
Submitted:
18 August 2023
Posted:
22 August 2023
You are already at the latest version
Abstract
Chronic Kidney Disease (CKD) and Cardiovascular Disease (CVD) are two devastating diseases that may occur in non-diabetics or individuals with diabetes and when combined is referred to as cardiorenal disease. The impact of cardiorenal disease on society, the economy and the healthcare system is enormous. Although there are numerous therapies for cardiorenal disease, one therapy showing a great deal of promise is sodium-dependent glucose cotransporter 2 (SGLT2) inhibitors. The SGLT family member, SGLT2, is often implicated in the pathogenesis of a range of diseases and dysregulation of the activity of SGLT2 markedly effects the transport of glucose and sodium across the luminal membrane of renal cells. Inhibitors of SGLT2 were developed based on the anti-diabetic action initiated by inhibiting renal glucose reabsorption, thereby increasing glucosuria. Of great medical significance, large-scale clinical trials utilising a range of SGLT2 inhibitors have demonstrated both metabolic and biochemical benefits via numerous novel mechanisms such as sympathoinhibition which will be discussed in this review. In summary, SGLT2 inhibitors clearly exert cardio-renal protection in diabetic and non-diabetic subjects in both pre-clinical and clinical settings by improving hyperglycemia, high blood pressure, hyperlipidemia and diabetic retinopathy. (188 Words)
Keywords:
diabetes
; cardiovascular
; renal
; SGLT1
; SGLT2
; therapy.
1. Introduction
Both Chronic Kidney Disease (CKD) and Cardiovascular Disease (CVD) are two of the most prevalent diseases globally. Chronic Kidney Disease is a progressive condition that affects over 10% (over 800 million) of the global population [1]. However, according to the World Health Organisation, CVD is the leading cause of death globally, taking an estimated 17.9 million lives every year.
An even more disturbing phenomenon occurring now is the combination of cardiac and renal dysfunction known as cardiorenal disease. In fact, it is now known that many individuals dealing with CKD don’t actually reach the stage of dialysis because they die of heart disease [2]. Why this is the case, is because CKD is multifactorial and could be related to a whole range of reasons, including impaired coronary flow reserve (ratio of the maximal or hyperemic flow down a coronary vessel to the resting flow), reduced aortic compliance (the ability of the arterial wall to distend and increase volume with increasing transmural pressure), increase in the level of angiotensin II, changes in the concentrations of essential vitamins like potassium, calcium and magnesium as well as fibrosis in the hearts of those patients on dialysis [3].
Diabetic Kidney Disease (DKD) develops in approximately 40% of patients with type 2 diabetes (T2D) and 30% of patients with type 1 diabetes (T1D) and is the leading cause of chronic kidney disease (CKD) and end-stage renal disease [4,5]. The mortality risk associated with DKD has increased by 31.1% and increases with worsening disease severity [6]. It is reported that DKD affects males and females equally and it rarely develops before 10 years duration of T1D [7]. The humanistic, societal, and economic impact of DKD is enormous. It places a significant burden on the health care system and seriously affects the physical health and quality of life of the patients [8]. In the United States alone, as of 2013, kidney disease costs the society 50 billion dollars, with an additional 31 billion dollars spent on dialysis [9].
At present, there are a multitude of therapies that are used for cardio-renal disease. Some of these include pharmacological agents such as diuretics, vasodilators, angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARB’s) [10]. In fact, it has been shown that in an Italian diabetic population affected by both DKD and diabetic retinopathy, the role of multifactorial intervention achieved by using a combination of angiotensin converting enzyme inhibitors and angiotensin II receptor blockers resulted in improved outcomes [11]. Although standard treatments have been found to slow the progression of CKD, they do not halt the disease. Therefore, alternative treatments may be required [12]. Other emerging therapies that are currently undergoing clinical trials include Endothelin Receptor A Antagonists, complement inhibition, Janus kinase (JAK) inhibition, chemokine inhibition, renal denervation and of course, the topic of this review, sodium glucose co-transporter 2 (SGLT2) inhibitors.
2. What are Sodium Glucose Co-Transporters?
The entry of glucose into cells is regulated by facilitative glucose transporters (GLUTs) and sodium-dependent glucose cotransporters (SGLTs). Of the SGLT family, SGLT1 and SGLT2 are frequently investigated in a range of disease settings [13], as they play key roles in the transport of glucose and sodium across the brush border membrane of intestinal and renal cells [14]. Although SGLT1 is less researched than SGLT2, it is more widely expressed throughout the body and is found predominantly in the small intestine (Figure 1; Table 1) and only accounts for 5-10% of the glucose reabsorption in the kidneys. Our studies have shown that heightened Sympathetic Nervous System (SNS) activity upregulates this SGLT1 expression and therefore inhibition of this protein could also be beneficial in treating cardiometabolic disorders [15]. SGLT2 is a high-capacity, low affinity glucose co-transporter, mainly found in the S1 and S2 segments of the renal convoluted proximal tubules (Figure 1; Table 1), and is required for the reabsorption of a majority of the glucose (~90–95%) filtered by the kidney [16,17].
SGLT2 inhibitors (SGLT2i’s) have been developed based on the anti-diabetic action initiated by inhibiting renal glucose reabsorption thereby increasing urinary glucose excretion [[18]; Table 2]. As demonstrated by several large-scale clinical trials [19,20,21], SGLT2i’s are now recognised to be capable of altering a range of metabolic and biochemical parameters via novel mechanisms which will be discussed in this review, thereby exerting cardio-renal protection in diabetic and non-diabetic individuals [22,23].
One critical requirement before SGLT2i’s can be prescribed for the treatment of CKD is a functional glomerular filtration rate (GFR). The glomerular filtration rate is considered the optimal way to measure kidney function. In a healthy kidney, the glomerular filtration rate is 120 ml/min/1.73m2 but as CKD progresses it may decline to 60 ml/min/1.73m2 or less. Interestingly, studies have shown that SGLT2i’s are safe and beneficial to use in patients with a GFR above 30 ml/min/1.73m2 and can actually be used in subjects that have a GFR of less than 30 ml/min/1.73m2 as long as they are tolerating it well and are not on dialysis [24].
3. Use of selective SGLT2 Inhibition as an anti-diabetic therapy
There are many studies that have shown the beneficial cardiovascular and renal effects that SGLT2i can have in both T1D and T2D. In patients with T2D, SGLT2i treatments are now being considered as the first line of therapy because of its metabolic and cardio-renal benefits. As just mentioned, SGLT2i’s provide benefits by promoting the excretion of glucose in the urine therefore assisting with a reduction in hyperglycemia and subsequently a decrease in weight. However, aside from the metabolic benefits of SGLT2i’s, there are numerous other beneficial protective mechanisms, as outlined below.
3.1. Pre-clinical Studies
3.1.1. Blood Pressure Reduction
One common complication of patients with diabetes is hypertension, and although the anti-hypertensive therapies have improved over the years, there is still definitely room for improvement. Although SGLT2i are not predominantly prescribed as hypertensive medications, research has now shown that SGLT2i's have overwhelming beneficial effects in diabetic hypertensive patients. Mechanisms that may contribute to their anti-hypertensive action is their mild natriuresis, osmotic diuresis and weight loss effects in diabetic patients [31]. In human studies, both Empagliflozin (EMPA) [32] and Dapagliflozin (DAPA) [33] were associated with significant reductions in the blood pressure in diabetic patients compared to placebo. We have also demonstrated in our murine studies that SGLT2i may promote sympathoinhibition in the kidneys (Figure 2) and heart in diabetic mice and this may be an underlying mechanism for blood pressure reduction [34].
3.1.2. Improved Digestive Health
The intestinal microbiota is aggravated as diabetes progresses and during the development of DKD, there is an increased imbalance in the gut microbiota. The SGLT2i DAPA has been beneficial in lowering the level of dysbacteriosis and bile acids [35], altering the microbiota composition [36] and reducing succinate levels (pathogenic factor in diabetic retinopathy) [37], while the inhibitor EMPA reduces the lipopolysaccharide (LPS)-producing bacteria and increases the short-chain fatty acid (SCFA)-producing bacteria [38]. Additional inhibitors such as Luseogliflozin have also been found to be beneficial in altering the microbiota. When mice were given the SGLT2 inhibitor Luseogliflozin, there was a significant increase in the abundance of the species Syntrophothermus lipocalidus, Syntrophomonadaceae and Anaerotignum, which are all involved in the biosynthesis of important SCFA’s such as acetic acid, propionic acid and butyric acid [39].
3.1.3. Diabetic Retinopathy
Diabetic retinopathy is a common complication associated with diabetes and the SGLT2i’s EMPA [40] and DAPA [41] have improved diabetic retinopathy in T2D db/db mice. Empagliflozin has also been shown to mitigate ocular edema and microaneurysms in the retina as well as inhibit the mammalian target of raptomycin activation. One of the characteristics of diabetic retinopathy in the db/db mice is an increase in acellular capillary numbers [41] and DAPA has been shown to produce a substantial decrease in the acellular capillary numbers compared to placebo. Aside from this, inflammation is another main factor associated with diabetic retinopathy. According to these studies, both EMPA and DAPA have been shown to downregulate inflammatory and angiogenic factors such as Tumor Necrosis Factor-𝛼 (TNF-𝛼) [40,41], Interleukin 1-β (IL1-β) [41], Interleukin 6 (IL-6) [40], Vascular Cell Adhesion Molecule 1 (VCAM-1) [40] and Vascular Endothelial Growth Factor (VEGF) [40] in the retina.
3.1.4. Kidney Health
There have been numerous pre-clinical studies conducted which show the renoprotective effects of SGLT2i’s. Dapagliflozin treatment in db/db mice halted the progressive increases in albumineria and glomerulosclerosis [42] while in the Otsuka Long-Evans Tokushima Fatty (OLETF) T2D rat model, DAPA was shown to reverse renal oxidative stress markers as well as attenuate inflammatory cell infiltration, mesangial widening, interstitial fibrosis and total collagen content [43]. Luseogliflozin treatment in a T2D nephropathy rat model has been shown to prevent the fall in GFR and reduced the degree of glomerular injury, renal fibrosis and tubular necrosis compared to those on vehicle or insulin alone [44]. Empagliflozin treatment has also been found to ameliorate albuminuria and glomerular injury in db/db mice [45].
3.1.5. Cardiovascular Benefits
There have been many pre-clinical animal studies showing the cardioprotective effects of SGLT2i in T2D. When EMPA was administered to db/db mice over a 10-week period, it was shown to significantly ameliorate cardiac interstitial fibrosis, pericoronary arterial thickening, cardiac macrophage infiltration and the impairment of vascular dilation [45]. Further discussion of SGLT2i mediated cardiovascular benefits will be discussed later in the review.
3.1.6. Improved Cognitive Function in T2D
One of the most under-recognised but life changing effects of T2D is the decline in cognitive function. Therefore, the question as to whether SGLT2i’s reduce the cognitive impairment associated with T2D has been investigated in numerous animal studies. Empagliflozin has been shown to significantly prevent the impairment of cognitive function in the T2D db/db mice, due to its ability to attenuate cerebral oxidative stress, as well as increase cerebral Brain Derived Neurotrophic Factor (BDNF) levels [45].
3.2. Human Clinical Trials
There are a multitude of clinical trials that have been conducted utilizing the SGLT2 inhibitors EMPA, DAPA, Canagliflozin (CANA) and Ertugliflozin and they are outlined below.
3.2.1. Empagliflozin
The ground breaking clinical trial assessing the effectiveness of the SGLT2 inhibitor EMPA in preventing cardiovascular disease in diabetics is the Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients – Removing Excess Glucose (EMPA-REG) [19,46]. This trial demonstrated that when patients who had T2D as well as a high risk of cardiovascular events were treated with EMPA, mortality and hospitalizations due to heart failure were reduced compared to placebo [19]. Empagliflozin also promoted a slowing down of the progression of kidney disease, as well as a significantly lower risk of clinically relevant renal events [46].
3.2.2. Dapagliflozin
There are two main clinical trials evaluating the effectiveness of the SGLT2 inhibitor DAPA in diabetics when it comes to cardiovascular and kidney disease. The Dapagliflozin Effect on Cardiovascular Events – Thrombolysis in Myocardial Infarction 58 (DELCARE-TIMI 58) trial [20] recruited diabetics who had atherosclerotic cardiovascular disease and although it didn’t result in a higher or lower rate of Major Adverse Cardiovascular Events (MACE), it did lead to a lower rate of cardiovascular death or hospitalization for heart failure. In addition to this trial, the Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease (DAPA-CKD) study [47] found that not only did DAPA reduce the risk of a declining GFR level but it decreased the risk of end stage kidney disease or death from renal causes.
3.2.3. Canagliflozin
There are also two main clinical trials determining the effectiveness of the SGLT2 inhibitor CANA on cardiovascular disease in Type 2 diabetics. The first is the Canagliflozin Cardiovascular Assessment Study (CANVAS) [21] where they found that CANA not only reduced the risk of major adverse cardiovascular events in T2D patients at an increased risk of cardiovascular disease but it also offered renoprotective benefits such as the regression of albuminuria levels and a decrease in the need for renal-replacement therapy or death, when compared to placebo. In the second trial known as the Canagliflozin and Renal Endpoints in Diabetes with Established Nephropathy Clinical Evaluation (CREDENCE) study [48], they concluded that in patients who had both T2D and kidney disease, the risk of kidney failure and cardiovascular events was lower in the CANA group compared to the placebo group.
3.2.4. Ertugliflozin
The final major SGLT2 inhibitor clinical trial is the Evaluation of Ertugliflozin efficacy and Safety Cardiovascular Outcomes (VERTIS) study [49] where they investigated the effect of Ertugliflozin in patients with both T2D and cardiovascular disease. They found that not only did this inhibitor reduce the risk for first and total hospitalizations for heart failure but it also reduced the risk of death from heart failure/cardiovascular disease.
4. Use of selective SGLT2 Inhibition as a non-diabetic therapy
Although SGLT2 inhibitors were originally utilised for the treatment of type 2 diabetes specifically, this drug class is now also being used in non-diabetics to assist in protection against cardiorenal disease.
4.1. Preclinical Studies
4.1.1. Decreases Sympathetic Nervous System Activity
The SNS is a driver of hypertension, hyperglycemia and chronic kidney disease and remarkably our team and others have shown that SGLT2i’s may protect the kidneys and the heart through its sympathoinhibitory abilities [16,50]. In Apo E-/- mice, it was discovered that with the use of EMPA, norepinephrine (NE), the marker of heightened sympathetic activity was partially inhibited [51]. Our study with neurogenically hypertensive BPH/2J mice showed that DAPA lowered the NE and tyrosine hydroxylase (TH) levels in heart and kidneys [52].
Interestingly, the SNS performs diverse functions in different tissues. For instance, our team discovered that SGLT2 inhibition in the white adipose tissue (WAT) actually promoted sympathoexcitation and beiging. In a cohort of BPH/2J mice, DAPA was administered via oral gavage and the mice were found to have an increased level of tyrosine hydroxylase (TH) and norepinephrine expression in the WAT [52]. This is particularly exciting as beiging is a process that typically occurs during fasting or exercise. During beiging, there is an upregulation of Uncoupling Protein 1 (UCP1), but there is also an increase in the molecules a-Aminoisobutyric Acid, Irisin and Fibroblast growth factor 21 (FGF-21) [53].
4.1.2. Reductions in Blood Pressure
Studies have highlighted that SGLT2 inhibition promotes remarkable reductions in blood pressure. In our neurogenically hypertensive BPH/2J mice, treatment with DAPA significantly reduced systolic and diastolic blood pressure, as well as mean arterial pressure (Figure 3). This blood pressure reduction also correlated with a remarkable sympathoinhibitory effect in the kidneys [16].
4.1.3. Inflammation Control
One contributing pathogenic factor when it comes to both chronic kidney disease and heart disease is that of inflammation. In Apo E -/- mice, EMPA, DAPA and CANA were all found to reduce inflammatory markers. Empagliflozin reduced IL-1 and IL-6 [51], DAPA reduced IL-1, Interleukin 18 (IL-18) and the inflammasome marker NOD-LRR and Pyrin domain containing protein 3 (NLRP3) [54] whilst CANA reduced VCAM-1 and the Monocyte chemotactic protein-1 (MCP-1) inflammatory protein while increasing the TIMP metallopeptidase inhibitor 1 (TIMP-1) [18]. In our neurogenically hypertensive BPH/2J mice, we found that DAPA treatment reduced inflammation in the heart by significantly reducing the inflammatory cytokine IL-6 while at the same time increasing the anti-inflammatory cytokine Interleukin 10 (IL-10) [16].
4.1.4. Increases Ketone Levels
More and more research is now showing that ketone bodies are an efficient substrate for the heart [55] and the kidneys [56]. Empagliflozin has been shown in multiple studies to increase ketone bodies in patients with chronic heart failure [57], as well as in both ZSF1 [58] and ApoE knockout mice [59]. Although ketoacidosis is a topic of concern when it comes to utilization of SGLT2i’s, it is of much greater concern for those with T1D as opposed to T2D. Although ketoacidosis can occur in T2D patients not on insulin, a human study has shown that when T2D patients were admitted to hospital with COVID19, those who were administered SGLT2i therapy were at no greater risk of ketoacidosis than those not taking the inhibitors [60]. The subject of whether ketones increase or decrease SNS activity is still a controversy. In a pre-clinical study, it was found that the ketone body b-hydroxybutyrate suppresses SNS activity by antagonizing G protein coupled receptor 41 (GPR41) [61]. However, an alternative study involving rats showed that increased ketone body utilization did not suppress SNS activity and may stimulate it similarly to that seen with carbohydrates or fats [62]. In our future studies, we aim to assess whether ketone bodies suppress the SNS and consequently how they may promote cardiorenal health.
4.1.5. Improved Cardiovascular Health
Cardiomyopathy is a condition caused by inflammation in the cardiomyocytes, often through HFD consumption. In an in vitro study involving cultured rat H9c2 cardiomyocyte cells, treatment with the SGLT2 inhibitor DAPA attenuated hypertrophy, fibrosis and apoptosis. Furthermore, HFD fed mice were administered DAPA and this treatment improved the lipid profile as well as alleviated the HFD-induced cardiac dysfunction and cardiac inflammation [63].
4.1.6. Steatosis and Insulin Resistance
It is well known that SGLT2i’s lead to blood glucose reductions and weight loss in T2D. However, the influence of SGLT2 inhibition on high fat diet (HFD) induced obesity and insulin resistance is less well known. Preclinical studies in the C57BL/6J HFD mice found that when given the SGLT2i EMPA [64,65] or CANA [66], not only did it increase the urinary excretion of glucose but it also increased weight loss and attenuated hepatic steatosis in the treatment groups compared to vehicle. In addition, EMPA suppressed the HFD induced weight gain by enhancing fat utilization and browning and attenuated obesity induced inflammation and insulin resistance [64].
4.2. Human Clinical Trials
4.2.1. Empagliflozin
Empagliflozin is an SGLT2 inhibitor that has been approved for use in diabetics but it is now being increasingly used in human non-diabetics for cardiovascular and/or renal disease. In the Empagliflozin Outcome Trial in Patients with Chronic Heart Failure and a Reduced Ejection Fraction (EMPEROR-REDUCED) [67] it was concluded that patients on EMPA had a 25% lower risk of cardiovascular death or hospitalization for heart failure than those subjects on placebo irrespective of whether the patients had diabetes or not. Another trial known as the Empagliflozin Outcome Trial in Patients with Chronic Heart Failure with Preserved Ejection Fraction (EMPEROR-PRESERVED) [68] determined that EMPA treatment reduced the risk and severity of a broad range of inpatient and outpatient worsening heart failure events, therefore offering protective benefits. Aside from the EMPEROR trials, another clinical trial known as Empagliflozin in Acute Myocardial Infarction (EMMY) investigated the effect of EMPA on CVD [69]. This trial assessed the benefits of utilising EMPA in patients following acute myocardial infarction and found that EMPA significantly improved the echocardiographic functional and structural parameters. In addition, the EMMY clinical trial demonstrated that EMPA promoted a greater reduction in the N-terminal pro-hormone of brain natriuretic peptide (NT-proBNP) which is a heart failure marker. Finally, in order to ascertain the effect of EMPA on renal health, the Study of Heart and Kidney Protection with Empagliflozin (EMPA-KIDNEY) trial [70] was conducted which showed a lower risk of progression of kidney disease or death from cardiovascular causes compared to placebo.
4.2.2. Dapagliflozin
The second SGLT2 inhibitor that has been found to be beneficial in treating cardiovascular and renal disease in non-diabetics is DAPA. In the Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure (DAPA-HF) [71] and The Dapagliflozin Evaluation to Improve the Lives of Patients with Preserved Ejection Fraction Heart Failure (DELIVER) [72] clinical trials, patients on DAPA had a lowered risk of worsening heart failure or death from cardiovascular causes compared to placebo. To ascertain the effect DAPA has on renal health, the DAPA-CKD [47] and the Effects of the SGLT2 inhibitor Dapagliflozin on proteinuria in non-diabetic patients with Chronic Kidney Disease (DIAMOND) [73] trials were conducted. The DAPA-CKD trial showed a significant reduction in the risk of death from renal or cardiovascular causes and both trials showed that DAPA treatment reduced the GFR compared to placebo. While reduced GFR is a sign of progressive kidney disease, there is a phenomenon that occurs with SGLT2i known as the estimated GFR (eGFR) acute dip which is an acute reversible reduction in GFR. Of significance, the EMPA-REG [46], VERTIS-CV [49] and the CREDENCE [48] clinical trials have all confirmed that the dip in eGFR is not associated with progressive loss of long-term kidney function or acute kidney injury [74].
4.2.3. Ipragliflozin
Although not one of the main SGLT2i’s Ipragliflozin may also offer clinical potential, as demonstrated by a recent case study [75]. In this study, an 83-year-old man with chronic heart failure and T2D was hospitalized 4 times over 5 years, but with the use of Ipragliflozin, he displayed reduced cardiac sympathetic nerve activity and was not hospitalized for 2 years afterwards. The improved health of the patient may be due to the reduction in observed cardiac sympathetic nerve hyperactivity and this finding warrants further investigation of this inhibitor [75].
5. Discussion
5.1. Are Dual SGLT1/2 Inhibitors More Effective than Sole SGLT2 Inhibitors?
One of the burning questions at present is whether utilizing a dual SGLT1/2 inhibitor like Sotagliflozin (SOTA) may be more beneficial than sole SGLT2i's such as EMPA, CANA or DAPA when it comes to the treatment of cardiorenal disease in both diabetics or non-diabetics. As dual SGLT1/2 inhibition is a relatively new pharmacological therapy compared to sole SGLT2 inhibitors, the breadth of research findings is limited.
A study conducted in non-diabetic C57BL/6J mice found that treatment with SOTA attenuated cardiac hypertrophy and histological markers of cardiac fibrosis which were induced by the transverse aortic constriction (TAC) procedure [76].
Two clinical trials utilising SOTA are the Effect of Sotagliflozin on Cardiovascular Events in Patients with Type 2 Diabetes Post Worsening Heart Failure (SOLOIST-WHF) Trial [77] and the Effect of Sotagliflozin on Cardiovascular and Renal Events in Participants with Type 2 Diabetes and Renal Impairment Who Are At Cardiovascular Risk (SCORED) Trial [78]. Both the SOLOIST-WHF Trial and the SCORED Trial showed that in patients with T2D and CKD, the rate of hospitalization and urgent care visits for Heart Failure was reduced when the patients were administered SOTA compared to placebo. A new clinical trial, called the Sotagliflozin in Heart Failure with Preserved Ejection Fraction Patients (SOTA-P-CARDIA) trial [79] is currently underway to investigate the SOTA mediated cardiovascular effects and mechanisms of action in non-diabetic patients with heart failure with preserved ejection fraction (HFpEF).
5.2. Interesting Avenues for SGLT2i Therapy for the Treatment of T1D
To date, SGLT2i has not been clinically approved for the sole treatment of T1D, due to the concerns surrounding hypoglycemia and ketoacidosis. However, it is a field of research that is gaining momentum, both in the context of pre-clinical and clinical pilot studies.
5.2.1. Animal Studies Utilizing SGLT2i as a Treatment for T1D
Our team has conducted a great deal of research utilising our T1D Akimba mouse model. We have shown that SGLT2i may be a potential therapeutic for not just T2D but also T1D. When our Akimba mice were treated with the SGLT2i's DAPA [24,80], CANA [81] and EMPA [81], metabolic parameters such as fasting blood glucose levels, polydipsia (excessive thirst) and weight management were all improved. Aside from the metabolic advantages in our T1D mice, we determined that DAPA and EMPA conferred beneficial effects on (i) digestive health [37] by significantly increasing the beneficial short chain fatty acid butyric acid and (ii) diabetic retinopathy by reducing microvascular lesions [80,81,82] and reducing the pathogenic factor succinate [37].
Studies have shown that SGLT2i promotes an upregulation of the family member SGLT1 in the kidneys (Figure 4) and also causes a reduction in kidney size and an improvement in renal histology [83]. The compensatory upregulation of SGLT1 with SGLT2i warrants the use of dual SGLT1/2 inhibitors such as SOTA.
While we have studied the effects of SGLT2i in our Akita and Akimba mice with regards to kidney health, our future studies aim to determine how these inhibitors may also improve cardiovascular health in our T1D Akita mice as this strain is known to manifest diabetic cardiomyopathy with ageing [84].
5.2.2. Human Pilot Studies/Clinical Trials utilising SGLT2i as an addon to Insulin for Patients with Type 1 Diabetes
Due to the difficulty in managing insulin in T1D patients, there are many clinical trials and pilot studies that have investigated the effect of utilising the 3 main SGLT2 inhibitors, CANA [86], DAPA [87,88] or EMPA [89] as adjunctive therapies alongside insulin. While the inhibitors did promote ketoacidosis (KA), it was indicated that it was related to inadequately controlled insulin. Proper monitoring of glucose and ketone levels, as well as titration of the inhibitor/insulin may be able to control the incidence of ketoacidosis. The Empagliflozin as Adjunctive to Insulin Therapy (EASE) trial determined that a dose of 2.5mg/day of EMPA (phase 3) as opposed to a dose of 10mg/day of EMPA (phase 2) helped to reduce the incidence of KA and therefore the lower dose may be a viable treatment option.
All clinical trials including the Study of Effects of Canagliflozin as Add-on Therapy to Insulin in the Treatment of Participants With Type 1 Diabetes Mellitus (T1DM) [86] trial, the Dapagliflozin Evaluation in Patients With Inadequately Controlled Type 1 Diabetes (DEPICT-1) [87] and Efficacy and Safety of Dapagliflozin in Patients With Inadequately Controlled Type 1 Diabetes (DEPICT-2) [88] Dapagliflozin Trials and the EASE-2/3 [89] Empagliflozin trials showed that SGLT2i's promoted reductions in HbA1c, body weight and insulin requirements. Additionally, the afore mentioned clinical trials most importantly improved glycaemic control [90] after treatment, without producing any hypoglycemia.
5.3. Use of dual SGLT 1 / 2 Inhibitors in T1D
As highlighted above, there are many benefits to utilising SGLT2i’s for the treatment of T1D. This review has highlighted the promising emerging studies that have been conducted to show that SOTA is beneficial for T2D. A question that remains is whether the dual SGLT1/2 inhibitor, SOTA, may be beneficial for T1D and even surpass the benefits conferred by sole SGLT2 inhibitors. In our recent study utilising our T1D Akimba mice [85], we concluded that SOTA not only significantly decreased fasting blood glucose levels but also promoted healthy weight gain compared to vehicle counterparts. Aside from this, SOTA also improved the diabetes associated polydypsia. As mentioned previously, overactivation of the SNS is strongly associated with diabetes as well as cardiorenal disease and therefore understanding the effects that SOTA has on SNS activation is of critical importance. We found that SOTA therapy resulted in a reduction in the main neurotransmitter of the SNS, NE. This phenomenon is otherwise known as sympathoinhibition.
6. Conclusion
We have clearly demonstrated that SGLT2 inhibitors have enormous potential in improving renal and cardiovascular outcomes in patients with or without diabetes Figure 5). Although most research has been done in T2D, the use of SGLT2i in the treatment of T1D has also been found to be beneficial and definitely warrants further research.
Author Contributions
Conceptualisation, J.M. and V.B.M.; funding acquisition, L.H, V.B.M, M.P.S and J.M; writing—original draft, J.M. and V.B.M.; writing—review and editing, J.M., L.H., M.P.S. and V.B.M. All authors have read and agreed to the published version of the manuscript.
Funding
Diabetes Research WA.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not Applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
Jennifer Matthews, Lakshini Y. Herat and Vance B. Matthews declare that they have no conflict of interest. Markus P. Schlaich reports grants from Boehringer Ingelheim, while conducting the study.
References
- Kovesdy, C. Epidemiology of chronic kidney disease: an update 2022. Kidney Int Suppl 2011. 2022, 12(1), 7–11. [Google Scholar] [CrossRef] [PubMed]
- Keith, D.; Nichols, G.; Guillion, C.; Brown, J.; Smith, D. Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization. Arch Intern Med. 2004, 164(6), 659–663. [Google Scholar] [CrossRef] [PubMed]
- Aoki, J.; Nakajima, H.; Mori, M.; Sugimoto, T.; Hatori, M.; Tanimoto, S.; Amiya, E.; Hara, K. Clinical and pathologic characteristics of dilated cardiomyopathy in hemodialysis patients. Kidney Int. 2005, 67(1), 333–340. [Google Scholar] [CrossRef] [PubMed]
- Collins, A.; Foley, R.; Gilbertson, D.; Chen, S. United States Renal Data System public health surveillance of chronic kidney disease and end-stage renal disease. Kidney Int. Suppl. 2015, 5, 2–7. [Google Scholar] [CrossRef]
- Reutens, A. Epidemiology of diabetic kidney disease. Med. Clin. N. Am. 2013, 97, 1–18. [Google Scholar] [CrossRef]
- Hussain, S.; Chand Jamali, M.; Habib, A.; Hussain, M.; Akhtar, M.; Najmi, A. Diabetic kidney disease: An overview of prevalence, risk factors, and biomarkers. Clin. Epidemiol. Global Health. 2021, 9, 2–6. [Google Scholar] [CrossRef]
- Pavkov, M.; Bennett, P.; Knowler, W.; Krakoff, J.; Sievers, M.; Nelson, R. Effect of youth-onset type 2 diabetes mellitus on incidence of end-stage renal disease and mortality in young and middle-aged Pima Indians. JAMA. 2006, 296, 421–426. [Google Scholar] [CrossRef]
- Dasgupta, I. Cost of treating diabetic kidney disease. Indian J. Nephrol. 2014, 24, 139–140. [Google Scholar] [CrossRef]
- Breyer, M.; Susztak, K. Developing Treatments for Chronic Kidney Disease in the 21st Century. Semin. Nephrol. 2016, 36, 436–447. [Google Scholar] [CrossRef]
- Verma, D.; Firoz, A.; Garlapati, S.; Sathi, T.; Haris, M.; Dhungana, B.; Ray, B.; Shah, G.; Kc, B.; Paudel, P. Emerging treatments of Cardiorenal Syndrome: An update on Pathophysiology and Management. Cureus. 2021, 13(8), e17240.
- Sasso, F.; Pafundi, P.; Simeon, V.; De Nicola, L.; Chiodini, P.; Galiero, R.; Rinaldi, L.; Nevola, R.; Salvatore, T.; Sardu, C.; Marfella, R.; Adinolfi, L.; Minutolo, R. Efficacy and durability of multifactorial intervention on mortality and MACEs: A randomized clinical trial in type-2 diabetic kidney disease. Cardiovasc. Diabetol. 2021, 20, 145. [Google Scholar] [CrossRef]
- Breyer, M.; Susztak, K. The next generation of therapeutics for chronic kidney disease. Nat. Rev. Drug Discov. 2016, 15, 568–588. [Google Scholar] [CrossRef] [PubMed]
- Sano, R.; Shinozaki, Y.; Ohta, T. Sodium-glucose cotransporters: Functional properties and pharmaceutical potential. J Diabetes Investig. 2020, 11(4), 770–782. [Google Scholar] [CrossRef]
- Wright, E. The Intestinal Na+/- Glucose Cotransporter. Annu Rev Physiol. 1993, 55, 575–589. [Google Scholar] [CrossRef] [PubMed]
- Matthews, J.; Hibbs, M.; Herat, L.; Schlaich, M.; Matthews, V. The Sympathetic Nervous System Regulates Sodium Glucose Co-Transporter 1 Expression in the Kidney. Biomedicines. 2023, 11(3), 819. [Google Scholar] [CrossRef] [PubMed]
- Herat, L.; Magno, A.; Rudnicka, C.; Hricova, J.; Carnagarin, R.; Ward, N.; Arcambal, A.; Kiuchi, M.; Head, G.; Schlaich, M.; Matthews, V. SGLT2 Inhibitor-Induced Sympathoinhibition: A Novel Mechanism for Cardiorenal Protection. JACC Basic Transl. Sci. 2020, 5(2), 169–179. [Google Scholar] [CrossRef]
- Bailey, C.; Day, C.; Bellary, S. Renal Protection with SGLT2 inhibitors: Effects in Acute and Chronic Kidney Disease. Curr Diab Rep. 2022, 22(1), 39–52. [Google Scholar] [CrossRef]
- Chao, E.; Henry, R. SGLT2 Inhibition – a novel strategy for diabetes treatment. Nat Rev Drug Discov. 2010, 9(7), 551–559. [Google Scholar] [CrossRef]
- Zinman, B.; Wanner, C.; Lachin, J.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johanssen, E.; Woerle, H.; Broedl, U.; Inzucchi, S. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef]
- Wiviott, SD.; Raz, I.; Bonaca, M.; Mosenzon, O.; Kato, E.; Cahn, A.; Silverman, M.; Zelniker, T.; Kuder, J.; Murphy, S.; Bhatt, D.; Leiter, L.; McGuire, D.; Wilding, J.; Ruff, C.; Gause-Nilsson, I.; Fredriksson, M.; Johansson, P.; Langkilde, A.; Sabatine, M. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med. 2019, 380, 347–357. [Google Scholar] [CrossRef]
- Neal, B.; Perkovic, V.; Mahaffey, K.; Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N Engl J Med. 2017, 377, 644–657. [Google Scholar] [CrossRef]
- Xiang, B.; Zhao, X.; Zhou, X. Cardiovascular benefits of sodium glucose cotransporter 2 inhibitors in diabetic and nondiabetic patients. Cardiovasc Diabetol. 2021, 20(1), 78. [Google Scholar] [CrossRef]
- Dutka, M.; Bobinski, R.; Ulman-Wlodarz, I.; Hajduga, M.; Bujok, J.; Pajak, C.; Cwiertnia, M. Sodium glucose cotransporter 2 inhibitors: mechanisms of action in heart failure. Heart Fail Rev. 2021, 26(3), 603–622. [Google Scholar] [CrossRef] [PubMed]
- Shaffner, J.; Chen, B.; Malhotra, D.; Dworkin, L.; Gong, R. Therapeutic targeting of SGLT2: A New Era in the Treatment of Diabetes and Diabetic Kidney Disease. Front Endocrinol. 2021, 12, 749010. [Google Scholar] [CrossRef] [PubMed]
- Suga, T.; Kikuchi, O.; Kobayashi, M.; Matsui, S.; Yokota-Hashimoto, H.; Wada, E.; Kohno, D.; Sasaki, T.; Takeuchi, K.; Kakizaki, S.; Yamada, M.; Kitamura, T. SGLT1 in pancreatic a cells regulate glucagon secretion in mice, possibly explaining the distinct effects of SGLT2 inhibitors on plasma glucagon levels. Mol Metab. 2019, 19, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Vrhovac, I.; Eror, D.; Klessen, D.; Burger, C.; Breljak, D.; Kraus, O.; Radovic, N.; Jadrijevic, S.; Aleksic, I.; Walles, T.; Sauvant, C.; Sabolic, I.; Koepsell, H. Localizations of Na(+)-D-glucose cotransporters SGLT1 and SGLT2 in human kidney and of SGLT1 in human small intestine, liver, lung and heart. Pflugers Arch. 2015, 467(9), 1881–1898. [Google Scholar] [CrossRef]
- Herat, LY; Matthews, V; Rakoczy, E; Carnagarin R; Schlaich, M. Focusing on Sodium Glucose Co-transporter-2 (SGLT2) and its potential impact in diabetic retinopathy. International Journal of Endocrinology. 2018, 2018:9254126. [CrossRef]
- Tahara, A; Takasu, T; Yokono, M; Imamura, M; Kurosaki, E. Characterization and comparison of sodium-glucose cotransporter 2 inhibitors in pharmacokinetics, pharmacodynamics, and pharmacologic effects. J Pharmacol Sci. 2016, 130(3): 159-169. [CrossRef]
- Tahara, A; Takasu, T; Yokono, M; Imamura, M; Kurosaki, E. Characterization and comparison of sodium-glucose cotransporter 2 inhibitors: Part2. Antidiabetic effects in type 2 diabetic mice. J Pharmacol Sci. 2016, 131(3): 198-208. [CrossRef]
- Tahara, A; Takasu, T; Yokono, M; Imamura, M; Kurosaki, E. Characterization and comparison of sodium-glucose cotransporter 2 inhibitors: Part3. Effects on diabetic complications in type 2 diabetic mice. Eur J Pharmacol. 2017, 809: 163-171. [CrossRef]
- Majewski, C.; Bakris, G. Blood Pressure Reduction: An Added Benefit of Sodium-Glucose Cotransporter 2 Inhibitors in Patients with Type 2 Diabetes. Diabetes Care. 2015, 38(3), 429-430.
- Tikkanen, I.; Narko, K.; Zeller, C.; Green, A.; Salsali, A.; Broedl, U.; Woerle, H. Empagliflozin reduces blood pressure in patients with type 2 diabetes and hypertension. Diabetes Care. 2015, 38(3), 420–428. [Google Scholar] [CrossRef]
- Sjostrom, C.; Johansson, P.; Ptaszynska, A.; List, J.; Johnsson, E. Dapagliflozin lowers blood pressure in hypertensive and non-hypertensive patients with type 2 diabetes. Diab Vasc Dis Res. 2015, 12(5), 352–358. [Google Scholar] [CrossRef]
- Matthews, V.; Elliot, R.; Rudnicka, C.; Hricova, J.; Herat, L.; Schlaich, M. Role of the sympathetic nervous system in regulation of the sodium glucose cotransporter 2. J Hypertens. 2017, 35(10), 2059–2068. [Google Scholar] [CrossRef]
- Wu, J; Chen, Y; Yang, H; Gu, L; Ni, Z; Mou, S; Shen, J; Che, X. Sodium glucose co-transporter 2 (SGLT2) inhibition via dapagliflozin improves diabetic kidney disease (DKD) over time associated with increasing effect on the gut microbiota in db/db mice. Front Endocrinol. 2023, 14:1026040. [CrossRef]
- Lee, D; Battson, M; Jarrell, D; Hou, S; Ecton, K; Weir, T; Gentile, C. SGLT2 inhibition via dapagliflozin improves generalized vascular dysfunction and alters the gut microbiota in type 2 diabetic mice. Cardiovasc Diabetol. 2018, 17(1):62. [CrossRef]
- Herat, L.; Ward, N.; Magno, A.; Rakoczy, E.; Kiuchi, M.; Schlaich, M.; Matthews, V. Sodium glucose co-transporter 2 inhibition reduces succinate levels in diabetic mice. World J Gastroenterol. 2020, 26(23), 3225–3235. [Google Scholar] [CrossRef]
- Deng, L; Yang, Y; Xu, G. Empagliflozin ameliorates type 2 diabetes mellitus-related diabetic nephrophathy via altering the gut microbiota. Biochim Biophys Acta Mol Cell Biol Lipids. 2022, 1867(12): 159234. [CrossRef]
- Hata, S; Okamura, T; Kobayashi, A; Bamba, R; Miyoshi, T; Nakajima, H; Kitagawa, N; Hashimoto, Y; Majima, S; Senmaru, T; Okada, H; Ushigome, E; Nakanishi, N; Takakuwa, H; Sasano, R; Hamaguchi, M; Fukui, M. Gut Microbiota Changes by an SGLT2 Inhibitor, Luseogliflozin, Alters Metabolites Compared with Those in a Low Carbohydrate Diet in db/db Mice. Nutrients. 2022, 14(17): 3531. [CrossRef]
- Gong, Q; Zhang, R; Wei, F; Fang, J; Zhang, J; Sun, J; Sun, Q; Wang, H. SGLT2 inhibitor-empagliflozin treatment ameliorates diabetic retinopathy manifestations and exerts protective effects associated with augmenting branched chain amino acids catabolism and transportation in db/db mice. Biomedicine and Pharmacotherapy. 2022, 152:113222. [CrossRef]
- Luo, Q; Leley, S; Bello, E; Dhami, H; Mathew, D; Bhatwadekar, A. Dapagliflozin protects neural and vascular dysfunciton of the retinas in diabetes. BMJ Open Diabetes Res Care. 2022, 10(3):e002801. [CrossRef]
- Tang, L; Wu, Y; Tian, M; Sjostrom, C; Johansson, U; Peng, X; Smith, D; Huang, Y. Dapagliflozin slows the progression of the renal and liver fibrosis associated with type 2 diabetes. Am J Physiol Endocrinol Metab. 2017, 313(5): E563-E576. [CrossRef]
- Shin, S; Chung, S; Kim, S; Lee, E; Yoo, Y; Kim, J; Ahn, Y; Kim, E; Moon, S; Kim, M; Ko, S. Effect of Sodium-Glucose Co-Transporter 2 Inhibitor, Dapagliflozin, on Renal Renin-Angiotensin System in an Animal Model of Type 2 Diabetes. PLoS One. 2016, 11(11): e0165703.
- Kojima, N; Williams, J; Takahashi, T; Miyata, N; Roman, R. Effects of a new SGLT2 inhibitor, Luseogliflozin, on diabetic nephropathy in T2D rats. J Pharmacol Exp Ther. 2013, 345(3): 464-72. [CrossRef]
- Lin, B; Koibuchi, N; Hasegawa, Y; Sueta, D; Toyama, K; Uekawa, K; Ma, M; Nakagawa, T; Husaka, H; Kim-Mitsuyama, S. Glycemic control with empagliflozin, a novel selective SGLT2 inhibitor, ameliorates cardiovascular injury and cognitive dysfunction in obese and type 2 diabetic mice. Cardiovasc Diabetol. 2014, 13:148. [CrossRef]
- Wanner, C.; Inzucchi, S.; Lachin, J.; Fitchett, D.; Von Eynatten, M.; Mattheus, M.; Johansen, E.; Woerle, H.; Broedl, U.; Zinman, B. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N Eng J Med. 2016, 375, 323–334. [Google Scholar] [CrossRef]
- Heerspink, H.; Stefansson, B.; Correa-Rotter, R.; Chertow, G.; Greene, T.; Hou, F.; Mann, J.; McMurray, J.; Lindberg, M.; Rossing, P.; Sjostrom, D.; Toto, R.; Langkilde, A.; Wheeler, D. Dapagliflozin in Patients with Chronic Kidney Disease. N Eng J Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Perkovic, V.; Jardine, M.; Neal, B.; Bompoint, S.; Heerspink, H.; Charytan, D.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; Cannon, C.; Capuano, G.; Chu, P.; Zeeuw, D.; Greene, T.; Levin, A.; Pollock, C.; Wheeler, D.; Yavin, Y.; Zhang, H.; Zinman, B.; Meininger, G.; Brenner, B.; Mahaffey, K. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N Engl J Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [PubMed]
- Cannon, C.; Pratley, R.; Dagogo-Jack, S.; Mancuso, J.; Huyck, S.; Masiukiewicz, U.; Charbonnel, B.; Frederich, R.; Gallo, S.; Cosentino, F.; Shih, W.; Gantz, I.; Terra, S.; Cherney, D.; McGuire, D. Cardiovascular Outcomes with Ertugliflozin in Type 2 Diabetes. N Eng J Med. 2020, 383, 1425–1435. [Google Scholar] [CrossRef]
- Herat, L.; Matthews, J.; Azzam, O.; Schlaich, M.; Matthews, V. Targeting features of the metabolic syndrome through sympatholytic effects of SGLT inhibition. Curr Hypertens Rep. 2022, 24(3), 67–74. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wu, M.; Xu, B.; Kang, L. Empagliflozin Alleviates Atherosclerosis Progression by Inhibiting Inflammation and Sympathetic Activity in a Normoglycemic Mouse Model. J Inflamm Res. 2021, 14, 2277–2287. [Google Scholar] [CrossRef] [PubMed]
- Matthews, J.; Herat, L.; Magno, A.; Gorman, S.; Schlaich, M.; Matthews, V. SGLT-2 Inhibitor-Induced Sympathoexcitation in White Adipose Tissue: A Novel Mechanism of Beiging. Biomedicines. 2020, 8(11), 514. [Google Scholar] [CrossRef]
- Machado, S.; Pasquarelli-do-Nascimento, G.; Santos da Silva, D.; Farias, G.; de Oliveira Santos, I.; Baptista, L.; Magalhaes, K. Browning of the white adipose tissue regulation: new insights into nutritional and metabolic relevance in health and diseases. Nutr Metab. 2022, 19(1), 61. [Google Scholar] [CrossRef]
- Leng, W.; Ouyang, X.; Lei, X.; Wu, M.; Chen, L.; Wu, Q.; Deng, W.; Liang, Z. The SGLT-2 Inhibitor Dapagliflozin Has a Therapeutic Effect on Atherosclerosis in Diabetic ApoE-/- Mice. Mediators Inflamm. 2016. [CrossRef]
- Papazafiropoulou, A.; Georgopoulos, M.; Katsilambros, N. Ketone bodies and the heart. Arch Med Sci Atheroscler Dis. 2021, 6, e209–e214. [Google Scholar] [CrossRef]
- Qiu, Y.; Hu, X.; Xu, C.; Lu, C.; Cao, R.; Xie, Y.; Yang, J. Ketogenic diet alleviates renal fibrosis in mice by enhancing fatty acid oxidation through the free fatty acid receptor 3 pathway. Front Nutr. 2023, 10, 1127845. [Google Scholar] [CrossRef]
- Pietschner, R.; Kolwelter, J.; Bosch, A.; Striepe, K.; Jung, S.; Kannenkeril, D.; Ott, C.; Schiffer, M.; Achenbach, S.; Schmieder, R. Effect of empagliflozin on ketone bodies in patients with chronic heart failure. Cardiovascular Diabetology. 2021, 20(1), 219. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Farooq, M.; Gaertner, S.; Bruckert, C.; Qureshi, A.; Lee, H.; Benrahla, D.; Pollet, B.; Stephan, D.; Ohlmann, P.; Lessinger, J.; Mayoux, E.; Auger, C.; Morel, O.; Schini-Kerth, V. Empaglifozin improved systolic blood pressure, endothelial dysfunction and heart remodeling in the metabolic syndrome ZSF1 rat. Cardiovasc Diabetol. 2020, 19(1), 19. [Google Scholar] [CrossRef] [PubMed]
- Tomita, I.; Kume, S.; Sugahara, S.; Osawa, N.; Yamahara, K.; Yasuda-Yamahara, M.; Takeda, N.; Chin-Kanasaki, M.; Kaneko, T.; Mayoux, E.; Mark, M.; Yanagita, M.; Ogita, H.; Araki, S.; Maegawa, H. SGLT2 inhibition mediates protection from diabetic kidney disease by promoting ketone body-induced mTORC1 inhibition. Cell Metab. 2020, 32(3), 404-419.e6. [CrossRef]
- Khunti, K.; Ruan, Y.; Davies, J.; Field, B.; Harris, S.; Kosiborod, M.; Nagi, D.; Narendran, P.; Patel, D.; Ryder, R.; Varnai, K.; Wild, S.; Wilmot, E.; Rea, R. Association between SGLT2 Inhibitor Treatment and Diabetic Ketoacidosis and Mortality in People with Type 2 Diabetes Admitted to Hospital with COVID-19. Diabetes Care. 2022, 45(12), 2838–2843. [Google Scholar] [CrossRef] [PubMed]
- Kimura, I; Inoue, D; Maeda, T; Hara, T; Ichimura, A; Miyauchi, S; Kobayashi, M; Hirasawa, A; Tsujimoto, G. Short-chain fatty acids and ketones directly regulate sympathetic nervous system via G protein-coupled receptor 41 (GPR41). Proc Natl Acad Sci U S A. 2011, 108(19): 8030-8035. [CrossRef]
- Kolanowski, J; Young, J; Landsberg, L. Stimulatory influence of D(-)3-hydroxybutyrate feeding on sympathetic nervous system activity in the rat. Metabolism. 1994, 43(2): 180-5. [CrossRef]
- Lin, K.; Yang, N.; Luo, W.; Qian, J.; Zhu, W.; Ye, S.; Yuan, C.; Xu, D.; Liang, G.; Huang, W.; Shan, P. Direct cardio-protection of Dapagliflozin against obesity-related cardiomyopathy via NHE1/MAPK signaling. Acta Pharmacol Sin. 2022, 43(10), 2624–2635. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Nagata, N.; Nagashimada, M.; Zhuge, F.; Ni, Y.; Chen, G.; Mayoux, E.; Kaneko, S.; Ota, T. SGLT2 Inhibition by Empagliflozin Promotes Fat Utilization and Browning and Attenuates Inflammation and Insulin Resistance by Polarizing M2 Macrophages in Diet-induced Obese Mice. EbioMedicine. 2017, 20, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Radlinger, B; Ress, C; Folie, S; Salzmann, K; Lechuga, A; Weiss, B; Salvenmoser, W; Graber, M; Hirsch, J; Holfeld, J; Kremser, C; Moser, P; Staudacher, G; Jelenik, T; Roden, M; Tilg, H; Kaser, S. Empagliflozin protects mice against diet-induced obesity, insulin resistance and hepatic steatosis. Diabetologia. 2023, 66(4): 754-767. [CrossRef]
- Ji, W.; Zhao, M.; Wang, M.; Yan, W.; Liu, Y.; Ren, S.; Lu, J.; Wang, B.; Chen, L. Effects of canagliflozin on weight loss in high-fat-diet-induced obese mice. PLoS One. 2017, 12(6), e0179960. [Google Scholar] [CrossRef]
- Packer, M.; Anker, S.; Butler, J.; Filippatos, G.; Pocock, S.; Carson, P.; Januzzi, J.; Subodh, V.; Tsutsui, H.; Brueckmann, M.; Jamal, W.; Kimura, K.; Schnee, J.; Zeller, C.; Cotton, D.; Bocchi, E.; Bohm, M.; Choi, D.; Chopra, V.; Chuquiure, E.; Giannetti, N.; Janssens, S.; Zhang, J.; Gonzalez Juanatey, J.; Kaul, S.; Brunner-La Rocca, H.; Merkely, B.; Nicholls, S.; Perrone, S.; Pina, I.; Ponikowski, P.; Sattar, N.; Senni, M.; Seronde, M.; Spinar, J.; Squire, I.; Taddei, S.; Wanner, C.; Zannad, F. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N Eng J Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Packer, M.; Butler, J.; Zannad, F.; Filippatos, G.; Ferreira, J.; Pocock, S.; Carson, P.; Anand, I.; Doehner, W.; Haass, M.; Komajda, M.; Miller, A.; Pehrson, S.; Teerlink, J.; Schnaidt, S.; Zeller, C.; Schnee, J.; Anker, S. Effect of Empagliflozin on Worsening Heart Failure Events in Patients With Heart Failure and Preserved Ejection Fraction: EMPEROR-Preserved Trial. Circulation. 2021, 144(16), 1284–1294. [Google Scholar] [CrossRef]
- Lewinski, D; Kolesnik, E; Tripolt, N; Pferschy, P; Benedikt, M; Wallner, M; Alber, H; Berger, R; Lichtnauer, M; Saely, C; Moertl, D; Auersperg, P; Reiter, C; Rieder, T; Siller-Matula, J; Gager, G; Hasun, M; Weidinger, F; Pieber, T; Zechner, P; Herrmann, M; Zirlik, A; Holman, R; Oulhaj, A; Sourij, H. Empagliflozin in acute myocardial infarction: the EMMY trial. Eur Heart J. 2022, 43(41): 4421-4432. [CrossRef]
- Herrington, W.; Staplin, N.; Wanner, C.; Green, J.; Hauske, S.; Emberson, J.; Preiss, D.; Judge, P.; Mayne, K.; Ng, S.; Sammon, E.; Zhu, D.; Hill, M.; Stevens, W.; Wallendszus, K.; Brenner, S.; Cheung, A.; Liu, Z.; Li, J.; Hooi, L.; Liu, W.; Kadowaki, T.; Nangaku, M.; Levin, A.; Cherney, D.; Maggioni, A.; Pontremoli, R.; Deo, R.; Goto, S.; Rossello, X.; Tuttle, K.; Steubl, D.; Petrini, M.; Massey, D.; Eilbracht, J.; Brueckmann, M.; Landray, M.; Baigent, C.; Haynes, R. Empagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2023, 388(2), 117–127. [Google Scholar] [CrossRef]
- McMurray, J.; Solomon, S.; Inzucchi, S.; Kober, L.; Kosiborod, M.; Martinez, F.; Ponikowski, P.; Sabatine, M.; Anand, I.; Belohlavek, J.; Bohm, M.; Chiang, C.; Chopra, V.; deBoer, R.; Desai, A.; Diez, M.; Drozdz, J.; Dukat, A.; Ge, J.; Howlett, J.; Katova, T.; Kitakaze, M.; Ljungman, C.; Merkely, B.; Nicolau, J.; O’Meara, E.; Petrie, M.; Vinh, P.; Schou, M.; Tereshchenko, S.; Verma, S.; Held, C.; DeMets, D.; Docherty, K.; Jhund, P.; Bengtsson, O.; Sjostrand, M.; Langkilde, A. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N Eng J Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef]
- Solomon, S.; McMurray, J.; Claggett, B.; Boer, R.; DeMets, D.; Hernandez, A.; Inzucchi, S.; Kosiborod, M.; Lam, C.; Martinez, F.; Shah, S.; Desai, A.; Jhund, P.; Belohlavek, J.; Chiang, C.; Borleffs, C.; Comin-Colet, J.; Dobreanu, D.; Drozdz, J.; Fang, J.; Alcocer-Gamba, M.; Habeeb, W.; Han, Y.; Honorio, J.; Janssens, S.; Katova, T.; Kitakaze, M.; Merkely, B.; O’Meara, E.; Saraiva, J.; Tereshchenko, S.; Thierer, J.; Vaduganathan, M.; Vardeny, O.; Verma, S.; Pham, V.; Wilderang, U.; Zaozerska, N.; Bachus, E.; Lindholm, D.; Petersson, M.; Langkilde, A. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N Engl J Med. 2022, 387(12), 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Cherney, D.; Dekkers, C.; Barbour, S.; Cattran, D.; Abdul Gafor, AH.; Greasley, P.; Laverman, G.; Kun Lim, S.; Di Tanna, G.; Reich, H.; Vervloet, M.; Wong, M.; Gansevoort, R.; Heerspink, H. Effects of the SGLT2 inhibitor dapagliflozin on proteinuria in non-diabetic patients with chronic kidney disease (DIAMOND): a randomized, double-blind, crossover trial. Lancet Diabetes Endocrinol. 2020, 8(7), 582–593. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.; Cherney, D. Clinical Implications of an Acute Dip in eGFR after SGLT2 Inhibitor Initiation. Clin J Am Soc Nephrol. 2021, 16(8), 1278–1280. [Google Scholar] [CrossRef] [PubMed]
- Kiuchi, S.; Hisatake, S.; Kabuki, T.; Fujii, T.; Oka, T.; Dobashi, S.; Hashimoto, H.; Ikeda, T. Long-term use of ipragliflozin improved cardiac sympathetic nerve activity in a patient with heart failure: A case report. Drug Discov Ther. 2018, 12(1), 51-54.
- Young, S; Ryan, L; Mullins, T; Flint, M; Steane, S; Walton, S; Bielefeldt-Ohmann, H; Carter, D; Reichelt, M; Gallo, L. Sotagliflozin, a dual SGLT1/2 Inhibitor, improves cardiac outcomes in a mouse model of early heart failure without diabetes. Front Physiol. 2021, 12: 738594. [CrossRef]
- Bhatt, D; Szarek, M; Steg, P; Cannon, C; Leiter, L; McGuire, D; Lewis, J; Riddle, M; Voors, A; Metra, M; Lund, L; Komajda, M; Testani, J; Wilcox, C; Ponikowski, P; Lopes, R; Verma, S; Lapuerta, P; Pitt, B. Sotagliflozin in Patients with Diabetes and Recent Worsening Heart Failure. N Engl J Med. 2021, 384(2):117-128. [CrossRef]
- Bhatt, D.; Szarek, M.; Pitt, B.; Cannon, C.; Leiter, L.; McGuire, D.; Lewis, J.; Riddle, M.; Inzucchi, S.; Kosiborod, M.; Cherney, D.; Dwyer, J.; Scirica, B.; Bailey, C.; Diaz, R.; Ray, K.; Udell, J.; Lopes, R.; Lapuerta, P.; Steg, P. Sotagliflozin in Patients with Diabetes and Chronic Kidney Disease. N Engl J Med. 2021, 384(2), 129–139. [Google Scholar] [CrossRef] [PubMed]
- Perez, M; Rodriguez-Capitan, J; Requena-Ibanez, J; Santos-Gallego, C; Zafar, M; Escolar, G; Mancini, D; Mitter, S; Lam, D; Contreras, J; Fergus, I; Atallah-Lajam, F; Abascal, V; Lala, A; Moreno, P; Moss, N; Lerakis, S; Sanz, J; Fuster, V; Badimon, J. Rationale and Design of the SOTA-P-CARDIA Trial (ATRU-V): Sotagliflozin in HFpEF Patients Without Diabetes. Cardiovasc Drugs Ther. 2023. [CrossRef]
- Herat, L.; Matthews, J.; Ong, W.; Rakoczy, E.; Schlaich, M.; Matthews, V. Determining the Role of SGLT2 Inhibition with Dapagliflozin in the Development of Diabetic Retinopathy. Front Biosci. 2022, 27(12), 320. [Google Scholar] [CrossRef] [PubMed]
- Herat, L.; Matthews, J.; Rakoczy, E.; Schlaich, M.; Matthews, V. Comparing and Contrasting the Effects of the SGLT Inhibitors Canagliflozin and Empagliflozin on the Progression of Retinopathy. Front Biosci. 2023, 28(4), 83. [Google Scholar] [CrossRef]
- Matthews, J.; Herat, L.; Rooney, J.; Rakoczy, E.; Schlaich, M.; Matthews, V. Determining the Role of SGLT2 inhibition with Empagliflozin in the development of diabetic retinopathy. Biosci Rep. 2022, 42(3), BSR20212209. [Google Scholar] [CrossRef]
- Matthews, J; Schlaich, M; Rakoczy, E; Matthews, V; Herat, L. The Effect of SGLT2 Inhibition on Diabetic Kidney Disease in a Model of Diabetic Retinopathy. Biomedicines. 2022, 10(3): 522. [CrossRef]
- Kesherwani, V; Shahshahan, H; Mishra, P. Cardiac transcriptome profiling of diabetic Akita mice using microarray and next generation sequencing. PLoS One. 2017, 12(8): e0182828. [CrossRef]
- Herat, L.; Matthews, J.; Hibbs, M.; Rakoczy, E.; Schlaich, M.; Matthews, V. Combined SGLT1 and 2 inhibition is associated with improved glucose control and multi-organ protection in the type 1 diabetic Akimba mouse. iScience. 2023. [CrossRef]
- Henry, R; Thakkar, P; Tong, C; Polidori, D; Alba, M. Efficacy and Safety of Canagliflozin, a Sodium-Glucose Cotransporter 2 Inhibitor, as Add-on to Insulin in Patients with Type 1 Diabetes. Diabetes Care. 2015, 38(12): 2258-65. [CrossRef]
- Dandona, P; Mathieu, C; Phillip, M; Hansen, L; Griffen, S; Tschope, D; Thoren, F; Xu, J; Langkilde, A. Efficacy and safety of dapagliflozin in patients with inadequately controlled type 1 diabetes (DEPICT-1): 24 week results from a multicentre, double-blind, phase 3, randomised controlled trial. The Lancet. 2017, 5(11): 864-876. [CrossRef]
- Mathieu, C; Rudofsky, G; Phillip, M; Araki, E; Lind, M; Arya, N; Thoren, F; Scheerer, M; Iqbal, N; Dandona, P. Long-term efficacy and safety of dapagliflozin in patients with inadequately controlled type 1 diabetes (the DEPICT-2 study): 52-week results from a randomized controlled trial. Diabetes, Obesity and Metabolism. 2020, 22(9): 1516-1526. [CrossRef]
- Rosenstock, J; Marquard, J; Laffel, L; Neubacher, D; Kaspers, S; Cherney, D; Zinman, B; Skyler, J; George, J; Soleymanlou, N; Perkins, B. Empagliflozin as Adjunctive to Insulin Therapy in Type 1 Diabetes: The EASE Trials. Diabetes Care. 2018, 41(12): 2560-2569. [CrossRef]
- Paik, J; Blair, H. Dapagliflozin: A Review in Type 1 Diabetes. Drugs. 2019, 79(17): 1877-1884. [CrossRef]
- Zinman, B; Lachin, J; Inzucchi, S. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med (Letter). 2016, 374(11): 1094.
- Cefalo, C; Cinti, F; Moffa, S; Impronta, F; Sorice, G; Mezza, T; Pontecorvi, A; Giaccari, A. Sotagliflozin, the first dual SGLT inhibitor: current outlook and perspectives. Cardiovasc Diabetol. 2019, 18(1):20. [CrossRef]
Figure 1.
SGLT1 and SGLT2 sodium and glucose transport in intestinal lumen (SGLT1) and proximal tubule lumen in the kidneys (SGLT2).
Figure 1.
SGLT1 and SGLT2 sodium and glucose transport in intestinal lumen (SGLT1) and proximal tubule lumen in the kidneys (SGLT2).
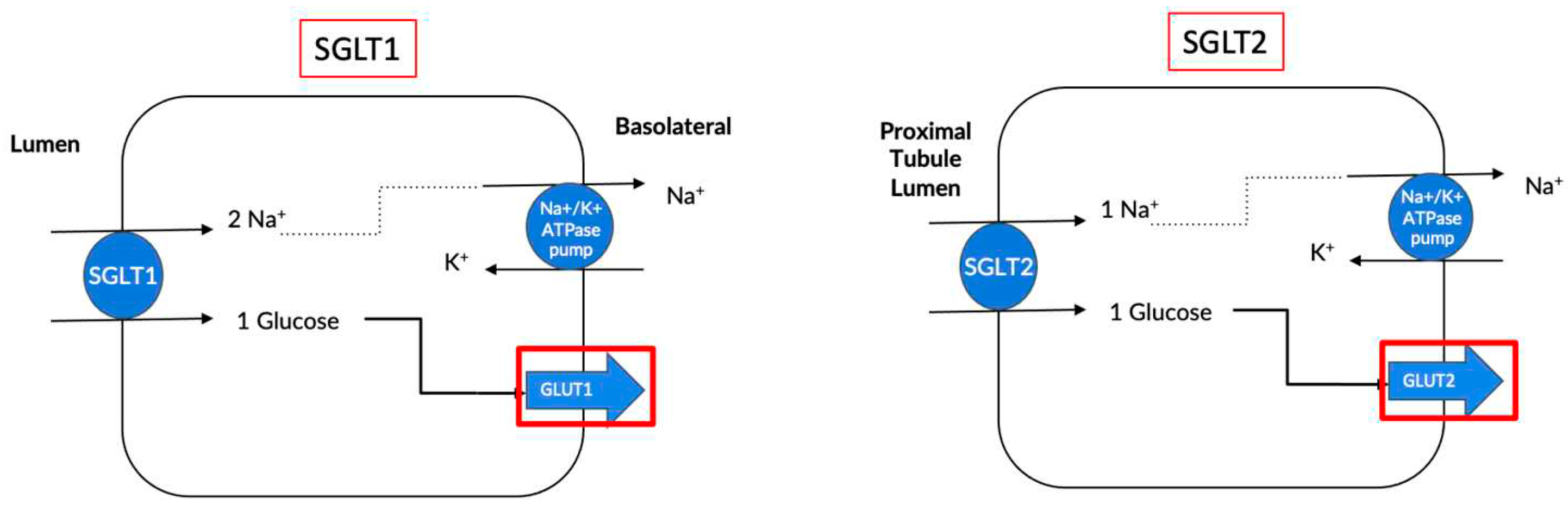
Figure 2.
Tyrosine hydroxylase expression in kidney. Representative immunohistochemistry images of tyrosine hydroxylase expression in kidney from mice fed chow (A), high-fat diet (B) or high-fat diet and DAPA treatment (C). Tyrosine hydroxylase staining is indicated with arrows. Magnification 200X. (D) Tyrosine hydroxylase quantitation, n = 3-5 mice per group; * P < 0.0012; Mean + SEM. (E) Noradrenaline content in kidney from HFD and HFD and DAPA mice, n = 4-13 mice/group; ** P < 0.05; Mean + SEM. Figure taken from [34].
Figure 2.
Tyrosine hydroxylase expression in kidney. Representative immunohistochemistry images of tyrosine hydroxylase expression in kidney from mice fed chow (A), high-fat diet (B) or high-fat diet and DAPA treatment (C). Tyrosine hydroxylase staining is indicated with arrows. Magnification 200X. (D) Tyrosine hydroxylase quantitation, n = 3-5 mice per group; * P < 0.0012; Mean + SEM. (E) Noradrenaline content in kidney from HFD and HFD and DAPA mice, n = 4-13 mice/group; ** P < 0.05; Mean + SEM. Figure taken from [34].
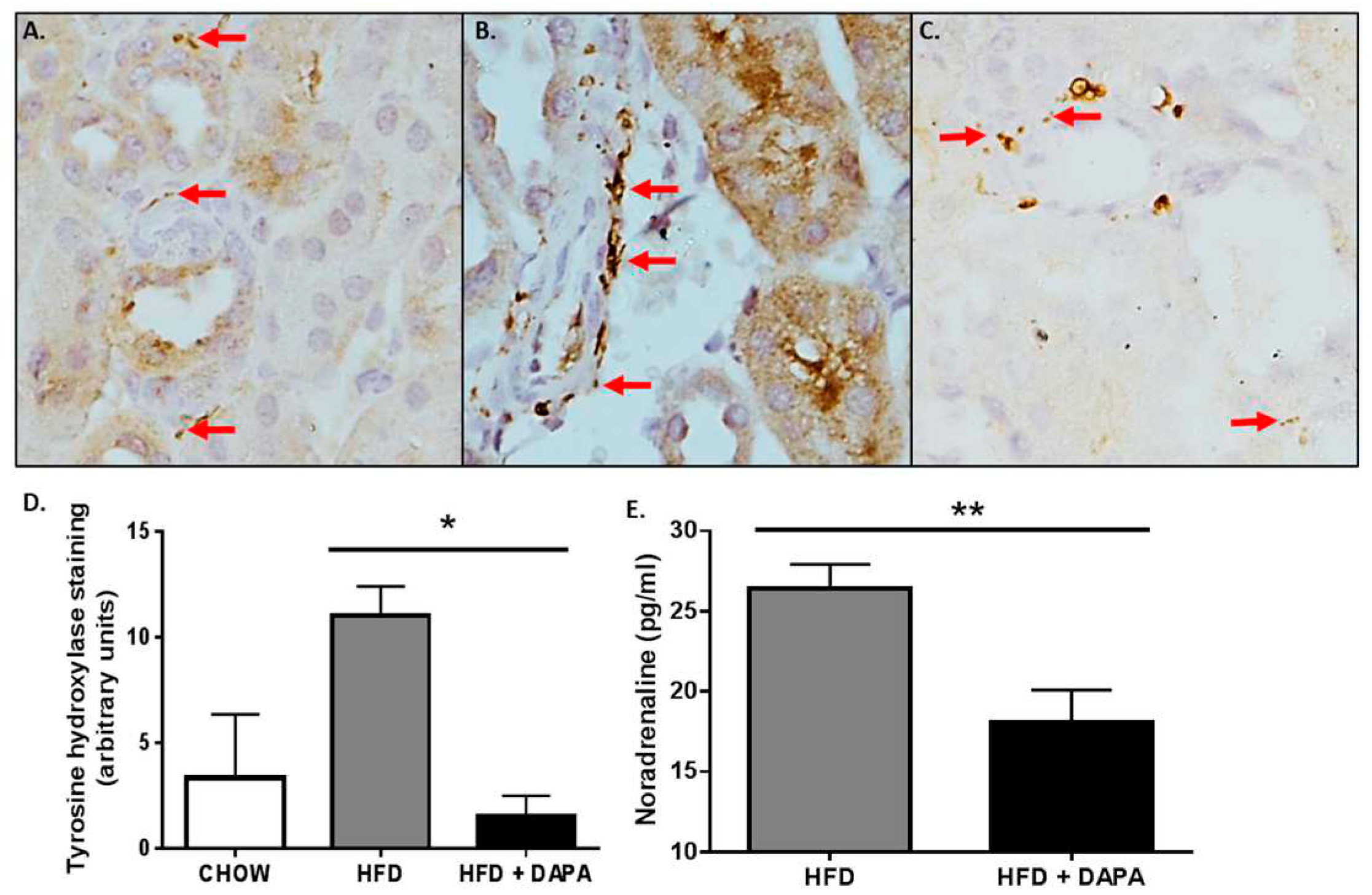
Figure 3.
SGLT2 inhibition with DAPA treatment prevents the increase in blood pressure in neurogenically hypertensive mice. Effects of DAPA treatment on (A) systolic blood pressure, (B) diastolic blood pressure and (C) mean arterial blood pressure were measured using a tail-cuff apparatus. n= 10-12 mice/group; *p= 0.006 ; **p= 0.0003 ; ***p= 0.0008 ; All data represented as mean ± SEM. Figure taken from [16].
Figure 3.
SGLT2 inhibition with DAPA treatment prevents the increase in blood pressure in neurogenically hypertensive mice. Effects of DAPA treatment on (A) systolic blood pressure, (B) diastolic blood pressure and (C) mean arterial blood pressure were measured using a tail-cuff apparatus. n= 10-12 mice/group; *p= 0.006 ; **p= 0.0003 ; ***p= 0.0008 ; All data represented as mean ± SEM. Figure taken from [16].
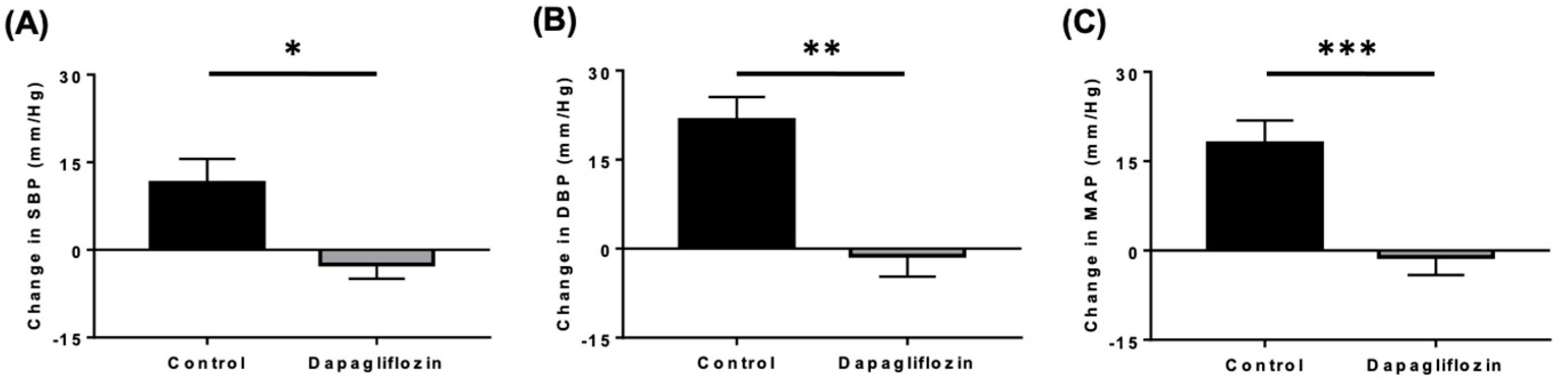
Figure 4.
SGLT2 inhibition results in increased luminal SGLT1 expression in renal tissue of diabetic Akimba mice. Representative SGLT1 immunohistochemistry images of renal tissue of mice treated with (A) vehicle or (B) Empagliflozin [EMPA] via drinking water (25 mg/kg/day) for 8 weeks. (C) Quantitation of SGLT1 intensity; n=3-4 mice/group; mean+SEM. **p=0.005. Black arrow = luminal SGLT1 expression. Intensity: 0 = absent – 3 = high intensity; FOV, Field of view. Figure taken from [85].
Figure 4.
SGLT2 inhibition results in increased luminal SGLT1 expression in renal tissue of diabetic Akimba mice. Representative SGLT1 immunohistochemistry images of renal tissue of mice treated with (A) vehicle or (B) Empagliflozin [EMPA] via drinking water (25 mg/kg/day) for 8 weeks. (C) Quantitation of SGLT1 intensity; n=3-4 mice/group; mean+SEM. **p=0.005. Black arrow = luminal SGLT1 expression. Intensity: 0 = absent – 3 = high intensity; FOV, Field of view. Figure taken from [85].
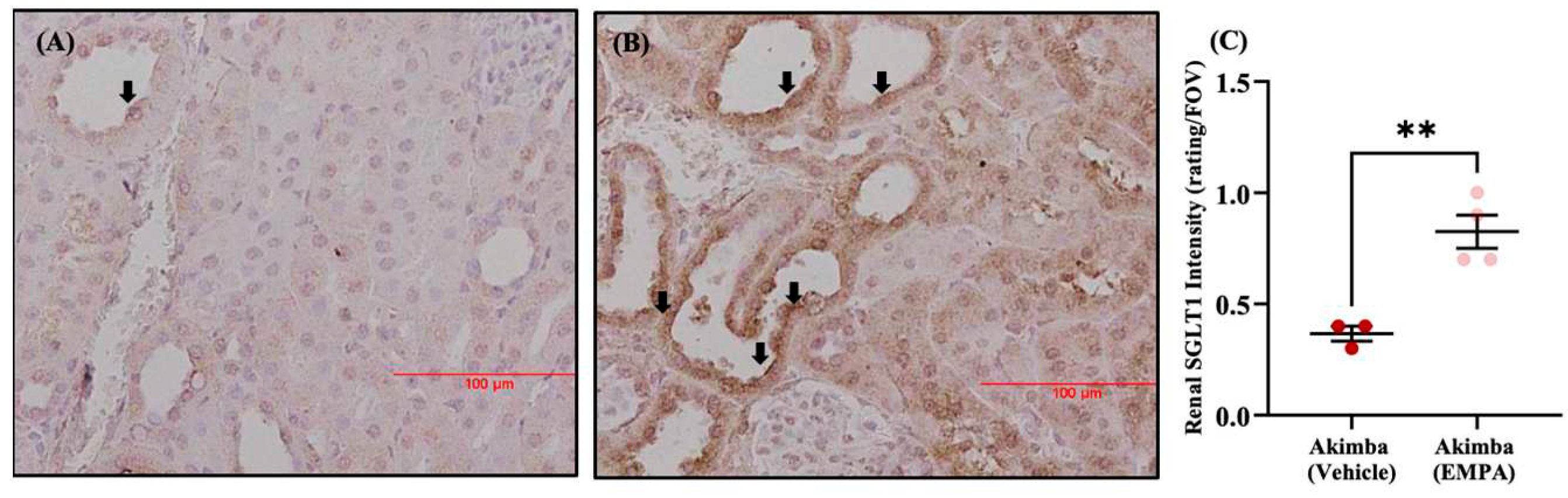
Figure 5.
Cardiorenal benefits of Sodium-Glucose Cotransporter 2 (SGLT2) inhibitors and proposed effects on SGLT1 activity. Sodium-Glucose Cotransporter 2; SGLT2, Sodium-Glucose Cotransporter 1; SGLT1, Empagliflozin’; EMPA, Dapagliflozin’; DAPA, Canagliflozin; CANA, CV; Cardiovascular, HF; heart failure and MI; myocardial infarction.
Figure 5.
Cardiorenal benefits of Sodium-Glucose Cotransporter 2 (SGLT2) inhibitors and proposed effects on SGLT1 activity. Sodium-Glucose Cotransporter 2; SGLT2, Sodium-Glucose Cotransporter 1; SGLT1, Empagliflozin’; EMPA, Dapagliflozin’; DAPA, Canagliflozin; CANA, CV; Cardiovascular, HF; heart failure and MI; myocardial infarction.
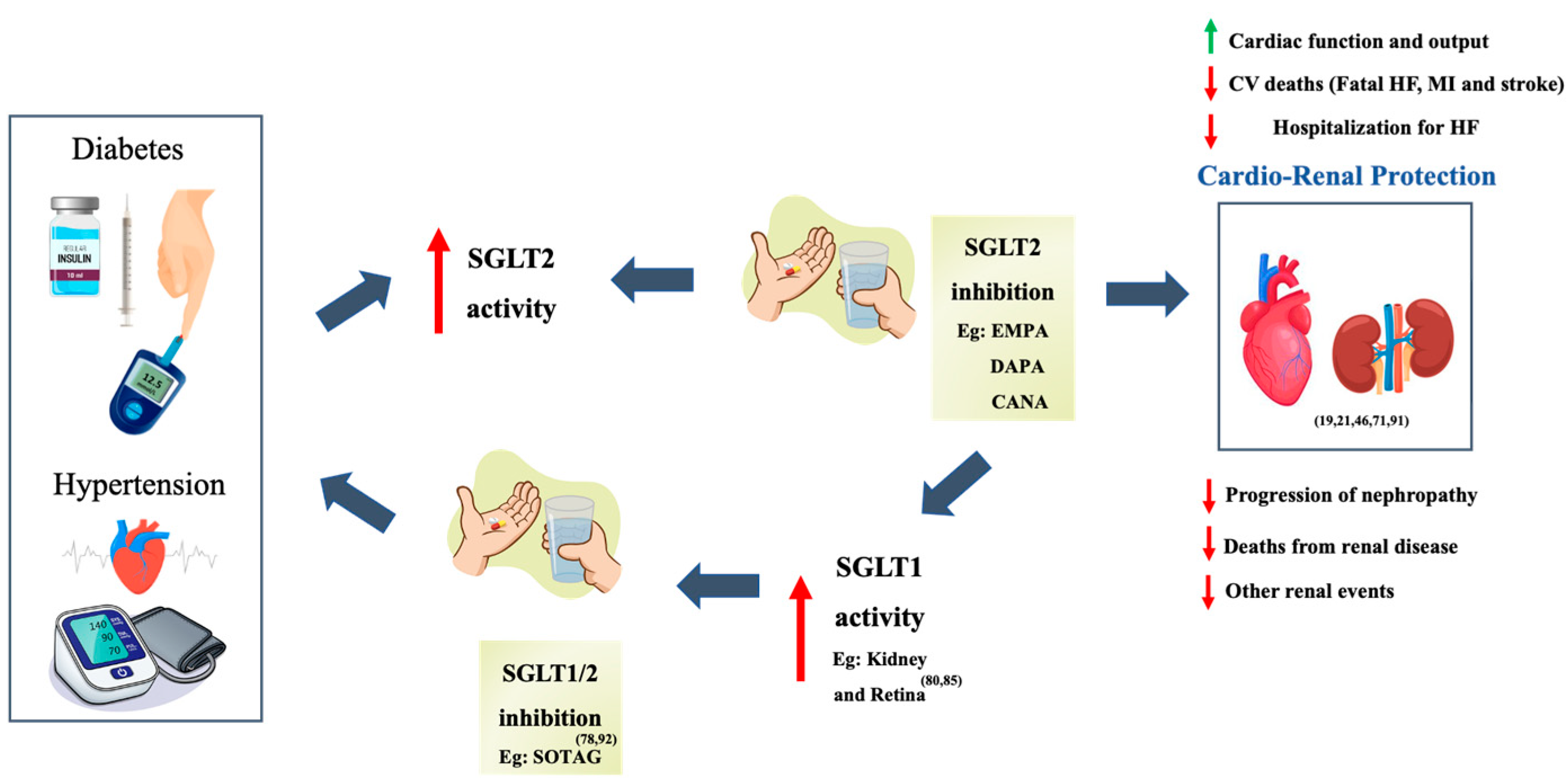

Table 1.
Areas of expression of SGLT1 and SGLT2 in the human body.
| Location | SGLT1 | SGLT2 |
|---|---|---|
| Small Intestine | Apical membrane, K and L cells (26). | Not expressed. |
| Eye | Retina (27). | Retina, cornea and lens (27). |
| Kidney | Section 3 of the proximal tubule. (15). | Section 1 and 2 of the proximal tubules (16). |
| Pancreas | Pancreatic alpha cells (25). | Not expressed. |
| Liver | Biliary duct cells (26). | Not expressed. |
| Heart | Capillaries (26). | Not expressed. |
Table 2.
Summary of key findings from the characterisation of Canagliflozin (CANA), Dapagliflozin (DAPA), Ipragliflozin, Empagliflozin (EMPA), Tofogliflozin and Luseogliflozin [28,29,30].
| Study Parameters | Key Findings |
|---|---|
|
Pharmacokinetic properties |
Longest plasma half-life: canagliflozin. |
| Longest half-life in the kidney: dapagliflozin. | |
| Highest distribution in the kidney: ipragliflozin. | |
| Drug distribution in the kidney suggested to be dependent on chemical structure. | |
|
Pharmacodynamic properties |
All SGLT2i’s increased urinary glucose excretion in dose-dependent manner. |
| Long-acting SGLT2i exhibited persistent action even after 18h post-dose. | |
| Close correlation between the duration of action, plasma drug concentration, drug distribution and kidney retention. | |
|
Pharmacologic properties |
Significant reductions in blood glucose and plasma insulin with all SGLT2i. |
| Significant improvement in glucose tolerance with all SGLT2i. | |
| Long-acting SGLT2i’s exert stronger anti-hyperglycaemic effects through persistent urine glucose excretion. | |
| Intermediate-acting SGLT2i may provide better glycaemic control when administered twice daily. | |
|
Anti-diabetic effects |
All SGLT2i significantly improved hyperglycaemia and hyperinsulinemia. |
| All SGLT2i significantly increased pancreatic insulin content by prevention of pancreatic exhaustion. | |
| Long-acting SGLT2i exert favourable glycaemic control over 24 hours and may have slightly enhanced anti-diabetic effects as compared to intermediate-acting SGLT2i. | |
|
Effects on diabetic complications |
All SGLT2i’s exhibited significant improvements/trends in obesity parameters (e.g. body and visceral fat weights, lipid metabolism markers), pro-inflammatory cytokines and endothelial dysfunction markers. |
| All SGLT2i’s significantly decreased or showed a decreasing trend in steatohepatitis parameters (e.g. liver weight, plasma levels of liver enzymes) and renal parameters (e.g. creatinine clearance, renal tubular injury markers). | |
| Long-acting SGLT2i (0.3 mg/kg) demonstrated slight superiority in comparison to intermediate-acting SGLT2i (3mg/kg) on several parameters (e.g. daily blood glucose control, visceral fat weight). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



