
Submitted:
07 August 2023
Posted:
22 August 2023
You are already at the latest version
Abstract
In view of the increasing age of cardiac surgery patients, questions arise about the expected postoperative quality of life and the hoped-for prolonged life expectancy. Little is known so far about this weighting by the patients concerned. This study aims to obtain information on the patient’s preferences. Between 2015 and 2017, data from 1349 consecutive patients from seven heart centers in Germany undergoing cardiac surgery were analyzed. Baseline data regarding the patient’s situation as well as a questionnaire regrading quality of life versus lifespan were taken preoperatively. Patients were divided by age into 4 groups: below 60, 60-70, 70-80, and above 80 years. As a result, if one had to decide between quality of life and length of life, about 60% of the male patients decided for quality of life, independent of their age. On the other hand, female patient’s decision for quality of life increased significantly with age, from 51% in the group below sixty to 76% in the group above eighty years. This finding suggests that the female patients adapt their preferences with age whereas male patients do not. This should impact further treatment decisions of elderly patients in cardiac surgery within a shared decision-making process.

Keywords:
patient’s preferences
; quality of life
; lifespan
; gender
Introduction
Cardiovascular diseases (CVDs) are the most common non-communicable diseases globally, taking an estimated 17.9 million lives yearly [1]. Most of these deaths are among people older than 65 years. Forty years ago, heart operations of patients aged 70 and older or in patients bearing a high risk of complications due to increased frailty were avoided due to the increased risk of perioperative complications. Nowadays, most of the patients within a cardiac surgery department are older than 70. Operative procedures target complex morbidities and combinations of ischemic, degenerative, and functional pathologies of the heart. Procedural adoptions have met the increasing risk profile of the patients, and surgeons successfully reduced mortality. However, different therapeutic strategies may focus on better long-term outcome on the one hand or improved short-term recovery on the other hand. While it can be assumed from young patients that the desire for a high quality of life and life extension is pronounced, this balance can shift in old age. With increasing age, postoperative quality of life can be more critical for these patients. However, the knowledge about the patient’s outcome preferences (longer lifespan versus higher quality of life) is sparse in cardiac surgery and data mainly originate from partner disciplines. Regarding the treatment of angina, 83% of the patients would “accept any treatment, no matter how extreme, to return to health” [2]. The severity of symptoms may have a deep impact on the patient ’s expectations regarding the treatment goals and the choice of treatment options. While patients suffering from heart failure decompensation predominantly wish symptomatic alleviation, recompensated patients on the other hand, might additionally focus on the extension of life expectancy [3]. A questionnaire-based study on 662 patients who attended health centers in Spain showed that the willingness to pay for a year of life filled with quality of life was also influenced by higher education and the income of the respondents[4]. Cancer patients are also at risk of high mortality, and more studies exist regarding the quality of life (QoL) and lifespan (LoL). The weighing up of QoL and LoL often touches on much more circumscribed periods of time, maybe perceived as more threatening, and is therefore discussed much more intensively and for longer than in cardiovascular medicine. In a study of 459 patients with advanced cancer, 55% equally valued QoL and LoL with 27% preferring QoL. This preference was stronger with older age and male gender [5]. In another study voting on hypothetical cancer cases, more than 20% of cancer patients voted for a treatment that prolongs survival regardless of QoL, whereas only about 2% of healthy oncology health-care professionals preferred this option. Maximizing QoL at the cost of life time was acceptable for 34% of laypersons, 23% of health-care professionals but only for 15% of the patients. Thus, in cancer patients, survival dominates the therapeutic goals in contrast to healthy individuals [6]. As a result, the severity of symptoms, as well as individual morbidity, age, gender and role as patient or practitioner, weigh therapy goals. Therefore, it is necessary to be aware that the optimal cardiovascular therapeutic concept from the practitioner's perspective does not necessarily correspond to the wishes and values of the (elderly) patients. Moreover, studies on a possible decision between QoL and LoL are missing in cardiac surgery, even though there is a general believing of heart surgeons that QoL gets more important for elderly patients.
Methods
Study Participants: Our goal was to enroll more than 1000 patients within seven departments for cardiac surgery in Germany, e.g., the Clinic for Cardiac Surgery of the University Hospital Halle (Saale), the Clinic for Cardiac and Vascular Surgery of the University Hospital Gießen, the Clinic for Cardiac Surgery of the Hospital of the Brothers of Charity in Trier, the Clinic for Cardiac and Thoracic Surgery of the University Hospital Lübeck, the Clinic for Cardiac Surgery of the University Hospital Erlangen, the Clinic for Cardiac Surgery of the University Hospital Dresden and the Clinic for Cardiac Surgery of the Heart Center Brandenburg in Bernau. The study protocol was approved by the local ethical boards of all seven hospitals. All participants provided a written informed consent. Inclusion criteria were elective cardiac surgery and age above 18. Exclusion criteria were emergency operations and dementia of the patients. 1349 patients were enrolled. The study was registered at the German Clinical Trials Register (DRKS00025218). Patient’s characteristics are shown in Table 1.
Statistical analysis
The sample size was based on feasibility and not by a confirmatory sample size calculation. To analyze the influence of age and gender on the preference of the patients with respect to long life vs. quality of life, logistic regression was used. Results are presented as odds ratios (OR) with 95% confidence intervals (95% CI) and p-values.
Results
To analyze the preference of patients regarding their personal aim of the heart operation, the study participants had to answer before the operation the following question: Regarding the possible outcome of the operation, if you have to choose one option, for which of the two options would you decide: a longer lifespan with reduced quality of life or a shorter lifespan with optimal quality of life? For analysis, patients were divided into 4 age groups: below 60, 60-70, 70-80, and above 80. To analyze the influence of age and gender on the preference of patients with respect to long life vs. quality of life, logistic regression was used. Because of the different results for males and females, respectively, data were analyzed together and stratified by gender. Results are presented as odds ratios in favor for QoL (OR) with 95% confidence intervals (95% CI) and p-values. In the total group (N=1349), we see a non-significant increase of the QoL option with age. After dividing the participants into both genders, it is clear that male patients do not change their decision with age. On the other side, females do adapt their answers to their age (Table 2). With increasing age, they chose significantly more and more Quality of Life as an operation preference.
Figure 1 show the percentage of patients within the four age groups choosing the QoL option. It is clearly seen that female patients change their minds whereas male patients do not adapt.
Discussion
The assumption of a healthy and fit person with regard to the needs of a sick or even a frail patient is highly subjective and probably only partially agrees with the treatment goals and risk avoidance. Ahman and Kendell therefore asked rhetorically “Clearly, surviving cardiac surgery is very important – but is survival the top priority for the 92-year old after bypass surgery who becomes unable to live independently again and whose quality of life is insufferable? Should quality of life be the main factor driving therapeutic decisions for the frail and elderly?” [7]. This predicts that during aging, the priority of the patients regarding the outcome of a heart operation may change. One of the greatest deficits in the therapy of elderly or decrepit cardiac surgical patients remains that there has not yet been any targeted, prospective independent data collection with regard to the therapy requirements in this patient group. In most cases, asking the simple question: “is life span important for you?”, patients will agree. The same is true if you ask the question using quality of life. Only if the patients have to decide between these both outcome options, one may see changes. Our data clearly show gender-specific differences regarding the decision between these two options. concerning major outcome wishes as quality of life versus length of life.
What can be the cause of this difference? In neuroscience, neurobiological differences between men and women (dimorphisms) are perceived in many neurological and psychiatric conditions, making sex an important factor [8].
To analyze “simulated“ real life decision making, the Iowa Gambling Task (IGT) can be used. Whereas women and men do not differ on choices for safe or risky options per se, it was reported that women may choose the safe option more often after a previous loss than men [9].
Genetic components can also be an interesting factor as for example the Val158Met polymorphism of the COMT gene. This gene encodes catechol-O-methyl-transferase, an enzyme that breaks down dopamine. Using the IGT performance in a healthy adult sample, Costa et al. could show that COMT can be a genetic marker underlying sex differences in decision-making [10].
Another explanation can be the differing real life situation of elderly men and women. Whereas in Germany in 2006, about 60% of 80 year old men are married, more than 50% of women are widows at the age of 70 [11]. As women live longer, older women in Europe were more than twice as likely to live alone compared to their male counterparts (United Nations, Department of Economic and Social Affairs, Population Division (2017). World Population Ageing 2017 - Highlights (ST/ESA/SER.A/397)). Due to this reason, quality of life maybe more important for women than for senior men. Our data suggest that maintaining their independence is more central for senior women than longevity.
To our knowledge, this is the first study demonstrating that female patients adapt their outcome preferences with age whereas male patients do not. Personal preferences of our senior patients should be addressed with an individualized treatment option plan within a shared decision making (SDM) process. In a review on shared decision making in the heart team, it was noted: “Despite recommendations in professional guidelines, SDM is not yet common practice in the Heart Team decision-making process in the treatment of patients” [12].
Some limitations of the study should be noted. Our study population was a population with a low to medium risk profile. This could have an impact on personal outcome preferences.
We believe that our data reflect senior cardiac surgery patient outcome preferences and open the field for more studies as well as for more individualized treatments.
References
- Group, W.C.R.C.W. World Health Organization cardiovascular disease risk charts: revised modAAels to estimate risk in 21 global regions. Lancet Glob Health 2019, 7, e1332–e1345. [Google Scholar] [CrossRef]
- Bowling, A.; Culliford, L.; Smith, D.; Rowe, G.; Reeves, B.C. What do patients really want? Patients' preferences for treatment for angina. Health Expect 2008, 11, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, L.W.; Hellkamp, A.S.; Leier, C.V.; Sopko, G.; Koelling, T.; Warnica, J.W.; Abraham, W.T.; Kasper, E.K.; Rogers, J.G.; Califf, R.M.; et al. Changing preferences for survival after hospitalization with advanced heart failure. J Am Coll Cardiol 2008, 52, 1702–1708. [Google Scholar] [CrossRef] [PubMed]
- Martin-Fernandez, J.; Polentinos-Castro, E.; del Cura-Gonzalez, M.I.; Ariza-Cardiel, G.; Abraira, V.; Gil-LaCruz, A.I.; Garcia-Perez, S. Willingness to pay for a quality-adjusted life year: an evaluation of attitudes towards risk and preferences. BMC Health Serv Res 2014, 14, 287. [Google Scholar] [CrossRef] [PubMed]
- Meropol, N.J.; Egleston, B.L.; Buzaglo, J.S.; Benson, A.B., 3rd; Cegala, D.J.; Diefenbach, M.A.; Fleisher, L.; Miller, S.M.; Sulmasy, D.P.; Weinfurt, K.P.; et al. Cancer patient preferences for quality and length of life. Cancer 2008, 113, 3459–3466. [Google Scholar] [CrossRef] [PubMed]
- Marta, G.N.; Del Nero, L.G.; Marta, G.N.; Mangabeira, A.; Critchi, G.; Kovacs, M.J.; Silva, J.L.; Saad, E.D. Treatment priorities in oncology: do we want to live longer or better? Clinics (Sao Paulo) 2014, 69, 509–514. [Google Scholar] [CrossRef]
- Rahman, I.A.; Kendall, S. Cardiac surgery in the very elderly: it isn’t all about survival. The British Journal of Cardiology 2020, 27, 3. [Google Scholar] [CrossRef]
- Ruigrok, A.N.; Salimi-Khorshidi, G.; Lai, M.C.; Baron-Cohen, S.; Lombardo, M.V.; Tait, R.J.; Suckling, J. A meta-analysis of sex differences in human brain structure. Neurosci Biobehav Rev 2014, 39, 34–50. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.M.; Chan, C.C.; Leung, A.W.; Fox, P.T.; Gao, J.H. Sex-related differences in neural activity during risk taking: an fMRI study. Cereb Cortex 2009, 19, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- Costa, D.S.; Bechara, A.; de Paula, J.J.; Romano-Silva, M.A.; Correa, H.; Lage, G.M.; Miranda, D.M.; Malloy-Diniz, L.F. Influence of COMT Val(158)Met polymorphism on emotional decision-making: A sex-dependent relationship? Psychiatry Res 2016, 246, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, E.; Menning, S.; Schelhase, T. Demografische Perspektiven zum Altern und zum Alter. Gesundheitsberichterstattung des Bundes 2009, Gesundheit und Krankheit im Alter, 21-30.
- Lindeboom, J.J.; Coylewright, M.; Etnel, J.R.G.; Nieboer, A.P.; Hartman, J.M.; Takkenberg, J.J.M. Shared Decision Making in the Heart Team: Current Team Attitudes and Review. Struct Heart 2021, 5, 163–167. [Google Scholar] [CrossRef]
Figure 1.
Gender and age dependent preferences of cardiac surgery patients.
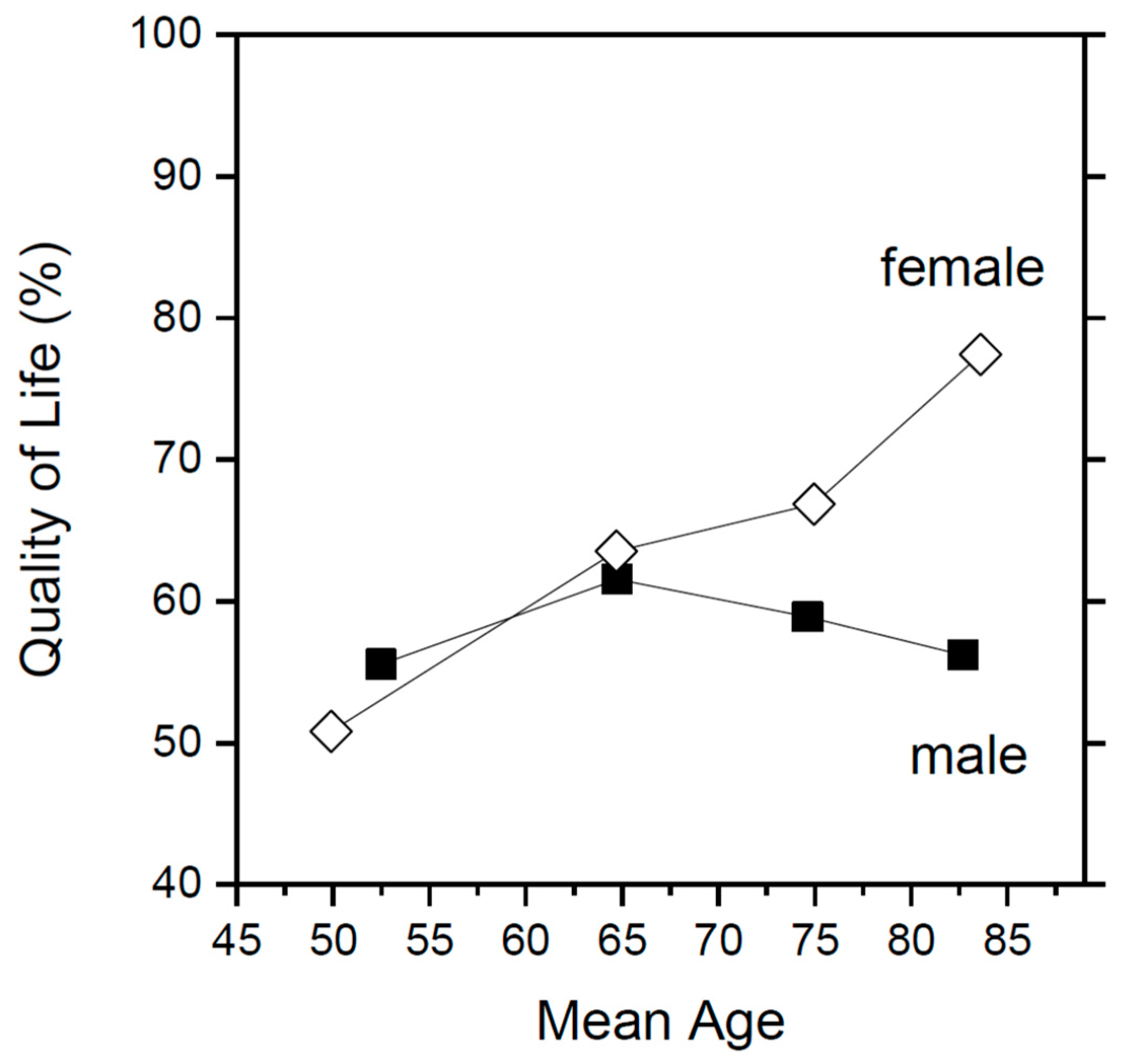

Table 1.
Patients characteristics.
| Patients (N) | 1349 |
|---|---|
| Age (years) | 68.49 ± 10.74 |
| Female (%) | 29.28 |
| BMI | 28.62 ± 5.24 |
| EuroScore II (%) | 3.71 ± 5.19 |
| STS Score (%) | 2.16 ± 2.87 |
| NYHA Score | 2.65 ± 0.79 |
| Angina Pectoris – CCSS | 2.00 ± 1.02 |
| Diabetes (%) | 35.80 |
| Hypertension (%) | 89.02 |
| Current smoker (%) | 17.36 |
| Lipid disorder (%) | 64.76 |
Table 2.
Patients preferences with respect to long life vs. quality of life by gender and age groups.
Table 2.
Patients preferences with respect to long life vs. quality of life by gender and age groups.
| Males (n=954) | Females (n=395) | Total (n=1349) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-value | OR | 95% CI | p-value | OR | 95% CI | p-value | |
| Age below 60 | 1.00 | 1.00 | 1.000 | ||||||
| Age 60-69 | 1.27 | 0.88 - 1.83 | 0.21 | 1.69 | 0.88 - 3.24 | 0.12 | 1.358 | 0.99 - 1.87 | 0.06 |
| Age 70-79 | 1.14 | 0.80 - 1.62 | 0.46 | 1.97 | 1.09 - 3.56 | 0.03 | 1.335 | 0.99 - 1.80 | 0.06 |
| Age above 80 | 1.02 | 0.63 - 1.64 | 0.95 | 3.32 | 1.52 - 7.23 | 0.003 | 1.482 | 0.99 - 2.21 | 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



