Submitted:
23 August 2023
Posted:
24 August 2023
You are already at the latest version
Abstract
FLASH-RT represents a novel therapeutic radiation modality that holds remarkable potential for mitigating radiation therapy’s adverse side effects. This cutting-edge technology allows for the sparing of healthy tissue while precisely targeting cancerous cells by administering an ultra-high dose-rates of typically between 10 and 30 Gy in less than a few hundred milliseconds. FLASH-RT has demonstrated impressive results in small-animal models, prompting scientists to adapt and advance existing technologies to make it a viable treatment option for humans. However, producing the ultra-high-dose-rate radiation required for the therapy remains a significant challenge. Several radiation sources, such as very high energy electrons (VHEEs), low energy electrons, x-rays, and protons, have been studied for their ability to deliver the necessary dose. Among them, FLASH-x-ray has gained the most attention owing to its capacity to penetrate deeply seated tumours. Despite the complexity of the process, the potential advantages of FLASH-RT make it an exciting area of research. To achieve the FLASH effect, high-frequency, pulsed irradiated accelerator technology can be employed. Sparing healthy tissue, it may allow for more aggressive and effective cancer treatments, leading to a better quality of life for patients. Ongoing research and development will be necessary to refine and optimize this approach to radiation therapy.
Keywords:
CONV-RT
; FLASH-RT
; ultra-high-dose-rate
; beam characteristics
; pulsed beams
; normal tissue sparing
1. Background
In recent decades, the discipline of radiation therapy (RT) for the treatment of cancer has experienced a substantial impact from technological innovation [1-5]. External Beam Radiation Therapy (EBRT), one of the current treatment options, is among the most effective when paired with immunotherapy, chemotherapy, and surgery [6-8]. Tumour volume, field sizes, and the depth of the tumour within the target organ are just a few of the variables that significantly impact the use of radiation treatment [9,10]. Despite being the most widely used and successful anti-tumour therapy, EBRT can cause both immediate and delayed tissue loss, specifically to neighbouring normal tissues. This issue even becomes more worrying when vital organs (e.g., the lungs and heart) are exposed to radiation [11]. According to clinical data, the patient undergoing conventional external beam Radiation Therapy (CONV-RT), typically receives 2 Gy fractions each day for five days a week during several weeks, which will be limited because of the toxicity to nearby vital and healthy tissue [1,12]. The limited received dose may prevent a tumour from being completely eliminated and impair the efficiency of radiation [11]. To address this problem, a new technology of RT known as FLASH Radiation Therapy (FLASH-RT) as an emerging technique in RT gained much interest [2, 5-8]. In FLASH-RT, tumour and surrounding tissues receive an ultra-high-dose rate in a fraction of second [13-16]. With the new radiation therapy technology, it is now possible to spare normal tissue while still effectively treating malignant cells [14, 17-20]. In FLASH-RT, normal tissue sparing refers to the ability to deliver adequate radiation to the tumour cells while minimizing exposure to neighbouring non-tumour organs [1, 20]. The 1970s striking small-animal studies (e.g., mice, zebrafish (embryo), cat, rat) which have been conducted for the thorax, lung, breast, skin, bone metastases, and brain tissues demonstrated a significant toxicity reduction in FLASH-RT than CONV-RT [21-23]. Three decades later, different aspects of the FLASH effect have been studied by Vincent Favaudon and Marie Catherine Vozenin’s team [1, 24]. Indeed, since demonstrating unparalleled protection for normal tissues with FLASH-RT, a differential effect between tumour and normal tissue has been described in this modality, and these effects have been corroborated by Lausanne [25, 26], Orsay [24], Grenoble [27], and Stanford [28, 29]. Thus, because of a number of factors, including a shorter irradiation time, higher curative doses than CONV-RT, and a differential effect between normal tissue and tumour that will be justified by several main hypotheses, this promising strategy has garnered the interest of many researchers [14,18, 20]. The next section of this review study will go into great length on these hypotheses. The positive outcome of the first FLASH-RT clinical trial in 2019 suggests that FLASH-RT may be an effective treatment option for a number of cancer types in individuals [28]. However, more clinical studies are required to thoroughly assess the FLASH-RT's safety and efficiency in humans. An important topic of research is how to make the FLASH effect more widely available so that more people can take advantage of this promising treatment. Although several appropriate sources have already been created, more studies are required to improve their functionality and guarantee their safety for clinical application. Potential sources for implementing the FLASH effect and improving our understanding of this modality include very high energy electrons (VHEEs), low energy electrons [1,3,20,21,29-31], x-rays [32,33], and protons beams [1,21, 34-37]. Accelerator communities such as Electron-Linac (E-Linac) can produce the required dose rate for both types of FLASH-electrons [14,38]. The pulsed irradiation of the accelerators produces high-frequency microwaves for different intervals. The high-frequency mostly rectangular microwaves are dependent on the source operating at around 3GHz [11]. In the most recent investigations, it was discovered that the FLASH-RT effect is possible to be replicated with 1–10 pulses lasting 1.8–2 microseconds, an total duration of < 200 ms with a pulse dose rate exceeding 1.8*105 Gy.s-1 [1]. Low energy electrons are useful for FLASH-RT, but their penetration depth is limited, making them more suited to treating shallow-seated cancers, whereas VHEEs are better suited to treating deep-seated tumours [3,14]. FLASH-proton has recently most commonly used for preclinical studies and clinical trials because of the energy deposition of the particles in Bragg-Peak (BP) and the finite range advantage [14,34,35]. The costly infrastructure required to implement the FLASH effect using FLASH-proton technology necessitates further investigation in order to compete with other FLASH-sources in terms of preclinical and clinical trials, and beyond. Recent studies reveal that the FLASH effect has been reported for single and multiple pulses in a wide range of instantaneous dose rates (IDR), as well as for clinical continuous wave (CW) delivery [21]. To date, FLASH-RT literature has been demonstrated using electrons by Loo et. al. 2017 [29], Subiel et al. 2014, 2017 [3,20], Vozenin et al. 2018 [38], and Jorge et al. 2019 [39]. Also, the FLASH-proton modality was improved by Buonanno et al. 2019 [35], and Kim et al. 2021 [37]. While the scarcity of ultra-high-dose-rate x-ray sources also limits FLASH-x-ray therapy, it has the potential to overcome some of the limitations of CONV-RT. Specifically, the highly penetrating nature of x-rays allows for treating deep-seated tumours that may be difficult to reach with other forms of radiation therapy. One of the main challenges in implementing FLASH-x-ray is designing efficient and durable bremsstrahlung conversion targets that can withstand the high beam power of MeV electron sources. Bremsstrahlung radiation can be generated when high-energy electrons are slowed down or deflected by high-Z materials [14,32]. The given target, on the other hand, should have exceptional ductility and a high melting point for bremsstrahlung x-ray conversion to occur with the greatest efficiency [14]. Researchers are exploring new target materials and geometries to optimize the bremsstrahlung conversion efficiency and durability. In addition to bremsstrahlung radiation, synchrotrons, and radioisotopes are also being explored as alternative sources of FLASH-x-ray radiation [32]. Montay-Gruel and co-workers 2020, 2021 [32], Gao et. Al. 2020 [19], and the Esplen team 2019, 2021, and 2022 [14,33] investigated the possibility of implementing the FLASH-x-ray technology for clinical studies. these modalities must overcome significant hurdles before they can be translated into clinical trials. This paper provides an overview of the key physical irradiation parameters in FLASH-RT, beam characteristics, and challenges ahead that need to be addressed for clinical implementation.
2. What is FLASH-RT? Non-Exclusive Hypotheses to Explain FLASH Effect
The new technology of RT, which is dubbed FLASH-RT is a promising modality that can reduce the trauma to normal tissue around the tumour using very short radiotherapy time and ultra-high-dose-rate irradiation [1,40-42]. This allows for a wider therapeutic window in RT and reduces the toxicity to normal tissue. This innovative radiation therapy method has demonstrated considerable promise in preserving or even improving the efficiency of radiation therapy against malignant cells while lowering toxicity in normal tissue [42-45]. Growing research suggests that other beam characteristics, such as instantaneous dose rate (IDR), period of exposure, Dose Per Pulse, and field size, should be accurately regulated and monitored in FLASH-RT, and thus, the Mean Dose Rate is not the only physical parameter of interest [20, 46]. It is believed that the Mean Dose Rate threshold to observe the FLASH effect lies around 40 Gy.s-1 [1,41,45]. Furthermore, the FLASH-RT exposure period is fractions of a second as opposed to CONV-RT's exposure length of a few minutes [43-45]. The repetition rate, duration of exposure, and number and width of the pulses play an important role in FLASH-RT technology [46]. This effect was first described using a mouse model for skin therapy in the 1970s [21-23], and it was further explored and enhanced by Vincent Favaudon and Marie Catherine Vozenin [25] in 2014. Recent findings in small animal models or different organ systems, such as the lung [25], brain [47], digestive tract [48-50], and skin [38], validated the FLASH effect's reduced normal tissue toxicity. Larger animals, such as mini-pigs, cats, and dogs, have also shown healthy tissue sparing [38,51]. Due to FLASH-RT's ultra-high dose rate, the groundbreaking experiments found increased radio-resistance. Also, a transitory acute radiation-induced hypoxia has been reported during ultra-high dose rate irradiation due to oxygen consumption and rediffusion into the irradiated volume to boost radio-resistance [52,53]. A few non-exclusive hypotheses which have been put forward to justify the differential between healthy tissues and tumours in the FLASH effect, will be thoroughly covered in this review work. These hypotheses are: oxygen depletion/Reactive Oxygen Species (ROS), DNA damage, Labile Iron Pool (LIP) availability, and immune-mediated [2,12,52,54]. FLASH irradiation at ultra-high dose rates has two direct and the indirect impacts on tissues [12]. In the indirect method, the cytotoxic superoxide anion and its protonated form, the hydroxyl radical, are produced as a result of the water radiolysis reaction (interaction of hydrated electrons ( and hydrogen radicals () and the generation of reactive oxygen species (ROS)(i.e., the hydroxyl radical) (see equation 1-a,b) [7,12,55]. By attaching to DNA, the generated hydroxyl free radicals can damage it in a way that is simple to fix [7,12,52]. However, when these free radicals interact with molecular oxygen, a peroxyl radical is produced, leading to a DNA damage that is challenging to repair. The results clearly show that oxygen deprivation can limit DNA damage because of radiation. The increasing trend of production of ROS and free radicals in tumour cells is due to several items including mutations in the mitochondrial DNA, mutations in the genomic DNA, and an increase in the metabolism activity [7].
Both FLASH-RT and CONV-RT exhibit significant oxygen level variations in normal tissue as compared to malignant tissue in Figure 1 [52]. After irradiation, rapid and large changes in O2 concentration, which are responsible for challenging DNA damage, are seen in normal tissue from CONV-RT to FLASH-RT while such behaviour is not seen in tumour tissue. Also, FLASH-RT causes normal tissue to lose oxygen, sparing normal tissue in the process while maintaining tumour control. Numerous studies have been conducted to comprehend how oxygen functions in FLASH-RT as opposed to CONV-RT. According to Adrian et al. (2020) [56], there is no longer a difference between FLASH-RT and CONV-RT in normoxic and hypoxic environments between 5 and 10 Gy, however, above 15 Gy FLASH demonstrated a substantial difference in cell survival for prostate malignancies. The survival up to 25 Gy was assessed using colony formation assays. According to Khan et al. [57], the FLASH effect caused the hypoxic core to envelop a significant portion of the well-oxygenated cells. They employed carbogen breathing to give healthy mice exposed to FLASH radiation more oxygen in the brain, negating FLASH's protective properties in the process. Cooper and co-workers [52] used the alkaline comet assay to investigate the influence of oxygen, total dose, and dose rate on the FLASH effect vs.% tail DNA (. The assay's alkaline variant finds breaks at alkaline labile locations, which were roughly estimated as Tail DNA, as well as single and double strand breaks. Whole blood samples were exposed to 6 MeV electron radiation at varied oxygen tensions and dose rates. They discovered that raising irradiation dose rates to extremely high levels may have the protective effect of lessening DNA damage in healthy tissues. They claimed that using water material to study the oxygen depletion effect is not a realistic mechanism in the human body. Such studies have come under fire for being inappropriate for the comparison of FLASH and CONV exposures. Figure 2 proves that increasing the total dose between CONV-RT and FLASH-RT from 5 Gy to 40 Gy, causes a substantial difference in DNA damage for 21%O2. For irradiation with 5 Gy FLASH, the difference in Tail DNA (mean value) between FLASH and CONV was 2%; for irradiation with 10 Gy FLASH, it rose to 3%. At 20, 30, and 40 Gy, the discrepancy increased significantly, with variances of 8%, 18%, and 28%, respectively. Additionally, a difference in the percentage of tail DNA damage for samples exposed to radiation was found by increasing the dose rate between FLASH and CONV. The results of the investigation support the hypothesis that FLASH may result in transient localized hypoxia that may be undetectable above or below a specific oxygen threshold.
The inherent factors like yield of DNA damage and clustered DNA damage are likely implicated in the difference in reaction between healthy and tumour tissue in FLASH. Using yH2AX as a marker of DNA double-strand breaks (DSBs), which are usually caused by faulty replication forks, reactive oxygen species (ROS), ionizing radiation, and physical or mechanical stress [58], FLASH was demonstrated to generate less DSBs than CONV [59]. Strand breaks caused by nucleotide changes, single-strand breaks (SSBs), or double-strand breaks (DSBs) can result in chromosome breakage and, as a result, gene loss. FLASH irradiation caused fewer DNA damage and spared lung progenitor cells compared to CONV [60]. FLASH inhibited senescence in both normal lung fibroblasts and lung progenitor cells [12,60,61]. Ultra high FLASH dose rates may also result in an increase in clustered DNA damage [12,62]. Massive cytosolic DNA induction brought on by FLASH RT can start the cGAS-STING as a DNA Damage Response (DDR) pathway (see Figure 3) [63]. The DDR is a crucial physiological signaling pathway for DNA damage repair. The approach is essential for maintaining genomic integrity. The DDR pathway in breast, ovarian, prostate, and pancreatic cancer has already been researched [64,65]. This intricate mechanism controls how DNA replication, cell growth, and ultimately cell survival take place. By repairing DNA damage, the DDR process plays a critical role in preserving genomic stability and integrity. cGAS-STING is a subcategory of genetoxic stress caused by DNA damage in tissues. To promote senescence, cell death, or tissue injury like fibrosis, this pathway increases the production of interferons (IFNs) and other innate immune proteins [12,62]. Therefore, differential cGAS-STING pathway activity between normal and tumour cells [58] may contribute to the FLASH effect in terms of tumour management and protecting tissue from damage such as fibrosis [60]. It is noteworthy to mention that he majority of human cancers have mutations in DDR signaling pathway genes such as MSH1 and MSH2, BRCA1 and BRCA2, RAD51C and RAD51D, CHK1 and CHK2 [12,66-69], which are mismatch repair, double strand break (DSB) repair, homologous recombination, and DNA damage checkpoint genes, respectively.
Iron (Fe) is a necessary element that is vital to many different biological processes, including DNA synthesis, cell division, and DNA damage and repair [70-72]. These links have led to a strong association between iron and the development of cancer. Iron regulatory protein expression is frequently altered in cancer cells. As an illustration, cancer cells typically upregulate transferrin (which increases iron intake) and downregulate ferroportin (which decreases intracellular iron efflux) [61,72]. These modifications raise the labile iron pool (LIP), or steady-state level of intracellular redox active iron. The LIP typically contains approximately 2% intracellular iron, which primarily exists as ferrous iron (Fe2+). The presence of the LIP distinguishes cancer cells from healthy cells metabolically. Cancerous cells have 2 to 4 times more labile iron and higher levels of the iron efflux pump transferrin receptor ferroportin than healthy cells [62]. The increased availability of Fe2+ in cancer cells causes the formation of FLASH induced-organic hydroperoxide, which is promptly removed by healthy cells with lower labile iron levels [70,71].
Inflammatory and immunological reactions, which shed light on the function of intrinsic components in the body, are another way to produce the FLASH effect. The multifunctional cytokine Transforming Growth Factor Beta (TGF-) which is a member of a transforming growth factor would behave differently in CONV-RT and FLASH-RT. As a result of this tendency ROS and DNA damage have decreased. More research is needed to determine how the CONV-RT and FLASH-RT differ in terms of T cell activation and localization. When compared to CONV, FLASH has been shown to boost T-lymphocyte recruitment into the tumour for lung treatment in mice. Furthermore, FLASH RT has been shown to promote immune cell infiltration of T cells and myeloid cells into tumour regions [12,73,74].
3. The Beam Description in FLASH-RT to Approach Clinical Trial
3.1. High Frequency Pulsed Beams
Accelerators, which naturally generate pulsed beams, are one of the primary methods for implementing FLASH-RT. Based on the parameters of the pulses such as duration and energy value transported in a pulse (i.e., Mean Dose Rate, ) which are dependent on the electron source characteristics and accelerating device, accelerators produce high-frequency microwaves at predetermined intervals. Depending on the intended use of the radiation, the typical rectangular pulse lasts 3.3 to 20 milliseconds. The majority of Linacs have pulse durations of 3-5 seconds and repetition rates of 200-400Hz, whereas cyclotron-based proton beams are categorized as quasi-continuous due to their short pulse durations and repetition rates of a few nanoseconds [12,73,74]. Furthermore, a specific beam's Dose Per Pulse, Dose Rate, Mean Dose Rate, and Total Treatment Time are crucial in describing the beam's characteristics. The temporal beam properties of FLASH-RT and CONV-RT are contrasted in Table 1. The Mean Dose Rate (), which represents the dose per fraction, is equal to 0.1 Gy.s-1 for CONV-RT and about 100 Gy.s-1 for FLASH-RT. The Dose Rate in a pulse dubbed instantaneous dose rate (IDR, ) is defined as the ratio of the delivered dose in one pulse per the pulse duration. This is a crucial distinction because, in contrast to the Mean Dose Rate () of 40 Gy.s-1 currently employed for preclinical trials to induce the FLASH effect, IDR in CONV-RT can be comparable to or even greater [46]. The previously reported FLASH-RT results are further supported by the considerable differences in Total Treatment Time between CONV-RT and FLASH-RT.
The provided information in Figure 4 summarizes previous preclinical studies of the FLASH effect using electrons, protons, and x-rays. Numerous provided studies have proved the occurrence of the FLASH effect over a broad range of IDR for single and multiple pulses, as well as for clinical continuous wave (CW) delivery. The FLASH effect has been documented for electron radiation in a dose rate range of 106-107 for a single pulse lasting 10-6 s, and 109-1010 for a duration of 10-9-10-8 s. Likewise, proton irradiation has also exhibited the FLASH effect, with shoot-through beams from clinical CW or isochronous cyclotrons operating effectively between 101 and 104. The dose rates for FLASH-RT delivery of numerous pulses (3–50) can range from 105 to 107 [1, 20].
3.2. FLASH-electron
Attempts have grown to prepare a beam which is capable of achieving the requisite dose rates for the clinical trial in FLASH-RT. To date, FLASH-VHEEs, FLASH-low-energy electrons, FLASH-x-ray, and FLASH-proton have been exploited for preclinical trials to cure cancer patients [13]. In modern radiotherapy, medical linear accelerators that generate electrons of up to 25 MeV can be applied for FLASH-low energy electrons to treat tumours [3,19]. Radiation must, however, be able to reach deep into the tissue to produce a therapeutic dose because the majority of malignancies are found at a depth of more than 15 cm inside the body [11,76]. Thus, using beam FLASH-low energy electron is improbable since the benefits of this technique generally apply to skin cancers or tumours that are close to the body's surface. Thus, employing photon or proton beam-based FLASH-RT, or alternatively using VHEEs is a potential solution to deliver the necessary dose. These approaches could overcome the constraints of low-energy electron beam FLASH-RT and provide a more viable treatment option for deep-seated malignancies. According to research, a tumour depth of 30 cm requires roughly 200–250 MeV of energy, which can be supplied utilizing FLASH-VHEEs [3,19]. Hornsey and Bewley [77] were pioneers in FLASH-VHEEs in the 1970s. They discovered that FLASH-VHEEs creates local hypoxia in the gut and postulated which may result radiation resistance in tissues, which might be interpreted as protection in normal tissue. One existing electron accelerator facility that can be used to implement FLASH-VHEEs is the 5Hz FAST SRF Linac, installed at Fermilab. It generates beams with the energy of 50 and 300 MeV, enabling it to instantly deliver 106 Gy per second and up to 1000 Gy for each pulse. Cornell University's CBETA CW recirculating energy recovery linac generates a 150 MeV beam with scanning ability of 106 Gy.s-1 at 200cm/ms [20]. Di Martino and co-workers [78] believed that since most of the accelerators used for FLASH-electron are accelerators used in industry or are modified medical accelerators, they could not execute beam parameters in real-time monitoring and deliver a precise and reproducible outputs. VHEEs were identified by Subiel et al. [3] as a substitute method for FLASH-RT implementation due to their enhanced dosimetric characteristics. The spectral profile of the beam as it travels through the water and the dosimetric characteristics of the VHEEs have been investigated in relation to electron bunch duration using Monte Carlo code and then were complemented using the IBA CC04 ionization chamber. They discovered that ultrashort high-dose-per-pulse VHEE beams considerably trigger ion recombination in the sentient volumes of typical online detectors. As a result, IBA CC04 is an inappropriate for ultrashort pulsed VHEE beam dosimetry using standard correction factors, as proved by the use of an IBA CC04 chamber for both 20 and 165 MeV. Thus, dosimetry must be established with the proper detectors to enable online dose measurements and additional systematic research must be conducted. Focused VHEEs for radiotherapy were investigated by Kokurewicz et al. [79] at the CERN Linear Electron Accelerator for Research (CLEAR) beamline using S-band radiofrequency accelerator. The depth-dose profile in the water phantom for 158 and 201 MeV focused beam and several f-numbers (f-number is f/D, where D is the diameter of the electron beam and f is the focal length of the lens) showed on-axis dose augmentation from 5 to 6 cm depth, supporting the idea that concentrated dose from focused VHEE beams is transferred to a specific volume deep within tissue. The results show that radiotherapy can be made more effective by precisely directing focused radiation beams of various f values at tumours or hypoxic regions. The study confirms that the focusing method for VHEEs can be used for FLASH irradiation. The photons and protons beams have similar geometric effects. Recent studies have been demonstrated that a focused photon beam can be generated using bremsstrahlung radiation [13] (also see the next section). The MCNP Monte Carlo dose calculation was done using the ultra-high dose rate electron beams utilizing the electron-scattering device which was fabricated at the Dongnam Institute of Radiological and Medical Sciences to establish the scattering device’s geometry [80]. In addition, the off-axis and depth dose distributions have been measured and calculated using radio-chromic materials. These observations allowed it to be established that the electron beams average energy for traveling through the scattering device is 4.3 MeV. The off-axis dose distribution's symmetry and flatness were found to be 0.11% and 2.33%, respectively. At a Source to Surface Distance (SSD) range of 20–90 cm, the dose per pulse varied between 0.2 and 4 Gy/pulse; this quantity was also subject to variations due to the heater current and radiofrequency power of the electron gun. The radiation rate was 180 Gy.s-1 at an SSD of 30 cm and a repetition rate of 100 Hz, which was sufficient for the preclinical FLASH tests. Additionally, the VHEEs dose is distinguished from the current low-energy therapeutic electrons by a significant transverse penumbra and little scattering at tissue surfaces. Although VHEE accelerators are currently more expensive and larger than low-energy electron clinical accelerators, new technologies like X-band radio-frequency (RF) accelerators and laser-plasma wake-field accelerators have made it possible to access VHEEs sources as compact VHEEs [79].
3.3. FLASH-x-ray
The relative rarity of ultra-high-dose-rate x-ray sources restricts the application of FLASH-x-ray in clinical practice [4, 13]. However, it’s very penetrating nature, which can be used to treat deep-seated tumours, has attracted attention [4,13,25]. There are three main ways to produce high energy x-rays (HEX) for FLASH-RT: synchrotron radiation, bremsstrahlung radiation, and radioisotopes [13]. Using gun electrons to accelerate electrons up to GeV, synchrotron radiation was accidentally discovered in 1946. After that, the electrons are contained in a ring with a big diameter where they can move freely and produce electromagnetic light when a magnetic field is applied. Synchrotron FLASH-x-ray modalities-specific technologies include synchrotron broad-beam radiation and synchrotron micro-beam radiation [32,81]. In the 1960s, Zeman and co-workers [82] reported surprising outcomes from the application of microscale beams in therapy in Brookhaven National Laboratory (BNL). They discovered that whereas 1 mm thick beamlets killed cerebral tissue and caused a hole, mice with normal tissues did not get any detrimental effects from 25 micrometer beam deuteron irradiation (neither blood vessel destruction nor their normal brain tissue architecture are described). Due to its capacity to treat malignancies while sparing normal tissue, synchrotron micro-beam radiation therapy (MRT) has gained popularity since that discovery [20, 83]. On the other hand, mice's entire bodies had been exposed to synchrotron broad-beam radiation treatment (SBBR) and micro-beam radiation therapy (MRT) decades earlier in Australia without exhibiting any typical tissue-sparing effects. Designing a suitable and highly effective electron-to-photon (i.e., bremsstrahlung radiation) converter is one of the difficulties in deploying FLASH-x-ray for clinical studies [13,32]. The process of accelerating light-charged particles (electrons) up to MeV and then impinging on high Z metal targets like tantalum (Ta) is dubbed Bremsstrahlung radiation which generates x-rays and heat [32]. This x-ray source is extremely useful in FLASH-x-ray radiotherapy and diagnostic imaging technology. As a result of electron beam’s interactions with the target, heat may be produced that causes the target to melt. A larger melting point T materials like tungsten (Z = 74, T = 3422◦C) or tantalum (Z = 73, T = 3017◦C) can be so efficient in comparison with other materials. Contrarily, gold is an inadequate target material for high dose rate x-ray generation due to its high Z = 79 but low T = 1064°C melting temperature. In conclusion, high Z-material converters must be used to maximize the effectiveness of bremsstrahlung x-ray conversion, and the best materials have high melting points and excellent ductility [13,32]. For this purpose, Esplen et. al. used a 2D-Gaussian monoenergetic electron source with a range of 300 keV to 10 MeV for the Advanced Rare Isotope Laboratory (ARIEL) e-linac which is located in TRIUMF. The target converter in FLASH-x-ray from the aforementioned study's computer-aided design (CAD) model is shown in Figure 5. The target thickness (t), electron beam size (2σ), and electron energy (E) are taken into consideration as being as follows: t = 500-1500 μm, 2σ = 2-10 mm, E = 8, 10 MeV and the effect of these parameters has been researched. Using the simplified model of the electron beam, the resultant dose was computed utilizing BEAMnrc Monte Carlo simulation code. The produced phase space data using BEAMnrc Monte Carlo code was applied to execute depth-dose simulations in water phantom type utilizing DOSXYZnrc code. In a case of the source-to-surface distance (SSD) of 7.5 cm, the absorbed dose was calculated in voxels with the volume of 0.2 mm3. Additionally, the reported dose rate at the phantom surface is up to 128 Gy. s-1 while this value at 1 cm depth is 85 Gy. s-1. The calculations were done for at 1 × 1 cm2 field size, a 1 mm thick Tantalum target, and a 7.5 cm SSD. Ta's strong temperature resistance and tolerance to radiation damage presented persuasive evidence for employing Ta as the target [13]. Gao et al. [18] generated HEX-FLASH by the PARTER (platform for advanced radiotherapy research) built on CTFEL (Chengdu THz Free Electron Laser facility) using the tungsten target. The applied linac in their study produces produce electrons with the energy range of 6 to 8 MeV and adjustable mean current of up to 10mA. To measure the dose received by each mouse, radiochromic (EBT3) film have been placed among the mice and the PMMA holder. To monitor the dose received by the mice, a CeBr3 scintillator type detector was installed downstream of the mice. The GEANT Monte Carlo code was used to run the simulation. The fast current transformer (FCT) devices accurately measured the electron beam's parameters, which were then fed into the GEANT Monte Carlo code. Three batches of the tumor-bearing mice were created: control group, FLASH group, and CONV group. Then, three separate experiments were conducted for whole-thorax irradiation and whole-abdomen irradiation. The mean tumor volume and the survival in tumor bearing mice were assessed in each group. Outcomes showed that in the thorax-irradiated healthy mice experiment a significant difference in survival among three group and the risks of death decreased 81% in FLASH group in comparison with CONV group. The reduction in risks of death in whole-abdomen irradiation was about 62% in FLASH group. A blue-staining areas were found in all three groups for whole-abdomen irradiation. The blue-staining area in control group was thin while for CONV group was thick. This area for FLASH was between control and CONV group. The blue-stained area demonstrated that the inflammatory response following radiation resulted in collagen fiber regeneration.
Third method to produce HEX is High-activity radioisotopes which have been taken into account for ultra-high dose-rate radiation. These include 60Co sources for both teletherapy and brachytherapy, as well as 192Ir seeds for brachytherapy. The discovery that the 60Co teletherapy source is only useful for treating superficial tumours makes it conceivable to use it for skin treatments. The difference in half-lives between 192Ir and 60Co, which are respectively 7.3 years and 74 days, is not significant for FLASH due to the short irradiation time (and can only be discussed in terms of unwanted radiation aspects), and the two sources can still generate extremely high dose rates that can be used to implement the FLASH effect. However, the employment of 60Co was restricted due to the development of more intricate shielding materials to attenuate the 60Co sources because of the difference average energy of 60Co, which is roughly 1.25 MeV, compared to 0.355 MeV for 192Ir sources [32].
3.4. FLASH-proton
One possible option to translate FLASH technology into clinical trials is the FLASH-proton strategy. The first clinical trial for an animal model in FLASH-proton was carried out by A. Patriarca et al. [16] and M. Buonanno et al. [35]. In the case of FLASH-proton, one of the main challenges is the limited availability of irradiators that can produce ultra-high-dose rates needed for FLASH-proton and the generated mean dose is far too low to elicit the FLASH [13]. While the costly infrastructure of FLASH-proton is the primary ongoing challenge for implementing the FLASH-proton, the energy deposition of proton in Bragg-Peak (BP) and using for deep-seated tumours made this method so interesting to investigate [79]. The finite range of protons, and consequently elimination the exit dose, which causes low-dose radiation bath and consequently minimizing the second cancer risk is the effectiveness of the FLASH-proton [84]. However, some biological uncertainties in proton therapy are disadvantage of this technology and future study in proton will be investigation of DNA damage in proton therapy [85]. The zebrafish embryo proton irradiation has been carried out by E. Beyreuther et al. [34] at the University of Proton Therapy Dresden (UPTD). The Cyclone 230 cyclotron, situated at the UPTD, is capable of generating a FLASH-like proton beam suitable for pre-clinical trials. In this study, the implementation of the FLASH proton beam was successful for a specific sample, and the results obtained were superior to those achieved with CONV-RT, albeit for a single dose point only. The experimental setup consists of a beam monitor-chamber (BM-IC) and a Bragg peak chamber (BP-IC) as secondary dosimeters and two scatterers located at Pos.1 and Pos.2. The scatterers in Pos.1 attenuated the proton fluence to achieve the desired dose for CONV-RT, while scatterers in Pos.2 enabled the delivery of the proton dose rate for FLASH-proton. Furthermore, EBT3 film was employed in front of the Markus ionization chamber (M-IC) or zebrafish embryos to evaluate beam divergence, emittance, and spot size. It is worth mentioning that researchers and scientists are currently exploring new beam technologies for FLASH-proton, including the use of proton pencil beam scanning techniques. While this technique precludes the use of radiation for full-volume irradiation, it permits the attainment of 3-D conformity. However, due to the beam size, the predicted irradiation time is longer than that for conventional FLASH-proton therapy. This is due to the step-and-shoot scanning technique employed for lateral and in-depth scanning using pencil beam scanning.
4. Future of FLASH-RT
At a key juncture in medical history, when cancer treatment has become a serious concern in the world, the research and efforts of FLASH radiation professionals can aid in the general use of this technique. To do this, the challenges ahead must be identified, and appropriate solutions to overcome these hurdles must be supplied. As noted in this and other colleagues' works, the identification of a suitable source capable of producing such a high dose to execute the FLASH effect is being researched. Several sources have been studied in medical centers for human samples and more extensively for animal samples, with encouraging findings. However, according to recent research of specialists in this sector, it appears that by removing the source-related constraints, this technology can make a significant jump in the field of medical sciences. We can look into high temperature plasma and UV laser sources for possible application in FLASH-x-rays for this purpose [86,87]. Also, because there haven't been many research on radioisotopes like 60Co and 192Ir, they could be a suitable alternative for large dose manufacturing. For example, the required activity does the cobalt source need to produce such a large dose (It is understudy by our team)? To achieve such a high dose, a few iridium seeds, which are extensively used in brachytherapy, must be irradiated. Furthermore, the shape of the radiation field (square or rectangular, …) would be of great interest, which has not yet been examined (It is understudy by our team). Moreover, the equipment required to perform the FLASH effect has already been supplied for tiny animal samples and slightly bigger samples, but can this equipment create an adequate radiation field for human samples? In addition, recently several studies found that the efficacy of treatment with CONV-RT and FLASH-RT can be so useful for patients. The effect of fractionated FLASH-RT on tumor is still in early stage [1].
5. Conclusions
FLASH-RT is a revolutionary technology that is still in its early stages of development. Many research offered evidence to support the success of the FLASH-RT method, which is encouraging. The researchers discovered that the FLASH effect requires a dose rate of 40 Gy.s-1 and an exposure time of a fraction of a second. Studies suggest that this technique significantly enhances the difference between normal and tumours, which may be explained by the following hypotheses: oxygen depletion/Reactive Oxygen Species (ROS), DNA damage, Labile Iron Pool (LIP) availability, and immune-mediated. One challenge in implementing the FLASH effect is producing an ultra-high-dose-rate beam, which is made possible by the development of high frequency pulsed accelerators. Numerous investigations have shown that the FLASH effect occurs throughout a wide range of IDR for one and multiple pulses, as well as for CW delivery. There are numerous obstacles to the broad application of this technology in patient treatment, which can only be overcome via the ongoing efforts of researchers in this field. Given the growing number of cancer patients throughout the world, the widespread use of this technology and the resolution of impending obstacles can lead to an increase in cancer patients' life expectancy.
References
- Bourhis J, Montay-Gruel P, Jorge P G, Bailat C, Petit B, Ollivier J, Jeanneret-Sozzi W, Ozsahin M, Bochud F, Moeckli R, Germond J F, Vozenin M C, 2019. Clinical translation of FLASH radiotherapy: Why and how? Journal of Radiotherapy and oncology. [CrossRef]
- Lin B, Gao F, Yang Y, Wu D, Zhang Y, Feng, G, Dai T, Du, X, 2021. FLASH Radiotherapy: History and Future, Journal of Frontiers in Oncology, 11, 644400. [CrossRef]
- SubielA, MoskvinV, WelshGH, Cipiccia S, Reboredo D, DesRosiers C, Jaroszynski D A, 2017. Challenges of dosimetry of ultra-short pulsed very high energy electron beams. Journal of Physica Medica, . [CrossRef]
- Poirier Y, Mossahebi S, Becker S, Koger B, Xu J, Lamichhane N, Maxim P G, Sawant A, 2021, Radiation shielding and safety implications following linac conversion to an electron FLASH-RT unit. Journal of Medical Physics, 48, 5396-5405. [CrossRef]
- Fielding, A L, 2023. Monte-Carlo techniques for radiotherapy applications II: equipment and source modelling, dose calculations and radiobiology, Journal of Radiotherapy in Practice. 22, 1–6. [CrossRef]
- Zhang G, Zhang Zh, Gao W, Quan H, 2023. Treatment planning consideration for very high-energy electron FLASH radiotherapy, Journal of Physica Medica, 107, 102539.
- Boscolo D, Scifoni E, Durantea M, Kramer M, Fuss M C,2021. May oxygen depletion explain the FLASH effect? A chemical track structure analysis, Journal of Radiotherapy and Oncology. [CrossRef]
- Rothwell B C, Lowe M, Kirkby N F, Merchant M J, Chadwick A L, Mackay R I, Hendry J H, Kirkby K J, 2021. Oxygen Depletion in Proton Spot Scanning: A Tool for Exploring the Conditions Needed for FLASH, Journal of Radiation, 290–304. [CrossRef]
- Khabaz R, Boodaghi R, Benam M R, Zanganeh V,2018. Estimation of photoneutron dosimetric characteristics in tissues/organs using an improved simple model of linac head, Journal of Applied Radiation and Isotopes, 133, 88-94. [CrossRef]
- Boodaghi Malidarre R, Khabaz R, Benam M R, Zanganeh V, 2020. A Feasibility Study to Reduce the Contamination of Photoneutrons and Photons in Organs/Tissues during Radiotherapy, Iranian Journal of Medical Physics, 17iation therapy, Reports of Practical Oncology and Radiotherapy, 27, 344–351.
- Matuszak N, Maria Suchorska W, Milecki P, Kruszyna-Mochalska M, Misiarz A, Pracz J, Malicki J, 2022. FLASH radiotherapy: an emerging approach in radiation therapy, Reports of Practical Oncology and Radiotherapy, 27, 344–351 DOI: . [CrossRef]
- Hageman E, Che P P, Dahele M, Slotman B J, Sminia P, 2022. Radiobiological Aspects of FLASH Radiotherapy, Journal of Biomolecules, 12, 1376. [CrossRef]
- Esplen N, Egoriti L, Paley B, Planche T, Hoehr C, Gottberg A, Bazalova-Carter M, 2022. Design optimization of an electron-to-photon conversion target for ultra-high dose rate x-ray (FLASH) experiments at TRIUMF, Journal of Physics in Medicine and Biology, 105003.
- Giuliano L, Franciosini G, Palumbo L, Aggar L, Dutreix M, Faillace L, Favaudon V, Felici G, Galante F, Mostacci A, Migliorati M, Pacitti M, Patriarca A, Heinrich S, 2023. Characterization of Ultra-High-Dose Rate Electron Beams with ElectronFlash Linac, Journal of Applied Sciences, 13, 631. [CrossRef]
- Borghini A, Vecoli C, Labate L, Panetta D, Andreassi MG, Gizzi LA, 2022. FLASH ultra-high dose rates in radiotherapy: preclinical and radiobiological evidence. Journal of Radiation Biology, 98,127-135. [CrossRef]
- Patriarca A, Fouillade C, Auger M, Martin F, Pouzoulet F, Nauraye C, Heinrich S, Favaudon V, Meyroneinc S, Dendale R, Mazal A, Poortmans P, Verrelle P, De Marzi L, 2018. Experimental set-up for FLASH proton irradiation of small animals using a clinical system, International Journal Radiation Oncology Biology, Physics, 102, 619-626.
- Bohlen T T, Germond J F, Bourhis J, Vozenin M C, Ozsahin E M, Bochud F, Bailat C, Raphael Moeckli R, 2022. Normal Tissue Sparing by FLASH as a Function of Single-Fraction Dose: A Quantitative Analysis, Journal of Radiation Oncology, Biology, Physics, 114, 1032-104.
- Gao F, Yang Y, Zhu H, Wang J, Xiao D, Zhou Z, Dai T, Zhang Y, Feng G, Li J, Lin B, Xie G, Ke Q, Zhou K, Li P, Shen X, Wang H, Yan L, Lao C, Shan L, Li M, Lu Y, Chen M, Feng S, Zhao J, Wu D, Du X. 2022. First demonstration of the FLASH effect with ultrahigh dose rate high-energy X-rays. Journal of Radiotherapy and Oncology, 166, 44-50. [CrossRef]
- Subiel A, Moskvin V, Welsh G H, Cipiccia S, Reboredo D, Evans P, Partridge M, DesRosiers C, Anania M P, Cianchi A, Mostacci A, Chiadroni E, Di Giovenale D, Villa F, Pompili R, Ferrario M, Belleveglia M, Di Pirro G, Gatti G, Vaccarezza C, Seitz B, C Isaac R, Brunetti E, Wiggins S M, Ersfeld B, Islam M R, Mendonca M S, Sorensen A, Boyd M, Jaroszynsk D A, 2014. Dosimetry of very high energy electrons (VHEE) for radiotherapy applications: using radiochromic film measurements and Monte Carlo simulations, Journal of Physics in Medicine and Biology, 59, 5811.
- Schulte R, Johnstone C, Boucher S, Esarey E, Geddes C G R, Kravchenko M, Kutsaev S, Loo Jr , Méot F, Mustapha B, Nakamura K, Nanni E A, Obst-Huebl L, Sampayan S E, Schroeder C B, Sheng K, Snijders A M, Snively E, Tantawi S G, Tilborg J V, 2022. Transformative Technology for FLASH Radiation Therapy: Journal of Applied Sciences,12, x. [CrossRef]
- Hornsey S, Alper T. 1966, Unexpected dose-rate effect in the killing of mice by radiation, Nature, 210:212–3. [CrossRef]
- Field SB, Bewley DK. 1974, Effects of dose-rate on the radiation response of rat skin. International journal of radiation biology and related studies in physics, chemistry, and medicine, 26, 259–67. [CrossRef]
- Hendry JH, Moore JV, Hodgson BW, Keene JP. 1982, The constant low oxygen concentration in all the target cells for mouse tail radionecrosis. Journal of Radiation Research, 92,172–81.
- Favaudon V,Caplier L, Monceau V, Oulet F P, Sayarath M,Fouillade C, Poupon M F, Brito I, Hupe P, Bourhis J, Hall J, Fontaine J J, Vozenin M C, 2014. Ultrahigh dose-rate FLASH irradiation increases the differential response between normal and tumor tissue in mice, Journal Science Translational Medicine, 6, 245.
- Montay-Gruel P, Petersson K, Jaccard M, Boivin G, Germond JF, Petit B, Doenlen R, Favaudon V, Bochud F, Bailat C, Bourhis J, Vozenin MC. 2017. Irradiation in a flash: Unique sparing of memory in mice after whole brain irradiation with dose rates above 100 Gy/s. Journal of Radiotherapy and Oncology 124:365–9. [CrossRef]
- Vozenin MC, De Fornel P, Petersson K, Favaudon V, Jaccard M, Germond JF, Petit B, Burki M, Ferrand G, Patin D, Bouchaab H, Ozsahin M, Bochud F, Bailat C, Devauchelle P, Bourhis J, 2018. The advantage of Flash radiotherapy confirmed in mini-pig and catcancer patients. Journal of Clinical Cancer Research. . CCR-17-3375. In press: clincanres.3375.2017. [CrossRef]
- Montay-Gruel P, Bouchet A, Jaccard M, Patin D, Serduc R, Aim W, Petersson K, Petit B, Bailat C, Bourhis J, Bräuer-Krisch E, Vozenin MC. 2018. X-rays can trigger the FLASH effect: ultra-high dose-rate synchrotron light source prevents normal brain injury after whole brain irradiation in mice. Journal of Radiotherapy and Oncology, 129:582–8. [CrossRef]
- Bourhis J, Sozzi W J , Jorge P G , Gaide O , Bailat C, Duclos F, Patin D, Ozsahin M, Bochud F, Germond J F , Moeckli R , Vozenin M C, 2019. Treatment of a first patient with FLASH-radiotherapy, Journal of Radiotherapy and Oncology, 139:18-22. [CrossRef]
- Loo B W, Schuler E, Lartey F M, Rafat M, King G J, Trovati S, Koong A C, and Maxim P, (P003) 2017. delivery of ultra-rapid flash radiation therapy and demonstration of normal tissue sparing after abdominal irradiation of mice. International Journal of Raditherapy and Oncology, 98, E16. [CrossRef]
- Jaccard M, Durán M T, Petersson K, Germond J F, Liger P, Vozenin M C, Bourhis J, Bochud F and Bailat C, 2018 High dose-per-pulse electron beam dosimetry: Commissioning of the Oriatron eRT6 prototype linear accelerator for preclinical use, Journal of Medical Physics 45 863–7.
- Lempart M, Blad B, Adrian G, Back S, Knoos T, Ceberg C and Petersson K, 2019. Modifying a clinical linear accelerator for delivery of ultrahigh dose rate irradiation, Journal of Radiotherapy and Oncology, 139 40–.
- Montay-Gruel P, Corde S, Laissue J A, Bazalova-Carter M, 2022. FLASH radiotherapy with photon beams, Journal of Medical Physics, 49, 2055-2067. [CrossRef]
- Bazalova-Carter M, Esplen N, 2019. On the capabilities of conventional x-ray tubes to deliver ultra-high (FLASH) dose rates, Journal of Medical Physics, 46, 5690–5.
- Beyreuther E, Brand M, Hans S, Hideghety K, Karsch L, Leßmann E, Schurer M, Szabo E R, Pawelke J, 2019. Feasibility of proton FLASH effect tested by zebrafish embryo irradiation Journal of Radiotherapy and Oncology, 139 46–50.
- Buonanno M, Grilj V and Brenner D J, 2019. Biological effects in normal cells exposed to FLASH dose rate protons, Journal of Radiotherapy and Oncology, 139 51–5.
- Darafsheh A, Hao Y, Zwart T, Wagner M, Catanzano D, Williamson J F, Knutson N, Sun B, Mutic S and Zhao T, 2020. Feasibility of proton FLASH irradiation using a synchrocyclotron for preclinical studies, Journal of Medical Physics, 47 4348–55.
- Kim MM, Verginadis II, Goia D, Haertter A, Shoniyozov K, Zou W, Maity A, Busch TM, Metz JM, Cengel KA, Dong L, Koumenis C, Diffenderfer ES. 2021. Comparison of FLASH Proton Entrance and the Spread-Out Bragg Peak Dose Regions in the Sparing of Mouse Intestinal Crypts and in a Pancreatic Tumor Model. Journal of Cancers 23, 4244. [CrossRef]
- Vozenin MC, De Fornel P, Petersson K, Favaudon V, Jaccard M, Germond JF, Petit B, Burki M, Ferrand G, Patin D, Bouchaab H, Ozsahin M, Bochud F, Bailat C, Devauchelle P, Bourhis J. 2019. The Advantage of FLASH Radiotherapy Confirmed in Mini-pig and Cat-cancer Patients. Journal of Clinical Cancer Research, 25,35-42. [CrossRef]
- Jorge PG, Jaccard M, Petersson K, Gondre M, Durán MT, Desorgher L, Germond JF, Liger P, Vozenin MC, Bourhis J, Bochud F, Moeckli R, Bailat C. 2019, Dosimetric and preparation procedures for irradiating biological models with pulsed electron beam at ultra-high dose-rate. Journal of Radiotherapy and Oncology, 139,34-39. [CrossRef]
- Schuler E, Trovati S, King G, Lartey F, Rafat M, Villegas M, Praxel A J, Billy W, Loo Jr, Maxim P G, 2017. Experimental platform for ultra-high dose rate flash irradiation of small animals using a clinical linear accelerator. Journal of Radiation Oncology and Biology Physics. 97, 195–203. [CrossRef]
- Levin D S, Ferretti C, Ristow N, Tecchio M, Friedman P S, Litzenberg D W, Bashkirov V, Schulte R, 2023. A Scintillator Beam Monitor for Real-Time FLASH Radiotherapy, arXiv preprint arXiv:2305.15306.
- Gao Y, Liu R, Wei C, Serdar C, Jun Z, Bradley J D, Liu T, Yang X, 2022. A potential revolution in cancer treatment: A topical review of FLASH radiotherapy, Journal Applied Clinical Medical Physics. 23,13790. [CrossRef]
- Vozenin M C, Hendry J H, Limoli C L, 2019. Biological benefits of ultra-high dose rate flash radiotherapy: sleeping beauty awoken, Journal of Clinical Oncology, 31 407–15.
- Yinghao LV, Yue LV, Wang Z, Lan T, Feng X, Chen H, Zhu J, Ma X, Du J, Hou G, Liao W,Yuan K, Wu H, 2022. FLASH radiotherapy: A promising new method for radiotherapy (Review), Journal of Oncology Letters, 24, 419. [CrossRef]
- Rezaee M, Iordachita I, Wong J W W, 2021. Ultra-high dose-rate (FLASH) x-ray irradiator for pre-clinical laboratory research, Journal of Physics in Medicine and Biology, 23, 66. [CrossRef]
- Ashraf M R, Rahman M, Zhang R, Williams B B, Gladstone D J, Pogue B W, Bruza P, 2020. Dosimetry for FLASH Radiotherapy: A Review of Tools and the Role of Radioluminescence and Cherenkov Emission, Frontiers in Physics, 8. [CrossRef]
- Zhu H, Xie D, Yang Y, Huang S, Gao X, Peng Y, Wang B, Wang J, Xiao D, Wu D, Li C, Qian C N, Deng X, 2022. Radioprotective effect of X-ray abdominal FLASH irradiation: Adaptation to oxidative damage and inflammatory response may be benefiting factors, Journal of Medical Physics, 49, 4812–4822.
- Zhang Q, Cascio E, Li C, Yang Q, Gerweck L E, Huang P, Gottschalk B, Flanz J, Schuemann J, 2020. FLASH investigations using protons: design of delivery system, preclinical setup and confirmation of FLASH effect with protons in animal systems. Journal of Radiation Research, 194, 656-664.
- Diffenderfer ES, Verginadis II, Kim MM, Shoniyozov K, Velalopoulou A, Goia D, Putt M, Hagan S, Avery S, Teo K, Zou W, Lin A, Swisher-McClure S, Koch C, Kennedy AR, Minn A, Maity A, Busch TM, Dong L, Koumenis C, Metz J, Cengel KA. 2020. Design, Implementation, and in Vivo Validation of a Novel Proton FLASH Radiation Therapy System. Journal of Radiation Oncology, Biology, Physics .106, 440-448. [CrossRef]
- Levy K, Natarajan S, Wang J, Chow S, T. Eggold J , E. Loo P, Manjappa R, Melemenidis S, M. Lartey F, Schuler E, Skinner L, Rafat M, Ko R, Kim A, H. Al-Rawi D, Eyben R V, Dorigo O, M. Casey K, E. Graves E, Bush K, S. Yu A, C. Koong A, G. Maxim P, W. Loo Jr. B, B. Rankin E, 2020. Abdominal FLASH irradiation reduces radiation-induced gastrointestinal toxicity for the treatment of ovarian cancer in mice. Journal of Scientific Report, 10, 21600.
- Bley C R , Wolf F , Goncalves Jorge P, Grilj V , Petridis I , Petit B , Bohlen T T , Moeckli R , Limoli C , Bourhis J , Meier V, Vozenin M C , 2022. Dose- and Volume-Limiting Late Toxicity of FLASH Radiotherapy in Cats with Squamous Cell Carcinoma of the Nasal Planum and in Mini Pigs. Journal of Clinical Research. 28, 3814-3823. [CrossRef]
- Cooper CR, Jones D, Jones G DD, Petersson K, 2022. FLASH irradiation induces lower levels of DNA damage ex vivo, an effect modulated by oxygen tension, dose, and dose rate, British Journal of Radiology, 95, 20211150.
- 53. Gao Y, Liu R, Chang C W, Charyyev S, Zhou J, Bradley J D, Liu T, Yang X, 2022, A potential revolution in cancer treatment: A topical review of FLASH radiotherapy, Journal of Medical Physics, 23,13790. [CrossRef]
- Lin B, Huang D, Gao F, Yang Y, Wu D, Zhang Y, Feng G, Dai T and Du X, 2022. Mechanisms of FLASH effect. Journal of Frontiers in Oncology, 12, 995612. [CrossRef]
- Pratx G, SKapp D, 2019. A computational model of radiolytic oxygen depletion during FLASH irradiation and its effect on the oxygen enhancement ratio, Journal of Physics in Medicine and Biology, 64, 185005.
- Adrian G, Konradsson E, Lempart M, Back S, Ceberg C, and Petersson K. 2020, The FLASH effect depends on oxygen concentration. British Journal of Radiology, 93, 20190702.
- Khan S, Bassenne M, Wang J, Manjappa R, Melemenidis S, Breitkreutz D Y, Maxim P G, Xing L, Loo B W, Pratx G, 2021. Multicellular Spheroids as In Vitro Models of Oxygen Depletion during FLASH Irradiation. Journal of Radiation Oncology, Biology, Physics, 110, 833–844.
- Arai H, Elliott A, Xiu J, Wang J, Battaglin F, Kawanishi N, Soni S, Zhang W, Millstein J, Sohal D, Goldberg R M, Hall M J, Scott A J, Khushman M, Hwang J J, Lou E , Weinberg B A , Marshall J L , Lockhart A C, Stafford P, Zhang J, Roberto Moretto R, Chiara Cremolini C, Michael Korn W, Lenz H J, 2021. The Landscape of Alterations in DNA Damage Response Pathways in Colorectal Cancer. Journal of Clinical Cancer Research, 27, 3234–3242.
- Buonanno M, Grilj V, Brenner D J, 2019. Biological Effects in Normal Cells Exposed to FLASH Dose Rate Protons. Journal of Radiotherapy and Oncology,139, 51–55.
- Fouillade C, Curras-Alonso S, Giuranno L, Quelennec E, Heinrich S, Bonnet-Boissinot S, Beddok A, Leboucher S, Karakurt HU, Bohec M, Baulande S, Vooijs M, Verrelle P, Dutreix M, Londono-Vallejo A, Favaudon V. 2020. FLASH Irradiation Spares Lung Progenitor Cells and Limits the Incidence of Radio-Induced Senescence. Journal of Clinical Cancer Research 26, 1497–1506.
- Spitz DR, Buettner GR, Limoli CL, 2019. Response to Letter Regarding “An Integrated Physico-Chemical Approach for Explaining the Differential Impact of FLASH versus Conventional Dose Rate Irradiation on Cancer and Normal Tissue Responses”. Journal of Radiotherapy and Oncology,139, 64–65.
- Zhou G, 2020. Mechanisms Underlying FLASH Radiotherapy, a Novel Way to Enlarge the Differential Responses to Ionizing Radiation between Normal and Tumor Tissues. Radiation Medicine and Protection, 1, 35-40.
- Li T, Chen Z J, 2018. The cGAS–cGAMP–STING pathway connects DNA damage to inflammation, senescence, and cancer, Journal of Experimental Medicine, 215, 1287–1299.
- Golan T, Hammel P, Reni M, Cutsem E V, Macarulla T, Hall M J, Park J O, Hochhauser D, Arnold D, Oh D Y, Reinacher-Schick A, Tortora G, Algul H, O’Reilly E M, McGuinness D, Cui K Y, Schlienger K, Y. Locker G, L. Kindler H, 2019. Maintenance Olaparib for Germline BRCA-Mutated Metastatic Pancreatic Cancer. The New England Journal of Medicine, 381, 317–327.
- Ray-Coquard I, Leary A, Pignata S, Cropet C, González-Martin A, Marth C, Nagao S, Vergote I, Colombo N, Maenpaa J, Selle F, Sehouli J, Lorusso D, Guerra Alia EM, Bogner G, Yoshida H, Lefeuvre-Plesse C, Buderath P, Mosconi AM, Lortholary A, Burges A, Medioni J, El-Balat A, Rodrigues M, Park-Simon TW, Dubot C, Denschlag D, You B, Pujade-Lauraine E, Harter P; PAOLA-1/ENGOT-ov25 investigators. Olaparib plus Bevacizumab as First-Line Maintenance in Ovarian Cancer. The New England Journal of Medicine, 381, 2416–2428.
- Wu S, Zhang Q, Zhang F, Meng F, Liu S, Zhou R, Wu Q, Li X, Shen L, Huang J, Qin J, Ouyang S, Xia Z, Song H, Feng X H, Zou J, Xu P, 2019. HER2 Recruits AKT1 to Disrupt STING Signalling and Suppress Antiviral Defence and Antitumour Immunity. Journal of Nature Cell Biology 21, 1027–104.
- Catalano F, Borea R, Puglisi S, Boutros A, Gandini A, Cremante M, Martelli V, Sciallero S, Puccini A, 2022. Targeting the DNA Damage Response Pathway as a Novel Therapeutic Strategy in Colorectal, Journal of Cancer, 14, 1388. [CrossRef]
- Mauri G, Arena S, Siena S , Bardelli A, Sartore-Bianchi A, 2020. The DNA damage response pathway as a land of therapeutic opportunities for colorectal cancer, Annals of Oncology, 31, 1135-1147.
- Lozano R, Castro E, Aragon I M, Cendon Y, Cattrini C, Lopez-Casas P P, Olmos D, 2021. Genetic aberrations in DNA repair pathways: a cornerstone of precision oncology in prostate cancer, British Journal of Cancer, 124, 552–563; [CrossRef]
- Michael S. Petronek, Douglas R. Spitz, Garry R. Buettner and Bryan G. Allen, 2019. Linking Cancer Metabolic Dysfunction and Genetic Instability through the Lens of Iron Metabolism, Journal of Cancers, 11, 1077. [CrossRef]
- Hinchliffe P, Sazanov L A, 2005. Organization of Iron-Sulfur Clusters in Respiratory Complex I. Journal of Science, 309, 771–774.
- Kruszewski M, 2003. Labile iron pool: the main determinant of cellular response to oxidative stress. Journal of Mutation Research, 53, 81-92. [CrossRef]
- Zhu H, Xie D, Wang Y, Huang R, Chen X, Yang Y, Wang B, Peng Y, Wang J, Xiao D, Wu D, Qian CN, Deng X. 2022. Comparison of intratumor and local immune response between MV X-ray FLASH and conventional radiotherapies. Journal of Clinical and Translation Radiation Oncology, 38, 138-146. [CrossRef]
- Zhang Z, Liu X, Chen D, and Yu J, 2022. Radiotherapy combined with immunotherapy: the dawn of cancer treatment, Signal Transduction and Targeted Therapy, 7, 258.
- Montay-Gruel P, Acharya M M, Gonçalves Jorge P, Petit B, Petridis IG, Fuchs P, Leavitt R, Petersson K, Gondre M, Ollivier J, Moeckli R, Bochud F, Bailat C, Bourhis J, Germond JF, Limoli CL, Vozenin MC, 2021. Hypofractionated FLASH-RT as an Effective Treatment against Glioblastoma That Re- 1190 duces Neurocognitive Side Effects in Mice. Clinical Cancer Research, 27, 775–784, 119. [CrossRef]
- Sarti A, De Maria P, Battistoni G, De Simoni M, Di Felice C, Dong Y, Fischetti M, Franciosini G, Marafini M, Marampon F, Mattei I, Mirabelli R, Muraro S, Pacilio M, Palumbo L, Rocca L, Rubeca D, Schiavi A, Sciubba A, Tombolini V, Toppi M, Traini G, Trigilio A and Patera V, 2021. Deep Seated Tumour Treatments With Electrons of High Energy Delivered at FLASH Rates: The Example of Prostate Cancer. Journal of Frontiers in Oncology 11, 777852. [CrossRef]
- Hornsey S, Bewley D K, 1971. Hypoxia in mouse intestine induced by electron irradiation at high dose-rates, Journal of Radiation Biology. 19, 479-483.
- 78. Di Martino F, Barca P, Barone S, Bortoli E, Borgheresi R, De Stefano S, Di Francesco M, Faillace L, Giuliano L, Grasso L, Linsalata S, Marfisi D, Migliorati M, Pacitti M, Palumbo L, Felici G, FLASH Radiotherapy With Electrons: Issues Related to the Production, Monitoring, and Dosimetric Characterization of the Beam, Journal of Frontiers in Physics, 8. [CrossRef]
- Kokurewicz K, Brunetti E, Curcio A, Gamba D, Garolfi L, Gilardi A, Senes E, Sjobak K N, Farabolini W, Corsini R, Jaroszynski D A, 2021. An experimental study of focused very high energy electron beams for radiotherapy, Communications Physics, 1-7. [CrossRef]
- 80. Jeong D H, Lee M, Lim H, Kang S K, Lee S J, Kim H C, Lee K, Kim S H, Lee D E, Jang K W, Electron beam scattering device for FLASH preclinical studies with 6- MeV LINAC, Journal of Nuclear Engineering and Technology. [CrossRef]
- Winick H, 1998, Synchrotron radiation sources—present capabilities and future directions. Journal of Synchrotron Radiation, 5, 168-175. [CrossRef]
- Zeman W, Curtis HJ, Baker CP, 1961. Histopathologic effect of high-energy-particle microbeams on the visual cortex of the mouse brain, Journal of Radiation Research, 15, 496–514.
- Eling L, Bouchet A, Nemoz C, Djonov V, Balosso J,Laissue J, Elke Brauer-Krisch E, Adam J F, Serduc R, 2019. Ultra high dose rate Synchrotron Microbeam Radiation Therapy. Preclinical Evidence in View of a Clinical Trabnsfer, Journal of Radiotherapy and Oncology, 139, 56-61.
- Hyer D E, Ding X, Rong, Y, 2021. Proton Therapy Needs Further Technological Development to Fulfill the Promise of Becoming a Superior Treatment Modality (Compared to Photon Therapy), Journal of Applied Clinical Medical Physics, 22, 4-11.
- Burnet N G, Mackay R I, Smith E D, Chadwick A L, Whitefield G A, Thomson D J, Lowe M, Kirbkby N F, Crellin A M, Kirkby K J, 2020. Proton Beam Therapy:Prospectives on the National Health Service England Clinical Service and Research Programme. British Journal of Radiology, 93, 201190873.
- Gaudin C, Lamoureux M, Rouille C, 2001. X-ray emission from a compact hot plasma: applications to radiology and mammography, Journal of Physics in Medicine and Biology, 46 835–851.
- Li D, Yang T, Wu M, Mei Z, Wang K, Lu C, Zhao Y, Ma W, Zhu K, Geng Y, Xiao C, Chen J, Lin C, Tajima T, Yan X, 2023. Introduction of Research Work on Laser Proton Acceleration and Its Application Carried out on Compact Laser–Plasma Accelerator at Peking University. Journal of Photonics 10, 132. [CrossRef]
Figure 1.
Relative oxygen pressure vs. radiation sensitivity. Adapted from cooper et al. (2020) [52].
Figure 1.
Relative oxygen pressure vs. radiation sensitivity. Adapted from cooper et al. (2020) [52].
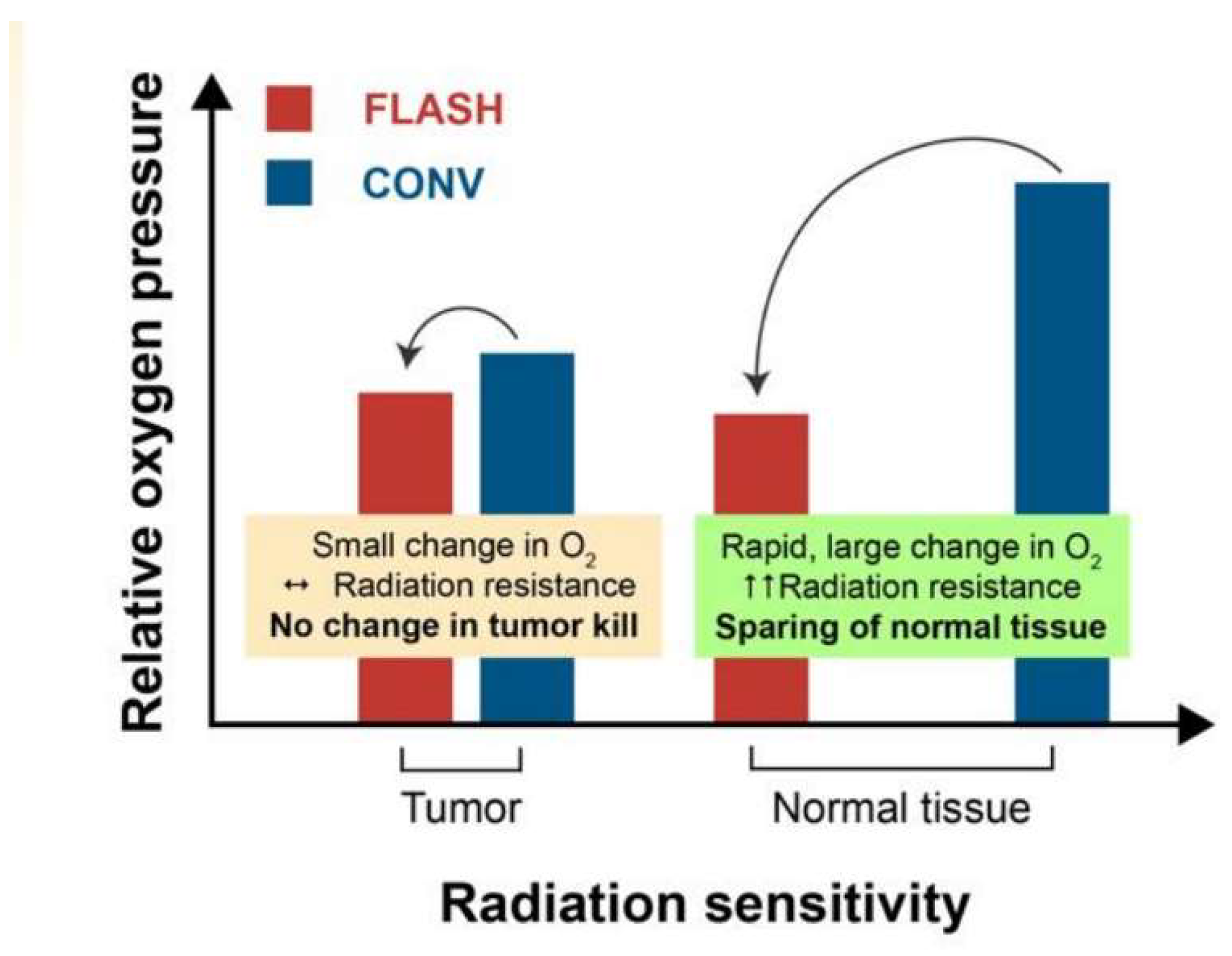
Figure 2.
Total dose rate vs. % tail DNA for 21% O2 concentration. Adapted from Cooper et al. (2020) [52].
Figure 2.
Total dose rate vs. % tail DNA for 21% O2 concentration. Adapted from Cooper et al. (2020) [52].
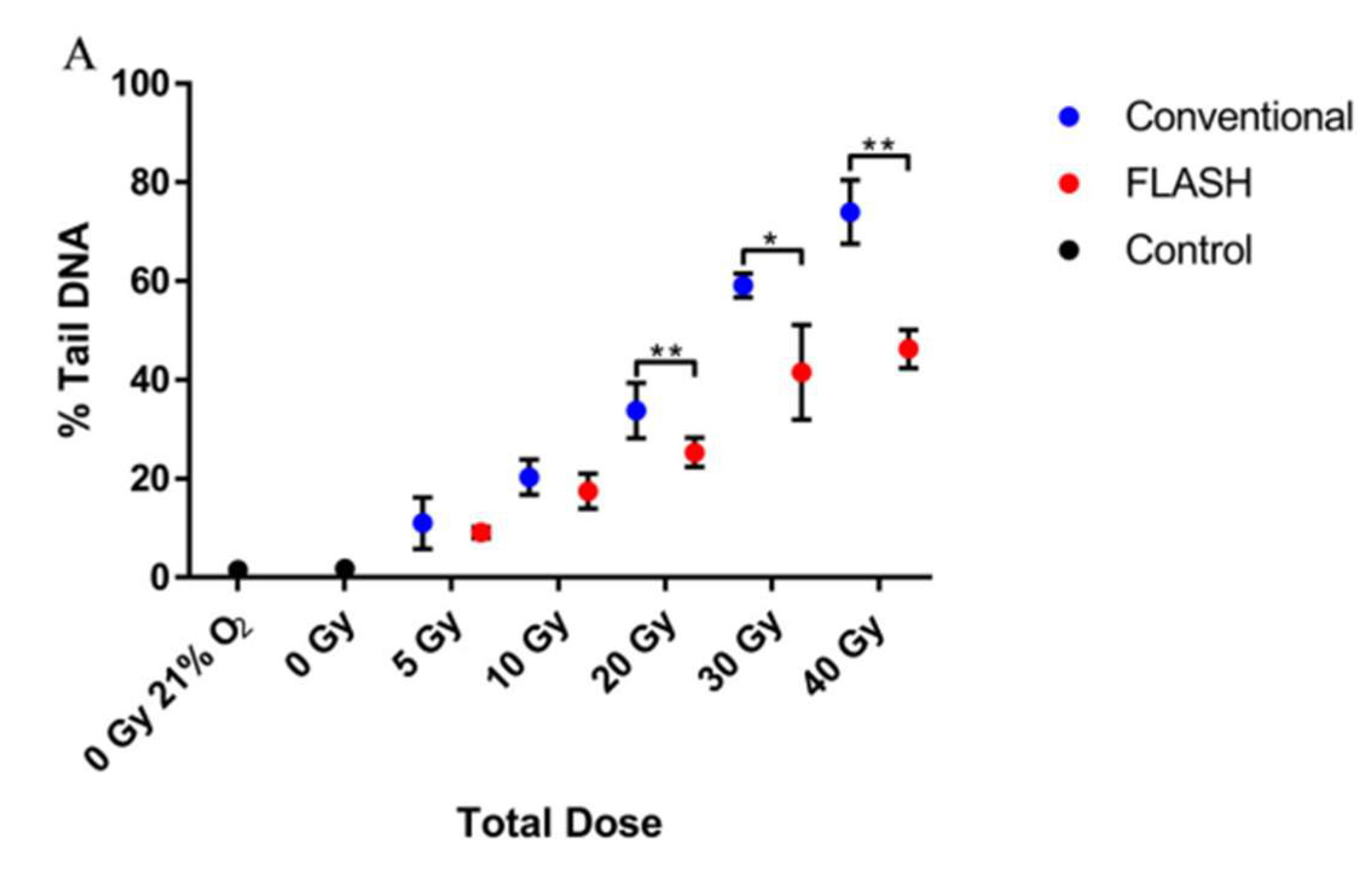
Figure 3.
Genetoxic Stress cause of DNA damages in tissues. Adapted from Li et al. (2018) [63].
Figure 3.
Genetoxic Stress cause of DNA damages in tissues. Adapted from Li et al. (2018) [63].
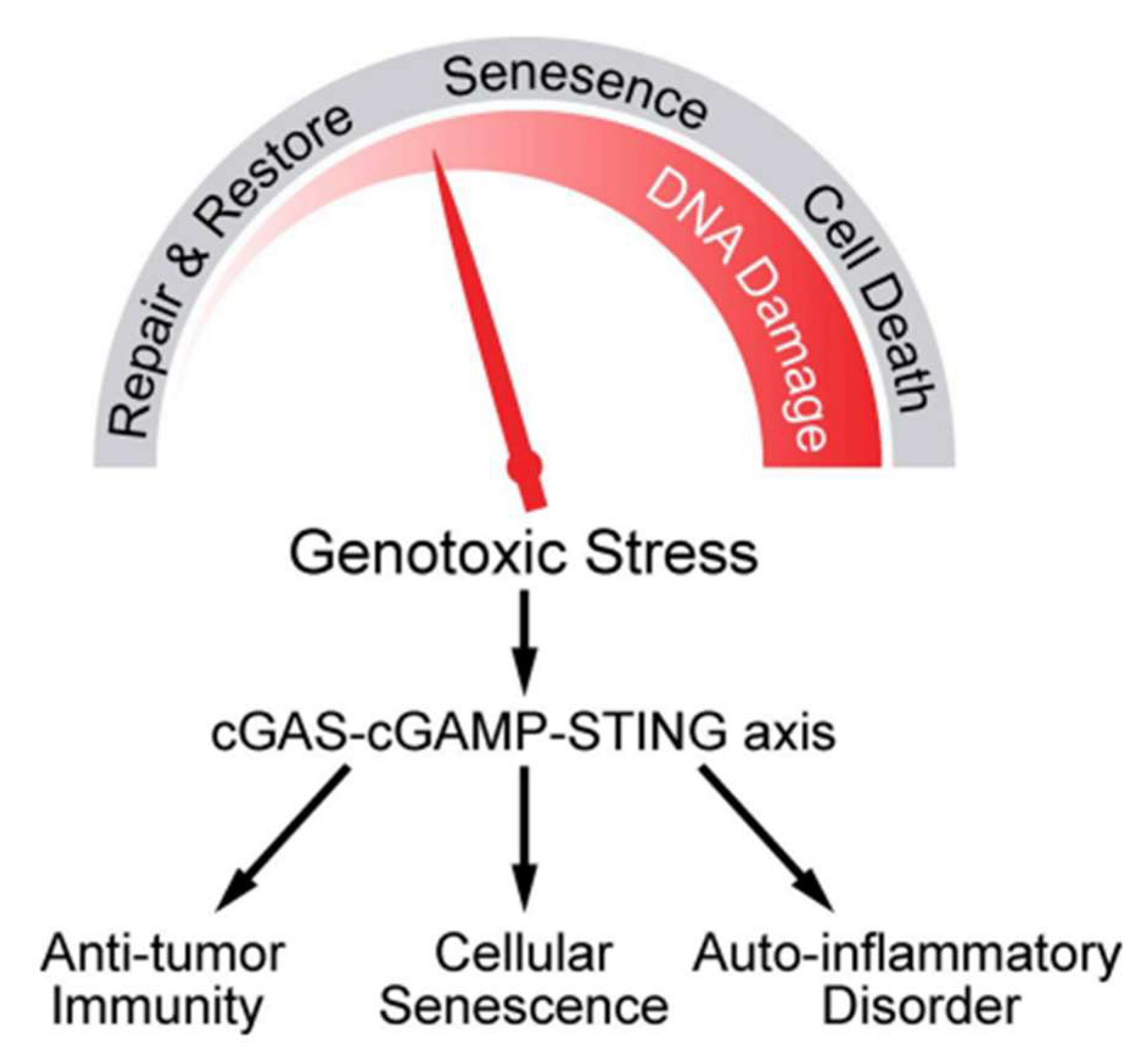
Figure 4.
Summary of preclinical studies using various radiation. Irradiation time for delivering 10 Gy vs. Dose rate in pulse/bunch for several previous studies. Adapted from Bourhis et al. (2019), Schulte et al. (2023), Montay-Gruel et al. (2021) [1, 20,75].
Figure 4.
Summary of preclinical studies using various radiation. Irradiation time for delivering 10 Gy vs. Dose rate in pulse/bunch for several previous studies. Adapted from Bourhis et al. (2019), Schulte et al. (2023), Montay-Gruel et al. (2021) [1, 20,75].

Figure 5.
The CAD model for the target converter in FLASH-x-ray. a) Components of target converter, OD=Outer Diameter, tAl=flange thickness, TIG = tungsten inert gas weld, b) view of the target window, c) assembled prototype Adapted from Esplen et al. (2022) [13].
Figure 5.
The CAD model for the target converter in FLASH-x-ray. a) Components of target converter, OD=Outer Diameter, tAl=flange thickness, TIG = tungsten inert gas weld, b) view of the target window, c) assembled prototype Adapted from Esplen et al. (2022) [13].
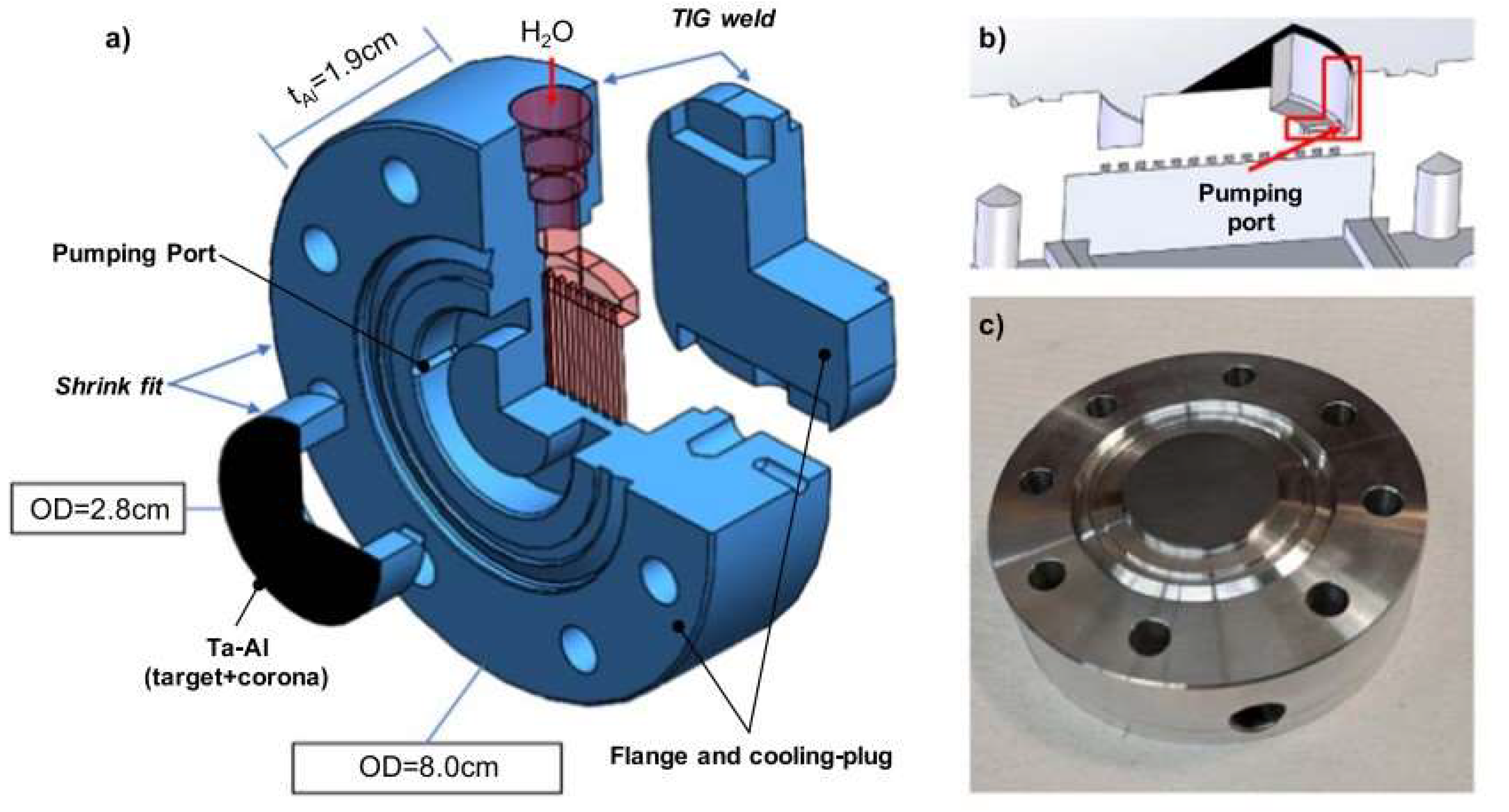
Figure 6.
Schematic representation of the experimental setup for FLASH-proto. Adapted from Beyreuther et al. (2019) [34].
Figure 6.
Schematic representation of the experimental setup for FLASH-proto. Adapted from Beyreuther et al. (2019) [34].
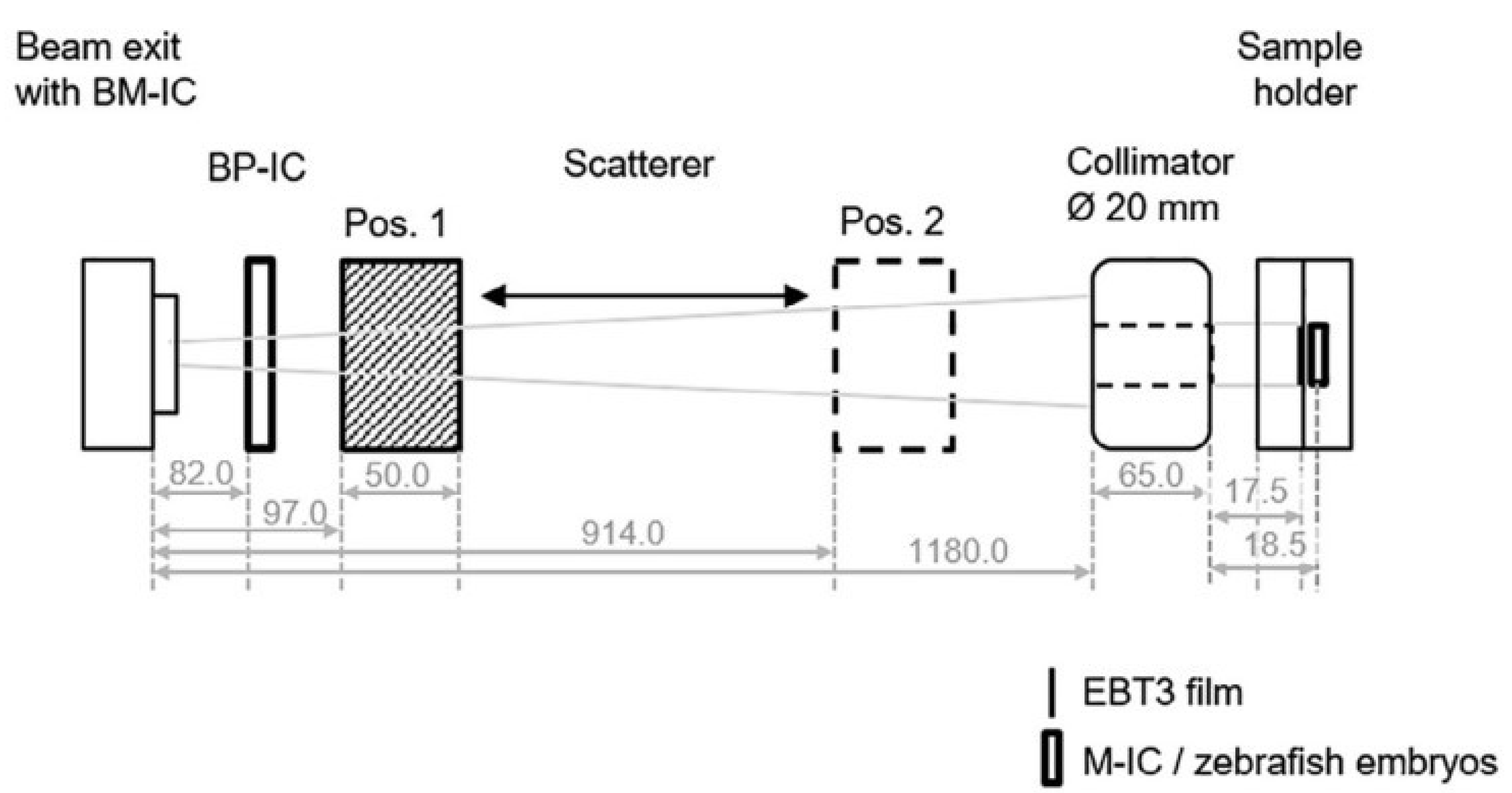

Table 1.
Temporal Beam characteristics of the CONV-RT and FLASH-RT, adapted from [46].
Table 1.
Temporal Beam characteristics of the CONV-RT and FLASH-RT, adapted from [46].
| Beam Characteristics | CONV-RT | FLASH-RT |
| Dose Per Pulse | ||
|
Dose Rate: Single Pulse |
||
|
Mean Dose Rate: Single Fraction |
||
|
Total Treatment Time T |
days. |
< 500 ms |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



