
Submitted:
30 August 2023
Posted:
31 August 2023
You are already at the latest version
Abstract
While biologic originators’ patents are expiring, biosimilars are emerging to take their place, offering significant cost savings to healthcare systems. Many challenges still need to be addressed in the clinical practice of inflammatory bowel disease (IBD). A global survey was organized to highlight physicians’ current knowledge and beliefs and to gain insight about their practical management and remaining concerns and obstacles associated with starting a biosimilar, switching from an originator to a biosimilar, or switching from one biosimilar to another (multiple switches and reverse switching). Fifteen physicians with expertise in the field of IBD from 13 countries attended a virtual international consensus meeting to develop practical guidance regarding biosimilar adoption worldwide, considering the survey results. Consensus was reached on 10 statements regarding biosimilar effectiveness, safety, indications and rationale, multiple switches, therapeutic drug monitoring of biosimilars, non-medical switching and future perspectives.
Keywords:
biosimilars
; bio-originators
; biologic drug
; ulcerative colitis
; Crohn’s disease
; interchangeability
; economics
1. Introduction
The Biologics Price Competition and Innovation Act of 2009 was enacted to promote competition and cost containment across medicine by creating a shortened regulatory pathway for biological products highly similar to licensed biologics (i.e., biosimilars) [1]. While biologic originators (i.e., bio-originators) patents are expiring, multiple biosimilars are emerging to take their place, offering significant cost-saving opportunities to healthcare systems [2,3].
From a regulatory perspective, a solid legal framework was established and since the approval of the first biosimilar, the European Medicines Agency (EMA) has introduced a dedicated route for biosimilar approval based on a comparability exercise to establish biosimilarity [2,4]. Biosimilars are tested in at least one indication of the originator in phase I and III clinical trials, and results may be extrapolated toward other indications [5,6]. Since the Food and Drug Administration (FDA) authorized the first biosimilar in the United States in 2015, the number of biosimilars in gastroenterology has increased significantly, with at least 41 biosimilar drugs approved to date [7].
Undoubtedly, many gastroenterologists are currently, or will soon be, given the opportunity to prescribe or asked to substitute a biosimilar for a bio-originator on which they have previously relied. Despite the emergence of biosimilars, it is unclear to what extent gastroenterologists are knowledgeable about and comfortable with and what their practical management implies [8]. Uptake has been dampened by several issues, including (1) gastroenterologists’ uncertainty if safety and efficacy evidence supports interchangeability with the bio-originator, (2) the complexity and dynamic nature of reverse and multiple switches, and (3) potential patient acceptance of using a biosimilar and related nocebo effect [9,10,11].
A 2017 survey of 1,201 international physicians that included various specialties (including gastroenterology) indicated a need for knowledge-based education about biosimilars [12]. This research highlighted specific gaps in knowledge about biosimilars, such as the inability to select the correct definition of the terms extrapolation and interchangeability related to biosimilar regulation and a poor ability to articulate the difference between biosimilars and originators. Thus, it is critically important to better understand gastroenterologists’ attitudes regarding biosimilars and their practical management while prescribing these drugs, as these factors affect biosimilar uptake and, ultimately, influence patient outcomes. We surveyed IBD physicians to get their feedback about their management and current challenges when starting a biosimilar, switching from an originator to a biosimilar or switching from one biosimilar to another one (reverse and multiple switching). Furthermore, we organized an international expert consensus meeting to develop and validate evidence-based statements to serve as guidance for biosimilar use in IBD.
2. Methods
2.1. Survey
We designed a cross-sectional survey targeted at clinicians involved in the care of IBD worldwide. From January to February 2023, participants were invited to take a survey hosted on an online platform. The link was sent via email through the mailing lists of IBD-scope, a webinar platform designed for healthcare professionals interested in IBD, and by personal invitation of physicians with a focus on IBD. Screening questions were included at the beginning of the survey to filter respondents out of the target population and email registration was used to prevent double participation. Responses were collected anonymously and permission for data collection was asked upon survey start. The survey and the invitation email were in English, and all questions were multiple-choice.
The questionnaire comprised 46 questions classified into 5 sections (Table 1): the first recorded demographics, specialty, and level of experience of participants (6 questions); the second focused on practices and attitudes toward biosimilar use in clinical practice (22 questions); the third was about interchangeability (reverse/multiple switches) (9 questions); the fourth addressed the nocebo effect and non-medical switch (5); and the last one included current and future perspectives (4 questions). Only demographic questions were mandatory, and the number of respondents was reported for each question to account for missing data. The full survey is provided in the Data Supplement.
The study was conducted and reported in compliance with the Consensus for Reporting of Survey Studies (CROSS) guidelines [13]. The CROSS checklist is available in the Data Supplement.
Excel (v16.71, Microsoft) was used to perform descriptive statistics and plot the charts.
2.2. Consensus meeting
A virtual consensus meeting including 15 experts in the field of IBD from 13 countries worldwide (Argentina, Brazil, Canada, France, Germany, Ireland, Italy, Japan, Portugal, Spain, Sweden, United Arab Emirates, and United States of America) was held on February 21st, 2023. Based on results of the global survey, 10 statements were formulated by 3 authors (FD, LPB, and SD) and were anonymously voted by all experts using a Delphi consensus methodology through a virtual platform.
Statements were approved if ≥75% of participants agreed. If agreement was not reached, the statement was discussed, rephrased, and re-voted. If no consensus was reached in the second round of votes, the statement was removed. New statements could also be formulated during the virtual meeting, discussed, and voted on. All experts were involved in drafting the manuscript and approved its final version.
3. Results
3.1. Survey
Part 1. Demographics, specialty, and level of experience of participants
In total, 234 physicians from 38 countries across all continents responded; 39% (99/234) were 30-40 years old, and female and male practitioners were fairly evenly represented in this population (102/234, 43.6% female) (Figure 1). Approximately 86% (202/234) were gastroenterologists and 2.5% (6/234) surgeons, and the remaining were internal medicine specialists (3/254), general practitioners (3/254) and other specialists (20/254). Most participants (174/234, 74.4%) were highly experienced, with more than 10 years of practice in the field of IBD. Regarding center size, 37.1% (87/234) worked in hospitals caring for >500 IBD patients per year, 38.5% (90/234) in institutions caring for 100-500 patients, and 24.3% (57/234) in centers with <100 patients.
Part 2. Practices and attitudes toward the use of biosimilar in clinical practice
Most participants (195/234, 83.3%) believed biosimilars are as effective and safe as the originator drugs, and only 3.9% (9/234) stated they are less effective and safe.
The largest proportion rated their overall confidence with biosimilars as moderate (average 8.5 on a scale from 0 to 10). However, participants rated their patients’ average rating of confidence as slightly lower (7.7 vs. 8.5).
Regarding extrapolation, approximately 75% (176/234) of the sample responded that biosimilar data from other immune-mediated inflammatory diseases (IMID) are valid and applicable to the IBD field.
When asked about their practical management, a high proportion of practitioners (195/234, 83.3%) reported that patients should be informed before switching and that physicians, more than nurses, pharmacists, government authorities, or residents, should deliver information. Although more than 70% (165/234) of participants tend to explain to patients what a biosimilar drug is and what the originator drug is, less than a third reported providing data and written material about biosimilars.
Almost all participants (>80%) were familiar with infliximab and adalimumab biosimilars, and they indicated lower costs and originators unavailability as the main reasons behind biosimilars’ uptake (54.7% and 15.8%, respectively). Of the practitioners, 72.2% (169/234) believed that biosimilars should not be prescribed only to bio-naïve patients, and the majority thought that switching is a non-medical decision, which is independent of patients’ outcomes (e.g., clinical, biochemical, and endoscopic remission). Therapeutic drug monitoring (TDM) with biosimilar trough levels and auto-antibodies measurement was performed by 43.2% (94/218) of participants. Almost half of practitioners experienced patients’ refusal to switch, but overall non-acceptance involved less than 5% of patients under their care. According to physicians, lower effectiveness (79/218, 36.2%) and disease flare (52/218, 23.8%) rather than safety concerns (17/218, 7.8%) were indicated as the main sources of fear for patients.
More than half of practitioners (133/218, 61.0%) still prescribe originators despite biosimilar availability. When asked why, explanations were extremely heterogeneous with more than 50% not selecting any of the proposed options (Figure 2). Of note, 17.4% (38/218) believed little data are available on biosimilars, and 11.9% (26/218) of respondents had no access to biosimilars in their hospital.
Part 3. Interchangeability (reverse and multiple switches)
Approximately a quarter of participants (57/218, 26.1%) switched from a biosimilar to the originator at least once. The main reasons for reverse switch were biosimilar unavailability (20/54, 37.0%), loss of response (15/54, 27.8%) and allergic reaction to a biosimilar (8/54, 14.8%).
When asked “In a patient treated with the originator drug and then switched to the biosimilar, have you ever prescribed the reverse switch to the originator drug?” almost 40% responded affirmatively. The decision regarding this modality of reverse switch was based on prior allergic reaction to the biosimilar (19/72, 26.4%), loss of response to the biosimilar (19/72, 26.4%), and unavailability of the first biosimilar (24/72 33.3%). In this specific scenario, most patients (68/72, 94.4%) achieved or maintained disease remission.
Over half of the respondents (93/184, 50.5%) switched from one biosimilar to another biosimilar of the same drug (multiple switches). Consistently with reverse, multiple switches led to disease remission and maintained remission in almost all cases. The top reasons among the 50.5% of respondents that have done multiple switches included: first biosimilar unavailability (60/93, 64.5%), allergic reactions (7/93, 7.5%), and loss of response (6/93, 6.4%).
Part 4. Nocebo effect and non-medical switch
Most physicians (159/184, 86.4%) were familiar with the concept of the nocebo effect, but approximately a third could not affirm whether their patients had ever experienced that. In addition, when physicians were aware of the nocebo effect in their patients, in most cases, they believed it involved less than <5% of them. More than half of IBD specialists (105/184, 57.1%) had patients undergoing non-medical switching, and among them, almost all (98/105, 93.3%) achieved or maintained clinical remission.
Part 5. Current and future perspectives
The availability of biosimilars impacts therapeutic choices according to many health-care practitioners (136/184, 73.9%). Most (96/184, 52.2%) believed they would be prescribing biosimilars of vedolizumab and ustekinumab, and generics of small molecules shortly. However, a relevant percentage (56/184, 30.4%) stated that the availability of the biosimilars of vedolizumab, ustekinumab, and generics of small molecule drug, such as tofacitinib, would not change the treatment algorithm of IBD patients. When asked for suggestions on how to implement the use of biosimilars in clinical practice, the need for long-term data was pointed out by the majority of respondents (93/184, 50.5%), followed by the need for randomized clinical trials to compare the efficacy and safety of biosimilars and originator drugs in patients with IBD (71/184, 38.6%), more information to patients provided by government authorities (60/184, 32.6%), and more patient engagement in the therapeutic decision (59/184, 32.1%) (Figure 3). Information delivered from patient associations and non-medical switch were also indicated by almost a third of respondents respectively.
3.2. Statements
Eight preliminary statements were approved in the first voting round. A list of the preliminary statements is included in the Data Supplement. Two statements were approved after the second round of voting. One was not approved during the second voting and was removed, ultimately leading to the approval of 10 statements (Table 2).
A consensus was reached for 10 out of the 11 statements (90.1%), with 100% agreement in eight statements (80.0%). This consensus endorses evidence from clinical trials and increasing experience from observational studies, which show that biosimilars are equivalent to reference products in terms of efficacy and safety profiles, including the extrapolation of the indications [14,15]. Both biologic-naïve patients and those already treated with the originator drugs are candidates for biosimilar switch. Certainly, the use of biosimilars in naïve patients is better accepted [16]. Indeed, patients who have responded to the originator drug may fear losing response and, thus, experience the nocebo effect. To overcome this limitation, adequate patient information is essential and has been associated with significant improvement in patient outcomes [17]. The main reason for switching from an originator drug to a biosimilar is cost-effectiveness. To date, no study has been specifically designed to evaluate the optimal timing for the biosimilar switch. However, based on the reliable efficacy and safety profile of biosimilars and their advantageous cost savings, switching to a biosimilar can be performed at any time. Since interchangeability allows a biosimilar product to be replaced by the reference product [18,19], multiple switches from one biosimilar to another are feasible in case of drug unavailability [20,21,22]. Conversely, there is limited evidence on the efficacy of switching from one biosimilar to another in case of loss of response. For this reason, it should not be recommended. The only rejected statement was the one concerning the reverse switch from the biosimilar to the originator drug. A Dutch retrospective multicenter study revealed that the reverse switch is performed in about 10% of cases due to worsening gastrointestinal symptoms, adverse effects, or loss of response [23]. Interestingly, approximately three-quarters of patients who lost response after switching to biosimilar regained response after a reverse switch to the originator. On the other hand, the lack of prospective studies evaluating the efficacy and safety of the reverse switch prevents us from recommending this strategy in clinical practice. Another crucial aspect regarding the switch to biosimilars is the need to monitor drug levels and anti-drug antibodies. There is substantial evidence about TDM of biologic therapies in IBD. Notably, there are no specific TDM assays for biosimilars. In addition, there are no data demonstrating a higher risk of immunogenicity with biosimilars. Therefore, there is no need to modify the regular practice of monitoring drug trough levels and anti-drug antibodies in patients switched from the originator drug to the biosimilar [24–26]. TDM should not be encouraged for patients just because of the switch to a biosimilar while they are in remission. Despite the notable advantages of the use of biosimilars, there are still patients who refuse the switch and prescribers who still prefer the originator drugs. The non-medical switch (i.e., a change to a patient’s medication for reasons other than lack of clinical response, safety issues, or poor compliance) could be the key to reducing costs associated with advanced therapies and increasing accessibility. A prospective multicenter study showed no differences in efficacy and safety between patients treated with the originator drugs and those who switched to biosimilars for non-medical reasons [27]. Similarly, a systematic review found no effectiveness, safety, or immunogenicity concerns with non-medical switch supporting its wide use [14]. Currently, only biosimilars of infliximab and adalimumab are available. Of note, the patents of vedolizumab and ustekinumab will soon expire, expanding the range of biosimilars [28,29]. A recent randomized clinical trial enrolling healthy volunteers compared the safety and immunogenicity of ustekinumab and its biosimilar [30]. No difference in the pharmacokinetics was identified, and the safety profile of the two drugs was also comparable. Non-anti-TNF biosimilars are expected to become available in the foreseeable future, potentially altering therapeutic algorithms in patients with IBD. TNF-antagonists are currently the first therapeutic option in most patients due to their efficacy, known safety, and low cost. Other biological drugs and small molecules are frequently used as subsequent lines of therapy unless there are contraindications to TNF inhibitors or there is a preference for another drug in the management of specific subpopulations (e.g., extraintestinal manifestations, elderly, co-morbidities, perianal disease, chronic pouchitis) [31,32,33]. The non-anti-TNF biosimilars, once approved by the regulatory authorities, will allow further reductions in healthcare costs and an increasingly personalized and tailored approach, selecting the most suitable drug for the individual patient regardless of the economic impact.
4. Discussion
Biologic therapies have led to significant improvements in the outcomes of patients with IBD, with the downside of increased healthcare costs [34]. The signature promises of biosimilars are to improve patient access to highly effective treatments earlier in the disease course, to decrease costs, and to maintain improved health outcomes. This represents an opportunity for gastroenterologists to deliver high-quality and high-value care. The present survey provides insights regarding IBD specialists’ practical management, beliefs and knowledge surrounding biosimilars. The subsequent International Delphi provides for the first-time consensus statements for the use of biosimilars in the treatment of patients with IBD. These consensus statements are intended to offer guidance to clinicians, healthcare organizations, pharmaceutical industry, and patients regarding the development and use of biosimilars for the treatment of IBD around the world.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Integral survey with responses, Table S2: CROSS checklist, Table 3: Preliminary statements.
Author Contributions
LPB and SD conceived the study. FD and VS equally contributed to manuscript drafting and created tables and figures. All authors critically reviewed the content of the paper and discussed the statements and contributed to the final manuscript.
Funding
The consensus was supported by Sandoz.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
None.
Conflicts of Interest
F D’Amico has served as a speaker for Sandoz, Janssen, Galapagos, and Omega Pharma; he has also served as advisory board member for Abbvie, Ferring, Galapagos, and Nestlè. V Solitano declares no conflict of interest. F Magro has served as a speaker and received honoraria from Merck Sharp & Dohme, Abbvie, Vifor, Falk, Laboratorios Vitoria, Ferring, Hospira, and Biogen. PA Olivera received consulting fees from Abbvie, Takeda, and Janssen and lecture fees from Takeda and Janssen. J Halfvarson has served as speaker and/or advisory board member for AbbVie, Celgene, Celltrion, Ferring, Galapagos, Gilead, Hospira, Janssen, MEDA, Medivir, MSD, Olink Proteomics, Pfizer, Prometheus Laboratories Inc., Sandoz/Novartis, Shire, Takeda, Thermo Fisher Scientific, Tillotts Pharma, Vifor Pharma, and UCB. He also has received grant support from Janssen, MSD, and Takeda. D Rubin reports consultation fees, research grants, royalties, or honorariaum from Janssen, Pfizer, Hospital for Sick Children (Canada), Ferring, AbbVie, Takeda, Atlantic Health System, Shire, Celgene, Lilly, Roche, ThermoFisher, and Bristol Myers Squibb. He has also received grant support from Takeda, and has served as a consultant for Abbvie, Altrubio, Aslan Pharmaceuticals, Athos Therapeutics, Bellatrix Pharmaceuticals, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene Chronicles, Corp/Syneos, ClostraBio, Connect BioPharma, Eco R1, Genentech/Roche, Gilead Sciences, Iterative Health, Janssen Pharmaceuticals, Kaleido Biosciences, Lilly, Pfizer, Prometheus Biosciences, Reistone, Seres Therapeutics, Takeda, Target RWE, and Trellus Health. Axel Dignass reports fees for participation in clinical trials, review activities such as data monitoring boards, statistical analysis and end point committees from Abivax, AbbVie, Arena Pharmaceuticals, Bristol Myers Squibb/Celgene, Dr Falk Foundation, Galapagos, Gilead, Janssen, and Pfizer; consultancy fees from AbbVie, Amgen, Arena Pharmaceuticals, Biogen, Boehringer Ingelheim, Bristol Myers Squibb/Celgene, Celltrion, Dr Falk Foundation, Ferring Pharmaceuticals, Fresenius Kabi, Galapagos, Janssen, Lilly, MSD, Pfizer, Pharmacosmos, Roche/Genentech, Sandoz/Hexal, Takeda, Tillotts, and Vifor Pharma; payment from lectures including service on speakers bureaus from AbbVie, Biogen, CED Service GmbH, Celltrion, Falk Foundation, Ferring, Galapagos, Gilead, High5MD, Janssen, Materia Prima, MedToday, MSD, Pfizer, Streamed-Up, Takeda, Tillotts, and Vifor Pharma; payment for manuscript preparation from Falk Foundation, Takeda, Thieme, and UniMed Verlag. S Al Awadhi declares no conflict of interest. T Kobayashi has served as a speaker, a consultant or an advisory board member for AbbVie, Ajinomoto Pharma, Asahi Kasei Medical, Astellas, Alfresa Pharma, Celltrion, Covidien, EA Pharma, Eisai, Eli Lilly, Ferring Pharmaceuticals, Gilead Sciences, Janssen, JIMRO, Kyorin Pharmaceutical, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical, Nippon Kayaku, Pfizer, Takeda Pharmaceutical, Thermo Scientific, Zeria Pharmaceutical, and received research funding from AbbVie, Alfresa Pharma, Asahi Kasei Medical, EA Pharma, Kyorin Pharmaceutical, Mochida Pharmaceutical, Nippon Kayaku, Otsuka Holdings, Sekisui Medical, Thermo Fisher Scientific, Zeria Pharmaceutical. NSF Queiroz has served as a speaker and advisory board member of Janssen, Takeda, and Abbvie. M Calvo has participated as a speaker, trainer, or consultant in projects funded by MSD Spain, AbbVie, Takeda, Janssen, Pfizer, Dr. Falk, Faes Farma, Ferring, and Tillotts. PG Kotze has received honoraria from AbbVie, Ferring, Janssen, Pfizer and Takeda as a speaker and member of advisory boards; he also received scientific research grants from Pfizer and Takeda. S Ghosh declares consulting fees from Pfizer, Janssen, AbbVie, Takeda, Bristol-Myers Squibb, Receptos, Celgene, Gilead, Eli Lilly and Boehringer Ingelheim and speaker fees from AbbVie, Janssen, Takeda, Ferring, Pfizer, Shield, and Falk Pharma; outside of the submitted work. L Peyrin-Biroulet has served as a speaker, consultant and advisory board member for Merck, Abbvie, Janssen, Genentech, Mitsubishi, Ferring, Norgine, Tillots, Vifor, Hospira/Pfizer, Celltrion, Takeda, Biogaran, Boerhinger-Ingelheim, Lilly, HAC Pharma, Index Pharmaceuticals, Amgen, Sandoz, Forward Pharma GmbH, Celgene, Biogen, Lycera, Samsung Bioepis, Theravance. S Danese has served as a speaker, consultant, and advisory board member for Schering-Plough, AbbVie, Actelion, Alphawasserman, AstraZeneca, Cellerix, Cosmo Pharmaceuticals, Ferring, Genentech, Grunenthal, Johnson and Johnson, Millenium Takeda, MSD, Nikkiso Europe GmbH, Novo Nordisk, Nycomed, Pfizer, Pharmacosmos, UCB Pharma and Vifor.
References
- Chen, B.; Nagai, S.; Armitage, J.O.; Witherspoon, B.; Nabhan, C.; Godwin, A.C.; Yang, Y.T.; Kommalapati, A.; Tella, S.H.; DeAngelis, C.; et al. Regulatory and Clinical Experiences with Biosimilar Filgrastim in the U.S., the European Union, Japan, and Canada. Oncologist 2019, 24, 537–548. [Google Scholar] [CrossRef] [PubMed]
- Solitano, V.; D’Amico, F.; Da Rio, L.; Peyrin-Biroulet, L.; Danese, S. The European Perspective and History on Biosimilars for the Treatment of Inflammatory Bowel Diseases. Crohns Colitis 360 2021, 3, otab012. [Google Scholar] [CrossRef]
- Danese, S.; Gomollon, F.; Governing, B.; Operational Board of, E. ECCO position statement: the use of biosimilar medicines in the treatment of inflammatory bowel disease (IBD). J Crohns Colitis 2013, 7, 586–589. [Google Scholar] [CrossRef]
- Jha, D.; Mishra, R.K.; Pandey, R. Biosimilars: Current regulatory perspective and challenges. J Pharm Bioallied Sci 2013, 5, 80–81. [Google Scholar] [CrossRef] [PubMed]
- Declerck, P.; Farouk-Rezk, M.; Rudd, P.M. Biosimilarity Versus Manufacturing Change: Two Distinct Concepts. Pharm Res 2016, 33, 261–268. [Google Scholar] [CrossRef]
- Desanvicente-Celis, Z.; Gomez-Lopez, A.; Anaya, J.M. Similar biotherapeutic products: overview and reflections. Immunotherapy 2012, 4, 1841–1857. [Google Scholar] [CrossRef] [PubMed]
- Danese, S.; Fiorino, G.; Michetti, P. Viewpoint: knowledge and viewpoints on biosimilar monoclonal antibodies among members of the European Crohn’s and Colitis Organization. J Crohns Colitis 2014, 8, 1548–1550. [Google Scholar] [CrossRef]
- Bernasko, N.; Clarke, K. Why Is There Low Utilization of Biosimilars in Inflammatory Bowel Disease Patients by Gastroenterology Advanced Practice Providers? Crohns Colitis 360 2021, 3, otab004. [Google Scholar] [CrossRef]
- Solitano, V.; D’Amico, F.; Fiorino, G.; Peyrin-Biroulet, L.; Danese, S. Biosimilar switching in inflammatory bowel disease: from evidence to clinical practice. Expert Rev Clin Immunol 2020, 16, 1019–1028. [Google Scholar] [CrossRef]
- D’Amico, F.; Solitano, V.; Peyrin-Biroulet, L.; Danese, S. Nocebo effect and biosimilars in inflammatory bowel diseases: what’s new and what’s next? Expert Opin Biol Ther 2021, 21, 47–55. [Google Scholar] [CrossRef]
- Maltz, R.M.; McClinchie, M.G.; Boyle, B.M.; McNicol, M.; Morris, G.A.; Crawford, E.C.; Moses, J.; Kim, S.C. Biosimilars for Pediatric Patients With Inflammatory Bowel Disease: Pediatric Gastroenterology Clinical Practice Survey. J Pediatr Gastroenterol Nutr 2023, 76, 616–621. [Google Scholar] [CrossRef]
- Cohen, H.; Beydoun, D.; Chien, D.; Lessor, T.; McCabe, D.; Muenzberg, M.; Popovian, R.; Uy, J. Awareness, Knowledge, and Perceptions of Biosimilars Among Specialty Physicians. Adv Ther 2017, 33, 2160–2172. [Google Scholar] [CrossRef]
- Sharma, A.; Minh Duc, N.T.; Luu Lam Thang, T.; Nam, N.H.; Ng, S.J.; Abbas, K.S.; Huy, N.T.; Marusic, A.; Paul, C.L.; Kwok, J.; et al. A Consensus-Based Checklist for Reporting of Survey Studies (CROSS). J Gen Intern Med 2021, 36, 3179–3187. [Google Scholar] [CrossRef]
- Bernard, E.J.; Fedorak, R.N.; Jairath, V. Systematic Review: Non-medical Switching of Infliximab to CT-P13 in Inflammatory Bowel Disease. Dig Dis Sci 2020, 65, 2354–2372. [Google Scholar] [CrossRef]
- Garcia-Beloso, N.; Altabas-Gonzalez, I.; Samartin-Ucha, M.; Gayoso-Rey, M.; De Castro-Parga, M.L.; Salgado-Barreira, A.; Cibeira-Badia, A.; Pineiro-Corrales, M.G.; Gonzalez-Vilas, D.; Pego-Reigosa, J.M.; et al. Switching between reference adalimumab and biosimilars in chronic immune-mediated inflammatory diseases: A systematic literature review. Br J Clin Pharmacol 2022, 88, 1529–1550. [Google Scholar] [CrossRef]
- Peyrin-Biroulet, L.; Lonnfors, S.; Roblin, X.; Danese, S.; Avedano, L. Patient Perspectives on Biosimilars: A Survey by the European Federation of Crohn’s and Ulcerative Colitis Associations. J Crohns Colitis 2017, 11, 128–133. [Google Scholar] [CrossRef]
- Haghnejad, V.; Le Berre, C.; Dominique, Y.; Zallot, C.; Guillemin, F.; Peyrin-Biroulet, L. Impact of a medical interview on the decision to switch from originator infliximab to its biosimilar in patients with inflammatory bowel disease. Dig Liver Dis 2020, 52, 281–288. [Google Scholar] [CrossRef]
- Jorgensen, K.K.; Olsen, I.C.; Goll, G.L.; Lorentzen, M.; Bolstad, N.; Haavardsholm, E.A.; Lundin, K.E.A.; Mork, C.; Jahnsen, J.; Kvien, T.K.; et al. Switching from originator infliximab to biosimilar CT-P13 compared with maintained treatment with originator infliximab (NOR-SWITCH): a 52-week, randomised, double-blind, non-inferiority trial. Lancet 2017, 389, 2304–2316. [Google Scholar] [CrossRef]
- Hanauer, S.; Liedert, B.; Balser, S.; Brockstedt, E.; Moschetti, V.; Schreiber, S. Safety and efficacy of BI 695501 versus adalimumab reference product in patients with advanced Crohn’s disease (VOLTAIRE-CD): a multicentre, randomised, double-blind, phase 3 trial. Lancet Gastroenterol Hepatol 2021, 6, 816–825. [Google Scholar] [CrossRef]
- Gros, B.; Plevris, N.; Constantine-Cooke, N.; Lyons, M.; O’Hare, C.; Noble, C.; Arnott, I.D.; Jones, G.R.; Lees, C.W.; Derikx, L. Multiple infliximab biosimilar switches appear to be safe and effective in a real-world inflammatory bowel disease cohort. United European Gastroenterol J 2023, 11, 179–188. [Google Scholar] [CrossRef]
- Mazza, S.; Piazza, O.S.N.; Conforti, F.S.; Fasci, A.; Rimondi, A.; Marinoni, B.; Casini, V.; Ricci, C.; Munari, F.; Pirola, L.; et al. Safety and clinical efficacy of the double switch from originator infliximab to biosimilars CT-P13 and SB2 in patients with inflammatory bowel diseases (SCESICS): A multicenter cohort study. Clin Transl Sci 2022, 15, 172–181. [Google Scholar] [CrossRef]
- Trystram, N.; Abitbol, V.; Tannoury, J.; Lecomte, M.; Assaraf, J.; Malamut, G.; Gagniere, C.; Barre, A.; Sobhani, I.; Chaussade, S.; et al. Outcomes after double switching from originator Infliximab to biosimilar CT-P13 and biosimilar SB2 in patients with inflammatory bowel disease: a 12-month prospective cohort study. Aliment Pharmacol Ther 2021, 53, 887–899. [Google Scholar] [CrossRef]
- Mahmmod, S.; Schultheiss, J.P.D.; van Bodegraven, A.A.; Dijkstra, G.; Gilissen, L.P.L.; Hoentjen, F.; Lutgens, M.; Mahmmod, N.; van der Meulen-de Jong, A.E.; Smits, L.J.T.; et al. Outcome of Reverse Switching From CT-P13 to Originator Infliximab in Patients With Inflammatory Bowel Disease. Inflamm Bowel Dis 2021, 27, 1954–1962. [Google Scholar] [CrossRef]
- Papamichael, K.; Afif, W.; Drobne, D.; Dubinsky, M.C.; Ferrante, M.; Irving, P.M.; Kamperidis, N.; Kobayashi, T.; Kotze, P.G.; Lambert, J.; et al. Therapeutic drug monitoring of biologics in inflammatory bowel disease: unmet needs and future perspectives. Lancet Gastroenterol Hepatol 2022, 7, 171–185. [Google Scholar] [CrossRef]
- Papamichael, K.; Stocco, G.; Ruiz Del Agua, A. Challenges in Therapeutic Drug Monitoring: Optimizing Biological Treatments in Patients With Inflammatory Bowel Disease and Other Immune-Mediated Inflammatory Diseases. Ther Drug Monit 2023. [Google Scholar] [CrossRef]
- Nguyen, N.H.; Solitano, V.; Vuyyuru, S.K.; MacDonald, J.K.; Syversen, S.W.; Jorgensen, K.K.; Crowley, E.; Ma, C.; Jairath, V.; Singh, S. Proactive Therapeutic Drug Monitoring Versus Conventional Management for Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis. Gastroenterology 2022, 163, 937–949 e932. [Google Scholar] [CrossRef]
- Lontai, L.; Gonczi, L.; Balogh, F.; Komlodi, N.; Resal, T.; Farkas, K.; Molnar, T.; Miheller, P.; Golovics, P.A.; Schafer, E.; et al. Non-medical switch from the originator to biosimilar and between biosimilars of adalimumab in inflammatory bowel disease - a prospective, multicentre study. Dig Liver Dis 2022, 54, 1639–1645. [Google Scholar] [CrossRef]
- Lamfers M, V.A.G.; Leenstra, S.; Venkatesan, S. Overview of the patent expiry of (non-)tyrosine kinase inhibitors approved for clinical use in the EU and the US. Generics and Biosimilars Initiative Journal (GaBI Journal) 2017, 6. [Google Scholar] [CrossRef]
- Epstein, M.S.; Ehrenpreis, E.D.; Kulkarni, P.M.; Gastroenterology, F.D.-R.M.C.o.t.A.C.o. Biosimilars: the need, the challenge, the future: the FDA perspective. Am J Gastroenterol 2014, 109, 1856–1859. [Google Scholar] [CrossRef]
- Chow, V.; Mytych, D.T.; Das, S.; Franklin, J. Pharmacokinetic Similarity of ABP 654, an Ustekinumab Biosimilar Candidate: Results from a Randomized, Double-blind Study in Healthy Subjects. Clin Pharmacol Drug Dev 2023. [Google Scholar] [CrossRef]
- Rogler, G.; Singh, A.; Kavanaugh, A.; Rubin, D.T. Extraintestinal Manifestations of Inflammatory Bowel Disease: Current Concepts, Treatment, and Implications for Disease Management. Gastroenterology 2021, 161, 1118–1132. [Google Scholar] [CrossRef]
- Singh, S.; Boland, B.S.; Jess, T.; Moore, A.A. Management of inflammatory bowel diseases in older adults. Lancet Gastroenterol Hepatol 2023, 8, 368–382. [Google Scholar] [CrossRef]
- D’Amico, F.; Fiorino, G.; Furfaro, F.; Allocca, M.; Roda, G.; Loy, L.; Zilli, A.; Solitano, V.; Peyrin-Biroulet, L.; Danese, S. Patient’s profiling for therapeutic management of inflammatory bowel disease: a tailored approach. Expert Rev Gastroenterol Hepatol 2020, 14, 765–773. [Google Scholar] [CrossRef]
- Liu, Y.; Yang, M.; Garg, V.; Wu, E.Q.; Wang, J.; Skup, M. Economic Impact of Non-Medical Switching from Originator Biologics to Biosimilars: A Systematic Literature Review. Adv Ther 2019, 36, 1851–1877. [Google Scholar] [CrossRef]
Figure 1.
Characteristics of survey respondents (a) age; (b) sex; (c) geographic representation.
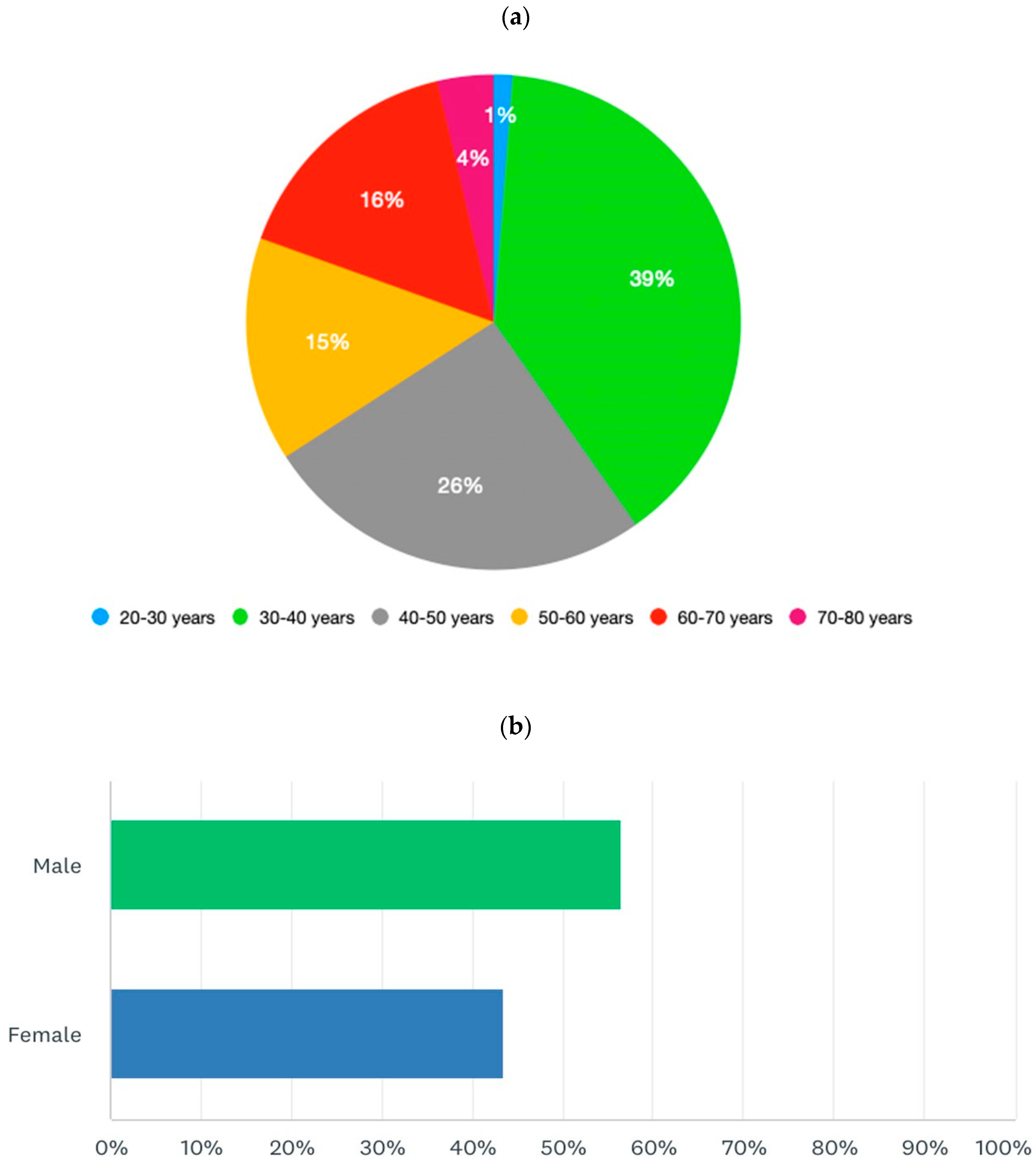
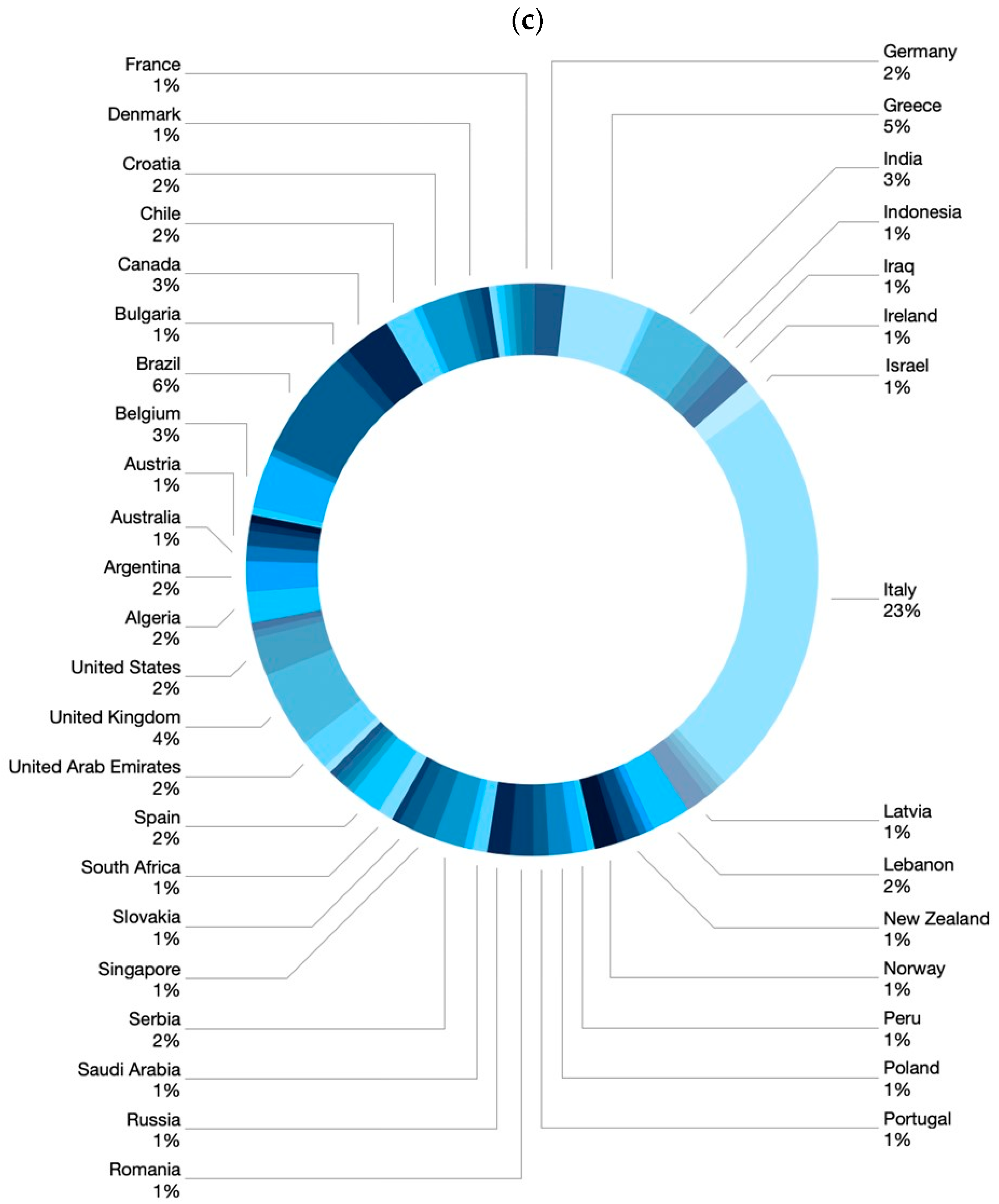
Figure 2.
Replies to Q27 “If you prescribe originator drugs despite the availability of the biosimilars, why do you prefer the originator drug?”.
Figure 2.
Replies to Q27 “If you prescribe originator drugs despite the availability of the biosimilars, why do you prefer the originator drug?”.

Figure 3.
Replies to Q46. “How would you implement the use of biosimilars in clinical practice (multiple answers are possible)?”.
Figure 3.
Replies to Q46. “How would you implement the use of biosimilars in clinical practice (multiple answers are possible)?”.
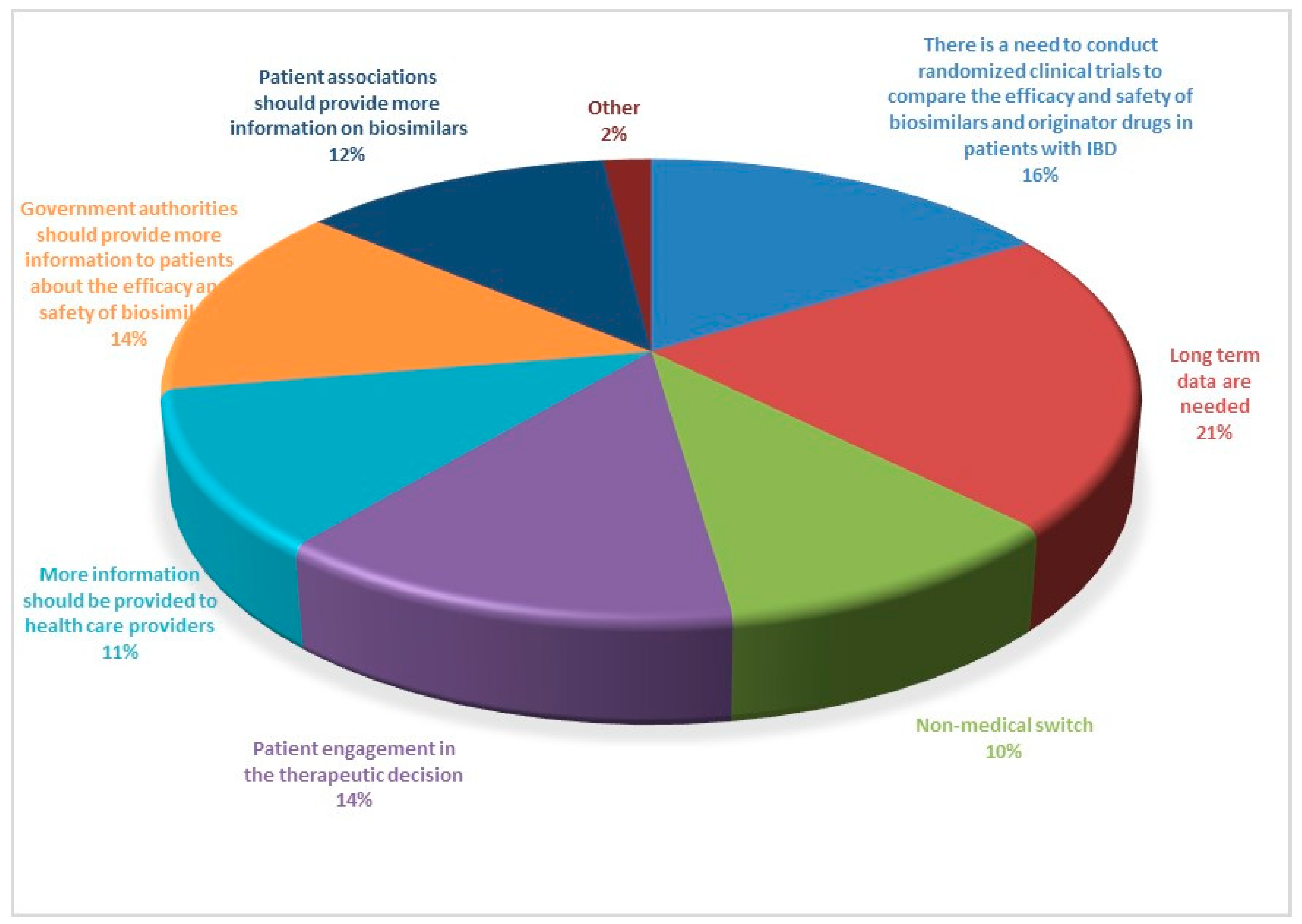

Table 1.
Survey and 5 domains.
|
Part 1 Demographics, specialty, and level of experience of participants Q1. Age in years Q2. Sex Q3. What country do you work in? Q4. What is your specialization? Q5. How many years of experience do you have in the field of IBD? Q6. How many IBD patients do you see per year? Part 2 Practices and attitudes toward the use of biosimilar in clinical practice Q7. In your opinion, which of the following statements is correct? Q8. How confident are you about the use of biosimilars using a scale from 0 (lowest value) to 10 (highest value)? Q9. How confident are your patients about the use of biosimilars using a scale from 0 (lowest value) to 10 (highest value)? Q10. Do you think the data on biosimilars extrapolated from other immune mediated inflammatory diseases are also valid in IBD? Q11. Do you think patients should be informed about what a biosimilar is before starting therapy? Q12. Who should provide information to patients about biosimilars? Q13. Before prescribing a biological drug, do you explain to patients what a biosimilar drug is and what the originator drug is? Q14. Do you provide patients with data comparing biosimilars and originator drugs? Q15. Do you provide written materials to patients informing them on the use of biosimilars? Q16. Have you ever prescribed biosimilars of infliximab? Q17. Have you ever prescribed biosimilars of adalimumab? Q18. Do you think biosimilars should only be prescribed to naïve patients? Q19. Have you ever switched a patient from the originator drug to the biosimilar? Q20. If you answered yes to question 19, why did you switch from the originator drug to the biosimilar? Q21. When do you switch from the originator to the biosimilar? Q22. Do you monitor drug trough levels and autoantibodies in patients switched to biosimilars? Q23. Do you have patients who have refused to start therapy with a biosimilar or switch to a biosimilar? Q24. If you have patients who refused to be treated with a biosimilar, what is the proportion of these patients? Q25. What is the main reason for patients’ refusal of the biosimilar? Q26. Despite the availability of biosimilars, do you prescribe originator drugs? Q27. If you prescribe originator drugs despite the availability of the biosimilars, why do you prefer the originator drug? Q28. In a patient candidate for biologic therapy, have you ever started IBD therapy using biosimilars? Part 3. Interchangeability (reverse and multiple switch) Q29. In a patient who started a biosimilar as first drug, have you ever switched to the originator drug? Q30. If you answered yes to question 29, why were the patients switched from the biosimilar to the originator drug (multiple answers are possible)? Q31. If you answered yes to question 29, did patients switched from the biosimilar to the originator drug achieve/maintain disease remission? Q32. Have you ever switched from one biosimilar to another biosimilar of the same drug (multiple switch)? Q33. If you have multiple switched patients, why were the patients switched from one biosimilar to another (multiple answers are possible)? Q34. Did multiple switched patients achieve/maintain disease remission? Q35. In a patient treated with the originator drug and then switched to the biosimilar, have you ever prescribed the reverse switch to the originator drug? Q36. If you have patients undergoing reverse switch, what was the reason for reverse switch (multiple answers are possible)? Q37. Did reverse switched patients achieve/maintain disease remission? Part 4. Nocebo effect and non-medical switch Q38. Do you know what the nocebo effect is? Q39. Have your patients ever experienced the nocebo effect? Q40. If your patients experienced the nocebo effect, what is the rate of nocebo effect among your patients? Q41. Do you have patients who underwent a non-medical switch? Q42. Did non-medical switched patients achieve/maintain disease remission? Part 5. Current and future perspectives Q43. Does the presence of biosimilars have an impact on your therapeutic choices? Q44. In the near future, will you be prescribing biosimilars of vedolizumab, ustekinumab, and tofacitinib? Q45. Do you think the availability of the biosimilars of vedolizumab, ustekinumab, and tofacitinib will change the treatment algorithm of IBD patients? Q46. How would you implement the use of biosimilars in clinical practice (multiple answers are possible)? |
Table 2.
Approved statements and agreement after the second round of voting.*after the second round of voting.
Table 2.
Approved statements and agreement after the second round of voting.*after the second round of voting.
| Statements | Agreement >75% (%) |
|
|---|---|---|
| 1 | Biosimilars are as effective and safe as the originator drugs. | 100% |
| 2 | Biosimilars can be used both in biologic-naïve patients and in patients already treated with the originator drugs. | 100% |
| 3 | The main reason for switching from an originator drug to a biosimilar is its lower cost. | 100% |
| 4 | Switch from an originator drug to a biosimilar can be performed at any time. | 82% |
| 5 | The switch from an originator drug to a biosimilar is effective and safe. | 100% |
| 6 | Multiple switches from one biosimilar to another are feasible in case of drug unavailability. | 100% |
| 7 | We do not recommend multiple switches in case of loss of response to a biosimilar. | 100%* |
| 8 | There is no need to modify the regular practice in monitoring drug trough levels and antibodies in patients switched from the originator drug to the biosimilar. | 90%* |
| 9 | The non-medical switch is a way to reduce costs associated with advanced therapies and increase accessibility. | 100% |
| 10 | In the near future, non-anti-TNF biosimilar drugs are expected to alter the therapeutic algorithm in patients with inflammatory bowel diseases. | 100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



