Submitted:
12 August 2023
Posted:
14 August 2023
You are already at the latest version
Abstract
To this day, use of oily eye drops and non-invasive retinal delivery remains a major challenge. Oily eye drops usually cause ocular irritation and interfere with normal function of the eye, while ocular injections for retinal drug delivery cause significant adverse effects and a high burden on the healthcare system. Here the authors report a novel topical Non-Invasive Ocular Delivery Platform (NIODP) through the periorbital skin for high efficiency anterior and posterior ocular delivery in a non-human primate model (NHP). A single dose of about 7mg JV-MD2 (omega-3 DHA) via the NIODP reached the retina at Cmax of 111µg/g and the cornea at Cmax of 66µg/g. NIODP also delivered JV-DE1, an anti-inflammatory agent in development for dry eye diseases, as efficiently as eye drops did to anterior segments of NHP. The topical NIODP seems to transport drug candidates through the cornea pathway to the anterior and via the conjunctiva/sclera pathway to the posterior segments of the eye. The novel NIODP method has the potential to reshape the landscape of ocular drug delivery, especially for oily eye drops and retinal delivery, where the success of treatment lies in the ocular tolerability and bioavailability of drugs in the target tissue.
Keywords:
Age-related Macular Degeneration (AMD)
; Cornea
; docosahexaenoic acid (DHA)
; drug delivery
; non-invasive ocular delivery platform (NIODP)
; ocular disease
; omega-3
; retina
; retinal delivery
; retinal dis
1. Introduction
Tolerability and suitability issues can limit the use of various materials or delivery routes for ocular drug administration, particularly for oily eye drop and retinal drug. While eye drops are very often used to treat ocular surface diseases, intravitreal injection or implant is mainly used to treat posterior ocular diseases. Since Vitravene® (fomivirsen sodium) became the first FDA approved intravitreally injected therapeutic agent in 1998, the ophthalmic pharmaceutical industry is in urgent need of a breakthrough in ocular drug delivery.
Topical eye drop administration is well known for its capacity to provide necessary and efficient pharmaceutically effective doses to most anterior ocular tissues, usually with higher local drug levels than oral administration and minimal systemic exposure and side effects [1,2]. While most active pharmaceutical ingredients are lipophilic, commercialized eye drops are often in a more ocularly tolerable aqueous formulation, which may be subjected to fast elimination by tears compared to an oily formulation. Eye drops containing castor oil vehicle have been found to cause corneal toxicity, which is not observed with the use of Aleurites, camelina, maize, and olive oils, suggesting that oil formulation may still be useful as ophthalmic formulations [2]. Although oily eye drop formulations may increase solubility and pharmacologic effects of the drug, they often cause ocular discomfort, such as vision blurring and foreign body sensation, due to high viscosity and refractive index of oily contents [2,3]. This is the main limiting factor for their use as eyedrop formulation.
Drug delivery to posterior segments of the eye is a major challenge due to the complex anatomy and dynamic physiological barrier that significantly affects availability of treatments. The physicochemical properties of drugs, formulations, delivery systems, and routes of administration are major factors affecting intraocular bioavailability and have been explored for effective ocular drug delivery [4]. Oral administration and eye drops are the two currently available non-invasive routes of delivery to treat ocular diseases. Due to blood-retina barrier, retinal bioavailability of drugs via oral administration is extremely low, and with very high unnecessary systemic exposure. In individual baboon neonates, it was demonstrated that absorption of DHA to retina from blood circulation reached a plateau when DHA in plasma or red blood cell (RBC) was approximately 6% weight of total fatty acids in the diet [5], therefore DHA in dietary supplement beyond a certain limit may not be absorbed into the retina. Also, the diet to RBC delivery of DHA in baboon neonates was mostly between 0.013% to 0.04% of dosed DHA, while the correlated diet to retina DHA delivery was in the range of 0.0003% to 0.001% [6]. Topical eye drops, a more direct route with lower systemic exposure, for posterior segment delivery have also been very inefficient. Only < 3% of the dosed drug amount reached the aqueous humor, and 0.001% or less reached the retina [7,8]. So, for the retinal delivery of DHA, the oral route would require mega systemic exposure, and oily eye drops would cause intolerable ocular adverse effects, both are very inefficient.
While orally administered drug reaches the retina through the blood circulation, topical eye drop is believed to channel the drug to the posterior ocular segments via two possible routes: (1) the cornea route, where a drug penetrates corneal surface, and continues to diffuse through anterior ocular tissues (aqueous humor, lens/iris/ciliary body), to vitreous humor, and then may reach the retina; and (2) the conjunctiva/sclera route, where a drug diffuses from conjunctiva of the ocular surface, through the scleral water channels/pores to reach the retina [7,9]. The concentration gradient of dissolved drug is the driving force for molecules to permeate through the lipophilic membrane barriers of the eye (i.e. conjunctiva and/or cornea), along the cornea and sclera pathways [7,10]. For a drug with favorable physicochemical properties (e.g. molecular weight, radius, charge and lipophilicity), the sclera pathway provides a bypass of the anterior segment barriers (the lens, iris, and ciliary body), allowing drug permeation to the back of the eye [11,12].
Although many rabbit and rodent studies claimed successful retinal delivery by applying high dose of small molecules or proteins in eye drop formulations, successful translation to larger species or clinical success has not yet been accomplished and topical eye drops for posterior segment delivery remain very inefficient [13,14,15]. In those rabbit and rodent studies, the amount of therapeutic agents reaching the retina were mostly in the range of 0.01 to 0.1µg/g concentration following a typical eye drop regimen [13,16,17,18,19], of which systemic exposure cannot be ruled out because of the small body volume of those animal models. Therefore, rabbit and rodent models may not be appropriate for studies of posterior segment drug delivery [13].
The current standard of care for retinal drug delivery is intravitreal injection or implant [20], and the efforts in improving retinal drug delivery are heavily focused on two aspects. The first is the slow released, long-acting ocular drug formulations /implants for macromolecules (such as anti-VEGF) or steroids to increase efficiency of delivery or to reduce frequency of injection. Recently, a second aspect emerged, concentrating on more targeted routes of delivery, such as subconjunctival, suprachoroidal, subretinal, and trans-scleral injections. These new delivery techniques, although may be less invasive, still require repeated injections to the eye. In addition, ocular injections are usually not suitable for delivery of small molecules as they tend to have short half-lives (usually less than 10 hours) of bioavailability in target tissues [9,14,21]. Other than use of steroids, such as dexamethasone intravitreal implant and triamcinolone intravitreal injection [22,23], there are currently no non-steroidal small molecules approved to treat retinal diseases. This is not because small molecules do not have the mechanism of action to treat such diseases, but rather due to hindered capacity of the currently available delivery methods. As a matter of fact, small molecules, such as vascular endothelial growth factor (VEGF) receptor inhibitors, platelet-derived growth factor receptor inhibitors, tyrosine kinases inhibitors, and complement inhibitors have been presented in scientific publications, and listed as ongoing pipeline of potential drug innovation for dry/wet age-related macular degeneration (AMD) and other retinal diseases [24,25,26,27]. The route of delivery is often by slow-release invasive implants, or oral administration with systemic exposure.
Here we describe the discovery of a novel Non-Invasive Ocular Delivery Platform (NIODP) that successfully delivered drug candidates not only to the front, but also to the back of the nonhuman primate (NHP) eye through topical administration to the periorbital skin. NIODP delivered JV-DE1, an anti-inflammatory agent in development for dry eye diseases, as efficiently as eye drops did to its target tissue of cornea. NIODP also successfully delivered JV-MD2, the docosahexaenoic acid (DHA) omega-3 fatty acid, which is not well tolerated as an eye drop at high dose, to both the cornea and the retina with high efficiency. Our studies demonstrated the potential of NIODP for high efficiency drug delivery for treatment of various ocular disorders, particularly for retinal diseases.
2. Materials and Methods
2.1. Compounds
The chemical structure of JV-DE1 and JV-MD2 are presented in Figure 1. JV-DE1 (a.k.a. JV-DE1, RO1138452, CAY10441) was custom synthesized at Raybow Pharmaceutical Science & Technology Co., Ltd., Hangzhou, China. JV-MD2 (DHA free acid) and compound-X (described in Section 2.5) were purchased from Sigma-Aldrich, MO, USA. These compounds also served as internal standards (IS) for relative analytical assays.
2.2. Formulations
JV-DE1 eye drop formulation: JV-DE1 was dissolved in 2.4% polyoxyl 35 castor oil and 0.2% glycerol in pH7.6 Tris-buffered saline to 2.4mg/ml (0.24% w/v).
Formulations for NIODP application: JV-DE1 was dissolved in medium-chain triglyceride oil to 5.3mg/g. JV-MD2 original stock of 98% was diluted in linoleic acid oil pre-dissolved with a compound-X. The final concentration of JV-MD2 was 215.21mg/g and Vitamin X was 16.14mg/g. A pen brush with 3-ml reservoir was used as applicator for each formulation.
2.3. Choice of Animals for Eye Drop & NIODP Ocular Biodisposition Studies
A pilot ocular biodisposition study is often utilized in research & discovery phase, prior to Good Laboratory Practices (GLP) Pharmacokinetic studies, to assess the feasibility of delivery route and reliability of the animal model, as well as minimize unnecessary use of animals to be sacrificed, especially in studies of higher species like non-human primates (NHP). The biodisposition describes a drug’s distribution (“where”) at a certain time point (“when”). As long as an ocular biodisposition study is designed so that it can answer the questions of “when” and “where” in a generally consistent trend, ideally in multiple time points, such study design has been acceptable by the FDA and in peer reviewed publications, especially when higher species were used in the studies [5,6,28,29,30].
Rabbits have been an ideal model to study topical eye drop formulation delivery, especially to the anterior chamber of the eye. Compared to rodents, rabbits share more common anatomical and biochemical features with humans, such as larger eye size [31]. Monkey was chosen for the initial NIODP concept validation as the most suited animal model for their hairless periorbital skin, size of eyeball, similarity to human ocular anatomy, in order to maximize the usually low animal-to-human translational success rate in non-invasive retinal delivery. Non-naïve NHPs washed out from previously unrelated studies were used for the experiment. For analytical method development and validation, ocular blank matrixes were harvested from animals of control group after unrelated terminal studies.
2.4. Biodisposition of JV-DE1 Eye Drops in New Zealand Rabbits
Five male New Zealand rabbits aged 4-7 months were used in this study. Animals were housed individually in polypropylene cages (530 mm×630 mm×320 mm) and in an environmentally monitored, well-ventilated conventional room maintained at a temperature of 18-26°C and a relative humidity of 40%-70%. Certified rabbit diet was provided ad libitum daily during the quarantine and study periods. Nutritional ingredients and designated chemicals of the diet were analyzed by a qualified institute once quarterly.
The in-life procedures and sample collections were performed at Joinn. A single dose of 50µL (120µg) per eye of the 0.24% JV-DE1 eye drop was applied to both eyes of the animals at time 0 using a pipet. The dose was chosen based on maximum amount deliverable as eye drop. Blood samples were collected from all five study animals at 0-hour pre-dosing. For every time point of 0.5, 2, 4, 8 and 24-hour post-dose, one animal was euthanized and ocular tissues (anterior sclera, aqueous humor, bulbar conjunctiva, ciliary body, cornea, iris, posterior sclera, and retina) of both eyes were collected. Plasma sample was collected before each euthanization.
Sample preparation and bioanalysis were performed at Medicilon. Solid ocular tissues were homogenized with 9 to 49-fold (1g tissue in 9ml to 49ml, w/v) of cold homogenization buffer (50% methanol/H2O). Aliquots of plasma or aqueous humor, as well as the homogenized tissue samples, were mixed with 8-fold volumes of 200ng/ml warfarin in methanol solution. After vortexing and centrifuging, an aliquot of supernatants was transferred to 96-well plate for LC-MS/MS analysis. JV-DE1 is a synthesized new chemical entity. The absence of the endogenous compound has been verified by a battery of pre-clinical GLP and non-GLP studies, including analytical studies in monkey, dog, and rabbit tissues (JeniVision data not shown).
2.5. Biodisposition of JV-DE1 and JV-MD2 Delivered via NIODP in Non-Human Primates
Four female Cynomolgus non-naive monkeys aged 3 - 4 years used for unrelated projects were washed out prior to this study. The monkey maintenance pelleted feed was purchased from Beijing HFK Bioscience Co. Ltd. or other qualified source and was provided ad libitum throughout the in-life portion of the study. During the acclimation period and the experiment, the animals were housed individually (1 monkey/cage) in stainless steel wire-mesh type cages in a group housing.
All experiments were performed at Medicilon. A single dose of about 31.2mg of the 5.3µg/mg JV-DE1 formulation, i.e. 165.3±4.6µg (mean ± SEM) per eye of JV-DE1 was applied to the right eye (OD); and a single dose of about 31.48 ± 0.43mg of the 215.2µg/mg JV-MD2 formulation, i.e. 6775±92µg (mean ± SEM) per eye was applied to the left eye (OS) of each animal at time 0 via NIODP [this formulation also contained 16.14µg/mg of compound-X (mean 508µg per OS), which did not penetrate beyond the periorbital skin, data not shown]. A pen brush was used to dose each formulation with three to four circular motions for even distribution. The doses of the test articles were selected based on their solubility/concentration with the maximum deliverable volume on the periorbital skin of the animals. The administered dose was calculated by weight difference of the pen brush before and after administration. Animals were restrained from eye rubbing in restraint chairs for 2 hours after dosing with access to food and drink. Blood sample was collected from one of the study animals at pre-dosing. For every time point of 0.5, 3, 6 and 24-hour post-dose, one animal was euthanized and ocular tissues (upper eyelid, cornea, retina, and vitreous humor) of both eyes were collected. Plasma samples were collected before each euthanization.
For convenience of tissue processing and sample extraction, only upper eyelids were collected to represent the entirety of the periorbital tissue. Ocular tissues were homogenized by adding 9-fold volume of 50% methanol/H2O to per gram of tissue. LC-MS/MS sample preparation: a 50μL aliquot of plasma, aqueous humor, vitreous humor, or tissue homogenate was thoroughly mixed with 250μL extraction solution of CHCl3/EtOH (1:1), then 210μL supernatant of the samples was transferred to a 96-well plate after centrifugation. Samples were evaporated in nitrogen gas (N2) until dried. Each sample was redissolved in 200μL MeOH, of which 2µl was injected for LC-MS/MS analysis.
2.6. LC-MS/MS Methods for JV-DE1 in Rabbit Plasma and Ocular Tissues
The Liquid Chromatography (LC) system comprised a Waters (Waters Corporation, UAS) Ultra Performance Liquid Chromatography (UPLC) equipped with an ACQUITY UPLC binary solvent manager, ACQUITY UPLC sample manager, ACQUTIY UPLC sample organizer and ACQUITY UPLC column heater HT. The Mass spectrometric (MS) analysis was performed using a Triple Quad 6500+ (Applied Biosystems/MDS Sciex) with an ESI Ionsource. The data acquisition and control system are created using Analyst 1.6.3 and 1.7.1 Software from Applied Biosystems/MDS Sciex. The LC/MS conditions for JV-DE1 are described in Table 1a–c.
2.7. LC-MS/MS Methods for JV-DE1 and JV-MD2 in Monkey Plasma and Ocular Tissues
The LC system is the same as the JV-DE1 in rabbit samples. The MS analysis was performed using a Triple Quad 5500 with an ESI Ionsource, and the data acquisition and control system is Analyst 1.6.3 Software from Applied Biosystems/MDS Sciex.
The LC/MS conditions for JV-DE1 are described in Table 2. The LC conditions were as follows: ACQUITY UPLC ® BEH C18 1.7μm, 2.1mm*50mm; the mobile phase Column A, 0.1% Formic acid in water and Column B, 0.1% Formic Acid in acetonitrile. The flow rate was 0.6ml/min, column temperature 50℃, and injection volume 2µL.
MS conditions: scan type: Positive MRM; Ion source: Turbo spray; Ionization model: ESI; nebulizer Gas1: 55psi; gas2: 55psi; curtain gas: 40psi; CAD: 10; ionspray: voltage 5500V; temperature: 550℃.
The LC/MS conditions for JV-MD2 (DHA) are described in Table 3. The LC conditions were as follows: ACQUITY UPLC ® BEH C18 1.7μm, 2.1mm*50mm; the mobile phase Column A, 10mm NH4AC in H2O and Column B, CAN. The flow rate was 0.5ml/min, column temperature 40℃, and injection volume 4µL.
MS conditions: scan type: Negative MRM; Ion source: Turbo spray; Ionization model: ESI; nebulizer gas1: 55psi; gas2: 55psi; curtain gas: 40psi; CAD: 9; ionspray voltage: 5500V; temperature: 550℃.
3. Results
3.1. JV-DE1 Ocular and Plasma Bioavailability Delivered by Eye Drops in New Zealand Rabbits—The Evolution of Eye Drop Administration to Glaucoma Drug Periorbital Delivery, to Discovery of the Non-Invasive Ocular Delivery Platform (NIODP)
The proprietary topical periorbital skin route (i.e. via the skin area around the eye orbit) for ocular drug delivery was first used to deliver JV-GL1, a prostanoid EP2 receptor agonist, to treat glaucoma, with successful intraocular pressure lowering effects in normotensive Cynomolgus monkeys [28] and in open-angle glaucoma or ocular hypertension patients of Phase 1b/2a clinical trial (data not shown).
JV-DE1 is an anti-inflammatory compound with dual antagonism on prostanoid IP receptor and platelet activating factor (PAF) [32]. It is in development at JeniVision for treatment of dry eye disease. When a 50-µL JV-DE1 eye drop formulation was administered by pipetting to the right eye (OD) at 120µg/eye of New Zealand rabbits (Table 4), it accumulated at high concentration in ocular surface tissues of bulbar conjunctiva (Cmax ~ 16µg/g) and cornea (Cmax ~ 12µg/g) as expected, follwed by anterior sclera (Cmax 1.7856µg/g), ciliary body/iris (Cmax 0.3049µg/g) and posterior sclera (Cmax 0.2395µg/g). The JV-DE1 also reached the retina at a Cmax of 0.0920µg/g, which is much higher than the 0.0026µg/g Cmax in vitreous humor. The JV-DE1 eye drops concentration gradient in ocular tissues (Figure 2) was consistent with its maximum ocular delivery efficiency (presented as % administered dose), which was conjunctiva (1.3929%) > cornea (0.8622%) > anterior sclera (0.2982%) > posterior sclera (0.0197%) > ciliary body/iris (0.0174%) > retina (0.0047%) > vitreous humor (0.0023%). There was no significant systemic exposure of JV-DE1 when applied via eye drops, as the drug concentration was no more than 0.001µg/ml in the plasma throughout the 0.5, 3-, and 6-hour post-dose time points, with 24-hour clearance.
Although the 0.0047% retinal delivery efficiency of JV-DE1 eye drop in rabbits was about 5-fold higher compared to the maximum of 0.001% efficiency usually seen in most eye drops dosed to lower animal species, a 10- to 100-fold increase of retinal delivery efficiency demonstrated in a large animal species is desirable to ensure clinical success. Since substantial increase of drug load is hard to achieve as an eye drop formulation due to limitations on drug solubility, ocular tolerability, and suitability, the follow up studies (as described in Section 3.2 and Section 3.3) on ocular drug delivery via the periorbital skin route was inspired in hope of achieving pharmaceutically effective retinal doses in larger animal species.
3.2. JV-DE1 Ocular and Plasma Bioavailability after a Single Dose NIODP Application in Non-Human Primates
JV-DE1 was topically applied on the periorbital skin at about 165.3µg/eye to the right eye (OD) of four Cynomolgus monkeys in this study (Table 5). A substantial quantity of the drug was found in the eyelid/periorbital skin (Cmax 26.54µg/g) and cornea (Cmax 9.30µg/g). On the other hand, retina (Cmax 0.0455µg/g) and vitreous humor (Cmax 0.0190µg/g) had the lowest drug levels. Therefore, the concentration gradient remained similar to the eye drop application, where the dosing site of NIODP (eyelid/periorbital skin) > cornea > retina > vitreous humor (Figure 3). The plasma concentrations remained ≤ 0.0003µg/ml, near the lower limit of quantitation (LLOQ, 0.0001µg/ml), showing no significant systemic exposure of JV-DE1 at dosed level via NIODP application, similar to the eye drop administration.
3.3. JV-MD2 Ocular and Plasma Bioavailability via NIODP in Non-Human Primates
JV-MD2 (DHA omega-3 free acid) was administered via NIODP at approximately 6775µg/eye to the left eye (OS) of four Cynomolgus monkeys. The endogenous levels of DHA in ocular tissues were determined during method validation from the mean of double blank matrix measured during method validation, where BLQ is below the limit of quantification, with lower limit of quantitation (LLOQ)=0.5µg/ml. Substantial quantities of JV-MD2 remained in eyelid/periorbital skin (11~420µg/g vs. the BLQ baseline), cornea (22~66µg/g vs. the BLQ baseline), and retina (47~111µg/g vs. the 17µg/g baseline), at all post-dose time points of 0.5-, 3-, 6- and 24-hour (Table 6). Of particular note is that JV-MD2 rapidly reached its Cmax of 111µg/g in retina within 0.5-hour post-dose from the endogenous level of 17µg/g. In the vitreous humor, JV-MD2 remained below BLQ at all timepoints except for at 24-hour post dose (2µg/ml). The JV-MD2 concentration gradient displayed as: the dosing site of NIODP (eyelid/periorbital skin) > retina > cornea >> vitreous humor. This is generally concordant with the maximum percentage of administered dose achieved within 30min of dosing, which was eyelid/periorbital skin (0.4288%) > retina (0.0343%) > cornea (0.0283%) >> vitreous humor. The post-dose plasma levels of JV-MD2 showed a range of 1~3µg/ml, with no significant fluctuation around the 2µg/ml pre-dosing baseline.
4. Discussion
According to the tissue concentration gradient (Figure 2) and % of administered dose in ocular tissues (Table 4) derived from the rabbit eye drop biodisposition study, most of the JV-DE1 followed a typical “corneal route”: cornea → anterior tissues (ciliary body/iris) → vitreous humor, where JV-DE1 lost the driving force to reach the retina; in the meantime, a small portion of the JV-DE1 may also have taken the “conjunctiva-sclera route”, i.e., conjunctiva → sclera → retina. Changing the site of delivery from ocular surface as eye drops to periorbital skin around the eye via NIODP did not improve retinal delivery of JV-DE1. Rather, the maximum delivery efficiency in the retina was about 10-fold lower, dropping from 0.0047% via eye drop application to 0.0005% via NIODP, albeit not in a head-to-head comparison, as the studies were conducted in different species. Nonetheless, the tissue concentration gradient again indicated that JV-DE1 achieved the retina mainly through the same conjunctiva-sclera pathway, just like the eye drops. JV-DE1 seems to bypass the vitreous humor to recah the retina, as in both delivery routes the retinal bioavalability seems to be higher that that in the vitreous humor.
Although both molecules are amphipathic, JV-DE1 can form an aqueous formulation, while JV-MD2 (DHA) is a fatty acid with much lower water solubility. The difference in physicochemical properties makes DHA easier to penetrate cell membrane and diffuse through biological tissues to achieve efficient transcellular and intracellular distribution. We have discovered a novel non-invasive ocular delivery platform, and demonstrated that application of less than 7mg of JV-MD2 (DHA) via NIODP can reach the Cmax of 66µg/g in the cornea and 111µg/g in the retina, where the delivery efficiencies were 0.01~0.42% in eyelid/periorbital skin (site of application), 0.01~0.03% in the cornea, and 0.01~0.04% in the retinal of NHPs. Similar to JV-DE1 (administered either as eye drops or via NIODP), JV-MD2 seems to reach the retina via the conjunctiva-sclera pathway when administered by NIODP, with a preferred distribution to retina over cornea (Figure 4). Interestingly, the biodistribution of JV-MD2 only appeared in the vitreous humor at 24-hour post dose but not in any earlier time points of 0.5-, 3-, and 6-hour post dose, also there was no endogenous DHA detected in the blank matrix. Thus, excess JV-MD2 may diffuse from the retina to vitreous humor over time, if other reasons such as animal-to-animal variation can be ruled out.
In contrast to the traditional eye drop administration that targets the cornea mostly for anterior ocular drug delivery, the conjunctival-scleral pathway previously has not been considered a major drug delivery route, although ocular drug penetration may occur via this pathway. The conjunctival-scleral pathway may provide a much larger surface area for drug absorption than the cornea [33]. Compared to the cornea, the relatively leaky and hydrophilic conjunctival tissue can provide approximately 230-fold larger intercellular spaces, more permeable even to macromolecules, such as proteins and peptides [3]. Connecting to the conjunctiva is the sclera, a network of collagen fibers, proteoglycans, and glycoproteins in an aqueous medium forming the scleral water channels 30~350nm in size [9,12], spacious enough for passage of macromolecules. For reference, the average molecular widths are 2.5nm for DNAs, 10nm for proteins, 100nm for a typical virus, and 1000nm for a bacterium [34]. The suprachoroid is located between the sclera and the choroid. Since choroid bleeds into the suprachoroid space (SCS), exchange of biomolecules between the choroid - SCS - sclera is barrier-free. Because of this permeability, and since suprachoroidal injection has more favorable safety profile compared to the intravitreal injection, this route has been under investigation since 2013 for retinal delivery [35]. The fenestrated capillaries in the choroid are very permeable and allow high concentration and rapid diffusion of nutrients in the extra-vascular space of the choroid [36]. Bruch’s membrane (BrM) is a thin layer of extracellular matrix selectively permeable membrane between the retina and choroid, which regulates the exchange of nutrients, oxygen, minerals, and visual cycle by-products through passive diffusion, influenced by the weight, size, and shape of the diffusing molecule. While some complement proteins, such as FHL-1, factor D, and C5a, are allowed to diffuse through, most complement proteins (including the low molecular weight C3a) are unable to do so [37,38]. Finally, before any drug reaches the retina, it must pass the retinal pigment epithelium (RPE), which also forms the outer blood-retina barrier (BRB), regulating drug permeability by physicochemical properties, such as molecular weight, lipophilicity, protein binding, and concentration gradient [12].
Age-related macular degeneration (AMD) in the elderly is the leading cause of irreversible vision loss. Early stages of AMD (dry AMD) are defined by the formation of lipid-rich deposits of drusen between the RPE and the BrM, as well as accumulation of choroidal macrophages. Geographic atrophy (GA), one of the advanced stages of AMD is characterized by confluent deterioration of RPE, photoreceptor and choroidal neovascularization. Wet (or neovascular) AMD, another advanced stages of AMD, is characterized by the invasive choroidal neovascularization (CNV) with accompanying macrophages accumulation into the retina breaking from the BrM, which leads to retinopathy [39]. Genetic variations of the innate immune system and poor diet are the two main factors contributing to drusen genesis and disease progression in AMD [40]. Mechanistic target of rapamycin (mTOR), a sensor of nutrient availability and growth factors, has been implicated in multiple diseases like cancer, diabetes and neurodegenerative, represented as inflammation, as well as aging, represented as “inflammaging” [41,42,43]. Activation of mTORC1 has been associated with formation of drusen-like deposits in photoreceptors, where supplement of dietary DHA alleviated most pathologies in a mouse model with advanced AMD pathologies [40]. Once daily intragastric administration of DHA effectively inhibited laser-induced CNV formation in mice, which was associated with suppressed protein expression of NF-κB, VGFER2, and VEGF, major players in the angiogenic pathway in cancer and advanced stages of AMD [44]. Upon induction of pathological stimuli, activated macrophages were recruited to the affected site, i.e. back of the eye in the case of AMD, to secrete proinflammatory cytokine, to recruit more macrophages and accelerate disease progression. Omega-3 fatty acids provoke major alterations on gene expression in macrophages to decrease cytokine production, while increasing phagocytosis and M2 macrophage phenotype. It is worthy of note that the anti-inflammatory effect mediated by DHA was more potent than that of EPA; the only cytokine secretion increased by omega-3 fatty acid treatment was the anti-inflammatory cytokine IL-10; while many other cytokines, such as IL-1β, TNF-α, and IL-6, were found decreased in omegga-3 fatty acid treated macrophages [45]. Therefore, the mechanism of action of DHA in early and intermediate dry AMD treatment is thought to suppress drusen genesis via mTORC inhibition, alter the function of macrophages toward anti-inflammation by inhibiting proinflammatory cytokine production, and mediate anti-neovascularization effects by inhibiting the effects of VEGF in the choroid and retina. Upon success in treating the early/intermediate stage dry AMD by DHA, it is logical to anticipate the prevention of late-stage AMD, wet AMD and Geographic Atrophy, where the prevalence of each is approximately 10% of all individuals with AMD [46,47] (Figure 5a).
In human clinical trials for dry AMD treatment, Georgiou and Prokopiou in 2015 reported preliminary but promising therapeutic results of taking 5g/day omega-3 in patients with mild to moderate visual impairment of dry AMD [48]. Then in 2022 ARVO annual meeting abstract, the same group reported that 3.7g daily oral administration of omega-3 fatty acids improved objective and subjective vision in patients with dry AMD and SD [49]. A peer reviewed article has not yet been published. In a 3-year randomized clinical study in patients with early lesions of AMD, the omega-3 (840mg/day DHA and 270mg/day EPA) supplemented patients who had high red blood cell membrane EPA and DHA levels were significantly protected against choroidal neovascularization of AMD compared with those in the olive oil placebo group [50]. Additionally, the preventative effect of omega-3 in AMD has been clearly demonstrated in large number of epidemiological studies, by different methodologies, populations and geographical sites with high degree of consistency [51]. However, no interventive treatment effect from omega-3 consumption was found in patients with advanced AMD [52]. This may be due to two reasons: (a) poor absorption and poor retinal delivery efficiency of orally administered omega-3, even with mega dosage [7,51,53]; (b) pharmaceutically effective doses for disease treatment are usually expected to be at least a few folds over the doses for disease prevention, where normal physiological levels are good enough for health keeping. For example, the European Food Safety Authority (EFSA) suggested that the amount of EPA+DHA required to lower triglyceride is 2–4 g/day and 3 g/day to lower blood pressure, which are about 4- to 13-fold over the recommended daily consumption postulates by the World Health Organization (WHO) to stay healthy [54].
A healthy retina contains a high concentration of DHA (active ingredient of JV-MD2), which is not only important in maintenance of normal retinal integrity and visual function, but also plays anti-inflammatory, antiapoptotic, and neuroprotective roles [54,55]. DHA analogs may act as anti-inflammatory lipid mediators to activate peroxisome proliferator-activated receptors (PPAR) and retinoid x receptors (RXR). DHA, as a natural ligand, induced a protective effect in rat retinal neuronal cultures to promote survival and differentiation of photoreceptors by activating RXR and the downstream signaling pathways [56]. The EC50 of DHA was about 5–10μm on human RXRα receptor and an oxidized form of DHA can be as potent as EC50 of 0.4μM on human PPARγ [57,58]. It was suggested that DHA and its more potent metabolites compete with the more biologically potent arachidonic acid on the COX-2 (IC50 18μM) signaling cascade and shift the proinflammatory state to being more anti-inflammatory [59,60]. DHA was able to suppress inflammation through reducing IL-1β production with potency of IC50 = 4.6µM in human THP-1 macrophage cell line [61]. DHA was also found to reduce the activity of protein kinase C (PKC), cAMP-dependent protein kinase A (PKA), mitogen-activated protein kinase (MAPK), and Ca21/ calmodulin-dependent protein kinase II (CaMKII) at IC50 34–36µM in in-vitro functional assays [62] (Figure 5b). For retinal diseases treatment, a local drug concentration of 3- to 10-fold over EC50 or IC50 are desirable, which may be readily achieved in the retina utilizing the NIODP, as demonstrated in our current study, where application of just 7mg/eye of DHA in NHP yielded retina DHA Cmax of 111µg/g (about 338µM). Success of drug treatment lies in the effective drug concentration deliverable to the target tissue [63]. We believe that much higher DHA retinal concentrations can be achieved via NIODP by using formulation with higher concentration and more frequent dosing, if necessary.
There is a potential that NIODP may be utilized for macromolecular therapeutics packed in liposomes for retinal delivery. Although there is a “500 Dalton rule” for passive skin penetration of chemical compounds and drugs [64], liposomes up to 600 nm in diameter have been reported as penetrating skin easily through intercellular lipids of the Stratum Corneum, which demonstrated applicability in transdermal drug delivery [65,66]. In posterior ocular delivery, nanocarriers have been reported to overcome the ocular barriers, as nanoparticles <250nm were usually easily taken up by retinal cells via endocytosis [9,67]. More effort of vigorous research may be necessary.
The NIODP via periorbital skin application is also a novel route for anterior ocular drug delivery. It has successfully delivered JV-GL1, a prostaglandin EP2 receptor agonist, for glaucoma treatment in a phase 1b/2a clinical trial with satisfactory efficacy, while avoiding ocular adverse effects commonly associated with prostaglandin eye drops when directly applied to the ocular surface. It is important to note that for issues of solubility or ocular tolerability, most of the hydrophobic vitamins and supplements, including omega-3, cannot be conveniently used as high dose eye drops. NIODP made it possible to deliver these molecules for potential treatment of anterior ocular diseases, such as dry eye disease, uveitis, etc., with minimum irritation or interference of normal ocular functions.
Notably, as most eye drops used in a range of reasonable ocular doses (0.01% ~0.5%), the systemic exposure of JV-DE1 was very low using both eye drops and NIODP as delivery routes with 24-hour clearance. Additionally, when delivered as a single dose at about 7mg per eye via NIODP, JV-MD2 also did not significantly change the baseline of omega-3 in the plasma. Therefore, while achieving breakthrough retinal delivery efficiency, the systemic exposure via NIODP application may not pose a great concern, which may also be determined by the physicochemical properties and biosafety profile of the drug.
In summary, similar to JV-DE1 applied via eye drops, both JV-DE1 and JV-MD2 applied via NIODP seem to reach the retina via the conjunctiva-sclera pathway. The potential advantages of NIODP include, (a) a breakthrough in non-invasive, high efficiency retinal delivery; (b) a much more ocularly tolerable delivery method than eye drops for therapeutic agents known to cause ocular adverse effects or interfere with normal function of the eye, such as drug ingredients causing eye irritation, or oily formulations causing vision blurriness and eye stress; (c) another topical ocular delivery route without significant systemic exposure, just like the traditional eye drop administration, but potentially more convenient for self-administration or administration by a care-giver.
5. Conclusions
The discovery of the novel non-invasive ocular delivery platform (NIODP) has opened new possibilities for effective topical delivery of currently difficult to deliver molecules to both front and back of the eye. NIODP is a combination of periorbital skin administration with topical drug formulation for ocular, particularly retinal, delivery. JV-MD2 (DHA) has been successfully delivered by NIODP at high efficiency and high bioavailability to the retina. When the essential fatty acid DHA with multi-anti-inflammatory mechanism of action reaches the retina at up to 10-fold concentration over the normal EC50 or IC50 of its molecular targets, better therapeutic efficacy is anticipated on retinal diseases, such as treating dry AMD, thus preventing late-stage AMD, and avoiding or minimizing frequency of invasive ocular injections. With further study and more experimental evidence, NIODP could deliver great opportunities to address the serious medical need in drug delivery for treatment of eye diseases without irritation or injection, and transform the retinal health landscape.
6. Patents
Patent (pending) resulting from the work reported in this manuscript: Delivery methods for Treating Eye Diseases, by W. Wang, D. Woodward, N. Snider.
Author Contributions
Conceptualization & methodology, JW; Data analysis, JW; interpretation & investigation, JW & NS; writing—original draft preparation, JW; writing—review and editing, JW & SN; visualization, JW; supervision, project administration & resource, JW. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
All experiments were conducted in accordance with the ARVO Statement on the Use of Animals in Ophthalmic and Vision Research. All experimental procedures followed protocols approved by the committee on animal research and ethics of the contracted research organizations: Joinn Laboratory Inc. (Suzhou, China) for rabbit studies, and Medicilon Preclinical Research LLC (Shanghai, China) for monkey studies.
Conflicts of Interest
JW and NS are employees of JeniVision.
References
- Mosteller, M.W.; Gebhardt, B.M.; Hamilton, A.M.; Kaufman, H.E., Penetration of topical cyclosporine into the rabbit cornea, aqueous humor, and serum. Arch Ophthalmol 1985, 103, 101-2. [CrossRef]
- Said, T.; Dutot, M.; Christon, R.; Beaudeux, J.L.; Martin, C.; Warnet, J.M.; Rat, P., Benefits and side effects of different vegetable oil vectors on apoptosis, oxidative stress, and P2X7 cell death receptor activation. Invest Ophthalmol Vis Sci 2007, 48, 5000-6. [CrossRef]
- Agarwal, P.; Craig, J.P.; Rupenthal, I.D., Formulation Considerations for the Management of Dry Eye Disease. Pharmaceutics 2021, 13. [CrossRef]
- Agrahari, V.; Mandal, A.; Agrahari, V.; Trinh, H.M.; Joseph, M.; Ray, A.; Hadji, H.; Mitra, R.; Pal, D.; Mitra, A.K., A comprehensive insight on ocular pharmacokinetics. Drug Deliv Transl Res 2016, 6, 735-754. [CrossRef]
- Sarkadi-Nagy, E.; Wijendran, V.; Diau, G.Y.; Chao, A.C.; Hsieh, A.T.; Turpeinen, A.; Nathanielsz, P.W.; Brenna, J.T., The influence of prematurity and long chain polyunsaturate supplementation in 4-week adjusted age baboon neonate brain and related tissues. Pediatr Res 2003, 54, 244-52. [CrossRef]
- Sarkadi-Nagy, E.; Wijendran, V.; Diau, G.Y.; Chao, A.C.; Hsieh, A.T.; Turpeinen, A.; Lawrence, P.; Nathanielsz, P.W.; Brenna, J.T., Formula feeding potentiates docosahexaenoic and arachidonic acid biosynthesis in term and preterm baboon neonates. J Lipid Res 2004, 45, 71-80. [CrossRef]
- Sripetch, S.; Loftsson, T., Topical drug delivery to the posterior segment of the eye: Thermodynamic considerations. Int J Pharm 2021, 597, 120332. [CrossRef]
- Hughes, P.M.; Olejnik, O.; Chang-Lin, J.E.; Wilson, C.G., Topical and systemic drug delivery to the posterior segments. Adv Drug Deliv Rev 2005, 57, 2010-32. [CrossRef]
- Tsai, C.H.; Wang, P.Y.; Lin, I.C.; Huang, H.; Liu, G.S.; Tseng, C.L., Ocular Drug Delivery: Role of Degradable Polymeric Nanocarriers for Ophthalmic Application. Int J Mol Sci 2018, 19. [CrossRef]
- Lakhani, P.; Patil, A.; Majumdar, S., Recent advances in topical nano drug-delivery systems for the anterior ocular segment. Ther Deliv 2018, 9, 137-153. [CrossRef]
- Molokhia, S.A.; Thomas, S.C.; Garff, K.J.; Mandell, K.J.; Wirostko, B.M., Anterior eye segment drug delivery systems: current treatments and future challenges. J Ocul Pharmacol Ther 2013, 29, 92-105. [CrossRef]
- Varela-Fernandez, R.; Diaz-Tome, V.; Luaces-Rodriguez, A.; Conde-Penedo, A.; Garcia-Otero, X.; Luzardo-Alvarez, A.; Fernandez-Ferreiro, A.; Otero-Espinar, F.J., Drug Delivery to the Posterior Segment of the Eye: Biopharmaceutic and Pharmacokinetic Considerations. Pharmaceutics 2020, 12. [CrossRef]
- Rodrigues, G.A.; Lutz, D.; Shen, J.; Yuan, X.; Shen, H.; Cunningham, J.; Rivers, H.M., Topical Drug Delivery to the Posterior Segment of the Eye: Addressing the Challenge of Preclinical to Clinical Translation. Pharm Res 2018, 35, 245. [CrossRef]
- Kim, H.M.; Woo, S.J., Ocular Drug Delivery to the Retina: Current Innovations and Future Perspectives. Pharmaceutics 2021, 13. [CrossRef]
- Gote, V.; Sikder, S.; Sicotte, J.; Pal, D., Ocular Drug Delivery: Present Innovations and Future Challenges. J Pharmacol Exp Ther 2019, 370, 602-624. [CrossRef]
- Nomoto, H.; Shiraga, F.; Kuno, N.; Kimura, E.; Fujii, S.; Shinomiya, K.; Nugent, A.K.; Hirooka, K.; Baba, T., Pharmacokinetics of bevacizumab after topical, subconjunctival, and intravitreal administration in rabbits. Invest Ophthalmol Vis Sci 2009, 50, 4807-13. [CrossRef]
- Davis, B.M.; Normando, E.M.; Guo, L.; Turner, L.A.; Nizari, S.; O'Shea, P.; Moss, S.E.; Somavarapu, S.; Cordeiro, M.F., Topical delivery of Avastin to the posterior segment of the eye in vivo using annexin A5-associated liposomes. Small 2014, 10, 1575-84. [CrossRef]
- de Cogan, F.; Hill, L.J.; Lynch, A.; Morgan-Warren, P.J.; Lechner, J.; Berwick, M.R.; Peacock, A.F.A.; Chen, M.; Scott, R.A.H.; Xu, H.; Logan, A., Topical Delivery of Anti-VEGF Drugs to the Ocular Posterior Segment Using Cell-Penetrating Peptides. Invest Ophthalmol Vis Sci 2017, 58, 2578-2590. [CrossRef]
- Sigurdsson, H.H.; Konraethsdottir, F.; Loftsson, T.; Stefansson, E., Topical and systemic absorption in delivery of dexamethasone to the anterior and posterior segments of the eye. Acta Ophthalmol Scand 2007, 85, 598-602. [CrossRef]
- Hartman, R.R.; Kompella, U.B., Intravitreal, Subretinal, and Suprachoroidal Injections: Evolution of Microneedles for Drug Delivery. J Ocul Pharmacol Ther 2018, 34, 141-153. [CrossRef]
- Del Amo, E.M.; Rimpela, A.K.; Heikkinen, E.; Kari, O.K.; Ramsay, E.; Lajunen, T.; Schmitt, M.; Pelkonen, L.; Bhattacharya, M.; Richardson, D.; Subrizi, A.; Turunen, T.; Reinisalo, M.; Itkonen, J.; Toropainen, E.; Casteleijn, M.; Kidron, H.; Antopolsky, M.; Vellonen, K.S.; Ruponen, M.; Urtti, A., Pharmacokinetic aspects of retinal drug delivery. Prog Retin Eye Res 2017, 57, 134-185. [CrossRef]
- Karti, O.; Saatci, A.O., Intravitreal Dexamethasone Implant in the Treatment of Non-Infectious Uveitic Macular Edema. Med Hypothesis Discov Innov Ophthalmol 2018, 7, 169-175.
- Villegas, V.M.; Gold, A.S.; Wildner, A.; Latiff, A.; Murray, T.G., Intravitreal triamcinolone acetonide: a "real world" analysis of visual acuity, pressure and outcomes. Int J Ophthalmol 2016, 9, 789-91.
- Cao, L.; Weetall, M.; Bombard, J.; Qi, H.; Arasu, T.; Lennox, W.; Hedrick, J.; Sheedy, J.; Risher, N.; Brooks, P.C.; Trifillis, P.; Trotta, C.; Moon, Y.C.; Babiak, J.; Almstead, N.G.; Colacino, J.M.; Davis, T.W.; Peltz, S.W., Discovery of Novel Small Molecule Inhibitors of VEGF Expression in Tumor Cells Using a Cell-Based High Throughput Screening Platform. PLoS One 2016, 11, e0168366.
- Roskoski, R., Jr., The role of small molecule platelet-derived growth factor receptor (PDGFR) inhibitors in the treatment of neoplastic disorders. Pharmacol Res 2018, 129, 65-83. [CrossRef]
- Kaiser, P.K. Retina Pipeline 2021 Ongoing Innovation Wet AMD. https://retinatoday.com/images/retina-pipeline/retina-pipeline-2021/pdfs-for-download/Wet-AMD-Retina-Pipeline-Poster.pdf (accessed 1-20-2022).
- Kaiser, P.K. Retina Pipeline 2021 Ongoing Innovation Dry AMD. . https://retinatoday.com/images/retina-pipeline/retina-pipeline-2021/pdfs-for-download/Dry-AMD-Retina-Pipeline-Poster.pdf (accessed 1-20-2022).
- Woodward, D.F.; Wang, J.W.; Coleman, R.A.; Woodrooffe, A.J.; Clark, K.L.; Stamer, W.D.; Tao, G.; Fan, S.; Toris, C.B., A Highly Effective and Ultra-Long-Acting Anti-Glaucoma Drug, with a Novel Periorbital Delivery Method. J Ocul Pharmacol Ther 2019, 35, 265-277. [CrossRef]
- Dilbeck, M.D.; Spahr, Z.R.; Nanjappa, R.; Economides, J.R.; Horton, J.C., Columnar and Laminar Segregation of Retinal Input to the Primate Superior Colliculus Revealed by Anterograde Tracer Injection Into Each Eye. Invest Ophthalmol Vis Sci 2022, 63, 9. [CrossRef]
- Zarbin, M.A.; Novack, G., N-of-1 Clinical Trials: A Scientific Approach to Personalized Medicine for Patients with Rare Retinal Diseases Such as Retinitis Pigmentosa. J Ocul Pharmacol Ther 2021, 37, 495-501. [CrossRef]
- Zernii, E.Y.; Baksheeva, V.E.; Iomdina, E.N.; Averina, O.A.; Permyakov, S.E.; Philippov, P.P.; Zamyatnin, A.A.; Senin, II, Rabbit Models of Ocular Diseases: New Relevance for Classical Approaches. CNS Neurol Disord Drug Targets 2016, 15, 267-91. [CrossRef]
- Bley, K.R.; Bhattacharya, A.; Daniels, D.V.; Gever, J.; Jahangir, A.; O'Yang, C.; Smith, S.; Srinivasan, D.; Ford, A.P.; Jett, M.F., RO1138452 and RO3244794: characterization of structurally distinct, potent and selective IP (prostacyclin) receptor antagonists. Br J Pharmacol 2006, 147, 335-45. [CrossRef]
- Watsky, M.A.; Jablonski, M.M.; Edelhauser, H.F., Comparison of conjunctival and corneal surface areas in rabbit and human. Curr Eye Res 1988, 7, 483-6. [CrossRef]
- NanoSense Lesson 2: Scale of Objects ...Student Materials. https://nanosense.sri.com/activities/sizematters/sizeandscale/SM_Lesson2Student.pdf.
- Chiang, B.; Jung, J.H.; Prausnitz, M.R., The suprachoroidal space as a route of administration to the posterior segment of the eye. Adv Drug Deliv Rev 2018, 126, 58-66. [CrossRef]
- Tornquist, P.; Alm, A.; Bill, A., Permeability of ocular vessels and transport across the blood-retinal-barrier. Eye (Lond) 1990, 4 ( Pt 2), 303-9. [CrossRef]
- Hammadi, S.; Tzoumas, N.; Ferrara, M.; Meschede, I.P.; Lo, K.; Harris, C.; Lako, M.; Steel, D.H., Bruch's Membrane: A Key Consideration with Complement-Based Therapies for Age-Related Macular Degeneration. J Clin Med 2023, 12. [CrossRef]
- Clark, S.J.; McHarg, S.; Tilakaratna, V.; Brace, N.; Bishop, P.N., Bruch's Membrane Compartmentalizes Complement Regulation in the Eye with Implications for Therapeutic Design in Age-Related Macular Degeneration. Front Immunol 2017, 8, 1778. [CrossRef]
- Ambati, J.; Atkinson, J.P.; Gelfand, B.D., Immunology of age-related macular degeneration. Nat Rev Immunol 2013, 13, 438-51. [CrossRef]
- Cheng, S.Y.; Cipi, J.; Ma, S.; Hafler, B.P.; Kanadia, R.N.; Brush, R.S.; Agbaga, M.P.; Punzo, C., Altered photoreceptor metabolism in mouse causes late stage age-related macular degeneration-like pathologies. Proc Natl Acad Sci U S A 2020, 117, 13094-13104. [CrossRef]
- Casciano, F.; Zauli, E.; Rimondi, E.; Mura, M.; Previati, M.; Busin, M.; Zauli, G., The role of the mTOR pathway in diabetic retinopathy. Front Med (Lausanne) 2022, 9, 973856. [CrossRef]
- Leonardi, G.C.; Accardi, G.; Monastero, R.; Nicoletti, F.; Libra, M., Ageing: from inflammation to cancer. Immun Ageing 2018, 15, 1. [CrossRef]
- Zou, Z.; Tao, T.; Li, H.; Zhu, X., mTOR signaling pathway and mTOR inhibitors in cancer: progress and challenges. Cell Biosci 2020, 10, 31. [CrossRef]
- Li, X.; Gao, S.; Zhang, Y.; Xin, M.; Zuo, C.; Yan, N.; Xia, Q.; Zhang, M., Dihydroartemisinin Inhibits Laser-Induced Choroidal Neovascularization in a Mouse Model of Neovascular AMD. Front Pharmacol 2022, 13, 838263. [CrossRef]
- Gutierrez, S.; Svahn, S.L.; Johansson, M.E., Effects of Omega-3 Fatty Acids on Immune Cells. Int J Mol Sci 2019, 20. doi:10.3390/ijms20205028.
- sccessed 7/27).
- Georgiou, T.; Prokopiou, E., The New Era of Omega-3 Fatty Acids Supplementation: Therapeutic Effects on Dry Age-Related Macular Degeneration. J Stem Cells 2015, 10, 205-15.
- Prokopiou, K.; Kolovos, P.; Tsangari, H.; Bandello, F.; Rossetti, L.M.; Mastropasqua, L.; Mohand-Said, S.; Georgiou, T., A prospective, multicentre, randomised, double-blind study designed to assess the potential effects of omega-3 fatty acids supplementation in dry age-related macular degeneration or Stargardt disease. Investigative Ophthalmology & Visual Science 2022, 63.
- Souied, E.H.; Delcourt, C.; Querques, G.; Bassols, A.; Merle, B.; Zourdani, A.; Smith, T.; Benlian, P.; Nutritional, A.M.D.T.S.G., Oral docosahexaenoic acid in the prevention of exudative age-related macular degeneration: the Nutritional AMD Treatment 2 study. Ophthalmology 2013, 120, 1619-31.
- Souied, E.H.; Aslam, T.; Garcia-Layana, A.; Holz, F.G.; Leys, A.; Silva, R.; Delcourt, C., Omega-3 Fatty Acids and Age-Related Macular Degeneration. Ophthalmic Res 2015, 55, 62-9. [CrossRef]
- Edelhauser, H.F.; Rowe-Rendleman, C.L.; Robinson, M.R.; Dawson, D.G.; Chader, G.J.; Grossniklaus, H.E.; Rittenhouse, K.D.; Wilson, C.G.; Weber, D.A.; Kuppermann, B.D.; Csaky, K.G.; Olsen, T.W.; Kompella, U.B.; Holers, V.M.; Hageman, G.S.; Gilger, B.C.; Campochiaro, P.A.; Whitcup, S.M.; Wong, W.T., Ophthalmic drug delivery systems for the treatment of retinal diseases: basic research to clinical applications. Invest Ophthalmol Vis Sci 2010, 51, 5403-20. [CrossRef]
- Khoo, H.E.; Ng, H.S.; Yap, W.S.; Goh, H.J.H.; Yim, H.S., Nutrients for Prevention of Macular Degeneration and Eye-Related Diseases. Antioxidants (Basel) 2019, 8. [CrossRef]
- Querques, G.; Forte, R.; Souied, E.H., Retina and omega-3. J Nutr Metab 2011, 2011, 748361.
- Calder, P.C., Omega-3 fatty acids and inflammatory processes. Nutrients 2010, 2, 355-74. doi:10.3390/nu2030355.
- German, O.L.; Monaco, S.; Agnolazza, D.L.; Rotstein, N.P.; Politi, L.E., Retinoid X receptor activation is essential for docosahexaenoic acid protection of retina photoreceptors. J Lipid Res 2013, 54, 2236-2246. [CrossRef]
- Lengqvist, J.; Mata De Urquiza, A.; Bergman, A.C.; Willson, T.M.; Sjovall, J.; Perlmann, T.; Griffiths, W.J., Polyunsaturated fatty acids including docosahexaenoic and arachidonic acid bind to the retinoid X receptor alpha ligand-binding domain. Mol Cell Proteomics 2004, 3, 692-703. doi:10.1074/mcp.m400003-mcp200.
- Itoh, T.; Yamamoto, K., Peroxisome proliferator activated receptor gamma and oxidized docosahexaenoic acids as new class of ligand. Naunyn Schmiedebergs Arch Pharmacol 2008, 377, 541-7.
- Calder, P.C., Omega-3 polyunsaturated fatty acids and inflammatory processes: nutrition or pharmacology? Br J Clin Pharmacol 2013, 75, 645-62.
- Li, X.; Yu, Y.; Funk, C.D., Cyclooxygenase-2 induction in macrophages is modulated by docosahexaenoic acid via interactions with free fatty acid receptor 4 (FFA4). FASEB J 2013, 27, 4987-97. [CrossRef]
- Iverson, C.; Bacong, A.; Liu, S.; Baumgartner, S.; Lundstrom, T.; Oscarsson, J.; Miner, J.N., Omega-3-carboxylic acids provide efficacious anti-inflammatory activity in models of crystal-mediated inflammation. Sci Rep 2018, 8, 1217. [CrossRef]
- Mirnikjoo, B.; Brown, S.E.; Kim, H.F.; Marangell, L.B.; Sweatt, J.D.; Weeber, E.J., Protein kinase inhibition by omega-3 fatty acids. J Biol Chem 2001, 276, 10888-96.
- Djebli, N.; Khier, S.; Griguer, F.; Coutant, A.L.; Tavernier, A.; Fabre, G.; Leriche, C.; Fabre, D., Ocular Drug Distribution After Topical Administration: Population Pharmacokinetic Model in Rabbits. Eur J Drug Metab Pharmacokinet 2017, 42, 59-68. [CrossRef]
- Bos, J.D.; Meinardi, M.M., The 500 Dalton rule for the skin penetration of chemical compounds and drugs. Exp Dermatol 2000, 9, 165-9. [CrossRef]
- Schramlova, J.; Blazek, K.; Bartackova, M.; Otova, B.; Mardesicova, L.; Zizkovsky, V.; Hulinska, D., Electron microscopic demonstration of the penetration of liposomes through skin. Folia Biol (Praha) 1997, 43, 165-9.
- Souto, E.B.; Macedo, A.S.; Dias-Ferreira, J.; Cano, A.; Zielinska, A.; Matos, C.M., Elastic and Ultradeformable Liposomes for Transdermal Delivery of Active Pharmaceutical Ingredients (APIs). Int J Mol Sci 2021, 22. [CrossRef]
- Bisht, R.; Mandal, A.; Jaiswal, J.K.; Rupenthal, I.D., Nanocarrier mediated retinal drug delivery: overcoming ocular barriers to treat posterior eye diseases. Wiley Interdiscip Rev Nanomed Nanobiotechnol 2018, 10. [CrossRef]
Figure 1.
Chemical Structures of (a) JV-DE1 (RO1138452, CAY10441), 4,5-dihydro-N-[4-[[4-(1-methylethoxy)phenyl]methyl]phenyl]-1H-imadazol-2-amine, formula weight 309.4; and (b) JV-MD2 (DHA), cis-4,7,10,13,16,19-Docosahexaenoic acid, formula weight 328.49.
Figure 1.
Chemical Structures of (a) JV-DE1 (RO1138452, CAY10441), 4,5-dihydro-N-[4-[[4-(1-methylethoxy)phenyl]methyl]phenyl]-1H-imadazol-2-amine, formula weight 309.4; and (b) JV-MD2 (DHA), cis-4,7,10,13,16,19-Docosahexaenoic acid, formula weight 328.49.
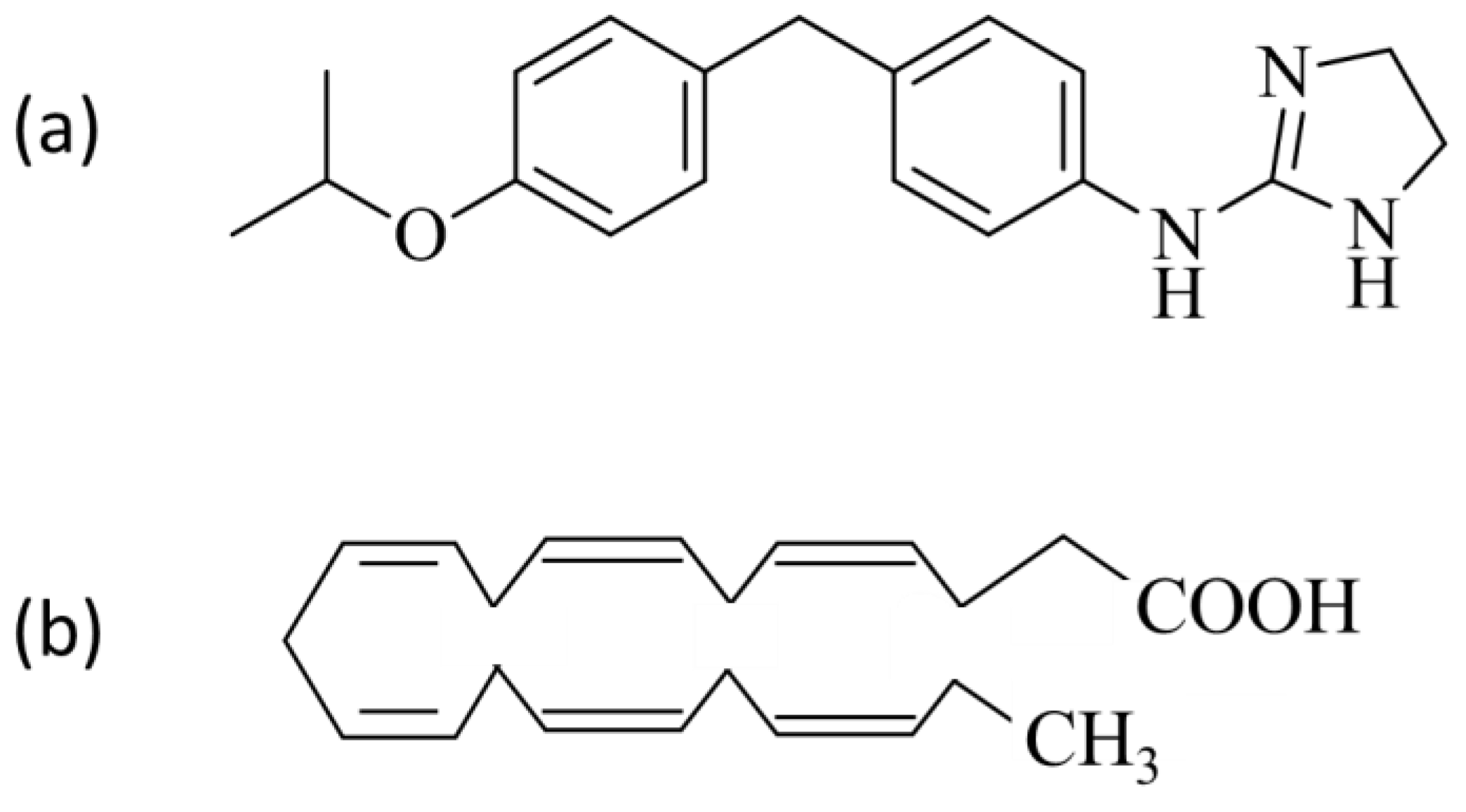
Figure 2.
JV-DE1 bioavailability in New Zealand rabbit plasma and ocular tissues administered as eye drops. A single dose of JV-DE1 (120µg/eye) was delivered to the right eyes (OD). N=4 animals in study. The JV-DE1 level is presented as µg/g of solid tissues, or µg/ml of aqueous tissues.
Figure 2.
JV-DE1 bioavailability in New Zealand rabbit plasma and ocular tissues administered as eye drops. A single dose of JV-DE1 (120µg/eye) was delivered to the right eyes (OD). N=4 animals in study. The JV-DE1 level is presented as µg/g of solid tissues, or µg/ml of aqueous tissues.
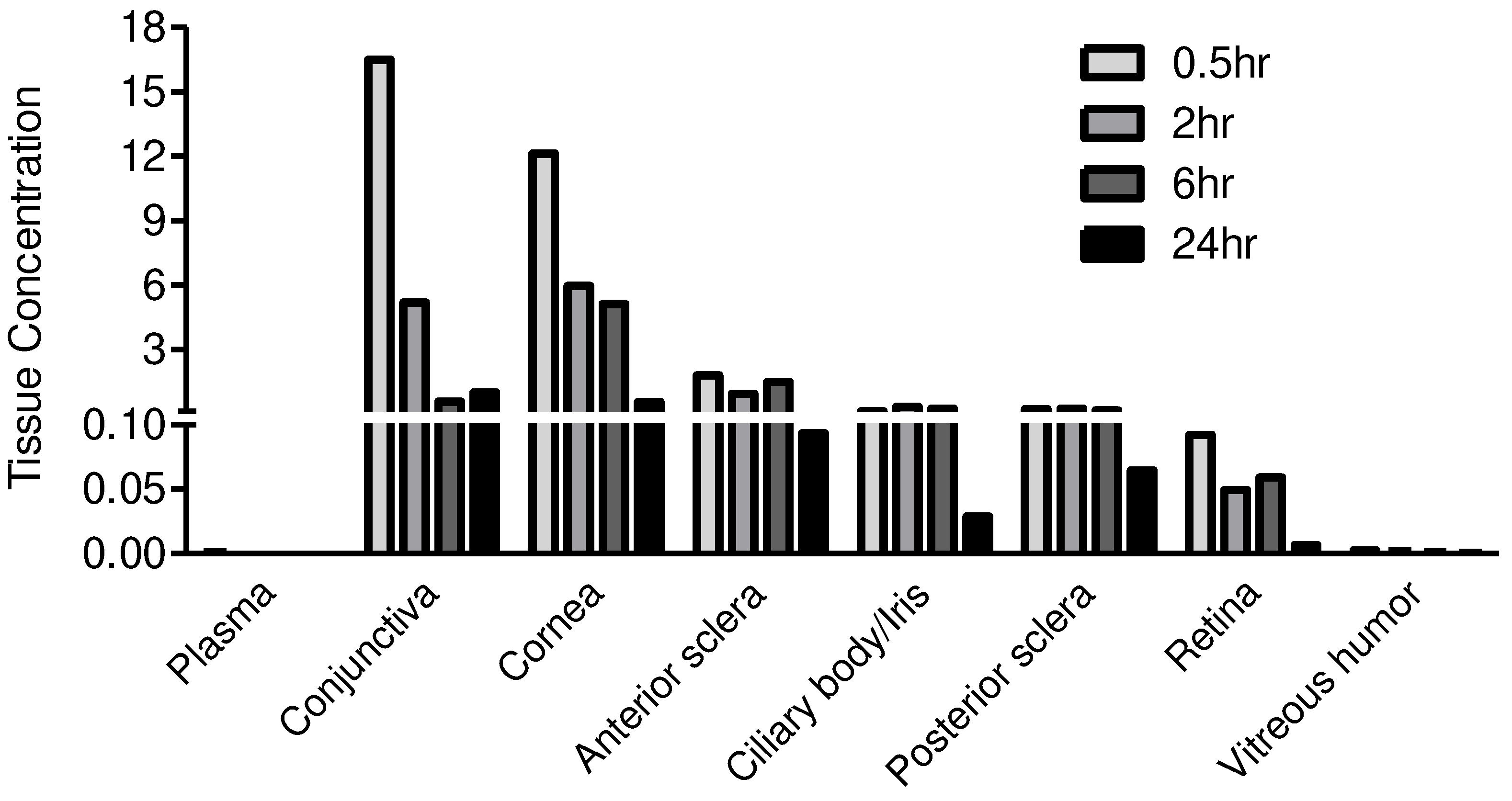
Figure 3.
JV-DE1 bioavailability in monkey plasma and ocular tissues delivered via NIODP. A single dose of JV-DE1 was administered to the right eye (OD) at 165.4µg/eye (mean). Eyelid/periorbital skin is collectively labled as “Eyelid”.N=4 animals in study. The JV-DE1 level is presented as µg/g of solid tissue, or µg/ml of fluid samples.
Figure 3.
JV-DE1 bioavailability in monkey plasma and ocular tissues delivered via NIODP. A single dose of JV-DE1 was administered to the right eye (OD) at 165.4µg/eye (mean). Eyelid/periorbital skin is collectively labled as “Eyelid”.N=4 animals in study. The JV-DE1 level is presented as µg/g of solid tissue, or µg/ml of fluid samples.
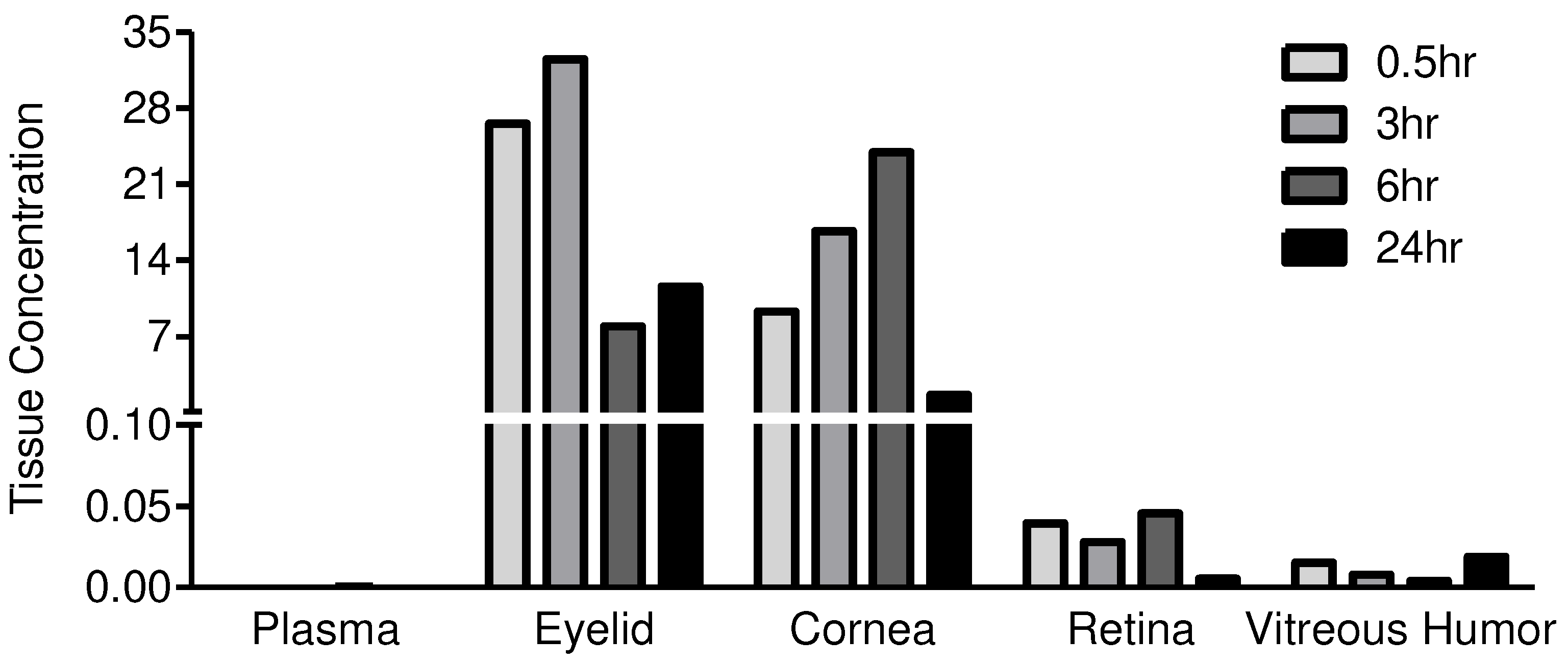
Figure 4.
JV-MD2 bioavailability in monkey plasma and ocular tissues delivered via NIODP. A single dose of JV-MD2 was administered at 6775µg/eye (mean) to the left eye (OS). Eyelid/periorbital skin is collectively labled as “Eyelid”. N=4 animals in study. The JV-MD2 level is presented as µg/g of solid tissue or µg/ml of fluid sample.
Figure 4.
JV-MD2 bioavailability in monkey plasma and ocular tissues delivered via NIODP. A single dose of JV-MD2 was administered at 6775µg/eye (mean) to the left eye (OS). Eyelid/periorbital skin is collectively labled as “Eyelid”. N=4 animals in study. The JV-MD2 level is presented as µg/g of solid tissue or µg/ml of fluid sample.
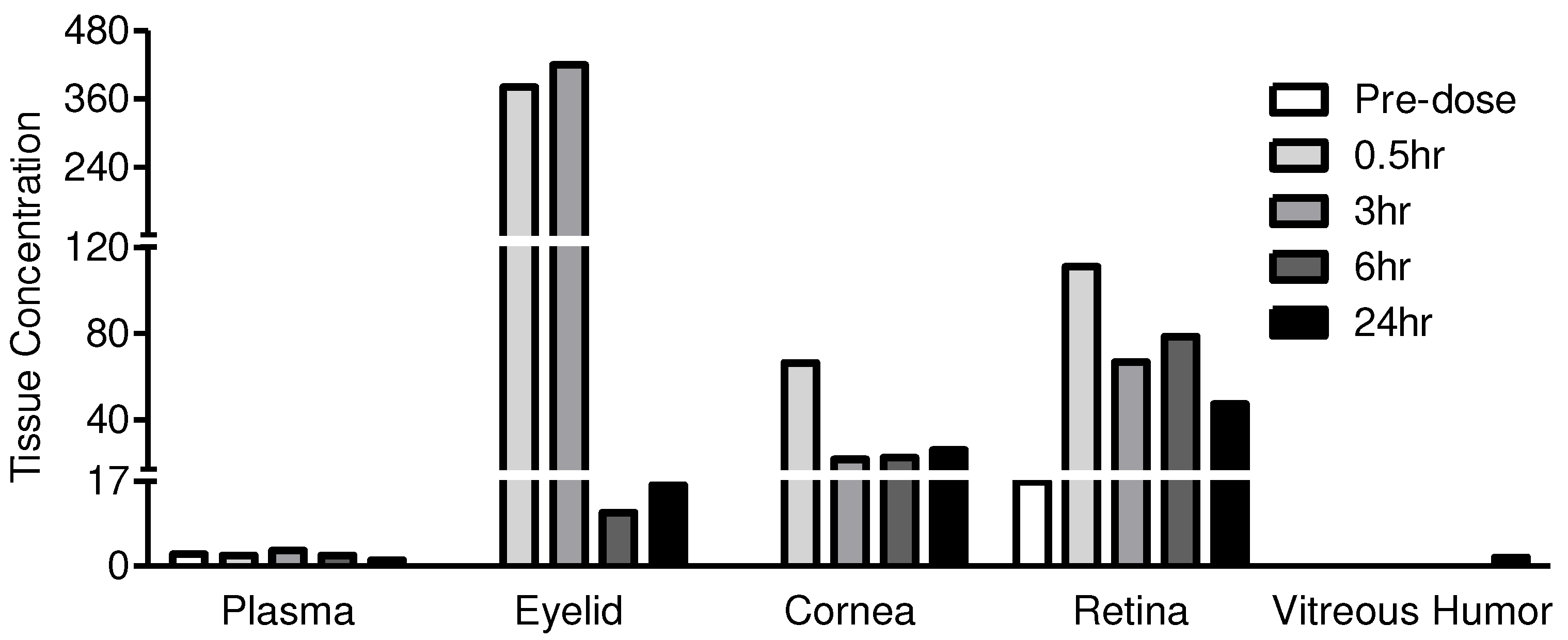
Figure 5.
MOA and pharmacological effects of DHA on AMD. (a) The anti-inflammatory effects of DHA on drusen genesis, proinflammatory cytokine secretion and macrophage accumulation in choroid and retina. (b) DHA molecular target, potency, and retinal delivery efficiency through various routes. IS, immune system; RPE, retinal pigment epithelium; BrM, Bruch's Membrane; MP, macrophages.
Figure 5.
MOA and pharmacological effects of DHA on AMD. (a) The anti-inflammatory effects of DHA on drusen genesis, proinflammatory cytokine secretion and macrophage accumulation in choroid and retina. (b) DHA molecular target, potency, and retinal delivery efficiency through various routes. IS, immune system; RPE, retinal pigment epithelium; BrM, Bruch's Membrane; MP, macrophages.
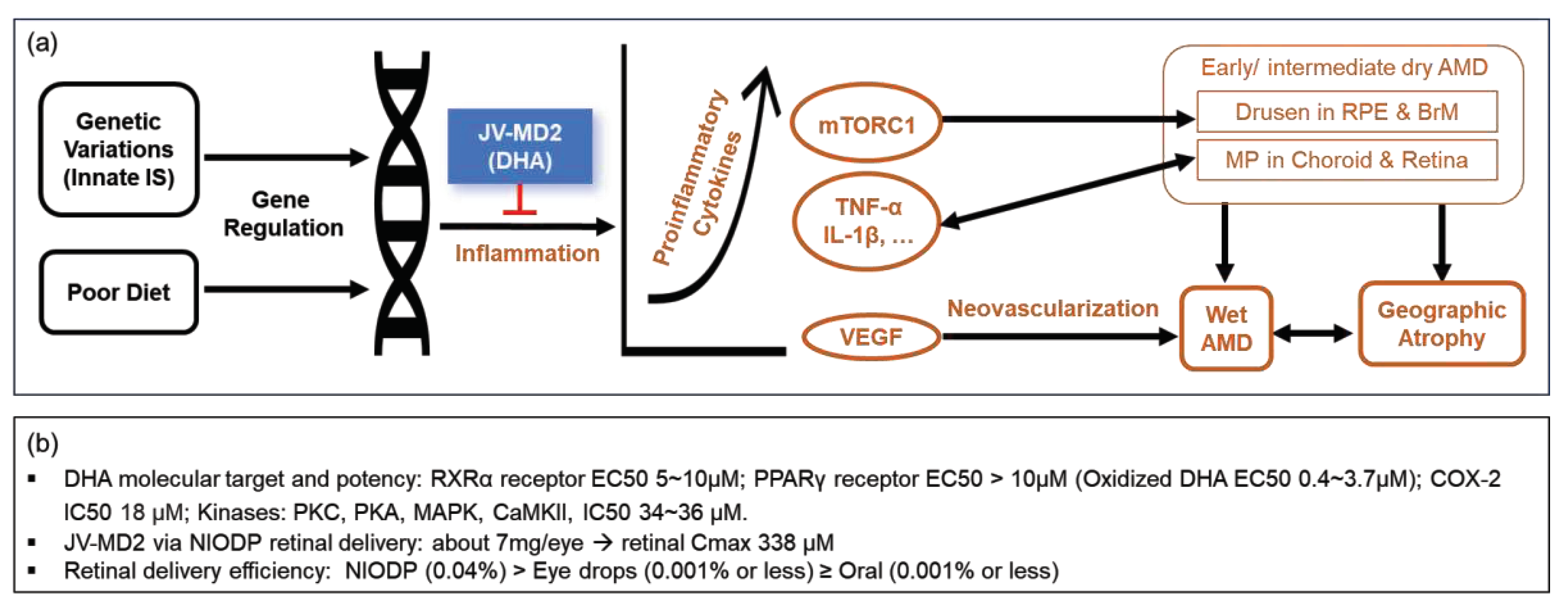

Table 1.
(a) LC conditions for JV-DE1 in rabbit plasma samples. (b) LC conditions for JV-DE1 in rabbit ocular tissues. (c) MS conditions for JV-DE1 in rabbit plasma and ocular tissues.
Table 1.
(a) LC conditions for JV-DE1 in rabbit plasma samples. (b) LC conditions for JV-DE1 in rabbit ocular tissues. (c) MS conditions for JV-DE1 in rabbit plasma and ocular tissues.
| Items | Detail Information | |||||||
|---|---|---|---|---|---|---|---|---|
| (a) | ||||||||
| Column | Waters BEH C18 1.7μm (50×2.10mm) | |||||||
| Column temperature | 50 °C | |||||||
| Auto-sampler temperature | 4 °C | |||||||
| Mobile Phase | MPA: 0.1% Formic Acid (FA) in water MPB: 0.1% Formic Acid (FA) in acetonitrile (ACN) |
|||||||
| Gradient elution | Flow rate | 0.6ml/min | ||||||
| Time/min | MPA (%) | MPB (%) | ||||||
| Initial | 75.0 | 25.0 | ||||||
| 1.30 | 5.0 | 95.0 | ||||||
| 1.75 | 5.0 | 95.0 | ||||||
| 1.76 | 75.0 | 25.0 | ||||||
| 2.00 | 75.0 | 25.0 | ||||||
| Injection Volume | 3μL | |||||||
| (b) | ||||||||
| Column | Waters BEH C18 1.7μm (50×2.10mm) | |||||||
| Column temperature | 50 °C | |||||||
| Auto-sampler temperature | 4 °C | |||||||
| Mobile Phase | MPA: 0.1% FA and 1mM NH4Ac in H2O/ACN (95:5, v:v) MPB: 0.1% FA and 1mM NH4Ac in H2O/ACN (5:95, v:v) |
|||||||
| Gradient elution | Flow rate | 0.6ml/min | ||||||
| Time/min | MPA (%) | MPB (%) | ||||||
| Initial | 60.0 | 40.0 | ||||||
| 1.00 | 2.0 | 98.0 | ||||||
| 1.30 | 2.0 | 98.0 | ||||||
| 1.31 | 60.0 | 40.0 | ||||||
| 1.50 | 60.0 | 40.0 | ||||||
| Injection Volume Valco Valve |
2μL 0.3min: switch into mass, 0.8min: switch into waste |
|||||||
| (c) | ||||||||
| Ion Source | Ion Spray Voltage: 5500V CAD: 10 |
|||||||
| CUR: 40psi | ||||||||
| Gas1: 55psi | ||||||||
| Gas2: 55psi | ||||||||
| Temperature: 450°C (plasma); 550°C (eye tissue and aqueous humor) | ||||||||
| Resolution Q1: unit | ||||||||
| Resolution Q3: unit | ||||||||
| MR Pause: 5.007msec | ||||||||
| Model | ESI, Positive, MRM | |||||||
| Mass Parameters (plasma) |
Analyte and IS | Q1/Q3 | Dwell time (ms) | DP (v) |
EP (v) |
CE (v) |
CXP (v) |
|
| JV-DE1 | 309.8/266.3 | 150 | 150 | 10 | 46 | 13 | ||
| Tolbutamide | 271.1/172.0 | 150 | 70 | 10 | 18 | 13 | ||
| Mass Parameters (eye tissue and aqueous humor) |
Analyte and IS | Q1/Q3 | Dwell time (ms) | DP (v) |
EP (v) |
CE (v) |
CXP (v) |
|
| JV-DE1 | 309.8/266.3 | 80 | 150 | 10 | 46 | 13 | ||
| Tolbutamide | 271.1/172.0 | 80 | 70 | 10 | 18 | 13 | ||
Table 2.
LC/MS process conditions of JV-DE1 in monkey plasma and ocular tissues. LC conditions.
| Time/min | Flow Rate (mL/min) | A% | B% |
|---|---|---|---|
| Initial | 0.6 | 75 | 25 |
| 1.30 | 0.6 | 5 | 95 |
| 1.75 | 0.6 | 5 | 95 |
| 1.76 | 0.6 | 75 | 25 |
| 2.00 | 0.6 | 75 | 25 |
Table 3.
LC/MS process conditions of JV-MD2 (DHA) in monkey plasma and ocular tissues. LC conditions.
Table 3.
LC/MS process conditions of JV-MD2 (DHA) in monkey plasma and ocular tissues. LC conditions.
| Time/min | Flow Rate (mL/min) | A% | B% |
|---|---|---|---|
| Initial | 0.5 | 40 | 60 |
| 2.20 | 0.5 | 10 | 90 |
| 2.50 | 0.5 | 10 | 90 |
| 2.51 | 0.5 | 40 | 60 |
| 2.90 | 0.5 | 40 | 60 |
Table 4.
JV-DE1 in New Zealand Rabbits following a single eye drop administration in the right eye.
| Test Article | JV-DE1 | |||||
|---|---|---|---|---|---|---|
| Dosing site | Topical eye drop (OD) | |||||
| Rabbit ID. | All | 2036281 | 2036282 | 2036283 | 2036281 | |
| Time (h) | 0 | 0.5 | 3 | 6 | 24 | |
| Dose Level (μg/eye) | 0 | 120 | 120 | 120 | 120 | |
| Drug in Plasma (μg/mL) | BLQ | 0.0010 | 0.0003 | 0.0001 | BLQ | |
| Drug in Vitreous humor (μg/mL) | NF | 0.0026 | 0.0017 | 0.0012 | 0.0004 | |
| Drug in OD Tissues (μg/g) |
Conjunctiva | NF | 16.4919 | 5.1781 | 0.5660 | 0.9937 |
| Cornea | NF | 12.1249 | 5.9526 | 5.1255 | 0.5422 | |
| Anterior sclera | NF | 1.7856 | 0.9263 | 1.4785 | 0.0932 | |
| Ciliary body/Iris | NF | 0.1054 | 0.3049 | 0.2314 | 0.0289 | |
| Posterior sclera | NF | 0.2090 | 0.2395 | 0.1512 | 0.0645 | |
| Retina | NF | 0.0920 | 0.0491 | 0.0589 | 0.0068 | |
| Vitreous humor (μg/mL) | NF | 0.0026 | 0.0017 | 0.0012 | 0.0004 | |
| % Administered Dose |
Conjunctiva | 1.3929 | 0.4477 | 0.1288 | 0.1467 | |
| Cornea | 0.8622 | 0.4239 | 0.3709 | 0.0254 | ||
| Anterior sclera | 0.2982 | 0.1068 | 0.2139 | 0.0127 | ||
| Ciliary body/Iris | 0.0084 | 0.0174 | 0.0137 | 0.0021 | ||
| Posterior sclera | 0.0153 | 0.0323 | 0.0197 | 0.0088 | ||
| Retina | 0.0047 | 0.0036 | 0.0037 | 0.0004 | ||
| Vitreous humor | 0.0023 | 0.0012 | 0.0007 | 0.0004 | ||
OD: right eye. BLQ: Below the limit of quantification and was given a value of 0 in relevant calculations; LLOQ: lower limit of quantitation, = 0.0001µg/ml and was given a value of 0 in relevant calculations thereafter. Delivery efficienty = % of administered dose = 100x (Drug Content in Tissue (μg))/Dose Level (μg/eye). NF: not found in undosed animals of various preclinical species (JeniVision data not shown), as JV-DE1 is a synthetic novel chemical entity.
Table 5.
JV-DE1 in Cynomolgus monkeys following a single dose administration via NIODP.
| Test Article | JV-DE1 | |||||
|---|---|---|---|---|---|---|
| Dosing site | Periorbital skin, OD | |||||
| Animal No. | 101 | 101 | 102 | 103 | 104 | |
| Time (h) | 0 | 0.5 | 3 | 6 | 24 | |
| Dose Level (μg/eye) | 0 | 179.1 | 160.6 | 162.2 | 159.3 | |
| Drug in Plasma (μg/mL) | BLQ | 0.0001 | 0.0002 | 0.0003 | BLQ | |
| Drug in OD Tissues (μg/g) |
Eyelid/Periorbital skin | NF | 26.5354 | 32.4547 | 7.9456 | 11.5978 |
| Cornea | NF | 9.2993 | 16.6887 | 23.9295 | 1.6213 | |
| Retina | NF | 0.0396 | 0.0279 | 0.0455 | 0.0055 | |
| Vitreous humor (μg/ml) | NF | 0.0152 | 0.0079 | 0.0039 | 0.0190 | |
| % Administered Dose |
Eyelid/Periorbital skin | 0.6370 | 1.4956 | 0.3477 | 0.7501 | |
| Cornea | 0.1921 | 0.3430 | 0.5900 | 0.0326 | ||
| Retina | 0.0004 | 0.0004 | 0.0005 | 0.0002 | ||
| Vitreous humor | 0.0047 | 0.0029 | 0.0031 | 0.0018 | ||
OD: right eye. BLQ: Below the limit of quantification and was given a value of 0 in relevant calculations. LLOQ: lower limit of quantitation, = 0.0001µg/ml and was given a value of 0 in relevant calculations thereafter. Delivery efficienty = % of administered dose = 100x (Drug Content in Tissue (μg))/Dose Level (μg/eye). NF: not found in undosed animals of various preclinical species (JeniVision data not shown), as JV-DE1 is a synthetic novel chemical entity.
Table 6.
JV-MD2 in Cynomolgus monkeys after a single dose administration via NIODP.
| .Test Article | JV-MD2 (Docosahexaenoic acid, DHA) | |||||
|---|---|---|---|---|---|---|
| Dosing site | Periorbital skin, OS | |||||
| Animal No. | 101 | 101 | 102 | 103 | 104 | |
| Time (h) | 0 | 0.5 | 3 | 6 | 24 | |
| Dose Level (μg/eye) | 0 | 6568 | 6768 | 7018 | 6747 | |
| Drug in Plasma (µg/mL) | 2 | 2 | 3 | 2 | 1 | |
| Drug in OS Tissues (µg/g) |
Eyelid/Periorbital skin | BLQ* | 381 | 420 | 11 | 16 |
| Cornea | BLQ* | 66 | 22 | 22 | 26 | |
| Retina | 17* | 111 | 67 | 79 | 47 | |
| Vitreous humor | BLQ* | 0 | 0 | 0 | 2 | |
| % Administered Dose |
Eyelid/Periorbital skin | 0.4288 | 0.3844 | 0.0149 | 0.0197 | |
| Cornea | 0.0283 | 0.0109 | 0.0149 | 0.0173 | ||
| Retina** | 0.0343 | 0.0264 | 0.0228 | 0.0175 | ||
| Vitreous humor | 0.0000 | 0.0000 | 0.0000 | 0.0236 | ||
OS: left eye. BLQ: Below the limit of quantification and was given a value of 0 in relevant calculations. LLOQ: lower limit of quantitation, =0.5µg/ml and was given a value of 0 in relevant calculations thereafter. Delivery efficiency = % of administered dose = 100x (Drug Content in Tissue (μg))/Dose Level (μg/eye). *Mean of calculated endogenous DHA from the double blank matrix measured during method validation. **Eendogenous DHA was subtracted when calculating % Administered Dose in the retina.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



