
Submitted:
22 August 2023
Posted:
23 August 2023
You are already at the latest version
Abstract
Disseminated or military tuberculosis (TB) is defined as the presence of at least two non-contiguous sites of Mycobacterium tuberculosis, occurring as a result of progressive primary infection, reactivation and spread of a latent focus or due to iatrogenic origin. Disseminated TB represents a life-threatening condition, especially in at-risk children and when the diagnosis and treatment are delayed. We report on a case of a 3-year old boy who presented with long-lasting unrecognised disseminated TB that was successfully managed in a low-resource setting.
Keywords:
tuberculosis
; disseminated TB
; low-income setting
1. Introduction
Tuberculosis (TB) is among the top ten causes of death worldwide. TB represents a marker of inequality as the overwhelming burden of TB is found among low- and middle-income countries, where it is estimated that over 90% of global TB cases and deaths occur [1]. Disseminated or military tuberculosis is defined as the presence of at least two non-contiguous sites resulting from lymphohematogenous dissemination of Mycobacterium tuberculosis, occurring as a result of progressive primary infection, reactivation and spread of a latent focus or due to iatrogenic origin [2]. Disseminated TB represents a life-threatening condition, especially in at-risk children and when the diagnosis and treatment are delayed [3,4]. Clinical presentation of disseminated TB is nonspecific, it is commonly associated with fever of unknown origin and, depending on involved sites, with other generic symptoms attributable to other common diseases [5]. In addition, in particular in low-income settings, the paucity of tools available for confirmatory laboratory diagnosis, such as low sensitivity of acid-fast bacilli (AFB) smear, time-consuming cultures, and the inability to easily detect miliary changes in chest X-ray, makes the diagnosis a very challenging task [5]. The time from symptoms presentation to the diagnosis is highly variable ranging from few days to several months depending on health professionals training, diagnostic tools and clinical presentation that usually includes subacute or chronic constitutional symptoms such as fever, weight loss, and night sweats. Commonly, most children are treated on the basis of a combination of clinical and radiologic signs suggestive of TB without bacteriological confirmation [6]. To date, mortality due to disseminated TB is still high, ranging from 25% to 30% mainly due to the delay in diagnosing and the onset of meningismus, liver cirrhosis, leukopenia, leukocytosis, advancing age, presence of underlying disease, altered mental status, and night sweats [7]. In the present paper a case on a 3-year old boy who presented with long-lasting unrecognised disseminated TB that was successfully managed in a low-resource setting, is reported.
2. Case report
A 3-year-old boy was transferred, on June 2023, from a rural health centre to a regional hospital in Mozambique due to suspected acute flaccid paralysis and paraparesis. Eight months before, October 2022, he developed intermittent fever, which improved with paracetamol administration. In December 2022 the clinical status evolved with the appearance of a swelling in the right wrist, treated with an incision and drainage and prescription of paracetamol and antibiotic in a rural health centre. After a week, another swelling appeared in the region of the spine and an oedema in the right ankle, accompanied by intense and progressive pain and paracetamol was prescribed in the same health centre. In April 2023, the condition worsened with increased swelling in the spine region, worsening pain, difficulty in sitting and walking. He also mentioned occasional dry cough, night sweats, asthenia and weight loss, denying chest pain and dyspnea. Due to the worsening conditions,the health centre decided to transfer the boy to a regional hospital, but due to lack of means, the mother was recommended to wait at home with the boy for the availability of transport. After two more months and the further worsening of the condition he was transferred to the regional hospital on suspicion of acute flaccid paralysis and paraparesis. He presented with a deformity of the lumbar spine (Figure 1a), solution of skin continuity on the anterior surface of the distal 1/3 of the right forearm, measuring approximately 2.5x1.5cm (Figure 1b) and a cold soft oedema in the region of the right ankle (Figure 1c). He also presented a pathological gait (Alderman), with tendency to support the left arm over the waist. The initial diagnosis was Pott's Disease and he started the specific following treatment on daily regimen of 2 HRZE+10 HRE anti-tubercular therapy in which four drugs isoniazid (H), rifampicin (R), ethambutol (E) and pyrazinamide (Z) for 2 months followed by three drugs (HRE) for 10 months. The curettage was performed on the wound that was subsequently cleaned and medicated daily. Five days after starting treatment, he developed an episode of generalised tonic-clonic seizures lasting two minutes without sphincter relaxation, associated with fever. The biochemical test performed at admission, after 2 and 5 days are reported in Table 1.
In addition to those tests at admission HIV and GeneXpert MTB/RIF resulted negative. After 5 days also albumin, total proteins, bilirubin, iron and cholesterol were performed and resulted in normal ranges. Plain X-ray of the spine showed loss of anterior and posterior alignment of L2 and L3, change in height of the L2 vertebral body and altered bone density of the L2 and L3 vertebral bodies (Figure 2). The chest X-ray showed heterogeneous infiltrate in both lung fields (Figure 3a) while the X-ray of the right forearm showed an osteolytic lesion in the distal 1/3 of the radius (Figure 3b) and the X-ray of the right leg showed signs of calcaneal osteolysis (Figure 3c). Based on clinical history, examination and X-ray results, the diagnosis of disseminated TB, including Pott's Disease pulmonary and cutaneous TB was made. The conditions improved slowly but consistently, with gait improvement healing of the forearm injury and reduction of ankle oedema. The boy was discharged after 23 days with one-year prescribed treatment and follow-up in 12 months if no complication will occur.
3. Discussion
This case contains the main characteristics of the health systems in low-income countries including lack of trained health workers, lack of means in heath centres in the community system, and lack of effective health policies in combating endemic diseases such as TB. Mozambique has one of the highest TB burden in the world, with an estimated TB incidence rate of 551/100.000 population in 2015. Moreover, TB treatment covers only 38% of the population, and an increasing rate of TB–HIV co-infection is usually documented (49% of TB patients were HIV-positive) [8]. Despite these dramatic data, TB and especially disseminated TB remains still underrecognized and undiagnosed as the results of lack of well trained health workers and adequate tools for assessment and correct follow-up. In particular, in the present case, eight months passed from the first visit to the correct diagnosis. The reasons for such a delay are multiple. First of all, the child had no specific TB symptoms and health workers were not able to identify the disease, then the rural health centre was not properly equipped for deeper investigation. Finally, two additional months were necessary to wait the possibility to transfer the child. As precise and timely diagnosis is crucial in order to have favourable prognosis, it is mandatory on one hand to strengthen existing structures and, on the other to find alternative solutions. In this regard, recent evidence suggest the possible role of Stool Xpert MTB/RIF on stool samples especially in sub-Saharan setting although diagnostic accuracy and cost-effectiveness are still under investigation [9]. Despite possible future solutions, it is mandatory to support and collaborate in defeating TB, not only for low-income countries but also in terms of global and globalised health. Importantly, the recent Covid-19 pandemic highlighted the weakness of world health systems and high-income countries are increasingly exposed to TB due to immigrants from regions with a high rate of TB and a high prevalence of multidrug-resistant or extensively drug-resistant TB [10]. Another important aspect is the mutual link between TB and some non-communicable diseases that represent an increasing burden worldwide. This association creates a vicious circle, with TB increasing non-communicable disease complications and vice versa, it also makes diagnosis and management more difficult and worsens disease course and outcomes [11].
4. Conclusions
These evidences, although rising just from a case report, allows one to stipulate some considerations. Firs of all it is mandatory and urgent to strength the creation and implementation of tailored health policies for all countries affected by TB including screening protocols for migrants in an integrated, culturally-sensitive, social determinant- driven manner. It is also crucial to enable health workers and health facilities to achieve correct and timely diagnosis. Finally, as a pharmacological approach is necessary in the treatment in TB and costs of treatment per patient are significantly high, particular attention should be paid to social determinants of TB that influenceits contraction, as well as outcome, in low-resource settings.
Informed Consent Statement
Written informed consent was obtained from the parents of the child for publication of this case report and any accompanying images.
Conflicts of Interest
all authors declare no conflict of interest
References
- Di Gennaro, F.; Pizzol, D.; Cebola, B.; Stubbs, B.; Monno, L.; Saracino, A.; Luchini, C.; Solmi, M.; Segafredo, G.; Putoto, G.; et al. Social determinants of therapy failure and multi drug resistance among people with tuberculosis: A review. Tuberculosis 2017, 103, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Swaminathan, S.; Rekha, B. Pediatric Tuberculosis: Global Overview and Challenges. Clin. Infect. Dis. 2010, 50, S184–S194. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.Y.; Dosa, K.; Fuad, A.; Ibrahim, W.; Alaini, A.; Osman, L.; Albadri, M.; Yassin, M.A.D. Disseminated Tuberculosis among Adult Patients Admitted to Hamad General Hospital, Qatar: A Five Year Hospital Based Study. Mycobact. Dis. 2016, 6. [Google Scholar] [CrossRef]
- Marotta, C.; Gennaro, F.; Pizzol, D.; Madeira, G.; Monno, L.; Saracino, A.; Putoto, G.; Casuccio, A.; Mazzucco, W. The At Risk Child Clinic (ARCC): 3 Years of Health Activities in Support of the Most Vulnerable Children in Beira, Mozambique. Int. J. Environ. Res. Public Heal. 2018, 15, 1350. [Google Scholar] [CrossRef] [PubMed]
- Didel, S.; Purohit, A.; Vyas, V.; Kumar, P. Disseminated tuberculosis in children—a difficult diagnose depends on how far we can go. BMJ Case Rep. 2020, 13, e237192. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, M.; Nordholm, A.-C.; Ssekyanzi, B.; Byamukama, O.; Orikiriza, P.; Tusabe, T.; Nyehangane, D.; Taremwa, I.M.; Turyashemererwa, E.; Wobudeya, E.; et al. Mortality and Cause of Death in Children With Presumptive Disseminated Tuberculosis. Pediatrics 2023, 151. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.K.; Mohan, A.; Sharma, A. Miliary tuberculosis: A new look at an old foe. J. Clin. Tuberc. Other Mycobact. Dis. 2016, 3, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Pizzol, D.; Veronese, N.; Marotta, C.; Di Gennaro, F.; Moiane, J.; Chhaganlal, K.; Monno, L.; Putoto, G.; Mazzucco, W.; Saracino, A. Predictors of therapy failure in newly diagnosed pulmonary tuberculosis cases in Beira, Mozambique. BMC Res. Notes 2018, 11, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Segala, F.V.; Papagni, R.; Cotugno, S.; De Vita, E.; Susini, M.C.; Filippi, V.; Tulone, O.; Facci, E.; Lattanzio, R.; Marotta, C.; et al. Stool Xpert MTB/RIF as a possible diagnostic alternative to sputum in Africa: a systematic review and meta-analysis. Front. Public Heal. 2023, 11, 1117709. [Google Scholar] [CrossRef] [PubMed]
- Di Gennaro F, Cotugno S, Fasano M, Ricciardi A, Ronga L, Lattanzio R, Grimaldi A, Bavaro DF, Ciarallo M, Garzone S, De Iaco G, Guido G, Fiore JR, Brindicci G, Santoro CR, Sica S, Iacovazzi TL, Santantonio TA, Saracino A. High risk of unsuccessful treatment outcome in migrant population with tuberculosis: Data from three Italian hospitals. Front Public Health. 2023 Jan 10;10:1024474.
- Di Gennaro F, Marotta C, Antunes M, Pizzol D. Diabetes in active tuberculosis in low-income countries: to test or to take care? Lancet Glob Health. 2019 Jun;7(6):e707.
Figure 1.
Disseminated tuberculosis at presentation in a 3-years old boy: deformity of the lumbar spine (1a), solution of skin continuity on the distal right forearm (1b) and cold soft oedema in the right ankle (1c).
Figure 1.
Disseminated tuberculosis at presentation in a 3-years old boy: deformity of the lumbar spine (1a), solution of skin continuity on the distal right forearm (1b) and cold soft oedema in the right ankle (1c).

Figure 2.
Plain X-ray of the spine.
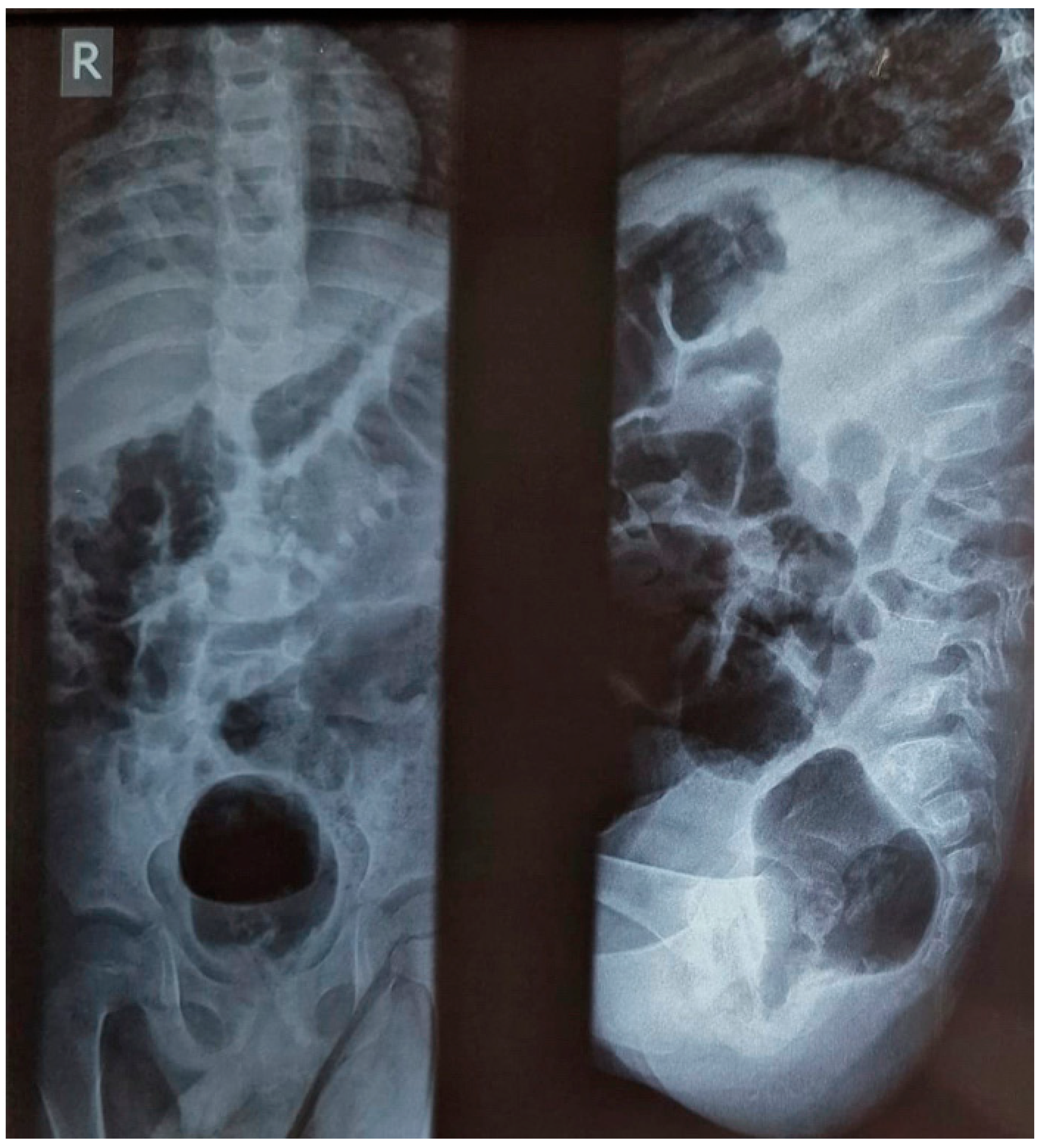
Figure 3.
The chest x-ray (3a), X-ray of the right forearm (3b) and the X-ray of the right leg (3c).
Figure 3.
The chest x-ray (3a), X-ray of the right forearm (3b) and the X-ray of the right leg (3c).
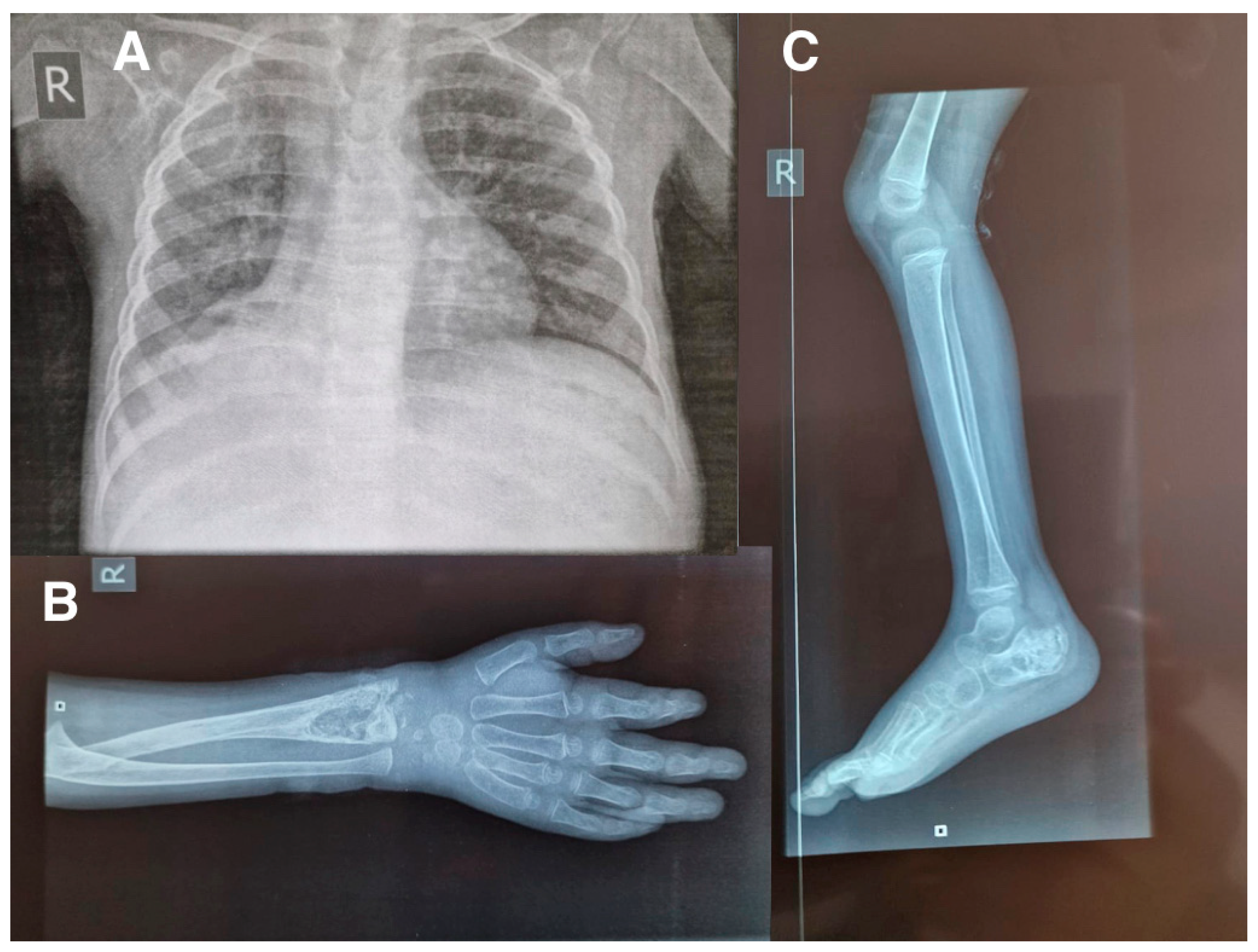

Table 1.
Biochemical results performed at admission, after 2 and 5 days.
| Parameter | Admission | 2 days after | 5 days after |
|---|---|---|---|
| WBC | 13.3x103/uL | 15.04x103/uL | 14.17x103/uL |
| LYM | 5.8 (43.7%) | 5.5 (37%) | 6.36 (44.9%) |
| NEUT | 6.5 (48.7%) | 7.9 (52.5%) | 5.88 (41.4%) |
| RBC | 4.77x106/uL | 4.62x106/uL | 4.72x106/uL |
| HGB | 7.5g/dl | 7.4g/dl | 7.7g/dl |
| MCV | 57.9 fL | 54.1fL | 54.2fL |
| MCH | 15.7 pg | 16.0pg | 16.3pg |
| MCHC | 27.2g/dl | 29.6g/dl | 30.1g/dl |
| PLT | 1000x103/uL | 944x103/uL | 1030x103/uL |
| Na | 133 mEq/L | NR | 132.9 mEq/L |
| K | 4.37 mEq/L | NR | 5.44 mEq/L |
| Cl | 98 mEq/L | NR | 98 mEq/L |
| Creatinine | 20.3 umol/L | NR | 22.33 umol/L |
| ALT | 16.54 U/L | NR | 26 U/L |
| AST | 31.33 U/L | NR | 43 U/L |
| Urea | 3.01 mg/dL | NR | 2.47 mg/dL |
| Glucose | 4.86 mmol/L | NR | 3.5 mmol/L |
| ESR | 51mm/h | NR | NR |
ALT: Alanine aminotransferase; AST: Aspartate aminotransferase; Cl: chlorine; ESR: erythrocyte sedimentation rate; HGB: haemoglobin; K: potassium; LYM: lymphocytes; MCV: mean corpuscular volume; MCH: mean corpuscular haemoglobin; MCHC: mean cell haemoglobin concentration; Na: sodium; NEUT: neutrophils; PLT: platelets; RBC: red blood cells; WBC: white blood cells.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



