
Submitted:
31 August 2023
Posted:
01 September 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background:
In March 2020, a COVID-19 outbreak associated with the Falles Festival in Borriana, Spain, led to significant infections.
Methods:
In June 2022, we conducted a cross-sectional follow-up study of 473 socially engaged adults aged 18 to 64, examining the cumulative experience after SARS-CoV-2 infection and vaccination responses. Data included demographic details, lifestyle habits, medical history, infection records, and vaccinations from a population-based vaccine registry. Blood samples were analyzed for SARS-CoV-2 antibodies and cellular immunity. We employed a doubly robust inverse weighted probability analysis to estimate the booster vaccine dose's impact on long COVID prevalence and symptom count.
Results:
28.1% of participants met the WHO criteria for long COVID, with older individuals showing higher rates. Not complying with long COVID criteria associated with factors including O blood group, higher occupational status, physical activity, three vaccine doses, strong SARS-CoV-2-S-reactive IFNγ‐producing‐CD8+ response, and infection during the Omicron period. Conversely, increased age, high or low social activity, underlying health conditions, a severe initial COVID episode, and reinfection associated with higher long COVID likelihood. A booster dose, compared to one or two doses, reduced long COVID risk by 74% (95% CI: 56.4% to 91.7%) and symptom count by 55.2% (95% CI: 31.6% to 78.7%).
Conclusion:
Long COVID was prevalent in a significant portion of those who contracted COVID-19, underscoring the need for sustained follow-up and therapeutic strategies. Vaccinations, notably the booster dose, had a substantial beneficial effect on long-term infection outcomes, affirming the vaccination’s role in mitigating SARS-CoV-2 infection consequences.
Keywords:
Long COVID
; SARS-CoV-2 Vaccination
; Booster Dose
; Cellular Immunity
; Prevalence
; Risk Factors
; Human.
1. Introduction
At the time of writing there have been globally 767,518,723 confirmed cases of COVID-19, including 6,947,192 deaths, as reported to WHO [1]. Early in the pandemic, there already were reports of persistent and prolonged effects after acute COVID-19[2]. An unwelcome outcome of the SARS-CoV-2 pandemic has been non-recovery of health as before the infection due to the persistence of symptoms in a substantial number of infected subjects[3,4,5,6]. Patients themselves call it “long COVID”[7,8].
Overall, the percent of COVID-19 cases with post COVID symptoms has been estimated at a prevalence between of 43% and 23%[6,9,10], and 10%–16% in vaccinated cases[4,10]. Most long COVID cases are in non-hospitalized patients with a mild acute illness[4,6].
The diagnosis and definition of post-acute sequelae of coronavirus disease 2019 or long-COVID is an ongoing medical challenge that is not yet solved[11,12]. According to the World Health Organization (WHO) clinical case definition[13,14], post COVID-19 condition occurs in individuals with a history of probable or confirmed SARS-CoV-2 infection, usually three months from the onset of COVID-19, with symptoms that last for at least two months and cannot be explained by an alternative diagnosis. Long COVID-19 is now recognized as a multi-organ disease with a broad spectrum of manifestations[4,11,15]. Common long COVID symptoms include anosmia and dysgeusia, fatigue, shortness of breath cognitive dysfunction, hair loss, chest pain, cough, myalgia, and respiratory disorders among others, and generally have an impact on everyday functioning [3,16].
Research looking at the impact of vaccination on existing Long COVID has yielded varying results[10,17,18]. The benefit of COVID-19 vaccines on post-COVID-19 condition needs furthers study and gathering of evidence.
In March 2020 we had the opportunity to study and outbreak of 570 COVID-19 cases among 1,338 persons attending mass gathering events in Borriana, a city in the Castellón province, Valencia Region, in Spain[19]. We conducted two follow-up studies of this cohort, the first in June 2020 [31], the second in October 2020 [21]. In the second study we found that, six months after the infection, 33% of the COVID-19 cases complained of persistent symptoms [20]. The vaccination campaign started in Spain at the end of December 2020, by the end of June 2022, 97 million doses had been distributed in Spain overall, with a rate of vaccination in the overall population (one or two doses of vaccine as appropriate) of 86 % and 56% with a booster dose[21].
In June 2022 we conducted a third follow-up study. At this time, we could observe the impact on the cohort of the exposure to the Alfa, Delta, and Omicron BA.1 and BA.2 variants, and to the SARS-CoV-2 vaccination that started on the first trimester of 2021. Our aim is to describe the prevalence of long COVID, factors associated, clinical manifestations, antibody and cellular immune responses, and vaccination impact of a third booster dose compared to two doses on the risk of long COVID in a selected subset of the Borriana cohort, two years after the pandemic onset.
2. Materials and Methods
- Study Design
The origin of the Borriana COVID19 cohort and the study methods have been described in previous publications[19,20,22,23]. In short, in March 2020 a COVID-19 outbreak took place during a series of mass gathering events with 3,200 participants around the Falles Festival in Borriana, a city of 34,000 inhabitants, in the Castellon province, Valencia Community (Spain). The outbreak resulted in 536 laboratory-confirmed cases of COVID-19 among 1,132 subjects coming from an original stratified sample of 1,663 participants [19]. We performed a second serological and epidemiological follow-up in October 2020 [20,22,23].
We describe here the third follow-up of the Borriana COVID19 retrospective cohort study that we conducted in June 2022. We invited to participate the 1,132 subjects with valid laboratory test results in the first follow-up [19]. Our primary objective was to study the prevalence and factors associated with long COVID in socially engaged adults. The study population was restricted to cohort members who accepted our invitation, provided informed consent, were aged ≥18 and <65 years old, and had experienced at least one COVID-19 episode by June 2022 (Figure 1). While there's considerable debate about comparing post-COVID symptoms between those infected and those uninfected with SARS-CoV-2, we deemed it essential to explore differences specifically among the infected to provide a more focused understanding of the post-infection experience.
- Ethics
The Research Ethics Committee of the Health Department La Plana University Hospital, approved the study protocol (registry number 2961). All procedures were conducted according to good clinical epidemiological practices[24,25]. All participants provided signed informed consent to participate in the study.
- Data collection.
Health staff from the University Hospital La Plana of Vila-real, the Public Health Centre of Castelló, and the health centres of Borriana, Vila-real, Onda, and La Vall d’Uixó obtained the informed consent, collected blood samples, completed the data collection form by face-to-face or phone interviews, and acquired information on vaccines administered (vaccine brand, and vaccination dates) consulting the population-based Valencia Region Vaccine Information System (VIS). From the interview we obtained demographic data (age, sex), number of household members, occupation and education levels, lifestyle (smoking habit, alcohol consumption, physical exercise, intensity of social contacts, leisure, or work), body mass index (BMI = kg/m2, obesity ≥ 30.0), underlying chronic illnesses and SARS-CoV-2 infection and reinfection information. By each infection episode, we obtained the date of infection, symptoms, duration of the illness, medical consultation, admission, and diagnostic tests performed. We also collected information on return to the usual state of health, health recovery, post COVID sequelae, duration of the sequelae, and the presence of 31 symptoms at the time of the interview. Participants were asked to complete the Generalized Anxiety Disorder Screener (GAD-7) and Patient Health Questionnaire 9 (PHQ-9) questionnaires in their validated Spanish versions [26,27,28,29]. At the time of the interview researchers were unaware of long COVID status.
- Laboratory procedures.
Laboratory procedures in the previous follow-up studies are described in a previous publication[30]. For the current follow-up, sera were tested by chemoluminiscence immunoassay (CLIA)) (Alinity | Anti-SARS-CoV-2 S and N, Abbot Laboratories, Chicago, USA); the S assay targets the SARS-CoV-2 spike protein, and the N assay targets antibodies to the nucleocapsid protein. We interpret anti-N as a proxy for previous SARS-CoV-2 infection[31]. We also determined the vitamin D sera levels, and if not already available the blood group. All tests were performed at the Microbiology Service Laboratory of the University Hospital de la Plana, Vila-real.
In December 2022, we obtained additional blood samples in a subset of 225 cohort members to determine cell immunity against the Wuhan and Omicron BA.2 variants of concern (VOC). Determinations were with flow cytometry functional cellular assays based on the detection of markers of T cell activation such as IFN-ɣ release assay QIAGEN’s QuantiFERON SARS-CoV-2[32]. Enumeration of SARS-CoV-2-S-reactive IFNγ-producing-CD8+ and CD4+ T cells in fresh heparinized whole blood was carried out by flow cytometry for intracellular cytokine staining (BD Fastimmune, Becton Dickinson and Company-Biosciences, San Jose, CA) as previously described[33,34] (Supplement Cellular Immunity, methods). Specimens were assayed at the Microbiology Service of the Hospital Clínico Universitario of Valencia (HCU).
- Statistical analysis
- Outcomes and exposure definitions
- SARS-CoV-2 infection, Long COVID and number of reported symptoms.
We defined SARS-CoV-2 infection by either recall or a previously positive laboratory test, regardless of symptoms. We defined long COVID in individuals with symptoms for at least two months and three months from the date of a previous SARS-CoV-2 infection [13,14]. We computed the number of symptoms per subject from the positive answers to the presence of any of 31 symptoms in the face-to-face interview.
- Infection period
We considered four major time periods of SARS-CoV-2 infection as per the predominant VOC in Spain in each period[35,36]: Wuhan-D164G (any infection <1 January 2021), Alfa (any infection ≥ 1 January 2021 and < 1 August 2021), Delta (infection ≥ 1 August 2021 and before 1 December 2021) and Omicron (infection ≥ 1 December 2021 to June 2022) (Figure 2).
- Priming and booster
We defined subjects as primed 14 days after receiving one, two doses and boosted 14 days after the third dose. Subjects that did not comply with the former criteria, not vaccinated or with missing vaccination dates were excluded from the analysis of the booster effect on long COVID.
- Descriptive analysis
We assessed differences by long COVID status in the distribution of sociodemographic factors, exposures, clinical manifestations, and immune status. We considered standardized mean differences (SMD) ≥ 0.2 to indicate a nonnegligible difference in the mean or prevalence of a covariate by long COVID status [37], SMD are not influenced by sample size and allow for the comparison of the relative balance of variables measured in different units[38]. We used the T-test, Chi-squared (χ²) test, non-parametric test for bivariate comparisons and trend test for ordinal variables, we considered a difference as significant if bilateral p-value was <0.05. We assessed departure from linearity in categorical ordered variables, and interaction between potential confounders by the likelihood ratio test. We estimated the odds ratio (OR) associated with sociodemographic factors and other risk factors using unadjusted bivariate logistic regression.
- Inferential analysis
To estimate the effect of the booster dose on the risk of long COVID and the number of symptoms per subject we restricted our analysis to the subjects with a first infection during the period of the third dose roll, January 2022 onward, and compared the risk of long Covid and the number of symptoms in boosted vs. primed with one or two doses. As a sensitivity analysis, we performed the same analysis restricted to those with their first infection in March 2020, a period well before the introduction of SARSCoV-2 vaccines (Figure 2). We estimate the booster impact as the adjusted treatment effect obtained from doubly robust inverse-probability weighting[39]. We used previous knowledge and directed acyclic graphs (DAG) [13,14] to define the variables to improve comparability and exchangeability between the comparison groups and to clarify the minimum set of variables to perform the adjusted analysis (Supplemental Fig1), following both criteria we adjusted by age, as a categorical variable, 18-24, 25-34, 35-49, 50-64; blood group, as four categories variable; occupational class, qualified and over compared to other; household membership size in two categories, one or two, and two or more members; body mass index as ≥30 or lower; and outpatient consultation for the 1st episode, yes or no. The booster effect as relative risk reduction (RRR) is estimated as the ((risk in those no boosted - risk in boosted group)/ risk in those no boosted)) *100. The RRR confidence intervals are computed by the delta method, for possibly nonlinear combinations of parameter estimates[40]. We considered 95% confidence intervals to reject the null hypothesis of no effect when the unity value was not contained.
- Statistical package
We performed all analysis with STATA 18® (StataCorp, 4905 Lakeway Drive College Station, Texas 77845 USA).
3. Results
3.1. Major characteristics of the included subjects.
We included 473 individuals aged 18-64 previously infected with SARS-CoV-2. The mean age of all subjects was 41.9 ± 12.9 (mean ± standard deviation). Females outnumbered males (300 vs 173; 63.4% vs 33.8%) (Table 1). Regarding other characteristics, 288 (62.9%) of the included individuals were at least qualified skilled; 216 (46.6%) had a university education level; 262 (55.4%) reported regular physical activity; 190 (40.5%) were smokers or ex-smokers; 143 (30.6%) had underlying illness and 133 (28.3%) were obese. Only 9 (1.9%) of all subjects had not received at least one vaccine dose; 315 (66.9%) had their first infection in the Wuhan and 134 (28.5%) in the Omicron period (Figure 2 and Table 1), finally, 120 (25.4%) recollected a second COVID episode. The prevalence of long COVID was higher in those who were infected during the Ancestral (Wuhan) period (99 out of 315; 31.4%) as compared to the Omicron period (23 out of 134; 17.2%), (p=0.002).
3.2. Factors associated with long COVID.
We found that 133 (28.1%) of the 473 included cohort members met the criteria for long COVID (Figure 1). We observed the prevalence of long COVID to increase with advancing age, with a proportion of 10.0 % (7 out of 70) in the 18 to 24 age group, 29.4 % (74 out of 252) in the 25 to 49 age group, and 34.4 % (52 out of 151) in the 50 to 64 age group with a significant trend for age (p=0.0010). Long COVID patients were older than non-long COVID patients (44.5± 11.7 vs 40.8±13.2; SMD -0.30, not shown in Table 1). When comparing individuals with and without long COVID, we found that the O blood group, higher occupational class, more than two household members, regular physical activity, three vaccine doses and infection in the Omicron period were related to a lower prevalence of long COVID. Contrary wise, in addition to age, a minimal or high level of social activity, underlying illnesses and reinfection were related to a higher probability of long COVID (Table 1).
3.3. COVID episode characteristic and long COVID status.
Long COVID was more prevalent among individuals who suffered a more severe initial COVID-19 episode in comparison to their counterparts who did not experience long COVID, as presented in Table 2. Long COVID patients, after their initial SARS-CoV-2 infection, reported a higher frequency of symptomatic episodes (90.2% vs. 72.8%), of longer duration (12.9 vs 7.0 days), with more outpatient consultations (58.0% vs 40.7%), and hospital admissions (6.8% vs 1.8%) as compared to the cohort members who did not meet the criteria for long COVID definition. With regards to reinfection, it was observed that the presence of symptoms, medical consultations and admissions were more common (SMD>0.2) in long COVID patients, however, all estimated OR CI were nonsignificant (Table 2).
3.4. Post COVID outcomes
In total, 77.8% of the included members identified themselves as fully recovered following their SARS-CoV-2 infection. Furthermore, 81.4% perceived their current health status as either good or excellent, while 73.8% reported being as healthy as prior to their infection. A noteworthy proportion of individuals without long COVID demonstrated superior parameters across these three outcomes in comparison to subjects who experienced long COVID (Table 2). A significantly greater number of long COVID patients reported experiencing sequelae (84.2%) when contrasted with those without long COVID (9.7%). In addition, individuals with long COVID were at a significantly higher risk of anxiety (OR, 1.79; 1.18-2.72) or depression (OR, 1.82; 1.15-2.86) as compared to their counterparts without long COVID.
3.5. Reported symptoms.
At the time of the follow-up in June 2022, all participants were queried regarding the existence of a battery of 31 symptoms. The mean number of symptoms reported was 2.2 ± 3.22, with a notable significant difference in the number of symptoms reported between no long COVID and long COVID subjects, 1.6 ± 2.7 versus 3.8 ± 3.9, SMD -0.6550, p=0.0001 (Table 2; p-value not shown). There was no observable variation in the number of symptoms reported in those with a singular COVID-19 infection compared to those with a reinfection (mean ± standard deviation) 2.1 ± 3.1 symptoms versus 2.7 ± 3.9, SMD -0.1747, p= 0.1043 (data not shown).
As illustrated in Figure 3 and Table 3, there was a noteworthy differentiation in the prevalence of 15 out of the 31 symptoms between individuals with long COVID and those without. The symptoms that exhibited the most substantial differences in absolute percentage points and were most frequently reported include fatigue/tiredness and hair-loss (with a difference greater than 20% and present in 40.6% and 33.8% of long COVID subjects, respectively). Other symptoms with notable differences include dysgeusia, restlessness, dyspnoea, memory loss, difficulty in concentration, anxiety, and insomnia. Although less frequent, visual flashes, speech difficulties, and nausea or vomiting were still considerably more prevalent in individuals with long COVID, with a standardized mean difference (SMD) greater than 0.2.
3.6. Vaccine booster dose impact on long COVID prevalence and the number of reported symptoms.
After excluding nine non vaccinated and three infected <14 days after vaccine administration, and with no further exclusions, 319 (69.2%) cohort members were immunized with a third dose or boosted, and 142 (30.8%) had received one or two vaccine doses.
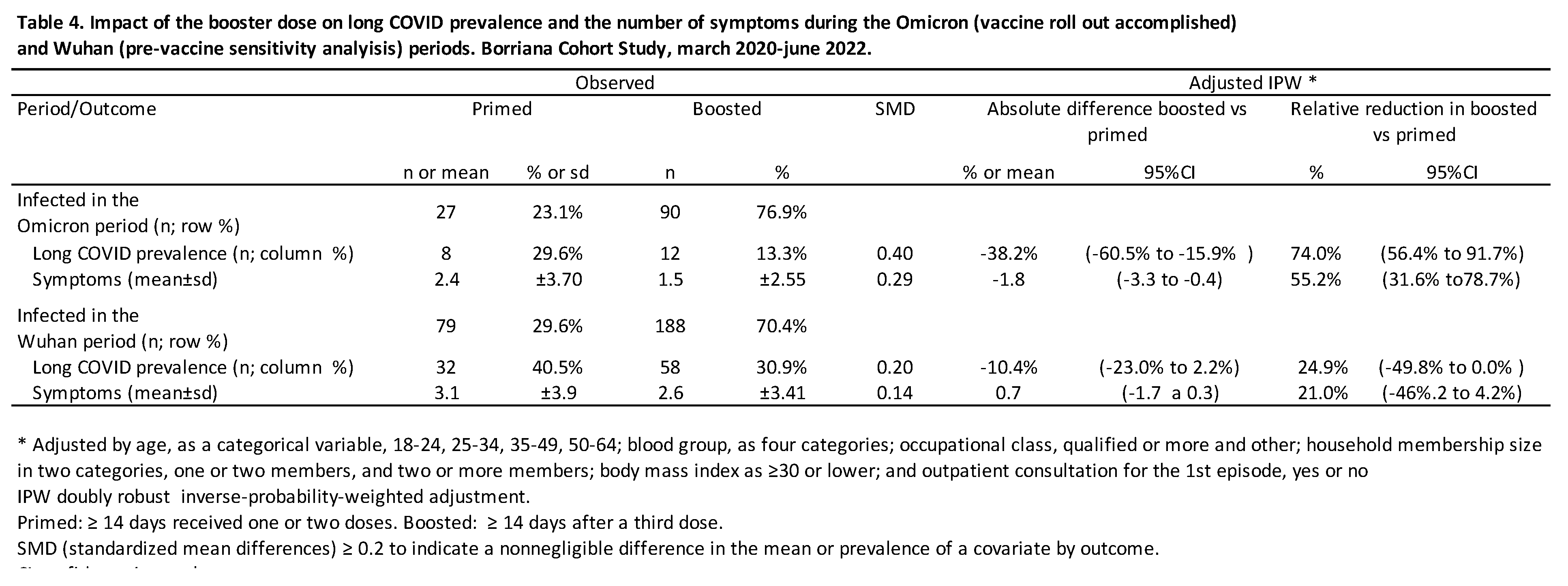
When performing the analysis restricted to the 117 cohort members with their first infection during the Omicron period and on or after the 1st of January 2022, the period of the third dose rollout (Figure 2), 90 (76.9%) were boosted and 27 (23.1%) were primed. The unadjusted prevalence of long COVID was 13.3 % among boosted and 29.6 % in those primed; SMD=0.40. The number of symptoms was 1.5 ± 2.6 in boosted compared to 2.4±3.7 in primed; SMD, 0.29.
In the adjusted analysis, we have estimated an absolute reduction in the prevalence (%) of long COVID of -38.2% (-60.5% to -15.9%) among boosted subjects compared to primed subjects. Furthermore, an adjusted RRR of 74.0% (56.4% to 91.7%) was observed in boosted subjects compared to primed ones. In terms of the number of symptoms, we noted that boosted subjects experienced a mean reduction of -1.8 (-3.3 to -0.4) symptoms when compared to primed subjects. The adjusted RRR in those who were boosted vs. primed was 55.2% (31.6% to 78.7%) (Table 4).
3.7. Sensitivity analysis
To assess the sensitivity of our findings, we estimated the booster effect on the prevalence of long COVID and the number of symptoms experienced by individuals who had their first infection in March 2020, well before the vaccine became available. Of the 267 cohort members, a total of 188 (70.4%) were boosted, while 79 (29.6%) were primed. The unadjusted observed prevalence of long COVID was 40.5% in boosted subjects and 30.9% in primed ones, which is indicative of a non-negligible difference, with an SMD of 0.20. In terms of the number of symptoms, the primed group reported 3.1 ±3.9, while the boosted group reported 2.6 ±3.4, with no evidence of a difference between the groups, as indicated by an SMD of 0.14. In the adjusted analysis, all the confidence intervals were compatible with either no significant booster effect or a null booster effect (Table 4).
4. Discussion
4.1. Summary of Key Findings
Our study, based on the Borriana COVID-19 cohort in the Valencia Region of Spain, provides valuable insights into the prevalence, risk factors, clinical manifestations, and vaccination impact in the number of symptoms and the likelihood of long COVID in socially engaged adults who had experienced at least one SARS-CoV-2 infection episode from March 2020 till June 2022.
Using the long COVID WHO definition[13,14], we observed that long COVID was present in one in three cohort members after their initial SARS-CoV-2 infection. Our findings suggest that increasing age, low social class and social support, underlying illnesses, reinfection, and severity of the first episode are associated with a higher risk of long COVID. Subjects with long COVID reported a poorer perception of their health status, experienced an average of four persistent symptoms compared to two in subjects without long COVID, and more frequently experienced moderate to severe anxiety or depression than those without long COVID. Notably, our data indicate that receiving a booster dose of the COVID-19 vaccine may be associated with a lower prevalence of long COVID and fewer reported symptoms.
4.2. Long COVID definition and comparison groups.
Our study supports that long COVID is not a rare outcome, aligning with previously published estimates, in ranges from 25% to 46% in nonhospitalized patients [6,9]. The higher prevalence of long COVID by age group in our cohort is consistent with other studies[41,42]; emphasizing the need for targeted interventions to prevent long COVID also in the less than 65 years old age group. In addition to age, the association of long COVID with social factors, genetic profile, and underlying disorders observed in our study is also in line with the existing literature[4,6,41,43]. Although we did not identify a differential risk by gender we cannot discard it, as we observed a 18% higher risk in females, albeit not reaching significance.
While there is evidence of prolonged immune activation in severe COVID-19 cases, the relationship between this immune activation and long COVID symptoms is complex and not directly correlated [44]. A number of studies considered parameters of antibody and T cell immunity to SARS-CoV-2 antigens, especially S and N, to evaluate the hypothesis that the risk of long COVID might be associated with an abnormally high or low immune response to acute infection[45]. We have observed that a SARS-CoV-2-S-reactive IFNγ-producing-CD8+ response was significantly associated with a lower risk of long COVID (Table 1). It has been described how CD8+ cytotoxic lymphocytes interrupt viral replication by secreting antiviral cytokines (IFN-gamma and TNF-alpha) and directly killing infected cells, negatively correlating with stages of disease progression[46].
Previous infection with pre-Omicron variants is one of the risk factors for post-acute sequelae of SARS-CoV-2 symptoms[6]. The current estimates of the prevalence of post-COVID symptoms and functional impairment are mostly based on infection with early variants of SARS-CoV-2 [47]. Some authors have described as we also have observed a lower risk of long COVID in subjects infected during the Omicron period suggesting that infection by BA.1 and BA.2 lineages was of less severity than previous variants. It has been suggested that the better outcomes could be due to the immunity provided by previous infection and vaccination. We provide relevant information circumscribed to those infected in the Omicron period and show the salutary effect of booster doses of vaccines. Supporting this hypothesis, we found an inverse-probability-weighted adjusted prevalence of long COVID at the time of follow-up to be 51.6% (30.4% to 72.8%) in those who received only the primary vaccine series, compared to 13.4% (6% to 20.8%) in those who received a booster dose (data not shown). We speculate that, although the overall burden of COVID has diminished, the possibility of adverse outcomes following SARS-CoV-2 infection with new circulating variants should not be discounted, especially among socially active adults who have not received updated vaccine protection or whose vaccine protection has waned.
4.3. Vaccination and Long COVID
Our findings contribute to the growing body of evidence on the potential benefits of COVID-19 vaccination in reducing the risk of long COVID[48,49] and specially in those less than 65 as reported by others [50].
Recent systematic reviews conclude that vaccination before SARS-CoV-2 infection could reduce the risk of subsequent long COVID; but, that the effect of vaccination on people with pre-existing long COVID was inconsistent, with some studies showing symptom improvement and others not[18]. Vaccination with two doses could be more effective than a single dose in reducing the risk of developing long COVID [48]. Vaccination before Omicron BA.1 infection including the receipt of booster vaccines was not associated with a significant protective effect against the number of post-acute COVID-19 symptoms [51], whereas others report that symptoms were less common in vaccinated versus nonvaccinated individuals with Omicron infection [47]. Current studies do not report specific evidence on the impact of a booster or third dose of the COVID-19 vaccine on long-COVID in patients who have already been infected[45,52].
Our results suggests that individuals who received a booster dose of the vaccine, and were infected during the Omicron period, reported fewer long COVID symptoms and a lower prevalence of long COVID compared to those who were primed. This is a significant finding, given the global push for booster vaccinations. Additionally, our sensitivity analysis, focusing on individuals with their first infection before the vaccine rollout, did not show a significant booster effect, supporting the validity of our findings regarding the positive vaccination impact.
4.4. Strengths of the Study.
The major strengths of our study reside in the follow-up of the cumulative experience during more than two years of a well-defined and studied incipient cohort, with broad data collection, the use of a population-based vaccine registry, determination of markers of the immune response, and a robust statistical analysis. We argue, additionally, the relevance of comparing the outcomes among socially active community dwelling 18-64 of age adults, previously infected with SARS-CoV-2 at the time of follow-up. The collection of data was unaffected by prior knowledge on the long COVID status of the cohort members included in the study, more than 85% of COVID episodes were laboratory confirmed with no differences between subjects without or with long COVID criteria. The distribution of risk factors, episode characteristics, outcomes, and immune responses between the two groups was consistent with previously published systematic reviews [3,5,6,41,53]. Accordingly, we contend that our findings are pertinent for evaluating and interpreting the prevalence, risk factors, clinical outcomes, and vaccination impact on long COVID among the subjects in our cohort who were included in the June 2022 follow-up.
4.5. Limitations
Our study has several limitations. The cohort is based in a specific region of Spain, which limits the generalizability of our findings. Additionally, our study is observational, and while we employed a doubly robust inverse probability weighting for our impact estimations, residual confounding may still be present. The reliance on self-reported symptoms and medical history may also introduce recall bias. We used a cross-sectional approach, and we analyze vaccination impact and long COVID characteristics as a fixed clinical condition at the time of follow-up, as a cumulative experience. We cannot discard selection bias due to self-reference bias as suggested by the overrepresented female group, at 63.4% although females were overrepresented in the first study (60.1%) and the second follow-up (62.2%). The overrepresentation of females has been also reported, however, on other observational studies[51] being in some cases as high as 80%, whereas in others it was males those who were overrepresented[54]. Finally, we did not conduct an analysis based on vaccine type, time elapsed since vaccination, or the timing of vaccination relative to infection. This was due to the short post-vaccination follow-up period and the limited sample size. Nonetheless, we can speculate that calendar time would act as a non-differential bias, potentially biasing our results toward the null hypothesis. This makes our findings on the cumulative impact of booster doses at the time of the follow-up particularly relevant. We do not include potential adverse vaccination effects. Adverse vaccination effects have the potential to skew study results, particularly if they result in differential uptake of booster doses. These effects may also be correlated with other variables of interest, such as age or pre-existing conditions, thereby confounding the study outcomes. Our sensitivity analysis partially accounts for this potential bias. Future studies may need to address these limitations to refine our understanding further. The current findings should be interpreted considering these limitations.
4.6. Clinical Implications
Our findings underscore the importance of comprehensive care for individuals recovering from COVID-19, particularly those with identified risk factors for long COVID. The potential benefit of booster vaccinations in reducing long COVID prevalence and the number of persistent symptoms, as suggested by our data, may inform, and reinforce public health policies regarding vaccination strategies in the coming seasons.
5. Conclusions
In conclusion, our study provides important insights into the prevalence, risk factors and clinical manifestations of long COVID in the Borriana cohort in Spain. Our findings suggest a potential protective effect of booster vaccinations against long COVID even in those under 65 years of age. Our findings contribute to a better understanding of who is at higher risk of long COVID and provide additional evidence for the benefits of vaccination, providing for a more focused follow-up and management of COVID patients and targeted social support and public health interventions. As SARS-CoV-2 continues to circulate and evolve, ongoing research into long COVID, its risk factors, and potential mitigation and therapeutic strategies, including vaccination, remains a global priority.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Laboratory methods. Supplement Cellular Immunity, methods. Supplemental Table 1. Comparison of the characteristics of COVID-19 episodes by immunization status: analysis of primed individuals (with prior COVID-19 infection, having received one, or two doses) versus those who received a third booster dose. Supplementary Table 2. Participant characteristics associated with immunization, comparing between those primed (with prior COVID-19 infection and having received one, or two doses) and those who received a third booster dose. Supplementary Figure 1 DAG analysis
Author Contributions
Conceptualization: SDM, AAP, MRPS, JPB, AOS, GBM, MGT, OPO, DST, MSU. Methodology: JPB, AAP, SDM, MRPS, AOS. Data management, SDM. AAP, MRSP, JPB, GBM, MGT, OPO, DST, MSU. Formal analysis: JPB, AAP, MRPS. Writing original draft: JPB. Review and editing, JPB, AAP, MRPS, SDM, AOS, GBM, MGT, OPO, DST, MSU. Project management, SDM, AAP, MRSP, AOS. GBM, MGT, OPO, DST, MSU. Funding acquisition, AOS, SDM, JPB. All authors have read and agreed to the published version of the manuscript.
Funding
Project funded by Conselleria de Sanitat Universal i Salut Pública (Generalitat Valenciana, Spain) and the EU Operational Program of the European Regional Development Fund (ERDF) for the Valencian Community 2014–2020, within the framework of the REACT-EU programme, as the Union’s response to the COVID-19 pandemic.
Institutional Review Board Statement
This study (BO-CO-COVID-2 FALLAS DE BORRIANA) has been approved by the Ethics Committee of the University Hospital de la Plana, Vila-real. Date 14 October 2021 (IRB number 2961).
Informed Consent Statement
Written informed consent provided by all participants.
Data Availability Statement
Available from the authors upon reasoned request.
Acknowledgments
We thank the participants in this study and organization team of each falla of Borriana for their support and help. In addition, we wish to thank Belen Cervera-Ferrer, Ursula Clerig-Arnau, Claudia Dols-Bernad, Paula Vidal-Utrillas, Sonia Valls-López, María Dolores Llopico- Vilanova, Irene Suarez-Linares, María Soledad Carregui-Alagarda, and Belen Martinez-Martinez for your assistance and help.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO. WHO Coronavirus (COVID-19) Dashboard. In: Dashboard WHE, Homepage WC-, editors.2023.
- Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, Stevens JS, et al. Post-acute COVID-19 syndrome. Nat Med. 2021;27:601-15.
- Aiyegbusi OL, Hughes SE, Turner G, Rivera SC, McMullan C, Chandan JS, et al. Symptoms, complications and management of long COVID: a review. J R Soc Med. 2021;114:428-42. [CrossRef]
- Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023:1-14.
- Groff D, Sun A, Ssentongo AE, Ba DM, Parsons N, Poudel GR, et al. Short-term and Long-term Rates of Postacute Sequelae of SARS-CoV-2 Infection: A Systematic Review. JAMA Netw Open. 2021;4:e2128568.
- Chen C, Haupert SR, Zimmermann L, Shi X, Fritsche LG, Mukherjee B. Global Prevalence of Post-Coronavirus Disease 2019 (COVID-19) Condition or Long COVID: A Meta-Analysis and Systematic Review. J Infect Dis. 2022;226:1593-607.
- Callard F, Perego E. How and why patients made Long Covid. Soc Sci Med. 2021;268:113426. [CrossRef]
- Alwan NA. Lessons from Long COVID: working with patients to design better research. Nat Rev Immunol. 2022;22:201-2. [CrossRef]
- Ballouz T, Menges D, Anagnostopoulos A, Domenghino A, Aschmann HE, Frei A, et al. Recovery and symptom trajectories up to two years after SARS-CoV-2 infection: population based, longitudinal cohort study. BMJ. 2023;381:e074425.
- Azzolini E, Levi R, Sarti R, Pozzi C, Mollura M, Mantovani A, et al. Association Between BNT162b2 Vaccination and Long COVID After Infections Not Requiring Hospitalization in Health Care Workers. JAMA. 2022;328:676-8. [CrossRef]
- Turner S, Khan MA, Putrino D, Woodcock A, Kell DB, Pretorius E. Long COVID: pathophysiological factors and abnormalities of coagulation. Trends Endocrinol Metab. 2023;34:321-44. [CrossRef]
- Talla A, Vasaikar SV, Szeto GL, Lemos MP, Czartoski JL, MacMillan H, et al. Persistent serum protein signatures define an inflammatory subcategory of long COVID. Nat Commun. 2023;14:3417. [CrossRef]
- Soriano JB, Murthy S, Marshall JC, Relan P, Diaz JV, Condition WHOCCDWGoP-C-. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect Dis. 2022;22:e102-e7. [CrossRef]
- World Health Organization. Public health surveillance for COVID-19: interim guidance. July 22, 2022 ed2022.
- Spinicci M, Graziani L, Tilli M, Nkurunziza J, Vellere I, Borchi B, et al. Infection with SARS-CoV-2 Variants Is Associated with Different Long COVID Phenotypes. Viruses. 2022;14:2367.
- Mizrahi B, Sudry T, Flaks-Manov N, Yehezkelli Y, Kalkstein N, Akiva P, et al. Long covid outcomes at one year after mild SARS-CoV-2 infection: nationwide cohort study. BMJ. 2023;380:e072529.
- Al-Aly Z, Bowe B, Xie Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat Med. 2022;28:1461-7.
- Notarte KI, Catahay JA, Velasco JV, Pastrana A, Ver AT, Pangilinan FC, et al. Impact of COVID-19 vaccination on the risk of developing long-COVID and on existing long-COVID symptoms: A systematic review. EClinicalMedicine. 2022;53:101624. [CrossRef]
- Domenech-Montoliu S, Pac-Sa MR, Vidal-Utrillas P, Latorre-Poveda M, Del Rio-Gonzalez A, Ferrando-Rubert S, et al. "Mass gathering events and COVID-19 transmission in Borriana (Spain): A retrospective cohort study". PLoS One. 2021;16:e0256747. [CrossRef]
- Domenech-Montoliu S, Puig-Barbera J, Pac-Sa MR, Vidal-Utrillas P, Latorre-Poveda M, Del Rio-Gonzalez A, et al. Complications Post-COVID-19 and Risk Factors among Patients after Six Months of a SARS-CoV-2 Infection: A Population-Based Prospective Cohort Study. Epidemiologia (Basel). 2022;3:49-67.
- Ministerio de Sanidad. Alertas y emergencias sanitarias Alertas de salud pública de actualidad Eventos de salud pública en seguimiento Enfermedad por SARS-CoV-2 (COVID-19) Vacuna Covid-19Cuadro de mando resumen de datos de vacunación. 2023.
- Domènech-Montoliu S, Puig-Barberà J, Pac-Sa MR, Vidal-Utrillas P, Latorre-Poveda M, Rio-González AD, et al. ABO Blood Groups and the Incidence of Complications in COVID-19 Patients: A Population-Based Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2021;18:10039-. [CrossRef]
- Domènech-Montoliu S, Puig-Barberà J, Pac-Sa MR, Vidal-Utrillas P, Latorre-Poveda M, Del Rio-González A, et al. Persistence of Anti-SARS-CoV-2 Antibodies Six Months after Infection in an Outbreak with Five Hundred COVID-19 Cases in Borriana (Spain): A Prospective Cohort Study. Covid. 2021;1:71-82.
- Hoffmann W, Latza U, Baumeister SE, Brunger M, Buttmann-Schweiger N, Hardt J, et al. Guidelines and recommendations for ensuring Good Epidemiological Practice (GEP): a guideline developed by the German Society for Epidemiology. Eur J Epidemiol. 2019;34:301-17. [CrossRef]
- von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4:e296.
- Garcia-Campayo J, Zamorano E, Ruiz MA, Pardo A, Perez-Paramo M, Lopez-Gomez V, et al. Cultural adaptation into Spanish of the generalized anxiety disorder-7 (GAD-7) scale as a screening tool. Health Qual Life Outcomes. 2010;8:8. [CrossRef]
- Lowe B, Decker O, Muller S, Brahler E, Schellberg D, Herzog W, et al. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med Care. 2008;46:266-74. [CrossRef]
- Diez-Quevedo C, Rangil T, Sanchez-Planell L, Kroenke K, Spitzer RL. Validation and utility of the patient health questionnaire in diagnosing mental disorders in 1003 general hospital Spanish inpatients. Psychosom Med. 2001;63:679-86. [CrossRef]
- Huang FY, Chung H, Kroenke K, Delucchi KL, Spitzer RL. Using the Patient Health Questionnaire-9 to measure depression among racially and ethnically diverse primary care patients. J Gen Intern Med. 2006;21:547-52. [CrossRef]
- Domenech-Montoliu S, Puig-Barbera J, Guerra-Murcia O, Pac-Sa MR, Orrico-Sanchez A, Gomez-Lanas L, et al. ABO Blood Groups and Incidence of COVID-19 in the Mass Gathering Events in Borriana (Spain), March 2020: A Retrospective Cohort Study. Epidemiologia (Basel). 2023;4:63-73. [CrossRef]
- National S-C-SAEG. Performance characteristics of five immunoassays for SARS-CoV-2: a head-to-head benchmark comparison. Lancet Infect Dis. 2020;20:1390-400.
- Tormo N, Gimenez E, Martinez-Navarro M, Albert E, Navalpotro D, Torres I, et al. Performance comparison of a flow cytometry immunoassay for intracellular cytokine staining and the QuantiFERON(R) SARS-CoV-2 test for detection and quantification of SARS-CoV-2-Spike-reactive-IFN-gamma-producing T cells after COVID-19 vaccination. Eur J Clin Microbiol Infect Dis. 2022;41:657-62.
- Albert E, Burgos JS, Peiro S, Salas D, Vanaclocha H, Gimenez E, et al. Immunological response against SARS-CoV-2 following full-dose administration of Comirnaty(R) COVID-19 vaccine in nursing home residents. Clin Microbiol Infect. 2022;28:279-84.
- Torres I, Albert E, Gimenez E, Alcaraz MJ, Botija P, Amat P, et al. B- and T-cell immune responses elicited by the Comirnaty(R) COVID-19 vaccine in nursing-home residents. Clin Microbiol Infect. 2021;27:1672-7.
- Centro de Coordinación de Alertas y Emergencias Sanitarias. Evaluaciones rápidas de riesgo de las variantes de SARS-CoV-2 en España. Evaluaciones rápidas de riesgo de las variantes de SARS-CoV-2 en España: Ministerio de Sanidad; 2023.
- Hodcroft E. CoVariants. Overview of Variants in Countries. Covariants.org.
- Normand ST, Landrum MB, Guadagnoli E, Ayanian JZ, Ryan TJ, Cleary PD, et al. Validating recommendations for coronary angiography following acute myocardial infarction in the elderly: a matched analysis using propensity scores. J Clin Epidemiol. 2001;54:387-98.
- Austin PC. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivariate Behav Res. 2011;46:399-424. [CrossRef]
- Robins JM, Hernán MA, Brumback B. Marginal structural models and causal inference in epidemiology. Epidemiology (Cambridge, Mass). 2000;11:550-60. [CrossRef]
- Phillips PCB, Park JY. On the Formulation of Wald Tests of Nonlinear Restrictions. Econometrica. 1988;56:1065-83. [CrossRef]
- Tsampasian V, Elghazaly H, Chattopadhyay R, Debski M, Naing TKP, Garg P, et al. Risk Factors Associated With Post-COVID-19 Condition: A Systematic Review and Meta-analysis. JAMA Intern Med. 2023;183:566-80.
- Perlis RH, Santillana M, Ognyanova K, Safarpour A, Lunz Trujillo K, Simonson MD, et al. Prevalence and Correlates of Long COVID Symptoms Among US Adults. JAMA Netw Open. 2022;5:e2238804. [CrossRef]
- Wu SC, Arthur CM, Jan HM, Garcia-Beltran WF, Patel KR, Rathgeber MF, et al. Blood group A enhances SARS-CoV-2 infection. Blood. 2023;142:742-7.
- Santopaolo M, Gregorova M, Hamilton F, Arnold D, Long A, Lacey A, et al. Prolonged T-cell activation and long COVID symptoms independently associate with severe COVID-19 at 3 months. Elife. 2023;12:e85009. [CrossRef]
- Altmann DM, Whettlock EM, Liu S, Arachchillage DJ, Boyton RJ. The immunology of long COVID. Nat Rev Immunol. 2023:Online ahead of print.
- Moga E, Lynton-Pons E, Domingo P. The Robustness of Cellular Immunity Determines the Fate of SARS-CoV-2 Infection. Front Immunol. 2022;13:904686.
- Nehme M, Vetter P, Chappuis F, Kaiser L, Guessous I, CoviCare Study T. Prevalence of Post-Coronavirus Disease Condition 12 Weeks After Omicron Infection Compared With Negative Controls and Association With Vaccination Status. Clin Infect Dis. 2023;76:1567-75. [CrossRef]
- Watanabe A, Iwagami M, Yasuhara J, Takagi H, Kuno T. Protective effect of COVID-19 vaccination against long COVID syndrome: A systematic review and meta-analysis. Vaccine. 2023;41:1783-90.
- Byambasuren O, Stehlik P, Clark J, Alcorn K, Glasziou P. Effect of covid-19 vaccination on long covid: systematic review. BMJ Medicine. 2023;2. [CrossRef]
- Taquet M, Dercon Q, Harrison PJ. Six-month sequelae of post-vaccination SARS-CoV-2 infection: A retrospective cohort study of 10,024 breakthrough infections. Brain Behav Immun. 2022;103:154-62.
- Kahlert CR, Strahm C, Gusewell S, Cusini A, Brucher A, Goppel S, et al. Post-Acute Sequelae After Severe Acute Respiratory Syndrome Coronavirus 2 Infection by Viral Variant and Vaccination Status: A Multicenter Cross-Sectional Study. Clin Infect Dis. 2023;77:194-202. [CrossRef]
- Wynberg E, Han AX, Boyd A, van Willigen HDG, Verveen A, Lebbink R, et al. The effect of SARS-CoV-2 vaccination on post-acute sequelae of COVID-19 (PASC): A prospective cohort study. Vaccine. 2022;40:4424-31.
- O'Mahoney LL, Routen A, Gillies C, Ekezie W, Welford A, Zhang A, et al. The prevalence and long-term health effects of Long Covid among hospitalised and non-hospitalised populations: A systematic review and meta-analysis. EClinicalMedicine. 2023;55:101762. [CrossRef]
- Richard SA, Pollett SD, Fries AC, Berjohn CM, Maves RC, Lalani T, et al. Persistent COVID-19 Symptoms at 6 Months After Onset and the Role of Vaccination Before or After SARS-CoV-2 Infection. JAMA Netw Open. 2023;6:e2251360.
Figure 1.
Study flowchart.
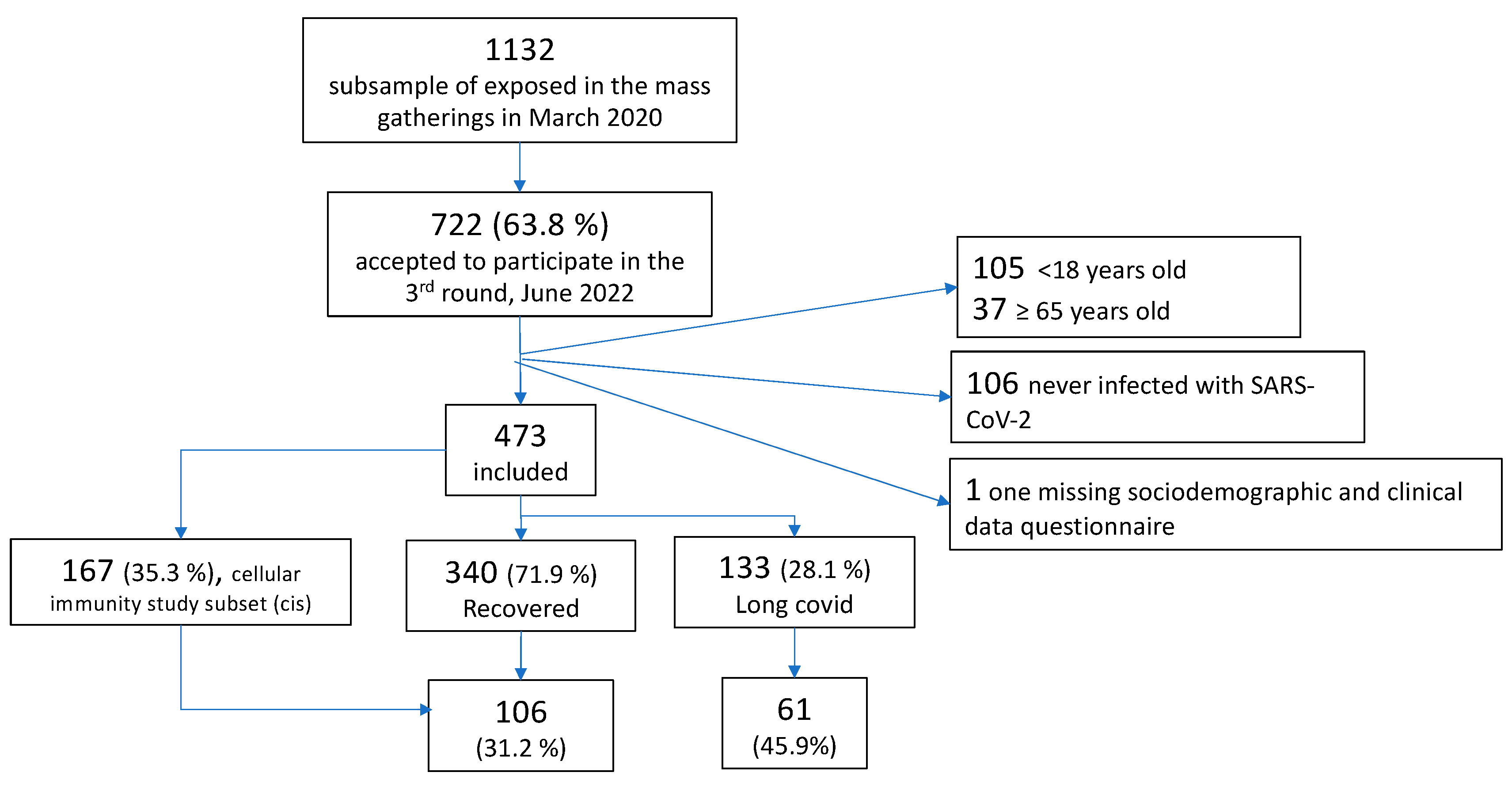
Figure 2.
Timeline of first infection, reinfection, and vaccination (1st, 2nd, and 3rd doses) and VOC circulating periods for subjects included in the third follow-up study, June 2022. Borriana Cohort, 2020-2022.
Figure 2.
Timeline of first infection, reinfection, and vaccination (1st, 2nd, and 3rd doses) and VOC circulating periods for subjects included in the third follow-up study, June 2022. Borriana Cohort, 2020-2022.
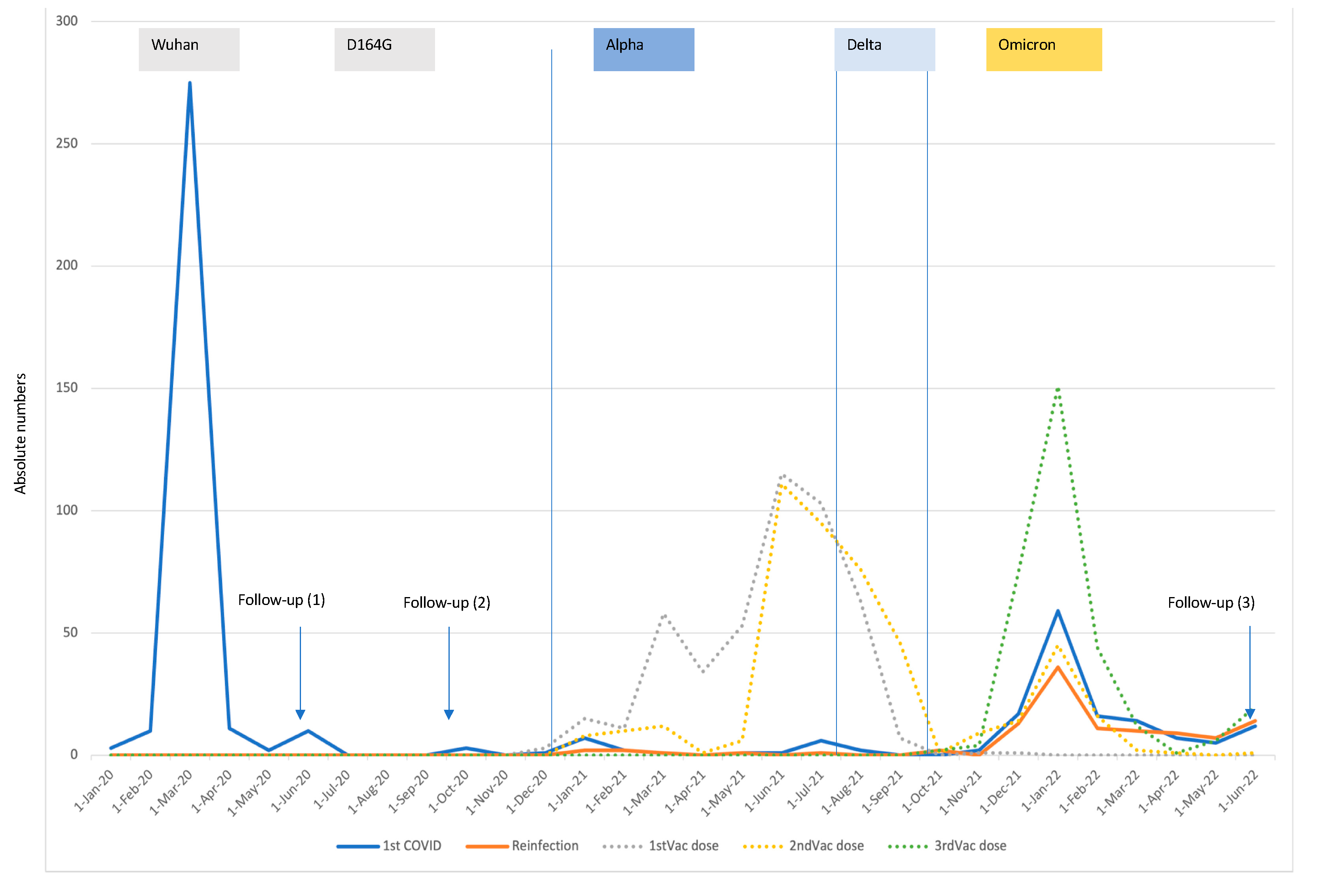
Figure 3.
Symptoms post-COVID and their distribution by long COVID status.
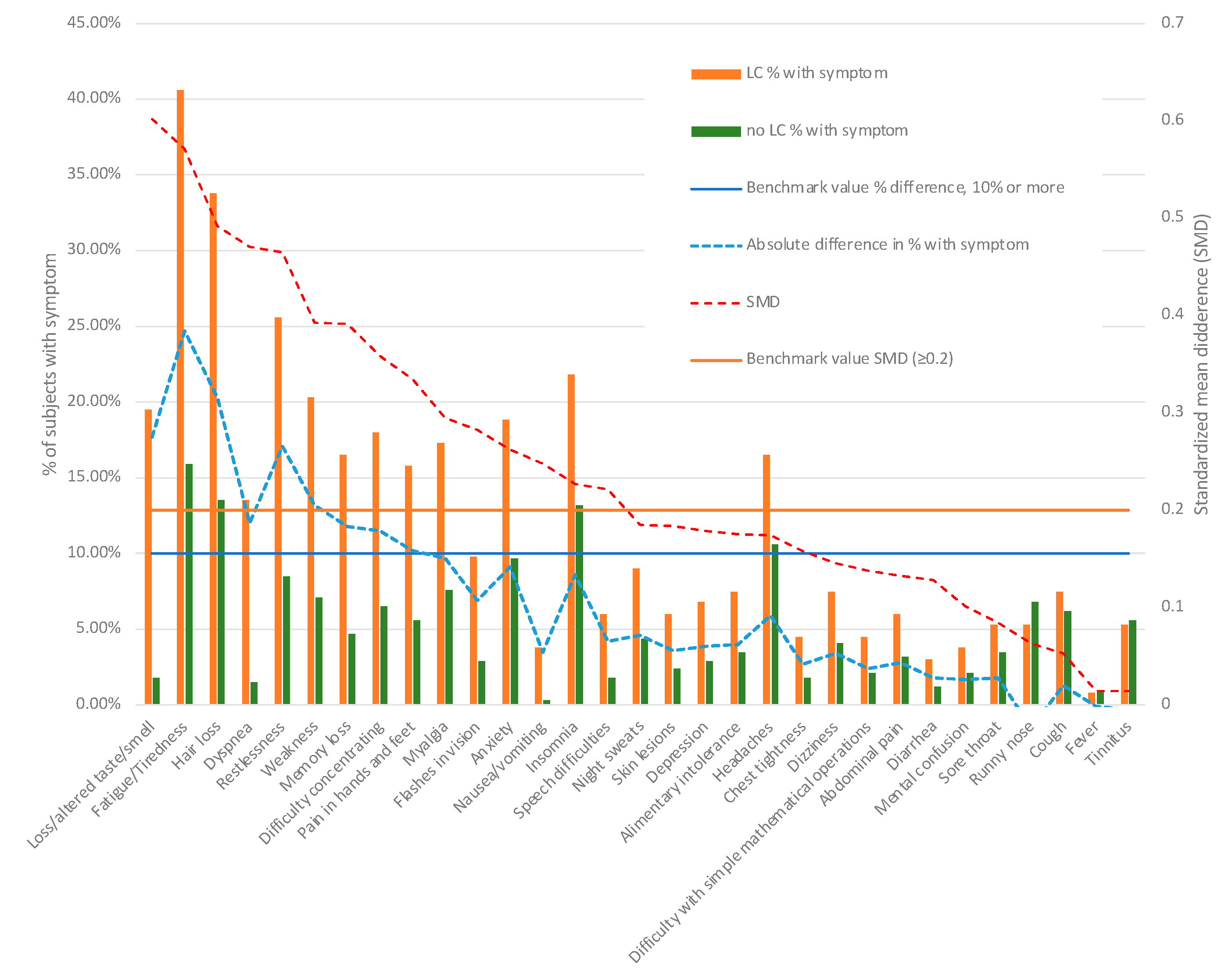

Table 1.
Factors associated with Long COVID.
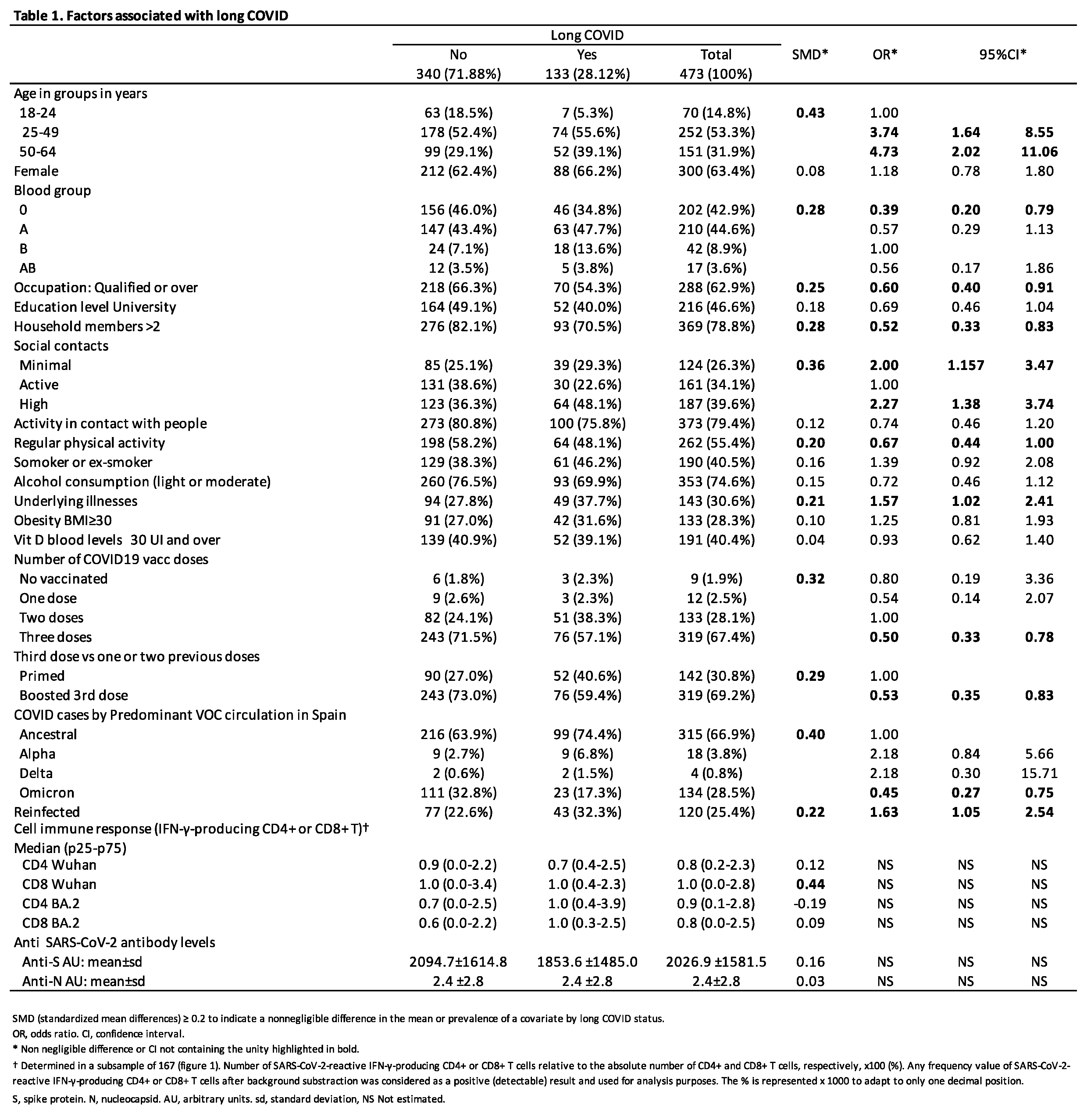 |
Table 2.
Characteristics of SARS-CoV-2 infection and its associated outcomes, both in aggregate and stratified by long COVID status.
Table 2.
Characteristics of SARS-CoV-2 infection and its associated outcomes, both in aggregate and stratified by long COVID status.
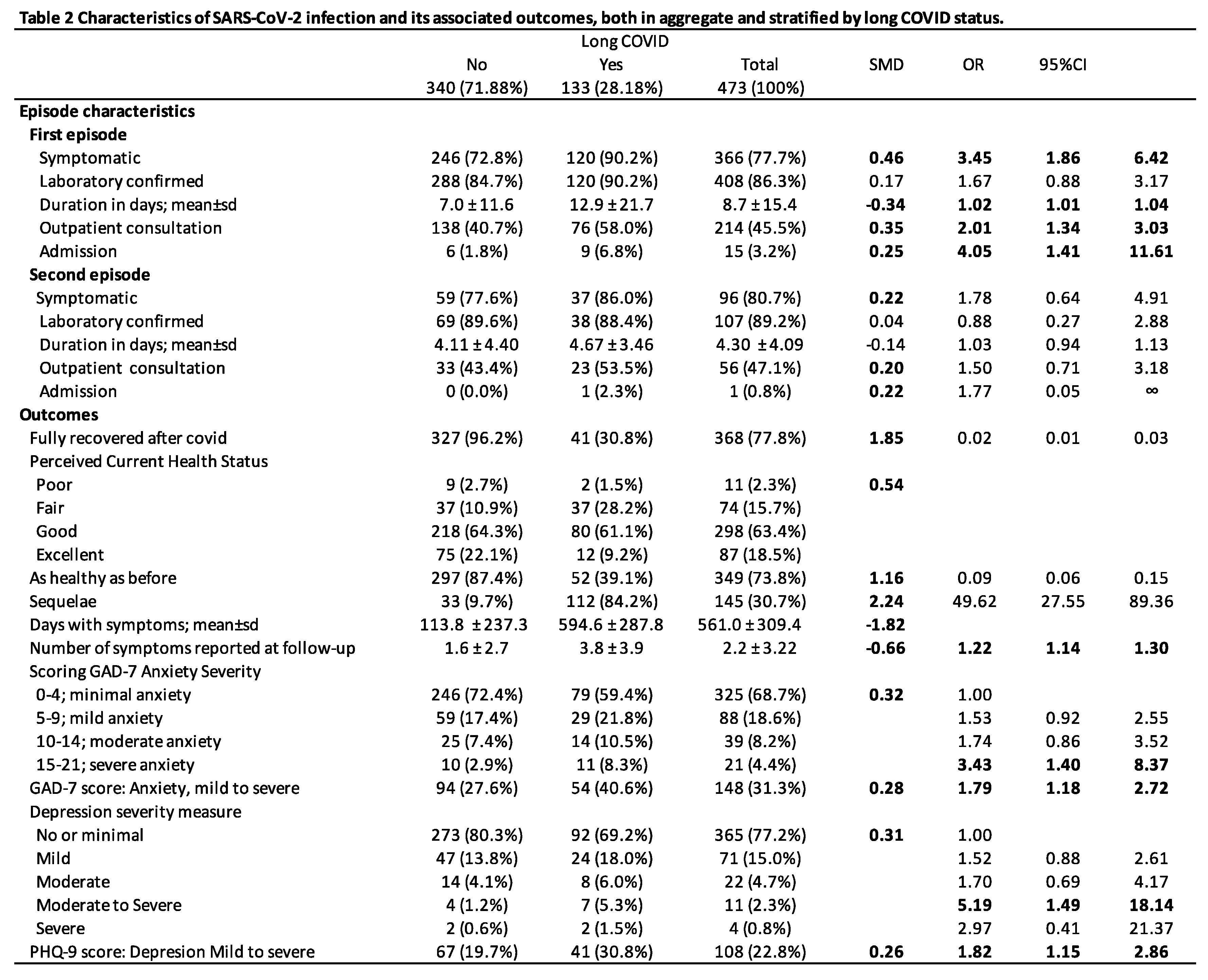 |
Table 3.
Symptoms reported by subjects who met the criteria for long COVID and those who did not.
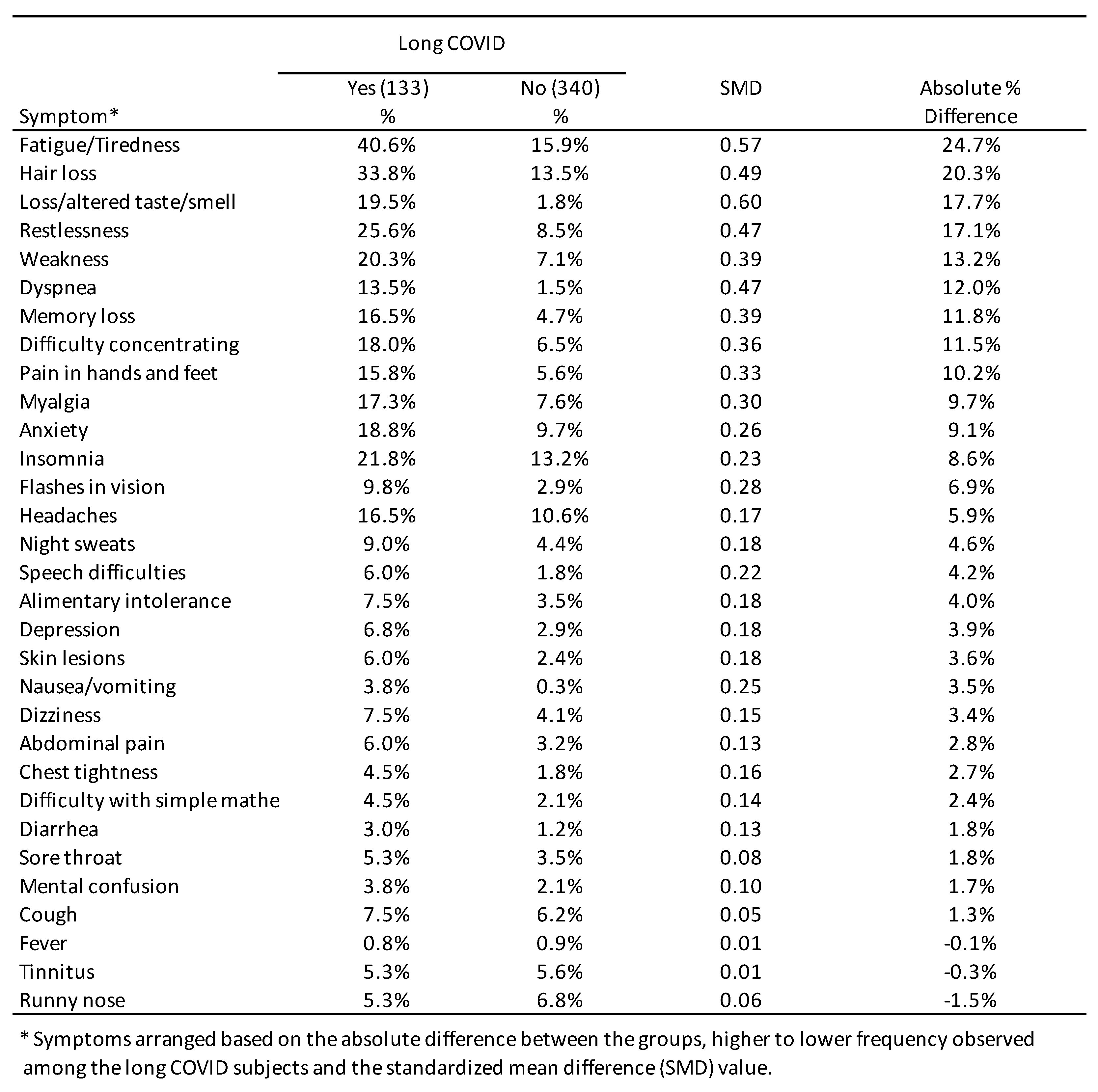 |
Table 4.
Impact of the booster dose on long COVID prevalence and the number of symptoms during the Omicron (vaccine roll out accomplished) and Wuhan (pre-vaccine sensitivity analysis) periods. Borriana Cohort Study, March 2020–June 2022.
Table 4.
Impact of the booster dose on long COVID prevalence and the number of symptoms during the Omicron (vaccine roll out accomplished) and Wuhan (pre-vaccine sensitivity analysis) periods. Borriana Cohort Study, March 2020–June 2022.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



