Submitted:
13 August 2023
Posted:
14 August 2023
You are already at the latest version
Abstract
In recent years, the field of radiotherapy has witnessed remarkable advancements with the integration of artificial intelligence (AI) technologies into clinical practice.
Traditionally, radiotherapy treatment planning has been a labor-intensive process, requiring meticulous manual segmentation and optimization. With the advent of AI, particularly deep learning algorithms, the accuracy and efficiency of target delineation and organ-at-risk segmentation have significantly improved. AI-driven algorithms analyze voluminous medical imaging data, enabling rapid and precise contouring, thus expediting the planning phase and reducing inter-observer variability.
Furthermore, AI's role extends to treatment plan optimization, where it intelligently explores vast parameter spaces to generate optimal plans tailored to individual patients. This not only saves dosimetrists' time but also enhances plan quality by accounting for complex anatomical variations and personalized clinical goals.
In the realm of treatment delivery, AI-powered real-time image guidance enhances the accuracy of patient positioning, ensuring precise radiation targeting. Adaptive radiotherapy, enabled by AI, allows on-the-fly plan modifications in response to anatomical changes, significantly improving treatment accuracy in scenarios like tumor shrinkage or weight loss.
Beyond planning and delivery, AI algorithms contribute to outcome prediction by analyzing historical patient data and treatment responses. This predictive capability aids clinicians in making informed decisions and refining treatment strategies for better prognoses.
Despite the revolutionary potential, challenges remain in seamlessly integrating AI into clinical workflows. Ethical considerations, data privacy, and algorithm interpretability necessitate cautious implementation. Additionally, fostering interdisciplinary collaboration between AI experts and radiation oncologists is imperative to harness the technology's full potential.
This paper explores the impact of AI in four key areas of radiotherapy: automated segmentation, dosimetric and machine quality assurance, adaptive radiation therapy, and clinical outcome prediction.
Keywords:
artificial intelligence
; radiotherapy
; workflow
; accuracy
Introduction
Artificial intelligence (AI) is the simulating of natural human intelligence through the creation and application of algorithms executed in a dynamic computing environment. Its use has extends to various fields, including healthcare, particularly in radiation oncology. The goal is to enhance the speed and accuracy of radiation therapy processing, as well as improve efficiency, safety, and overall treatment quality [1,2].
Indeed, the radiotherapy (RT) workflow is a complex and time-consuming multi- step process that requires coordination among different health professionals with diverse expertise.
In fact , from planning target volume and healthy tissue image segmentation, inverse planning and dose optimization, to adaptive radiation therapy and quality assurance , AI and deep learning methods have an unprecedented impact to revolutionize radiation therapy workflow given the significant dependence of radiotherapy on imaging modalities, digital data processing and advanced software algorithms [3].
Despite agreeing on the effectiveness of AI, using advanced modeling techniques and sophisticated algorithms is usually unintelligible to radiotherapy staff that can be barrier to its integration into clinical practice .Besides, it's important to note that while AI shows promise in radiotherapy, it should always be used in conjunction with clinical expertise and human oversight [4].
The decisions and final responsibility for patient care should ultimately rest with qualified healthcare professionals.
Overall, AI holds great promise in advancing radiation oncology and improving patient outcomes. However, it is crucial to approach its implementation with caution, ensuring that it complements human expertise rather than replacing it entirely. This balance will lead to better patient care and advancements in the field of radiotherapy.
The main focus of our overview is on the AI-based methods that have been either implemented or proposed in Radiotherapy in recent years. The primary objective is to promote a more deliberate and thoughtful adoption of the existing solutions. Simultaneously, we emphasize potential challenges that could hinder their implementation in clinical practice and explore potential strategies to overcome these barriers.
- Automated Segmentation
The main aim of radiation therapy is to safely administer a lethal dose of radiation to the tumor while sparing surrounding healthy tissues.
Accordingly, the most key phase is the delineation of the target volume. It’s the most time-consuming step and requires an even high level of anatomical knowledge leading to significant delays in RT treatment [5].
Currently, in current clinical practice, target volume and OAR contouring is delineated manually for each computed tomography CT slice with low levels of automation and significant inter and intra -observer variability impacting quality of treatment plan optimization [6].
Furthemore, the majority of segmentation algorithms used in clinical settings are atlas-based methods. These algorithms rely on a set of previously labeled reference images and use them to generate segmentations for new target scans.
The atlas-based segmentation process typically involves the following steps:
- -
- Image Registration: The algorithm aligns the reference images (atlases) to the new target scan using image registration techniques. Image registration ensures that the anatomical structures in the atlases are aligned with those in the target scan, even if they have slight differences in position or orientation.
- -
- Atlas Fusion: Once the atlases are aligned with the target scan, the algorithm combines information from multiple atlases to create a fused or probabilistic representation of the segmentation. This fusion step helps to account for inter-subject variability and improves the accuracy of the final segmentation.
- -
- Segmentation Propagation: the fused atlas information is then propagated to the target scan to generate the final segmentation. This propagation can be achieved using various methods, such as deformable registration or label fusion techniques.
While these algorithms have been valuable in automating the segmentation process and providing initial segmentations, they do come with several drawbacks that have hindered their widespread adoption and have limited their effectiveness in certain scenarios :
- -
- Insufficient adaptation to patient variability: Atlas-based methods rely on pre-segmented reference images, which might not adequately represent the variability in anatomy among different patients. This can lead to inaccuracies in segmenting structures, especially when dealing with patients who have unique anatomical variations or postsurgical changes.
- -
- Inadequate handling of local anatomical changes: Tumors or other pathological conditions can cause significant changes to local anatomy. Atlas-based algorithms may not be able to account for these changes appropriately, leading to systematic errors in the segmentations.
- -
- High manual editing requirements: The segmentations generated by atlas-based algorithms often require substantial manual editing by experts to achieve clinically acceptable results. This defeats the purpose of automation and can be time-consuming.
To overcome these problems, auto-contouring (AC) performed by deep learning software as a result of significant advances in computing technique and data accumulation, have been widely integrated into radiotherapy clinical practice to reduce workload pressures, errors and delineation variability between different clinicians, and to expedite the delineation process [7,8] (Figure 1).
These methods can automatically learn to segment structures without the need for explicit atlases. They often require larger amounts of annotated training data but have shown promising results in many medical imaging applications [9].
In recent years, convolutional neural networks (CNNs) have emerged as popular deep learning models for improving segmentation accuracy, with many implementations utilizing U-Nets or V-Nets [10].
Many software products powered by deep learning algorithms are available to automate the contouring process enhancing productivity and enabling clinicians to focus more on critical decision-making aspects of radiotherapy such as MIM SurePlan™ AutoContour, RayStation® Deep Learning Contouring, Mirada RTx AutoContour and VelocityAI AutoSeg.
By analyzing the position and intensity of voxels along with contextual information from surrounding voxels, these models can segment and classify structures in medical images more accurately.
The advantages of deep learning models for medical image segmentation include:
- -
- Automated Feature Learning: Deep learning models can learn hierarchical representations of the data, automatically discovering relevant features for segmentation tasks.
- -
- Higher Accuracy: Deep learning models have shown to outperform traditional methods, especially in complex and challenging segmentation tasks, due to their ability to learn intricate patterns and subtle differences.
- -
- Reduced Manual Intervention: These models reduce the need for extensive manual contouring, saving time and reducing inter-observer variability.
- -
- Generalization: Once trained on a diverse dataset, deep learning models can generalize well to new and unseen data, making them more robust in different clinical scenarios.
- -
- Scalability: Deep learning models can be trained on large datasets, allowing them to benefit from increased data availability and improving performance.
It's important to emphasize that the success of deep learning models in medical image segmentation relies heavily on the availability of high-quality annotated data. Annotated data consists of medical images with corresponding ground truth segmentations created by expert clinicians. The larger and more diverse the annotated dataset, the better the deep learning model can generalize to new and unseen cases.
Head and neck cancers present a unique set of challenges in radiation therapy treatment planning due to the complexity of the anatomy and the necessity to contour numerous organs at risk (OARs) [11].
A recent study evaluated the interest of deep learning (DL) to address these challenges[12]. The authors concluded that DL autosegmentation significantly reduced the time required for head and neck OAR contouring compared to manual segmentation as well as subsequent revisions. The mean time for initial manual contouring was 2.3 hours, while DL autosegmentation took only 0.7 hours, resulting in a 76% reduction in total time. The revision time was also reduced by 35% with DL autosegmentation .
Absolutely, while the AI-powered tools mentioned above have undoubtedly improved the efficiency, accuracy, and consistency of contouring in radiotherapy treatment planning, they are not without challenges. Auto-segmentation algorithms face several obstacles that can affect their performance and reliability:
- -
- Variability in patient anatomy and image acquisition protocols: Each patient's anatomy is unique, and different medical centers may use various imaging protocols. This variability can lead to challenges in training AI models to handle diverse cases effectively.
- -
- Limited research datasets: AI models rely on large and diverse datasets for training, validation, and testing. However, there might be limitations in the availability of comprehensive and well-curated datasets, leading to potential biases or incomplete representations of certain anatomical structures.
- -
- Lack of quality assurance tools: Assessing the accuracy and reliability of AI-generated contours is essential in radiotherapy planning. The absence of standardized and efficient quality assurance tools can make it difficult to validate the accuracy of auto-segmentation results.
- -
- Clinical validation and regulatory hurdles: Incorporating AI tools into clinical practice requires thorough validation and regulatory approval. This process can be time-consuming and complex, slowing down the integration of AI technologies into routine clinical workflows.
Despite these challenges, ongoing research and development in the field of AI and medical imaging are continuously addressing these issues. Advancements in AI algorithms, larger and more diverse datasets, and the development of robust quality assurance tools will likely contribute to further improvements in auto-segmentation accuracy and overall efficiency in radiotherapy treatment planning. It is essential to acknowledge these challenges while continuing to invest in research and innovation to harness the full potential of AI in improving cancer treatment outcomes.
- 2.
- Dosimetric and machine Quality Assurance
Dosimetric and Machine Quality Assurance (QA) play crucial roles in radiation therapy and medical imaging. These processes involve verifying and ensuring the accuracy and safety of radiation delivery and imaging equipment, respectively [13].The implementation of AI in this field has the potential to further enhance the QA processes and improve treatment outcomes.
- -
- Dosimetric Quality Assurance and AI: Dosimetric QA involves verifying the accuracy of radiation dose delivery in radiation therapy. This is essential to ensure that the prescribed dose is accurately delivered to the target area while minimizing radiation exposure to surrounding healthy tissues [14].
AI can play a significant role in dosimetric QA by:
- Treatment Planning: AI algorithms can assist in generating optimized treatment plans by analyzing patient-specific data, tumor characteristics, and radiation delivery constraints. These algorithms can help improve plan quality, reduce planning time, and enhance consistency.
- Dose Calculation: AI can be used to improve the accuracy and efficiency of dose calculation algorithms, ensuring that the delivered dose aligns with the planned dose.
- Treatment Plan Verification: AI can be utilized to verify treatment plans by comparing planned and delivered doses, identifying potential discrepancies, and suggesting necessary adjustments.
- Patient-specific QA: AI can aid in analyzing patient-specific data and historical treatment data to predict potential treatment-related issues or outcomes. This can help personalize treatments for each patient.
- -
- Machine Quality Assurance and AI: Machine QA involves ensuring the proper functioning and calibration of radiation therapy and medical imaging machines. Regular QA checks are necessary to guarantee the accuracy and safety of these devices [15].
AI can be employed in machine QA in the following ways:
- Image Quality Assurance: AI algorithms can be used to analyze medical images, assess image quality, and detect any artifacts or inconsistencies that may affect diagnosis or treatment planning.
- Fault Detection: AI can be integrated into the monitoring systems of radiation therapy machines and imaging devices to detect anomalies or malfunctions in real-time. This early warning system can help prevent potential errors.
- Automated Testing: AI-powered automation can streamline the QA testing process for machines, making it more efficient and reducing the burden on medical physicists and technologists.
- Predictive Maintenance: By analyzing data from the machines, AI can predict when maintenance is required, reducing downtime and optimizing the lifespan of the equipment.
The advantage of AI in this context lies in its ability to handle complex and diverse data types, detect subtle patterns, and predict potential issues with the equipment or treatment process. Additionally, AI models can learn from historical data and adapt to new information, making them potentially more sensitive to rare events or outliers.
To this end, the development of various algorithms enriched by incorporating advanced AI techniques has significantly contributed to improving healthcare processes, particularly in the analysis of large datasets. These algorithms have found applications in optimizing treatment plans, predicting treatment response, enhancing patient-specific quality assurance processes, and identifying patterns and correlations in medical data. Some examples of such algorithms and software tools include Varian AI-Pathway Companion, RayStation, and Radformation ClearCheck [16,17,18].
These algorithms and software tools represent a growing trend in healthcare where AI is exploited to analyze large datasets, extract meaningful insights and optimize various aspects of patient care, including treatment planning, prediction of treatment response, and quality assurance.
By leveraging AI in these areas, radiotherapy QA processes can be enhanced, leading to improved treatment accuracy, safety, and overall quality. However, it is important to ensure rigorous validation, regulatory compliance, and ongoing research to maximize the benefits of AI in radiotherapy QA.
- 3.
- Adaptive radiation therapy:
During a radiation treatment course, anatomical changes, geometrical uncertainties in reproducing the target volume position, and variations in patient positioning can occur over 6-7 weeks. To compensate for these factors, a wide additional margin is often added around the gross tumor volume, resulting in increased radiation dose to healthy tissues [19].
Adaptive radiation therapy offers a solution by allowing daily adjustments to the treatment plan secondary to tumor, morphological and anatomical modifications during treatment courses to more precisely target the tumor, spare normal tissues, and potentially improve the local tumor control and overall survival by enhancing the target coverage [20].
Long awaited for this promise therapy breakthrough , AI and advancements in machine learning have played a crucial role in translating the adaptive radiotherapy from a concept to clinical reality by automating segmentation and recontouring of the daily CBCT images and enhancing deformable image registration to analyze the inter-fractional anatomic changes.
While adaptive radiotherapy has been successfully tested for pelvis and abdomen cancers, ongoing evaluation is being conducted for other treatment sites [21,22].
- Offline: between fractions to address slow progressive anatomical changes during the treatment course caused by weight loss and tumor regression.
- Online: before the fraction to consider for tumors with potentially significant interfractional target and normal structures variations, especially in the abdomen and pelvis radiotherapy.
- Real time: during the treatment of fractions to enhance the accuracy of radiotherapy for moving target suche as lung and liver cancer fundamentally improving safety and efficacy.
The Varian Ethos system is a cutting-edge medical technology developed by Varian Medical Systems. It serves as a self-contained online adaptive solution, meaning it can adapt treatment plans for prostate patients in real-time based on daily anatomical changes observed during treatment [25].
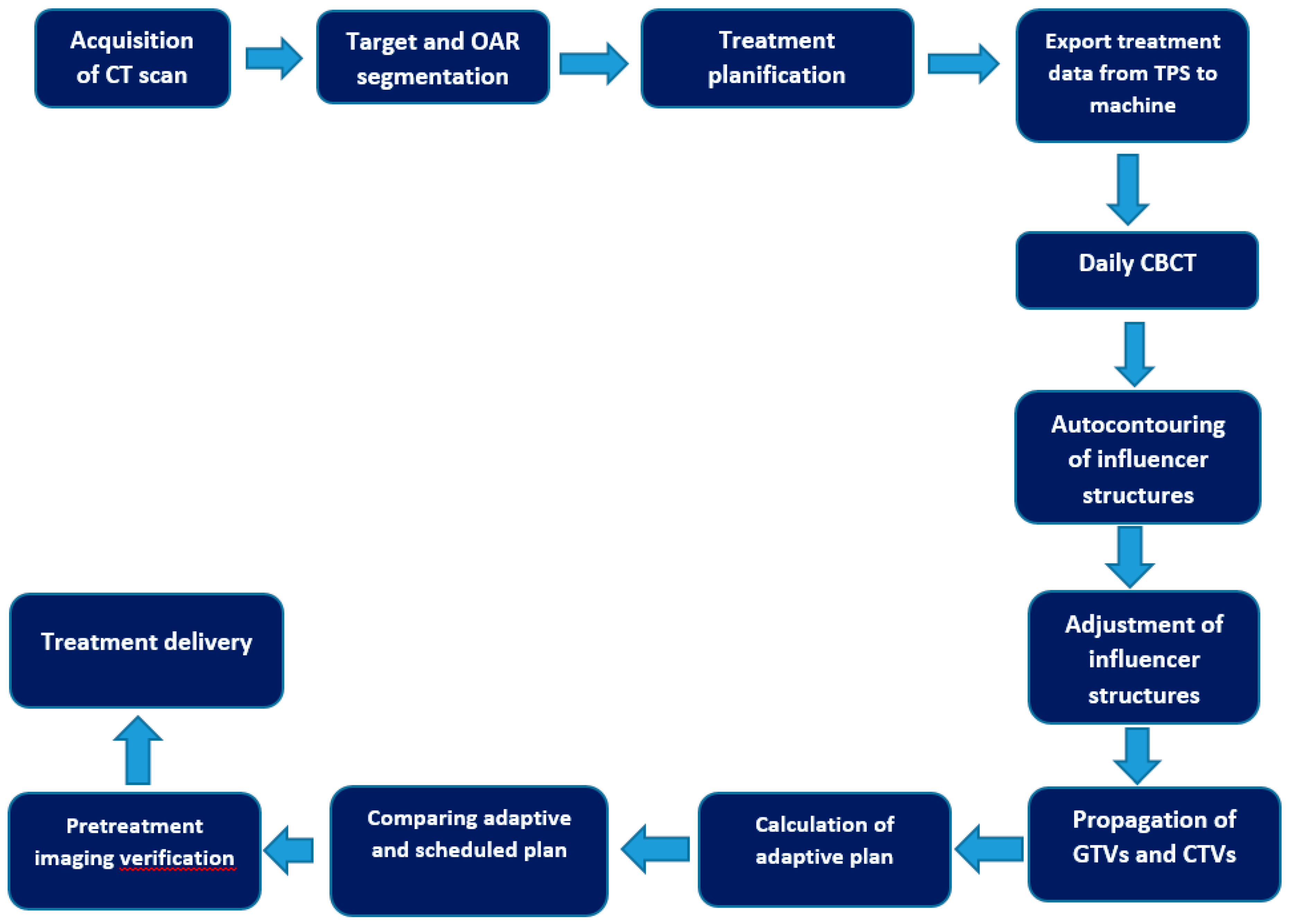
Below is a step-by-step workflow used on Ethos for online adaptive prostate patients [26] (Figure 2):
- -
- Auto-contouring using AI: The process begins with the use of artificial intelligence (AI) to automatically contour or delineate "influencer" structures. These structures are important in guiding the subsequent steps of the adaptive process.
- -
- Adjustment of Influencer Structures: After the AI-generated initial contours, a user (medical professional) can review and make adjustments to these influencer structures if necessary, ensuring their accuracy and relevance for the patient.
- -
- Structure-Guided Deformable Image Registration (DIR): The next step involves creating a deformable image registration (DIR) between the initial planning computed tomography (CT) scan and the acquired cone beam computed tomography (CBCT) scan. This DIR ensures that the images from different time points are aligned correctly.
- -
- Elastic DIR for Mobile and Non-Mobile Regions: Two types of DIR are used based on the nature of the anatomical region being considered. For gross tumor volumes (GTVs) and clinical target volumes (CTVs) that are considered mobile, a structure-guided DIR is utilized. For non-mobile regions, an elastic DIR is employed.
- -
- Propagation of GTVs and CTVs: Using the DIR results, the GTVs and CTVs from the planning CT are propagated or transferred to the CBCT, considering their mobility characteristics.
- -
- Propagation of Non-Influencer OARs and Synthetic CT Generation: Other organs at risk (OARs) that are not part of the influencer structures are propagated using the elastic DIR. Additionally, a synthetic CT is generated by deforming the planning CT into the CBCT geometry. This synthetic CT is used to provide density information for dose calculations in the treatment geometry.
- -
- Validation of Synthetic CT: The accuracy of the synthetic CT is validated on a patient-specific basis by visually checking the agreement between the synthetic CT and the acquired CBCT.
- -
- Generation of Adaptive Plan: A new treatment plan, referred to as the "adaptive plan," is generated based on a predefined "planning directive," optimized to the patient's anatomical changes on that specific day.
- -
- Reference Plan Recalculation: The original treatment plan (reference plan) is recalculated based on the daily anatomical changes observed, and it becomes the "scheduled plan."
- -
- Treatment Plan Selection: The radiation oncologist can choose between the "scheduled plan" and the "adaptive plan" for the treatment session.
- -
- Pre-treatment and Post-treatment QA: The plan selected for treatment receives quality assurance (QA) before treatment using calculation-based QA. After treatment, log file-based QA is performed using Mobius, another Varian Medical Systems product.
In summary, the Varian Ethos system combines AI-driven auto-contouring, deformable image registration, and synthetic CT generation to adapt treatment plans based on daily anatomical changes. The system allows for personalized and precise radiation therapy throughout the treatment course.
- Haut du formulaire
This innovative therapy holds great promise in improving the precision and effectiveness of radiation treatment, ultimately leading to better patient outcomes.
A Study by Ahunbay et al. suggests that using different online adaptive strategies for prostate treatment resulted in improved dose coverage to the PTV while reducing of 13 % of the radiation dose to the rectum which is an important organ-at-risk in prostate radiation therapy [27].
More recently, Sibolt et al. evaluated the clinical implementation of the Ethos system across a range of pelvic sites, including prostate cancer. Eight retrospective prostate plans were included in the study. Analysis of the treatment fractions revealed that in 76% of the fractions, either no edits or only minor edits were needed for the influencer contours .In 88% of the fractions, the adaptive plan was selected. This indicates that the adaptive strategy was applied in the majority of the treatment sessions [28].
While adaptive radiotherapy offers several advantages, there are also some limitations to consider:
- -
- Resource Intensive: Implementing adaptive radiotherapy requires additional specialized equipment and software, as well as a skilled and experienced team to perform frequent imaging and replanning. This can lead to increased costs and a higher demand on department resources.
- -
- Time-consuming: The process of acquiring new images, analyzing them, and creating a revised treatment plan takes time. This can potentially prolong the overall treatment time, which may not be ideal for some patients.
- -
- Radiation exposure: The process of acquiring additional imaging for replanning may expose the patient to extra radiation, though modern imaging techniques aim to minimize this additional dose.
- -
- Limited Changes during Treatment: While adaptive radiotherapy allows for some modification during the treatment course, there are still limitations to what can be achieved. Major anatomical changes, such as significant tumor shrinkage or patient weight loss, may be challenging to address fully with adaptive planning alone.
- -
- Clinical Evidence and Guidelines: Although adaptive radiotherapy shows promise, the evidence supporting its benefits is still evolving. There may be varying protocols and guidelines for its use across different treatment centers.
- -
- Patient Selection: Not all patients may benefit from adaptive radiotherapy. The decision to use this technique depends on various factors, including the type and location of the tumor, the stage of the disease, and the overall health of the patient.Haut du formulaire
- 4.
- Clinical outcome Prediction
Traditionally, outcome prediction models (OPMs) in radiotherapy have relied on factors such as tumor control probability, normal tissue complication probability and the linear quadratic (LQ) model to predict tumor radiosensitivity [29].
However, numerous other factors are involved in the outcome and radio-sensitibility prediction such as tumor heterogeneity, radiation dose, and exposure volume, and hypoxia, ability to repair damage, cell cycle position, and age at radiation, collagen disease and lifestyle [30].
Indeed, the integration of advanced big-data analytics and multi omics information has shown great potential in improving radiotherapy outcomes. The field of radiomics, which involves extracting quantitative features from medical images such as positron emission tomography (PET) scans, has gained prominence in recent years. By analyzing a large number of radiomic features from PET images, machine learning algorithms can help predict treatment responses and toxicity more accurately.
Furthermore, the inclusion of various types of omics data, such as cytokines, gene expression microarrays, and RNA sequencing, allows for a more comprehensive understanding of the molecular and genetic characteristics of tumors [31]. Integrating this information with radiomics data enables a more holistic approach to personalized medicine.
The key advantages of using big-data analytics and multi omics integration in radiotherapy include:
- -
- Precision Medicine: The ability to analyze a patient's specific tumor characteristics at a molecular level can lead to personalized treatment plans that are tailored to their unique genetic makeup, improving treatment efficacy and reducing side effects.
- -
- Predictive Models: Machine learning algorithms trained on large datasets can identify patterns and relationships between various omics data and treatment outcomes. These predictive models can help clinicians make more informed decisions about the best course of treatment for individual patients.
- -
- Early Detection of Treatment Response: By continuously monitoring omics data during treatment, it becomes possible to detect early signs of radiotherapy response or resistance. This early detection can allow for timely adjustments to the treatment plan to optimize outcomes.
- -
- Toxicity Prediction and Mitigation: Understanding the complex interactions among different omics data can also help predict and mitigate potential treatment-related side effects, improving patients' quality of life during and after radiotherapy.
- -
- Research and Drug Development: The analysis of big data in radiotherapy can also contribute to research and the development of new therapeutic strategies and drug targets
Several proposed deep learning models were evaluated for different tumor sites such as head and neck and lung cancers and showed higher sensitivity to predict the severity of acute dysphagia, xerostomia, oral mucositis ,radiation induced pneumonitis and oesophagitis after radiation exposure in comparison to traditional radiosensitivity parameters [32].
A recent retrospective study demonstrates the successful application of AI algorithms trained on clinical data from electronic medical records to predict the risk of acute toxicities in patients undergoing radiotherapy or chemoradiotherapy. The study achieved a sensitivity of 81.0% and specificity of 67.3% using the best-performing gradient tree-boosting method [33].
Nevertheless, the use in radiotherapy prognostic modeling is still limited with relatively few published papers over the last few years. Continued research and validation are necessary to further explore the potential of these advanced models and their integration into clinical practice for improved prognostic predictions in radiotherapy.
Conclusion
Artificial intelligence has made tremendous strides in impacting radiotherapy. While AI tools have significantly enhanced the efficiency, accuracy, and overall quality of radiotherapy, it is important to note the role of human validation and expertise remains crucial in ensuring the accuracy and reliability of AI-generated results.
Despite the promising potential of AI in radiotherapy, challenges remain. As mentioned earlier, one significant challenge is the need to ensure that AI algorithms and models are understandable and interpretable to healthcare professionals. Transparency in AI's decision-making process is essential to gain trust and acceptance among clinicians.
Moreover, robust validation and integration of AI systems into existing clinical workflows are critical to ensure their safety and efficacy. Patient data privacy and security must also be carefully addressed to comply with regulatory standards and maintain patient confidentiality.
In conclusion, AI has the capacity to revolutionize radiotherapy by improving treatment planning, delivery, and monitoring processes. While it offers exciting opportunities, its successful integration requires a collaborative effort between AI experts and healthcare professionals to ensure that it complements clinical expertise and ultimately benefits patients.
Author Contributions
Conceptualization, F.K and H.E. original draft preparation, F.K, H.E,Z.D; writing—review and editing, F.K.; supervision, Z.D. All authors have read and agreed to the published version of the manuscript. Funding: This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Haug, C.J.; Drazen, J.M. Artificial Intelligence and Machine Learning in Clinical Medicine, 2023. N Engl J Med. 2023, 388, 1201-1208. [CrossRef]
- Aung, Y.Y.M.; Wong, D.C.S.; Ting, D.S.W. The promise of artificial intelligence: a review of the opportunities and challenges of artificial intelligence in healthcare. Br Med Bull. 2021, 139, 4-15. [CrossRef]
- Huynh, E.; Hosny, A.; Guthier, C.; et al. Artificial intelligence in radiation oncology. Nat Rev Clin Oncol 2020, 17, 771–781. [CrossRef]
- Deborah Richards, Paul Formosa, Sarah Bankins, et al. Medical AI and human dignity: Contrasting perceptions of human and artificially intelligent (AI) decision making in diagnostic and medical resource allocation contexts. Computers in Human Behavior Volume 133, August 2022, 107296. [CrossRef]
- Mercieca, S.; Belderbos, J.S.A.; van Herk, M. Challenges in the target volume definition of lung cancer radiotherapy. Transl Lung Cancer Res. 2021, 10, 1983-1998. [CrossRef]
- Wong, J.; Fong, A.; McVicar, N.; et al.Comparing deep learning-based auto-segmentation of organs at risk and clinical target volumes to expert inter-observer variability in radiotherapy planning. Radiother Oncol. 2020, 144, 152-158. [CrossRef]
- Harrison, K.; Pullen, H.; Welsh, C.; et al. Machine Learning for Auto-Segmentation in Radiotherapy Planning. Clin Oncol (R Coll Radiol). 2022, 34, 74-88. [CrossRef]
- Sherer, M.V.; Lin, D.; Elguindi, S.; et al. Metrics to evaluate the performance of auto-segmentation for radiation treatment planning: A critical review. Radiother Oncol. 2021, 160, 185-191. [CrossRef]
- Hobbis, D.; Yu, N.Y.; Mund, K.W.; et al. First Report On Physician Assessment and Clinical Acceptability of Custom-Retrained Artificial Intelligence Models for Clinical Target Volume and Organs-at-Risk Auto-Delineation for Postprostatectomy Patients. Pract Radiat Oncol. 2023, 13, 351-362. [CrossRef]
- Sakashita, N.; Shirai, K.; Ueda, Y.; et al. Convolutional neural network-based automatic liver delineation on contrast-enhanced and non-contrast-enhanced CT images for radiotherapy planning. Rep Pract Oncol Radiother. 2020, 25, 981-986. [CrossRef]
- Peng Y-l Chen, L.; Shen, G.-z.; et al. Interobserver variations in the delineation of target volumes and organs at risk and their impact on dose distribution in intensity-modulated radiation therapy for nasopharyngeal carcinoma. Oral Oncol 2018, 82, 1–7. [CrossRef]
- Lucido, J.J.; DeWees, T.A.; Leavitt, T.R.; et al. Validation of clinical acceptability of deep-learning-based automated segmentation of organs-at-risk for head-and-neck radiotherapy treatment planning. Front Oncol. 2023, 13, 1137803. [CrossRef]
- 13. Maria F. Chan,Alon Witztum, and Gilmer Valdes. Integration of AI and Machine Learning in Radiotherapy QA. Front. Artif. Intell., 29 September 2020.
- El Naqa, I.; Irrer, J.; Ritter, T.; et al. Machine learning for automated quality assurance in radiotherapy: a proof of principle using EPID data description. Med. Phys. 46, 1914–1921. [CrossRef]
- Tucker JNethertona b Carlos, E. et al. The Emergence of Artificial Intelligence within Radiation Oncology Treatment Planning. Oncology 2021, 99, 124–134 125. [CrossRef]
- Henkel, M.; Horn, T.; Leboutte, F.; et al. Initial experience with AI Pathway Companion: Evaluation of dashboard-enhanced clinical decision making in prostate cancer screening. PLoS One 2022, 17, e0271183. [CrossRef]
- RayStation: External beam treatment planning system. Medical Dosimetry 2018, 43, 168-176. [CrossRef]
- Pokharel S, Pacheco A, Tanner S. Assessment of efficacy in automated plan generation for Varian Ethos intelligent optimization engine. J Appl Clin Med Phys. 2022, 23, e13539. [CrossRef]
- van der Horst, A.; Houweling, A.C.; van Tienhoven, G.; et al. Dosimetric effects of anatomical changes during fractionated photon radiation therapy in pancreatic cancer patients. J Appl Clin Med Phys. 2017, 18, 142-151. [CrossRef]
- Sonke, J.J.; Aznar, M.; Rasch, C. Adaptive Radiotherapy for Anatomical Changes. Semin Radiat Oncol. 2019, 29, 245-25. [CrossRef]
- Shelley, C.E.; Barraclough, L.H.; Nelder, C.L.; et al. Adaptive Radiotherapy in the Management of Cervical Cancer: Review of Strategies and Clinical Implementation. Clin Oncol (R Coll Radiol) 2021, 33, 579-590. [CrossRef]
- Åström, L.M.; Behrens, C.P.; Calmels, L. ; et al. Online adaptive radiotherapy of urinary bladder cancer with full re-optimization to the anatomy of the day: Initial experience and dosimetric benefits. Radiother Oncol. 2022, 171, 37-42. [CrossRef]
- Weppler, S.; Quon, H.; Banerjee, R.; et al. Framework for the quantitative assessment of adaptive radiation therapy protocols. J Appl Clin Med Phys. 2018, 19, 26-34. [CrossRef]
- Green, O.L.; Henke, L.E.; Hugo, G.D. Practical Clinical Workflows for Online and Offline Adaptive Radiation Therapy. Semin Radiat Oncol. 2019, 29, 219-227. [CrossRef]
- 25. Hu, Y.; Byrne, M.; Archibald-Heeren, B.; et al. Validation of the preconfigured Varian Ethos Acuros XB Beam Model for treatment planning dose calculations: A dosimetric study. J Appl Clin Med Phys 2020, 21, 27-42. [CrossRef]
- Byrne, M.; Archibald-Heeren, B.; Hu, Y.T.; et al.Varian ethos online adaptive radiotherapy for prostate cancer: Early results of contouring accuracy, treatment plan quality, and treatment time. J Appl Clin Med Phys. 2022, 23, e13479. [CrossRef]
- Ahunbay, E.E.; Peng, C.; Holmes, S.; et al. Online adaptive replanning method for prostate radiotherapy. Int J Radiat Oncol Biol Phys. 2010, 77, 1561-1572.
- Sibolt, P.; Andersson, L.M.; Calmels, L.; et al. Clinical implementation of artificial intelligence-driven cone-beam computed tomography-guided online adaptive radiotherapy in the pelvic region. Phys Imaging Radiat Oncol. 2021, 17, 1-7.
- Niraula, D.; Cui, S.; Pakela, J.; et al. Current status and future developments in predicting outcomes in radiation oncology. Br J Radiol. 2022, 95, 20220239. [CrossRef]
- Lambin, P.; van Stiphout, R.G.; Starmans, M.H.; et al. Predicting outcomes in radiation oncology--multifactorial decision support systems. Nat Rev Clin Oncol. 2013, 10, 27-40. [CrossRef]
- El Naqa, I.; Kerns, S.L.; Coates, J.; et al. Radiogenomics and radiotherapy response modeling. Phys Med Biol. 2017, 62, R179-R206. [CrossRef]
- Alkhadar, H.; Macluskey, M.; White, S.; et al. Comparison of machine learning algorithms for the prediction of five-year survival in oral squamous cell carcinoma. J Oral Pathol Med. 2021, 50, 378–84.
- Isaksson, L.J.; Pepa, M.; Zaffaroni, M.; et al. Machine Learning-Based Models for Prediction of Toxicity Outcomes in Radiotherapy. Front. Oncol. 10, 790. [CrossRef]
Figure 1.
Applications of artificial intelligence in the radiation therapy workflow.
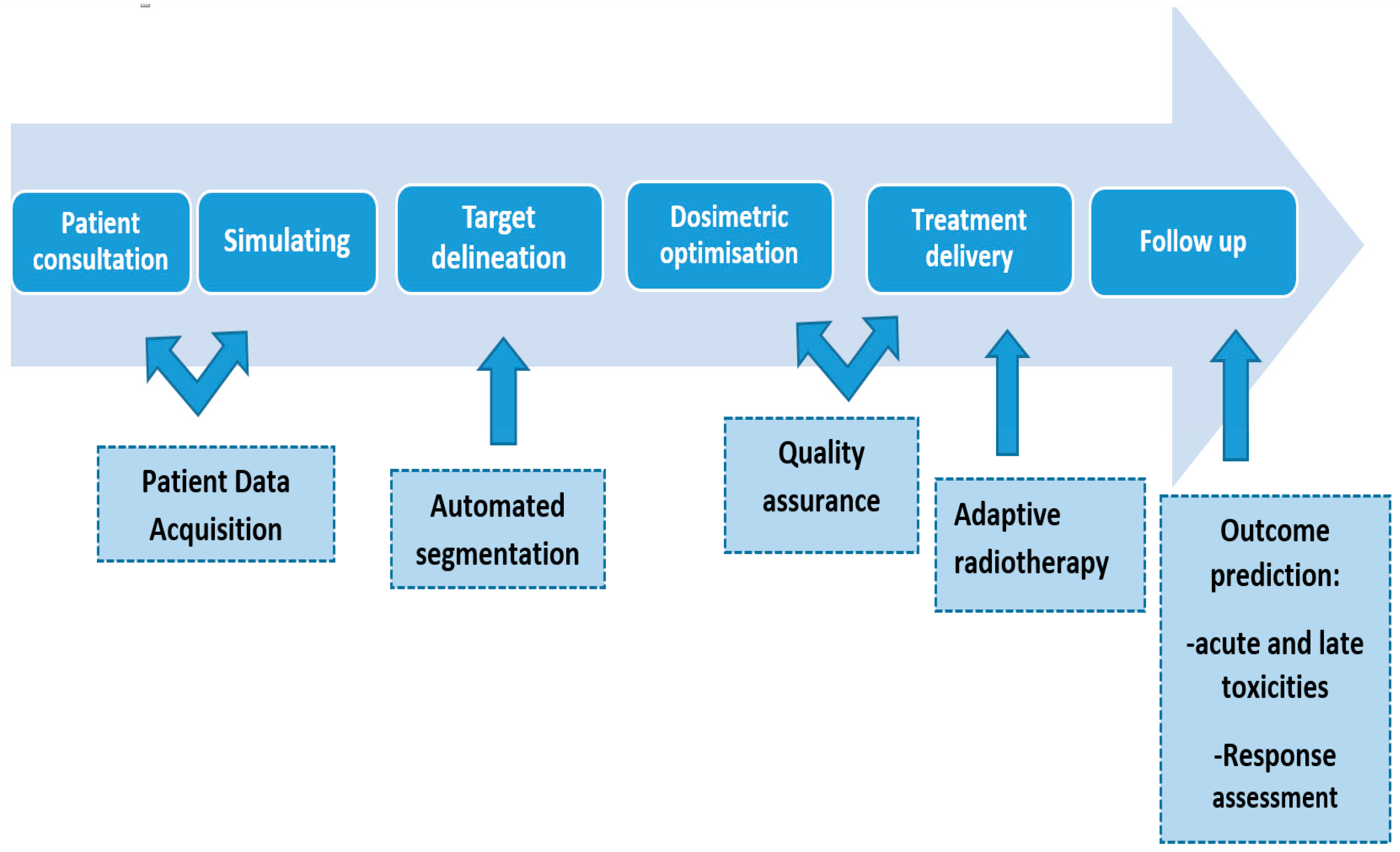
Figure 2.
Main steps of online adaptive radiotherapy workflow .
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



