
Submitted:
25 August 2023
Posted:
28 August 2023
You are already at the latest version
Abstract
In the Emergency Department (ED), pain is one of the symptoms that is most frequently reported, making it one of the most significant issues for the emergency physician, but is frequently under treated. Intravenous (IV), oral (PO), and intramuscular (IM) delivery are the standard methods for administering acute pain relief. Firstly, we compared the safety and efficacy of IN analgesia to other conventional routes of analgesia to assess if IN analgesia may be an alternative for the management of acute pain in ED. Secondary, we analyzed the incidence and severity of adverse events (AEs) and rescue analgesia required. We performed a systematic review-based keywords in Pubmed/Medline, Scopus, EMBASE, the Cochrane Library and Controlled Trials Register finding only twenty randomized Clinical trials eligible in the timeline 1992-2022. A total of 2098 patients were analyzed and compared to intravenous analgesia showing no statistical difference in adverse effects. In addition, intranasal analgesia also has a rapid onset and quick absorption. Fentanyl and ketamine are two intranasal drugs that appear promising and may be taken simply and safely while providing effective pain relief. IN is simple to administer, non-invasive, rapid onset and quick absorption; it might be a viable choice in a variety of situations to reduce patient suffering or delays in pain management. Analgesia needs to be tailored to each patient's features and type of pain: IN Fentanyl and Ketamine look promising and may be administered easily and safely while providing effective pain relief.
Keywords:
intranasal administration
; emergency department
; migraine
; primary headache disorder
; analgesics
; acute pain management
; pain
; ketamine
; fentanyl
; paracetamol
; ketorolac
; nsaid
1. Introduction
Acute pain is one of the most frequent symptoms in patients presenting to the Emergency Department (ED), deriving from various conditions, such as trauma, injuries, headache, renal colic, cancer, etc.
Due to its heterogeneity, it frequently represents a challenge for the emergency physicians and data indicates that inadequate pain management is rather typical [1, 2].
There are many medications that can be administered, moreover using different routes. The qualities needed in the drugs we want to provide in emergency care are quickness, effectiveness, and safety. The most common routes for acute analgesia are per os (PO), intravenous (IV) and intramuscular (IM). In patients who need quick analgesia or who may have a nihil per os condition, the per os (PO) route may not be the simplest to use. However, even the intravenous administration may not be very convenient because it requires the placement of a peripheral catheter, therefore the patient must have a good venous patrimony and the hospital requires qualified personnel available.
On the other hand, IM administration frequently causes the patient discomfort. Additionally, the medication takes longer to absorb via muscle, delaying the beginning of the analgesic action.
In this scenario, because of his safety, the simplicity of administration, the non- invasive route, the quick effect, and the fact that doesn’t require a peripheral catheter, the intranasal (IN) method has become increasingly popular. Currently, it is regarded as a good substitute to the classic methods of drugs administration. Additionally, the nasal mucosa is highly vascularized and rich in capillaries; this results in a more rapid absorption and an early onset of analgesia [3,4]. Even this route of administration may have restrictions, for example in facial trauma, or bleeding nose or whit mucus.
The primary goal of the study was to compare the differences in pain scores between IN analgesics and active comparator or placebo from baseline to the time specified in the RCT. Adverse event (AE), frequency and severity as well as the need for rescue analgesia (if available) were secondary outcomes.
There is a little published material regarding opioid IN administration. Due to their difficulty in taking oral or intravenous drugs, most of the studies were conducted on pediatric patients [5,6]. Less studies have been performed on adults.
To our knowledge, only one review that takes a comprehensive look at the use of intranasal analgesia in emergency care and includes a small number of trials [6].
Probably the lack of studies is due to the poor habit of using drugs with this route, few devices to use and poor staff training. In recent years, literature about the effectiveness of intranasal analgesia is increasing.
2. Materials and Methods
We conducted a literature review on the main databases, such as PubMed, the Cochrane Library, Medline, Embase, Scopus in the timeline 1992-2022, using the keywords: emergency departement, intranasal administration, analgesics, migraine, acute pain (MeSH Terms). This review was structured according to the PRISMA statement and encoded in PROSPERO with number CRD42022383622. [7]
We selected all the Randomized controlled trials (RCTs) published in English and evaluating the use of IN analgesia in the Emergency Care.
Only adult patients who had received at least one dosage of IN analgesia for acute pain in the Emergency Room and Prehospital Care were the only ones selected for these studies.
3. Results
20 clinical trials were included in this review. These trials were conducted all around the world, mostly in America and Asia.
In order to assess the effectiveness and impact of the analgesics, validated pain scales were utilized in every trial that was looked at. The frequency of AEs and the requirement for rescue analgesia were also considered by these scales. The inclusion criteria of the patients participating in the trials were as follow: only adults were selected; were included patients receiving IN analgesia compared to OS, IV, or a combination of different routes. Pregnant patients were not allowed. Patients were also excluded if they had used analgesics within the previous hours or if they had hemodynamic or respiratory instability, or disorientation. Patients who couldn’t provide informed consent (due to clinical impossibilities or to language barrier) were also excluded. Even patients who reported an allergy or an intolerance to the trial drug were ineligible.
The sample needed for each RCT was calculated for obtaining 80% or 90% statistical power.
The results are summarized in Table 2. Below we list the main pathologies responsible for acute pain management in the ED, and the implications of intranasal analgesia in these areas.
3.1. Headache
As known, triptans are frequently used to treat acute migraine; among all, Sumatriptan is one of the most used. The oral formulation is the most prescribed, although it has several limitations, such as absorption variation and onset differences that influence the efficacy. Triptans also have well known side effects that may restrict their effectiveness and tolerability. Few studies have investigated the use of intranasal analgesia for migraine or headache in ED [8, 9].
A study conducted by Meredith et al. (2003) involved acute migraine. They examined the pain relief using the Visual Analogue Scale (VAS), after the administration of IV Ketorolac versus nasal Sumatriptan. The study found that while both medications decreased migraine-related pain, IV Ketorolac was more efficient. However, this study has several limitations due to the limited sample size and the lack of AEs recorded [10].
Another trial examined the potential for IN Lidocaine to treat migraine; however, it was no more successful than placebo, even in addition to IV Metoclopramide (Avcu et al., 2017). The second outcome of the trial was the requirement for rescue medication, which was IV Fentanyl. Patient pain severity was assessed using the Numeric Rating Scale (NRS). Nevertheless, local discomfort brought on by Lidocaine may be a confounding factor in the patient’s perceived outcome [11].
Benish et al. released the THINK Trial in 2019 with the aim of comparing the analgesia with IV metoclopramide and diphenhydramine vs. IN ketamine among patients with primary headache in ED. All 56 of the patients they enrolled were adults. The VAS scale was used to assess changes in pain, and the results showed that standard medication was not superior to Ketamine in the recruited patients. However, this RCT had several limitations. For instance, it was a single blind trial and patients in the control arm could have received IV Ketorolac or Dexamethasone in addition to the standard therapy, which could have influenced the comparison of analgesic effectiveness.
Savari et al. (2022) compared IN ketamine to IV ketorolac; the group treated with IN ketamine had a greater reduction in pain intensity, but they also had more adverse effects such as fatigue, dizziness, discomfort, nausea, hypertension. [13]
3.2. Trauma and injuries
One of the most frequent causes of pain in ED patients is trauma, which frequently requires a combination of IM and/or IV drugs. Recently, there was an increase in the use of IN analgesics [14].
Shimonovic et al. (2016) compared IN ketamine to IV or IM morphine; despite ketamine has been well studied as analgesic agent, the IN administration has recently been introduced in ED. Instead, there is a lack of knowledge on the use of morphine in literature. They enrolled a sample of 90 patients and randomized them into three groups; all the three groups showed a similar level of pain relief. The study shows that IN Ketamine can be used as an analgesic in emergencies since it demonstrated efficacy and safety comparable to IV and IM Morphine, and no sever AEs were noted [15].
Blancher et al. (2019) compared IN sufentanil versus IV morphine, assessing NRS at 30 minutes, with 4 hours follow-up: they found some severe respiratory AEs (reporting a number neeeded to harm = 17), questioning the safety of this medication. [16]
Chew et al. (2017), in a small open-label study, compared IN fentanyl added to IV tramadol and metoclopramide, showing an improvement in VAS score at 10 minutes, with transient side effects such as lowering in blood pressure and dizziness. [17]
In 2019 was performed a clinical trial on adult patients with isolated limb injuries; Lemoel et al [18] examined two analgesic strategies: the usual treatment with IV analgesics including opioids as rescue, versus a single dose of IV Sufentanyl followed by IV multimodal analgesia. The second approach improved pain relief after 30 minutes without experiencing any serious AEs, and the need for opioids or IV analgesia has decreased. The majority of AEs were mild and temporary, nevertheless they discovered a significantly high rate of respiratory events when compared to prior studies. This is likely due to ongoing monitoring of the vital signs, which may have detected events without a clinical correlation.
Tongbua et al. (2022) recently showed non-inferiority of IN ketamine compared to IV morphine for acute musculoskeletal pain in elderly, with a quick and sustained effect (up to 120 minutes), without a significant difference in AEs. [19]
3.3. Renal colic
In the Emergency Department, renal colic is a common cause of abdominal discomfort that frequently requires a combination of analgesics, such as non-steroidal anti-inflammatory drugs and opiates; one of the most used is Ketamine. In fact, numerous randomized trials have compared IN therapies to IV analgesia [20].
Farnia et al. (2017) compared IN ketamine to IV morphine, observing a statistically significant reduction in pain score, although the small sample size suggested the need for larger studies [21].
This conclusion was also supported by thre study conducted by Pouraghaei et al. in 2021, which examined these two drugs showing comparable pain relief efficacy in renal colic and no relevant adverse effect [25].
In another study, Desmopressin was suggested as an alternative to the most often used medication. The study compared Indomethacin alone versus Indomethacin with IN Desmopressin for the management of renal colic pain. However, Jalili et al. did not find IN Desmopressin to be more efficient than Indomethacin alone when compared to IN Ketamine [22].
In a comparison between IN Ketamine and IV Fentanyl, Mozafari et al. (2020) discovered that ketamine was less efficient than Fentanyl and was more likely to cause side effects[23].
Nazemian et al. (2020) compared IN to IV fentanyl added to IV ketorolac. They found IN fentanyl effective in pain control though significantly less than IV fentanyl; they concluded that this option could be considered in situations wheren obtaining IV route could lead to a delay in pain control, such as overcrowded ED. [24]
3.4. Other situations
3.4.1. Prehospital
To our knowledge, two RCT have assessed IN analgesia in a prehospital setting.
Rickard et al. (2007) compared IN fentanyl to IV morphine, demonstrating a similar VAS reduction without a significant difference in AEs; a limitation of this trial was the lack of blindings [26].
Andolfatto et al. (2019) compared IN ketamine to placebo when added to standard care (Nitrous Oxide), finding an improvement of pain control without severe AEs. (27)
3.4.2. Breakthrough cancer pain
A high percentage of cancer patients experience physical pain, which is frequently a chronic discomfort that ranges from moderate to severe. Breakthrough pain is a term used to describe the exacerbations of this type of pain that often occur in patients who are already receiving analgesic treatment, including opioids.
Considering the challenges associated with getting a venous route in cancer patients, IN analgesia may be helpful in treating cancer patient’s pain.
Unfortunately, there are few clinical studies of analgesic therapy for cancer patients in ED.
Only one small non-inferiority open-label RCT (Banala et al., 2020) compared IN fentanyl to IV hydromorphone in patients presenting at the ED with severe breakthrough cancer pain. Two out of three evaluations recommended the use of IN Fentanyl, which also has the benefit of requiring less time to administer. However, due to a protocol deviation (calculated by the researchers presuming that the active arm and the control one was comparable) and lack of blinding, this trial was conducted without knowing the actual pain score at baseline. This RCT might have important bias [28].
3.4.3. Acute pain (back and abdominal pain)
Sin et al. (2019) compared IN sufentanil to IV morphine in the treatment of abdominal and low back pain, finding equal improvement in NRS and AEs; the study’s limitations include a small sample size and lack of data on IV morphine rescue analgesia. [29]
4. Discussion
Pain control is universally considered an important issue, especially in ED patients; because pain affects a patient’s quality of life, it is crucial to get the right treatment. Despite the availability of multimodal medications, analgesic therapy is frequently insufficient [30].
IN fentanyl and ketamine have already shown their safety in pharmacokinetics trials. These drugs have an higher bioavailability thanks to their fast absorption via the nasal mucosa, and the lack of fist pass effect. It is important to remember IN route restrictions like pathologic changes to the nostrils and a limited amount of administrable volume [4,31,32].
Although there are limited trials available in the ED context, the potential benefits of IN therapies, such as rapid and simple administrations with prompt absorption, may improve pain control in ED and prehospital setting. Sub dissociative doses of Ketamine were proven to be safe and helpful in patients out-of-hospital too by a retrospective large-sample trial [33].
Low dosage ketamine analgesia in patients with severe acute pain is becoming more and more promising due to its analgesic efficacy (similar to opioids), potential to maintain circulatory stability and respiratory reflexes, and neuroprotection in patients with acute brain damage [34,35,36].
Opioids are being used extensively to treat acute pain, although they can have side effects that vary on dosage, including weakness, dizziness, nausea, and constipation. Due to this, the importance of multimodal analgesia with opioid-sparing techniques should be considered, especially considering the worrying data about opioid abusers. Ketamine appears to be useful in lowering the demand for opioids [37,38]. Due to its sympathomimetic action, the most significant Ketamine contraindication is coronary illness or cardiological pathologies [39].
IN route may help for severe pain requiring quick management (such as trauma or breakthrough cancer pain). Bioavailability of IN opioids depends on the specific molecule, being rather high for fentanyl and sufentanil thanks to their lipophilic structure [40, 41, 42].
Regarding the safety profile, most AEs recorded were moderate, not needing medical intervention. According to the literature, dizziness was the most common. Confusion, a brief drop in blood pressure, nausea, and vomiting were also usual AEs. A small percentage of patients receiving opiate-based treatment also occasionally experienced transient bradypnea or oxygen saturation below 90%, necessitating a short-time administration of oxygen therapy. Only a minor number of serious AEs were observed in few trials (with a small sample size).
For patients presenting with headache, IN ketamine was found more effective than IV ketorolac, despite of a higher prevalence of side effects [9-12].
When compared to IV morphine for the treatment of pain due to traumatic injuries, IN ketamine demonstrated non-inferiority effect; in fact, ketamine has a morphine-sparing effect. Early IN Sufentanyl administration (after triage) can enhance pain management and reduce the need for IV analgesia. Like this, adding IN Fentanyl to IV Tramadol resulted in a higher decrease in pain score after 10 minutes. Only one research reported some significant AEs when IN Sufentanyl was compared to IV Morphine [15,19]. However, Ketamine, Fentanyl, and Morphine are thought to be the finest analgesics, per data found in the literature. The fastest onset is achieved with Ketamine and Fentanyl. Similar results on the therapy of traumatic pain were reported by Abu et al. in their review [30].
In small research, IN Ketamine was found to be more effective than IV Morphine for patients with renal colic; another trial revealed that IN ketamine and IV morphine were equally beneficial. Although IN fentanyl was proven to be less efficient than IV fentanyl, it may still be used when placing a venous catheter could be difficult (such as overcrowding or lack of trained healthcare providers) [21-25].
Given that prehospital treatment is sometimes provided by paramedics, who are only trained to administer certain medications, IN analgesia may aid in the quick delivery of pain relief in this scenario. There aren’t many research regarding this in the literature, but in this case, IN fentanyl was found to be just as effective as IV morphine, while IN ketamine led to a fastest onset in pain relief [26,27]. A recent review (Fernandez et al.,2021) reaffirmed the safety of ketamine used outside of hospitals, with a limited rate of AEs [33].
5. Conclusions
In this study, we examined the literature about the effectiveness of IN analgesia for managing acute pain in the ED. The review included 19 RCT trials with a combined enrollment of 2098 patients. The strength of the evidence varied between weak and moderate. When compared to IV analgesia, the data showed no statistically significant difference in adverse effects, confirming the safety of IN medicines. Additionally, IN analgesia has been shown to be safe, non-invasive, simple to administer, and has a rapid onset and quick absorption.
These findings suggest that it might be a viable choice in a variety of situations to reduce patient suffering or delays in pain management, or when accessing an intravenous route may be challenging due to clinical circumstances or a shortage of qualified healthcare professionals. In particular in busy EDs, a standardized protocol for early analgesic administration may aid in pain treatment.
Analgesia needs to be tailored to each patient’s features, type of pain, and clinical environment. IN Fentanyl and Ketamine look promising and may be administered easily and safely while providing effective pain relief.
For this review we could not find randomized trials including patients presenting with alteration of mental status, and respiratory or hemodynamic instability, probably because of the potential impact of narcotics on breath or arterial blood pressure; none of the studies included pregnant women.
This could be a major limitation considering that, in the Emergency Care, pain and respiratory or hemodynamic instability often coexist.
The absence of follow-up in this evaluation (just one research included a follow-up at 48–72 hours) makes it impossible to determine if these patients need additional medications in the hours or days that followed, or the frequency of subsequent adverse events (AEs). The fact that patient recruitment was completed only when researchers were available and without knowledge of the full population and the characteristics of patients who presented with pain to the ED raises the possibility of bias.
Some of the trials included were conducted on a small sample. There were few studies from Europe and Oceania; most trials were conducted in Asia or America, and no trials were undertaken in Africa. Only a small number of RCTs from Iran included patients who were 15 years old or older, whereas all the other studies included participants who were 18 years old or older. The risk of local irritation or side effects, as well as the comparison of the IN medication to placebo with a difference in pain control following the injection of analgesic or saline solution, were other possible sources of bias. In some cases (such as breakthrough cancer pain) only open label trials were found.
Summary
Why is this topic important?
This topic is important because intranasal analgesia is an alternative and a valid way to treat acute pain more promptly and with less discomfort for the patient.
What does this review attempt to show?
This review attempts to show that IN is simple to administer, non-invasive, and has rapid onset and quick absorption; it might be a viable choice in a variety of situations to reduce patient suffering or delays in pain management.
What are the key findings?
The key findings are: intranasal administration; emergency department; acute pain management.
How is patient care impacted?
Briefly patient care is impacted by: early onset of analgesia; non-invasive route; less discomfort during hospitalization
References
- Saunders M, Adelgais K, Nelson D. Use of intranasal fentanyl for the relief of pediatric orthopedic trauma pain. Acad Emerg Med. 2010 Nov;17(11):1155-61. [CrossRef] [PubMed]
- Todd KH, Ducharme J, Choiniere M, Crandall CS, Fosnocht DE, Homel P, Tanabe P; PEMI Study Group. Pain in the emergency department: results of the pain and emergency medicine initiative (PEMI) multicenter study. J Pain. 2007 Jun;8(6):460-6. [CrossRef] [PubMed]
- McBride, DL. Emergency Departments Increasingly Administering Medications through the Nose. J Pediatr Nurs. 2017 Nov-Dec;37:132-133. [CrossRef] [PubMed]
- Pires A, Fortuna A, Alves G, Falcão A. Intranasal drug delivery: how, why and what for? J Pharm Pharm Sci. 2009;12(3):288-311. [CrossRef] [PubMed]
- Cole J, Shepherd M, Young P. Intranasal fentanyl in 1-3-year-olds: a prospective study of the effectiveness of intranasal fentanyl as acute analgesia. Emerg Med Australas. 2009 Oct;21(5):395-400. [CrossRef] [PubMed]
- Sin B, Wiafe J, Ciaramella C, Valdez L, Motov SM. The use of intranasal analgesia for acute pain control in the emergency department: A literature review. Am J Emerg Med. 2018 Feb;36(2):310-318. [CrossRef] [PubMed]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29;372:n71. [CrossRef]
- Silberstein S, Winner PK, McAllister PJ, Tepper SJ, Halker R, Mahmoud RA, Siffert J. Early Onset of Efficacy and Consistency of Response Across Multiple Migraine Attacks From the Randomized COMPASS Study: AVP-825 Breath Powered® Exhalation Delivery System (Sumatriptan Nasal Powder) vs Oral Sumatriptan. Headache. 2017 Jun;57(6):862-876. [CrossRef] [PubMed]
- Dodick D, Brandes J, Elkind A, Mathew N, Rodichok L. Speed of onset, efficacy and tolerability of zolmitriptan nasal spray in the acute treatment of migraine: a randomised, double-blind, placebo-controlled study. CNS Drugs. 2005;19(2):125-36. [CrossRef] [PubMed]
- Meredith JT, Wait S, Brewer KL. A prospective double-blind study of nasal sumatriptan versus IV ketorolac in migraine. Am J Emerg Med. 2003 May;21(3):173-5. [CrossRef] [PubMed]
- Avcu N, Doğan NÖ, Pekdemir M, Yaka E, Yılmaz S, Alyeşil C, Akalın LE. Intranasal Lidocaine in Acute Treatment of Migraine: A Randomized Controlled Trial. Ann Emerg Med. 2017 Jun;69(6):743-751. [CrossRef] [PubMed]
- Benish T, Villalobos D, Love S, Casmaer M, Hunter CJ, Summers SM, April MD. The THINK (Treatment of Headache with Intranasal Ketamine) Trial: A Randomized Controlled Trial Comparing Intranasal Ketamine with Intravenous Metoclopramide. J Emerg Med. 2019 Mar;56(3):248-257.e1. [CrossRef] [PubMed]
- Sarvari HR, Baigrezaii H, Nazarianpirdosti M, Meysami A, Safari-Faramani R. Comparison of the efficacy of intranasal ketamine versus intravenous ketorolac on acute non-traumatic headaches: a randomized double-blind clinical trial. Head Face Med. 2022 Jan 3;18(1):1. [CrossRef]
- Shrestha R, Pant S, Shrestha A, Batajoo KH, Thapa R, Vaidya S. Intranasal ketamine for the treatment of patients with acute pain in the emergency department. World J Emerg Med. 2016;7(1):19-24. [CrossRef]
- Shimonovich S, Gigi R, Shapira A, Sarig-Meth T, Nadav D, Rozenek M, West D, Halpern P. Intranasal ketamine for acute traumatic pain in the Emergency Department: a prospective, randomized clinical trial of efficacy and safety. BMC Emerg Med. 2016 Nov 9;16(1):43. [CrossRef]
- Blancher M, Maignan M, Clapé C, et al. Intranasal sufentanil versus intravenous morphine for acute severe trauma pain: A double-blind randomized non-inferiority study. PLoS Med. 2019;16(7):e1002849. Published 2019 Jul 16. [CrossRef]
- Chew KS, Shaharudin AH. An open-label randomized controlled trial on the efficacy of adding intranasal fentanyl to intravenous tramadol in patients with moderate to severe pain following acute musculoskeletal injuries. Singapore Med J. 2017;58(10):601-605. [CrossRef]
- Lemoel F, Contenti J, Cibiera C, Rapp J, Occelli C, Levraut J. Intranasal sufentanil given in the emergency department triage zone for severe acute traumatic pain: a randomized double-blind controlled trial. Intern Emerg Med. 2019 Jun;14(4):571-579. [CrossRef] [PubMed]
- Tongbua S, Sri-On J, Thong-On K, Paksophis T. Non-inferiority of intranasal ketamine compared to intravenous morphine for musculoskeletal pain relief among older adults in an emergency department: a randomised controlled trial. Age Ageing. 2022 Mar 1;51(3):afac073. [CrossRef] [PubMed]
- Golzari SE, Soleimanpour H, Rahmani F, Zamani Mehr N, Safari S, Heshmat Y, Ebrahimi Bakhtavar H. Therapeutic approaches for renal colic in the emergency department: a review article. Anesth Pain Med. 2014 Feb 13;4(1):e16222. [CrossRef]
- Farnia MR, Jalali A, Vahidi E, Momeni M, Seyedhosseini J, Saeedi M. Comparison of intranasal ketamine versus IV morphine in reducing pain in patients with renal colic. Am J Emerg Med. 2017 Mar;35(3):434-437. [CrossRef] [PubMed]
- Pouraghaei M, Moharamzadeh P, Paknezhad SP, Rajabpour ZV, Soleimanpour H. Intranasal ketamine versus intravenous morphine for pain management in patients with renal colic: a double-blind, randomized, controlled trial. World J Urol. 2021 Apr;39(4):1263-1267. [CrossRef] [PubMed]
- Jalili M, Shirani F, Entezari P, Hedayatshodeh M, Baigi V, Mirfazaelian H. Desmopressin/indomethacin combination efficacy and safety in renal colic pain management: A randomized placebo controlled trial. Am J Emerg Med. 2019 Jun;37(6):1009-1012. [CrossRef] [PubMed]
- Mozafari J, Maleki Verki M, Motamed H, Sabouhi A, Tirandaz F. Comparing intranasal ketamine with intravenous fentanyl in reducing pain in patients with renal colic: A double-blind randomized clinical trial. Am J Emerg Med. 2020 Mar;38(3):549-553. [CrossRef] [PubMed]
- Nazemian N, Torabi M, Mirzaee M. Atomized intranasal vs intravenous fentanyl in severe renal colic pain management: A randomized single-blinded clinical trial. Am J Emerg Med. 2020 Aug;38(8):1635-1640. [CrossRef] [PubMed]
- Rickard C, O’Meara P, McGrail M, Garner D, McLean A, Le Lievre P. A randomized controlled trial of intranasal fentanyl vs intravenous morphine for analgesia in the prehospital setting. Am J Emerg Med. 2007 Oct;25(8):911-7. [CrossRef]
- Andolfatto G, Innes K, Dick W, Jenneson S, Willman E, Stenstrom R, Zed PJ, Benoit G. Prehospital Analgesia With Intranasal Ketamine (PAIN-K): A Randomized Double-Blind Trial in Adults. Ann Emerg Med. 2019 Aug;74(2):241-250. [CrossRef] [PubMed]
- Banala SR, Khattab OK, Page VD, Warneke CL, Todd KH, Yeung SJ. Intranasal fentanyl spray versus intravenous opioids for the treatment of severe pain in patients with cancer in the emergency department setting: A randomized controlled trial. PLoS One. 2020 Jul 10;15(7):e0235461. [CrossRef]
- Sin B, Jeffrey I, Halpern Z, Adebayo A, Wing T, Lee AS, Ruiz J, Persaud K, Davenport L, de Souza S, Williams M. Intranasal Sufentanil Versus Intravenous Morphine for Acute Pain in the Emergency Department: A Randomized Pilot Trial. J Emerg Med. 2019 Mar;56(3):301-307. [CrossRef] [PubMed]
- Abu-Snieneh HM, Alsharari AF, Abuadas FH, Alqahtani ME. Effectiveness of pain management among trauma patients in the emergency department, a systematic review. Int Emerg Nurs. 2022 May;62:101158. [CrossRef] [PubMed]
- Nardi-Hiebl S, Ndieyira JW, Al Enzi Y, Al Akkad W, Koch T, Geldner G, Reyher C, Eberhart LHJ. Pharmacokinetic Characterisation and Comparison of Bioavailability of Intranasal Fentanyl, Transmucosal, and Intravenous Administration through a Three-Way Crossover Study in 24 Healthy Volunteers. Pain Res Manag. 2021 Nov 29;2021:2887773. [CrossRef]
- Nave R, Schmitt H, Popper L. Faster absorption and higher systemic bioavailability of intranasal fentanyl spray compared to oral transmucosal fentanyl citrate in healthy subjects. Drug Deliv. 2013 Jun-Jul;20(5):216-23. [CrossRef] [PubMed]
- Fernandez AR, Bourn SS, Crowe RP, Bronsky ES, Scheppke KA, Antevy P, Myers JB. Out-of-Hospital Ketamine: Indications for Use, Patient Outcomes, and Associated Mortality. Ann Emerg Med. 2021 Jul;78(1):123-131. [CrossRef] [PubMed]
- Balzer N, McLeod SL, Walsh C, Grewal K. Low-dose Ketamine For Acute Pain Control in the Emergency Department: A Systematic Review and Meta-analysis. Acad Emerg Med. 2021 Apr;28(4):444-454. [CrossRef] [PubMed]
- Gao M, Rejaei D, Liu H. Ketamine use in current clinical practice. Acta Pharmacol Sin. 2016 Jul;37(7):865-72. [CrossRef]
- Zanza C, Piccolella F, Racca F, Romenskaya T, Longhitano Y, Franceschi F, Savioli G, Bertozzi G, De Simone S, Cipolloni L, La Russa R. Ketamine in Acute Brain Injury: Current Opinion Following Cerebral Circulation and Electrical Activity. Healthcare (Basel). 2022 Mar 17;10(3):566. [CrossRef]
- Zanza C, Romenskaya T, Zuliani M, Piccolella F, Bottinelli M, Caputo G, Rocca E, Maconi A, Savioli G, Longhitano Y. Acute Traumatic Pain in the Emergency Department. Diseases. 2023 Mar 3;11(1):45. [CrossRef]
- Bouida W, Bel Haj Ali K, Ben Soltane H, Msolli MA, Boubaker H, Sekma A, Beltaief K, Grissa MH, Methamem M, Boukef R, Belguith A, Nouira S. Effect on Opioids Requirement of Early Administration of Intranasal Ketamine for Acute Traumatic Pain. Clin J Pain. 2020 Jun;36(6):458-462. [CrossRef] [PubMed]
- Green SM, Roback MG, Kennedy RM, Krauss B. Clinical practice guideline for emergency department ketamine dissociative sedation: 2011 update. Ann Emerg Med. 2011 May;57(5):449-61. [CrossRef] [PubMed]
- Grassin-Delyle S, Buenestado A, Naline E, Faisy C, Blouquit-Laye S, Couderc LJ, Le Guen M, Fischler M, Devillier P. Intranasal drug delivery: an efficient and non-invasive route for systemic administration: focus on opioids. Pharmacol Ther. 2012 Jun;134(3):366-79. [CrossRef] [PubMed]
- Daoust R, Paquet J, Cournoyer A, Piette È, Morris J, Lessard J, Castonguay V, Williamson D, Chauny JM. Side effects from opioids used for acute pain after emergency department discharge. Am J Emerg Med. 2020 Apr;38(4):695-701. [CrossRef] [PubMed]
- Zanza C, Longhitano Y, Lin E, Luo J, Artico M, Savarese B, Bonato V, Piccioni A, Franceschi F, Taurone S, Abenavoli L, Berger JM. Intravenous Magnesium - Lidocaine - Ketorolac Cocktail for Postoperative Opioid Resistant Pain: A Case Series of Novel Rescue Therapy. Rev Recent Clin Trials. 2021;16(3):288-293. [CrossRef] [PubMed]
- Savioli G, Ceresa IF, Gri N, Bavestrello Piccini G, Longhitano Y, Zanza C, Piccioni A, Esposito C, Ricevuti G, Bressan MA. Emergency Department Overcrowding: Understanding the Factors to Find Corresponding Solutions. J Pers Med. 2022 Feb 14;12(2):279. [CrossRef]
- Zanza C, Tornatore G, Naturale C, Longhitano Y, Saviano A, Piccioni A, Maiese A, Ferrara M, Volonnino G, Bertozzi G, Grassi R, Donati F, Karaboue MAA. Cervical spine injury: clinical and medico-legal overview. Radiol Med. 2023 Jan;128(1):103-112. [CrossRef]
Figure 1.
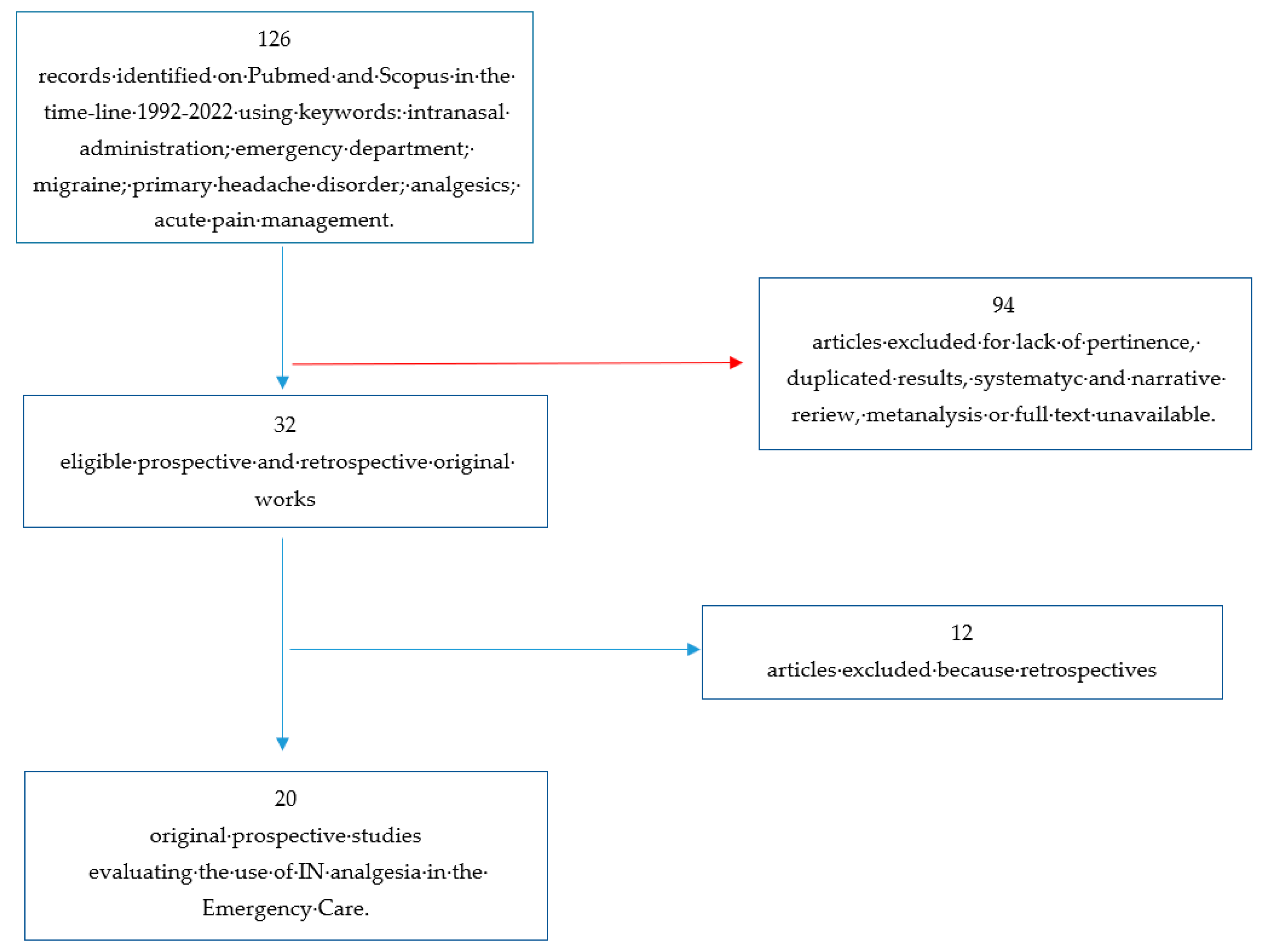

Table 1.
| First Author | Randomization process | Deviation from intended intervention | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall |
|---|---|---|---|---|---|---|
| Dodich et al |  |
|
|
|
|
|
| Meredith et al |  |
|
|
|
|
 |
| Avcu et al | |
|
|
|
|
|
| Benish et al | |
|
|
|
|
|
| Sarvai et al | |
|
|
|
|
|
| Shrestha et al | |
|
|
|
|
|
| Shimonovic et al | |
|
|
|
|
|
| Blancher et al | |
|
|
|
|
|
| Chew et al | |
|
|
|
|
|
| Leomoel et al | |
|
|
|
|
|
| Tongbual et al | |
|
|
|
|
|
| Silberstein et al | |
|
|
|
|
|
| Pouraghaei et al | |
|
|
|
|
|
| Jalili et al | |
|
|
|
|
|
| Mozafari et al | |
|
|
|
|
|
| Nazemian et al | |
|
|
|
|
|
| Rickard et al | |
|
|
|
|
|
| Andolfatto et al | |
|
|
|
|
|
| Banala et al | |
|
|
|
|
|
| Sin et al | |
|
|
|
|
|
Table 3.
Description of the study analyzed.
| Author | Year | Intervention | Population | Objective | Findings |
|---|---|---|---|---|---|
| Dodick et al | 2005 | IN zolmitriptan for headache | afer exclusions 1740; 886 zolmitriptan, 854 placebo | Headache reduction at 15 min, 30 min, 1 h, 2 h | Response rate superior in zolmitriptan (66,2%) vs placebo (35,0%) p<0,001 |
| Meredith et al | 2003 | IN zolmitriptan vs IV ketorolac for headache | 29; 16 sumatriptan, 13 ketorolac | Headache reduction at 1 h | Both achieved significant pain reduction, however ketorolac was superior in reducing VAS |
| Avcu et al | 2017 | IN lidocaine for headache | after exclusion 162; 81 lidocaine, 81 placebo | Headache reduction at 15 and 30 min | No difference in pain reduction |
| Benish et al | 2019 | IN ketamine vs IV metoclopramide for headache | after exclusion 53; 27 ketamine, 26 placebo | Headache reduction at 30 min and requirement for rescue analgesia at 60 min | No difference in pain reduction |
| Sarvari et al | 2022 | IN ketamine vs IV ketorolac for headache | afer exclusions 140; 70 ketamine, 70 ketorolac | Headache reduction at 30, 60, 120 min | Ketamine had more analgesic effect than intravenous ketorolac in a shorter time |
| Shrestha et al | 2016 | Effectiveness of IN ketamine in pain reduction (various acute injuries) | 39 patients | Pain reduction at 15, 30, 60 min | IN ketamine reduced VAS pain scores to a clinically significant degree in 80% of patients |
| Shimonovic et al | 2016 | IN ketamine vs IV morphine vs IM morphine in acute traumatic pain | 90 patients; 34 IN ketamine, 26 IV morphine, 30 IM morphine | Pain at 5 min interval from 0 to 60 min | IN ketamine may provide analgesia clinically equal to IV or IM morphine |
| Blancher et al | 2019 | IN sufentanil vs IV morphine in acute pain | 157 patients; 77 IN sufentanil, 80 IV morphine | Non-inferiority study | IN sufentanil was non-inferior to IV morphine |
| Chew et al | 2017 | IN fentanil plus IV tramadol vs IV tramadol in acute pain | 20 patients; 10 IN fentanil plus IV tramadol, 10 IV tramadol | Pain reduction at 10 min | Greater reduction in the mean VAS score among the patients in the fentanyl + tramadol arm |
| Lemoel et al | 2019 | IN sufentanil vs IN placebo in acute pain (all plus IV multimodal analgesia) | 144 patients; 72 IN sufentanil, 72 IN placebo | Proportion of VAS < 3 at 30 min | IN sufentanil determines a 20% absolute increase in proportion of patients reaching pain relief |
| Tongbual et al | 2022 | IN ketamine vs IV morphine in musculoskeletal pain in ED | 74 patients; 37 IN ketamine, 37 IN morphine | Pain reduction at 30 min | IN ketamine provides analgesic efficacy comparable (non-inferior) to IV morphine |
| Silberstein et al | 2017 | Sumatriptan nasal powder (with IN delivery system) vs oral sumatriptan in migraine | 1531 migraine events; 765 nasal powder, 766 oral sumatriptan | Headache reduction at 30 min | Sumatriptan powder provided greater reduction in migraine pain intensity |
| Pouraghaei et al | 2021 | IN ketamine vs IV morphine in renal colic | 200 patients; 100 IN ketamine, 100 IV morphine | Pain reduction at 15, 30, 60 min | IN ketamine has the same efcacy as IV morphine in renal colic pain control |
| Jalili et al | 2019 | Indomethacin plus IN desmopressin vs indomethacin plus IN placebo in renal colic | 124 patients; 62 IN desmopressin, 62 IN placebo | Pain reduction | Desmopressin as an adjunct to NSAIDs in the management of renal colic, does not significantly improve pain relief |
| Mozafari et al | 2020 | IN ketamine vs IV fentanil in renal colic | 130 patients; 65 IN ketamine, 65 IV fentanil | Pain reduction at 5, 15, 30 min | The effect of IN ketamine was less significant than of IV fentanil |
| Nazemian et al | 2020 | IN fentanil plus IV ketorolac vs IV fentanil plus IV ketorolac in renal colic | 220 patients; 110 IN fentanil, 110 IV fentanil | Pain reduction at 60 min | The mean pain score was higher in the IN group. Nevertheless, the pain intensity significantly and consecutively reduced in bothg roups during the study |
| Rickard et al | 2007 | IV morphine vs IN fentanil in prehospital analgesia | 258 patients; 122 IV morphine, 136 IN fentanil | Difference between baseline and destination pain score | No difference in pain reduction |
| Andolfatto et al | 2019 | Effectiveness of IN ketamine in pain reduction in prehospital setting | 120 patients; 60 IN ketamine, 60 IN placebo | Pain reduction at 2 and 30 min | Intranasal ketamine provides clinically significant pain reduction and improved comfort compared with intranasal placebo |
| Banala et al | 2020 | IN fentanil vs IV hydromorphone in cancer pain in ED setting | 82 patients; 42 IN fentanil, 42 IV hydromorphone | Pain reduction at 60 min | Two of three analyses supported non-inferiority of INF versus IVH, while one analysis was inconclusive |
| Sin et al | 2019 | IN sufentanil vs IV morphine in acute pain in ED | 60 patients; 30 IN sufentanil, 30 IV morphine | Efficacy and safety of IN sufentanil in ED | IN resulted in safe analgesia, comparable with IV morphine |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



