
Submitted:
20 August 2023
Posted:
21 August 2023
You are already at the latest version
Abstract
Erectile dysfunction (ED) is the inability to achieve or maintain an erection during sexual performance. ED is one of the most common and neglected complications of diabetes. Almost 35-75% of diabetic men around the world suffer from ED. Although the exact mechanism by which diabetes causes ED is not well understood. However, several studies suggested it may be related to damage to the nerve and vessels that supply the penis.
Keywords:
Diabetes
; Erectile dysfunction
; microvascular complications
; diabetic sexual health
; men’s sexual health
Introduction:
Sexual health is essential to the general health and well-being of people, couples, and families, as well as the social and economic growth of communities and countries. According to World Health Organization (WHO), Sexual health is a state of physical, emotional, mental and social well-being related to sexuality; it is not merely the absence of disease, dysfunction or infirmity [1]. Sexual health is more than just the absence of disease and the presence of positive sexual experiences, intimacy, and well-being. It is a fundamental aspect of overall health and a key component of comprehensive health care [2]. It involves having a positive and respectful attitude towards sexuality, seeking pleasure and fulfillment during sexual interactions, and abstaining from discrimination and violence. Erectile dysfunction (ED) is an interconnected concepts with sexual health that emphasize the significance of addressing sexual well-being for individuals experiencing difficulties to achieve or maintain an erection. It is a common disorder that affects millions of men’s sexual health worldwide [10, 11]. The significance of managing sexual disorders, particularly ED, cannot be understated due to its tremendous impact on numerous aspects of individuals’ lives. ED can be defined as the inability to achieve or maintain sufficient rigidity of the penis for sexual intercourse [12]. Several factors are included for normal erectile functions such as sexual desire or libido for the partner, enough circulation of blood from the iliac artery to the corpora cavernosal which is responsible for erecting and rigid enough for adequate penetration, the ejaculation of sperm, and a good sense of orgasm [13]. According to International Consultation Committee for Sexual Medicine, the prevalence of ED was 1%–10% in men younger than 40 years, 2%–9% among men between 40 and 49 years, and it increased to 20%–40% among men between 60–69 years, reaching the highest rate in men older than 70 years (50%–100%) [14].
In the modern world, metabolic disorders are increasing rapidly due to the changes in the lifestyle, diet and environmental factors. Diabetes is one of the common metabolic disorders in which the body cannot produce enough insulin or the peripheral cells resist to use insulin effectively [3-5]. The number of diabetic patients increasing day by day with an estimated 422 million people worldwide [6]. According to WHO diabetes is the major cause of blindness, kidney failure, heart attacks, stroke and lower limb amputation. In 2019, 2 million deaths occur due to diabetes and its complications which considered that diabetes is one of the deadliest noncommunicable diseases after cardiovascular diseases (CVD) and cancer [7]. Insulin resistance, autoimmune disease, hormonal imbalances, pancreatic damage, and genetic mutations are the known etiology of diabetes. Obesity, a sedentary lifestyle, aging, high blood pressure, and high cholesterol are the culprits behind this etiology [8]. Diabetes is associated with both microvascular (diabetic retinopathy, neuropathy, and nephropathy) and macrovascular (CVD) complications [5]. People with diabetes have a higher risk of CVD which includes coronary heart diseases (CHD), hypertension, elevated low-density lipoprotein-cholesterol (LDL), and obesity [9].
Diabetes can significantly effect on intimate health for both man and women. Women with diabetes are the higher group of sexual disorders than that of healthy women. Lack of vaginal lubrication, pain during sexual intercourse, and inability to orgasm are all symptoms of high or low blood glucose levels. Diabetic women also experience higher rate of depression which may cause low sexual drive [10]. According to the statement of American Diabetes Association, Men and women experience low libido as a result of poorly managed diabetes [11]. Several studies have shown that ED is more in men with diabetes compared to healthy men [12]. On average, ED occurs 10–15 years earlier in patients with diabetes compared to non-diabetic. The proposed mechanism behind ED in diabetes includes central and autonomic diabetic neuropathy, endothelial dysfunction, and smooth muscle dysfunction [13]. The involvement of neuropathic and angiopathic changes due to high blood glucose contributes to ED [14]. Intimate relationships and sexual satisfaction can be negatively impacted by managing a chronic condition like diabetes since these emotions can cause stress, anxiety, and sadness. Moreover, Intimate health can also be negatively impacted by diabetes physically and psychologically which may lead to damaging relationships and communication and emotional connection issues in partnerships.
Men with diabetes are much more likely to have ED than men without diabetes. A study over 1503 participants by Corona and colleague observed that, patient with diabetes 19.4% have mild, mild-to-moderate 15.4%, moderate 10.4%, and severe 21.6% patient are suffering from ED [15]. Another meta-analysis by XU Wang et all, shows that the overall prevalence of ED in diabetic men without DS was 37.4% [16]. Another study on 9858 diabetic men reported 3534 (35%) suffering from ED [17].
In this review, we will focus on the evidences linking Diabetes & ED, treatment options, research and advances in Diabetes-Related ED as it is very important to emphasize sexual health along with management of ED that allows individuals can approach their sexual wellbeing holistically. Promoting overall sexual well-being improves not the quality of life but also enhance reproductive health which plays a crucial role in maintaining a stable human population.
Materials and methods:
Three authors independently conducted systematic retrieval of PubMed, EMBASE, Cochrane, and Web of Science, and the retrieval time was up to March 20, 2023. Searching includes, erectile dysfunction OR sexual dysfunction OR impotence OR diabetic sexual health OR men’s sexual health. This system review is reported in accordance with the preferred reporting items of the system review and meta-analysis (PRISMA) (Figure 1)
Understanding Diabetes:
Diabetes is a chronic health condition characterized by high blood sugar levels. Our bodies convert carbs from food into glucose, which serves as our main energy source. Insulin is a hormone made by the pancreatic beta cells that helps glucose get into cells to be used for energy. In diabetes pancreas doesn't produce any insulin at all or uses it improperly. Glucose then stays in blood and doesn’t reach your cells.
There are three main types of diabetes:
Type 1 diabetes: This type happens when the body's immune system unintentionally targets and kills the pancreatic cells that make insulin. As a result, little or no insulin is produced by the body. Type 1 diabetes often develops in childhood or adolescence, persons with type 1 diabetes must receive lifelong insulin therapy to survive[18].
Type 2 diabetes: The most common form of diabetes, accounting for the majority of cases is type 2 diabetes. In type 2 the pancreatic beta cell cannot produce enough insulin and peripheral tissue also develop insulin resistance. Obesity, poor physical activity, high carbohydrate diet maybe the most common cause of type 2 and can develop at any age mostly in adults. Life style modification, oral anti hypoglycemic drug or insulin therapy is the most acceptable treatment for type 2 diabetes [19].
Gestational diabetes: When blood sugar levels rise too high during pregnancy, gestational diabetes (GD), a kind of diabetes, begins to form. GD usually appears during the middle of pregnancy, between 24 and 28 weeks. Unlike type 1 diabetes, gestational diabetes is not brought on by a deficiency in insulin, but rather by other hormones produced throughout pregnancy that may reduce the effectiveness of insulin, a condition known as insulin resistance. After birth, gestational diabetes symptoms go away. In the United States, gestational diabetes is recognized in 3 to 8% of all pregnant women [20].
Diabetes has both acute and chronic complications. It has a significant impact on overall health, impacting several body systems and perhaps causing a number of issues if glycemic index is poorly maintained. Long term complications such as[21].
Diabetes vasculopathy, in which increased blood sugar reduce elasticity of the blood capillaries and leads them to constrict, which reduces blood flow. Reducing the flow of blood and oxygen, increase the risk of high blood pressure and damage to both major and small blood vessels. High blood pressure is a risk factor for heart disease [22].
Cardiovascular complications, Diabetes is an independent risk factor for CVD in both men and women, according to a substantial body of epidemiological and pathological research [23-25]. Women with diabetes tend to lose a large portion of their natural defenses against getting CVD [26].65% of people with diabetes have CVDs identified as the reason of death [27]. Diabetes is a standalone risk factor for numerous types of CVD such as heart attacks, strokes, and peripheral artery disease. These disorders are facilitated by high blood sugar levels as well as additional risk factors like high blood pressure and high cholesterol [28].
Kidney Complications, Possibly the most significant site of microvascular damage in diabetes is the kidney [29]. Due to their condition and/or additional co-morbidities including hypertension and nephron loss brought on by aging, a significant portion of people with diabetes will acquire kidney disease [30]. The prevalence and severity of chronic kidney disease (CKD) can be used to identify those who are more likely to experience unfavorable health outcomes and die young [31].
Nerve Complications, Diabetic neuropathy is one of the most common complications of diabetes [32-34]. The result of persistent hyperglycemia, a downstream metabolic cascade that involves increased polyol pathway flux, increased formation of advanced glycation end products, excessive cytokine release, activated protein kinase C, exaggerated oxidative stress, and other confounding factors results in peripheral nerve injury
Eye Complications, The most common and distinctive microvascular consequence of diabetes is diabetic retinopathy, which continues to be the dominant factor in avoidable blindness in persons in their working years[35]. It is identified in a third of people with diabetes and associated with higher risk of fatal systemic vascular consequences such stroke, coronary heart disease, and heart failure. For reducing the risk of retinopathy development and progression, optimal regulation of blood pressure, blood sugar, and perhaps blood lipids must still be maintained[36].
Increased risk of infection: Patients with diabetes mellitus are more likely to get infectious infections, which could lead to an increase in morbidity [37]. The hyperglycemic environment that promotes immune dysfunction (such as damage to neutrophil function, depression of the antioxidant system, and humoral immunity), micro- and microangiopathies, neuropathy, decrease in the antibacterial activity of urine, gastrointestinal and urinary dysmotility, and greater number of medical interventions in these patients is what leads to the higher frequency of infections in diabetic patients[38] [39]. Mental health issue, the ongoing stress of treating diabetes might exacerbate mental health issues or leave one feeling anxious, depressed, or overwhelmed. According to the Centers for Disease Control and Prevention (CDC), one-third to half of diabetics report diabetes-related anxiety over an 18-month period [40].
Effects of diabetes on intimate health:
Diabetes can have a significant impact on sexual function as diabetes effects nerve and blood Vessel. However, the pathophysiology of ED in diabetes is multifactorial, which includes both psychological and organic factors (which play major roles in ED). This condition can affect both men and women, resulting in such problems as erectile dysfunction in men and decreased arousal and lubrication in women [41]. Diabetes also leads to imbalance of sexual hormones which might affect the sexual desire in both male and female. This could results reduced sexual activity [42]. Women with diabetes experience vaginal dryness due to impairment of blood supply and nerve damage in the vagina which ultimately cause the painful or uncomfortable sexual intercourse and make the intimacy challenging [43]. People with diabetes are more susceptible to infections. Due to the high blood sugar the vaginal pH has been changed and which allow yeast and bacteria to grow and causes vaginal infection. Women with vaginal infection are suffering for whitish and foul vaginal smell which can cause discomfort during sexual intercourse [44]. Diabetes leads to emotional imbalance such as anxiety, depression, and self-esteem issues which can further impact sexual well-being[45]. Due to diabetic autonomic neuropathy the sensation in the vagina and penis is reduced which contribute difficulties achieving arousal and orgasm [46]. Diabetes also leads to urinary incontinence which may cause embarrassment and limiting sexual activity. Men and women suffering from diabetes also experience infertility. In man the sperm movement reduce while diabetes causes ovulation defect in women [46, 47].
Erectile Dysfunction: Causes and Symptoms:
Erectile dysfunction also known to as “impotence,” referred to consistent and recurrent inability of a man to achieve and maintain an erection sufficient for satisfactory sexual activity. It is frequently linked to a confluence of emotional, psychological, and physical causes. Physical disorders like diabetes, cardiovascular disease, high blood pressure, obesity, hormone imbalances, nerve damage, and some drugs can all have an impact on ED [48]. Multiple sclerosis, Parkinson's disease, and injuries to the spinal column or pelvic region are examples of neurological conditions that might interfere with erection-inducing nerve signals [49]. Certain medication such as antihypertensive eg, Hydrochlorothiazide- Benazepril, Chlorthalidone, etc, Antidepressants, anti-anxiety drugs, and antiepileptic drugs eg, Fluoxetine, Tranylcypromine etc, Antihistamines, Non-steroidal anti-inflammatory drugs, Parkinson's disease medications, Antiarrythmics, Histamine H2-receptor antagonists, Muscle relaxants, Prostate cancer medications, Chemotherapy drugs are involved in ED [50]. Unhealthy life style such as, Smoking, inactivity, poor diet, being overweight or obese, metabolic syndrome, and binge drinking are all modifiable risk factors for ED [51-53]. Stress and anxiety are mental health issues that can impact how the brain communicates with the body to cause a physical response. Stress and anxiety can prevent the brain from communicating with the penis to allow for increased blood flow during an erection [54].
Symptoms of ED:
ED may be a serious indicator that a man's vascular system is becoming obstructed, which is a sign of cardiovascular disease. According to several research, men with ED are significantly more likely to get a heart attack, a stroke, or leg circulation issues. The most common symptoms of ED are difficulty of achieving or maintaining erection firm enough for sexual activity. Due to stress and heightened sensitivity, ED can occasionally cause premature ejaculation. Reduced sexual desire is another symptom of ED [55].
The Interplay of Diabetes and Erectile Dysfunction:
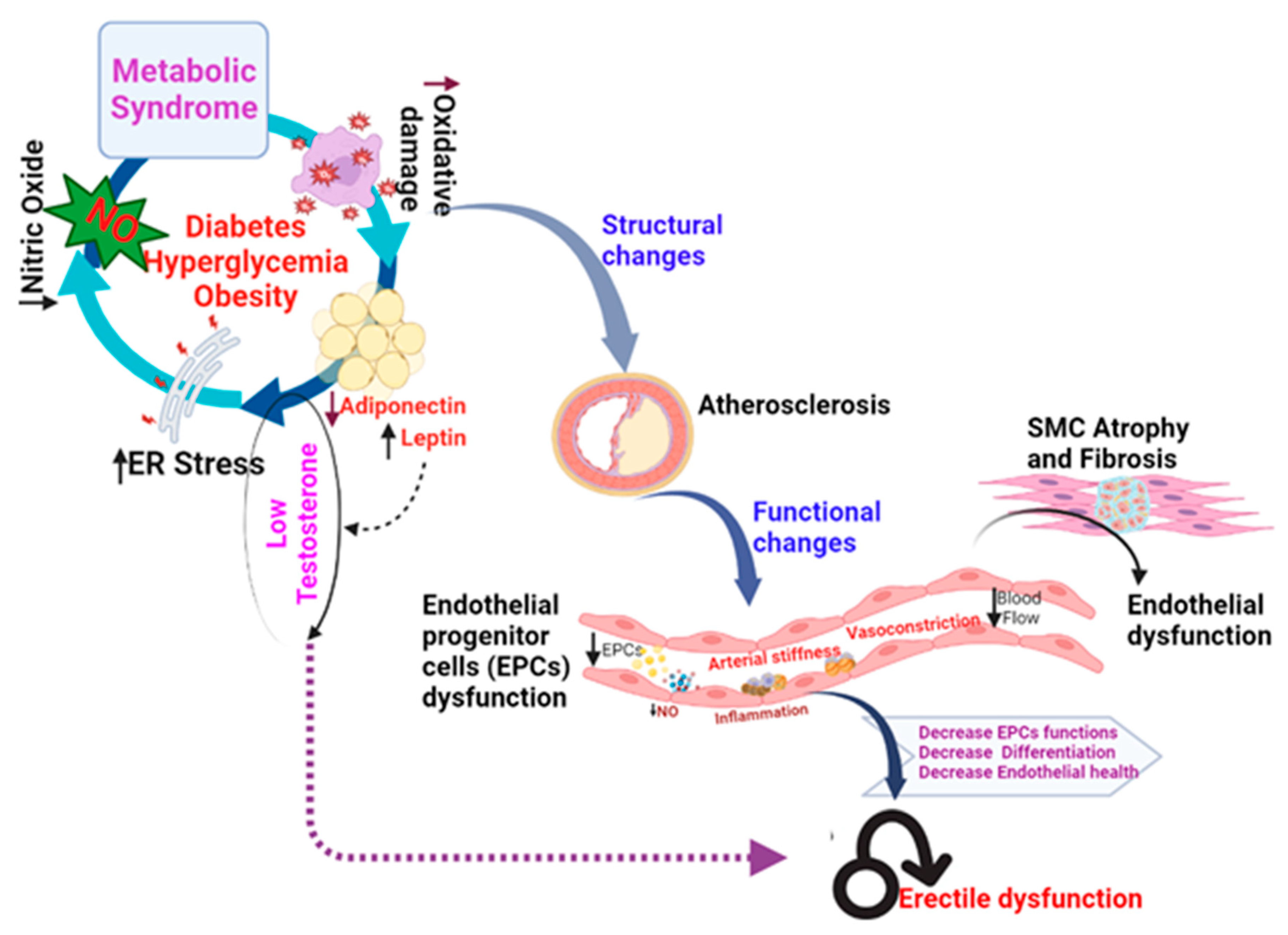
The pathophysiology of ED (Figure 2) in diabetes is multifaceted and is influenced by both psychological and organic variables (which are key contributors to ED), as well as psychological and relational problems, which frequently overlap. Visceral obesity, neuropathy, insulin resistance, and hypogonadism are examples of the postulated mechanisms of ED in diabetic individuals [56].
Vascular Damage:
Diabetic vasculopathy includes macroangiopathy, microangiopathy, and endothelial dysfunction.
Microvascular Damage, diabetes has the potential to harm the smaller blood vessels, which includes the penis. The blood flow to the erectile tissues is decreased as a result of this microvascular injury, making it challenging to obtain and maintain an erection [57]. Atherosclerosis, a disorder in which cholesterol and other chemicals build up in the walls of arteries, narrowing them and limiting blood flow, can be brought on by high blood sugar levels. This decreased blood supply to the penile arteries might make it more difficult to get and keep an erection[53, 58, 59] .Endothelial dysfunction, is the term used to describe a variety of clinical disorders, such as altered anticoagulation and anti-inflammatory actions, poor control of vascular development, and dysregulated vascular remodeling. When endothelium-dependent smooth muscle relaxation declines as a result of decreased or increased nitric oxide (NO) bioactivity in the vasculature, this condition is known as endothelial dysfunction[60-62].
Neural Damage:
Diabetic Peripheral Neuropathy:
It is still unknown exactly how DPN works. But in both type 1 and type 2 diabetes, hyperglycemia is typically recognized as the root cause of DPN. Numerous putative pathways that might aid in the development of DPN are mentioned in recent literature. Reactive oxygen species (ROS) [63], damage to the microvasculature, a reduction in neurotrophic factors, a reduction in the blood flow to the nerves , a reduction in the integrity of the neurons, a reduction in the speed of nerve conduction, and nerve energy failure are all caused by excessive intracellular glucose accumulation[64, 65]. A group of researcher from Johns Hopkins University School of Medicine, did a study titled as, Association of Peripheral Neuropathy with Erectile Dysfunction in US Men observed, There was a significant association of peripheral neuropathy with erectile dysfunction [66]. S Furukawa et al, did a Dogo study with Japanese patients aged <65 years with type 2 diabetes mellitus, the prevalence values of diabetic neuropathy and severe ED were 47.0 and 39.0%, respectively [67].
Diabetic Autonomic Neuropathy:
Diabetes mellitus patients frequently develop diabetic autonomic neuropathy (DAN), a kind of neuropathy marked by dysfunction brought on by damage to peripheral autonomic nerves. The cardiovascular, gastrointestinal, genitourinary, sudomotor and vasomotor, and neuroendocrine systems are only a few of the many organ systems that may be affected by a wide range of symptoms [46]. Autonomic nerves control involuntary functions, including the relaxation of smooth muscles in the penis during arousal. Diabetes-related autonomic neuropathy can disrupt this process, making it challenging for the penis to fill with blood and achieve an erection. R. Quadri et al, conduct a human study and observed, DAN is associated with severe ED [68, 69]. A group of researcher from University of Michigan, observed men with type 1 diabetes with autonomic neuropathy, observed ED [70].
Neurotransmitter Imbalance:
Blood flow during erection and detumescence is regulated by peripheral neurotransmitters that are released from sympathetic (noradrenaline, ATP) and parasympathetic (acetylcholine, nitric oxide, and vasoactive intestinal peptide) nerves entering the corpora cavernosa, corpus spongiosum, and glans penis [71]. Dopamine, nitric oxide, glutamate, acetylcholine, oxytocin, ACTH, MSH, and pro-VGF are among the neurotransmitters that are involved in the central regulation of erection; other neurotransmitters include those that inhibit erection (such as noradrenaline, enkephalins, GABA, and endocannabinoids); or in case of serotonin both facilitate and inhibit erectile function [72]. Type 2 diabetes, characterized by insulin resistance, has been linked to dopamine imbalance. Kleinridders et al. observed that mice lacking the insulin receptor in the brain display decreased dopamine release in the striatum and involve disruption of dopaminergic pathways[73] .
Chronic Inflammation:
In diabetes due to continuous elevated blood glucose chronic inflammation develops. A complicated cascade of immunological reactions involving numerous immune cells, cytokines, and chemokines is set off by this prolonged hyperglycemia. Inflammatory mediator such as fibrinogen, C-reactive protein, interleukin (IL)-6, plasminogen activator inhibitor-1, sialic acid is involved in chronic inflammation in diabetic patient [74]. Although inflammation is a typical reaction to damage or infection, in people with diabetes, this response is dysregulated and contributes to the development of endothelial dysfunction, a sign of vascular dysfunctions [75]. Endothelial dysfunction is characterized by a complicated pathophysiology that is based on the uncoupling of endothelial nitric oxide synthase and the activation of endothelial cells in response to stimulation by numerous inflammatory mediators (molecular patterns, oxidized lipoproteins, and cytokines). These inflammatory reaction ultimately compromised the blood flow ability of the penile arteries, which ultimately resulting reduce the successful erection [76]. Moreover, chronic inflammatory mediators contribute damaging of the nerve cells which transport signals from penis to brain. As a result, neural communication required for initiating and maintaining an erection can be disrupted. In conclusion, persistent high blood glucose leads to chronic inflammation which creates a hostile environment that compromises both the vascular and neuronal components necessary for normal sexual performance [77].
Oxidative Stress:
Oxidative stress is a phenomenon caused by an imbalance between production and accumulation of oxygen reactive species (ROS) in cells and tissues that leads to biological system to detoxify these reactive products[5, 33, 78]. Although ROS are normally produced as by-products of oxygen metabolism and can play a number of physiological roles (including cell signaling), they are also greatly increased by xenobiotics such as antiblastic drugs and environmental stressors like UV, ionizing radiation, pollutants, and heavy metals. This imbalance results in cell and tissue damage (oxidative stress). The activation of the hexosamine pathway, nuclear factor-B (Nf-b), p38 mitogen-activated protein kinase (p38 MAPK), c-jun NH2 terminal kinase/stress-activated protein kinase (JNK/SAPK), or toll-like receptors (TLRs) results in the death of mitochondria under oxidative stress [79]. High glucose levels can cause cells to overproduce ROS, especially in the mitochondria. Oxidative stress leads to damage of DNA, lipids, protein and other cellular components. Oxidative stress is crucial in the setting of ED because it exacerbates the damage brought on by chronic inflammation [80]. Similar to chronic inflammation, oxidative stress damages endothelial cells directly and impairs their capacity to produce nitric oxide, which results in endothelial dysfunction. Furthermore, oxidative stress alters the ratio of ROS to antioxidants in blood vessels, favoring vasoconstriction (the narrowing of blood vessels), and decreasing the relaxation required for optimal blood flow during sexual excitement [81]. Additionally, oxidative stress directly affects nerves by damaging their myelin covering of the nerve. Oxidative stress can impede the coordination required to achieve an erection by interfering with the connection between the nerve cells involved in sexual response and the blood vessels of the penis [82].
Other risk factors that contribute to the ED:
Obesity:
Erectile dysfunction (ED) is usually linked to obesity, which is a serious global public health concern. An internal pathologic environment known as common soil may exist between the two disorders. Inflammation, oxidative stress, and the ensuing insulin and leptin resistance are their primary pathophysiologic mechanisms. Additionally, obesity and comorbid medical disorders, such as ED, are connected in terms of severity [83]. According to De Souza et al., rats with ED caused by high-calorie diets had endothelial damage. Obesity is a distinct risk factor for ED, according to a 14-year prospective research [84]. Fillo et al. observed, males with abdominal obesity had a higher incidence rate of ED, and the rate rose proportionally to the severity of obesity[85].
Smoking:
Cigarette smoking is the main preventable cause of disease and mortality. Smoking cigarettes can cause cardiovascular dysfunction and is now known to be a separate risk factor for the onset of erectile dysfunction, a more serious type of vascular disease. The NO pathway is involved in the signal transduction process causing ED that is well understood [86]. Smoke has been demonstrated to have an impact on both of the NOS isoforms that make up smoking, the neuronal and endothelial varieties [87]. Smoking harms blood vessels from the inside out, inhibiting elastic dilation even in the presence of potent paracrine signals. As a result of pathological elastic fiber calcification brought on by smoking, the extracellular matrix's elastin is changed, resulting in stiffer arteries [88].
Sedentary Lifestyle:
The onset of both ED and diabetes is frequently influenced by a sedentary lifestyle. Physical inactivity affects erectile function negatively, and exercise therapies in both experimental and clinical settings have been proven to enhance sexual responses and cardiovascular health in general [89]. Men who have symptoms of the metabolic syndrome have been reported to have improved erectile performance when eating a Mediterranean-style diet and consuming fewer calories. Additionally, it has been shown in both clinical and experimental studies that combining the two interventions improves erectile function further[90]. This additional benefit is probably due to a decrease in metabolic disturbances (such as inflammatory markers and insulin resistance), a reduction in visceral adipose tissue, and an improvement in vascular function (such as increased endothelial function) [90].
High Blood Pressure and Cardiovascular Disease:
Diabetes frequently comorbid with cardiovascular disease and high blood pressure (hypertension), which dramatically worsens ED[91]. The endothelium may become unable to provide the required dilatation in the penile vascular bed in response to sexual arousal, generating persistent impairment in erection, which appears to be the link between both disorders. On the other hand, there is still room for debate regarding the true impact of antihypertensive medications on erectile function[92]. Some studies have indicated that men with vasculogenic ED who lack conventional risk factors also have vascular disease, demonstrating the importance of ED as a clinical early cardiovascular risk sign [93].
Psychological Factors:
Even though they are unrelated to diabetes, psychological elements including stress, anxiety, and depression can exacerbate the effects of ED [94]. Depression, anxiety, and other stress-related emotions are viewed as cognitive interferences that prevent sexual arousal by diverting focus away from erotic stimuli. Enhancing attentional focus on sexual cues and reducing distractions like worry, conflict, or other pressures are the objectives of sex therapy[95].
Strategies for Managing and Preventing Erectile Dysfunction in Diabetic Individuals:
Medications and treatments for ED:
For erectile dysfunction (ED), there are many treatment options, ranging from minimally invasive techniques to more invasive treatments.
Oral Medications (Phosphodiesterase type 5 inhibitors - PDE5 inhibitors):
The four oral PDE5 inhibitors that are commercially accessible in the United States are tadalafil (Cialis, Eli Lilly), sildenafil (Viagra, Pfizer), vardenafil (Levitra and Staxyn, Bayer/GlaxoSmithKline), and avanafil (Stendra, Vivus), a medication that was just recently licensed. Although they can cause adverse effects like headaches, flushing, nasal congestion, and digestive problems, they are mostly safe and effective [96].
Penile Injection:
Injections of platelet-rich plasma (PRP) and stem cell therapy (SCT) are two suggested restorative therapies for these issues. SCT includes the collection of mesenchymal stem cells or stromal vascular fractions from various tissue sources and their injection. PRP is created autologously from a patient's plasma and then administered by injection into the penile tissue. According to studies in basic science, these treatments restore damaged penile tissue and encourage both new cellular and vascular growth. Human studies on SCT[65] and PRP for PD and ED have produced encouraging outcomes with minor negative effects [97].
Vacuum Erection Devices (VEDs):
Vacuum erection devices (VED) are nonsurgical, noninvasive, conservative methods of treating erectile dysfunction (ED). To keep the erection, a constriction ring is positioned at the base of the penis. Men who choose a non-medication approach or those who have not responded well to previous treatments may find that VEDs are an effective alternative [98].
Intraurethral Suppositories:
A suppository that is placed into the urethra known as alprostadil. The drug promotes blood flow to the penis by being absorbed through the urethral lining. This technique, which is similar to injections, can be successful but can also result in little discomfort or a burning sensation [99].
Natural Therapies:
Numerous natural products claiming to revive erection and sexual vitality are available to consumers. Most naturally occurring substances lack sufficient clinical trials to establish efficacy, according to an analysis of the empirical data that is currently available [100, 101]. However, there is some evidence that arginine, yohimbine, Panax ginseng, Maca, and Ginkgo biloba may be beneficial for erectile dysfunction [102, 103].
Surgical Interventions:
Penile Implants: Inflatable or semi-rigid implants are surgically placed within the penis. They provide the person control over the erection's timing and length. Vascular Surgery: When inadequate blood flow to the penis is the main cause of ED, surgical treatments can be performed to enhance blood flow there. Venous Ligation Surgery: This procedure involves cutting off veins that let blood exit the penis, which helps to keep an erection in place.
Management of ED in diabetic patient:
Maintaining optimal blood sugar control is the key to reducing the risk of Erectile Dysfunction in individuals with diabetes. By keeping normal blood sugar improve blood flow, safeguard the health of your blood vessels, and lower your risk of ED. Losing weight is highly advised to enhance erectile function since it can raise testosterone levels primarily by enhancing testicular function and decreasing the conversion of testosterone to oestradiol via aromatase activity in adipose tissue[104]. Physical inactivity is one of the most crucial reversible risk factors. Through many mechanisms including the regulation of arterial pressure, the synthesis of nitric oxide, the hormone system, and the metabolism of glucose and lipids, regular exercise has been demonstrated to improve erectile function. Additionally, studies demonstrate that exercise and the common medications for the treatment of impotence work together synergistically [105, 106].
Conclusion:
Physical and psychological variables interact in a complex way in the connection between diabetes and erectile dysfunction (ED). Diabetes has a major negative effect on vascular and brain health, which helps to cause and advance ED. This review emphasizes and affirms the significance of effectively managing DM patients who are having ED, emphasizing the importance of comorbidities with diabetes responsible for ED. Targeted treatment for enhanced erectile function may be possible with an understanding of the many causes of ED in T2DM patients.
References
- PAHO/WHO and P. A. H. Organization, "Sexual and Reproductive Health," 2002.
- S. Gruskin, V. Yadav, A. Castellanos-Usigli, G. Khizanishvili, and E. Kismödi, "Sexual health, sexual rights and sexual pleasure: meaningfully engaging the perfect triangle," (in en). [CrossRef]
- "Diabetes Quick Facts | Basics | Diabetes | CDC," 2022-09-21T01:30:51Z 2022.
- M. M. Mohib et al., "Protective role of green tea on diabetic nephropathy—A review," (in en), , 2016. Available online: http://www.editorialmanager.com/cogentbio.
- M. MS et al., "Glucagon Prevents Cytotoxicity Induced by Methylglyoxal in a Rat Neuronal Cell Line Model," Biomolecules, vol. 11, no. 2, 02/15/2021 2021. [CrossRef]
- "CDC Global Health - Infographics - World Diabetes Day," 2020-01-13T03:23:26Z 2020.
- "Diabetes - PAHO/WHO | Pan American Health Organization," 2022.
- M. MS et al., "Glucagon-Like Peptide-1 Receptor Agonist Protects Dorsal Root Ganglion Neurons against Oxidative Insult," Journal of diabetes research, vol. 2019, 02/21/2019 2019. [CrossRef]
- F. Cosentino and G. E. Assenza, "Diabetes and inflammation," (in eng), Herz, vol. 29, no. 8, pp. 749-59, Dec 2004. [CrossRef]
- W. K, K. C, and F. J, "Sexual health and function in women with diabetes," Diabetic medicine : a journal of the British Diabetic Association, vol. 38, no. 11, 2021 Nov 2021. [CrossRef]
- D. Association. "Sex and Diabetes | ADA.". Available online: https://diabetes.org/healthy-living/sexual-health/sex-diabetes.
- R. RC, W. R, S. S, and G. N, "Epidemiology of erectile dysfunction: the role of medical comorbidities and lifestyle factors," The Urologic clinics of North America, vol. 32, no. 4, 2005 Nov 2005. [CrossRef]
- K. Y et al., "High prevalence of erectile dysfunction in diabetes: a systematic review and meta-analysis of 145 studies," Diabetic medicine : a journal of the British Diabetic Association, vol. 34, no. 9, 2017 Sep 2017. [CrossRef]
- T. D, B. DS, S. VK, P. AK, and Y. BK, "Association Between Erectile Dysfunction and Type 2 Diabetes Mellitus," Journal of Nepal Health Research Council, vol. 19, no. 2, 09/06/2021 2021. [CrossRef]
- C. G, G. CB, C. D, G. P, and N. E, "Sexual dysfunction at the onset of type 2 diabetes: the interplay of depression, hormonal and cardiovascular factors," The journal of sexual medicine, vol. 11, no. 8, 2014 Aug 2014. [CrossRef]
- W. X, Y. X, C. Y, W. S, and W. W, "High Prevalence of Erectile Dysfunction in Diabetic Men With Depressive Symptoms: A Meta-Analysis," The journal of sexual medicine, vol. 15, no. 7, 2018 Jul 2018. [CrossRef]
- F. D et al., "Erectile dysfunction in diabetic subjects in Italy. Gruppo Italiano Studio Deficit Erettile nei Diabetici," Diabetes care, vol. 21, no. 11, 1998 Nov 1998. [CrossRef]
- T. CC and P. LH, "Update on diabetes classification," The Medical clinics of North America, vol. 99, no. 1, 2015 Jan 2015. [CrossRef]
- C. A and J. FR, "[Classification of diabetes: an increasing heterogeneity]," Revue medicale suisse, vol. 11, no. 477, 06/03/2015 2015.
- A. N, A. F, B. MJ, M. M, G. F, and K. IJ, "Gestational diabetes insipidus: a review of an underdiagnosed condition," Journal of obstetrics and gynaecology Canada : JOGC = Journal d'obstetrique et gynecologie du Canada : JOGC, vol. 32, no. 3, 2010 Mar 2010. [CrossRef]
- C. A and P. F, "Variability of risk factors and diabetes complications," Cardiovascular diabetology, vol. 20, no. 1, 05/07/2021 2021. [CrossRef]
- B. T et al., "Epigenetic basis of diabetic vasculopathy," Frontiers in endocrinology, vol. 13, 12/09/2022 2022. [CrossRef]
- W. PW, D. A. RB, L. D, B. AM, S. H, and K. WB, "Prediction of coronary heart disease using risk factor categories," Circulation, vol. 97, no. 18, 05/12/1998 1998. [CrossRef]
- Sjoholm and T. Nystrom, "Endothelial inflammation in insulin resistance," (in eng), Lancet, vol. 365, no. 9459, pp. 610-2, Feb 12-18 2005. [CrossRef]
- M. HC and M. CA, "Determinants of atherosclerosis in the young. Pathobiological Determinants of Atherosclerosis in Youth (PDAY) Research Group," The American journal of cardiology, vol. 82, no. 10B, 11/26/1998 1998. [CrossRef]
- B. V and P. I, "Coronary heart disease risk factors in women," European heart journal, vol. 15, no. 11, 1994 Nov 1994. [CrossRef]
- D. Deshpande, P. AD Deshpande, MPH, is Research Assistant Professor, Division of Health Behavior Research, Department of Medicine, Washington University School of Medicine, St Louis, MO 63110 (USA). At the time of manuscript preparation and submission, Dr Deshpande was Assistant Professor, Department of Community Health, Saint Louis University School of Public Health, St Louis, Missouri., M. Harris-Hayes, P. M Harris-Hayes, DPT, OCS, is Assistant Professor, Program in Physical Therapy, Washington University School of Medicine., M. Schootman, and P. M Schootman, is Associate Professor, Division of Health Behavior Research, Department of Medicine, Washington University School of Medicine., "Epidemiology of Diabetes and Diabetes-Related Complications," Physical Therapy, vol. 88, no. 11, pp. 1254-1264, 2023. [CrossRef]
- S. PH et al., "The effect of diabetes mellitus on prognosis and serial left ventricular function after acute myocardial infarction: contribution of both coronary disease and diastolic left ventricular dysfunction to the adverse prognosis. The MILIS Study Group," Journal of the American College of Cardiology, vol. 14, no. 1, 1989 Jul 1989. [CrossRef]
- B. G et al., "Estimated glomerular filtration rate, albuminuria and mortality in type 2 diabetes: the Casale Monferrato study," Diabetologia, vol. 50, no. 5, 2007 May 2007. [CrossRef]
- T. MC, W. AJ, B. OJ, C. ME, and M. TH, "The burden of chronic kidney disease in Australian patients with type 2 diabetes (the NEFRON study)," The Medical journal of Australia, vol. 185, no. 3, 08/07/2006 2006. [CrossRef]
- D. JP, P. HH, H. LG, R. M, R. G, and L. JB, "Renal Dysfunction in the Presence of Normoalbuminuria in Type 2 Diabetes: Results from the DEMAND Study," Cardiorenal medicine, vol. 2, no. 1, 2012 Feb 2012. [CrossRef]
- M. S. Mohiuddin et al., "Glucagon Prevents Cytotoxicity Induced by Methylglyoxal in a Rat Neuronal Cell Line Model," Biomolecules, vol. 11, no. 2, 2021. [CrossRef]
- M. Mohabbulla Mohib et al., "Protective role of green tea on diabetic nephropathy—A review," Cogent Biology, vol. 2, no. 1, p. 1248166, 2016/12/31 2016. [CrossRef]
- M. Motegi et al., "Deficiency of glucagon gene-derived peptides induces peripheral polyneuropathy in mice," Biochem Biophys Res Commun, vol. 532, no. 1, pp. 47-53, 10/29/2020 2020. [CrossRef]
- L. KY, H. WH, L. YB, W. CY, and C. TJ, "Update in the epidemiology, risk factors, screening, and treatment of diabetic retinopathy," Journal of diabetes investigation, vol. 12, no. 8, 2021 Aug 2021. [CrossRef]
- C. N, M. P, and W. TY, "Diabetic retinopathy," Lancet (London, England), vol. 376, no. 9735, 07/10/2010 2010. [CrossRef]
- K. S, "Diabetes and infection: is there a link?--A mini-review," Gerontology, vol. 59, no. 2, 2013 2013. [CrossRef]
- G. H, "[Infection and diabetes]," La Revue de medecine interne, vol. 14, no. 1, 1993 Jan 1993. [CrossRef]
- J. Casqueiro, J. Casqueiro, and C. Alves, "Infections in patients with diabetes mellitus: A review of p... : Indian Journal of Endocrinology and Metabolism," 2023. [CrossRef]
- CDCgov, "Diabetes and Mental Health | CDC," 2023-05-15T09:11:07Z 2023.
- C. Rask-Madsen and G. L. King, "Vascular complications of diabetes: mechanisms of injury and protective factors," (in eng), Cell Metab, vol. 17, no. 1, pp. 20-33, Jan 08 2013. [CrossRef]
- B. MEH, K. EKH, S. RB, S. E, and H. A, "Sexual dysfunction in women with type 1 diabetes in Norway: A qualitative study of women's experiences," Diabetic medicine : a journal of the British Diabetic Association, vol. 39, no. 7, 2022 Jul 2022. [CrossRef]
- S. A and R. U, "Intimacy and women with type 2 diabetes: an exploratory study using focus group interviews," The Diabetes educator, vol. 29, no. 4, 2003 Jul-Aug 2003. [CrossRef]
- L. Mohammed, G. Jha, I. Malasevskaia, H. K. Goud, and A. Hassan, "The Interplay Between Sugar and Yeast Infections: Do Diabetics Have a Greater Predisposition to Develop Oral and Vulvovaginal Candidiasis?," (in en), Cureus, vol. 13, 2021/02/18 2021. [CrossRef]
- A. Bickett and H. Tapp, "Anxiety and diabetes: Innovative approaches to management in primary care," (in en), https://doi.org/10.1177/1535370216657613, research-article 2016-07-06 2016. [CrossRef]
- A.-M. N, P.-B. R, W. H, and S. AV, "Autonomic neuropathy and urologic complications in diabetes," Autonomic neuroscience : basic & clinical, vol. 229, 2020 Dec 2020. [CrossRef]
- D. GL et al., "The effects of diabetes on male fertility and epigenetic regulation during spermatogenesis," Asian journal of andrology, vol. 17, no. 6, 2015 Nov-Dec 2015. [CrossRef]
- S. R and G. H, "Erectile dysfunction," Lancet (London, England), vol. 381, no. 9861, 01/12/2013 2013. [CrossRef]
- F. JF et al., "Combined Transplantation of Mesenchymal Stem Cells and Endothelial Progenitor Cells Restores Cavernous Nerve Injury-Related Erectile Dysfunction," The journal of sexual medicine, vol. 15, no. 3, 2018 Mar 2018. [CrossRef]
- T.-P. D, I. N, R. K, and V. C, "Interactions between erectile dysfunction, cardiovascular disease and cardiovascular drugs," Nature reviews. Cardiology, vol. 19, no. 1, 2022 Jan 2022. [CrossRef]
- R. Ng et al., "Smoking, drinking, diet and physical activity—modifiable lifestyle risk factors and their associations with age to first chronic disease," International Journal of Epidemiology, vol. 49, no. 1, pp. 113-130, 2023. [CrossRef]
- C. M, R. A, B. PS, B. F, and K. A, "Direct actions of adiponectin on changes in reproductive, metabolic, and anti-oxidative enzymes status in the testis of adult mice," General and comparative endocrinology, vol. 279, 08/01/2019 2019. [CrossRef]
- C. M, R. A, B. PS, and K. A, "Protective role of adiponectin against testicular impairment in high-fat diet/streptozotocin-induced type 2 diabetic mice," Biochimie, vol. 168, 2020 Jan 2020. [CrossRef]
- R. Velurajah, O. Brunckhorst, M. Waqar, I. McMullen, and K. Ahmed, "Erectile dysfunction in patients with anxiety disorders: a systematic review," (in En), International Journal of Impotence Research, OriginalPaper vol. 34, no. 2, pp. 177-186, 2021-02-18 2021. [CrossRef]
- @mayoclinic, "Erectile dysfunction - Symptoms and causes," 2023.
- M. I. Maiorino, G. Bellastella, and K. Esposito, "Diabetes and sexual dysfunction: current perspectives," (in English), Diabetes, Metabolic Syndrome and Obesity, vol. 7, pp. 95-105, 2023. [CrossRef]
- F. C, K. A, I. K, D. P, K. M, and D. K, "Microvascular Complications of Type 2 Diabetes Mellitus," Current vascular pharmacology, vol. 18, no. 2, 2020 2020. [CrossRef]
- A. Ponholzer et al., "Is penile atherosclerosis the link between erectile dysfunction and cardiovascular risk? An autopsy study," (in En), International Journal of Impotence Research, OriginalPaper vol. 24, no. 4, pp. 137-140, 2012-03-22 2012. [CrossRef]
- D. W, C. M, P. S, S. HA, and O. L, "Adipocyte CAMK2 deficiency improves obesity-associated glucose intolerance," Molecular metabolism, vol. 53, 2021 Nov 2021. [CrossRef]
- M. DB, C. HC, and K. PJ, "Pharmacologic management of peripheral vascular disease," The Surgical clinics of North America, vol. 78, no. 3, 1998 Jun 1998. [CrossRef]
- M. Choubey. "Growth Hormone and Insulin-like Growth Factor-I: Novel Insights into the Male Reproductive Health." https://scholar.google.com/citations?view_op=view_citation&hl=en&user=-oBBDNsAAAAJ&citation_for_view=-oBBDNsAAAAJ:ye4kPcJQO24C.
- A. Ranjan, M. Choubey, T. Yada, and A. Krishna, "Immunohistochemical localization and possible functions of nesfatin-1 in the testis of mice during pubertal development and sexual maturation," (in En), Journal of Molecular Histology, OriginalPaper vol. 50, no. 6, pp. 533-549, 2019-09-20 2019. [CrossRef]
- V. AM, M. LL, B. C, and F. EL, "Short-term hyperglycemia produces oxidative damage and apoptosis in neurons," FASEB journal : official publication of the Federation of American Societies for Experimental Biology, vol. 19, no. 6, 2005 Apr 2005. [CrossRef]
- F. EL, N. KA, J. TS, and B. DLH, "New Horizons in Diabetic Neuropathy: Mechanisms, Bioenergetics, and Pain," Neuron, vol. 93, no. 6, 03/22/2017 2017. [CrossRef]
- S. Akter, M. Choubey, M. M. Mohib, S. Arbee, M. A. T. Sagor, and M. S. Mohiuddin, "Stem Cell Therapy in Diabetic Polyneuropathy: Recent Advancements and Future Directions," (in en), Brain Sciences, Review vol. 13, no. 2, p. 255, 2023-02-02 2023. [CrossRef]
- M. Caitlin W. Hicks, MS Dan Wang, MS B. Gwen Windham, MD, MHS Elizabeth Selvin, PhD, MPH, "Association of Peripheral Neuropathy with Erectile Dysfunction in US Men - The American Journal of Medicine," 2020. [CrossRef]
- F. S et al., "Diabetic peripheral neuropathy and prevalence of erectile dysfunction in Japanese patients aged," International journal of impotence research, vol. 29, no. 1, 2017 Jan 2017. [CrossRef]
- Q. R et al., "Autonomic neuropathy and sexual impotence in diabetic patients: analysis of cardiovascular reflexes," Andrologia, vol. 21, no. 4, 1989 Jul-Aug 1989. [CrossRef]
- S. A, C. M, B. P, and K. A, "Adiponectin and Chemerin: Contrary Adipokines in Regulating Reproduction and Metabolic Disorders," Reproductive sciences (Thousand Oaks, Calif.), vol. 25, no. 10, 2018 Oct 2018. [CrossRef]
- R. Pop-Busui et al., "Cardiovascular Autonomic Neuropathy, Erectile Dysfunction and Lower Urinary Tract Symptoms in Men with Type 1 Diabetes: Findings from the DCCT/EDIC," (in EN), research-article 2015-06 2015. [CrossRef]
- A. KE, "Mechanisms of penile erection and basis for pharmacological treatment of erectile dysfunction," Pharmacological reviews, vol. 63, no. 4, 2011 Dec 2011. [CrossRef]
- M. R. Melis, F. Sanna, and A. Argiolas, "Dopamine, Erectile Function and Male Sexual Behavior from the Past to the Present: A Review," (in en), Brain Sciences, Review vol. 12, no. 7, p. 826, 2022-06-24 2022. [CrossRef]
- K. A et al., "Insulin resistance in brain alters dopamine turnover and causes behavioral disorders," Proceedings of the National Academy of Sciences of the United States of America, vol. 112, no. 11, 03/17/2015 2015. [CrossRef]
- S. Tsalamandris, "The Role of Inflammation in Diabetes: Current Concepts and Future Perspectives," 2023. [CrossRef]
- M. Y. Donath and S. E. Shoelson, "Type 2 diabetes as an inflammatory disease," (in En), Nature Reviews Immunology, ReviewPaper vol. 11, no. 2, pp. 98-107, 2011-01-14 2011. [CrossRef]
- P. Theofilis et al., "Inflammatory Mechanisms Contributing to Endothelial Dysfunction," (in en), Biomedicines, Review vol. 9, no. 7, p. 781, 2021-07-06 2021. [CrossRef]
- R. Dantzer, "Neuroimmune Interactions: From the Brain to the Immune System and Vice Versa," (in en), https://doi.org/10.1152/physrev.00039.2016, review-article 2017 Dec 20 2017. [CrossRef]
- M. S. Mohiuddin et al., "Glucagon-Like Peptide-1 Receptor Agonist Protects Dorsal Root Ganglion Neurons against Oxidative Insult," (in eng), J Diabetes Res, vol. 2019, p. 9426014, 2019. [CrossRef]
- M. Wronka, J. Krzemińska, E. Młynarska, J. Rysz, and B. Franczyk, "The Influence of Lifestyle and Treatment on Oxidative Stress and Inflammation in Diabetes," (in en), International Journal of Molecular Sciences, Review vol. 23, no. 24, p. 15743, 2022-12-12 2022. [CrossRef]
- Y. P et al., "Liraglutide Ameliorates Erectile Dysfunction via Regulating Oxidative Stress, the RhoA/ROCK Pathway and Autophagy in Diabetes Mellitus," Frontiers in pharmacology, vol. 11, 08/12/2020 2020. [CrossRef]
- R. S et al., "Environmental Factors-Induced Oxidative Stress: Hormonal and Molecular Pathway Disruptions in Hypogonadism and Erectile Dysfunction," Antioxidants (Basel, Switzerland), vol. 10, no. 6, 05/24/2021 2021. [CrossRef]
- M. Taskiran, H. P. H. Department of Urology, Gaziantep 34010, Turkey, K. Dogan, and F. o. M. Department of Urology, Istinye University, Istanbul 34010, Turkey, "The efficacy of systemic inflammatory response and oxidative stress in erectile dysfunction through multi-inflammatory index: a prospective cross-sectional analysis," The Journal of Sexual Medicine, vol. 20, no. 5, pp. 591-596, 2023. [CrossRef]
- S. Y. P. Ki Hak Moon, Yong Woon Kim, "Obesity and Erectile Dysfunction: From Bench to Clinical Implication," World J Mens Health, no. 37(2), pp. 138-147, 2019. [CrossRef]
- d. S. ILL et al., "Hypercaloric Diet Establishes Erectile Dysfunction in Rat: Mechanisms Underlying the Endothelial Damage," Frontiers in physiology, vol. 8, 10/04/2017 2017. [CrossRef]
- F. J, L. M, O. M, B. J, and L. P, "Importance of Different Grades of Abdominal Obesity on Testosterone Level, Erectile Dysfunction, and Clinical Coincidence," American journal of men's health, vol. 11, no. 2, 2017 Mar 2017. [CrossRef]
- J. R. Kovac, Labbate, C., Ramasamy, R., Tang, D. and Lipshultz, L.I. (2015). Effects of cigarette smoking on erectile dysfunction. [CrossRef]
- X. Y, G. H, N. C, R. J, and G.-C. NF, "Effect of long-term passive smoking on erectile function and penile nitric oxide synthase in the rat," The Journal of urology, vol. 157, no. 3, 1997 Mar 1997. [CrossRef]
- X. Guo, M. J. Oldham, M. T. Kleinman, R. F. Phalen, and G. S. Kassab, "Effect of cigarette smoking on nitric oxide, structural, and mechanical properties of mouse arteries," (in en), https://doi.org/10.1152/ajpheart.00376.2006, research-article 2006 Nov 01 2006. [CrossRef]
- G. H, L. CM, G. C, and A. J. K, "Physical Activity to Improve Erectile Function: A Systematic Review of Intervention Studies," Sexual medicine, vol. 6, no. 2, 2018 Jun 2018. [CrossRef]
- H. JL, M. MT, K. M, and A. MA, "Beneficial impact of exercise and obesity interventions on erectile function and its risk factors," The journal of sexual medicine, vol. 6 Suppl 3, 2009 Mar 2009. [CrossRef]
- A. A. de Oliveira, D. o. B. a. C. E. a. S. Laboratory of Vascular Physiology, Florida Institute of Technology, Melbourne, Florida, USA, K. P. Nunes, and D. o. B. a. C. E. a. S. Laboratory of Vascular Physiology, Florida Institute of Technology, Melbourne, Florida, USA, "Hypertension and Erectile Dysfunction: Breaking Down the Challenges," American Journal of Hypertension, vol. 34, no. 2, pp. 134-142, 2023. [CrossRef]
- V. M et al., "Update of the position paper on arterial hypertension and erectile dysfunction," Journal of hypertension, vol. 38, no. 7, 2020 Jul 2020. [CrossRef]
- H.-C. J, B.-G. V, Z. P, and C. A, "Understanding Erectile Dysfunction in Hypertensive Patients: The Need for Good Patient Management," Vascular health and risk management, vol. 28, no. 2, 2001 May 2001. [CrossRef]
- R. RC, "Psychogenic erectile dysfunction. Classification and management," The Urologic clinics of North America, vol. 28, no. 2, 20. [CrossRef]
- S. AD, "Psychologic factors in the multidisciplinary evaluation and treatment of erectile dysfunction," The Urologic clinics of North America, vol. 15, no. 1, 1988 Feb 1988.
- D. H. W. Lau, S. Kommu, F. H. Mumtaz, R. J. Morgan, C. S. Thompson, and D. P. Mikhailidis, "The Management of Phosphodiesterase-5 (PDE5) Inhibitor Failure," Current Vascular Pharmacology, vol. 4, no. 2, pp. 89-93, 2023. [CrossRef]
- A. MH, T. N, and C. S, "Platelet-Rich Plasma Injections for Erectile Dysfunction and Peyronie's Disease: A Systematic Review of Evidence," Sexual medicine reviews, vol. 10, no. 2, 2022 Apr 2022. [CrossRef]
- K. S, C. MC, C. SY, C. H, and R. MR, "Novel Emerging Therapies for Erectile Dysfunction," The world journal of men's health, vol. 39, no. 1, 2021 Jan 2021. [CrossRef]
- L. R, "Review of intraurethral suppositories and iontophoresis therapy for erectile dysfunction," International journal of impotence research, vol. 12 Suppl 4, 2000 Oct 2000. [CrossRef]
- F. M. Md. Ehsan Uddin Talukder, Rashu Barua, Samsad Sultana, Farhana Yesmin, Mohammad Sayedul Islam, Robiul Hasan Bhuiyan, "In vitro Assessment of Cytotoxic Activity of Hybrid Variety of Momordica charantia (Bitter Gourd)," 2023. [CrossRef]
- M. E. U. T. Rashu Barua, Mohammad Sayedul Islam, Farhana Yesmin, Kanchan Chakma, Md Golam Kabir, Robiul Hasan Bhuiyan, "Nutritional Analysis and Phytochemical Evaluation of Bitter Gourd (Momordica Charantia) from Bangladesh," 2020. [CrossRef]
- R. Barua et al., "Antioxidant and Cytotoxic Activity of Crude Flavonoid Fraction from the Fruits of Hybrid Variety of Momordica charantia (Bitter Gourd)," (in en), Journal of Pharmaceutical Research International, pp. 778-786, 2014/02/07 2014. [CrossRef]
- R. Barua et al., "Bioinformatics and Functional Analyses Implicate Potential Roles for EOGT and L-fringe in Pancreatic Cancers," (in en), Molecules, Communication vol. 26, no. 4, p. 882, 2021-02-07 2021. [CrossRef]
- P. V and R. M, "Erectile dysfunction and diabetes: a review of the current evidence-based medicine and a synthesis of the main available therapies," Diabetes & metabolism, vol. 38, no. 1, 2012 Feb 2012. [CrossRef]
- D. Y et al., "Erectile dysfunction, physical activity and physical exercise: Recommendations for clinical practice," Andrologia, vol. 51, no. 5, 2019 Jun 2019. [CrossRef]
- M. DR, B. AL, D. G, E. K, and I. LJ, "Erectile hydraulics: maximizing inflow while minimizing outflow," The journal of sexual medicine, vol. 11, no. 5, 2014 May 2014. 14 May. [CrossRef]
Figure 1.
PRISMA flow diagram reflecting the literature review and the total number of articles cited in the review. (PRISMA: Preferred Reporting Items for Systematic reviews and Meta-Analyses).
Figure 1.
PRISMA flow diagram reflecting the literature review and the total number of articles cited in the review. (PRISMA: Preferred Reporting Items for Systematic reviews and Meta-Analyses).
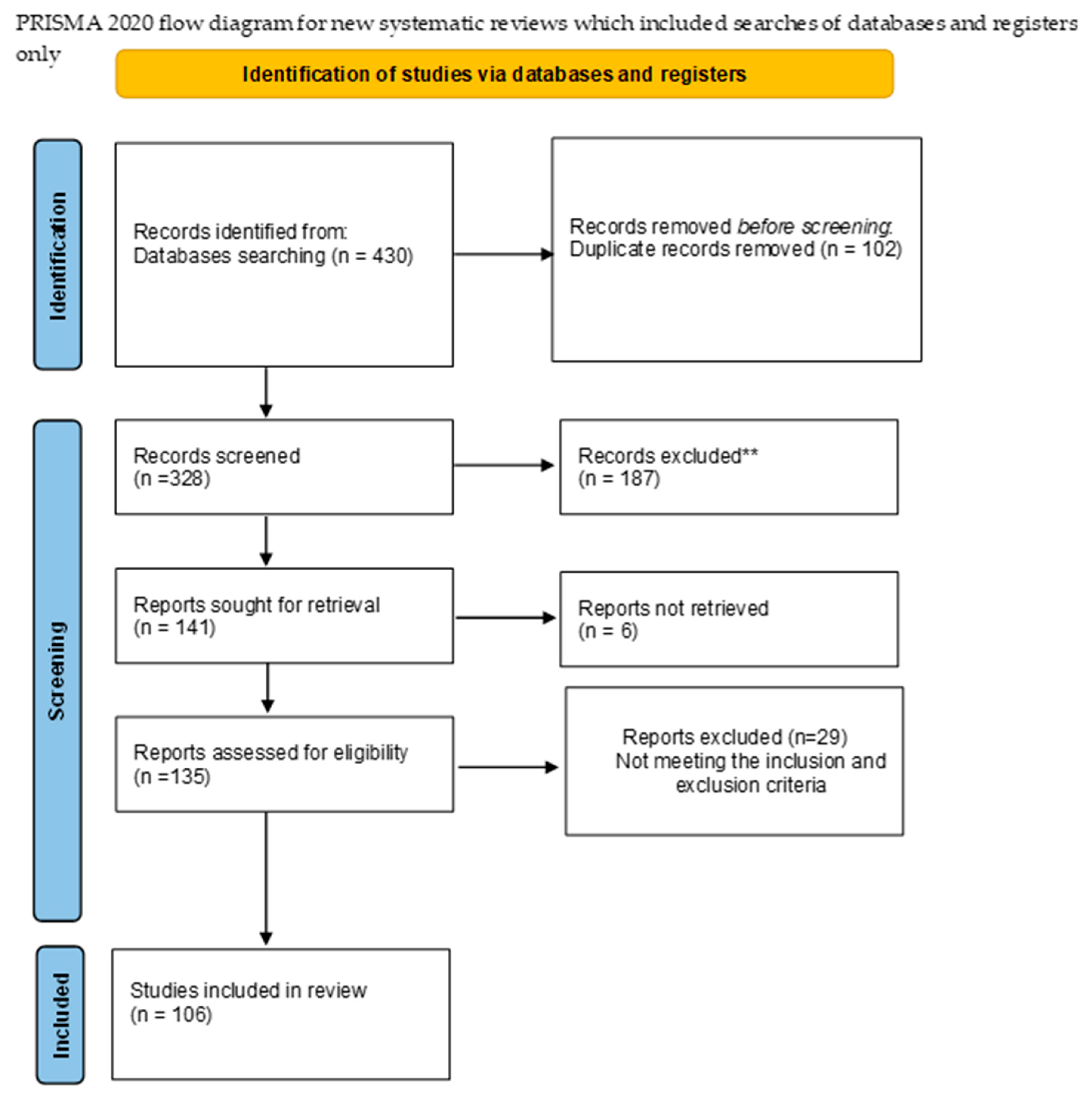
Figure 2.
Mechanism erectile dysfunction due to diabetes.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



