
Submitted:
05 August 2023
Posted:
22 August 2023
You are already at the latest version
Abstract
Childbirth education classes represent an antenatal tool for supporting pregnant women and couples in increasing knowledge on pregnancy, delivery, breastfeeding, and newborn care. The aim of this study was to investigate the impact of the additional lesson to the prenatal course regarding the advantage of the vaccination on mitigation of maternal anxiety. An observational study was designed including participants in childbirth education classes, comparing courses enhanced by the extra lesson on vaccination during pregnancy versus those lacking it. Assessment of the impact of prenatal educational on vaccine was measured by using validated questionnaires (State-Trait Anxiety Inventory, STAI; Perceived Stress Scale, PSS; World Health Organization- Five Well-Being Index, WHO-5). A total of 145 pregnant women participated to the investigation by answering to the online survey. Of them, 33 patients (22.8%) belong to the course without lesson on vaccine, while 112 (77.2%) participated to online prenatal education inclusive of additional meeting on usefulness to get vaccinated during pregnancy. No statistical differences were found between study groups in demographics and perinatal outcomes. Participants to enriched course reported lower basal anxiety levels than those without lesson on vaccine (STAI-State, normal score <40, 30 vs. 19%, p-value 0.041; STAI-State, mild score 40-50, 78 vs 67%, p-value 0.037). With reference to the last two weeks, maternal wellbeing level was improved by the added class (score >13 as measurement of wellbeing: 62% vs 80%, p-value<0.05). Moderate perceived stress assessed by PSS was found in those pregnant women without prenatal education on vaccine (64 vs 50%, p-value 0.042). The introduction of a lesson regarding on vaccination during pregnancy in the program of prenatal education courses improves maternal anxiety levels and wellbeing, in addition to reducing perceived stress.
Keywords:
pregnancy
; vaccine
; health literacy
; prenatal education classes
1. Introduction
Nowadays, vaccination is one of the most successful and cost-effective public health interventions, mainly when the increased vaccine uptake endorses immunization programs. In this scenario, a pivotal role might be played by the hesitancy, defined as the reluctance or refusal to vaccinate despite the availability of vaccines, also listed as one of the ten threats to global health by the World Health Organization (WHO) [1].
In Italy, a significant and constant decrease in coverage from 2012 to 2017 for all vaccines at all age-groups has been reported. In response, the National Vaccination Prevention Plan 2017-2019 was proposed with effective and homogeneous strategies to be implemented throughout the national territory [2]. In this scenario, early vaccine programs against COVID-19 have recorded suboptimal coverage in certain geographical areas or among vulnerable population groups [3,4,5,6,7], although the high rates of infections worldwide [8]. Multilevel strategies have been planned to improve vaccine uptake, in order to increase the confidence in vaccination and reduce hesitancy, mainly among people at higher risk. In Italy, an additional call to get vaccinated was promoted by the Conferenza Episcopale Italiana, the permanent assembly that assumes specific relevance in the relationships between the Italian State and the Catholic Church.
In obstetrics, COVID-19 pandemic has emphasized the pivotal role of vaccination during pregnancy for minimizing the detrimental effects of infectious diseases on the feto-maternal dyad. However, pregnant women have generally a negative attitude to receive vaccination, as described in reports from flu and pertussis coverage during pregnancy [9,10]. Inadequate information, concerns about the fetal safety, and underestimation of the risks related to both illness and infection are the most common explanations for vaccine hesitancy among pregnant women. In agreement with the definition of Bussink-Voorend, vaccine hesitancy represents ‘a psychological state of indecisiveness that people may experience when making a decision regarding vaccination”, regardless of their final choice [11]. A growing body of evidence has demonstrated the crucial role played by health professionals in this decision-making process, so to be the most trusted sources of health- and vaccine-related information for pregnant women [12,13,14,15,16,17].
In Italy, the offer to get vaccinated after the availability of Covid-19 vaccines in December 2021 was initially limited only to high-risk categories, such as health care professionals, nursing homes residents, highly vulnerable patients, and people aged ≥ 80 years [18]. At this stage, pregnancy was not considered a priority status and excluded from vaccination call. From the Italian Obstetric Surveillance System (ItOSS) no recommendation to vaccine pregnant women was indicated. Following not only the main findings from medical literature focused on the outcomes of Sars-Cov-2 infections worldwide, inclusive of the higher risk of stillbirth and/or other complications and severe illness among women with Covid-19, but also of the safe and effective profile of vaccination against Covid-19 both for the mother and for the child [19,20,21,22,23,24], national recommendations changed accordingly. Italian women of childbearing age started being vaccinated on 20th May 2021, followed by people aged 30–39 (on May 27) and 12–29 (on June 2); and on September 24, the Italian Ministry of Health published the Circular No.43293 indicating vaccination at any stage of pregnancy and during breastfeeding [25].
Unfortunately, the heterogeneous position regarding COVID-19 vaccine during pregnancy has determined fear and confusion among pregnant women over the time. In this context, the importance of health care professionals’ advice and official recommendations for pregnant women has been empathized [26,27,28]. A specific communication context requiring special communication skills has been emerging. Additional efforts have been planned, ranging from individual/collective counseling to dedicated open day to vaccine pregnant women, by using also modern tool for communication [29,30].
Childbirth education classes are antenatal health promotion and educational activities offered to pregnant women and their partners, playing a promising public health and empowerment tool [31]. In Italy, childbirth education classes can be offered both by public institutions and private providers. In absence of clear guidelines or standards, the program might include 3-7 sessions provided by a midwife, besides other professionals (i.e., gynecologists, pediatricians, and anesthetists). The percentage of Italian women who attend childbirth education classes stands at 61.7% in the North, 55% in the Centre, 32.5% in the South and 36.7% on the Islands with significant reduction rates for foreign national (23.3%), mainly due to the limited offer of specialized courses [32,33].
On May 2021, Italian Society of Obstetrics and Gynecology (SIGO) published a position paper with the aim to sensitize to get vaccine against COVID-19 all pregnant women defined as delicate people and all health care professionals involved in prenatal care to promote vaccination sharing updated evidence on its safety and efficacy [34].
Current prenatal education for parents regarding pregnancy, labor, birth, and neonatal care are lacking in an ad hoc intervention on usefulness to get vaccinated during pregnancy against flu, pertussis, and COVID-19. Therefore, we aimed to explore the impact of an additional lesson on vaccination during pregnancy and to assess its impact on maternal anxiety by using well-established questionnaires.
2. Materials and Methods
2.1. Study Design, Population and Ethics
An observational study was designed including participants to childbirth education classes, comparing courses enhanced by the supplementary lesson on vaccination during pregnancy versus those lacking it.
San Paolo University Hospital in Milan offers to all pregnant women a mixed prenatal course inclusive of online and in presence lessons for a total of 11, with a general duration of 7 weeks starting from 30 until 36 weeks of gestation. The duration of the meetings reached 90 minutes as median, divided into a narrative and Q&A part, each of them with a duration of 45 minutes. Different health professionals are involved, such as midwifes, obstetricians, pediatricians, anesthesiologists, psychologists. The chosen topics are the following: 1. labor; 2. birth; 3. postnatal period; 4. early neonatal care; 5. at home neonatal care; 6. preventive strategies for perineum damage; 7. pain relief strategies during labor; 8. medical intervention during labor; 9. focus on paternal role; 10. vaccination during pregnancy; 11. emotional aspects during pregnancy, birth and postpartum.
Since March 2022, a special lesson on vaccination during pregnancy was added to the program of our prenatal education. Overall information was organized in slides presentation, available for all participants at the end of the course and inclusive of email address for additional questions. Participants to the enriched course were allocated in the study group and matched with those unexposed to lesson or meeting on vaccination, defined as control group. The inclusion criteria included age between 18–45 years, being able to read and write Italian, not having any mental illness, the possibility to receive educational messages by using an access to the Internet and virtual networks. Exclusion criteria included language barrier, age less than 18 years, having not participating in more than one face-to-face training session and not completing questionnaires.
All patients signed an informed consent form at the beginning of the course. The study was included in the project for assessing the performance of the quality of care (ASST Santi Paolo Carlo, n. 2170, September 2022).
2.2. Questionnaires and Measurements
An anonymous online structured questionnaire was sent through emails. The questionnaire was structured in two sections:
- -
- Part-A finalized to acquire items in maternal characteristics and perinatal outcomes (maternal age, ethnicity, country of birth, education level, working status, smoking status, medical and obstetric history, perinatal outcomes). Data reported by patients were confirmed by reviewing electronic medical records.
- -
- Part-B finalized to assess the impact of prenatal educational on vaccine measured by using validated questionnaires (State-Trait Anxiety Inventory, STAI; Perceived Stress Scale, PSS; World Health Organization- Five Well-Being Index, WHO-5) addressed to the patients. All tests were administrated in Italian translation.
STAI is a validated scale for scoring anxiety, able to measure both trait anxiety (STAI-T) and state anxiety (STAI-S). An abnormal value of STAI was considered when >40 [35].
WHO-5 is one of the most sensitive and valid patient-reported outcome measures (PROMs) of subjective well-being and can be also used as a highly sensitive screening tool for depression. Time reference is related to last two weeks. The raw score ranges from 0 to 25, 0 representing worst possible and 25 representing the best possible quality of life [36].
PSS is a stress assessment instrument, originally developed in 1983, remains a choice for helping understand how different situations affect feelings and perceived stress during the last month. Individual scores on the PSS can range from 0 to 40 with higher scores indicating higher perceived stress. Scores ranging from 0-13 would be considered low stress, 14-26 moderate stress and 27-40 high perceived stress, respectively [37].
2.3. Statistical Analysis
Descriptive statistics were calculated for the variables considered, and data are expressed as n (%) for categorical variables and median (standard deviation) for continuous variables. Chi-square or Fisher exact tests were used to compare group differences of categorical variables and Wilcoxon or Mann–Whitney U test for continuous variables. Pearson’s correlation was used to calculate the relationship between variables. A two-sided p-value of <0.05 was considered significant.
3. Results
A total of 149 pregnant women were enrolled in the study, 4 (5,9%) of them were excluded after declination to participate in the investigation, leaving the study population inclusive of 145 pregnant women willing to answer to the online survey. Of them, 33 patients (22.8%) belong to the prenatal education without lesson on vaccine, while 112 (77.2%) participated to prenatal education inclusive of additional class on usefulness to get vaccinated during pregnancy.
In Table 1 maternal characteristics and pregnancy outcomes were reported. Both groups were similar, and no statistical differences were found between study groups in all demographic issues.
In Table 2 pregnancy outcomes were reported. No statistical differences were found between study groups perinatal outcomes. In particular, no additional complication at birth were found as predominant in one of two groups.
Participants to enriched course reported lower anxiety level than those without class on vaccination during pregnancy. A significant decrease in basal conditions (STAI-S, normal score, 30 vs. 19%, p-value 0.041), and a decrease of mild levels (STAI-S, mild score, 78 vs 67%, p-value 0.037) were calculated, as represented in Figure 1.
During the last two weeks, maternal wellbeing level, assessed by WHO-5 WBI as a short and generic global rating scale measuring subjective well-being, was improved by the added class on vaccination during pregnancy, as demonstrated by the raised rates of scores (score >13 as measurements of wellbeing: 62% vs 80%, p-value<0.05) (Figure 2).
In Figure 3, moderate perceived stress assessed by PSS was found in those pregnant women without prenatal education on vaccine (64 vs 50%, p-value 0.042).
4. Discussion
To the best of our knowledge, for the first time a study shows the benefits on maternal anxiety, wellbeing, and depression by prenatal education courses enriched by added lesson on getting vaccinated during pregnancy. As expected, among participants without information from health care providers there was not only greater fear of abnormal perinatal outcomes induced by the vaccine, but also low scores of maternal wellbeing and moderate perceived stress over the time.
Infections in pregnancy can have deleterious effects on the maternal health and on the developing fetus, largely dependent on the timing of infection. General and specific benefits of vaccination during pregnancy are the prevention of maternal morbidity and mortality, reduction of risks of intrauterine infection and fetal disease [38]. The key mechanism that protects neonates from severe infective diseases is associated to the passive transfer of antibodies via placenta and human milk [39].
Despite vaccination is one of the most cost-effective ways of avoiding disease, it remains an open challenge. Estimates by WHO report that the immunization might prevent 4-5 million deaths every year in all age groups from diseases like diphtheria, tetanus, pertussis, influenza and measles [40]. Additionally, if global vaccination coverage improves, an additional 1.5 million deaths could be avoided [40]. Vaccine hesitancy refers to the reluctance or refusal to vaccinate despite the availability of vaccines represents one of the ten threats to global health by the WHO [1]. Several reasons why people choose not to vaccinate could be listed, such as complacency, lack of confidence, and inconvenience in accessing vaccines [41]. For that reason, it seems decisive the role of health workers, especially those in communities, as the most trusted advisor and influencer of vaccination decisions in giving reliable information on vaccines [42]. In a previous study, we demonstrated an increase in getting vaccinated among pregnant women by monthly webinars on updated literature, open chat to ask and obtain answers on personal concerns about safety, efficacy and the rapid development and approval of the vaccines, and open days in partnership with one of the main vaccination centers in Milan, Italy [30].
Among pregnant women an increased risk of severe disease, partially due to the pregnancy-induced shift from cell-mediated immunity (Th1 response) to humoral immunity (Th2 response), has been described [43]. The physiological adaptation enables the semi-allogenic fetus to be protected from immunologic rejection, but these adaptive changes render pregnant women more susceptible to severe disease [44,45]. At the same time, pregnancy corresponds to the most delicate experience for women and couples, where the fear to damage the baby is endless, so much to restrain any protective action believed to be harmful regardless.
Influenza infection in pregnancy has been associated with increased maternal morbidity and possible adverse neonatal outcomes. Also, during the first months of life, maternal antibodies offer some protection to the newborn [46]. Thus, inactivated influenza vaccination during pregnancy can be a way to increase protection against influenza in the newborn, as recommended by WHO [36]. Before COVID-19, influenza vaccine was the most widely recommended during pregnancy worldwide, mainly due the protective role played against potentially life-threatening disease in both pregnant people and their infants up to six months of age [47,48]. Despite this, only few countries reported immunization rates in pregnant people above 50% [48].
Similarly, pertussis, an extremely contagious infection of the respiratory system, transmitted by the Gram-negative bacterium Bordetella pertussis, can affect individuals of all ages but has a higher incidence in the pediatric age group and a more significant impact on infants and immunocompromised individuals. In Italy, it has been shown that among pertussis hospitalizations, 64% of cases involved subjects less than 1 year old [49]. The trivalent vaccine (dTap) should ideally be administered around the 28th gestational week or anytime between the 27th and 36th gestational weeks, as indicated in the National Vaccination Plan 2017–2021 by the Ministry of Health [2]. This allows a pregnant woman to produce enough antibodies. However, limited knowledge around vaccines, some unclear recommendations by health professionals, unprecise indications at the legislative level, and difficulty of being immunized during prenatal consultations, has contributed to the poor diffusion of vaccination culture and the failure to achieve an adequate level of vaccination uptake among pregnant women. [50]
There is a growing body of evidence that the SARS- CoV-2 pandemic has increased maternal anxiety and this condition may worsen the decision-making process on all vaccination [6,7], also in those countries most affected by the first COVID-19 wave [30,52,53]. Our findings regarding the increase of the STAI-S scores on the vaccination agrees with this overall trend. These findings might emphasize the impact of the vaccination process on mental health, mainly in women with a negative attitude toward the vaccine and unexposed to educational benefits by professionals in feto-maternal medicine.
Childbirth education classes represent a health promotion and primary prevention tool within the antenatal support educational process. A growing body of evidence emphasize the value of prenatal education classes routinely incorporated into maternity care for several reasons, such as maternal management of pain using a range of coping strategies [54], reducing cesarean section rates for the low-risk population [55] preparing for early parenting skills [56], perineal wound healing in postnatal women who experienced of a tear or episiotomy, or both [57]. In Italy, antenatal education classes have been included in the national project on maternal and child health, called as ‘Progetto Obiettivo Materno Infantile – POMI’ [58], assigning a pivotal role to midwifes in the educational program in addition to their well-established support activities during delivery [59]. Our study adds knowledge on strategies for improving maternal wellbeing during pregnancy by suggesting revised methodological approaches of health literacy inclusive of additional tools. Due to the be part of fragile population, pregnant women remain a priority for the vaccination coverage and health care professionals are called to act against underestimation of vaccine efficacy and lack of trust, possibly with extra efforts, in team and by using current social media for reaching the largest number of women of childbearing age.
The major strengths of the present study include a very well-characterized population of pregnant women who followed a structured intervention. Moreover, the use of different validated questionnaires with clinical applicability to assess mental stress, well-being and sleep quality provided rigor and validity to the results of the study. To note, the use of validated questionnaires may mitigate the potential misclassification of self-reported data, along with the inherent risk of inaccuracies in the measurements.
The study has some limitations. Firstly, most women enrolled were of Caucasian ethnicity, middle to high socio-economical level, without language barrier; hence, the results should not be extrapolated to other populations with different characteristics. Secondly, questionnaire missed involving partners in the antenatal education process as a strategy for improving maternal and neonatal outcomes. Thirdly, the small sample size could de require confirmation in more large study population.
5. Clinical Implications and Future Challenges
Based only on current actions, it is unlikely that alone will offer significant success in overall vaccine up-take in pregnancy. Moving from this, strategies for addressing vaccine hesitancy among pregnant people require reevaluation. To design interventions based on multiple levels of factors influencing vaccine hesitancy may offer more success than individual-level interventions alone. Prenatal education classes represent an effective educational solution to improve women’s awareness of the benefits of vaccination during pregnancy. Our findings encourage the inclusion of an extra lesson to the training program by health care providers in health service centers. They can also be a basis for applying health literacy promotion methods on getting vaccinated when pregnant.
6. Conclusions
The introduction of a lesson regarding on vaccination during pregnancy in the program of prenatal education courses improves psychological well-being and mental health of pregnant women. By a modest effort by health care professionals involved in prenatal education models, a great result in public health can be reached, both in terms of improved quality of life for pregnant women and ameliorate immunization for newborns. As a performance at very low cost, the health literacy on vaccination during pregnancy should be a fixed part of all prenatal education courses for improving from the beginning the feto-maternal health.
Author Contributions
ST conceived the study, oversaw the project, analyses, drafted and edited the manuscript. DP helped conceive the study. SP managed the data. EB, ECDA, MF, AG, JM, IP, MT, MT, SG, DP, AMM procured data.
Funding
None.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Approval n. 2170/2022.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Deidentified data will be shared upon request.
Acknowledgments
All patients involved in the study for the time spent in answering to our questionnaires.
Conflicts of Interest
The authors declare no conflict of interest.
References
- https://www.who.int/news/item/18-08-2015-vaccine-hesitancy-a-growing-challenge-for-immunization-programmes.
- https://www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.
- Scendoni, R.; Fedeli, P.; Cingolani, M. The State of Play on COVID-19 Vaccination in Pregnant and Breastfeeding Women: Recommendations, Legal Protection, Ethical Issues and Controversies in Italy. Healthcare (Basel). 2023, 11, 328. [Google Scholar] [CrossRef] [PubMed]
- De Brabandere, L.; Hendrickx, G.; Poels, K.; Daelemans, W.; Van Damme, P.; Maertens, K. Influence of the COVID-19 pandemic and social media on the behaviour of pregnant and lactating women towards vaccination: a scoping review. BMJ Open. 2023, 13, e066367. [Google Scholar] [CrossRef] [PubMed]
- Gorgui, J.; Atallah, A.; Boucoiran, I.; Gomez, Y.H.; Bérard A; the CONCEPTION Study Group. SARS-CoV-2 vaccine uptake and reasons for hesitancy among Canadian pregnant people: a prospective cohort study. CMAJ Open. 2022, 10, E1034–E1043. [Google Scholar] [CrossRef]
- Sarantaki, A.; Kalogeropoulou, V.E.; Taskou, C.; Nanou, C.; Lykeridou, A. COVID-19 Vaccination and Related Determinants of Hesitancy among Pregnant Women: A Systematic Review and Meta-Analysis. Vaccines (Basel). 2022, 10, 2055. [Google Scholar] [CrossRef] [PubMed]
- Marín-Cos, A.; Marbán-Castro, E.; Nedic, I.; Ferrari, M.; Crespo-Mirasol, E.; Ventura, L.F.; Zamora, B.N.; Fumadó, V.; Menéndez, C.; Martínez Bueno, C.; Llupià, A.; López, M.; Goncé, A.; Bardají, A. “Maternal Vaccination Greatly Depends on Your Trust in the Healthcare System”: A Qualitative Study on the Acceptability of Maternal Vaccines among Pregnant Women and Healthcare Workers in Barcelona, Spain. Vaccines (Basel). 2022, 10, 2015. [Google Scholar] [CrossRef] [PubMed]
- https://www.worldometers.
- Vilca, L.M.; Cesari, E.; Tura, A.M. Barriers and facilitators regarding influenza and pertussis maternal vaccination uptake: a multi-center survey of pregnant women in Italy. Eur J Obstet Gynecol Reprod Biol. 2020, 247, 10–15. [Google Scholar] [CrossRef]
- Maurici, M.; Dugo, V.; Zaratti, L.; et al. Knowledge and attitude of pregnant women toward flu vaccination: a cross-sectional survey. J Matern Fetal Neonatal Med. 2016, 29, 3147–3150. [Google Scholar] [CrossRef]
- Bussink-Voorend, D.; Hautvast, J.L.; Vandeberg, L.; Visser, O.; Hulscher, M.E. A systematic literature review to clarify the concept of vaccine hesitancy. Nat Hum Behav 2022, 1–15. [Google Scholar] [CrossRef]
- Wilson, R.J.; Paterson, P.; Jarrett, C.; Larson, H.J. Understanding factors influencing vaccination acceptance during pregnancy globally: A literature review. Vaccine 2015, 33, 6420–6429. [Google Scholar] [CrossRef]
- Agricola, E.; Gesualdo, F.; Alimenti, L. Knowledge attitude and practice toward pertussis vaccination during pregnancy among pregnant and postpartum Italian women. Hum Vacc Immunother 2016, 12, 1982–1988. [Google Scholar] [CrossRef]
- Myers, K.L. Predictors of maternal vaccination in the United States: An integrative review of the literature. Vaccine 2016, 34, 3942–3949. [Google Scholar] [CrossRef] [PubMed]
- D’Alessandro, A.; Napolitano, F.; D’Ambrosio, A.; Angelillo, I.F. Vaccination knowledge and acceptability among pregnant women in Italy. Hum Vacc Immunother 2018, 14, 1573–1579. [Google Scholar] [CrossRef] [PubMed]
- Poliquin, V.; Greyson, D.; Castillo, E. A systematic review of barriers to vaccination during pregnancy in the Canadian context. JOGC 2019, 41, 1344–1355. [Google Scholar] [CrossRef] [PubMed]
- Scatigna, M.; Appetiti, A.; Pasanisi, M.; D’Eugenio, S.; Fabiani, L.; Giuliani, A.R. Experience and attitudes on vaccinations recommended during pregnancy: survey on an Italian sample of women and consultant gynecologists. Hum Vacc Immunother 2022, 18, 1–8. [Google Scholar] [CrossRef]
- https://www.epicentro.iss.
- DeSisto, C.L.; Wallace, B.; Simeone, R.M. Risk for stillbirth among women with and without COVID-19 at delivery hospitalization — United States, March 2020–September 2021. MMWR Morb Mortal Wkly Rep 2021, 70, 1640–1645. [Google Scholar] [CrossRef]
- Conti, M.G.; Terreri, S.; Terrin, G. SARS-CoV-2 infection versus vaccination in pregnancy: Implications for maternal and infant immunity. Clin Infect Dis Published online 2022.
- Tanne, J.H. Covid-19: Vaccination during pregnancy is safe, finds large US study. Brit Med J 2022, 7, o27. [Google Scholar] [CrossRef]
- De Rose, D.U.; Salvatori, G.; Dotta, A.; Auriti, C. SARS-CoV-2 vaccines during pregnancy and breastfeeding: a systematic review of maternal and neonatal outcomes. Viruses 2022, 14, 539. [Google Scholar] [CrossRef]
- Dick, A.; Rosenbloom, J.I.; Gutman-Ido, E.; Lessans, N.; Cahen-Peretz, A.; Chill, H.H. Safety of SARS-CoV-2 vaccination during pregnancy- obstetric outcomes from a large cohort study. BMC Pregnancy Childbirth 2022, 22, 166. [Google Scholar] [CrossRef]
- Ma, Y.; Deng, J.; Liu, Q.; Du, M.; Liu, M.; Liu, J. Effectiveness and safety of COVID-19 vaccine among pregnant women in real-world studies: a systematic review and meta-analysis. Vaccines 2022, 10, 246. [Google Scholar] [CrossRef]
- https://www.iss. 2022.
- Huddleston, H.G.; Jaswa, E.G.; Lindquist, K.J. COVID-19 vaccination patterns and attitudes among American pregnant individuals. Am J Obstet Gynecol 2022, 4, 100507. [Google Scholar] [CrossRef] [PubMed]
- Stuckelberger, S.; Favre, G.; Ceulemans, M. SARS-CoV-2 vaccine willingness among pregnant and breastfeeding women during the first pandemic wave: a crosssectional study in Switzerland. Viruses 2021, 13, 1199. [Google Scholar] [CrossRef] [PubMed]
- Tao, L.; Wang, R.; Han, N. Acceptance of a COVID-19 vaccine and associated factors among pregnant women in China: a multi-center cross-sectional study based on health belief model. Hum Vacc Immunother 2021, 17, 2378–2388. [Google Scholar] [CrossRef] [PubMed]
- Triunfo, S.; Marconi, A.M. Promoting the Use of Modern Communication Tools to Increase Vaccine Uptake in Pregnancy. JAMA Pediatr. 2023. [Google Scholar] [CrossRef] [PubMed]
- Triunfo, S.; Iannuzzi, V.; Podda, M. Reducing vaccine hesitancy in pregnancy by the health literacy model inclusive of modern communication tools. Arch Obstet Gynecol. 2023. [Google Scholar] [CrossRef]
- Ministero della Sanità. Progetto Obiettivo Materno Infantile D.M. 24 aprile 2000 pag.
- Grandolfo, M.E.; Donati, S.; Giusti, A. Indagine conoscitiva sul percorso nascita. Aspetti metodologici e risultati nazionali. I: Roma, 2002. [Google Scholar]
- ISTAT Gravidanza, parto, allattamento al seno 2004-2005. Roma: Istat, 2006.
- https://www.sigo.it/wpontent/uploads/2021/05/PositionPaper_Gravidanza_Vaccinazione_anti_COVID_05.05.2021.
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press, 1983.
- WHO Wellbeing Measures in Primary Health Care/The Depcare Project. WHO Regional Office for Europe: Copenhagen. 1998.
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. Journal of Health and Social Behavior 1983, 24, 386–396. [Google Scholar] [CrossRef]
- Novillo, B.; Martínez-Varea, A. COVID-19 Vaccines during Pregnancy and Breastfeeding: A Systematic Review. J Pers Med. 2022, 13, 40. [Google Scholar] [CrossRef]
- Pillai, A.; Nayak, A.; Tiwari, D.; Pillai, P.K.; Pandita, A.; Sakharkar, S.; Balasubramanian, H.; Kabra, N. COVID-19 Disease in Under-5 Children: Current Status and Strategies for Prevention including Vaccination. Vaccines (Basel). 2023, 11, 693. [Google Scholar] [CrossRef]
- https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019.
- Demir, R.; Kaya Odabaş, R. A systematic review to determine the anti-vaccination thoughts of pregnant women and the reasons for not getting vaccinated. J Obstet Gynaecol. 2022, 42, 2603–2614. [Google Scholar] [CrossRef]
- Bisset, K.A.; Paterson, P. Strategies for increasing uptake of vaccination in pregnancy in high-income countries: A systematic review. Vaccine. 2018, 36, 2751–2759. [Google Scholar] [CrossRef]
- Bent Formby, Immunologic Response in Pregnancy: Its Role in Endocrine Disorders of Pregnancy and Influence on the Course of Maternal Autoimmune Diseases. Endocrinology and Metabolism Clinics of North America 1995, 24, 87–205.
- Tan, E.K.; Tan, E.L. Alterations in physiology and anatomy during pregnancy. Best Pract Res Clin Obstet Gynaecol 2013, 27, 791e802. [Google Scholar] [CrossRef] [PubMed]
- Mackin, D.W.; Walker, S.P. The historical aspects of vaccination in pregnancy. Best Pract Res Clin Obstet Gynaecol. 2021, 76, 13–22. [Google Scholar] [CrossRef]
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J. Estimates of global seasonal influenza-associated respiratory mortality: a modelling study. Lancet. 2018, 391, 1285–1300. [Google Scholar] [CrossRef] [PubMed]
- Lafond, K.E.; Porter, R.M.; Whaley, M.J.; Suizan, Z.; Ran, Z.; Aleem, M.A.; Thapa, B.; Sar, B.; Proschle, V.S.; Peng, Z. Global burden of influenza-associated lower respiratory tract infections and hospitalizations among adults: a systematic review and meta-analysis. PLoS Med 2021, 18, e1003550. [Google Scholar] [CrossRef]
- Regan, A.K.; Fiddian-Green, A. Protecting pregnant people & infants against influenza: A landscape review of influenza vaccine hesitancy during pregnancy and strategies for vaccine promotion. Hum Vaccin Immunother. 2022, 18, 2156229. [Google Scholar]
- Brosio, F.; Kuhdari, P.; Cocchio, S.; Stefanati, A.; Baldo, V.; Gabutti, G. Impact of pertussis on the Italian population: Analysis of hospital discharge records in the period 2001–2004. Int. J. Infect. Dis. 2020, 91, 143–148. [Google Scholar] [CrossRef]
- Gabutti, G.; Cetin, I.; Conversano, M.; Costantino, C.; Durando, P.; Giuffrida, S. Experts’ Opinion for Improving Pertussis Vaccination Rates in Adolescents and Adults: A Call to Action. Int. J. Environ. Res. Public Health 2022, 19, 4412. [Google Scholar] [CrossRef]
- Skjefte, M.; Ngirbabul, M.; Akeju, O. COVID-19 vaccine acceptance among pregnant women and mothers of young children: results of a survey in 16 countries. Eur J Epidemiol. 2021, 36, 197–211. [Google Scholar] [CrossRef]
- Mappa, I.; Luviso, M.; Distefano, F.A.; Carbone, L.; Maruotti, G.M.; Rizzo, G. Women perception of SARS-CoV-2 vaccination during pregnancy and subsequent maternal anxiety: a prospective observational study. J Matern Fetal Neonatal Med. 2022, 35, 6302–6305. [Google Scholar] [CrossRef]
- Engjom, H.; van den Akker, T.; Aabakke, A.; Ayras, O.; Bloemenkamp, K.; Donati, S.; Cereda, D.; Overtoom, E.; Knight, M. Severe COVID-19 in pregnancy is almost exclusively limited to unvaccinated women - time for policies to change. Lancet Reg Health Eur. 2022, 13, 100313. [Google Scholar] [CrossRef] [PubMed]
- Escott, D.; Slade, P.; Spiby, H. Preparation for pain management during childbirth: the psychological aspects of coping strategy development in antenatal education. Clin Psychol Rev. 2009, 29, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Ronco, S. Literature Review of the Association Between Prenatal Education and Rates of Cesarean Birth Among Women at Low Risk. Nurs Womens Health. 2021, 25, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Lau, R.; Hutchinson, A. A narrative review of parental education in preparing expectant and new fathers for early parental skills. Midwifery. 2020, 84, 102644. [Google Scholar] [CrossRef]
- O’Kelly, S.M.; Moore, Z.E. Antenatal maternal education for improving postnatal perineal healing for women who have birthed in a hospital setting. Cochrane Database Syst Rev. 2017, 12, CD012258. [Google Scholar] [CrossRef]
- Ministero della Sanità. Progetto Obiettivo Materno Infantile D.M. 24 aprile 2000 pag.8.
- Ricchi, A.; La Corte, S.; Molinazzi, M.T.; Messina, M.P.; Banchelli, F.; Neri, I. Study of childbirth education classes and evaluation of their effectiveness. Clin Ter. 2020, 170, e78–e86. [Google Scholar]
Figure 1.
Distribution of maternal anxiety level, assessed by scores of STAI-Trait and STAI-State according to the presence or absence of additional lesson on vaccination during pregnancy.
Figure 1.
Distribution of maternal anxiety level, assessed by scores of STAI-Trait and STAI-State according to the presence or absence of additional lesson on vaccination during pregnancy.
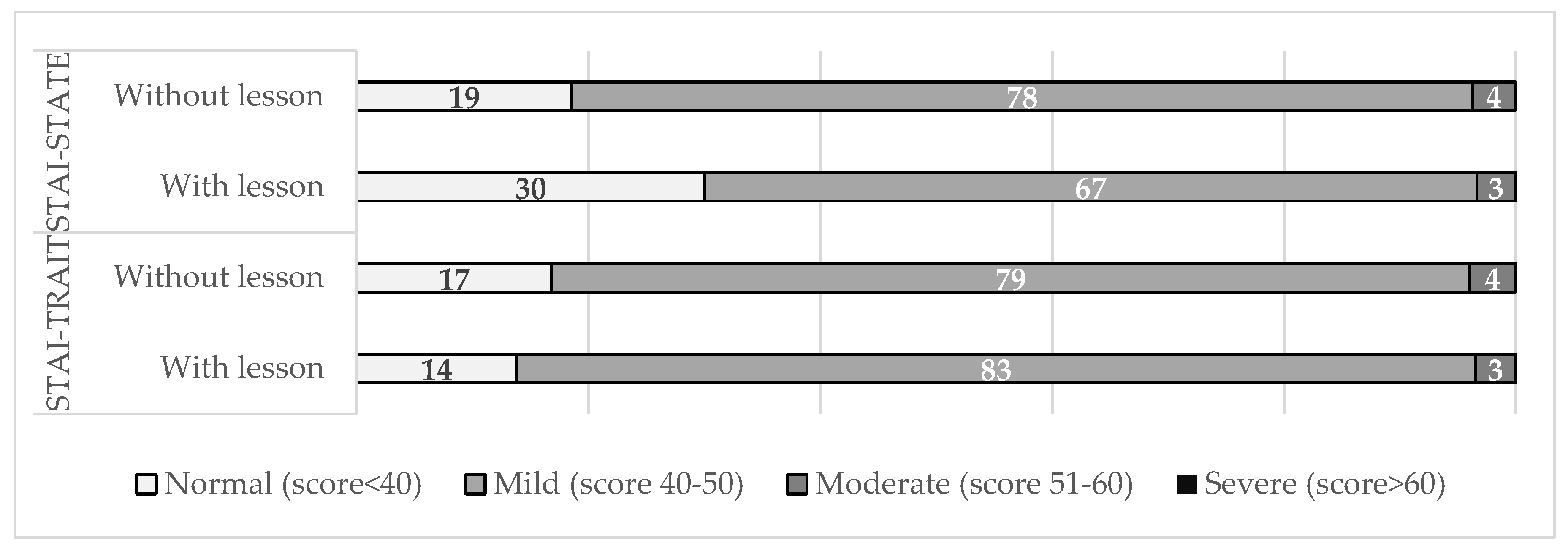
Figure 2.
Distribution of maternal wellbeing level, assessed by scores of WHO-5 WBI according to the presence or absence of additional lesson on vaccination during pregnancy.
Figure 2.
Distribution of maternal wellbeing level, assessed by scores of WHO-5 WBI according to the presence or absence of additional lesson on vaccination during pregnancy.
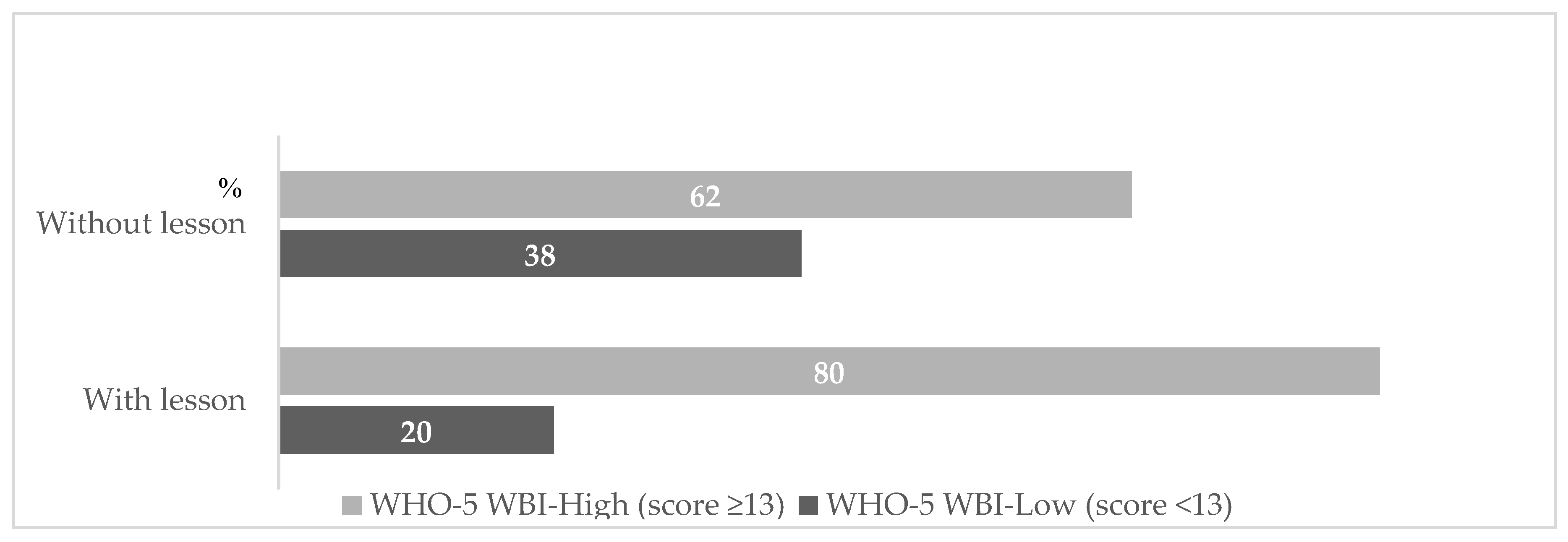
Figure 3.
Distribution of maternal perceived stress levels, assessed by scores of PSS according to the presence or absence of additional lesson on vaccination during pregnancy.
Figure 3.
Distribution of maternal perceived stress levels, assessed by scores of PSS according to the presence or absence of additional lesson on vaccination during pregnancy.
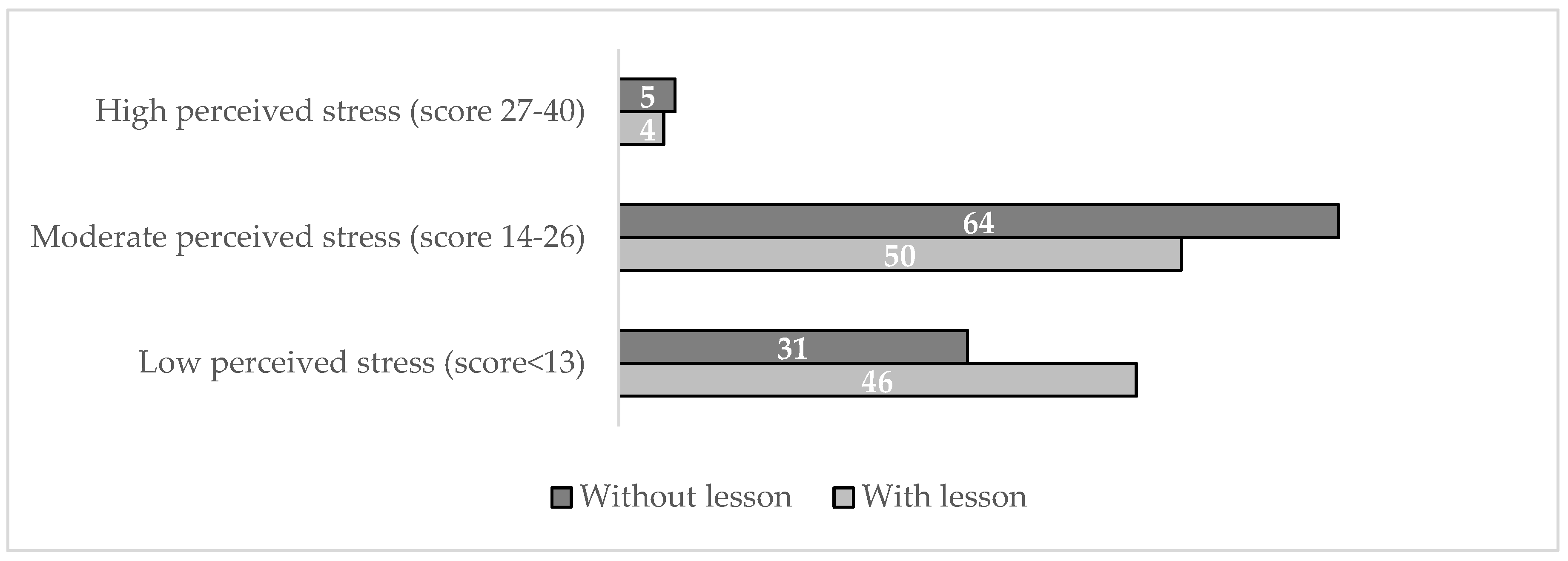

Table 1.
Maternal characteristics of the study population according to the additional lesson to the childbirth education classes on vaccination during pregnancy.
Table 1.
Maternal characteristics of the study population according to the additional lesson to the childbirth education classes on vaccination during pregnancy.
| Variables | Absence of lesson | Presence of lesson | p-value |
|---|---|---|---|
| on vaccines | on vaccines | ||
| (n=33) | (n=112) | ||
| Maternal age (years) | 33.9 (4) | 33.7 (5.1) | 0.207 |
| Ethnicity | |||
| - Caucasian | 32 (97) | 106 (93.8) | 0.007 |
| -Latino-American | 1 (3) | 3 (2.7) | 0.916 |
| -Asian | 0 (0) | 2 (1.8) | 0.443 |
| -African | 0 (0) | 1 (0.9) | 0.294 |
| Education Level | |||
| -Low | 3 (9.1) | 4 (3.6) | 0.221 |
| -Medium | 11 (33.3) | 44 (39.3) | 0.177 |
| -High | 19 (57.6) | 64 (57.1) | 0.095 |
| Working status | |||
| -Employed | 25 (75.8) | 99 (88.4) | 0.267 |
| -Unemployed | 8 (24.2) | 13 (11.6) | 0.64 |
| Smoking status | |||
| -None | 29 (87.9) | 97 (86.6) | 0.956 |
| -Smokers | 4 (12.1) | 15 (13.4) | 0.121 |
| Marital status | |||
| -Married o living with partner | 31 (93.9) | 110 (98.2) | 0.867 |
| -Unmarried | 2 (6.1) | 2 (1.8) | 0.503 |
| Alcohol abuse | 0 (0) | 0 (0) | - |
| Substance abuse | 0 (0) | 0 (0) | - |
Table 2.
Perinatal outcomes of the study population according to the additional lesson to the childbirth education classes on vaccination during pregnancy.
Table 2.
Perinatal outcomes of the study population according to the additional lesson to the childbirth education classes on vaccination during pregnancy.
| Variables | Absence of lesson | Presence of lesson | |
|---|---|---|---|
| on vaccines | on vaccines | p-value | |
| (n=33) | (n=112) | ||
| Medical condition | |||
| -Diabetes | 2 (6.1) | 5 (4.5) | 0.721 |
| - Hypertension | 1 (3) | 3 (2.7) | 0.916 |
| -Thyroid disease | 2 (6.1) | 15 (13.4) | 0.297 |
| -Neurological disease | 2 (6.1) | 4 (3.6) | 0.547 |
| - Autoimmune disease | 1 (3) | 4 (3.6) | 0.916 |
| Parity | |||
| -Primiparous | 22 (66.3) | 87 (77.7) | 0.622 |
| - Multiparous | 11 (33.3) | 25 (22.3) | 0.329 |
| Labor induction | 11 (33.3) | 46 (41.1) | 0.592 |
| Mode of delivery | |||
| -Vaginal delivery | 22 (66.6) | 65 (58) | 0.661 |
| -Instrumental delivery | 2 (6.1) | 13 (11.6) | 0.400 |
| -Elective cesarean section | 2 (6.1) | 14 (12.5) | 0.345 |
| -Emergent cesarean section | 7 (21.2) | 20 (17.9) | 0.721 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



