
Submitted:
30 August 2023
Posted:
31 August 2023
You are already at the latest version
Abstract
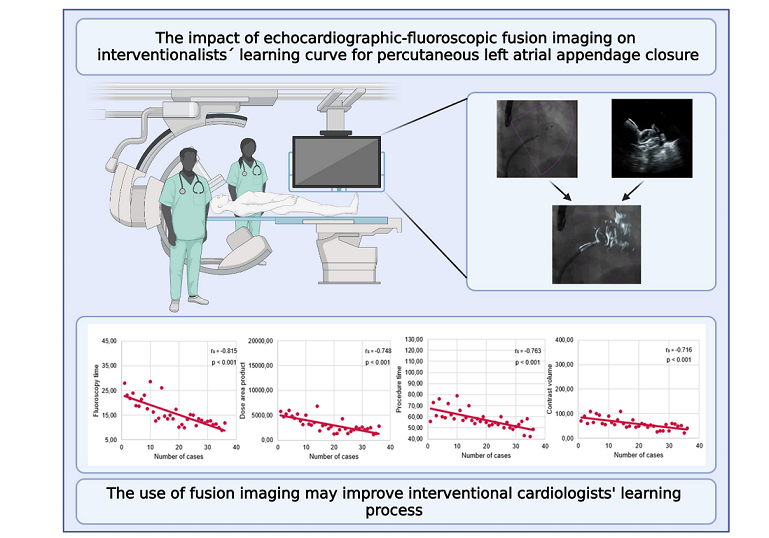
Due to the complex and variable anatomy of the left atrial appendage, percutaneous left atrial appendage closure (LAAC) can be challenging. In this study, we investigated the impact of fusion imaging (FI) on the LAAC learning curve of 2 interventionalists. The first interventionalist (IC 1) was initially trained without FI and continued his training with FI. The second interventionalist (IC 2) performed all procedures with FI. We compared the first 36 procedures without FI of IC 1 (group 1) with his next 36 interventions with FI (group 2). Furthermore, group 1 was compared to 36 procedures of IC 2 who directly started his training with FI (group 3). Group 1 demonstrated that the learning curve without FI has a flat course with weak correlations for fluoroscopy time, contrast volume, and procedure time, but not for dose area product. Group 2 with FI showed improvement with a steep course and strong correlations for all 4 parameters. In group 3 we also saw a steep progression with strong correlations. Furthermore, the mean measurements of the procedural parameters in the groups with FI decreased significantly as indicator for procedural efficacy. We demonstrated that FI may improve the learning curve of experienced and non-experienced ICs.
Keywords:
structural heart disease
; left atrial appendage closure
; fusion imaging
; learning curve
1. Introduction
Percutaneous left atrial appendage closure (LAAC) has become a commonly used alternative for stroke prevention worldwide in patients with non-valvular atrial fibrillation, who are not eligible for oral anticoagulation (class IIb recommendation) [1]. Large multicenter trials such as PROTECT AF, PREVAIL, or PRAGUE-17 have already shown that LAAC provides comparable stroke prevention to vitamin K antagonists (VKAs) or novel oral anticoagulants (NOACs), with a reduction in complications such as bleeding or mortality [2,3]. Periprocedural imaging is essential when performing LAAC due to the considerable differences in size, shape, and relationship to neighboring structures such as left pulmonary artery, left upper pulmonary vein, and circumflex artery [4]. Besides, percutaneous interventions involve challenges such as navigation of the catheter and implantation of the device on a beating heart as well as the learning curve of the interventionalists [5]. Recent studies demonstrated that by improving the aspects such as design of the devices, periprocedural imaging, and the experience of cardiologists, the complication rate of periinterventional life-threatening events such as pericardial effusion with cardiac tamponade, ischemic stroke, arrhythmias, bleeding, and increased 30-day mortality was significantly reduced [6]. Intraprocedural steps such as a transseptal puncture (TSP), optimal device sizing, and ultimately the implantation of the occlude device require great precision, because underestimation can lead to dislocation of the occluder device or peri-device leak, and oversizing may cause tamponade or embolization as well [7,8]. Thus, optimizing the interventionalist’s learning curve is of foremost importance as emphasized by current European and American expert consensus [9,10]. Previous studies have shown that the performance and safety of percutaneous LAAC have steadily improved with operator experience, and that 30 procedures are required to reach proficiency and optimize clinical outcomes [11,12]. It is recommended to perform procedural imaging with transoesophageal echocardiography (TEE) or intracardiac echocardiography (ICE) [6,13]. Unfortunately, although TEE allows visualization of the soft tissues of the cardiac structures, there are limitations in the visualization of the catheter systems and devices used, therefore the simultaneous use of fluoroscopy is indispensable [14]. Through the application of fusion imaging (FI), the interventionalist no longer needs to mentally combine information from both imaging modalities, which can be very complex and require a good spatial imagination [15]. Instead, they are fused in real-time and displayed on one screen and on the same image. This, guidance and navigation of catheters or devices while performing procedures can be facilitated [16]. We recently demonstrated the procedural advantages of FI for LAAC [17]: It reduces the procedure time, the time to transseptal puncture, and the periprocedural amount of contrast agent. Data about real-time echocardiography-fluoroscopy fusion imaging´s (FI) impact on the interventionalist’s learning curve during LAAC are lacking. Therefore, we aimed to evaluate its impact on an interventional cardiologist’s (IC) learning curve.
2. Materials and Methods
2.1. Study design
We performed a retrospective single-center study and analyzed data of two interventional cardiologists (ICs), who performed 273 LAAC between 2011 and 2022 at our heart center (see Figure 1). The first interventionalist (IC 1) was experienced in both coronary and structural interventions (level of competence V defined by EAPCI [18]) and worked with FI (N = 180; + FI) and without FI (N = 36; -FI). The second interventionalist (IC 2) was also experienced (level of competence IV) but was a novice at LAAC. Furthermore, he performed all procedures with FI (N = 57) as the FI technique was already established when he started his training.
The first 36 procedures without FI of IC 1 (group 1) were compared with his next 36 interventions with FI (group 2). Furthermore, group 1 was analyzed with the first 36 procedures of the IC 2 which were performed with FI right from the beginning (group 3). According to the Declaration of Helsinki, the study was approved by the local ethics committee (number 5277R) and registered at clinical trials (NCT02608008). Written informed consent was obtained from all patients.
2.2. Intervention
All procedures were performed minimally invasive under conscious sedation and local anesthesia in our catheterization laboratory according to a standardized protocol [19]. Only TEE and fluoroscopy were used for periprocedural guidance. Initially, TEE was used to exclude a possible left atrial appendage (LAA) thrombus and active endocarditis, which would be a contraindication to perform the intervention. A radial arterial catheter was inserted to monitor and measure hemodynamics. Under echocardiographic and fluoroscopic guidance, the transseptal puncture was performed posteriorly and inferiorly. After a successful transseptal puncture, the transseptal sheath and a pigtail catheter were advanced to the left atrium, and anticoagulation with heparin was started to prevent potential thrombus formation. During the examination, the activated clotting time was regularly monitored to achieve a target value of approximately 250 seconds. The sizing of the implanted device was based on the maximum Landing zone diameter according to the manufacturer's instructions. After the implantation, we confirmed the final position of the device using TEE, tug-test, and injections of contrast medium.
2.3. Real-time echocardiography-fluoroscopy fusion (FI) imaging during LAAC
FI has been recently introduced and aims to facilitate essential steps during structural heart disease interventions [20]. It is a sophisticated tool that allows a real-time two- and/or three-dimensional TEE imaging and fluoroscopic imaging overlay using the EchoNavigator ® System Release II (Philips Healthcare, Andover, MA). Calibration of TEE probe with fluoroscopy is achieved by an automatic tracking and localization of the TEE probe in relation to the C-arm angulation, based on fluoroscopic imaging data. The calibration was performed in Right Anterior Oblique (RAO) 30° / Cranial 20° und RAO 30° / Caudal 20° and within a few seconds. When the co-registration was successful, both the C-arm and TEE probes were detected, and an overlay of both imaging modalities was displayed in real-time. Furthermore, static markers could be set to gain a better orientation in a regions of interest like site of TSP, coumadin ridge, and circumflex artery. Fluoroscopy is essential for catheter and devices visualization whereas echocardiography provides spatial orientation. When the image is readjusted, these markers are automatically updated. With echocardiographic data continuously displayed within the fluoroscopic images, it was possible to accurately follow the anatomy of the soft issue anatomy under continuous accordance with respiratory and cardiac cycle movements [21].
2.4. Learning curve and procedural parameters
To evaluate the learning curve, the changes in procedure parameters over time were considered and presented as correlations. The following procedural parameters were investigated: procedural success, procedure time (PT), contrast volume (CV), fluoroscopy time (FT), and dose area product (DAP). Outcome analysis included patient characteristics and complications according to the Munich consensus [22] such as pericardial effusion, bleeding, vascular complications, ischemic and hemorrhagic stroke, dislocation, and arrhythmia.
Successful performance of the procedure was defined as successful implantation of an occluder device. Total procedure time was defined as the time from local anesthesia to completion of TEE with documentation of a good result. Fluoroscopy time was expressed in minutes, whereas the area-dose product was expressed in cGy*cm2. To evaluate and asses the severity of bleeding symptoms we used the ISTH/SSC bleeding assessment tool [23]. All haemorrhages with a score of 4 points (blood transfusion, replacement therapy or desmopressin) were considered. Arteriovenous fistula, pseudoaneurysm, arterial stenosis, or groin bleeding were all considered vascular complications.
2.5. Statistical analysis
Statistical data analysis was performed using SPSS Statistics (version 27.0, SPSS Inc., IBM, Armonk, NY). To prove the normal distribution of the data the Shapiro–Wilk test was performed. Categorical variables were expressed as absolute numbers with percentages. Continuous variables were expressed as medians with interquartile range (IQR) or mean with standard deviation (SD). For continuous variables, Mann-Whitney-U-Test or Kruskal-Wallis were used. The learning curves were analysed by correlation analysis by Spearman's rho. Statistical significance was defined at P-Values < 0.05.
3. Results
3.1. Patient characteristics
The mean age was between 74 and 78 years (74.81 ± 9.12 vs. 78.03 ± 6.23 vs. 75.11 ± 9.12, p = 0.222). There were no significant differences in patient characteristics between the three groups besides Has-Bled Score: 3 ± 1 vs 4 ± 1 vs 2 ± 1 (P < 0.001). The most common comorbidities included: arterial hypertension 88.89 % vs. 91.67 % vs. 94.44 %, p = 0.695), hypercholesterolemia (83.33 % vs. 77.78 % vs. 72.22 %, p = 0.526), and coronary artery disease (CAD) (80.56 % vs. 61.11 % vs. 55.56 %, p = 0.064). Further details are displayed in Table 1.
3.2. Learning curve analyses
All procedures were performed successfully with the ACP/Amplatzer™ Amulet™ LAA Occluder (Abbott, Chicago, Illinois). The courses of the learning curves over time are presented in Figure 2.
3.3. Learning curve analysis of Interventionalist 1:
Group 1 (IC 1, without FI) reveals a flat course with weak correlations for fluoroscopy time (rs = - 0.255, p = 0.133), procedure time (rs = - 0.066, p = 0.702) and contrast volume (rs = - 0.041, p = 0.812). Only for the dose area product, the correlation was moderate (rs = - 0.521, p = 0.002).
Group 2 (IC 1, with FI) showed improvement with a steep course and strong correlations for all parameters: fluoroscopy time (rs = -0.691, P < 0.001), dose area product (rs = -0.727, p < 0.001), procedure time (rs = -0.821, P < 0.001) and contrast volume (rs = -0.761, p < 0.001).
3.4. Learning curve analysis of Interventionalist 2
The analysis of IC 2 with FI’s (group 3) learning curve revealed a steep progression of the learning curve and strong correlations were shown as follows: fluoroscopy time (rs = -0.815, p < 0.001), dose area product (rs = -0.748, p = 0.001), procedure time (rs = 0.763, p < 0.001) and contrast volume (rs = 0.716, p = 0.001).
3.5. Analysis of FI’s impact on learning curves
As a next step we assessed the influence of FI on the learning curves by comparing IC 1 learning curve with (group 1) and without FI (group 2). Furthermore, we evaluated IC 1 and 2 learning curve (group 2 and 3) with FI, with IC 1 curve without FI (group 1). Procedural parameters in the groups with FI improved significantly compared to the group without FI (see Table 2 and Table 3).
Considering the fluoroscopy time, we demonstrated a significant difference between the first 36 procedures of IC 1 without FI (group1; 18.55 min ± 8.33 min) and his next 36 procedures with FI (group 2; 12.45 min ± 4.47 min) (p < 0.001). Comparing the latter group with IC 2 (group 3, with FI) (13.65 min ± 7.02 min), fluoroscopy time was also significantly shorter (p = 0.038). Furthermore, dose area product differed significantly in the first group (IC 1, without FI (5034.05 cGy*cm2 ± 4303.95 cGy*cm2)) compared to the second (IC 1 without FI, (4368.60 cGy*cm2 ± 2087.25 cGy*cm2, p = 0.039)) and third group (IC 2, with FI (2787.20 cGy*cm2 ± 2284.38 cGy*cm2, p < 0.001)). The procedure time was significantly longer in the group without FI (group 1, IC 1) with 68.50 min ± 26.75 min significantly longer than in group 2 and 3 (59.00 min ± 7.50 min, p = 0.004) and group 3 (56.50 min ± 7.00 min, p = 0.003). In the group without FI 145.00 ml ± 100.00 ml contrast medium was used. This was significantly more than in the second group (IC 1, with FI; 63.50 ml ± 30.00 ml, P < 0.001) and in the third group (IC 2, with FI; 55.00 ml ± 22.50 ml, p < 0.001).
3.6. Procedural complications
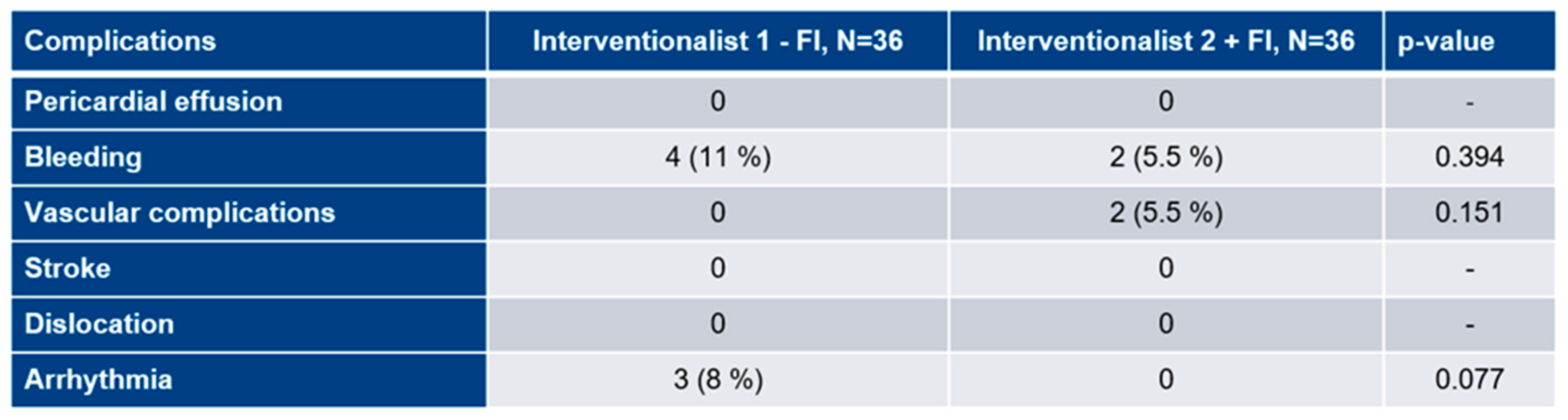
There was no significant difference in procedural complications comparing group 1 without FI and the groups 2 and 3 with FI (see Table 4 and Table 5): 4 patients in the group without FI suffered a bleeding with an ISTH/SSC score of 4 (11%). In group 2 there was one patient (p = 0.164) whereas in group 3 two patients (p = 0.392). Arrhythmias occurred in 3 subjects in the first group only (p = 0.077). However, there were no vascular complications in the group without FI. In comparison, there was one vascular complication in the second group and two in the third group (p = 0.151). No pericardial effusion, stroke, or dislocation were observed in all groups.
4. Discussion
The purpose of this study was to evaluate the impact of real-time FI on the learning curve of interventionalists during left atrial appendage closure.
Based on the analysis of our data, the findings are as follows:
- Left atrial appendage closure learning curve has a flat course without FI.
- FI may improve the left atrial appendage closure learning curve.
- Even highly experienced interventionalists may benefit from FI guidance in their early phase of left atrial appendage closure training.
The initial stages during interventional cardiology training are crucial for acquiring the necessary skills and ensuring patient safety, as the expert consensus summarized the key points of training of new interventionalists: "master the technique, know the device, know the patient" [19,24]. Depending on the complexity of the procedures, the progressions may vary [25]. In contrast to basic diagnostic procedures, such as coronary angiography, more complex interventions, such as structural heart interventions, may require a longer training period [26]. Salemi et al. showed based on data of 207 interventionalists that risk-adjusted in-hospital outcomes were improved by increased TAVR experience of operators [27]. Chhatriwalla et al. demonstrated that also the operator experience of transcatheter mitral valve repair was associated with improvements in procedural success, reduction of procedure time, and procedural complications [28].
Besides, structural heart disease interventions require not only an enhanced training in technical skills but also a thorough training in multimodal imaging in order to gain comprehensive knowledge of cardiac anatomy, in particularly for LAAC, of the left atrium, LAA, and surrounding structures [29]. Due to the highly variable and complex LAA anatomy e.g., the LAAC can be challenging [30]. Jung et al. demonstrated in a large multicenter study involving 83 hospitals and a total of 13651 LAAC procedures that 30 cases are necessary to achieve optimal safety of LAAC [12]. Therefore, we performed our analysis of the learning curves of both interventional cardiologists based on this study and divided our study population in three groups with at least > 30 patients. Despite of the retrospective fashion of our study, we were able to demonstrate that FI guidance leads to a steep improvement of the learning curve already during initial phase of training comparing to the group without FI and a flat learning curve. The pivotal role of imaging during LAAC and its impact on the early operator learning curve was also demonstrated by Wang et al. in a single-center study with 53 patients [31]. Hereby, the application of three-dimensional computed tomographic image guidance to WATCHMAN implantation and the impact on the early operator learning curve was assessed and it demonstrated that it could have a positive impact. In contrast to three-dimensional computed tomographic imagine FI is a tool that facilitates spatial orientation in real-time, by integrating information from fluoroscopic and echocardiographic images as one overlay in the Cath lab [32]. Furthermore, there were no differences in the occurrence of complications when assessing FI guidance. Interestingly, Ledwoch et al. showed in a study with 90 patients that, the population was divided into 3 groups, that procedure time, fluoroscopy time, and contrast volume were reduced across the 3 groups [11]. Furthermore, in-hospital complications decreased significantly and the compression grade of the occluder device was chosen higher with an increasing learning curve. As a matter of fact, our study demonstrated that FI guidance might be useful during training through optimizing the learning curve, thereby achieving less procedure time, decreased amount of contrast agent as well as dose-area product and less fluoroscopy time faster than without FI.
5. Limitations
Our study has a few limitations. First, this is a single-center analysis. Second, the data were collected retrospectively. Further multicenter, prospective, randomized studies with more cardiologists, patients, and implantations with other LAA closure systems are needed to prove the usefulness of FI during an IC training.
6. Summary
This is the first study to examine the impact of FI on the learning curve for LAAC. We demonstrated that FI may improve the learning process of interventional cardiologists. FI may be beneficial especially during the first phase of training by facilitating three-dimensional spatial understanding and orientation and thus providing more confidence to an IC in training.
Authors Contributions
Study concept and design: Kanschik, Afzal, Zeus. Acquisition, analysis, or interpretation of data: All authors. Drafting of the manuscript: Kanschik, Afzal. Critical revision of the manuscript for important intellectual content: Heidari, Klein, Polzin, Veulemanns, Kelm, Jung, Zeus. Statistical analysis: Kanschik, Afzal. Obtained funding: none. Administrative, technical, or material support: Kanschik, Afzal, Zeus. Study supervision: Afzal, Zeus.
Funding
This research received no external funding.
Institutional Review Board Statement
According to the Declaration of Helsinki, the study was approved by the local ethics committee (number 5277R) and registered at clinical trials (NCT02608008).
Informed Consent Statement
Written informed consent was obtained from all patients.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| BMI | Body Mass Index |
| CAD | Coronary Artery Disease |
| CKD | Chronic Kidney Disease |
| COPD | Chronic Obstructive Pulmonary Disease |
| CV | Contrast Volume |
| DAP | Dose Area Product |
| EAPCI | European Association of Percutaneous Cardiovascular Interventions |
| FI | Fusion Imaging |
| FT | Fluoroscopy Time |
| IC | Interventional Cardiologist |
| IQR | Interquartile Range |
| LA | Left Atrium |
| LAA | Left Atrial Appendage |
| LAAC | Left Atrial Appendage Closure |
| MACE | Major Adverse Cardiac Events |
| NOAC | Novel oral anticoagulant |
| PT | Procedure Time |
| RAO | Right Anterior Oblique |
| SD | Standard Deviation |
| TEE | Transoesophageal Echocardiography |
| TSP | Transseptal Puncture |
| VKA | Vitamin K Antagonist |
References
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrom-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Reddy, V.Y.; Doshi, S.K.; Kar, S.; Gibson, D.N.; Price, M.J.; Huber, K.; Horton, R.P.; Buchbinder, M.; Neuzil, P.; Gordon, N.T.; et al. 5-Year Outcomes After Left Atrial Appendage Closure: From the PREVAIL and PROTECT AF Trials. J Am Coll Cardiol 2017, 70, 2964–2975. [Google Scholar] [CrossRef] [PubMed]
- Osmancik, P.; Herman, D.; Neuzil, P.; Hala, P.; Taborsky, M.; Kala, P.; Poloczek, M.; Stasek, J.; Haman, L.; Branny, M.; et al. 4-Year Outcomes After Left Atrial Appendage Closure Versus Nonwarfarin Oral Anticoagulation for Atrial Fibrillation. J Am Coll Cardiol 2022, 79, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Wunderlich, N.C.; Beigel, R.; Swaans, M.J.; Ho, S.Y.; Siegel, R.J. Percutaneous interventions for left atrial appendage exclusion: options, assessment, and imaging using 2D and 3D echocardiography. JACC Cardiovasc Imaging 2015, 8, 472–488. [Google Scholar] [CrossRef] [PubMed]
- Biaggi, P.; Sager, D.F.; Kulling, J.; Kuest, S.; Wyss, C.; Hurlimann, D.; Reho, I.; Buhler, I.; Noll, G.; Huber, M.; et al. Potential Value of Fusion Imaging and Automated Three-Dimensional Heart Segmentation During Transcatheter Aortic Valve Replacement. J Am Soc Echocardiogr 2020, 33, 516–517.e511. [Google Scholar] [CrossRef]
- Holmes, D.R., Jr.; Korsholm, K.; Rodés-Cabau, J.; Saw, J.; Berti, S.; Alkhouli, M.A. Left atrial appendage occlusion. EuroIntervention 2023, 18, e1038–e1065. [Google Scholar] [CrossRef]
- Qamar, S.R.; Jalal, S.; Nicolaou, S.; Tsang, M.; Gilhofer, T.; Saw, J. Comparison of cardiac computed tomography angiography and transoesophageal echocardiography for device surveillance after left atrial appendage closure. EuroIntervention 2019, 15, 663–670. [Google Scholar] [CrossRef]
- Freixa, X.; Aminian, A.; Tzikas, A.; Saw, J.; Nielsen-Kudsk, J.E.; Ghanem, A.; Schmidt, B.; Hildick-Smith, D. Left atrial appendage occlusion with the Amplatzer Amulet: update on device sizing. J Interv Card Electrophysiol 2020, 59, 71–78. [Google Scholar] [CrossRef]
- Simsek, B.; Kostantinis, S.; Karacsonyi, J.; Hakeem, A.; Prasad, A.; Prasad, A.; Bortnick, A.E.; Elbarouni, B.; Jneid, H.; Abbott, J.D.; et al. Educational Experience of Interventional Cardiology Fellows in the United States and Canada. JACC Cardiovasc Interv 2023, 16, 247–257. [Google Scholar] [CrossRef]
- Joshi, A.; Wragg, A. Simulator Training in Interventional Cardiology. Interv Cardiol 2016, 11, 70–73. [Google Scholar] [CrossRef]
- Ledwoch, J.; Krollmann, C.; Staubach, S.; Hug, M.; Strohm, H.; Mudra, H. Learning Curve Assessment for Percutaneous Left Atrial Appendage Closure With the WATCHMAN Occluder. J Interv Cardiol 2016, 29, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.G.; Simard, T.; Killu, A.; Harris, A.A.; Hohmann, S.F.; Holmes, D.R.; Alkhouli, M. Learning Curve and Outcomes of Left Atrial Appendage Closure. JACC Cardiovasc Interv 2021, 14, 2750–2752. [Google Scholar] [CrossRef] [PubMed]
- Berti, S.; Pastormerlo, L.E.; Korsholm, K.; Saw, J.; Alkhouli, M.; Costa, M.P.; Odenstedt, J.; Packer, E.J.; Tondo, C.; Santoro, G.; et al. Intracardiac echocardiography for guidance of transcatheter left atrial appendage occlusion: An expert consensus document. Catheter Cardiovasc Interv 2021, 98, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Jungen, C.; Zeus, T.; Balzer, J.; Eickholt, C.; Petersen, M.; Kehmeier, E.; Veulemans, V.; Kelm, M.; Willems, S.; Meyer, C. Left Atrial Appendage Closure Guided by Integrated Echocardiography and Fluoroscopy Imaging Reduces Radiation Exposure. PLoS One 2015, 10, e0140386. [Google Scholar] [CrossRef]
- Balzer, J.; Zeus, T.; Hellhammer, K.; Veulemans, V.; Eschenhagen, S.; Kehmeier, E.; Meyer, C.; Rassaf, T.; Kelm, M. Initial clinical experience using the EchoNavigator(®)-system during structural heart disease interventions. World J Cardiol 2015, 7, 562–570. [Google Scholar] [CrossRef]
- Zorinas, A.; Zakarkaitė, D.; Janušauskas, V.; Austys, D.; Puodžiukaitė, L.; Zuozienė, G.; Samalavičius, R.S.; Jovaišienė, I.; Davidavičius, G.; Ručinskas, K.; et al. Technical Recommendations for Real-Time Echocardiography and Fluoroscopy Imaging Fusion in Catheter-Based Mitral Valve Paravalvular Leak and Other Procedures. J Clin Med 2022, 11. [Google Scholar] [CrossRef]
- Afzal, S.; Piayda, K.; Hellhammer, K.; Veulemans, V.; Wolff, G.; Heidari, H.; Stuwe, D.; Kanschik, D.; Polzin, A.; Kelm, M.; et al. Real-time echocardiography-fluoroscopy fusion imaging for left atrial appendage closure: prime time for fusion imaging? Acta Cardiol 2021, 76, 1004–1012. [Google Scholar] [CrossRef]
- Van Belle, E.; Teles, R.C.; Pyxaras, S.A.; Kalpak, O.; Johnson, T.W.; Barbash, I.M.; De Luca, G.; Kostov, J.; Parma, R.; Vincent, F.; et al. EAPCI Core Curriculum for Percutaneous Cardiovascular Interventions (2020): Committee for Education and Training European Association of Percutaneous Cardiovascular Interventions (EAPCI). A branch of the European Society of Cardiology. EuroIntervention 2021, 17, 23–31. [Google Scholar] [CrossRef]
- Glikson, M.; Wolff, R.; Hindricks, G.; Mandrola, J.; Camm, A.J.; Lip, G.Y.H.; Fauchier, L.; Betts, T.R.; Lewalter, T.; Saw, J.; et al. EHRA/EAPCI expert consensus statement on catheter-based left atrial appendage occlusion - an update. EuroIntervention 2020, 15, 1133–1180. [Google Scholar] [CrossRef]
- Jone, P.N.; Haak, A.; Petri, N.; Ross, M.; Morgan, G.; Wiktor, D.M.; Gill, E.; Quaife, R.A.; Messenger, J.C.; Salcedo, E.E.; et al. Echocardiography-Fluoroscopy Fusion Imaging for Guidance of Congenital and Structural Heart Disease Interventions. JACC Cardiovasc Imaging 2019, 12, 1279–1282. [Google Scholar] [CrossRef]
- Afzal, S.; Piayda, K.; Hellhammer, K.; Veulemans, V.; Wolff, G.; Heidari, H.; Stüwe, D.; Kanschik, D.; Polzin, A.; Kelm, M.; et al. Real-time echocardiography-fluoroscopy fusion imaging for left atrial appendage closure: prime time for fusion imaging? Acta Cardiol 2021, 76, 1004–1012. [Google Scholar] [CrossRef]
- Tzikas, A.; Holmes, D.R., Jr.; Gafoor, S.; Ruiz, C.E.; Blomstrom-Lundqvist, C.; Diener, H.C.; Cappato, R.; Kar, S.; Lee, R.J.; Byrne, R.A.; et al. Percutaneous left atrial appendage occlusion: the Munich consensus document on definitions, endpoints, and data collection requirements for clinical studies. Europace 2017, 19, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Rodeghiero, F.; Tosetto, A.; Abshire, T.; Arnold, D.M.; Coller, B.; James, P.; Neunert, C.; Lillicrap, D. ISTH/SSC bleeding assessment tool: a standardized questionnaire and a proposal for a new bleeding score for inherited bleeding disorders. J Thromb Haemost 2010, 8, 2063–2065. [Google Scholar] [CrossRef] [PubMed]
- Aeckersberg, G.; Gkremoutis, A.; Schmitz-Rixen, T.; Kaiser, E. The relevance of low-fidelity virtual reality simulators compared with other learning methods in basic endovascular skills training. J Vasc Surg 2019, 69, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Kalra, A.; Bhatt, D.L.; Kleiman, N.S. A 24-Month Interventional Cardiology Fellowship: Learning Motor Skills Through Blocked Repetition. JACC Cardiovasc Interv 2017, 10, 210–211. [Google Scholar] [CrossRef]
- Kleiman, N.S.; Welt, F.G.P.; Truesdell, A.G.; Sherwood, M.; Kadavath, S.; Shah, P.B.; Klein, L.W.; Hogan, S.; Kavinsky, C.; Rab, T. Should Interventional Cardiologists Super-Subspecialize?: Moving From Patient Selection to Operator Selection. JACC Cardiovasc Interv 2021, 14, 97–100. [Google Scholar] [CrossRef]
- Salemi, A.; Sedrakyan, A.; Mao, J.; Elmously, A.; Wijeysundera, H.; Tam, D.Y.; Di Franco, A.; Redwood, S.; Girardi, L.N.; Fremes, S.E.; et al. Individual Operator Experience and Outcomes in Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv 2019, 12, 90–97. [Google Scholar] [CrossRef]
- Chhatriwalla, A.K.; Vemulapalli, S.; Szerlip, M.; Kodali, S.; Hahn, R.T.; Saxon, J.T.; Mack, M.J.; Ailawadi, G.; Rymer, J.; Manandhar, P.; et al. Operator Experience and Outcomes of Transcatheter Mitral Valve Repair in the United States. J Am Coll Cardiol 2019, 74, 2955–2965. [Google Scholar] [CrossRef]
- Bertsche, D.; Pfisterer, M.; Dahme, T.; Schneider, L.M.; Metze, P.; Vernikouskaya, I.; Rasche, V. MRI-based training model for left atrial appendage closure. Int J Comput Assist Radiol Surg 2023. [Google Scholar] [CrossRef]
- Sawant, A.C.; Seibolt, L.; Sridhara, S.; Rodriguez, J.; Distler, E.; Murarka, S.; Lazkani, M.; Kumar, A.; Kanwar, N.; Prakash, M.P.H.; et al. Operator Experience and Outcomes after Transcatheter Left Atrial Appendage Occlusion with the Watchman Device. Cardiovasc Revasc Med 2020, 21, 467–472. [Google Scholar] [CrossRef]
- Wang, D.D.; Eng, M.; Kupsky, D.; Myers, E.; Forbes, M.; Rahman, M.; Zaidan, M.; Parikh, S.; Wyman, J.; Pantelic, M.; et al. Application of 3-Dimensional Computed Tomographic Image Guidance to WATCHMAN Implantation and Impact on Early Operator Learning Curve: Single-Center Experience. JACC Cardiovasc Interv 2016, 9, 2329–2340. [Google Scholar] [CrossRef] [PubMed]
- Afzal, S.; Veulemans, V.; Balzer, J.; Rassaf, T.; Hellhammer, K.; Polzin, A.; Kelm, M.; Zeus, T. Safety and efficacy of transseptal puncture guided by real-time fusion of echocardiography and fluoroscopy. Neth Heart J 2017, 25, 131–136. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Study flowchart. LAAC – Left atrial appendage closure; FI – Fusion imaging.
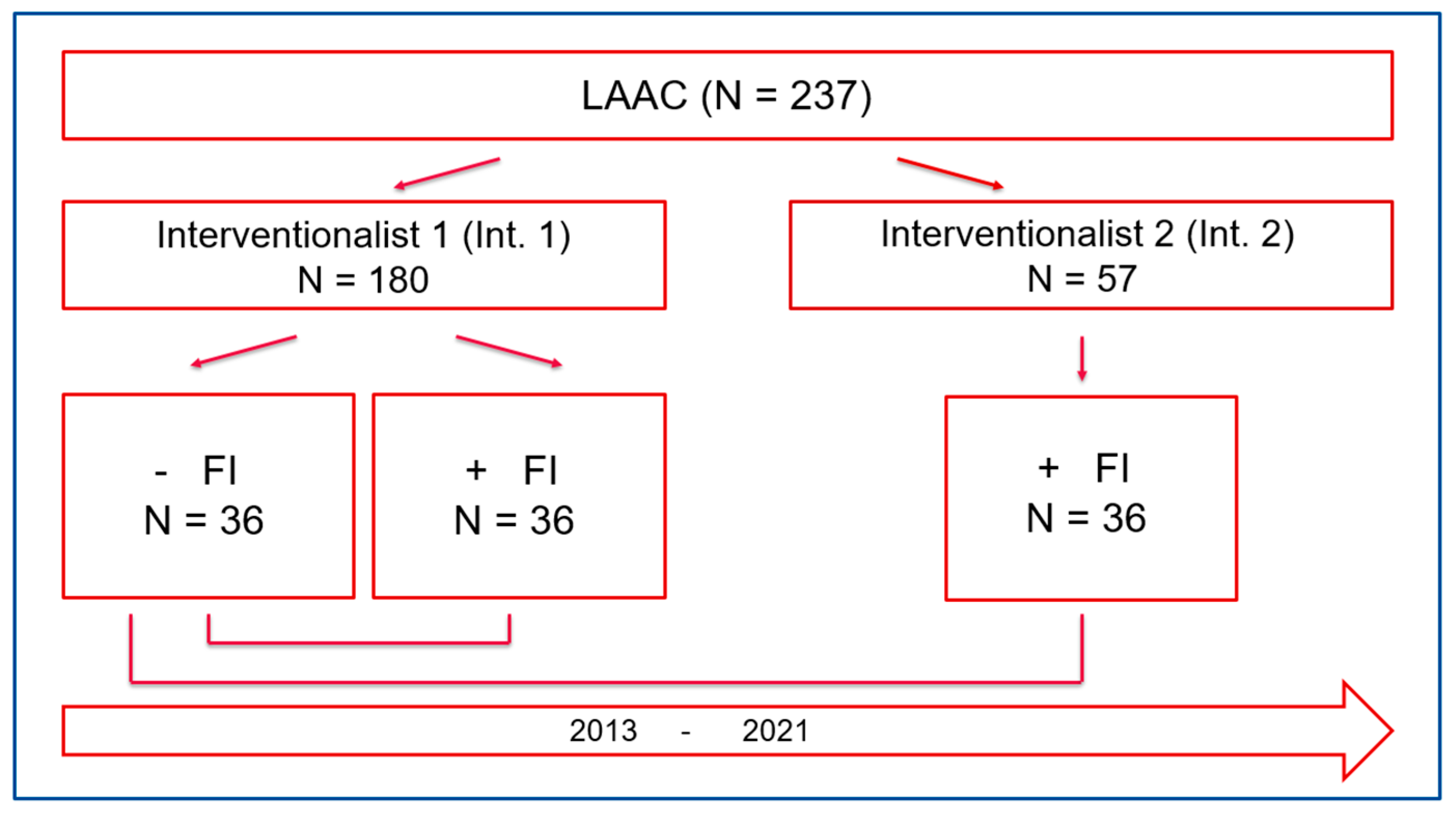
Figure 2.
The course of the learning curve over time. In group 1 (Interventionalist 1, -FI) the learning curve was flat, and the correlations were weak except for DAP. In groups 2 (Interventionalist 1, +FI) and 3 (Interventionalist 2, +FI) the course was steep with strong correlations for all parameters. FI – Fusion imaging.
Figure 2.
The course of the learning curve over time. In group 1 (Interventionalist 1, -FI) the learning curve was flat, and the correlations were weak except for DAP. In groups 2 (Interventionalist 1, +FI) and 3 (Interventionalist 2, +FI) the course was steep with strong correlations for all parameters. FI – Fusion imaging.
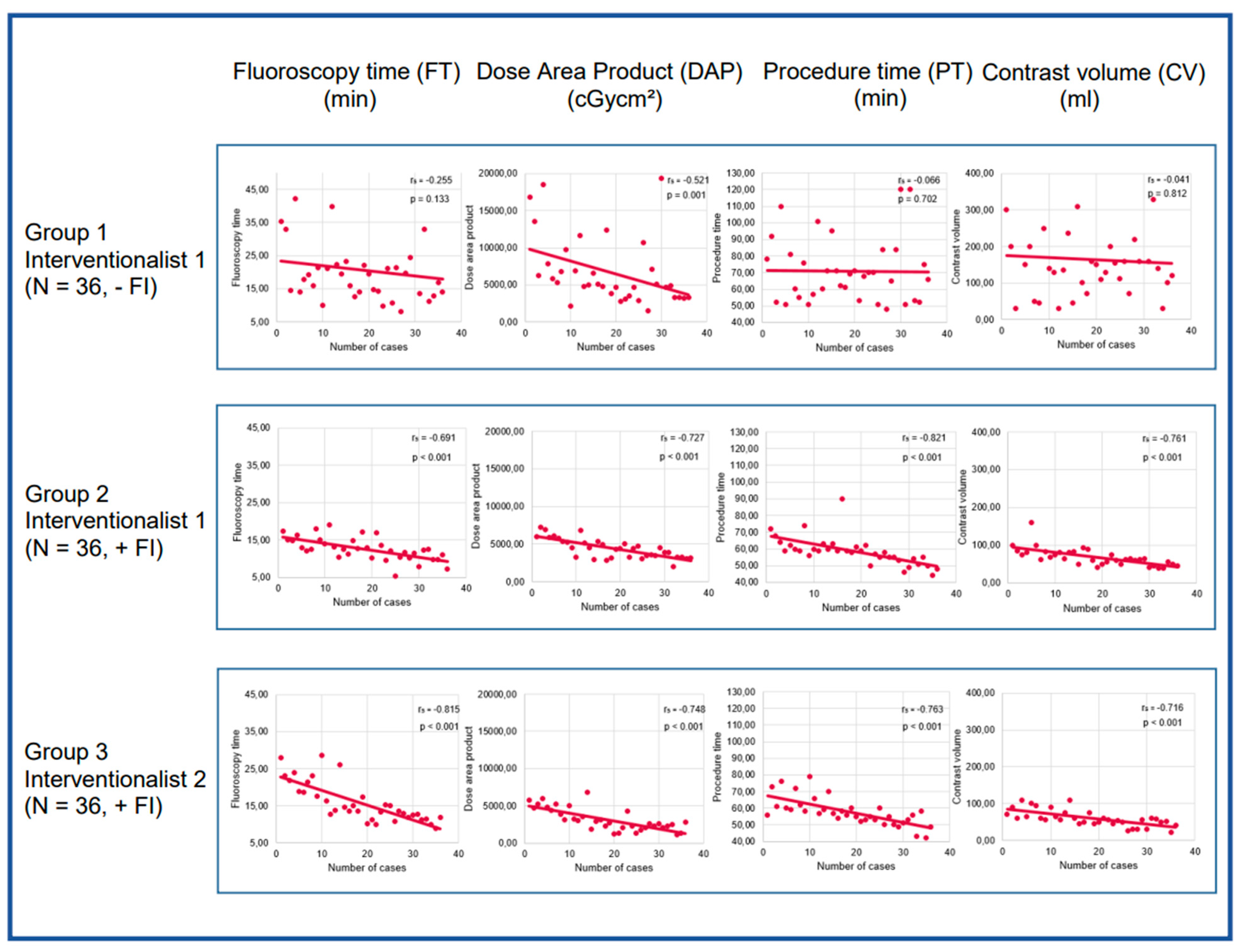

Table 1.
Patient characteristics.
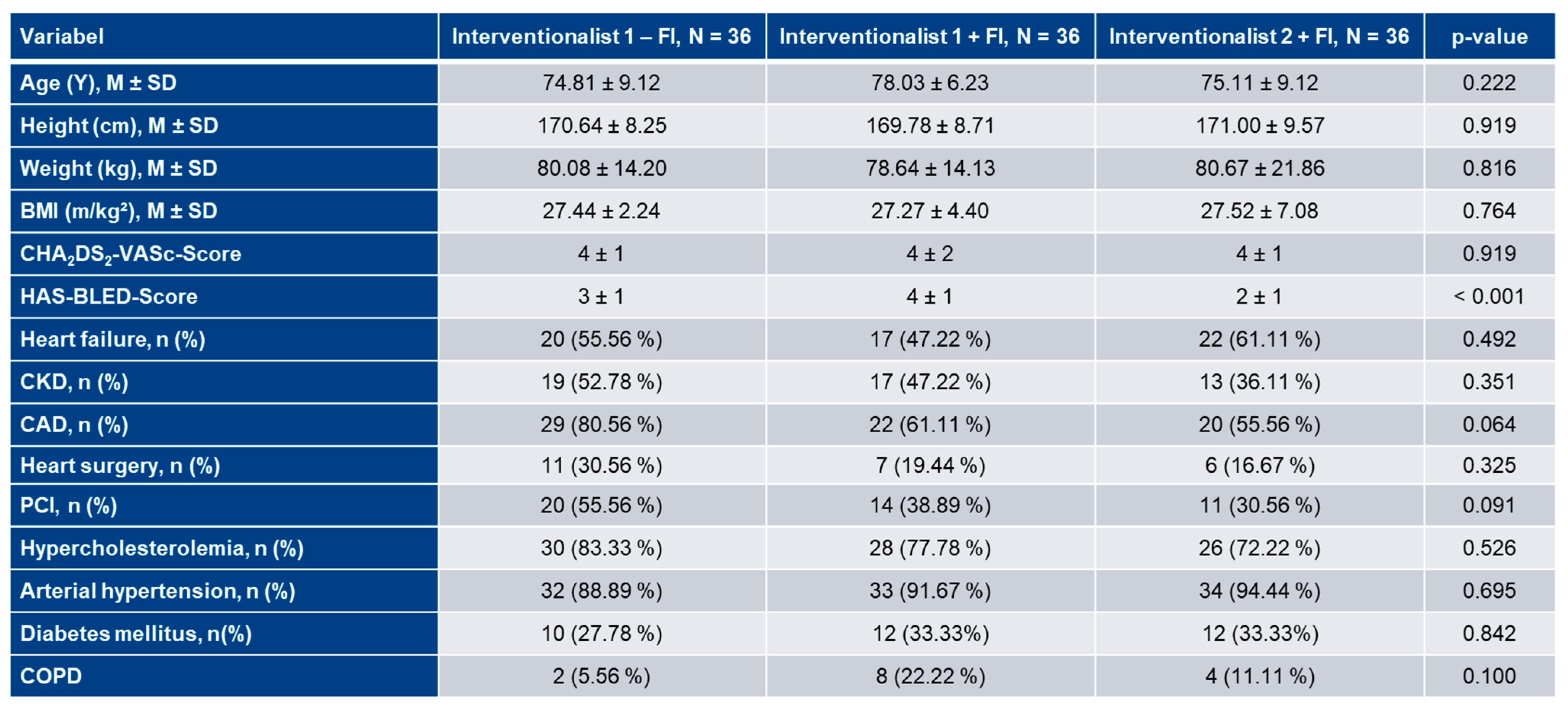 |
BMI – Body Mass Index; CKD – Chronic Kidney Disease; CAD – Coronary Artery Disease; PCI – Percutaneous Coronary Intervention; COPD - Chronic Obstructive Pulmonary Disease.
Table 2.
Comparison of measurements between group 1(Interventionalist 1, -FI) and 2 (Interventionalist 1, + FI). min – Minutes; ml – Milliliter; cGy – Zentigrey; cm – centimeter; FI – fusion imaging.
Table 2.
Comparison of measurements between group 1(Interventionalist 1, -FI) and 2 (Interventionalist 1, + FI). min – Minutes; ml – Milliliter; cGy – Zentigrey; cm – centimeter; FI – fusion imaging.
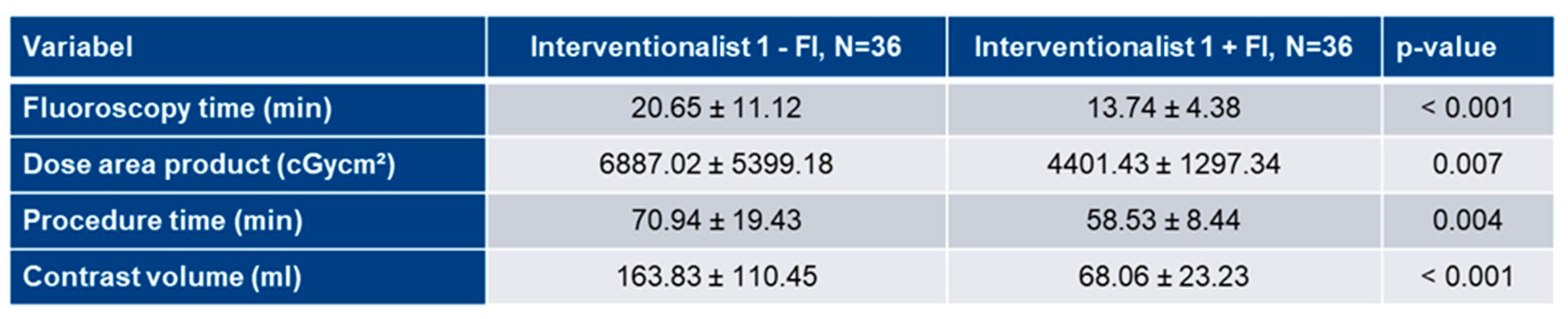 |
Table 3.
Comparison of measurements between group 1 (Interventionalist 1, -FI) and 3 (Interventionalist 2, +FI). min – Minutes; ml – Milliliter; cGy – Zentigrey; cm – centimeter; FI – fusion.
Table 3.
Comparison of measurements between group 1 (Interventionalist 1, -FI) and 3 (Interventionalist 2, +FI). min – Minutes; ml – Milliliter; cGy – Zentigrey; cm – centimeter; FI – fusion.
 |
Table 4.
Comparison of complications between group 1(Interventionalist 1, -FI) and 2 (Interventionalist 1, +FI). FI – fusion imaging.
Table 4.
Comparison of complications between group 1(Interventionalist 1, -FI) and 2 (Interventionalist 1, +FI). FI – fusion imaging.
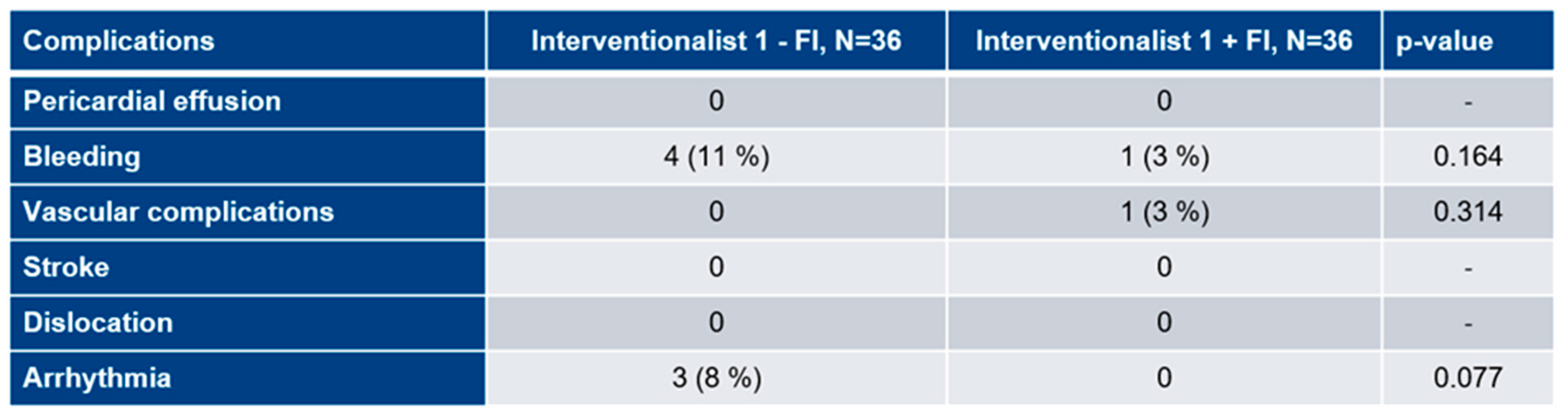 |
Table 5.
Comparison of complications between group 1(Interventionalist 1, -FI) and 3(Interventionalist 1, +FI). FI – fusion imaging.
Table 5.
Comparison of complications between group 1(Interventionalist 1, -FI) and 3(Interventionalist 1, +FI). FI – fusion imaging.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



