Submitted:
11 August 2023
Posted:
15 August 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Suicide is a global public health concern that has enormous social and psychological 1 implications for individuals, families, and communities affected. While the rate of suicide in the 2 UK has remained steady over the years mainly due to the various approaches to detection and 3 management of suicidal ideation, it is still one of the main causes of mortality amongst people 4 between the age of 20 – 34 years. The recent global events such as the COVID-19 pandemic, global 5 warming, war, and various environmental catastrophes means that suicide and suicidal ideation 6 is expected to increase especially among younger people. Thus, evidence-based, population-wide 7 preventative approach will be needed to ameliorate the predicted increase in suicide. Also, to 8 understand the effects of some of the suicide prevention approaches, objective and universal risk 9 assessment approach is required. However, there is no universally accepted preventative approach 10 or tools of assessment. This review examines current advances in suicide prevention in the United 11 Kingdom. It examines the epidemiology, risk factors, as well as the strengths and limitations of 12 the various suicide risk assessment and prevention tools currently in use. We hope to obtain a 13 deeper understanding of how these approaches have evolved and their impact on enhancing mental 14 health and preventing suicide ideation in the UK. We present an in-depth review of existing suicide 15 prevention research and policies, while proposing areas for future research and improvement.16
Keywords:
Suicidal ideation
; Suicide prevention
; Mental health
; COVID- 19
; Public health
1. Introduction
Suicide is a global public health issue that has significant social and psychological consequences for individuals, families, and communities affected by it. The availability of mental health support for people at risk of suicide is crucial in suicide prevention and is of high priority in the United Kingdom [1]. Suicide among children and young people remains particularly worrying, as it is the leading cause of death in the UK for those aged 20–34 [2]. Since the COVID-19 pandemic, suicide has become a serious public health concern, with young people being disproportionately affected [2].
The publication of national suicide prevention strategies for England and Scotland in 2002 demonstrated an increasing understanding of the magnitude of the problem two decades before. These initiatives were designed to bring about reductions in completed suicides in England and Scotland by 2010 and 2013, respectively [3]. During the coalition government, a new strategy document titled "Preventing Suicide in England" was produced in 2012 (Department of Health, 2012). Like the previous 2002 prevention strategy document, the 2012 strategy document set out to reduce suicide rate in the general population across the UK and to provide better support for those bereaved or affected by suicide.
In February 2016, four years after "Preventing Suicide in England" was published, the NHS (National Health Service) Five Year Forward View for Mental Health was published. This marked the start of a ten-year effort to reform mental health care in the UK. The report included a commitment to reduce England’s suicide rate by 10% (relative to 2015 levels) by 2020 (House of Commons Library, 2022). The NHS Long Term Plan (January 2019) indicated that this target is achievable, although in England and Wales, the suicide rate in 2020 has not fallen compared with 2005.
This study will look at the present state of suicide prevention, including major risk factors, trends in annual suicide rate, effectiveness, and limitations of targeted interventions and preventive measures, screening and assessment tools, and future directions. By conducting an in-depth review of current scholarship and national data sources, we hope to provide a comprehensive overview of the suicide landscape in the United Kingdom and identify potential areas for future suicide research and prevention initiatives. We may also gain better understanding of how the various preventive approaches have evolved and their impact on improving mental health and preventing suicidal behaviour across the diverse demographics in the UK population.
2. Epidemiology of Suicide in the UK
The epidemiological research into suicide provides vital insights into the complex patterns, various risk factors, and underlying dynamics of this truly tragic phenomenon. Using data from reputable sources like the Office of National Statistics (ONS), Public Health Scotland (PHS), and Northern Ireland Statistics and Research Agency (NISRA), suicide remains a major problem in the United Kingdom and the world. According to ONS records, there were an estimated 5,583 suicides registered in England and Wales in 2021, which reflects a rate of 10.7 deaths per 100,000 population, which is higher than in 2020 (10.0 per 100,000) but consistent with the pre-pandemic rates in 2018 and 2019. However, the decline in the rate of suicide in 2020 and increase in 202 has been linked to the delays in death registrations due to the COVID-19 pandemic (Office for National Statistics, 2022).
According to Public Health Scotland data, there were 753 probable suicides in Scotland in 2021, which equates to a concerning rate of approximately 13.8 deaths per 100,000 population. In addition, Northern Ireland experienced its highest incidence of suicide deaths since 2015, with 237 reported in 2021. This equates to approximately 14.3 deaths per 100,000 population, a startling increase of 18 deaths (8.2%) from the previous year’s total, indicating a rising trend. The statistics depicts an irregular but bleak picture and emphasise the need for holistic suicide prevention efforts across the United Kingdom.
Suicide rates in the UK exhibit striking disparities between various demographic groups. For instance, males consistently have higher suicide rates than females in the UK. In 2021, the male suicide rate in England and Wales was 16.0 per 100,000 population, an increase of statistical significance from the previous year’s rate of 15.4 per 100,000. Similarly, the death rate for females increased from 4.9 per 100,000 in 2020 to 5.5 per 100,000 in 2021. During the same period, Scotland reported both male and female suicide rates that were especially concerning. According to Public Health Scotland (PHS) statistics for the end of the year 2021, the crude suicide rate for males was 21.2 per 100,000 population, while for females it was 6.7 per 100,000. In comparison to England, Wales, and Scotland, Northern Ireland’s age-standardized rates were significantly higher for both male and female. They report 21.5 suicides per 100,000 population and 7.3 per 100,000 for female, indicating a dire situation that requires immediate attention. Overall, the ratio of male to female suicide rate seems constituent at 3:1 across the UK.
Suicide rates in the UK also differs across different age groups. According to data from the Office for National Statistics (ONS), it is evident that individuals in the middle age group exhibit the highest rates of suicide in England and Wales. The highest age-specific suicide rate for females was among those aged 45 to 49 (7.8 deaths per 100,000), while for males it was between those aged 50 and 54 (22.7 deaths per 100,000) (Office for National Statistics, 2022).
Similarly, Scotland saw a troubling pattern among middle-aged men and women aged 45 to 54, who had particularly high age-specific suicide rates. According to PHS, there were around 32.3 male deaths per 100,000 population in this demographic group, which is almost three times more than the females, who had an average rate of 11.2 per 100,000 (Public Health Scotland, 2022) and 50% more than those recorded in England and Wales. Unfortunately, statistics on Northern Ireland’s suicide rate by age-group and per 100,000 population are currently unavailable; nonetheless, for men, the age ranges with the highest number of suicides are 25-29 (22 deaths) and 45-49 (22 deaths), while for females, the age ranges with the highest number of suicides are 20-24 (10 deaths) and 50-54 (8 fatalities) (Statistics Unit NISRA, 2022).
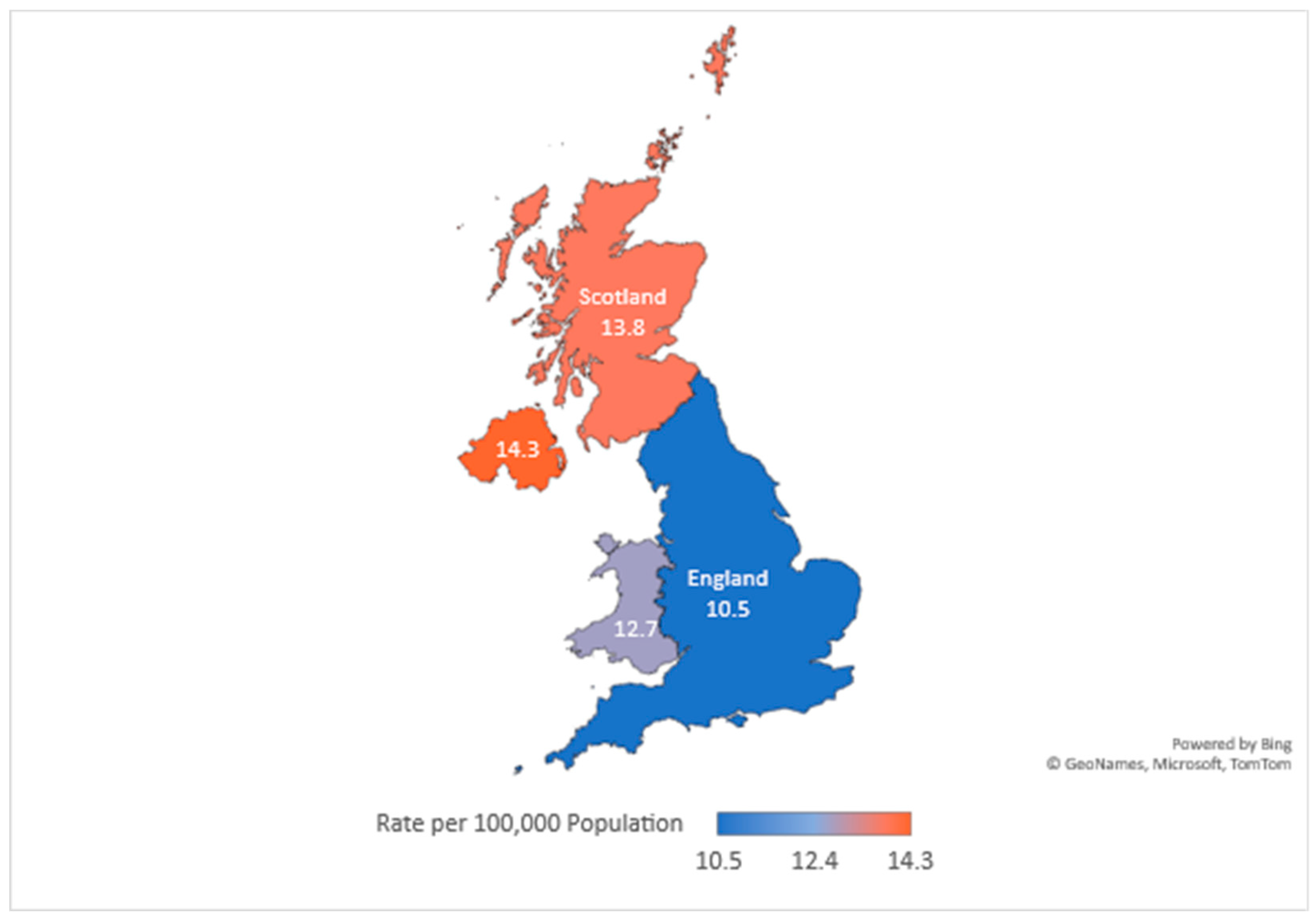
Figure 1.
Suicide rate per 100,000 people in the United Kingdom showing the variation across England, Northern Ireland, Scotland, and Wales. The figure is based on publicly available data on the number of registered deaths due to suicide in the year 2022.
Figure 1.
Suicide rate per 100,000 people in the United Kingdom showing the variation across England, Northern Ireland, Scotland, and Wales. The figure is based on publicly available data on the number of registered deaths due to suicide in the year 2022.
3. Risk Factors for Suicide
Suicide risk in the UK is influenced by a variety of causes which may be environmental, individual and/or clinical in nature [4]. The environmental triggers could be due to societal structure, community dynamics, and negative or lack of relationships while individual factors include mental disorders, economic shock, chronic diseases etc [5]. Generally, suicidal behaviour is strongly associated with mental health disorders, notably depression, social isolation, drug addiction, prior suicide attempts, and socioeconomic disadvantage among others [6]. The link between psychiatric disorders and suicide is has been extensively studied and established even though suicide is not a disorder. Indeed, around 90% patients who died of suicide have been shown experimentally to have some sorts of mental disorder [7,8].
One of the most common mental disorders associated with suicidal thoughts and suicide is depression. The term depression defines a persistent mood disorder characterized by elongated period of sadness, high irritability, loss of interest, emptiness and low motivation that may result in poor cognitive and physical functioning (2021). Thus, unipolar depression may lead to inability to perform daily responsibility and was estimated in 2002 by the World Health Organization (WHO) as the fourth highest cause of global disability and predicted to possibly rise to second place by 2030 [9]. Aside from the physical effect of depression, persistent and chronic course of depression has been linked with suicidality and suicide. For instance, in a previous study that investigated the link between depression and suicide, Handley et al showed a significant correlation between depression severity and suicidality which was independent of sex. However, duration of depression and the presence and number of psychiatric comorbidities were the only factors linked with suicide attempts [10]. This finding corroborated a previous similarly aimed study which reported that repeated self-harm is mainly linked with longer or repeated exposure to adverse childhood experience [11].
Further, social isolation, which describes the feeling of not belonging to one’s immediate social environment exemplified by lone living, self-reported loneliness, few or no friends, broken or conflicting family, social withdrawal, is a major driver of suicidal behaviour and suicide [12,13,14]. Indeed, the feeling of belongingness and social integration is classically considered a protective factor which is inversely correlated with suicide (Durkheim, 1951). In a study involving over 500,000 adults between the age of 37 and 73 living in the UK, Shaw et al showed that loneliness especially in single men (living alone or with non-partner) increases the risk of death by suicide [15]. Thus, corroborating a previous study performed in Germany, which showed an increased risk of suicide linked with lone-living [16]. In a recent meta-analysis of 40 studies by Calati et al, objective and subjective social isolation were found to be significantly linked with suicidal thought and behaviour [12].
There is a body of evidence showing a strong link between drug dependence and an increased risk suicide [17,18,19]. For instance, according to the 2010 Global Burden of Disease Study, alcohol misuse is the second leading risk factor for mental-health-related suicide, surpassed only by depression (Ferrari et al., 2014). Further, cocaine dependence was shown by Pavarin and Fioritti as a major risk factor for suicide in Italy [20]. Drug dependence is generally defined as a persistent, strong, and uncontrollable tendency to take substances and characterized by physical, social, physiological, and psychological dysfunction [21,22]. In a study performed by Oyefeso et al on 298 suicide cases, drug addiction was shown to be a significant driving factor for suicide in the UK [23]. This was recently corroborated by Bailey et al who reported an increased risk of suicide in adults with high blood alcohol concentration and cocaine use [24].
While depression and drug dependency are the main risk factors of suicide both in the UK and globally, other factors such as previous suicide attempt, socioeconomic disadvantage (e.g., poverty, financial debt, unstable family, poor education job loss etc) also contributes significantly to suicide (see [25] for more).
4. Screening and Assessment Tools
Effective suicide prevention is a complex approach that involves rigorous screening and thorough assessment of those at risk. Suicide assessment tools or instruments are critical in the early identification and assessment of people who have suicidal tendencies [26]. Suicide assessment and screening instruments include self-reporting questionnaires, interviews, and clinician-administered assessments among others. Several criteria must be examined to make an accurate assessment of suicide risk. Variables such as previous suicide attempts, psychiatric history, present mental health condition, and access to means of self-harm are all factors to consider [27].
Healthcare professionals can better understand an individual’s degree of susceptibility and design appropriate intervention strategies by obtaining information on these aspects through effective screening approaches. It is important to note that the effectiveness of suicide prevention measures may differ across regions or countries due to social or cultural factors influencing opinions and views towards mental health disorders, including suicide [28]. Indeed, several screening and assessment instruments have been developed and implemented in the United Kingdom to support healthcare professionals in identifying those at risk of suicide.
- The Columbia-Suicide Severity Rating Scale (C SSRS)
The Columbia-Suicide Severity Rating Scale (CSSRS) is a 19-item questionnaire commonly used instrument to assess suicidal ideation and behaviour. It assesses the intensity, duration, and frequency of suicidal ideation, as well as past suicide attempts, through a series of detailed queries [29]. The CSSRS has demonstrated high levels of validity and reliability and is utilised in a variety of research and clinical settings (Jang, et al. 2014). For instance, in a population of 1451 patients with Huntington’s disease from various European countries (including the UK), van Duijin et al successfully used CSSRS to detect suicidal ideation and behaviour [30]. Further, Manning et al showed the C-SSRS as a valuable tool in assessing suicidal ideation and behaviour and correlated well with the Children and Young People-Mental Health Self-Harm Assessment in Paediatric healthcare Environments (CYP-MH SAPhE) scale [31]. However, the CSSRS has several limitations associated with self-reporting including recall error. Also, as suicidal ideation fluctuates over time, it may not convey the dynamic nature of suicide risk [32,33]. Indeed, in a study assessing the ability of the C-SSRS to accurately and fully assess suicidal ideation and behavioural spectrum, Giddens et al purported the scale to be “conceptually and psychometrically flawed” [34].
- SuicideIdeation Questionnaire (SIQ)
The Suicide Ideation Questionnaire (SIQ) is a commonly utilised self-report instrument for assessing the severity of suicidal ideation in adult as well as in children and young people. In addition to the standard SIQ questionnaire, there are two other SIQ forms: a 30-item high school form for students in grades 10 through 12 (15–18 years old) and a 15-item junior high school form for children in grades 7–9 (12–14 years old), also refer to as SIQ-JR [35]. It provides a structured method for measuring the frequency, duration, and intensity of suicidal ideation. The SIQ has demonstrated excellent psychometric properties, making it applicable in clinical and research settings. The efficacy of dialectical behaviour therapy (DBT) for adolescents at risk of suicide was investigated in a randomised control trial conducted by McCauley et al. The assessment of suicidal ideation was performed using the SIQ-JR form, with a sample size of 173 participants aged between 12 and 18 years [36]. As with other self-report measures, the SIQ may be susceptible to response biases and may not reflect the complex and dynamic nature of suicide risk, which may influence its evaluation [35].
- Beck Scale for Suicide Ideation (B SSI)
The Beck Scale for Suicide Ideation (SSI) is a commonly employed self-report measure that assesses the intensity of suicidal ideation, comparable to the (SIQ). It evaluates a person’s attitude towards and preparedness for suicide. The SSI is practicable and simple to administer, making it appropriate for clinical and research applications. In research by Zhang and Brown, they examined high school students (n = 292) in China’s rural areas using the Chinese translation of the Scale for Suicide Ideation. The findings showed that the SSI had good item-total correlations and internal reliability. These results showed that the SSI is a highly reliable psychometric tool for assessing suicidal thoughts in Chinese populations [37]. As a self-reporting instrument, the SSI may be susceptible to response biases and may not adequately capture the multifaceted elements that make up the risk of suicide. This is a significant limitation of self-reporting assessment instruments [38].
- ManchesterSelf-Harm Rule (MSHR)
The Manchester Self-Harm Rule (MSHR) is a clinical instrument designed for predicting the likelihood of future suicide attempts following self-harm presentations. It incorporates multiple risk factors indicators, such as previous self-harm, age, and gender, to identify high-risk individuals. A risk-stratification model was created for emergency department (ED) clinicians to use in assessing patients who present with thoughts of self-harm The instrument yields encouraging results and may aid in ED evaluation and the provision of psychiatric services to patients at higher risk [39]. While the MSHR has demonstrated high levels of sensitivity and specificity, its applicability to a variety of populations and settings requires additional research [39].
- EcologicalMomentary Assessment (EMA)
Ecological Momentary Assessment (EMA) is the process of gathering real-time data on people’s thoughts, feelings, and behaviours using mobile devices. It routinely checks people’s psychological and behavioural features in real-time for a set length of time [40]. Technological advances have increased the feasibility of EMA measures: instead of undergoing assessments based on retrospective self-report or performed in non-representative laboratory settings, participants can now provide time and context-specific data via their smartphones. The EMA is a potentially beneficial tool in clinical practise, but it is not without limitations, such as questionnaire fatigue and issues regarding ethics [41,42].
- Other assessment tools
For adequate prevention of suicidal ideation and suicide, the usefulness good assessment tool cannot be overemphasized. Indeed, aside from the ones mentioned above, various other suicide assessment tools have been successfully used both in the UK and around the world. This includes the adolescent version of the suicide probability scales (SPS), developed in in 1989 by Cull and Gill [43] and later modified by Go et al [44], and covers four main assessments for homelessness, hostility, negative evaluation of self, and suicidal ideation. The SPS is mainly limited by lack of data on its validity. Also, the Beck hopelessness scale (BHS) measures overall negative perception of the future (pessimism). BHS was developed by Beck et al in 1974 [45] and validated by Kim et al [46] recently in 2015 with reported good test-retest reliability and validity in predicting depression and anxiety. Also worth mentioning are the Reasons for Living scales [47,48,49,50], Screening for Depression and Thoughts of Suicide scale [51], Suicidal Imagery Questionnaire [52], Depressive Symptom Inventory-Suicidality Subscale (Joiner Jr et al., 2002), Suicide Risk Scale for Medical Inpatients [53] etc. For a comprehensive review on the various tools available for assessment of suicidal ideation and suicide please see [54,55].
Machine Learning in Suicide prevention
In recent years, machine learning and artificial intelligence have been used extensively in suicide research and prevention especially in terms of data generation through algorithms such as natural language processing (NLP), that use existing data from physical clinical records and electronic health records (EHRs) for the identification of people at higher risk of suicide. Indeed, computational algorithms based on NLP can provide a low-cost and resource-efficient alternative to more expensive methods according to a recent systematic review [56]. Machine learning (ML) is a branch of artificial intelligence (AI) that describes various algorithms, associated with the efficient handling of data (especially big data) to perform various human task in logical and reproducible manner (Jordan and Mitchell 2015; Mahesh 2020). Such task may include prediction of outcomes (prognosis), or detection of events (diagnosis) often below the threshold of human detection.
In the context of suicide research, machine learning (ML) has typically been applied to the prediction or intervention of suicide cases. In a South London hospital, Cliffe et al. applied machine learning techniques to electronic health records. The study found that attribute agreements for the precision of positive mentions of self-harm were 0.96 and for suicidality they were 0.80, demonstrating the dependability of the tools for identifying EHRs reporting self-harm or suicidal behaviour [57]. Another study, by Mens et al, used machine learning to predict suicide behaviour using general practise data. Their study utilised data from a nationwide representative primary care database including over 1.5 million patients to develop a risk stratification model that accurately identified individuals at high risk for suicide behaviour [58]. These machine-learning approaches have shown promise in enhancing the accuracy of suicide risk assessment by integrating diverse data sources and identifying patterns that may not be identifiable using conventional statistical methods.
Further, social media sites create massive volumes of user-generated content that can be used for suicide risk assessment. For detecting people at risk, machine learning algorithms can analyse language patterns, mood, and other indications in social media posts. For instance, [59] developed an algorithm that analysed tweets to predict suicide risk among young adults. Such techniques have the potential to provide early diagnosis and intervention for at-risk individuals using their historical data like Facebook posts or tweets.
Mobile Applications for suicide prevention.
The proliferation of mobile technology has present unique opportunities for the provision of mental health care and the implementation of suicide prevention measures. Mobile devices can support the deployment of personalised applications, commonly known as apps, which offer various functionalities such as emotional assistance, self-reporting, and behavioural coaching. Mobile applications have demonstrated significant potential in facilitating suicide prevention interventions due to their capacity to provide immediate support and interventions during critical moments and in real-life situations. This is particularly valuable given the volatile nature of suicide ideation and behaviour, which can change very quickly [60,61]. Indeed, mobile phones and mobile applications (apps) have gained significance in suicide prevention initiatives in recent years, providing new and accessible methods for screening and evaluation.
The "Stay Alive" app, created by Grassroots Suicide Prevention, is one of the most popular smartphone apps in the United Kingdom. The NHS has validated the app, which is intended to assist people in crisis with quick help and services. The app includes information on local crisis helplines, self-help strategies, a safety plan, and a LifeBox in which users can keep important pictures and memories (NHS England » Stay Alive, n.d.). The "Stay Alive" app is a portable and accessible resource that allows users to get help when they need it. Apart from Stay Alive, ReMinder is another app that has gain popularity, ReMinder is an app that provides users with a configurable template to build their safety plan using a combination of free text and pre-added options. The software assesses the user’s mood with a self-reported depressive test (K-10), allows users to store multimedia content for use in a crisis, gives information via a Tweeter feed, and provides users with access to emergencies helplines and members of the user’s support network via the smartphone application [62].
Torok et al. found in a randomised controlled trial that self-guided digital interventions that directly target suicidal ideation are efficacious immediately post-intervention. Indirect interventions (targeting depression rather than suicide) did not significantly reduce suicidal ideation. The study also suggests that digital interventions should be promoted and extensively disseminated, particularly in areas where access to health services is limited or non-existent [63]. Apart from mobile apps, emerging digital technologies such as online platforms, chatbots, and virtual reality have also shown promise in suicide prevention [64,65]. In their research, Lin et al. construct a virtual reality group counselling (VRGC) system that can be used to help students alleviate school-related stress [66]. The research demonstrates promising results and provides a platform for future clinical trials to evaluate and enhance the automated virtual reality chatbot counselling system. These digital tools provide individuals at risk with accessible and cost-effective means of receiving support, information, and interventions at any time and place. Although there are some encouraging ways to using apps and other digital solutions for suicide prevention and follow-up, the technical and human components have yet to be studied and analysed. For example, health professionals should be encouraged to support the design and development of applications that aid in suicide prevention in order to humanise these apps and improve the success of the intervention they support [67].
5. Conclusion and Future Directions
This review study has shown important developments in suicide prevention in the UK, highlighting the significance of comprehensive and integrated approaches to this urgent public health issue. Despite the recent significant advances, there are still important areas that need additional research and development for more successful preventative efforts.
Firstly, using digital technology to reach those who are at risk of suicide has demonstrated to be quite promising. To evaluate the effectiveness of mobile applications particularly designed for preventing suicidal ideation, additional study is however required. We can better understand these applications’ potential significance in suicide prevention and adapt their capabilities to meet the varied requirements of at-risk populations by undertaking rigorous studies to assess their effect and integration with current mental health services.
Furthermore, various age groups, genders, and ethnicity have significantly varying suicide prevalence rates, necessitating personalised interventions to address the problems that certain demographic groups face. The prevention of suicide would not be successful with a one-size-fits-all strategy. To make sure that preventive efforts are more suited to and accessible to vulnerable populations, future research should concentrate on creating and assessing culturally sensitive and demographic-specific interventions.
Additionally, it is crucial that we improve data gathering techniques to deepen our understanding of suicide trends and risk factors. To find discrepancies and create specialised preventive efforts, statistics on suicide must regularly contain demographic information, such as race and religious views. Additionally, uniform data collecting across the UK is essential for more accurate comparisons and assessments. England, Wales, Scotland, and Northern Ireland must work together to simplify data gathering procedures and guarantee a comprehensive strategy for suicide prevention on a national level.
Consequently, the development and deployment of several suicide screening and assessment tools has aided advances in suicide prevention in the UK. Among the commonly used tools are the Columbia-Suicide Severity Rating Scale, Manchester Self-Harm Rule, Suicide Ideation Questionnaire, and Beck Scale for Suicide Ideation, each with its own strengths and limitations. Furthermore, new tools such as the Ecological Momentary Assessment (EMA), machine learning and artificial intelligence-based algorithms, and mobile applications such as the "Stay Alive", “ReMinder” apps provide new prospects for enhanced suicide risk assessment and prevention. Continued study and assessment are required to improve the accuracy, efficacy, and accessibility of these tools, which will ultimately contribute to a reduction in the number of suicides in the UK.
Finally, this review emphasises the need of continued research and collaborative efforts in promoting suicide prevention in the UK. We can make substantial steps in reducing the impact of suicide and establishing a culture that prioritises mental health and well-being for all by investing in novel digital tools, tailored interventions, and enhanced data gathering practises. Policymakers, academics, and stakeholders must collaborate to adopt evidence-based practises and create a comprehensive and humane strategy to suicide prevention across the country.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Alves, V.M.; Francisco, L.C.; Melo, A.R.D.; Novaes, C.R.; Belo, F.M.; Nardi, A.E. Trends in suicide attempts at an emergency department. Revista Brasileira de Psiquiatria 2017, 39, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Maguire, A.; Ross, E.; Reilly, D. Parental mental health and risk of poor mental health and death by suicide in offspring: A population-wide data-linkage study. Epidemiology and Psychiatric Sciences 2022, 31. [Google Scholar] [CrossRef] [PubMed]
- K.K., *!!! REPLACE !!!*; Pillai, J.S.S.K.; Gill, K.O. K.K.; Pillai, J.S.S.K.; Gill, K.O.; & Hui.; Swami., 2010.
- Turecki, G.; Brent, D.A.; Gunnell, D.; O’connor, R.C.; Oquendo, M.A.; Pirkis, J.; Stanley, B.H. Suicide and suicide risk. Nature Reviews Disease Primers 2019, 5. [Google Scholar] [CrossRef] [PubMed]
- Health, W. ; O., 2014.
- Zakowicz, P.; Skibin´ska, M.; Wasicka-Przewoz´na, K.; Skulimowski, B.; Was´niewski, F.; Chorzepa, A.; Róz˙an´ski, M.; Twarowska- Hauser, J.; Pawlak, J. Impulsivity as a Risk Factor for Suicide in Bipolar Disorder. Frontiers in Psychiatry 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Arsenault-Lapierre, G.; Kim, C.; Turecki, G. Psychiatric diagnoses in 3275 suicides: A meta-analysis. BMC Psychiatry 2004, 4, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Bertolote, J.M.; Fleischmann, A. Suicide and psychiatric diagnosis: A worldwide perspective. World Psychiatry 2002, 1, 181–181. [Google Scholar]
- Mathers, C.D.; Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med 2006, 3. [Google Scholar] [CrossRef]
- Handley, T.; Rich, J.; Davies, K.; Lewin, T.; Kelly, B. The challenges of predicting suicidal thoughts and behaviours in a sample of rural Australians with depression. International Journal of Environmental Research and Public Health 2018, 15, 928–928. [Google Scholar] [CrossRef]
- Cleare, S.; Wetherall, K.; Clark, A.; Ryan, C.; Kirtley, O.J.; Smith, M.; Connor, R.C. Adverse childhood experiences and hospital-treated self-harm. International Journal of Environmental Research and Public Health 2018, 15, 1235–1235. [Google Scholar] [CrossRef]
- Calati, R.; Ferrari, C.; Brittner, M.; Oasi, O.; Olié, E.; Carvalho, A.F.; Courtet, P. Suicidal thoughts and behaviors and social isolation: A narrative review of the literature. Journal of Affective Disorders 2019, 245, 653–667. [Google Scholar] [CrossRef]
- Joiner, T.E. , 2005.
- Orden, K.A.V.; Witte, T.K.; Cukrowicz, K.C.; Braithwaite, S.R.; Selby, E.A.; Joiner, T.E. The interpersonal theory of suicide. Psychological Review 2010, 117, 575–575. [Google Scholar] [CrossRef] [PubMed]
- Shaw, R.J.; Cullen, B.; Graham, N.; Lyall, D.M.; Mackay, D.; Okolie, C.; Pearsall, R.; Ward, J.; John, A.; Smith, D.J. Living alone, loneliness and lack of emotional support as predictors of suicide and self-harm: A nine-year follow up of the UK Biobank cohort. Journal of Affective Disorders 2021, 279, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Näher, A.F.; Rummel-Kluge, C.; Hegerl, U. Associations of Suicide Rates With Socioeconomic Status and Social Isolation: Findings From Longitudinal Register and Census Data. Frontiers in Psychiatry 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Miles, C.P. Conditions predisposing to suicide: A review. The Journal of Nervous and Mental Disease 1977, 164, 231–246. [Google Scholar] [CrossRef] [PubMed]
- Miller, N.S.; Mahler, J.C.; Gold, M.S. Suicide risk associated with drug and alcohol dependence. Journal of Addictive Diseases 1991, 10, 49–61. [Google Scholar] [CrossRef]
- Yuodelis-Flores, C.; Ries, R.K. Addiction and suicide: A review. The American Journal on Addictions 2015, 24, 98–104. [Google Scholar] [CrossRef]
- Pavarin, R.M.; Fioritti, A. Mortality trends among cocaine users treated between 1989 and 2013 in northern Italy: Results of a longitudinal study. Journal of Psychoactive Drugs 2018, 50, 72–80. [Google Scholar] [CrossRef]
- Hasin, D.; Hatzenbuehler, M.L.; Keyes, K.; Ogburn, E. Substance use disorders: Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) and International Classification of Diseases. Addiction 2006, 101, 59–75. [Google Scholar] [CrossRef]
- Miyasato, K. Nihon Rinsho 2010, 68, 1431–1436. 68.
- Oyefeso, A.; Ghodse, H.; Clancy, C.; Corkefy, J.M. Suicide among drug addicts in the UK. The British Journal of Psychiatry 1999, 175, 277–282. [Google Scholar] [CrossRef]
- Bailey, J.; Kalk, N.J.; Andrews, R.; Yates, S.; Nahar, L.; Kelleher, M.; Paterson, S. Alcohol and cocaine use prior to suspected suicide: Insights from toxicology. Drug and Alcohol Review 2021, 40, 1195–1201. [Google Scholar] [CrossRef]
- Haw, C.; Hawton, K.; Niedzwiedz, C.; Platt, S. , 2013.
- Bond, K.S.; Cottrill, F.A.; Mackinnon, A.; Morgan, A.J.; Kelly, C.M.; Armstrong, G.; Kitchener, B.A.; Reavley, N.J.; Jorm, A.F. Effects of the Mental Health First Aid for the suicidal person course on beliefs about suicide, stigmatising attitudes, confidence to help, and intended and actual helping actions: An evaluation. International Journal of Mental Health Systems 2021, 15. [Google Scholar] [CrossRef] [PubMed]
- Parameshwaraiah, S.T.; Manohar, S.; Thiagarajan, K. SUICIDE ATTEMPTS AND RELATED RISK FACTORS IN PATIENTS ADMITTED TO TERTIARY CARE CENTRE IN SOUTH INDIA. Journal of Evolution of Medical and Dental Sciences 2018, 7, 2916–2920. [Google Scholar] [CrossRef]
- Azizabadi, Z.; Aminisani, N.; Emamian, M.H. Socioeconomic inequality in depression and anxiety and its determinants in Iranian older adults. BMC Psychiatry 2022, 22. [Google Scholar] [CrossRef] [PubMed]
- Posner, K.; Brent, D.; Lucas, C.; Gould, M.; Stanley, B.; Brown, G.; Fisher, P.; Zelazny, J.; Burke, A.; Oquendo, M. Columbia-suicide severity rating scale (C-SSRS); Vol. 10, 2008.
- Duijn, E.V.; Vrijmoeth, E.M.; Giltay, E.J.; Landwehrmeyer, G.B. Suicidal ideation and suicidal behavior according to the C-SSRS in a European cohort of Huntington’s disease gene expansion carriers. Journal of Affective Disorders 2018, 228, 194–204. [Google Scholar] [CrossRef]
- Manning, J.C.; Carter, T.; Walker, G.; Coad, J.; Aubeeluck, A. Assessing risk of self-harm in acute paediatric settings: A multicentre exploratory evaluation of the CYP-MH SAPhE instrument. BMJ Open 2021, 11. [Google Scholar] [CrossRef]
- Lindh, Å.U.; Waern, M.; Beckman, K.; Renberg, E.S.; Dahlin, M.; Runeson, B. Short term risk of non-fatal and fatal suicidal behaviours: The predictive validity of the Columbia-Suicide Severity Rating Scale in a Swedish adult psychiatric population with a recent episode of self-harm. BMC Psychiatry 2018, 18. [Google Scholar] [CrossRef]
- Posner, K.; Brown, G.K.; Stanley, B.; Brent, D.A.; Yershova, K.V.; Oquendo, M.A.; Currier, G.W.; Melvin, M.A.G.; Greenhill, L.; Shen, S.; et al. , 2011.
- Giddens, J.M.; Sheehan, K.H.; Sheehan, D.V. The Columbia-Suicide Severity Rating Scale (C-SSRS): Has the ‘Gold Standard’ Become a Liability? Innov Clin Neurosci 2014, 11, 66–80. [Google Scholar]
- Reynolds, W.M. Suicidal ideation questionnaire (SIQ). Psychological Assessment Resources 1987. [Google Scholar]
- Mccauley, E.; Berk, M.S.; Asarnow, J.R.; Adrian, M.; Cohen, J.; Korslund, K.; Avina, C.; Hughes, J.; Harned, M.; Gallop, R.; et al. , 2018.
- Zhang, J.; Brown, G.K. Psychometric properties of the scale for suicide ideation in China. Archives of Suicide Research 2007, 11, 203–210. [Google Scholar] [CrossRef]
- Beck, A.T.; Kovacs, M.; Weissman, A. Assessment of Suicidal Intention: The Scale for Suicide Ideation. Journal of Consulting and Clinical Psychology 1979, 47, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.; Kapur, N.; Dunning, J.; Guthrie, E.; Appleby, L.; Mackway-Jones, K. A Clinical Tool for Assessing Risk After Self-Harm. Annals of Emergency Medicine 2006, 48, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Gee, B.L.; Han, J.; Benassi, H.; Batterham, P.J. , 2020.
- Kivelä, L.; Does, W.A.J.V.D.; Riese, H.; Antypa, N. , 2022.
- Sedano-Capdevila, A.; Porras-Segovia, A.; Bello, H.J.; Baca-García, E.; Barrigon, M.L.; Barrigon, M.L. SECTION EDITOR) Use of Ecological Momentary Assessment to Study Suicidal Thoughts and Behavior: A Systematic Review; 2021.
- Cull, J.G.; Gill, W.S. Suicide probability scale. Journal of Consulting and Clinical Psychology 1988. [Google Scholar]
- Go, H.J.; Kim, D.J.; Lee, H.P. A validation study of the suicide probability scale for adolescents (SPS-A). Journal of Korean Neuropsychiatric Association 2000, 680–690. [Google Scholar]
- Beck, A.T.; Weissman, A.; Lester, D.; Trexler, L. The measurement of pessimism: The hopelessness scale. Journal of Consulting and Clinical Psychology 1974, 42, 861–861. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Lee, E.H.; Hwang, S.T.; Hong, S.H.; Lee, K.; Kim, J.H. Reliability and validity of the Korean version of the Beck Hopelessness Scale. Journal of Korean Neuropsychiatric Association 2015, 54, 84–90. [Google Scholar] [CrossRef]
- Gutierrez, P.M.; Osman, A.; Barrios, F.X.; Kopper, B.A.; Baker, M.T.; Haraburda, C.M. Development of the reasons for living inventory for young adults. Journal of Clinical Psychology 2002, 58, 339–357. [Google Scholar] [CrossRef]
- Linehan, M.M.; Goodstein, J.L.; Nielsen, S.L.; Chiles, J.A. Reasons for staying alive when you are thinking of killing yourself: The reasons for living inventory. Journal of Consulting and Clinical Psychology 1983, 51, 276–276. [Google Scholar] [CrossRef]
- Osman, A.; Kopper, B.A.; Barrios, F.X.; Osman, J.R.; Besett, T.; Linehan, M.M. The brief reasons for living inventory for adolescents (BRFL-A). Journal of Abnormal Child Psychology 1996, 24, 433–443. [Google Scholar] [CrossRef]
- Westefeld, J.S.; Cardin, D.; Deaton, W.L. Development of the college student reasons for living inventory. Suicide and Life-Threatening Behavior 1992, 22, 442–453. [Google Scholar]
- Kim, J.; Kang, E.; Jeong, J.W.; Paik, J.W. Korean suicide risk screening tool and its validity. The Journal of the Korea Contents Association 2013, 13, 240–250. [Google Scholar] [CrossRef]
- Ko, S.; You, S. Development and validation of the suicidal imagery questionnaire. Kor J Clin Psychol 2020, 39, 1–14. [Google Scholar] [CrossRef]
- Park, S.W.; Lee, J.H.; Lee, E.K.; Song, J.J.; Park, H.S.; Hwang, S.Y.; Lee, M.S. Development of the suicide risk scale for medical inpatients. Journal of Korean Medical Science 2018, 33. [Google Scholar] [CrossRef] [PubMed]
- Baek, I.C.; Jo, S.; Kim, E.J.; Lee, G.R.; Lee, D.H.; Jeon, H.J. A review of suicide risk assessment tools and their measured psychometric properties in Korea. Frontiers in Psychiatry 2021, 12, 679779–679779. [Google Scholar] [CrossRef]
- Ghasemi, P.; Shaghaghi, A.; Allahverdipour, H. Measurement Scales of Suicidal Ideation and Attitudes: A Systematic Review Article. Health Promot Perspect 2015, 5, 156–168. [Google Scholar] [CrossRef]
- Arowosegbe, A.; Oyelade, T. Application of Natural Language Processing (NLP) in Detecting and Preventing Suicide Ideation: A Systematic Review. International Journal of Environmental Research and Public Health 2023, 20. [Google Scholar] [CrossRef]
- Cliffe, C.; Seyedsalehi, A.; Vardavoulia, K.; Bittar, A.; Velupillai, S.; Shetty, H.; Schmidt, U.; Dutta, R. Using natural language processing to extract self-harm and suicidality data from a clinical sample of patients with eating disorders: A retrospective cohort study. BMJ Open 2021, 11. [Google Scholar] [CrossRef]
- Mens, K.V.; Elzinga, E.; Nielen, M.; Lokkerbol, J.; Poortvliet, R.; Donker, G.; Heins, M.; Korevaar, J.; Dückers, M.; Aussems, C.; et al. Applying machine learning on health record data from general practitioners to predict suicidality. Internet Interventions 2020, 21, 100337–100337. [Google Scholar] [CrossRef]
- O’dea, B.; Larsen, M.E.; Batterham, P.J.; Calear, A.L.; Christensen, H. , 2017.
- Larsen, M.E.; Nicholas, J.; Christensen, H. A systematic assessment of smartphone tools for suicide prevention. PLoS ONE 2016, 11. [Google Scholar] [CrossRef]
- Nuij, C.; Ballegooijen, W.V.; Ruwaard, J.; Beurs, D.D.; Mokkenstorm, J.; Duijn, E.V.; Winter, R.F.P.D.; Connor, R.C.; Smit, J.H.; Riper, H.; et al. Smartphone-based safety planning and self-monitoring for suicidal patients: Rationale and study protocol of the CASPAR (Continuous Assessment for Suicide Prevention And Research) study. Internet Interventions 2018, 13, 16–23. [Google Scholar] [CrossRef]
- Martinengo, L.; Galen, L.V.; Lum, E.; Kowalski, M.; Subramaniam, M.; Car, J. Suicide prevention and depression apps’ suicide risk assessment and management: A systematic assessment of adherence to clinical guidelines. BMC Medicine 2019, 17. [Google Scholar] [CrossRef] [PubMed]
- Torok, M.; Han, J.; Baker, S.; Werner-Seidler, A.; Wong, I.; Larsen, M.E.; Christensen, H. , 2020.
- Pham, K.T.; Nabizadeh, A.; Selek, S. Artificial Intelligence and Chatbots in Psychiatry. Psychiatric Quarterly 2022, 93, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Torous, J.; Bucci, S.; Bell, I.H.; Kessing, L.V.; Faurholt-Jepsen, M.; Whelan, P.; Carvalho, A.F.; Keshavan, M.; Linardon, J.; Firth, J. The growing field of digital psychiatry: Current evidence and the future of apps, social media, chatbots, and virtual reality. World Psychiatry 2021, 20, 318–335. [Google Scholar]
- Lin, A.P.C.; Trappey, C.V.; Luan, C.C.; Trappey, A.J.C.; Tu, K.L.K. A Test Platform for Managing School Stress Using a. Virtual Reality Group Chatbot Counseling System. Applied Sciences 2021, 11, 9071–9071. [Google Scholar]
- Castillo-Sánchez, G.; Camargo-Henríquez, I.; Muñoz-Sánchez, J.L.; Franco-Martín, M.; Torre-Díez, I.D.L. Suicide Prevention Mobile Apps: Descriptive Analysis of Apps from the Most Popular Virtual Stores. JMIR MHealth and UHealth 2019, 7. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



