
Submitted:
16 August 2023
Posted:
18 August 2023
You are already at the latest version
Abstract
This study assessed the potential of back extensor strength as an alternative marker of frailty. A total of 560 farmers were included. Computed tomography scans measured fat and muscle mass volumes at the mid-L4 vertebral level. Back extensor strength was measured in a seated posture. Multivariate linear regression analyzed the associations between back extensor strength and trunk muscle/fat compositions. The participants were divided into two groups based on back extensor strength. Propensity score matching, multivariate logistic regression, and Extreme Gradient Boosting (XGBoost) were employed to evaluate the relationship between Fried's frailty criteria and back extensor strength. Back extensor strength exhibited positive associations with abdominal muscle volume (r = 1.12) as well as back muscle volume (r = 0.89) (p < 0.05). Lower back extensor strength was linked to more frail status, such as reduced grip strength, walking speed, and fre-quent self-reported exhaustion. Multivariate logistic regression indicated a significant association between lower back extensor strength and higher Fried frailty score (OR, 0.990; p<0.05). XGBoost analysis identified back extensor strength as the most important predictor (gain = 0.502) for frailty, surpassing the significance of age (gain = 0.325). These findings suggested the potential of back extensor strength as an alternative frailty marker.
Keywords:
muscle strength
; frailty
; machine learning
1. Introduction
Frailty is a geriatric condition characterized by increased vulnerability to external stressors [1]. It has been associated with adverse health outcomes, including higher mortality rates, increased risk of falls, and chronic diseases [2]. In 2001, Fried proposed a frailty assessment using five physical components, including grip strength [3]. Subsequently, various frailty classifications have been developed and implemented in clinical and research settings [4,5]. However, Fried’s frailty remains widely used and recognized for frailty assessment [6,7].
After Fried proposed grip strength as a frailty criterion, it has been shown to be an objective and reliable predictor of health outcomes [8,9]. However, it is important to note that grip strength is influenced by various factors beyond aging-related changes. Lifestyle factors, such as nutrition and depression status, have also been shown to impact grip strength [10,11]. Studies conducted in eleven European countries have revealed that even economic crises, such as a decrease in gross domestic product (GDP), can be associated with reduced grip strength [12]. These findings highlight the multifactorial nature of grip strength and emphasize the need to consider a comprehensive range of determinants when interpreting its significance as a frailty marker. Grip strength is not solely reflective of age-related decline but is influenced by a complex interplay of individual, societal, and economic factors.
As an alternative approach, researchers have studied muscle strength in different body parts [13]. By investigating muscle strength beyond hand grip, they aim to capture a more comprehensive understanding of an individual’s physical function and overall frailty status. Furthermore, the development of newly advanced dynamometers has enabled a wide range of muscle strength measurements, providing new possibilities for assessing muscle strength in multiple parts of the body, not just limited to hand grip strength [14,15].
The back extensor muscles play a crucial role in maintaining posture, stability, and overall trunk function [16]. Weakness or dysfunction in these muscles may contribute to balance issues, gait abnormalities, and increased vulnerability to falls, which are key components of frailty [17]. Understanding the impact of back extensor strength on frailty could have significant clinical implications.
The aim of this cross-sectional study was to explore the relationship between back extensor strength and trunk muscle/fat compositions, with a specific focus on investigating the potential of back extensor strength as an alternative marker of frailty. This study utilized a specifically designed chair equipped with a portable dynamometer to assess the strength of the back extensors. We anticipated a correlation between frailty status and back extensor strength, which could be explained by trunk muscle/fat composition. By investigating these associations, the study aimed to contribute to the understanding of the role of back extensor strength in frailty and its potential utility as a frailty marker.
2. Materials and Methods
2.1. Participants
For participant enrollment, a total of 446 eligible participants were selected from the Farmers’ Cohort for Agricultural Work-Related Musculoskeletal Disorders study conducted from 2013 to 2014, and 339 participants were selected from individuals involved in farming. The characteristics of participants have been detailed in previous study [18]. In consideration of the physically demanding nature and varied ergonomic tasks involved in farming [19,20] that contribute to specific changes in muscle volume, individuals who were not engaged in farming were excluded from the study. As a result, 590 individuals actively involved in farming participated in this study [21]. To mitigate the influence of external factors that could cause a decline in muscle volume, we excluded 21 participants with a history of spine surgery, as it is known to induce para-spinal muscle atrophy [22]. Additionally, nine participants with missing back extensor strength data were not included in the cross-sectional analysis, resulting in a total of 560 participants in the final analysis (Figure 1).
2.2. Measurements
2.2.1. Frailty Score
Frailty was measured based on Fried’s five criteria. Each criterion had values of 1 or 0: weight loss (weight loss in the past year ≥ 4.5 kg), self-reported exhaustion (at least three days a week), low physical activity (metabolic equivalent within the lowest 20%, adjusted for sex), slowness (usual 4-m gait speed within the lowest 20%, adjusted for sex and height), and weakness (grip strength within the lowest 20%, adjusted for body mass index and sex). Based on the number of satisfied criteria, participants were divided into two groups, non-frail (frailty score of 0–2) and frail (frailty score of 3–5).
Exhaustion was defined by answering the following question from the Center for Epidemiological Studies Depression Scale: “I felt all I did was an effort” for three or more days per week. Physical activity was assessed using the Korean version of the International Physical Activity Questionnaire [23]. To determine slowness, participants were divided into four groups based on sex and the median value of height, and the lowest 20% of the 4-m gait speed was calculated for each group and used as the cutoff value for slowness. Grip strength was measured three times on both hands, and the mean of these three values was calculated for each hand. The higher mean grip strength from both hands was selected for further analysis. To determine the weakness of grip strength, participants were divided into four groups based on sex and the median value of body mass index (BMI), and the lowest 20% of the grip strength was calculated for each group and used as the cutoff value for weakness.
2.2.2. Back Extensor Strength
The isometric strength of the back extensor was measured using the PrimusRS system (BTE Technologies Inc., Hanover, MD, USA) while participants were seated in a high chair to prevent their feet from touching the floor [24]. The height of the anchoring cable was modified to the height of the participants’ T7 spinous process level, and a seatbelt was used to stabilize the participants’ thighs. Participants were asked to push back as far as possible, which took 3 seconds with isometric back extension. The cable anchored to the chest harness was pulled, and the isometric strength was measured. This process was repeated five times, and the mean of the three median values (excluding the maximum and minimum values) was used.
2.2.3. Trunk Muscle/Fat Mass
The trunk muscle/fat mass measurement protocol in this study has been previously explained [25]. Ten consecutive computed tomography (CT) images at the mid-L4 vertebral level were acquired using a Philips MX 8000 IDT CT scanner (Philips Medical Systems, Cleveland, OH, USA), with exposure at 200 mAs, tube voltage set at 120 kV, and 1 mm thickness of slice. Total muscle mass (TMM, cm3) and total fat mass (TFM, cm3) in the trunk region were obtained using image processing software (Extended Brilliance Workspace version 4.5.3; Philips Healthcare, Best, The Netherlands). Pre-defined radiation attenuation ranges were used to demarcate adipose (from -190 HU to -30 HU) and muscle (-29 HU to +150 HU) tissues. TMM was subdivided into back muscle mass (BMM, cm3), psoas muscle mass (PMM, cm3), and abdominal muscle mass (AMM, cm3). BMM and PMM were derived manually from the TMM. AMM was obtained by subtracting PMM and BMM from TMM. The BMM consisted of the multifidus, iliocostalis lumborum, longissimus, and quadratus lumborum muscles. Visceral fat mass (VFM, cm3) was calculated by manually outlining the inner abdominal wall, and subcutaneous fat mass (SFM, cm3) was calculated by subtracting the VFM from the TFM. To reduce bias, one technician performed all scan and image processing procedures.
2.3. Statistical Analyses
All analyses were performed using R version 4.2.2. (The R Foundation, Vienna, Austria), Windows 10 [26]. Statistical significance was set at p<.05. The baseline characteristics of the study participants were presented and compared in two ways: between men and women; and between age < 65 years and age ≥ 65 years. Categorical variables are expressed as numbers and percentages and were compared using the chi-squared test. Continuous variables were expressed as the mean and standard deviation and were compared using Student’s t-test. A linear regression analysis was performed to examine the relationship between trunk muscle/fat composition and back extensor strength. We analyzed the presence of multicollinearity using the variance inflation factor (VIF), with covariates having absolute values of VIF > 10 indicating multicollinearity [27].
To determine the relative importance of covariates in linear regression, relative weight analysis (RWA) was calculated [28]. The absolute value of the RWA was used to indicate the correlation between the covariate and back extensor strength, with positive and negative RWA values indicating a positive and negative relationship with back extensor strength, respectively.
2.3.1. Propensity Score Matching
The participants were divided into two groups based on their back extensor strength, with the lowest 20% strength considered as one group and the rest as the higher group. Since the result of descriptive analysis, as shown in Table 1 and Table 2, indicated a significant relationship between sex, age, frailty, and back extensor strength, we performed propensity score (PS) matching of age and sex. The purpose of PS matching was to reduce the confounding effects by adjusting for confounding factors. PS is the conditional probability of an individual being in a certain group, based on covariates or predictor variables in the model [29]. Many researchers have used PS matching in medical and social science studies to reduce selection bias [30,31]. The nearest neighbor (NN) with a PS caliper, which imposed a tolerance level on the maximum PS distance, was used to match the two groups to reduce the risk of bad matches when the closest neighbor is located far away [32]. The matching ratio between the two groups was set as high as possible to increase the number of participants in the analysis. The standardized mean difference (SMD) of covariates was used to evaluate how well the two groups were paired, and an SMD less than 0.1 was accepted as the confounding bias was significantly reduced [33].
2.3.2. Multivariate Logistic Regression
To determine the potential of back extensor strength as a frailty parameter, we conducted a multivariate logistic regression analysis of frailty. We included age, sex, and BMI as covariates in frailty prediction, as these factors are commonly used covariates in strength assessments of frailty [34]. Odds ratios (OR) and 95% confidence intervals (CI) were calculated.
2.3.3. Extreme Gradient Boosting
To demonstrate the possibility of using back extensor strength as a frailty parameter, we performed Extreme Gradient Boosting (XGBoost) [35]. XGBoost is a novel gradient-boosting algorithm that has been proven to enhance the computing power of classification and regression models. The XGBoost model for frailty prediction was performed in two steps: (1) the grid search method was used to determine the optimal XGBoost hyperparameters, and (2) the optimal XGBoost model was repeated 100 times to calculate the CI of the performance parameters.
First, we used the grid search method to optimize the XGBoost hyperparameters (maximum depth of a tree, learning rate, gamma, subsample ratio of the training instance, minimum sum of instance weight, and subsample ratio of columns). For the grid search, the maximum depth of a tree was set to 2, 4, 6, 8, 10, and 12; the learning rate was set to 0.001, 0.0025, 0.005, 0.01, 0.02, 0.04, 0.06, 0.08, 0.1, 0.2, and 0.5; gamma was set to 0, 0.1, 0.5, 1, 2, and 5; the subsample ratio of the training instance was set to 0.75, and 1; the minimum sum of instance weights was set to 1, 2, and 3; the subsample ratio of columns was set to 0.75 and 1. Approximately 4,752 combinations of possible hyperparameters were used in XGBoost, and the root mean square error (RMSE) of each model was compared.
To prevent overfitting, we used five-fold cross-validation. Our study population was split into five groups (“five folds”) equally. In the first iteration, the first fold was used as the test dataset, and the other four folds were used as the training dataset. Using a single combination of hyperparameters, the process was repeated until all folds were used as a test dataset (five iterations). The RMSE of XGBoost was calculated by averaging the results of the five iterations, and the RMSEs of all XGBoost models were compared. The minimum RMSE of XGBoost was obtained: learning rate=0.2, maximum depth of a tree=2, gamma=2, subsample ratio of columns=0.75, minimum sum of instance weight=3, and subsample ratio of the training instance=0.75.
The optimal hyperparameters were then used to perform XGBoost to evaluate frailty with back extensor strength. The optimal XGBoost model was trained to evaluate the group with frailty (frailty score ≥3). In this study, 70% of the participants were used as the training set, and 30% of the participants were used as the test set. The cutoff value for frailty prediction was selected based on Youden’s index [36]. The performance of the optimal XGBoost model was evaluated by calculating the area under the receiver operating characteristic curve [37], with an area under the curve (AUC) of 0.5 considered as null accuracy, and a higher AUC considered as better accuracy. Other classification evaluation metrics, such as accuracy, precision, recall, and f1 score, were also evaluated to assess the predictive power of back extensor strength in the XGBoost classification.
The feature importance of each variable was estimated, and the model provided ‘gain’ as the importance of the feature in the frailty prediction tree branches [38]. The gain for each feature was calculated by dividing the sum of the gains for the feature by the sum of the gains for all the features. Features with higher gains were considered more important in XGBoost model construction. All analyses were repeated 100 times to estimate a 95% CI.
3. Results
3.1. Participant Characteristics
Of the 560 participants, 255 were male, and 305 were female (Table 1). The average age of the participants was 58.0±7.0 years, with an average of 58.5±7.0 years for men and 57.5±6.9 years for women. The muscle/fat compositions, such as TMM, BMM, PMM, AMM, VFM, and SFM, differed between men and women. Female participants had a lower waist circumference than males (p<.001). The CT results showed higher VFM in men (p<.001) and higher SFM in women (p<.001). Men had higher TMM, BMM, PMM, and AMM values (p<.001). In terms of frailty, men exhibited a faster walking speed (p<.05), higher grip strength, and higher back extensor strength (p<.001). There were no significant differences between sexes in terms of age, BMI, TFM, unintentional weight loss, self-reported exhaustion, physical activity, or Fried’s frailty score.
The participants were divided into two categories based on age to capture the impact of aging on trunk muscle/fat compositions (Table 2). There were 90 participants aged ≥65 years and 470 participants aged <65 years. The cutoff age of 65 years in this study was based on the definition of an aging society in Korea [39]. The CT results showed higher TMM, PMM (p<.05), and BMM (p<.001) in participants aged < 65 years. Also, grip strength, back extensor strength (p<.05), and walking speed (p<.001) were higher in the < 65 years group than in the ≥ 65-years group. The frailty score was higher in participants aged ≥ 65 years than in those aged < 65 years (p<.001). Waist circumference, BMI, and fat mass measurements showed no significant differences between the age groups.
3.2. Linear Regression Analysis of Trunk Muscle/Fat Compositions and the Back Extensor Strength
Table 3 shows the results of multivariate linear regression. Since age and sex had confounding effects (Table 1 and Table 2), these factors were adjusted for in the regression analysis. After adjusting for age and sex, a clear trend was observed (p<.05) in which higher back extensor strength was associated with increased AMM (r=1.12) and BMM (r=0.89). The PMM, VFM, and SFM were not significantly related to back extensor strength. Each absolute value of the VIF was <10, indicating that there was no multicollinearity issue. A relative weight analysis showed that AMM (relative weight=0.089) was the most significant predictor among the trunk muscle/fat components, and being female compared with male (relative weight=-0.118) was the most important predictor among all the parameters used.
3.3. PS Matching of the Group with the Lowest 20% Back Extensor Strength
The characteristics of the two groups were compared. One group had a lower back extensor strength of 20%, while the other group had a higher back extensor strength. Before PS matching, the age and sex covariates showed an SMD > 0.1 (Table 4). After PS matching (with a match ratio of 1:3 and a caliper of 0.01), 108 participants from the lowest 20% group and 279 participants from the higher group remained with an SMD < 0.1. Differences between the two groups were assessed using the t-test for continuous variables and the chi-square test for categorical variables. Table 4 shows that grip strength, self-reported exhaustion, and walking speed were significantly different (p<.05) between the lowest 20% back extensor strength group and the higher group, with the lowest 20% back extensor strength group showing greater frailty.
3.4. Back Extensor Strength as a New Predictor of Frailty
The results of the multivariate logistic regression showed that higher back extensor strength was significantly associated with lower odds of frailty (OR, 0.990, 95% CI, 0.983–0.997; p<.05), whereas aging was associated with increased odds of frailty (OR, 1.088, 95% CI, 1.025-1.160, p<.05). The analysis included sex and BMI as confounding factors; however, these factors were not significant predictors of frailty (Table 5).
The results of XGBoost for frailty prediction (frailty score ≥ 3 or not) showed that back extensor strength was the most important predictor of frailty (gain=0.502±0.006), and was more important than age (gain=0.325±0.005), BMI (gain=0.145±0.005), and sex (gain=0.026±0.002). The XGBoost model had an AUC of 0.579±0.004, accuracy of 0.71±0.05, precision of 0.10±0.01, recall of 0.56±0.04, and f1 score of 0.15±0.01 (Figure 2 and Table 6).
4. Discussion
The results of this study revealed a significant association between lower back extensor strength and reduced muscle volume in both the abdominal and back muscles. Additionally, participants with lower back extensor strength exhibited higher levels of frailty according to Fried’s criteria, which was characterized by weaker grip strength, slower walking speed, and more frequent feelings of exhaustion. Both the multivariate logistic regression and the XGBoost model analyses consistently demonstrated that back extensor strength was a highly significant factor of frailty, according to Fried’s criteria. The study revealed that back extensor strength’s importance in predicting frailty was greater than that of age alone, suggesting that the impact of back extensor strength on frailty outcomes outweighed the influence of age.
Previous studies have demonstrated associations between frailty and various muscle strength and volume, including the lower limb, forearm, and trunk [40,41]. However, there is a scarcity of studies that investigate the relationship between muscle strength, muscle volume, and frailty simultaneously. In this study, we evaluated both trunk muscle/fat volume and back extensor strength in the same group of participants. Through the concurrent analysis of muscle volume and muscle strength, our findings suggest a potential association between lower frailty status and increased back extensor strength, alongside increased volume in the abdominal and back muscles. In terms of rehabilitation medicine, exercise programs focused on strengthening the back extensor strength by targeting the abdominal and back muscles can be beneficial for older adults.
Descriptive analysis revealed a difference in muscle/fat composition between sexes, even when considering individuals had similar ages and BMI. Specifically, men exhibited larger visceral fat, while women demonstrated larger subcutaneous fat. These results were supported by previous studies that explained the hormonal differences between the sexes. The primary male sex steroid, androgen, stimulated muscle growth, and increased proliferation, contributing to higher levels of muscle mass in men [42]. Adipose tissues express estrogen receptors with higher activity in subcutaneous fat than in visceral fat. The elevated levels of estradiol in women act more through subcutaneous fat receptors, resulting in decreased lipolysis [43], which leads to higher SFM in women and higher VFM in men.
The multivariate linear regression analysis, which examined the relationship between trunk muscle/fat composition and back extensor strength, showed that specific parts of the trunk were associated with muscle strength. These findings align with a previous study, which also reported a significant correlation between higher back extensor strength and increased body mass and non-fat body mass, as measured using the skinfold thickness evaluation from the Durnin and Womersley method [44]. In our study, we obtained trunk muscle volume measurements using a CT scan. These specifically measured trunk muscle volumes revealed a significant linear relationship between increased back extensor strength and specific parts of the trunk, the higher abdominal and back muscles.
This study showed that the XGBoost model had low predictive power for Fried’s frailty, as measured by metrics such as AUC, accuracy, precision, recall, and f1 score. This outcome can be attributed to the multifactorial nature of Fried’s frailty criteria, including walking speed, physical activities, self-reported exhaustion, unintentional weight loss, and muscle strength. Using limited input variables such as age, sex, BMI, and back extensor strength, resulted in the limited predictive power of this XGBoost model. However, despite this limitation, the XGBoost model still outperformed the null classifier (AUC=0.5) and highlighted back extensor strength as the most influential feature among all the covariates, even more important than the age factor. These results suggest that back extensor strength may be useful in identifying individuals who are at risk of frailty.
Trunk muscle strength was assessed in this study since it has a significant effect on health outcomes. Decreased muscle volume in the lower trunk region at the mid-lumbar level has been reported to be associated with pulmonary, hepatic, and systemic dysfunctions [45]. Furthermore, researchers have emphasized back extensor strength because of its association with fall prevention in older adults, balance deficits, and other age-related symptoms. Older adults who have experienced falls tend to exhibit lower back extensor strength compared to those who have not [46]. Several studies showed that core strengthening program, which targeted the maximal isometric strength of trunk flexors, extensors, and rotators, has shown associations with delaying frailty status by achieving improvements in various aspects such as spinal mobility (maximal extension to flexion and left to right flexion of the trunk), dynamic balance (stride velocity and the Functional Reach test), and functional mobility (Timed Up and Go test) [47,48].
The trunk serves as a kinetic link that facilitates the transfer of torque and angular momentum between the upper and lower extremities during various activities [49]. This emphasizes that core strength is a significant factor in everyday performance and sports-related activities for individuals of all ages [14]. Moreover, back extensor strength has been associated not only with the risk of dependence on activities of daily living and occupational skills in daily life [50], but also with multiple age-related symptoms, such as osteoporosis, low back pain, and Parkinson’s disease [51,52]. Based on these studies, it is likely that there exist significant correlations between back extensor strength and the aging process.
Our proposition of using back extensor strength as a potential marker of frailty aligns with the concept of a vicious cycle of frailty [53]. With aging, muscles experience changes in both quality and quantity, leading to an increase in interleukin-6 and C-reactive protein levels, which stimulate inflammatory mechanisms and the aging process [54]. These inflammatory changes can lead to chronic disorders associated with systemic low-level inflammation and decreased functionality in daily life [54,55]. Since the back extensor muscles contain more muscle cells than the forearm muscles that generate grip strength, we anticipate a more pronounced decrease in resting metabolism and physical activity, potentially exacerbating the aging process.
Previous studies explored the relationship between frailty and muscle strength in different body parts, such as the connection between lower-limb muscle strength and walking speed [56]. However, this study is the first to demonstrate that not only walking speed but also self-reported exhaustion was associated with back extensor strength. This result suggests that back extensor strength can be considered a more general factor for frailty.
Our study does not propose that back extensor strength should replace grip strength as a measure of frailty. Instead, it proposes back extensor strength as an additional option for evaluating frailty. Back extensor strength can be particularly valuable when grip strength measurements are impractical, such as in cases where a cast is present on the hand. Through the combined assessment of trunk muscle volume, we have discovered the importance of trunk muscle volume in the aging process, suggesting that increasing trunk muscle strength can also be significant in preventing frailty.
Despite the widespread use of grip strength as a convenient measurement, its variability based on different postures, affecting the precision of the data, has been reported. Maximum grip strength is found in a standing posture, with the shoulder fixed forward at 45 degrees, the elbow at 90 degrees, and the wrist and forearm in a neutral position [57]. Assessing back extensor strength was done in the sitting position on a chair equipped with a portable dynamometer, allowing for improved joint stabilization, especially in the hip and knee [24,58]. This controlled position ensures reliable measurements of back extensor strength, making it a potentially reliable indicator of muscle strength, including trunk sarcopenia, similar to grip strength.
In the past, methods for measuring back extensor strength were expensive and cumbersome, which acted as a barrier to data acquisition [59]. However, recent studies have used portable dynamometers, which made back extensor strength more available in clinical settings. Moreover, the portable dynamometer provided data that were as accurate as those obtained using traditional methods [24]. As a result, we anticipate that the increased availability and accuracy of portable dynamometers will lead to more frequent analyses of back extensor strength in the future.
This study had two limitations. Firstly, the participants consisted of farmers, who are likely to have higher levels of physical activity compared to the overall population. As a result, the findings may not fully represent the general population. Secondly, frailty was defined using Fried’s criteria, which focused on specific physical components. Adopting a broader definition of frailty that incorporates overall age-related biomarkers, such as hypertension, macular degeneration, and hearing loss, as the target outcomes of the prediction model could provide a clear understanding of the relationship between aging and muscle strength. By considering a more comprehensive definition of frailty, future studies may offer valuable insights into the multifaceted nature of frailty and its potential connections to muscle strength, facilitating more holistic approaches to frailty assessment and intervention in older adults.
5. Conclusions
Our findings demonstrated a significant linear relationship between back extensor strength and the volumes of abdominal and back muscles. Furthermore, back extensor strength showed associations with multiple parameters of Fried’s frailty, positioning it as a significant indicator of frailty. The findings of this study suggest that exercise programs targeted at strengthening the abdominal and back muscles may be linked to a reduced frailty status. In conclusion, the measurement of back extensor strength could serve as an alternative tool for evaluating frailty.
Author Contributions
Conceptualization, Methodology, Validation: T.K. and S.B.; Formal analysis, Data Curation, Software, Writing – original draft: T.K; Supervision, Validation, Writing review & editing: S.B.; Project administration, Funding acquisition: E.-K.K, G.K., H.-W.P., and S.B. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by a Research Grant for Kangwon Center for Farmers’ Safety and Health from the Korean Ministry of Agriculture, Food and Rural Affairs.
Institutional Review Board Statement
This study protocol was reviewed and approved by the Institutional Review Board of Kangwon National University Hospital, approval no. 2016-03-008), and written informed consent was obtained from all participants. The study was registered with the Clinical Research Information Service.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data underlying this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors have no conflicts of interest to declare.
References
- Morley, J.E.; Vellas, B.; Van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.; Doehner, W.; Evans, J. Frailty consensus: a call to action. Journal of the American Medical Directors Association 2013, 14, 392–397. [Google Scholar]
- Rockwood, K.; Stadnyk, K.; MacKnight, C.; McDowell, L.; Hébert, R. A brief clinical instrument to classify frailty in elderly people. Lancet (British edition) 1999, 353, 205–206. [Google Scholar]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G. Frailty in older adults: evidence for a phenotype. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Mitnitski, A.B.; Mogilner, A.J.; Rockwood, K. Accumulation of deficits as a proxy measure of aging. TheScientificWorldJournal 2001, 1, 323–336. [Google Scholar] [PubMed]
- Xue, Q.-L. The frailty syndrome: definition and natural history. Clinics in geriatric medicine 2011, 27, 1–15. [Google Scholar] [PubMed]
- Dent, E.; Kowal, P.; Hoogendijk, E.O. Frailty measurement in research and clinical practice: a review. European journal of internal medicine 2016, 31, 3–10. [Google Scholar] [PubMed]
- Cesari, M.; Gambassi, G.; Abellan van Kan, G.; Vellas, B. The frailty phenotype and the frailty index: different instruments for different purposes. Age and ageing 2014, 43, 10–12. [Google Scholar] [CrossRef]
- Marano, L.; Carbone, L.; Poto, G.E.; Gambelli, M.; Nguefack Noudem, L.L.; Grassi, G.; Manasci, F.; Curreri, G.; Giuliani, A.; Piagnerelli, R. Handgrip strength predicts length of hospital stay in an abdominal surgical setting: the role of frailty beyond age. Aging Clinical and Experimental Research 2022, 34, 811–817. [Google Scholar]
- Syddall, H.; Cooper, C.; Martin, F.; Briggs, R.; Aihie Sayer, A. Is grip strength a useful single marker of frailty? Age and ageing 2003, 32, 650–656. [Google Scholar] [CrossRef]
- Norman, K.; Stobäus, N.; Gonzalez, M.C.; Schulzke, J.-D.; Pirlich, M. Hand grip strength: outcome predictor and marker of nutritional status. Clinical nutrition 2011, 30, 135–142. [Google Scholar]
- Marques, A.; de Matos, M.G.; Henriques-Neto, D.; Peralta, M.; Gouveia, É.R.; Tesler, R.; Martins, J.; Gomez-Baya, D. Grip strength and depression symptoms among middle-age and older adults. In Proceedings of the Mayo Clinic Proceedings; 2020; pp. 2134–2143. [Google Scholar]
- Antonova, L.; Bucher-Koenen, T.; Mazzonna, F. Long-term health consequences of recessions during working years. Social Science & Medicine 2017, 187, 134–143. [Google Scholar]
- Farrow, M.; Biglands, J.; Tanner, S.F.; Clegg, A.; Brown, L.; Hensor, E.; O’Connor, P.; Emery, P.; Tan, A. The effect of ageing on skeletal muscle as assessed by quantitative MR imaging: an association with frailty and muscle strength. Aging clinical and experimental research 2021, 33, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Akuthota, V.; Nadler, S.F. Core strengthening. Archives of physical medicine and rehabilitation 2004, 85, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.X.; Yao, J.; Zirek, Y.; Reijnierse, E.M.; Maier, A.B. Muscle mass, strength, and physical performance predicting activities of daily living: a meta-analysis. Journal of cachexia, sarcopenia and muscle 2020, 11, 3–25. [Google Scholar] [CrossRef] [PubMed]
- Banno, T.; Arima, H.; Hasegawa, T.; Yamato, Y.; Togawa, D.; Yoshida, G.; Yasuda, T.; Oe, S.; Mihara, Y.; Ushirozako, H. The effect of paravertebral muscle on the maintenance of upright posture in patients with adult spinal deformity. Spine deformity 2019, 7, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Granacher, U.; Gollhofer, A.; Hortobágyi, T.; Kressig, R.W.; Muehlbauer, T. The importance of trunk muscle strength for balance, functional performance, and fall prevention in seniors: a systematic review. Sports medicine 2013, 43, 627–641. [Google Scholar] [CrossRef]
- Jo, H.; Baek, S.; Park, H.-w.; Lee, S.-A.; Moon, J.; Yang, J.E.; Kim, K.S.; Kim, J.Y.; Kang, E.K. Farmers’ cohort for agricultural work-related musculoskeletal disorders (farm) study: study design, methods, and baseline characteristics of enrolled subjects. Journal of epidemiology 2016, JE20140271. [Google Scholar] [CrossRef]
- Bassett, D.R.; Schneider, P.L.; Huntington, G.E. Physical activity in an Old Order Amish community. Medicine & Science in Sports & Exercise 2004, 36, 79–85. [Google Scholar]
- Baek, S.; Park, J.; Kyoung Kang, E.; Kim, G.; Kim, H.; Park, H.-W. Association Between Ergonomic Burden Assessed Using 20-Item Agricultural Work-Related Ergonomic Risk Questionnaire and Shoulder, Low Back, and Leg Pain in Korean Farmers. Journal of Agromedicine 2023, 28, 532–544. [Google Scholar] [CrossRef]
- Park, K.H.; Baek, S.; Kang, E.K.; Park, H.-w.; Kim, G.; Kim, S.H. The Association Between Sagittal Plane Alignment and Disc Space Narrowing of Lumbar Spine in Farmers. Annals of Rehabilitation Medicine 2021, 45, 294–303. [Google Scholar] [CrossRef]
- Pourtaheri, S.; Issa, K.; Lord, E.; Ajiboye, R.; Drysch, A.; Hwang, K.; Faloon, M.; Sinha, K.; Emami, A. Paraspinal muscle atrophy after lumbar spine surgery. Orthopedics 2016, 39, e209–e214. [Google Scholar] [CrossRef] [PubMed]
- Chun, M.Y. Validity and reliability of Korean version of international physical activity questionnaire short form in the elderly. Korean journal of family medicine 2012, 33, 144. [Google Scholar] [CrossRef] [PubMed]
- Park, H.-w.; Baek, S.; Kim, H.Y.; Park, J.-G.; Kang, E.K. Reliability and validity of a new method for isometric back extensor strength evaluation using a hand-held dynamometer. Annals of rehabilitation medicine 2017, 41, 793–800. [Google Scholar] [CrossRef] [PubMed]
- Baek, S.; Park, H.-w.; Kim, G. Associations Between Trunk Muscle/Fat Composition, Narrowing Lumbar Disc Space, and Low Back Pain in Middle-Aged Farmers: A Cross-Sectional Study. Annals of Rehabilitation Medicine 2022, 46, 122. [Google Scholar] [CrossRef]
- Chen, T.; He, T.; Benesty, M.; Khotilovich, V.; Tang, Y.; Cho, H.; Chen, K. Xgboost: extreme gradient boosting. R package version 0.4-2 2015, 1, 1–4. [Google Scholar]
- Alin, A. Multicollinearity. Wiley interdisciplinary reviews: computational statistics 2010, 2, 370–374. [Google Scholar] [CrossRef]
- Johnson, J.W. A heuristic method for estimating the relative weight of predictor variables in multiple regression. Multivariate behavioral research 2000, 35, 1–19. [Google Scholar] [CrossRef]
- Rosenbaum, P.R.; Rubin, D.B. The central role of the propensity score in observational studies for causal effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Thoemmes, F.J.; Kim, E.S. A systematic review of propensity score methods in the social sciences. Multivariate behavioral research 2011, 46, 90–118. [Google Scholar] [CrossRef] [PubMed]
- Kim, T. The impact of working hours on pregnancy intention in childbearing-age women in Korea, the country with the world’s lowest fertility rate. PLOS ONE 2023, 18, e0288697. [Google Scholar] [CrossRef]
- Austin, P.C. Some methods of propensity-score matching had superior performance to others: results of an empirical investigation and Monte Carlo simulations. Biometrical Journal: Journal of Mathematical Methods in Biosciences 2009, 51, 171–184. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate behavioral research 2011, 46, 399–424. [Google Scholar] [CrossRef]
- Massy-Westropp, N.M.; Gill, T.K.; Taylor, A.W.; Bohannon, R.W.; Hill, C.L. Hand Grip Strength: age and gender stratified normative data in a population-based study. BMC research notes 2011, 4, 1–5. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. Xgboost: A scalable tree boosting system. In Proceedings of the Proceedings of the 22nd acm sigkdd international conference on knowledge discovery and data mining, 2016; pp. 785–794.
- Bantis, L.E.; Nakas, C.T.; Reiser, B. Construction of confidence regions in the ROC space after the estimation of the optimal Youden index-based cut-off point. Biometrics 2014, 70, 212–223. [Google Scholar] [CrossRef] [PubMed]
- Bradley, A.P. The use of the area under the ROC curve in the evaluation of machine learning algorithms. Pattern recognition 1997, 30, 1145–1159. [Google Scholar] [CrossRef]
- Hastie, T.; Tibshirani, R.; Friedman, J. The elements of statistical learning. Springer series in statistics; New York, NY, USA, 2001. [Google Scholar]
- Jang, I.-Y.; Lee, H.Y.; Lee, E. Geriatrics fact sheet in Korea 2018 from national statistics. Annals of geriatric medicine and research 2019, 23, 50. [Google Scholar] [CrossRef]
- Batista, F.S.; Gomes, G.A.d.O.; D’Elboux, M.J.; Cintra, F.A.; Neri, A.L.; Guariento, M.E.; Souza, M.d.L.R.d. Relationship between lower-limb muscle strength and functional independence among elderly people according to frailty criteria: a cross-sectional study. Sao Paulo Medical Journal 2014, 132, 282–289. [Google Scholar] [CrossRef]
- Armamento-Villareal, R.; Aguirre, L.; Napoli, N.; Shah, K.; Hilton, T.; Sinacore, D.; Qualls, C.; Villareal, D. Changes in thigh muscle volume predict bone mineral density response to lifestyle therapy in frail, obese older adults. Osteoporosis international 2014, 25, 551–558. [Google Scholar] [CrossRef]
- Staiano, A.; Katzmarzyk, P. Ethnic and sex differences in body fat and visceral and subcutaneous adiposity in children and adolescents. International journal of obesity 2012, 36, 1261–1269. [Google Scholar] [CrossRef]
- Lönnqvist, F.; Thörne, A.; Large, V.; Arner, P. Sex differences in visceral fat lipolysis and metabolic complications of obesity. Arteriosclerosis, thrombosis, and vascular biology 1997, 17, 1472–1480. [Google Scholar] [CrossRef]
- Mannion, A.; Adams, M.; Cooper, R.; Dolan, P. Prediction of maximal back muscle strength from indices of body mass and fat-free body mass. Rheumatology (Oxford, England) 1999, 38, 652–655. [Google Scholar] [CrossRef] [PubMed]
- Loosen, S.H.; Schulze-Hagen, M.; Püngel, T.; Bündgens, L.; Wirtz, T.; Kather, J.N.; Vucur, M.; Paffenholz, P.; Demir, M.; Bruners, P. Skeletal muscle composition predicts outcome in critically ill patients. Critical care explorations 2020, 2. [Google Scholar] [CrossRef] [PubMed]
- Kasukawa, Y.; Miyakoshi, N.; Hongo, M.; Ishikawa, Y.; Noguchi, H.; Kamo, K.; Sasaki, H.; Murata, K.; Shimada, Y. Relationships between falls, spinal curvature, spinal mobility and back extensor strength in elderly people. Journal of bone and mineral metabolism 2010, 28, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Granacher, U.; Lacroix, A.; Muehlbauer, T.; Roettger, K.; Gollhofer, A. Effects of core instability strength training on trunk muscle strength, spinal mobility, dynamic balance and functional mobility in older adults. Gerontology 2013, 59, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Borghuis, J.; Hof, A.L.; Lemmink, K.A. The importance of sensory-motor control in providing core stability: implications for measurement and training. Sports medicine 2008, 38, 893–916. [Google Scholar] [CrossRef] [PubMed]
- Behm, D.G.; Drinkwater, E.J.; Willardson, J.M.; Cowley, P.M. The use of instability to train the core musculature. Applied physiology, nutrition, and metabolism 2010, 35, 91–108. [Google Scholar] [CrossRef]
- Rantanen, T.; Avlund, K.; Suominen, H.; Schroll, M.; Frändin, K.; Pertti, E. Muscle strength as a predictor of onset of ADL dependence in people aged 75 years. Aging clinical and experimental research 2002, 14, 10–15. [Google Scholar]
- Bridgewater, K.J.; Sharpe, M.H. Trunk muscle training and early Parkinson’s disease. Physiotherapy Theory and Practice 1997, 13, 139–153. [Google Scholar] [CrossRef]
- Handa, N.; Yamamoto, H.; Tani, T.; Kawakami, T.; Takemasa, R. The effect of trunk muscle exercises in patients over 40 years of age with chronic low back pain. Journal of orthopaedic science 2000, 5, 210–216. [Google Scholar] [CrossRef]
- Fried, L.P.; Hadley, E.C.; Walston, J.D.; Newman, A.B.; Guralnik, J.M.; Studenski, S.; Harris, T.B.; Ershler, W.B.; Ferrucci, L. From bedside to bench: research agenda for frailty. Science of Aging Knowledge Environment 2005, 2005, pe24–pe24. [Google Scholar] [CrossRef]
- Bruunsgaard, H. Physical activity and modulation of systemic low-level inflammation. Journal of leukocyte biology 2005, 78, 819–835. [Google Scholar] [CrossRef] [PubMed]
- Taaffe, D.R.; Harris, T.B.; Ferrucci, L.; Rowe, J.; Seeman, T.E. Cross-sectional and prospective relationships of interleukin-6 and C-reactive protein with physical performance in elderly persons: MacArthur studies of successful aging. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences 2000, 55, M709–M715. [Google Scholar] [CrossRef] [PubMed]
- Batista, F.S.; Gomes, G.A.d.O.; Neri, A.L.; Guariento, M.E.; Cintra, F.A.; Sousa, M.d.L.R.d.; D’Elboux, M.J. Relationship between lower-limb muscle strength and frailty among elderly people. Sao Paulo Medical Journal 2012, 130, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Meena, M.L.; Sain, M.K.; Dangayach, G.S. Impact of posture and upper-limb muscle activity on grip strength. International Journal of Occupational Safety and Ergonomics 2019, 25, 614–620. [Google Scholar] [CrossRef] [PubMed]
- Verna, J.L.; Mayer, J.M.; Mooney, V.; Pierra, E.A.; Robertson, V.L.; Graves, J.E. Back extension endurance and strength: the effect of variable-angle roman chair exercise training. Spine 2002, 27, 1772–1777. [Google Scholar] [CrossRef]
- Freivalds, A.; Fotouhi, D.M. Comparison of dynamic strength as measured by the cybex and mini-gym isokinetic dynamometers. International Journal of Industrial Ergonomics 1987, 1, 189–208. [Google Scholar] [CrossRef]
Figure 1.
Flow diagram of the study. FARM, a farmers’ cohort for agricultural work-related musculoskeletal disorders.
Figure 1.
Flow diagram of the study. FARM, a farmers’ cohort for agricultural work-related musculoskeletal disorders.
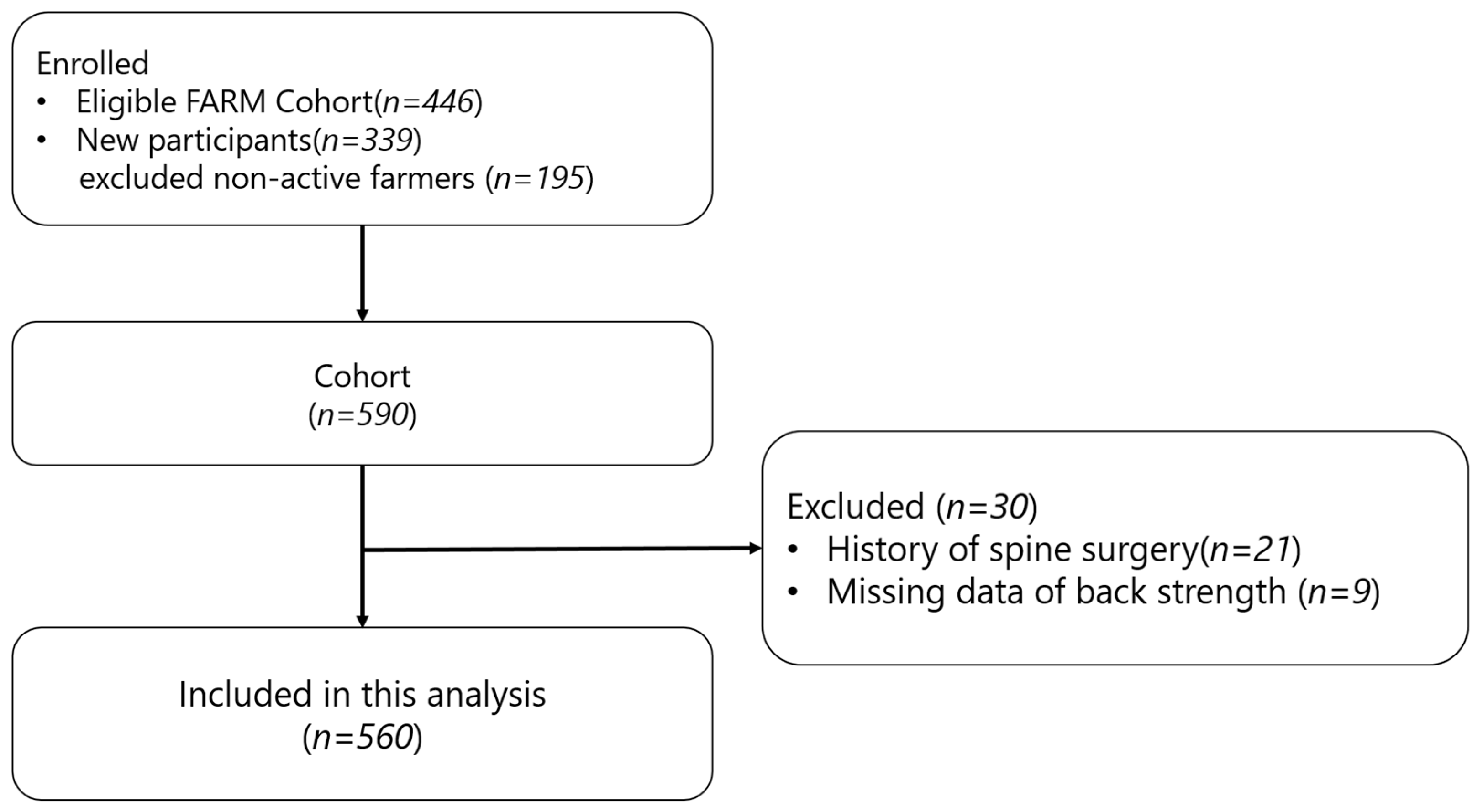
Figure 2.
The feature importance ranking of XGBoost for frailty: back extensor strength and confounding. XGBoost, Extreme Gradient Boosting; BMI, body mass index.
Figure 2.
The feature importance ranking of XGBoost for frailty: back extensor strength and confounding. XGBoost, Extreme Gradient Boosting; BMI, body mass index.
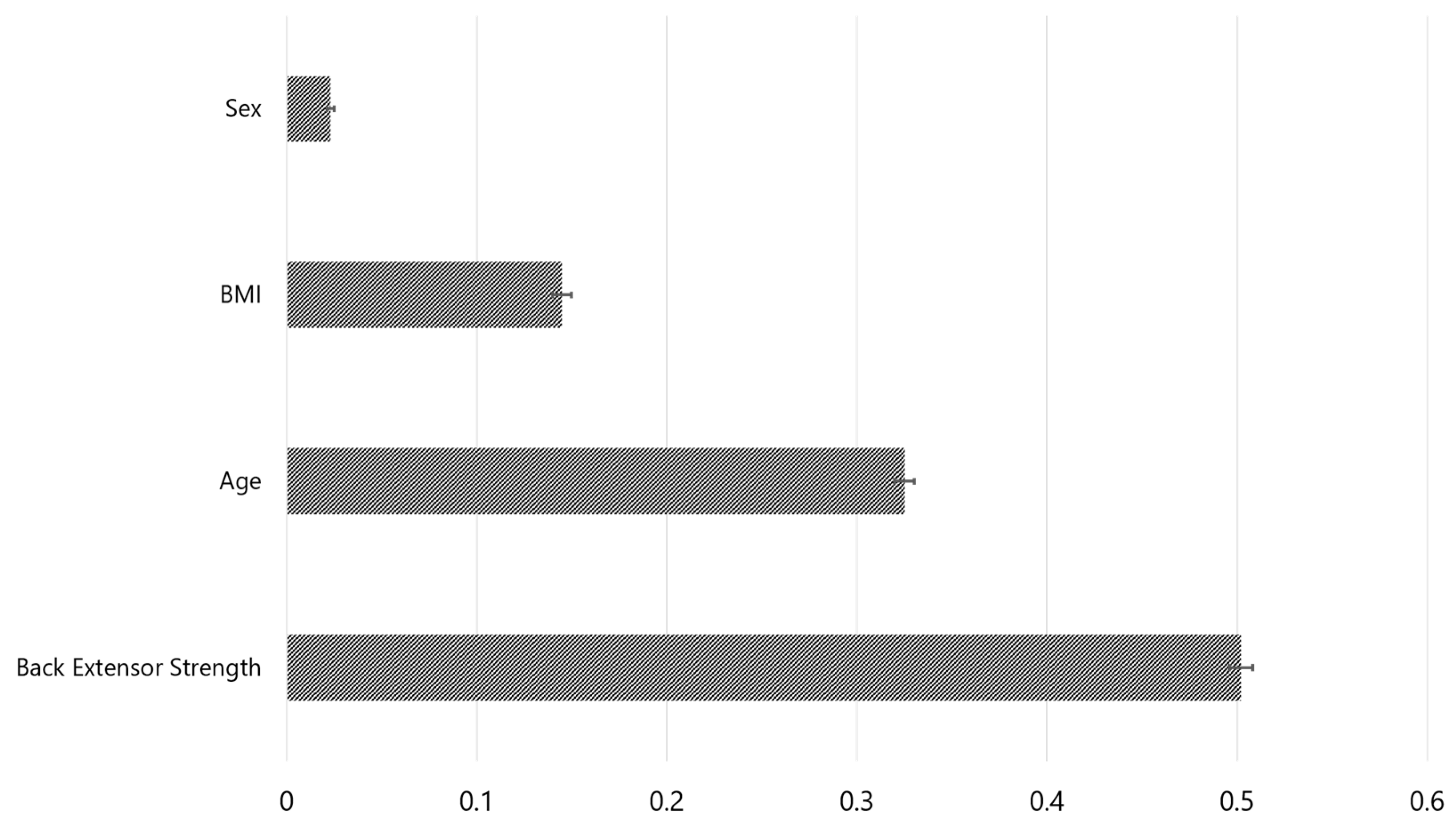

Table 1.
Participant characteristics by sex groups.
| Both (n = 560) | Male (n = 255) | Female (n = 305) | p-value | |
|---|---|---|---|---|
| Age | 58.0±7.0 | 58.5±7.0 | 57.5±6.9 | .130 |
| Waist circumference (cm) | 86.2±9.3 | 89.6±9.1 | 83.3±8.5 | < .001 |
| BMI () | 25.6±3.1 | 25.6±3.1 | 25.5±3.0 | .989 |
| TFM (cm3) | 282.3±93.6 | 272.7±100.6 | 290.3±86.7 | .059 |
| VFM (cm3) | 103.6±45.5 | 116.1±50.0 | 93.2±38.4 | < .001 |
| SFM (cm3) | 178.7±66.5 | 156.6±63.1 | 197.1±63.7 | < .001 |
| TMM (cm3) | 130.1±30.0 | 155.9±22.2 | 108.6±15.2 | < .001 |
| BMM (cm3) | 57.6±11.6 | 66.0±9.3 | 50.6±8.2 | < .001 |
| PMM (cm3) | 19.4±6.9 | 25.3±5.2 | 14.4±3.2 | < .001 |
| AMM (cm3) | 53.2±14.7 | 64.6±12.9 | 43.7±7.7 | < .001 |
| Grip strength (Kgf) | 28.7±10.2 | 37.7±7.2 | 21.3±5.1 | < .001 |
| Back extensor strength (N) | 262.7±93.8 | 321.0±96.6 | 213.9±55.9 | < .001 |
| Walking speed (m/s) | 1.0±0.2 | 1.1±0.2 | 1.0±0.2 | .005 |
| Unintentional weight loss (≥4.5kg) | 60 (10.7%) | 24 (9.4%) | 36 (11.8%) | .660 |
| Self-reported exhaustion (≥3 days/week) | 44 (7.9%) | 14 (5.5 %) | 30 (9.8%) | .163 |
| Physical activity (MET-min/week) | 5622±5657 | 5821±5453 | 5455±5827 | .673 |
| Frailty score (%) | .678 | |||
| 0 | 257 (45.9%) | 113 (44.3%) | 144 (47.2%) | |
| 1 | 189 (33.8%) | 97 (38.0%) | 92 (30.2%) | |
| 2 | 82 (14.6%) | 35 (13.7%) | 47 (15.4%) | |
| 3 | 26 (4.6%) | 8 (3.1%) | 18 (5.9%) | |
| 4 | 6 (1.1%) | 2 (0.8%) | 4 (1.3%) |
BMI, body mass index; TFM, total fat mass; VFM, visceral fat mass; SFM, superficial fat mass; TMM, total muscle mass; BMM, back muscle mass; PMM, psoas muscle mass; AMM, abdominal muscle mass. Values are expressed as mean ± standard deviation or n (%). p values are based on the t-test, chi-square test, and Fisher’s exact test.
Table 2.
Participant characteristics by age groups.
| Age < 65 (n = 470) | Age ≥ 65 (n = 90) | p-value | |
|---|---|---|---|
| Sex (male %) | 210 (44.7%) | 45 (50%) | .416 |
| Waist circumference (cm) | 85.9±9.5 | 87.5±8.2 | .099 |
| BMI () | 25.6±3.1 | 25.5±2.8 | .758 |
| TFM (cm3) | 281.8±93.4 | 284.6±95.1 | .913 |
| VFM (cm3) | 102.4±45.8 | 110.2±43.5 | .051 |
| SFM (cm3) | 179.5±66.0 | 174.4±69.2 | .302 |
| TMM (cm3) | 131.7±30.3 | 121.8±27.3 | .008 |
| BMM (cm3) | 58.4±11.4 | 53.1±11.8 | < .001 |
| PMM (cm3) | 19.7±7.0 | 17.6±5.8 | .013 |
| AMM (cm3) | 53.6±15.0 | 51.1±13.1 | .219 |
| Grip strength (Kgf) | 29.2±10.4 | 26.1±8.9 | .020 |
| Back extensor strength (N) | 266.5±93.4 | 242.4±93.7 | .015 |
| Walking speed (m/s) | 1.1±0.2 | 1.0±0.1 | < .001 |
| Unintentional weight loss (≥ 4.5kg) | 48 (10.2%) | 12 (13.3%) | .490 |
| Self-reported exhaustion (≥3 days/week) | 32 (6.8%) | 12 (13.3%) | .058 |
| Physical activity (MET-min/week) | 5646±5573 | 5498±6112 | .573 |
| Frailty score (%) | < .001 | ||
| 0 | 236 (50.2%) | 21 (23.3%) | |
| 1 | 157 (33.4%) | 32 (35.6%) | |
| 2 | 56 (11.9%) | 26 (28.9%) | |
| 3 | 16 (3.4%) | 10 (11.1%) | |
| 4 | 5 (1.1%) | 1 (1.1%) |
BMI, body mass index; TFM, total fat mass; VFM, visceral fat mass; SFM, superficial fat mass; TMM, total muscle mass; BMM, back muscle mass; PMM, psoas muscle mass; AMM, abdominal muscle mass. Values are expressed as mean ± standard deviation or n (%). p values are based on the t-test, chi-square test, and Fisher’s exact test.
Table 3.
Multivariate linear regression analysis for the predictor variable of back extensor strength.
Table 3.
Multivariate linear regression analysis for the predictor variable of back extensor strength.
| Coefficient | Standard error | t | p-value | VIF | Relative Weight | |
|---|---|---|---|---|---|---|
| Constant | 209.661 | 42.076 | 4.983 | 8.39E-7 | ||
| AMM | 1.122 | 0.398 | 2.819 | .005 | 3.571 | 0.089 |
| PMM | 0.121 | 0.878 | 0.139 | .890 | 3.812 | 0.077 |
| BMM | 0.887 | 0.419 | 2.113 | .035 | 2.485 | 0.077 |
| VFM | 0.010 | 0.088 | 0.120 | .905 | 1.688 | 0.013 |
| SFM | 0.062 | 0.056 | 1.103 | .270 | 1.486 | -0.005 |
| Age | -1.823 | 0.508 | -3.583 | < .001 | 1.312 | -0.017 |
| Sex | 72.901 | 12.417 | 5.871 | 7.48E-9 | 3.985 | -0.118 |
VIF, variance inflation factor; AMM, abdominal muscle mass; PMM, psoas muscle mass; BMM, back muscle mass; VFM, visceral fat mass; SFM, subcutaneous fat mass; Sex, female.
Table 4.
Propensity score matching for back extensor strength and Fried’s frailty.
| Before propensity score matching | After propensity score matching | |||||||
|---|---|---|---|---|---|---|---|---|
| Low 20% back extensor strength (n = 114) |
The higher (n = 444) |
SMD | p-value | Low 20% back extensor strength (n = 108) |
The higher (n = 279) |
SMD | p-value | |
| Age | 60.6±6.2 | 57.3±7.0 | 0.532 | < .001 | 59.9±5.7 | 59.4±5.7 | 0.002 | 0.423 |
| Female | 54.4% | 54.5% | -0.002 | 1.000 | 55.6% | 55.9% | -0.019 | 1.000 |
| Grip | 25.4±10.2 | 29.6±10.0 | < .001 | 25.2±10.3 | 28.7±9.9 | 0.001 | ||
| Wt. loss | 13.2% | 10.1% | .447 | 13.0% | 6.8% | 0.082 | ||
| Exhaust | 15.8% | 5.6% | .001 | 16.7% | 6.8% | 0.006 | ||
| Activity | 5372±5051 | 5706±5811 | .708 | 5340±4998 | 5559±5520 | 0.800 | ||
| Gait speed | 1.0±0.2 | 1.1±0.2 | < .001 | 1.0±0.2 | 1.1±0.2 | 0.002 | ||
SMD, standardized mean difference; Grip, grip strength (N); Wt. loss, unintentional weight loss (≥ 4.5 kg); exhaustion, self-reported exhaustion (≥ 3 days/week); physical activity (MET-min/week), gait speed, and walking speed (m/s).
Table 5.
Result of the multivariate logistic regression analysis.
| Risk Factor | Coefficient | Standard error | Odds ratio (95% CI) | P value |
|---|---|---|---|---|
| Back Extensor strength | -0.009 | 0.003 | 0.990 (0.983-0.997) | .008 |
| BMI | 0.026 | 0.061 | 1.027 (0.907-1.156) | .664 |
| Age | 0.084 | 0.031 | 1.088 (1.025-1.160) | .007 |
| Sex | -0.108 | 0.488 | 0.897 (0.350-2.413) | .824 |
| Constant | -6.325 |
CI, confidence interval; BMI, body mass index; Sex, being female.
Table 6.
Result of the XGBoost model.
| Characteristics | Values |
|---|---|
| Feature importance in Fried’s frailty prediction | |
| Back extensor strength | 0.502±0.006 |
| Age | 0.325±0.005 |
| BMI | 0.145±0.005 |
| Sex | 0.026±0.002 |
| Predictive performance of XGBoost | |
| AUC | 0.579±0.004 |
| Accuracy | 0.71±0.05 |
| Precision | 0.10±0.01 |
| Recall | 0.56±0.04 |
| F1 score | 0.15±0.01 |
XGBoost, extreme gradient boosting; BMI, body mass index; Sex, female; AUC, area under the curve.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



