
Submitted:
31 August 2023
Posted:
01 September 2023
You are already at the latest version
Abstract
The loop and knot securities of 2 braided and 2 monofilament sutures of four diameters (3.0, 2.0, 0, 1) were evaluated with a tensiometer for four 4-throw knots known to be secure with a 2.0 polyfilament suture. Loop security of monocryl 1 is low, being 14.7 + 3.0 Newton (N) for a 3-throw half-knot (H3) and 15.4 + 2.4 N and 28.3+ 10 N for 2 (SSs) and 4-throw (SSsSsSs) symmetrical sliding half-hitches. This is lower than 18, 24, and 46 N for similar knots with vicryl. Polyfilament sutures have excellent knot security for all diameters. Occasionally, some slide to open with slightly lower knot security, especially for larger diameters, although not clinically problematic. Knot se-curity of monofilament sutures was unpredictable for all 4 knots, especially for larger diameters, resulting in many clinically insecure knots. A secure monofilament knot requires a 6-throw knot with 2 symmetrical sliding half-hitches or 2 symmetrical half-knots secured with 4 asymmetric blocking half-hitches. In conclusion, with polyfilament sutures, 4 or 5-throw half-knot or half-hitch sequences result in secure knots. For monofilament sutures, loop and knot security is much less, half-knot combinations should be avoided, and secure knots require 6-throw knots with 4 asym-metric half hitches. This conclusion is valid for gynecologic laparoscopic and open surgery, and for surgery in general.
Keywords:
knot sequences
; half-knots
; half-hitches
; knot rotation
; knot security
; loop security
; laparoscopic surgery
; open surgery
; gynaecological surgery
1. Introduction
Suturing and knot-tying are important skills in surgery. Knot and loop security can be measured with a tensiometer with progressively increasing forces until the suture breaks or slides to open [1-5]. Knot security is the resistance to the opening of a knot, which is needed to keep tissues together after surgery. Loop security is the resistance to opening the first throw of half knots or one or more sliding half hitches. Since laparoscopic surgery does not permit two-hand knot tying, keeping traction on both suture ends as done in open surgery, loop security is essential to keep the edges approximated until the knot is secured or finalised [4,6]. Knot security and loop security vary with the total number of throws and the number, sequence and rotation of half-knots [7] or half-hitches used. Unfortunately, the forces needed for loop and knot security of different tissues in gynaecological and abdominal surgery have been poorly documented. However, common sense suggests that during coughing, forces on the abdominal fascia and on the promontory after promontofixation are much higher than those needed for bowel or vaginal cuff suturing.
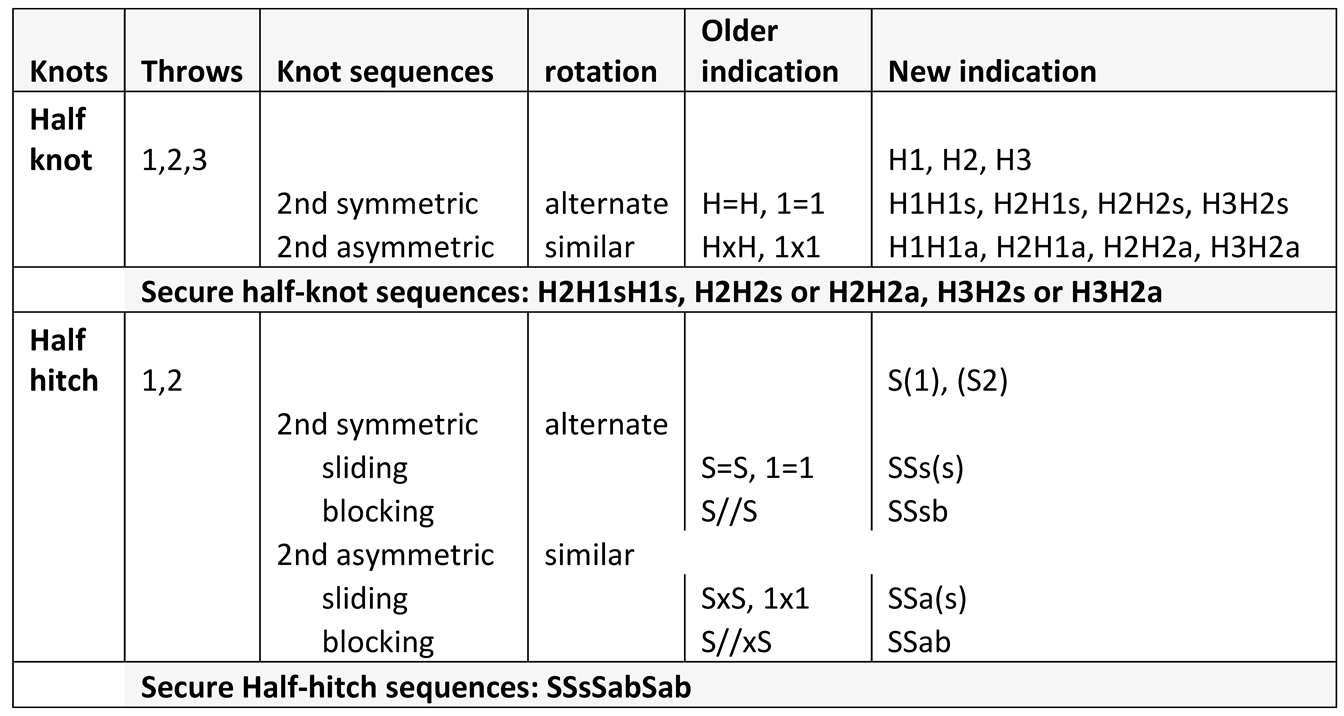
Surgical knots (for an overview [8]) are sequences of half-hitches (S) or half-knots (H) (Table 1), except cinch knots. Half-hitches result from pulling one end of the suture, called the passive end. Half-knots (H) require symmetrical pulling of both ends. Half-hitches generally consist of 1 throw and half-knots of 1 to 3 throws. For half-knots, loop security increases with the number of throws [9]. For half-knots and half-hitches, alternate rotation of the same active end, in comparison with the previous one, improves knot security [4,9-12]. Half-knot sequences with opposite rotation result in a flat square knot, visually recognised as symmetrical in 1 plane [10]. Similarly, half-hitch sequences with opposite rotation remain in one plane and squeeze the passive end symmetrically and firmly. For both half knots and half hitches, changing the active and passive ends has a similar effect on the knot as changing rotation; therefore, for blocking half hitches or with bimanual suturing, similar rotation improves knot security [13]. Secure knots of polyfilament sutures need 4 or 5 throws, such as a 2 or 3-throw half-knot, followed by a 2-throw half knot or the surgical knot (a 2-throw half-knot followed by 2 symmetrical 1-throw half-knots). Secure half-hitch sequences need 2 symmetrical half-hitches followed by 2 asymmetrical blocking half-hitches. For knots such as H2H2 and H3H2 sequences, rotation only marginally affects security, with asymmetrical sequences being slightly better [9,10,14]. A different class of knots are cinch knots [15] or sliding knots that can be blocked when in place by reorganising the knot structure by pulling the active end, such as the Röder knot [16].
During traction, the 3-D reorganisation of the knot structure can occasionally result in lower knot security. This is poorly investigated since at least 40 knots are needed to detect 5% insecure knots [9,10]. Tying forces affect knot security, but most important is the low loop security of a 1 or 2-throw half knot, which is easily destabilised by tissue forces or by little traction on one of the ends of the first loop when making the second half knot, or by not tying the second half-knot perfectly symmetrical. This risk increases when the surgeon is less experienced, the suture ends are short, or knot tying is more difficult because it is deeper or less accessible. Although not investigated, it seems logical that the risk will be less when the loop security is better, such as with a 3-throw half knot. This 3-D reorganisation explains the variable knot security with occasionally dangerous knots when security is less than 5 or 10 N [10].
Knot and loop security is affected by the diameter of the suture and by different sliding and friction characteristics of mono and polyfilament sutures in the tissue and the knot. Since it was poorly documented, we investigated the loop and knot security of 2 polyfilament and 2 monofilament sutures of 4 diameters.
2. Materials and Methods
3.1. Terminology of knots.
Knot classification, tying, and testing were described in detail previously [9,10,14]. Knots are defined by their type, number of throws and rotation: an ‘H’ for half-knots or ‘S’ for half-hitches, followed by the number of throws and the rotation of the active end in comparison with the previous one (‘s’ for symmetric knot resulting from alternate rotation and ‘a’ for asymmetric after similar rotation ). In addition, for half-hitches, an ‘s’ indicates a sliding and ‘b’ is a blocking sequence. However, this terminology can be simplified by omitting in half-hitches, the number of throws if 1, and the s of sliding to avoid confusion with symmetric. Important for surgeons is to realise that changing the active and passive ends, as occurs with bimanual suturing or when transforming a sliding in a blocking half hitch, has the same effect as changing rotation. Thus, SSsSsbSab means a second symmetrical and sliding half-hitch (made by alternate rotation). The third half-hitch is also made by alternate rotation (and therefore called symmetric) but results in an asymmetric blocking half-hitch (lower quality) after changing active and passive ends. ). The third half-hitch was made by similar rotation (and therefore called asymmetric), resulting in a symmetric blocking half-hitch ( stronger) after changing active and passive ends.
This terminology emphasises rotation since this is what the surgeon does. He only has to remember that alternate rotation of the active end is the rule since it results in a symmetric knot sequence superior to the asymmetric knot sequence made by a similar rotation. However, when the active and passive ends are changed to make a blocking half-hitch, he has to start with a similar rotation, resulting in an asymmetric (sliding) half-hitch becoming a symmetric blocking half-hitch after changing the active and passive ends. This is less confusing than the previous terminology (Table 1), describing the final knot sequence as symmetric with’ =‘, asymmetric with ‘x’, and blocking with ‘//’ without mentioning rotation.
3.2. Aim of the Study, Knot Combinations and Power Estimations
This study aimed to investigate the effect of suture diameter (suture sizes) and type suture on loop and knot security. Loop stability is documented only for half knots, and 2 and 4 symmetric and asymmetric half hitches with polyglactin 2.0. Since it is important for secure knots, loop stability was measured for 3-throw half-knots (H3) and 2, 4, or 6 symmetrical half-hitches with a monofilament (Monocryl) suture. In addition, we estimated the loop security of 2 symmetrical half-knots (H1H1s) and for a 2-throw half-hitch (S2) which are sliding with monocryl 1. For knot security, we investigated 4 diameters (3.0, 2.0, 0 and 1) of 2 braided sutures ( vicryl - polyglactin and mersilene - polyethylene terephthalate) and 2 monofilament sutures ( PDS - polydioxane and monocryl- lubricant coated poliglecaprone ) for 4-throw knot sequences considered secure knots with Vicryl, such as SSsSabSab, H2H2a, H2H2s and H2H1sH1s. Because of the high incidence of insecure 4-throw knots with larger monofilament sutures, 5-knot sequences were investigated (Figure 4), such as 3 or 2 sliding with 2 or 3 blocking half hitches (SssSsSabSab and SssSabSabSab), the sliding H1H1s with 3 blocking half-hitches (H1H1sSabSabSab) and the S2 with 3 blocking half-hitches (S2SabSabSab).
All knots were made by the same experienced person (AR) with close supervision of eventual mistakes by IC, and knots were block-randomised for each experiment. Thus, for four groups, 1 knot of each group was made before starting the second series. A factorial design was used with 10 knots for each type of suture.
Institutional review board (IRB) approval was not needed for experiments in vitro not involving humans or animals, as confirmed in writing by the IRB of Leuven University.
3.3. Knot tying and testing
Using Romeo’s gladiator knot-tying technique, standardised laparoscopic knots were made as described [17]. Sutures of 18 cm were tied around a 15-mm plastic tube using the different knot combinations to be evaluated. After knot tying, the suture threads were cut at exactly 10 mm to permit the detection of some sliding. These loops were subsequently mounted on the hooks of a digital dynamometer (Sauter FH 500 capacity 500 NW) and tested at 200 mm/min. With increasing forces, the knot combination slipped to open or blocked, causing the suture to break. The two endpoints thus are breaking or sliding to open and the force (N) at which the knot slips to open or breaks. Testing was done at the Research Educational Centre of Turin University.
3.4. Statistics
Statistical evaluation was done with SAS [18], and means, and SDs are given unless indicated otherwise. A factorial design with 10 knots in each cell and 4 types of sutures, 4 diameters and 4 knots, has a statistical power of 540 knots permitting in addition to evaluate interaction [19]. This was analysed by 2-way analysis of variance for non-Gaussian distributions (proc GLM).
Differences between 2 groups were evaluated with Wilcoxon signed rank test.
3. Results
Loop security of monocryl 1 is low, with large standard deviations indicating variability. Loop security is 2.7 + 1.0 N for H2, 14.7 + 3.0 N for H3, 15.4 + 2.4 N for SSs, 28.3+ 10 N for SSsSsSs, 26.5 + 11.5 N for SSsSsSsSsSs, 9.9 +5.1 N for S2S1 and 17.7 + 6.2 N for H1H1s.
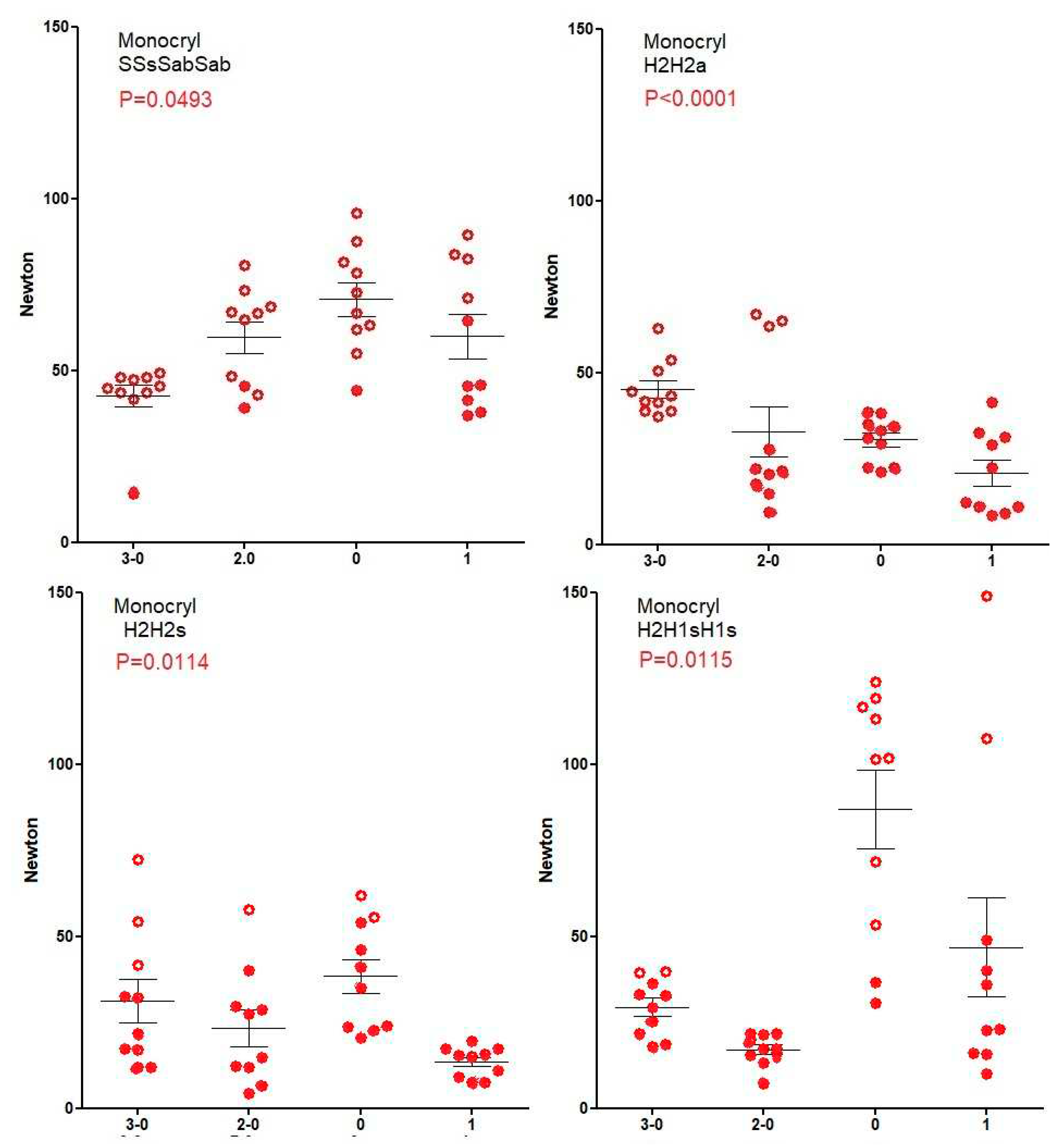
Knot security of vicryl (Figure 1), mersilene (Figure 2) increases (Spearman) with suture diameter for all 4 knots (All p<0.0001) since breaking forces of sutures increase. However, for PDS (Figure 3), knot security only increases with suture diameter for SSsSabSab (P<0.0001), H2H2s (P=0.0128)and H2H1sH1s (P<0.0001) but not for H2H2a (P=0.7). For monocryl (Figure 4), knot security slightly increases only for SSsSabSab (P=0.0493) and H2H1sH1S (P=0.0115) and decreases for H2H2 (P<0.0001) and H2H2s (P=0.0114). This is caused by the unpredictable number of knots sliding to open, being 22% for polyfilament and 51% for monofilament sutures (<0.0001) and increasing when suture diameters are larger (all P=0.0171). However, this increase with diameter is not consistent neither for type of sutures (vicryl P<0.0001, PDS P=0.0003, monocryl P<0.0001, mercilene P=0.67) nor for the knot combination (SSsSabSab P=0.4692, H2H2a P=0.0001, H2H2s P=0.1184, H2H1sH1s P=0.1340). Also, the excellent H3H2a knot with Vicryl results in many insecure knots with monocryl 1 (not shown)
All 2 or 3-way analyses of variance comparing simultaneously knot types, diameter and mono or polyfilament sutures ( n=320) confirmed that knot security increases with the Diameter (P<0.0001) and when polyfilament (P<0.0001) for all knot types. The percentage of knots sliding open also increase with the Diameter (P=0.0124) and when monofilament sutures (P<0.0001). With polyfilament sutures, the security of the 4 knot types was clinically comparable, notwithstanding minor differences (all p<0.0001 except between H2H2s and H2H1sH1s). With monofilament sutures, SSsSabSab was superior to the half-knot combinations for knot security (P<0.0001 but P=0.076 versus H2H1sH1s) with fewer knots sliding to open ( P<0.0001 and P=0.0004 versus H2H1sH1s).
Figure 4.
Knot security of Monocryl. Open circles indicate knots that break and closed circles knots that slide to open. Mean, SEM, and P-values for the correlation of knot security with suture diameter are indicated.
Figure 4.
Knot security of Monocryl. Open circles indicate knots that break and closed circles knots that slide to open. Mean, SEM, and P-values for the correlation of knot security with suture diameter are indicated.
To investigate which knot combinations resulted in reliable monofilament sutures, 5-throw combinations were investigated (Figure 5). Surprisingly all 5-throw combinations with 3 blocking half-hitches were secure irrespective of the base being SSs, H1H1s or S2.is section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
4. Discussion
Surprisingly, after so many years of surgery and more than 30 years after the introduction of the tensiometer, the definitions and our understanding of loop and knot stability are still limited. Traditionally, with open surgery, bimanual knot tying was designed to permit constant traction on both suture ends, thus preventing loop instability and the reliability of the surgical knot (H2H1sH1s) was not questioned. In laparoscopic surgery, loop stability became an issue since bimanual knot tying was no longer possible. Especially the higher forces in orthopaedic, endoscopic surgery needed loop security for tight knots. Research in postoperative adhesion formation pointed to the volume of knots as adhesiogenic. Sutures were improved for tissue reaction, resorption and infection risk, resulting in monofilament, easily sliding sutures with high tensile strength and, more recently, barbed sutures. However, their loop or knot security characteristics for different knot sequences were poorly investigated. Also, the required knot stability for different tissues was poorly addressed. Even the definition of knot stability varied from the mean resistance to opening or breaking to the percentages of sutures breaking without indication of forces. This led to the (erroneous) conclusion that knot security did not vary with the suture diameter [7]. The concept of knot security was challenged with the observations that the surgical knot occasionally resulted in dangerous or insecure knots opening with forces of less than 5 or 30 Newton respectively [9] and that half knots are easily destabilised, resulting in unpredictable reorganisation during knot tying [10]. These observations with 2.0 polyfilament sutures prompted the investigation of monofilament sutures and sutures of a different diameter.
The terminology of knots is confusing since alternative rotation is needed for a symmetric flat square knot, and similar rotation results in a poor asymmetric granny knot. Changing active and passive ends has the same result as changing rotation. This explains that similar rotation, and thus an asymmetric sequence on the passive end, results in a (more secure) symmetric sequence on the new passive end after changing active to passive ends.
Loop security of a monofilament suture, as monocryl 1, is only 15 N for a 3-throw half-knot (H3) and 28N for 4 symmetrical sliding half hitches, which is lower than the 18 N and 45 N for a polyfilament suture. Therefore, when a high loop security is needed, it is suggested to use polyfilament sutures and 3 symmetrical sliding half hitches for monofilament sutures. If loop security is still insufficient, a fourth asymmetrical sliding half-hitch can be added, to be changed into a symmetrical blocking half-hitch by quickly pulling the active end when in place.
For polyfilament sutures, all 4-throw knot types, such as 4 half hitches, two 2-throw half knots and a surgical knot, are secure knots for all diameters. The overall 22% unpredictable behaviour increases with the suture diameter, with knots sliding to open with slightly lower knot security, some less than 50N but without dangerous knots of less than 10N. This confirms previous observations that for vicryl 3.0, 4.0 and 5.0, 5-throws of a flat square are not always secure.
With monofilament sutures, unpredictable behaviour is more frequent, and 51% of knots slide open, especially for larger suture diameters. The best results are obtained with 2 sliding and 2 blocking half hitches, but the knot security is too variable to consider this a secure knot. Monofilament sutures such as PDS and monocryl need at least five throws for a secure knot, confirming previous observations that secure knots often require five throws [9,20]. Surprisingly, three asymmetrical blocking half hitches secure all knots whether the 2-throw base was SSs, S2 or H1H1s.
These observations also confirm that monofilament sutures and half knot combination should be avoided, since with monocryl 1, all H2H2a, H2H2s and H3H2a and H3H2s were insecure or dangerous. This is consistent with the report that 10% of 4-throw half knots (H1H1sH1sH1s) with PDS opened and that even 6 throw half knots (H2H1sH1sH1s H3H2sH1sH1s) were insecure [21].
5. Conclusions
These results confirm [13] the superiority of half hitches in gynaecological surgery. Half hitch sequences are preferred when a high loop security is needed because of the traction of the tissues to be approximated. They not only have higher loop security, but they add flexibility. If the loop security of 2 sliding half-hitches is insufficient, a third symmetrical sliding half-hitch, and if still insufficient, a fourth asymmetrical sliding half-hitch can be added. The latter can, if necessary, be transformed into a blocking half hitch by quickly changing active and passive ends.
Secure knots with polyfilament sutures require at least 4 throws, and H2H1sH1s or H2H2a or H2H2s or SSsSabSab have comparable knot security. Monofilament sutures require at least a 5-throw knot with 3 asymmetrical blocking half hitches for a secure knot. Half-hitches, moreover, risk less being destabilised during knot tying. Therefore, they are the preferred knots in deep gynaecological suturing with the simple rule of alternative rotation for sliding and similar rotation for blocking sequences. These being minimal requirements, it remains a clinical judgment to add an extra half-hitch or half-knot, which is an additional argument for using half hitches instead of half knots.
Author Contributions
AR and PK conceived the experiments, which were performed by AR IC and MG. All authors reviewed, commented and approved the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The IRB board of KULeuven Gasthuisberg confirmed in writing that for experiments not involving human or animal tissues, IRB board approval was not requested.
Informed Consent Statement
Not applicable.
Data Availability Statement
Original data will be made available by simple request to the corresponding author.
Acknowledgments
No acknowledgements.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Thacker, J.G.; Rodeheaver, G.; Moore, J.W.; Kauzlarich, J.J.; Kurtz, L.; Edgerton, M.T.; Edlich, R.F. Mechanical performance of surgical sutures. Am J Surg 1975, 130, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Trimbos, J.B.; Booster, M.; Peters, A.A. Mechanical knot performance of a new generation polydioxanon suture (PDS-2). Acta Obstet Gynecol Scand 1991, 70, 157–159. [Google Scholar] [CrossRef] [PubMed]
- Trimbos, J.B.; Van Rijssel, E.J.; Klopper, P.J. Performance of sliding knots in monofilament and multifilament suture material. Obstet Gynecol 1986, 68, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Trimbos, J.B. Security of various knots commonly used in surgical practice. Obstet Gynecol 1984, 64, 274–280. [Google Scholar] [PubMed]
- Tera, H.; Aberg, C. Tensile strengths of twelve types of knot employed in surgery, using different suture materials. Acta chirurgica Scandinavica 1976, 142, 1–7. [Google Scholar]
- Burkhart, S.S.; Wirth, M.A.; Simonich, M.; Salem, D.; Lanctot, D.; Athanasiou, K. Knot Security in Simple Sliding Knots and Its Relationship to Rotator Cuff Repair: How Secure Must the Knot Be? Arthroscopy: The Journal of Arthroscopic & Related Surgery 2000, 16, 202–207. [Google Scholar] [CrossRef]
- Silver, E.; Wu, R.; Grady, J.; Song, L. Knot Security- How is it Affected by Suture Technique, Material, Size, and Number of Throws? J Oral Maxillofac Surg 2016, 74, 1304–1312. [Google Scholar] [CrossRef]
- Chisnall, RC Analysing knots and ligatures: Tying principles, knot characteristics and structural changes. Forensic Sci Int 2020, 313, 110272. [CrossRef] [PubMed]
- Romeo, A.; Rocha, C.L.; Fernandes, L.F.; Asencio, F.A.; Zomer, M.T.; Fujimoto, C.; Ussia, A.; Wattiez, A.; Koninckx, P.R.; Kondo, W. What is the Best Surgeon’s Knot? Evaluation of the Security of the Different Laparoscopic Knot Combinations. J Minim Invasive Gynecol 2018, 25, 902–911. [Google Scholar] [CrossRef] [PubMed]
- Romeo, A.; Fernandes, L.F.; Cervantes, G.V.; Botchorishvili, R.; Benedetto, C.; Adamyan, L.; Ussia, A.; Wattiez, A.; Kondo, W.; Koninckx, P.R. Which Knots Are Recommended in Laparoscopic Surgery and How to Avoid Insecure Knots. J Minim Invasive Gynecol 2020, 27, 1395–1404. [Google Scholar] [CrossRef] [PubMed]
- Schubert, D.C.; Unger, J.B.; Mukherjee, D.; Perrone, J.F. Mechanical performance of knots using braided and monofilament absorbable sutures. Am J Obstet Gynecol 2002, 187, 1438–1440, discussion 1441-1432. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, N.; Trimbos, J.B. Strength of sliding knots in multifilament resorbable suture materials. Gynecological Surgery 2012, 9, 433–437. [Google Scholar] [CrossRef] [PubMed]
- Romeo, A.; Cipullo, I.; Kondo, W.; Benedetto, C.; Amro, B.; Ussia, A.; Wattiez, A.; Koninckx, P.R. The importance of rotation to teach secure half-hitch sequences in surgery. FVVOG 2023, in press. [Google Scholar]
- Kondo, W.; Zomer, M.T.; Hayashi, R.M.; Fernandes, L.F.; Fujimoto, C.; Romeo, A. Different Blocking Sequences Performed by Laparoscopy. J Minim Invasive Gynecol 2018, 25, 773. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, M.W. Laparoscopic intracorporeal cinch knots: changing the square knot paradigm. J Minim Invasive Gynecol 2012, 19, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Mannu, G.S.; Sudul, M.K.; Bettencourt-Silva, J.H.; Cumber, E.; Li, F.; Clark, A.B.; Loke, Y.K. Closure methods of the appendix stump for complications during laparoscopic appendectomy. Cochrane Database of Systematic Reviews 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Liceaga, A.; Fernandes, L.F.; Romeo, A. Romeo’s gladiator rule: knots, stitches and knot tying techniques. A tutorial based on a few simple rules.; Endopress: Tuttlingen, Germany, 2013. [Google Scholar]
- Inc, SI. SAS; SAS Institute Inc: Cary New York, 2020. [Google Scholar]
- Armitage, P.; Berry, G. Factorial designs. Statistical methods in medical research. 2nd edn ed.; Publications, B.S., Ed.; Blackwell Scientific Publications: Oxford, UK, 1987. [Google Scholar]
- Tidwell, J.E.; Kish, V.L.; Samora, J.B.; Prud’homme, J. Knot security: how many throws does it really take? Orthopedics 2012, 35, e532–537. [Google Scholar] [CrossRef] [PubMed]
- Sanders, R.E.; Kearney, C.M.; Buckley, C.T.; Jenner, F.; Brama, P.A. Knot Security of 5 Metric (USP 2) Sutures: Influence of Knotting Technique, Suture Material, and Incubation Time for 14 and 28 Days in Phosphate Buffered Saline and Inflamed Equine Peritoneal Fluid. Vet Surg 2015, 44, 723–730. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Knot security of vicryl. Open circles indicate knots that break and closed circles knots that slide to open. Mean, SEM, and P-values for the correlation of knot security with suture diameter are indicated.
Figure 1.
Knot security of vicryl. Open circles indicate knots that break and closed circles knots that slide to open. Mean, SEM, and P-values for the correlation of knot security with suture diameter are indicated.
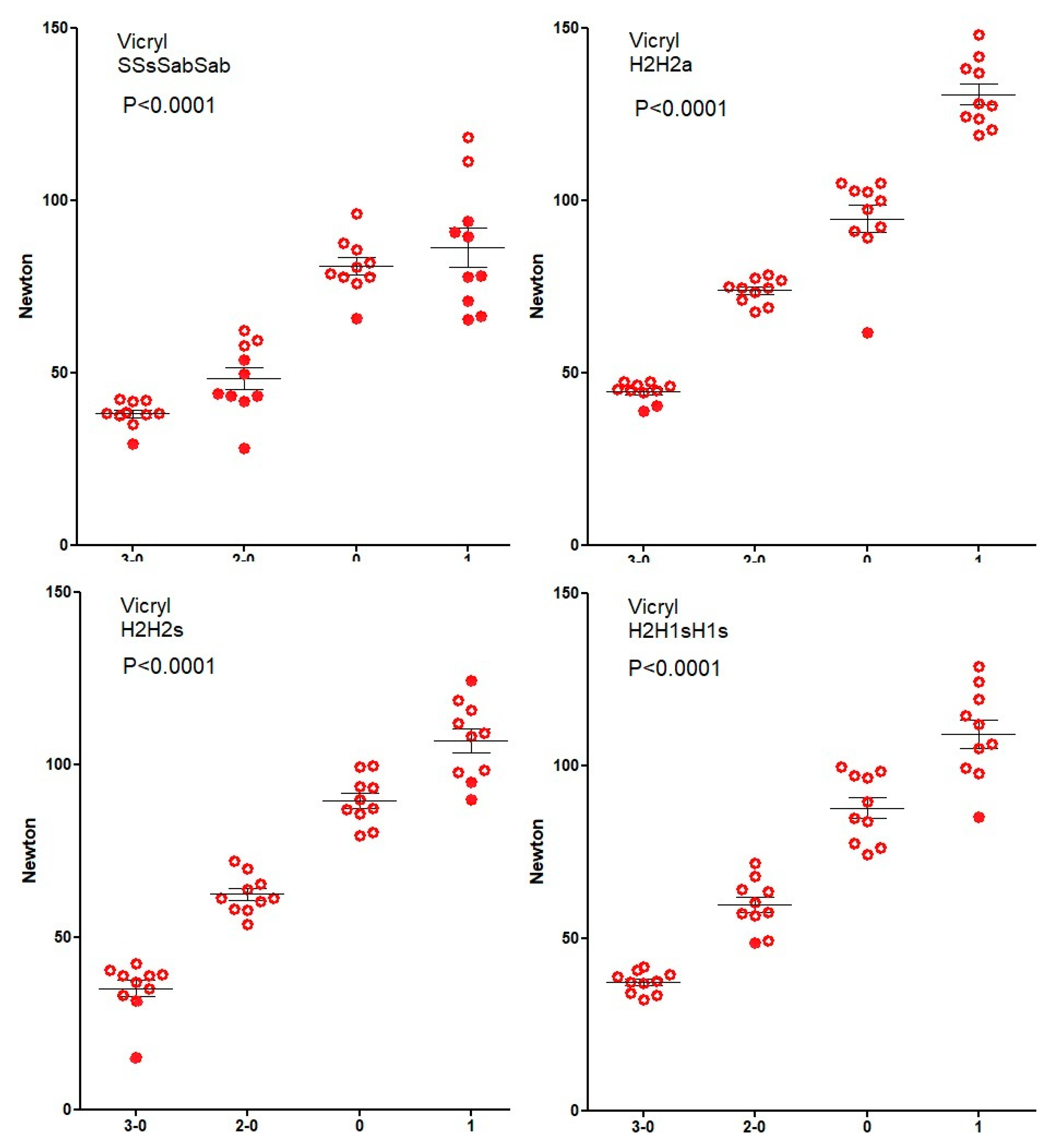
Figure 2.
Knot security of Mersilene. Open circles indicate knots that break and closed circles knots that slide to open. Mean, SEM, and P-values for the correlation of knot security with suture diameter are indicated.
Figure 2.
Knot security of Mersilene. Open circles indicate knots that break and closed circles knots that slide to open. Mean, SEM, and P-values for the correlation of knot security with suture diameter are indicated.
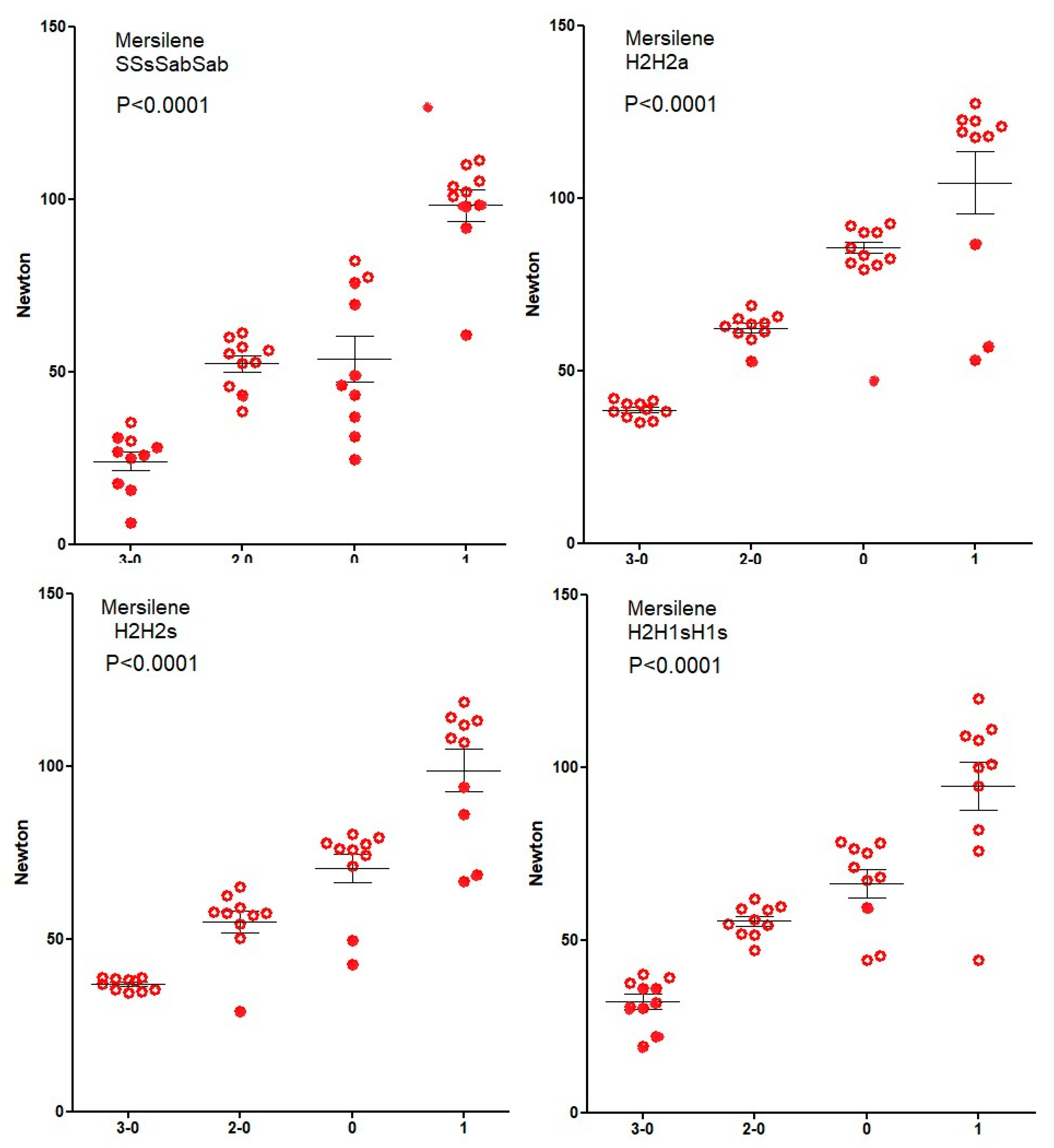
Figure 3.
Knot security of PDS. Open circles indicate knots that break and closed circles knots that slide to open. Mean, SEM, and P-values for the correlation of knot security with suture diameter are indicated.
Figure 3.
Knot security of PDS. Open circles indicate knots that break and closed circles knots that slide to open. Mean, SEM, and P-values for the correlation of knot security with suture diameter are indicated.
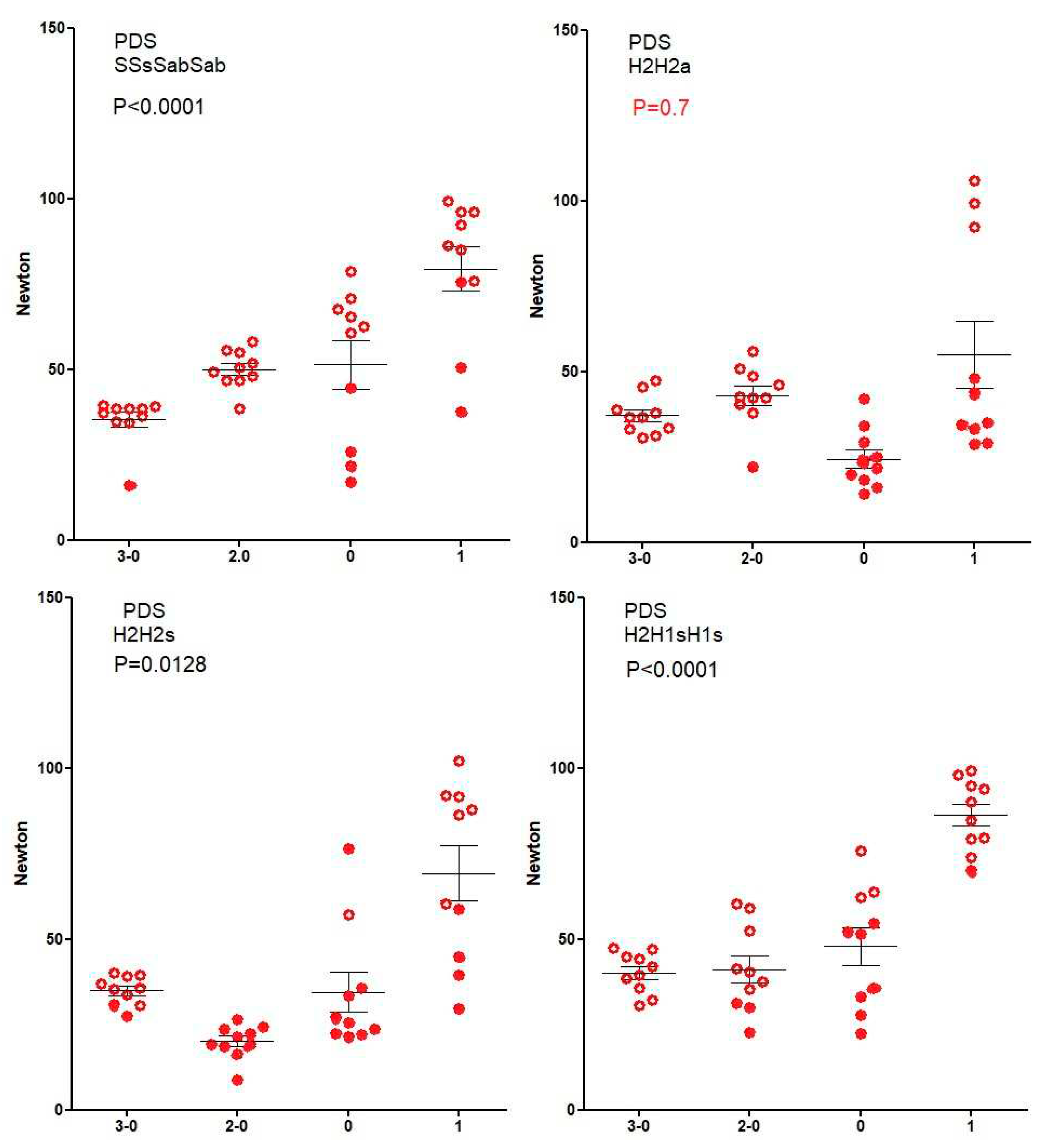
Figure 5.
Knot security of Monocryl 1, for 5-throw knots composed of 3 sliding + 2 blocking, 2 sliding + 3 blocking, and a 2-throw + 3 blocking half-hitches, and an asymmetrical square knot + 3 blocking half hitches.
Figure 5.
Knot security of Monocryl 1, for 5-throw knots composed of 3 sliding + 2 blocking, 2 sliding + 3 blocking, and a 2-throw + 3 blocking half-hitches, and an asymmetrical square knot + 3 blocking half hitches.
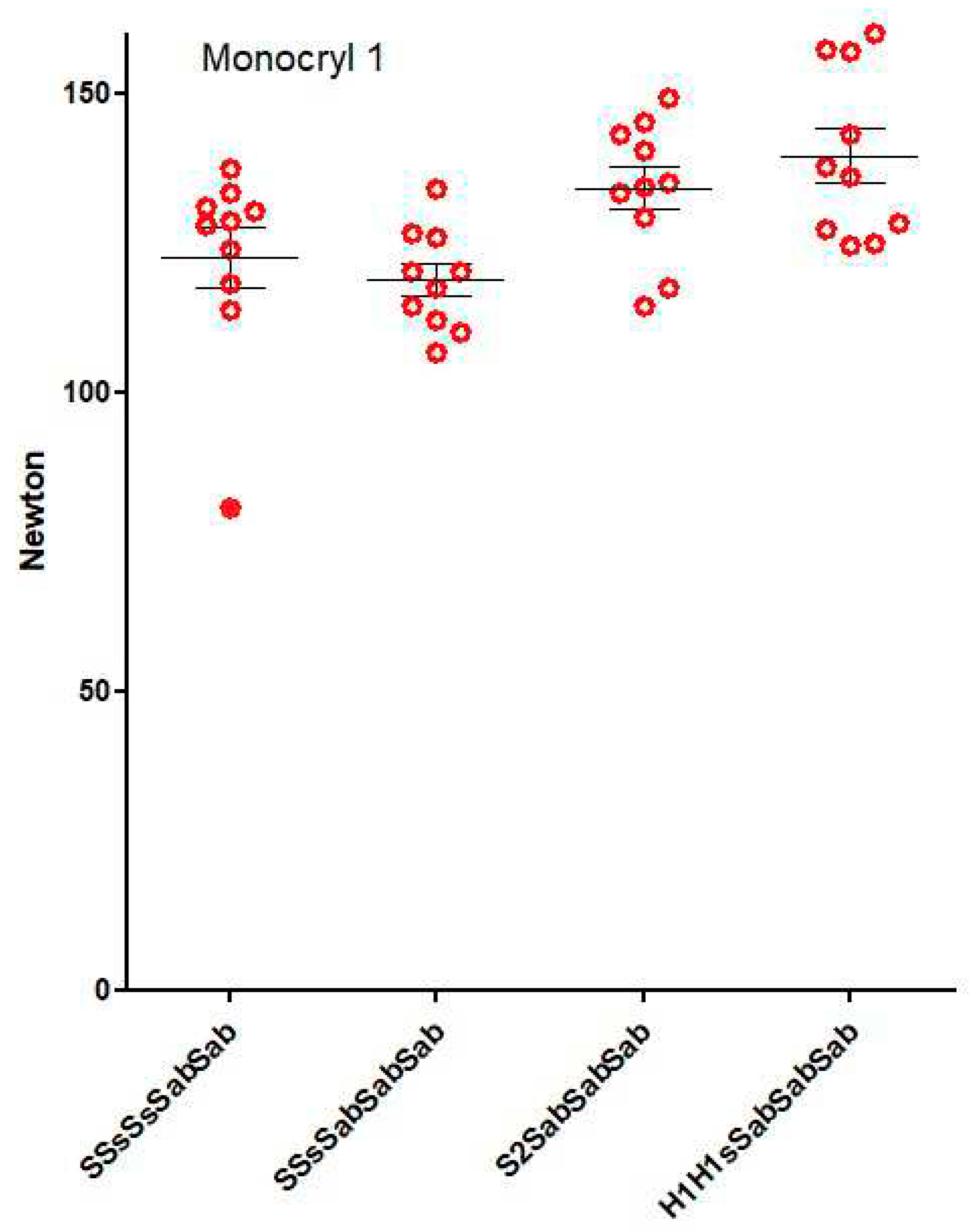

Table 1.
Knot sequences are indicated by their geometry. A flat square knot is symmetric and results
from an alternate rotation of the same active end. A granny knot is asymmetric and results from a
similar rotation of the same active end. Changing the active and passive ends has the same effect as
changing rotation. Knot sequences used to be indicated with = for symmetric (also called identical),
x for asymmetric and // for blocking. We prefer a more intuitive indication, with the type of each
half-knot (H) or hitch (S), followed by the type of knot, using ‘s’ for symmetric (alternate rotation
around the passive end or mono manual suturing) and ‘a’ for asymmetric (similar rotation around
the passive tread). For half-hitches is indicated whether they are sliding (s) or blocking (b) after
changing active and passive ends. For half-hitches, the number of throws is not indicated since
always one, and sliding is not indicated to avoid confusion with the s of symmetric. A 2-throw halfhitch
results from the transformation of a 2-throw half-knot.
Table 1.
Knot sequences are indicated by their geometry. A flat square knot is symmetric and results
from an alternate rotation of the same active end. A granny knot is asymmetric and results from a
similar rotation of the same active end. Changing the active and passive ends has the same effect as
changing rotation. Knot sequences used to be indicated with = for symmetric (also called identical),
x for asymmetric and // for blocking. We prefer a more intuitive indication, with the type of each
half-knot (H) or hitch (S), followed by the type of knot, using ‘s’ for symmetric (alternate rotation
around the passive end or mono manual suturing) and ‘a’ for asymmetric (similar rotation around
the passive tread). For half-hitches is indicated whether they are sliding (s) or blocking (b) after
changing active and passive ends. For half-hitches, the number of throws is not indicated since
always one, and sliding is not indicated to avoid confusion with the s of symmetric. A 2-throw halfhitch
results from the transformation of a 2-throw half-knot.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



