
Submitted:
25 August 2023
Posted:
29 August 2023
You are already at the latest version
Abstract
(1) Importance of problem: Breast cancer accounted for 685.000 deaths globally in 2020, and half of all cases occur in women with no specific risk factor beside gender and age-group. During last 4 decades we see a reduction by 40% of age-standardized breast cancer [1], which in turn means that the number of mastectomies performed for younger women increased, raising the need for adequate breast reconstructive surgery. Advances in oncological treatment have made it possible to limit the extent of what represents radical surgery for breast cancer, yet in the past decade, we see a marked trend toward mastectomy in breast conserving surgery eligible patients [2]. Prophylactic mastectomy has also registered an upward trend [3,4]. This trend together with new indication for breast reconstruction like chest feminization in transgender patients [5] have increased the need for breast reconstruction surgery. (2) Purpose: The purpose of this study is to analyze the types of reconstructive procedures, their indications, their limitations, their functional results and the safety profiles when used during the integrated treatment plan of the oncologic patient; (3) Methods: We conducted an extensive literature review of the main reconstructive techniques, especially the autologous procedures, summarized the findings and presented a few cases from our own experience for exemplification of the usage of breast reconstruction in oncologic patients. (4) Conclusions: Breast reconstruction has become a necessary step in the treatment of most breast cancers and many reconstructive techniques are now routinely practiced. Microsurgical techniques are considered the "gold standard", but they are not accessible to all services, from a technical or financial point of view, so pediculated flaps remain the safe and reliable option, along with alloplastic procedures, to improve the quality of life of these patients.
Keywords:
breast reconstruction
; reconstruction following mastectomy
; prophylactic mastectomy
; chest feminization
; transgender
; implant reconstruction of breast
; immediate reconstruction
; delayed reconstruction
; two-stage breast reconstruction
; autologous breast reconstruction
1. Introduction
Breast cancer is the most commonly diagnosed neoplasm in the female population in the world [6]. It is the leading cause of cancer related death in women in most countries of the world, except in developed countries, where it ranks second after lung tumors. However, mortality has been steadily declining for over 30 years, with an average 5-year survival of 86% and 75% at 10 years [7]. This trend is attributed both to the increase in the effectiveness of oncological treatments and to early screening and screening programs.
Breast reconstruction is an important component of breast cancer treatment. With the increase of life expectancy, it has become essential to ensure a good quality of life for patients, forcing a continuous evolution of surgical techniques and their. Breast reconstruction is necessary not only after performing a radical mastectomy, but also after conservative interventions on the breast that have not been accompanied by an optimal aesthetic effect. The need to complete the surgical treatment of breast cancer with breast reconstruction derives from the beneficial impact at the psychological level, respectively at the level body image, of sexuality and general quality of life of patients [8]. In recent years the ever-increasing number of patients opting for prophylactic mastectomy due to genetic predisposition for developing breast cancer or family history of cancer [3,4,9,10,11] has given birth to a new type of integrated treatment plan in oncology.
Although not the focus of this study, breast reconstruction has another extremely important indication in recent years, namely for chest feminization of Male-to-Female Transgender patients. In combination with hormone and psychological therapy breast enhancement is the most common physical modification in this populational subset [5,12,13,14], contributing to the reduction of the patient’s dysphoria. For this purpose, all surgical reconstructive techniques used in patients with mastectomies can be employed.
This study reviews the main techniques, especially the autologous procedures and investigates available data from the literature indicating their indications and results.
2. Problem at hand
2.1. Dimension of problem
Breast cancer accounted for 685.000 deaths globally in 2020, and half of all cases occur in women with no specific risk factor. During last 4 decades we see a reduction by 40% of age-standardized breast cancer [1], which in turn means that the number of mastectomies performed for younger women increased, raising the need for adequate reconstructive surgery. Breast cancer is the most prevalent form of cancer in the World, with a total of 7.8 million women alive in 2020 who were diagnosed with a form of this malady in the previous 5-year period [1]. Advances in oncological treatment, which have prolonged survivorship after breast cancer, also made it possible to limit the extent of what represents radical surgery for breast cancer, yet in the past decade, we see a marked trend toward mastectomy in breast conserving surgery (BCS) eligible patients [2]. Prophylactic mastectomy has also registered an upward trend [3,4]. This trend together with new indication for breast reconstruction like chest feminization in transgender patients [5,12,14] or the need to resolve the asymmetry of the contralateral breast [15,16,17], have increased the need for breast reconstruction surgery.
2.2. Mastectomy vs. Breast-conserving surgery
Many breast cancer patients elect to have a radical mastectomy, rather than a conservative surgical procedure, even though they are perfect candidates for BCS, maintaining the high frequency of mastectomy. Patients opting for mastectomies over BCS usually do not choose taking into account histology, localization or aggressiveness of tumor, but rather more subjective reasons like lack of trust that BCS can offer the same likelihood of cure as a more extensive procedure [18] or fear of additional procedures. The surgeon’s recommendation is a key factor in the decision-making process, but it is overshadowed by the patient's fear of cancer [19].
2.3. Lymphadenectomy and sentinel-lymph node biopsy
Radical surgery for breast cancer is comprised of the excision of the tumor (mastectomy or various breast conserving techniques) and a procedure addressed to the axillary lymph nodes (inferior lymphadenectomy, extensive lymphadenectomy or identification and excision of the sentinel lymph nodes using radioactive material or intravital dyes like Indocyanine green or Methylene Blue). The extension of the excision of the lymphatic tissue can influence the results of the reconstruction of the breast in both immediate and delayed settings by increasing the number of complications. Complete axillary lymph node dissection has a more pronounced effect when compared to limited lymphadenectomy of sentinel lymph node excision and is associated with a greater probability of implant loss independent of associated radiotherapy [20,21]. There are studies that proved that the excision of each node increases the risk of reconstructive surgery complication by 4% [21]. The same study concluded that the removal of 4 or more lymph nodes can adversely affect the immediate reconstructive procedure by seroma formation or even implant loss [21]. However, the complications after immediate reconstruction of breast are associated with the use of implants. For this reason, in patients requiring axillary lymph node dissection, the oncoplastic surgeon should offer the autologous methods of reconstruction [20].
Half of the patients with mastectomy for breast cancer elect to undergo reconstructive surgery [22,23] due to aesthetics considerations and improved quality of life [24,25,26,27] through reduced body dysmorphia. Yet, following reconstruction, many patients experience sequelae like functional limitations of upper limb (strength and mobility) and pain [27,28,29]. Axillary lymphadenectomy can cause neurological syndromes like pain and paresthesia and limitations of mobility after reconstructive surgery. This effect can be reduced by preserving the sensitive nerves during lymphadenectomy [30].
2.4. Impact of radiotherapy in surgical options and results
After reconstructive surgery, radiation therapy may affect the aspect of the operated breast, including altered skin color and rigidity. It can also lead to capsular contraction which mandates the removal of implant. Patients undergoing radiation therapy after reconstructive surgery need to be advised about the possibility of additional corrective surgery[31].
2.5. Quality of life following surgery for breast cancer
After mastectomy, patient report a significant alteration of quality of life (QoL) through a series of mechanisms: body dysmorphia affecting both emotional and sexual functioning, especially in younger patients [32], pain and limited mobility in ipsilateral upper limb, phycological effects like negative emotions as sadness, low mood, dejection [33]. Although, there is a significant reduction of the alteration of QoL following immediate breast reconstruction, many women tend to underestimate the impact of the mastectomy and to be overly optimistic about the impact of reconstructive surgery, and a significant part of them (up to 20 % in some studies) come to regret breast reconstruction [32,34]. This particular aspect needs to be taken into account when discussing breast reconstruction with the patients in order to make sure she has realistic expectations.
When discussing QoL in patients who underwent mastectomies, we can’t leave out the problems caused by breast asymmetry especially in large size breasts, leading to alterations of the skeletal system (like scoliosis). Asymmetry of breast can occur even in patients with reconstructive surgery after mastectomy, when the procedure was unilateral and was done with implants. The remaining breast tends to be more ptotic, resulting in undesired aesthetic effects and causing the patient to request corrective surgery of contralateral breast.
2.6. Oncologic follow-up and results after reconstructive surgery
Breast reconstruction surgery is a safe procedure from the oncological point of view, regardless of using an autologous or implant-based method for reconstruction and regardless of immediate or delayed timing of procedure [35], and does not increase the local or systemic recurrence rates or disease-free and overall survival [36,37]. The type of reconstructive surgery after mastectomy does not influence the recurrence rate independent of aggressive histology of tumor [38], lymphatic invasion and positive resection margins [39].
Another safety concern after breast reconstruction following radical mastectomy is the possibility of detection of recurrence, since autologous tissue below the skin flap may interfere with the detection of recurrent nodules, and fatty necrosis can confuse the diagnostic [40,41]. Recurrence after reconstructive surgery using implants may be challenging to detect beneath the implant [42].
3. Breast reconstruction
3.1. Timing of breast reconstruction – immediate or delayed
Breast reconstruction is classified by type and time of surgery. Immediate reconstruction takes place at the same time as mastectomy, and secondary (or delayed) reconstruction is performed from a few months to several years away from mastectomy. Currently, it is performed at least three months after the end of radiotherapy and generally at about a year after it [43]. The two main types of reconstruction are with implant or autologous tissue; they can also be used together in mixed procedures.
Immediate breast reconstruction (Figure 1.) has certain benefits over the secondary one, especially in terms of patient satisfaction, quality of life and psychological status post-mastectomy [44]. These patients are relatively more protected from the psychological effect of mastectomy and studies have shown a stable evolution of quality of life and satisfaction of this group compared to patients receiving delayed reconstruction [45,46]. In the latter case, the quality of life is significantly improved with the reconstructive procedures, ultimately the results being equalized in the long run [47]. Also, after the immediate reconstruction, a more natural and aesthetic result is obtained, the intervention being usually associated with a skin-sparing mastectomy, which respects the inframammary groove and keeps the skin intact, intervention proven safe from the oncological point of view by a series of studies, provided the correct selection of patients [48,49,50,51]. An important factor for selection is the appreciation of the thickness of the skin flap, this being correlated with the aesthetic results and with the possible postoperative complications [52]. Patients undergo fewer major surgeries and require fewer days of hospitalization, recovering faster postoperatively. From an oncological point of view, immediate reconstruction is considered safe and has been shown not to increase the risk of local recurrence compared to mastectomy without reconstruction [53,54], at the same time, this technique does not change the effectiveness of adjuvant radiotherapy [55].
Despite the many benefits of immediate reconstruction, many surgeons choose to postpone the operation for a secondary time (Figure 2.), often for reasons of oncological safety. The definite diagnosis of malignancy of radiologically detected breast tumors is made more and more frequently by guided biopsy, and the real extension of the tumor tissue can be evaluated macroscopically only intraoperatively, and microscopically only when examining the mastectomy piece. Thus, the subsequent therapeutic attitude is often decided intraoperatively [56]. However, in order to evaluate the quality and thickness of the skin flap intended for immediate breast reconstruction, mammography, breast ultrasound and magnetic resonance imaging (MRI) can be used preoperatively to complete the clinical examination. The results of these investigations guide the decision on surgery for immediate breast reconstruction and have been shown to be true to intraoperative findings. The thickness of the flap is important in choosing the type of implant used, but also for avoiding postoperative complications such as skin necrosis. [52].
The indications of radiotherapy, typically applied to patients at high risk of recurrence (> 4 positive lymph nodes or positive resection margins), tend to expand, studies proving its usefulness in patients with 1-3 positive lymph nodes [57,58,59]. Although radiotherapy does not contraindicate immediate reconstruction, the higher rate of complications, especially in implant-only reconstructions, is a second reason why in these patients either a two-stage reconstruction or a delayed reconstruction is chosen [60].
3.2. Two-stage breast reconstruction
In 2002, the technique of two-stage breast reconstruction was initially described, especially to improve the results in cases associated with radiotherapy [61]. The ionizing radiation used on either the chest wall or the axilla irreversibly alters the tissues in the irradiated field, regardless of their nature. In the short term, erythema and scaling of the skin can appear, and in the long-term severe fibrosis, telangiectasia, hyperpigmentation and tissue atrophy [62]. Under these conditions, many surgeons prefer to place a tissue expander at the time of mastectomy, preserved during radiotherapy, which aims to maintain both the shape and the skin needed for final reconstruction [63]. The expander can be filled at the time of the intervention, or progressively, subsequently, depending on the condition of the flaps and the center where the intervention is carried out [64]. It can be partially emptied before radiotherapy sessions, in order to favor the alignment of the irradiation fields, but this step is not always necessary [65]. Subsequently - it is recommended no later than 3 months after the completion of radiotherapy - the second stage of reconstruction is done, usually with autologous tissue. For patients who do not require adjuvant radiotherapy, the recommendation is that the second stage of reconstruction be performed no later than two weeks after mastectomy [60].
3.3. Breast reconstruction with implant
Regarding the type of intervention, at present, it is estimated that 80% of breast reconstructions are performed with an implant [63]. This type of intervention is shorter, easier from a technical point of view, and postoperative recovery is faster. In the long run, however, complications are more common than those in cases of breast augmentation (30% at 5 years compared to 12% at 5 years) and are accentuated by the history of radiation therapy [64,65]. The main complications are capsular contracture, implant rupture, hematoma, and infections [66]. They remain preferred for many surgeons because they avoid the complications of the donor areas and generate lower costs, and in the absence of radiotherapy or in a two-stage reconstruction, it is a simple solution with good aesthetic results. Acellular dermal matrices (ADMs) are used either as a first intention to support the implant in the lower pole, not covered by the pectoralis major, or in reinterventions [67]. These biological materials are made from human, bovine or porcine dermis processed to remove all cellular components - which can generate an immune response - and keeping the extracellular matrix containing mainly collagen (85%) along with proteoglycans, glycosaminoglycans and elastin, arranged in a network, in the meshes of which the host cells are arranged [68]. This integration of the matrix provides good support for the breast prosthesis and a high-quality capsule, resulting in a natural appearance of the final reconstructed breast. The high costs are the main disadvantage and make dermal substitutes inaccessible on a large scale. With the increase in accessibility, it is estimated that the approach to implant reconstructions in a single stage will change significantly.
3.4. Autologous breast reconstruction techniques
Autologous techniques are considered by many authors the gold standard in breast reconstruction. They consist in restoring the contour and volume of the mammary gland with the help of either rotating, pediculated flaps, which retain their vascular source, or micro-surgically freely transferred from other areas of the body, most often from the abdomen. The intervention can be performed immediately or delayed, like the implant reconstruction. Moreover, if the volume provided by the flap is not sufficient, other techniques such as free transfer of autologous fat (lipofilling) or placement of an implant may be associated [69].
- The advantages of flap reconstruction
Flap reconstruction offers several advantages, including improving the quality of irradiated tissue by bringing healthy tissue into a scar area; the final appearance after reconstruction is a natural one that mimics in time the physiological ptosis of the contralateral breast, does not require reinterventions for replacement after a period of time, can be used in patients who do not want or do not tolerate an implant and is the recommended type of reconstruction for the radio-treated patients [70].
- b. Types of transferred free flaps
First described in 1989 by Koshima and Soeda [71], the freely transferred flap based on the inferior epigastric artery (DIEP) has long become the preferred alternative in autologous breast reconstruction in specialized centers [71]. Other free flaps described, but rarely used in practice are TRAM (transverse rectus abdominis myocutaneous flap) - more commonly used in its pediculated version; TUG (transverse upper gracilis flap); SGAP (upper gluteal artery perforator flap) or IGAP (lower gluteal artery flap). Lower limb flaps are indicated in selected cases, in the absence of a suitable abdominal donor area or in patients with previous interventions at this level [72].
- c) Latissimus dorsi pediculated flap
First described by Tansini for covering chest wall defects in 1906, the latissimus dorsi pediculated flap began to be used in breast reconstruction after almost 70 years [73]. Until the middle of the twentieth century, the radical mastectomy technique described by Halsted recommended either grafting or second-hand healing of the resulting defect, strongly contraindicating any form of reconstruction, as it was considered to "hide possible recurrences and promote the spread of tumor cells" [74].
The evolution of oncological treatments, a better understanding of the pathology and the increase of patients' life expectancy, together with the appearance of breast implants changed the approach of these cases, so that Schneider and Botswick described, in 1977 and 1978 respectively, the latissimus dorsi flap accompanied by the implant in restoring the physiological contour and ptosis of the breast after a mastectomy [75,76]. Subsequently, Papp and McCraw modified the flap, including subcutaneous adipose tissue overlying the muscle, in order to achieve implant-free reconstruction [77].
Although no longer the gold standard in autologous reconstruction, the reliability and predictability of its anatomy still make it preferred by many surgeons for delayed reconstructions and also the preferred rescue option in the event of free transfer flaps failure [78]. Currently, its primary indications are in patients who do not have sufficient reserves for a free flap, with a personal history of abdominal interventions, or with significant comorbidities such as obesity, diabetes or in smoking patients [79].
The most common complications are seromas in the donor area, usually easy to treat without further intervention. Associated with alloplastic procedures, capsular contracture has been described more frequently in association with implants and less frequently in two-stage reconstructions, when the implant is preceded by an expander. Rare complications are contour defects in the donor area, limited shoulder mobility, decreased muscle strength in the arm and the scapula alatae [80].
4. Discussion
Breast surgery has rapidly evolved in parallel with oncological treatments, so if in 1970 the safety of reconstruction after a mastectomy was still questioned, today it is indicated for most patients who want it, so today the task of choosing the most appropriate technique for each case is on the shoulders of the surgeon. With all the options available, the surgeon chooses the right technique taking into account his own experience and preference, available resources and factors related to the patient, such as breast size to be reconstructed, skin quality, type of mastectomy indicated, disease stage, adjuvant treatments, surgical history, the general condition of the patient and last but not least her preference.
The contraindications of reconstruction are relatively few, limited to patients with a precarious general condition, which do not allow an elective intervention, as well as cases with a definite unfavorable life prognosis, which do not justify additional interventions. Also, patients with unrealistic expectations about the end result or who do not accept postoperative scars are not good candidates for reconstruction [81]. Age is no longer considered a contraindication to either the procedure itself or the choice of surgical technique, although, for reasons beyond the general condition and possible associated diseases, techniques involving freely transferred flaps are not usually indicated in patients over 65 years [43].
Oncological surgery, tumorectomy or mastectomy, as the case may be, contribute significantly to the end result. The decision on whether or not to preserve the mammary gland in early cases is still a matter of debate. A study by Veronesi et al [82] followed the evolution of 700 women with tumors <2cm for 20 years showed that breast preservation interventions (tumorectomies / lumpectomies) do not change the long-term survival when compared to mastectomies, although the local recurrence rate is higher in the first situation; Morrow and co-workers [83] also showed that, for stages 0-II, a third of patients end up requiring a mastectomy. The American Society of Breast Surgery has recommended breast preservation whenever possible, and the association with adjuvant oncological treatments such as chemo- and radiotherapy [84]. However, more recent data from the United States show an increase in the preference for mastectomies, especially prophylactic, in patients with and without BRCA 1/2 mutations [85].
The long-term benefit of this radical gesture has been demonstrated in cases with the presence of mutations, or in familial cases, in studies such as that performed by Boughey et al [86], which followed a group of 385 women with a family history and stage I or II tumors, and noting that, after 17 years, survival was significantly improved in patients with bilateral mastectomy, while another study by the same author [87] shows that bilateral mastectomy increases hospitalization costs and the number of on-call visits in the first 2 years, recommending that these data be explained to patients before making a decision.
Hoskin et al [88] conducted a study in the USA on 3195 women operated for breast tumors over a period of 5 years, between 2009 and 2014. Of the patients who required mastectomy, the proportion of patients who opted for immediate reconstruction increased by 31%. The percentage of prophylactic bilateral mastectomies with immediate reconstruction increased by 20%, while for the same intervention, but without reconstruction, the percentage decreased by 10%, from 22 to 12%.
Complications after intervention are not significantly different between tumoral and healthy breasts, but in the case of bilateral procedures, the complication rate increases significantly compared to unilateral ones, from 6.3% to 10.6%, according to some authors [89], respectively from 4.2% at 7.6%, according to other studies [90], this aspect being one of the main criticisms brought to this trend.
Statistics on the incidence of breast cancer in Romania are limited. The existence of a national patient record that would include, among other things, the stage at the time of diagnosis, would contribute to the understanding of epidemiology and would facilitate a unified, multidisciplinary approach and faster access of patients to treatments. From the experience of oncological surgery centers, many patients with breast cancer who present for treatment are detected in advanced stages locally, with larger tumors and often with clinically or radiological lymph node involvement. This situation significantly changes the surgical indications and, implicitly, the reconstructive options. Although surgical excision is sometimes possible primarily through the radical mastectomy technique, patients usually receive neoadjuvant chemotherapy. Given the stage of the disease, reconstruction in such cases is most often delayed until the completion of oncological treatments [91]. However, the evolution in the diagnosis and treatment of breast cancer has led to the development of oncoplastic surgery that allows not only the preservation of the breast, but also to obtain better aesthetic results in oncological safety conditions [92].
A number of studies have evaluated the safety of immediate breast reconstruction in neoadjuvant-treated patients with favorable results. A meta-analysis conducted in 2020 by Varghese et al [93], evaluates 17 observational studies, comprising of 3429 cases and reveals that it does not increase the risks of perioperative complications such as hematoma, seroma or difficult wound healing and does not delay adjuvant treatment. The study, instead, showed a lower rate of complications in younger patients, as well as a higher complications rate in patients who smoke or have a high body mass index. Also, patients with large breasts (> 600g) had a higher complication rate. Neoadjuvant chemotherapy slightly increases the risk of complications related to implant or expander and insignificant risks related to autologous procedures, the same authors note.
The effect of adjuvant chemotherapy on the results of reconstruction is difficult to estimate, as most patients also benefit from radiation therapy during treatment. One study showed a relative risk of liponecrosis of 4.8 in cases where immediate reconstruction with free flap was performed [94].
Radiation therapy, with its increasingly varied indications in the context of breast cancer, significantly changes postoperative outcomes. The impact on the complications of reconstruction is significantly increased in the case of alloplastic procedures, better results being observed in autologous reconstructions. El-Sabawi and colleagues [95] performed a systematic analysis on radiotherapy-treated patients in which they observed that those with autologous reconstruction had a lower rate of postoperative complications (30.9% vs. 41.3%) with the prevalence of complications related to wound healing, hematomas, and seromas, while infections and reinterventions prevailed in cases where the implant was used. The failure of the intervention occurred in 16.8% for alloplastic procedures and only 1.6% for autologous ones. When radiotherapy was performed on the temporary device, the complication rate was higher than when it was performed on the permanent implant (18.8% and 14.4% respectively).
Among the autologous procedures, the latissimus dorsi myocutaneous flap has long been the basic choice for reconstruction, associated or not with an implant. Almost any patient can benefit from this technique due to the reliability and versatility of this flap. The main controversies are related to the transferred volume, the aesthetic result and the secondary functional deficit of the shoulder and arm.
As early as 1986, Russel and colleagues [96] observed that although there is a decrease in scapular girdle muscle function immediately postoperatively and this effect may be more evident in athletic or elderly patients, this deficit does not have a significant impact on daily activities - except in athletes, skiers, swimmers, climbers - and fades in about 6 months due to the development of synergistic musculature. In a 2015 study, Yang and colleagues [97] showed that at 3 months, muscle strength was comparable to preoperative levels, but the limitation of activity and patients' perception remained altered until about 1 year after surgery.
Regarding the aesthetic result of the reconstruction, Lindegren and collaborators [98] conducted a study on 70 irradiated patients who benefited from secondary autologous reconstruction. The study compared the perception of patients and surgeons on the results after latissimus dorsi flap or DIEP. Surgeons preferred results after DIEP, because of the natural shape and volume of the breast, however, patients were more satisfied with the results of the latissimus dorsi flap, an unexpected result by the authors, probably correlated with the higher satisfaction in the latter case regarding the scar of the donor area. Another study had the opposite results, on a larger group of patients, but a small percentage of irradiated patients [99].
The appropriate volume for larger breasts can be recreated either by a combination with the implant or by serial lipofilling sessions or changing the skin palette to include more subcutaneous adipose tissue [100].
5. Conclusions
Breast reconstruction has become a necessary step in the treatment of most breast cancers and many reconstructive techniques are now routinely practiced. Microsurgical techniques are considered the "gold standard", but they are not accessible to all services, from a technical or financial point of view, so pediculated flaps remain the safe and reliable option, along with alloplastic procedures, to improve the quality of life of these patients.
Author Contributions
Conceptualization, I-M.D. and L.S.; methodology, I-M.D. and I.P.; validation, S-O.I. and C.C.; data curation, H.D., C.C., D.L.S., A.S.G. and D.L.; writing—original draft preparation, I-M.D., E.C. and V.R; writing—review and editing, E.C. and V.R.; supervision, L.S. and D-C.S.; project administration, L.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of Bucharest Oncological Institute “Prof. Dr. Alexandru Trestioreanu” (approval number 9676 from 31st of July 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. All the photos included come from the authors' collection (I.P.) and the consent of the respective patients was specifically obtained to use these photos for scientific purposes.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO Statistics on Breast Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/breast-cancer (accessed on 22 July 2023).
- Kummerow, K.L.; Du, L.; Penson, D.F.; Shyr, Y.; Hooks, M.A. Nationwide Trends in Mastectomy for Early-Stage Breast Cancer. JAMA Surg 2015, 150, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, T.M.; Habermann, E.B.; Grund, E.H.; Morris, T.J.; Virnig, B.A. Increasing Use of Contralateral Prophylactic Mastectomy for Breast Cancer Patients: A Trend toward More Aggressive Surgical Treatment. J Clin Oncol. 2007, 25, 5203–5209. [Google Scholar] [CrossRef]
- Soran, A.; Kamali Polat, A.; Johnson, R.; McGuire, K.P. Increasing Trend of Contralateral Prophylactic Mastectomy: What Are the Factors behind This Phenomenon? Surgeon. 2014, 12, 316–322. [Google Scholar] [CrossRef]
- Patel, H.; Samaha, Y.; Ives, G.; Lee, T.-Y.; Cui, X.; Ray, E. Chest Feminization in Male-to-Female Transgender Patients: A Review of Options. [CrossRef]
- Ferlay, J.; Steliarova-Foucher, E.; Lortet-Tieulent, J.; Rosso, S.; Coebergh, J.W.W.; Comber, H.; Forman, D.; Bray, F. Cancer Incidence and Mortality Patterns in Europe: Estimates for 40 Countries in 2012. Eur J Cancer 2013, 49, 1374–1403. [Google Scholar] [CrossRef] [PubMed]
- Sancho-Garnier, H.; Colonna, M. Epidémiologie Des Cancers Du Sein Breast Cancer Epidemiology. 2019.
- Overview of Breast Reconstruction – UpToDate. Available online: https://www.uptodate.com/contents/overview-of-breast-reconstruction?search=Overview%20of%20breast%20reconstruction&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 (accessed on 21 July 2023).
- Angelos, P.; Kohler, L.; Professor, A.; Bedrosian, I.; Euhus, D.M.; Herrmann, V.M.; Katz, S.J.; Pusic, A.; Surg, A.; Author, O. Prophylactic Mastectomy: Challenging Considerations for the Surgeon HHS Public Access Author Manuscript. Ann Surg Oncol 2015, 22, 3208–3212. [Google Scholar] [CrossRef] [PubMed]
- Dragun, A.E.; Pan, J.; Riley, E.C.; Kruse, B.; Wilson, M.R.; Rai, S.; Jain, D. Increasing Use of Elective Mastectomy and Contralateral Prophylactic Surgery among Breast Conservation Candidates: A 14-Year Report from a Comprehensive Cancer Center. Am J Clin Oncol. 2013, 36, 375–380. [Google Scholar] [CrossRef]
- Metcalfe, K.A.; Eisen, A.; Poll, A.; Candib, A.; McCready, D.; Cil, T.; Wright, F.; Demsky, R.; Mancuso, T.; Sun, P.; et al. Frequency of Contralateral Prophylactic Mastectomy in Breast Cancer Patients with a Negative BRCA1 and BRCA2 Rapid Genetic Test Result. Ann Surg Oncol 2021, 28, 4967–4973. [Google Scholar] [CrossRef] [PubMed]
- Miller, T.J.; Wilson, S.C.; Massie, J.P.; Morrison, S.D.; Satterwhite, T. Breast Augmentation in Male-to-Female Transgender Patients: Technical Considerations and Outcomes. JPRAS Open 2019, 21, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Bekeny, J.C.; Zolper, E.G.; Fan, K.L.; Del Corral, G. Breast Augmentation for Transfeminine Patients: Methods, Complications, and Outcomes. Gland Surg 2020, 9, 788–796. [Google Scholar] [CrossRef]
- Bekeny, J.C.; Zolper, E.G.; Manrique, O.J.; Fan, K.L.; Corral, G. Del Breast Augmentation in the Transgender Patient: Narrative Review of Current Techniques and Complications. Ann Transl Med 2021, 9, 611–611. [Google Scholar] [CrossRef]
- Khan, U.D. Preoperative Planning and Breast Implant Selection for Volume Difference Management in Asymmetrical Breasts. Plast Aesthet Res 2017, 4, 108–115. [Google Scholar] [CrossRef]
- Patlazhan, G.; Shkolnaya, O.; Torubarov, I.; Gomes, M. Our 10 Years’ Experience in Breast Asymmetry Correction. Aesthetic Plast Surg 2020, 44, 706–715. [Google Scholar] [CrossRef]
- Peterson, B.; Alajmi, H.; Ladak, A.; Samargandi, O.A. Breast Equalization Augmentation: The Use of Ultrasonic Assisted Liposuction for Correction of Primary Breast Asymmetry with Bilateral Augmentation. Aesthetic Plast Surg 2022, 46, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Benedict, S.; Cole, D.J.; Baron, L.; Baron, P. Factors Influencing Choice Between Mastectomy and Lumpectomy for Women in the Carolinas; 2001; Vol. 76;
- Nold, R.J.; Beamer, R.L.; Helmer, S.D.; McBoyle, M.F. Factors Influencing a Woman’s Choice to Undergo Breast-Conserving Surgery versus Modified Radical Mastectomy. Am J Surg 2000, 180, 413–418. [Google Scholar] [CrossRef]
- Wang, F.; Peled, A.W.; Chin, R.; Fowble, B.; Alvarado, M.; Ewing, C.; Esserman, L.; Foster, R.; Sbitany, H. The Impact of Radiation Therapy, Lymph Node Dissection, and Hormonal Therapy on Outcomes of Tissue Expander-Implant Exchange in Prosthetic Breast Reconstruction. Plast Reconstr Surg 2016, 137, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Verma, R.; Klein, G.; Dagum, A.; Khan, S.; Bui, D.T. The Effect of Axillary Lymph Node Sampling during Mastectomy on Immediate Alloplastic Breast Reconstruction Complications. In Proceedings of the Plastic and Reconstructive Surgery - Global Open; Lippincott Williams and Wilkins, May 1 2019; Vol. 7; p. 2224. [Google Scholar]
- Morrow, M.; Li, Y.; Alderman, A.K.; Jagsi, R.; Hamilton, A.S.; Graff, J.J.; Hawley, S.T.; Katz, S.J. Access to Breast Reconstruction After Mastectomy and Patient Perspectives on Reconstruction Decision Making. JAMA Surg 2014, 149, 1015–1021. [Google Scholar] [CrossRef]
- Steffen, L.E.; Johnson, A.; Levine, B.J.; Mayer, D.K.; Avis, N.E. Met and Unmet Expectations for Breast Reconstruction in Early Posttreatment Breast Cancer Survivors. Plastic Surgical Nursing 2017, 37, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, E.G.; Cederna, P.S.; Lowery, J.C.; Davis, J.A.; Myra Kim, H.; Roth, R.S.; Goldfarb, S.; Izenberg, P.H.; Houin, H.P.; Shaheen, K.W.; et al. Prospective Analysis of Psychosocial Outcomes in Breast Reconstruction: One-Year Postoperative Results from the Michigan Breast Reconstruction Outcome Study; 2000; Vol. 106;
- Rubino, C.; Figus, A.; Lorettu, L.; Sechi, G. Post-Mastectomy Reconstruction: A Comparative Analysis on Psychosocial and Psychopathological Outcomes. Journal of Plastic, Reconstructive and Aesthetic Surgery 2007, 60, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Helms, R.L.; O’Hea, E.L.; Corso, M. Helms, R.L.; O’Hea, E.L.; Corso, M. Body Image Issues in Women with Breast Cancer. 2008, 13, 313–325. [CrossRef]
- Reddy, K.G.; Strassle, P.D.; McGuire, K.P. Role of Age, Tumor Grade, and Radiation Therapy on Immediate Postmastectomy Breast Reconstruction. Clin Breast Cancer 2018, 18, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.U.; Day, S.J.; Pencek, M.; Roussel, L.O.; Christiano, J.G.; Punekar, I.R.; Koltz, P.F.; Langstein, H.N. Functional Return after Implant-Based Breast Reconstruction: A Prospective Study of Objective and Patient-Reported Outcomes. J Plast Reconstr Aesthet Surg 2020, 73, 850–855. [Google Scholar] [CrossRef] [PubMed]
- Myung, Y.; Choi, B.; Kwon, H.; Heo, C.Y.; Kim, E.K.; Kang, E.; Jeong, J.H.; Yang, E.J. Quantitative Analysis of Shoulder Function and Strength after Breast Reconstruction: A Retrospective Cohort Study. Medicine 2018, 97. [Google Scholar] [CrossRef]
- Rotaru, V.; Chitoran, E.; Cirimbei, C.; Cirimbei, S.; Simion, L. Preservation of Sensory Nerves During Axillary Lymphadenectomy, Proceedings of the 35th Balkan Medical Week, Athens, Greece, 25-27 September 2018 Available online:. Available online: https://www.webofscience.com/wos/woscc/full-record/WOS:000471903700045 (accessed on 20 July 2023).
- Doherty, C.; Mcclure, J.A.; Baxter, N.N.; Brackstone, M. Complications From Postmastectomy Radiation Therapy in Patients Undergoing Immediate Breast Reconstruction: A Population-Based Study-NC-ND License (Http://Creativecommons.Org/Licenses/by-Nc-Nd/4.0/). 2023. [CrossRef]
- Fortunato, L.; Loreti, A.; Cortese, G.; Spallone, D.; Toto, V.; Cavaliere, F.; Farina, M.; La Pinta, M.; Manna, E.; Detto, L.; et al. Regret and Quality of Life After Mastectomy With or Without Reconstruction. Clin Breast Cancer 2021, 21, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Kuliński, W.; Kosno, M. QUALITY OF LIFE IN WOMEN AFTER MASTECTOMY. CLINICAL AND SOCIAL STUDY. Wiad Lek 2021, 74, 429–435. [Google Scholar] [CrossRef]
- Lee, C.N.H.; Pignone, M.P.; Deal, A.M.; Blizard, L.; Hunt, C.; Huh, R.; Liu, Y.J.; Ubel, P.A. Accuracy of Predictions of Patients with Breast Cancer of Future Well-Being after Immediate Breast Reconstruction. JAMA Surg 2018, 153. [Google Scholar] [CrossRef]
- Qin, Q.; Tan, Q.; Lian, B.; Mo, Q.; Huang, Z.; Wei, C. Postoperative Outcomes of Breast Reconstruction after Mastectomy A Retrospective Study. 2018. [CrossRef]
- De La Cruz, L.; Moody, A.M.; Tappy, E.E.; Blankenship, S.A.; Hecht, E.M. Overall Survival, Disease-Free Survival, Local Recurrence, and Nipple–Areolar Recurrence in the Setting of Nipple-Sparing Mastectomy: A Meta-Analysis and Systematic Review. Ann Surg Oncol 2015, 22, 3241–3249. [Google Scholar] [CrossRef] [PubMed]
- Petit, J.Y.; Gentilini, O.; Rotmensz, N.; Rey, P.; Rietjens, M.; Garusi, C.; Botteri, E.; De Lorenzi, F.; Martella, S.; Bosco, R.; et al. Oncological Results of Immediate Breast Reconstruction: Long Term Follow-up of a Large Series at a Single Institution. Breast Cancer Res Treat 2008, 112, 545–549. [Google Scholar] [CrossRef]
- Ha, J.H.; Hong, K.Y.; Lee, H.B.; Moon, H.G.; Han, W.; Noh, D.Y.; Lim, J.; Yoon, S.; Chang, H.; Jin, U.S. Oncologic Outcomes after Immediate Breast Reconstruction Following Mastectomy: Comparison of Implant and Flap Using Propensity Score Matching. BMC Cancer 2020, 20. [Google Scholar] [CrossRef]
- Fujihara, M.; Yamasaki, R.; Ito, M.; Shien, T.; Maeda, R.; Kin, T.; Ueno, A.; Kajiwara, Y.; Kawasaki, K.; Ichimura, K.; et al. Risk Factors of Local Recurrence Following Implant-Based Breast Reconstruction in Breast Cancer Patients. BMC Women’s Health 2021, 21. [Google Scholar] [CrossRef]
- Mammography in the Evaluation of Masses in Breasts Reconstruction : Annals of Plastic Surgery. Available online: https://journals.lww.com/annalsplasticsurgery/Abstract/1998/09000/Mammography_in_the_Evaluation_of_Masses_in_Breasts.1.aspx (accessed on 22 July 2023).
- Hsu, W.; Sheen-Chen, S.M.; Eng, H.L.; Ko, S.F. Mammographic Microcalcification in an Autogenously Reconstructed Breast Simulating Recurrent Carcinoma. 2018, 94, 574–576. [CrossRef]
- Juanpere, S.; Perez, E.; Huc, O.; Motos, N.; Pont, J.; Pedraza, S. Imaging of Breast Implants—a Pictorial Review. Insights into Imaging 2011, 2, 653–670. [Google Scholar] [CrossRef]
- Mathelin, C.; Bruant-Rodier, C. Indications for Breast Reconstruction after Mastectomy According to the Oncological Situation. Annales de Chirurgie Plastique Esthetique 2018, 63, 580–584. [Google Scholar] [CrossRef]
- Atisha, D.; Alderman, A.K.; Lowery, J.C.; Kuhn, L.E.; Davis, J.; Wilkins, E.G. Prospective Analysis of Long-Term Psychosocial Outcomes in Breast Reconstruction: Two-Year Postoperative Results from the Michigan Breast Reconstruction Outcomes Study. Ann Surg 2008, 247, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Platt, J.; Zhong, T. Patient-Centered Breast Reconstruction Based on Health-Related Quality-of-Life Evidence. Clin Plast Surg 2018, 45, 137–143. [Google Scholar] [CrossRef]
- Zhong, T.; McCarthy, C.; Min, S.; Zhang, J.; Beber, B.; Pusic, A.L.; Hofer, S.O.P. Patient Satisfaction and Health-Related Quality of Life after Autologous Tissue Breast Reconstruction: A Prospective Analysis of Early Postoperative Outcomes. Cancer 2012, 118, 1701–1709. [Google Scholar] [CrossRef] [PubMed]
- Zhong, T.; Hu, J.; Bagher, S.; Vo, A.; O’Neill, A.C.; Butler, K.; Novak, C.B.; Hofer, S.O.P.; Metcalfe, K.A. A Comparison of Psychological Response, Body Image, Sexuality, and Quality of Life between Immediate and Delayed Autologous Tissue Breast Reconstruction: A Prospective Long-Term Outcome Study. In Proceedings of the Plastic and Reconstructive Surgery; Lippincott Williams and Wilkins, October 1 2016; Vol. 138; pp. 772–780. [Google Scholar]
- Simmons, R.M.; Fish, S.K.; Gayle, L.; La Trenta, G.S.; Swistel, A.; Christos, P.; Osborne, M.P. Local and Distant Recurrence Rates in Skin-Sparing Mastectomies Compared With Non-Skin-Sparing Mastectomies; 1999.
- Toth, B.A.; Lappert, P. Modified Skin Incisions for Mastectomy: The Need for Plastic Surgical Input in Preoperative Planning. Plast Reconstr Surg. 1991, 87, 1048–1053. [Google Scholar] [CrossRef]
- Kroll, S.; Khoo, A.; Singletary, E.; Ames, F.; Wang, B.G.; Reece, G.; Miller, M.; Evans, G.; Robb, G. Local Recurrence Risk after Skin-Sparing and Conventional Mastectomy: A 6-Year Follow-Up. Plast Reconstr Surg 1999, 104, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Galimberti, V.; Vicini, E.; Corso, G.; Morigi, C.; Fontana, S.; Sacchini, V.; Veronesi, P. Nipple-Sparing and Skin-Sparing Mastectomy: Review of Aims, Oncological Safety and Contraindications. Breast 2017, 34, S82–S84. [Google Scholar] [CrossRef] [PubMed]
- Radu, M.; Bordea, C.; Noditi, A.; Blidaru, A. Assessment of Mastectomy Skin Flaps for Immediate Implant-Based Breast Reconstruction. J Med Life 2018, 11, 137–145. [Google Scholar]
- Huang, C.J.; Hou, M.F.; Lin, S.D.; Chuang, H.Y.; Huang, M.Y.; Fu, O.Y.; Lian, S.L. Comparison of Local Recurrence and Distant Metastases between Breast Cancer Patients after Postmastectomy Radiotherapy with and without Immediate TRAM Flap Reconstruction. Plast Reconstr Surg 2006, 118, 1079–1086. [Google Scholar] [CrossRef]
- Gieni, M.; Avram, R.; Dickson, L.; Farrokhyar, F.; Lovrics, P.; Faidi, S.; Sne, N. Local Breast Cancer Recurrence after Mastectomy and Immediate Breast Reconstruction for Invasive Cancer: A Meta-Analysis. The Breast 2012, 21, 230–236. [Google Scholar] [CrossRef]
- Strålman, K.; Mollerup, C.L.; Kristoffersen, U.S.; Elberg, J.J. Long-Term Outcome after Mastectomy with Immediate Breast Reconstruction. Acta Oncol (Madr) 2008, 47, 704–708. [Google Scholar] [CrossRef] [PubMed]
- Kronowitz, S.J. Delayed-Immediate Breast Reconstruction: Technical and Timing Considerations. Plast Reconstr Surg 2010, 125, 463–474. [Google Scholar] [CrossRef]
- Gradishar, W.J.; Lurie, R.H.; Blair, S.L.; San Diego Moores Cancer Center Harold Burstein, U.J.; Center Amy Cyr, C.; Elias, A.D.; Forero, A.; Hermes Giordano, S.; Goldstein, L.J.; Isakoff, S.J.; et al. Invasive Breast Cancer NCCN Guidelines ® NCCN Breast Cancer Panel Members; 2016; Vol. 14;
- Harris, E.E.R.; Freilich, J.; Lin, H.Y.; Chuong, M.; Acs, G. The Impact of the Size of Nodal Metastases on Recurrence Risk in Breast Cancer Patients with 1-3 Positive Axillary Nodes after Mastectomy. Int J Radiat Oncol Biol Phys 2013, 85, 609–614. [Google Scholar] [CrossRef] [PubMed]
- McBride, A.; Allen, P.; Woodward, W.; Kim, M.; Kuerer, H.M.; Drinka, E.K.; Sahin, A.; Strom, E.A.; Buzdar, A.; Valero, V.; et al. Locoregional Recurrence Risk for Patients with T1,2 Breast Cancer with 1-3 Positive Lymph Nodes Treated with Mastectomy and Systemic Treatment. Int J Radiat Oncol Biol Phys 2014, 89, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Kronowitz, S.J.; Hunt, K.K.; Kuerer, H.M.; Babiera, G.; McNeese, M.D.; Buchholz, T.A.; Strom, E.A.; Robb, G.L. Delayed-Immediate Breast Reconstruction. Plast Reconstr Surg 2004, 113, 1617–1628. [Google Scholar] [CrossRef]
- See, M.S.F.; Farhadi, J. Radiation Therapy and Immediate Breast Reconstruction: Novel Approaches and Evidence Base for Radiation Effects on the Reconstructed Breast. Clin Plast Surg 2018, 45, 13–24. [Google Scholar] [CrossRef]
- Bellini, E.; Pesce, M.; Santi, P.L.; Raposio, E. Two-Stage Tissue-Expander Breast Reconstruction: A Focus on the Surgical Technique. Biomed Res Int 2017, 2017. [Google Scholar] [CrossRef]
- Cemal, Y.; Albornoz, C.R.; Disa, J.J.; Mccarthy, C.M.; Mehrara, B.J.; Pusic, A.L.; Cordeiro, P.G.; Matros, E. A Paradigm Shift in U.S. Breast Reconstruction: Part 2. the Influence of Changing Mastectomy Patterns on Reconstructive Rate and Method. Plast Reconstr Surg 2013, 131, 320e–326e. [Google Scholar] [CrossRef] [PubMed]
- Sherine, E.G.; Woods, J.E.; O’Fallon, M.; Beard, M.; Kurland, L.T.; Melton, J.L. Complications Leading to Surgery after Breast Implantation. New England Journal of Medicine 1997, 336, 677–682. [Google Scholar] [CrossRef]
- Percec, I.; Bucky, L.P. Successful Prosthetic Breast Reconstruction after Radiation Therapy. Ann Plast Surg 2008, 60, 527–531. [Google Scholar] [CrossRef]
- Thamm, O.C.; Andree, C. Immediate Versus Delayed Breast Reconstruction: Evolving Concepts and Evidence Base. Clin Plast Surg 2018, 45, 119–127. [Google Scholar] [CrossRef]
- Nahabedian, M.Y. Acellular Dermal Matrices in Primary Breast Reconstruction. Plast Reconstr Surg 2012, 130, 44S–53S. [Google Scholar] [CrossRef]
- Uitto, J.; Olsen, D.R.; Fazio, M.J. Extracellular Matrix of the Skin: 50 Years of Progress. Journal of Investigative Dermatology 1989, 92, S61–S77. [Google Scholar] [CrossRef]
- Ho, A.Y.; Hu, Z.I.; Mehrara, B.J.; Wilkins, E.G. Radiotherapy in the Setting of Breast Reconstruction: Types, Techniques, and Timing. Lancet Oncol 2017, 18, e742–e753. [Google Scholar] [CrossRef]
- Chen, V.W.; Lin, A.; Hoang, D.; Carey, J. Trends in Breast Reconstruction Techniques at a Large Safety Net Hospital: A 10-Year Institutional Review. Annals of Breast Surgery 2018, 2, 14–14. [Google Scholar] [CrossRef]
- Koshima, I.; Soeda, S. Inferior Epigastric Artery Skin Flaps without Rectus Abdominis Muscle. Journal of Plastic Surgery 1989, 42, 645–648. [Google Scholar] [CrossRef]
- Healy, C.; Allen, R.J. The Evolution of Perforator Flap Breast Reconstruction: Twenty Years after the First DIEP Flap. J Reconstr Microsurg 2014, 30, 121–126. [Google Scholar] [CrossRef]
- Maxwell, P. Iginio Tansini and the Origin of the Latissimus Dorsi Musculocutaneous Flap. Plast Reconstr Surg 1989, 65, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Champaneria, M.C.; Wong, W.W.; Hill, M.E.; Gupta, S.C. The Evolution of Breast Reconstruction: A Historical Perspective. World J Surg 2012, 36, 730–742. [Google Scholar] [CrossRef]
- Bostwick, J.; Vasconez, L.O.; Jurkiewicz, M.J. Breast Reconstruction after a Radical Mastectomy. Plast Reconstr Surg 1978, 61, 682–693. [Google Scholar] [CrossRef] [PubMed]
- Schneider, W.J.; Hill, H.L.; Brown, R.G. LATISSIMUS DORSI MYOCUTANEOUS FLAP FOR BREAST RECONSTRUCTION. Br J Plast Surg 1977, 30, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Papp, C.; McCraw, J.B. Autogenous Latissimus Breast Reconstruction. Clin Plast Surg 1998, 25, 261–266. [Google Scholar] [CrossRef]
- DeLong, M.R.; Tandon, V.J.; Rudkin, G.H.; Da Lio, A.L. Latissimus Dorsi Flap Breast Reconstruction-A Nationwide Inpatient Sample Review. Ann Plast Surg 2017, 78, S185–S188. [Google Scholar] [CrossRef] [PubMed]
- Spear, S.L.; Clemens, M.W. Latissimus Dorsi Flap Breast Reconstruction. Plastic Surgery. 3rd ed. 2012, 370–392. [Google Scholar]
- Hardwicke, J.T.; Prinsloo, D.J. An Analysis of 277 Consecutive Latissimus Dorsi Breast Reconstructions: A Focus on Capsular Contracture. Plast Reconstr Surg 2011, 128, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Warren, A.G.; Morris, D.J.; Houlihan, M.J.; Slavin, S.A. Breast Reconstruction in a Changing Breast Cancer Treatment Paradigm. Plast Reconstr Surg 2008, 121, 1116–1126. [Google Scholar] [CrossRef]
- Veronesi, U.; Cascinelli, N.; Mariani, L.; Greco, M.; Saccozzi, R.; Luini, A.; Aguilar, M.; Marubini, E. Twenty-Year Follow-up of a Randomized Study Comparing Breast-Conserving Surgery with Radical Mastectomy for Early Breast Cancer. N Engl J Med 2002, 347, 1227–1232. [Google Scholar] [CrossRef]
- Morrow, M.; Jagsi, R.; Alderman, A.K.; Griggs, J.J.; Hawley, S.T.; Hamilton, A.S.; Graff, J.J.; Katz, S.J. Surgeon Recommendations and Receipt of Mastectomy for Treatment of Breast Cancer. JAMA : the journal of the American Medical Association 2009, 302, 1551. [Google Scholar] [CrossRef]
- Boughey, J.C.; Attai, D.J.; Chen, S.L.; Cody, H.S.; Dietz, J.R.; Feldman, S.M.; Greenberg, C.C.; Kass, R.B.; Landercasper, J.; Lemaine, V.; et al. Contralateral Prophylactic Mastectomy (CPM) Consensus Statement from the American Society of Breast Surgeons: Data on CPM Outcomes and Risks. Ann Surg Oncol 2016, 23, 3100. [Google Scholar] [CrossRef]
- Panchal, H.; Matros, E. Current Trends in Postmastectomy Breast Reconstruction. Plast Reconstr Surg 2017, 140, 7S–13S. [Google Scholar] [CrossRef]
- Boughey, J.C.; Hoskin, T.L.; Degnim, A.C.; Sellers, T.A.; Johnson, J.L.; Kasner, M.J.; Hartmann, L.C.; Frost, M.H. Contralateral Prophylactic Mastectomy Is Associated with a Survival Advantage in High-Risk Women with a Personal History of Breast Cancer. Ann Surg Oncol 2010, 17, 2702. [Google Scholar] [CrossRef]
- Boughey, J.C.; Schilz, S.R.; Van Houten, H.K.; Zhu, L.; Habermann, E.B.; Lemaine, V. Contralateral Prophylactic Mastectomy with Immediate Breast Reconstruction Increases Healthcare Utilization and Cost. Ann Surg Oncol 2017, 24, 2957–2964. [Google Scholar] [CrossRef] [PubMed]
- Hoskin, T.L.; Hieken, T.J.; Degnim, A.C.; Jakub, J.W.; Jacobson, S.R.; Boughey, J.C. Use of Immediate Breast Reconstruction and Choice for Contralateral Prophylactic Mastectomy. Surgery 2016, 159, 1199–1209. [Google Scholar] [CrossRef] [PubMed]
- Erdahl, L.; Shah, A.R.; Boughey, J.C.; Hieken, T.J.; Hoskin, T.L.; Degnim, A.C. Comparison of Side-Specific Complications After Contra lateral Prophylactic Mastectomy vs. Treatment Mastectomy for Unilateral Breast Cancer. Ann Surg Oncol 2014, 37, 46–47. [Google Scholar]
- Osman, F.; Saleh, F.; Jackson, T.D.; Corrigan, M.A.; Cil, T. Increased Postoperative Complications in Bilateral Mastectomy Patients Compared to Unilateral Mastectomy: An Analysis of the NSQIP Database. Ann Surg Oncol 2013, 20, 3212–3217. [Google Scholar] [CrossRef]
- Jones, C.; Lancaster, R. Evolution of Operative Technique for Mastectomy. Surg Clin North Am 2018, 98, 835–844. [Google Scholar] [CrossRef]
- Blidaru, A.; Bordea, C.I.; Ichim, E.; El Houcheimi, B.; Matei Purge, I.; Noditi, A.; Sterie, I.; Gherghe, M.; Radu, M. Breast Cancer Surgery in Images. Chirurgia (Bucur) 2017, 112, 486–492. [Google Scholar] [CrossRef]
- Varghese, J.; Gohari, S.S.; Rizki, H.; Faheem, I.; Langridge, B.; Kümmel, S.; Johnson, L.; Schmid, P. A Systematic Review and Meta-Analysis on the Effect of Neoadjuvant Chemotherapy on Complications Following Immediate Breast Reconstruction. Breast 2021, 55, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Chen, Y.; Chen, J.; Chen, J.; Yang, B.; Li, J.; Huang, X.; Shen, Z.; Shao, Z.; Yu, P.; et al. Adjuvant Chemotherapy Increases the Prevalence of Fat Necrosis in Immediate Free Abdominal Flap Breast Reconstruction. J Plast Reconstr Aesthet Surg 2014, 67, 461–467. [Google Scholar] [CrossRef] [PubMed]
- El-Sabawi, B.; Sosin, M.; Carey, J.N.; Nahabedian, M.Y.; Patel, K.M. Breast Reconstruction and Adjuvant Therapy: A Systematic Review of Surgical Outcomes. J Surg Oncol 2015, 112, 458–464. [Google Scholar] [CrossRef]
- Russell, R.C.; Pribaz, J.; Zook, E.G.; Leighton, W.D.; Eriksson, E.; Smith, C.J. Functional Evaluation of Latissimus Dorsi Donor Site. Plast Reconstr Surg 1986, 78, 336–344. [Google Scholar] [CrossRef]
- Yang, J.D.; Huh, J.S.; Min, Y.S.; Kim, H.J.; Park, H.Y.; Jung, T. Du Physical and Functional Ability Recovery Patterns and Quality of Life after Immediate Autologous Latissimus Dorsi Breast Reconstruction: A 1-Year Prospective Observational Study. Plast Reconstr Surg 2015, 136, 1146–1154. [Google Scholar] [CrossRef] [PubMed]
- Lindegren, A.; Halle, M.; Docherty Skogh, A.C.; Edsander-Nord, A. Postmastectomy Breast Reconstruction in the Irradiated Breast: A Comparative Study of DIEP and Latissimus Dorsi Flap Outcome. Plast Reconstr Surg 2012, 130, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Yueh, J.H.; Slavin, S.A.; Adesiyun, T.; Nyame, T.T.; Gautam, S.; Morris, D.J.; Tobias, A.M.; Lee, B.T. Patient Satisfaction in Postmastectomy Breast Reconstruction: A Comparative Evaluation of DIEP, TRAM, Latissimus Flap, and Implant Techniques. Plast Reconstr Surg 2010, 125, 1585–1595. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Mohan, A.T.; Vijayasekaran, A.; Hou, C.; Sur, Y.J.; Morsy, M.; Saint-Cyr, M. Maximizing the Volume of Latissimus Dorsi Flap in Autologous Breast Reconstruction with Simultaneous Multisite Fat Grafting. Aesthet Surg J 2016, 36, 169–178. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Patient with stage Ia invasive ductal carcinoma of left breast and BRCA positive status – she underwent bilateral subcutaneous mastectomy with left sentinel lymph node identification using Indocyanine green followed by immediate bilateral reconstruction with 350 cc round implants: A and B. Aspect before reconstructive surgery; C. and D. Aspect at 3 months after reconstructive surgery.
Figure 1.
Patient with stage Ia invasive ductal carcinoma of left breast and BRCA positive status – she underwent bilateral subcutaneous mastectomy with left sentinel lymph node identification using Indocyanine green followed by immediate bilateral reconstruction with 350 cc round implants: A and B. Aspect before reconstructive surgery; C. and D. Aspect at 3 months after reconstructive surgery.

Figure 2.
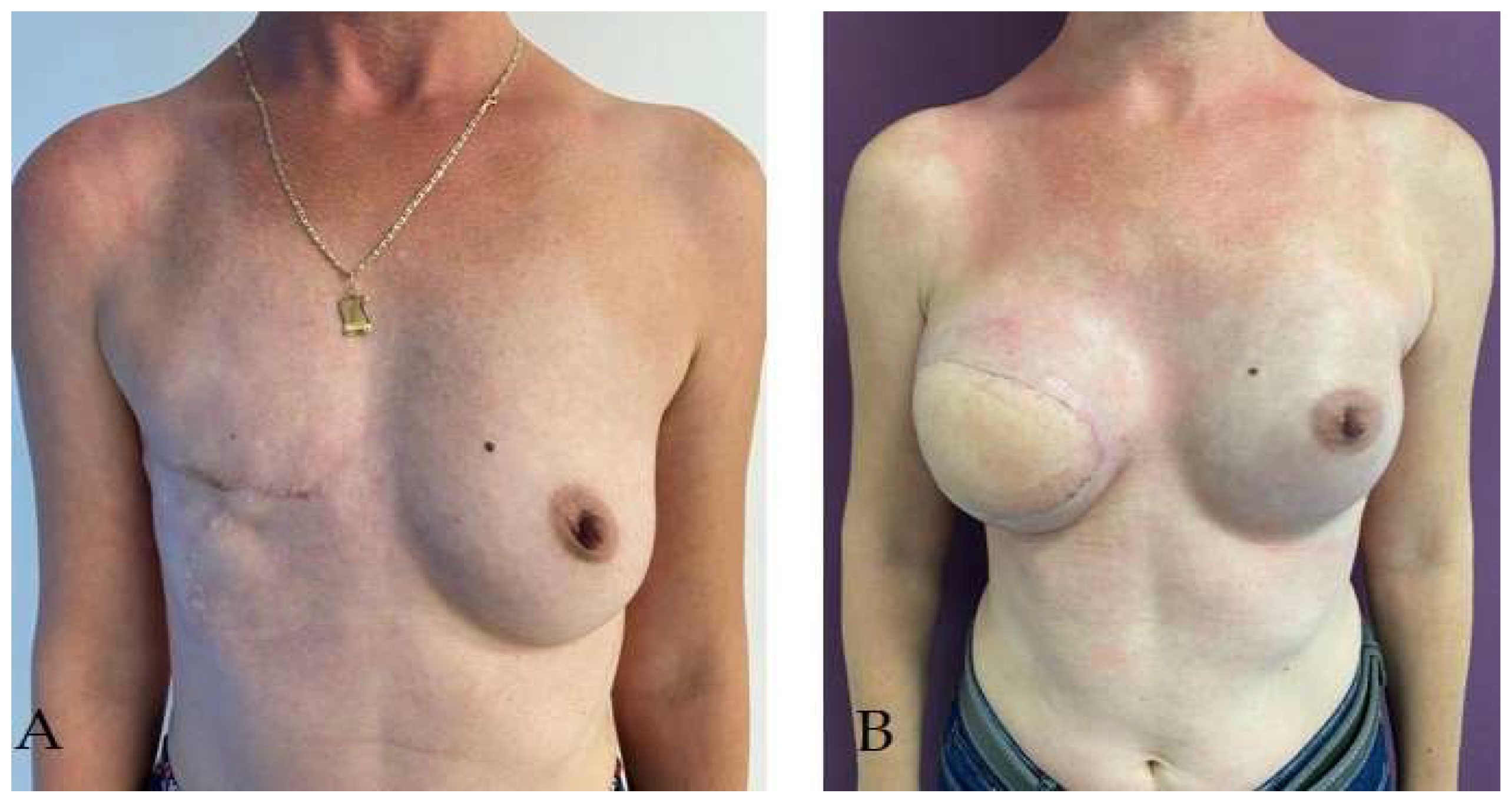
Patient with right radical mastectomy for breast cancer followed by radiotherapy – she underwent right breast delayed reconstruction using latissimus dorsi pediculated flap and a 225cc round implant. A. Aspect before reconstructive surgery; B. Aspect at 3 months after reconstructive surgery.
Figure 2.
Patient with right radical mastectomy for breast cancer followed by radiotherapy – she underwent right breast delayed reconstruction using latissimus dorsi pediculated flap and a 225cc round implant. A. Aspect before reconstructive surgery; B. Aspect at 3 months after reconstructive surgery.

Figure 3.
Patient with right radical mastectomy for breast cancer followed by radiotherapy – she underwent right breast delayed reconstruction using latissimus dorsi pediculated flap and a 320cc round implant simultaneous with prophylactic left subcutaneous mastectomy (due to BRCA positive status) with immediate reconstruction using a pediculated inferior dermoadipous flap and a 350cc round implant: A. Aspect before reconstructive surgery; B. Aspect at 3 months after reconstructive surgery.
Figure 3.
Patient with right radical mastectomy for breast cancer followed by radiotherapy – she underwent right breast delayed reconstruction using latissimus dorsi pediculated flap and a 320cc round implant simultaneous with prophylactic left subcutaneous mastectomy (due to BRCA positive status) with immediate reconstruction using a pediculated inferior dermoadipous flap and a 350cc round implant: A. Aspect before reconstructive surgery; B. Aspect at 3 months after reconstructive surgery.

Figure 4.
Bilateral prophylactic mastectomy in patient with BRCA positive status and heavy family history of breast cancer – immediate reconstruction using 325cc round implant and pediculated inferior dermoadipous flap followed by nipple-areola complex graft: A. Aspect before reconstructive surgery; B. Aspect at 3 months after reconstructive surgery; C. Final aspect at 32 months after reconstructive surgery.
Figure 4.
Bilateral prophylactic mastectomy in patient with BRCA positive status and heavy family history of breast cancer – immediate reconstruction using 325cc round implant and pediculated inferior dermoadipous flap followed by nipple-areola complex graft: A. Aspect before reconstructive surgery; B. Aspect at 3 months after reconstructive surgery; C. Final aspect at 32 months after reconstructive surgery.
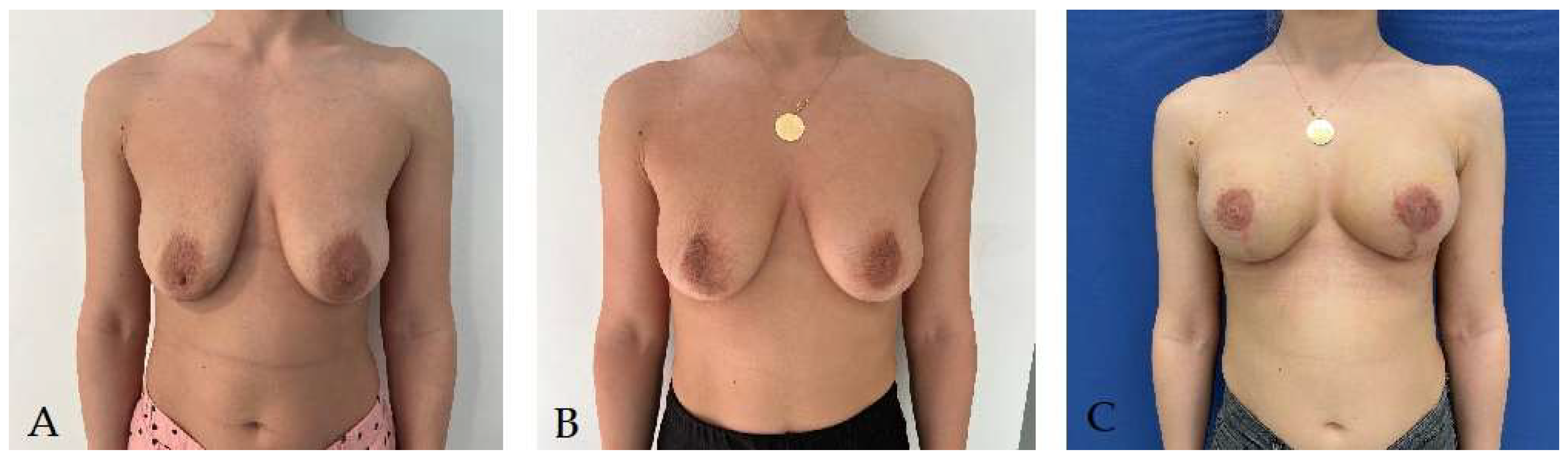
Figure 5.
Patient with right radical mastectomy for breast cancer – she underwent right breast delayed reconstruction using latissimus dorsi pediculated flap and a 275cc round implant simultaneous with prophylactic left subcutaneous mastectomy (due to BRCA positive status) with immediate reconstruction using a 325cc round implant: A. Aspect before reconstructive surgery; B. Aspect at 3 months after reconstructive surgery.
Figure 5.
Patient with right radical mastectomy for breast cancer – she underwent right breast delayed reconstruction using latissimus dorsi pediculated flap and a 275cc round implant simultaneous with prophylactic left subcutaneous mastectomy (due to BRCA positive status) with immediate reconstruction using a 325cc round implant: A. Aspect before reconstructive surgery; B. Aspect at 3 months after reconstructive surgery.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



