
Submitted:
18 August 2023
Posted:
22 August 2023
You are already at the latest version
Abstract
Tumour microenvironment, composed of pro- and anti-tumour immune cells, affects cancer cells behaviour. We aimed to evaluate if tumour-infiltrating lymphocyte (TIL) density and TILs subtypes in core biopsies at diagnosis of breast cancer patients could predict pathologic complete response (pCR; ypT0/is ypN0) from neoadjuvant systemic therapy (NST). The TIL subtypes were determined based on the proportions of presumably anti-tumour (CD8+, CXCL13+) and pro-tumour (PD-1+, FOXP3+) immune cells. A prospective, non-interventional study including 171 participants undergoing NST was performed. The median TIL density for the entire cohort was 10% (IQR: 3.5-23.8), and 59 (35%) patients achieved pCR. TIL density was positively associated with pCR (univariately and multivariably). In the multivariable logistic regression model, TIL density was an independent predictor of pCR (p=0.012, OR 1.27; 95% CI 1.05-1.54) when controlled for age (p=0.232), Ki-67 (p=0.001), node-negative status (p=0.024), and HER2+/triple negative vs luminal B-like subtype (p<0.001). In our sample, higher proportions of PD-1+ TILs and FOXP3+ TILs were associated with a higher probability of pCR but the association was not statistically significant. In the exploratory multivariable analysis, we showed that only higher CD8+ TILs were associated with pCR. In conclusion, TIL density and its subtypes are associated with pCR.
Keywords:
breast cancer
; pathologic complete response
; tumour-infiltrating lymphocytes
; neoadjuvant systemic therapy
; CD8 antigen
; forkhead box P3
; programmed cell death 1 receptor
; chemokine CXCL13
1. Introduction
Breast cancer is the most common type of cancer and also one of the leading causes of cancer-related mortality in women globally [1]. Five-year survival rates vary dramatically on the stage at presentation (being 99% in stages 0–IA, and 27% only in stage IV) [2]. In the last decade, the management of breast cancer shifted from primary surgical treatment to neoadjuvant systemic treatment (NST) in highly proliferative subtypes (human epidermal growth factor receptor 2 (HER2) positive, triple negative (TN), and some luminal B-like) [3,4,5]. This concept assumes that NST eradicates potential microscopic metastases and the evidence that achieving a pathologic complete response (pCR) confers improved long-term survival. In patients without pCR achievement, the outcome could be further improved by tailoring the post-neoadjuvant treatment [6].
Adaptive immune response has an important role in cancer growth modulation through the mechanisms of avoiding immune destruction of cancer cells and promoting inflammation [7]. Most notably, a high density of tumour-infiltrating lymphocytes (TIL) has been linked with improved outcomes in colon, ovarian, lung, and breast cancer [8,9,10,11,12]. In early breast cancer, patients with high TIL density had higher probability of pCR after NST [12], irrespective of breast cancer subtype [13]. However, only in TN and HER2-positive subtypes higher TIL density contributed to prolonged progression-free survival (PFS) and overall survival (OS), while in the luminal B-like subtype that was not the case [13,14]. Stromal TIL consists of T cells, B cells, and natural killer cells in various proportions; in breast cancer, typically 75%, 20%, and 5%, respectively. The TIL subtypes further dictate the entire TIL action, thus steering cancer progression toward a more or less favorable clinical outcome [15,16,17]. In-depth research of T-cells in TIL in breast cancer patients revealed that CD8+ T-cell infiltration has been associated with a favorable clinical outcome, however, cancer cells could develop several resistance mechanisms against CD8+ T-cell anti-tumour activity [18,19,20,21,22,23,24]. They could secrete into the tumour microenvironment immunosuppressive cytokines (interleukin 6 (IL-6), IL-17, and tumour growth factor beta (TGF-β)), which has been associated with a poor clinical outcome [25,26]. Moreover, these cytokines also increase the levels of tumour-associated macrophages, regulatory T cells and myeloid-derived suppressor cells in the tumour microenvironment, which further limit CD8+ T-cell tumour infiltration and activity [8,25,27,28,29,30]. This coupled with the upregulation of programmed death ligand 1 (PD-L1) gene expression, further contributing to immunosuppression [31]. Programmed death receptor 1 (PD-1) is a cellular receptor expressed on antigen-presenting T cells. Binding with its ligands PD-L1 or PD-L2, which are normally expressed on antigen-presenting cells and aberrantly on tumour cells, leads to an inhibition of the effector functions of T-cells. PD-1+ TILs were found frequently in HER2+ and basal-like tumours (part of the TN subtype). In basal and luminal B-like subtypes, PD-1+ TIL was associated with a worse prognosis [32,33,34], however, in some studies, it significantly correlated with higher TIL expression and an improved probability of pCR [34,35].
Regulatory T cells in TIL have been associated with a worse prognosis, irrespective of the breast cancer subtype [8,36,37,38]. Regulatory T-lymphocytes are a subpopulation of CD4+ T-lymphocytes with the immune phenotype CD4+ CD25+ forkhead box P3 (FOXP3+). In a healthy tissue environment, they suppress and modulate the immune responses in order to prevent autoimmune reactions. In breast cancerogenesis, the fraction of FOXP3+ T-lymphocytes increases considerably with the progression from healthy breast tissue to ductal carcinoma in situ and eventually to invasive ductal carcinoma [39,40]. In the breast cancer microenvironment, FOXP3+ lymphocytes were strongly associated with both lower relapse free survival (RFS) and OS [41,42,43]. FOXP3 expression in cytoplasma of tumor cells was of no prognostic significance, however a high infiltration of FOXP3+ lymphocytes accompanied by a cytoplasmic FOXP3+ tumor was the most detrimental phenotype [37]. Other reports, however, depicted that CD4+ regulatory T cells seemed to be capable of inhibiting invasive breast cancer development from pre-invasive breast cancer by suppressing pro-tumorigenic T helper 2 cell responses [44]. Yeong et al. has shown that a combination of high densities of FOXP3+, CD8+ T-cells and CD20+ B cells is associated with a favorable prognosis in TN subtype [42,45].
The above-noted conflicting findings clearly show that at evaluation of the percentage of FOXP3+ TIL, the percentage of CD8+ TIL should also be taken into consideration. Specifically, it is highly important to describe the ratio between the different subsets of TIL components to better understand the nature of tumour microenvironment regulation in terms of its pro- or anti-tumour effect [46,47].
Gene expression profiling was used to look at TIL in primary breast cancer. This showed that both CD4+ T-lymphocytes and follicular T-helper cells expressed CXCL-13. While their immune functions are currently less well understood, researchers believe CXCL-13-expressing T-helper cells play a significant role in attracting immune cells to the tumour microenvironment, regulating antigen-specific B-cell responses, as well as promoting the formation of tertiary lymphoid structures, thus generating germinal centers for local memory B-cell differentiation at the tumour location [48,49,50]. Studies on the expression of CXCL13 genes showed that CXCL13 significantly correlated with improved disease-free survival [15]. One study showed that CXCL13 expression was a significant predictor of a pCR [48].
However, prospective studies evaluating the contribution of different pro- and anti-tumour TILs to pCR are extremely scarce. The goal of this study was to analyze TIL density and TIL subtypes in core biopsies of breast cancer patients before NST and investigate their possible predictive role for pCR when treated with NST in a whole cohort and according to the breast cancer subtypes. To that end, TIL subtypes were assessed as the proportion of (presumably) anti-tumour (CD8+, CXCL13+) and (presumably) pro-tumour (PD-1+, FOXP3+) immune cells in TIL specimens. Our first hypothesis was that patients with a high TIL density would have a higher probability of pCR after NST compared to those with a low TIL. The second hypothesis was that higher CD8+ TILs, higher CXCL13+ TILs, lower PD-1+ TILs and lower FOXP3+ TILs are associated with a higher probability of pCR. We also investigated TIL and its subtypes within different molecular subtypes of breast cancer and examine their association with other clinicopathologic parameters.
2. Materials and Methods
2.1. Patients and treatment
We conducted a prospective, non-interventional study in patients with early breast cancer who were treated with NST, followed by breast and axillary surgery. All patients were treated at the Institute of Oncology Ljubljana. Inclusion criteria were female older than 18 years, diagnosed with early breast cancer of stages IIA (cT2N0M0) to IIIB (cT4a-cN0-1M0), luminal B-like, HER2+-luminal, HER2+-non-luminal, and TN subtype, regardless of menopausal status, and intended for NST treatment.
Exclusion criteria included the luminal A-like subtype (progesterone receptors (PR) >20% and/or Ki-67 ≤10%), metastatic disease, patients not understanding Slovenian, and ineligibility for the NST. Before inclusion in the study, all patients provided informed consent. The Slovenian Medical Ethics Commission approved the study (No. 0120-133/2017-2, dated June 8, 2017). All procedures were carried out in accordance with the Helsinki Declaration and Good Clinical Practice.
During the diagnostic and staging procedures of breast cancer, patients underwent a clinical examination, laboratory blood analysis, bilateral mammography, breast ultrasound and ultrasound-guided core needle biopsy, radiopaque clip insertion in the breast tumour, ultrasound of tumour-side axillary and supraclavicular lymph nodes, fine-needle aspiration of any suspicious lymph node, and a breast MRI scan (unless mastectomy was planned). For metastatic disease exclusion, a contrast computer tomography scan of the thoracic and abdominal organs and bone scintigraphy were performed.
Patients were treated with NST according to European Society for Medical Oncology (ESMO) recommendations at the time [3,4]. Shortly, chemotherapy consisted of sequential therapy with anthracyclines and taxanes (4 cycles of doxorubicin or epirubicin/cyclophosphamide followed by 12 cycles of weekly paclitaxel or 3–4 cycles of 5-fluorouracil/epirubicin/cyclophosphamide followed by 3–4 cycles of docetaxel). At the attending oncologist’s discretion, a dose-dense regimen was delivered. Similarly, in cases of contraindications, anthracycline-free schemas were used. Patients with HER2+ breast cancer tumours received anti-HER-2 therapy alongside taxane administration [3,4]. Breast surgery took place 3-6 weeks after the end of NST. Adjuvant radiation, endocrine and anti-HER2 therapy and postneoadjuvant capecitabine in TNBC were applied according to guidelines [3,4,51].
2.1.1. Endpoints
The primary endpoint was the probability of pCR after NST, defined as the absence of invasive carcinoma in the breast (in situ carcinoma could be present) and in the axilla (ypT0/is ypN0) [52].
2.2. Pathohistological Examinations
On the pre-treatment paraffin-embedded tumour block (core biopsy specimen), standard tumour characteristics (pathohistological subtype, grade, expression of estrogen receptors (ER) and PR, HER2 status, Ki-67) were performed. Patients were regarded as HER2+ if immunohistochemistry (IHC) was 3+, in the case of IHC 2+ fluorescent in situ histochemistry was performed, and ratio ≥2 was regarded as HER2+. Patients were regarded as luminal B-like, if ER ≥1%, PR ≤20%, Ki-67 >10% and HER2-. In the case of HER2+, ER 0% and PR 0% result, patients were regarded as HER2+-non-luminal, and in case of HER2+ and ER ≥1% and/or PR ≥1% they were regarded as HER2+-luminal. TN subtype was defined as ER 0%, PR 0% and HER2- [3,4]. For TIL density evaluation, one representative hematoxylin eosin (HE) stained tissue slice was used. TIL density was evaluated by two independent blinded pathologists, sub-specialized in breast cancer pathology, and the average of both TIL assessments was taken for the analysis. TIL density evaluation was performed in accordance with the guidelines of the International TIL Working Group 2014 and the International Immuno-Oncology Biomarker Working Group 2017 [12,53,54]. Briefly, all cells in the intra-tumour stroma that exhibited the characteristics of mononuclear immune cells, were classified as TIL cells. TIL density was expressed as the percentage of the intra-tumour stroma surface area occupied by TIL and was expressed using a numerical variable ranging from 0% to 100%. TIL density was also dichotomised into a low TIL density group (0-59%) and a high TIL density group (60-100%), according to Denkert et al [12]. For TIL phenotyping, additional tissue slices were stained separately for CD8, CXCL13, FOXP3, and PD-1 positive cells. The percentage of TIL in the intra-tumour stroma, occupied by the above-mentioned markers, was assessed and counted by a pathologist at 400x magnification, where the average cell percentage from four visual fields was used to determine the target cell percentage in each sample.
2.3. Assay Methods
Immunohistochemical examination of FOXP3, CD8, PD-1, and CXCL13 was performed on 2-4 µm thick fresh formalin paraffin-embedded tissue sections dried at 56 ⁰C for 2 hours, using a fully automated IHC staining system Ventana Benchmark Ultra (Ventana ROCHE Inc, Tucson, AZ, USA).
CD8, FOXP3 and PD1 epitopes were retrieved with heat induced epitope retrieval (HIER) using Cell Conditioning Solution 1 (Ventana ROCHE inc. Tucson, AZ, USA; cat. No. 950-124) for 88 minutes at 100⁰C, while CXCL13 epitope was retrieved with proteolysis using Protease I (Ventana ROCHE inc. Tucson, AZ, USA; cat. No. 760-2018) for 8 min at 37⁰C.
Retrieved epitopes were detected using monoclonal antibodies directed against CD8 (DAKO Agilent technologies Inc. Santa Clara, CA, USA; cat. No. M7103; clone C8/144B; diluted at 1:100), FOXP3 (Epitomics, Rocklin, CA, USA; cat. No. AC0304RUO; clone EP340; diluted at 1:200), PD1 (CellMarque, Rocklin, CA, USA; cat. No. 315M; clone MRQ22; diluted at 1:800) and CXCL13 (R&D systems Minneapolis, MN, USA; cat. No. MAB8012; clone 53602; diluted at 1:25).
All primary antibodies were incubated on board for 60 minutes at 37⁰C and visualized using the 3-step multimer detection system OptiView DAB IHC Detection Kit (Ventana ROCHE Inc. Tucson, AZ, USA; cat. No. 760-700) according to the manufacturer's instructions. Visualization of CXCL13 and PD1 was enhanced using OptiView Amplification Kit (Ventana ROCHE inc. Tucson, AZ; USA cat. No. 760 099).
Normal appendix was used as control for the 4 antigens. Optimal staining reactions were considered as follows: CD8 - strong distinct membranous staining in subepithelial and interfollicular cytotoxic T-cells, FOXP3 - moderate intensity distinct nuclear staining in regulatory T-cells, PD1 - strong distinct membranous staining in the germinal center associated helper T-cells and CXCL13 - strong distinct cytoplasmic staining in the germinal center associated follicular helper T-cells and follicular dendritic cells. All other cells must stain negatively for these antigens.
2.4. Statistical Analysis
2.4.1. Sample size
With the planned sample of 180 patients, a chi-square test with a significance level of 0.05 achieves 80% power to reject the null hypothesis of no association between TIL (high ≥60% or low) and pCR (yes or no) if Cohen’s effect size W is at least 0.21. This effect size corresponds to the difference in the probability of pCR between high and low TIL group of at least 29% if we assume that in population 30% achieve pCR (based on [55]) and 12% belong in the high TIL group (based on [12]). When analysing TIL as a numerical variable, we are able to detect even smaller effect sizes.
2.4.2. Data analysis
Numerical variables were presented with medians and interquartile ranges (IQR), and categorical variables with frequencies and percentages. In addition to the descriptive statistics, the association of each patient or tumour characteristic with pCR was evaluated by univariate logistic regression, where p values were adjusted using Holm’s method to control the family-wise error rate. The distribution of TILs was presented graphically using boxplots. The difference between TIL measurements by two pathologists was presented by Bland-Altman plot (supplement material). On bar plots for the proportion of pCR in separate TIL groups, 95% Clopper-Pearson’s exact confidence intervals (CIs) were presented.
The association between TIL and pCR was assessed in a multivariable logistic model, where we controlled for age, nodal stage, Ki-67 (numerical) and cancer subtypes (two groups based on different biology: combined HER2+ luminal, HER2+non-luminal and TN vs. luminal B-like subtype). The model meets the requirement for a sufficient number of events per variable with 59 events (achieved pCR) and 5 estimated coefficients (the selection of independent variables was predetermined and based on background knowledge). In exploratory analysis (supplement material), separate multivariable models were fitted to explore the association between pCR and separate TIL subtypes (CD8+, CXCL13+, FOXP3+, PD1+) using the same independent variables as in the main model for TIL. All logistic models were fitted using Firth’s bias reduction method, odds ratios (ORs) were reported together with 95% CIs. The discriminative ability of the multivariable logistic models was estimated by means of the ROC (receiver operating characteristic) curve analysis reporting the area under the ROC curve (AUC).
In the exploratory analysis (supplement material), association between TILs and various clinical and histopathologic characteristics (tumour grade and size, categorised Ki-67, nodal status, breast cancer subtype) was evaluated using Mann–Whitney or Kruskal-Wallis test for numerical TILs and Fisher’s exact test for dichotomised TIL, where p values were adjusted using Holm’s method to control the family-wise error rate.
An (adjusted) p value of less than 0.05 was considered statistically significant. The analysis was performed with the help of relevant open-source libraries in Python 3.8.5. and SPSS, IBM Co., v. 22.
3. Results
3.1. Patient population
Between February 2018 and March 2021, we enrolled 268 patients. Of those, 171 met the inclusion criteria, and all were included in the final analysis (Figure 1).
The median age of patients was 48 years (IQR 41.7–57.4). Of them, 91 (53%) were of the luminal B-like subtype, 32 (19%) had HER2+ luminal, 16 (9%) had HER2+ non-luminal, and 32 (19%) had the TN subtype. Patients’ tumour and clinical characteristics are presented in Table 1 (second column). Briefly, 161 patients (96%) had invasive carcinoma of no special type. The majority were grade 3 (124, 73%); the median Ki-67 was 30% (IQR 20–50); the median tumour size was 30.5 mm (IQR 23.3–40), and 125 (73%) of patients were node positive. A pCR was achieved in 59 (35%) patients.
The results of univariate analysis for a comparison of the clinicopathologic characteristics of patients who achieved pCR to their counterparts, are also presented in Table 1. There was a statistically significant difference in the probability of pCR among breast cancer subtypes (adjusted p<0.001 ). The highest probability of pCR was in patients with the HER2+-non-luminal subtype (88%), and the lowest amongst patients with the luminal B-like subtype (18%). Grade 3 tumours and tumours with high Ki-67 had a higher probability of pCR (both adjusted p<0.001). In our sample, patients with negative lymph nodes had a higher probability of pCR, and this difference could not be generalised to the population (adjusted p = 0.335).
3.2. Association of TIL and its subtypes with pCR
3.2.1. TIL Density and its association with pCR
The median TIL density in all patients was 10% (IQR 3.5-23.8). The median interobserver absolute difference was 5.0 (IQR 0.5-14.5) (Figure S1), interobserver variability was low at low TIL density, but high at high TIL density (Figure S2). The HER2+ non-luminal subtype had the highest median value of TIL (22.5%), followed by the TN subtype (16.3%). The distribution of TIL (expressed as a numerical value) among the breast cancer subtypes is presented in Figure S3. Based on the predetermined cutoff of 60%, 161 (94%) tumours belonged to the low TIL group and 10 (6%) to the high TIL group. In this high TIL group, 5 patients (31%) belonged to luminal B-like, 4 (27%) to TN, and 1 (7%) to the HER2+ non-luminal subtype. The representative IHC slides of low and high TIL are presented in Figure 2 (A1, A2).
TIL categorization into the low and high categories did not show a significant association with either of the clinicopathological characteristics, however numerical TIL was significantly positively associated with tumour grade and Ki-67 (both adjusted p=0.002) (Table S1). For instance, median TIL in G3 tumours was 12.5%, compared to only 5% in G2 tumours. Similarly, tumours with high Ki-67 (>40%) had median TIL of 17.5% compared to 5% in low Ki-67 (10-20%).
Importantly, numerical TIL density was associated with pCR (univariate analysis, adjusted p=0.005) (Table 1, Figure 3). A higher probability of pCR (60% vs. 33%) was observed also when comparing the high TIL group with the low TIL group (cut-off of 60%), but the difference was not statistically significant (p=0.088, adjusted p=0.615). In Figure 4, we present an explorative analysis of the proportion of pCR according to breast cancer subtypes and their TIL density. TIL group 0–10% had substantially lower pCR than the rest. In all subtypes, the probability of pCR was 100% when TIL was 75–100% (however, small sample sizes in these groups of patients imply large confidence intervals). In the HER2+ non-luminal subtype, the probability of pCR was high regardless of the TIL density (again with large confidence intervals).
In our multivariable model, numerical TIL concentration was shown as an independent factor for the prediction of pCR when controlled for age, Ki-67, lymph nodes (positive/negative) and molecular subtypes (dichotomised into luminal B/other) with p=0.012 (Table 2). The model discriminated the data well with AUC=0.817. With an increase in TIL density by 10%, the odds for pCR increased by 27%. Patients with clinically negative axillary lymph nodes had 2.5 times higher odds for pCR than node-positive patients. Patients with HER2+/TN breast cancer subtypes had 5.1 times higher odds of achieving pCR compared to those with the luminal B-like subtype. For patients with an increase in Ki-67 for 10%, the odds for pCR increased for 38%.
3.2.2. TIL Subtypes and their association with pCR
Representative IHC slides of TILs subtypes are presented on Figure 2 (low expression: B2-E2; high expression: B1-E1). Investigation on TIL subtypes revealed that CD8+ TIL was the most prevalent component of TIL with a median of 40.0% (IQR 30.0–50.0), whereas other TIL subtypes were present in lower percentages: CXCL13+ TILs median was 1% (IQR 0.5–2.0), PD1+ TILs was 2% (IQR 0.0–5.0), and FOXP3+ TILs was 4% (IQR 1.0–7.0) (Table 1, Figure 5). 31%, 21%, and 5% of tumours did not express any PD-1, CXCL13, or FOXP3, respectively. Figure 6 (A–D) shows the distribution of TIL subtypes among the breast cancer subtypes. Shortly, all breast cancer subtypes had similarly high CD8+ TILs (median 40-45%). There was no difference of expression of CXCL13+ TILs among the breast cancer subtypes. On the other side, (presumably) pro-tumour TIL subtypes PD-1+ TILs and FOXP3+ TILs showed the tendency to be more prevalent in the TN and HER2+ non-luminal subtypes (Figure 6, Table S1). The correlations between TIL subtypes with clinicopathological characteristics are shown in Table S1. There was a statistically significant association between PD-1+ TILs and grade (adjusted p=0.015) and Ki-67 (adjusted p=0.024), and between FOXP3+ TILs and grade (adjusted p=0.012), although these differences were not meaningful. We also found an association of CXCL13+ TILs with the tumour stage (adjusted p=0.051).
Surprisingly, PD-1+ TILs and FOXP3+ TILs were positively associated with pCR in our sample, though the association was not significant in univariate or multivariable analysis.
In the exploratory multivariable analysis, only CD8+TIL (numerical) was significantly associated with pCR when controlled for age, Ki-67, lymph nodes (positive/negative) and molecular subtypes (dichotomised as luminal B/other), p = 0.045 (Table S2). Increasing CD8+ TILs by 10% increases the odds for pCR by 31%. The model discriminated the data well with AUC=0.807. Similar exploratory multivariable analysis for CXCL13+ TILs, PD-1+ TILs and FOXP3+ TILs did not show association with pCR (Tables S3, S4 and S5).
4. Discussion
In our prospective non-interventional study, performed in early breast cancer patients undergoing NST, we have been investigated the possible role of pre-treatment TIL density and TIL subtypes on achieving pCR. Our data clearly confirmed the first hypothesis that patients with a high TIL density would have a higher probability of pCR after NST compared to those with a low TIL.
On the other hand, our second hypothesis, that higher CD8+ TILs, higher CXCL13+ TILs, lower PD-1+ TILs and lower FOXP3+ TILs are associated with a higher probability of pCR, was partially confirmed: only high CD8+ TILs were associated with pCR in the multivariable model (exploratory analysis). Surprisingly, on our sample, a higher probability of pCR was associated with a higher percentage of PD-1+ TILs and FOXP3+ TILs but these associations were not statistically significant in multivariable models nor in univariate analyses. Other independent predictive factors for a higher probability of pCR were the HER2+ non-luminal/TN subtype, high Ki-67 and grade (univariate analyses, adjusted for multiple comparisons).
In this study, we added TIL density evaluation to the routine histopathological analysis of the tumour sample analysis before treatment. TIL density in our cohort was positively associated with grade and Ki-67 (Table S1). Median TIL was 12.5% and 17.5% in G3 and high Ki-67 (Ki-67>40%) tumors, respectively. A similar correlation of high TIL with high Ki-67 and grade was reported in some other studies [56,57,58].
In our sample, patients with HER2+ non-luminal subtype had the highest median percentage of TIL (22.5%) among the four different subtypes but this difference could not be generalised to the population (adjusted p=0.085) (Table S1).
In our sample only 10 patients had high TIL (>60%) and 6 of them (60%) achieved pCR compared to 33% pCR in low TIL group but association between dichotomised TIL (cut-off 60%) and pCR was not statistically significant. The reason could be the small number of patients in the high TIL group, or a too-high TIL cutoff value.
Similar but significant findings, however, were reported in the GeparDuo cohort, where a subgroup of lymphocyte-predominant breast cancer (>60% of either stromal or intratumoral lymphocytes) had a probability of pCR of 41.7% in comparison with 9.3% in the other group [12,59]. Additionally, in the GeparDuo and GeparTrio cohort, the odds ratio for pCR increased with the extent of TILs [60]. Tumours without any TILs had a probability of pCR of 7.2%, while those with lymphocyte predominant breast cancer had a probability of pCR of 40% [12,53,61]. It should be noted that the probability of pCR was 12.8% and 17% in GepardDuo and GepardTrio cohort, respectively, whereas it was 35% in our study. We used a TIL cutoff of 60% because it was the standard used by researchers in large neo- or adjuvant trials at the time our study was designed used cut-off between 50% and 60% [59,62,63,64,65,66,67,68,69]. Numerous other studies, performed in the meantime, showed substantially lower cutoffs for high TIL to be appropriate to distinguish between patients who benefited for pCR prediction. The cutoff, however, depends on a breast cancer subtype [63]. Recently, the St. Gallen consensus meeting for the TN subtype recommended a cutoff of 50%. This cutoff was based on relapse-free survival (RFS) data, not pCR data, and emphasized a very favorable outcome in small TN tumours without adjuvant chemotherapy treatment [70]. For HER2+ subtypes, even lower cutoffs (5-40%) are reported to be prognostic for pCR [62,63]. Our sample size of 171 patients with 59 achieving pCR (events) was too small to allow for a cut-off determination.
In our study, numerical TIL was significantly associated with pCR in univariate analysis (Table 1) and revealed as an independent factor for pCR in a multivariable model (Table 2). Increasing TIL by 10% will increase the odds for pCR by 27% (Table 2). Figure 3 indicates that a dichotomised TIL is not suitable for determination of the association with pCR. Figure 4 suggests that all subtypes of breast cancer have been linked to higher percentages of pCR when the TIL density is high on our sample, but our sample size did not permit an additional inferential subgroup analysis. Similarly, in GeparSixto trial it was shown that increased levels of stromal TILs predict pCR in the whole and also in TN and HER2+ cohort [65,71]. Our multivariable model confirmed HER2+/TN subtype and node-negative status as additional independent predictive factors for a higher probability of pCR. These findings are in accordance with reports of others [12,62,63,71,72,73,74,75].
It is now increasingly clear that the tumour microenvironment is composed of heterogenous tumour cells and the host's endogenous stroma, which together undergo changes as the disease progresses. Importantly, stromal cells are becoming recognised as key players in the development of the tumour microenvironment, metastasis, immune infiltration and inflammation, and resistance to chemotherapeutic agents [76,77,78].
Our investigation revealed CD8+ TILs as the most prevalent among studied TILs, with a median of 40% of total TIL (Table 1, Figure 5). Additionally, all breast cancer subtypes had similarly high CD8+ TILs (median 40-45%). On the contrary, presumably pro-tumour TIL subtypes (PD-1+ TILs and FOXP3+ TILs) tended to be more prevalent in the TN and HER2+ non-luminal subtypes (Figure 6, Table S1).
In our sample, numerical CD8+ TILs did not show any association with grade, Ki-67, tumour size, nodal stage, or subtypes (Table S1). However, numerical CD8+ TIL was significantly associated with pCR in a multivariable model (exploratory analysis, Table S2). Odds for pCR increased by 31% with increase of CD8+ TILs by 10%.
From other reports, there is some evidence that the possible role of CD8+ T-cells is greater in hormone receptor-negative breast cancers. In a study evaluating 1854 breast cancer samples, Baker et al. has shown improved disease specific survival in patients with high CD8+ TIL in ER-negative tumors only. On the contrary, in low grade ER-positive tumours a high CD8+ TIL was associated with inferior outcome [79]. CD8+ infiltrates were seen in 60% of TNBCs. In concordance with our results, CD8+ TILs were found to be an independent predictive factor for pCR [80,81].
CXCL13+ TILs represented only a median of 1% of total TIL, it was similarly expressed in all cancer subtypes. We found an association only with the tumour stage. In two other studies, CXCL13 expression was associated with higher tumour grade (grades 2–3), positive nodes, ER-negative status, longer metastasis-free survival, and a stronger prognostic effect in HER2-positive breast cancer [49,82]. In the third study, a four-gene signature that includes CXCL13 was predictive for the extent of lymphocytic infiltration after NST in TNBC. The increase of the value of these signatures was associated with a better distant relapse-free survival, adding novel prognostic information for this aggressive breast cancer subtype [83].
In our patients, PD-1+ TILs expression was associated with high tumor grade and high Ki-67, similar to the findings of others [34,35,84]. Importantly, we observed that a higher percentage of pCR is associated with higher PD-1+ TILs, but this association was not significant when generalized to the population. A significant association of PD-1 expression with higher TIL scores and pCR in early breast cancer, however, was demonstrated by Denkert et al. [65]. This suggests that PD-1 expression may be a useful biomarker for predicting response to NST in breast cancer patients. Further studies are needed to confirm these findings and determine the potential clinical implications.
FOXP3+ TILs were, surprisingly, positively associated with pCR in our sample (not statistically significant). In our sample TN and HER2+ non-luminal subtypes had a slightly higher median expression of FOXP3+ TILs than other subtypes, but this could not be generalised to the population. Loi et al. reported the highest percentage of FOXP3+ cells in the TN subtype [61], but the median percentage in that study was 70%, which is substantially higher than in our study (4%). FOXP3+ TILs are known to disrupt anti-tumour immunity by suppressing the effector functions of various immune cells and have been implicated in the escape of cancer cells from immunosurveillance [85,86]. Increased levels of FOXP3+ cells were strongly associated with an increased risk of early and late relapse, lower RFS and OS [12] and lower percentage of pCR [19]. In our study, on the contrary, FOXP3+ TILs and pCR were positively associated, but the association was not significant. Some other authors, especially in recent years, also found a positive association of FOXP3+ TILs with pCR [43,87,88]. Sun et al. reported subtype-specific improvement of pCR (OR: 1.20, 95% CI 1.02-1.40) and OS for HER2+ subtype of breast cancer [43]. The possible mechanism underlying this paradoxical observation could be the higher efficacy of chemotherapeutic treatments in a highly immunosuppressive environment. Namely, it has been reported that some chemotherapeutic agents, particularly cyclophosphamide, can inhibit FOXP3+ cells. Chemotherapy might be more effective in tumours with high levels of FOXP3 + TILs, and this in turn could facilitate tumour attack by CD8+ TILs and help to achieve pCR [43]. Furthermore, tumors having high CD8+/FOXP3+ ratio were more sensitive to anthracycline and taxane chemotherapy [22] and had higher pCR, especially the TN and HER2+ subtype [22,89].
To summarize, our data suggest that an evaluation of TIL subtypes by IHC could add additional predictive information for pCR beyond TIL density alone. More sophisticated and expensive techniques, like software guided immune cell evaluation, could improve the accuracy of TIL subtype evaluation. However, we have to take into consideration that these techniques may suffer from pre analytical and interpretative inconsistencies, which could impair their reproducibility and widespread application in daily practice. It is very important to clearly define each immune cell subset studied. For example, Fillion et al. reported CD4 expression not only in T cells but also in a subpopulation of monocytes, causing a bias and discrepancies in results and interpretation between studies [90].
This study has some limitations. Firstly, core needle biopsy sample could not be fully representative of the whole tumour's heterogeneity; however, it is used everywhere as a standard test to decide on the type of first treatment. Secondly, the visual method of TIL scoring is prone to intra- and inter-observer variability. In our case, interobserver variability was low at low TIL density, but high at high TIL density (Figures S1 and S2 ). In the case of high dis-concordance, a consensus decision between pathologists should be done. Thirdly, immunophenotyping of TIL includes few types of immune cells only, not taking into consideration other subtypes of lymphocytes, natural killer cells and cytokines or non-immune cells like macrophages, neutrophils, myeloid-derived stem cells, etc.
There are several strengths to our study. First, our study is very valuable, because it was a prospective study that included a substantial fraction of the patients treated with NST in a three-years period. Second, for our pathology department, the study was very important, because, within the study procedures, we initiated systematic scoring of TIL in core biopsies of breast cancer samples, and the method is now ready to be implemented into routine clinical work. TIL density is evaluated using HE stained sections only, which makes it practical for routine use. Also, the preoperative breast cancer tumour board meetings were set up at the beginning of our study, resulting in better decision-making about treatment sequence for all newly diagnosed breast cancer patients. We believe that the incorporation of TIL density measurements can be easily incorporated into routine pathology, especially in low-to-middle-income countries, but some run-in time is needed, as was the case with the Ki-67 method.
Further implication of our work: There is still much work to be done in the field of TIL biomarkers, especially in the course of immunotherapy treatment, which has been approved for the treatment of the TN subtype of breast cancer. The link between pCR, when treated with immunotherapy, and TIL subtypes should be investigated. Such research could pave the way for personalized treatment plans based on TIL biomarkers, leading to improved outcomes for breast cancer patients. Additionally, future studies could explore the potential of TIL biomarkers in predicting responses to other forms of cancer treatment beyond immunotherapy. In the future, machine learning techniques may help us further standardize the TIL evaluation and find important immune phenotypes.
To sum up, TIL scoring is a new biomarker that could be used in clinical practice. It remains open if PD-1+ TILs and FOXP3+ TILs are linked with a higher or lower response to chemotherapeutics used in the neoadjuvant treatment of breast cancer.
5. Conclusions
TIL scoring is a new biomarker associated with achieving pCR with NST independently of known pathohistological factors, that could be easily incorporated into routine pathologic evaluation. It remains open if TIL subtypes, linked with presumably pro-tumour characteristics, such as PD-1+ TILs and FOXP3+ TILs are linked with a higher or lower response to chemotherapeutics used in the NST of breast cancer.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, C.G.K. and K.G.; methodology, P.D., B.G., A.K.I. and K.G.; formal analysis, K.G., B.M.G. and N.R.; investigation, K.G. and C.G.K.; writing—original draft preparation, K.G. and P.D.; writing—review and editing, C.G.K. and N.R.; visualization, B.M.G..; supervision, C.G.K.; funding acquisition, C.G.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Slovenian Research Agency: P3-0321: Prognostic and predictive factors for response in treatment of different types of cancer and P3-0289: Characteristics of malignant neoplasms important for diagnosis, prognosis and treatment outcome.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Slovenian Medical Ethics Commission (No. 0120-133/2017-2, dated June 8, 2017).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data will be available after considering the aim of further use.
Acknowledgments
We would like to thank Ana Demšar and Branko Zakotnik, who helped us prepare the study protocols. We would also like to thank our research nurses and all the members of our preoperative multidisciplinary mammary board, who helped with patient enrollment, diagnostics and treatment. Special thanks of course goes to all the patients for agreeing to participate in the study.
Conflicts of Interest
The authors declare no conflict of interest related to this article.
References
- Cancer Today. Available online: https://gco.iarc.fr/today/ (accessed on 23 October 2022).
- ECIS-European Cancer Information System. https://ecis.jrc.ec.europa.eu (, date last accessed). 25 March.
- Senkus, E.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rutgers, E.; Zackrisson, S.; Cardoso, F. Primary Breast Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Annals of Oncology 2015, 26, v8–v30. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E. Early Breast Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Annals of Oncology 2019, 30, 1194–1220. [Google Scholar] [CrossRef] [PubMed]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.-J.; Albain, K.S.; André, F.; Bergh, J.; et al. Personalizing the Treatment of Women with Early Breast Cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Annals of Oncology 2013, 24, 2206–2223. [Google Scholar] [CrossRef]
- Minckwitz, G. von; Untch, M.; Blohmer, J.-U.; Costa, S.D.; Eidtmann, H.; Fasching, P.A.; Gerber, B.; Eiermann, W.; Hilfrich, J.; Huober, J.; et al. Definition and Impact of Pathologic Complete Response on Prognosis After Neoadjuvant Chemotherapy in Various Intrinsic Breast Cancer Subtypes. Journal of Clinical Oncology 2012, 30, 1796–1804. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The Next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Nelson, M.A.; Ngamcherdtrakul, W.; Luoh, S.-W.; Yantasee, W. Prognostic and Therapeutic Role of Tumor-Infiltrating Lymphocyte Subtypes in Breast Cancer. Cancer and Metastasis Reviews 2021, 40, 519–536. [Google Scholar] [CrossRef]
- Pagès, F.; Berger, A.; Camus, M.; Sanchez-Cabo, F.; Costes, A.; Molidor, R.; Mlecnik, B.; Kirilovsky, A.; Nilsson, M.; Damotte, D.; et al. Effector Memory T Cells, Early Metastasis, and Survival in Colorectal Cancer. New England Journal of Medicine 2005, 353, 2654–2666. [Google Scholar] [CrossRef]
- Hwang, W.-T.; Adams, S.F.; Tahirovic, E.; Hagemann, I.S.; Coukos, G. Prognostic Significance of Tumor-Infiltrating T Cells in Ovarian Cancer: A Meta-Analysis. Gynecologic Oncology 2012, 124, 192–198. [Google Scholar] [CrossRef]
- Dieu-Nosjean, M.-C.; Antoine, M.; Danel, C.; Heudes, D.; Wislez, M.; Poulot, V.; Rabbe, N.; Laurans, L.; Tartour, E.; Chaisemartin, L. de; et al. Long-Term Survival for Patients With Non–Small-Cell Lung Cancer With Intratumoral Lymphoid Structures. Journal of Clinical Oncology 2008, 26, 4410–4417. [Google Scholar] [CrossRef]
- Denkert, C.; Loibl, S.; Noske, A.; Roller, M.; Müller, B.M.; Komor, M.; Budczies, J.; Darb-Esfahani, S.; Kronenwett, R.; Hanusch, C.; et al. Tumor-Associated Lymphocytes As an Independent Predictor of Response to Neoadjuvant Chemotherapy in Breast Cancer. Journal of Clinical Oncology 2010, 28, 105–113. [Google Scholar] [CrossRef]
- Denkert, C.; Minckwitz, G. von; Darb-Esfahani, S.; Lederer, B.; Heppner, B.I.; Weber, K.E.; Budczies, J.; Huober, J.; Klauschen, F.; Furlanetto, J.; et al. Tumour-Infiltrating Lymphocytes and Prognosis in Different Subtypes of Breast Cancer: a Pooled Analysis of 3771 Patients Treated with Neoadjuvant Therapy. The Lancet Oncology 2018, 19, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Loi, S.; Sirtaine, N.; Piette, F.; Salgado, R.; Viale, G.; Eenoo, F.V.; Rouas, G.; Francis, P.; Crown, J.P.A.; Hitre, E.; et al. Prognostic and Predictive Value of Tumor-Infiltrating Lymphocytes in a Phase III Randomized Adjuvant Breast Cancer Trial in Node-Positive Breast Cancer Comparing the Addition of Docetaxel to Doxorubicin With Doxorubicin-Based Chemotherapy: BIG 02-98. Journal of Clinical Oncology 2013, 31, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Gu-Trantien, C.; Loi, S.; Garaud, S.; Equeter, C.; Libin, M.; Wind, A. de; Ravoet, M.; Buanec, H.L.; Sibille, C.; Manfouo-Foutsop, G.; et al. CD4 Follicular Helper T Cell Infiltration Predicts Breast Cancer Survival. Journal of Clinical Investigation 2013, 123, 2873–2892. [Google Scholar] [CrossRef] [PubMed]
- Zgura, A.; Gales, L.; Bratila, E.; Anghel, R. Relationship between Tumor Infiltrating Lymphocytes and Progression in Breast Cancer. Mædica - a Journal of Clinical Medicine 2018, 13, 317–320. [Google Scholar] [CrossRef]
- Muntasell, A.; Rojo, F.; Servitja, S.; Rubio-Perez, C.; Cabo, M.; Tamborero, D.; Costa-Garcı́a Marcel; Martı́nez-Garcia Marı́a; Menéndez Sı́lvia; Vazquez, I. ; et al. NK Cell Infiltrates and HLA Class I Expression in Primary HER2 Breast Cancer Predict and Uncouple Pathological Response and Disease-Free Survival. Clinical Cancer Research 2019, 25, 1535–1545. [Google Scholar] [CrossRef] [PubMed]
- Egelston, C.A.; Avalos, C.; Tu, T.Y.; Rosario, A.; Wang, R.; Solomon, S.; Srinivasan, G.; Nelson, M.S.; Huang, Y.; Lim, M.H.; et al. Resident Memory CD8 T Cells within Cancer Islands Mediate Survival in Breast Cancer Patients. JCI Insight 2019, 4. [Google Scholar] [CrossRef]
- Ali, H.R.; Provenzano, E.; Dawson, S.-J.; Blows, F.M.; Liu, B.; Shah, M.; Earl, H.M.; Poole, C.J.; Hiller, L.; Dunn, J.A.; et al. Association between CD8 T-Cell Infiltration and Breast Cancer Survival in 12 439 Patients. Annals of Oncology 2014, 25, 1536–1543. [Google Scholar] [CrossRef]
- Ibrahim, E.M.; Al-Foheidi, M.E.; Al-Mansour, M.M.; Kazkaz, G.A. The Prognostic Value of Tumor-Infiltrating Lymphocytes in Triple-Negative Breast Cancer: a Meta-Analysis. Breast Cancer Research and Treatment 2014, 148, 467–476. [Google Scholar] [CrossRef]
- Mahmoud, S.M.A.; Paish, E.C.; Powe, D.G.; Macmillan, R.D.; Grainge, M.J.; Lee, A.H.S.; Ellis, I.O.; Green, A.R. . Tumor-infiltrating CD8+ lymphocytes predict clinical outcome in breast cancer. Journal of Clinical Oncology 2011, 29, 1949–1955. [Google Scholar] [CrossRef]
- Miyashita, M.; Sasano, H.; Tamaki, K.; Chan, M.; Hirakawa, H.; Suzuki, A.; Tada, H.; Watanabe, G.; Nemoto, N.; Nakagawa, S.; et al. Tumor-Infiltrating CD8 and FOXP3 Lymphocytes in Triple-Negative Breast Cancer: Its Correlation with Pathological Complete Response to Neoadjuvant Chemotherapy. Breast Cancer Research and Treatment 2014, 148, 525–534. [Google Scholar] [CrossRef]
- Matsumoto, H.; Thike, A.A.; Li, H.; Yeong, J.; Koo, S.-lin; Dent, R.A.; Tan, P.H.; Iqbal, J. Increased CD4 and CD8-Positive T Cell Infiltrate Signifies Good Prognosis in a Subset of Triple-Negative Breast Cancer. Breast Cancer Research and Treatment 2016, 156, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Stovgaard, E.S.; Nielsen, D.; Hogdall, E.; Balslev, E. Triple Negative Breast Cancer – Prognostic Role of Immune-Related Factors: a Systematic Review. Acta Oncologica 2017, 57, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Gatti-Mays, M.E.; Balko, J.M.; Gameiro, S.R.; Bear, H.D.; Prabhakaran, S.; Fukui, J.; Disis, M.L.; Nanda, R.; Gulley, J.L.; Kalinsky, K.; et al. If We Build It They Will Come: Targeting the Immune Response to Breast Cancer. npj Breast Cancer 2019, 5. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, K.; Sakurai, M.; Yamamoto, Y.; Suzuki, E.; Tsuda, M.; Kataoka, T.R.; Hirata, M.; Nishie, M.; Nojiri, T.; Kumazoe, M.; et al. Alteration of Specific Cytokine Expression Patterns in Patients with Breast Cancer. Scientific Reports 2019, 9. [Google Scholar] [CrossRef]
- Doedens, A.L.; Stockmann, C.; Rubinstein, M.P.; Liao, D.; Zhang, N.; DeNardo, D.G.; Coussens, L.M.; Karin, M.; Goldrath, A.W.; Johnson, R.S. Macrophage Expression of Hypoxia-Inducible Factor-1 Suppresses T-Cell Function and Promotes Tumor Progression. Cancer Research 2010, 70, 7465–7475. [Google Scholar] [CrossRef]
- Ruffell, B.; Chang-Strachan, D.; Chan, V.; Rosenbusch, A.; Ho, C.M.T.; Pryer, N.; Daniel, D.; Hwang, E.S.; Rugo, H.S.; Coussens, L.M. Macrophage IL-10 Blocks CD8 T Cell-Dependent Responses to Chemotherapy by Suppressing IL-12 Expression in Intratumoral Dendritic Cells. Cancer Cell 2014, 26, 623–637. [Google Scholar] [CrossRef]
- Almand, B.; Clark, J.I.; Nikitina, E.; Beynen, J. van; English, N.R.; Knight, S.C.; Carbone, D.P.; Gabrilovich, D.I. Increased Production of Immature Myeloid Cells in Cancer Patients: A Mechanism of Immunosuppression in Cancer. The Journal of Immunology 2001, 166, 678–689. [Google Scholar] [CrossRef]
- Ngamcherdtrakul, W.; Yantasee, W. SiRNA Therapeutics for Breast Cancer: Recent Efforts in Targeting Metastasis, Drug Resistance, and Immune Evasion. Translational Research 2019, 214, 105–120. [Google Scholar] [CrossRef]
- Chen, L.; Han, X. Anti–PD-1/PD-L1 Therapy of Human Cancer: Past, Present, and Future. Journal of Clinical Investigation 2015, 125, 3384–3391. [Google Scholar] [CrossRef]
- Burugu, S.; Asleh-Aburaya, K.; Nielsen, T.O. Immune Infiltrates in the Breast Cancer Microenvironment: Detection, Characterization and Clinical Implication. Breast Cancer 2016, 24, 3–15. [Google Scholar] [CrossRef]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Carvajal, R.D.; Sosman, J.A.; Atkins, M.B.; et al. Safety, Activity, and Immune Correlates of Anti–PD-1 Antibody in Cancer. New England Journal of Medicine 2012, 366, 2443–2454. [Google Scholar] [CrossRef] [PubMed]
- Kitano, A.; Ono, M.; Yoshida, M.; Noguchi, E.; Shimomura, A.; Shimoi, T.; Kodaira, M.; Yunokawa, M.; Yonemori, K.; Shimizu, C.; et al. Tumour-Infiltrating Lymphocytes Are Correlated with Higher Expression Levels of PD-1 and PD-L1 in Early Breast Cancer. ESMO Open 2017, 2, e000150. [Google Scholar] [CrossRef] [PubMed]
- Vidula, N.; Yau, C.; Rugo, H.S. Programmed Cell Death 1 (PD-1) Receptor and Programmed Death Ligand 1 (PD-L1) Gene Expression in Primary Breast Cancer. Breast Cancer Research and Treatment 2021, 187, 387–395. [Google Scholar] [CrossRef]
- Ishigami, E.; Sakakibara, M.; Sakakibara, J.; Masuda, T.; Fujimoto, H.; Hayama, S.; Nagashima, T.; Sangai, T.; Nakagawa, A.; Nakatani, Y.; et al. Coexistence of Regulatory B Cells and Regulatory T Cells in Tumor-Infiltrating Lymphocyte Aggregates Is a Prognostic Factor in Patients with Breast Cancer. Breast Cancer 2018, 26, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Takenaka M, Seki N, Toh U, Hattori S, Kawahara A, Yamaguchi T, et al. FOXP3 Expression in Tumor Cells and Tumor-Infiltrating Lymphocytes Is Associated with Breast Cancer Prognosis. Molecular and Clinical Oncology 2013, 1, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Usman, A.N.; Ahmad, M.; Sinrang, A.W.; Natsir, S.; Takko, A.B.; Ariyandy, A.; Ilhamuddin, I.; Eragradini, A.R.; Hasan, I.I.; Hasyim, S. FOXP3 Regulatory T Cells on Prognosis of Breast Cancer. Breast Disease 2023, 42, 213–218. [Google Scholar] [CrossRef]
- Lal, A.; Chan, L.; DeVries, S.; Chin, K.; Scott, G.K.; Benz, C.C.; Chen, Y.-Y.; Waldman, F.M.; Hwang, E.S. FOXP3-Positive Regulatory T Lymphocytes and Epithelial FOXP3 Expression in Synchronous Normal, Ductal Carcinoma in Situ, and Invasive Cancer of the Breast. Breast Cancer Research and Treatment 2013, 139, 381–390. [Google Scholar] [CrossRef]
- Khaja, A.S.S.; Toor, S.M.; Salhat, H.E.; Faour, I.; Haq, N.U.; Ali, B.R.; Elkord, E. Preferential Accumulation of Regulatory T Cells with Highly Immunosuppressive Characteristics in Breast Tumor Microenvironment. Oncotarget 2017, 8, 33159–33171. [Google Scholar] [CrossRef]
- Bates, G.J.; Fox, S.B.; Han, C.; Leek, R.D.; Garcia, J.F.; Harris, A.L.; Banham, A.H. Quantification of Regulatory T Cells Enables the Identification of High-Risk Breast Cancer Patients and Those at Risk of Late Relapse. Journal of Clinical Oncology 2006, 24, 5373–5380. [Google Scholar] [CrossRef]
- Yeong, J.; Thike, A.A.; Lim, J.C.T.; Lee, B.; Li, H.; Wong, S.-C.; Hue, S.S.S.; Tan, P.H.; Iqbal, J. Higher Densities of Foxp3 Regulatory T Cells Are Associated with Better Prognosis in Triple-Negative Breast Cancer. Breast Cancer Research and Treatment 2017, 163, 21–35. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, Y.; Lu, F.; Zhao, X.; Nie, Z.; He, B. The Prognostic Values of FOXP3 Tumor-Infiltrating T Cells in Breast Cancer: a Systematic Review and Meta-Analysis. Clinical and Translational Oncology 2023, 25, 1830–1843. [Google Scholar] [CrossRef] [PubMed]
- Martinez, L.M.; Robila, V.; Clark, N.M.; Du, W.; Idowu, M.O.; Rutkowski, M.R.; Bos, P.D. Regulatory T Cells Control the Switch From in Situ to Invasive Breast Cancer. Frontiers in Immunology 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Yazaki, S.; Shimoi, T.; Yoshida, M.; Sumiyoshi-Okuma, H.; Arakaki, M.; Saito, A.; Kita, S.; Yamamoto, K.; Kojima, Y.; Nishikawa, T.; et al. Integrative Prognostic Analysis of Tumor–Infiltrating Lymphocytes, CD8, CD20, Programmed Cell Death-Ligand 1, and Tertiary Lymphoid Structures in Patients with Early-Stage Triple-Negative Breast Cancer Who Did Not Receive Adjuvant Chemotherapy. Breast Cancer Research and Treatment 2022, 197, 287–297. [Google Scholar] [CrossRef]
- Peng, G.-L.; Li, L.; Guo, Y.-W.; Yu, P.; Yin, X.-J.; Wang, S.; Liu, C.-P. CD8 Cytotoxic and FoxP3 Regulatory T Lymphocytes Serve as Prognostic Factors in Breast Cancer. American Journal of Translational Research 2019, 11, 5039–5053. [Google Scholar] [PubMed]
- Solis-Castillo, L.A.; Garcia-Romo, G.S.; Diaz-Rodriguez, A.; Reyes-Hernandez, D.; Tellez-Rivera, E.; Rosales-Garcia, V.H.; Mendez-Cruz, A.R.; Jimenez-Flores, J.R.; Villafana-Vazquez, V.H.; Pedroza-Gonzalez, A. Tumor-Infiltrating Regulatory T Cells, CD8/Treg Ratio, and Cancer Stem Cells Are Correlated with Lymph Node Metastasis in Patients with Early Breast Cancer. Breast Cancer 2020, 27, 837–849. [Google Scholar] [CrossRef] [PubMed]
- Song, I.H.; Heo, S.-H.; Bang, W.S.; Park, H.S.; Park, I.A.; Kim, Y.-A.; Park, S.Y.; Roh, J.; Gong, G.; Lee, H.J. Predictive Value of Tertiary Lymphoid Structures Assessed by High Endothelial Venule Counts in the Neoadjuvant Setting of Triple-Negative Breast Cancer. Cancer Research and Treatment 2017, 49, 399–407. [Google Scholar] [CrossRef]
- Chen, L.; Huang, Z.; Yao, G.; Lyu, X.; Li, J.; Hu, X.; Cai, Y.; Li, W.; Li, X.; Ye, C. The Expression of CXCL13 and Its Relation to Unfavorable Clinical Characteristics in Young Breast Cancer. Journal of Translational Medicine 2015, 13. [Google Scholar] [CrossRef]
- Dangaj, D.; Bruand, M.; Grimm, A.J.; Ronet, C.; Barras, D.; Duttagupta, P.A.; Lanitis, E.; Duraiswamy, J.; Tanyi, J.L.; Benencia, F.; et al. Cooperation between Constitutive and Inducible Chemokines Enables T Cell Engraftment and Immune Attack in Solid Tumors. Cancer Cell 2019, 35, 885–900.e10. [Google Scholar] [CrossRef]
- Masuda, N.; Lee, S.-J.; Ohtani, S.; Im, Y.-H.; Lee, E.-S.; Yokota, I.; Kuroi, K.; Im, S.-A.; Park, B.-W.; Kim, S.-B.; et al. Adjuvant Capecitabine for Breast Cancer after Preoperative Chemotherapy. New England Journal of Medicine 2017, 376, 2147–2159. [Google Scholar] [CrossRef]
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Costantino, J.P.; Wolmark, N.; Bonnefoi, H.; Cameron, D.; Gianni, L.; Valagussa, P.; et al. Pathological Complete Response and Long-Term Clinical Benefit in Breast Cancer: the CTNeoBC Pooled Analysis. The Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; Eynden, G.V. den; Baehner, F.L.; Penault-Llorca, F.; et al. The Evaluation of Tumor-Infiltrating Lymphocytes (TILs) in Breast Cancer: Recommendations by an International TILs Working Group 2014. Annals of Oncology 2015, 26, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Hendry, S.; Salgado, R.; Gevaert, T.; Russell, P.A.; John, T.; Thapa, B.; Christie, M.; Vijver, K. van de; Estrada, M.V.; Gonzalez-Ericsson, P.I.; et al. Assessing Tumor-Infiltrating Lymphocytes in Solid Tumors: A Practical Review for Pathologists and Proposal for a Standardized Method from the International Immuno-Oncology Biomarkers Working Group: Part 2: TILs in Melanoma, Gastrointestinal Tract Carcinomas, Non–Small Cell Lung Carcinoma and Mesothelioma, Endometrial and Ovarian Carcinomas, Squamous Cell Carcinoma of the Head and Neck, Genitourinary Carcinomas, and Primary Brain Tumors. Advances in Anatomic Pathology 2017, 24, 311–335. [Google Scholar] [CrossRef] [PubMed]
- Golicnik, J.P.; Gazic, B.; Ovcaricek, T.; Matos, E.; Borstnar, S. Prognostic Value of Routinely Determined Tumor Infiltrating Lymphocytes in Triple-Negative Breast Cancer. Journal of Clinical Oncology 2014, 32, 1125–1125. [Google Scholar] [CrossRef]
- Okcu, O.; Öztürk, S.D.; Öztürk, Çiğdem; Şen, B. ; Yasin, A. İrem; Bedir, R. Tumor-Infiltrating Lymphocytes (TILs)/Volume and Prognosis: The Value of TILs for Survival in HER2 and TN Breast Cancer Patients Treated with Chemotherapy. Annals of Diagnostic Pathology 2022, 58, 151930. [Google Scholar] [CrossRef]
- Jang, N.; Kwon, H.J.; Park, M.H.; Kang, S.H.; Bae, Y.K. Prognostic Value of Tumor-Infiltrating Lymphocyte Density Assessed Using a Standardized Method Based on Molecular Subtypes and Adjuvant Chemotherapy in Invasive Breast Cancer. Annals of Surgical Oncology 2018, 25, 937–946. [Google Scholar] [CrossRef]
- Mohammed, A.A.; Elsayed, F.M.; Algazar, M.; Rashed, H.E. Predictive and Prognostic Value of Tumor- Infiltrating Lymphocytes for Pathological Response to Neoadjuvant Chemotherapy in Triple Negative Breast Cancer. Gulf Journal of Oncology 2022, 1, 53–60. [Google Scholar]
- Minckwitz, G. von; Raab, G.; Caputo, A.; Schütte, M.; Hilfrich, J.; Blohmer, J.U.; Gerber, B.; Costa, S.D.; Merkle, E.; Eidtmann, H.; et al. Doxorubicin With Cyclophosphamide Followed by Docetaxel Every 21 Days Compared With Doxorubicin and Docetaxel Every 14 Days As Preoperative Treatment in Operable Breast Cancer: The GEPARDUO Study of the German Breast Group. Journal of Clinical Oncology 2005, 23, 2676–2685. [Google Scholar] [CrossRef]
- Denkert, C. Diagnostic and Therapeutic Implications of Tumor-Infiltrating Lymphocytes in Breast Cancer. Journal of Clinical Oncology 2013, 31, 836–837. [Google Scholar] [CrossRef]
- Loi, S.; Michiels, S.; Salgado, R.; Sirtaine, N.; Jose, V.; Fumagalli, D.; Kellokumpu-Lehtinen, P.-L.; Bono, P.; Kataja, V.; Desmedt, C.; et al. Tumor Infiltrating Lymphocytes Are Prognostic in Triple Negative Breast Cancer and Predictive for Trastuzumab Benefit in Early Breast Cancer: Results from the FinHER Trial. Annals of Oncology 2014, 25, 1544–1550. [Google Scholar] [CrossRef]
- Wein, L.; Savas, P.; Luen, S.J.; Virassamy, B.; Salgado, R.; Loi, S. Clinical Validity and Utility of Tumor-Infiltrating Lymphocytes in Routine Clinical Practice for Breast Cancer Patients: Current and Future Directions. Frontiers in Oncology 2017, 7. [Google Scholar] [CrossRef]
- Loi, S.; Michiels, S.; Adams, S.; Loibl, S.; Budczies, J.; Denkert, C.; Salgado, R. The Journey of Tumor-Infiltrating Lymphocytes as a Biomarker in Breast Cancer: Clinical Utility in an Era of Checkpoint Inhibition. Annals of Oncology 2021, 32, 1236–1244. [Google Scholar] [CrossRef] [PubMed]
- Pruneri, G.; Vingiani, A.; Denkert, C. Tumor Infiltrating Lymphocytes in Early Breast Cancer. The Breast 2018, 37, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Denkert, C.; Minckwitz, G. von; Brase, J.C.; Sinn, B.V.; Gade, S.; Kronenwett, R.; Pfitzner, B.M.; Salat, C.; Loi, S.; Schmitt, W.D.; et al. Tumor-Infiltrating Lymphocytes and Response to Neoadjuvant Chemotherapy With or Without Carboplatin in Human Epidermal Growth Factor Receptor 2–Positive and Triple-Negative Primary Breast Cancers. Journal of Clinical Oncology 2015, 33, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Issa-Nummer, Y.; Darb-Esfahani, S.; Loibl, S.; Kunz, G.; Nekljudova, V.; Schrader, I.; Sinn, B.V.; Ulmer, H.-U.; Kronenwett, R.; Just, M.; et al. Prospective Validation of Immunological Infiltrate for Prediction of Response to Neoadjuvant Chemotherapy in HER2-Negative Breast Cancer – A Substudy of the Neoadjuvant GeparQuinto Trial. PLoS ONE 2013, 8, e79775. [Google Scholar] [CrossRef] [PubMed]
- West, N.R.; Milne, K.; Truong, P.T.; Macpherson, N.; Nelson, B.H.; Watson, P.H. Tumor-Infiltrating Lymphocytes Predict Response to Anthracycline-Based Chemotherapy in Estrogen Receptor-Negative Breast Cancer. Breast Cancer Research 2011, 13. [Google Scholar] [CrossRef]
- Dieci, M.V.; Mathieu, M.C.; Guarneri, V.; Conte, P.; Delaloge, S.; Andre, F.; Goubar, A. Prognostic and Predictive Value of Tumor-Infiltrating Lymphocytes in Two Phase III Randomized Adjuvant Breast Cancer Trials. Annals of Oncology 2015, 26, 1698–1704. [Google Scholar] [CrossRef]
- Kotoula, V.; Chatzopoulos, K.; Lakis, S.; Alexopoulou, Z.; Timotheadou, E.; Zagouri, F.; Pentheroudakis, G.; Gogas, H.; Galani, E.; Efstratiou, I.; et al. Tumors with High-Density Tumor Infiltrating Lymphocytes Constitute a Favorable Entity in Breast Cancer: a Pooled Analysis of Four Prospective Adjuvant Trials. Oncotarget 2015, 7, 5074–5087. [Google Scholar] [CrossRef]
- Jong, V.M.T. de; Wang, Y.; Hoeve, N.D. ter; Opdam, M.; Stathonikos, N.; Jóźwiak, K.; Hauptmann, M.; Cornelissen, S.; Vreuls, W.; Rosenberg, E.H.; et al. Prognostic Value of Stromal Tumor-Infiltrating Lymphocytes in Young, Node-Negative, Triple-Negative Breast Cancer Patients Who Did Not Receive (Neo)Adjuvant Systemic Therapy. Journal of Clinical Oncology 2022, 40, 2361–2374. [Google Scholar] [CrossRef]
- Minckwitz, G. von; Schneeweiss, A.; Loibl, S.; Salat, C.; Denkert, C.; Rezai, M.; Blohmer, J.U.; Jackisch, C.; Paepke, S.; Gerber, B.; et al. Neoadjuvant Carboplatin in Patients with Triple-Negative and HER2-Positive Early Breast Cancer (GeparSixtoGBG 66): a Randomised Phase 2 Trial. The Lancet Oncology 2014, 15, 747–756. [Google Scholar] [CrossRef]
- Minckwitz, G. von; Rezai, M.; Loibl, S.; Fasching, P.A.; Huober, J.; Tesch, H.; Bauerfeind, I.; Hilfrich, J.; Eidtmann, H.; Gerber, B.; et al. Capecitabine in Addition to Anthracycline- and Taxane-Based Neoadjuvant Treatment in Patients With Primary Breast Cancer: Phase III GeparQuattro Study. Journal of Clinical Oncology 2010, 28, 2015–2023. [Google Scholar] [CrossRef]
- Untch, M.; Loibl, S.; Bischoff, J.; Eidtmann, H.; Kaufmann, M.; Blohmer, J.-U.; Hilfrich, J.; Strumberg, D.; Fasching, P.A.; Kreienberg, R.; et al. Lapatinib versus Trastuzumab in Combination with Neoadjuvant Anthracycline-Taxane-Based Chemotherapy (GeparQuinto, GBG 44): a Randomised Phase 3 Trial. The Lancet Oncology 2012, 13, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Untch, M.; Jackisch, C.; Schneeweiss, A.; Conrad, B.; Aktas, B.; Denkert, C.; Eidtmann, H.; Wiebringhaus, H.; Kümmel, S.; Hilfrich, J.; et al. Nab-Paclitaxel versus Solvent-Based Paclitaxel in Neoadjuvant Chemotherapy for Early Breast Cancer (GeparSepto—GBG 69): a Randomised, Phase 3 Trial. The Lancet Oncology 2016, 17, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Heppner, B.I.; Untch, M.; Denkert, C.; Pfitzner, B.M.; Lederer, B.; Schmitt, W.; Eidtmann, H.; Fasching, P.A.; Tesch, H.; Solbach, C.; et al. Tumor-Infiltrating Lymphocytes: A Predictive and Prognostic Biomarker in Neoadjuvant-Treated HER2-Positive Breast Cancer. Clinical Cancer Research 2016, 22, 5747–5754. [Google Scholar] [CrossRef] [PubMed]
- Bussard, K.M.; Mutkus, L.; Stumpf, K.; Gomez-Manzano, C.; Marini, F.C. Tumor-Associated Stromal Cells as Key Contributors to the Tumor Microenvironment. Breast Cancer Research 2016, 18. [Google Scholar] [CrossRef]
- Baxevanis, C.N.; Fortis, S.P.; Perez, S.A. The Balance between Breast Cancer and the Immune System: Challenges for Prognosis and Clinical Benefit from Immunotherapies. Seminars in Cancer Biology 2021, 72, 76–89. [Google Scholar] [CrossRef]
- Negro, G.; Aschenbrenner, B.; Brezar, S.K.; Cemazar, M.; Coer, A.; Gasljevic, G.; Savic, D.; Sorokin, M.; Buzdin, A.; Callari, M.; et al. Molecular Heterogeneity in Breast Carcinoma Cells with Increased Invasive Capacities. Radiology and Oncology 2020, 54, 103–118. [Google Scholar] [CrossRef]
- Baker, K.; Lachapelle, J.; Zlobec, I.; Bismar, T.A.; Terracciano, L.; Foulkes, W.D. Prognostic Significance of CD8 T Lymphocytes in Breast Cancer Depends upon Both Oestrogen Receptor Status and Histological Grade. Histopathology 2011, no–no. [Google Scholar] [CrossRef]
- Virassamy, B.; Caramia, F.; Savas, P.; Sant, S.; Wang, J.; Christo, S.N.; Byrne, A.; Clarke, K.; Brown, E.; Teo, Z.L.; et al. Intratumoral CD8 T Cells with a Tissue-Resident Memory Phenotype Mediate Local Immunity and Immune Checkpoint Responses in Breast Cancer. Cancer Cell 2023, 41, 585–601.e8. [Google Scholar] [CrossRef]
- Seo, A.N.; Lee, H.J.; Kim, E.J.; Kim, H.J.; Jang, M.H.; Lee, H.E.; Kim, Y.J.; Kim, J.H.; Park, S.Y. Tumour-Infiltrating CD8 Lymphocytes as an Independent Predictive Factor for Pathological Complete Response to Primary Systemic Therapy in Breast Cancer. British Journal of Cancer 2013, 109, 2705–2713. [Google Scholar] [CrossRef]
- Heimes, A.-S.; Madjar, K.; Edlund, K.; Battista, M.J.; Almstedt, K.; Elger, T.; Krajnak, S.; Rahnenführer, J.; Brenner, W.; Hasenburg, A.; et al. Subtype-Specific Prognostic Impact of Different Immune Signatures in Node-Negative Breast Cancer. Breast Cancer Research and Treatment 2017, 165, 293–300. [Google Scholar] [CrossRef]
- Criscitiello, C.; Bayar, M.A.; Curigliano, G.; Symmans, F.W.; Desmedt, C.; Bonnefoi, H.; Sinn, B.; Pruneri, G.; Vicier, C.; Pierga, J.Y.; et al. A Gene Signature to Predict High Tumor-Infiltrating Lymphocytes after Neoadjuvant Chemotherapy and Outcome in Patients with Triple-Negative Breast Cancer. Annals of Oncology 2018, 29, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Han, M.; Li, J.; Wu, S.; Wu, C.; Yu, Y.; Liu, Y. Comparison of the Tumor Immune Microenvironment Phenotypes in Different Breast Cancers after Neoadjuvant Therapy. Cancer Medicine 2022, 12, 2906–2917. [Google Scholar] [CrossRef] [PubMed]
- Ding, Z.-C.; Zhou, G. Cytotoxic Chemotherapy and CD4 Effector T Cells: An Emerging Alliance for Durable Antitumor Effects. Clinical and Developmental Immunology 2012, 2012, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Wing, J.B.; Tanaka, A.; Sakaguchi, S. Human FOXP3 Regulatory T Cell Heterogeneity and Function in Autoimmunity and Cancer. Immunity 2019, 50, 302–316. [Google Scholar] [CrossRef] [PubMed]
- West, N.R.; Kost, S.E.; Martin, S.D.; Milne, K.; deLeeuw, R.J.; Nelson, B.H.; Watson, P.H. Tumour-Infiltrating FOXP3 Lymphocytes Are Associated with Cytotoxic Immune Responses and Good Clinical Outcome in Oestrogen Receptor-Negative Breast Cancer. British Journal of Cancer 2012, 108, 155–162. [Google Scholar] [CrossRef]
- Goda, N.; Sasada, S.; Shigematsu, H.; Masumoto, N.; Arihiro, K.; Nishikawa, H.; Sakaguchi, S.; Okada, M.; Kadoya, T. The Ratio of CD80.167em\hspace0.167emlymphocytes to Tumor-Infiltrating Suppressive FOXP30.167em\hspace0.167emeffector Regulatory T Cells Is Associated with Treatment Response in Invasive Breast Cancer. Discover Oncology 2022, 13. [Google Scholar] [CrossRef]
- Asano, Y.; Kashiwagi, S.; Goto, W.; Kurata, K.; Noda, S.; Takashima, T.; Onoda, N.; Tanaka, S.; Ohsawa, M.; Hirakawa, K. Tumour-Infiltrating CD8 to FOXP3 Lymphocyte Ratio in Predicting Treatment Responses to Neoadjuvant Chemotherapy of Aggressive Breast Cancer. British Journal of Surgery 2016, 103, 845–854. [Google Scholar] [CrossRef]
- Filion, L.G.; Izaguirre, C.A.; Garber, G.E.; Huebsh, L.; Aye, M.T. Detection of Surface and Cytoplasmic CD4 on Blood Monocytes from Normal and HIV-1 Infected Individuals. Journal of Immunological Methods 1990, 135, 59–69. [Google Scholar] [CrossRef]
Figure 1.
CONSORT flow diagram for the study.
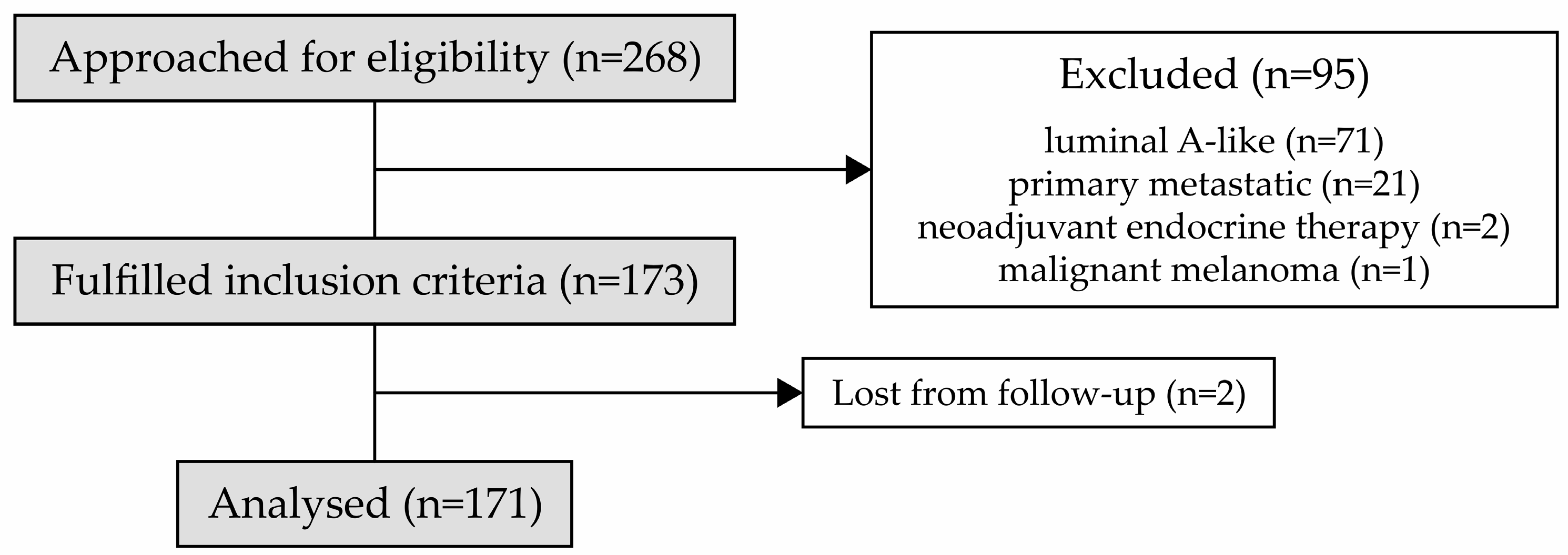
Figure 2.
Histopathological slides of patients with total tumour-infiltrating lymphocytes (TIL) (high on A1 and low on A2) and TILs subtypes (CD8+ TILs, CXCL13+ TILs, PD-1+ TILs and FOXP3+ TILs) (high on B1, C1, D1, E1; low on B2, C2, D2, E2).
Figure 2.
Histopathological slides of patients with total tumour-infiltrating lymphocytes (TIL) (high on A1 and low on A2) and TILs subtypes (CD8+ TILs, CXCL13+ TILs, PD-1+ TILs and FOXP3+ TILs) (high on B1, C1, D1, E1; low on B2, C2, D2, E2).
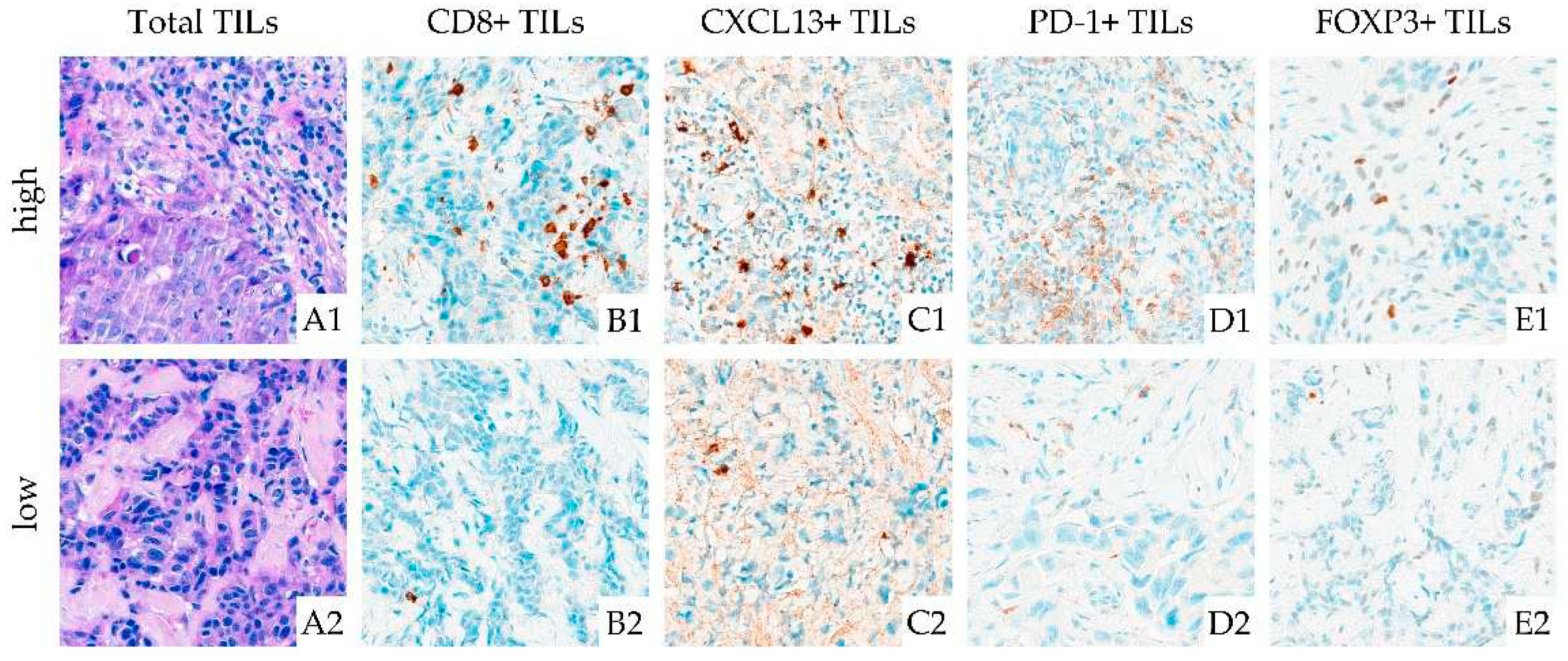
Figure 3.
The proportion of pathologic complete response (pCR) in 10% tumour-infiltrating lymphocyte (TIL) groups, together with 95% confidence intervals.
Figure 3.
The proportion of pathologic complete response (pCR) in 10% tumour-infiltrating lymphocyte (TIL) groups, together with 95% confidence intervals.
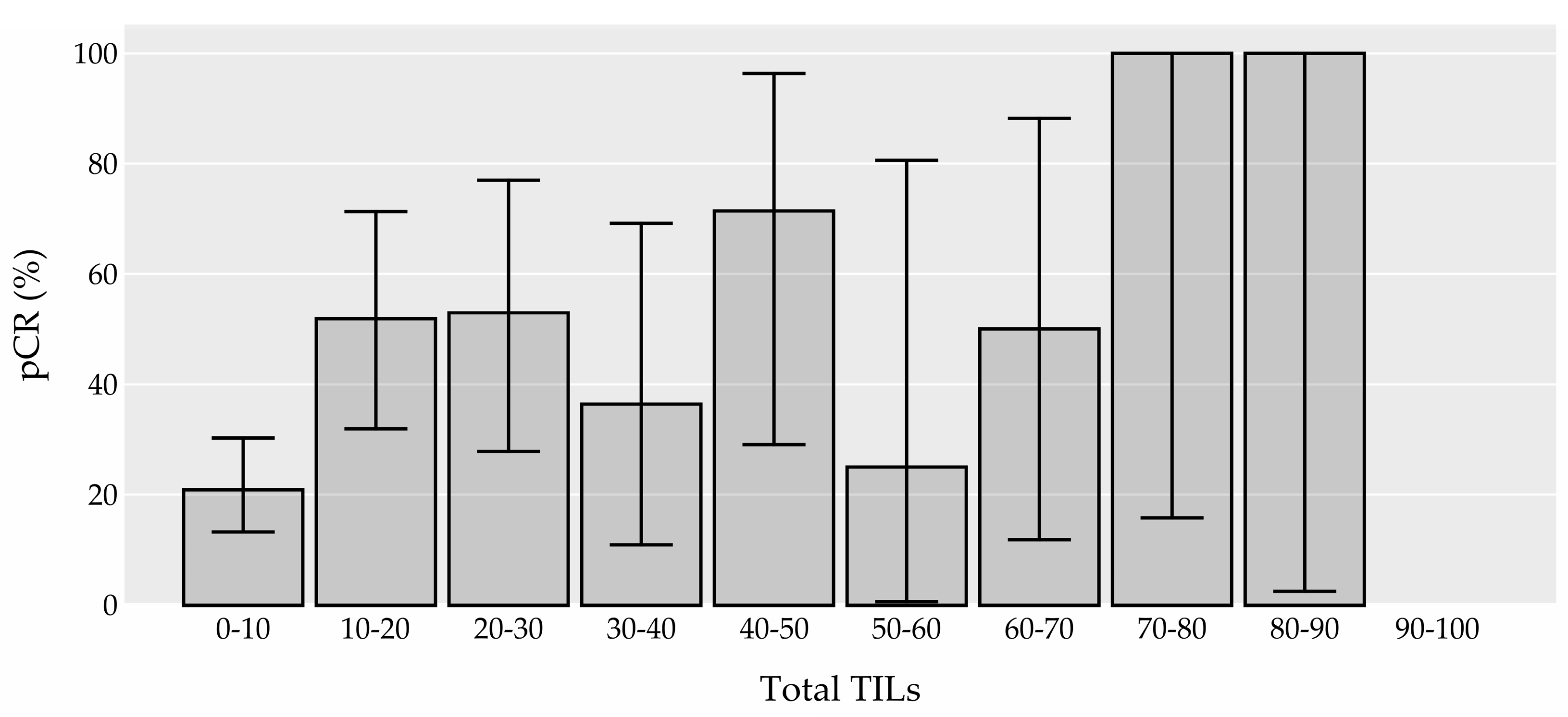
Figure 4.
The proportion of pathologic complete response (pCR) in 25% tumour-infiltrating lymphocyte (TIL) groups in different molecular subtypes, together with 95% confidence intervals. Abbreviations: HER-2: human epidermal growth factor receptor 2
Figure 4.
The proportion of pathologic complete response (pCR) in 25% tumour-infiltrating lymphocyte (TIL) groups in different molecular subtypes, together with 95% confidence intervals. Abbreviations: HER-2: human epidermal growth factor receptor 2
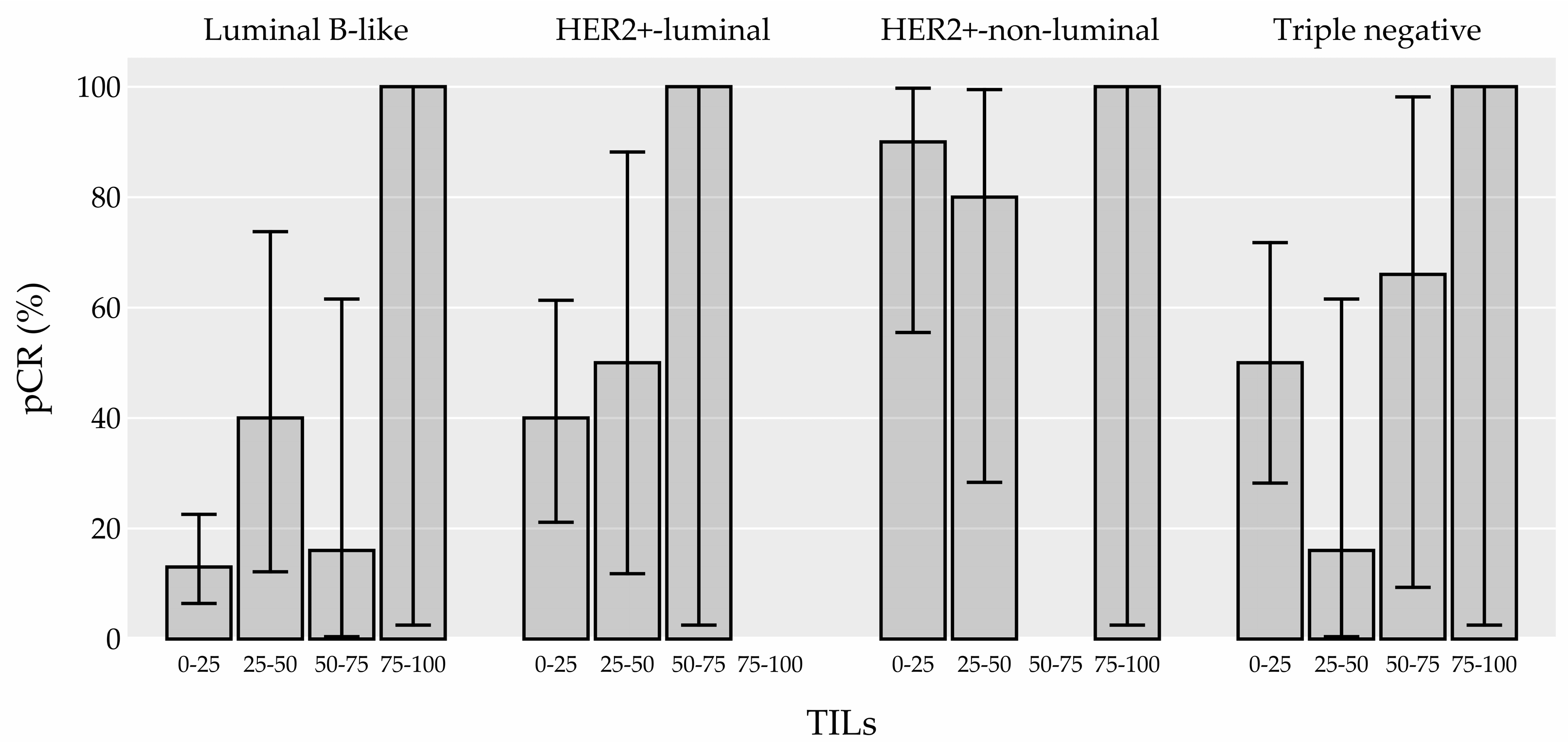
Figure 5.
Tumour-infiltrating lymphocytes (TIL) density (in percentages) in the whole TIL group and according to TILs subtypes, boxplots. Abbreviations: min: minimum; max: maximum; q3: 3rd quartile; q1: 1st quartile; TIL: tumour-infiltrating lymphocytes.
Figure 5.
Tumour-infiltrating lymphocytes (TIL) density (in percentages) in the whole TIL group and according to TILs subtypes, boxplots. Abbreviations: min: minimum; max: maximum; q3: 3rd quartile; q1: 1st quartile; TIL: tumour-infiltrating lymphocytes.
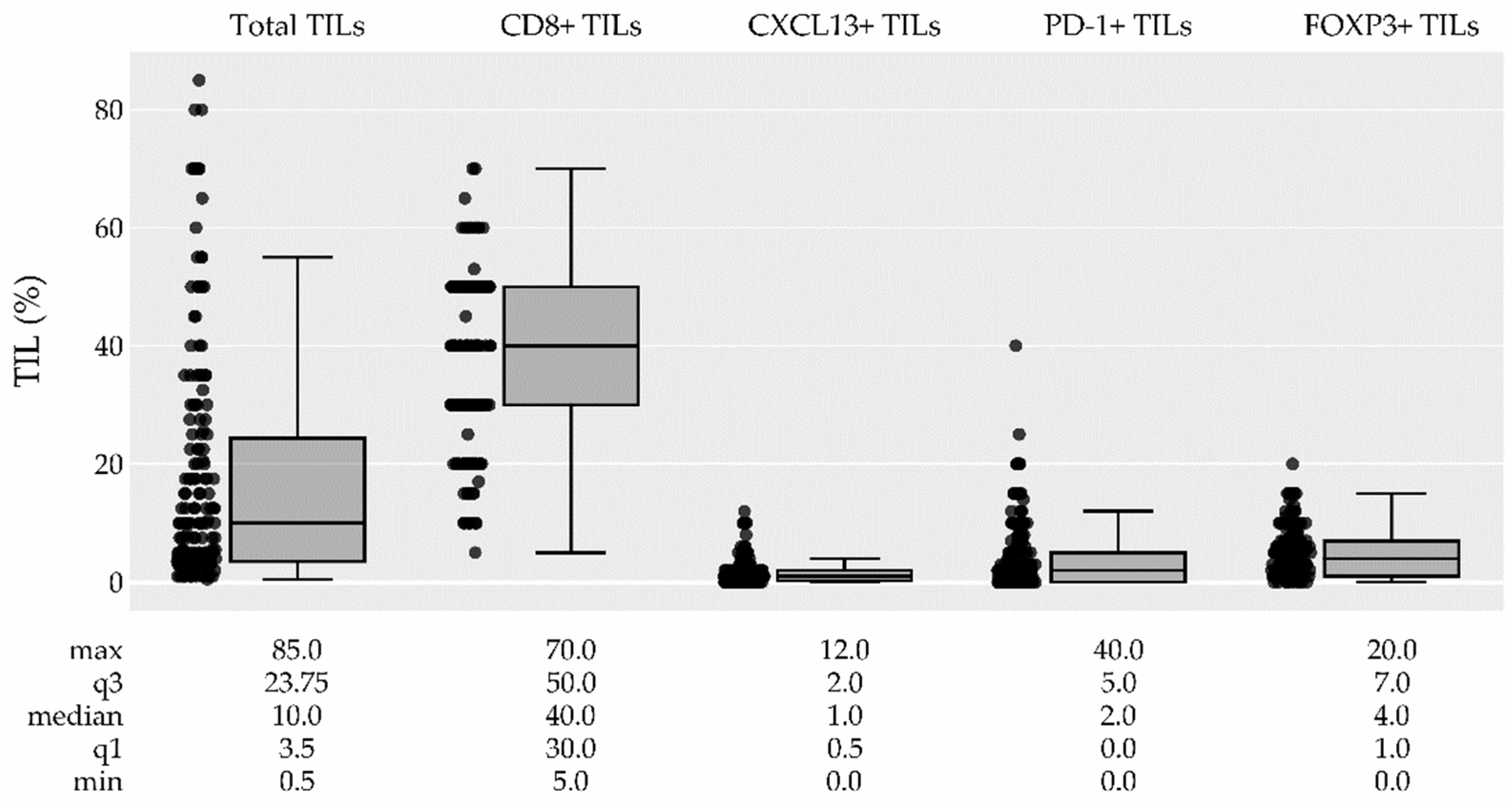
Figure 6.
The distribution of CD8+ TILs (a), CXCL13+ TILs (b), PD-1+ TILs (c) and FOXP3+ TILs (d) among the breast cancer subtypes, boxplots. Abbreviations: min: minimum; max: maximum; q3: 3rd quartile; q1: 1st quartile; TIL: tumour-infiltrating lymphocytes; HER-2: human epidermal growth factor receptor 2.
Figure 6.
The distribution of CD8+ TILs (a), CXCL13+ TILs (b), PD-1+ TILs (c) and FOXP3+ TILs (d) among the breast cancer subtypes, boxplots. Abbreviations: min: minimum; max: maximum; q3: 3rd quartile; q1: 1st quartile; TIL: tumour-infiltrating lymphocytes; HER-2: human epidermal growth factor receptor 2.
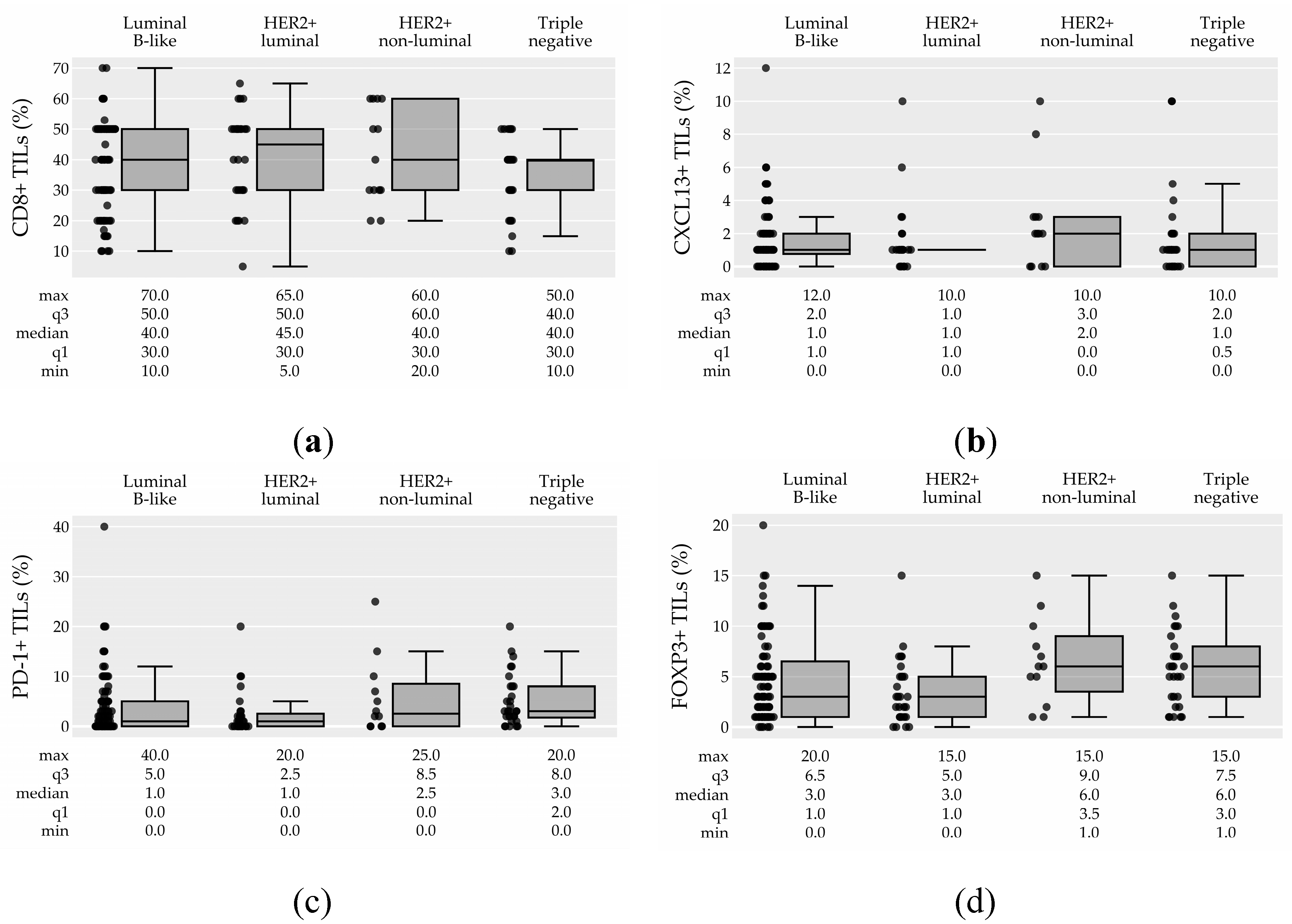

Table 1.
Univariate analysis of patients’ characteristics and tumour features, and their association with pathologic complete response (pCR) .
Table 1.
Univariate analysis of patients’ characteristics and tumour features, and their association with pathologic complete response (pCR) .
| Characteristic (number of missing values) |
All patients (n=171) | Patients with pCR (n=59) | Patients without pCR (n=112) |
OR (95% CI) | p-value | Adjusted p-value† |
||
|---|---|---|---|---|---|---|---|---|
| Age median (IQR) (0) | 48.4 (41.7-57.4) | 46.4 (39.4-56.0) | 49.0 (44.7-57.5) | 0.97 (0.94-1.00) | 0.046 | 0.510 | ||
| Histology n (%) (2) | 0.014 | 0.176 | ||||||
| IBC of no special type | 161 (96.0%) | 58 (36.0%) | 103 (64.0%) | 7.35 (0.84-964.63) | 0.077 | 0.613 | ||
| ILC | 6 (4.0%) | 0 (0.0%) | 6 (100.0%) | ref. | ref. | ref. | ||
| Other | 2 (1.0%) | 0 (0.0%) | 2 (100.0%) | 2.60 (0.01-553.14) | 0.642 | 1.000 | ||
| Grade n (%) (1) | ||||||||
| Grade 3 | 124 (73.0%) | 54 (44.0%) | 70 (56.0%) | 5.83 (2.41-16.89) | <0.001 | <0.001 | ||
| Grade 2 | 46 (27.0%) | 5 (11.0%) | 41 (89.0%) | ref. | ref. | ref. | ||
| Molecular subtype n (%) (0) | <0.001 | <0.001 | ||||||
| Luminal B-like | 91 (53.0%) | 16 (18.0%) | 75 (82.0%) | ref. | ref. | |||
| Her2+-luminal | 32 (19.0%) | 14 (44.0%) | 18 (56.0%) | 3.59 (1.50-8.65) | 0.004 | 0.058 | ||
| Her2+-non-luminal | 16 (9.0%) | 14 (88.0%) | 2 (12.0%) | 26.54 (7.23-144.62) | <0.001 | < 0.001 | ||
| Triple negative | 32 (19.0%) | 15 (47.0%) | 17 (53.0%) | 4.05 (1.71-9.77) | 0.002 | 0.023 | ||
| Ki-67 median (IQR) (1) | 30.0 (20.0-50.0) | 50.0 (30.0-60.0) | 30.0 (20.0-40.0) | 1.04 (1.02-1.05) | <0.001 | < 0.001 | ||
| Ki-67 n (%) (1) | <0.001 | <0.001 | ||||||
| 10-20% | 46 (27.0%) | 3 (7.0%) | 43 (93.0%) | ref. | ref. | ref. | ||
| 20-40% | 66 (39.0%) | 25 (38.0%) | 41 (62.0%) | 7.64 (2.58-30.11) | <0.001 | 0.002 | ||
| >40% | 58 (34.0%) | 31 (53.0%) | 27 (47.0%) | 14.24 (4.78-56.53) | <0.001 | < 0.001 | ||
| Tumor stage n (%) (15) | 0.325 | 1.000 | ||||||
| T1 (≤20mm) | 25 (16.0%) | 10 (40.0%) | 15 (60.0%) | ref. | ref. | ref. | ||
| T2 (>20≤50) | 113 (72.0%) | 39 (35.0%) | 74 (65.0%) | 0.78 (0.33-1.92) | 0.584 | 1.000 | ||
| T3 (>50 mm) | 18 (12.0%) | 6 (33.0%) | 12 (67.0%) | 0.77 (0.22-2.60) | 0.670 | 1.000 | ||
| Lymph nodes n (%) (0) | ||||||||
| Positive | 125 (73.0%) | 37 (30.0%) | 88 (70.0%) | ref. | ref. | ref. | ||
| Negative | 46 (27.0%) | 22 (48.0%) | 24 (52.0%) | 2.17 (1.09-4.33) | 0.028 | 0.335 | ||
| Total TILs median (IQR) (0) | 10.0 (3.5-23.8) | 17.5 (7.5-35.0) | 5.0 (3.0-17.5) | 1.03 (1.01-1.05) | <0.001 | 0.005 | ||
| Total TILs n (%) (0) | ||||||||
| Low (<60%) | 161 (94.0%) | 53 (33.0%) | 108 (67.0%) | ref. | ref. | ref. | ||
| High (≥60%) | 10 (6.0%) | 6 (60.0%) | 4 (40.0%) | 2.93 (0.85-10.99) | 0.088 | 0.615 | ||
| CD8+ TILs median (IQR) (12) | 40.0 (30.0-50.0) | 40.0 (30.0-50.0) | 40.0 (27.5-50.0) | 1.02 (1.00-1.04) | 0.122 | 0.731 | ||
| CXCL13+ TILs median (IQR) (16) | 1.0 (0.5-2.0) | 1.0 (1.0-2.0) | 1.0 (0.0-2.0) | 1.03 (0.89-1.19) | 0.673 | 1.000 | ||
| PD-1+ TILs median (IQR) (14) | 2.0 (0.0-5.0) | 3.0 (1.0-8.0) | 1.0 (0.0-5.0) | 1.05 (1.00-1.12) | 0.053 | 0.510 | ||
| FOXP3+ TILs median (IQR) (13) | 4.0 (1.0-7.0) | 5.0 (2.0-7.0) | 3.0 (1.0-6.0) | 1.08 (1.00-1.18) | 0.051 | 0.510 | ||
† p values are adjusted for multiple comparisons between groups. Univariate analysis was performed. Statistically significant adjustet p-values are presented in bold. Abbreviations: IBC: invasive breast carcinoma; ILC: invasive lobular carcinoma; TIL: tumour-infiltrating lymphocytes; pCR: pathologic complete response; OR: odds ratio; HER-2: human epidermal growth factor receptor 2; CI: confidence interval; ref.: reference; IQR: interquartile range; n: number.
Table 2.
Multivariable model of prognostic factors for pathological complete response (AUC=0.817, loglikelihood ratio test p<0.001).
Table 2.
Multivariable model of prognostic factors for pathological complete response (AUC=0.817, loglikelihood ratio test p<0.001).
| Characteristic | OR (95% CI) | p-value | |
|---|---|---|---|
| Total TILs (per 10%) | 1.27 (1.05-1.54) | 0.012 | |
| Age | 0.98 (0.95-1.01) | 0.232 | |
| Ki-67 (per 10%) | 1.38 (1.13-1.70) | 0.001 | |
| Negative lymph nodes | 2.51 (1.13-5.69) | 0.024 | |
| HER2+-luminal, HER2+-non-luminal, TN vs lumB | 5.11 (2.43-11.36) | <0.001 |
Statistically significant p-values are presented in bold. TIL: tumour-infiltrating lymphocytes; TN: triple negative subtype; lumB: luminal B subtype; HER-2: human epidermal growth factor receptor 2; OR: odds ratio; CI: confidence interval; AUC: area under the curve.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



