
Submitted:
17 August 2023
Posted:
21 August 2023
You are already at the latest version
Abstract
The emergence of drug-resistant strains of M. tuberculosis (Mtb) and the phenomenon of phe-notypic tolerance to drugs challenge the goal of tuberculosis (TB) elimination worldwide. By using the ex vivo cultures of alveolar macrophages obtained from lung tissues of TB patients after intensive antimicrobial chemotherapy before surgery, different subpopulations of multi-drug-tolerant Mtb with a spectrum of phenotypic and growth features were identified in the same TB lesions. Our results indicative of not only passive mechanisms generating nonheritable resistance of Mtb to antibiotics, which are associated mainly with a lack of Mtb growth, but also some active mechanisms of Mtb persistence, such as cell wall and metabolic pathway remod-eling. In one of the subpopulations, non-acid-fast Mtb have undergone significant repro-gramming with the restoration of acid-fastness, lipoarabinomannan expression and replication in host cells of some patients after withdrawal of anti-TB drugs. Our data indicate the universal stress protein Rv2623 as a clinically relevant biomarker of Mtb that have lost acid-fastness in human lungs. The studies of Mtb persistence, dormancy, and resumption and the identification of biomarkers characterizing these phenomena are very important to develop vaccines and drug regimens with the individualized management of patients for overcoming the re-sistance/tolerance crisis in anti-TB therapy.
Keywords:
pulmonary tuberculosis
; Mycobacterium tuberculosis
; alveolar macrophages
; drug tolerance
; persistence
; dormancy
; biomarkers
; non-acid-fastness
; Rv2623
1. Introduction
Tuberculosis (TB) is caused by the pathogen Mycobacterium tuberculosis (Mtb) and remains to be the leading bacterial cause of death in the world [1]. Today, the global TB eradication is compromised by an increasingly rapid spread of multidrug resistant (MDR) and extensively drug resistant (XDR) TB, which need to be treated with complex combinations of drugs for an extremely prolonged stretch of time, while no cure is often achieved [2,3,4,5]. The pathogen can become tolerant to antibiotics as a result of drug-resistant mutations in the Mtb genes that confer resistance, which is both irreversible and heritable [6,7,8]. Another possible cause of TB treatment failure is transient drug tolerance in Mtb which is not associated with genomic changes and is defined as phenotypic resistance or persistence [9,10,11,12]. Persistence is the ability of microorganisms to survive prolonged exposure to drugs to which they are fully susceptible, which is thought to be related to the specific physiological states of Mtb [13,14,15]. It is believed that the development of persistent Mtb in hostile microenvironments, for example, within macrophages or inside granulomatous tissue lesions, is a major barrier to the timely and relapse-free treatment of human TB disease because the current TB drug regimen poorly addresses this pathogen [16,17,18,19].
It is assumed that persistent Mtb constitute a reservoir of slow-growing or growth-arrested bacteria, in which many antibiotic target sites are inactive, thereby explaining the ineffectiveness of bactericidal antibiotics [20,21,22]. Several observations correlate the physiological state of the pathogen with dormancy, which is usually associated with the inability of Mtb to grow on solid media, its reduced metabolic and growth rates, resulting from alteration of gene expression, and tolerance to antibiotics owing to lack of replication and cell wall remodeling [23,24,25].
In laboratory practice, the “dormancy” phenotype of Mtb can be induced by different environmental stresses including starvation, hypoxia, oxidative stress, interaction of pathogen with their host, exposure to antibiotics, and multiple combinations of these [17,26]. Multiple experimental models have been developed to study the persistent/dormant population of Mtb, including long-term stationary phase cultures, the Wayne model, the Cornell murine and other animal models, single-cell level studies using microfluidics and time-lapse microscopy, to name some (reviewed in [16,21,26,27,28]). While the characterization of Mtb and other mycobacterial species in these models has discovered some mechanisms by which persistent Mtb emerge and revealed in them the physiological changes that form the basis for their dormancy and multidrug tolerance, no apparent marker of dormant Mtb has been identified yet [12,22,25,28,29,30]. Also, it is impossible to determine which of the Mtb states in the experimental assays is relevant to human TB disease, where complex interactions between the patient, pathogen, pathological and pharmacological (in the context of antibiotic therapy) factors exist in the specific conditions of the development of Mtb infection [31,32]. Defining the cell state of Mtb in the human TB disease is hindered by the lack of available experimental methods to investigate Mtb persistence and dormancy in the patients’ tissues, primarily of the lungs, since Mtb is mainly spread through aerosols and engulfed by alveolar macrophages.
For a deeper understanding of the molecular and cellular biology of Mtb and the mechanisms of their survival in the lung tissues of TB patients, we have developed a technique to produce ex vivo cell cultures, mainly of alveolar macrophages, from the lung parts surgically removed from patients with pulmonary TB [33]. As we found in one of our previous works, when replicating bacteria line up along their longitudinal axes in a close parallel arrangement and set themselves into “braids” or “ropes”, Mtb cords are revealed in the patients’ alveolar macrophages, and these cords are associated with increased Mtb virulence in the guinea pig model of TB disease [34]. We have also found that Mtb with different virulence, occurring solitary and as colonies, with or without cording morphology, are exclusively intravacuolar pathogens with intact phagosomal membranes in the viable host cells of TB patients [35]. In a special study, we indicated that the Mtb-infected alveolar macrophages in the ex vivo cell cultures were isolated from TB patients’ lung tissues and were not the result of Mtb uptake after ex vivo expansion [36]. We identified not only cavity walls, but also tuberculoma walls with insufficient inflammation and excessive fibrosis as being the main niches for Mtb survival in alveolar macrophages among the patients’ lung TB lesions examined [37]. While some Mtb were found in the colonies, including those with cording morphology, the growth potential of Mtb in the alveolar macrophages of TB patients at the time of surgery and ex vivo expansion of cells remained unknown.
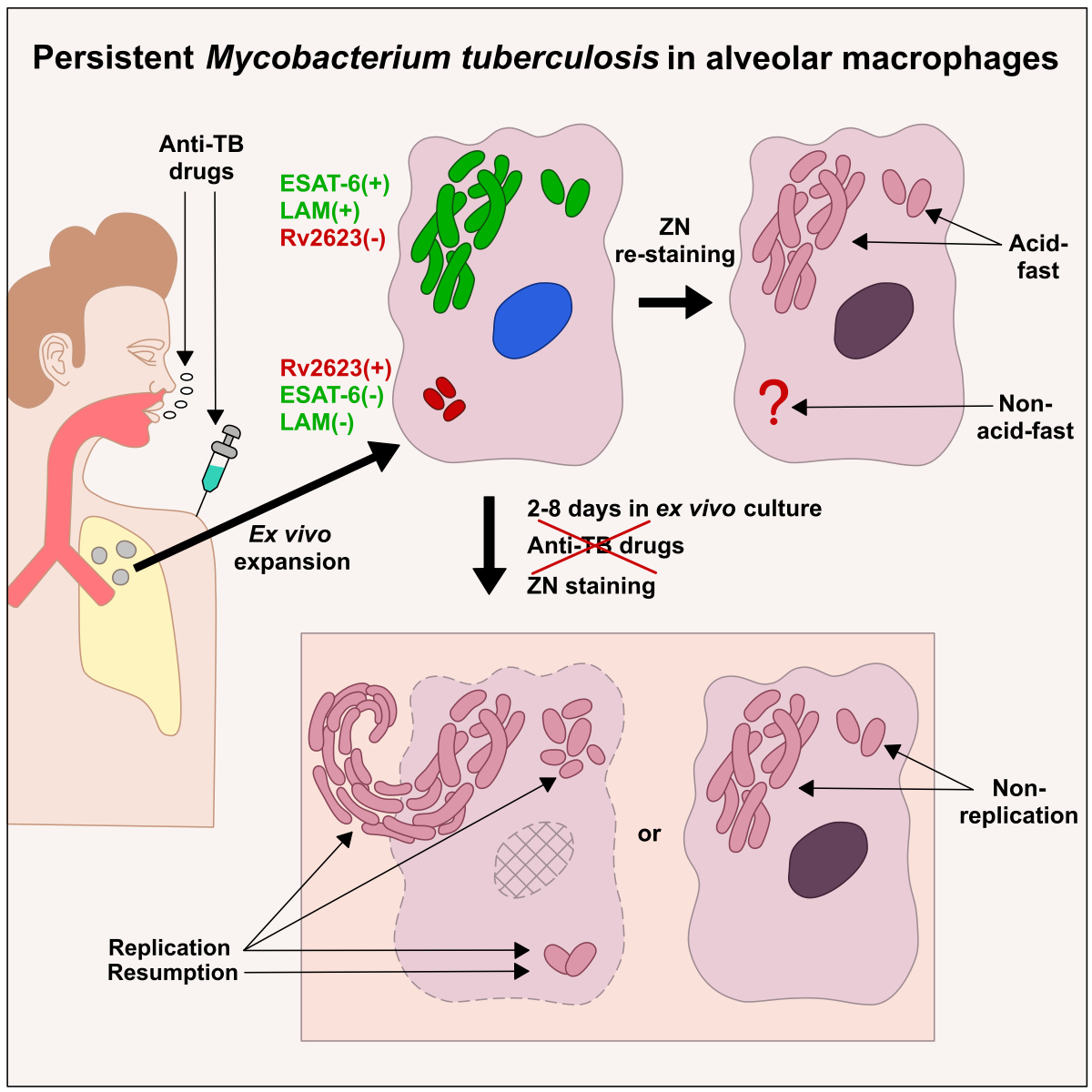
In this study, we used prolonged ex vivo cultures of alveolar macrophages obtained from the lung lesions of patients with pulmonary TB to understand the mechanisms underlying Mtb survival in host cells under an intensive antimicrobial chemotherapy before surgery. We have identified persistent Mtb infection in the patients’ lungs, where the different subpopulations of multidrug-tolerant Mtb that exhibited a spectrum of phenotypic and growth characteristics coexisted in the same lesions. The Mtb were able to resume growth quickly, especially when in colonies with cording morphology, in the cells of some patients in a long-term ex vivo culture under antibiotic-free conditions. Shortly after that resumption, non-acid-fast Mtb from one of the subpopulations underwent considerable reprogramming with the restoration of their acid-fastness, expression of glycolipid lipoarabinomannan (LAM) in the cell envelope and active replication in the alveolar macrophages of some patients. We have also found Mtb expressing the universal stress protein domain-containing protein Rv2623 from the dormancy survival regulator (DosR)-dependent regulon, which had an acid-fast-negative phenotype and none of the virulence factors LAM or 6-kDa early secretory antigenic target (ESAT-6) protein expression in the alveolar macrophages of all patients. Rv2623 protein expression may be used as a clinically relevant biomarker of the Mtb that have lost acid-fastness – and so may the Mtb dynamics in the prolonged ex vivo cell cultures be as a biomarker of the growth status and physiological state of the pathogen in the host cells of TB patients at the time of surgery and, supposedly, a hallmark of infection relapse after the cessation of the antibiotic treatment.
2. Results
2.1. Nonheritable persistence of Mtb in alveolar macrophages is the main culprit of treatment failure in TB patients
2.1.1. Mtb-infected alveolar macrophages are determined for all the patients after an intensive anti-TB chemotherapy
To determine the pathways of Mtb survival in the lungs of patients with pulmonary TB, we simultaneously studied Mtb infection in alveolar macrophages (1) in the ex vivo cell cultures obtained previously from surgically removed lung TB lesions, such as cavity (cav) wall (patient 6) and tuberculoma (tub) walls (patients 24, 25, and 27–29), and the lung tissues distant from the cavities and tuberculomas (dist or without labeling, ‘distant lung tissue samples’ throughout) for patients 1–5 and 7–29 [33,35,36,37], and (2) on the histological sections obtained from the same lung specimens. Patients 4, 15, 23, 28, and 29 had been treated with the first-line anti-TB drugs isoniazid, rifampicin, ethambutol, and pyrazinamide before surgery (Table 1). The treatment of the other patients involved the use of complex combinations of antibiotics, including the first-line anti-TB drugs, especially pyrazinamide, and the second-line anti-TB drugs fluoroquinolones (ofloxacin or levofloxacin), cycloserine, rifabutin, prothionamide, para-aminosalicylic acid, and injectable antibiotics (capreomycin and aminoglycosides, such as amikacin and kanamycin). The acid-fast Mtb, as solitary and in colonies, with cording morphology or as irregular clumps, positive for the LAM, ESAT-6, and the cell wall 38-kDa phosphate binding glycoprotein PstS-1 (Ag38) expression, were found in some alveolar macrophages (‘infected alveolar macrophages’ throughout) both after ex vivo culture for 16–18 hours and on the histological sections for all the patients studied (Figure 1a-d). The Mtb clinical isolates grown on dense Löwenstein-Jensen (L-J) medium were only from the resected lung tissues of patients 6, 8, 10, 11, and 20 (Table 1); however, a substantial number of infected alveolar macrophages (out of the total number of the cells examined, >1% were the host cells with Mtb) was determined in the ex vivo cell cultures of patients 3, 5, 9, and 24 (tub) (Figure 1B).
Thus, Mtb were able to survive a large number of bactericidal antibiotics that had been given to the patients in a clinical setting for a long time and had different abilities to grow, i.e., to activate cell division, on a dense medium after surgery.
2.1.2. Mtb are genetically susceptible to the many antibiotics used in clinical settings
When antimicrobial treatment fails, Mtb often become resistant to antibiotics due to mutations in their genes implicated in drug resistance [4,8,38]. Genetic analysis revealed (1) heterogeneity in the presence/absence of mutations to the Mtb genes associated with resistance to isoniazid (katG, inhA), rifampicin (rpoB), ethambutol (embB), fluoroquinolones (gyrA), capreomycin and aminoglycosides (rrs, eis) and (2) variation in the number of Mtb genes affected by these mutations among the patients regardless of the duration of intensive anti-TB chemotherapy before surgery (Table 1). At the same time, although patients 4, 13, and 29 with the wild-type resistance-associated genes in Mtb DNA treated with the first-line anti-TB drugs, including the essential antibiotics isoniazid and rifampicin, and the therapy for patients 2, 8, and 14 with the wild-type rpoB gene in Mtb DNA involved rifampicin or rifabutin in combination with other antibiotics, the alveolar macrophages of these patients were found to be infected with Mtb (Figure 1b-d). Also, although the wild-type gyrA, rrs and eis genes were present in Mtb DNA of most patients and the treatment regimens included fluoroquinolones for patients 21, 24, 25, and 27, capreomycin/aminoglycosides for patients 2, 3, 5, 7, 11, 12, and 19, and a combination of these antibiotics for patients 1, 16, 22, and 26, these patients’ alveolar macrophages were found to be infected with this pathogen. A similar situation was observed for patients 4–6, 8, 14, 21, 22, and 29 with the wild-type embB gene in Mtb DNA following treatment with ethambutol.
Thus, Mtb that survived drug attacks in alveolar macrophages are likely to be genetically susceptible to the many antibiotics that were used in the treatment of most patients before surgery.
2.1.3. Mtb survive in alveolar macrophages after exposure to bactericidal antibiotics in a long-term ex vivo culture
Treatment failure may also be associated with the inability of effective anti-TB drugs to penetrate lung TB lesions and achieve adequate antimicrobial concentrations at infection sites in human tissues, where the pathogen resides [38,39]. This situation prompted us to estimate the efficacy of Mtb killing in the ex vivo cell cultures of patients 10, 14, and 15 after three-day exposure to three concentrations of the standard-of-care anti-TB drugs isoniazid (1, 5, and 10 µg/ml), rifampicin (40, 60, and 80 µg/ml), ofloxacin (2, 5, and 10 µg/ml), kanamycin (30, 40, and 50 µg/ml) or capreomycin (30, 40, and 50 µg/ml). The concentrations of these bactericidal antibiotics, which target different pathways of the Mtb biogenesis [40], corresponded to the critical, intermediate, and maximum doses used to test Mtb tolerance under antibiotic pressure on L-J medium in laboratory settings [41]. Furthermore, we assessed the Mtb load in the alveolar macrophages of patients 16–19 exposed only to the critical concentrations of isoniazid (1 µg/ml) and ofloxacin (2 µg/ml) under the same conditions.
At all concentration tested, acid-fast Mtb, as solitary and in colonies, including those with cording morphology, were revealed in living alveolar macrophages without apoptotic or necrotic morphology for all the patients (Figure 1c, Figure S1a,b), while Mtb with heritable resistance to the antibiotics used were found only in patient 10 (Table 1). In our analysis, the number of infected alveolar macrophages often did not differ substantially between the drug-treated cell cultures—even those exposed to the maximum concentrations—and the untreated controls analyzed simultaneously on day 5 (D5) or 6 (D6) after ex vivo expansion of alveolar macrophages. This result was up to expectation for the isoniazid-treated alveolar macrophages of patients 10, 14–19 and rifampicin-treated alveolar macrophages of patients 10, 15 due to the presence of the resistance-associated mutations in the katG and rpoB genes in Mtb DNA, respectively. However, bactericidal activity was low in the alveolar macrophages of patients 14 and 15 after exposure to other antibiotics and in the ex vivo cell cultures of patients 16, 17, and 19 exposed to ofloxacin: although the pathogen was susceptible to these antibiotics (Table 1), it showed phenotypic resistance to them. A notable reduction in the number of infected alveolar macrophages was detected only for patient 18 after exposure to ofloxacin.
Taken together, our data suggest that although Mtb remain genetically susceptible to most anti-TB drugs that were used for intensive antimicrobial therapy before surgery, they develop phenotypic multidrug tolerance or persistence to antibiotic treatment and, therefore, represent the population of bacteria that persist in alveolar macrophages for an extended period of time.
2.2. Mtb resume active growth in the alveolar macrophages of some patients in the prolonged ex vivo cell cultures after withdrawal of anti-TB drugs
Growth arrest is regarded as the main hypothesis to explain the persistence of Mtb, because the physiological state of non-replication renders bacteria drug insensitive owing to a low target activity [8,13,29]. To assess the growth status of the pathogen (those capable of replicating to be tagged as ‘replicating’, and those incapable of replicating and only surviving in colonies, including those with cording morphology, to be tagged as ‘non-replicating’) at the time of surgery, we analyzed the Mtb loads in the patients’ alveolar macrophages stained by the Ziehl-Neelsen (ZN) method after a long-term ex vivo culture under antibiotic-free conditions on days 2, 3 and 4 (D2–D4) and/or on each of days 5–8 (D5-D8) after ex vivo expansion of alveolar macrophages (Figure 1b-d).
In the prolonged ex vivo cell cultures, we observed a gradual increase in the number of alveolar macrophages with increased Mtb loads in them for patients 4, 6 (cav), 7–10, 14, 18, 24 (tub), and 27 (tub) (Figure 1b-d). Also, an increased number of host cells containing upward of 10 Mtb, predominantly in colonies with cording morphology or in colonies occurring as irregular clumps, was detected simultaneously with a decrease in the number of alveolar macrophages containing from 3 to 9 Mtb in each of most of these patients (Figure 1d). For the alveolar macrophages of patient 6 (cav), increased replication rates of Mtb in colonies with cording morphology resulted in the disruption of some host cells with morphological signs of necrotic cell death (nucleus-free cells, chromatolysis, compromised cytoplasmic membranes and leakage of cell components) and the extracellular formation of large braids or cords with more than 40 acid-fast and LAM-positive Mtb in each of them on day 6 (D6) of ex vivo culture (Figure 2a, b).
Some increase in the number of alveolar macrophages with Mtb appearing in the form of colonies, whether as irregular clumps or with cording morphology, were observed in the prolonged ex vivo cell cultures for patients 2, 20, 22, 23, and 26; however, the Mtb load in host cells did not increase over time for the other patients, including 24 (dist) and 27 (dist), thereby indicating a very slow division rate and/or the absence of Mtb replication in the alveolar macrophages (Figure 1b). Therefore, the Mtb colonies, including those with cording morphology for patients 3, 19, 22, and 26, were likely to have been formed in the patients’ host cells long before surgery. This assumption was confirmed by the absence of TB lesions and symptoms of TB disease in the guinea pigs infected with the lung tissue inoculums of patient 19 with a large number of Mtb colonies with cording morphology in them [34].
Thus, our data indicate that persistent Mtb are able to resume active growth in the alveolar macrophages of some patients during the first days in a long-term ex vivo culture under antibiotic-free conditions and then to destroy host cells containing cords with numerous actively replicating Mtb in them.
2.3. Acid-fast and LAM-positive Mtb with an atypical morphology appear in the alveolar macrophages of some patients in a long-term ex vivo culture under antibiotic-free conditions
In the prolonged ex vivo cell cultures of patients 4, 7–9, 18, 20, and 27 (tub), the number of infected alveolar macrophages increased about two- to six-fold from hours 16-18 to D5-D6 of ex vivo culture under antibiotic-free conditions (Figure 1b, c). We also detected some increase in the number of infected alveolar macrophages in the prolonged ex vivo cell cultures of patients 2, 6 (cav), 10, 13, 14, 23, and 24 (tub). To our surprise, a substantial increase in the number of alveolar macrophages with one Mtb bacterium in each was revealed in the prolonged ex vivo cell cultures of patients 4, 14, and 24 (tub). Additionally, no change in the number of alveolar macrophages with one Mtb bacterium in each was observed for patients 6 (cav), 7, 8, 18 and 27 (tub) after a long-term ex vivo culture (Figure 1d), even though we expected a substantial decrease, because active Mtb replication was observed in the alveolar macrophages of these patients.
Moreover, in the alveolar macrophages of patient 6 (cav), we detected shorter rod-shaped Mtb from 0.7 to 2.1 μm in size (the mean being 1.4 ± 0.1 μm, n = 40), on D3 of ex vivo culture, while some earlier, after ex vivo culture for 18 hours, only long filamentous Mtb from 3.8 to 7.5 μm in size (the mean being 6.6 ± 0.3 μm, n = 40) had been observed (P < 0.001, Figure 2a, c, d). We also detected alveolar macrophages with shorter acid-fast or LAM-positive rod-shaped Mtb appearing as clusters of two or more bacteria, including those paired in a V-shaped manner, in viable host cells with or without filamentous Mtb, whether solitary or in colonies with cording morphology, in them (Figure 2a, c, d). The V-shape of an Mtb colony is known to characterize the late stages of Mtb cell division [42,43]. For the other patients, we did not notice such striking differences in the shape or size of the Mtb re-established in the host cells over the period of observation, because Mtb with a different morphology – filamentous/elongated rod-shaped Mtb in colonies with cording morphology and shorter rod-shaped Mtb, solitary and as irregular clumps – were detected in alveolar macrophages after ex vivo culture for 16-18 hours (Figure 1a).
Given our data, we hypothesized that the re-established acid-fast and LAM-positive Mtb that could not be detected in alveolar macrophages by traditional analyses, including the ZN method and immunofluorescent staining for virulence factors of the pathogen, after ex vivo culture for 16-18 hours could nevertheless re-establish in the prolonged ex vivo cell cultures of some patients after withdrawal of anti-TB drugs and other environmental stresses, such as hypoxia or nutrient deficiency. We called the phenomenon of a sudden appearance of the acid-fast pathogen expressing virulence factors in alveolar macrophages, where it had not been previously detected by traditional methods, “Mtb resumption”.
Thus, analysis of the patients’ alveolar macrophages after a long-term ex vivo culture under antibiotic-free conditions allows us not only to ascertain the Mtb growth status and ability to quickly resume division in host cells, but also to detect the resumption of acid-fast and LAM-positive Mtb in them. Therefore, Mtb dynamics can serve as a biomarker of both active and inactive physiological states of the pathogen in the patients’ lungs at the time of surgery. Additionally, this analysis allows us to make predictions about possible increased risks of Mtb infection in patients after cessation of anti-TB chemotherapy.
2.4. Mtb within and outside alveolar macrophages of TB patients are devoid of lipophilic inclusions
As “… the term dormancy should only apply to bacterial cells and specifically those that are capable of regrowth: it should be a reversible phenomenon…” in [25] (p. 139), we suggested that the re-established Mtb could belong to the subpopulation of dormant bacteria that survived exposure to antibiotics and other environmental stresses in a specific phenotypical state in the patients’ alveolar macrophages. Although Mtb with lipophilic inclusions in them have been studied only in late stationary phase cultures and some human sputum samples after Auramine-Nile red labeling [44,45], the presence of lipophilic inclusions in Mtb is supposed to be a sign of their dormancy phenotype [25,44,45,46].
In our work, the lipophilic inclusions in Mtb were examined with use of the LAM or ESAT-6 immunofluorescent and Nile red dual-staining for detection of the pathogen and lipids, respectively, in the ex vivo cell cultures of the patients. Although we have previously detected foamy and lipid-rich alveolar macrophages that contained a large amount of lipid droplets in them both in the ex vivo cell cultures and on the histological sections for some patients [35,36], none was detected in the cytoplasm of filamentous or shorter rod-shaped Mtb within and outside alveolar macrophages of the patients after ex vivo culture for 16-18 hours (Figure S2). The ESAT-6-positive Mtb did not produce intracellular lipophilic inclusions in the alveolar macrophages of the Mtb-infected guinea pig with clinical signs of TB disease, either (see Figure S6B in [35]). On the other hand, we did not observe any Nile red-positive Mtb not expressing the virulence factors LAM and ESAT-6.
Thus, the absence of lipophilic inclusions in the cytoplasm of Mtb did not allow us to use this marker as a means to ascertain the dormant state of the pathogen in the patients’ alveolar macrophages. Therefore, other biomarkers are needed.
2.5. Rv2623-positive Mtb are detected only in stationary phase cultures, but not in exponential phase cultures of Mtb Beijing clinical isolates
The induction of Mtb persistence and dormancy is believed to be accompanied by global changes in gene expression due to activation of stress response regulatory mechanisms, including the DosR two-component system with the DosR-dependent regulon composed of more than 50 genes [24,28,47]. Some of these genes, for example, dosR, Rv3130c, hspX (acr), fdxA, and narX, were found to be constitutively overexpressed in Mtb clinical isolates belonging to the Beijing genotype family [48]. In our work, the Mtb DNA from the resected lung tissues belonged to the Beijing lineage for most patients, excluding patients 3 and 4 [34,35,36]. Therefore, we decided to study the expression of another DosR regulon protein known as the universal stress protein Rv2623, because their usp (rv2623) gene was among the most highly induced genes of mycobacteria, including Mtb, in various experimental models, such as hypoxia [49,50], in vitro infection of mouse and human macrophages [51], and chronical infection in the mouse lungs [52]. As was noted in some models, Rv2623 expression can contribute to the restriction of Mtb replication, activation of the dormancy-signaling pathway and the induction of Mtb persistence in host cells [53,54].
Originally, we analyzed the expression of the Mtb markers LAM, Ag38, and Rv2623 in the stationary phase cultures of high- and low-virulence Mtb clinical isolates obtained from the resected lung tissues of patients 6, 8, 10, 20 and 11, respectively, all in the Beijing genotype family [33,34]. After 3 months of Mtb incubation (D90) on dense L-J medium under standard conditions, we observed the rise of non-acid-fast Mtb in bacterial spots obtained from the cultures of all Mtb clinical isolates (Figure 3). In an immunofluorescence assay with dual-staining of Mtb, we identified four types of expression of the Mtb markers in the total population, where some Mtb expressed the following markers at once: (1) LAM and Ag38, (2) Ag38 and LAM, with the former prevailing, (3) LAM and Rv2623, with the former prevailing, and (4) Rv2623 alone (Figure 3). These types of Mtb marker expression were determined in the stationary phase cultures of all Mtb clinical isolates, with LAM/Ag38-positive Mtb being prevalent. Rv2623-positive Mtb with the normal rod-shaped morphology made up approximately 10% of the bacteria in stationary phase cultures of the Mtb clinical isolates examined.
After analysis of Mtb in stationary phase cultures, some Mtb from these cultures were replated onto fresh L-J medium under standard conditions. On day 20 (D20) after replating, we revealed only more elongated rod-shaped acid-fast Mtb, with LAM and Ag38 expressing in exponential phase cultures, where no Rv2623-positive Mtb were observed (Figure 3). The correlation between Rv2623 expression and a long-term survival of Mtb in stationary phase cultures under nutrient-limited conditions indicated a possible association of this marker with the stress-induced dormancy response of the pathogen.
Thus, we hypothesized that the expression of Rv2623 protein may be used as a marker of the dormant state of Mtb, including Beijing family strains, in the alveolar macrophages of TB patients.
2.6. Rv2623-positive Mtb not expressing the virulence factors LAM and ESAT-6 are identified in the alveolar macrophages of all the patients studied
Using an immunofluorescence assay with dual-staining of Mtb, we analyzed the expression of two combinations of Mtb markers at once – LAM and Rv2623 or ESAT-6 and Rv2623 – in the pathogen in the alveolar macrophages of patients 5 and 10–29 after ex vivo culture for 16-18 hours and, in parallel, on the histological sections. Of note, each of the virulence factors LAM and ESAT-6 was targeted using the polyclonal antiserum normally recognizing multiple epitopes of the Mtb antigens. As a result, we detected LAM- and ESAT-6-positive Mtb not expressing Rv2623 protein and, vice versa, Rv2623-positive Mtb not expressing the virulence factors LAM and ESAT-6 in the alveolar macrophages on the cytological and histological preparations and in the caseous center of tuberculomas and small granulomas on the histological sections (Figure 4a, Figure S3a,b). Rv2623-positive rod-shaped Mtb were found to occur as solitary and in clusters of two or more bacteria, including V-shaped pairs, but not as colonies with cording morphology, where only LAM- or ESAT-6-positive filamentous Mtb were discerned (Figure 4a, c, Figure S3b). We did not notice substantial differences in the size of most rod-shaped Mtb, solitary or in colonies as irregular clumps, expressing distinct Mtb markers, although the Rv2623-positive Mtb were overall shorter. We did not observe LAM- or ESAT-6- and Rv2623-positive Mtb at once in the same alveolar macrophages in ex vivo culture, while such host cells were identified on the histological sections (for example, patient 24 (tub) in Figure 4a). At the same time, these Mtb markers were often detected as occurring together in the same intracellular granules of some alveolar macrophages, along with or without the marker-positive Mtb in them, on the histological sections and in the ex vivo cell cultures of the patients (Figure S3c).
The number of alveolar macrophages with Rv2623-positive Mtb in them ranged from about 10% to almost 50% of host cells between the patients and their lung TB lesions (Figure S3a). Furthermore, since the data obtained for the majority of the patients after ex vivo culture for 16-18 hours were in a good agreement with histological data, we compared only histological data obtained for the patients’ lung specimens divided into four groups (Figure 4b). The compilation of these groups was based on an anatomical and a histological examination of the patients’ lung TB lesions with the assessment of the extent of fibrosis coupled with activation of stress factors (see the table below the graph in Figure 4b), such as the synthesis of the master pro-inflammatory transcriptional regulator nuclear factor-kappa B (NF-κB), the enzyme inducible nitric oxide synthase (iNOS), resulting in the production of nitric oxide, and cyclooxygenase 2 (COX-2), and the production of reactive oxygen species (ROS), which, for the most patients studied, were assessed in some of our previous works [35,37]. The hostile stresses, especially low oxygen tension and high nitric oxide, are considered to activate the DosR-dependent regulon in Mtb, this activation including the upregulation of the Rv2623 protein expression (reviewed in [28]). The lung specimens of the “tuberculomas” group were characterized by excessive fibrosis and insufficient inflammation with a lack of generation of stress factors in the tuberculoma walls of patients 22 and 24–29 (n=7). For the distant lung TB tissues, the specimens of patients 5, 10, 22, and 23 (n=4) with extensive fibrosis and the reduced activation of stress factors in alveolar macrophages were included to the “type 1” group. The lung samples of patients 14 and 24–26 (n=4) with focal fibrosis and patients 15 and 27–29 (n=4) with minimal signs of fibrosis were assigned to the “type II” and “type III” groups, respectively. In the latter groups, a higher level of pro-inflammatory and microbicidal factors was identified in alveolar macrophages. Although TB lesions of all the groups had different morphological characteristics and hostile environments, they displayed approximately identical Rv2623-positive Mtb (solitary or as colonies) loads in the alveolar macrophages, for each group, about a third of host cells were infected (Figure 4b). Changes in the parameters tested between the groups failed to reach statistical significance. Also, some places with Rv2623-positive Mtb in them were detected in the caseous center of tuberculomas for patients 22 and 24–26 (n=4), when half of these places had colonies of Rv2623-positive Mtb (Figure 4b, Figure S3b).
Rv2623-positive Mtb, solitary or in colonies, excluding those with cording morphology, were also found in the alveolar macrophages of patients 1–4 and 6 (cav) after ex vivo culture for 16-18 hours (Figure 4c). At the same time, no lipophilic inclusions were detected in the cytoplasm of Rv2623-positive rod-shaped Mtb, solitary or in colonies as irregular clumps, or Rv2623-negative filamentous Mtb in colonies with cording morphology on the same cytological preparations for these patients (Figure 4c).
The examination of the pathogen on the histological sections of the resected lung tissues of patients 32 and 33, who had not been given anti-TB treatment before surgery, revealed Rv2623-positive Mtb, solitary and in colonies as irregular clumps, in both alveolar macrophages and the caseum of the tuberculoma walls and, in parallel, the distant lung tissue parts (Figure S4). Rv2623-positive Mtb did not express the virulence factors LAM and ESAT-6 or intracellular lipophilic inclusions, either. Of note, Rv2623-positive Mtb did not colocalize with filamentous actin in the alveolar macrophages (Figure S4). The numbers of the patients’ alveolar macrophages with Rv2623-positive Mtb in them, as well as the Mtb loads analyzed on the histological sections by the ZN method, were compared with the data obtained from the histological sections for the other patients after intensive antimicrobial chemotherapy before surgery (data not shown).
Thus, Rv2623-positive Mtb, mainly belonging to the Beijing genotype family, are revealed in alveolar macrophages and necrotic caseum in the lung tissues of all the patients studied, regardless of the type of TB lesions or environmental niches for Mtb survival, and the courses of intensive anti-TB therapy with various sets of antibiotics or without any anti-TB treatment before surgery. No expression of the virulence factors LAM and ESAT-6 is detected in any of the Rv2623-positive Mtb.
2.7. Rv2623-positive Mtb are acid-fast-negative in the alveolar macrophages of patients and guinea pig with TB disease
Remodeling the cell envelope composition in Mtb is expected to lead to alterations in cell wall permeability [55,56] and to an acid-fast-negative phenotype of the pathogen that is not resistant to decolorization by acid alcohol solutions in the ZN method. These characteristics are thought to be associated with the dormant state of Mtb during pathogen survival in the experimental models of TB infection (reviewed in [25,57,58,59]) and the lung tissues of TB patients [60,61]. The absence of the main cell wall glycolipid LAM in the Rv2623-positive Mtb prompted us to examine the acid-fast property of such Mtb by comparing the patients’ infected alveolar macrophages on confocal immunofluorescent images after ex vivo culture for 16-18 hours with the same alveolar macrophages re-stained by the ZN method. Previously, we have used this strategy of re-staining cell preparations to establish the unique features of Mtb lifestyle in host cells [35].
On the ZN re-stained cell preparations of patients 10–29, we did not find any acid-fast Mtb in alveolar macrophages with the previously identified Rv2623-positive Mtb, solitary and in colonies, in them (Figure 5). Additionally, we revealed a lack of acid-fast staining for Rv2623-positive Mtb in alveolar macrophages of the guinea pig with clinical signs of TB disease (Figure 5). The guinea pig was infected in a special study to assess the efficiency of infection control measures in TB hospital departments [35]. The same procedures, first with an immunofluorescence assay of Rv2623-positive Mtb and then with ZN re-staining for identification of acid-fast Mtb, were applied to cells obtained from the lung tissues of this animal after ex vivo culture for 20 hours. Remarkably, we also found the guinea pig’ alveolar macrophage containing both two shorter rod-shaped Rv2623-positive Mtb, which were non-acid-fast after ZN re-staining, and acid-fast filamentous Mtb that had not express the Rv2623 marker in the previous immunofluorescence assay (Figure 5). Therefore, neither Rv2623-positive Mtb demonstrated an acid-fastness nor did acid-fast Mtb express the Rv2623 protein in the alveolar macrophages. The LAM- and ESAT-6-positive Mtb were mainly acid-fast in the patients’ alveolar macrophages after ZN re-staining, while solitary shorter Mtb were occasionally non-acid-fast (for example, in patient 27 (tub) in Figure 5). In a mouse model of latent TB infection, we also detected LAM-positive, but non-acid-fast mycobacteria after ZN re-staining in granuloma cells obtained from the spleens of mice infected with the Bacillus Calmette-Guérin (BCG) vaccine (see Figure 5a in [62]).
After ZN re-staining, we did not identify any dead Rv2623-positive Mtb in the alveolar macrophages of the patients or the guinea pig: dead bacteria would have stained blue by the dye hematoxylin in our analysis due to an altered cell wall permeability and the destroyed plasma membrane. Therefore, the Rv2623-positive Mtb were characterized by an altered cell envelope, but an intact plasma membrane in the alveolar macrophages during TB disease. Therefore, substantial changes in cell wall composition and structure did not compromise the viability of the Rv2623-positive Mtb in host cells. Whether the Rv2623-positive Mtb replicate in colonies observed in the host cells and quickly restore the biosynthesis of LAM, acid-fastness, and growth in the alveolar macrophages after withdrawal of anti-TB drugs, remains to be known. On the whole, our results confirmed the existence of viable Mtb with an acid-fast-negative phenotype in the lungs of TB patients and animals and uncovered a significant number of host cells with non-acid-fast Mtb in them in various lung TB lesions of the patients studied. This phenomenon is undetectable by ZN staining, which is one of the main methods to detect Mtb in the diagnosis of TB infection and disease, and leads to underestimation of the Mtb burden in the human lungs.
Thus, our data suggest that the universal stress protein Rv2623 is likely to be a clinically relevant biomarker of viable Mtb that had lost their acid-fastness in the patients’ lungs. The identification of this Mtb signature has important potential therapeutic implications, including vaccine development, for the treatment and prevention of the human TB disease.
2.8. Subpopulations of phenotypically and physiologically distinct Mtb coexist in the same lung tissues of TB patients, no matter what lesion type
In our work, we have identified two main pools of Mtb in the total population of the pathogen persisting in the alveolar macrophages of TB patients, which were studied with the use of ex vivo cell cultures and, in parallel, the histological sections. The Mtb were phenotypically different in these pools and were mostly characterized by the presence or absence of the acid-fast property and expression of the virulence factors LAM and ESAT-6 or universal stress protein Rv2623, respectively (Table 2 and Table S1, Figure 6). Within each pool of Mtb, the pathogen survived as solitary bacteria or in colonies, including those with cording morphology (this applies only to the acid-fast Mtb), in host cells and demonstrated various growth potentials in the prolonged ex vivo cell cultures after withdrawal of anti-TB drugs, including the resumption of acid-fast and LAM-positive Mtb that replicated in the alveolar macrophages of some patients.
Based on the phenotypic and physiological features of the pathogen, we divided the total Mtb population in the alveolar macrophages of the patients into ten subpopulations (Table 2 and Table S1, Figure 6). The Mtb that were capable of actively replicating in a long-term ex vivo culture were assigned to subpopulations 2, 4, 6, and 7, while the Mtb with arrested growth were assigned to subpopulations 1, 3, and 5. Normally, we observed the different Mtb subpopulations in the patients’ host cells, no matter what type of TB lesions (Table 2 and Table S1). So, the re-established Mtb in subpopulation 7 were detected in the alveolar macrophages of many patients (Table 2). The same Mtb subpopulations were detected in the host cells obtained both from the cavity wall of patient 6 and the distant lung tissue sample of patient 10. The same Mtb subpopulations were revealed in the alveolar macrophages from both the tuberculoma walls and the distant lung tissue samples of patients 25, 28, and 29. However, Mtb subpopulations were others in the alveolar macrophages obtained from various lung TB lesions of patients 24 and 27 (Table S1).
Overall, the presence of the phenotypically and physiologically different subpopulations of drug-tolerant Mtb in the same lung tissues is indicative of not only passive mechanisms generating nonheritable resistance to multiple bactericidal antibiotics, which are associated mainly with a lack of Mtb growth in host cells, but also some active mechanisms of Mtb persistence, such as cell wall and metabolic pathway remodeling, which together help the pathogen survive anti-TB chemotherapy and other environmental stresses in infected alveolar macrophages.
3. Discussion
Our data indicate that phenotypically multidrug-tolerant Mtb not acquiring genetic mutations for resistance to the antibiotics used adopt diverse survival strategies in the alveolar macrophages of patients with active TB disease. The pathogen is able to survive antimicrobial chemotherapy in various subpopulations that are characterized by different phenotypic and physiologic features and coexist in various lung TB lesions. The characterization of the pathogen growth status identified acid-fast Mtb both in the growth-arrested state and with the ability to active division, as well as the re-established Mtb with the restoration of their acid-fastness, LAM synthesis, and replication, in the prolonged ex vivo cultures of the patients’ alveolar macrophages after withdrawal of anti-TB drugs. Additionally, Rv2623-positive Mtb having an acid-fast-negative phenotype and not expressing the virulence factors LAM and ESAT-6 were revealed for each TB patient studied. Taken together, our findings demonstrate a complex composition of Mtb infection in the lungs of TB patients, where the pathogen can dynamically change under the modified environmental conditions.
We could not determine whether the Rv2623-positive non-acid-fast Mtb quickly transformed into the LAM-positive and acid-fast Mtb or the re-established Mtb belonged to other subpopulations that were not detected in our work. However, the behavior of the Mtb re-established in the prolonged ex vivo cultures of the patients’ alveolar macrophages after withdrawal of anti-TB drugs resembled the behavior of the pathogen re-established after termination of anti-TB treatment in the Cornell murine model of Mtb persistence and dormancy [63,64], while it took this phenomenon several weeks to take shape in mice and only some days in the ex vivo cell cultures of TB patients. Note that Mtb were unculturable for both mice in the Cornell model and most TB patients after antimicrobial chemotherapy, although the Mtb DNA was detected in the PCR-analysis in all studies [33,65]. On the whole, further analysis of the phenomenon of Mtb resumption in the alveolar macrophages of TB patients should include the identification of the mechanisms of its development and the question of involvement of Rv2623-positive Mtb.
Interestingly, both the regrowth and resumption of the pathogen in the alveolar macrophages of some patients were achieved without the use of any special resuscitation-promoting factors or other products of Mtb in a long-term ex vivo culture, while many substances were necessary for resuscitation of Mtb in the different in vitro dormancy models with a wide spectrum of stressful conditions in stationary phase [66,67,68,69] and from the sputum of patients with active TB disease [70], while the Mtb transition from a dormant, nonreplicating state to an actively dividing state was estimated by a standard colony-forming assay. We hypothesize that Mtb, as an intravacuolar pathogen in the viable host cells of TB patients [35], are likely to be able to monitor stressful environments, including exposure to anti-TB drugs, through the interaction of the Mtb phagosomes and human endocytic pathways, as we have established previously [35], and to quickly resume the growth in favorable conditions, especially in colonies with cording morphology, for some patients. It is likely that some Rv2623-positive Mtb reside within phagosomes in the patients’ alveolar macrophages and interact with the host endosomal system for monitoring environmental conditions. These assumptions, however, require further studies.
It remains in question whether the phenotype of the Rv2623-positive non-acid-fast Mtb is a reliable indication of the dormant state of the pathogen in the lungs of TB patients, because higher levels of the Rv2623 protein in the cerebrospinal fluid has been proposed as a diagnostic biomarker of not only active, but also latent TB meningitis in humans [71]. Additionally, the Rv2623 protein was identified as a negative regulator in the cell envelope lipid biosynthesis [54] with, as expected, a decrease in LAM during the entry of Mtb into non-growth persistence and dormancy [72]. In our work, the morphological signs of Rv2623-positive Mtb were compared with the morphology of acid-fast and LAM- or ESAT-6-positive rod-shaped Mtb detected in the lungs of the patients, and were found to be significantly different from the characteristics of coccoid Mtb isolated in some in vitro models of Mtb dormancy [67,73,74] and from the infected animal tissues and the cavitary walls of TB patients [75]. At the same time, the signatures of Mtb clinical isolates on dense L-J medium in our study were similar to the characteristics of the model object M. smegmatis in stationary phase cultures and after exposure to different stress signals, which were also characterized by a loss of LAM expression and acid-fastness, but rapidly regained these properties after replating onto fresh medium [55,76,77]. Taken together, these results strongly suggest that the modulation of the LAM content that was detected in both the pathogenic and non-pathogenic mycobacteria, is a well-coordinated, growth phase- and environmental signal-regulated process likely affecting the cell wall integrity and unique acid-fast property of mycobacteria. On the whole, while in vitro and in vivo animal models remain some of the main sources of knowledge about the mechanisms of Mtb survival under multiple stressful conditions (reviewed in [68,69]), they are unlikely to reflect the actual situation in human TB disease or the true interaction between the pathogen and host cells under the treatment of TB patients. Therefore, future studies of Mtb persistence, dormancy, and resumption as well as the identification of biomarkers characterizing these phenomena and the growth features of the pathogen in humans are very important.
In our study, we have identified several biomarkers that characterize Mtb persistence in the alveolar macrophages of TB patients. First, Mtb dynamics in the prolonged ex vivo cell cultures after withdrawal of anti-TB drugs may represent a biomarker of the growth status and the physiological state of the pathogen, whether solitary and in colonies, including those with cording morphology, in the patients’ host cells at the time of surgery. Secondly, our analysis makes allows a possible reactivation of Mtb infection to be predicted in patients after cessation of antibiotic therapy and makes it possible to make more accurate inferences about the presence of higher-virulence Mtb than our previous suggestion, that is analysis of Mtb cording formation in the alveolar macrophages of TB patients [34]. In fact, initiating the regrowth of persistent/dormant Mtb followed by exposure to anti-TB drugs as one of the anti-TB treatment approaches (reviewed in [13,78]) can quickly eliminate drug-tolerant cells of the pathogen, as we detected in the prolonged ex vivo cell culture of patient 18 after exposure to ofloxacin. However, this strategy is extremely unsafe, because it is difficult to control the activity of this process in the patients’ host cells, as we observed in the prolonged ex vivo cell cultures of patient 6.
We have previously noted [79], a sudden emergence of fibroblast-like cells in prolonged ex vivo cell cultures may indicate the presence of mesenchymal stem cells in the lung TB lesions, which were detected for the tuberculoma wall of patient 27, but not for any other patients or TB lesions. Interestingly, we did not reveal any Mtb in these cells, although mesenchymal stem cells are expected to be a reservoir of Mtb infection in human TB disease and thus help the pathogen survive the anti-TB drug experience [80]. Therefore, it is necessary to proceed further with analysis of human host cells with the use of the opportunities provided by the ex vivo cell cultures obtained from different lung tissues of TB patients.
Thirdly, the Rv2623 protein may be used as a clinically relevant biomarker of Mtb that had lost their acid-fastness in the patients’ lungs. We also assume that the Rv2623-positive and non-acid-fast state of Mtb is common for some pathogens that have survived in both human TB lesions and animal lungs and is not related to anti-TB drug exposure alone. These assumptions, however, need to be studied. In addition, other mechanisms can lead to a loss of acid-fastness in Mtb, for example, those associated with defects in the biosynthesis of mycolic acids in the pathogen during TB infection of mice [81,82].
In the whole, a deeper understanding of the molecular and cellular biology of persistent Mtb in the lungs of TB patients, including transition of the pathogen from dormant nonreplicating state into an actively dividing state, is critical to improve the management of the disease and design more effective drugs or drug regimen to eradicate Mtb infection worldwide.
4. Materials and Methods
4.1. Patients and lung tissue samples
Lung tissue specimens were obtained from 29 patients with clinically active pulmonary TB at the Department of Thoracic Surgery of the Ural Research Institute for Phthisiopulmonology (Yekaterinburg, Russia) affiliated with the National Medical Research Center of Tuberculosis and Infectious Diseases of the Ministry of Health of the Russian Federation (Moscow, Russia) over the period from August 2014 to July 2018 as described in [33,35,36,37]. The patients’ nomenclature used is explained in [33]. These patients were residents of the Ural province of Russian Federation and had received TB treatment supervised by their local clinics. These patients had been characterized in detail (age, treatment, attendant diseases, surgery and others) previously in Table 1 and Tables S1–S4 in [33,35,36,37]. Lung tissue samples were also obtained from patients 32 (59 years old, male, without attendant diseases, surgery – upper lobe of right lung) and 33 (55 years old, female, without attendant diseases, surgery – upper lobe of right lung) with pulmonary TB at the Department of Thoracic Surgery of the Novosibirsk Regional Clinical Oncology Dispensary (Novosibirsk, Russia) over the period from November 2022 to March 2023. The diagnosis of patients 32 and 33 were verified by the pathomorphological studies of the lung lesions after surgery. Patients 32 and 33 were residents of the Siberia province and the Sakha Republic (Yakutia) of Russian Federation, respectively, and had not received any TB treatment before surgery. All patients gave written informed consent for collection of clinical correlates, tissue collection, research testing under the Ethics Committees of the Ural Research Institute for Phthisiopulmonology of the National Medical Research Center of Tuberculosis and Infectious Diseases- and Novosibirsk Regional Clinical Oncology Dispensary-approved protocols (27/2014/07/02 and 15/2021/11/16). Patient studies were conducted according to the Declaration of Helsinki. All the patients studied had tuberculomas and other fibrotic and caseotic TB lesions in the lungs and had been referred for the surgical management of pulmonary TB. Seven patients (6–10, 22, and 23) had cavities in the lungs. Immediately after surgery, pieces of lung tissues (~ 0.5-30 g) obtained from lung parts about 5 cm away from macroscopic TB lesions (tuberculomas and cavities) were collected for patients 1–5, 7–29, 32, and 33, pieces of the tuberculoma walls were collected for patients 24, 25, 27–29, 32, and 33, and only the cavity wall was collected for patient 6.
4.2. Analysis of drug-resistance mutations in Mtb genes
For isolation of mycobacterial DNA, the lung tissue samples obtained from the surgically resected lung parts of patients 1–29 were incubated for 60 minutes in 0.5 ml of Amplitube-Prep solution for Mtb inactivation (Sintol, Moscow, Russia), then an Amplitube-PB kit (Sintol, Russia) was used for DNA extraction. Mutations associated with resistance to isoniazid (katG, inhA), rifampicin (rpoB), ethambutol (embB), fluoroquinolones (gyrA, gyrB), capreomycin and aminoglycosides (rrs, eis) were analyzed using a microarray TB-TEST assay (BIOCHIP-IMB, Moscow, Russia) according to the manufacturer’s instructions.
4.3. Bacterial strains and cultures
The highly and low virulent Mtb clinical isolates 14-329, 14-319, 15-169, 15-446, and 15-218 were obtained from the lung tissue homogenates of patients 6, 8, 10, 20, and 11, respectively, with pulmonary tuberculosis (TB) during our earlier work [33,34] and used in this study. The Mtb clinical strains were cultured on dense L-J medium (Himedia Laboratories, India) at +37°C under standard conditions. The aliquots of the Mtb strains from each stationary and, after replating of Mtb onto fresh L–J medium, exponential phase culture were added to an uncoated glass microscope slide, dried, fixed with 10% formaldehyde solution in PBS for 10 min at room temperature.
4.4. Ex vivo isolation and culture of human cells
Alveolar macrophages from the specimens of surgically resected lung lesions of patients 1–29 were produced as described in [33,35,36,37]. In brief, samples of lung tissue were cut into small pieces and, for separating cell suspension containing alveolar macrophages from closed granulomatous fibrotic tissue, were further rubbed through a metal screen of a sieve with pores 0.5-2.0 mm in diameter in phosphate-buffer saline (PBS, pH 7.4). Cell pellets were centrifuged at 400 g for 5 minutes at room temperature and placed to 24-well plates (Orange Scientific, Belgium) with cover glasses (~ 8 x 8 mm in size) in the bottom and cultured for 16-18 hours in 0.5 ml of RPMI 1640 complete growth medium containing 10% fetal bovine serum, 2 mM glutamine and 50 µg/ml gentamicin (BioloT, Russian Federation) at +37 °C in an atmosphere containing 5% CO2. At hours 16-18 of ex vivo culture, after removal of growth medium with dead cell debris, monolayer cultures of human cells on the cover slips were washed twice with PBS for removal of nonadherent cells. In this time point, more than 90% of cells obtained from the cavity and tuberculoma walls and distant parts of resected lung tissue of all studied patients were found to be alveolar macrophages [33,35,36,37]. Besides alveolar macrophages, five more cell types were observed: dendritic cells, neutrophils, lymphocytes, fibroblasts, and multinucleate Langhans giant cells, but the population sizes of these cells were much lower (see Table S3 and Table 1 in [33,36]). Further, some ex vivo cell cultures of the patients were cultured in 0.5 ml of the complete growth medium without any antibiotics for 2-8 days at +37 °C in an atmosphere containing 5% CO2. Then, some ex vivo cell cultures of the patients were exposed with the different concentrations (see text) of anti-TB drugs: isoniazid (Sigma-Aldrich, USA, I3377), rifampicin (Nanjing Pars Biochem, China, R6056), ofloxacin (Sigma-Aldrich, USA, O8757), kanamycin (Sigma-Aldrich, USA, K4000), or capreomycin (Nanjing Pars Biochem, China, MB1047), – in the complete growth medium for 3 days at +37 °C in an atmosphere containing 5% CO2.
4.5. Guinea pig infection and ex vivo isolation of animal cells
Experiments involving animals were performed in accordance with “The Guidelines for Manipulations with Experimental Animals” issued by the Russian Ministry of Health (guideline 755) and European convention for the protection of vertebrate animals used for experimental and other scientific purposes (ETS no. 123, Strasbourg) and were approved by the Ethical Committee of the Ural Research Institute for Phthisiopulmonology of the National Medical Research Center of Tuberculosis and Infectious Diseases (Yekaterinburg, Russia, 27/2014/07/02). Female outbred guinea pig (10 weeks old, 320 g) was obtained from the Science and Production Association for Medical and Immunological Preparations (Mikrogen, Bashkortostan, Russia) and maintained under standard vivarium conditions, with water and food provided ad libitum. This guinea pig was infected with 0.5 ml of washout from the hands of the nurse in PBS into the right inguinal fold as described in [35] to determine the degree of Mtb contamination in the TB hospital departments and to evaluate the efficiency of infection control measures. After infection, guinea pig was closely monitored, paying attention to clinical and morphologic sings of TB disease. At day 79 post infection, the guinea pig with clinical signs of TB disease were euthanized and examined macroscopically and histologically for changes and TB lesions in the right lung, liver and spleen. Also, the lung piece of this guinea pig was homogenized in PBS and plated on L–J medium as described in [34]. After 4 weeks of incubation at +37 °C with obligatory visual control on a weekly basis, mycobacterial colonies were identified and confirmed as being Mtb using standard procedures. Cells were isolated from the left lung of this guinea pig following the same procedure as for the alveolar macrophages from the resected lungs of the TB patients and then cultured in 0.5 ml of the complete growth medium under the same conditions as human cells. At hour 20 of ex vivo culture, only alveolar macrophages (~ 80% of the cell population) and polymorphonuclear neutrophils (~ 20% of the cell population) were observed in the guinea pig cell cultures.
4.6. Cell staining
At hours 16-18 of ex vivo culture, after removal of growth medium with dead cell debris, some monolayer cultures of human cells on cover slips were washed with PBS and fixed with 4% formaldehyde solution in PBS for 10 minutes at room temperature. To visualize acid-fast Mtb within host cells, after washing with PBS, some cell preparations were stained by the ZN method. After ZN staining, the cells were further counterstained with Mayer’s hematoxylin. The other cell cultures were used for staining with antibodies and other reagents. In the experiments using Nile red dye (Thermo Fisher Scientific, USA, N1142), the cell preparations were incubated with 10 µM of the dye for 15 minutes at +37 °C in 5% CO2 before fixation. Then, they were fixed as described above, washed with PBS, blocked in PBS solution containing 2% BSA, and finally incubated first with rabbit polyclonal primary antibodies to Mycobacteria LAM (Abcam, England, ab20832) diluted 1:200 or Mtb ESAT-6 (courtesy of E.V. Deineko of the Institute of Cytology and Genetics, Novosibirsk, Russia) diluted 1:300 or mouse monoclonal primary antibodies to Mtb Rv2623 (Abcam, England, ab24291) diluted 1:1000. Some of the human fixed cell preparations were washed with PBS, permeabilized with 0.3% Triton X-100 solution in PBS for 2 minutes, blocked, and incubated first with the appropriate primary antibodies to Mycobacteria LAM or Mtb ESAT-6 or with primary antibodies to Mtb Rv2623 and LAM or ESAT-6 as described above or with mouse monoclonal primary antibodies to Mtb 38-kDa protein (Abcam, England, ab183165) diluted 1:1000. After a long-term ex vivo culture of the patients’ alveolar macrophages with the different concentrations of anti-TB drugs or under antibiotic-free conditions, the human cells on cover slips were fixed with 4% formaldehyde solution in PBS and stained by the ZN method as described above. Some of the fixed cell preparations of patient 6 were treated within 2 minutes in 0.3% Triton-X100 solution in PBS, blocked, and stained with the appropriate primary antibodies to Mycobacteria LAM as described above.
At hour 20 of ex vivo culture, the guinea pig’s cells on cover slips were washed with PBS, fixed with 4% formaldehyde solution in PBS for 10 minutes, and stained by the ZN method or, after permeabilization with 0.3% Triton X-100 solution in PBS for 2 minutes, for Mtb Rv2623 as described above.
Some of the fixed spots with stationary or exponential phase cultures of Mtb clinical isolates on glass microscope slides were stained by the ZN method. Other Mtb preparations were incubated with the appropriate primary antibodies to Mycobacteria LAM and Mtb Ag38 or Mtb Rv2623 as described above.
For all cell preparations, fluorescent visualization of bound primary antibodies was achieved using goat polyclonal secondary antibodies to rabbit IgG conjugated with DyLight 488 or DyLight 594 (Thermo Fisher Scientific, USA, 35553 or 35561, respectively) and to mouse IgG conjugated with Alexa 488 or Alexa 555 (Thermo Fisher Scientific, USA, A-11001 or A-21422, respectively) diluted 1:400 each. The cell preparations were incubated with the appropriate antibodies for 60 minutes at room temperature. Fluorescent staining was analyzed using the VECTASHIELD® Mounting Medium with DAPI (4΄,6-diamidino-2-phenylindole) (Vector Laboratories, USA, H-1200).
The patients’ alveolar macrophages stained for Mycobacteria LAM or Mtb ESAT-6 and Mtb Rv2623 were analyzed all along the cells’ height by confocal microscopy and, after washing from VECTASHIELD® Mounting Medium in PBS for 20 minutes, re-stained for acid-fast Mtb by the ZN method. After ZN re-staining, the cells were further counterstained with Mayer’s hematoxylin. Then, alveolar macrophages with acid-fast Mtb were viewed using an Axioskop 2 plus light microscope (Zeiss). Finally, the patients’ host cells on the confocal fluorescent images were compared with alveolar macrophages on the ZN images. The same procedures with analysis of immunofluorescent staining, then re-staining for acid-fast Mtb by the ZN method, and examination of the cytological preparations were applied to guinea pig’s alveolar macrophages.
4.7. Histology
The histological sections of the resected lung tissues of TB patients were prepared as described in [37]. In brief, the resected lung parts of the TB patients were cut into pieces. One portion of lung pieces was collected for producing alveolar macrophages as described above. The other portion of lung pieces was fixed with 4% formaldehyde solution in PBS (pH 7.4) for 20 hours at +4 °C. After fixation, the lung tissues were washed with PBS, incubated with 30% sucrose in PBS (pH 7.4) for 20 hours at +4 °C, frozen in Tissue-Tek O.C.T. Compound (Sakura Finetek, USA, 4583) at -25 °C, and sectioned at 16-µm slides on a Microtome Cryostat HM550 (Microm, Germany) at the Shared Center for Microscopic Analysis of Biological Objects of the Institute of Cytology and Genetics, SB RAS (Novosibirsk, Russian Federation). Sections were air-dried on SuperFrost Plus slides (Thermo Fisher Scientific, USA) and stained by the ZN method and further counterstained with Mayer’s hematoxylin. Some of the histological sections were first blocked and incubated with Nile red dye or rabbit monoclonal primary antibodies to human CD14 (Spring Bioscience, USA, M492) diluted 1:100 and primary antibodies to Mtb Ag38 as described above. Some of the histological sections were treated within 45 minutes in 0.3% Triton-X100 solution, blocked, and incubated with the appropriate antibodies to the Mtb antigens as described above. In addition, some of the histological sections were incubated with Alexa 488- or TRITC-labeled phalloidin dye (Thermo Fisher Scientific, USA, A12379 or Sigma-Aldrich, USA, P1951, respectively) diluted 1:100 each and primary antibodies to Mycobacteria LAM or Mtb Rv2623 as described above. Fluorescent visualization of Mtb and CD14 was achieved using secondary goat polyclonal fluorochrome-conjugated antibodies as described above. All the histological sections were incubated with the appropriate primary antibodies for 20 hours at +4 °C and with the appropriate secondary antibodies for 60 minutes at room temperature. Fluorescent staining was analyzed using the ProLong Gold Antifade Mountant with DAPI (Thermo Fisher Scientific, USA, P36935).
4.8. Microscopy
The histological sections, cytological and other preparations were examined at the Shared Center for Microscopic Analysis of Biological Objects of the Institute of Cytology and Genetics, SB RAS (Novosibirsk, Russian Federation), using an Axioskop 2 plus microscope (Zeiss) and objectives with various magnifications (Zeiss), and photographed using an AxioCam HRc camera (Zeiss); the images were analyzed using the AxioVision 4.7 microscopy software (Zeiss). Cell preparations stained with fluorescent dyes were examined under an LSM 780 laser scanning confocal microscope (Zeiss) using the LSM Image Browser and ZEN 2010 software (Zeiss). The human cells and Mtb in host cells were counted separately on each preparation for each patient in each test. More than 1000 alveolar macrophages were analyzed at each cytological preparation for each patient. The size of Mtb was analyzed using the ImageJ software. For the histological preparations, three un-serial tissue sections from each individual sample were analyzed for each patient.
4.9. Statistical analyses
Statistical data processing was performed using Prism (GraphPad Software) and Microsoft Excel 2010 with each statistical test, definitions of mean and standard error of the mean (SEM), and the number of samples per group (n, referring to individual cells or the lung tissues of TB patients) indicated in the corresponding text, figure legends, and panels. Statistical significance for the comparisons between the datasets was determined using Student’s t-test. Differences were considered statistically significant at P ˂ 0.05.
5. Conclusions
Our data indicate the presence of multiple forms of Mtb infection with various microbial compositions and pathological signs for each TB patient studied. Drug-tolerant Mtb that persist in alveolar macrophages of TB patients under an intensive antimicrobial chemotherapy before surgery exhibit a spectrum of phenotypic and physiologic features and coexist in various lung TB lesions. The pathogen can dynamically change with the restoration of their acid-fastness, LAM expression, and active division in the prolonged ex vivo cell cultures of some patients after withdrawal of anti-TB drugs. Rv2623-positive Mtb having an acid-fast-negative phenotype and not expressing the virulence factors LAM and ESAT-6 are revealed for all TB patients. In conclusion, our findings demonstrate a complex composition of Mtb infection in the lungs of TB patients and provide a new insight into the pathogenesis of Mtb during human TB disease. A better understanding of the mechanisms and pathways of pathogen survival in human lungs is the key to develop vaccines and drug regimens with the individualized management of TB patients for overcoming the resistance/tolerance crisis in the treatment of Mtb infection toward global TB eradication.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: M. tuberculosis (Mtb) are able to survive exposure to different concentrations of anti-TB drugs in the ex vivo cultures of alveolar macrophages obtained from the distant lung tissues of patient 10 with XDR-TB and patient 14 with isoniazid-resistant TB; Figure S2: Intracellular lipophilic inclusions are not found in the Mtb located both within and outside the alveolar macrophages obtained from the tuberculoma walls (tub) and the tissues distant from the macro-TB lesions of the patients’ resected lung parts on representative confocal 3D or single immunofluorescent images stained by the Mtb LAM- or ESAT-6-specific antibodies (green signal) and Nile red dye (red signal) after ex vivo culture for 16-18 hours; Figure S3: Rv2623-positive Mtb present in alveolar macrophages and necrotic caseum in various lung TB lesions of all the patients studied; Figure S4: Rv2623-positive Mtb identified in alveolar macrophages in tuberculoma (tub) walls and tissues distant (dist) from the macro-TB lesions of patients 32 and 33 without any anti-TB treatment before surgery; Table S1: Subpopulations (SP) of Mtb in alveolar macrophages of patients with pulmonary TB.
Author Contributions
Conceptualization, E.G.U. and N.I.E.; methodology, E.G.U.; software, E.G.U.; validation, E.G.U. and N.I.E.; formal analysis, E.G.U.; investigation, E.G.U. and N.I.E; resources, E.G.U. and N.I.E.; data curation, E.G.U.; writing—original draft preparation, E.G.U.; writing—review and editing, E.G.U. and N.I.E.; visualization, E.G.U.; supervision, E.G.U.; project administration, E.G.U. All authors have read and agreed to the published version of the manuscript.
Funding
This research was carried out according to the State Budgeted Project no. 1021050400914-1-1.6.4 of the Ministry of Science and Higher Education of the Russian Federation for the Federal Research Center of Fundamental and Translational Medicine. This research received no external funding. The work was performed using the equipment of the Centers for Collective Use “Spectrometric Measurements” and “Proteomic Analysis”, supported by funding from the Ministry of Science and Higher Education of the Russian Federation (agreement No. 075-15-2021-691).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committees of the Ural Research Institute for Phthisiopulmonology of the National Medical Research Center of Tuberculosis and Infectious Diseases (27/2014/07/02) and Novosibirsk Regional Clinical Oncology Dispensary (15/2021/11/16).
Informed Consent Statement
Informed written consent was obtained from all patients involved in the study.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Acknowledgments
The authors are thankful to PhD S.I. Bayborodin and T.E. Aleshina (Federal Research Center Institute of Cytology and Genetics, Novosibirsk, Russia), E.M. Petrunina, PhD T.V. Umpeleva, PhD D.V. Vakhrusheva, and Prof. S.N. Skornyakov (Ural Research Institute for Phthisiopulmonology, National Medical Research Center of Tuberculosis and Infectious Diseases of Ministry of Health of the Russian Federation, Yekaterinburg, Russia), PhD V.V. Kozlov (Novosibirsk Regional Clinical Oncology Dispensary, Russia) and MMedSci. M.S. Gileva (Novosibirsk State University, Russia) for technical support.
Conflicts of Interest
The authors declare that they have no competing interests. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- World Health Organization. In Global tuberculosis report; 2022.
- World Health Organization. Drug-resistant TB: Surveillance and response. Supplement to Global tuberculosis report 2014; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Beltran, C.G.G.; Heunis, T.; Gallant, J.; Venter, R.; du Plessis, N.; Loxton, A.G.; Trost, M.; Winter, J.; Malherbe, S.T.; Kana, B.D.; et al. Investigating non-sterilizing cure in TB patients at the end of successful anti-TB therapy. Front. Cell. Infect. Microbiol. 2020, 10, 443. [Google Scholar] [CrossRef] [PubMed]
- Müller, B.; Borrell, S.; Rose, G.; Gagneux, S. The heterogeneous evolution of multidrug-resistant Mycobacterium tuberculosis. Trends in Genetics 2013, 29, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Olaru, I.D.; Lange, C.; Heyckendorf, J. Personalized medicine for patients with MDR-TB. J. Antimicrob. Chemother. 2016, 71, 852–855. [Google Scholar] [CrossRef] [PubMed]
- Prozorov, A.A.; Zaichikova, M.V.; Danilenko, V.N. Mycobacterium tuberculosis mutants with multidrug resistance: History of origin, genetic and molecular mechanisms of resistance, and emerging challenges. Russ. J. Genet. 2012, 48, 1–14. [Google Scholar] [CrossRef]
- Koch, A.; Cox, H.; Mizrahi, V. Drug-resistant tuberculosis: Challenges and opportunities for diagnosis and treatment. Curr. Opin. Pharmacol. 2018, 42, 7–15. [Google Scholar] [CrossRef]
- Schrader, S.M.; Vaubourgeix, J.; Nathan, C. Biology of antimicrobial resistance and approaches to combat it. Sci. Transl. Med. 2020, 12, 549. [Google Scholar] [CrossRef]
- Sterwart, G.R.; Robertson, B.D.; Young, D.B. Tuberculosis: A problem with persistence. Nat. Rev. Microbiol. 2003, 1, 97–105. [Google Scholar] [CrossRef]
- Connolly, L.E.; Edelstein, P.H.; Ramakrishnan, L. Why is long-term therapy required to cure tuberculosis? PLoS Med. 2007, 4, e120. [Google Scholar] [CrossRef]
- Antonova, A.V.; Gryadunov, D.A.; Zimenkov, D.V. Molecular mechanisms of drug tolerance in Mycobacterium tuberculosis. Mol. Biol. 2018, 52, 372–384. [Google Scholar] [CrossRef]
- Boldrin, F.; Provvedi, R.; Mazzabo, L.C.; Segafreddo, G.; Manganelli, R. Tolerance and persistence to drugs: A main challenge in the fight against Mycobacterium tuberculosis. Front. Microbiol. 2020, 11, 1924. [Google Scholar] [CrossRef]
- Helaine, S.; Kugelberg, E. Bacterial persisters: Formation, eradication, and experimental systems. Trends Microbiol. 2014, 22, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Van den Bergh, B.; Fauvart, M.; Michiels, J. Formation, physiology, ecology, evolution and clinical importance of bacterial persisters. FEMS Microbiol. Rev. 2017, 41, 219–251. [Google Scholar] [CrossRef] [PubMed]
- Moldoveanu, A.L.; Rycroft, J.A.; Helaine, S. Impact of bacterial persisters on their host. Curr. Opin. Microbiol. 2021, 59, 1–7. [Google Scholar] [CrossRef]
- Nathan, C.; Barry III, C.E. TB drug development: Immunology at the table. Immunol. Rev. 2015, 264, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Gold, B.; Nathan, C. Targeting phenotypically tolerant Mycobacterium tuberculosis. Microbiol. Spectrum 2017, 5, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Mandal, S.; Njikan, S.; Kumar, A.; Early, J.V.; Parish, T. The relevance of persisters in tuberculosis drug discovery. Microbiology 2019, 165, 492–499. [Google Scholar] [CrossRef]
- Dartois, V.; Rubin, E.J. Anti-tuberculosis treatment strategies and drug development: Challenges and priorities. Nat. Rev. Microbiol. 2022, 20, 685–701. [Google Scholar] [CrossRef]
- Du, P.; Sohaskey, C.D.; Shi, L. Transcriptional and physiological changes during Mycobacterium tuberculosis reactivation from non-replicating persistence. Front. Microbiol. 2016, 7, 1346. [Google Scholar] [CrossRef]
- Hartman, T.E.; Wang, Z.; Jansen, R.S.; Gardete, S.; Rhee, K.Y. Metabolic perspectives on persistence. Microbiol. Spectrum 2017, 5, 5–11. [Google Scholar] [CrossRef]
- Ehrt, S.; Schnappinger, D.; Rhee, K.Y. Metabolic principles of persistence and pathogenicity in Mycobacterium tuberculosis. Nat. Rev. Microbiol. 2018, 16, 496–507. [Google Scholar] [CrossRef]
- Chao, M.C.; Rubin, E.J. Letting sleeping dos lie: Does dormancy play a role in tuberculosis? Annu. Rev. Microbiol. 2010, 64, 293–311. [Google Scholar] [CrossRef] [PubMed]
- Gengenbacher, M.; Kaufmann, S.H.E. Mycobacterium tuberculosis: Success through dormancy. FEMS Microbiol. Rev. 2012, 36, 514–532. [Google Scholar] [CrossRef] [PubMed]
- Lipworth, S.; Hammond, R.J.H.; Baron, V.O.; Hu, Y.; Coates, A.; Gillespie, S.H. Defining dormancy in mycobacterial disease. Tuberculosis 2016, 99, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Campaniço, A.; Harjivan, S.G.; Warner, D.F.; Moreira, R.; Lopes, F. Addressing latent tuberculosis: New advances in mimicking the disease, discovering key targets, and designing hit compounds. Int. J. Mol. Sci. 2020, 21, 8854. [Google Scholar] [CrossRef] [PubMed]
- Wayne, L.G.; Sohaskey, C.D. Nonreplicating persistence of Mycobacterium tuberculosis. Annu. Rev. Microbiol. 2001, 55, 139–163. [Google Scholar] [CrossRef] [PubMed]
- Joshi, H.; Kandari, D.; Bhatnagar, R. Insights into the molecular determinants involved in Mycobacterium tuberculosis persistence and their therapeutic implications. Virulence 2021, 12, 2721–2749. [Google Scholar] [CrossRef]
- Goossens, S.N.; Sampson, S.L.; Van Rie, A. Mechanisms of drug-induced tolerance in Mycobacterium tuberculosis. Clin. Microbiol. Rev. 2021, 34, 1–21. [Google Scholar] [CrossRef]
- Lake, M.A.; Adams, K.N.; Nie, F.; Fowler, E.; Verma, A.K.; Dei, S.; Teodori, E.; Sherman, D.R.; Edelstein, P.H.; Spring, D.R.; et al. The human proton pump inhibitors inhibit Mycobacterium tuberculosis rifampicin efflux and macrophage-induced rifampicin tolerance. Proc. Natl. Acad. Sci. USA 2023, 120, e2215512120. [Google Scholar] [CrossRef]
- Torrelles, J.B.; Schlesinger, L.S. Integrating lung physiology, immunology and tuberculosis. Trends Microbiol. 2017, 25, 688–697. [Google Scholar] [CrossRef]
- Park, H.-E.; Lee, W.; Shin, M.-K.; Shin, S.J. Understanding the reciprocal interplay between antibiotics and host immune system: How can we improve the anti-mycobacterial activity of current drugs to better control tuberculosis? Front. Immunol. 2021, 12, 703060. [Google Scholar] [CrossRef]
- Ufimtseva, E.; Eremeeva, N.; Petrunina, E.; Umpeleva, T.; Karskanova, S.; Baiborodin, S.; Vakhrusheva, D.; Skornyakov, S. Ex vivo expansion of alveolar macrophages with Mycobacterium tuberculosis from the resected lungs of patients with pulmonary tuberculosis. PLoS ONE 2018, 13, e0191918. [Google Scholar] [CrossRef] [PubMed]
- Ufimtseva, E.G.; Eremeeva, N.I.; Petrunina, E.M.; Umpeleva, T.V.; Baiborodin, S.I.; Vakhrusheva, D.V.; Skornyakov, S.N. Mycobacterium tuberculosis cording in alveolar macrophages of patients with pulmonary tuberculosis is likely associated with increased mycobacterial virulence. Tuberculosis 2018, 112, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ufimtseva, E.; Eremeeva, N.; Baiborodin, S.; Umpeleva, T.; Vakhrusheva, D.; Skornyakov, S. Mycobacterium tuberculosis with different virulence reside within intact phagosomes and inhibit phagolysosomal biogenesis in alveolar macrophages of patients with pulmonary tuberculosis. Tuberculosis 2019, 114, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Ufimtseva, E.; Eremeeva, N.; Bayborodin, S.; Umpeleva, T.; Vakhrusheva, T.; Skornyakov, S. Analysis of Mycobacterium tuberculosis uptake by alveolar macrophages after ex vivo expansion indicates processing host cells with pathogen actually from lung tissue of patients with pulmonary tuberculosis. Int. J. Mycobacteriol. 2020, 9, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Ufimtseva, E.G.; Eremeeva, N.I.; Umpeleva, T.V.; Vakhrusheva, D.V.; Skornyakov, S.N. Mycobacterium tuberculosis load in host cells and the antibacterial activity of alveolar macrophages are linked and differentially regulated in various lung lesions of patients with pulmonary tuberculosis. Int. J. Mol. Sci. 2021, 22, 3452. [Google Scholar] [CrossRef]
- Castro, R.A.D.; Borrell, S.; Gagneux, S. The within-host evolution of antimicrobial resistance in Mycobacterium tuberculosis. FEMS Microbiol. Rev. 2021, 45, fuaa071. [Google Scholar] [CrossRef]
- Ordonez, A.A.; Wang, H.; Magombedze, G.; Ruiz-Bedoya, C.A.; Srivastava, S.; Chen, A.; Tucker, E.W.; Urbanowski, M.E.; Pieterse, L.; Cardozo, E.F.; et al. Dynamic imaging in patients with tuberculosis reveals heterogeneous drug exposures in pulmonary lesions. Nature Med. 2020, 26, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Marimani, M.; Ahmad, A.; Duse, A. The role of epigenetics, bacterial and host factors in progression of Mycobacterium tuberculosis infection. Tuberculosis 2018, 113, 200–214. [Google Scholar] [CrossRef]
- Phthisiology. National guidelines; (In Russian). Perelman, M.I., Ed.; GEOTAR-Media: Moscow, Russia, 2007; ISBN 978-5-9704-0497-3. [Google Scholar]
- Dahl, J.L. Electron microscopy analysis of Mycobacterium tuberculosis cell division. FEMS Microbiol. Lett. 2004, 240, 15–20. [Google Scholar] [CrossRef]
- Thanky, N.R.; Young, D.B.; Robertson, B.D. Unusual features of the cell cycle in mycobacteria: Polar-restricted growth and the snapping-model of cell division. Tuberculosis 2007, 87, 231–236. [Google Scholar] [CrossRef]
- Garton, N.J.; Christensen, H.; Minnikin, D.E.; Adegbola, R.A.; Barer, M.R. Intracellular lipophilic inclusions of mycobacteria in vitro and in sputum. Microbiology 2002, 148, 2951–2958. [Google Scholar] [CrossRef] [PubMed]
- Garton, N.J.; Waddell, S.J.; Sherratt, A.L.; Lee, S.-M.; Smith, R.J.; Senner, C.; Hinds, J.; Rajakumar, K.; Adegbola, R.A.; Besra, G.S.; et al. Cytological and transcript analyses reveal fat and lazy persister-like bacilli in tuberculous sputum. PLoS Med. 2008, 5, e75. [Google Scholar] [CrossRef] [PubMed]
- Mekonnen, D.; Derbie, A.; Mihret, A.; Yimer, S.A.; Tønjum, T.; Gelaw, B.; Nibret, E.; Munshae, A.; Waddell, S.J.; Aseffa, A. Lipid droplets and the transcriptome of Mycobacterium tuberculosis from direct sputa: A literature review. Lipids Health Dis. 2021, 20, 129. [Google Scholar] [CrossRef] [PubMed]
- Boon, C.; Dick, T. How Mycobacterium tuberculosis goes to sleep: The dormancy survival regulator DosR a decade later. Future Microbiol. 2012, 7, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Reed, M.B.; Gagneux, S.; DeRiemer, K.; Small, P.M.; Barry III, C.E. The W-Beijing lineage of Mycobacterium tuberculosis overproduces triglycerides and has the DosR dormancy regulon constitutively upregulated. J. Bacteriol. 2007, 189, 2583–2589. [Google Scholar] [CrossRef]
- Park, H.-D.; Guinn, K.M.; Harrell, M.I.; Liao, R.; Voskuil, M.I.; Tompa, M.; Schoolnik, G.K.; Sherman, D.R. Rv3133c/dosR is a transcription factor that mediates the hypoxic response of Mycobacterium tuberculosis. Mol. Microbiol. 2003, 48, 833–843. [Google Scholar] [CrossRef]
- Karakousis, P.C.; Yoshimatsu, T.; Lamichhane, G.; Woolwine, S.C.; Nuermberger, E.L.; Grosset, J.; Bishai, W.R. Dormancy phenotype displayed by extracellular Mycobacterium tuberculosis within artificial granulomas in mice. J. Exp. Med. 2004, 200, 645–657. [Google Scholar] [CrossRef]
- Monahan, I.M.; Betts, J.; Banerjee, D.K.; Butcher, P.D. Differential expression of mycobacterial proteins following phagocytosis by macrophages. Microbiology 2001, 147, 459–471. [Google Scholar] [CrossRef]
- Shi, L.; Jung, Y.J.; Tyagi, S.; Gennaro, M.L.; North, R.J. Expression of Th1-mediated immunity in mouse lungs induces a Mycobacterium tuberculosis transcription pattern characteristic of nonreplicating persistence. Proc. Natl. Acad. Sci. USA 2003, 100, 241–246. [Google Scholar] [CrossRef]
- Drumm, J.E.; Mi, K.; Bilder, P.; Sun, M.; Lim, J.; Bielefeldt-Ohmann, H.; Basaraba, R.; So, M.; Zhu, G.; Tufariello, J.M.; et al. Mycobacterium tuberculosis universal stress protein Rv2623 regulates bacillary growth by ATP-binding: Requirement for establishing chronic persistent infection. PLoS Pathog. 2009, 5, e1000460. [Google Scholar] [CrossRef]
- Glass, L.N.; Swapna, G.; Chavadi, S.S.; Tufariello, J.M.; Mi, K.; Drumm, J.E.; Lam, T.T.; Zhu, G.; Zhan, C.; Vilchéze, C.; et al. Mycobacterium tuberculosis universal stress protein Rv2623 interacts with the putative ATP binding cassette (ABC) transporter Rv1747 to regulate mycobacterial growth. PLoS Pathog. 2017, 13, e1006515. [Google Scholar] [CrossRef]
- Fukuda, T.; Matsumura, T.; Ato, M.; Hamasaki, M.; Nishiuchi, Y.; Murakami, Y.; Maeda, Y.; Yoshimori, T.; Matsumoto, S.; Kobayashi, K.; et al. Critical roles for lipomannan and lipoarabinomannan in cell wall integrity of mycobacteria and pathogenesis of tuberculosis. mBio 2013, 4, e00472-12. [Google Scholar] [CrossRef]
- Guerin, M.E.; Korduláková, J.; Alzari, P.M.; Brennan, P.J.; Jackson, M. Molecular basis of phosphatidylmyo-inositol mannoside biosynthesis and regulation in mycobacteria. J. Biol. Chem. 2010, 285, 33577–33583. [Google Scholar] [CrossRef]
- Vilchèze, C.; Kremer, L. Acid-fast positive and acid-fast negative Mycobacterium tuberculosis: The Koch paradox. Microbiol. Spectrum 2017, 5, TBTB2-0003. [Google Scholar] [CrossRef] [PubMed]
- Stokas, H.; Rhodes, H.L.; Purdy, G.E. Modulation of the M. tuberculosis cell envelope between replicating and non-replicating persistent bacteria. Tuberculosis 2020, 125, 102007. [Google Scholar] [CrossRef] [PubMed]
- Allué-Guardia, A.; García, J.I.; Torrelles, J.B. Evolution of drug-resistant Mycobacterium tuberculosis strains and their adaptation to the human lung environment. Front. Microbiol. 2021, 12, 612675. [Google Scholar] [CrossRef] [PubMed]
- Seiler, P.; Ulrichs, T.; Bandermann, S.; Pradl, L.; Jörg, S.; Krenn, V.; Morawietz, L.; Kaufmann, S.H.E.; Aichele, P. Cell-wall alterations as an attribute of Mycobacterium tuberculosis in latent infection. J. Infect. Dis. 2003, 188, 1326–1331. [Google Scholar] [CrossRef] [PubMed]
- Ulrichs, T.; Lefmann, M.; Reich, M.; Morawietz, L.; Roth, A.; Brinkmann, V.; Kosmiadi, G.A.; Seiler, P.; Aichele, P.; Hahn, H.; et al. Modified immunohistological staining allows detection of Ziehl–Neelsen-negative Mycobacterium tuberculosis organisms and their precise localization in human tissue. J. Pathol. 2005, 205, 633–640. [Google Scholar] [CrossRef]
- Ufimtseva, E. Differences between Mycobacterium-host cell relationships in latent tuberculous infection of mice ex vivo and mycobacterial infection of mouse cells in vitro. J. Immun. Res. 2016, 2016, 4325646. [Google Scholar] [CrossRef]
- McCune, R.M.; Feldmann, F.M.; Lambert, H.P.; McDermott, W. Microbial persistence. I. The capacity of tubercle bacilli to survive sterilization in mouse tissues. J. Exp. Med. 1966, 123, 445–468. [Google Scholar] [CrossRef]
- McCune, R.M.; Feldmann, F.M.; McDermott, W. Microbial persistence. II. Characteristics of the sterile state of tubercle bacilli. J. Exp. Med. 1966, 123, 469–486. [Google Scholar] [CrossRef]
- de Wit, D.; Wootton, M.; Dhillon, J.; Mitchison, D.A. The bacterial DNA content of mouse organs in the Cornell model of dormant tuberculosis. Tuber. Lung Dis. 1995, 76, 555–562. [Google Scholar] [CrossRef]
- Shleeva, M.O.; Bagramyan, K.; Telkov, M.V.; Mukamolova, G.V.; Young, M.; Kell, D.B.; Kaprelyants, A.S. Formation and resuscitation of ‘nonculturable’ cells of Rhodococcus rhodochrous and Mycobacterium tuberculosis in prolonged stationary phase. Microbiology 2002, 148, 1581–1591. [Google Scholar] [CrossRef]
- Shleeva, M.O.; Kudykina, Y.K.; Vostroknutova, G.N.; Suzina, N.E.; Mulyukin, A.L.; Kaprelyants, A.S. Dormant ovoid cells of Mycobacterium tuberculosis are formed in response to gradual external acidification. Tuberculosis 2011, 91, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Veatch, A.V.; Kaushal, D. Opening Pandora’s box: Mechanisms of Mycobacterium tuberculosis resuscitation. Trends Microbiol. 2018, 26, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Salina, E.G.; Makarov, V. Mycobacterium tuberculosis dormancy: How to fight a hidden danger. Microorganisms 2022, 10, 2334. [Google Scholar] [CrossRef] [PubMed]
- Mukamolova, G.V.; Turapov, O.; Malkin, J.; Woltmann, G.; Barer, M.R. Resuscitation-promoting factors reveal an occult population of tubercle bacilli in sputum. Am. J. Respir. Crit. Care Med. 2010, 181, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.K.; Nayak, A.R.; Husain, A.A.; Panchbhai, M.S.; Chandak, N.; Purohit, H.J.; Taori, G.M.; Daginawala, H.F.; Kashyap, R.S. Mycobacterial dormancy regulon protein Rv2623 as a novel biomarker for the diagnosis of latent and active tuberculous meningitis. Dis. Markers 2013, 35, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Dulberger, C.L.; Rubin, E.J.; Boutte, C.C. The mycobacterial cell envelope — a moving target. Nat. Rev. Microbiol. 2020, 18, 47–59. [Google Scholar] [CrossRef]
- Velayati, A.A.; Farnia, P. Morphological characterization of Mycobacterium tuberculosis. In Understanding tuberculosis - deciphering the secret life of the bacilli; Cardona, P.-J., Ed.; InTech: Vienna, Austria, 2012; pp. 149–166. [Google Scholar]
- Jakkala, K.; Ajitkumar, P. Hypoxic non-replicating persistent Mycobacterium tuberculosis develops thickened outer layer that helps in restricting rifampicin entry. Front. Microbiol. 2019, 10, 2339. [Google Scholar] [CrossRef]
- Khomenko, A.G. The variability of Mycobacterium tuberculosis in patients with cavitary pulmonary tuberculosis in the course of chemotherapy. Tubercle 1987, 68, 243–253. [Google Scholar] [CrossRef] [PubMed]
- Dhiman, R.K.; Dinadayala, P.; Ryan, G.J.; Lenaerts, A.J.; Schenkel, A.R.; Crick, D.C. Lipoarabinomannan localization and abundance during growth of Mycobacterium smegmatis. J. Bacteriol. 2011, 193, 5802–5809. [Google Scholar] [CrossRef] [PubMed]
- Rahlwes, K.C.; Osman, S.H.; Morita, Y.S. Role of LmeA, a mycobacterial periplasmic protein, in maintaining the mannosyltransferase MptA and its product lipomannan under stress. mSphere 2020, 5, e01039-20. [Google Scholar] [CrossRef] [PubMed]
- Yiling, G.; Shuliang, G. Controlling strategy of dormant Mycobacterium tuberculosis. Chin. Med. J. 2014, 127, 3316–3321. [Google Scholar] [CrossRef]
- Ufimtseva, E.G.; Eremeeva, N.I. Mesenchymal stem cells in different lung lesions from patients with pulmonary tuberculosis. Genes & Cells 2022, 27, 237–238. (In Russian) [Google Scholar]
- Jain, N.; Kalam, H.; Singh, L.; Sharma, V.; Kedia, S.; Das, P.; Ahuja, V.; Kumar, D. Mesenchymal stem cells offer a drug-tolerant and immune-privileged niche to Mycobacterium tuberculosis. Nat. Commun. 2020, 11, 3062. [Google Scholar] [CrossRef]
- Bhatt, A.; Fujiwara, N.; Bhatt, K.; Gurcha, S.S.; Kremer, L.; Chen, B.; Chan, J.; Porcelli, S.A.; Kobayashi, K.; Besra, G.S.; et al. Deletion of kasB in Mycobacterium tuberculosis causes loss of acid-fastness and subclinical latent tuberculosis in immunocompetent mice. Proc. Natl. Acad. Sci. USA 2007, 104, 5157–5162. [Google Scholar] [CrossRef]
- Vilchèze, C.; Molle, V.; Carrère-Kremer, S.; Leiba, J.; Mourey, L.; Shenai, S.; Baronian, G.; Tufariello, J.; Hartman, T.; Veyron-Churlet, R.; et al. Phosphorylation of KasB regulates virulence and acid-fastness in Mycobacterium tuberculosis. PLoS Pathog. 2014, 10, e1004115. [Google Scholar] [CrossRef]
Figure 1.
M. tuberculosis (Mtb) survive a long-term antimicrobial chemotherapy of TB patients and resume active growth in alveolar macrophages of some patients in the prolonged ex vivo cell cultures after withdrawal of anti-TB drugs. (a) Mtb are acid-fast after Ziehl-Neelsen (ZN) staining and produce the virulence factors LAM, ESAT-6, and Ag38 stained with appropriate specific antibodies (green or red signals) in alveolar macrophages after ex vivo culture for 18 hours and on the histological sections obtained from the resected lung tuberculoma wall of patient 24 after treatment with multiple antibiotics before surgery. Single and double arrows point to rod-shaped and filamentous Mtb in colonies as clumps and with cording morphology, respectively, on representative cytochemical and confocal 3D immunofluorescent images. Nuclei are stained by DAPI (blue signal). Collagen fibers are strongly autofluorescent (green signal) on histological immunofluorescent images. The scale bars are 10 μm each; (b-d) Mtb loads are estimated in the ex vivo cultures of alveolar macrophages obtained from the cavity (cav) or tuberculoma (tub) walls and the tissues distant (dist or without labeling) from the macro-TB lesions of the patients’ resected lung parts; (b, c) The number of alveolar macrophages with any Mtb (solitary or as colonies, including those with cording morphology), with the colonies of Mtb, including the cords, and with Mtb only in cord-colonies in them, all expressed as the percentage of the total number of alveolar macrophages stained by the ZN method, represents the Mtb load in host cells of patients after ex vivo culture for 16-18 hours (16-18 h) and from two to eight days (D2-D8) without treatment with anti-TB drugs, and (c) after three days of ex vivo exposure to different concentrations of antibiotics, such as isoniazid (H), rifampicin (R), ofloxacin (Of), kanamycin (K), or capreomycin (Cap). Red arrows point to a trend towards increase in the number of Mtb-infected alveolar macrophages in the prolonged ex vivo cell cultures at D2-D8 versus 18 h. The numbers of patients, whose prolonged ex vivo cell cultures were characterized by this trend, are marked by red ovals; (c) Exposure of the patients’ alveolar macrophages to different concentrations of antibiotics does not eliminate drug-resistant or drug-susceptible Mtb in host cells in ex vivo culture during three days of treatment with anti-TB drugs; (d) Quantification of the alveolar macrophages with a particular number of Mtb in them expressed as the percentage of the total number of the Mtb-infected alveolar macrophages done for the patients, whose numbers are marked by red ovals in (b, c), after ex vivo culture for 18 h and D2-D6. Red and blue arrows point to trends towards, respectively, an increase and a decrease in the number of alveolar macrophages with a particular number of Mtb in them after ex vivo culture for various time points.
Figure 1.
M. tuberculosis (Mtb) survive a long-term antimicrobial chemotherapy of TB patients and resume active growth in alveolar macrophages of some patients in the prolonged ex vivo cell cultures after withdrawal of anti-TB drugs. (a) Mtb are acid-fast after Ziehl-Neelsen (ZN) staining and produce the virulence factors LAM, ESAT-6, and Ag38 stained with appropriate specific antibodies (green or red signals) in alveolar macrophages after ex vivo culture for 18 hours and on the histological sections obtained from the resected lung tuberculoma wall of patient 24 after treatment with multiple antibiotics before surgery. Single and double arrows point to rod-shaped and filamentous Mtb in colonies as clumps and with cording morphology, respectively, on representative cytochemical and confocal 3D immunofluorescent images. Nuclei are stained by DAPI (blue signal). Collagen fibers are strongly autofluorescent (green signal) on histological immunofluorescent images. The scale bars are 10 μm each; (b-d) Mtb loads are estimated in the ex vivo cultures of alveolar macrophages obtained from the cavity (cav) or tuberculoma (tub) walls and the tissues distant (dist or without labeling) from the macro-TB lesions of the patients’ resected lung parts; (b, c) The number of alveolar macrophages with any Mtb (solitary or as colonies, including those with cording morphology), with the colonies of Mtb, including the cords, and with Mtb only in cord-colonies in them, all expressed as the percentage of the total number of alveolar macrophages stained by the ZN method, represents the Mtb load in host cells of patients after ex vivo culture for 16-18 hours (16-18 h) and from two to eight days (D2-D8) without treatment with anti-TB drugs, and (c) after three days of ex vivo exposure to different concentrations of antibiotics, such as isoniazid (H), rifampicin (R), ofloxacin (Of), kanamycin (K), or capreomycin (Cap). Red arrows point to a trend towards increase in the number of Mtb-infected alveolar macrophages in the prolonged ex vivo cell cultures at D2-D8 versus 18 h. The numbers of patients, whose prolonged ex vivo cell cultures were characterized by this trend, are marked by red ovals; (c) Exposure of the patients’ alveolar macrophages to different concentrations of antibiotics does not eliminate drug-resistant or drug-susceptible Mtb in host cells in ex vivo culture during three days of treatment with anti-TB drugs; (d) Quantification of the alveolar macrophages with a particular number of Mtb in them expressed as the percentage of the total number of the Mtb-infected alveolar macrophages done for the patients, whose numbers are marked by red ovals in (b, c), after ex vivo culture for 18 h and D2-D6. Red and blue arrows point to trends towards, respectively, an increase and a decrease in the number of alveolar macrophages with a particular number of Mtb in them after ex vivo culture for various time points.
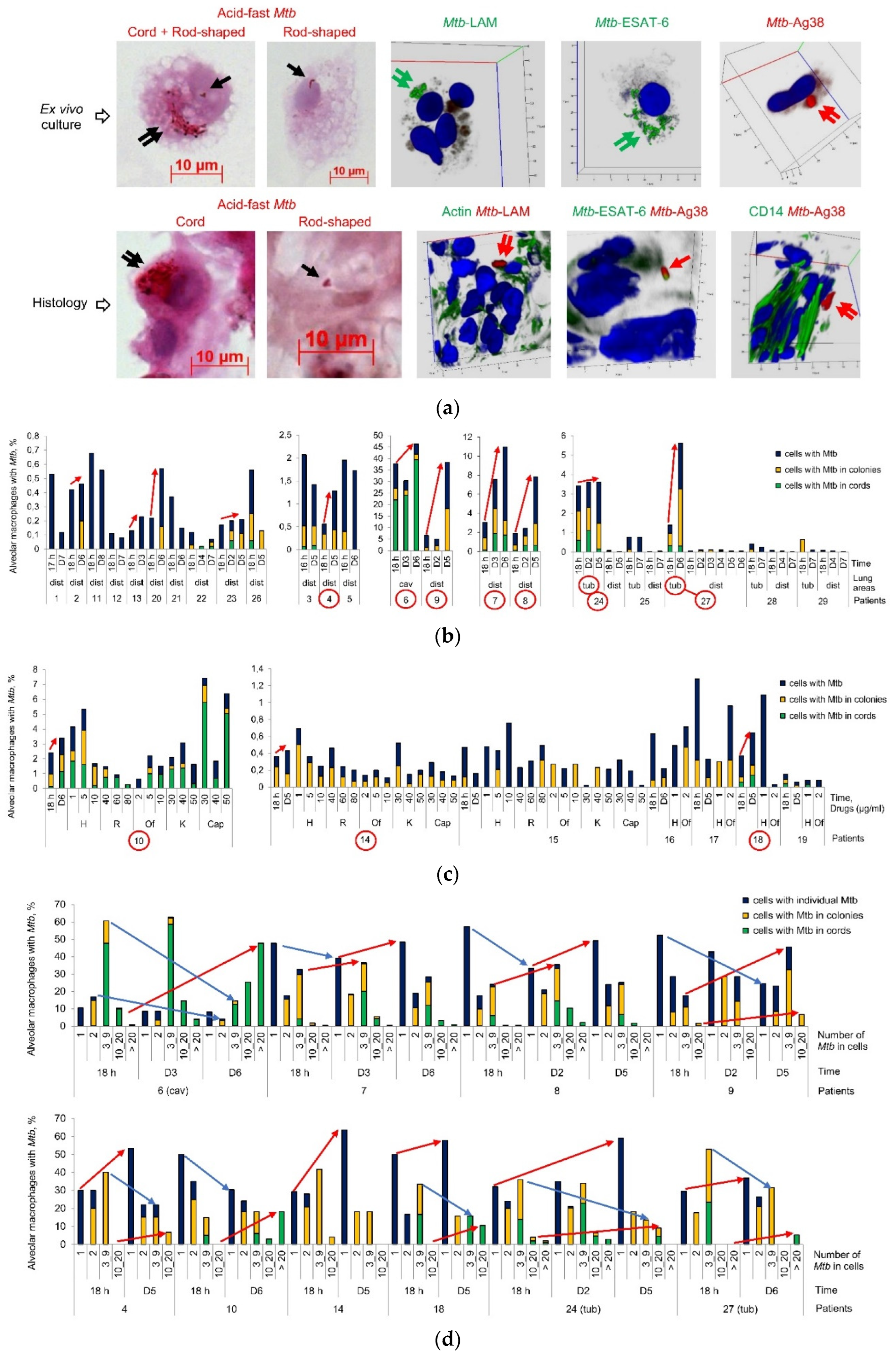
Figure 2.
M. tuberculosis (Mtb) with a distinct morphology re-establish in alveolar macrophages obtained from the cavity wall of patient 6 in the prolonged ex vivo cell cultures after withdrawal of anti-TB drugs. (a) Representative cytochemical and confocal 3D immunofluorescent images demonstrate Mtb with a distinct morphology, which are acid-fast after ZN staining and express LAM, stained with specific antibodies (green signal), in the patient’ alveolar macrophages after ex vivo culture at different time points. Single green and red arrows point to Mtb with a long filamentous and a shorter rod-shaped morphology, respectively. Double black and green arrows point to colonies with cording morphology and filamentous Mtb in them. Nuclei are stained by DAPI (blue signal). The scale bars are 10 μm each; (b) The number of viable and dead alveolar macrophages with different numbers of Mtb in colonies with cording morphology in them is expressed as the percentage of the total number of infected alveolar macrophages after ex vivo culture at all time points; (c) The number of alveolar macrophages with any short rod-shaped Mtb (solitary or as colonies) and with the colonies of Mtb with a shorter rod-shaped morphology are expressed as the percentage of the total number of the patient’ alveolar macrophages with acid-fast Mtb (filamentous or as rod-shaped) in them after ex vivo culture at all time points; (d) The number of viable alveolar macrophages with a particular number of filamentous Mtb (solitary or as colonies), with short rod-shaped Mtb (solitary or as colonies), and with the colonies of short rod-shaped Mtb in them expressed as the percentage of the total number of the patient’ alveolar macrophages with a particular number of acid-fast Mtb (filamentous or as rod-shaped) in them after a long-term ex vivo culture for D3 and D6.
Figure 2.
M. tuberculosis (Mtb) with a distinct morphology re-establish in alveolar macrophages obtained from the cavity wall of patient 6 in the prolonged ex vivo cell cultures after withdrawal of anti-TB drugs. (a) Representative cytochemical and confocal 3D immunofluorescent images demonstrate Mtb with a distinct morphology, which are acid-fast after ZN staining and express LAM, stained with specific antibodies (green signal), in the patient’ alveolar macrophages after ex vivo culture at different time points. Single green and red arrows point to Mtb with a long filamentous and a shorter rod-shaped morphology, respectively. Double black and green arrows point to colonies with cording morphology and filamentous Mtb in them. Nuclei are stained by DAPI (blue signal). The scale bars are 10 μm each; (b) The number of viable and dead alveolar macrophages with different numbers of Mtb in colonies with cording morphology in them is expressed as the percentage of the total number of infected alveolar macrophages after ex vivo culture at all time points; (c) The number of alveolar macrophages with any short rod-shaped Mtb (solitary or as colonies) and with the colonies of Mtb with a shorter rod-shaped morphology are expressed as the percentage of the total number of the patient’ alveolar macrophages with acid-fast Mtb (filamentous or as rod-shaped) in them after ex vivo culture at all time points; (d) The number of viable alveolar macrophages with a particular number of filamentous Mtb (solitary or as colonies), with short rod-shaped Mtb (solitary or as colonies), and with the colonies of short rod-shaped Mtb in them expressed as the percentage of the total number of the patient’ alveolar macrophages with a particular number of acid-fast Mtb (filamentous or as rod-shaped) in them after a long-term ex vivo culture for D3 and D6.
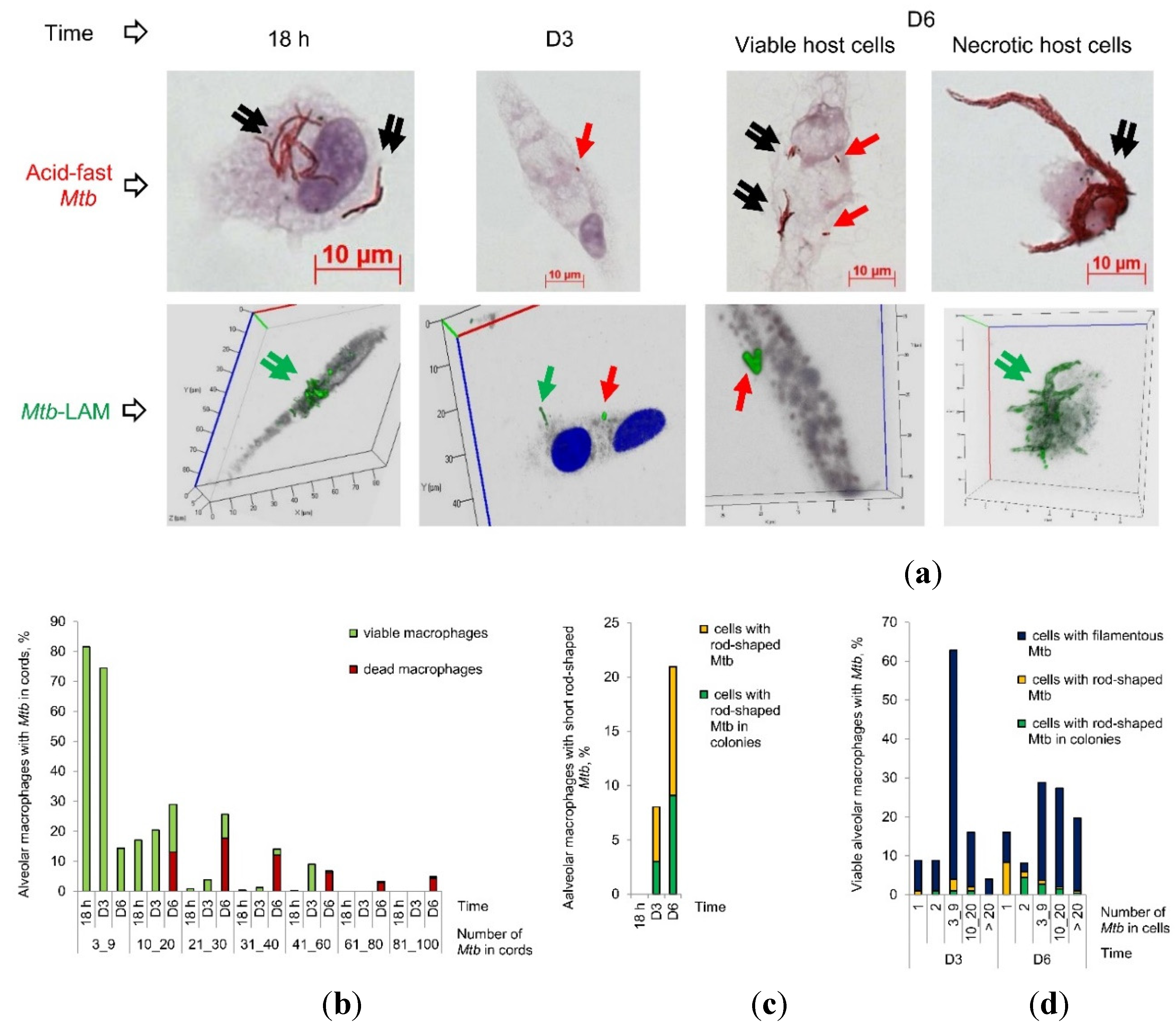
Figure 3.
M. tuberculosis (Mtb) clinical isolates obtained from the lung tissues of patients 6 and 10 produce the universal stress protein Rv2623 only in stationary phase (D90), but not in exponential phase (D20 after replating onto fresh L-J medium) cultures on dense L-J medium. Representative cytochemical images of Mtb after ZN staining and the merged confocal immunofluorescent and phase contrast images of Mtb stained with appropriate specific antibodies (green and red signals) are demonstrated. White short and long arrows on the merged images and profile graphs, respectively, point to the same Rv2623-positive Mtb with no LAM production in them. Yellow arrows on the merged images point to the areas for constructing profile graphs. The scale bars are 10 μm each.
Figure 3.
M. tuberculosis (Mtb) clinical isolates obtained from the lung tissues of patients 6 and 10 produce the universal stress protein Rv2623 only in stationary phase (D90), but not in exponential phase (D20 after replating onto fresh L-J medium) cultures on dense L-J medium. Representative cytochemical images of Mtb after ZN staining and the merged confocal immunofluorescent and phase contrast images of Mtb stained with appropriate specific antibodies (green and red signals) are demonstrated. White short and long arrows on the merged images and profile graphs, respectively, point to the same Rv2623-positive Mtb with no LAM production in them. Yellow arrows on the merged images point to the areas for constructing profile graphs. The scale bars are 10 μm each.
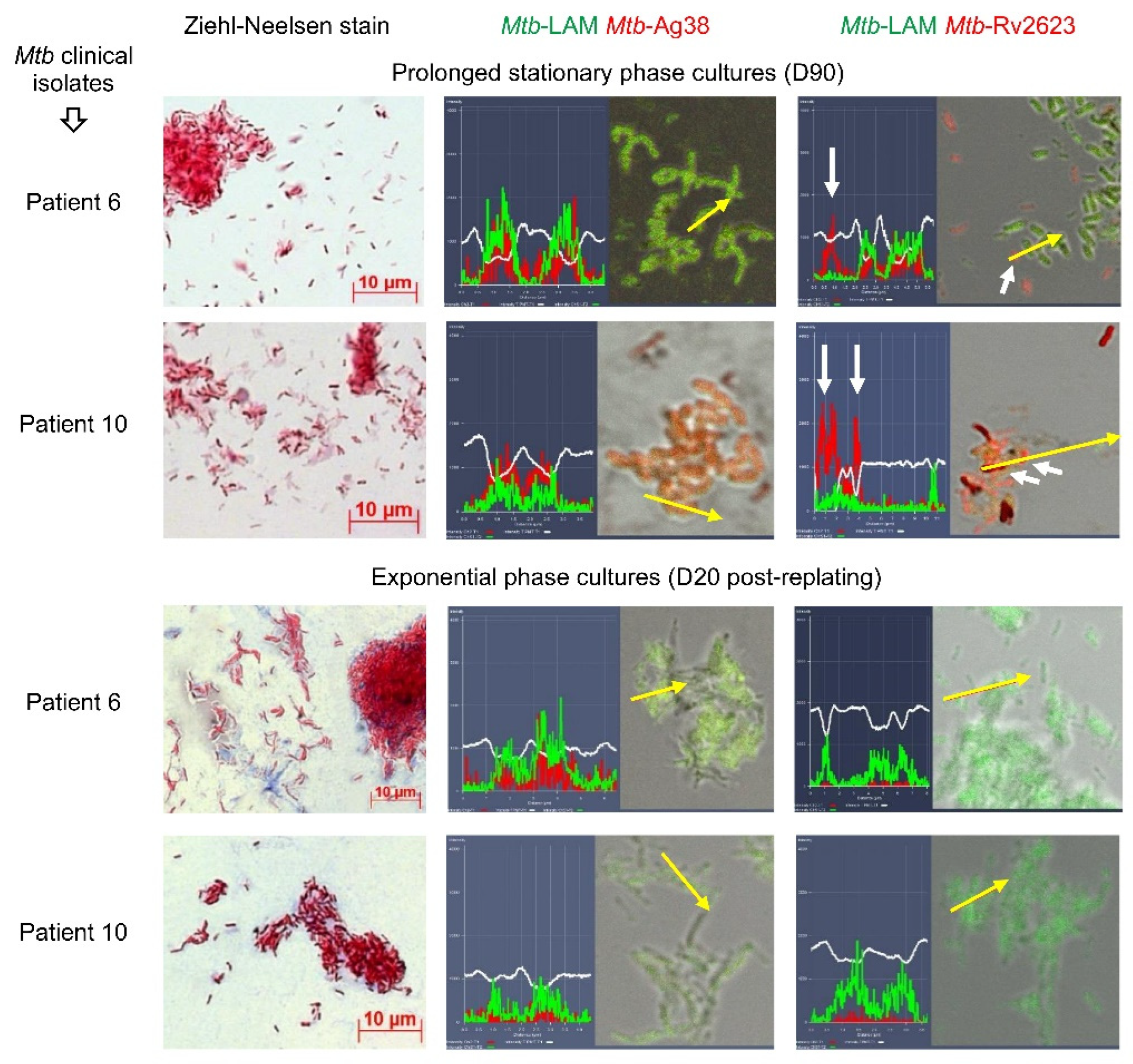
Figure 4.
Rv2623-positive Mtb not expressing the virulence factors LAM and ESAT-6 are identified in the alveolar macrophages of TB patients. (a) Representative confocal 3D immunofluorescent images stained simultaneously with appropriate specific antibodies demonstrate LAM- or ESAT-6-positive Mtb (green signal) not expressing the Rv2623 protein and, vice versa, Rv2623-positive Mtb (red signal) not expressing the virulence factors LAM and ESAT-6 in the patients’ alveolar macrophages on the histological sections and after ex vivo culture for 16-18 hours. Close-ups of the parts of the images with Mtb, solitary and in colonies, including those with cording morphology, are shown in the upper left or right corners. Green and red arrows point to the LAM- or ESAT-6- and Rv2623-positive Mtb, respectively; (a, c) Mtb are characterized in alveolar macrophages obtained from the cavity (cav) and tuberculoma (tub) walls and the tissues distant (dist or without labeling) from the macro-TB lesions of the patients’ resected lung parts. To the right of the 3D immunofluorescent images and (c) the image after ZN re-staining: profile images of the arrow-marked Mtb are shown. Yellow arrows point to the areas for constructing profile graphs. Nuclei are stained by DAPI (blue signal). Double arrows point to Mtb in colonies with cording morphology; (b) The number of alveolar macrophages or caseous regions with any Rv2623-positive Mtb (single or as colonies) and with the colonies of Rv2623-positive Mtb, both expressed as the percentage of the total number of host cells or caseous regions with LAM- or ESAT-6- and Rv2623-positive Mtb in them on the histological sections. The total data of two dual-staining on the LAM/Rv2623- and ESAT-6/Rv2623-markers of Mtb for each patient are used for the construction of the graph. Mean ± SEM. Below the graph, the table presents four groups of patients with different TB lesions and characteristics, including the extent of fibrosis and activation of stress factors. Symbols (+), (++), and (+++) indicate activation of stress factors in a single, rare, and the majority of the alveolar macrophages examined; (c) Representative confocal 3D immunofluorescent images demonstrate the absence of intracellular lipophilic inclusions stained by the Nile red dye (red signal), in the Rv2623-positive Mtb stained with specific antibodies (green signal), in the patients’ alveolar macrophages after ex vivo culture for 16-18 hours. Green and black arrows point to Rv2623-positive Mtb and acid-fast Mtb in colonies with cording morphology, respectively. The scale bar is 10 μm.
Figure 4.
Rv2623-positive Mtb not expressing the virulence factors LAM and ESAT-6 are identified in the alveolar macrophages of TB patients. (a) Representative confocal 3D immunofluorescent images stained simultaneously with appropriate specific antibodies demonstrate LAM- or ESAT-6-positive Mtb (green signal) not expressing the Rv2623 protein and, vice versa, Rv2623-positive Mtb (red signal) not expressing the virulence factors LAM and ESAT-6 in the patients’ alveolar macrophages on the histological sections and after ex vivo culture for 16-18 hours. Close-ups of the parts of the images with Mtb, solitary and in colonies, including those with cording morphology, are shown in the upper left or right corners. Green and red arrows point to the LAM- or ESAT-6- and Rv2623-positive Mtb, respectively; (a, c) Mtb are characterized in alveolar macrophages obtained from the cavity (cav) and tuberculoma (tub) walls and the tissues distant (dist or without labeling) from the macro-TB lesions of the patients’ resected lung parts. To the right of the 3D immunofluorescent images and (c) the image after ZN re-staining: profile images of the arrow-marked Mtb are shown. Yellow arrows point to the areas for constructing profile graphs. Nuclei are stained by DAPI (blue signal). Double arrows point to Mtb in colonies with cording morphology; (b) The number of alveolar macrophages or caseous regions with any Rv2623-positive Mtb (single or as colonies) and with the colonies of Rv2623-positive Mtb, both expressed as the percentage of the total number of host cells or caseous regions with LAM- or ESAT-6- and Rv2623-positive Mtb in them on the histological sections. The total data of two dual-staining on the LAM/Rv2623- and ESAT-6/Rv2623-markers of Mtb for each patient are used for the construction of the graph. Mean ± SEM. Below the graph, the table presents four groups of patients with different TB lesions and characteristics, including the extent of fibrosis and activation of stress factors. Symbols (+), (++), and (+++) indicate activation of stress factors in a single, rare, and the majority of the alveolar macrophages examined; (c) Representative confocal 3D immunofluorescent images demonstrate the absence of intracellular lipophilic inclusions stained by the Nile red dye (red signal), in the Rv2623-positive Mtb stained with specific antibodies (green signal), in the patients’ alveolar macrophages after ex vivo culture for 16-18 hours. Green and black arrows point to Rv2623-positive Mtb and acid-fast Mtb in colonies with cording morphology, respectively. The scale bar is 10 μm.
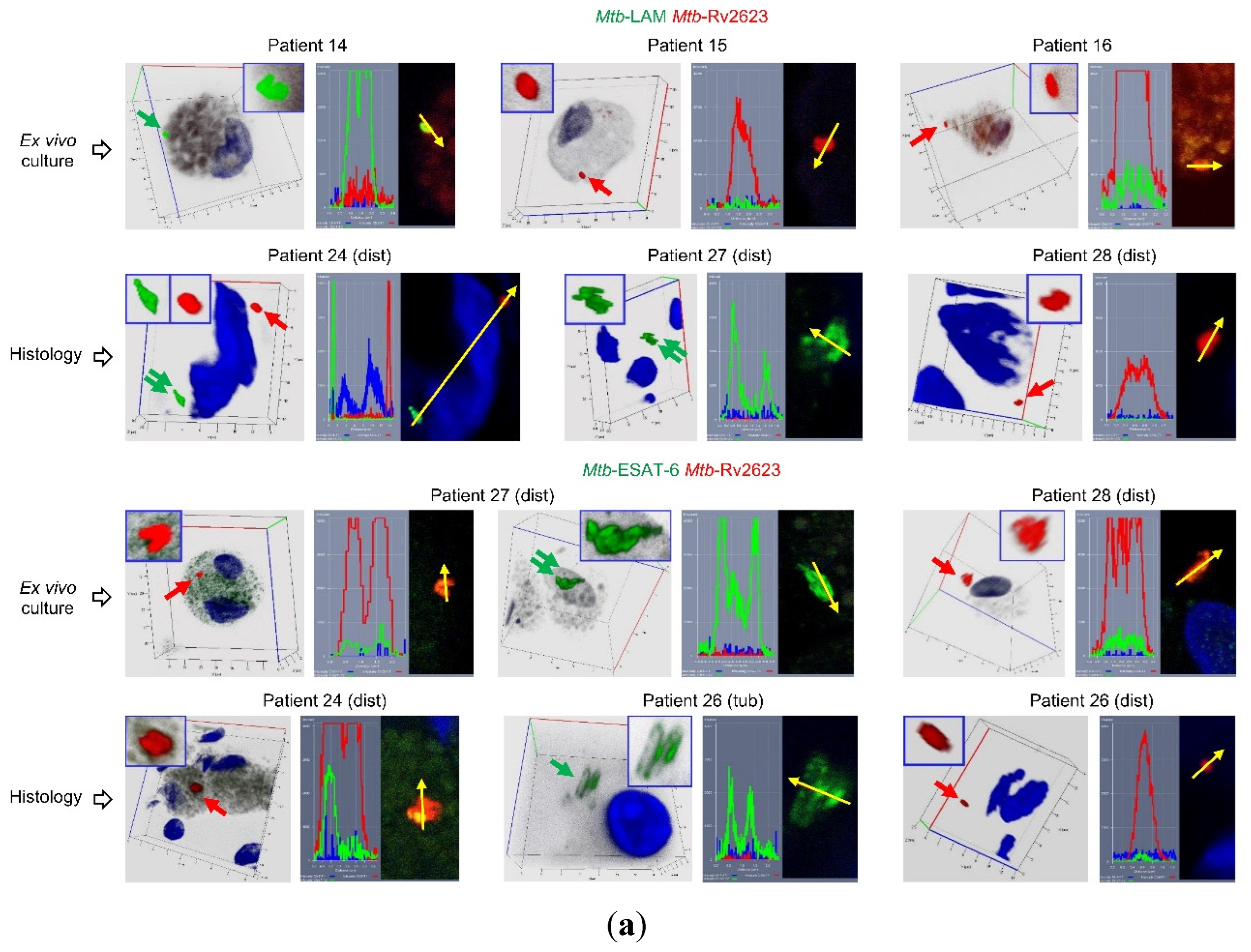
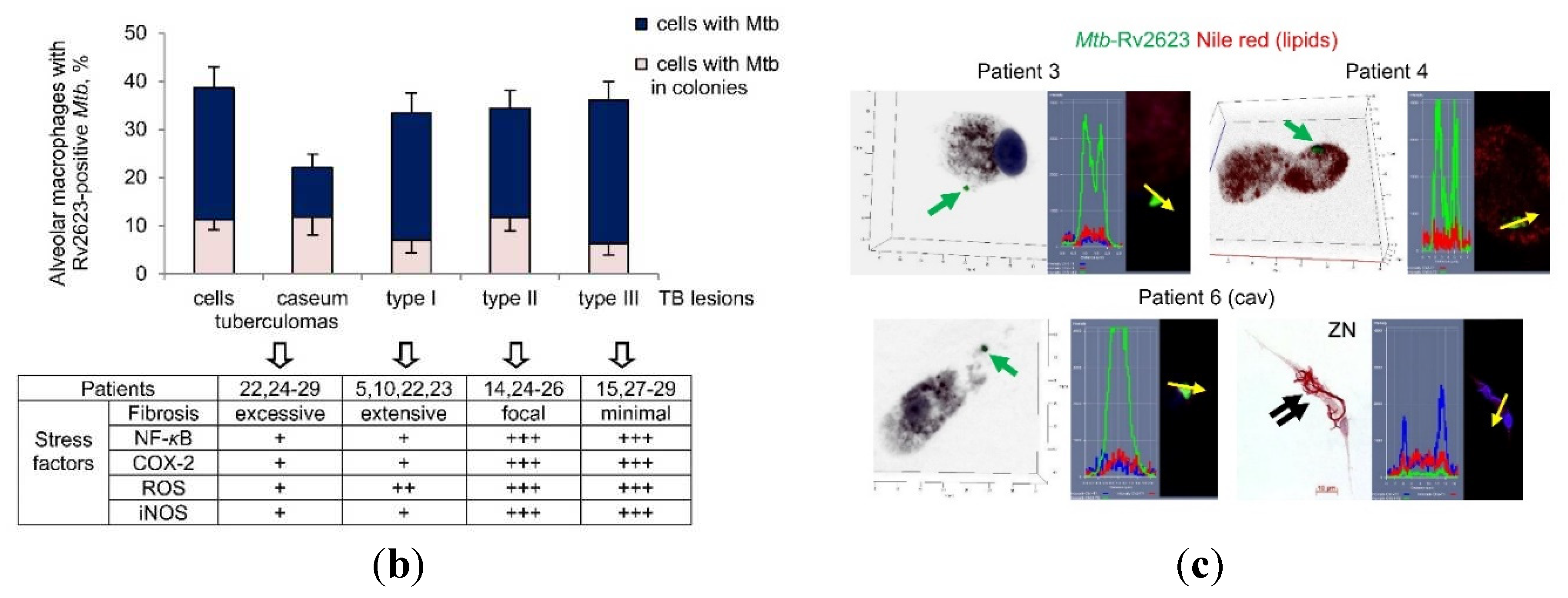
Figure 5.
Rv2623-positive M. tuberculosis (Mtb) reveal an acid-fast-negative phenotype in alveolar macrophages of patients and guinea pig with TB disease. Representative confocal 3D or single immunofluorescent images of host cells stained with antibodies reacting with the Mtb LAM or ESAT-6 (green signal) and Mtb Rv2623 (red signal) markers, and images of the same host cells after ZN re-staining (ZN) demonstrate Rv2623-positive Mtb, solitary and as colonies, with an acid-fast-negative phenotype in the patients’ and guinea pig’s alveolar macrophages after ex vivo culture for 18-20 hours. Nuclei are stained by DAPI (blue signal). Close-ups of the parts of the images with Mtb, solitary and in colonies, including those with cording morphology, are shown in the upper left or right corners. Green and red arrows point to the LAM- or ESAT-6- and Rv2623-positive Mtb, respectively. Brown short arrows point to the host cells with the Rv2623-positive Mtb in them. Black arrows point to the acid-fast Mtb on the ZN images. Double arrows point to Mtb in colonies with cording morphology Mtb are characterized in the ex vivo cultures of alveolar macrophages and, in parallel, on the histological sections obtained from the cavity (cav) and tuberculoma (tub) walls and the tissues distant (dist or without labeling) from the macro-TB lesions of the patients’ resected lung parts. The scale bars are 10 μm each.
Figure 5.
Rv2623-positive M. tuberculosis (Mtb) reveal an acid-fast-negative phenotype in alveolar macrophages of patients and guinea pig with TB disease. Representative confocal 3D or single immunofluorescent images of host cells stained with antibodies reacting with the Mtb LAM or ESAT-6 (green signal) and Mtb Rv2623 (red signal) markers, and images of the same host cells after ZN re-staining (ZN) demonstrate Rv2623-positive Mtb, solitary and as colonies, with an acid-fast-negative phenotype in the patients’ and guinea pig’s alveolar macrophages after ex vivo culture for 18-20 hours. Nuclei are stained by DAPI (blue signal). Close-ups of the parts of the images with Mtb, solitary and in colonies, including those with cording morphology, are shown in the upper left or right corners. Green and red arrows point to the LAM- or ESAT-6- and Rv2623-positive Mtb, respectively. Brown short arrows point to the host cells with the Rv2623-positive Mtb in them. Black arrows point to the acid-fast Mtb on the ZN images. Double arrows point to Mtb in colonies with cording morphology Mtb are characterized in the ex vivo cultures of alveolar macrophages and, in parallel, on the histological sections obtained from the cavity (cav) and tuberculoma (tub) walls and the tissues distant (dist or without labeling) from the macro-TB lesions of the patients’ resected lung parts. The scale bars are 10 μm each.
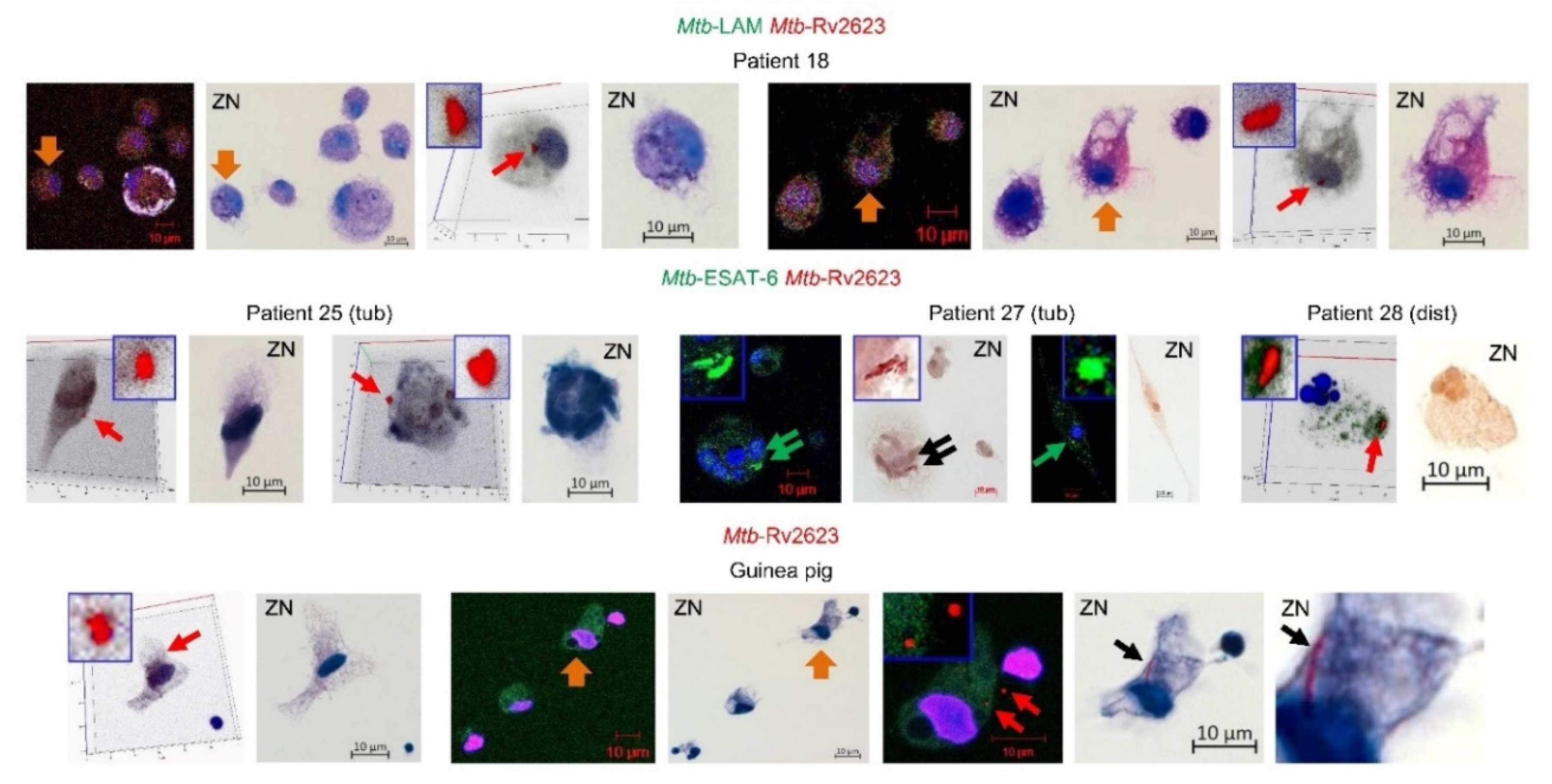
Figure 6.
The schematic picture represents different subpopulations of multidrug-tolerant Mtb with a spectrum of phenotypic and growth features in alveolar macrophages of TB patients. The numbers of Mtb subpopulations from Table 2 are shown in yellow circles.
Figure 6.
The schematic picture represents different subpopulations of multidrug-tolerant Mtb with a spectrum of phenotypic and growth features in alveolar macrophages of TB patients. The numbers of Mtb subpopulations from Table 2 are shown in yellow circles.
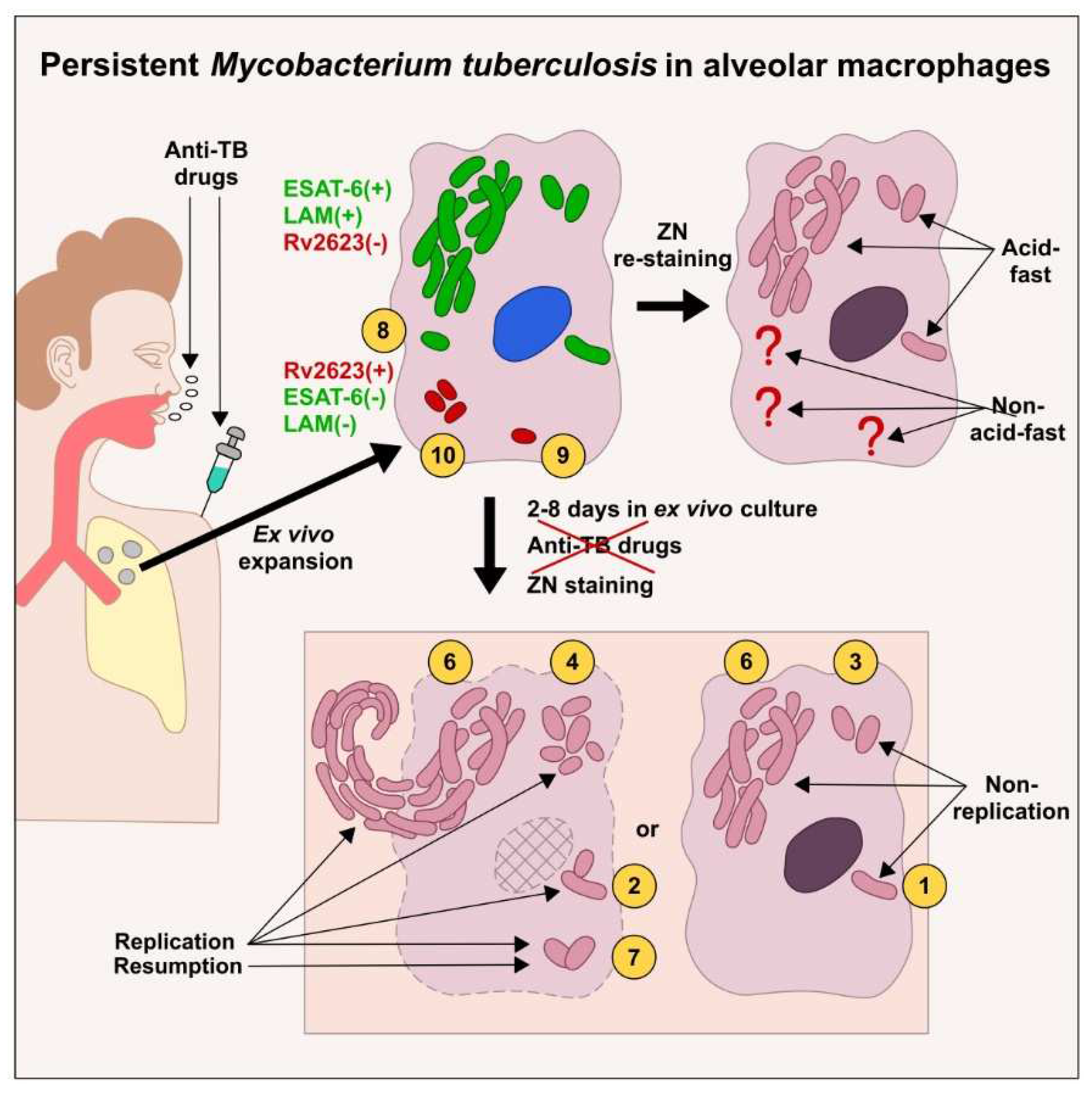

Table 1.
Drug-resistance mutations in the M. tuberculosis (Mtb) genes for the patients with pulmonary TB included in the study.
Table 1.
Drug-resistance mutations in the M. tuberculosis (Mtb) genes for the patients with pulmonary TB included in the study.
| Patients | Mutations in the Mtb genes associated with drug resistance to | Diagnosis | Treatment1 | Virulence2 | Mtb isolate3 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| H | R | E | Fq | AK | Drugs | Mo nths | ||||||
| katG | inhA | rpoB | embB | gyrA | rrs | eis | ||||||
| 1 | S315T1 | wt | S531L | wt | wt | wt | wt | MDR TB | Z Pt Cap Pas Cs Of | 24 | n.d. | - |
| 2 | S315T1 | wt | wt | wt | wt | wt | wt | TB | H R Z Pt Cap | 9 | n.d. | - |
| 3 | S315T1 | wt | S531L | wt | wt | wt | wt | MDR TB | H Z Pt Cap Pas Cs | 9 | n.d. | - |
| 4 | wt | wt | wt | wt | wt | wt | wt | TB | H R Z E | 5 | n.d. | - |
| 5 | S315T1 | wt | S531L | wt | wt | wt | wt | MDR TB | H R Z E Pt Cap Cs | 11 | L | - |
| 6 | S315T1 | wt | S531L | wt | wt | a1401g | wt | MDR TB | Z E Pt Cap Сs | 155 | H | + |
| 7 | S315T1 | wt | S531L | M306I | wt | wt | wt | MDR TB | H Z E Pt Cap Cs | 5 | n.d. | - |
| 8 | S315T1 | wt | wt | wt | wt | wt | wt | TB | H Z E Pt Rfd | 5 | H | + |
| 9 | S315T1 | wt | S531L | wt | wt | g1484t | wt | MDR TB | Z Rfd Cap Pas Cs | 31 | n.d. | - |
| 10 | S315T1 | wt | S531L | M306V | D94G | a1401g | wt | XDR TB | Z E Pt Cap Pas Cs | 41 | H | + |
| 11 | S315T1 | wt | S531L | wt | wt | wt | wt | MDR TB | Z Pt Cap Pas Cs | 74 | L | + |
| 12 | S315T1 | wt | S531L | wt | wt | wt | wt | MDR TB | Z Pt Cap Pas Cs | 19 | L | - |
| 13 | wt | wt | wt | wt | wt | wt | wt | TB | H R Z Pt Pas | 3 | L | - |
| 14 | S315T1 | wt | wt | wt | wt | wt | wt | TB | R Z E Pas | 6 | L | - |
| 15 | S315T1 | wt | S531L | M306V | wt | wt | wt | MDR TB | H R Z E | 58 | L | - |
| 16 | S315T1 | c15t | S531L | M306V | wt | wt | wt | MDR TB | Z Pt Cap Pas Cs Of | 40 | L | - |
| 17 | S315T1 | wt | S531L | M306V | wt | wt | wt | MDR TB | H Rfd Z E | 5 | L | - |
| 18 | S315T1 | wt | S531L | M306V | wt | wt | wt | MDR TB | H R Z E | 27 | IM | - |
| 19 | S315T1 | wt | S531L | wt | wt | wt | wt | MDR TB | Z Pt Cap Pas Cs | 26 | L | - |
| 20 | S315T1 | wt | S531L | M306V | wt | wt | wt | MDR TB | H Z E Rfd | 113 | H | + |
| 21 | wt | wt | wt | wt | wt | wt | wt | TB | Z E Pas Cs Of | 14 | L | - |
| 22 | S315T1 | wt | H526N | wt | wt | wt | wt | MDR TB | Z E Pas Cs K Of | 5 | L | - |
| 23 | S315T1 | t8g | S531L | D354A | wt | wt | c12t | MDR TB | H R Z E | 12 | L | - |
| 24 | S315T1 | wt | S531L | G406A | wt | wt | c12t | MDR TB | Z Pt Cap Pas Cs Lfx | 7 | L | - |
| 25 | S315T1 | wt | S531L | M306V | wt | wt | g10a | MDR TB | Z Pt Cap Pas Lfx | 9 | L | - |
| 26 | S315T1 | wt | S531L | G406A | wt | wt | wt | MDR TB | Z Pt Pas Cs K Lfx | 9 | L | - |
| 27 | S315T1 | wt | S531L | M306V | wt | wt | c14t | MDR TB | E Am Cs Lfx | 6 | L | - |
| 28 | ND | ND | ND | ND | ND | ND | ND | TB | H R Z E | 3 | L | - |
| 29 | wt | wt | wt | wt | wt | wt | wt | TB | H R Z E | 9 | L | - |
ND, not determined; n.d., not done; wt, wild type; (+), is present; (-), is absent. 1 before surgery. Drugs: AK, aminoglycosides; Am, amikacin; Cap, capreomycin; Cs, cycloserine; E, ethambutol; Fq, fluoroquinolones; H, isoniazid; K, kanamycin; Lfx, levofloxacin; Of, ofloxacin; Pas, para-aminosalicylic acid; Pt, protionamide; R, rifampicin; Z, pyrazinamide. 2 was characterized in the guinea pig model of TB disease [34]. Degree: L, low; IM, intermediate; H, high. 3 was grown on L-J medium [33].
Table 2.
Features of the M. tuberculosis (Mtb) that survived antibiotic therapy of patients with pulmonary TB.
Table 2.
Features of the M. tuberculosis (Mtb) that survived antibiotic therapy of patients with pulmonary TB.
| Mtb phenotypes | SP | TB patients | |||
|---|---|---|---|---|---|
| Acid-fastness | Markers | Survival state1 | Growth status2 | ||
| + | + LAM + ESAT-6 – Rv2623 |
solitary | non-replicating | 1 | all the patients and lung TB lesions studied |
| replicating | 2 | 2–4, 6 (cav), 7–10, 17, 18, 20, 22, 23, 24 (tub), 27 (tub) | |||
| in colonies (as irregular clumps) |
non-replicating | 3 | 3–5, 6 (cav), 7–10, 14–19, 22, 23, 24 (tub and dist), 25 (tub and dist), 26, 27–29 (tub and dist) | ||
| replicating | 4 | 4, 6 (cav), 7–10, 16–18, 22, 23, 24 (tub), 27 (tub) | |||
| in colonies with cording morphology |
non-replicating | 5 | 3, 19, 22, 26 | ||
| replicating | 6 | 6 (cav), 7, 8, 10, 18, 24 (tub), 27 (tub) | |||
| re-established2 | replicating | 7 | 4, 6 (cav), 7–10, 13, 14, 18, 20, 23, 24 (tub), 27 (tub) | ||
| – | solitary | ns | 8 | 14–16, 18, 24 (tub), 27 (tub) | |
| – LAM – ESAT-6 + Rv2623 |
solitary | ns | 9 | all the patients and lung TB lesions studied | |
| in colonies (as irregular clumps) |
ns | 10 | 3, 4, 6 (cav), 10, 14–16, 18,19, 22, 23, 24 (tub and dist), 25 (tub and dist), 26, 27–29 (tub and dist) | ||
SP, subpopulations; (+), is present; (–), is absent; ns, not studied. The phenotype of Mtb was determined in alveolar macrophages obtained from the cavity (cav) and tuberculoma (tub) walls and the tissues distant (dist or without labeling) from the macro-TB lesions of the patients’ resected lung parts after 1ex vivo culture for 16-18 hours and in 2the prolonged ex vivo cell cultures after withdrawal of anti-TB drugs.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



