
Submitted:
30 August 2023
Posted:
01 September 2023
You are already at the latest version
Abstract
Arrhythmic sudden cardiac death (SCD) has an annual prevalence of 1 per 1000 while 75% of the victims suffer from ischemic and 10% from non-ischemic or hypertrophic cardiomyopathy. Altogether, these three entities account for more than 80% of the total SCD victims. Guidelines for implantable cardiac defibrillators are still dominated by LVEF<30% from the MADIT II study. In terms of arrhythmic risk stratification, the PRESERVE-EF study restored in clinical practice the two-step arrhythmic risk stratification approach based on Electrocardiographic non-invasive risk factors (NIRFs) guiding to electrophysiological study. In our times with the multiple cardiac imaging methods and artificial intelligence applications availability, this two-step approach based on integrated arrhythmia mechanisms detection, emerges as an efficient SCD risk stratification paradigm for these three entities but also for the patients with congenital heart disease.
Keywords:
arrhythmic sudden cardiac death
; risk stratification
; non-invasive risk factors
; NIRFs
; electrophysiology study
; two-step approach
; cardiomyopathy
1. Introduction
Sudden cardiac death (SCD) has an annual prevalence of 1 per 1000 [1], with the underlying pathology being Ischemic (ICM) in 75% and Non-Ischemic (NICM) or Hypertrophic Cardiomyopathy (HCM) in 10% of the victims [2,3]. Altogether, these three entities may account for more than 80% of the total SCD cases.
Figure 1.
Causes of SCD. Adapted from Wong, Heart Lunc Circ (2018) [3].
Figure 1.
Causes of SCD. Adapted from Wong, Heart Lunc Circ (2018) [3].
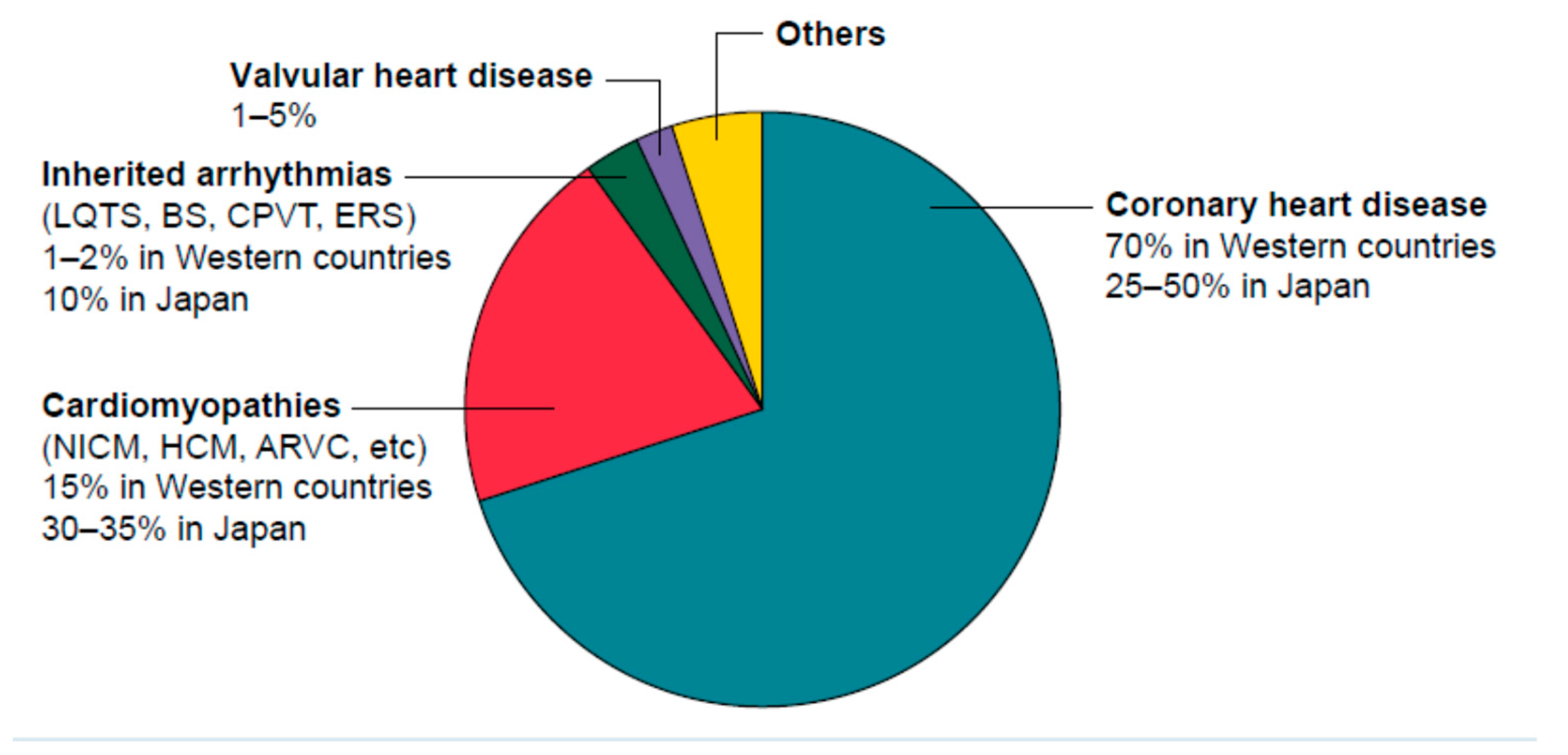
Annual SCD rate ranges from 0.6% to 3% in ICM [4,5], 1% in NICM [6], and 1% in HCM [7]. Primary prevention of SCD according current Guidelines is based on left ventricular ejection fraction (LVEF) for the ICM and NICM patients and is based on HCM SCD Risk-score for the HCM patients [8]. These approaches are not achieving sufficient sensitivity and specificity to identify patients at high SCD risk. By establishing an effective arrhythmic risk stratification (ARS) strategy for these three distinct entities, theoretically, 80% of the total future SCD victims seem possible to be protected with an ICD [9]. Recently published results from the PRESERVE EF study [10] restored the two-step ARS approach in clinical practice.
2. Myocardial fibrosis: the common arrhythmia initiation substrate in organic heart disease.
The common substrate for ventricular arrhythmia initiation and maintenance is myocardial fibrosis [11]. Arrhythmogenic fibrotic areas are present in the post-infarcted myocardial segments in ICM, in the left ventricular septum or left ventricular free wall in NICM, and interstitially in the left ventricular wall in HCM [12].
3. The two step approach: Non-invasive risk factors (NIRFs) guiding to programmed ventricular stimulation in electrophysiology study.
The presence of fibrosis may be detected directly by Non-Invasive Risk Factors (NIRFs), i.e. Late Gadolinium Enhancement in Cardiac MRI [13], or indirectly by Signal Averaged ECG Late Potentials [14,15]. The possible risk for arrhythmogenic burst of such fibrotic substrate may be assessed and classified as low, middle, and truly high with the stepwise use of NIRFs and Electrophysiology study (EPS) [16]. Such a two-step strategy was first proposed by Pedretti, R. et al. in 1993 when 303 acute myocardial infarction patients with an LVEF<40% were evaluated — a positive EPS was found to be the best predictor of arrhythmic events among patients preselected by NIRFs, demonstrating 81% sensitivity [17]. Several more studies with impaired LVEF patients and a similar two-step design announced sensitivity ranging between 33%-78% [18-20] (table 1). ARS based on this two-step approach was interrupted in 2002 after the results of the MADIT II study [5] were published; LVEF<30%, which was the study's enrollment criterion, started to dominate ICD implantation guideline recommendations [8] until today. The reason why LVEF, an anatomic-functional index per se, also predicts future arrhythmic events and its limitations has been explained in detail [9,16]. From an ARS point of view, the MADIT II study was not a typical risk stratification study; it did not seek to determine the individuals running the highest arrhythmic risk and discriminate them from those who were free of risk. One could say that it was rather aiming to clinically establish ICDs versus amiodarone in a broad post myocardial infarction patients sample preselected with a depressed LVEF<30%, i.e. a specific population for which a high annual SCD rate with frequent end-points was anticipated. Indeed, the main hypothesis was confirmed within only 20 months of follow-up [5].

Table 1.
Two-step design arrhythmic risk stratification for sudden cardiac death studies.
| Study | n | EF | Therapy | NIRFs | NIRFS+ | EPS(n) | EPS + | Follow up (m) |
End Points (n) |
Sens/Spec/PPV/NPV |
|---|---|---|---|---|---|---|---|---|---|---|
| Pedretti, [17], 1993 |
303 Post- AMI |
<40% | Thromb | EF<40% SAECG VPCs |
(≥2)* 67/303 |
47/67 | 20/47 | 17 | 19 | Sens = 81% Spec = 97% PPV = 65% NPV= 99% |
| Zoni Berisso [18], 1996 |
286 Post-AMI |
≤40% | Thromb (46%) | EF<40% SAECG VPCs NSVT |
(≥1) * | 103/286 | 16 /103 | 12 | 10 | Sens = 55% Spec = 99% PPV = 67% |
| Andersen [19], 1999 |
657 Post- AMI |
47% | Thromb | EF<40% VPCs NSVT | (≥1)* 304/657 | 146/304 | 22/146 | 37 | 24 | Sens = 44% Spec = 86% PPV = 18% NPV= 96% |
| Schmidt [20], 2001 |
1436 Post- AMI |
32% | ThrombAngiopl | EF SAECG VPCs HRV |
(≥3) * 248/1436 |
98/248 | 21/98 | 19 | 7/21 | Sens = 78% Spec = 84% PPV = 33% NPV= 97% |
| Gatzoulis PRESERVE-EF [10], 2019 |
575 Post- AMI |
≥40% | Angiopl CABG |
VPCs NSVT SAECG QTc TWA DC+HRT HRV |
(≥1) * 204/575 |
152/204 | 41/152 | 32 | 9 | Sens = 100% Spec = 93% PPV = 22% NPV= 100% |
AMI = acute myocardial infarction, Angiopl= angioplasty, CABG=coronary artery bypass grafting, DC= deceleration capacity of heart rate, EF=left ventricular ejection fraction, EPS= Electrophysiology study, HRT= heart rate turbulence, HRV= heart rate variability, NIRF= non-invasive risk factor, NPV= negative predictive value, NSVT= non-sustain ventricular tachycardia, n= number, post-MI= post myocardial infarction, PPV= positive predictive value, QTc= QT interval corrected for heart rate, SAECG= signal averaged ECG, sens= sensitivity, spec= specificity, Thromb= thrombolysis, TWA= T wave alternans, VPCs= ventricular premature complexes, * NIRFs cutoff point for PVS referral.
4. PRESERVE EF study, in 2019, restores the two-step arrhythmic risk stratification approach in clinical practice.
The abandoned two-step approach was recalled 17 years later, in 2019, by the PRESERVE-EF study [10]. Arrhythmic SCD victims among post-MI patients with a preserved left ventricular systolic function and LVEF>40% remained undetected by the guideline-proposed screening tool of LVEF<35%. These victims would suddenly die, with an estimated frequency of 0.6% per year [4], but would remain undetected. As a consequence, a different approach for an accurate detection of the truly high SCD-risk patients within this population was the sine qua non. The PRESERVE- EF study applied a stepwise algorithm (Figure 2).
In the first step, extended electrocardiographic NIRFs from ambulatory-ECG were used for the discrimination of low- and intermediate- arrhythmogenic risk patients. NIRFs may reflect both the presence and activity of different arrhythmogenic mechanisms that, irrespective of the left ventricular systolic function, may be present or absent, active or inactive [9,10,16] (Table 2).
Every intermediate arrhythmic-risk patient with at least one positive NIRF was further investigated with EPS. Patients with both positive NIRFs and EPS were considered as truly high arrhythmic-risk and were protected by an ICD. Patients without positive NIRFs are considered as low arrhythmic-risk, while patients with positive NIRFs, but negative EPS, are considered as intermediate arrhythmic-risk and receive follow-up. The prevalence of NIRFs in the PRESERVE EF study is presented in table 3. The total sample was 575 post-MI patients (age=57 years) with preserved left ventricular systolic function (LVEF=50.8%). Nine (n=9) Major Arrhythmic Events (MAEs) were observed during a 32-month follow-up. The MAE prevalence in the total sample of 575 patients was 1.5%. The implementation of the first step of the algorithm determined an intermediate arrhythmic-risk subpopulation of 204 patients out of 575 patients in total, with at least one NIRF present. In this subpopulation, the MAE prevalence increased from 1.5% to 4.4%. When this subpopulation underwent EPS as per the second step, 41 out of 152 patients developed arrhythmia (152 out of the 204 patients who gave their informed consent to participate in EPS). This third group of 41 EPS-positive patients represented the subpopulation at true high arrhythmic-risk, the MAE prevalence accounting for 22% (Figure 2).
Table 3.
Prevalence of non-invasive risk factors in the PRESERVE-EF study.
| NIRF | Prevalence in the total Preserve-EF (n=577) | Prevalence in the High arrhythmic risk group (n=41) | Prevalence in 9 MAE/SCD patients |
|---|---|---|---|
| LPs (%) | 13.8 | 51.2 | 78 (7/9) |
| NSVT (%) | 8.6 | 46.3 | 66 (6/9) |
| QTc (%) | 13.6 | 36.6 | 55 (5/9 |
| VPBs (%) | 10.8 | 39 | 33 (3/9) |
| TWA (%) | 6.8 | 24.4 | 11 (1/9) |
| SDNN (%) | 2.8 | 9.8 | 0 (0/9) |
| HRT&DC (%) | 2.8 | 9.8 | 0 (0/9) |
Prevalence of non-invasive risk factors in the total sample, in the truly high-risk group, detected after the two-step, electrophysiology inclusive approach, and in patients with major arrhythmic events during a 32-months follow-up, as investigated in the PRESERVE-EF study. DC: Deceleration capacity from heart rate dynamics; HRT: Heart rate turbulence from heart rate dynamics; LPs: Late potentials from signal-averaged electrocardiogram; MAE: Major arrhythmic event; NIRF: Non-invasive risk factor; NSVT: Non-sustained ventricular tachycardia; QTc: Corrected according to Fridericia formula QT interval; SDNN: Standard deviation of normal to normal beats from heart rate variability analysis; TWA: T wave alternans; VPBs: Ventricular premature beats. Modified after permission from reference [9].
5. Two-step approach, stratifies the SCD risk, in heart failure with mid range ejection fraction, in non-ischemic and in hypertrophic cardiomyopathy patients.
Current ARS in NICM and HCM is based on LVEF and SCD-HCM Risk score, respectively [8]. Both approaches are imperfect [28,29]. The emerging use of Cardiac MRI is promising [12] but, considering that fibrosis may be present in 34% of NICM [30] and 41% of HCM patients [31] as well as that the SCD annual rate for these entities is only 1% [6,7], it is not evident whether all such patients would be considered good candidates for ICDs . Prospective clinical trials with Cardiac MRI-guided ICD implantation design are required to establish the number needed to treat [32]. Cardiac MRI seems to be an ideal NIRF that can assess the presence of arrhythmogenic substrate. It is unknown whether MRI is also sufficient to answer the question of the potential arrhythmogenic triggering of this substrate. According to the two-step approach, this question is answered through the second step by EPS [10,33]. Focusing on SCD prediction it is important that, apart from ICM, published results supporting the usage of a two-step risk stratification approach for HFmrEF [33], NICM [ 34] and HCM [35] are also available (Table 4).
An extended two-step algorithm for clinical use that individualize and stratifies the arrhythmic SCD risk in all these three distinct cardiomyopathy entities, targeting more than 80 % of SCD victims was already proposed in 2017 [36] (Figure 3). The ongoing RECONSIDER study risk stratifies NICM patients with depressed but also with preserved left ventricular systolic function, applying this two-step algorithm [37].
6. Current status.
While ARS, based on a sole NIRF prediction model or on multiple NIRFs prediction models, without being followed by a second EPS step, seems insufficient to support a decision for ICD implantation [38-41], the application of a combined two-step strategy improves ARS [10,17-20,33]. Similarly, a simple EPS, which ignores the NIRFs first-step, may expose all patients to EPS. The optimal ARS, according to the PRESERVE-EF study, should incorporate both steps. The first one involves searching for NIRFs, investigating each patient for potential detection of the existence of arrhythmogenic substrate and the activation of arrhythmia mechanisms, classifying each distinct patient as low or intermediate risk, according to their arrhythmic status as it is reflected by NIRFs. The second step, involving inducibility in the EPS, detects the truly high arrhythmic risk subgroup. This sequential approach represents a personalized ARS strategy. In the PRESERVE-EF study, all patients (n=575) were initially investigated by NIRFs, but only 35.5% were found eligible for further risk stratification in the second step through an EPS. After the procedure, 41 out of 152 patients were inducible, and finally, 37 out of 41 consented and received an ICD. Nine appropriate ICD activations occurred during the 32 months of follow-up. This ARS strategy achieved a Number-Needed-to-Treat (NNT) of 4.5 (9/41). In fact, this low NNT originated from a pyramid of 575 included patients. The application of such a sequential two-step ARS approach for the remaining patients, i.e., those who did not have an ICD implanted, was also proven safe, as no SCDs occurred in the intermediate and low arrhythmic-risk subgroups during follow-up. To address the question of how NIRFs evolve over time, a sub-analysis of the PRESERVE-EF study was conducted using NIRFs extracted from two distinct time periods: baseline and 1 year later. Regarding the prevalence of NIRFs, it was found to be consistent on a population basis but were few patients without NIRFs at baseline who developed NIRFs at the 1-year mark and vice versa. This finding highlighted the need for NIRFs reassessment during long-term follow-up with a referral for EPS as the arrhythmogenic substrate evolves [42]. Examining the interrelations between NIRFs and left ventricular systolic function, another sub-analysis concluded that SAECG LPs and NSVT were independently associated with reduced LVEF and served as predictors of mildly reduced LVEF as opposed to preserved LVEF [43]. Regarding these two NIRFs, SAECG LPs and NSVT, it's important to emphasize that their prevalence within the high arrhythmic risk group (n=41) in the PRESERVE-EF study was 51% and 46% respectively. Additionally, among the 9 patients with an implanted ICD who experienced major arrhythmic event end-points, 7 out of 9 (78%) had LPs and 6 out of 9 (66%) had NSVT (Table 3) [9,10] The importance of SAECG LPs and NSVT as the dominant NIRFs, was also underlined by another two-step ARS study involving heart failure patients with mid-range ejection fraction [33]. For this combination of NIRFs, it can be inferred that the arrhythmogenic substrate may be detected by SAECG LPs while the arrhythmogenic potential and triggering predisposition of this substrate could be identified through NSVT. In cases where both NIRFs are present, the possibility of fatal arrhythmias occurring increases. There is accumulated recent evidence that some NIRFs may be extracted from short resting Holter (SRH) ECG recordings of 30-45min duration also, thus facilitating the clinical cardiologist’ office workup [44-47]. Furthermore the ability of which NIRFs are able to predict EPS results among the post-myocardial infarction patients with LVEF>40% was the subject of another sub study of PRESERVE-EF. Indeed this sub study revealed NSVT ≥1episode/24 h and SAECG-LPs ≥2/3 cutoff points, in conjunction with a LVEF < 50%, to be significant predictors of inducibility [48]. An Artificial Intelligence (AI) analysis of NIRFs using the Nearest Neighbour (NN) algorithm to predict a positive EPS achieved an accuracy of 72.2% with N set to 7 [49]. Nevertheless, it is concluded from these studies that the ultimate decision regarding ICD implantation should be founded upon a positive EPS, which remains irreplaceable in risk stratification [48,49]. In congenital heart disease, SCD is a leading cause of death The combination of surgical incisions, myocardial scar and residual or new anatomical abnormalities form the substrate for ventricular arrhythmias Although these patients represent a heterogeneous population, a two-step ARS strategy may be applied also[50,51].
Author Contributions
Conceptualization, P.A.; investigation, P.A., A.K., I.D., A.L.; resources, P.A., A.X., N.M.; writing—original draft preparation, P.A.; writing—review and editing, P.A., C.K.A., P.D., D.T.; supervision, K.A.G., K.To., S.S., K.Ts.; All authors have read and agreed to the published version of the manuscript.” .
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Straus, S.M.; Bleumink, G.S.; Dieleman, J.P.; van der Lei, J.; Stricker, B.H.; Sturkenboom, M.C. The incidence of sudden cardiac death in the general population. J Clin Epidemiol. 2004, 57, 98–102. [Google Scholar] [CrossRef]
- Chugh, S.S.; Reinier, K.; Teodorescu, C.; Evanado, A.; Kehr, E.; Al Samara, M.; Mariani, R.; Gunson, K.; Jui, J. Epidemiology of sudden cardiac death: clinical and research implications. Prog Cardiovasc Dis. 2008, 51, 213–228. [Google Scholar] [CrossRef]
- Wong, C.X.; Brown, A.; Lau, D.H.; Chugh, S.S.; Albert, C.M.; Kalman, J.M.; Sanders, P. Epidemiology of Sudden Cardiac Death: Global and Regional Perspectives. Heart Lung Circ. 2019, 28, 6–14. [Google Scholar] [CrossRef]
- Ikeda, T.; Yoshino, H.; Sugi, K.; Tanno, K.; Shimizu, H.; Watanabe, J.; Kasamaki, Y.; Yoshida, A.; Kato, T. Predictive value of microvolt T-wave alternans for sudden cardiac death in patients with preserved cardiac function after acute myocardial infarction: results of a collaborative cohort study. J Am Coll Cardiol. 2006, 48, 2268–2274. [Google Scholar] [CrossRef]
- Moss, A.J.; Zareba, W.; Hall, W.J.; Klein, H.; Wilber, D.; J. ; Cannom, D.S.; Daubert, J.P.; Higgins, S.L.; Brown, M.W.; Andrews, M.L. Multicenter Automatic Defibrillator Implantation Trial II Investigators. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002, 346, 877–883. [Google Scholar] [CrossRef]
- Kadish, A.; Dyer, A.; Daubert, J.P.; Quigg, R.; Estes, N.A.; Anderson, K.P.; Calkins, H.; Hoch, D.; Goldberger, J.; Shalaby, A.; Sanders, W.E.; Schaechter, A.; Levine, J.H. Defibrillators in Non-Ischemic Cardiomyopathy Treatment Evaluation (DEFINITE) Investigators. Prophylactic defibrillator implantation in patients with nonischemic dilated cardiomyopathy. N Engl J Med 2004, 350, 2151–2158. [Google Scholar] [CrossRef]
- Elliott, P.M.; Gimeno, J.R.; Thaman, R.; Shah, J.; Ward, D.; Dickie, S.; Tome Esteban, M.T.; McKenna, W.J. Historical trends in reported survival rates in patients with hypertrophic cardiomyopathy. Heart 2006, 92, 785–791. [Google Scholar] [CrossRef]
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; Winkel, B.G.; Behr, E.R.; Blom, N.A.; Charron, P.; Corrado, D.; Dagres, N.; de Chillou, C.; Eckardt, L.; Friede, T.; Haugaa, K.H.; Hocini, M.; Lambiase, P.D.; Marijon, E.; Merino, J.L.; Peichl, P.; Priori, S.G.; Reichlin, T.; Schulz-Menger, J.; Sticherling, C.; Tzeis, S.; Verstrael, A.; Volterrani, M. ESC Scientific Document Group. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart, J. 2022, ahead of print. [CrossRef]
- Arsenos, P.; Gatzoulis, K.A.; Tsiachris, D.; Dilaveris, P.; Sideris, S.; Sotiropoulos, I.; Archontakis, S.; Antoniou, C.K.; Kordalis, A.; Skiadas, I.; Toutouzas, K.; Vlachopoulos, C.; Tousoulis, D.; Tsioufis, K. Arrhythmic risk stratification in ischemic, non-ischemic and hypertrophic cardiomyopathy: A two-step multifactorial, electrophysiology study inclusive approach. World J Cardiol. 2022, 14, 139–151. [Google Scholar] [CrossRef] [PubMed]
- Gatzoulis, K.A.; Tsiachris, D.; Arsenos, P.; Antoniou, C.K.; Dilaveris, P.; Sideris, S.; Kanoupakis, E.; Simantirakis, E.; Korantzopoulos, P.; Goudevenos, I.; Flevari, P.; Iliodromitis, E.; Sideris, A.; Vassilikos, V.; Fragakis, N.; Trachanas, K.; Vernardos, M.; Konstantinou, I.; Tsimos, K.; Xenogiannis, I.; Vlachos, K.; Saplaouras, A.; Triantafyllou, K.; Kallikazaros, I.; Tousoulis, D. Arrhythmic risk stratification in post-myocardial infarction patients with preserved ejection fraction: the PRESERVE EF study. Eur Heart, J. 2019, 40, 2940–2949. [Google Scholar] [CrossRef] [PubMed]
- Disertori, M.; Masè, M.; Ravelli, F. Myocardial fibrosis predicts ventricular tachyarrhythmias. Trends Cardiovasc Med. 2017, 27, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Kariki, O.; Antoniou, C.K.; Mavrogeni, S.; Gatzoulis, K.A. Updating the Risk Stratification for Sudden Cardiac Death in Cardiomyopathies: The Evolving Role of Cardiac Magnetic Resonance Imaging. An Approach for the Electrophysiologist. Diagnostics (Basel). 2020, 10, 541. [Google Scholar] [CrossRef] [PubMed]
- Disertori, M.; Rigoni, M.; Pace, N.; Casolo, G.; Masè, M.; Gonzini, L.; Lucci, D.; Nollo, G.; Ravelli, F. Myocardial fibrosis assessment by LGE is a powerful predictor of ventricular tachyarrhythmias in ischemic and nonischemic LV dysfunction. A meta-analysis. J Am Coll Cardiol Img. 2016, 9, 1046–1055. [Google Scholar] [CrossRef] [PubMed]
- Gatzoulis, K.A.; Carlson, M.D.; Biblo, L.A.; Rizos, I.; Gialafos, J.; Toutouzas, P.; Waldo, A.L. ; Time domain analysis of the signal averaged electrocardiogram in patients with a conduction defect or a bundle branch block. Eur Heart, J. 1995, 16, 1912–1919. [Google Scholar] [CrossRef] [PubMed]
- Gatzoulis, K.A.; Arsenos, P.; Trachanas, K.; Dilaveris, P.; Antoniou, C.; Tsiachris, D.; Sideris, S.; Kolettis, T.M.; Tousoulis, D. Signal-averaged electrocardiography: Past, present, and future. J Arrhythm. 2018, 34, 222–229. [Google Scholar] [CrossRef]
- Arsenos, P.; Gatzoulis, K.; Dilaveris, P.; Manis, G.; Tsiachris, D.; Archontakis, S.; Vouliotis, AI.; Sideris, S.; Stefanadis, C. Arrhythmic sudden cardiac death: substrate, mechanisms and current risk stratification strategies for the post-myocardial infarction patient. Hellenic J Cardiol. 2015, 54, 301–315. [Google Scholar]
- Pedretti, R.; Etro, M.D.; Laporta, A.; Sarzi Braga, S.; Carù, B. Prediction of late arrhythmic events after acute myocardial infarction from combined use of noninvasive prognostic variables and inducibility of sustained monomorphic ventricular tachycardia. Am J Cardiol. 1993, 71, 1131–1141. [Google Scholar] [CrossRef]
- Zoni-Berisso, M.; Molini, D.; Mela, G.S.; Vecchio, C. Value of programmed ventricular stimulation in predicting sudden death and sustained ventricular tachycardia in survivors of acute myocardial infarction. Am J Cardiol. 1996, 77, 673–680. [Google Scholar] [CrossRef]
- Andresen, D.; Steinbeck, G.; Brüggemann, T.; Müller, D.; Haberl, R.; Behrens, S.; Hoffmann, E.; Wegscheider, K.; Dissmann, R.; Ehlers, H.C. Risk stratification following myocardial infarction in the thrombolytic era: a two-step strategy using noninvasive and invasive methods. J Am Coll Cardiol. 1999, 33, 131–138. [Google Scholar] [CrossRef]
- Schmitt, C.; Barthel, P.; Ndrepepa, G.; Schreieck, J.; Plewan, A.; Schömig, A.; Schmidt, G. Value of programmed ventricular stimulation for prophylactic internal cardioverter-defibrillator implantation in postinfarction patients preselected by noninvasive risk stratifiers. J Am Coll Cardiol. 2001, 37, 1901–1907. [Google Scholar] [CrossRef]
- Arsenos, P.; Gatzoulis, K.A.; Dilaveris, P.; Gialernios, T.; Sideris, S.; Lazaros, G.; Archontakis, S.; Tsiachris, D.; Kartsagoulis, E.; Stefanadis, C. The rate-corrected QT interval calculated from 24-hour Holter recordings may serve as a significant arrhythmia risk stratifier in heart failure patients. Int J Cardiol. 2011, 147, 321–323. [Google Scholar] [CrossRef]
- Verrier, R.L.; Nearing, B.D.; La Rovere, M.T.; Pinna, G.D.; Mittleman, M.A.; Bigger, J.T. Jr; Schwartz, P.J. ATRAMI Investigators. Ambulatory electrocardiogram-based tracking of T wave alternans in post myocardial infarction patients to assess risk of cardiac arrest or arrhythmic death. J Cardiovasc Electrophysiol. 2003, 14, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Maggioni, A.P.; Zuanetti, G.; Franzosi, M.G.; Rovelli, F.; Santoro, E.; Staszewsky, L.; Tavazzi, L.; Tognoni, G. Prevalence and prognostic significance of ventricular arrhythmias after acute myocardial infarction in the fibrinolytic era. GISSI-2 results. Circulation. 1993, 87, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, T.; Hashimoto, K.; Yoshioka, K.; Miwa, Y.; Yodogawa, K.; Watanabe, E.; Nakamura, K.; Nakagawa, M.; Nakamura, K.; Watanabe, T.; Yusu, S.; Tachibana, M.; Nakahara, S.; Mizumaki, K.; Ikeda, T. Risk stratification for cardiac mortality using electrocardiographic markers based on 24-hour Holter recordings: the JANIES-SHD study. J Cardiol. 2020, 75, 155–163. [Google Scholar] [CrossRef] [PubMed]
- La Rovere, M.T.; Bigger, J. T.Jr; Marcus, F.I.; Mortara, A.; Schwartz, P.J. Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI (Autonomic Tone and Reflexes After Myocardial Infarction) Investigators. Lancet. 1998, 351, 478–484. [Google Scholar] [CrossRef]
- Bauer, A.; Kantelhardt, J.W.; Barthel, P.; Schneider, R.; Mäkikallio, T.; Ulm, K.; Hnatkova, K.; Schömig, A.; Huikuri, H.; Bunde, A.; Malik, M.; Schmidt, G. Deceleration capacity of heart rate as a predictor of mortality after myocardial infarction: cohort study. Lancet. 2006, 367, 1674–1681. [Google Scholar] [CrossRef]
- Bauer, A.; Barthel, P.; Schneider, R.; Ulm, K.; Müller, A.; Joeinig, A.; Stich, R.; Kiviniemi, A.; Hnatkova, K.; Huikuri, H.; Schömig, A.; Malik, M.; Schmidt, G. Improved Stratification of Autonomic Regulation for risk prediction in post-infarction patients with preserved left ventricular function (ISAR-Risk). Eur Heart, J. 2009, 30, 576–583. [Google Scholar] [CrossRef]
- Køber, L.; Thune, J.J.; Nielsen, J.C.; Haarbo, J.; Videbæk, L.; Korup, E.; Jensen, G.; Hildebrandt, P.; Steffensen, F.H.; Bruun, N.E.; Eiskjær, H.; Brandes, A.; Thøgersen, A.M.; Gustafsson, F.; Egstrup, K.; Videbæk, R.; Hassager, C.; Svendsen, J.H.; Høfsten, D.E.; Torp-Pedersen, C.; Pehrson, S. DANISH Investigators. Defibrillator Implantation in Patients with Nonischemic Systolic Heart Failure. N Engl J Med. 2016, 375, 1221–1230. [Google Scholar] [CrossRef]
- Maron, B.J.; Casey, S.A.; Chan, R.H.; Garberich, R.F.; Rowin, E.J.; Maron, M.S. Independent Assessment of the European Society of Cardiology Sudden Death Risk Model for Hypertrophic Cardiomyopathy. Am J Cardiol. 2015, 116, 757–764. [Google Scholar] [CrossRef]
- Halliday, B.P.; Baksi, A.J.; Gulati, A.; Ali, A.; Newsome, S.; Izgi, C.; Arzanauskaite, M.; Lota, A.; Tayal, U.; Vassiliou, V.S.; Gregson, J.; Alpendurada, F.; Frenneaux, M.P.; Cook, S.A.; Cleland, J.G.F.; Pennell, D.J.; Prasad, S.K. Outcome in Dilated Cardiomyopathy Related to the Extent, Location, and Pattern of Late Gadolinium Enhancement. JACC Cardiovasc Imaging. 2019, 12 Pt 2, 1645–1655. [Google Scholar] [CrossRef]
- Adabag, A.S.; Maron, B.J.; Appelbaum, E.; Harrigan, C.J.; Buros, J.L.; Gibson, C.M.; Lesser, J.R.; Hanna, C.A.; Udelson, J.E.; Manning, W.J.; Maron, M.S. Occurrence and frequency of arrhythmias in hypertrophic cardiomyopathy in relation to delayed enhancement on cardiovascular magnetic resonance. J Am Coll Cardiol. 2008, 51, 1369–1374. [Google Scholar] [CrossRef]
- Selvanayagam, J.B.; Hartshorne, T.; Billot, L.; Grover, S.; Hillis, G.S.; Jung, W.; Krum, H.; Prasad, S.; McGavigan, A.D. Cardiovascular magnetic resonance-GUIDEd management of mild to moderate left ventricular systolic dysfunction (CMR GUIDE): Study protocol for a randomized controlled trial. Ann Noninvasive Electrocardiol. 2017, 22, e12420. [Google Scholar] [CrossRef] [PubMed]
- Arsenos, P.; Gatzoulis, K.A.; Doundoulakis, I.; Dilaveris, P.; Antoniou, C.K.; Soulaidopoulos, S.; Sideris, S.; Sotiropoulos, I.; Tousoulis, D. Arrhythmic risk stratification in heart failure mid-range ejection fraction patients with a non-invasive guiding to programmed ventricular stimulation two-step approach. J Arrhythm. 2020, 36, 890–898. [Google Scholar] [CrossRef] [PubMed]
- Gatzoulis, K.A.; Vouliotis, A.I.; Tsiachris, D.; Salourou, M.; Archontakis, S.; Dilaveris, P.; Gialernios, T.; Arsenos, P.; Karystinos, G.; Sideris, S.; Kallikazaros, I.; Stefanadis, C. Primary prevention of sudden cardiac death in a nonischemic dilated cardiomyopathy population: reappraisal of the role of programmed ventricular stimulation. Circ Arrhythm Electrophysiol. 2013, 6, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Gatzoulis, K.A.; Georgopoulos, S.; Antoniou, C.K.; Anastasakis, A.; Dilaveris, P.; Arsenos, P.; Sideris, S.; Tsiachris, D.; Archontakis, S.; Sotiropoulos, E.; Theopistou, A.; Skiadas, I.; Kallikazaros, I.; Stefanadis, C.; Tousoulis, D. Programmed ventricular stimulation predicts arrhythmic events and survival in hypertrophic cardiomyopathy. Int J Cardiol. 2018, 254, 175–181. [Google Scholar] [CrossRef]
- Gatzoulis, K.A.; Sideris, A.; Kanoupakis, E.; Sideris, S.; Nikolaou, N.; Antoniou, C.K.; Kolettis, T.M. Arrhythmic risk stratification in heart failure: Time for the next step? Ann Noninvasive Electrocardiol. 2017, 22, e12430. [Google Scholar] [CrossRef]
- Gatzoulis, K.A.; Dilaveris, P.; Arsenos, P.; Tsiachris, D.; Antoniou, C.K.; Sideris, S.; Kolettis, T.; Kanoupakis, E.; Sideris, A.; Flevari, P.; Vassilikos, V.; Kappos, K.; Maounis, T.; Katsivas, A.; Kotsakis, A.; Karvounis, H.; Kossyvakis, C.; Leventopoulos, G.; Kalpakos, D.; Tousoulis, D. ReCONSIDER study Investigators. Arrhythmic risk stratification in nonischemic dilated cardiomyopathy: The ReCONSIDER study design - A two-step, multifactorial, electrophysiology-inclusive approach. Hellenic J Cardiol. 2021, 62, 169–172. [Google Scholar] [CrossRef]
- Hohnloser, S.H.; Kuck, K.H.; Dorian, P.; Roberts, R.S.; Hampton, J.R.; Hatala, R.; Fain, E.; Gent, M.; Connolly, S.J. DINAMIT Investigators. Prophylactic use of an implantable cardioverter-defibrillator after acute myocardial infarction. N Engl J Med. 2004, 351, 2481–2488. [Google Scholar] [CrossRef]
- Steinbeck, G.; Andresen, D.; Seidl, K.; Brachmann, J.; Hoffmann, E.; Wojciechowski, D.; Kornacewicz-Jach, Z.; Sredniawa, B.; Lupkovics, G.; Hofgärtner, F.; Lubinski, A.; Rosenqvist, M.; Habets, A.; Wegscheider, K.; Senges, J. IRIS Investigators. Defibrillator implantation early after myocardial infarction. N Engl J Med. 2009, 361, 1427–1436. [Google Scholar] [CrossRef]
- Bigger, J.T. Jr. Prophylactic use of implanted cardiac defibrillators in patients at high risk for ventricular arrhythmias after coronary-artery bypass graft surgery. Coronary Artery Bypass Graft (CABG) Patch Trial Investigators. N Engl J Med. 1997, 337, 1569–1575. [Google Scholar] [CrossRef]
- Goldberger, J.J. Evidence-based analysis of risk factors for sudden cardiac death. Heart Rhythm. 2009, 6 (Suppl. S3), S2–S7. [Google Scholar] [CrossRef]
- Xenogiannis, I.; Gatzoulis, K.A.; Flevari, P.; Ikonomidis, I.; Iliodromitis, E.; Trachanas, K.; Vlachos, K.; Arsenos, P.; Tsiachris, D.; Tousoulis, D.; Brilakis, E.S.; Alexopoulos, D. Temporal changes of noninvasive electrocardiographic risk factors for sudden cardiac death in post-myocardial infarction patients with preserved ejection fraction: Insights from the PRESERVE-EF study. Ann Noninvasive Electrocardiol. 2020, 25, e12701. [Google Scholar] [CrossRef] [PubMed]
- Tsimos, K.P.; Korantzopoulos, P.; Arsenos, P.; Doundoulakis, I.; Tsiachris, D.; Antoniou, C.K.; Krikonis, K.; Sideris, S.; Dilaveris, P.; Triantafyllou, K.; Soulaidopoulos, S.; Kanoupakis, E.; Fragakis, N.; Sideris, A.; Trachanas, K.; Iliodromitis, E.; Tousoulis, D.; Tsioufis, K.; Kolettis, T.M.; Gatzoulis, K.A. Association of non-invasive electrocardiographic risk factors with left ventricular systolic function in post-myocardial infarction patients with mildly reduced or preserved ejection fraction: Insights from the PRESERVE-EF study. Ann Noninvasive Electrocardiol. 2022, 27, e12946. [Google Scholar] [CrossRef] [PubMed]
- La Rovere, M.T.; Pinna, G.D.; Maestri, R.; Mortara, A.; Capomolla, S.; Febo, O.; Ferrari, R.; Franchini, M.; Gnemmi, M.; Opasich, C.; Riccardi, P.G.; Traversi, E.; Cobelli, F. Short-term heart rate variability strongly predicts sudden cardiac death in chronic heart failure patients. Circulation. 2003, 107, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Arsenos, P.; Gatzoulis, K.A.; Dilaveris, P.; Sideris, S.; Tousoulis, D. T wave alternans extracted from 30-minute short resting Holter ECG recordings predicts mortality in heart failure. J Electrocardiol. 2018, 51, 588–591. [Google Scholar] [CrossRef]
- Arsenos, P.; Gatzoulis, K.A.; Laina, A.; Doundoulakis, I.; Soulaidopoulos, S.; Kordalis, A.; Oikonomou, G.; Triantafyllou, K.; Fragakis, N.; Vasilikos, V.; Tsioufis, K. QT interval extracted from 30-minute short resting Holter ECG recordings predicts mortality in heart failure. J Electrocardiol. 2022, 72, 109–114. [Google Scholar] [CrossRef]
- Triantafyllou, K.; Fragakis, N.; Gatzoulis, K.A.; Antoniadis, A.; Giannopoulos, G.; Arsenos, P.; Tsiachris, D.; Antoniou, C.K.; Trachanas, K.; Tsimos, K.; Vassilikos, V. Risk assessment of post-myocardial infarction patients with preserved ejection fraction using 45-minute short resting Holter electrocardiographic recordings. Annals of Non-Invasive Electrocardiology, 2023; To be published. [Google Scholar]
- Trachanas, K.; . Sideris, S.; Arsenos, P.; Tsiachris, D.; Antoniou, C.-K.; Dilaveris, P.; Triantafyllou, K.; Xenogiannis, I.; Tsimos, K.; Efremidis, M.; Kanoupakis, E.; Flevari, P.; Vassilikos, V.; Sideris, A.; Korantzopoulos, P.; Tousoulis, D.; Tsioufis, K.; Gatzoulis, K. Noninvasive risk factors for the prediction of inducibility on programmed ventricular stimulation in post-myocardial infarction patients with an ejection fraction ≥40% at risk for sudden cardiac arrest: Insights from the PRESERVE-EF study. Ann Noninvasive Electrocardiol. 2022, 27, e12908. [Google Scholar] [CrossRef]
- Xintarakou, A.; Arsenos, P.; Gatzoulis, K.A.; Manis, G.; Trachanas, K.; Soulaidopoulos, S.; Dilaveris, P.; Doundoulakis, I.; Kordalis, A.; Laina, A.; Xydis, P.; Tsimos, K.; Korantzopoulos, P.; Kolettis, T.; Tsioufis, K. Prediction of programmed ventricular stimulation inducibility using machine learning in post-myocardial infarction patients at risk for sudden cardiac arrest with preserved ejection fraction≥40% European Heart Journal, Volume 43, Issue Supplement_2, October 2022, ehac544.681. 20 October. [CrossRef]
- Gatzoulis K,; Frogoudaki, A. ; Brili, S.; Stefanadis, C. Implantable defibrillators: from the adult cardiac to the grown up congenital heart disease patient. Int J Cardiol. 2004, 97 (Suppl 1), 117–122. [Google Scholar] [CrossRef]
- Brili, S.; Aggeli, C.; Gatzoulis, K.; Tzonou, A.; Hatzos, C.; Pitsavos, C.; Stefanadis, C.; Toutouzas, P. Echocardiographic and signal averaged ECG indices associated with non-sustained ventricular tachycardia after repair of tetralogy of fallot. Heart. 2001, 85, 57–60. [Google Scholar] [CrossRef]
Figure 2.
The PRESERVE-EF study’s two-step arrhythmic risk stratification algorithm. In the total sample of patients the estimated prevalence of major arrhythmic events (MAE) during the 32-months follow-up was 1.5%. Implementation of the algorithm with the detection of the NIRFs in the first step determines the intermediate-risk subpopulation, with the MAE prevalence accounting for 4.4%. In the second step, the Programmed Ventricular Stimulation determines the actual high-risk subpopulation, with a prevalence reaching 22%. Of the 37 patients with implantable cardioverter defibrillator, there were 9 true activations during the 32-months follow-up. Neither sudden cardiac death (SCD) nor inappropriate ICD activations were observed during follow-up. Modified with permission from references [9,10].
Figure 2.
The PRESERVE-EF study’s two-step arrhythmic risk stratification algorithm. In the total sample of patients the estimated prevalence of major arrhythmic events (MAE) during the 32-months follow-up was 1.5%. Implementation of the algorithm with the detection of the NIRFs in the first step determines the intermediate-risk subpopulation, with the MAE prevalence accounting for 4.4%. In the second step, the Programmed Ventricular Stimulation determines the actual high-risk subpopulation, with a prevalence reaching 22%. Of the 37 patients with implantable cardioverter defibrillator, there were 9 true activations during the 32-months follow-up. Neither sudden cardiac death (SCD) nor inappropriate ICD activations were observed during follow-up. Modified with permission from references [9,10].
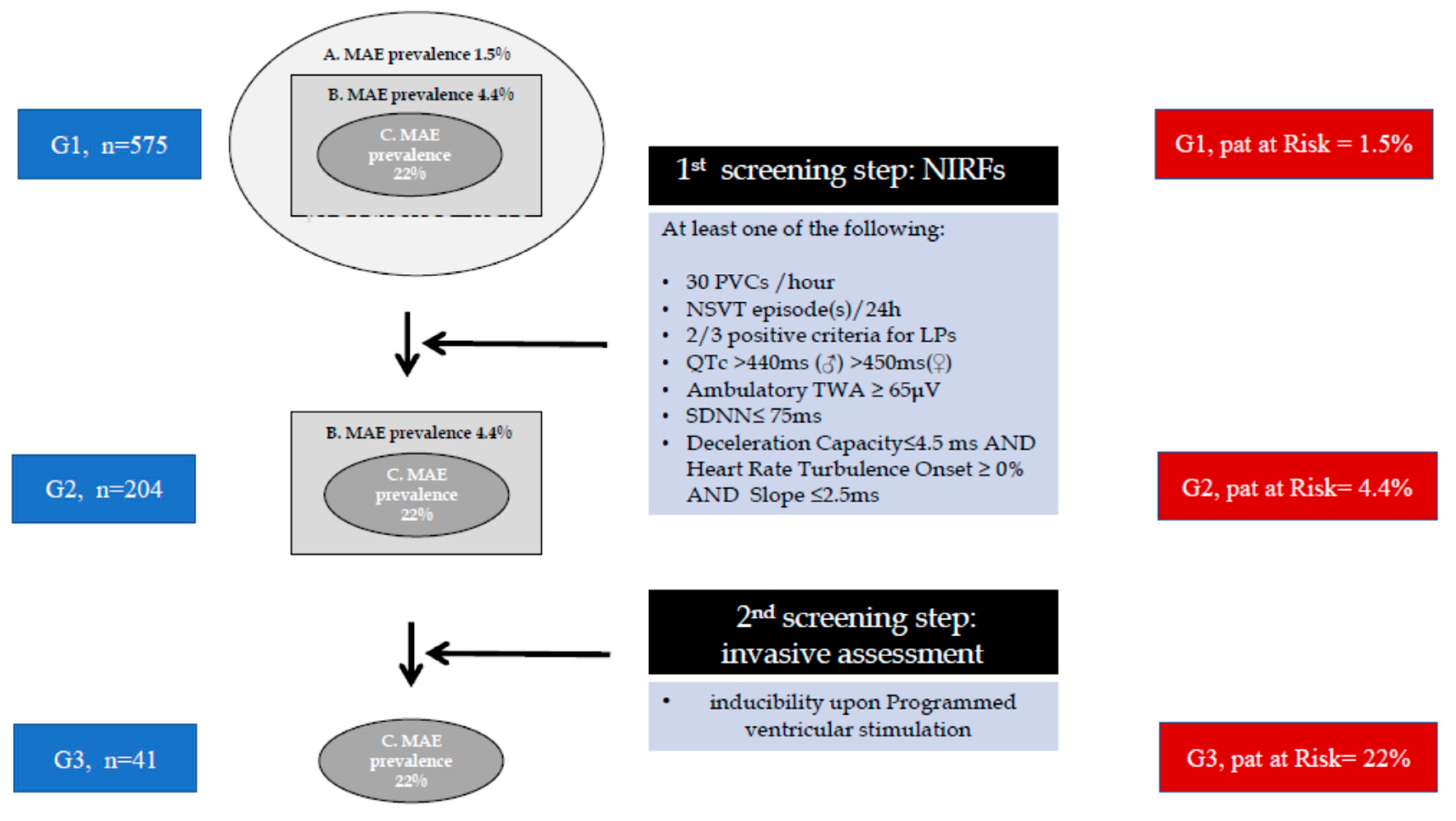
Figure 3.
Emerging new sudden cardiac death risk stratification paradigm. It is based on newer evidence, incorporating competing mortality assessments, as well as non-invasive and invasive tests. Non-invasive tests are performed before programmed ventricular stimulation (PVS) to assess the likelihood of functional circuit formation. PVS is pivotal in determining the potential for arrhythmia sustainability and guiding treatment, especially in intermediate and low-risk patients. “Observe and Follow-up” involves repeating tests for NIRF annually and PVS every 3–5 years. NIRFs (noninvasive ECG risk factors) including the presence of late potentials (≥ 2/3 criteria), frequent premature ventricular contractions (≥ 30/h), non-sustained VT (≥ 1/24 h), abnormal heart rate turbulence (onset ≥ 0% and slope ≤ 2.5ms) and reduced deceleration capacity (≤ 4.5 ms), positive T wave alternans (≥ 65 μV), decreased heart rate variability (SDNN < 70ms), prolonged QTc interval (> 440 ms in males and > 450 ms in females). Modified with permission from reference [36]. .
Figure 3.
Emerging new sudden cardiac death risk stratification paradigm. It is based on newer evidence, incorporating competing mortality assessments, as well as non-invasive and invasive tests. Non-invasive tests are performed before programmed ventricular stimulation (PVS) to assess the likelihood of functional circuit formation. PVS is pivotal in determining the potential for arrhythmia sustainability and guiding treatment, especially in intermediate and low-risk patients. “Observe and Follow-up” involves repeating tests for NIRF annually and PVS every 3–5 years. NIRFs (noninvasive ECG risk factors) including the presence of late potentials (≥ 2/3 criteria), frequent premature ventricular contractions (≥ 30/h), non-sustained VT (≥ 1/24 h), abnormal heart rate turbulence (onset ≥ 0% and slope ≤ 2.5ms) and reduced deceleration capacity (≤ 4.5 ms), positive T wave alternans (≥ 65 μV), decreased heart rate variability (SDNN < 70ms), prolonged QTc interval (> 440 ms in males and > 450 ms in females). Modified with permission from reference [36]. .
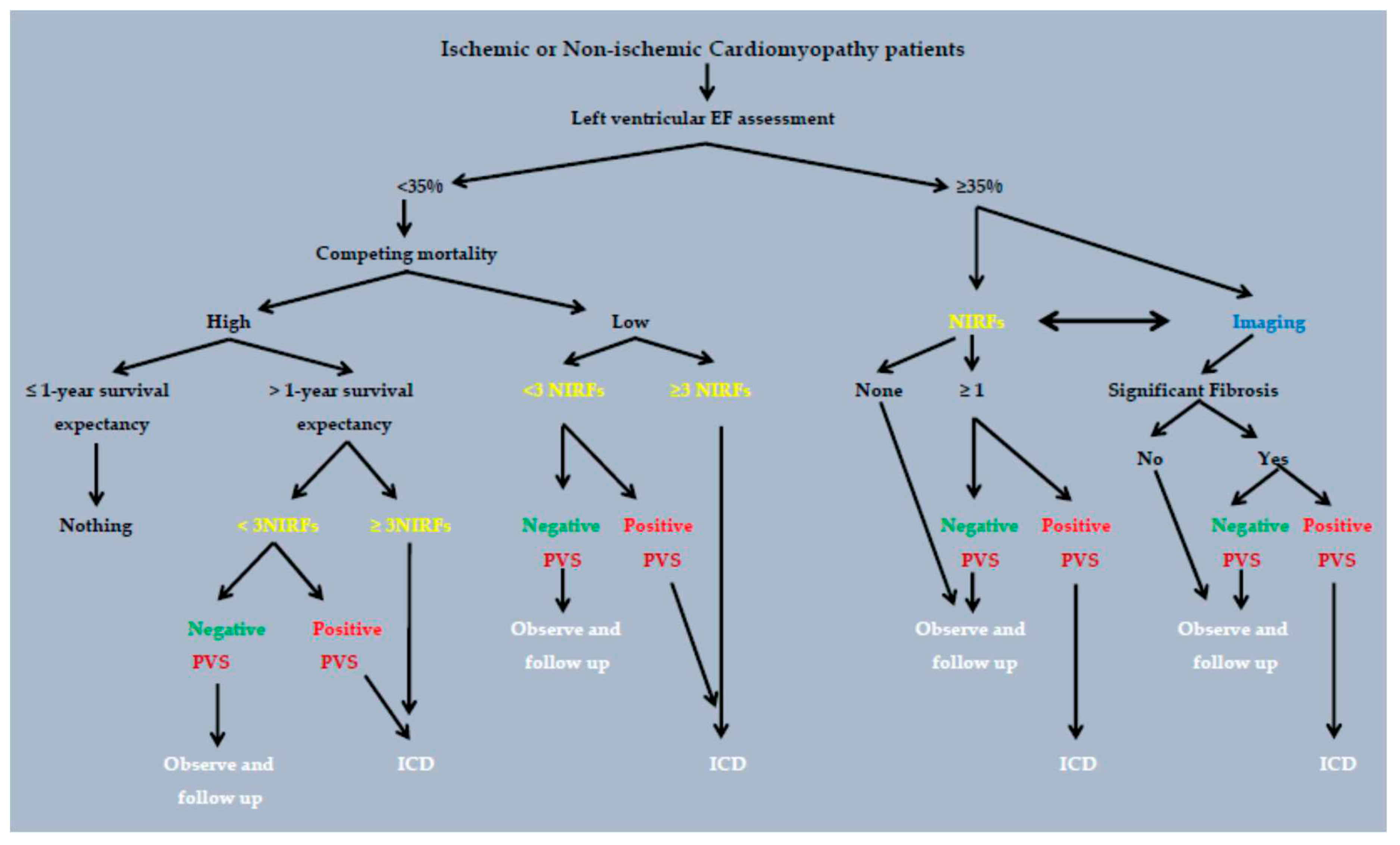
Table 2.
Abnormal values and connection of every non-invasive risk factor with the arrhythmogenic mechanisms in the PRESERVE-EF study.
Table 2.
Abnormal values and connection of every non-invasive risk factor with the arrhythmogenic mechanisms in the PRESERVE-EF study.
| Non-invasive risk factors (NIRFs) | Abnormal cut-off values | Mechanisms |
|---|---|---|
| SAECG LPs [14] | 2/3 possitive criteria | fibrotic areas, slow conduction reentry |
| QTc [21] | ≥440ms(♂), ≥450ms(♀) | prolonged repolarization, EAD, DAD |
| TWA [22] | ≥65μV (2-channels) | APD and Ca2+ alternans, steep APDR and CVR , steep FSRCR |
| VPBs [23] | ≥30/24h | automaticity (Ca2+oscillations), reentry |
| NSVT [24] | ≥1 episode/24h | automaticity (Ca2+oscillations), reentry |
| SDNN [25] | ≤75ms | enhanced sympathetic tone, autonomic imbalance |
| DC / HRT [26,27] | DC≤4.5ms HRTonset≥0%, HRT slope≤2.5ms |
vagal and sympathetic ANS dysfunction |
ANS=Autonomic nervous system; APD=Action potential duration; APDR=Action potential duration restitution; CVR= Conduction velocity restitution; DAD=Delayed afterdepolarization; DC=Deceleration capacity from heart rate dynamics; EAD= Early afterdepolarization; FSRCR=Fractional sarcoplasmic reticulum Ca2+ release; HRT= Heart rate turbulence; LPs= Late potentials from signal-averaged electrocardiogram; NSVT=Non-sustained ventricular tachycardia; QTc=Corrected according to Fridericia formula QT interval; SAECG=Signal-averaged electrocardiogram; SDNN= Standard deviation of normal to normal beats from heart rate variability analysis; TWA= T wave alternans; VPBs= Ventricular premature beats. Modified after permission from reference [9].
Table 4.
Two-step and Electrophysiology study design arrhythmic risk stratification studies investigated HFmEF, NICM and HCM populations.
Table 4.
Two-step and Electrophysiology study design arrhythmic risk stratification studies investigated HFmEF, NICM and HCM populations.
| Study | n | EF | Therapy | NIRFs searched |
NIRFS+ | EPS(n) | EPS + | Follow up (months) | EndPoints (n) |
Sens/Spe/PPV/NPV |
|---|---|---|---|---|---|---|---|---|---|---|
| Arsenos [33], 2020 |
48 Post-MI NICM |
45% | Thromb Angiopl | SAECG VPCs NSVT |
(≥1)* 32/48 |
32 | 14/32 | 41 | 9 | Sens = 87% Spec = 71% PPV = 50% NPV= 94% |
| Gatzoulis [34], 2013 |
158 NICM |
39 with EF>35%119 with EF≤35% |
ICDs | Syncope NSVT VPCs |
158 | 44/158 | 46 | 39 | Sens = 85% Spec = 91% PPV = 75% NPV= 95% |
|
| Gatzoulis [35], 2018 |
203 HCM |
64% | ICDs | Family Hist Syncope NSVT Hypot. Resp. Wall≥30 |
(≥1) * 203 |
203 | 79/203 | 60 | 20 | Sens = 95% Spec = 67% PPV = 24% NPV= 99% |
AMI=acute myocardial infarction, Angiopl=angioplasty, EF= left ventricular ejection fraction, EPS=electrophysiology study, HCM:=hypertrophic cardiomyopathy, HFmEF=heart failure with mid-range ejection fraction, HRV= heart rate variability, NICM= non-ischemic cardiomyopathy, NIRF= non-invasive risk factor, NPV=negative predictive value. NSVT=non-sustain ventricular tachycardia, n=number, post-MI=post myocardial infarction, PPV=positive predictive value, SAECG=signal averaged ECG, sens=sensitivity, spec=specificity, Thromb=thrombolysis, VPCs=ventricular premature complexes, *NIRFs cutoff point for PVS referral.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



