
Submitted:
22 August 2023
Posted:
23 August 2023
You are already at the latest version
Abstract
The persistent burden of chronic hepatitis B among ≤5-year-old children in Africa suggests missed opportunities for controlling mother-to-child transmission (MTCT) of the hepatitis B virus (HBV). This scoping review maps the evidence base on the risk of HBV MTCT, the status of HBV MTCT mitigation strategies including hepatitis B birth-dose vaccination, and the role of systems complexity on the suboptimal adoption and performance of hepatitis B birth-dose vaccination programs in Africa. Overall, 88 peer-reviewed and grey literature sources published between 2000–2022 were included in this review. The evidence base consistently argues for a growing risk of HBV MTCT amidst the HIV co-epidemic in the region. Without universal HBV screening programs integrated within broader antenatal care services, current selective hepatitis B birth-dose vaccination is unlikely to effectively interrupt HBV MTCT. We underscore critical health systems-related barriers to universal adoption and optimal performance of hepatitis B birth-dose vaccination programs in the region. To better conceptualize the role of complexity and system-wide effects on the observed performance of the program, we propose an adapted systems-based logic model. Ultimately, exploring contextualized complex systems approaches to scaling-up universal hepatitis B birth-dose vaccination programs should form an integral part of the regional research agenda.
Keywords:
Africa
; birth-dose
; hepatitis B
; health systems
; maternal and child health
; vaccine
1. Introduction
Chronic hepatitis B caused by persistent infection with the hepatitis B virus (HBV) is a major public health threat in endemic regions like the World Health Organization (WHO) Africa region [1]. Chronic infection with HBV poses a 15–25% lifetime risk of acquiring liver cirrhosis or hepatocellular carcinoma [1,2]. Thus, the fact that ~90% of babies born to mothers testing positive for the hepatitis B surface (HBsAg) or e (HBeAg) antigens will develop a chronic infection raises significant global public health concern [1]. Debates on the leading route of transmission driving the epidemic in Africa have previously favored horizontal transmission in early childhood [3,4]. However, a growing body of evidence now suggests an epidemiological shift towards HBV mother-to-child-transmission (MTCT) or vertical transmission. Increased risk of HBV MTCT has been detected among pregnant women in several WHO Africa member states [2,5,6,7,8,9,10,11,12,13,14,15]. This shift in the epidemiology of the disease cannot be addressed outside of the disproportionate HIV epidemic faced by the WHO Africa region (66% [25 million] of the global total of people living with HIV reside in Africa) [16,17,18]. Co-infection with HBV and HIV is common and associated with higher likelihood of HBV MTCT compared to HBV mono-infection [19,20].
While the WHO Western Pacific region has more chronic HBV carriers (115 million or 5.9% [95% Uncertainty Interval (UI) 4.9–7.3] vs 82 million or 7.5% [95% UI 5.7–10.5] of the population in the WHO Africa region), the highest proportion of children younger than 5 years of age living with HBV are in Africa, estimated at 2.5% which surpasses the global prevalence of 0.9% [95% UI 0.7–1.6] [16,17]. This suggests that the WHO Africa region is on course to having one of the largest populations of chronic HBV carriers compared to any other region without urgent and intensive public health intervention. Fortunately, chronic hepatitis B is entirely vaccine preventable [1]. Universal hepatitis B infant vaccination has been adopted in all 47 WHO Africa member states since the early 1990s, maintaining relatively good coverage rates (72% in 2022) [21]. Despite this, the continued burden of chronic hepatitis B among children younger than 5 years of age suggests missed opportunities for controlling HBV MTCT in the WHO Africa region.
Universal hepatitis B birth-dose vaccination is recommended for the prevention of HBV MTCT and has been endorsed by the WHO for all member states since 2009 [1,22,23,24]. It forms an integral part of the World Health Assembly’s Global Health Sector Strategy (GHSS) on viral hepatitis, 2016–2021, which aims to eliminate viral hepatitis as a global public health threat by 2030 [25]. Globally, 111 of 194 WHO member states have adopted universal hepatitis B birth-dose vaccination programs [26,27] with coverage rates reaching 45% in 2022 [21]. Despite the commitment of the WHO Africa regional office to the GHSS goal [28], the adoption of universal hepatitis B birth-dose vaccination programs has been slow with only 15 of 47 member states adopting it to date [29,30]. Furthermore, dismal coverage of the hepatitis B birth-dose vaccine in the WHO Africa region (18% in 2022) suggests significant programmatic challenges [21].
Identifying barriers to the adoption and optimal performance of hepatitis B birth-dose vaccination programs alone, though helpful, is unlikely to inform the development of sustainable solutions. To achieve whole-of-systems gains, it has been suggested that critical attention should be given to the broader health systems delivering health interventions [31,32]. Because health systems can adapt to changes in the local environment and are composed of other complex systems (i.e., people at the center of the health system), they are recognized as complex systems [33,34]. Acknowledging the influence of health systems complexity may assist in strengthening the capacity to support interventions like hepatitis B birth-dose vaccination. Interventions themselves can also introduce some degree of complexity when characterized by multiple interacting components, limited degree of flexibility of implementation, non-linear causal pathways, and feedback loops [35,36,37,38]. Some argue therefore, that key consideration should be given to the complex interaction between interventions and the health systems they are embedded in [33,39]. We posit that research enquiries, including evidence syntheses, adopting complex systems perspectives could uncover richer explanations for the suboptimal performance of hepatitis B birth-dose vaccination programs in the WHO Africa region [36,38].
2. Materials and Methods
2.1. Objectives of the review
The overarching purpose of this scoping review was to better understand the breadth and depth of evidence on the status of hepatitis B birth-dose vaccination programs in the WHO Africa region and explore the potential for further research enquiry into the role of systems complexity. For this purpose, we address the following objectives:
- To describe current knowledge on the risk of HBV MTCT in the WHO Africa region.
- To describe the status of HBV MTCT mitigation strategies including hepatitis B birth-dose vaccination programs.
- To explore health systems capacity to support hepatitis B birth-dose vaccination programs in the WHO Africa region.
2.2. Methods
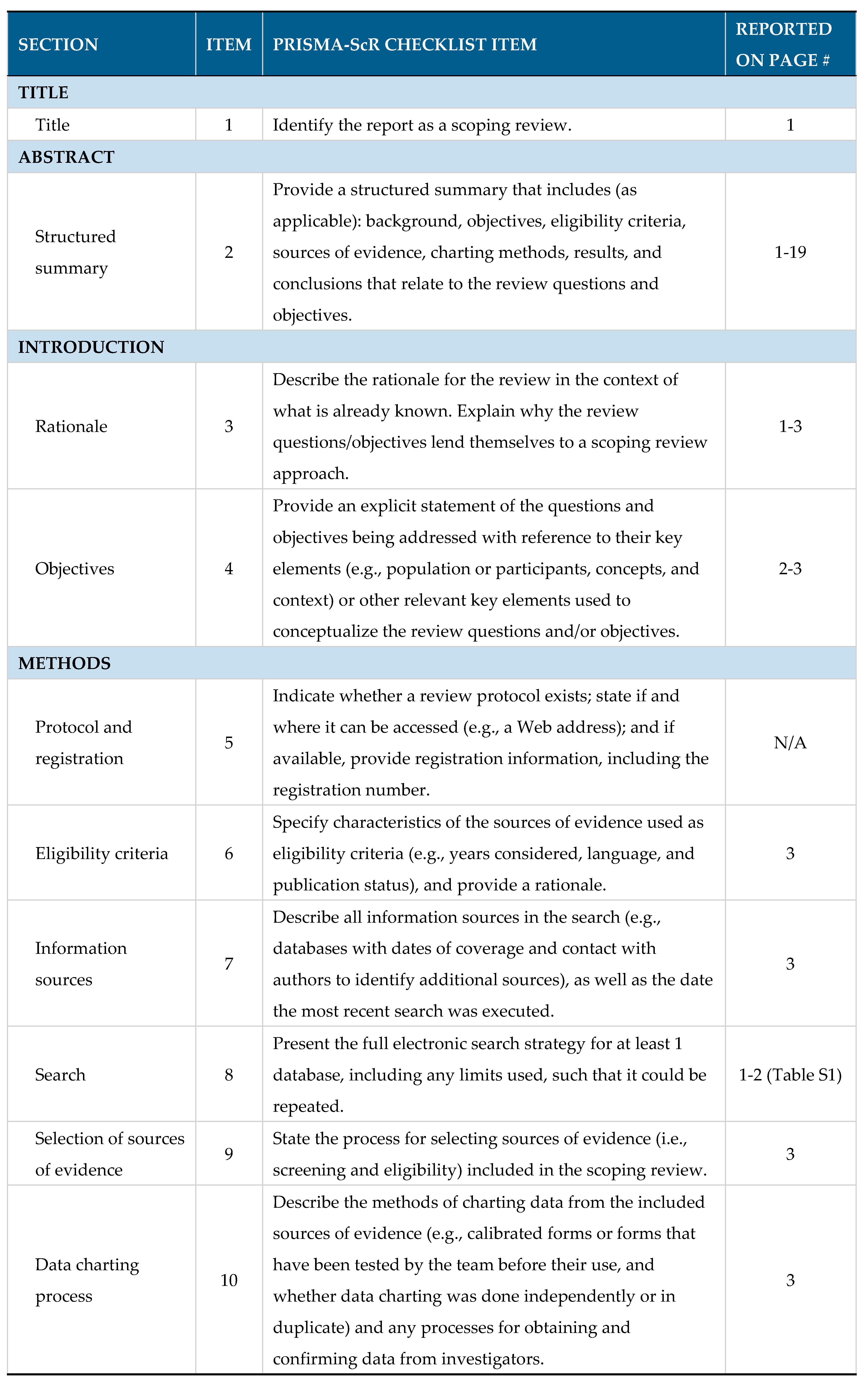
This scoping review was conducted in alignment with the Joanna Briggs Institute guidelines on scoping reviews together with the PRISMA extension for Scoping Reviews (PRISMA-ScR) checklist (see Table A1 in the Appendix) [40,41].
Several electronic databases and platforms were consulted for peer-reviewed literature, namely, PubMed, Scopus, Web of Science and EBSCOhost (Academic Search Premier, Africa-Wide Information, CINAHL, Health Source: Nursing/Academic Edition, and APA PsycInfo). Additionally, grey literature was sourced from organizational websites like WHO (http://www.who.int/), United Nations International Children’s Fund (UNICEF, https://www.unicef.org/) and Gavi, the Vaccine Alliance (http://www.gavi.org/). Supplementary searches for peer-reviewed and grey literature were sourced by reviewing bibliographies and performing additional internet searches on Google Scholar. Developed with guidance from an information specialist, the search strategy included synonyms of keywords and terms like hepatitis B, hepatitis B vaccines, birth dose, and birth dose vaccine (Table S1 in the Supplementary Material).
Only relevant literature published in English were considered. To map the progress and challenges of adopting hepatitis B birth-dose vaccination programs overtime and ensure that a wide scope of evidence was assessed, relevant literature published within the last 22 years (2000–2022) were sourced. All search yields were imported to Mendeley Reference Manager® [42] and after removal of duplicate records, exported to Rayyan® [43]. Here, titles, abstracts and full texts were screened against the inclusion and exclusion criteria, and eligible articles selected for this review. Data charting involved extraction of information like author name, year of publication, title, study setting, study design, and main outcomes, from full text articles which were then reported as narrative summaries.
3. Results
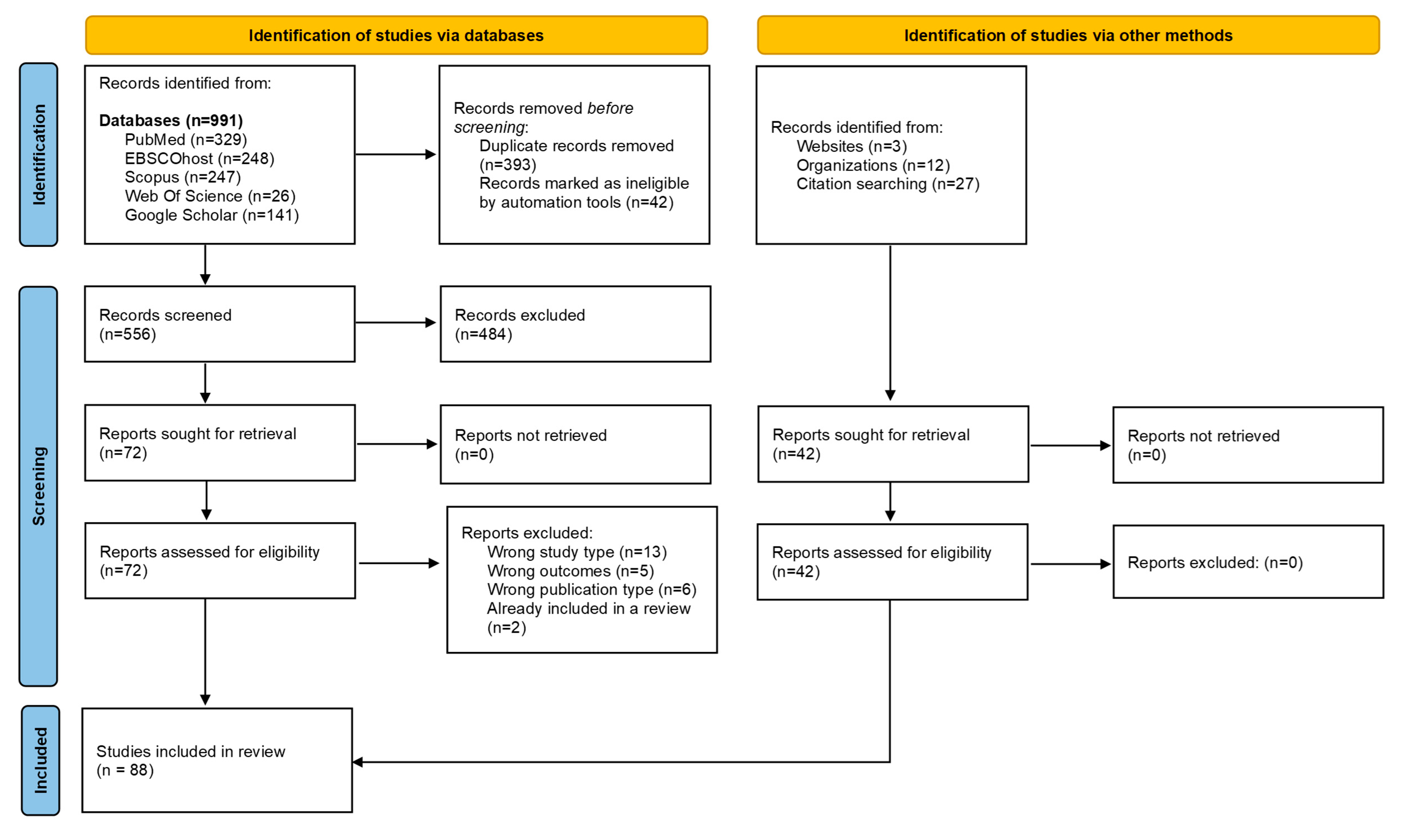
A total of 991 records were retrieved from all the databases searched. After de-duplication, abstract, title, and full text screening, 72 unique records were identified. Of the 72 records, 46 reported on relevant research conducted in the WHO Africa region. Additional published literature sources were identified through supplementary searches and judged to be eligible for inclusion. Overall, 88 literature sources were included in this scoping review (Figure 1). These varied across study types, and included quantitative and qualitative empirical studies, scoping and systematic reviews, commentaries and expert opinions and international guidelines, organizational webpages, reports, and theses (Table S2). The findings of this scoping review are organized and reported under three key themes.
3.1. Status of HBV MTCT in the WHO Africa region
Areas of high endemicity are defined as having an HBsAg prevalence of ≥8%, moderate endemicity between 2–7% and low endemicity <2% in the general population [2,6]. In Africa, an estimated HBsAg prevalence of 7.5% is recorded and it is considered home to approximately 88% of the world’s 296 million chronic carriers [1,3,16,17]. Historically, horizontal transmission was known to drive the epidemic in the region [3]. In recent decades a shift towards vertical transmission has been observed and is cited to be influenced by the HIV epidemic [3,19]. Despite this, strategies employed to control the burden of hepatitis B depend almost solely on the 1992 WHO recommendation of universal hepatitis B infant vaccination commencing at 4 or 6 weeks of life [5]. In the absence of strategies targeting the interruption of vertical transmission, the cycle of chronic infection continues to fuel the morbidity and mortality caused by HBV-related cirrhosis and hepatocellular carcinoma [2,15]. The immaturity of the neonatal immune system increases the risk of viral replication and is suggested as the reason for delayed clearance of HBeAg [44], whereas acute infections in immunocompetent adults are likely to be cleared [15]. In a meta-analysis of HBV infection among women in sub-Saharan Africa, HBeAg positivity was shown to increase the risk of vertical transmission to 38.3% compared to 4.8% in HBeAg negative women [45]. Therefore, assessing the prevalence of HBV MTCT, the influence of HIV co-infection, and the strategies available for effective prevention of HBV MTCT in Africa is essential.
3.1.2. Growing prevalence of HBV MTCT
It is established that HBV MTCT depends on the presence of increased maternal infectiousness, correlating with HBeAg positivity [1]. Historically, women of child-bearing age in Africa are considered to have relatively low prevalence of HBeAg (0.5–3.5%) compared to that in South and South-East Asia (78%) [5,6,46]. Growing evidence on the risk of HBV MTCT in the African region now suggests moderate to high endemicity of HBV infection among pregnant women and women of child-bearing age [2,5,6,47]. A recent review by Breakwell et al., identified 75 studies across 18 countries in Africa which report HBeAg positivity rate among pregnant women ranging from 3.3% in Zimbabwe to 28.5% in Nigeria [2]. Studies assessing perinatal transmission in mother-child pairs by testing HBsAg and HBeAg prevalence in mothers and their offspring, have also found high rates of paired positivity [2,5,6], more so in those mothers positive for HBeAg or with high HBV DNA levels [2,5,6]. It is worth noting that the risk of vertical transmission has been found to remain present but reduced in 2–10% of HBeAg negative pregnant women within the region [5].
In a 2016 situational report compiled by the WHO Africa regional office, scarcity of evidence on chronic HBV infection and the risk of perinatal transmission in Africa were identified by 6 countries as one of the barriers to hepatitis B birth-dose introduction [48]. Since then, the knowledgebase has developed and consistently points to a growing risk of vertical transmission within the region [7,8,9,10,11,12,13,14,15,49], as presented in Table 1. All studies report moderate to high HBV prevalence among pregnant or postpartum women. This is demonstrated by the high HBsAg prevalence among pregnant women in countries like Ethiopia (6.9%), Cameroon (7.7%), The Gambia (9.2%), South Sudan (11%) and Uganda (11.8%) [7,8,9,10,11]. In comparison, moderate HBsAg prevalence rates have been reported among pregnant women in countries like the Republic of Congo (2.7%), Tanzania (3.9%), South Africa (4.5%) and Burkina Faso (4.8%) [12,13,14,15]. Evidently substantial variations exist in the burden of disease across countries, with the highest HBsAg prevalence rates noted in the Central and West African regions [5,50].
Figure 1.
PRISMA flow diagram of literature search, screening, and selection process [51].
Figure 1.
PRISMA flow diagram of literature search, screening, and selection process [51].
3.1.3. HIV-HBV co-infection and the increased risk of HBV MTCT
Accompanying the high burden of HBV infections in the region is the simultaneous burden of HIV infection [20]. It is estimated that 18 million HIV positive women reside in Africa, of whom the majority are of child-bearing age [1]. Given that those who are co-infected with HIV have a greater prevalence of HBeAg positivity, higher HBV DNA levels, and are subject to frequent reactivation of latent HBV infections, the risk of HBV MTCT in HIV co-infected pregnant women is increased compared to that in their HBV mono-infected counterparts [19]. A global review of HIV-HBV co-infections cited a 4.6% midpoint prevalence of HBsAg from 23 studies involving pregnant women [52]. Several studies in Africa have demonstrated the significant risk of vertical transmission of HBV in both HIV seropositive and negative populations [19,23,53]. It is estimated that around 10% of HBV infected pregnant women are HBeAg positive regardless of HIV serostatus, although significant disparities exist in the risk of HBV MTCT within the region [47]. This has been demonstrated by the high HBeAg positivity rates among HBsAg positive pregnant women across the region like the Democratic Republic of Congo (10%), Burkina Faso (11.5%), Uganda (14.9%), South Africa (16.6%) and Cameroon (26.1%) [7,10,13,14,15]. In two South African studies comparing HBsAg positive pregnant women stratified by HIV status, no significant difference in HBeAg positivity between either group was found [19,23]. The widespread availability of HBV-active antiviral therapy for those living with HIV, offers a plausible explanation for the similarities in prevalence of HBeAg positivity between HIV positive and negative pregnant women [1,20]. Studies in Uganda, Senegal, Zambia, and Cameroon have demonstrated the protective effect of HBV-active antiviral therapy in preventing HBV MTCT [7,49,53,54]. These available antiviral therapies like lamivudine, telbivudine, tenofovir, and entecavir have largely been proven effective and safe in reducing HBV viral loads in pregnant women [1]. Unfortunately, access and procurement of these medications have been limited to HIV positive populations leaving HBV mono-infected pregnant women at greater risk for vertical transmission [1,4,20].
3.2. Mitigation strategies for prevention of HBV MTCT in the WHO Africa region
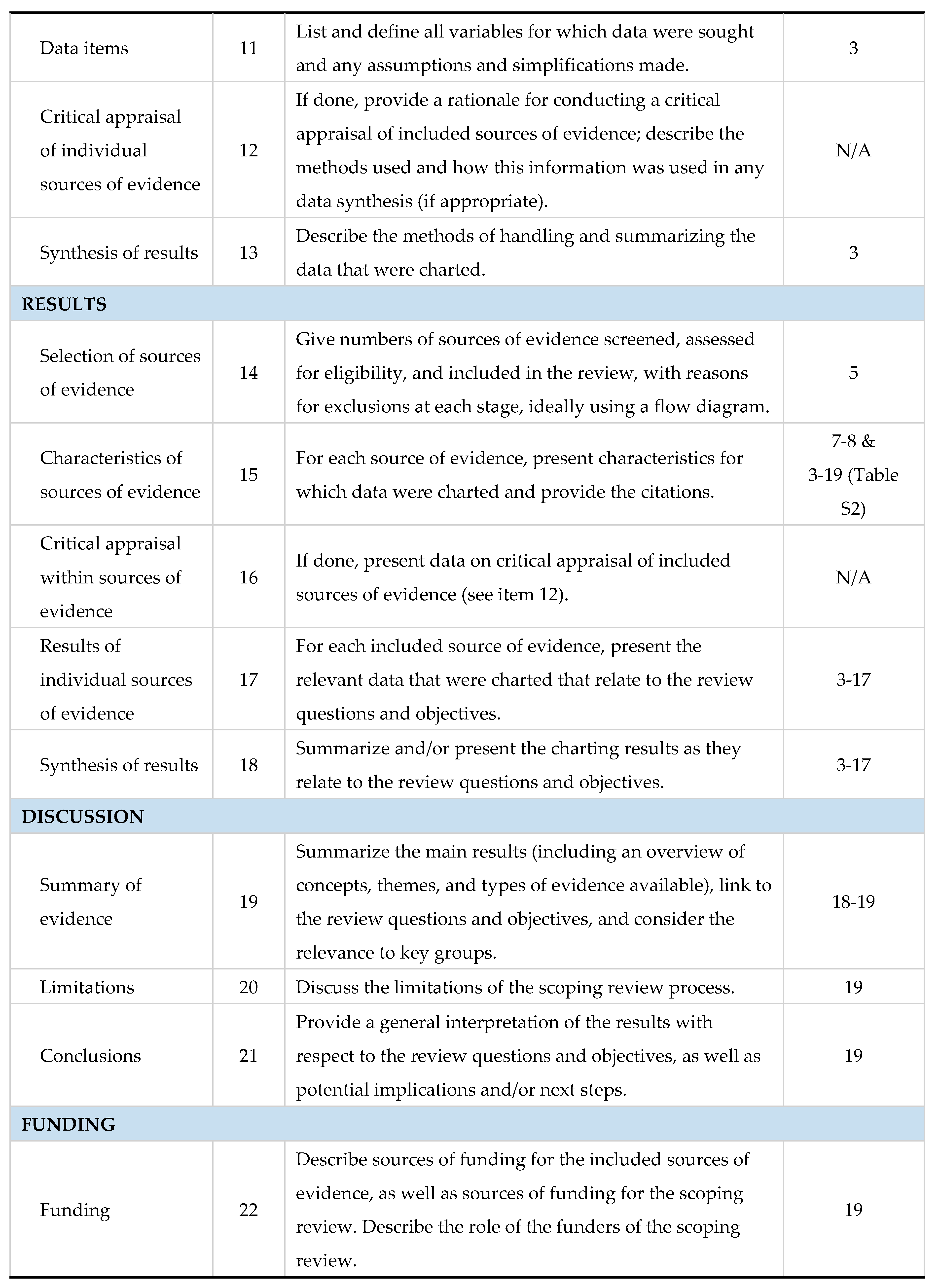
Safe and effective strategies are available for prevention of HBV MTCT to neonates and infants from as early as the in-utero stage as shown in Figure 2. Antenatal screening has the advantage of identifying those at risk for HBV MTCT who can then be timely linked to appropriate care such as HBV-active antiviral prophylaxis [47]. During antenatal visits, pregnant women should also be provided with information on HBV infection, the lifetime risk for chronic liver disease associated with HBV MTCT, and the prevention strategies available to them and their babies including hepatitis B birth-dose vaccination [23,47]. Unfortunately, for some African countries, antenatal screening for HBV infection can be expensive and impractical if laboratory facilities are not situated close to antenatal clinics [23,47]. Despite this, feasibility of antenatal screening for HBV infection has been proven in South Africa [15], and cost-effectiveness demonstrated in Namibia as part of the national HBV MTCT prevention package [3]. Maximum gains can be achieved if HBV antenatal screening is integrated with existing HIV and syphilis point-of-care testing infrastructure [15,55].
Antiviral prophylaxis offered in the third trimester to at-risk pregnant women has been proven to suppress maternal viral loads and decrease the likelihood of HBV MTCT [4,15,20]. The HBV-active antiviral prophylaxis is safe, effective, and readily available in Africa [20,47]. Despite this, and as alluded to previously, access for HBV mono-infected pregnant women in the region appears limited given that there are no subsidized HBV-active antiviral programs [20,47]. To the contrary, HBV-HIV co-infected pregnant women have access to lifesaving prophylaxis through established HIV treatment programs [20,47]. The fixed combination dosage of HBV-active antivirals prescribed for the treatment of HIV is subsidized, leaving resource-constrained settings having to pay higher prices for treatment for HBV mono-infection [20]. This calls for further interventions at the policy level to improve access to low-cost antiviral prophylaxis for HBV mono-infected pregnant women as part of HBV MTCT prevention strategies [47].
For neonates born to women living with chronic HBV infection, hepatitis B immunoglobulin (HBIG) offers further benefit in preventing HBV MTCT by providing passive immunization to HBV exposed neonates particularly when administered within 24 hours of birth [3]. According to the international guidelines from key special interest groups like the American, and the European Association for the Study of Liver Disease, HBV exposed infants should receive both HBIG and a birth-dose of the hepatitis B vaccine [56,57]. In high income countries the standard of care includes both interventions [20,55]. In low resource settings, the high cost and the logistics of cold chain storage and administration of HBIG limit its acceptability as an HBV MTCT prevention strategy [3,4,15,20,47,55].
Although all strategies have shown effectiveness [23,58], universal hepatitis B birth-dose vaccination has demonstrated both high cost-effectiveness [1,22] and suitability for the African context [23]. Unlike HBIG, the hepatitis B birth-dose vaccine is stable outside of the cold chain [59], and therefore improves accessibility in low- and middle- income countries (LMICs) [60]. It also presents a feasible opportunity for integration into existing infrastructure like the Expanded Programme on Immunization and prevention of HIV MTCT packages [14]. Hence universal hepatitis B birth-dose vaccination offers an equitable solution to accelerating regional progress towards achieving global elimination of hepatitis B by 2030. Between 75–95% of vertical transmissions can be prevented by vaccinations alone if the birth-dose is followed by completion of at least 3 doses of the hepatitis B vaccine in infancy [22]. The global coverage of hepatitis B birth-dose vaccination has steadily improved from 5% in 2000 to 45% in 2022 [21], although this is well below the GHSS 2030 target of 90% [25]. Among all 6 WHO regions, the coverage rate of the hepatitis B birth-dose vaccine in Africa is significantly dismal at 18%, compared to 80% in the Western Pacific; 65% in the Americas; 58% in South-East Asian; 42% in European; and 32% in the Eastern Mediterranean regions [21]. This suboptimal coverage is independent of the number of African countries who have adopted universal hepatitis B birth-dose vaccination programs [29,30,61]. As shown in Figure 3, only 15 member states currently offer this intervention; Algeria, Angola, Botswana, Cabo Verde, The Gambia, Mauritania, Namibia, Nigeria, São Tomé and Príncipe, Senegal, Cote d’Ivoire, Benin, Equatorial Guinea, and Ethiopia all have universal hepatitis B birth-dose policies in place, whereas Mauritius currently provides selective hepatitis B birth-dose vaccination to HBV exposed neonates [2,29,30]. It is important to note that while other African countries have not adopted a national universal hepatitis B birth-dose vaccination policy [29], they may provide targeted hepatitis B birth-dose vaccination to infants born to HBeAg positive mothers in certain sub-regions or health facilities, as per national guidelines for prevention of MTCT or as part of project-based programs like research studies conducted in order to motivate for national implementation [14,15]. In this regard, there may be an underestimation of the true coverage of the hepatitis B birth-dose vaccine in Africa compared to what is officially reported to the WHO [21,62]. Without universal and optimal screening programs to identify all at-risk pregnant women, these targeted approaches may encounter significant challenges. Nevertheless, the low implementation of universal hepatitis B birth-dose vaccination within Africa is concerning given the growing risk of HBV MTCT in this region.
Despite the lack of region-wide adoption of hepatitis B birth-dose vaccination, universal hepatitis B infant vaccination programs have been successful at reducing the incidence of horizontally transmitted HBV infection in under 5-year-olds, leading to a significant reduction in the burden of the disease worldwide [63]. The WHO Africa regional office reports that all 47 member states have introduced routine childhood hepatitis B vaccination with the majority (94%) using the pentavalent vaccine (a combination vaccine for diphtheria, tetanus, hepatitis B, pertussis, and Haemophilus influenzae type B), administered in a 3-dose schedule at 6, 10 and 14 weeks of life [2]. However, various studies have demonstrated ongoing HBV infection in children despite the receipt of all 3 doses [4,64,65,66,67], suggesting susceptibility to infection from exposure early on at birth [19]. It is therefore clear that the current strategy is insufficient at interrupting HBV MTCT which carries a higher likelihood of life-long infection and fatal outcomes.
3.2.1. Barriers to adopting universal hepatitis B birth-dose vaccination programs
The evidence presented so far argues for a growing risk of HBV MTCT in Africa. The 2017 Global Hepatitis Report emphasizes the fact that hepatitis B birth-dose vaccination remains the cornerstone of preventing vertical transmission [63] due to its cost-effectiveness and far-reaching lifesaving benefits [3]. It is therefore considered a non-negotiable component in the HBV MTCT prevention package for the region [3]. Cost-effectiveness of hepatitis B birth-dose vaccination in particular, has been researched widely across Africa, and proven beneficial in countries within west, east, south and central Africa [3,22,68,69,70,71,72,73]. Despite this, and as mentioned above, only 15 member states have adopted the vaccine as part of their national immunization programs at the time of compiling this review, having already missed interim targets set by the WHO Africa regional office of 25 countries adopting the vaccine by 2020 [28].
Key barriers to the adoption of hepatitis B birth-dose vaccination in countries within the region are cited in the 2016 WHO African regional situational report [48]. As reported by member states, these include (i) lack of financial support from Gavi, the Vaccine Alliance (10 countries), (ii) the need for further evidence on the burden of chronic HBV infection and the risk of perinatal transmission in Africa (6 countries), (iii) insufficient cold chain storage (3 countries), (iv) a high proportion of home births (2 countries), and (v) the lack of trained health care workers (HCWs) in attending to birth or conducting post-natal visits (2 countries) [48]. Tamandjou Tchuem et al., further cite a lack of political willingness, poor service delivery arrangements, and inadequate cold-chain systems as reasons for the delay in introducing universal hepatitis B birth-dose vaccination in Africa [47]. These findings suggest the need for further high-level political commitment and system-wide approaches to mitigate these barriers and strengthen prevention of HBV MTCT in Africa [47].
3.2.2. Challenges faced by established hepatitis B birth-dose vaccination programs
In countries that have universal hepatitis B birth-dose vaccination programs in place, coverage estimates reported by the WHO and UNICEF, consistently show sub-optimal and disparate uptake of the hepatitis B birth-dose vaccine (Figure 4). For example, in 2021 WHO estimates indicated that the coverage of the hepatitis B birth-dose vaccine ranged from 25% in The Gambia, 52% in Nigeria to 96% in Algeria [21,62]. These disparate coverage rates may not provide comprehensive information on the timeliness of vaccination. In addition, they suggest persistent programmatic challenges in those countries reporting suboptimal coverage rates. Several studies have investigated the programmatic barriers to optimal uptake of the hepatitis B birth-dose vaccine in Africa, using both quantitative and qualitative research approaches. Some of the barriers reported across the literature include the lack of relevant policies at both national and health facility levels [73,74], lack of funding or out-of-pocket payment requirements [75], poor monitoring and evaluation systems [73,74], lack of integration with the maternal and child health package [14,74], lack of awareness about HBV infection and hepatitis B birth-dose vaccination among pregnant women [75,76], geographical inaccessibility of immunization clinics [75,77], inaccessibility due to allotted vaccination days [74,75], frequent stock outs [75,78], home births [79,80], lack of outreach services [74], mistrust of HCWs handling newborns [76], birth-dose administered on discharge only [74], poor knowledge on contraindications among HCWs, and the absence of delineated staff [74]. Limited access consistently emerges as a common thread across these reported barriers, whether it be the inability of national governments to secure necessary, sustainable financing mechanisms to procure hepatitis B birth-dose vaccines, limited access to information on birth-dose vaccination, geographical access barriers including limited access to immunization clinics, and frequently mentioned, poor access to the birth-dose vaccine for home births. In relation to the challenges associated with home births, expert opinions have reiterated the importance of encouraging institutional delivery, as the coverage of hepatitis B birth-dose vaccination is correlated with the rate of skilled birth attendance and institutional delivery, globally [81]. In a previous systematic review addressing Nigeria’s position on vertical transmission of hepatitis B, the rate of institutional delivery was reported to be only 35% and those attending antenatal care, 58% [6]. Consequently, hepatitis B birth-dose vaccine coverage in Nigeria remains sub-optimal (52%) despite integration with the national immunization schedule [21,80,82]. While calls for improved institutional delivery are valid [1,2,81], it remains important that national health systems become more responsive to cultural contexts where home births and isolation periods post-birth are concerned [2,76,77]. This may require tailored approaches to expanding the reach of the hepatitis B birth-dose vaccine within the African setting. This may include conducting community outreach and linkage to vaccination services and increasing community awareness through maternal education on HBV and hepatitis B birth-dose vaccination [2,6,77]. At the governance and policy level, there is a need to strengthen political commitment and prioritization of global HBV elimination targets [1,47,81,83].
3.2.3. Poor adherence to timely hepatitis B birth-dose vaccination
A priority concern facing hepatitis B birth-dose vaccination programs in Africa is the poor adherence to the recommended time of administration [2,84]. The Strategic Advisory Group of Experts on Immunization recommend administering the hepatitis B birth-dose within the first 24 hours of life, although it remains effective against perinatal infection if administered within 7 days [2], and still beneficial in preventing early horizontal transmission if administered after 7 days [24]. Yet national policies in the region recommend a range of what is considered acceptable timely administration of hepatitis B birth-dose vaccination, from 24 hours to as long as 2 weeks in countries like Namibia [2]. A study in Senegal found that only 54.5% of infants were vaccinated within 24 hours and in total 58% within 7 days [79]. The situation is even more concerning in São Tomé and Príncipe where only 1.1% of infants have been reported to receive their hepatitis B birth-dose vaccination within 24 hours of life [85]. In The Gambia, a review of 10 years of coverage data in a district found that only 1% of infants were vaccinated with hepatitis B birth-dose within 24 hours, 5% within 7 days and 58% within 28 days of life [2,77]. Similarly, in Nigeria, among children admitted to an emergency room, the mean age at hepatitis B birth-dose vaccination was 28 days [2]. Delayed uptake of the hepatitis B birth-dose vaccine could lead to the program being judged as ineffective at interrupting MTCT as neonates who do not receive the vaccine on time will have increased susceptibility to HBV infection. Furthermore, this inconsistency in adherence to the timing may negatively impact the potential for greater and effective uptake and adoption of hepatitis B birth-dose vaccination in other parts of the region.
Observations on other birth-dose vaccines in the region could offer further insights into the performance of programs with the same overall specification. In Africa, coverage of all three recommended birth-dose vaccines, namely, BCG, OPV and hepatitis B birth-dose vaccines, were estimated by the WHO/UNICEF at 75%, 70% and 17% in 2021, respectively [21]. While coverage data clearly shows poorer uptake of the hepatitis B birth-dose vaccine compared to BCG and OPV, it does not provide an indication of the timeliness of uptake of these vaccines. A systematic review by Bassoum et al., sought to investigate the timeliness of birth-dose vaccinations in sub-Saharan Africa and found that most neonates received their birth-dose vaccines within the first month of life, with coverage at this timepoint as follows; BCG at 71.7%; OPV at 76.1%; hepatitis B birth-dose at 60.8% [61]. In comparison, coverage rates followed a downward trend on day 7 (BCG at 48.7%, OPV at 53.8%, and hepatitis B birth-dose at 21.5%) and on day 0–1 (BCG at 14.2% and hepatitis B birth-dose at 1.3%) [61]. Coverage of OPV for the day 0–1 time point was not recorded by any of the included studies [61]. Overall, it is evident that within the Africa region, hepatitis B birth-dose vaccination programs achieve the lowest coverage rates and timeliness [61]. It is possible that the increased coverage and timeliness of BCG and OPV birth-dose vaccines can be attributed to their near-universal adoption (both vaccines have been included in the national immunization programs of 45 and 39 member states, respectively) and longstanding programs within Africa [61]. In comparison, universal hepatitis B birth-dose vaccination is only available in a limited number (15) of member states [61]. Nevertheless, greater efforts are required to ensure timely administration of the hepatitis B birth-dose vaccine. Such efforts will have to be guided by context specific evidence on the barriers to timely administration and uptake of the hepatitis B birth-dose vaccine. Without timely intervention, the combination of low vaccine coverage and the non-adherence to the recommended time of administration may hamper efforts to achieve viral hepatitis elimination as a public health threat.
3.3. State of health systems and hepatitis B birth-dose vaccination programs in the WHO Africa region
Global agencies have recognized well-functioning health systems as crucial to the optimal performance of so-called vertical health programs, and in attaining global health targets [32,86,87]. Despite effective and affordable interventions as well as access to international donor funding, fragile and fragmented health systems are often incapable of delivering key health services of adequate volume and quality [31,32,87]. Identifying programmatic barriers, though essential, is likely only an indication of the weaknesses that exist across the broader health system.
The country context has a considerable influence on the capabilities of the health system to effectively support the performance of health programs. Accordingly, barriers to the adoption and optimal performance of universal hepatitis B birth-dose vaccination programs in the region may be unique to the health systems that deliver them. For example, it has been previously suggested that countries with prolonged civil unrest and unstable governance, as observed previously in countries like Uganda and South Sudan, experience negative implications in the functioning of their health programs including hepatitis B birth-dose vaccination [11]. Furthermore, while countries like Nigeria contribute the largest amount of research on HBV MTCT in the region, the evidence generated has so far not translated into optimal coverage rates of the hepatitis B birth-dose vaccine [2,21]. Similarly, The Gambia, with more than 10 years of access to universal hepatitis B birth-dose vaccination continues to experience inconsistencies with coverage rates [2,21]. This may point to the influence of contextual health systems issues in these settings and may call for a “deeper understanding of the linkages, relationships, interactions and behaviors among elements that make up the entire system” [34]. Such an approach is better referred to as ‘systems thinking’ [34], and as health systems are inherently complex [35], a more ‘complex systems thinking’ approach could be adopted. This could allow for the anticipation of system-wide effects as well as undesired synergies, which can then better inform mitigation strategies [34]. In doing so, system-level interventions can be modified, and more comprehensive evaluations designed for better monitoring of effects [34,87].
3.3.1. Conceptual models for the assessment of health systems capacity
According to the WHO, a health system encompasses “all organizations, people and actions whose primary intent it is to promote, restore and maintain health” [88]. This definition extends beyond just the delivery of health services and includes the acknowledgment of a complex people-centered system requiring the exploration and collaboration of multiple sectors for the attainment of health [88]. To promote a common understanding of health systems, the WHO provides a framework consisting of six dimensions (service delivery; health workforce; information; medical products, vaccines, and technologies; financing; and leadership and governance) referred to as building blocks [31,88]. Though several conceptual frameworks have attempted to capture the elements of health system performance in its entirety [86,88,89,90], the WHO health systems framework has become the most quoted framework in recent works [31].
Even though the WHO framework is effective in clarifying essential functions of the health system [88] it has been criticized for depicting the six dimensions in silos [31]. Realistically, it is the interdependence between the dimensions that is recognized as paramount entry points for addressing programmatic challenges [88]. The interpretation of this model by de Savigny and Adam better explores the interaction between the dimensions in a non-linear relationship centered around the people within the health system [34]. The multiple relationships and interactions between the dimensions therefore result in the creation of a system [34]. Van Olmen et al., further emphasize the broader context in which a health system is embedded, the influence of its principles and values, and includes the population as part of the system [91]. Taken together, these conceptual models [34,88,91] emphasize the fact that health systems are complex systems [34]. Furthermore, complex systems are “dynamic, with interacting components — at various geographical levels — that lead to adaptation and emergence of new dynamics” [31].
3.3.2. Complexity as a characteristic of hepatitis B birth-dose vaccination programs
Though it is established that not all interventions will benefit from a systems-thinking approach, complex interventions are likely to have profound effects across the system, more so in weak health systems [34]. Among all three birth-dose vaccines endorsed by the WHO (BCG, OPV, hepatitis B birth-dose), universal hepatitis B birth-dose vaccination programs in Africa have performed the poorest, a fact likely attributable to the complexity of the intervention found in the limited degree of flexibility afforded in its requirement of timely administration within 24 hours of life [38,61]. This has raised concerns on task shifting, cold storage, data capturing and policy change [14,73,74], proving the complexity of the intervention across most, if not all, the health systems building blocks. Characteristics describing intervention complexity have been conceptualized by many [34,37,39] and collated in a comprehensive list in Petticrew et al., assisting in the identification of sources of complexity [38]. With this in mind, it is likely that that other sources of complexity associated with the intervention, or the health system could provide further explanations for the underperformance of hepatitis B birth-dose vaccination programs in this region. In seeking complex explanations, complex approaches should be considered [36]. Using the principles of complex systems thinking and applying a systems lens in assessing existing hepatitis B birth-dose vaccination programs could facilitate a richer understanding of the aforementioned barriers and inform interventions aimed at scaling up the delivery of the program.
3.3.3. A systems-based logic model for assessing complexity within hepatitis B birth-dose vaccination programs
We propose a systems-based logic model for understanding the role of complexity within hepatitis B birth-dose vaccination programs and the health systems that deliver them (Figure 5). This model is an adaptation of the template designed by Rohwer et al., for systematic reviews of complex interventions and builds on previous related frameworks [92,93,94]. It depicts the system in which interactions among the participants, the intervention (hepatitis B birth-dose vaccination), and the context, take place [94]. The intervention is divided into theory, design, and delivery, with the expansion of these subcomponents into key aspects like process of execution, delivery mechanisms and agents. Program implementation requires details on policy, financing, providers, organization and structure, while context requires the description of the geographical, epidemiological, socio-cultural and economic, ethical, legal, and political landscapes. Finally, outcomes are categorized into short, inter-mediate and long term, with consideration for the nature of these outcomes [94]. Application of this model in future evidence syntheses on hepatitis B birth-dose vaccination programs in the African region may provide a means of conceptualizing complexity and system-wide effects, making findings more accessible to a broad range of decision- and policy- makers [94].
4. Discussion
While previous reviews have applied a systems thinking lens, both at global [84] and regional [78] levels, they fall short in the representation of research evidence from the WHO Africa region, rendering generalizability problematic. Additionally, these previous reviews have not fully appreciated systems complexity or the diverse contextual underpinnings of hepatitis B birth-dose vaccination programs in the WHO Africa region. This could potentially limit regional efforts to implement evidence-based, context specific public health interventions aimed at encouraging further adoption of universal hepatitis B birth-dose vaccination programs and strengthening the performance of programs that are already in existence.
With the use of evidence synthesis approaches, efforts have been made to better understand the barriers to the adoption of universal hepatitis B birth-dose vaccination, optimal vaccine coverage, and overall performance of the program across Africa. In 2017, Breakwell et al., published a MEDLINE literature review citing (i) timely administration, (ii) high prevalence of home births, (iii) the lack of services available to reach infants born at home, (iv) and unreliable vaccine supply, as challenges limiting improved adoption and coverage of the hepatitis B birth-dose vaccination program [2]. Dionne-Odom et al., further undertook a PubMed literature review which categorized four barriers to improved performance of hepatitis B birth-dose vaccination in the region, and these included, (i) limited awareness of HBV prevalence and preventative measures, (ii) vaccine availability, (iii) out of facility deliveries and (iv) cold chain storage requirements [1]. Moreover, a WHO systematic review on the global compliance with timely hepatitis B birth-dose vaccination reported a paucity of research evidence from the WHO Africa region compared to other regions, with only four publications representing four African countries meeting the inclusion criteria for that review [48]. Of the four, only one publication described programmatic barriers which suggested that living in rural areas was the most weighted risk factor limiting access to the hepatitis B birth-dose vaccine post-delivery [48,77].
To date, two previous scoping reviews have applied a systems-thinking perspective in identifying practices to improve the implementation of hepatitis B birth-dose vaccination [78,84]. In 2012, the WHO Immunization, Vaccines and Biologicals department, summarized and appraised implementation evidence from 65 studies using the WHO health systems framework to categorize barriers and facilitators [84]. Recommendations emerging from that review ranged across all building blocks, some of which included encouraging governments to adopt a central policy on universal hepatitis B birth-dose vaccination as well as setting clear guidelines on the definition of ‘timely administration’, the meticulous tracking of pregnancies and birth by community HCWs to improve hepatitis B birth-dose vaccine coverage, and the usage of single dose vials to discourage the practice of delaying hepatitis B birth-dose vaccination due to concerns with wastage when using multi-dose vials [84]. While that review sought to provide guidance for LMICs in implementing universal hepatitis B birth-dose vaccination programs, none of the included studies were from Africa or focused on the complexity of the intervention or system. More recently in 2022, Boisson et al., sought to identify literature focused on introducing hepatitis B birth-dose vaccination programs and barriers to uptake in sub-Saharan Africa [78]. The authors of this review summarized and categorized 39 relevant reports based on determinants of implementation at the policy, facility, and community levels [78]. Findings ranged from policy advocacy, facility supply and stockouts, to community HCW involvement, among other factors [78]. Again, while the authors sought to provide an overview of experiences from sub-Saharan Africa, the scoping extended to research conducted in the South-East Asian region and only included 13 publications from sub-Saharan Africa of the total 39 included studies [78]. Thus, while the evidence-based recommendations from these reviews are comprehensive and may meet the needs of policy makers and immunization program managers in some LMICs, the findings may not always be generalizable to the African context.
This scoping review of research evidence published over the last 22 years reports compelling evidence on the growing risk of HBV MTCT within the WHO Africa region, spurred by the considerable burden of HIV co-infections. Building on the findings of previous reviews, we contribute critical system-wide barriers underpinning the weak adoption and performance of hepatitis B birth-dose vaccination programs in this region [2,48,78,84]. Taken together, these findings underscore the urgency to scale-up universal hepatitis B birth-dose vaccination programs across Africa with careful consideration for underlying systems complexities. Key strengths of this scoping review include adherence to published methodological guidelines and the use of a systematic literature search across multiple electronic databases and relevant organizational websites. Despite this, our findings will have to be considered in light of some methodological limitations. While scoping reviews provide comprehensive and up-to-date information on a topic of focus, other evidence synthesis approaches like systematic reviews provide superior evidence with the lowest risk of bias. In addition, our review only included studies published in English, limiting the generalizability of the findings to Francophone and Lusophone countries from which potentially relevant research outputs may have been excluded.
5. Conclusions
The dearth of synthesized evidence needed to inform health system strengthening efforts to support hepatitis B birth-dose vaccination programs within Africa creates challenges in the adoption and effective performance of this pivotal intervention. By intensifying investments in health systems strengthening efforts, it is possible to achieve optimal service delivery and ultimately improved health outcomes within the population. Such efforts will have to be informed by robust, context-specific evidence. Future research directions should include the exploration of contextualized complex systems approaches to scaling-up hepatitis B birth-dose vaccination programs within the African region.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Literature search strategy for the scoping review; Table S2: Summary of data extracted from included literature.
Author Contributions
Conceptualization, T.S-R., J.O. and E.A-D.; methodology, T.S-R.; formal analysis, T.S-R.; data curation, T.S-R.; writing—original draft preparation, T.S-R.; writing—review and editing, J.O. and E.A-D.; visualization, T.S-R. and E.A-D; supervision, J.O. and E.A-D.; project administration, T.S-R.; funding acquisition, E.A-D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. The APC was supported by the Gilead Research Scholars Program in Public Health.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The complete search strategy and a summary of all extracted data is provided in the supplementary material.
Acknowledgments
The authors thank Namhla Madini for providing guidance with the development of the search strategy and the literature search process during this scoping review.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A

Table A1.
Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist [41].
Table A1.
Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist [41].
References
- Dionne-Odom, J.; Njei, B.; Tita, A. Elimination of Vertical Transmission of Hepatitis B in Africa: A Review of Available Tools and New Opportunities. Clin Ther 2018, 40, 1255–1267. [Google Scholar] [CrossRef]
- Breakwell, L.; Tevi-Benissan, C.; Childs, L.; Mihigo, R.; Tohme, R. The Status of Hepatitis B Control in the African Region. Pan Afr Med J 2017, 27, 17. [Google Scholar] [CrossRef]
- Tamandjou Tchuem, C.R.; Andersson, M.I.; Wiysonge, C.S.; Mufenda, J.; Preiser, W.; Cleary, S. Prevention of Hepatitis B Mother-to-Child Transmission in Namibia: A Cost-Effectiveness Analysis. Vaccine 2021, 39, 3141–3151. [Google Scholar] [CrossRef]
- Chotun, N.; Nel, E.; Cotton, M.F.; Preiser, W.; Andersson, M.I. Hepatitis B Virus Infection in HIV-Exposed Infants in the Western Cape, South Africa. Vaccine 2015, 33, 4618–4622. [Google Scholar] [CrossRef] [PubMed]
- Howell, J.; Lemoine, M.; Thursz, M. Prevention of Materno-Foetal Transmission of Hepatitis B in Sub-Saharan Africa: The Evidence, Current Practice and Future Challenges. J Viral Hepat 2014, 21, 381–396. [Google Scholar] [CrossRef] [PubMed]
- Sadoh, A.; Sadoh, W. Does Nigeria Need the Birth Dose of the Hepatitis B Vaccine? Niger J Paediatr 2014, 41, 104–109. [Google Scholar] [CrossRef]
- Sone, L.; Voufo, R.; Dimodi, H.; Kengne, M.; Gueguim, C.; Nnanga, N.; Oben, J.; Ngondi, J. Prevalence and Identification of Serum Markers Associated with Vertical Transmission of Hepatitis B in Pregnant Women in Yaounde, Cameroon. Int. j MCH AIDS 2017, 6, 69–74. [Google Scholar] [CrossRef]
- Bittaye, M.; Idoko, P.; Ekele, B.A.; Obed, S.A.; Nyan, O. Hepatitis B Virus Sero-Prevalence amongst Pregnant Women in the Gambia. BMC Infect Dis 2019, 19, 259. [Google Scholar] [CrossRef]
- Umare, A.; Seyoum, B.; Gobena, T.; Haile Mariyam, T. Hepatitis B Virus Infections and Associated Factors among Pregnant Women Attending Antenatal Care Clinic at Deder Hospital, Eastern Ethiopia. PLoS One 2016, 11, e0166936. [Google Scholar] [CrossRef]
- Bayo, P.; Ochola, E.; Oleo, C.; Mwaka, A.D. High Prevalence of Hepatitis B Virus Infection among Pregnant Women Attending Antenatal Care: A Cross-Sectional Study in Two Hospitals in Northern Uganda. BMJ Open 2014, 4, e005889. [Google Scholar] [CrossRef]
- Kirbak, A.L.S.; Ng’ang’a, Z.; Omolo, J.; Idris, H.; Usman, A.; Mbabazi, W.B. Sero-Prevalence for Hepatitis B Virus among Pregnant Women Attending Antenatal Clinic in Juba Teaching Hospital, Republic of South Sudan. Pan Afr. Med. J 2017, 26. [Google Scholar] [CrossRef]
- Rashid, S.; Kilewo, C.; Aboud, S. Seroprevalence of Hepatitis B Virus Infection among Antenatal Clinic Attendees at a Tertiary Hospital in Dar Es Salaam, Tanzania. Tanzan J Health Res 2014, 16, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Guingané, A.N.; Bougouma, A.; Sombié, R.; King, R.; Nagot, N.; Meda, N.; Van de Perre, P.; Tuaillon, E. Identifying Gaps across the Cascade of Care for the Prevention of HBV Mother-to-child Transmission in Burkina Faso: Findings from the Real World. Liver Int. 2020, 40, 2367–2376. [Google Scholar] [CrossRef]
- Thompson, P.; Morgan, C.E.; Ngimbi, P.; Mwandagalirwa, K.; Ravelomanana, N.L.R.; Tabala, M.; Fathy, M.; Kawende, B.; Muwonga, J.; Misingi, P.; et al. Arresting Vertical Transmission of Hepatitis B Virus (AVERT-HBV) in Pregnant Women and Their Neonates in the Democratic Republic of the Congo: A Feasibility Study. Lancet Glob Health 2021, 9, e1600–9. [Google Scholar] [CrossRef] [PubMed]
- Chotun, N.; Preiser, W.; van Rensburg, C.J.; Fernandez, P.; Theron, G.B.; Glebe, D.; Andersson, M.I. Point-of-Care Screening for Hepatitis B Virus Infection in Pregnant Women at an Antenatal Clinic: A South African Experience. PLoS One 2017, 12, e0181267. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021. Accountability for the Global Health Sector Strategies 2016-2021: Actions for Impact.; World Health Organization: Geneva, 2021. [Google Scholar]
- World Health Organization Web Annex 1. Key Data at a Glance. In Global progress report on HIV, viral hepatitis and sexually transmitted infections, 2021. Accountability for the global health sector strategies 2016–2021: actions for impact; World Health Organization: Geneva, 2021. [Google Scholar]
- United Nations Children’s Fund Global and Regional Trends Available online:. Available online: https://data.unicef.org/topic/hivaids/global-regional-trends/ (accessed on 15 August 2023).
- Andersson, M.I.; Maponga, T.G.; Ijaz, S.; Barnes, J.; Theron, G.B.; Meredith, S.A.; Preiser, W.; Tedder, R.S. The Epidemiology of Hepatitis B Virus Infection in HIV-Infected and HIV-Uninfected Pregnant Women in the Western Cape, South Africa. Vaccine 2013, 31, 5579–5584. [Google Scholar] [CrossRef]
- Maponga, T.G.; Matteau Matsha, R.; Morin, S.; Scheibe, A.; Swan, T.; Andrieux-Meyer, I.; Spearman, C.W.; Klein, M.B.; Rockstroh, J.K. Highlights from the 3rd International HIV/Viral Hepatitis Co-Infection Meeting - HIV/Viral Hepatitis: Improving Diagnosis, Antiviral Therapy and Access. Hepatol Med Policy 2017, 2, 1–9. [Google Scholar] [CrossRef]
- United Nations Children’s Fund Immunization Coverage Estimates Data Visualization Available online:. Available online: https://data.unicef.org/resources/immunization-coverage-estimates-data-visualization/ (accessed on 15 August 2023).
- Anderson, S.; Harper, L.M.; Dionne-Odom, J.; Halle-Ekane, G.; Tita, A.T.N.; Dionne-Odom, J.; Halle-Ekane, G. A Decision Analytic Model for Prevention of Hepatitis B Virus Infection in Sub-Saharan Africa Using Birth-Dose Vaccination. Int J of Gynae Obstet 2018, 141, 126–132. [Google Scholar] [CrossRef]
- Diale, Q.; Pattinson, R.; Chokoe, R.; Masenyetse, L.; Mayaphi, S. Antenatal Screening for Hepatitis B Virus in HIV-Infected and Uninfected Pregnant Women in the Tshwane District of South Africa. South African Medical Journal 2016, 106, 97–100. [Google Scholar] [CrossRef]
- World Health Organization Hepatitis B Vaccines: WHO Position Paper, July 2017 – Recommendations. Vaccine 2019, 37, 223–225. [CrossRef]
- World Health Organization Global Health Sector Strategy on Viral Hepatitis 2016-2021. Towards Ending Viral Hepatitis.; World Health Organization: Geneva, 2016; ISBN 9789241503501. [Google Scholar]
- de Villiers, M.J.; Nayagam, S.; Hallett, T.B. The Impact of the Timely Birth Dose Vaccine on the Global Elimination of Hepatitis B. Nat Commun 2021, 12, 6223. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Immunization Coverage Available online:. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 15 August 2022).
- World Health Organization Regional Office for Africa Prevention, Care and Treatment of Viral Hepatitis in the African Region: Framework for Action, 2016-2020; World Health Organization: Geneva, 2017.
- Kabore, J. Hepatitis B Birth Dose (HepB BD) Vaccination in the WHO African Region. In Proceedings of the Building a community of practice to assist hepB birth dose introduction in African countries, 2021., March 17-18 2021.; Coalition for Global Hepatitis Elimination. [Google Scholar]
- Njuguna, H. HepB-BD and Infant HepB3 Coverage Status in Africa. In Proceedings of the Hepatitis B Birth Dose in the African region: Bridging science and advocacy to eliminate mother-to-child transmission of HBV, August 22 2022. [Google Scholar]
- Mounier-Jack, S.; Griffiths, U.K.; Closser, S.; Burchett, H.; Marchal, B. Measuring the Health Systems Impact of Disease Control Programmes: A Critical Reflection on the WHO Building Blocks Framework. BMC Public Health 2014, 14, 278. [Google Scholar] [CrossRef] [PubMed]
- Travis, P.; Bennet, S.; Haines, A.; Pang, T.; Bhutta, Z.; Hyder, A.; Pielemeier, N.; Mills, A.; Evans, T. Overcoming Health-Systems Constraints to Achieve the Millenium Development Goals. Lancet 2004, 364, 900–906. [Google Scholar] [CrossRef] [PubMed]
- Shiell, A.; Hawe, P.; Gold, L. Complex Interventions or Complex Systems? Implications for Health Economic Evaluation. BMJ 2008, 336, 1281. [Google Scholar] [CrossRef] [PubMed]
- Systems Thinking for Health Systems Strengthening; de Savigny, D. , Adam, T., Eds.; World Health Organization: Geneva, 2009. [Google Scholar]
- Evidence Synthesis for Health Policy and System: A Method Guide; Langlois, E. V, Daniels, K., Akl, E.A., Eds.; World Health Organization: Geneva, 2018; ISBN 9789241514552. [Google Scholar]
- Petticrew, M. When Are Complex Interventions “Complex”? When Are Simple Interventions “Simple”? Eur J Public Health 2011, 21, 397–398. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; Macintyre, S.; Mitchie, S.; Nazareth, I.; Petticrew, M. Developing and Evaluating Complex Interventions: The New Medical Research Council Guidance. Bmj 2008, 337, 979–983. [Google Scholar] [CrossRef]
- Petticrew, M.; Anderson, L.; Elder, R.; Grimshaw, J.; Hopkins, D.; Hahn, R.; Krause, L.; Kristjansson, E.; Mercer, S.; Sipe, T.; et al. Complex Interventions and Their Implications for Systematic Reviews: A Pragmatic Approach. J Clin Epidemiol 2013, 66, 1209–1214. [Google Scholar] [CrossRef]
- Hawe, P.; Shiell, A.; Riley, T. Theorising Interventions as Events in Systems. Am J Community Psychol 2009, 43, 267–276. [Google Scholar] [CrossRef]
- JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI, 2020; ISBN 978-0-6488488-0-6.
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Reiswig, J. Mendeley. Journal of the Medical Library Association 2010, 98, 193–194. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—a Web and Mobile App for Systematic Reviews. Syst Rev 2016, 5, 210. [Google Scholar] [CrossRef]
- Shimakawa, Y.; Bottomley, C.; Njie, R.; Mendy, M. The Association between Maternal Hepatitis B e Antigen Status, as a Proxy for Perinatal Transmission, and the Risk of Hepatitis B e Antigenaemia in Gambian Children. BMC Public Health 2014, 14, 532. [Google Scholar] [CrossRef] [PubMed]
- Keane, E.; Funk, A.L.; Shimakawa, Y. Systematic Review with Meta-Analysis: The Risk of Mother-to-Child Transmission of Hepatitis B Virus Infection in Sub-Saharan Africa. Aliment Pharmacol Ther 2016, 44, 1005–1017. [Google Scholar] [CrossRef] [PubMed]
- Ekra, D.; Herbinger, K.-H.; Konate, S.; Leblond, A.; Fretz, C.; Cilote, V.; Douai, C.; Da Silva, A.; Gessner, B.D.; Chauvin, P. A Non-Randomized Vaccine Effectiveness Trial of Accelerated Infant Hepatitis B Immunization Schedules with a First Dose at Birth or Age 6 Weeks in Côte d’Ivoire. Vaccine 2008, 26, 2753–2761. [Google Scholar] [CrossRef] [PubMed]
- Tamandjou Tchuem, C.R.; Maponga, T.G.; Chotun, N.; Preiser, W.; Andersson, M.I. Is Hepatitis B Birth Dose Vaccine Needed in Africa? Pan Afr Med J 2017, 27, 18. [Google Scholar] [CrossRef]
- World Health Organization Global Compliance with Hepatitis B Vaccine Birth Dose and Factors Related to Timely Schedule. A Review. 2016.
- Seremba, E.; Van Geertruyden, J.P.; Ssenyonga, R.; Opio, C.K.; Kaducu, J.M.; Sempa, J.B.; Colebunders, R.; Ocama, P. Early Childhood Transmission of Hepatitis B Prior to the First Hepatitis B Vaccine Dose Is Rare among Babies Born to HIV-Infected and Non-HIV Infected Mothers in Gulu, Uganda. Vaccine 2017, 35, 2937–2942. [Google Scholar] [CrossRef]
- Ott, J.J.; Stevens, G.A.; Groeger, J.; Wiersma, S.T. Global Epidemiology of Hepatitis B Virus Infection: New Estimates of Age-Specific HBsAg Seroprevalence and Endemicity. Vaccine 2012, 30, 2212–2219. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. International Journal of Surgery 2021, 88, 105906. [Google Scholar] [CrossRef]
- Platt, L.; French, C.E.; McGowan, C.R.; Sabin, K.; Gower, E.; Trickey, A.; McDonald, B.; Ong, J.; Stone, J.; Easterbrook, P.; et al. Prevalence and Burden of HBV Co-infection among People Living with HIV: A Global Systematic Review and Meta-analysis. J Viral Hepat 2020, 27, 294–315. [Google Scholar] [CrossRef]
- Sichone, V.; Vwalika, B. Prevalence of Hepatitis B Virus, HIV and HBV Coinfection and Associated Factors in Pregnant Women Attending Antenatal Care at the University Teaching Hospital, Lusaka, Zambia. Med J Zambia 2019, 46, 10–18. [Google Scholar] [CrossRef]
- Gueye, S.; Diop-Ndiaye, H.; Lo, G.; Guindo, I.; Dia, A.; Sow-Sall, A.; Gaye-Diallo, A.; Mboup, S.; Toure-Kane, C. HBV Carriage in Children Born From HIV-Seropositive Mothers in Senegal: The Need of Birth-Dose HBV Vaccination. J Med Virol 2016, 88, 815–819. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Prevention of Mother-to-Child Transmission of Hepatitis B Virus: Guidelines on Antiviral Prophylaxis in Pregnancy; World Health Organization: Geneva, 2020; ISBN 9789240002708.
- Terrault, N.A.; Bzowej, N.H.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Murad, M.H. AASLD Guidelines for Treatment of Chronic Hepatitis B. Hepatology 2016, 63, 261–283. [Google Scholar] [CrossRef] [PubMed]
- Lampertico, P.; Agarwal, K.; Berg, T.; Buti, M.; Janssen, H.L.A.; Papatheodoridis, G.; Zoulim, F.; Tacke, F. EASL 2017 Clinical Practice Guidelines on the Management of Hepatitis B Virus Infection. J Hepatol 2017, 67, 370–398. [Google Scholar] [CrossRef]
- Jooste, P.; van Zyl, A.; Adland, E.; Daniels, S.; Hattingh, L.; Brits, A.; Wareing, S.; Goedhals, D.; Jeffery, K.; Andersson, M.; et al. Screening, Characterisation and Prevention of Hepatitis B Virus (HBV) Co-Infection in HIV-Positive Children in South Africa. Journal of Clinical Virology 2016, 85, 71–74. [Google Scholar] [CrossRef]
- Hipgrave, D.B.; Maynard, J.E.; Biggs, B.-A. Improving Birth Dose Coverage of Hepatitis B Vaccine. Bull World Health Organ 2006, 84, 65–71. [Google Scholar] [CrossRef]
- Dadari, I.K.; Zgibor, J.C. How the Use of Vaccines Outside the Cold Chain or in Controlled Temperature Chain Contributes to Improving Immunization Coverage in Low- and Middle-Income Countries (LMICs): A Scoping Review of the Literature. J Glob Health 2021, 11, 4004. [Google Scholar] [CrossRef]
- Bassoum, O.; Kimura, M.; Dia, A.T.; Lemoine, M.; Shimakawa, Y. Coverage and Timeliness of Birth Dose Vaccination in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. Vaccines (Basel) 2020, 8, 301. [Google Scholar] [CrossRef]
- World Health Organization Hepatitis B Vaccination Coverage Available online:. Available online: https://immunizationdata.who.int/pages/coverage/HEPB.html (accessed on 15 August 2023).
- World Health Organization Global Hepatitis Report 2017; World Health Organization: Geneva, 2017.
- Sanou, A.M.; Ilboudo, A.K.; Meda, Z.C.; Togozia, A.; Coulibaly, A.; Sagna Tani, A.C.; Dramane, K.; Tarnagda, Z. Hepatitis B Vaccination in Burkina Faso: Prevalence of HBsAg Carriage and Immune Response in Children in the Western Region. J Infect Dev Ctries 2018, 12, 1002–1008. [Google Scholar] [CrossRef]
- Apiung, T.; Ndanu, T.A.; Mingle, J.A.A.; Sagoe, K.W.C. Hepatitis B Virus Surface Antigen and Antibody Markers in Children at a Major Paediatric Hospital after the Pentavalent DTP-HBV-Hib Vaccination. Ghana Med J 2017, 51, 13–19. [Google Scholar] [CrossRef]
- Metodi, J.; Aboud, S.; Mpembeni, R.; Munubhi, E. Immunity to Hepatitis B Vaccine in Tanzanian Under-5 Children. Ann Trop Paediatr 2010, 30, 129–136. [Google Scholar] [CrossRef]
- Breakwell, L.; Marke, D.; Kaiser, R.; Tejada-Strop, A.; Pauly, M.D.; Jabbi, S.; Yambasu, S.; Kabore, H.J.; Stewart, B.; Sesay, T.; et al. Assessing the Impact of the Routine Childhood Hepatitis B Immunization Program and the Need for Hepatitis B Vaccine Birth Dose in Sierra Leone, 2018. Vaccine 2022, 40, 2741–2748. [Google Scholar] [CrossRef] [PubMed]
- Gosset, A. Introducing Birth-Dose Hepatitis B Vaccination Would Be Cost Effective in Burkina Faso. PharmacoEcon Outcomes News 2021, 883, 21–24. [Google Scholar] [CrossRef]
- Gosset, A.; Nishimwe, M.L.; Diallo, M.Y.; Deroo, L.; Diallo, A.; Ba, E.H.; Carrieri, P.M.; Sokhna, C.; Vray, M.; Shimakawa, Y.; et al. The Costs of Introducing the Hepatitis B Birth Dose Vaccine into the National Immunization Programme in Senegal (NéoVac Study). Vaccines (Basel) 2021, 9, 521. [Google Scholar] [CrossRef]
- Memirie, S.T.; Desalegn, H.; Naizgi, M.; Nigus, M.; Taddesse, L.; Tadesse, Y.; Tessema, F.; Zelalem, M.; Girma, T. Introduction of Birth Dose of Hepatitis B Virus Vaccine to the Immunization Program in Ethiopia: An Economic Evaluation. Cost Eff Resour Alloc 2020, 18, 23. [Google Scholar] [CrossRef] [PubMed]
- Klingler, C.; Thoumi, A.I.; Mrithinjayam, V.S. Cost-Effectiveness Analysis of an Additional Birth Dose of Hepatitis B Vaccine to Prevent Perinatal Transmission in a Medical Setting in Mozambique. Vaccine 2012, 31, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Reardon, J.M.; O’Connor, S.M.; Njau, J.D.; Lam, E.K.; Staton, C.A.; Cookson, S.T. Cost-Effectiveness of Birth-Dose Hepatitis B Vaccination among Refugee Populations in the African Region: A Series of Case Studies. Confl Health 2019, 13, 5. [Google Scholar] [CrossRef]
- Hagan, J.E.; Carvalho, E.; Souza, V.; Queresma Dos Anjos, M.; Abimbola, T.O.; Pallas, S.W.; Tevi Benissan, M.C.; Shendale, S.; Hennessey, K.; Patel, M.K. Selective Hepatitis B Birth-Dose Vaccination in São Tomé and Príncipe: A Program Assessment and Cost-Effectiveness Study. Am J Trop Med Hyg 2019, 101, 891–898. [Google Scholar] [CrossRef]
- Moturi, E.; Tevi-Benissan, C.; Hagan, J.E.; Shendale, S.; Mayenga, D.; Murokora, D.; Patel, M.; Hennessey, K.; Mihigo, R. Implementing a Birth Dose of Hepatitis B Vaccine in Africa: Findings from Assessments in 5 Countries. J Immunol Sci 2018, Suppl, 31–40. [Google Scholar] [CrossRef]
- Okenwa, U.J.; Dairo, M.D.; Uba, B.; Ajumobi, O. Maternal Reasons for Non-Receipt of Valid Hepatitis B Birth Dose among Mother-Infant Pairs Attending Routine Immunization Clinics, South-East, Nigeria. Vaccine 2019, 37, 6894–6899. [Google Scholar] [CrossRef]
- Nankya-Mutyoba, J.N.; Surkan, P.J.; Makumbi, F.; Aizire, J.; Kirk, G.D.; Ocama, P.; Atuyambe, L.M. Hepatitis B Birth Dose Vaccination for Newborns in Uganda: A Qualitative Inquiry on Pregnant Women’s Perceptions, Barriers and Preferences. J Virus Erad 2021, 7, 100039. [Google Scholar] [CrossRef] [PubMed]
- Miyahara, R.; Jasseh, M.; Gomez, P.; Shimakawa, Y.; Greenwood, B.; Keita, K.; Ceesay, S.; D’Alessandro, U.; Roca, A. Barriers to Timely Administration of Birth Dose Vaccines in The Gambia, West Africa. Vaccine 2016, 34, 3335–3341. [Google Scholar] [CrossRef] [PubMed]
- Boisson, A.; Goel, V.; Yotebieng, M.; Parr, J.B.; Fried, B.; Thompson, P. Implementation Approaches for Introducing and Overcoming Barriers to Hepatitis B Birth-Dose Vaccine in Sub-Saharan Africa. Glob Health Sci Pract 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Périères, L.; Marcellin, F.; Lo, G.; Protopopescu, C.; Ba, E.H.; Coste, M.; Kane, C.T.; Maradan, G.; Diallo, A.; Sokhna, C.; et al. Hepatitis B Vaccination in Senegalese Children: Coverage, Timeliness, and Sociodemographic Determinants of Non-Adherence to Immunisation Schedules (ANRS 12356 AmBASS Survey). Vaccines (Basel) 2021, 9, 510. [Google Scholar] [CrossRef] [PubMed]
- Olakunde, B.O.; Adeyinka, D.A.; Olakunde, O.A.; Ogundipe, T.; Oladunni, F.; Ezeanolue, E.E. The Coverage of Hepatitis B Birth Dose Vaccination in Nigeria: Does the Place of Delivery Matter? Trans R Soc Trop Med Hyg 2021, 116, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Allison, R.D.; Patel, M.K.; Tohme, R.A. Hepatitis B Vaccine Birth Dose Coverage Correlates Worldwide with Rates of Institutional Deliveries and Skilled Attendance at Birth. Vaccine 2017, 35, 4094–4098. [Google Scholar] [CrossRef]
- Schweitzer, A.; Akmatov, M.K.; Krause, G. Hepatitis B Vaccination Timing: Results from Demographic Health Surveys in 47 Countries. Bull World Health Organ 2017, 95, 199–209G. [Google Scholar] [CrossRef]
- Maponga, T.G.; Nwankwo, C.; Matthews, P.C. Sustainable Development Goals for HBV Elimination in South Africa: Challenges, Progress, and the Road Ahead. South African Gastroenterol Rev 2019, 17, 15–25. [Google Scholar]
- Immunization Vaccines and Biologicals Practices to Improve Coverage of the Hepatitis B Birth Dose Vaccine; World Health Organization: Geneva, 2017.
- Cheung, C.K. Proportion of Children Born to Infected Mothers at Risk of Contracting Hepatitis B, and Associated Risk Factors for Inadequate Hepatitis B Timely Birth Dose Vaccination: Analysis of the São Tomé and Príncipe Demographic Health Survey Program Data, 2008–2009, Uppsala Universitet, 2017.
- Kruk, M.; Freedman, L.P. Assessing Health System Performance in Developing Countries: A Review of the Literature. Health Policy (New York) 2008, 85, 263–276. [Google Scholar] [CrossRef]
- Samb, B.; Evans, T.; Dybul, M.; Atun, R.; Moatti, J.P.; Nishtar, S.; Wright, A.; Celletti, F.; Hsu, J.; Kim, J.Y.; et al. An Assessment of Interactions between Global Health Initiatives and Country Health Systems. The Lancet 2009, 373, 2137–2169. [Google Scholar] [CrossRef]
- World Health Organization Everybody’s Business: Strengthening Health Systems to Improve Health Outcomes: WHO’s Framework for Action; World Health Organization: Geneva. 2007.
- Arah, O.A.; Klazinga, N.S.; Delnoij, D.M.J.; Ten Asbroek, A.H.A.; Custers, T. Conceptual Frameworks for Health Systems Performance: A Quest for Effectiveness, Quality, and Improvement. Int J Qual Health Care 2003, 15, 377–398. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Frenk, A.J. A Framework for Assessing the Performance of Health Systems. Bull World Health Organ 2000, 78, 717–731. [Google Scholar] [PubMed]
- Van Olmen, J.; Criel, B.; Bhojani, U.; Marchal, B.; Van Belle, S.; Chenge, F.; Hoeree, T.; Pirard, M.; Van Damme, W.; Kegels, G. The Health System Dynamics Framework: The Introduction of an Analytical Model for Health System Analysis and Its Application to Two Case-Studies. Health Culture and Society 2012, 2, 1–21. [Google Scholar] [CrossRef]
- Amponsah-Dacosta, E.; Amponsah-Dacosta, E.; Kagina, B.M.; Olivier, J. Health Systems Constraints and Facilitators of Human Papillomavirus Immunization Programmes in Sub-Saharan Africa: A Systematic Review. Health Policy Plan 2020, 35, 701–717. [Google Scholar] [CrossRef]
- Shen, A.K.; Fields, R.; McQuestion, M. The Future of Routine Immunization in the Developing World: Challenges and Opportunities. Glob Health Sci Pract 2014, 2, 381–394. [Google Scholar] [CrossRef] [PubMed]
- Rohwer, A.; Pfadenhauer, L.; Burns, J.; Brereton, L.; Gerhardus, A.; Booth, A.; Oortwijn, W.; Rehfuess, E. Series: Clinical Epidemiology in South Africa. Paper 3: Logic Models Help Make Sense of Complexity in Systematic Reviews and Health Technology Assessments. J Clin Epidemiol 2017, 83, 37–47. [Google Scholar] [CrossRef]
Figure 2.
Summary of strategies for the prevention of HBV MTCT [2,4,5,22.]
Figure 3.
Progress in adoption and coverage of hepatitis B birth-dose vaccination in WHO Africa member states [21,30,62].
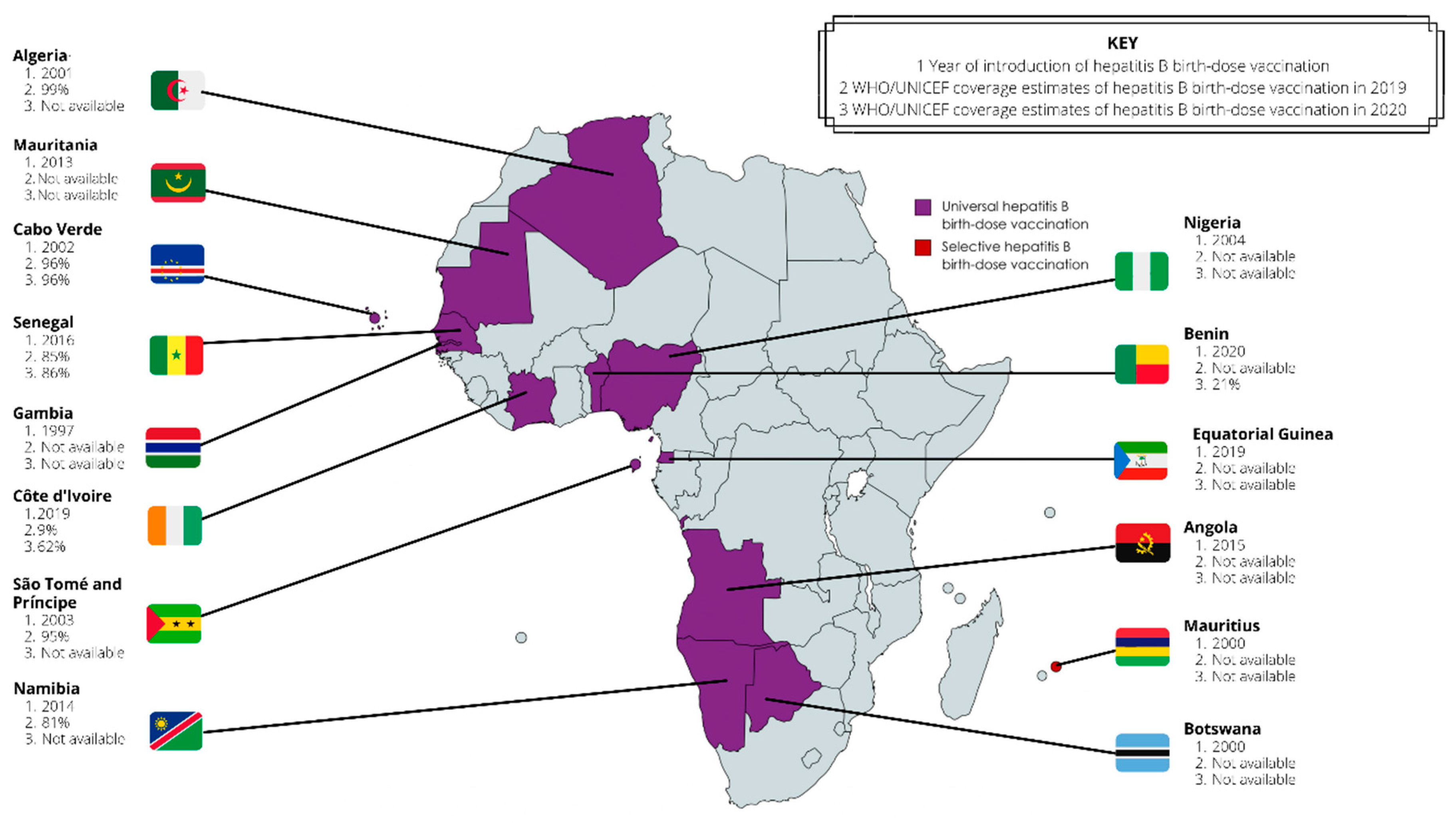
Figure 4.
Coverage of hepatitis B birth-dose vaccination in the WHO Africa region between 2000–2021 based on (A) WHO/UNICEF estimates vs (B) Official country estimates reported to WHO/UNICEF via the joint reporting form [21,62].
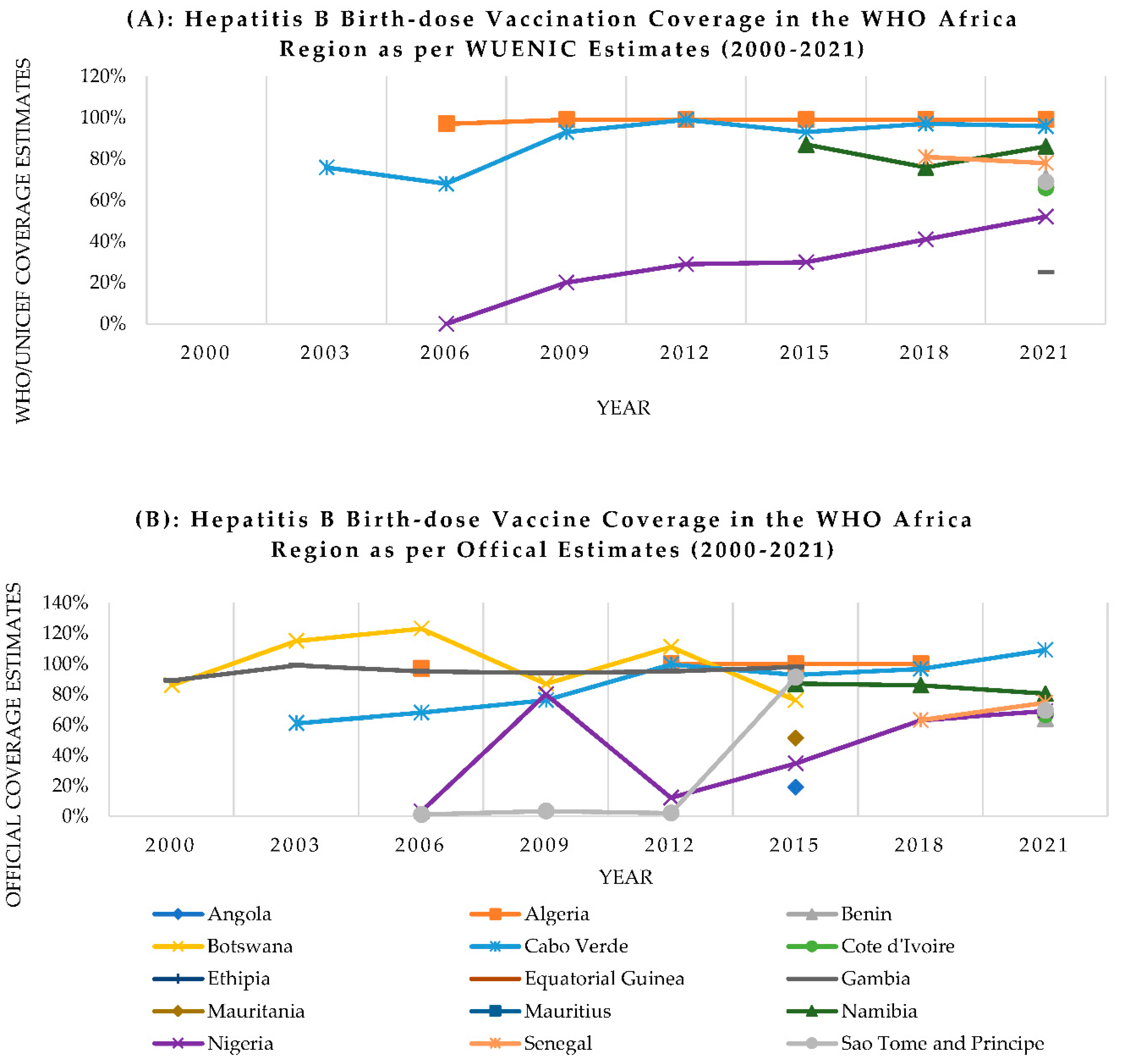
Figure 5.
Systems-based logic model for understanding complexity of hepatitis B birth-dose vaccination programs [94].
Figure 5.
Systems-based logic model for understanding complexity of hepatitis B birth-dose vaccination programs [94].
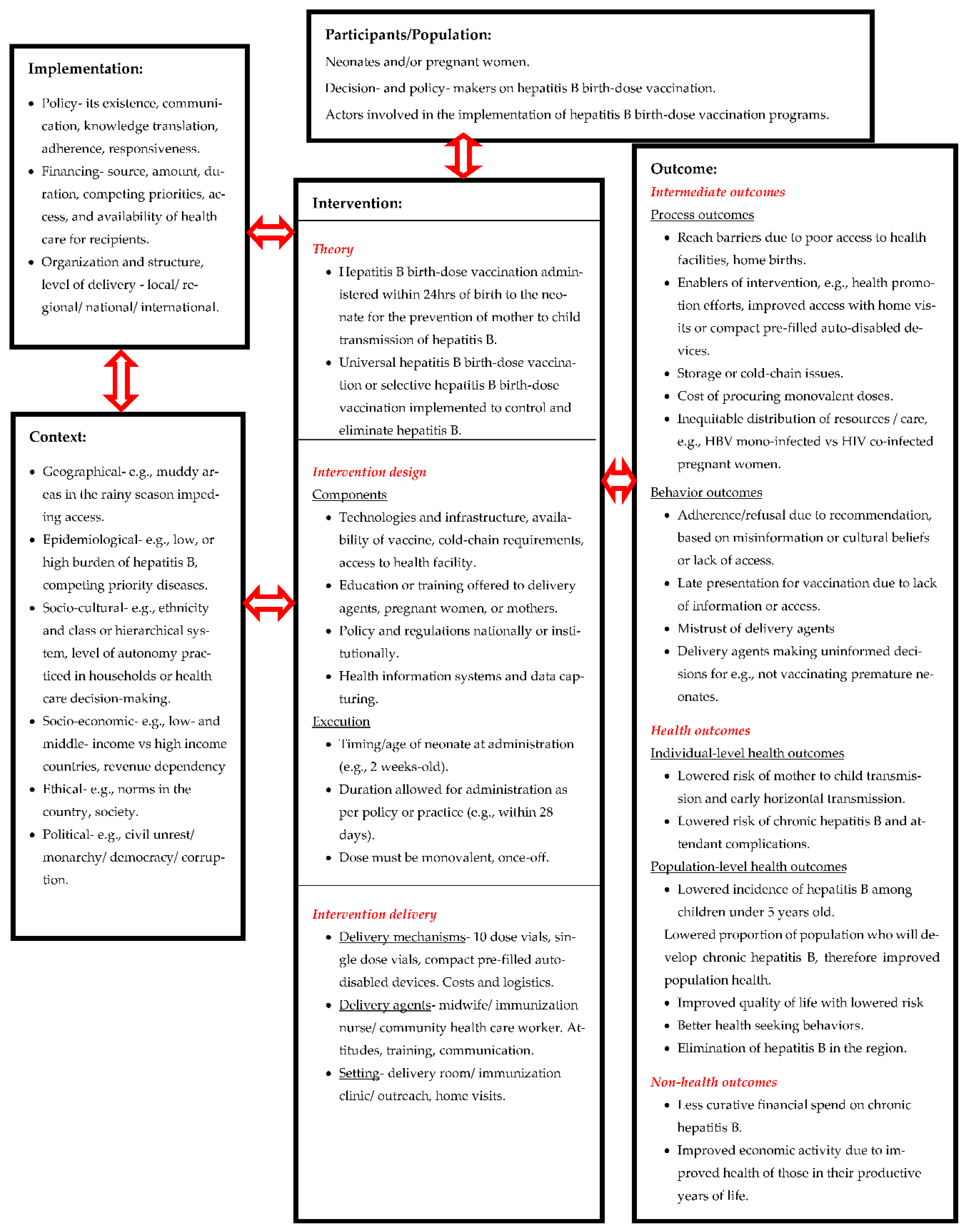
Table 1.
Growing evidence on the risk of HBV MTCT in the WHO Africa region.
| Study No. | Author, year | Setting | Study design | Population | Summary of key findings |
|---|---|---|---|---|---|
| 1 | Rashid et al., 2007 [12] | Tanzania | Cross-sectional | Pregnant women |
|
| 2 | Bayo et al., 2014 [10] | Uganda | Cross-sectional | Pregnant women |
|
| 3 | Howell et al., 2014 [5] | Sub-Saharan Africa | Literature Review | Pregnant women and women of childbearing age |
|
| Mother-child pairs |
|
||||
| 4 | Sadoh et al., 2014 [6] | Nigeria | Literature Review | Pregnant women and women of childbearing age |
|
| Mother-child pairs |
|
||||
| 5 | Umare et al., 2016 [9] | Ethiopia | Cross-sectional | Pregnant women |
|
| 6 | Breakwell et al., 2017 [2] | WHO AFRO | Literature review | Pregnant women |
|
| Mother-child pairs |
|
||||
| 7 | Chotun et al., 2017 [15] | South Africa | Prospective cohort | Pregnant women |
|
| Infants |
|
||||
| 8 | Kirbak et al., 2017 [11] | South Sudan | Cross-sectional | Pregnant women |
|
| 9 | Seremba et al., 2017 [49] | Uganda | Cross-sectional | Mothers |
|
| Infants |
|
||||
| 10 | Sone et al., 2017 [7] | Cameroon | Prospective cross-sectional | Pregnant women |
|
| Infants |
|
||||
| 11 | Bittaye et al., 2019 [8] | The Gambia | Cross-sectional | Pregnant women |
|
| 12 | Guingané et al., 2020 [13] | Burkina Faso | Prospective cohort | Pregnant women |
|
| Infants |
|
||||
| 13 | Thompson et al., 2021 [14] | Democratic Republic of Congo | Cohort | Pregnant women |
|
| Infants |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



