
Submitted:
18 August 2023
Posted:
31 August 2023
You are already at the latest version
Abstract
Background: Sepsis still represents a major public health issue worldwide, and immune system plays a main role during infections and therefore its activity is mandatory to resolve this clinical condition In this report we aimed to retrospectively verify in real life setting the possible usefulness of Pentameric IgM plus antibiotic in recovering patients with sepsis after major abdominal surgery Materials/methods: We reviewed, from January 2013 until December 2018, all adult patients admitted in ICU for Sepsis or Septic shock (2) after major abdominal surgery. Among these patients, were identified those that according to legal indication and licence in Italy, were treated with Pentameric IgM plus antibiotic (Group A) or with antibiotic alone (Group B). We analysed the following parameters were evaluated: Blood gas analysis, Lactate, CRP, Procalcitonin, Endotoxin activity, Liver and Renal Function, Coagulation, Blood Cell count at different time points (Every 48 hrs for at least 7 days. Differences between groups have been analysed by Fisher’s exact test or Chi square test for categorical variables. Mann–Whitney U test or Kruskal–Wallis test have instead been performed to compare continuous variables. Univariate and Multivariate analysis were also performed Results: Over a period of 30 months 24 patients were enrolled in Group A and 20 patients in Group B. In those subjects no statistical differences have been found in terms of bacterial or fungal infection isolates, when detected in a blood culture test, or in inflammatory index, SOFA score, lactate levels and mortality rate. A 48hrs response was statistically more frequent in Group B than in Group A, while no differences were found in the other clinical and laboratory evaluation. Conclusions: Based on our results, the use of pentameric IgM do not seem to give any clinical advantage in sepsis after to major abdominal surgery.
Keywords:
Pentaglobin
; Sepsis
; Infectionm Abdominal infection
1. Introduction
Sepsis still represents a major public health concern worldwide being characterized by organ dysfunction and related dysregulated host response (1-3). The current approach for sepsis includes the early eradication of septic foci, administration of anti-infective agents, and maintenance of hemodynamic stability through fluid administration and vasopressors (1,3,4). This treatment is the cornerstone for sepsis and, in particular, septic shock (4). Main difficulties to treat sepsis are related to its complexity that depends on the types of infectious microorganisms (such as bacteria, fungi), with related differences in terms of virulence and resistance to antibiotics. Further, the different infected body sites, especially in patients with several comorbidities may have a significant impact on the outcome (1). Coupled to these evidences we should also consider that these patients may vary in their ability to response to infection (due to hyper-inflammation, immune paralysis) and treatments increasing the complexity of the disease. Regarding the immune paralysis, sepsis has been defined as a life-threatening organ dysfunction caused by a dysregulated host response to infection (5). The host response is characterized by inflammatory storm and concurrent immunosuppression, which promote tissue damage, down-regulation of activating cell-surface molecules, T cell depletion and increased apoptosis of immune cells (6). This imbalance of immune system may determine a profound dysfunction of the innate and adaptive immunity (7) and play a role in patient outcomes, particularly in elderly and patients with pre-existing immune disorders. Since the use of only anti-inflammatory drugs failed in reducing mortality, the use of therapies designed to re-establish the immune system seems plausible. Several therapeutic options have been suggested to improve the outcome of sepsis and its clinical complications as septic shock and multiple organ dysfunction syndrome; more recently it has been proposed that improving opsonizing ability of immune system may reduce bacterial virulence. In this field, despite guidelines do not recommend the use of immunomodulatory treatment based on pentameric IgM (Pentaglobin, an immunoglobulin M-enriched immunoglobulin), this treatment schedule has been proposed in some scientific reports (2,8). Rationale on this kind of therapeutic approach is controversial because no clear consensus on its real benefits in clinical practice is provided. The advantage of this therapy relies on its pleiotropic effects on inflammation and immune system (9). Further, evidence from in vitro and in vivo studies and few clinical data have supported this use (8). Previous guidelines suggested against the use of polyclonal intravenous immunoglobulins in sepsis, but based on weak efficacy data (10). However, results from recent trials and systematic meta-analyses indicate that intravenous IgM-enriched immunoglobulins may be effective in sepsis (11-13). The aim of our retrospective observational study was to verify, in real life setting, if the pentameric IgM-enriched immunoglobulin may improve clinical outcome and survival when early associated to antibiotic treatment in patients with sepsis admitted in the Intensive Care Unit (ICU).
2. Methods
2.1. Study design
A retrospective medical records review was performed to include anonymized data on patients admitted for sepsis or septic shock after major abdominal surgery in the ICU of our hospital (AORN Ospedali dei Colli, Napoli, Italia and AORN A Cardarelli, Napoli, Italy) for the period from January 2013 to March 2019. Data were related to adult patients (≥ 18 years) diagnosed and treated for sepsis or septic shock, according to international guidelines and or National/Regional guidelines indication throughout the retrospective period of evaluation (2,13-15). Pentameric IgM when used were according to licence of use in Italy, (AIFA Italian Drug Regulatory Agency). Particularly collected data were divided in two groups Group A patients underwent pentameric plus antibiotics and patients selected from the same cohort of surgical procedures but treated with antibiotics alone (Group B) (Figure 1). Demographic data and relevant comorbidities were recorded for all patients as far as laboratory markers and clinical outcomes. According to clinical practice, the following parameters were evaluated every 48 hours: blood gas analysis, lactate, crp, procalcitonin, endotoxin activity, liver and renal function, coagulation, and blood cell count. Empirical antibiotic treatment was planned for all patients and was based on their legal indications and license of use in Europe and Italy as well as Regional and Hospital guidelines or after infectious disease consultant assessment. Mainly all empiric treatment in patients with abdominal infection were based on the following schedule: Tigecycline + Piperacilin-Tazobactam. This therapeutic schedule was modified according to scientific evidences from Infectious disease group in surgery of AORN A. Cardarelli (16) and national/regional guidelines as well as microbiological isolates when required. Antifungals were used when required according to previous score system (17).
2.2. Study endpoints
The primary endpoint was to evaluate the 48 hours response (reduction of Fever, inotrope drugs, CRP, Leukocyte and increase in Blood pressure). The secondary endpoint was mortality rate and sepsis resolution (withdrawn of inotropes drugs, absence of fever, reduction of inflammatory parameters, discharge in ward within 28th day).
2.3. Ethics approval
According to the local legislation, a retrospective study does not require ethical approval. For the use of retrospective data, this study was conducted in accordance with the Declaration of Helsinki 1975 and its later amendments. All patients’ data were fully anonymized and were analyzed retrospectively. For this type of study, formal consent was not required according to the current national established by the Italian Medicines Agency, and according to the Italian Data Protection Authority, neither ethical committee approval nor informed consent was required for anonymized data, as confirmed and approved by the Ethical Committee of “Aziende Ospedaliere di Rilievo Nazionale e di Alta Specializzazione—A.Cardarelli/Santobono—Pausilipon” as part of larger study (Protocol Number 00000926 of 11 January 2022).
2.4. Statistical analysis
Statistical analysis was performed looking for differences between groups by using the Fisher’s exact test or Chi square test for categorical variables. Mann–Whitney U test or Kruskal–Wallis test have instead been performed to compare continuous variables. Univariate and Multivariate analysis were also performed. P values below 0.05 were considered statistically significant. All analyses were performed with the SPSS software (IBM, Armonk, New York), version 24. Data are shown as either median and range, in the case of continuous variables or number and percentage, for categorical variables.
3. Results
Overall, data related to 44 patients (29 men and 15 women) were retrieved from medical records. Specifically, 24 patients (18 men and 6 women) were evaluated as eligible in Group A and 20 patients (11 men and 9 women) in Group B. Clinical data of all patients are summarized in Table 1. No difference was observed for demographic (age and sex) and clinical characteristics (BMI, smoke, potus, diabetes, and metabolic syndrome) at baseline between groups (Table 2). No statistical difference was found in terms of bacterial or fungal infections, when detected in a blood culture test, or in inflammatory index, SOFA score, lactate levels and mortality rate (Table 2). The primary endpoint showed that a 48 hours response was statistically more frequent in Group B than in Group A, while no difference was in the secondary endpoint. The only further statistically difference was in median ICU stay that resulted to be prolonged (over 14 days) in patients of Group A compared to those in Group B (Table 2).
Figure
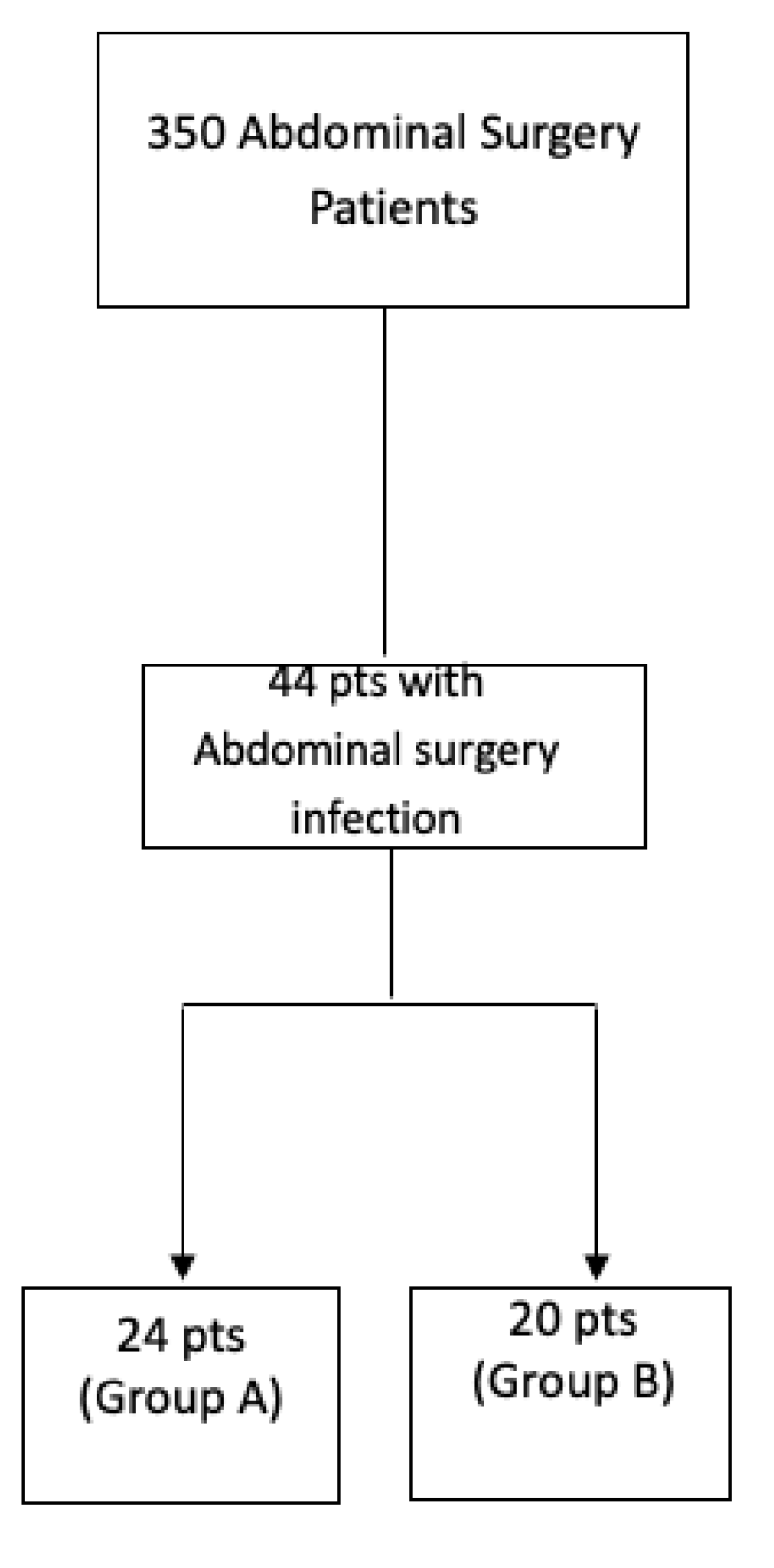
Figure shows the flowchart of evaluated patients in the retrospective analysis (January 2013- March 2019)
4. Discussion
Sepsis and its complications as septic shock remains a critical issue in healthcare because still associated to increased morbidity and mortality of affected inpatients in emergency departments and or in ICU. Nevertheless a multidisciplinary clinical approach and tailored treatment based on antibiotics, antifungals when necessary, fluids, steroids and vasopressors represents a gold standard that may improve clinical outcome and to reduce on mortality (2). The use of immunoglobulins to treat sepsis is mainly based on the rationale of modulating the inflammatory reaction and supporting the immune system in the fight against pathogens (17). Preclinical evidence showed that the infusion of IgM-enriched immunoglobulins can shift the inflammatory response towards an anti-inflammatory profile (17). IgM-enriched immunoglobulins can normalize capillary perfusion by reducing leukocyte adhesion in experimental models (18). Moreover, IgM-enriched immunoglobulins showed to enhance the anti-inflammatory response by increasing IL-10 levels and reducing TNF-alpha in bronchoalveolar lavage fluid of pneumonia models (19). In this clinical setting the use of intravenous human immunoglobulin (IVIG) to improve the sepsis outcome of patients underwent to abdominal surgery is still matter of discussion (20-22). In our study, according to other literature evidences too (12,17), we found that after major abdominal surgery, a therapeutic approach based on pentameric IgM plus antibiotic treatment did not seem to improve the natural history of sepsis, in terms of outcome and mortality compared to a therapy schedule based on the sole antibiotic. On the contrary, a meta-analysis, including 15 randomized clinical trials (712 patients) and four cohort studies (818 patients), found a reduction in mortality rates with IgM-enriched immunoglobulin for sepsis (Risk Ratio 0.60; 95%CI 0.52–0.69). Subgroup analyses also showed that these findings were consistent in reference to treatment duration, daily dose, total dose, variety of disease, severity scores, follow-up duration, study design, and year of publication (24). However, this meta-analysis mainly compared IgM-enriched immunoglobulin with placebo. Further we also did not find any differences in term of endotoxin activity assay between the two groups. Indeed endotoxin is expression of systemic inflammation due to abdominal infection sustained by gram negative bacteria (25). Despite the mechanisms related to the possible effects of pentameric IgM on different settings of patients is still not clear, our findings, even if based on a retrospective study, underline the importance to lead a better and more exhaustive evaluation of the use of Pentameric IgM instead of a too easy empiric use. Our study also carries some limitations. First, the small sample size may under-power the detection of differences in some parameters such as mortality or other major outcomes. Therefore, our results should be considered as exploratory and as the first step into a deeper knowledge on how and when to use pentameric immunoglobulin. However and in conclusion, based on our results, we can deduce that the use of pentameric IgM for sepsis after major abdominal surgery did not seem to give any clinical advantage at short term and at 28 days when death and duration of stay in ICU are considered as outcomes. Given the small sample size, these results must be seen as exploratory and need to be confirmed by other larger population based studies.
References
- Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801. [Google Scholar] [CrossRef]
- Rhodes A, Evans LE, Alhazzani W, Levy MM, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock:2016. Crit Care Med. 2017, 45, 486–552.
- Kyriazopoulou E, Leventogiannis K, Norrby-Teglund A, et al. Macrophage activation-like syndrome: an immunological entity associated with rapid progression to death in sepsis. BMC Med 2017, 15, 172. [Google Scholar]
- Artenstein AW, Higgins TL, Opal SM. Sepsis and scientific revolutions. Crit Care Med. 2013, 41, 2770–2772. [Google Scholar] [CrossRef] [PubMed]
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Tang BM, Huang SJ, McLean AS. Genome-wide transcription profiling of human sepsis: a systematic review. Crit Care. 2010, 14, R237. [Google Scholar] [CrossRef]
- Tamayo E, Fernandez A, Almansa R, Carrasco E, Heredia M, Lajo C, Goncalves L, Gomez-Herreras JI, de Lejarazu RO, Bermejo-Martin JF. Pro- and anti-inflammatory responses are regulated simultaneously from the first moments of septic shock. Eur Cytokine Netw. 2011, 22, 82–87. [Google Scholar] [CrossRef]
- Alejandria MM, Lansang MAD, Dans LF, Mantaring III JB. Intravenous immunoglobulin for treating sepsis, severe sepsis and septic shock. Cochrane Database of SystematicReviews 2013, Issue 9. Art. No.: CD001090.
- Werdan K, Pilz G, Bujdoso O, Fraunberger P, Neeser G, Schmieder RE, Viell B, Marget W, Seewald M, Walger P, et al. Score-based immunoglobulin G therapy of patients with sepsis: the SBITS study. Crit Care Med. 2007, 35, 2693–2701. [Google Scholar]
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally ME, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef]
- Cavazzuti I, Serafni G, Busani S, Rinaldi L, Biagioni E, Buoncristiano M, Girardis M. Early therapy with IgM-enriched polyclonal immunoglobulin in patients with septic shock. Intensive Care Med. 2014, 40, 1888–1896. [Google Scholar] [CrossRef]
- Giamarellos-Bourboulis EJ, Tziolos N, Routsi C, Katsenos C, Tsangaris I, Pneumatikos I, Vlachogiannis G, Theodorou V, Prekates A, Antypa E, et al. Improving outcomes of severe infections by multidrug-resistant pathogens with polyclonal IgM-enriched immunoglobulins. Clin Microbiol Infect. 2016, 22, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Dellinger RP, Levy MM, Rhodes A, et al; Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013, 41, 580–637. [Google Scholar] [CrossRef] [PubMed]
- Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- http://regione.campania.it/assets/documents/procedura-applicativa-delle-linee.pdf.
- Perrella A, Esposito C, Amato G, Perrella O, Migliaccio C, Pisaniello D, Calise F, Cuomo O, Santaniello W. Antifungal prophylaxis with liposomal amphotericin B and caspofungin in high-risk patients after liver transplantation: impact on fungal infections and immune system. Infect Dis (Lond). 2016, 48, 161–166. [Google Scholar] [CrossRef]
- Alejandria MM, Lansang MA, Dans LF, Mantaring JB III. Intravenous immunoglobulin for treating sepsis, severe sepsis and septic shock. Cochrane Database Syst Rev. 2013, 16, Cd001090. [Google Scholar]
- Prescott HC, Sussman JB, Wiersinga WJ. Postcritical illness vulnerability. Curr Opin Crit Care. 2020, 26, 500–507. [Google Scholar] [CrossRef]
- Kakoullis L, Pantzaris ND, Platanaki C, Lagadinou M, Papachristodoulou E, Velissaris D. The use of IgM-enriched immunoglobulin in adult patients with sepsis. J Crit Care. 2018, 47, 30–35. [Google Scholar] [CrossRef]
- Barratt-Due A, Sokolov A, Gustavsen A, Hellerud BC, Egge K, Pischke SE, et al. Polyvalent immunoglobulin signifcantly attenuated the formation of IL-1β in Escherichia coli-induced sepsis in pigs. Immunobiology. 2013, 218, 683–689. [Google Scholar] [CrossRef]
- Hofman JN, Fertmann JM, Vollmar B, Laschke MW, Jauch KW, Menger MD. Immunoglobulin M-enriched human intravenous immunoglobulins reduce leukocyte-endothelial cell interactions and attenuate microvascular perfusion failure in normotensive endotoxemia. Shock. 2008, 29, 133–139. [Google Scholar] [CrossRef]
- Vaschetto R, Clemente N, Pagni A, Esposito T, Longhini F, Mercalli F, et al. A double blind randomized experimental study on the use of IgM-enriched polyclonal immunoglobulins in an animal model of pneumonia developing shock. Immunobiology. 2017, 222, 1074–1080. [Google Scholar] [CrossRef]
- Rodríguez A, Rello J, Neira J, et al. Effects of high-dose of intravenous immunoglobulin and antibiotics on survival for severe sepsis undergoin surgery. Shock 2005, 23, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Cui J, Wei X, Lv H, Li Y, Li P, Chen Z, Liu G. The clinical efficacy of intravenous IgM-enriched immunoglobulin (pentaglobin) in sepsis or septic shock: a meta-analysis with trial sequential analysis. Ann Intensive Care. 2019, 9, 27. [Google Scholar] [CrossRef] [PubMed]
- Perrella, A. , Carannante, N., Capoluongo, N., Mascolo, A., Capuano, A. Endotoxin: Structure Source and Effects. Endotoxin Induced-Shock: a Multidisciplinary Approach in Critical Care, 2023, pp. 1–11.

Table 1.
Baseline characteristics of the entire cohort of study (n = 44).
| Parameter | |
|---|---|
| Age (yrs), median [IQR] | 53.5 [45.2 – 59.7] |
| Sex, n (%) Male Female |
29 (65.9) 15 (34.1) |
| BMI, median [IQR] | 23.5 [22 – 25] |
| Smoke, n (%) | 22 (50) |
| Potus, n (%) | 12 (27.3) |
| Diabetes, n (%) | 8 (18.2) |
| Metabolic syndrome, n (%) | 7 (15.9) |
| Lactates at EAB, median [IQR] | 2.15 [1.73 – 3] |
| SOFA Score, median [IQR] | 8 [7 – 8] |
| Leukocytosis, median [IQR] Baseline 72 h 96 h |
20.5 [18 – 22.3] 18 [16 – 20] 16 [13.2 – 18] |
| PCT, median ]IQR] Baseline 48 h |
4.5 [2 – 8] 5 [3 – 6] |
| EAA, median ]IQR] Baseline 72 h |
0.6 [0.5 – 0.7] 0.51 [0.5 – 0.6] |
| PCR, median ]IQR] Baseline 48 h |
183.5 [147 – 254] 124 [109 – 181] |
| Therapy, n (%) Pentaglobin + antibiotic Only antibiotic |
24 (54.5) 20 (45.5) |
| Major abdominal surgery, n (%) | 34 (77.3) |
| Inotrops, n (%) | 17 (38.6) |
| Inotrops drugs, n (%) | 21 (47.7) |
| Acidosis at EGA, n (%) | 23 (52.3) |
| ICU Stay over 15 days, n (%) | 21 (47.7) |
| Response at 48hrs, n (%) | 23 (52.3) |
| Exitus, n (%) | 11 (25) |
| Infected devices, n (%) | 15 (34.1) |
| Fungal infections, n (%) | 4 (9.1) |
| Bacteria, n (%) Gram-negative Gram positive |
35 (79.5) 9 (20.5) |
In table are reported all analyzed parameters during ICU stay. Data are expressed ad either number and percentage or median and interquartile range (IQR). EAA means endotoxin activity assay. Potus means alcool abuse.
Table 2.
Baseline Characteristics According to pentaglobin therapy: univariate and multivariate analysis (n = 44).
Table 2.
Baseline Characteristics According to pentaglobin therapy: univariate and multivariate analysis (n = 44).
| Univariate analysis | |||
|---|---|---|---|
| Parameter | Pentaglobin+Antibiotic (n=24) | Antibiotic (n=20) |
p |
| Age (yrs), median [IQR] | 48.5 [45.2 – 57] | 57.5 [47 – 61.7] | 0.125 |
| Sex, n (%) Male Female |
18 (75) 6 (25) |
11 (65) 9 (35) |
0.210 |
| BMI, median [IQR] | 23 [22 – 25] | 24 [23 – 26] | 0.204 |
| Smoke, n (%) | 14 (58.3) | 8 (40) | 0.364 |
| Potus, n (%) | 5 (20.8) | 7 (35) | 0.329 |
| Diabetes, n (%) | 3 (12.5) | 5 (25) | 0.436 |
| Metabolic syndrome, n (%) | 2 (8.3) | 5 (25) | 0.217 |
| SOFA Score, median [IQR] | 8 [7 – 9] | 8 [7 – 8] | 0.360 |
| Lactates at EAB, median [IQR] | 2.3 [1.85 – 3] | 2 [1.55 – 3.75] | 0.849 |
| Leukocytosis, median [IQR] Baseline 72 h 96 h |
19.5 [17.2 – 22.3] 18 [16 – 20.7] 15.3 [12.2 – 18] |
21 [19 – 22.8] 18 [16 – 20] 16 [15.2 – 18] |
0.293 0.785 0.414 |
| PCT, median ]IQR] Baseline 48 h |
3.5 [2 – 7.5] 5 [2 – 7] |
5 [3.13 – 8.75] 5 [4 – 6] |
0.129 0.403 |
| EAA, median ]IQR] Baseline 72 h |
0.6 [0.5 – 0.7] 0.56 [0.5 – 0.6] |
0.55 [0.4 – 0.7] 0.5 [0.5 – 0.67] |
0.457 0.772 |
| PCR, median ]IQR] Baseline 48 h |
202 [153 – 242.2] 123 [108.2 – 174.7] |
163.5 [135.2 – 258.2] 146 [110 – 191.2] |
0.548 0.333 |
| Major abdominal surgery, n (%) | 17 (70.8) | 17 (85) | 0.304 |
| Inotrop, n (%) | 11 (45.8) | 6 (30) | 0.359 |
| Inotrops drugs, n (%) | 14 (58.3) | 7 (35) | 0.143 |
| Acidosis at EGA, n (%) | 12 (50) | 11 (55) | 0.771 |
| ICU Stay over 14 days, n (%) | 17 (70.8) | 4 (20) | 0.001 |
| Response at 48hrs, n (%) | 6 (25) | 17 (85) | 0.000 |
| Exitus, n (%) | 6 (25) | 5 (25) | 1.000 |
| Infected devices, n (%) | 11 (45.8) | 4 (20) | 0.111 |
| Fungal infections, n (%) | 2 (8.3) | 2 (10) | 1.000 |
| Bacteria, n (%) Gram-negative MDR^ Gram positive |
20 (83.3) 4 (16.6) 4 (16.7) |
15 (75) 3(15)5 (25) |
0.710 n.s. 0.710 |
Table shows the results related to the analyzed variables in both groups. Statistically significant differences were found in ICU stay over 14 days and Response at 48hrs. No differences have been found in bacterial infections. ^ Gram negative MDR including Klebsiella KPC, in this case the following therapeutic schedule was used (Colimicine plus Tigecycline plus Meropenem. * Data are expressed ad either number and percentage or median and interquartile range (IQR). EAA means Endotoxin activity assay. Inotrops refers to the use of one dru, Inotrop drugs refers to the combiantion of vasocative drugs. Infected devices referes to central vein catheter. Potus means alcool abuse.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



