
Submitted:
16 August 2023
Posted:
18 August 2023
You are already at the latest version
Abstract
Hypoxia, associated with abnormal vessel growth, is a characteristic feature of many solid tumors that increases their metastatic potential and resistance to radiotherapy. Carbon ion radiation therapy, alone or in combination with other treatments, is one of the most promising treatments for hypoxic tumors because the oxygen enhancement ratio decreases with increasing particle LET. Nevertheless, the current clinical practice does not yet fully benefit from using carbon ions for tackling hypoxia. Here we give an overview of the existing experimental and clinical evidence supporting the efficacy of C-ion radiotherapy in overcoming hypoxia-induced radioresistance, followed by a discussion of the strategies proposed to enhance it, including different approaches to maximize the LET in the tumors.
Keywords:
hipoxya
; carbon ions
; LET
; particle therapy
1. Introduction
In the field of cancer treatments, carbon ion (12C) beams are usually considered to be an attractive option for cases where conventional radiation therapy approaches have limitations, offering improved tumor control while preserving patients' quality of life. According to the statistics of the Particle Therapy Cooperation Group [1], there are 14 centers operating in Europe and Asia that provide cancer treatments with accelerated 12C beams. Furthermore, after the first patient treatments with various heavy ions at Lawrence Berkeley National Laboratory (LBNL) in 1975–1992 [2], carbon therapy will soon be back to the USA with the facility about to open in Mayo Clinic, Jacksonville [3].
Carbon ions, like protons, exhibit a characteristic dose distribution known as the Bragg peak, depositing most of their energy at the tumor site, thus minimizing damage to critical organs beyond the target area [4]. When compared to light ions, they have a smaller lateral dose penumbra at greater depths that makes the treatment plans more conformal than in proton therapy [5]. However, the main benefit of C-ion radiotherapy (CIRT) lies in its superior biological effectiveness, attributed to the densely ionizing nature of 12C-ions at in the Bragg peak region [6]. Ionization density is described by the linear energy transfer (LET) which is proportional to z2/β2 [4] and is therefore especially high for heavy, slow ions. High-LET radiation induce a higher fraction of direct DNA damage compared to X-rays, where most of the damage comes by free radical produced in water, and the lesions are more difficult to repair [6]. From the treatment planning point of view, this enhanced cell kill leads to an increase in the peak-to-plateau ratio in the spread-out Bragg peak (SOBP) and allows for an increase in biological tumor dose without causing additional normal tissue toxicity.
In the past years, the trends in the 12C physics research are switching to investigations addressing the treatments’ precision, speed, and costs [7], while the radiobiology actively studies the impact of 12C irradiation the tumor microenvironment and signaling pathways [8,9,10,11].
One of the main reasons to use ions heavier than protons in the original Berkeley pilot study was the possibility of overcoming the hypoxia-induced radioresistance [12]. In the Berkeley trial, ions as heavy as argon were used, but toxicity was too high. Carbon was selected first in Japan and then in Europe because it has a relatively low LET in the entrance channel and relatively high LET in the SOBP [6]. However, in the current clinical practice, the mean LET in the target region is often too low to induce a significant sensitization of hypoxic tumors. In this contribution, we explore potential strategies to optimize CIRT treatment outcomes for hypoxic tumors, seeking to enhance its efficacy.
2. Tumor hypoxia and radioresistance
Hypoxia [13] is a characteristic feature of solid tumors, associated with their disrupted and heterogeneous vascular network, which is known to correlate with poor prognosis in cancer patients. Briefly, tumors develop their vascular system via angiogenesis utilizing the blood supply from the host organ. However, in tumors there is no appropriate balance between pro- and anti-angiogenic signals [14], and the tumor neovasculature is rather chaotic, dilated, and leaky, sharing the both the regular and chaotic features of venules, arterioles, and capillaries [15]. Thus, it is no able anymore to meet the metabolic demands of the developing tumor, leading to the formation of oxygen-deficient regions [16]. There is no strict and universal hypoxia threshold for all the tumor types, however, it is suggested that at partial oxygen pressure (pO2) levels below approximately 35 mmHg physiological activities and functions become progressively restricted [17].
Lack of oxygen can have a significant impact on the production of circulating tumor cells (CTCs) and on the metastatic capacity of cancer cells [18]. Hypoxia-induced epithelial-mesenchymal transition contributes to CTC generation, promoting migratory and invasive properties [19]. Furthermore, poorly oxygenated regions in the primary tumor induce angiogenesis-related gene expression, facilitating CTC entry into the bloodstream [20,21].
Hypoxia triggers the activation of hypoxia-inducible factors (HIFs), including the HIF-1, which regulates the expression of dozens of genes and mediates pathways influencing metabolism, angiogenesis, cell growth and differentiation, survival, and apoptosis [22,23]. HIFs are found to be elevated in various cancer types [24], making them important targets for pharmacological intervention [25].
Usually, there are two hypoxia types distinguished: chronic and acute. Chronic, or diffusion-limited hypoxia, caused by limitations in oxygen diffusion from tumor microvessels, was first suggested based on the histological data from bronchus carcinoma patients [26]. On the other hand, acute (perfusion-limited) hypoxia is caused by a temporary complete or partial blood vessel shut down, leading to fluctuations in microvascular oxygen supply [27]. Often, solid tumors contain regions of intermittent, or cycling hypoxia with spatial and temporal fluctuations in oxygen levels [28,29,30].
Regardless of its type (although there is evidence for acute hypoxia to have stronger impact [31]), hypoxia affects the radiotherapy outcomes, due to the crucial role of oxygen the biological effectiveness of radiation. Already in 1950s it was demonstrated that tissues with increased oxygenation are more radiosensitive compared to hypoxic ones [32]. This effect is usually explained by the oxygen fixation hypothesis [33,34]. It postulates that most DNA can be repaired after being damaged with radicals, produced during the interaction of radiation with biological matter; however, that repair is more difficult or impossible (becomes ‘fixed’) when caused by the product of a radical and an oxygen molecule (peroxyl radical).
In radiotherapy, the hypoxia-induced radioresistance is typically described by the oxygen enhancement ratio (OER), i.e., the ratio between the radiation dose in hypoxia and the radiation dose in fully oxygenated conditions (air) resulting in the same biological effect. In conventional radiotherapy OER can reach a maximum value of 3 [35]. The decrease of OER observed with increasing levels of pO2 in tissue can be characterized with a sigmoid curve [36].
3. CIRT for hypoxic tumors: evidence of effectiveness
3.1. Decrease of OER with increasing particle LET: mechanisms and in vitro data
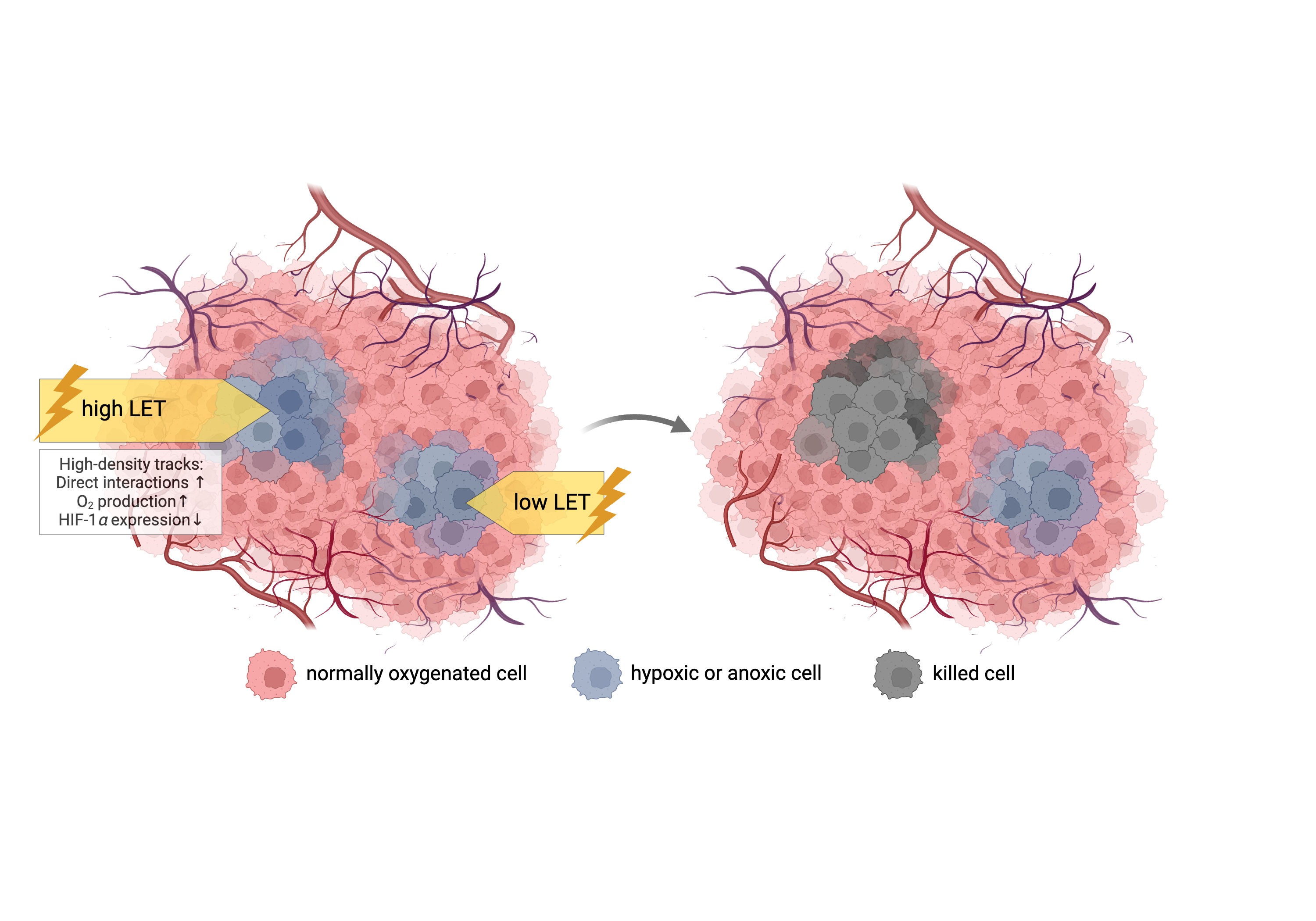
Multiple approaches have been proposed to mitigate hypoxia-induced radioresistance in the past decades, either involving agents that either increase oxygen delivery or radiosensitize or preferentially kill the hypoxic cells, physics-based approaches such dose painting with boosting the radiation dose to the hypoxic areas, and finally the use of high-LET heavy ions. As previously noted, heavy ions produce damage predominantly through direct interaction with the biological targets and are therefore less dependent on free radical production and surrounding oxygen concentrations [37]. In addition, at high-LET there is an increased the production of the molecular oxygen capable of reacting with DNA and damaging it further [38]. In fact, free radical recombination occurs frequently along tracks with high ionization density [39]. In addition, the O2 track concentrations calculated by Monte Carlo compare very well with the O2 concentrations estimated from the "effective" amounts of oxygen needed to produce the observed reduction in OER [40], supporting the “oxygen in the track” hypothesis [38].
The track effects and production of reactive oxygen species modulate HIF expression [41,42] which is reduced following 12C irradiation compared to X-rays [43,44]. Carbon ions seems to be able to induce equal cell killing both in chronic and acute hypoxia, while in anoxia the cells are more resistant in acute conditions [45,46].
Experiments with neutrons and alpha particles had shown many years ago the OER decrease for high-LET radiation. A full OER-LET relationship was originally measured at the LBNL [47] and later confirmed at NIRS (now QST) in Japan [48]. The measured OER values ranged from 3 (photons) down to 1 for heavy ions at LET > 300 keV/μm in cells irradiated with 12C or 20Ne ions. A later modeling study [49] utilized a large pool of experimental OER values measured for particles ranging from protons to argon ions in the LET range of less than 1 keV/µm up to almost 1 MeV/µm. Experimental works in the past years have been further expanding the in vitro data sets, including the OER dependency on both particle LET and cells oxygenation [50].
At present, there are multiple models based mainly on the in vitro data which attempt to describe the OER(LET, pO2) dependencies [49,50,51,52,53,54,55] and include them in the optimization of the treatment plans (see the example in Figure 1). All models predict an approximately two-fold decrease of the OER only starting from LET ~100 keV/µm, with dropping down to 1 at values > 200-300 keV/µm.
3.2. 12С radiation for hypoxic tumors: preclinical studies
Pioneering studies conducted at the LBNL were the first to measure the OER after exposure to heavy ions [56,57] in vivo. The authors compared the efficacy of Si, Ne, and C ions on treatment of rat rhabdomyosarcoma tumors, showing that OER reduced with increasing beam LET for animals in hypoxia, induced by nitrogen gassing of the animal.
A few decades later, a study employing a xenograft model of human non-small cell lung cancer further demonstrated substantial differences between X-rays and 12C ion radiation: the latter induced a 9-fold reduction in HIF-1α levels and significantly delayed the tumor growth [58]. Studies in Japan [59,60] involved mice with squamous cell carcinoma cells injected into the hind limbs, and hypoxia was induced by limb clamping. The in vivo-in vitro colony assays of the extracted irradiated tumor cells further validated the reduced OER values of samples irradiated with carbon in comparison to those exposed to X-rays. An interesting observation pertained to the dynamics of OER decrease: in vitro OER values decreased gradually and then rapidly with increasing LET, while in vivo OER values decreased more slowly with increasing LET. A series of works from Heidelberg [61,62,63] with clamped prostate carcinomas at various differentiation levels in rats provided additional evidence for the decreasing impact of tumor intrinsic characteristics, with hypoxia among them, on the radioresistance against 12C radiation. They found that OER on vitro was higher than in vivo, possibly caused by the impact of the factors in the microenvironment, such as immune response. With regards to the behavior of these factors under hypoxia, the knowledge remains very scarce. For example, the only attempt to look at the immunogenic cell death following 12C irradiation was done in vitro by measuring calreticulin and programmed cell death ligand 1 (PDL1) expression, and no impact of 12C in hypoxia was found [64].
3.3. Benefits of CIRT for hypoxic tumors: clinical evidence
Despite the increasing in vitro and in vivo evidence supporting the potential of high-LET radiation to tackle hypoxia, the clinical evidence that 12C beams increase tumour control probability (TCP) in hypoxic tumors remains scarce. Positive results are obtained in two highly hypoxic tumors: pancreas adenocarcinoma and uterine cervix cancer.
3.3.1. Pancreatic cancer
Characteristic features of pancreatic cancer are the immunosuppressive tumor microenvironment [65] and significantly higher hypoxia levels than most solid tumors [66,67] contributing to increased invasiveness and therapy resistance. A unique feature of pancreatic tumors histology is the extensive desmoplasia surrounding the tumor tissue [68]. Furthermore, a complex relationship between fibrosis and hypoxia amplifies each other reinforcing its metastatic phenotype. Despite decades of research, the five-year survival rate for locally advanced pancreatic cancers (LAPC) remains low at 5-10% [69,70] with photon radiotherapy being inefficient due to the high hypoxia levels and proximity to organs at risk (OARs) [70].
The clinical trials in Japan show promising outcomes of LAPC treatment with 12C beams used in combination with chemotherapy (gemcitabine). At NIRS, in Phase I trial with 26 patients receiving doses from 30 Gy (RBE) up to 36.8 Gy (RBE) followed by a resection in 21 patients, resulted in a remarkable 5-year overall survival rate of 42% [71]. Another NIRS trial combined 12C therapy with concurrent gemcitabine, leading to 2-year overall survival rates of 35% in all patients and 48% in the high-dose group with stage III LAPC [72]. Encouraging results have also been reported from Gunma and Chiba for 12C re-irradiation in treating local recurrences [73,74]. A model of chemoradiotherapy for LAPC showed that Japanese results are superior in terms of TCP to all trials with X-rays in Europe or USA [75]. In Europe, there are currently two trials ongoing: PIOPPO Protocol at CNAO [76] to study the effectiveness of 12C neoadjuvant treatment and phase II PACK in Heidelberg [77] investigating carbon ion treatments for LAPC and locally recurrent pancreatic cancers.
3.3.2. Cervical cancer
Uterine cervical cancer is another example of hypoxic cancer that can be efficiently treated with 12C beams. Being highly hypoxic in both primary and especially recurrent forms [78] , these tumors exhibit poor control rates as compared to oxygenated cases [79].
The outcomes of the clinical 12C treatments in 1995-2000 at NIRS in Japan, during which the pO2 was measured with an oxygen electrode in the individual patients, show comparable disease-free survival and local control rates between hypoxic and oxygenated tumors, indicating the reduction of hypoxia-induced tumor radioresistance with 12C ions [80]. This was the first clinical attempt to directly demonstrate the ability of LET beams to decrease OER and successfully control hypoxic tumors. More recent fundings from Japan’s working group of gynecological tumors [81,82] further demonstrate favorable 5- and 10-year local control rates for cervical carcinomas treated with carbon beams.
4. Tumor reoxygenation and local oxygenation changes
One of the main rationales for fractionation in radiotherapy is tumor reoxygenation [83], i.e., supplying oxygen to the surviving previously hypoxic tumor regions (Figure 2), which in certain conditions can outweigh the effects of sublethal injury repair and regeneration.
A review of the outcomes of the radiotherapy coupled with hypoxia imaging with PET tracers for different tumor sites (primarily head and neck), shows that in all the analyzed studies tumor hypoxia is reduced in the treatment course [84]. A significant drop of hypoxia level often occurs after two weeks of treatment, and the status of reoxygenation at this time point can be indicative of a treatment success or failure [85,86,87,88]. Success in reoxygenation is therefore a necessary step for the success of fractionated radiotherapy.
Two types of oxygenations have been described [52]: slow reoxygenation of chronically hypoxic cells resulting from tumor shrinkage, and changes in acute hypoxia between treatment fractions. The success of carbon treatments for hypoxic tumors can be partly attributed to a careful selection of fractionation schemes, enabling local oxygenation changes to occur between fractions. Therefore, reoxygenation can contribute to the successful clinical trials described in section 3.3.
It is interesting to note that early studies at NIRS showed an accelerated reoxygenation after 12C-ions compared to X-rays irradiation. In particular, a mouse tumor study [89] compared the reoxygenation in squamous cell carcinoma and mammary sarcoma on the hind limbs after the priming irradiation either inside 12C SOBP or X-rays and observed faster reoxygenation after the carbon treatment for two out of three tested tumors. A similar conclusion was reached in a later study [90] demonstrating that C-ion irradiation reoxygenated the fibrosarcomas earlier and deeper in space as compared to the X-rays. An early explanation of these effects was attributed to the so-called random killing of both normoxic and hypoxic cells with carbon ions [91], while a recent study in a rat model explains it with increased tumor vessel perfusion and permeability [92]. Either ways, these old data suggest that a C-ion boost before conventional fractionation treatment with X-rays may improve reoxygenation. Because reoxygenation has a strong prognostic value, testing the oxygenation rate in pre-clinical and clinical settings with C-ions is a very promising research strategy.
5. Is carbon LET high enough?
In treatment planning, several beams of different energies are used to produce an SOBP. Especially for large tumors, this leads unavoidably to a “dilution” of the LET values, which will still be very high for the single Bragg peak but will have a much lower mean value. The highest values of dose-averaged LET (LETd) will be typically reached around the planning tumor volume (PTV) edges, remaining rather low to medium in the core where hypoxia often occurs, leading to inferior clinical outcomes in larger tumors. If the margins around the gross tumor volume (GTV) are large, this leads to a relatively low-LET distribution exactly where it would be more needed, i.e., in the hypoxic sub-volumes of the GTV. Furthermore, equal target dose coverage can be achieved with plans resulting in very different LET distributions [93]. For C-ions, a common range of the LETd in the tumor core is 30–80 keV/µm (Figure 3 A-C) yielding OER values not lower than 2–2.5 (Figure 1). Consequently, the oxygen effect can compromise the treatment outcome not only in X-ray radiotherapy but also in CIRT [52].
A clear correlation between the C-ion LETd distributions and tumor control was demonstrated for pancreatic cancer [94] (Figure 3 D), chondrosarcoma [95] (Figure 3 E) and sacral chordoma [96] patients. In those trials, local recurrence was correlated to low LETd values, suggesting that LETd maps could be used to classify patients into high or low-risk groups for recurrences in high-dose regions [97]. However, it must be stressed that low LETd values are associated to large tumors, whose prognosis is worse than small tumors for reasons that have nothing to do with LET maps. In fact, a retrospective analysis of uterine carcinoma patients treated with C-ions found no direct correlation between severe rectal complications and LETd values [98].
6. Strategies to maximize the carbon ion LET and their limitations
6.1. Simultaneous integrated boost
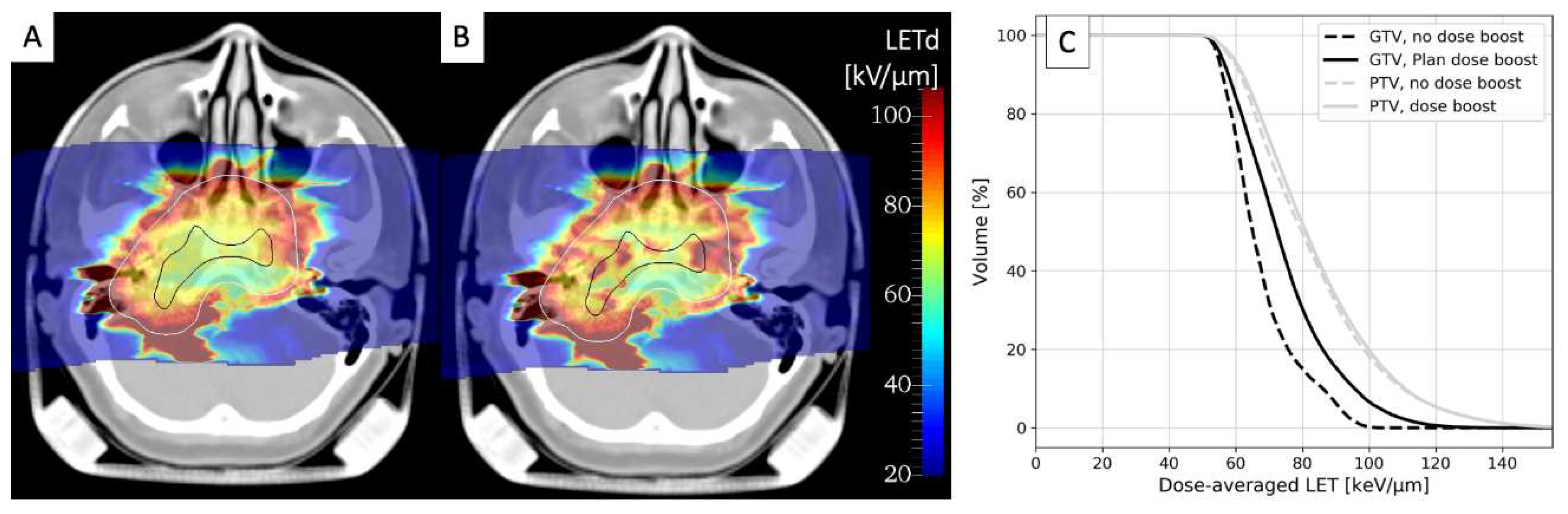
The only approach currently used in clinical trials that might improve the LETd distribution in 12C treatments is the simultaneously integrated boost (SIB). While the main rationale for this approach, coming from intensity-modulated radiotherapy (IMRT) with X-rays, is to deliver a dose boost to selected target sub-regions during the irradiation, this also shifts the LETd distribution to higher values. In Figure 4 we compare the LETd distributions for a chordoma treatment plan optimized for a uniform PTV dose (A) and the one with GTV SIB (B). As it can be seen from the LETd-volume histograms (C) the LETd distribution in the GTV is significantly improved, while almost no changes are visible in the PTV. Whereas SIB is already a standard approach in IMRT, it is under test with CIRT in three ongoing clinical trials – for head and neck adenoid cystic carcinoma in CNAO [99,100] and for prostate [101,102] and pancreatic [103] tumors in Shanghai.
6.2. Arc therapy
Another promising strategy in particle therapy is arc therapy, where beam delivery comes from multiple angles using the gantry rotating around the patient. Originally aimed at enhancing dose conformity and plan robustness, arc therapy has the additional benefit of increasing LET values within the tumor [105]. With arc therapy, the maximum of LET for C-ions moves from the tumor edges to its center, making the plan less sensitive to the presence of hypoxia in the tumor core [54,106].
Arc CIRT requires rotating gantries with high magnetic rigidity compared to proton gantries. Despite the use of novel superconductive technologies, C-ion gantries remain indeed large and expensive. At the moment, only 5 facilities (one in Germany, two in Japan and two in South Korea) use C-ion gantries. A possible breakthrough in this field is to deliver radiotherapy to patients in upright position [107]; however, we will have to deal with rotation speed, acceleration, angular range, and the tolerance of the patients to these parameters [108]. In addition, both gantry or patient rotation need to combine beam raster scanning with the live rotation of the beam or the target.
6.3. LET painting
There are of course other options to increase the LETd in the GTV. For example, the so-called blocking technique is proposed at MedAustron for bulky tumors with the idea of introducing field blocking structures to stop the beams few centimeters beyond the midplane of the GTV. This approach can increase and concentrate the high LETd in the tumor center, at the same time reducing it in adjoining organs at risk, as was demonstrated with pelvic sarcoma plans, and is about to be implemented in the upcoming prospective clinical study [109].
For more adaptive and personalized approaches, the detection of hypoxic tumor sub-targets and their incorporation into treatment planning is essential, going beyond standard RBE-weighted optimization. “LET painting” is a treatment plan method to adapt particles’ LET throughout the tumor PTV according to its oxygenation [93,110]. The LET boosting of hypoxic regions is achieved by applying treatment fields with dose ramps in the SOBP, generated following the position and shape of the hypoxic tumor volume identified through functional imaging. This approach, either alone or in combination with dose-painting techniques, has the potential to increase the tumor control probability [111]. NIRS is currently preparing a trial for head and neck tumors aimed at assessing the safety and effectiveness of LET painting, even though without coupling the approach with hypoxia imaging [112].
When both the pO2 and LET are used in the optimization process using modified algorithms to compute the biological effect in a mixed radiation field, we have a “kill painting” [50,51] to achieve uniform tumor cell killing for any oxygenation distribution in the PTV. This optimization requires intra-tumor oxygenation maps and an OER model describing the corresponding subvolumes radiosensitivity, including its LET dependence. The optimizer redistributes particle fluences in different energy slices, effectively increasing LET in the target center.
6.4. Multi-ions
Even superior, albeit more intricate strategy involves the integration of multiple ion beams within a single treatment plan, profiting from physical and the radiobiological properties of several relevant ions simultaneously. In this context, carbon ions can be employed for targeting a small hypoxic fraction of the tumor or even replaced with heavier ions, such as oxygen 16O [113]. A simple approach is to use carbon ions for boosting the LET locally in a proton plan [93]. The idea is to increase the LET in the GTV keeping a low toxicity in the normal tissue. An extension of this concept developed at NIRS is intensity modulated composite particle therapy [114] that optimizes both dose and LET distributions by combining light and heavy ions within a single treatment plan. Followed by the adaptations of the stochastic microdosimetric kinetic used for the biological optimization, this approach was further expanded to account for the pO2-dependent OER by boosting the LET values in hypofractionated treatments [115]. A similar outcome, where the heavy high-LET ions are automatically assigned to hypoxic subvolumes, while the rest of the tumor dose is delivered by the light ion beams, is also achieved with the strategy proposed at GSI where the above-mentioned kill painting approach was upgraded to handle multiple ion species [116].
6.5. Carbon PATHY
The treatment of large bulky tumors has several problems both in conventional and particle therapy. These tumors tend to be very hypoxic and sometimes they can be so large that a full dose coverage in radiotherapy is not possible. To tackle such tumors, Slavisa Tubin developed an IMRT approach called PArtial Tumor irradiation targeting HYpoxic segment (PATHY) [117]. The treatment aims at exploiting the bystander effect and immune activation in large hypoxic tumors by irradiating the hypoxic sub-volume and sparing the peritumoral immune tumor microenvironment. In fact, the peritumoral environment contains blood-lymphatic vessels and lymph nodes, sparing of which would enhance the immune response of the treatment. The first clinical results with IMRT in large, unresecatable tumors were very promising [118]. Carbon ions seem to be ideal modality for PATHY treatment both in terms of irradiation precision, reduced OER in the bystander-target volume and stronger immunogenic cell death compared to X-rays [119]. When he moved to the C-ion center MedAustron, Dr. Tubin and his colleagues started in fact carbon-PATHY studies with the ultimate goal of reducing the tumor volume to the point that surgery is possible [120]. A phase I/II clinical trial is currently ongoing at MedAustron to evaluate feasibility and effectiveness of Carbon-PATHY for unresectable bulky tumors [121].
6.6. Challenges of LET optimization
Despite the elegance of the above-described solutions, their implementation into clinical practice remains hindered by several unresolved questions.
First, most of them require the precise model for the OER dependence on particle LET and tissue oxygenation, and despite the large number of existing models mentioned in section 3.1, the optimal function, remains unknown. Additionally, these models heavily rely on in vitro cell survival data, which might lead to the uncertainties in the estimations of in vivo effects. Thus, further efforts are essential to understand the biological, chemical and physics basics of hypoxia radioresistance leading to the development of a more accurate OER model.
Secondly, painting techniques require non-invasive hypoxia imaging tools with high temporal and spatial resolutions. There is a wide range of techniques proposed for this purpose, ranging from already more conventional PET- or MRI-based approaches to recently proposed alternatives such as Cherenkov-excited phosphorescence [122] to functional near-infrared spectroscopy [123]. Despite that, the information obtained with any of these methods is still considered not reliable enough for treatment planning [124,125,126]. Among the open issues is also the imaging resolution that remains limited with respect to the tumor microenvironment. Differentiation between different forms of hypoxia (diffusion-limited, perfusion-limited, or anaemic), which cannot yet be tackled with functional imaging techniques, was proven to be important [127] employing tumor models with heterogeneous oxygenation [128]. Furthermore, pO2 quantification is strongly affected on the choice a well-oxygenated reference region and its assigned oxygenation level which is used to normalize tracer uptake using conversion functions [129].
7. Comparison to pharmaceutical approaches
CIRT is a physical tool to overcome hypoxia and must be compared with pharmaceutical approaches. A typical example of OER-reducing drug that can be used in radiotherapy are the hypoxic cell-radiation sensitizers nitroimidazoles that are found to mimic the effect of oxygen in the radiochemical process, and at a clinically acceptable toxicity level can theoretically lead the reduction of OER down to the values of 1.5-2 [130]. However, the only one used in the clinical practice routinely and only for treatments of head & neck squamous cell carcinoma in Denmark and Norway according to [131], is nitroimidazole-based nimorazole. The meaningfulness of combining nitroimidazoles with CIRT is yet to be evaluated.
Experimental evidence also suggests that targeting HIF-1α together with CIRT could be a promising therapeutic strategy for hypoxic tumors [132]. Among the promising approaches [132], notable are the tumor targeted lipid-based CRISPR/Cas9 delivery [133] or nanoparticle-based delivery of HIF-1α inhibitors such as lificiguat [134]. Other studies propose using inhibitors of the tumor heat shock protein 90 (HSP90) which controls the activity and stabilization of HIF-1α [135,136], and which is shown to enhance the resistance to CIRT [137]. PU-H71 could be a promising candidate for the role; however, so far, the evidence of combining it with 12C radiation is limited to in vitro studies in normoxia [137,138].
Hypoxia-activated prodrugs (HAP) are already in use in clinical trials. HAP are activated by reduction facilitated by cellular oxidoreductases [139] and can thus selectively ‘sterilize’ hypoxic tumor cells either by damaging their DNA or targeting proteins associated with tumorigenesis. Based on their design and activation mechanism, HAPs can be divided into several categories, including quinones, nitroaromatics, aliphatic and hetero-aromatic N-oxides (detailed overviews can be found in [140,141]) with tirapazamine, PR-104 and TH-302 being probably the most prominent ones. Although combining HAP with conventional radiation can be an elegant solution [142] which in theory could eliminate the need for CIRT for treating hypoxic tumors, their clinical application was so far hampered by high patient toxicities despite the promising preclinical results. These failures are commonly attributed to the to the lack of reliable biomarkers predictive of the hypoxia status of the tumor and thus lack of patient stratification based on the levels of tumor hypoxia [143,144,145,146].
8. Conclusions and future directions
While the use of protons in radiotherapy is motivated by the physical properties, heavy ions are more justified by their biological characteristics. Cornelius Tobias decided to treat tumors with heavy ions in the LBNL pilot trial essentially to overcome hypoxia radioresistance [12]. However, the clinical evidence for CIRT's effectiveness in controlling hypoxic tumors remains limited and further clinical trials, ideally with quantitative assessment of the levels of hypoxia, are needed to validate its efficacy in a broader range of cancer types.
Furthermore, our knowledge on OER-LET relationship is largely based on cell studies in vitro. Animal experiments assessing the OER of 12C show that, despite the generally similar trends, the in vitro and in vivo values and their dependencies on LET differ from each other. This, in turn, raises the need for the more in-depth preclinical studies looking at the immune response or cell communication specifically in hypoxic conditions, a topic already clinically exploited in PATHY (see section 6.5), as well as at the possible accelerated reoxygenation by C-ions (see section 4). Preferably, in such studies the hypoxia needs to be induced in more natural ways, since the commonly used tumor clamping hinders the supply of nutrients and increases the pressure in the tumor capillaries, potentially affecting the measured OER by inducing secondary cell death.
Nevertheless, there is the undeniable scientific and clinical evidence of increased particle’s LET impact on the cell kill and tumor response in hypoxia, and there are multiple approaches proposed to control it. Some of them, such as SIB, LET blocking and LET painting are about to be tested in the upcoming respective clinical trials. The results of these trials will be crucial to decide the next steps. However, if they are not associated to functional hypoxia imaging e.g., by PET, the results may remain unconclusive. More sophisticated techniques such as carbon-arc or multi-ions first require additional improvements in the beam delivery or imaging technologies.
Author Contributions
O.S. and M.D. have collected the literature. O.S. prepared the first draft. All authors have read and agreed to the published version of the manuscript.
Funding
This work was partly funded by the ERC grant 883425 BARB.
Acknowledgments
We thank Dr. Alexander Helm for the fruitful discussions about the radiobiology of hypoxia.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Particle Therapy Co-Operative Group Particle Therapy Facilities in Clinical Operation. Accessed August 10, 2023. Https://Www.Ptcog.Site/Index.Php/Facilities-in-Operation-Public.
- Castro, J.R. Results of Heavy Ion Radiotherapy. Radiat Environ Biophys 1995, 34, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Pompos, A.; Foote, R.L.; Koong, A.C.; Le, Q.T.; Mohan, R.; Paganetti, H.; Choy, H. National Effort to Re-Establish Heavy Ion Cancer Therapy in the United States. Front Oncol 2022, 12. [Google Scholar] [CrossRef]
- Durante, M.; Paganetti, H. Nuclear Physics in Particle Therapy : A Review. Reports on Progress in Physics 2016, 79, 96702. [Google Scholar] [CrossRef] [PubMed]
- Schardt, D.; Elsässer, T.; Schulz-ertner, D. Heavy-Ion Tumor Therapy : Physical and Radiobiological Benefits. Review of Modern Physics 2010, 82, 383–425. [Google Scholar] [CrossRef]
- Tinganelli, W.; Durante, M. Carbon Ion Radiobiology. Cancers (Basel) 2020, 12, 3022. [Google Scholar] [CrossRef]
- Graeff, C.; Volz, L.; Durante, M. Emerging Technologies for Cancer Therapy Using Accelerated Particles. Prog Part Nucl Phys 2023, 131, 104046. [Google Scholar] [CrossRef] [PubMed]
- Schaue, D.; McBride, W.H. Opportunities and Challenges of Radiotherapy for Treating Cancer. Nat Rev Clin Oncol 2015, 12, 527–540. [Google Scholar] [CrossRef]
- Mohamad, O.; Makishima, H.; Kamada, T. Evolution of Carbon Ion Radiotherapy at the National Institute of Radiological Sciences in Japan. Cancers (Basel) 2018, 10, 66. [Google Scholar] [CrossRef] [PubMed]
- Durante, M.; Flanz, J. Charged Particle Beams to Cure Cancer: Strengths and Challenges. Semin Oncol 2019, 46, 219–225. [Google Scholar] [CrossRef]
- Durante, M.; Debus, J.; Loeffler, J.S. Physics and Biomedical Challenges of Cancer Therapy with Accelerated Heavy Ions. Nature Reviews Physics 2021, 3, 777–790. [Google Scholar] [CrossRef]
- Tobias, C.A. Failla Memorial Lecture. The Future of Heavy-Ion Science in Biology and Medicine. Radiat Res 1985, 103, 1–33. [Google Scholar] [CrossRef] [PubMed]
- Mckeown, S.R. Defining Normoxia, Physoxia and Hypoxia in Tumours — Implications for Treatment Response. British Journal of Radiology 2014, 87, 20130676. [Google Scholar] [CrossRef]
- Dvorak, H.F. Tumors: Wounds That Do Not Heal. New England Journal of Medicine 1986, 315, 1650–1659. [Google Scholar] [CrossRef] [PubMed]
- Bergers, G.; Benjamin, L.E. Tumorigenesis and the Angiogenic Switch. Nat Rev Cancer 2003, 3, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Horsman, M.R.; Vaupel, P. Pathophysiological Basis for the Formation of the Tumor Microenvironment. Front Oncol 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Höckel, M.; Vaupel, P. Tumor Hypoxia: Definitions and Current Clinical, Biologic, and Molecular Aspects. J Natl Cancer Inst 2001, 93, 266–276. [Google Scholar] [CrossRef]
- Lin, D.; Shen, L.; Luo, M.; Zhang, K.; Li, J.; Yang, Q.; Zhu, F.; Zhou, D.; Zheng, S.; Chen, Y.; et al. Circulating Tumor Cells: Biology and Clinical Significance. Signal Transduct Target Ther 2021, 6, 404. [Google Scholar] [CrossRef]
- Hapke, R.Y.; Haake, S.M. Hypoxia-Induced Epithelial to Mesenchymal Transition in Cancer. Cancer Lett 2020, 487, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Micalizzi, D.S.; Maheswaran, S.; Haber, D.A. A Conduit to Metastasis: Circulating Tumor Cell Biology. Genes Dev 2017, 31, 1827–1840. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Zhang, H.; Jiang, X.; Qian, C.; Liu, Z.; Luo, D. Factors Involved in Cancer Metastasis: A Better Understanding to “Seed and Soil” Hypothesis. Mol Cancer 2017, 16, 176. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, P. Activation of the HIF Pathway in Cancer. Curr Opin Genet Dev 2001, 11, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Choudhry, H.; Harris, A.L. Advances in Hypoxia-Inducible Factor Biology. Cell Metab 2018, 27, 281–298. [Google Scholar] [CrossRef]
- Semenza, G.L. Defining the Role of Hypoxia-Inducible Factor 1 in Cancer Biology and Therapeutics. Oncogene 2010, 29, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Semenza, G.L. Pharmacologic Targeting of Hypoxia-Inducible Factors. Annu Rev Pharmacol Toxicol 2019, 59, 379–403. [Google Scholar] [CrossRef]
- Thomlinson, R.H.; Gray, L.H. The Histological Structure of Some Human Lung Cancers and the Possible Implications for Radiotherapy. Br J Cancer 1955, 9, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Kimura, H.; Braun, R.D.; Ong, E.T.; Hsu, R.; Secomb, T.W.; Papahadjopoulos, D.; Hong, K.; Dewhirst, M.W. Fluctuations in Red Cell Flux in Tumor Microvessels Can Lead to Transient Hypoxia and Reoxygenation in Tumor Parenchyma. Cancer Res 1996, 56, 5522–5528. [Google Scholar]
- Dewhirst, M.W.; Cao, Y.; Moeller, B. Cycling Hypoxia and Free Radicals Regulate Angiogenesis and Radiotherapy Response. Nat Rev Cancer 2008, 8, 425–437. [Google Scholar] [CrossRef]
- Michiels, C.; Tellier, C.; Feron, O. Cycling Hypoxia: A Key Feature of the Tumor Microenvironment. Biochimica et Biophysica Acta (BBA) - Reviews on Cancer 2016, 1866, 76–86. [Google Scholar] [CrossRef]
- Saxena; Jolly Acute vs. Chronic vs. Cyclic Hypoxia: Their Differential Dynamics, Molecular Mechanisms, and Effects on Tumor Progression. Biomolecules 2019, 9, 339. [Google Scholar] [CrossRef] [PubMed]
- van der Heijden, M.; de Jong, M.C.; Verhagen, C.V.M.; de Roest, R.H.; Sanduleanu, S.; Hoebers, F.; Leemans, C.R.; Brakenhoff, R.H.; Vens, C.; Verheij, M.; et al. Acute Hypoxia Profile Is a Stronger Prognostic Factor than Chronic Hypoxia in Advanced Stage Head and Neck Cancer Patients. Cancers (Basel) 2019, 11, 583. [Google Scholar] [CrossRef]
- Gray, L.H.; Conger, A.D.; Ebert, M.; Hornsey, S.; Scott, O.C.A. The Concentration of Oxygen Dissolved in Tissues at the Time of Irradiation as a Factor in Radiotherapy. Br J Radiol 1953, 26, 638–648. [Google Scholar] [CrossRef]
- Hall, E.J.; Giaccia, A.J. Radiobiology for the Radiologist; 7th ed.; Lippincottt Williams & Wilkins, 2012;
- Robert Grimes, D.; Partridge, M. A Mechanistic Investigation of the Oxygen Fixation Hypothesis and Oxygen Enhancement Ratio. Biomed Phys Eng Express 2015, 1, 045209. [Google Scholar] [CrossRef] [PubMed]
- Horsman, M.; Wouters, B.; Joiner, M.; Overgaard, J. The Oxygen Effect and Fractionated Radiotherapy. In Basic Clinical Radiobiology Fourth Edition; CRC Press, 2009; pp. 207–216.
- Wouters, B.G.; Brown, J.M. Cells at Intermediate Oxygen Levels Can Be More Important Than the “Hypoxic Fraction” in Determining Tumor Response to Fractionated Radiotherapy. Radiat Res 1997, 147, 541. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, R.; Ito, A.; Tomita, M.; Tsukada, T.; Yatagai, F.; Noguchi, M.; Matsumoto, Y.; Kase, Y.; Ando, K.; Okayasu, R.; et al. Contributions of Direct and Indirect Actions in Cell Killing by High-LET Radiations. Radiat Res 2009, 171, 212–218. [Google Scholar] [CrossRef]
- Alper, T.; Bryant, P.E. Reduction in Oxygen Enhancement Ratio with Increase in LET: Tests of Two Hypotheses. Int J Radiat Biol 1974, 26, 203–218. [Google Scholar] [CrossRef] [PubMed]
- LaVerne, J.A. Track Effects of Heavy Ions in Liquid Water. Radiat Res 2000, 153, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Meesungnoen, J.; Jay-Gerin, J.-P. High-LET Ion Radiolysis of Water: Oxygen Production in Tracks. Radiat Res 2009, 171, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Qutub, A.A.; Popel, A.S. Reactive Oxygen Species Regulate Hypoxia-Inducible Factor 1α Differentially in Cancer and Ischemia. Mol Cell Biol 2008, 28, 5106–5119. [Google Scholar] [CrossRef] [PubMed]
- Movafagh, S.; Crook, S.; Vo, K. Regulation of Hypoxia-Inducible Factor-1a by Reactive Oxygen Species : New Developments in an Old Debate. J Cell Biochem 2015, 116, 696–703. [Google Scholar] [CrossRef] [PubMed]
- Wozny, A.-S.; Lauret, A.; Battiston-Montagne, P.; Guy, J.-B.; Beuve, M.; Cunha, M.; Saintigny, Y.; Blond, E.; Magne, N.; Lalle, P.; et al. Differential Pattern of HIF-1α Expression in HNSCC Cancer Stem Cells after Carbon Ion or Photon Irradiation: One Molecular Explanation of the Oxygen Effect. Br J Cancer 2017, 116, 1340–1349. [Google Scholar] [CrossRef] [PubMed]
- Valable, S.; Gérault, A.N.; Lambert, G.; Leblond, M.M.; Anfray, C.; Toutain, J.; Bordji, K.; Petit, E.; Bernaudin, M.; Pérès, E.A. Impact of Hypoxia on Carbon Ion Therapy in Glioblastoma Cells: Modulation by LET and Hypoxia-Dependent Genes. Cancers (Basel) 2020, 12, 2019. [Google Scholar] [CrossRef] [PubMed]
- Ma, N.-Y.; Tinganelli, W.; Maier, A.; Durante, M.; Kraft-Weyrather, W. Influence of Chronic Hypoxia and Radiation Quality on Cell Survival. J Radiat Res 2013, 54, i13–i22. [Google Scholar] [CrossRef] [PubMed]
- Tinganelli, W.; Ma, N.-Y.; Von Neubeck, C.; Maier, A.; Schicker, C.; Kraft-Weyrather, W.; Durante, M. Influence of Acute Hypoxia and Radiation Quality on Cell Survival. J Radiat Res 2013, 54, i23–i30. [Google Scholar] [CrossRef] [PubMed]
- Blakely, E.A.; Ngo, F.Q.H.; Curtis, S.B.; Tobias, C.A. Heavy-Ion Radiobiology: Cellular Studies. Adv Radiat Biol 1984, 11, 295–389. [Google Scholar]
- Furusawa, Y.; Fukutsu, K.; Aoki, M.; Itsukaichi, H.; Eguchi-Kasai, K.; Ohara, H.; Yatagai, F.; Kanai, T.; Ando, K. Inactivation of Aerobic and Hypoxic Cells from Three Different Cell Lines by Accelerated (3)He-, (12)C- and (20)Ne-Ion Beams. Radiat Res 2000, 154, 485–496. [Google Scholar] [CrossRef] [PubMed]
- Wenzl, T.; Wilkens, J.J. Modelling of the Oxygen Enhancement Ratio for Ion Beam Radiation Therapy. Phys Med Biol 2011, 56, 3251–3268. [Google Scholar] [CrossRef]
- Tinganelli, W.; Durante, M.; Hirayama, R.; Krämer, M.; Maier, A.; Kraft-Weyrather, W.; Furusawa, Y.; Friedrich, T.; Scifoni, E. Kill-Painting of Hypoxic Tumours in Charged Particle Therapy. Sci Rep 2015, 5, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Scifoni, E.; Tinganelli, W.; Weyrather, W.K.; Durante, M.; Maier, A.; Krämer, M. Including Oxygen Enhancement Ratio in Ion Beam Treatment Planning: Model Implementation and Experimental Verification. Phys Med Biol 2013, 58, 3871–3895. [Google Scholar] [CrossRef] [PubMed]
- Antonovic, L.; Lindblom, E.; Dasu, A.; Bassler, N.; Furusawa, Y.; Toma-Dasu, I. Clinical Oxygen Enhancement Ratio of Tumors in Carbon Ion Radiotherapy: The Influence of Local Oxygenation Changes. J Radiat Res 2014, 55, 902–911. [Google Scholar] [CrossRef] [PubMed]
- Strigari, L.; Torriani, F.; Manganaro, L.; Inaniwa, T.; Dalmasso, F.; Cirio, R.; Attili, A. Tumour Control in Ion Beam Radiotherapy with Different Ions in the Presence of Hypoxia: An Oxygen Enhancement Ratio Model Based on the Microdosimetric Kinetic Model. Phys Med Biol 2018, 63, 065012. [Google Scholar] [CrossRef]
- Mein, S.; Tessonnier, T.; Kopp, B.; Harrabi, S.; Abdollahi, A.; Debus, J.; Haberer, T.; Mairani, A. Spot-Scanning Hadron Arc (SHArc) Therapy: A Study With Light and Heavy Ions. Adv Radiat Oncol 2021, 6, 100661. [Google Scholar] [CrossRef] [PubMed]
- Inaniwa, T.; Kanematsu, N. Event-by-Event Approach to the Oxygen-Effect-Incorporated Stochastic Microdosimetric Kinetic Model for Hypofractionated Multi-Ion Therapy. J Radiat Res 2023, 64, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, T.S.; Curtis, S.B.; Crabtree, K.E.; Tenforde, S.D.; Schilling, W.A.; Howard, J.; Lyman, J.T. In Vivo Cell Survival and Volume Response Characteristics of Rat Rhabdomyosarcoma Tumors Irradiated in the Extended Peak Region of Carbon- and Neon-Ion Beams. Radiat Res 1980, 83, 42. [Google Scholar] [CrossRef]
- Tenforde, T.S.; Afzal, S.M.J.; Parr, S.S.; Howard, J.; Lyman, J.T.; Curtis, S.B. Cell Survival in Rat Rhabdomyosarcoma Tumors Irradiated in Vivo with Extended-Peak Silicon Ions. Radiat Res 1982, 92, 208. [Google Scholar] [CrossRef] [PubMed]
- Subtil, F.S.B.; Wilhelm, J.; Bill, V.; Westholt, N.; Rudolph, S.; Fischer, J.; Scheel, S.; Seay, U.; Fournier, C.; Taucher-Scholz, G.; et al. Carbon Ion Radiotherapy of Human Lung Cancer Attenuates HIF-1 Signaling and Acts with Considerably Enhanced Therapeutic Efficiency. The FASEB Journal 2014, 28, 1412–1421. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, R.; Uzawa, A.; Takase, N.; Matsumoto, Y.; Noguchi, M.; Koda, K.; Ozaki, M.; Yamashita, K.; Li, H.; Kase, Y.; et al. Evaluation of SCCVII Tumor Cell Survival in Clamped and Non-Clamped Solid Tumors Exposed to Carbon-Ion Beams in Comparison to X-Rays. Mutation Research/Genetic Toxicology and Environmental Mutagenesis 2013, 756, 146–151. [Google Scholar] [CrossRef]
- Hirayama, R.; Uzawa, A.; Obara, M.; Takase, N.; Koda, K.; Ozaki, M.; Noguchi, M.; Matsumoto, Y.; Li, H.; Yamashita, K.; et al. Determination of the Relative Biological Effectiveness and Oxygen Enhancement Ratio for Micronuclei Formation Using High-LET Radiation in Solid Tumor Cells: An in Vitro and in Vivo Study. Mutation Research/Genetic Toxicology and Environmental Mutagenesis 2015, 793, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Glowa, C.; Karger, C.P.; Brons, S.; Zhao, D.; Mason, R.P.; Huber, P.E.; Debus, J.; Peschke, P. Carbon Ion Radiotherapy Decreases the Impact of Tumor Heterogeneity on Radiation Response in Experimental Prostate Tumors. Cancer Lett 2016, 378, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Glowa, C.; Peschke, P.; Brons, S.; Neels, O.C.; Kopka, K.; Debus, J.; Karger, C.P. Carbon Ion Radiotherapy: Impact of Tumor Differentiation on Local Control in Experimental Prostate Carcinomas. Radiation Oncology 2017, 12, 174. [Google Scholar] [CrossRef] [PubMed]
- Glowa, C.; Peschke, P.; Brons, S.; Debus, J.; Karger, C.P. Intrinsic and Extrinsic Tumor Characteristics Are of Minor Relevance for the Efficacy of Split-Dose Carbon Ion Irradiation in Three Experimental Prostate Tumors. Radiotherapy and Oncology 2019, 133, 120–124. [Google Scholar] [CrossRef]
- Huang, Y.; Huang, Q.; Zhao, J.; Dong, Y.; Zhang, L.; Fang, X.; Sun, P.; Kong, L.; Lu, J.J. The Impacts of Different Types of Radiation on the CRT and PDL1 Expression in Tumor Cells Under Normoxia and Hypoxia. Front Oncol 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Ho, W.J.; Jaffee, E.M.; Zheng, L. The Tumour Microenvironment in Pancreatic Cancer — Clinical Challenges and Opportunities. Nat Rev Clin Oncol 2020, 17, 527–540. [Google Scholar] [CrossRef] [PubMed]
- Koong, A.C.; Mehta, V.K.; Le, Q.T.; Fisher, G.A.; Terris, D.J.; Brown, J.M.; Bastidas, A.J.; Vierra, M. Pancreatic Tumors Show High Levels of Hypoxia. International Journal of Radiation Oncology*Biology*Physics 2000, 48, 919–922. [Google Scholar] [CrossRef] [PubMed]
- Erkan, M.; Kurtoglu, M.; Kleeff, J. The Role of Hypoxia in Pancreatic Cancer: A Potential Therapeutic Target? Expert Rev Gastroenterol Hepatol 2016, 10, 301–316. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Zheng, Y.; Yang, F.; Zhu, L.; Zhu, X.-Q.; Wang, Z.-F.; Wu, X.-L.; Zhou, C.-H.; Yan, J.-Y.; Hu, B.-Y.; et al. The Molecular Biology of Pancreatic Adenocarcinoma: Translational Challenges and Clinical Perspectives. Signal Transduct Target Ther 2021, 6, 249. [Google Scholar] [CrossRef] [PubMed]
- Ansari, D.; Tingstedt, B.; Andersson, B.; Holmquist, F.; Sturesson, C.; Williamsson, C.; Sasor, A.; Borg, D.; Bauden, M.; Andersson, R. Pancreatic Cancer: Yesterday, Today and Tomorrow. Future Oncology 2016, 12, 1929–1946. [Google Scholar] [CrossRef] [PubMed]
- Liermann, J.; Shinoto, M.; Syed, M.; Debus, J.; Herfarth, K.; Naumann, P. Carbon Ion Radiotherapy in Pancreatic Cancer: A Review of Clinical Data. Radiotherapy and Oncology 2020, 147, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Shinoto, M.; Yamada, S.; Yasuda, S.; Imada, H.; Shioyama, Y.; Honda, H.; Kamada, T.; Tsujii, H.; Saisho, H. Phase 1 Trial of Preoperative, Short-Course Carbon-Ion Radiotherapy for Patients with Resectable Pancreatic Cancer. Cancer 2013, 119, 45–51. [Google Scholar] [CrossRef]
- Shinoto, M.; Yamada, S.; Terashima, K.; Yasuda, S.; Shioyama, Y.; Honda, H.; Kamada, T.; Tsujii, H.; Saisho, H.; Asano, T.; et al. Carbon Ion Radiation Therapy With Concurrent Gemcitabine for Patients With Locally Advanced Pancreatic Cancer. International Journal of Radiation Oncology*Biology*Physics 2016, 95, 498–504. [Google Scholar] [CrossRef]
- Okamoto, M.; Shiba, S.; Okazaki, S.; Miyasaka, Y.; Shibuya, K.; Kiyohara, H.; Ohno, T. Feasibility and Safety of Repeated Carbon Ion Radiotherapy for Locally Advanced Unresectable Pancreatic Cancer. Cancers (Basel) 2021, 13, 665. [Google Scholar] [CrossRef]
- Hagiwara, Y.; Yamada, S.; Isozaki, Y.; Takiyama, H.; Shinoto, M.; Kawashiro, S.; Bhattacharyya, T.; Nemoto, K.; Tsuji, H. Efficacy and Feasibility of Re-Irradiation Using Carbon Ions for Pancreatic Cancer That Recurs after Carbon-Ion Radiotherapy. Clin Transl Radiat Oncol 2021, 26, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Durante, M.; Tommasino, F.; Yamada, S. Modeling Combined Chemotherapy and Particle Therapy for Locally Advanced Pancreatic Cancer. Front Oncol 2015, 5. [Google Scholar] [CrossRef]
- Vitolo, V.; Cobianchi, L.; Brugnatelli, S.; Barcellini, A.; Peloso, A.; Facoetti, A.; Vanoli, A.; Delfanti, S.; Preda, L.; Molinelli, S.; et al. Preoperative Chemotherapy and Carbon Ions Therapy for Treatment of Resectable and Borderline Resectable Pancreatic Adenocarcinoma: A Prospective, Phase II, Multicentre, Single-Arm Study. BMC Cancer 2019, 19, 922. [Google Scholar] [CrossRef]
- Liermann, J.; Naumann, P.; Hommertgen, A.; Pohl, M.; Kieser, M.; Debus, J.; Herfarth, K. Carbon Ion Radiotherapy as Definitive Treatment in Non-Metastasized Pancreatic Cancer: Study Protocol of the Prospective Phase II PACK-Study. BMC Cancer 2020, 20, 947. [Google Scholar] [CrossRef] [PubMed]
- Höckel, M.; Schlenger, K.; Höckel, S.; Aral, B.; Schäffer, U.; Vaupel, P. Tumor Hypoxia in Pelvic Recurrences of Cervical Cancer. Int J Cancer 1998, 79, 365–369. [Google Scholar] [CrossRef]
- Suzuki, Y.; Nakano, T.; Ohno, T.; Kato, S.; Niibe, Y.; Morita, S.; Tsujii, H. Oxygenated and Reoxygenated Tumors Show Better Local Control in Radiation Therapy for Cervical Cancer. International Journal of Gynecological Cancer 2006, 16, 306–311. [Google Scholar] [CrossRef]
- Nakano, T.; Suzuki, Y.; Ohno, T.; Kato, S.; Suzuki, M.; Morita, S.; Sato, S.; Oka, K.; Tsujii, H. Carbon Beam Therapy Overcomes the Radiation Resistance of Uterine Cervical Cancer Originating from Hypoxia. Clinical Cancer Research 2006, 12, 2185–2190. [Google Scholar] [CrossRef] [PubMed]
- Okonogi, N.; Wakatsuki, M.; Kato, S.; Shiba, S.; Kobayashi, D.; Kiyohara, H.; Karasawa, K.; Ohno, T.; Nakano, T.; Kamada, T.; et al. Long-Term Outcomes of Carbon-Ion Radiotherapy for Locally Advanced Squamous Cell Carcinoma of the Uterine Cervix. Anticancer Res 2018, 38, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Irie, D.; Okonogi, N.; Wakatsuki, M.; Kato, S.; Ohno, T.; Karasawa, K.; Kiyohara, H.; Kobayashi, D.; Tsuji, H.; Nakano, T.; et al. Carbon-Ion Radiotherapy for Inoperable Endometrial Carcinoma. J Radiat Res 2018, 59, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Withers, H.R. The Four R’s of Radiotherapy. In Advances in Radiation Biology; Academic Press: New York, 1975; pp. 241–247. [Google Scholar]
- Stieb, S.; Eleftheriou, A.; Warnock, G.; Guckenberger, M.; Riesterer, O. Longitudinal PET Imaging of Tumor Hypoxia during the Course of Radiotherapy. Eur J Nucl Med Mol Imaging 2018, 45, 2201–2217. [Google Scholar] [CrossRef]
- Zips, D.; Zöphel, K.; Abolmaali, N.; Perrin, R.; Abramyuk, A.; Haase, R.; Appold, S.; Steinbach, J.; Kotzerke, J.; Baumann, M. Exploratory Prospective Trial of Hypoxia-Specific PET Imaging during Radiochemotherapy in Patients with Locally Advanced Head-and-Neck Cancer. Radiotherapy and Oncology 2012, 105, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Wiedenmann, N.E.; Bucher, S.; Hentschel, M.; Mix, M.; Vach, W.; Bittner, M.-I.; Nestle, U.; Pfeiffer, J.; Weber, W.A.; Grosu, A.L. Serial [18F]-Fluoromisonidazole PET during Radiochemotherapy for Locally Advanced Head and Neck Cancer and Its Correlation with Outcome. Radiotherapy and Oncology 2015, 117, 113–117. [Google Scholar] [CrossRef]
- Löck, S.; Perrin, R.; Seidlitz, A.; Bandurska-Luque, A.; Zschaeck, S.; Zöphel, K.; Krause, M.; Steinbach, J.; Kotzerke, J.; Zips, D.; et al. Residual Tumour Hypoxia in Head-and-Neck Cancer Patients Undergoing Primary Radiochemotherapy, Final Results of a Prospective Trial on Repeat FMISO-PET Imaging. Radiotherapy and Oncology 2017, 124, 533–540. [Google Scholar] [CrossRef]
- Sanduleanu, S.; Hamming-Vrieze, O.; Wesseling, F.W.R.; Even, A.J.G.; Hoebers, F.J.; Hoeben, A.; Vogel, W. V.; Tesselaar, M.E.T.; Parvin, D.; Bartelink, H.; et al. [18F]-HX4 PET/CT Hypoxia in Patients with Squamous Cell Carcinoma of the Head and Neck Treated with Chemoradiotherapy: Prognostic Results from Two Prospective Trials. Clin Transl Radiat Oncol 2020, 23, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Oya, N.; Sasai, K.; Shibata, T.; Takagi, T.; Shibuya, K.; Koike, S.; Nojima, K.; Furusawa, Y.; Ando, K.; Hiraoka, M. Time Course of Reoxygenation in Experimental Murine Tumors after Carbon-Beam and X-Ray Irradiation. J Radiat Res 2001, 42, 131–141. [Google Scholar] [CrossRef]
- Fukawa, T.; Takematsu, K.; Oka, K.; Koike, S.; Ando, K.; Kobayashi, H.; Tanishita, K. Differences in PO2 Peaks of a Murine Fibrosarcoma between Carbon-Ion and X-Ray Irradiation. J Radiat Res 2004, 45, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Ando, K. Accelerated Reoxygenation of a Murine Fibrosarcoma after Carbon-Ion Radiation. Int J Radiat Biol 1999, 75, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Bendinger, A.L.; Seyler, L.; Saager, M.; Debus, C.; Peschke, P.; Komljenovic, D.; Debus, J.; Peter, J.; Floca, R.O.; Karger, C.P.; et al. Impact of Single Dose Photons and Carbon Ions on Perfusion and Vascular Permeability: A Dynamic Contrast-Enhanced MRI Pilot Study in the Anaplastic Rat Prostate Tumor R3327-AT1. Radiat Res 2019, 193, 34. [Google Scholar] [CrossRef]
- Bassler, N.; Jäkel, O.; Søndergaard, C.S.; Petersen, J.B. Dose- and LET-Painting with Particle Therapy. Acta Oncol 2010, 49, 1170–1176. [Google Scholar] [CrossRef]
- Hagiwara, Y.; Bhattacharyya, T.; Matsufuji, N.; Isozaki, Y.; Takiyama, H.; Nemoto, K.; Tsuji, H.; Yamada, S. Influence of Dose-Averaged Linear Energy Transfer on Tumour Control after Carbon-Ion Radiation Therapy for Pancreatic Cancer. Clin Transl Radiat Oncol 2020, 21, 19–24. [Google Scholar] [CrossRef]
- Matsumoto, S.; Lee, S.H.; Imai, R.; Inaniwa, T.; Matsufuji, N.; Fukahori, M.; Kohno, R.; Yonai, S.; Okonogi, N.; Yamada, S.; et al. Unresectable Chondrosarcomas Treated With Carbon Ion Radiotherapy: Relationship Between Dose-Averaged Linear Energy Transfer and Local Recurrence. Anticancer Res 2020, 40, 6429–6435. [Google Scholar] [CrossRef]
- Molinelli, S.; Magro, G.; Mairani, A.; Allajbej, A.; Mirandola, A.; Chalaszczyk, A.; Imparato, S.; Ciocca, M.; Fiore, M.R.; Orlandi, E. How LEM-Based RBE and Dose-Averaged LET Affected Clinical Outcomes of Sacral Chordoma Patients Treated with Carbon Ion Radiotherapy. Radiotherapy and Oncology 2021, 163, 209–214. [Google Scholar] [CrossRef]
- Morelli, L.; Parrella, G.; Molinelli, S.; Magro, G.; Annunziata, S.; Mairani, A.; Chalaszczyk, A.; Fiore, M.R.; Ciocca, M.; Paganelli, C.; et al. A Dosiomics Analysis Based on Linear Energy Transfer and Biological Dose Maps to Predict Local Recurrence in Sacral Chordomas after Carbon-Ion Radiotherapy. Cancers (Basel) 2022, 15, 33. [Google Scholar] [CrossRef]
- Okonogi, N.; Matsumoto, S.; Fukahori, M.; Furuichi, W.; Inaniwa, T.; Matsufuji, N.; Imai, R.; Yamada, S.; Kanematsu, N.; Tsuji, H. Dose-Averaged Linear Energy Transfer per Se Does Not Correlate with Late Rectal Complications in Carbon-Ion Radiotherapy. Radiotherapy and Oncology 2020, 153, 272–278. [Google Scholar] [CrossRef]
- Mastella, E.; Molinelli, S.; Magro, G.; Russo, S.; Bonora, M.; Ronchi, S.; Ingargiola, R.; Jensen, A.D.; Ciocca, M.; Vischioni, B.; et al. In Silico Feasibility Study of Carbon Ion Radiotherapy With Simultaneous Integrated Boost for Head and Neck Adenoid Cystic Carcinoma. Front Oncol 2021, 11. [Google Scholar] [CrossRef]
- Simultaneous Integrated Boost in Carbon Ion Radiotherapy for Head and Neck Adenoid Cystic Carcinoma (SIBACIRT). ClinicalTrials.Gov Identifier: NCT05733910. Updated May 25, 2023. Accessed August 9, 2023. Https://Clinicaltrials.Gov/Study/NCT05733910.
- Hu, W.; Li, P.; Hong, Z.; Guo, X.; Pei, Y.; Zhang, Z.; Zhang, Q. Functional Imaging-Guided Carbon Ion Irradiation with Simultaneous Integrated Boost for Localized Prostate Cancer: Study Protocol for a Phase II Randomized Controlled Clinical Trial. Trials 2022, 23, 934. [Google Scholar] [CrossRef]
- Functional Image-Guided Carbon Ion Irradiation With Simultaneous Integrated Boost for Prostate Cancer. ClinicalTrials.Gov Identifier: NCT05010343. Updated November 15, 2021. Accessed August 9, 2023. Https://Clinicaltrials.Gov/Study/NCT05010343.
- Ablative Carbon Ion Radiotherapy With Pencil Beam Scanning for Locally Advanced Unresectable Pancreatic Cancer. ClinicalTrials.Gov Identifier: NCT05424159. Updated June 24, 2022. Accessed August 9, 2023. Https://Clinicaltrials.Gov/Study/NCT05424159.
- Gemmel, A.; Hasch, B.; Ellerbrock, M.; Kraft-Weyrather, W.; Krämer, M. Biological Dose Optimization with Multiple Ion Fields. Phys Med Biol 2008, 53, 6691–6701. [Google Scholar] [CrossRef]
- Li, X.; Ding, X.; Zheng, W.; Liu, G.; Janssens, G.; Souris, K.; Barragán-Montero, A.M.; Yan, D.; Stevens, C.; Kabolizadeh, P. Linear Energy Transfer Incorporated Spot-Scanning Proton Arc Therapy Optimization: A Feasibility Study. Front Oncol 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Mein, S.; Tessonnier, T.; Kopp, B.; Schömers, C.; Harrabi, S.; Abdollahi, A.; Debus, J.; Haberer, T.; Mairani, A. Biological Dose Optimization for Particle Arc Therapy Using Helium and Carbon Ions. International Journal of Radiation Oncology*Biology*Physics 2022, 114, 334–348. [Google Scholar] [CrossRef] [PubMed]
- Volz, L.; Sheng, Y.; Durante, M.; Graeff, C. Considerations for Upright Particle Therapy Patient Positioning and Associated Image Guidance. Front Oncol 2022, 12. [Google Scholar] [CrossRef]
- Hegarty, S.; Hardcastle, N.; Korte, J.; Kron, T.; Everitt, S.; Rahim, S.; Hegi-Johnson, F.; Franich, R. Please Place Your Seat in the Full Upright Position: A Technical Framework for Landing Upright Radiation Therapy in the 21st Century. Front Oncol 2022, 12. [Google Scholar] [CrossRef]
- Nachankar, A.; Schafasand, M.; Hug, E.; Carlino, A.; Stock, M.; Góra, J.; Fossati, P. Retrospective Evaluation of LET Distribution in Carbon-Ion Radiotherapy for Pelvic Sarcomas and LET Optimization by Blocking Method: The MedAustron Approach. In Proceedings of the Proceedings to the 61th Annual Conference of the Particle Therapy Cooperative Group; 2023.
- Bassler, N.; Toftegaard, J.; Lühr, A.; Sørensen, B.S.; Scifoni, E.; Krämer, M.; Jäkel, O.; Mortensen, L.S.; Overgaard, J.; Petersen, J.B. LET-Painting Increases Tumour Control Probability in Hypoxic Tumours. Acta Oncol (Madr) 2014, 53, 25–32. [Google Scholar] [CrossRef]
- Malinen, E.; Søvik, Å. Dose or ‘LET’ Painting – What Is Optimal in Particle Therapy of Hypoxic Tumors? Acta Oncol (Madr) 2015, 54, 1614–1622. [Google Scholar] [CrossRef]
- Kohno, R.; Koto, M.; Ikawa, H.; Lee, S.H.; Sato, K.; Hashimoto, M.; Inaniwa, T.; Shirai, T. High-LET Irradiation in Clinical Carbon-Ion Beam with the LET Painting Technique for Head and Neck Cancer Patients. Adv Radiat Oncol 2023, 101317. [Google Scholar] [CrossRef]
- Sokol, O.; Scifoni, E.; Tinganelli, W.; Kraft-Weyrather, W.; Wiedemann, J.; Maier, A.; Boscolo, D.; Friedrich, T.; Brons, S.; Durante, M.; et al. Oxygen Beams for Therapy: Advanced Biological Treatment Planning and Experimental Verification. Phys. Med. Biol. 2017, 62, 7798. [Google Scholar] [CrossRef]
- Inaniwa, T.; Kanematsu, N.; Noda, K.; Kamada, T. Treatment Planning of Intensity Modulated Composite Particle Therapy with Dose and Linear Energy Transfer Optimization. Phys Med Biol 2017, 1–23. [Google Scholar] [CrossRef]
- Inaniwa, T.; Kanematsu, N.; Shinoto, M.; Koto, M.; Yamada, S. Adaptation of Stochastic Microdosimetric Kinetic Model to Hypoxia for Hypo-Fractionated Multi-Ion Therapy Treatment Planning. Phys Med Biol 2021, 66, 205007. [Google Scholar] [CrossRef]
- Sokol, O.; Krämer, M.; Hild, S.; Durante, M.; Scifoni, E. Kill Painting of Hypoxic Tumors with Multiple Ion Beams. Phys Med Biol 2019, 64. [Google Scholar] [CrossRef]
- Tubin, S.; Popper, H.H.; Brcic, L. Novel Stereotactic Body Radiation Therapy (SBRT)-Based Partial Tumor Irradiation Targeting Hypoxic Segment of Bulky Tumors (SBRT-PATHY): Improvement of the Radiotherapy Outcome by Exploiting the Bystander and Abscopal Effects. Radiation Oncology 2019, 14, 21. [Google Scholar] [CrossRef]
- Tubin, S.; Gupta, S.; Grusch, M.; Popper, H.H.; Brcic, L.; Ashdown, M.L.; Khleif, S.N.; Peter-Vörösmarty, B.; Hyden, M.; Negrini, S.; et al. Shifting the Immune-Suppressive to Predominant Immune-Stimulatory Radiation Effects by SBRT-PArtial Tumor Irradiation Targeting HYpoxic Segment (SBRT-PATHY). Cancers (Basel) 2020, 13, 50. [Google Scholar] [CrossRef] [PubMed]
- Durante, M.; Brenner, D.J.; Formenti, S.C. Does Heavy Ion Therapy Work Through the Immune System? International Journal of Radiation Oncology*Biology*Physics 2016, 96, 934–936. [Google Scholar] [CrossRef] [PubMed]
- Tubin, S.; Fossati, P.; Carlino, A.; Martino, G.; Gora, J.; Stock, M.; Hug, E. Novel Carbon Ion and Proton Partial Irradiation of Recurrent Unresectable Bulky Tumors (Particle-PATHY): Early Indication of Effectiveness and Safety. Cancers (Basel) 2022, 14, 2232. [Google Scholar] [CrossRef] [PubMed]
- Tubin, S.; Vozenin, M.C.; Prezado, Y.; Durante, M.; Prise, K.M.; Lara, P.C.; Greco, C.; Massaccesi, M.; Guha, C.; Wu, X.; et al. Novel Unconventional Radiotherapy Techniques: Current Status and Future Perspectives – Report from the 2nd International Radiation Oncology Online Seminar. Clin Transl Radiat Oncol 2023, 40, 100605. [Google Scholar] [CrossRef]
- Cao, X.; Rao Allu, S.; Jiang, S.; Jia, M.; Gunn, J.R.; Yao, C.; LaRochelle, E.P.; Shell, J.R.; Bruza, P.; Gladstone, D.J.; et al. Tissue PO2 Distributions in Xenograft Tumors Dynamically Imaged by Cherenkov-Excited Phosphorescence during Fractionated Radiation Therapy. Nat Commun 2020, 11, 573. [Google Scholar] [CrossRef]
- Myllylä, T.; Korhonen, V.; Karthikeyan, P.; Honka, U.; Lohela, J.; Inget, K.; Ferdinando, H.; Karhula, S.S.; Nikkinen, J. Cerebral Tissue Oxygenation Response to Brain Irradiation Measured during Clinical Radiotherapy. J Biomed Opt 2023, 28. [Google Scholar] [CrossRef]
- Horsman, M.R.; Mortensen, L.S.; Petersen, J.B.; Busk, M.; Overgaard, J. Imaging Hypoxia to Improve Radiotherapy Outcome. Nat Rev Clin Oncol 2012, 9, 674–687. [Google Scholar] [CrossRef]
- Gérard, M.; Corroyer-Dulmont, A.; Lesueur, P.; Collet, S.; Chérel, M.; Bourgeois, M.; Stefan, D.; Limkin, E.J.; Perrio, C.; Guillamo, J.-S.; et al. Hypoxia Imaging and Adaptive Radiotherapy: A State-of-the-Art Approach in the Management of Glioma. Front Med (Lausanne) 2019, 6. [Google Scholar] [CrossRef]
- Busk, M.; Overgaard, J.; Horsman, M.R. Imaging of Tumor Hypoxia for Radiotherapy: Current Status and Future Directions. Semin Nucl Med 2020, 50, 562–583. [Google Scholar] [CrossRef]
- Schiavo, F.; Toma-Dasu, I.; Lindblom, E.K. Perfusion-Limited Hypoxia Determines the Outcome of Radiation Therapy of Hypoxic Tumours. In Oxygen Transport to Tissue XLIII. Advances in Experimental Medicine and Biology; Scholkmann, F., LaManna, J., Wolf, U., Eds.; Springer, 2022; Vol. 1395, pp. 249–254.
- Schiavo, F.; Kjellsson Lindblom, E.; Toma-Dasu, I. Towards the Virtual Tumor for Optimizing Radiotherapy Treatments of Hypoxic Tumors: A Novel Model of Heterogeneous Tissue Vasculature and Oxygenation. J Theor Biol 2022, 547, 111175. [Google Scholar] [CrossRef]
- Lazzeroni, M.; Toma-Dasu, I.; Ureba, A.; Schiavo, F.; Wiedenmann, N.; Bunea, H.; Thomann, B.; Baltas, D.; Mix, M.; Stoykow, C.; et al. Quantification of Tumor Oxygenation Based on FMISO PET: Influence of Location and Oxygen Level of the Well-Oxygenated Reference Region. In Oxygen Transport to Tissue XLI. Advances in Experimental Medicine and Biology; Ryu, P.D., LaManna, J., Harrison, D., Lee, S.S., Eds.; Springer, 2020; Vol. 1232, pp. 177–182.
- Overgaard, J. Hypoxic Radiosensitization: Adored and Ignored. Journal of Clinical Oncology 2007, 25, 4066–4074. [Google Scholar] [CrossRef]
- Sørensen, B.S.; Horsman, M.R. Tumor Hypoxia: Impact on Radiation Therapy and Molecular Pathways. Front Oncol 2020, 10. [Google Scholar] [CrossRef]
- Wozny, A.-S.; Gauthier, A.; Alphonse, G.; Malésys, C.; Varoclier, V.; Beuve, M.; Brichart-Vernos, D.; Magné, N.; Vial, N.; Ardail, D.; et al. Involvement of HIF-1α in the Detection, Signaling, and Repair of DNA Double-Strand Breaks after Photon and Carbon-Ion Irradiation. Cancers (Basel) 2021, 13, 3833. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Xie, H.; Liu, Y.; Xia, C.; Cun, X.; Long, Y.; Chen, X.; Deng, M.; Guo, R.; Zhang, Z.; et al. Knockdown of Hypoxia-Inducible Factor-1 Alpha by Tumor Targeted Delivery of CRISPR/Cas9 System Suppressed the Metastasis of Pancreatic Cancer. Journal of Controlled Release 2019, 304, 204–215. [Google Scholar] [CrossRef]
- Lang, J.; Zhao, X.; Wang, X.; Zhao, Y.; Li, Y.; Zhao, R.; Cheng, K.; Li, Y.; Han, X.; Zheng, X.; et al. Targeted Co-Delivery of the Iron Chelator Deferoxamine and a HIF1α Inhibitor Impairs Pancreatic Tumor Growth. ACS Nano 2019, 13, 2176–2189. [Google Scholar] [CrossRef]
- Xiong, L.; Zhao, T.; Huang, X.; Liu, Z.; Zhao, H.; Li, M.; Wu, L.; Shu, H.; Zhu, L.; Fan, M. Heat Shock Protein 90 Is Involved in Regulation of Hypoxia-Driven Proliferation of Embryonic Neural Stem/Progenitor Cells. Cell Stress Chaperones 2009, 14, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Kataria, N.; Martinez, C.-A.; Kerr, B.; Zaiter, S.S.; Morgan, M.; McAlpine, S.R.; Cook, K.M. C-Terminal HSP90 Inhibitors Block the HIF-1 Hypoxic Response by Degrading HIF-1α through the Oxygen-Dependent Degradation Pathway. Cellular Physiology and Biochemistry 2019, 53, 480–495. [Google Scholar] [CrossRef] [PubMed]
- Li, H.K.; Matsumoto, Y.; Furusawa, Y.; Kamada, T. PU-H71, a Novel Hsp90 Inhibitor, as a Potential Cancer-Specific Sensitizer to Carbon-Ion Beam Therapy. J Radiat Res 2016, 57, 572–575. [Google Scholar] [CrossRef]
- Lee, Y.; Li, H.K.; Masaoka, A.; Sunada, S.; Hirakawa, H.; Fujimori, A.; Nickoloff, J.A.; Okayasu, R. The Purine Scaffold Hsp90 Inhibitor PU-H71 Sensitizes Cancer Cells to Heavy Ion Radiation by Inhibiting DNA Repair by Homologous Recombination and Non-Homologous End Joining. Radiotherapy and Oncology 2016, 121, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Wilson, W.R.; Hay, M.P. Targeting Hypoxia in Cancer Therapy. Nat Rev Cancer 2011, 11, 393–410. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Arambula, J.F.; Koo, S.; Kumar, R.; Singh, H.; Sessler, J.L.; Kim, J.S. Hypoxia-Targeted Drug Delivery. Chem Soc Rev 2019, 48, 771–813. [Google Scholar] [CrossRef]
- Li, Y.; Zhao, L.; Li, X.-F. Targeting Hypoxia: Hypoxia-Activated Prodrugs in Cancer Therapy. Front Oncol 2021, 11. [Google Scholar] [CrossRef]
- Mistry, I.N.; Thomas, M.; Calder, E.D.D.; Conway, S.J.; Hammond, E.M. Clinical Advances of Hypoxia-Activated Prodrugs in Combination With Radiation Therapy. International Journal of Radiation Oncology*Biology*Physics 2017, 98, 1183–1196. [Google Scholar] [CrossRef] [PubMed]
- Higgins, G.S.; O’Cathail, S.M.; Muschel, R.J.; McKenna, W.G. Drug Radiotherapy Combinations: Review of Previous Failures and Reasons for Future Optimism. Cancer Treat Rev 2015, 41, 105–113. [Google Scholar] [CrossRef]
- Hunter, F.W.; Wouters, B.G.; Wilson, W.R. Hypoxia-Activated Prodrugs: Paths Forward in the Era of Personalised Medicine. Br J Cancer 2016, 114, 1071–1077. [Google Scholar] [CrossRef]
- Spiegelberg, L.; Houben, R.; Niemans, R.; de Ruysscher, D.; Yaromina, A.; Theys, J.; Guise, C.P.; Smaill, J.B.; Patterson, A. V.; Lambin, P.; et al. Hypoxia-Activated Prodrugs and (Lack of) Clinical Progress: The Need for Hypoxia-Based Biomarker Patient Selection in Phase III Clinical Trials. Clin Transl Radiat Oncol 2019, 15, 62–69. [Google Scholar] [CrossRef]
- Anduran, E.; Dubois, L.J.; Lambin, P.; Winum, J.-Y. Hypoxia-Activated Prodrug Derivatives of Anti-Cancer Drugs: A Patent Review 2006 – 2021. Expert Opin Ther Pat 2022, 32, 1–12. [Google Scholar] [CrossRef]
Figure 1.
Oxygen enhancement ratio vs. dose-averaged LET at different oxygenation levels (pO2) according to the model [50] adapted for the parameters for the CHO cell line.
Figure 1.
Oxygen enhancement ratio vs. dose-averaged LET at different oxygenation levels (pO2) according to the model [50] adapted for the parameters for the CHO cell line.
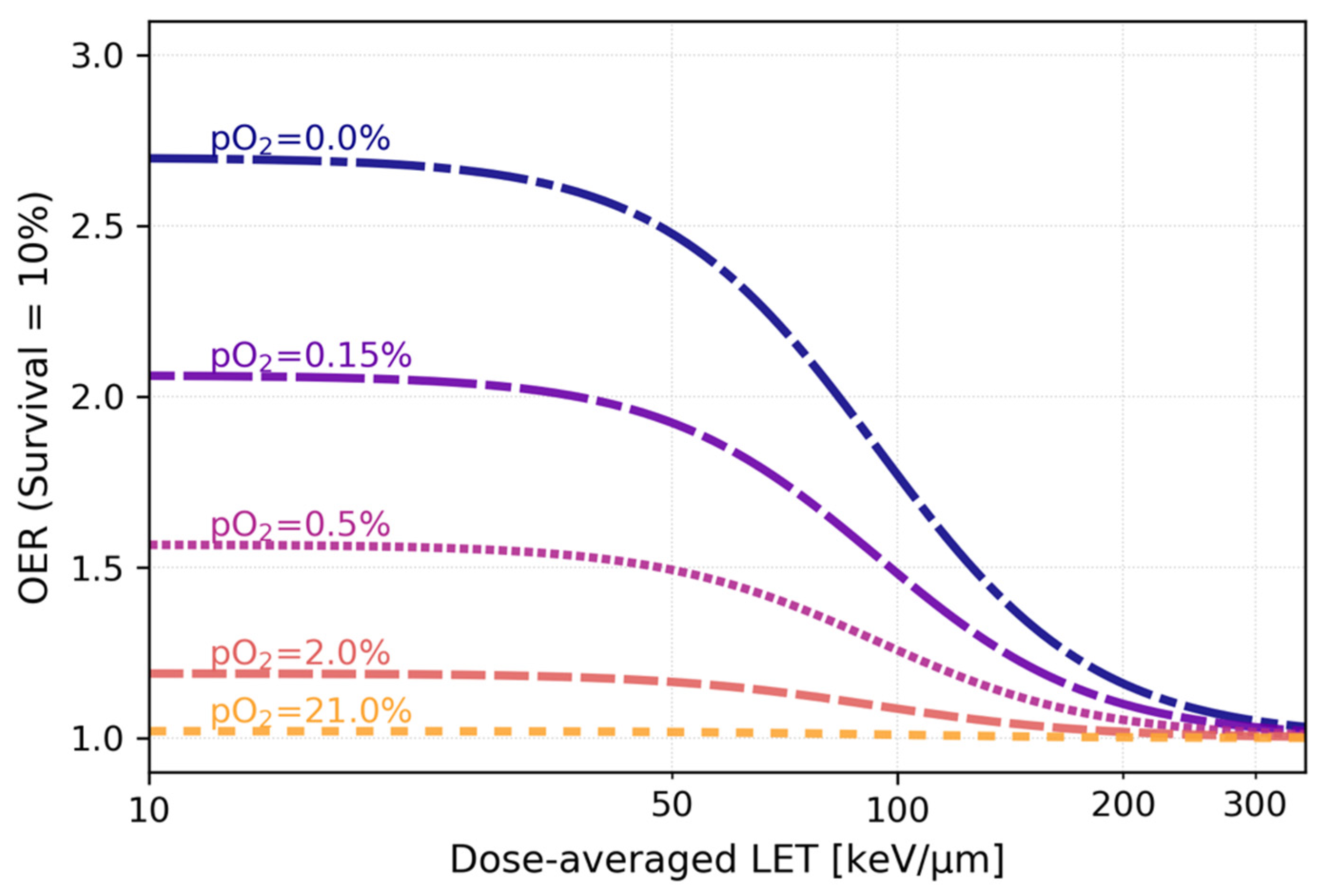
Figure 2.
Tumor reoxygenation following irradiation. Death of irradiated normoxic (red color) cells causes the tumor shrinkage, which, in turn, would lead to the regrowth of blood vessels and supply of previously hypoxic (blue color) cells with oxygen, increasing their radiosensitivity. Created with BioRender.com.
Figure 2.
Tumor reoxygenation following irradiation. Death of irradiated normoxic (red color) cells causes the tumor shrinkage, which, in turn, would lead to the regrowth of blood vessels and supply of previously hypoxic (blue color) cells with oxygen, increasing their radiosensitivity. Created with BioRender.com.
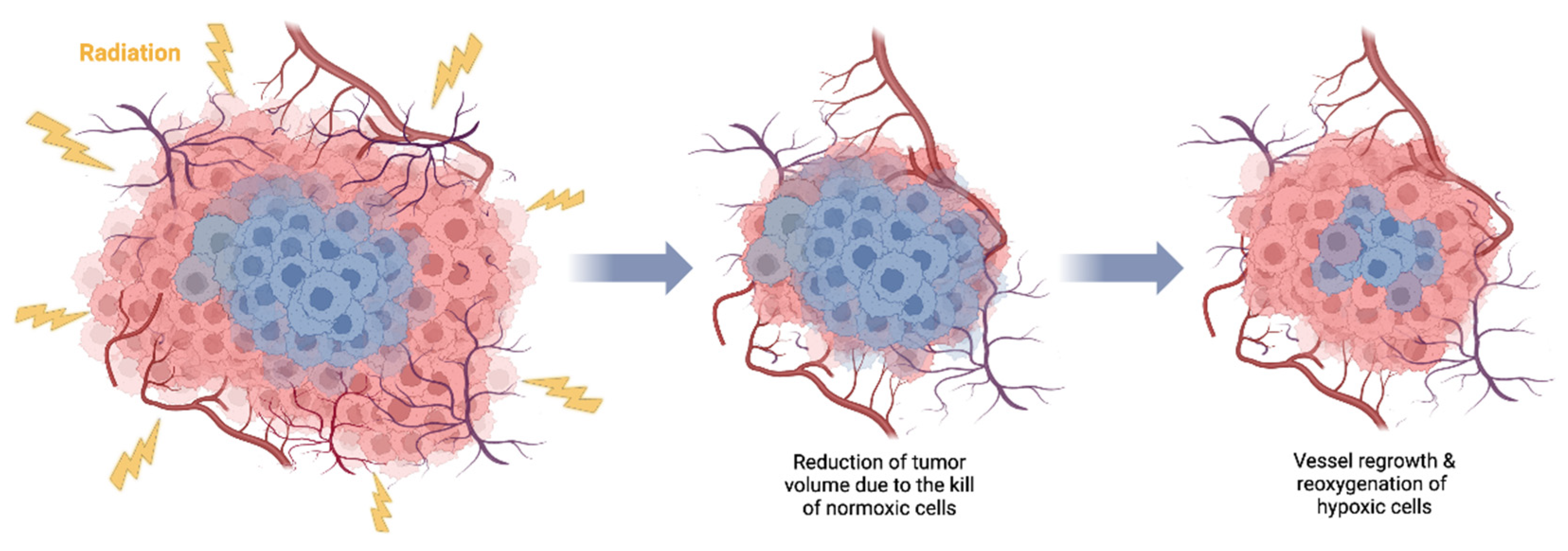
Figure 3.
A-C: a representative case of pancreatic tumor treated with carbon-ion radiotherapy (A - dose distribution, B - dLET distribution, C - dLET distribution above 50 keV/ μm; adapted from [94]). D: comparison of minimum values of dLET within the GTVs of pancreatic tumors with local control or local failure; adapted from [94]. E: average LETd values in the PTVs of chondrosarcomas and their correlation with tumor volumes and recurrencies (black squares - non-recurrent cases, red circles denote - recurrent cases); no recurrencies were observed for tumors smaller than approximately 300 ml. Adapted from [95].
Figure 3.
A-C: a representative case of pancreatic tumor treated with carbon-ion radiotherapy (A - dose distribution, B - dLET distribution, C - dLET distribution above 50 keV/ μm; adapted from [94]). D: comparison of minimum values of dLET within the GTVs of pancreatic tumors with local control or local failure; adapted from [94]. E: average LETd values in the PTVs of chondrosarcomas and their correlation with tumor volumes and recurrencies (black squares - non-recurrent cases, red circles denote - recurrent cases); no recurrencies were observed for tumors smaller than approximately 300 ml. Adapted from [95].
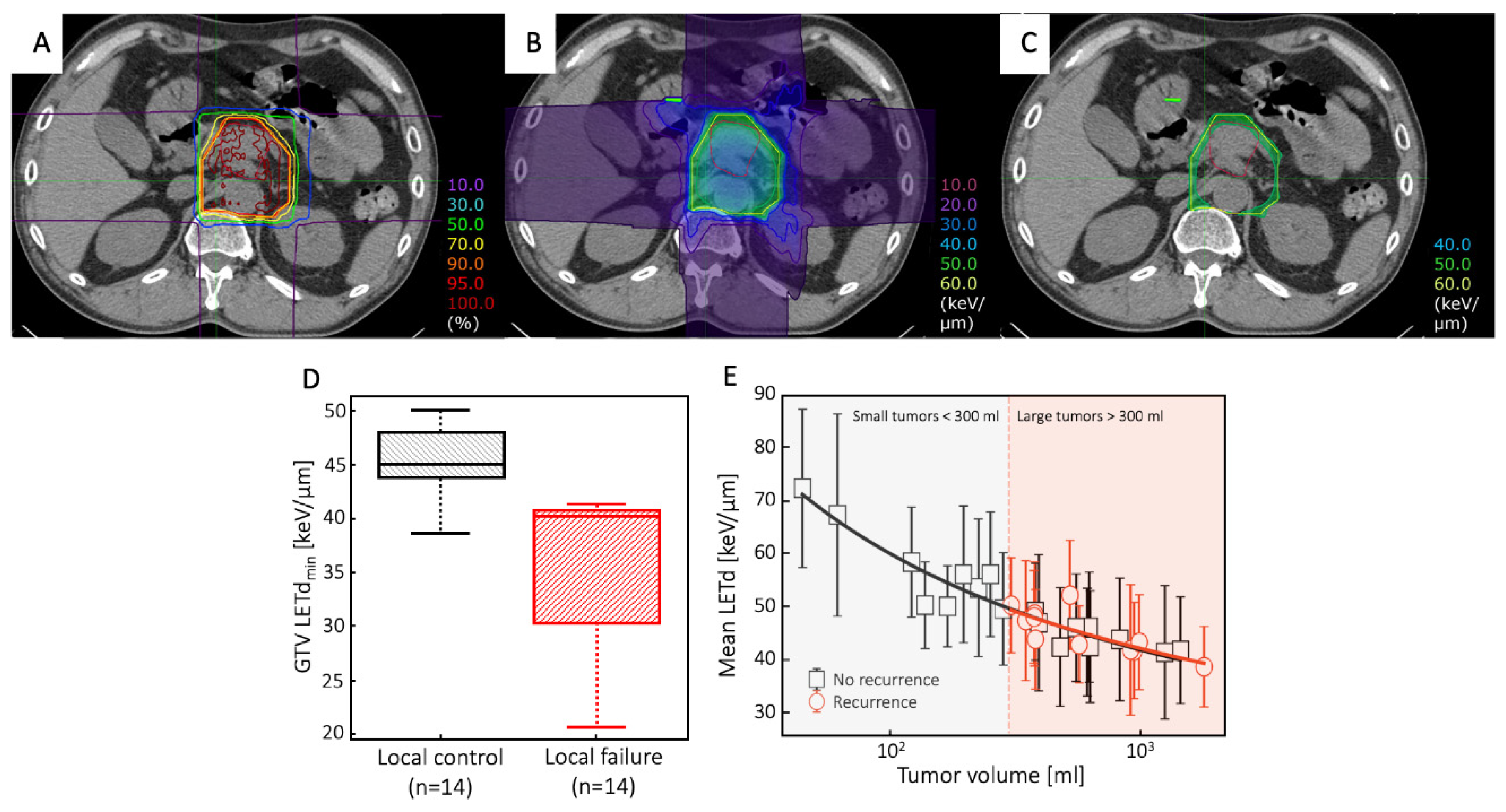
Figure 4.
LETd distribution calculated in 12C two-field treatment plan for chordoma optimized either for a uniform PTV dose of 3 Gy(RBE) (A) or for additional GTV dose boost of 1.5 Gy(RBE) (B). White and black contours represent PTV and GTV, respectively. C: LETd-volume histograms for boosted (solid lines) and non-boosted treatment plans (dashed lines) for tumor GTV (black lines) and PTV (grey lines). Calculations were performed using GSI in-house treatment planning software TRiP98 [104]. Anonymized CT data is taken from the pilot project repository of GSI, where treatment was performed, according to the German law. Informed consent is waived by the ethical committee of the University of Heidelberg for anonymized plans used for research plans.
Figure 4.
LETd distribution calculated in 12C two-field treatment plan for chordoma optimized either for a uniform PTV dose of 3 Gy(RBE) (A) or for additional GTV dose boost of 1.5 Gy(RBE) (B). White and black contours represent PTV and GTV, respectively. C: LETd-volume histograms for boosted (solid lines) and non-boosted treatment plans (dashed lines) for tumor GTV (black lines) and PTV (grey lines). Calculations were performed using GSI in-house treatment planning software TRiP98 [104]. Anonymized CT data is taken from the pilot project repository of GSI, where treatment was performed, according to the German law. Informed consent is waived by the ethical committee of the University of Heidelberg for anonymized plans used for research plans.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



