
Submitted:
06 September 2023
Posted:
08 September 2023
You are already at the latest version
Abstract
Preterm birth (PB) is a leading cause of perinatal morbidity and mortality. PB prediction is per-formed by measuring cervical length, with a detection rate of around 70%. Although it is known that a cytokine-mediated inflammatory process is involved in the pathophysiology of PB, no screening method implemented in clinical practice includes cytokine levels as a predictor varia-ble. Here, we quantified cytokines in cervical-vaginal mucus of pregnant women (18-23.6 weeks of gestation) with high- or low-risk for PB determined by cervical length, collecting relevant obstetric information. IL-2, IL-6, IFN-γ, IL-4, and IL-10 were significantly higher in the high-risk group, while IL-1ra was lower. Two different models for PB prediction were created using the Random Forest machine-learning algorithm: the full model with 12 clinical variables and cyto-kine values, and the adjusted model, including the most significant variables -maternal age, IL-2, and cervical length- (detection rate 66 vs 87%, false positive rate 12 vs 3.33%, false negative rate 28 vs 6.66%, and area under the curve 0.722 vs 0.875, respectively). The adjusted model integrat-ing cytokines showed a detection rate 8 points higher than the gold standard calculator, which may allow us to identify PB risk more accurately and implement strategies for preventive in-terventions
Keywords:
preterm delivery
; screening
; artificial intelligence
; inflammatory response
; interleukin-2
; cervical length
1. Introduction
Preterm birth is a major public health issue concerning perinatal mortality, long-term morbidity, and economic burden, with a worldwide prevalence of 5-18%, 90% of which occurs in developing countries [1,2]. Spontaneous preterm birth (SPB) is defined as the delivery of the fetus before 37 weeks’ gestation, calculated by the last menstrual period or reliable first-trimester ultrasound, without any medical intervention to induce this outcome [3]. Although evidence suggests that preterm labor is a heterogeneous condition triggered by multiple factors [4,5], the inflammatory response elicited at the maternal-fetal interface is considered a hallmark of the pathology. The increase in the local cytokine release that orchestrates the inflammatory response is observed cases with intrauterine infection and spontaneous preterm labor that is not associated with infection, thereby described as the intrauterine inflammatory response syndrome [6].
In vivo, cytokines are part of the molecular network mediating innate immune and inflammatory responses [7]. All cytokines expressed locally in the cervix participate in complex interactions with prostaglandins and nitric oxide, which regulate the production of extracellular matrix proteases and other factors associated with the cervical shortening, rupture of membranes, and uterine contractions that lead to labor either at preterm or term [6,8,9]. An increase in the pro-inflammatory cytokines IL-6 and IL-8 in the cervical-vaginal fluid has been associated with cervical effacement [10,11], while an increased TNF-α is associated with cervical ripening [12]. On the other hand, IL-10 concentration has been identified as the main anti-inflammatory cytokine involved in PB pathogenesis [13]. So far, the results of studies analyzing the relationship between cytokines and PB are inconsistent, and none have identified a biomarker that can accurately predict preterm delivery [7]. These inconsistencies can be explained by the complexity of the local inflammatory processes and the heterogeneity of the pathways that trigger PB.
There is a pathophysiological association between preterm premature rupture of membranes (PPROM) and PB, both triggered when the intrauterine or maternal environment is hostile. Moreover, PPROM is among the leading causes of preterm birth [14], probably due to the onset of an intrauterine infectious/inflammatory process, which produces an imbalance in cytokine production, disrupting the tight junctions of the membranes and rupturing the amniotic sac [15]. Some cytokines associated with PPROM and PB in placental tissue are IL-1β, IL-6, IL-8, and transforming growth factor (TGF-β) [16].
Among the screening techniques to detect women at high-risk for PB, the most used measurement in clinical practice is cervical length (CL), obtained by vaginal ultrasound in the second trimester of gestation, with a detection rate of 50 to 70%. Also, some clinical calculators incorporate CL, gestational age, and obstetric history to provide a patient-specific risk for developing PB. The calculator that is considered the gold standard in clinical practice is the Fetal Medicine Foundation (FMF) calculator, having a detection rate for preterm spontaneous birth <28 weeks = 75%, 28-30 weeks = 57%, 31-33 weeks = 46%, and 34-36 weeks = 24%, considering a false positive rate of 10% [17].
In recent years, artificial intelligence has been used in different healthcare fields to predict, prevent, diagnose, and monitor different pathologies, even in obstetrics [18]. Models using machine learning are more accurate than risk calculators as they analyze massive data and, through algorithms, identify patterns to make predictions [19]; furthermore, it has been proposed that machine learning models can be helpful in personalized pregnancy management, especially in low- and middle-income countries [18]. The goal of identifying women at high-risk for developing PB is to individualize the clinical follow-up and offer medical preventive strategies (e.g., progesterone) that reduce by up to 90% the risk of preterm birth in women with a history of this outcome and by 42% in pregnant women with short cervix detected in second-trimester screening [20].
Although the role of cytokines as critical mediators in the inflammatory process that triggers labor has been demonstrated [21], very few predictive models consider their measurement in the PB screening process [22,23,24]. However, none have been implemented in clinical practice. Therefore, this study aimed to characterize the cytokine profile in cervical-vaginal mucus in pregnant women with high- and low-risk for PB and then integrate them in a PB screening model using a predictive machine learning analysis.
2. Results
A total of 60 pregnant women were recruited, including 40 participants who were considered at low-risk and 20 at high-risk for PB. The low-risk group had a prevalence of spontaneous preterm birth before 37 gestation weeks of 7.5% versus 45% in the high-risk group. The maternal characteristics of both groups are shown in Table 1. The study groups were similar in age, maternal BMI, socioeconomic level, smoking, and gestational age at which CL was measured. As expected, CL was significantly lower in the group of women at high risk for PD (p = 0.02).
2.1. Cytokine profile in low- and high-risk for PB women
The mean concentration of the pro-inflammatory cytokines IL-2, IL-6, and IFN- γ were significantly higher in the high-risk group (p = 0.001). Regarding cytokines with anti-inflammatory function, an increase in the concentration of IL-4 and IL-10 was found in the women at high-risk for PB (p = 0.001). In contrast, the IL-1ra concentration was significantly lower (p < 0.01) compared to women in the low-risk for PB group. Table 2, Figure 1.
2.2. Machine learning predictive model
Two predictive models were generated by machine learning analysis. The full model, which included all predictor variables, showed a detection rate of 66%, with FPR = 12%, FNR = 28%, and an AUC of 0.722. The adjusted model that included only the most statistically significant variables (Maternal age, CL, and IL-2 concentration) showed a detection rate of 87%, with FPR = 3.33%, FNR = 6.66%, and an AUC of 0.875. To compare our model with the performance of the calculator used by the FMF, we entered our data in the FMF’s online calculator (https://fetalmedicine.org/research/assess/preterm/cervix), obtaining the following results: a detection rate of 79%, with FPR = 6.60%, FNR = 11.66% (Table 3, Figure 2). The relevance of each predictor in the adjusted model was 26% for maternal age, 38% for CL, and 36% for IL-2 concentration (Figure 2).
3. Discussion
In this study, we first focused on the characterization of inflammatory cytokine profiles in cervical-vaginal mucus in pregnant women with high- and low-risk for PB, as classified according to the CL measured in the second trimester of gestation. In agreement with previous reports, a higher concentration of IL-2, IL-6, and IFN-γ was found in the cervical-vaginal samples of the high-risk group, and a higher concentration of IL-1ra in the low-risk group [26,27,28].
On the other hand, IL-4 and IL-10 were found to be increased in the high-risk group, in contrast to what was expected according to the inflammatory pathogenesis of PB [29]. These differences could be explained by the complexity of the inflammatory processes involved in PB and owing to the different methodologies and designs used in other studies [30]. Elevation of anti-inflammatory cytokines in the high-risk group for PB could be a physiological attempt to moderate the inflammatory process to maintain homeostasis; this hypothesis was previously proposed by Wang et al., as they found that IL-37 (an anti-inflammatory cytokine) was elevated in the fetal membranes of women with preterm labor, as an attempt to stop the inflammatory process caused by IL-6 [31].
IL-6 is a critical mediator in infection and inflammation and one of the most studied biomarkers associated with cervical shortening in preterm labor. In our study, IL-6 was found to increase in cervical-vaginal samples from the high-risk group, which coincides with that reported by other studies [32]. Goepfert et al. found that cervical IL-6 concentrations measured at 24 weeks of gestational age (wGA) were elevated in women who had preterm delivery before 32 wGA compared to women whose pregnancies were carried to term, and this finding was even more evident in women with a history of preterm delivery [32,33,34]. In our study, 40% of the women in the high-risk group had a history of a previous delivery before 37 wGA [33,34,35].
In our study, a higher concentration of IFN-γ was found in the group of patients at high-risk for preterm delivery. Accordingly, in a recent report by Sandoval-Colin et al. it was found a positive correlation between elevated IFN-γ, TNF-α, IL-1β, IL-6, and the onset of labor [22], in what appears to be a functional “maturation” of the immune system due to the inflammatory response. Additionally, it has been described that the activation of Th1 cells may increase the secretion of TNF-α, INF-γ, and IL-1β in the fetal membranes and the amniotic fluid in preterm labor [36].
IL-1ra belongs to the IL-1 family of cytokines with an anti-inflammatory action [37]; our study found IL-1ra to be higher in patients at low-risk for PB. To our knowledge, there is no literature on the cervical concentration of this cytokine in the pathogenesis of preterm delivery; however, our IL-1ra results could be well compared with those of the soluble IL-6 receptor (sIL-6r) that has been associated with a reduction in the risk of preterm delivery (RR 0.4 CI 95% 0.15–0.80) [38,39].
IL-2 is crucial for maintaining immune homeostasis, and a correlation has been previously demonstrated between elevated IL-2 levels and chronic inflammation [40]. Few studies have demonstrated the relevance of IL-2 and its receptor in the pathogenesis of preterm labor; the possible explanation is that in normal pregnancy, the concentrations of IL-2 and its receptor are relatively low and difficult to measure, but in the case of preterm labor, an increase of this interleukin has been demonstrated that could imply the chronicity of an inflammatory process and not the acute response as in the case of IL-6 [41].
In most previous publications concerning cytokines in cervical-vaginal fluid, the elevated concentrations of IL-10 have been proposed as a protective factor for preterm delivery [42,43], as belongs to the group of cytokines with anti-inflammatory activity. In our study, the highest concentrations were observed in the high-risk group, which is in agreement with the study by Vogel et al. reporting that elevated IL-10 concentrations could also be associated with an increased risk of preterm delivery (RR 3.1 CI 95% 0.96–9.7) [44], as a response to an inflammatory mechanism that was previously initiated [42].
In the second phase of our study, we developed an artificial intelligence model for PB prediction using machine learning (ML), incorporating the quantification of cytokines, as they are the crucial mediators of the inflammatory process observed in preterm labor. Machine learning is the engine that is driving advances in the development of artificial intelligence. The main areas that may benefit from ML techniques in the medical field are diagnosis and outcome prediction; ML can transform how medicine works [19,45]. AI methods in medical care could facilitate individual pregnancy management and improve public health, especially in low- and middle-income countries. ML allows us to analyze interactions between variables different from what we are conventionally used to, overcoming limitations such as sample size and data distribution. In our study, two predictive models were performed, the full and the adjusted models. The full model included all the predictor variables (obstetric history, CL, and concentration of all the cytokines measured). The ML analysis allowed us to choose only the variables with the highest predictive significance to build and train the adjusted model that included only maternal age, CL, and IL-2 concentration. Our results demonstrated that the adjusted model, even when it included a smaller number of variables, had a better predictive performance; this is possible because of the type of analysis used, where the variables that full the model are eliminated to improve performance [45,46,47].
In most studies involving cytokines in high- and low-risk groups for PB, the classification only consideres obstetric history [48]. So, one of the main strengths of our work is that we studied the cervical-vaginal fluid concentration of the principal cytokines involved in the inflammatory process in patients classified as high- and low-risk for PB by CL, the gold standard in current screening and a variable which itself indicates the onset of cervical shortening and therefore the phase prior to the onset of labor. Additionally, the screening was performed at the appropriate weeks of gestation according to international guidelines [49] and was not biased by interventions such as cerclage or progesterone before measurement. Besides, the presence of vaginal infection during sampling for cytokine determination was ruled out.
Another contribution of our work is comparing the FMF calculator and the predictive model obtained by the Random Forest analysis. With this analysis, we demonstrate that if we add the measurement of IL-2 to the prediction model, we can increase by 8 percentage points the detection rate reported by the gold standard in clinical practice, which would help to identify more accurately those cases at high-risk for PB allowing to implement preventive medical strategies (e.g., progesterone) that can offer an efficiency up to 90% [50,51].
The main limitation of our study is the number of patients included; however, it was possible to identify differences between the groups with significant statistical power. Considering the construction of the model, this fact is compensated by the nature of the analysis performed since the Random Forest analysis builds the ideal model and then replicates it thousands of times to test its efficiency [52]. However, we consider that a more significant number of patients is required to strengthen the model to be used as a reference for PB prediction in clinical practice [53].
As we aimed to design an effective screening model for PB with the inclusion of clinically applicable markers based on cost, availability, efficacy, and timeliness of the test, the next step is undoubtedly to perform a cost/benefit analysis to assess whether adding the IL-2 measurement to the screening model is endorsed by the resources saved with the risk detection and prevention of PB.
Our results contribute to a better understanding of the cervical-vaginal inflammatory network elicited in patients classified as high- and low-risk for preterm delivery according to the current screening gold standard. The prediction model integrating cytokines in cervical-vaginal mucus showed a DR 8 points higher than the gold standard used in clinical practice, with a lower FNR. The increase in DR with the reduction in FNR may allow us to identify women at risk for PB more accurately and implement strategies to prevent this outcome. Our work could represent a significant advance in screening and reducing the prevalence of PB, a goal that has not being achieved in the last 30 years yet.
4. Materials and Methods
4.1. Ethics statement
The study was conducted at the Instituto Nacional de Perinatologia in Mexico City between January 2019 and December 2021. The protocol was approved by the Ethics, Research, and Biosafety Internal Review Boards (2017-2-69). Women who met the inclusion criteria were invited to participate, and they read and signed the informed consent form.
4.2. Study population
Recruitment at convenience was performed by considering women who attended the Maternal-Fetal Medicine Department at the Instituto Nacional de Perinatologia in Mexico City to screen for PB with a singleton 18–23.6 weeks of gestation pregnancy. Clinical data, including age, weight, pregestational weight, socioeconomic status, smoking, history of preterm delivery, gestational age by date of last period and corroborated by first trimester US, presence of urinary or vaginal infections, use of antibiotics, follow-up of pregnancy until its termination, were collected. Fetuses with structural alterations or women with a confirmed diagnosis of isthmic cervical incompetence were not included. The primary outcome was considered to be spontaneous preterm birth, defined as the delivery of the fetus before 37 weeks’ gestation, calculated by the last menstrual period or reliable first-trimester ultrasound, without any medical intervention that produced this outcome [3].
Participants were classified as having high- or low-risk for developing PB according to the cervical length measurement, using a cut-off point <20 mm in patients with a history of preterm delivery and <25 mm for patients without a history of PB [25]. Our institutional protocol was applied in high-risk patients by administering micronized progesterone 200 mg vaginally every 24 h, with a follow-up every 2–3 weeks. Progesterone treatment was initiated after being classified as a high-risk patient based on CL measurement. No patient was receiving progesterone before being classified.
4.3. Sample collection
A cervical-vaginal mucus sample from the posterior vaginal fornix was obtained using a dacron polyester-tipped swab that was rinsed in collection buffer containing 1X PBS, 0.05% Tween-20, 1% BSA, and a protease Inhibitor Cocktail (Roche). Samples in collection buffer were centrifuged at 3200 rpm, 15 min at 4 °C, and the supernatants were stored at -80°C until further cytokine analysis. Before preservation, an aliquot was tested to rule out subclinical vaginal or uterine infection by fresh examination and negative microbiological cultures.
4.4. Cervical-vaginal cytokine quantification
Cytokine concentration in cervical-vaginal mucus was measured using the Luminex X-Map platform with the Bio-Plex Pro Human Cytokine 10-plex that includes IL-2, IL-4, IL-6, IL-8, IL-10, INF-γ, TNF-α, IL-1β, IL-12p70, and IL-1ra (Cat 12020756). The protocol was performed according to the manufacturer's instructions, and the value for each cytokine was expressed as pg/ml. Inter- and intra-assay variation was <10%.
4.5. Statistical analysis
Data were analyzed with the SPSS software, version 24. Descriptive statistics were performed to characterize groups: for qualitative variables, frequency measures expressed in percentages were used, while for quantitative variables, measures of central tendency (mean, median), and measures of dispersion standard deviation (SD). Data distribution was verified before the statistical analysis with Kolmogorov–Smirnov test. Cytokine concentration was evaluated, and differences between groups were assessed using the Mann-Whitney U test. The Chi-square test was used to calculate the difference in proportions. No sample size calculation was performed beforehand, but the statistical power was calculated for all variables with significant differences to verify that it was greater than 80%.
4.6. Machine learning model
A Random Forest classifier model was created to predict the incidence of preterm infants using 12 clinical variables (women´s age, weight, pregestational weight, socioeconomic status, smoking history, parity, previous preterm delivery, gestational age at screening (date of last period and corroborated by first-trimester US), precedent urinary or vaginal infections, use of antibiotics, and gestational age at the time of pregnancy resolution) and 10 cervical-vaginal cytokine determinations (IL-2, IL-4, IL-6, IL-8, IL-10, INF-γ, TNF-α, IL-1β, IL-12p70, and IL-1ra), to create the first full model. To adjust the model, we performed hyperparameter selection by out-of-bag error and simple cross-validation, resulting in 50 trees, 1 mtry (number of predictors considered in each split), and 1 as maximum depth, thus generating the adjusted model. The models were analyzed in a mathematical matrix to determine false positive rates (FPR) and false negative rates (FNR), their overall efficiency, as well as to compare the area under the ROC curves (AUC).
Author Contributions
Conceptualization, H.B.-O.; methodology, M.J.R.-S., A.E.-N. and A.F.-P.; formal analysis, H.B.-O., G.E.-G. and J.M.-O.; writing—original draft, H.B.-O. and G.E.-G.; funding acquisition, H.B.-O.; resources, H.B.-O., G.E.-G., M.J.R.-S., I.C.-A., A.E.-N., A.F.-P., R.G.-C. and J.C.E.-A.; writing—review and editing, H.B.-O., G.E.-G., I.C.-A., and A.F.-P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Instituto Nacional de Perinatología (Grant 2017-2-69).
Institutional Review Board Statement
The study was conducted at the Instituto Nacional de Perinatologia in Mexico City between January 2019 and December 2021. The protocol was approved by the Ethics, Research, and Biosafety Internal Review Boards (2017-2-69).
Informed Consent Statement
Women who met the inclusion criteria were invited to participate, and they read and sign the informed consent form.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
References
- Griggs, K.M.; Hrelic, D.A.; Williams, N.; McEwen-Campbell, M.; Cypher, R. Preterm Labor and Birth: A Clinical Review. MCN Am J Matern Child Nurs 2020, 45, 328-337. [CrossRef]
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.B.; Narwal, R.; Adler, A.; Vera Garcia, C.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162-2172. [CrossRef]
- Menon, R.; Torloni, M.R.; Voltolini, C.; Torricelli, M.; Merialdi, M.; Betrán, A.P.; Widmer, M.; Allen, T.; Davydova, I.; Khodjaeva, Z.; et al. Biomarkers of spontaneous preterm birth: An overview of the literature in the last four decades. Reprod Sci 2011, 18, 1046-1070. [CrossRef]
- Romero, R.; Dey, S.K.; Fisher, S.J. Preterm labor: One syndrome, many causes. Science 2014, 345, 760-765. [CrossRef]
- Di Renzo, G.C.; Tosto, V.; Giardina, I. The biological basis and prevention of preterm birth. Best Pract Res Clin Obstet Gynaecol 2018, 52, 13-22. [CrossRef]
- Wei, S.Q.; Fraser, W.; Luo, Z.C. Inflammatory cytokines and spontaneous preterm birth in asymptomatic women: A systematic review. Obstet Gynecol 2010, 116, 393-401. [CrossRef]
- Simhan, H.N.; Bodnar, L.M.; Kim, K.H. Lower genital tract inflammatory milieu and the risk of subsequent preterm birth: An exploratory factor analysis. Paediatr Perinat Epidemiol 2011, 25, 277-282. [CrossRef]
- Taylor, B.D.; Holzman, C.B.; Fichorova, R.N.; Tian, Y.; Jones, N.M.; Fu, W.; Senagore, P.K. Inflammation biomarkers in vaginal fluid and preterm delivery. Hum Reprod 2013, 28, 942-952. [CrossRef]
- Socha, M.W.; Flis, W.; Pietrus, M.; Wartęga, M.; Stankiewicz, M. Signaling Pathways Regulating Human Cervical Ripening in Preterm and Term Delivery. Cells 2022, 11. [CrossRef]
- Torbé, A.; Czajka, R. Proinflammatory cytokines and other indications of inflammation in cervico-vaginal secretions and preterm delivery. Int J Gynaecol Obstet 2004, 87, 125-130. [CrossRef]
- Dowd, J.; Laham, N.; Rice, G.; Brennecke, S.; Permezel, M. Elevated interleukin-8 concentrations in cervical secretions are associated with preterm labour. Gynecol Obstet Invest 2001, 51, 165-168. [CrossRef]
- Ashford, K.; Chavan, N.R.; Wiggins, A.T.; Sayre, M.M.; McCubbin, A.; Critchfield, A.S.; O'Brien, J. Comparison of Serum and Cervical Cytokine Levels throughout Pregnancy between Preterm and Term Births. AJP Rep 2018, 8, e113-e120. [CrossRef]
- Zaga-Clavellina, V.; Flores-Espinosa, P.; Pineda-Torres, M.; Sosa-González, I.; Vega-Sánchez, R.; Estrada-Gutierrez, G.; Espejel-Núñez, A.; Flores-Pliego, A.; Maida-Claros, R.; Estrada-Juárez, H.; et al. Tissue-specific IL-10 secretion profile from term human fetal membranes stimulated with pathogenic microorganisms associated with preterm labor in a two-compartment tissue culture system. J Matern Fetal Neonatal Med 2014, 27, 1320-1327. [CrossRef]
- Gomez, R.; Romero, R.; Edwin, S.S.; David, C. Pathogenesis of preterm labor and preterm premature rupture of membranes associated with intraamniotic infection. Infect Dis Clin North Am 1997, 11, 135-176. [CrossRef]
- Licini, C.; Tossetta, G.; Avellini, C.; Ciarmela, P.; Lorenzi, T.; Toti, P.; Gesuita, R.; Voltolini, C.; Petraglia, F.; Castellucci, M.; et al. Analysis of cell-cell junctions in human amnion and chorionic plate affected by chorioamnionitis. Histol Histopathol 2016, 31, 759-767. [CrossRef]
- Tossetta, G.; Paolinelli, F.; Avellini, C.; Salvolini, E.; Ciarmela, P.; Lorenzi, T.; Emanuelli, M.; Toti, P.; Giuliante, R.; Gesuita, R.; et al. IL-1β and TGF-β weaken the placental barrier through destruction of tight junctions: An in vivo and in vitro study. Placenta 2014, 35, 509-516. [CrossRef]
- Celik, E.; To, M.; Gajewska, K.; Smith, G.C.; Nicolaides, K.H. Cervical length and obstetric history predict spontaneous preterm birth: Development and validation of a model to provide individualized risk assessment. Ultrasound Obstet Gynecol 2008, 31, 549-554. [CrossRef]
- Kim, H.Y.; Cho, G.J.; Kwon, H.S. Applications of artificial intelligence in obstetrics. Ultrasonography 2023, 42, 2-9. [CrossRef]
- Arain, Z.; Iliodromiti, S.; Slabaugh, G.; David, A.L.; Chowdhury, T.T. Machine learning and disease prediction in obstetrics. Curr Res Physiol 2023, 6, 100099. [CrossRef]
- Dodd, J.M.; Flenady, V.J.; Cincotta, R.; Crowther, C.A. Progesterone for the prevention of preterm birth: A systematic review. Obstet Gynecol 2008, 112, 127-134. [CrossRef]
- Meyyazhagan, A.; Kuchi Bhotla, H.; Pappuswamy, M.; Tsibizova, V.; Al Qasem, M.; Di Renzo, G.C. Cytokine see-saw across pregnancy, its related complexities and consequences. Int J Gynaecol Obstet 2023, 160, 516-525. [CrossRef]
- Sandoval-Colin, D.E.; Godines-Enriquez, M.S.; Espejel-Núñez, A.; Beltrán-Montoya, J.J.; Picazo-Mendoza, D.A.; de la Cerda-Ángeles, J.C.; Bello-Chavolla, O.Y.; Meraz-Cruz, N.; Chavira-Suárez, E.; Vadillo-Ortega, F. Cervicovaginal Cytokines to Predict the Onset of Normal and Preterm Labor: A Pseudo-longitudinal Study. Reprod Sci 2023, 30, 221-232. [CrossRef]
- Park, J.W.; Park, K.H.; Lee, S.Y. Noninvasive prediction of intra-amniotic infection and/or inflammation in women with preterm labor: Various cytokines in cervicovaginal fluid. Reprod Sci 2013, 20, 262-268. [CrossRef]
- Cetin, O.; Karaman, E.; Alisik, M.; Erel, O.; Kolusari, A.; Sahin, H.G. The evaluation of maternal systemic thiol/disulphide homeostasis for the short-term prediction of preterm birth in women with threatened preterm labour: A pilot study. J Obstet Gynaecol 2022, 42, 1972-1977. [CrossRef]
- Berghella, V.; Palacio, M.; Ness, A.; Alfirevic, Z.; Nicolaides, K.H.; Saccone, G. Cervical length screening for prevention of preterm birth in singleton pregnancy with threatened preterm labor: Systematic review and meta-analysis of randomized controlled trials using individual patient-level data. Ultrasound Obstet Gynecol 2017, 49, 322-329. [CrossRef]
- Yavari Kia, P.; Baradaran, B.; Shahnazi, M.; Asghari Jafarabadi, M.; Khaze, V.; Pourasad Shahrak, S. Maternal Serum and Cervicovaginal IL-6 in Patients with Symptoms of Preterm Labor. Iran J Immunol 2016, 13, 229-236.
- Hanna, N.; Bonifacio, L.; Reddy, P.; Hanna, I.; Weinberger, B.; Murphy, S.; Laskin, D.; Sharma, S. IFN-gamma-mediated inhibition of COX-2 expression in the placenta from term and preterm labor pregnancies. Am J Reprod Immunol 2004, 51, 311-318. [CrossRef]
- Buxton, M.A.; Meraz-Cruz, N.; Sanchez, B.N.; Foxman, B.; Castillo-Castrejon, M.; O'Neill, M.S.; Vadillo-Ortega, F. Timing of Cervico-Vaginal Cytokine Collection during Pregnancy and Preterm Birth: A Comparative Analysis in the PRINCESA Cohort. Int J Environ Res Public Health 2021, 18. [CrossRef]
- Chatterjee, P.; Chiasson, V.L.; Bounds, K.R.; Mitchell, B.M. Regulation of the Anti-Inflammatory Cytokines Interleukin-4 and Interleukin-10 during Pregnancy. Front Immunol 2014, 5, 253. [CrossRef]
- Park, J.S.; Park, C.W.; Lockwood, C.J.; Norwitz, E.R. Role of cytokines in preterm labor and birth. Minerva Ginecol 2005, 57, 349-366.
- Wang, L.; Liu, Z.; Huang, D.; Ran, Y.; Zhang, H.; He, J.; Yin, N.; Qi, H. IL-37 Exerts Anti-Inflammatory Effects in Fetal Membranes of Spontaneous Preterm Birth via the NF-κB and IL-6/STAT3 Signaling Pathway. Mediators Inflamm 2020, 2020, 1069563. [CrossRef]
- Gilman-Sachs, A.; Dambaeva, S.; Salazar Garcia, M.D.; Hussein, Y.; Kwak-Kim, J.; Beaman, K. Inflammation induced preterm labor and birth. J Reprod Immunol 2018, 129, 53-58. [CrossRef]
- Goepfert, A.R.; Goldenberg, R.L.; Andrews, W.W.; Hauth, J.C.; Mercer, B.; Iams, J.; Meis, P.; Moawad, A.; Thom, E.; VanDorsten, J.P.; et al. The Preterm Prediction Study: Association between cervical interleukin 6 concentration and spontaneous preterm birth. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Am J Obstet Gynecol 2001, 184, 483-488. [CrossRef]
- Challis, J.R.; Lockwood, C.J.; Myatt, L.; Norman, J.E.; Strauss, J.F., 3rd; Petraglia, F. Inflammation and pregnancy. Reprod Sci 2009, 16, 206-215. [CrossRef]
- Paternoster, D.M.; Stella, A.; Gerace, P.; Manganelli, F.; Plebani, M.; Snijders, D.; Nicolini, U. Biochemical markers for the prediction of spontaneous pre-term birth. Int J Gynaecol Obstet 2002, 79, 123-129. [CrossRef]
- Helmo, F.R.; Alves, E.A.R.; Moreira, R.A.A.; Severino, V.O.; Rocha, L.P.; Monteiro, M.; Reis, M.A.D.; Etchebehere, R.M.; Machado, J.R.; Corrêa, R.R.M. Intrauterine infection, immune system and premature birth. J Matern Fetal Neonatal Med 2018, 31, 1227-1233. [CrossRef]
- Smith, A.J.; Humphries, S.E. Cytokine and cytokine receptor gene polymorphisms and their functionality. Cytokine Growth Factor Rev 2009, 20, 43-59. [CrossRef]
- Gonçalves, L.F.; Chaiworapongsa, T.; Romero, R. Intrauterine infection and prematurity. Ment Retard Dev Disabil Res Rev 2002, 8, 3-13. [CrossRef]
- Mitsuyama, K.; Matsumoto, S.; Rose-John, S.; Suzuki, A.; Hara, T.; Tomiyasu, N.; Handa, K.; Tsuruta, O.; Funabashi, H.; Scheller, J.; et al. STAT3 activation via interleukin 6 trans-signalling contributes to ileitis in SAMP1/Yit mice. Gut 2006, 55, 1263-1269. [CrossRef]
- Gaffen, S.L.; Liu, K.D. Overview of interleukin-2 function, production and clinical applications. Cytokine 2004, 28, 109-123. [CrossRef]
- Alvarez-de-la-Rosa, M.; Rebollo, F.J.; Codoceo, R.; Gonzalez Gonzalez, A. Maternal serum interleukin 1, 2, 6, 8 and interleukin-2 receptor levels in preterm labor and delivery. Eur J Obstet Gynecol Reprod Biol 2000, 88, 57-60. [CrossRef]
- Cao, X.L.; Zhou, X.Y.; Xu, N.X.; Chen, S.C.; Xu, C.M. Association of IL-4 and IL-10 Polymorphisms With Preterm Birth Susceptibility: A Systematic Review and Meta-Analysis. Front Immunol 2022, 13, 917383. [CrossRef]
- Busse, M.; Zenclussen, A.C. IL-10 Producing B Cells Protect against LPS-Induced Murine Preterm Birth by Promoting PD1- and ICOS-Expressing T Cells. Cells 2022, 11. [CrossRef]
- Vogel, I.; Goepfert, A.R.; Thorsen, P.; Skogstrand, K.; Hougaard, D.M.; Curry, A.H.; Cliver, S.; Andrews, W.W. Early second-trimester inflammatory markers and short cervical length and the risk of recurrent preterm birth. J Reprod Immunol 2007, 75, 133-140. [CrossRef]
- Bertini, A.; Salas, R.; Chabert, S.; Sobrevia, L.; Pardo, F. Using Machine Learning to Predict Complications in Pregnancy: A Systematic Review. Front Bioeng Biotechnol 2021, 9, 780389. [CrossRef]
- Mohammad, N.S.; Nazli, R.; Zafar, H.; Fatima, S. Effects of lipid based Multiple Micronutrients Supplement on the birth outcome of underweight pre-eclamptic women: A randomized clinical trial. Pak J Med Sci 2022, 38, 219-226. [CrossRef]
- Saberi-Karimian, M.; Khorasanchi, Z.; Ghazizadeh, H.; Tayefi, M.; Saffar, S.; Ferns, G.A.; Ghayour-Mobarhan, M. Potential value and impact of data mining and machine learning in clinical diagnostics. Crit Rev Clin Lab Sci 2021, 58, 275-296. [CrossRef]
- Oskovi Kaplan, Z.A.; Ozgu-Erdinc, A.S. Prediction of Preterm Birth: Maternal Characteristics, Ultrasound Markers, and Biomarkers: An Updated Overview. J Pregnancy 2018, 2018, 8367571. [CrossRef]
- Glover, A.V.; Manuck, T.A. Screening for spontaneous preterm birth and resultant therapies to reduce neonatal morbidity and mortality: A review. Semin Fetal Neonatal Med 2018, 23, 126-132. [CrossRef]
- Jung, E.Y.; Park, J.W.; Ryu, A.; Lee, S.Y.; Cho, S.H.; Park, K.H. Prediction of impending preterm delivery based on sonographic cervical length and different cytokine levels in cervicovaginal fluid in preterm labor. J Obstet Gynaecol Res 2016, 42, 158-165. [CrossRef]
- Norman, J.E. Progesterone and preterm birth. Int J Gynaecol Obstet 2020, 150, 24-30. [CrossRef]
- Lee, K.S.; Ahn, K.H. Artificial Neural Network Analysis of Spontaneous Preterm Labor and Birth and Its Major Determinants. J Korean Med Sci 2019, 34, e128. [CrossRef]
- Giouleka, S.; Tsakiridis, I.; Kostakis, N.; Koutsouki, G.; Kalogiannidis, I.; Mamopoulos, A.; Athanasiadis, A.; Dagklis, T. Preterm Labor: A Comprehensive Review of Guidelines on Diagnosis, Management, Prediction and Prevention. Obstet Gynecol Surv 2022, 77, 302-317. [CrossRef]
Figure 1.
Differences in cytokines measured in cervical mucus. Boxplots showing (A) Pro-inflammatory cytokines (IL-2, IL-6, and IFN- γ) and (B) Anti-inflammatory cytokines (IL-4, IL1ra, and IL-10) with significant differences between women at low risk (n=40) and high risk (n=20) for preterm birth. **p < 0.01, ***p < 0.001.
Figure 1.
Differences in cytokines measured in cervical mucus. Boxplots showing (A) Pro-inflammatory cytokines (IL-2, IL-6, and IFN- γ) and (B) Anti-inflammatory cytokines (IL-4, IL1ra, and IL-10) with significant differences between women at low risk (n=40) and high risk (n=20) for preterm birth. **p < 0.01, ***p < 0.001.
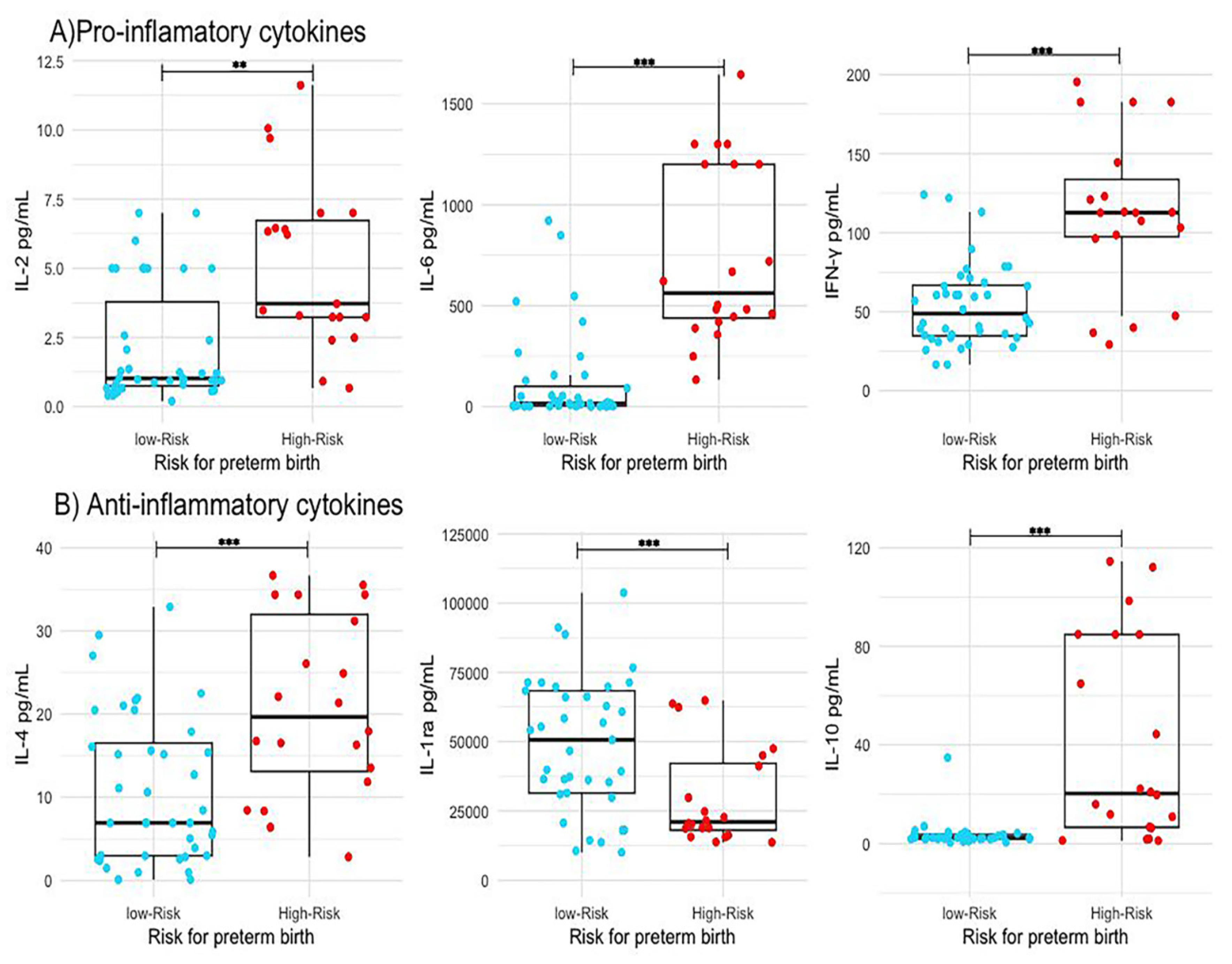
Figure 2.
Performance of the models generated by machine learning. (A) Full model including all the variables studied as predictors. (B) Adjusted model including only the variables with the highest statistical relevance (CL, IL2, and maternal age). (C) ROC curves of the two proposed models: red, Full model with an AUC = 0.722 and green, Adjusted model with an AUC = 0.879. CL: Cervical Length, BMI: Body Mass Index, RMA: Risk Maternal Age, IL: Interleukin, TNFA: Tumor Necrosis Factor-α, IFNG: Interferon-γ, SEL: Socioeconomic Level.
Figure 2.
Performance of the models generated by machine learning. (A) Full model including all the variables studied as predictors. (B) Adjusted model including only the variables with the highest statistical relevance (CL, IL2, and maternal age). (C) ROC curves of the two proposed models: red, Full model with an AUC = 0.722 and green, Adjusted model with an AUC = 0.879. CL: Cervical Length, BMI: Body Mass Index, RMA: Risk Maternal Age, IL: Interleukin, TNFA: Tumor Necrosis Factor-α, IFNG: Interferon-γ, SEL: Socioeconomic Level.
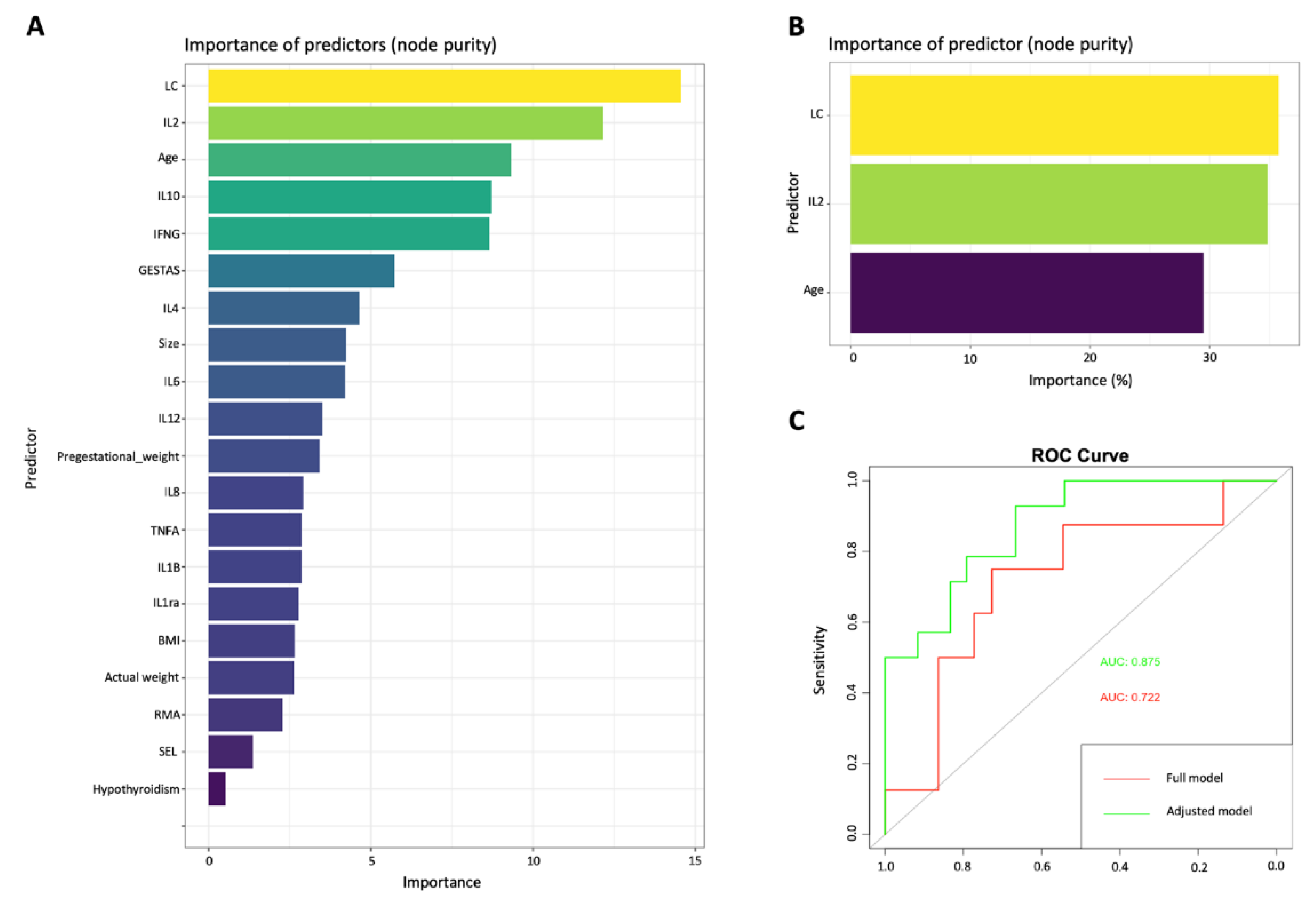

Table 1.
Baseline characteristics and clinical data of pregnant women included in the study.
| Low Risk for Preterm Delivery (n = 40) |
High Risk for Preterm Delivery (n = 20) |
p-value | |
|---|---|---|---|
| Age (years) | 29 (±7.1) | 31 (±5.8) | 0.25 |
| Pregestational weight (Kg) | 63.7 (±13.7) | 67.8 (±13.5) | 0.08 |
| Pregestational BMI (Kg/m2) | 25.2 (±5.4) | 27.5 (±5.3) | 0.12 |
| Socio-economic level median (Minimum and maximum value) |
2 (1–4) | 2 (1–5) | 0.12 |
| Smoking n (%) | 1 (2.5) | 0 (0) | 0.45 |
| History of preterm delivery n (%) |
0 (0) | 8 (40) | 0.01** |
| Gestational age at time of cervical length measurement, (weeks of gestation) | 21.0 (±1.5) | 21.2 (±2.0) | 0.25 |
| Cervical length (mm) | 33.8 (±5.8) | 13.1 (±7.7) | 0.02* |
| SPB < 28 WG n (%) | 0 | 2 (10%) | 0.001*** |
| SPB 28-34 WG n (%) | 2 (5%) | 6 (30%) | 0.001*** |
| SPB > 34 WG n (%) | 1 (2.5%) | 1 (5%) | 0.01** |
WG: weeks of gestation, SPB: spontaneous preterm birth. Mean, median, standard deviation, minimum and maximum value, comparations with Mann Whitney U and Chi-square Test, p-value. * p<0.05, ** p<0.01, ***p<0.001.
Table 2.
Pro-inflammatory and anti-inflammatory cytokine profile in cervical-vaginal fluid at 18.0–23.6 weeks of gestation in high (n = 20) and low risk (n = 40) groups for preterm birth.
Table 2.
Pro-inflammatory and anti-inflammatory cytokine profile in cervical-vaginal fluid at 18.0–23.6 weeks of gestation in high (n = 20) and low risk (n = 40) groups for preterm birth.
| Cytokine | Risk group for preterm birth |
Mean ± SD pg/ml |
p-value |
|---|---|---|---|
| Pro-inflammatory cytokines | |||
| IL-1β | High-Risk | 763.87 (±1505.99) | 0.814 |
| Low-Risk | 587.94 (±1432.56) | ||
| IL-2 | High-Risk | 5.63 (±1.48) | 0.01** |
| Low-Risk | 3.60 (±6.07) | ||
| IL-6 | High-Risk | 856.29 (±1.98) | 0.001*** |
| Low-Risk | 118.32 (±0.48) | ||
| IL-8 | High-Risk | 5882.35 (±5638.79) | 0.381 |
| Low-Risk | 9695.78 (±11,070.29) | ||
| IL-12 | High-Risk | 0.49 (±0.49) | 0.304 |
| Low-Risk | 0.34 (0.29) | ||
| TNF-α | High-Risk | 104.17 (±74.62) | 0.115 |
| Low-Risk | 78.63 (±50.32) | ||
| IFN-γ | High-Risk | 117.49 (±53.42) | 0.001*** |
| Low-Risk | 54.17 (±26.37) | ||
| Anti-inflammatory cytokines | |||
| IL-4 | High-Risk | 20.98 (±10.78) | 0.001*** |
| Low-Risk | 10.83 (±8.92) | ||
| IL-10 | High-Risk | 40.44 (±41.23) | 0.001*** |
| Low-Risk | 3.56 (±5.22) | ||
| IL-1ra | High-Risk | 29,768 (±17,596) | 0.002*** |
| Low-Risk | 58,377 (±40,841) | ||
Mean, standard deviation, comparations with Mann Whitney U Test, p-value. * p<0.05, ** p<0.01, ***p<0.001.
Table 3.
Comparison between the two proposed classifiers models: “Full model”, “Adjusted model” and Fetal Medicine Foundation (FMF) calculator.
Table 3.
Comparison between the two proposed classifiers models: “Full model”, “Adjusted model” and Fetal Medicine Foundation (FMF) calculator.
| Random Forest “Full model” | Random Forest “Adjusted model” | Fetal Medicine Foundation Calculator | ||||||
|---|---|---|---|---|---|---|---|---|
| Predicted | Real | Predicted | Real | Predicted | Real | |||
| Term | Preterm | Term | Preterm | Term | Preterm | |||
| Term | 14 | 6 | Term | 20 | 1 | Term | 36 | 4 |
| Preterm | 2 | 1 | Preterm | 2 | 7 | Preterm | 7 | 13 |
| Detection rate | 65% | Detection rate | 87.7% | Detection rate | 79% | |||
| False positive rate | 12% | False positives rate | 3.33% | False positives rate | 6.6% | |||
| False negative rate | 28% | False negatives rate | 6.66% | False negatives rate | 11.66% | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



