisfactorily answered all the questions which they provided in-depth information regarding their objectives, design study, outcomes, and conclusions. Only 2 out of the 17 papers achieved a score of less than 80% and most of them achieved more than 80%. These findings indicate the reviewed papers are high quality.
3.3. Data Characteristics & Details
Table 2 presents a list of data used from the 17 reviewed articles. The source of data can be categorized into two which are patients and images. Most of the articles use subjects which are patients to obtain images and only four articles [15,16,17,18] use solely readily-images as their dataset. Three studies used private datasets and one paper did not state the source of the dataset. The number of subjects or data participated in the studies varied with the highest being 3240 images and the lowest being 10 patients. Three studies involved a wide range age individual (aged between 11 and 86) [17,19,20] and ten studies focused on adolescents and middle-aged individuals (aged between 10 to 30 years old) [15,21,22,23,24,25,26,27,28,29] while four studies did not provide the age information of the dataset. Fourteen studies provided the required details of the data included in the investigations such as inclusion and exclusion criteria. The other three studies did not provide extensive and clear details on the dataset which lead to bias.
3.4. Assessment Methods for Scoliosis Diagnosis.
The goal of conducting a systematic review is to reduce the likelihood of potential biases by thoroughly searching and examining all published papers. All the characteristics and design study in diagnosing scoliosis such as imaging modality/instrumentation, parameter/landmark evaluated, software or tools used, the assessment mechanism and plane/view used give an influence on accuracy and precision of the study. These variables have an impact on the method that must be considered in evaluation of both the outcomes and inferences. Table 3 presents the variables utilized by the reviewed articles of assessment method of scoliosis diagnosis. These data can help to provide supplementary information by comparing methods on the scoliosis diagnosis studies.
Instrumentation or imaging modality is very crucial in capturing the structure of the spine to obtain good image quality because it affects the accuracy of scoliosis diagnosis. Six out of eighteen studies used common and conventional imaging modality such as X-ray, computed tomography (CT), and ultrasound [15,16,17,25,30,31] while other researchers [18,19,20,21,22,23,24,26,27,28,32] use uncommon instrumentation like rasterstereography, camera, EOS imaging, scanner, and 3D laser profilemeter. Special mention to Sikidar et al. [29] as the study did not collect data as image which it used EMG and GRF data.
The critical aspect of the diagnosis of scoliosis deformities is the parameters or landmark evaluated during the assessment as it utilized as a metric that determines the existence of scoliosis on a person. The gold standard parameter that currents clinicians used is Cobb Angle which [18,24] utilized in their studies. A study [15] provide no evaluated parameter as the study used image processing for the assessment whereas authors constructed new parameter or improvised from the current parameter to evaluate scoliosis. The new parameters used for scoliosis evaluation are vertebrae as landmark [19,21], rasterstereographic measurements [22], COL [25], scolioscan angle [26], DIPA [28], BAI [30], EMG and GRF [29], and 3D scoliosis angle [31].
Three possible approaches have been employed for the assessment method of scoliosis diagnosis where five scholarly articles devoted on artificial intelligence study [15,16,22,24,29], nine articles studies on image processing [17,19,21,23,25,28,30,31] and four articles studied on building a system to diagnose the scoliosis [18,20,26,27]. Digital image processing has become the most common form in the medical field as it is the most efficient and cheapest method. Previous studies have tested the scoliosis assessment by using various image processing techniques including 3D reconstructions of spine and rib cage[21], segmentation and superimposition [23], COL [25] , photogrammetry [28], BAI method [30], automatic analysis and measurement of 3D spine images [17,31]. Studies on artificial intelligence implemented deep learning, machine learning and supervised learning in assessment of scoliosis while computer aided systems including GUI analysis tools, Scolioscan system, ScolioMedIS system, and 3D laser triangulation system were built to identify and recognize the scoliosis.
3.5. Other Variability used in the study.
The outcome and findings of the reviewed articles can be summarized in Table 4. There are two possible approaches that have been used for the investigation of scoliosis where thirteen studies performed their design study quite the same pattern where the patients need to do quite the same procedure for the data collection and acquisition. The patients need to execute the validated posture in front of the instrumentation or imaging modality to obtain the spine images. But this differs from authors [15,16,17,18] where the data acquisition collected from the previous or available data from repository collection.
It can be observed from the articles, scoliosis can be identified from multiple planes’ view which from the frontal, sagittal, lateral, transverse, and anterior posterior plane. Majority of the scholars studied scoliosis deformity using only one view plane which is coronal or frontal plane [15,18,23,25,26,28,30]. While five studies using two plane and four studies using three view planes [17,19,21,24] to assess the scoliosis deformity. The selection of view plane during the scoliosis deformity assessment plays an important role in giving a better view of the spine. Based on the reviewed articles, a variety of statistical significance methods were used to validate the method of the scoliosis assessment, and this can be proven in the findings in Table 4. When classifying scoliosis, artificial intelligence studies [15,22,24,29] obtain the maximum accuracy 90.7 % and the lowest accuracy 50%. While other authors contend that their approach is comparable to and performs better than the one currently employed by clinicians in the diagnosis of scoliosis or existing scoliosis method.
4. Discussion
The purpose of this systematic review study was to evaluate the technique or mechanism for diagnosing scoliosis by examining the characteristics and metrics that are frequently employed in imaging. Analyzing the parameters employed in each inquiry in depth is necessary to comprehend the assessment mechanism. Seventeen publications were considered in the current study for thorough review. Quality evaluation functioned as the primary methodological consideration to address the inconsistent methodological reporting by ensuring that the constraints of the examined research were considered. None of the articles that were assessed received a score below 70%, which was regarded as the acceptable average. The search method used for this review's constraint of solely English-language articles. There were only three databases utilized to search for articles, therefore some articles could have been overlooked. The criteria for identifying scoliosis deformity were restricted to imaging, hence data from any method of scoliosis deformity evaluation beside imaging were excluded from the paper.
Participants' characteristics, parameter/landmark, assessment method, modality, software, and instruments utilized in the research' outcomes may all be further examined in the evaluated articles. Data characteristics were varied, and there was a propensity to group data according to gender, quantity, and details of data (age, inclusion criteria and exclusion criteria), thus it limited the analysis for certain groups in this reviewed paper. The dataset suggested to have broader range of age and not limited to adolescent and young age. This is because scoliosis can happen to all generations. From the details provided of the data used in the studies, most of the data confirmed to have scoliosis diagnosis from the clinicians. Thus, it is proposed to use data that do not have confirmation of scoliosis by the clinicians for variability. As we can see, researchers have established several useful methods for diagnosing scoliosis deformity. Choosing appropriate factors, such as instrumentation, imaging modality, and parameter or landmark evaluation, is crucial to the success of the study.
In this review, most methods focus on two-dimensional or one-dimensional view and just a few used three-dimensional view for their data. Recent study of scoliosis deformity assessment has an interest on three-dimensional view because it gives better and specific view of the spine so that clinicians can grasp accurate diagnosis in scoliosis. Three-dimensional view where it gives image of spine in three position which are frontal, sagittal, and transverse which is far better compared to others because can clearly show the abnormal angle rotation of the scoliosis that cannot be view in frontal plane. One-view plane which is frontal plane suitable for quick early if spinal deformities, but this cannot give specific and accurate about the curve severity and the spine deformities angle. This is quite significant in decision making by the clinicians for the followed-up treatment.
Next, various parameter or landmark evaluation in scoliosis detection had been utilized in their studies. Cobb angle is the most common metric in determining the level of scoliosis that categorized a person has mild, moderate, and severe scoliosis. It is also quite simple and easier for computation for all assessment approaches whether in image processing or artificial intelligence since it is just calculating angle from two point of abnormal spine curvature however this can be implemented in frontal plane only. Next, Scolioscan angle, DIPA and 3D scoliosis angle are the improvement metrics adapted from Cobb angle significantly exerts evaluation in diagnosing because they evaluated in three-dimensional view and has the same diagnosis concept with Cobb angle. Metrics that evaluate the curve severity of spine by utilizing points or coordinates on spine such as BAI and extreme points or 3D coordinate exerts specific diagnosis values in the curvature of spine. Identifying the curvature severity of spine can aid clinicians in planning treatment accurately rather than just categorizing patients into mild, moderate, and severe. Some papers used human anatomical for the evaluation parameters such as vertebrae in thoracic, spinal, and pelvic region, and rasterstereographic measurements which presents the abnormality of spine clearly, but these metrics are quite complex and tedious for diagnosis. This is because they calculate details each of the abnormal measurements and values occurs on the spine. However, GRF and EMG have proven to be effective metric but ability of the metric in detecting scoliosis in real-world scenario is limited since the instrument used for analysis can only be done through experiment in laboratory.
Apparently, three studies use the common imaging modality which is X-ray and two studies use MRI or CT-scan to acquire spine images. MRI or CT-scan set out higher quality image than X-ray, but still radioactivity from both modalities should be considered since X-ray has low radioactive which is safer and cheaper. Clinicians commonly use X-ray imaging for scoliosis detection, and it is particularly suitable for first-time diagnosis or detection of scoliosis in its early stages. Several studies [33,34] have proven that X-ray can be a good modality accompanied with advanced algorithm mechanism in scoliosis diagnosis. Another 11 studies implemented new and atypical modalities in obtaining the spine image which need to consider the cost-effectiveness and image quality obtained when using the modalities. Image quality used is very important as it can affect the outcome of diagnosis thus modalities that can yield high quality image is the best however, other factors such as radioactivity and cost need to be considered for the assessment.
As we can see, it is found that some studies implemented back surface topography techniques in the diagnosis to get the measurements as it can reduce the exposure of radioactivity to humans. Methods in this review that implement this concept are rasterstereography, photogrammetry, 3D reconstructions of spine and rib cage, 3D structure analysis of human torso and triangulation system that integrated back surface analysis and landmark localization. However according to study [35], the author said that back surface topography techniques need to be performed with great precision due to uneven and variability nature of the human’s back anatomy. Parameters use in these notions for scoliosis measurement requires more complex, elaborate and details of human geometry as we can see in the studies [17,19,20,21,22,28,31] and this must be followed by advanced mathematical algorithm or image processing for the analysis. This requires utilization of advanced instruments or tools that are not familiar to medical practitioners and may not stimulate them to use the instruments due to the distinct and complicated procedures[36]. The most current research focuses on scoliosis diagnosis using artificial intelligence and particularly image processing approaches. Image processing involved many steps including acquisition, enhancement, restoration, recognition and segmentation and the steps may engage in the process according to the desired needs and it is the process of converting an image into a digital format and then executing various operations to extract relevant information. Studies that apply artificial intelligence (AI) [15,16,22,24,29,30] to diagnose scoliosis can improve the accuracy and efficiency of the diagnosis outcomes. AI in medicine can analyze complicated algorithms and self-learning that can work in a manner comparable to human brain and it can have several subfields such as machine learning (ML), deep learning (DL), and computer vision[37]. Three studies in this review employ machine learning where it consists of pattern recognition and analysis that can improve with experience from provided datasets. This can be supported with another study [9,38] which machine learning algorithm such as regression linear and support vector machine have successfully detected the scoliosis in early stage. Study [15] diagnose the scoliosis using deep learning as assessment mechanism and the DL algorithms are Faster-RCNN and Resnet which are commonly use in medical [39]. However, this study only classifies the scoliosis according curve severity grading and did not give specific measurements of the abnormality of the spine curve thus, this is not quite suitable and does not help the health professionals to plan treatment since they need specific data regarding the diagnosis. According to numerous studies [39,40,41,42,43], deep learning may be a strong technique with a high reputation in biomedical segmentation, however there are several limitations in terms of execution and process resources in this vertebral segmentation study. Computer vision is a process through which a computer learns and comprehends information and understanding from a sequence of images or videos [18,19,26,27,37] employ this approach. This is the highest-level difficulty since it involved in building autonomous system that can detect, diagnose and process provided data and then analyze them accurately which then portrays the analyzed information to the user. Thus, this gives much help to clinicians and can facilitate their efficiency in diagnosing scoliosis. These approaches have given ease to humans and can reduce human error especially in precise medical diagnosis yet, the complex and challenging journey to successfully utilized these in scoliosis assessment need to take into consideration. However, this conflicted with research that used gait analysis characteristics for the diagnosis, according to author Sikidar et al. [17] which can only be done through experiment in lab only.
Numerous studies compare their proposed scoliosis evaluation approach either to the method currently used by clinicians or existing approaches to demonstrate their method’s validity and achieve better performance of assessment. Since the new assessment methods validated by the authors themselves and there is no validation from the real-world scenario. Thus, there is room for improvement for the validity and reliability of the methods that can provide better indicators as guidance for followed-up treatment, surgical intervention, or assessment. It is quite challenging to compare findings from the reviewed papers since different studies employ various explicit and implicit statistical techniques for the evaluation of their proposed method. A technique to diagnose scoliosis that combines artificial intelligence with image processing research may be suggested, and the lack of research on automatically determining the degree of spinal curvature can be considered for future study.
5. Conclusions
The present study highlights seventeen publications, which were published from 2012 to 2022, pertaining to the assessment of scoliosis deformity. The review specifically centers on the assessment aspect, alongside other variable factors such as imaging modality, plane view, research design or protocol, and parameters evaluated in the detection of scoliosis deformity. The data collected in this paper satisfied the fundamental assessment requirements that could impact the ability to predict outcomes.
First, we found that there are three possible approaches addressed in assessment method of diagnosing scoliosis which are image processing, artificial intelligence and building a diagnosis system and all successfully in diagnosing scoliosis. The studies suggested that the most common approach is image processing assessment mechanism however other approaches are applicable to diagnose scoliosis. Next, all the analyzed studies implement a variety of variables in assessment methods according to their approaches. Since there is growing in development of more advanced scoliosis assessment in this area, therefore new potential assessment methods can be suggested to be implemented into real-practice scenario. Consistent evaluation methods are needed because of the irregularity and inconsistency of the evaluation from reviewed studies for comparison so that can demonstrate the superiority of the assessment methods. To gain a more comprehensive insight into the scoliosis deformity assessment process, various elements linked to scoliosis evaluation could be further explored to enhance and augment knowledge in this area.
Author Contributions
Conceptualization, K.S.B. and A.R.S.; methodology, N.N.H. and K.S.B.; validation, S.N.B. and A.R.S.; investigation, H.Y. and S.N.B.; resources, N.N.H. and N.A.M.; writing—original draft preparation, N.N.H. and N.A.M.; writing—review and editing, K.S.B. and M.F.I.; supervision, K.S.B. and H.Y.; funding acquisition, M.F.I. All authors have read and agreed to the published version of the manuscript.
Funding
The authors extend their appreciation to the King Salman Center For Disability Research for funding this work through Research Group no KSRG-2022-033.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data was created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgement
The authors extend their appreciation to the King Salman Center For Disability Research for funding this work through Research Group no KSRG-2022-033.
Conflicts of Interest
The authors declare no conflict of interest.
References
- C. Adam and G. Dougherty, “Applications of Medical Image Processing in the Diagnosis and Treatment of Spinal Deformity,” 2011, pp. 227–248. [CrossRef]
- “Adolescent Idiopathic Scoliosis: Diagnosis and Management | AAFP.” https://www.aafp.org/pubs/afp/issues/2014/0201/p193.html (accessed Feb. 13, 2023).
- D. Addai, J. Zarkos, and A. J. Bowey, “Current concepts in the diagnosis and management of adolescent idiopathic scoliosis,” Child’s Nervous System, vol. 36, no. 6, pp. 1111–1119, Jun. 2020. [CrossRef]
- J. J. Kelly et al., “Treatment of adolescent idiopathic scoliosis and evaluation of the adolescent patient,” Curr Orthop Pract, vol. 29, no. 5, pp. 424–429, Sep. 2018. [CrossRef]
- J. P. HORNE, R. FLANNERY, and S. USMAN, “Adolescent Idiopathic Scoliosis: Diagnosis and Management,” Am Fam Physician, vol. 89, no. 3, pp. 193–198, Feb. 2014, Accessed: Feb. 13, 2023. [Online]. Available: https://www.aafp.org/pubs/afp/issues/2014/0201/p193.html.
- D. Addai, J. Zarkos, and A. J. Bowey, “Current concepts in the diagnosis and management of adolescent idiopathic scoliosis”. [CrossRef]
- Karpiel, A. Ziębiński, M. Kluszczyński, and D. Feige, “A survey of methods and technologies used for diagnosis of scoliosis,” Sensors, vol. 21, no. 24. MDPI, Dec. 01, 2021. [CrossRef]
- B. Samuvel, V. Thomas, M. G. Mini, and J. Renjith Kumar, “A mask based segmentation algorithm for automatic measurement of Cobb angle from scoliosis x-ray image,” Proceedings - 2012 International Conference on Advances in Computing and Communications, ICACC 2012, pp. 110–113, 2012. [CrossRef]
- P. Shrestha, A. Singh, R. Garg, I. Sarraf, T. R. Mahesh, and G. Sindhu Madhuri, “Early Stage Detection of Scoliosis Using Machine Learning Algorithms; Early Stage Detection of Scoliosis Using Machine Learning Algorithms,” 2021 International Conference on Forensics, Analytics, Big Data, Security (FABS), vol. 1, 2021. [CrossRef]
- D. Ovadia, “Classification of adolescent idiopathic scoliosis (AIS),” J Child Orthop, vol. 7, no. 1, pp. 25–28, Feb. 2013. [CrossRef]
- L. Scaramuzzo, “Special Issue: ‘Spinal Deformity: Diagnosis, Complication and Treatment in Adolescent Patients,’” J Clin Med, vol. 12, no. 2, p. 525, Jan. 2023. [CrossRef]
- D. Moher, A. Liberati, J. Tetzlaff, and D. G. Altman, “METHODS OF SYSTEMATIC REVIEWS AND META-ANALYSIS Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement”. [CrossRef]
- K. Gunasekaran, K. S. Basaruddin, N. A. Muhayudin, and A. R. Sulaiman, “Corrective Mechanism Aftermath Surgical Treatment of Spine Deformity due to Scoliosis: A Systematic Review of Finite Element Studies,” BioMed Research International, vol. 2022. Hindawi Limited, 2022. [CrossRef]
- P. X. Ku, N. A. Abu Osman, and W. A. B. Wan Abas, “Balance control in lower extremity amputees during quiet standing: A systematic review,” Gait and Posture, vol. 39, no. 2. pp. 672–682, Feb. 2014. [CrossRef]
- J. Yang et al., “Development and validation of deep learning algorithms for scoliosis screening using back images,” Commun Biol, vol. 2, no. 1, Dec. 2019. [CrossRef]
- T. Liu et al., “A multi-scale keypoint estimation network with self-supervision for spinal curvature assessment of idiopathic scoliosis from the imperfect dataset,” Artif Intell Med, vol. 125, Mar. 2022. [CrossRef]
- S. Roy, A. T. D. Grünwald, A. Alves-Pinto, and R. Lampe, “Automatic analysis method of 3D images in patients with scoliosis by quantifying asymmetry in transverse contours,” Biocybern Biomed Eng, vol. 40, no. 4, pp. 1486–1498, Oct. 2020. [CrossRef]
- J. Hurtado-Avilés et al., “Validity and Absolute Reliability of the Cobb Angle in Idiopathic Scoliosis with TraumaMeter Software,” Int J Environ Res Public Health, vol. 19, no. 8, Apr. 2022. [CrossRef]
- A. T. D. Grünwald, S. Roy, and R. Lampe, “Scoliosis assessment tools to reduce follow-up X-rays,” J Orthop Translat, vol. 38, pp. 12–22, Jan. 2023. [CrossRef]
- D. Čelan, B. Jesenšek Papež, P. Poredoš, and J. Možina, “Laser triangulation measurements of scoliotic spine curvatures,” Scoliosis, vol. 10, no. 1, Sep. 2015. [CrossRef]
- J. Dubousset, B. Ilharreborde, and J. C. Le Huec, “Use of EOS imaging for the assessment of scoliosis deformities: Application to postoperative 3D quantitative analysis of the trunk,” European Spine Journal, vol. 23, no. SUPPL. 4, 2014. [CrossRef]
- T. Colombo et al., “Supervised and unsupervised learning to classify scoliosis and healthy subjects based on non-invasive rasterstereography analysis,” PLoS One, vol. 16, no. 12 December, Dec. 2021. [CrossRef]
- Y. Yıldırım, K. Tombak, S. Karaşin, İ. Yüksel, A. H. Nur, and U. Ozsoy, “Assessment of the reliability of hand-held surface scanner in the evaluation of adolescent idiopathic scoliosis,” European Spine Journal, vol. 30, no. 7, pp. 1872–1880, Jul. 2021. [CrossRef]
- S. Rothstock, H.-R. Weiss, D. Krueger, and L. Paul, “Clinical classification of scoliosis patients using machine learning and markerless 3D surface trunk data”. [CrossRef]
- Q. Wang, M. Li, E. H. M. Lou, and M. S. Wong, “Reliability and validity study of clinical ultrasound imaging on lateral curvature of adolescent idiopathic scoliosis,” PLoS One, vol. 10, no. 8, Aug. 2015. [CrossRef]
- Y. P. Zheng et al., “A reliability and validity study for Scolioscan: A radiation-free scoliosis assessment system using 3D ultrasound imaging,” Scoliosis Spinal Disord, vol. 11, no. 1, May 2016. [CrossRef]
- V. Luković, S. Ćuković, D. Milošević, and G. Devedžić, “An ontology-based module of the information system ScolioMedIS for 3D digital diagnosis of adolescent scoliosis,” Comput Methods Programs Biomed, vol. 178, pp. 247–263, Sep. 2019. [CrossRef]
- J. R. L. Navarro, C. T. Candotti, T. S. Furlanetto, V. H. Dutra, M. A. do Amaral, and J. F. Loss, “Validation of a Mathematical Procedure for the Cobb Angle Assessment Based on Photogrammetry,” J Chiropr Med, vol. 18, no. 4, pp. 270–277, Dec. 2019. [CrossRef]
- Sikidar, K. E. C. Vidyasagar, M. Gupta, B. Garg, and D. Kalyanasundaram, “Classification of mild and severe adolescent idiopathic scoliosis (AIS) from healthy subjects via a supervised learning model based on electromyogram and ground reaction force data during gait,” Biocybern Biomed Eng, vol. 42, no. 3, pp. 870–887, Jul. 2022. [CrossRef]
- D. Yang et al., “Semi-automatic method for pre-surgery scoliosis classification on X-ray images using Bending Asymmetry Index,” Int J Comput Assist Radiol Surg, vol. 17, no. 12, pp. 2239–2251, Dec. 2022. [CrossRef]
- P. Główka, W. Politarczyk, P. Janusz, Ł. Woźniak, and T. Kotwicki, “The method for measurement of the three-dimensional scoliosis angle from standard radiographs,” BMC Musculoskelet Disord, vol. 21, no. 1, Jul. 2020. [CrossRef]
- Y. shun Wong et al., “Is Radiation-Free Ultrasound Accurate for Quantitative Assessment of Spinal Deformity in Idiopathic Scoliosis (IS): A Detailed Analysis With EOS Radiography on 952 Patients,” Ultrasound Med Biol, vol. 45, no. 11, pp. 2866–2877, Nov. 2019. [CrossRef]
- Saylor, “Artificial Neural Network for the Estimation of Clinical Parameters from X-rays of Scoliotic Spines,” 2020.
- “Vertebra Segmentation for Spinal Deformity Assessment from X-ray Images - ProQuest.” https://www.proquest.com/docview/2570358625/F320EB77D7BE4628PQ/1?accountid=33397 (accessed Feb. 13, 2023).
- B. Drerup, “Rasterstereographic measurement of scoliotic deformity,” Scoliosis, vol. 9, no. 1, pp. 1–14, Dec. 2014. [CrossRef]
- Juliene Rodrigues Leite Navarro, B. Nichele da Rosa, and C. Tarragô Candotti, “Anatomical reference marks, evaluation parameters and reproducibility of surface topography for evaluating the adolescent idiopathic scoliosis: a systematic review with meta-analysis,” 2019. [CrossRef]
- V. Kaul, S. Enslin, and S. A. Gross, “History of artificial intelligence in medicine,” Gastrointest Endosc, vol. 92, no. 4, pp. 807–812, Oct. 2020. [CrossRef]
- K. Chen, X. Zhai, K. Sun, H. Wang, C. Yang, and M. Li, “A narrative review of machine learning as promising revolution in clinical practice of scoliosis,” Ann Transl Med, vol. 9, no. 1, p. 67, 2021. [CrossRef]
- S. Patel, “Deep learning models for image segmentation,” Proceedings of the 2021 8th International Conference on Computing for Sustainable Global Development, INDIACom 2021, pp. 149–154, Mar. 2021. [CrossRef]
- Ronneberger, P. Fischer, and T. Brox, “U-net: Convolutional networks for biomedical image segmentation,” Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics), vol. 9351, pp. 234–241, 2015. [CrossRef]
- Q. Zhang, Y. Du, Z. Wei, H. Liu, X. Yang, and D. Zhao, “Spine Medical Image Segmentation Based on Deep Learning,” 2021. [CrossRef]
- P. Cheng, Y. Yang, H. Yu, and Y. He, “Automatic vertebrae localization and segmentation in CT with a two-stage Dense-U-Net,” Scientific Reports |, vol. 11, p. 22156, 123AD. [CrossRef]
- W. Weng and X. Zhu, “INet: Convolutional Networks for Biomedical Image Segmentation,” IEEE Access, vol. 9, pp. 16591–16603, 2021. [CrossRef]
Figure 1.
PRISMA flowchart for study selection procedure from the reviewed articles.
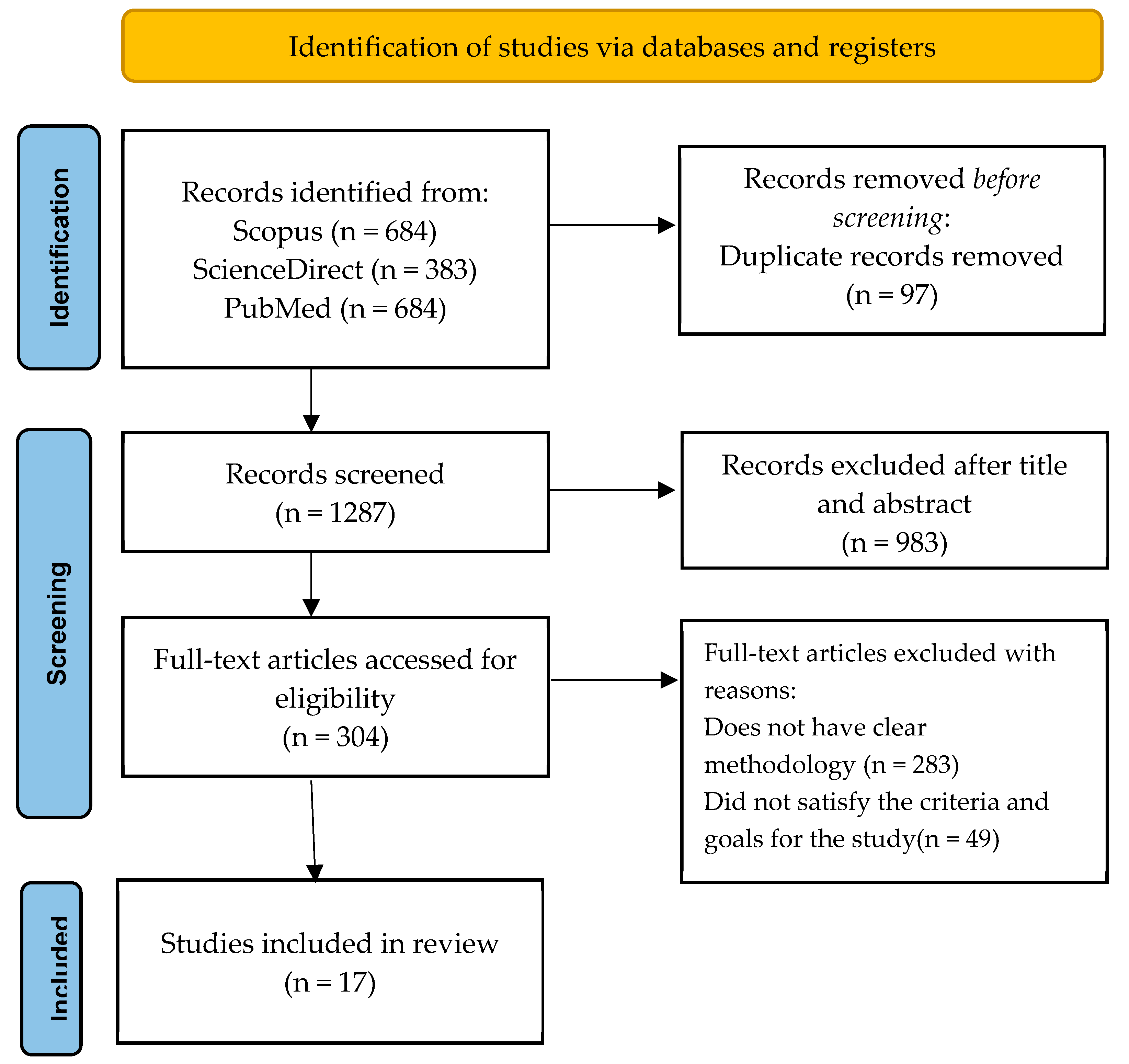

Table 1.
Overall Rating Score of the Reviewed Articles.
| Authors and Year | Questions | Overall Score | Overall (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | ||||
| Dubousset et al. (2014) [21] | 1 | 2 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 1 | 16/20 | 80.0 | |
| Colombo et al. (2021) [22] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 19/20 | 95.0 | |
| Yang et al. (2019) [15] | 2 | 1 | 2 | 2 | 2 | NA | 1 | 2 | 1 | 1 | 14/18 | 77.8 | |
| Yildirim et al. (2021) [23] | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 1 | 0 | 16/20 | 80.0 | |
| Grunwald et al. (2023) [19] | 1 | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 1 | 2 | 16/20 | 80.0 | |
| Rothstock et al. [24] | 2 | 2 | 1 | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 17/20 | 85.0 | |
| Liu et al. (2022) [16] | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 1 | 1 | 17/20 | 85.0 | |
| Wang et al. (2015) [25] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 18/20 | 90.0 | |
| Zheng et al. (2016) [26] | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 2 | 2 | 17/20 | 85.0 | |
| Lukovic et al. (2019) [27] | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 1 | 2 | 17/20 | 85.0 | |
| Navarro et al. (2019) [28] | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 18/20 | 90.0 | |
| Celan et al. (2015) [20] | 2 | 1 | 2 | 2 | 0 | 2 | 2 | 2 | 0 | 1 | 14/20 | 70.0 | |
| Yang et al. (2022) [30] | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 18/20 | 90.0 | |
| Sikidar et al. (2022) [29] | 2 | 2 | 2 | 2 | 0 | 1 | 2 | 2 | 1 | 2 | 16/20 | 80.0 | |
| Roy et al. (2020) [17] | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 17/20 | 85.0 | |
| Hurtado-Aviles et al. (2022) [18] | 2 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 1 | 2 | 17/20 | 85.0 | |
| Glowka et al. (2020) [31] | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 0 | 1 | 16/20 | 80.0 | |
Table 2.
Data’s Characteristics and Details.
| Authors | Source of data | Number Subject/ Data |
Gender | Details of Subject/Data |
|---|---|---|---|---|
| Dubousset et al. [21] | Patients | 49 | Male: 4 Female: 45 |
Age: 13 – 17 years old |
| Colombo et al. [22] | Healthy and scoliotic patients |
298 | Male: 135 Female: 163 |
Inclusion criteria: - Age: 14 – 30 years old Male or female Exclusion criteria: - Clinical background of vertebrae pathological condition of vertebrae whether congenital or acquired. Medical history of vertebral fractures and/or vertebral surgery. Disc protrusion/ hernia in any level of the spine diagnosis. Diagnosis of scoliosis is secondary to neurological, rheumatological and/or congenital conditions. AIS diagnosis through X-rays with Cobb angle greater than 45º. Any neurological and/or rheumatological conditions diagnosis. |
| Yang et al. [15] | Labeled images of unclothed backs and standing posterior-anterior X-ray images of spine or ultrasound images from normal and scoliosis patients |
3240 | Male: 1029 Female: 2211 |
Age: 10 - 20 years old Exclusion criteria: - Subjects exhibit nontrue scoliosis (attributed to pain or by leg discrepancy, amongst other factors). Other spine disorders or abnormalities in the back region (such as soft tissue mass, thoracic cage diseases, etc). |
| Yildirim et al. [23] | Patients | 42 | Male: 10 Female: 32 |
Age: 10 – 20 years old Caucasian ethnic group Exhibits a double spinal curve with convexity towards the right in thoracic region and convexity towards left in lumbar region. Exclusion criteria: - Gap between the umbilicus-medial malleolus and SIAS-medial malleolus on both right and left side must exceeds one centimeter. |
| Grunwald et al. [19] | Patients | 10 | Male: 5 Female: 5 |
Age: 11-50 years old. Show signs of spinal deformation. Able to stand upright without support. |
| Rothstock et al. [24] | Patients | 50 | NM | Age: 12 – 15 years old. Adolescent idiopathic scoliosis patients and are scheduled to have initial bracing to eliminate any potential artefacts from prior treatments or operations. |
| Liu et al. [16] | X-ray images in anterior-posterior (AP) and lateral (LAT) position | 400 images of 200 patients | NM | Height-width ratios of the image ratio from 1.85 to 2.16. Average image resolution is 3560 x 1740 x 3 pixels and resize into 1024 x 512 x 3 pixels. |
| Wang et al. [25] | Patients | 16 | Female: 16 | Inclusion criteria: Adolescent female. Age: 10-18 years. Cobb angle: 10º - 80º. No previous surgical treatments. MRI examination of the entire spine on the study day without the use of a brace. |
| Zheng et al. [26] | Patients | 49 | Male: 15 Female: 34 |
Age: 11 – 23 years. Exclusion criteria: Have metallic implants. BMI higher than 25 kg/m². Cobb angle larger than 50º. |
| Lukovic et al. [27] | Patients | 35 | Male: 15 Female: 20 |
Age: 11 to 18 years. |
| Navarro et al. [28] | Patients | 61 | NM | Age: 7 – 18 years. Eligibility criteria: Doctors requested to conduct a full-spine radiography. Have ability to maintain an upright position independently. Does not undergo surgical procedure in the spinal region. Absence of spina bifida, sixth lumbar vertebra, or fewer than 12 thoracic vertebrae. |
| Celan et al. [20] | Patients | 275 | Male: 129 Female: 146 |
Age: 16 – 82 years. Distributed into 2 groups which are scoliosis group that has been clinically confirmed scoliosis (28 patients) and control group that has been clinically confirmed physiological spinal curvatures (247 patients). |
| Yang et al. [30] | Patients | 30 | Male: 9 Female: 21 |
- |
| Sikidar et al. [29] | Patients | 16 | All female | Inclusion criteria: Age Range: 12–22 years. Cobb angle: (Healthy controls (HC) < 20º, 20º < Mild scoliosis (MS) < 40º, Severe scoliosis (SS) > 40º). Height range: 130 – 170 cm. Weight range: 25 – 65 kg. Exclusion criteria: Has neurodegenerative disorder such as ataxia, dystonia, Parkinson’s, etc. |
| Roy et al. [17] | Computed Tomography (CT) images |
26 | Male: 14 Female: 12 |
Age: 18 to 86 years. |
| Hurtado-Aviles et al. [18] | X-ray images | 21 | NM | Image resolution is 283.46 pixels/mm and printed in dimension of 350 by 430 mm. |
| Glowka et al. [31] | Patients | 41 | NM | Inclusion criteria: Presence of a main curve either in thoracic or lumbar region. Imaging modalities conducted throughout duration of the hospitalization: High quality plain-standing X-rays (PA and lateral) and thoracic and lumbar spine CT scans conducted as part of the preoperative protocol. Exclusion criteria: Scoliosis type other than the idiopathic, a lack of CT or PA and lateral standing X-ray data, and poor-quality X-rays. |
Table 3.
Variables of Scoliosis Deformity Assessment studies.
| Authors | Instrumentation/ Imaging Modality |
Parameters/Landmark Evaluated | Assessment Method of Scoliosis Diagnosis |
Software/ Tools |
|---|---|---|---|---|
| Dubousset et al. [21] | EOS imaging system |
Thoracic: Thoracic volume, mean spinal penetration (SPIm), apical spinal penetration (SPIa) Spinal and Pelvic: T4/T12 kyphosis, L1/S1 lordosis, Cobb angles of different curves; (lumbar, main thoracic, proximal thoracic), apical vertebral rotation (AVR), torsion index of main thoracic curve |
Three-dimensional reconstructions of spine and rib cage from EOS low dose biplanar stereoradiography |
IdefX (version 4.8.4, Arts et Metiers ParisTech) |
| Colombo et al. [22] | Rasterstereography | Rasterstereographic measurements: 40 VRS features including thoracic kyphosis angle, lumbar lordosis angle, lumbar fle´che, cervical fle´che, kyphotic apex |
Supervised and unsupervised machine learning (ML) | Video-Raster-Stereography (VRS), Formetric 4D system |
| Yang et al. [15] | Camera X-ray Ultrasound |
NA | Deep learning algorithms (DLAs): Faster-RCNN and Resnet | MATLAB |
| Yildirim et al. [23] | Hand-held 3D scanner device | Distance, angle, and geometric measurements |
Image processing after 3D scanning (Segmentation and superimposition) and 3D analysis (point to point distance calculation and colored deviation map) |
Artec studio software, Netfabb Basic software, GraphPad Prism software |
| Grunwald et al. [19] | Body scanner system incorporates both an infrared depth sensor and a RGB video camera. |
Thoracic, lumbar, thoraco-lumbar region. |
Graphical user interface (GUI) of body scanner image analysis tools |
Computer Aided Design (CAD), FEBio software |
| Rothstock et al. [24] | 3D depth sensor | Cobb Angle and Augmented Lehnert-Schroth (ALS) |
Machine learning (ML) | Python 3.1, Artec studio software |
| Liu et al. [16] | 2 plane view X-ray | 3D coordinate of spinal curvature |
A multi-scale keypoint estimation network and a self-supervision module |
Pytorch platform on NVIDIA RTX 2080Ti GPU |
| Wang et al. [25] | Ultrasound MRI |
COL | Measurements Center of laminae (COL) |
Custom developed software |
| Zheng et al. [26] | Scolioscan | Scolioscan angle | 3D ultrasound imaging method: Scolioscan system | Scolioscan |
| Lukovic et al. [27] |
Formetric DIERS raster-stereography scanner and Digital photo camera |
Cobb angle and Spinal curvature |
Ontology-based of the information system ScolioMedIS |
MATLAB |
| Navarro et al. [28] | Digital camera (Sony Cybershot DSC-F717, 5.0 megapixels, 512 Mb of memory, 5x optical zoom and 10x digital zoom) and radiography |
Digital Image-based Postural Assessment (DIPA) angle and Cobb angle |
Photogrammetry and radiographic evaluation |
DIPA software and MATLAB v7.9. |
| Celan et al. [20] | 3D laser profilemeter |
Extreme points in the antero-posterior (AP) and left-right (LR) views |
3D laser-triangulation system | NM |
| Yang et al. [30] | X-ray | Bending Asymmetry Index (BAI) | Semi-automatic X-ray based BAI method. 2 stages involved which are manual annotation and adjustment of pelvis level inclination and automatic generation of BAI values. |
NM |
| Sikidar et al. [29] | SMART DX100 | Electromyogram (EMG) and Ground Reaction Force (GRF) | Supervised learning model | Mokka open-source software (Version 0.6.2, 64 bit, Windows, Biomechanical Toolkit) |
| Roy et al. [17] | Computed Tomography (CT) scans |
Circularity, Difference between the areas located on the left and right of the spinous process (LRAsm) and Difference between the ratios of width/depth on each side of the centroid of the contour (ASR). |
Automatic analysis of 3D structure of human torso by quantifying asymmetry in transverse contours. | MATLAB and 3D slicer software |
| Hurtado-Aviles et al. [18] | X-ray | Cobb angle | Computer-aided measurement system | TraumaMeter software |
| Glowka et al. [31] | Computed Tomography and digitally reconstructed radiographs (DRRs) |
3D scoliosis angle | Measurement of the 3D angles between the upper-end vertebra’s upper endplate (three points coordinate) and lower-end vertebra’s lower endplate (three-points coordinate). |
DeVide Software |
* NM- Not mention; NA-Not available.
Table 4.
Data Extraction from reviewed articles.
| Authors | Protocol/Design of study | Plane/View | Outcome Measures |
|---|---|---|---|
| Dubousset et al. [21] | Patients in standing position in less than 15 min to obtain their specific 3D spinal reconstruction with the EOS system. Thoracic parameters were computed, and spinal and pelvic parameters were measured during the reconstructions. |
Axial Frontal Sagittal |
Mean pelvic incidence 54.3º (±14) Rotation of axial pelvic ranged between 2º and 6º Spinal parameters (Mean ± standard deviation) Cobb angle of main thoracic (61.2 ± 13º) AVR (19.9 ± 7º) Torsion index 15.8 ± 6 Proximal thoracic Cobb angle (30 ± 11º) Lumbar Cobb angle (42 ± 11º) T4-T12 kyphosis (18 ± 13º) L1-S1 lordosis (53.7 ± 14º) Thoracic parameters (Mean ± standard deviation) Thoracic volume (5056 mm³ ± 869) SPIa (13.3% ± 1.7) SPIm (8.7% ± 1.2) |
| Colombo et al. [22] | Patients maintain a static stance in an upright posture at a predetermined distance from camera for 6 seconds. Data acquisition (sample of pictures) obtained by Formetric 4D system. Then, data were undergone cleaning and normalization before proceeding to machine learning procedure. |
Frontal Sagittal |
Accuracy for unsupervised classifier ML for full set features achieved 61.7% and minimal set features achieved 72.2%. Accuracy for supervised classifier ML for full set features achieved 87.5% and 86.3%. While accuracy of minimal set features achieved 83.7% and 85.5%. |
| Yang et al. [15] | Subjects need to stand naturally, and for data acquisition conducted using multiple cameras. The patient’s back was captured disrobing above hip. Data collected from 3240 patients with images of labeled back and entire spine standing posterior-anterior X-ray images or ultrasound images which were used for training validation dataset. For external validation, 400 images were used for the process. Both training and external validation were performed for three algorithms which are cases with curve ≥ 10º, cases with curve ≥ 20º and curve severity grading. |
Frontal | Performance of DLAs was measured by accuracy, sensitivity, and specificity which the results as below: - Algorithm 1: Accuracy=75%, Sensitivity=80.67%, Specificity=58% Algorithm 2: Accuracy=87%, Sensitivity=84%, Specificity=90% Algorithm 3: Accuracy=55% |
| Yildirim et al. [23] | Patients’ back surface scanned with 3D hand-held scanner in three distinct positions (P1: stand with arms hanging at the sides, P2: stand with arms extended, P3: bend forward). Patients required to stabilize their body position as much as possible while maintaining normal breathing. Distance patients with scanner adjusted according to the distance indicator in Artec Studio software and 3D surfaces of the patients acquired. |
Frontal | The RMS and Cobb values in the thoracic were observed to have a significant correlation coefficency (r) (P1 = 0.80,P2 = 0.76, P3 = 0.71) and lumbar region (P1 = 0.56, P2 = 0.65, P3 = 0.63); |
| Grunwald et al. [19] | Patients need to maintain static and vertical stance while their arms slightly abducted in front of the scanner. The scanning duration took no more than 10 seconds. |
Coronal Transverse Sagittal |
Correlation coefficients of ρs>0.87 indicates strong correlation between Cobb angle and lateral deviation, between Cobb angle and rotation of the vertebrae. Parameters have potential to offer supplementary information. |
| Rothstock et al. [24] | Patients need to be positioned in vertical stance with their arms slightly extended away laterally from the torso on an electronic tumtable for full torso 360º 3D scanning. Reconstruction of 3D trunk surface was done by 3D software for data acquisition. Data analysis and classification were performed in term radiographic analysis and 3D surface topography. |
Coronal Transverse Sagittal |
Accuracy classification for curve severity = 90%. Accuracy classification for ALS = 50 – 72%. |
| Liu et al. [16] | Data acquisition of 400 full spine radiography images in anterior and lateral views from 200 patients. The dataset image resized and partitioned into two sets, training set (340 images) and validation set (60 images). Conventional augmentation method applied to the dataset. (Add gaussian noise and rotated up to 10 degrees randomly). |
Anterior-posterior and lateral | Average precision, AP= 81.5 AP with regarding both AP and LAT views. Pearson correlation coefficient (ρ) = 0.925. Statistical significance test: p-value = 0.02134. Null hypothesis states that there is no significant difference in the AP between proposed method and the average outcome of the other established method. Requires verification in real-world scenario. |
| Wang et al. [25] | Ultrasound scan was performed with following parameters: a frequency of 2.5MHz, an 18 cm penetration depth, gain 10%. Patients’ backs palpated and marked from C7 to S1 using a water-soluble marker for the scanning process. The patient laying on the scanning couch in supine position and received a total of 6 scans that evaluated by 2 raters which each rater with 3 scans. |
Coronal | Has significant intra- and inter-rater reliability to measure the coronal curvatures. (Both with ICC, (2, K) > 0.9, p < 0.05) There is no significant difference (p<0.05) found of COL method in ultrasound during measurement of coronal curvature at supine position. Bland-Altman method evinced an accord between these two methods, and it was found that Pearson’s correlation coefficient (r) has a high value (r>0.9, p<0.05). |
| Zheng et al. [26] | Subjects stands in front of the Scolioscan according to the locations of the four supporters at the scanner. Subjects scanned using the Scolioscan probe along the screening region. |
Coronal | Scolioscan angle measurement shows a remarkably commendable intra-rater and intra- operator reliability with ICC larger than 0.94 and 0.88 respectively.The angles measurement between Scolioscan angle and Cobb angle provide moderate to string associations with R2 greater than 0.72 for both thoracic and lumbar regions. It was observed that Scolioscan angle tends to slightly underestimate the extent of spinal deformity compared to Cobb angle. |
| Lukovic et al. [27] | System developed with the aid of an ontology – based module that implement four fundamental steps which are specification, conceptualization, formalization and implementation. |
Frontal Sagittal |
The system has capacity to classify spinal curvatures and produce statistical markers about spinal curvatures frequency, degree progression and Lenke classification system. |
| Navarro et al. [28] | Photogrammetry method: Patients subjected to a photographic register in orthostatic posture and has the same position as the radiograph method for the upper and lower limbs. The spinous process of the C7, T2, T4, T6, T8, T10, T12, l2, l4 and S2 vertebrae were marked using double-sided tape on to indicates as reference anatomic landmarks. Radiologic method: Patients assumed in a relaxed orthostatic posture with the trunk pressed against the grid and keep the upper limbs at the side of the body and the feet while radiologist obtained the full-spine radiographs. Inspiratory apnea maintained during the process of the radiograph. |
Coronal for photogrammetry and anteroposterior for radiography |
Thoracic, lumbar, and thoracolumbar scoliotic curve topographies were used to categorise the analyses. All the areas of the spine had high correlations (ranging from 0.72 to 0.81) and significant correlation coefficients (between 0.75 and 0.88). The mean difference was quite near to zero, while the root-mean-square error ranged from 5 to 11 degrees. The area under the curve, which ranged between 95% and 99 percent, was outstanding and noteworthy. |
| Celan et al. [20] | Patients in upright standing position and lean against to a foam affixed to the wall during the measurements. Arms were allowed to hang freely near body while hold their breath. |
Transversal Frontal |
The distances between the extreme points of the spine in the AP view were found to marginally different between the groups (p = 0.1), however the distances between the LR extreme points observed to have a greater significant difference in the scoliosis group compared to the control group (p < 0.001). The quotient LR/AP was determined to be statistically different in both groups (p < 0.001). Thus, this indicates that the method is proficient enough to differentiate between scoliotic and healthy subjects based on statistically differences. |
| Yang et al. [30] | Patients undergone X-ray scanning in three adopted postures which are anterior-posterior (AP) supine, left and right bending. |
Coronal | Between BAI and S-Cobb, the correlation value was R² = 0.730 (p 0.05). Out of 30 patients, 1 case was proven to have be incorrectly diagnosed while using the Lenke classification before and has now been corrected. All scoliotic curve types were correctly identified. |
| Sikidar et al. [29] | Dataset was obtained while the subjects in static pose (standing), and approximately 2 to 6 trials were captured during gait (walking) per subject, contingent on the subject’s level of comfort. Placement of markers adopted from Helen Hayes protocol at sampling frequency of 500 Hz. |
NA | The classification accuracy for SS, MS and HC group was 90.6%. The proposed model has capability detection of AIS in early stages and can be utilized by medical professionals to strategize treatments and remedical measures. |
| Roy et al. [17] | Data collected from the study conducted by the radiology department and underwent analysis of CT images. |
Sagittal Coronal Transverse |
Patients with thoracic scoliosis have larger value for both LRAsm and ASR which the degree of asymmetry was more pronounced in thoracic than in the lumbar region. Lumbar scoliosis patients have smaller value for both LRAsm and ASR which the asymmetry being less pronounced in thoracic than in the lumbar region. Circularity factor does not provide any indications of scoliosis-related asymmetries. |
| Hurtado-Aviles et al. [18] | X ray images collected from a digital image repository. |
Coronal | Utilization of the software TraumaMeter (Mean bias error (MBE) = 1.8º, Standard deviation (SD) = 0.65º) depicts a lower intra- observer measurement error compared to the conventional manual Cobb angle (MBE = 2.31º, SD = 0.83º). The MBE value of the inter-group (expert and novice) distributions differs significantly when using TraumaMeter or the manual method. The use of the software leads to reduction in the difference in error between the novice and expert observers in a statistically significant way. |
| Glowka et al. [31] | The study consists of four steps which are: - 1) 3D scoliosis angle calculation of computed tomography (CT). 2) 3D scoliosis angle calculation of digitally reconstructed radiographs (DRRs). 3) 3D scoliosis angle calculations comparison of CT versus DRRs. 4) Reproducibility and reliability evaluation of the proposed method of X-rays (PA and lateral). |
Posterior- anterior (PA) and lateral |
The 3D-angle measurements obtained with DRRs and CT (p > 0.05) were not significant different. However, a significant difference was found between the 3D-scoliosis angle and the Cobb angle measurements performed based on the X-rays. 3D angle measurements had high reproducibility and reliability value. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



