
Submitted:
06 September 2023
Posted:
07 September 2023
You are already at the latest version
Abstract
OPMDs (Oral Potentially Malignant Disorders) are a group of disorders affecting the oral mucosa that are characterized by aberrant cell proliferation and a higher risk of malignant transformation. Vitamin D (VitD) and its receptor (VDR) have been extensively studied for their potential contributions to the prevention and therapeutic management of a range of diseases and neoplastic conditions, including oral cancer. Observational studies suggest correlations between VitD deficiency and higher cancer risk, worse prognosis, and increased mortality rates. Interestingly, emerging data also reveals a link between VitD insufficiency and the onset or progression of OPMDs. Understanding the role of the VitD-VDR axis not only in established oral tumors but also in OPMDs might thus enable early detection and prevention of malignant transformation. With this article, we want to provide an overview of current knowledge about OPMDs and VitD, and investigate their potential association and ramifications for clinical management of OPMDs.
Keywords:
VitD
; VitD receptor
; OPMD
; SCC
; premalignancy
; white lesions
; red lesions
1. Oral potentially malignant disorders
Oral potentially malignant disorders (OPMDs) are a group of conditions characterized by abnormal changes in the oral mucosa that have the potential to progress to oral cancer. These disorders are considered to be a premalignant stage, meaning that if left untreated or unmonitored, they may develop into oral cancer (1). The most recent classification system for OPMDs was proposed by the World Health Organization (WHO) in 2017. This classification system categorizes OPMDs based on their clinical appearance, histological features, and risk of progression to oral cancer (2) (Figure 1). The main categories of OPMDs according to the WHO classification are Oral lichen planus (OLP), Leukoplakia, Proliferative verrucous Leukoplakia (PVL), Erythroplakia (EP), Erythroleukoplakia (ELP), Oral Submucous Fibrosis (OSF), Actinic keratosis (AK), Palatal lesions in reverse smokers, Oral lupus erythematosus (OLE), and Dyskeratosis congenital (DKC) (3).
1.1. Oral Lichen Planus (OLP)
Oral lichen planus (OLP) is distinguished clinically by bilateral white reticular patches on the buccal mucosa, tongue, lip, and gingivae. Despite being a frequent non-infectious oral cavity condition, the actual cause of OLP is still unknown. OLP should be diagnosed based on both clinical and histological features. Specific clinical and histological criteria are used to diagnose lichen planus (4). The occurrence of symmetrical, bilateral, white lesions affecting the buccal mucosa, tongue, lip, and gingiva is one of the clinical criteria. These lesions can take the form of white papular lesions or a lace-like network of slightly elevated white lines arranged in a reticular, annular, or linear pattern (5). Erosions and ulcerations may also be present. OLP may also present itself as desquamative gingivitis in some cases.
Histopathologically, OLP is characterized by hyperkeratosis, acanthosis (epithelium thickening), and a band-like lymphocytic infiltrate in the subepithelial layer. The basal layer may show liquefaction degeneration, where the cells appear rounded and separated from each other. There may also be evidence of vacuolar degeneration of the basal and/or suprabasal cell layers, as well as keratinocyte apoptosis known as civet bodies. Civatte bodies, which are degenerated epithelial cells, may be present also within the inflammatory infiltrate. The inability of epithelial regeneration caused by basal cell loss may cause epithelium thinning and, in rare cases, ulceration in the atrophic variety of lichen planus (4). A mixed inflammatory infiltrate may also be detected. These clinical and histological characteristics aid in effectively diagnosing and distinguishing lichen planus from other comparable disorders (6). A correct diagnosis is required to properly manage and treat the lesion (Figure 1a).
1.2. Leukoplakia
Leukoplakia refers to a white patch or plaque that cannot be scraped off or attributed to any other known cause. Leukoplakia can occur in different forms, such as homogeneous leukoplakia (uniform appearance) and non-homogeneous leukoplakia (speckled or nodular appearance). Leukoplakia is one of the most prevalent and commonly studied OPMDs seen in clinical practice and population surveys (Liu et al., 2019).
Several definitions of leucoplakia have been previously proposed. The WHO Collaborating Centre's definition, issued in 2007, was "A predominantly white plaque of questionable risk having excluded (other) known diseases or disorders that carry no increased risk for cancer" (2). When making a clinical diagnosis of oral Leukoplakia, the following criteria should be considered(7):
- Non-scrapable, primarily white patch/plaque.
- Homogenous Leukoplakia mainly presents itself with well-defined borders (in very few cases, it may present itself with diffuse, ill-defined borders.
- Non-homogeneous Leukoplakia has more diffuse boundaries and may contain red or nodular components in some incidences.
- Excluding the presence of any chronic traumatic irritation to the area (for example, sharp tooth edge, sharp prosthesis, wrong tooth brushing technique or habits).
- Doesn't disappear or improve after elimination of apparent traumatic causes.
- Doesn't disappear or fade away on tissue retraction or stretching (buccal mucous).
- Excluding all other red/white lesions (no other signs and symptoms fitting the presentation of other red/white lesions).
The histological picture of Leukoplakia may vary according to its clinical presentation. Typically, it shows hyperkeratosis, thickening of the surface layer of cells, and acanthosis, which involves the thickening of the underlying epithelium. Atypia and dysplasia may also be observed, including nuclear hyperchromatism, pleomorphism, loss of cellular polarity, increased normal and abnormal mitotic activity, as well as abnormal cellular maturation and individual cell keratinization (8, 9) (Figure 1b).
1.3. Proliferative verrucous Leukoplakia
Proliferative verrucous Leukoplakia (PVL) is a unique and aggressive OPMD. Variable clinical presentations and histological characteristics distinguish it, and it is associated with the highest risk of developing oral cancer compared to other OPMDs. PVL often begins as one or more leukoplakia lesions and spreads to several areas over time when isolated foci merge or adjacent foci combine (10). Due to its aggressive nature, it requires close monitoring, early discovery, and effective management to avoid malignant transformation.
Microscopically, PVL exhibits hyperkeratosis, acanthosis, and dysplastic changes comparable to Leukoplakia. It is mainly distinguished by the verrucous appearance and papillary projections. Severe dysplasia and even squamous cell carcinoma (SCC) may also be encountered (11)(Figure 1c).
1.4. Erythroplakia
Erythroplakia is a separate clinical entity characterized by a primarily red patch on the oral mucosa that cannot be classified clinically or pathologically as any other disease. It is characterized by a red patch or plaque that cannot be attributed to any other known cause (12). It is less common than Leukoplakia but is considered to have a higher risk of progression to oral cancer. Erythroplakia's solitary presentation distinguishes it from other disorders that affect several areas, such as erosive lichen planus, lupus erythematosus, and erythematous candidiasis (2).
Histopathologically, erythroplakia typically shows severe dysplasia and may sometimes even show carcinoma in situ (CIS) or invasive SCC. The epithelial cells exhibit almost all dysplastic criteria, especially cellular atypia, loss of cell maturation, and invasion of the underlying connective tissue in the case of SCC (13) (Figure 1d).
1.5. Erythroleukoplakia
Erythroleukoplakia is a mixed lesion with white and red areas in the same patch or plaque. It carries a higher risk of malignant transformation than leukoplakia/erythroplakia alone. Histologically, it shows mixed features of leucoplakia and Erythroplakia, exhibiting hyperkeratosis, acanthosis, and dysplasia similar to Leukoplakia and frequently demonstrates high dysplastic features suggesting CIS or invasive carcinoma, such as severe cellular atypia, increased mitotic activity, individual cell keratinization as well as loss of typical cell architecture and loss of cell polarity (12) (Figure 1e).
1.6. Oral Submucous Fibrosis (OSF)
Although not strictly categorized as an OPMD, OSF is characterized by the progressive fibrosis of the oral mucosa, leading to restricted mouth opening and potential malignant transformation. It is associated with chewing betel quid, a mixture containing areca nut and other ingredients. It is a well-known potentially malignant oral condition marked by fibrosis of the oral mucosa, including the submucosa (14). In moderate to severe cases, fibrosis can spread to the oropharynx and the upper portion of the esophagus. The accepted definition published by Kerr et al. is a chronic, insidious disease that begins with a loss of fibro-elasticity of the lamina propria. Fibrosis and epithelial atrophy develop in the lamina propria and submucosa of the oral mucosa as the disease advances (15).
Oral Submucous Fibrosis is distinguished clinically by the leathery mucosa, pallor, lack of tongue papillae, petechiae, and, on rare occasions, vesicles. OSF is also characterized by forming fibrous bands in the lips, cheek mucosa, and soft palate, resulting in limited mouth opening. The pathophysiology and clinical presentation of OSF are thought to be influenced by genetic predisposition and family history. The importance of early discovery, intervention, and regular monitoring of OSF in controlling the condition and preventing malignant change cannot be overstated (14).
Histopathological features include sub-epithelial fibrosis and hyalinization (glassy appearance), characterized by the excessive deposition of collagen in the sub-epithelial connective tissue as well as excessive thickening of connective tissue fibers. Other features may also be seen in the epithelium, such as hyperplasia, hyperkeratosis, and even atypia. The underlying connective tissue may occasionally show chronic inflammatory cell infiltration (16) (Figure 1f).
1.7. Actinic keratosis (AK)
Actinic keratosis (AK) or actinic cheilitis is caused by extended exposure to actinic (solar) radiation, most notably ultraviolet rays. It affects exposed regions of the face, most notably the skin and vermilion of the lower lip. The particular locations impacted are critical in clinical evaluation(17). AK is most typically seen in middle-aged, light-skinned males, particularly those who work outdoors. The disorder appears as isolated or generalized lesions with white flaking plaques or scaly patches with red regions intermingled. Less frequently, patients may merely notice lip dryness(18).
Histologically, AK shows epithelial hyperplasia or atrophy, abnormal maturation, varied degrees of ortho-keratinization or para-keratinization, cytological atypia, individual cell keratinization, and increased mitotic activity. The underlying lamina propria frequently demonstrates basophilic collagen degradation, elastosis, vasodilation, and pseudo-acanthosis. Pseudo acanthosis, which arises from the infiltration of abnormal keratinocytes into the underlying connective tissue, can complicate the diagnosis of AK and SCC due to the presence of these cellular clusters in successive sections of the lesions (19) (Figure 1g).
1.8. Nicotinic Stomatitis (Palatal lesion in reverse smokers)
Oral lesions can arise in reverse smoking, a tobacco habit in which the burning end of a cigarette or cigar is retained inside the mouth. Reverse smoking is most common in India, the Caribbean, Latin America, Sardinia, and some Pacific Islands. Except for pipe smokers, reverse smokers have up to 50% of all oral cancers discovered on the hard palate, usually unaffected by other OPMDs (20). It manifests itself clinically as thickened white plaques on the palate, mucosal nodularity, excrescences surrounding the orifices of small palatal mucosal glands, yellowish-brown staining, erythema, and ulceration may also be seen. The lesions might appear as red, white, or mixed red and white patches over a tobacco-stained backdrop (21).
Histopathologically, the epithelium typically shows hyperkeratosis and acanthosis accompanied by squamous metaplasia and hyperplasia of the salivary ducts approaching the surface. The underlying connective tissue and minor salivary glands show chronic inflammatory cell infiltration. Notably, no atypia or dysplasia are encountered in the histopathological picture; hence, the possibility of malignant transformation is minimal, which may vary according to the intensity and duration of exposure to the insult (20) (Figure 1h).
1.9. Oral lupus erythematosus (OLE)
Oral lupus erythematosus (OLE) is a subtype of lupus erythematosus, a chronic autoimmune illness. Oral lesions occur in around 20% of cases with systemic lupus erythematosus. Clinically, OLE is comparable to OLP. OLE generally manifests as a central circular zone of atrophic mucosa surrounded by white striae. The most commonly affected areas are the buccal mucosa, palate, and lips. Malignant changes in OLE lesions are uncommon in the oral cavity (22). Without Systemic symptoms, it may be difficult to distinguish between OLP and OLE intra-orally. Hence, malignancies originating in lupus erythematosus may be misclassified as malignancies arising in OLP. A complete clinical, histological, and systemic evaluation is required to identify and discriminate between the two disorders(23).
Histopathological features include interface dermatitis, characterized by sub-epithelial lymphocytic infiltration. Basal cell degeneration may also be encountered, as well as thickening of the basement membrane. The epithelium may vary in its histopathological presentation according to the clinical presentation, ranging from atrophic to hyperkeratotic changes and hyperplasia (22) (Figure 1i).
1.10. Dyskeratosis congenita (DKC)
Dyskeratosis congenital (DKC), also known as Zinsser-Cole-Engman syndrome, is a rare genetic disorder characterized by telomere disruption. It is regarded as a potentially malignant condition, with affected people having a greater incidence of oral cancer. The disorder usually appears in childhood and should be evaluated and ruled out in children who present with oral Leukoplakia. Attempts have been made to uncover potential markers for future malignant alterations inside DKC patients' oral lesions. In DKC patients, early detection and thorough monitoring of oral lesions are critical for timely intervention and management (24, 25).
Histopathologically, dyskeratosis congenita is characterized by the presence of dyskeratotic cells. These cells exhibit abnormal keratinization and demonstrate premature cell death, resulting in the formation of irregularly shaped keratin-filled bodies within the epithelium (24). Other features may include epithelial atrophy, acanthosis, inflammation, and basal cell layer vacuolization. Additionally, dysplastic changes can occur, ranging from mild to severe, which may indicate an increased risk of malignant transformation. The histopathological findings can vary depending on the disease's stage and severity and may overlap with other OPMDs (26) (Figure 1j).
- 1.
- Preventive measures and treatment options for OPMDs
Identifying effective preventative strategies and treatment options for OPMDs is very critical. Early diagnosis and treatment are crucial and essential because OPMDs can develop malignant changes (oral cancer) if left untreated. Taking proactive actions is becoming necessary to minimize the chances of occurrence of OPMDs or at least arrest their progression by employing effective preventive strategies. First, early detection and treatment can dramatically improve patient outcomes and prevent the development of oral cancer (27). Second, proper OPMD management can aid in the reduction of morbidity and fatality rates linked with oral cancer. It is recommended that healthcare practitioners effectively address risk factors and prevent the development of life-threatening oral cancer by intervening early (28). Third, OPMD prevention/effective treatment choices can decrease discomfort, pain, and functional restrictions, enhancing the overall quality of life for those affected by these problems. Timely management can also help to minimize invasive and lengthy treatment procedures, resulting in better patient experience/satisfaction. Moreover, focusing on preventative measures and early treatment saves money by lowering the burden of oral cancer treatment on healthcare systems and people(27-29).
- 2.
- Physiological Roles of Vitamin D and Vitamin D Receptor
In the last three decades, research on Vitamin D (VitD) has gained close attention and significance, both within and outside the scientific community. VitD was initially described as a fat-soluble vitamin, but currently, it is classified as a circulating pre-hormone. Calcitriol (1,25-dihydroxyVitD3) is the active form of VitD and a potent ligand of the VitD receptors (VDR) (30). VitD possesses crucial physiological functions in the human body(31). It regulates calcium and phosphorus levels in the body, aids in the absorption of these minerals from the intestine, and reduces their excretion from the kidneys, as well as regulating bone turnover and remodeling (32). VitD has attracted considerable interest from researchers and medical professionals due to its extraskeletal influence affecting multiple acute and chronic conditions (33).
The primary actions of VitD are mediated by a nuclear receptor, the VDR. It is involved in many essential cell functions, such as cell signaling, proliferation, apoptosis, and cell cycle(34, 35). VDR is activated by its ligand 1,25(OH)2D3 / Calcitriol. After VDR is stimulated/occupied by its ligand (Calcitriol), the receptor acts as a transcriptional regulator via binding to VitD response elements (VDRE), leading to target gene activation. Calcitriol binding to VDR initiates VDR-RXR dimerization. The ligand-bound VDR-RXR complex then binds to VDRE at multiple regulatory positions of the target gene (30, 36). Moreover, VDR plays a significant role in regulating innate and adaptive immune responses, which is closely related to several OPMDs (37). VDR signaling has been shown to enhance the production and release of anti-inflammatory cytokines, thereby reducing inflammation. VDR activation can also modulate the differentiation and activity of dendritic- and regulatory T-cells, thereby exerting an immunomodulatory effect on the adaptive immune system (38).
Vitamin D exists in two primary forms in the human body: VitD 3 (cholecalciferol) and VitD 2 (ergocalciferol). Among these, VitD 3 is considered the most important form for human health due to its greater bioavailability and superior biological activity compared to VitD 2 (39, 40). Hence, unless explicitly specified otherwise, the reference to VitD pertains to VitD 3. Although both forms undergo the same hydroxylation steps, VitD 2 has a relatively low influence on the total serum 25-OHD level. This may be related to its lower binding affinity to target proteins (41, 42). VitD 2 is obtained in minimal amounts in certain foods. A minimal amount of VitD 2 can also be acquired through foods such as wild mushrooms, beef, and dairy products (31, 43). Its role becomes only significant for subjects taking VitD 2 supplements (41, 42). The human body obtains VitD mainly from two different sources: non-dietary sources (sunlight exposure) and dietary sources. Furthermore, VitD can also be obtained from a third source, pharmacological supplementation (31) ( Figure 2).
The non-dietary source is the first and most important source in which VitD is produced in the skin. The VitD synthesis is a complex process mainly activated by the effect of natural sunlight, specifically ultraviolet B (UVB) radiation (wavelengths from 270 to 315nm) or artificial UVB rays (44, 45). Skin, representing the largest organ in the human body, is the primary location for the conversion of (pro-VitD) into a more active form (pre-VitD) (46, 47). Detailed steps of physiological VitD synthesis are shown in Figure 2 and can be found in more specialized VitD reviews (48, 49).
Besides production in the skin, VitD can also be absorbed via dietary sources. It was assumed that a sufficient supply of VitD could be obtained by consuming VitD-rich foods. However, such foods are not adequately consumed worldwide (to varying degrees) to cover the human body's need for VitD, often resulting in hypovitaminosis (43, 50). Moreover, fatty fish (such as salmon, herring, tuna, and mackerel), eggs, beef, and dairy products are foods high in VitD (31, 43). Different approaches have been implemented to combat hypovitaminosis D. Among all, food fortification is the most commonly implemented method (31, 51).
In addition to dietary sources and cutaneous synthesis via sunlight exposure, pharmacological supplementation is another crucial source of VitD. This method is often employed to effectively and efficiently treat and/or prevent VitD deficiency (52). Therefore, the optimal supplementation dosage has been controversially discussed for a long time. However, it is currently widely accepted that doses of more than 150,000 IU monthly are rarely necessary unless the person has a severe deficit (53, 54). The recommended range for the daily recommended dietary allowance of VitD is 600 to 800 IU (40 IU = 1 µg) (55). Under some circumstances, the recommended daily VitD consumption may be increased to 2000 IU to ensure adequate VitD supply or even 4000 IU in individuals with dark complexion, obesity, or other malabsorption conditions (39, 56).
The biological effects of Calcitriol are not limited to the bone. Calcitriol is also carried bound to DBP to other VDR-positive target tissue, such as the intestine, parathyroid gland, and others. It functions either in a genomic or non-genomic fashion (48). Clinical studies also have been studying the effect of VitD deficiency and supplementation on different acute and chronic diseases as well as cancer mortality (57-60). Interestingly, VitD deficiency is reported to be associated, among others, with infection severity and incidence, inflammatory disease, mental health, metabolism, aging, immunological responses, carcinogenesis, and cancer prognosis (57, 61, 62). VitD regulates a range of host defense mechanisms, including autophagy, apoptosis, cell differentiation, the release of cytokines and chemokines that promote inflammation, and, ultimately, the regulation of oxidative stress (40, 61, 63, 64).
Vitamin D deficiency has a high prevalence worldwide. In Europe, 13.0% or 40.4% of the general population exhibits VitD deficiency or insufficiency, respectively (65). Previous studies have linked VitD deficiency to a higher risk of cancer (66), as well as inflammatory conditions, such as rheumatoid arthritis, inflammatory bowel disease, and multiple sclerosis (67, 68). VitD deficiency has been studied extensively to have a better understanding of its influence on various populations. Research undertaken in several countries has revealed differing insufficiency levels in the general population. According to research, roughly 41% of adults in the United States are VitD deficient, with more significant percentages found in specific ethnic groups such as African Americans and Hispanics(69, 70). Similarly, prevalence rates in European countries ranged from 20% to 50% (65, 71). VitD deficiency is prevalent in older individuals due to age-related decreases in the skin's ability to synthesize VitD and lower dietary intake. According to studies, the incidence of insufficiency in this population might be as high as 70-80% in some areas(72, 73).
Research revealed that individuals are not all equally prone to VitD deficiency; specific groups are at high risk of developing VitD deficiency. Among these groups are individuals with darker skin tones, obesity, limited sun exposure, and individuals suffering from medical conditions that affect VitD metabolism and/or absorption (74). VitD deficiency prevalence varies according to geographic location, season, and individual population features.
- 3.
- Vitamin D and Head and Neck Cancer
Throughout the previous decades, VitD deficiency has been correlated to increased all-cause mortality, acute and chronic inflammatory diseases, cancer, and several autoimmune diseases (58). It has been demonstrated that high doses of Calcitriol can reduce the cancer cell proliferation rate (75, 76). That's why clinical research has been widely studying VitD's relevance in cancer development, prevention, and/or treatment, but unfortunately, the studies' outcomes have been inconsistent. However, the majority of the observational studies confirmed the positive correlation between increased VitD intake and lower cancer risk and/or improved prognosis (77, 78) (79).
In summary, Calcitriol, the active form of VitD, exerts multiple effects on cancer cells by binding to the VDR. The most well-described effects of Calcitriol are its anti-metastatic (80), antiproliferative, pro-differentiation (81), angiogenic, apoptotic, and pro-autophagy action (30, 40, 64). The antiproliferative activity involves cell-cycle arrest in the G0/G1 phase (82), induction of differentiation (81), and promotion of apoptosis (83). Calcitriol achieves these effects through both genomic and non-genomic pathways (78). Calcitriol stimulates gene expression in cell-cycle regulation, such as cyclin-dependent kinase inhibitors (CKIS) and tumor suppressor genes, resulting in G0/G1 cell-cycle arrest (Lo et al., 2022). Calcitriol also enhances apoptosis by inducing the expression of pro-apoptotic proteins, such as BAX, BAK, BAD, and BIM, and suppressing the expression of pro-survival proteins, such as BCL-2 (40) (83). In addition, Calcitriol influences the tumor microenvironment by modulating the activity of immune cells (Wu et al., 2019). It has been shown to suppress the secretion of pro-inflammatory cytokines and chemokines and to promote the differentiation of regulatory T cells, which can eventually suppress the activity of effector T cells (84). It also inhibits the differentiation of hematopoietic progenitor cells by down-regulating the expression of CD40, CD80, and CD86 (85).
Data regarding VitD/VDR's role in head and neck cancer (HNC) are still limited (86). The results of studies examining the effects of VitD levels and/or supplementation on HNC patients' outcomes are controversial. Some showed significant results (87) (88-91) (92, 93) and others failed to show a significant correlation (88, 94, 95). A limited number of studies have investigated the impacts of Vitamin D supplementation on outcomes for cancer patients. However, similarly, the results have also been controversial (96). Lathers et al showed that calcidiol intake reduced the presence of CD34+ immune suppressive cells, hence improving the patients' immune health, eventually affecting the disease prognosis (97). Many clinical studies agreed on the effectiveness of VitD if given at high doses in intermittent intervals. Other studies also recommended combination therapies in VitD to enhance the effect of the partner drug/s (98) (30) (99).
A notable aspect of the studies reviewed is that the majority focused on either VitD status or supplementation or VDR expression/polymorphism without examining both simultaneously in the same patient and correlating them to each other. It should be noted that VitD and VDR are closely interconnected, with VitD being required for VDR activation and VDR being necessary for VitD to exert its effects on cellular processes. Although each of these factors can influence OPMDs and SCC patient outcomes independently, the current literature lacks investigations of their interplay. The efficacy of VitD/calcitriol in the development and treatment of OPMDs and HNSCC remains unclear due to the limited and inconclusive data available. Further investigation is necessary to determine the optimal dosage and feasibility of incorporating VitD / calcitriol into standard treatment regimens.
- 4.
- Vitamin D and OPMDs
Besides the widely discussed functions of VitD/VDR in cancer, researchers have been investigating the link between VitD deficiency and the development of OPMD (100). Indeed, studies on the incidence of VitD insufficiency in people with OPMDs have found a strong correlation between low VitD levels and the development of these oral lesions. Clearly, VitD deficiency is widespread among those diagnosed with OPMDs. This incidence is due to various causes, including insufficient sun exposure, inadequate VitD intake, and underlying medical problems that interfere with its metabolism(1).
One study on leukoplakia patients found that people with low VitD levels had a higher likelihood of developing dysplastic alterations in the oral mucosa, indicating a possible role for VitD deficiency in the malignant transformation of Leukoplakia (101). Another study found a link between VitD deficiency and the severity of oral lichen planus, implying that low VitD levels may contribute to the advancement of this ailment(102). Understanding and resolving the link between VitD supply and OPMDs could have substantial implications for their prevention and clinical management (103). While there is no direct relationship between both, the protective effect of VitD against the development and progression of oral cancer may be correlated to its various biological functions (Figure 3), as discussed in the following.
First, VitD has immunomodulatory properties, influencing both the innate and adaptive immune systems. It has been proposed that maintaining optimal VitD levels may help regulate the immune system's response to precancerous changes in the oral mucosa, potentially reducing the risk of progression to oral cancer (104, 105). VitD receptors are found in the immune system and oral mucosal cells, indicating that VitD directly influences these tissues (104). In the context of OPMDs, optimal VitD levels may help modulate the immune response in the oral mucosa, potentially reducing the risk of progression to oral cancer. Conversely, VitD deficiency decreases immunological function and increases susceptibility to chronic inflammation, encouraging the onset or progression of OPMDs (28).
Secondly, VitD can inhibit the production of pro-inflammatory cytokines, such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-alpha), while promoting the production of anti-inflammatory cytokines like interleukin-10 (IL-10)(106-109). This balance is essential for preventing chronic inflammation, which is associated with cancer development. VitD has anti-inflammatory properties, and thus, by reducing inflammation, VitD may help prevent the progression of OPMDs to oral cancer (110-113).
Furthermore, VitD plays a crucial role in regulating cell proliferation, cell differentiation, and apoptosis. VitD has antiproliferative properties, limiting aberrant cell proliferation and lowering the chance of malignant transformation(1, 103). VitD can inhibit the proliferation of cancer cells, induce cell cycle arrest, and suppress the expression of genes involved in cell growth and survival pathways (114, 115). It can also modulate gene expression through epigenetic mechanisms. VitD has been shown to affect DNA methylation patterns and histone modifications, which can influence gene expression in cancer development and progression(116-118). Proper cell differentiation and apoptosis are essential for maintaining tissue integrity and preventing the accumulation of abnormal cells that can lead to oral cancer (119-122). Here, VitD promotes cell differentiation, favoring a more mature and specialized phenotype. It also induces apoptosis in cells with damaged DNA or other abnormalities. By promoting proper cell differentiation and apoptosis, VitD may help prevent the progression of OPMDs to oral cancer (40, 114, 115). VitD insufficiency has also been linked to an increased risk of oral cancer, highlighting the importance of VitD in OPMDs (40).
- 5.
- Discussion and Conclusions
Pre-clinical and clinical studies can improve our understanding of how premalignant lesions proceed to oral cancer. This input can be used to develop new preventative strategies, novel medicines, and more accurate risk assessment tools for OPMDs, ultimately improving patient outcomes and lowering the global burden of oral cancer. Food fortification and vitamin supplementation, particularly VitD, have emerged as potential strategies for reducing tumor burden and preventing malignant transformation. VitD has been recognized for its ability to increase cellular resistance to malignant transformations and enhance the efficacy of cancer treatments through supplementation. Several research groups investigated the potential link between VitD insufficiency and OPMDs, including Leukoplakia and oral lichen planus. VitD is generally needed for regulating cell proliferation, differentiation, and apoptosis, all of which are necessary for sustaining oral mucosal health.
To summarize, current data support a link between VitD insufficiency and the development or progression of OPMDs. VitD is essential for maintaining oral mucosal health, and its deficiency may contribute to the etiology of several illnesses. While the link between VitD insufficiency and OPMDs is becoming better recognized, further studies are needed to establish a causal relationship and define the appropriate role of VitD supplementation in preventing or treating these lesions. The prevalence of VitD deficiency in people with OPMDs emphasizes the necessity of correcting this nutritional deficiency to prevent and treat these oral diseases. Encouraging outcomes from studies demonstrate reduced inflammation, improved immune response, and decreased tumor growth with VitD supplementation in various cancers. Additional clinical trials are being conducted to investigate the possible therapeutic benefits of VitD supplementation in people with OPMDs. However, further research is needed to define its specific role, optimal dosage, and evidence-based guidelines for OPMD management. VitD supplementation should be used alongside traditional measures and under healthcare professional supervision.
It's important to note that the classification of OPMDs may continue to evolve as our understanding of these conditions improves. The WHO classification provides a framework for diagnosing and managing OPMDs and assessing the risk of malignant transformation(2). Yet, regular monitoring and appropriate interventions are recommended for individuals diagnosed with OPMDs to detect any signs of progression to oral cancer at an early stage.
Although the discussed molecular mechanisms provide insight into the potential relationship between VitD and OPMDs, research in this area is still emerging, and many aspects remain to be fully understood. Further studies are needed not only to elucidate the precise molecular pathways involved but also to identify the best effective treatments for optimizing VitD status in people at risk of OPMDs.
Conclusively, using VitD-based therapies to prevent or cure OPMDs presents both challenges and opportunities. Among the future challenges will be determining an effective and safe supplementation schedule by randomized controlled trials (RCTs) evaluating VitD supplementation as an adjuvant therapy for OPMDs (Figure 4). Individual differences in VitD metabolism and the possibility of VitD toxicity must also be considered. Mechanistic research is also required to identify the particular cellular and molecular pathways by which VitD influences the development and progression of OPMD. Such efforts will help to improve our understanding of the link between VitD and OPMDs, ultimately shaping evidence-based therapeutic guidelines.
Funding
This study was supported by DAAD/TransMed, DFG, Wegener Stiftung, and the Science Support Program of the University Hospital Mainz.
Acknowledgments
The authors would like to thank Sandra Olf for her excellent technical assistance.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Lorini L, Bescós Atín C, Thavaraj S, Müller-Richter U, Alberola Ferranti M, Pamias Romero J, et al. Overview of oral potentially malignant disorders: from risk factors to specific therapies. Cancers. 2021;13(15):3696. [CrossRef]
- Warnakulasuriya S, Kujan O, Aguirre-Urizar JM, Bagan JV, González-Moles M, Kerr AR, et al. Oral potentially malignant disorders: A consensus report from an international seminar on nomenclature and classification, convened by the WHO Collaborating Centre for Oral Cancer. Oral diseases. 2021 Nov;27(8):1862-80. PubMed PMID: 33128420. Epub 2020/11/01. eng. [CrossRef]
- Tilakaratne W, Jayasinghe RD. Oral Potentially Malignant Disorders (OPMDs). Atlas of dermatoses in pigmented skin. 2021:879-902. [CrossRef]
- Rad M, Hashemipoor MA, Mojtahedi A, Zarei MR, Chamani G, Kakoei S, et al. Correlation between clinical and histopathologic diagnoses of oral lichen planus based on modified WHO diagnostic criteria. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 2009;107(6):796-800. [CrossRef]
- Alaraik AF, Sollecito TP, Stoopler ET, Akintoye SO, Bindakhil MA. A Retrospective Pilot Study of the Clinical and Histopathological Features of Oral Lichen Planus: Comparison of the Diagnostic Criteria. 2022.
- Khamis AK, Aboushelib MN, Helal MH. Clinical Management Protocol for Dental Implants Inserted in Patients with Active Lichen Planus. Part II 4-Year Follow-Up. Journal of Prosthodontics. 2019;28(5):519-25. [CrossRef]
- Tovaru S, Costache M, Perlea P, Caramida M, Totan C, Warnakulasuriya S, et al. Oral Leukoplakia: A clinicopathological study and malignant transformation. Oral diseases. 2023;29(4):1454-63. [CrossRef]
- Evren I, Brouns ER, Poell JB, Wils LJ, Brakenhoff RH, Bloemena E, et al. Associations between clinical and histopathological characteristics in oral Leukoplakia. Oral diseases. 2023;29(2):696-706.
- Farah CS. Molecular, genomic and mutational landscape of oral Leukoplakia. Oral diseases. 2021;27(4):803-12. [CrossRef]
- Thompson LD, Fitzpatrick SG, Müller S, Eisenberg E, Upadhyaya JD, Lingen MW, et al. Proliferative verrucous Leukoplakia: an expert consensus guideline for standardized assessment and reporting. Head and neck pathology. 2021;15:572-87. [CrossRef]
- Upadhyaya JD, Fitzpatrick SG, Cohen DM, Bilodeau EA, Bhattacharyya I, Lewis JS, et al. Inter-observer variability in the diagnosis of proliferative verrucous Leukoplakia: clinical implications for oral and maxillofacial surgeon understanding: a collaborative pilot study. Head and Neck Pathology. 2020;14:156-65. [CrossRef]
- Parasuraman L, Bal M, Pai PS. Erythroplakia and erythroleucoplakia. Premalignant Conditions of the Oral Cavity. 2019:87-95.
- Lorenzo-Pouso AI, Lafuente-Ibáñez de Mendoza I, Pérez-Sayáns M, Pérez-Jardón A, Chamorro-Petronacci CM, Blanco-Carrión A, et al. Critical update, systematic review, and meta-analysis of oral erythroplakia as an oral potentially malignant disorder. Journal of Oral Pathology & Medicine. 2022;51(7):585-93.
- Yuwanati M, Ramadoss R, Kudo Y, Ramani P, Senthil Murugan M. Prevalence of oral submucous fibrosis among areca nut chewers: A systematic review and meta-analysis. Oral diseases. 2022. [CrossRef]
- Sarode SC, Gondivkar S, Gadbail A, Sarode GS, Yuwanati M. Oral submucous fibrosis and heterogeneity in outcome measures: a critical viewpoint. Future Oncology. 2021;17(17):2123-6. [CrossRef]
- Motgi AA, Shete MV, Chavan MS, Diwaan NN, Sapkal R, Channe P. Assessment of correlation between clinical staging, functional staging, and histopathological grading of oral submucous fibrosis. Journal of Carcinogenesis. 2021;20. [CrossRef]
- Reinehr CPH, Bakos RM. Actinic keratoses: review of clinical, dermoscopic, and therapeutic aspects. Anais Brasileiros de Dermatologia. 2020;94:637-57. [CrossRef]
- Balcere A, Konrāde-Jilmaza L, Pauliņa LA, Čēma I, Krūmiņa A. Clinical characteristics of actinic keratosis associated with the risk of progression to invasive squamous cell carcinoma: a systematic review. Journal of clinical medicine. 2022;11(19):5899. [CrossRef]
- Heerfordt IM, Poulsen T, Wulf HC. Actinic keratoses contiguous with squamous cell carcinomas are mostly non-hyperkeratotic and with severe dysplasia. Journal of Clinical Pathology. 2022;75(8):560-3. [CrossRef]
- Won J, Clark H. Palatal keratosis associated with reverse (or" backwards") smoking (PKARS). The New Zealand Medical Journal (Online). 2022;135(1562):104-7.
- Slootweg PJ, Merkx TA. Premalignant lesions of the oral cavity. Surgical pathology of the head and neck: CRC Press; 2019. p. 277-94.
- García-Ríos P, Pecci-Lloret MP, Oñate-Sánchez RE. Oral Manifestations of Systemic Lupus Erythematosus: A Systematic Review. International Journal of Environmental Research and Public Health. 2022;19(19):11910. [CrossRef]
- Cardoso IL, Leal F, Regis RC. Systemic lupus erythematosus and implications for the oral cavity. Journal of Medical Care Research and Review. 2020;3(9):444-53. [CrossRef]
- Noto Z, Tomihara K, Furukawa K, Noguchi M. Dyskeratosis congenita associated with Leukoplakia of the tongue. International Journal of Oral and Maxillofacial Surgery. 2016;45(6):760-3. [CrossRef]
- Sinha S, Trivedi V, Krishna A, Rao N. Dyskeratosis congenita-management and review of complications: a case report. Oman Medical Journal. 2013;28(4):281. [CrossRef]
- Moretti S, Spallanzani A, Chiarugi A, Muscarella G, Battini M. Oral carcinoma in a young man: a case of dyskeratosis congenita. Journal of the European Academy of Dermatology and Venereology. 2000;14(2):123-5. [CrossRef]
- Mohan P. Assessment of the feasibility of opportunistic screening for oral potentially malignant disorders and oral cancer at dental colleges in India: a public health initiative from Bengaluru. 2022.
- Kumari P, Debta P, Dixit A. Oral potentially malignant disorders: etiology, pathogenesis, and transformation into oral cancer. Frontiers in pharmacology. 2022;13:825266. [CrossRef]
- Iocca O, Sollecito TP, Alawi F, Weinstein GS, Newman JG, De Virgilio A, et al. Potentially malignant disorders of the oral cavity and oral dysplasia: A systematic review and meta-analysis of malignant transformation rate by subtype. Head & neck. 2020;42(3):539-55. [CrossRef]
- Chen J, Tang Z, Slominski AT, Li W, Żmijewski MA, Liu Y, et al. Vitamin D and its analogs as anticancer and anti-inflammatory agents. European Journal of Medicinal Chemistry. 2020 2020/12/01/;207:112738.
- Janoušek J, Pilařová V, Macáková K, Nomura A, Veiga-Matos J, Silva DDd, et al. Vitamin D: sources, physiological role, biokinetics, deficiency, therapeutic use, toxicity, and overview of analytical methods for detection of vitamin D and its metabolites. Critical Reviews in Clinical Laboratory Sciences. 2022:1-38. [CrossRef]
- Starczak Y, Reinke DC, Barratt KR, Ryan JW, Russell PK, Clarke MV, et al. Absence of vitamin D receptor in mature osteoclasts results in altered osteoclastic activity and bone loss. J Steroid Biochem Mol Biol. 2018 Mar;177:77-82. PubMed PMID: 29107736. [CrossRef]
- Vincent-Chong VK, DeJong H, Attwood K, Hershberger PA, Seshadri M. Pre-clinical Prevention Trial of Calcitriol: Impact of Stage of Intervention and Duration of Treatment on Oral Carcinogenesis. Neoplasia. 2019 Apr;21(4):376-88. PubMed PMID: 30875566. Pubmed Central PMCID: PMC6416727.
- Schweitzer A, Knauer SK, Stauber RH. Nuclear receptors in head and neck cancer: current knowledge and perspectives. International Journal of Cancer. 2010;126(4):801-9. [CrossRef]
- Warwick T, Schulz MH, Gilsbach R, Brandes RP, Seuter S. Nuclear receptor activation shapes spatial genome organization essential for gene expression control: lessons learned from the vitamin D receptor. Nucleic Acids Research. 2022;50(7):3745-63. [CrossRef]
- Haussler MR, Jurutka PW, Mizwicki M, Norman AW. Vitamin D receptor (VDR)-mediated actions of 1α, 25 (OH) 2vitamin D3: genomic and non-genomic mechanisms. Best practice & research Clinical endocrinology & metabolism. 2011;25(4):543-59.
- Carlberg C, Muñoz A. An update on vitamin D signaling and cancer. Seminars in cancer biology. 2020 May 30. PubMed PMID: 32485310. Epub 2020/06/03. eng. [CrossRef]
- Bakke D, Sun J. Ancient nuclear receptor VDR with new functions: microbiome and inflammation. Inflammatory bowel diseases. 2018;24(6):1149-54. [CrossRef]
- Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. The Journal of clinical endocrinology & metabolism. 2011;96(7):1911-30. [CrossRef]
- Khamis A, Gül D, Wandrey M, Lu Q, Knauer SK, Reinhardt C, et al. The Vitamin D Receptor–BIM Axis Overcomes Cisplatin Resistance in Head and Neck Cancer. Cancers. 2022;14(20):5131. [CrossRef]
- Bikle D, Christakos S. New aspects of vitamin D metabolism and action—Addressing the skin as source and target. Nature Reviews Endocrinology. 2020;16(4):234-52. [CrossRef]
- Saponaro F, Saba A, Zucchi R. An update on vitamin D metabolism. International journal of molecular sciences. 2020;21(18):6573.
- Minisola S, Ferrone F, Danese V, Cecchetti V, Pepe J, Cipriani C, et al. Controversies Surrounding Vitamin D: Focus on Supplementation and Cancer. Int J Environ Res Public Health. 2019 Jan 11;16(2). PubMed PMID: 30641860. Pubmed Central PMCID: PMC6352116. [CrossRef]
- Lehmann B, Querings K, Reichrath J. Vitamin D and skin: new aspects for dermatology. Experimental dermatology. 2004;13:11-5. [CrossRef]
- Holick MF. Vitamin D 2, editor: Humana Press; 2010.
- Carlberg C. Nutrigenomics of Vitamin D. Nutrients. 2019 Mar 21;11(3). PubMed PMID: 30901909.
- Deb S, Reeves AA, Lafortune S. Simulation of Physicochemical and Pharmacokinetic Properties of Vitamin D3 and Its Natural Derivatives. Pharmaceuticals (Basel). 2020 Jul 23;13(8). PubMed PMID: 32717896. [CrossRef]
- Lehmann B, Meurer M. Vitamin D metabolism. Dermatologic therapy. 2010;23(1):2-12.
- Bikle DD. Vitamin D: production, metabolism and mechanisms of action. Endotext [Internet]. 2021.
- Niedermaier T, Gredner T, Kuznia S, Schöttker B, Mons U, Lakerveld J, et al. Vitamin D food fortification in European countries: the underused potential to prevent cancer deaths. European Journal of Epidemiology. 2022;37(4):309-20. [CrossRef]
- Dunlop E, Kiely M, James AP, Singh T, Black LJ. The efficacy of vitamin D food fortification and biofortification in children and adults: a systematic review protocol. JBI Evidence Synthesis. 2020;Online First. PubMed PMID: 02174543-900000000-99831. [CrossRef]
- Moslemi E, Musazadeh V, Kavyani Z, Naghsh N, Shoura SMS, Dehghan P. Efficacy of vitamin D supplementation as an adjunct therapy for improving inflammatory and oxidative stress biomarkers: An umbrella meta-analysis. Pharmacological Research. 2022:106484. [CrossRef]
- Bouillon R, Gomez JMQ. Comparison of calcifediol with vitamin D for prevention or cure of vitamin D deficiency. The Journal of Steroid Biochemistry and Molecular Biology. 2023:106248. [CrossRef]
- Giustina A, Bouillon R, Dawson-Hughes B, Ebeling PR, Lazaretti-Castro M, Lips P, et al. Vitamin D in the older population: a consensus statement. Endocrine. 2023;79(1):31-44. [CrossRef]
- Gandini S, Boniol M, Haukka J, Byrnes G, Cox B, Sneyd MJ, et al. Meta-analysis of observational studies of serum 25-hydroxyvitamin D levels and colorectal, breast and prostate cancer and colorectal adenoma. Int J Cancer. 2011 Mar 15;128(6):1414-24. PubMed PMID: 20473927. Epub 2010/05/18. eng. [CrossRef]
- Billington EO, Burt LA, Rose MS, Davison EM, Gaudet S, Kan M, et al. Safety of high-dose vitamin D supplementation: secondary analysis of a randomized controlled trial. The Journal of Clinical Endocrinology & Metabolism. 2020;105(4):1261-73. [CrossRef]
- Farrell C-J, Herrmann M. Determination of vitamin D and its metabolites. Best practice & research Clinical endocrinology & metabolism. 2013;27(5):675-88.
- Bouillon R, Marcocci C, Carmeliet G, Bikle D, White JH, Dawson-Hughes B, et al. Skeletal and extraskeletal actions of vitamin D: current evidence and outstanding questions. Endocrine reviews. 2019;40(4):1109-51. [CrossRef]
- Heath AK, Kim IY, Hodge AM, English DR, Muller DC. Vitamin D Status and Mortality: A Systematic Review of Observational Studies. Int J Environ Res Public Health. 2019 Jan 29;16(3). PubMed PMID: 30700025. Pubmed Central PMCID: PMC6388383. [CrossRef]
- Migliaccio S, Di Nisio A, Magno S, Romano F, Barrea L, Colao AM, et al. Vitamin D deficiency: a potential risk factor for cancer in obesity? International Journal of Obesity. 2022 2022/04/01;46(4):707-17.
- Sîrbe C, Rednic S, Grama A, Pop TL. An Update on the Effects of Vitamin D on the Immune System and Autoimmune Diseases. International Journal of Molecular Sciences. 2022;23(17):9784. PubMed PMID: doi:10.3390/ijms23179784. [CrossRef]
- Filipe Rosa L, Petersen PP, Görtz LF, Stolzer I, Kaden-Volynets V, Günther C, et al. Vitamin A-and D-Deficient Diets Disrupt Intestinal Antimicrobial Peptide Defense Involving Wnt and STAT5 Signaling Pathways in Mice. Nutrients. 2023;15(2):376. [CrossRef]
- Shahrajabian MH, Cheng Q, Sun W. Vitamin C and D Supplements to Prevent the Risk of COVID-19. The Natural Products Journal. 2023;13(1):47-59. [CrossRef]
- Koll L, Gül D, Elnouaem MI, Raslan H, Ramadan OR, Knauer SK, et al. Exploiting Vitamin D Receptor and Its Ligands to Target Squamous Cell Carcinomas of the Head and Neck. International Journal of Molecular Sciences. 2023;24(5):4675. [CrossRef]
- Cashman KD, Dowling KG, Škrabáková Z, Gonzalez-Gross M, Valtueña J, De Henauw S, et al. Vitamin D deficiency in Europe: pandemic? The American journal of clinical nutrition. 2016;103(4):1033-44.
- Feldman D, Krishnan AV, Swami S, Giovannucci E, Feldman BJ. The role of vitamin D in reducing cancer risk and progression. Nature reviews cancer. 2014;14(5):342-57. [CrossRef]
- Bouillon R, Manousaki D, Rosen C, Trajanoska K, Rivadeneira F, Richards JB. The health effects of vitamin D supplementation: evidence from human studies. Nature Reviews Endocrinology. 2022 2022/02/01;18(2):96-110. [CrossRef]
- Tuna S, Aydin MA, Aydin MF. The Four Horsemen of the Apocalypse: Cancer, Depression, Vitamin D Deficiency, and Obesity: An Observational Study. Disease Markers. 2023;2023.
- Ginde AA, Liu MC, Camargo CA. Demographic differences and trends of vitamin D insufficiency in the US population, 1988-2004. Archives of internal medicine. 2009;169(6):626-32. [CrossRef]
- Looker AC, Johnson CL, Lacher DA, Pfeiffer CM, Schleicher RL, Sempos CT. Vitamin D status: United states, 2001–2006. NCHS data brief. 2011;59(59):1-8.
- Hagenau T, Vest R, Gissel T, Poulsen C, Erlandsen M, Mosekilde L, et al. Global vitamin D levels in relation to age, gender, skin pigmentation and latitude: an ecologic meta-regression analysis. Osteoporosis international. 2009;20:133-40. [CrossRef]
- Bischoff-Ferrari HA, Conzelmann M, Stähelin H, Dick W, Carpenter M, Adkin AL, et al. Is fall prevention by vitamin D mediated by a change in postural or dynamic balance? Osteoporosis international. 2006;17:656-63.
- Hilger J, Friedel A, Herr R, Rausch T, Roos F, Wahl DA, et al. A systematic review of vitamin D status in populations worldwide. British journal of nutrition. 2014;111(1):23-45. [CrossRef]
- Holick MF. Vitamin D deficiency. New England journal of medicine. 2007;357(3):266-81.
- Wietrzyk J, Milczarek M, Kutner A. The effect of combined treatment on head and neck human cancer cell lines with novel analogs of Calcitriol and cytostatics. Oncology research. 2007;16(11):517-25. PubMed PMID: 18306931. Epub 2008/03/01. eng. [CrossRef]
- Martinez-Reza I, Diaz L, Barrera D, Segovia-Mendoza M, Pedraza-Sanchez S, Soca-Chafre G, et al. Calcitriol Inhibits the Proliferation of Triple-Negative Breast Cancer Cells through a Mechanism Involving the Pro-inflammatory Cytokines IL-1beta and TNF-alpha. Journal of immunology research. 2019;2019:6384278. PubMed PMID: 31093512. Pubmed Central PMCID: PMC6481021. Epub 2019/05/17. eng.
- Garland CF, Gorham ED, Mohr SB, Garland FC. Vitamin D for cancer prevention: global perspective. Annals of epidemiology. 2009 Jul;19(7):468-83. PubMed PMID: 19523595. Epub 2009/06/16. eng. [CrossRef]
- Muñoz A, Grant WB. Vitamin D and cancer: an historical overview of the epidemiology and mechanisms. Nutrients. 2022;14(7):1448. [CrossRef]
- Hernández-Alonso P, Boughanem H, Canudas S, Becerra-Tomás N, Fernández de la Puente M, Babio N, et al. Circulating vitamin D levels and colorectal cancer risk: A meta-analysis and systematic review of case-control and prospective cohort studies. Critical Reviews in Food Science and Nutrition. 2023;63(1):1-17.
- Brozyna AA, Hoffman RM, Slominski AT. Relevance of Vitamin D in Melanoma Development, Progression and Therapy. Anticancer Res. 2020 Jan;40(1):473-89. PubMed PMID: 31892603. Pubmed Central PMCID: PMC6948187. [CrossRef]
- Carlberg C, Velleuer E. Vitamin D and the risk for cancer: A molecular analysis. Biochemical pharmacology. 2022;196:114735. [CrossRef]
- Lo CS-C, Kiang KM-Y, Leung GK-K. Anti-tumor effects of vitamin D in glioblastoma: Mechanism and therapeutic implications. Laboratory Investigation. 2022;102(2):118-25. [CrossRef]
- Virtanen JK, Nurmi T, Aro A, Bertone-Johnson ER, Hyppönen E, Kröger H, et al. Vitamin D supplementation and prevention of cardiovascular disease and cancer in the Finnish Vitamin D Trial: a randomized controlled trial. The American journal of clinical nutrition. 2022;115(5):1300-10. [CrossRef]
- Valdés-López JF, Velilla P, Urcuqui-Inchima S. Vitamin D modulates the expression of Toll-like receptors and pro-inflammatory cytokines without affecting Chikungunya virus replication, in monocytes and macrophages. Acta Tropica. 2022;232:106497. [CrossRef]
- Ali AJM, Hamoud MJM. Estimation the Relationship Between Vitamin D and Some Immune Parameters Among Patients with Graves' Disease. Pakistan Journal of Medical & Health Sciences. 2022;16(05):854-. [CrossRef]
- Henn M, Martin-Gorgojo V, Martin-Moreno JM. Vitamin D in Cancer Prevention: Gaps in Current Knowledge and Room for Hope. Nutrients. 2022;14(21):4512. [CrossRef]
- Gugatschka M, Kiesler K, Obermayer-Pietsch B, Groselj-Strele A, Griesbacher A, Friedrich G. Vitamin D status is associated with disease-free survival and overall survival time in patients with squamous cell carcinoma of the upper aerodigestive tract. European archives of oto-rhino-laryngology. 2011;268:1201-4. [CrossRef]
- Orell–Kotikangas H, Schwab U, Österlund P, Saarilahti K, Mäkitie O, Mäkitie AA. High prevalence of vitamin D insufficiency in patients with head and neck cancer at diagnosis. Head & neck. 2012;34(10):1450-5. [CrossRef]
- Afzal S, Bojesen SE, Nordestgaard BG. Low plasma 25-hydroxyvitamin D and risk of tobacco-related cancer. Clinical chemistry. 2013;59(5):771-80. [CrossRef]
- Fanidi A, Muller DC, Midttun Ø, Ueland PM, Vollset SE, Relton C, et al. Circulating vitamin D in relation to cancer incidence and survival of the head and neck and oesophagus in the EPIC cohort. Scientific reports. 2016;6(1):36017. [CrossRef]
- Mostafa BE-D, Abdelmageed HM, El-Begermy MM, Taha MS, Hamdy TA-E, Omran A, et al. Value of vitamin D assessment in patients with head and neck squamous cell cancer before treatment. The Egyptian Journal of Otolaryngology. 2016;32:279-86. [CrossRef]
- Bochen F, Balensiefer B, Körner S, Bittenbring JT, Neumann F, Koch A, et al. Vitamin D deficiency in head and neck cancer patients–prevalence, prognostic value and impact on immune function. Oncoimmunology. 2018;7(9):e1476817.
- Nejatinamini S, Debenham BJ, Clugston RD, Mawani A, Parliament M, Wismer WV, et al. Poor Vitamin Status is Associated with Skeletal Muscle Loss and Mucositis in Head and Neck Cancer Patients. Nutrients. 2018 Sep 5;10(9). PubMed PMID: 30189611. Pubmed Central PMCID: PMC6165496. Epub 2018/09/08. eng. [CrossRef]
- Arem H, Weinstein SJ, Horst RL, Virtamo J, Yu K, Albanes D, et al. Serum 25-Hydroxyvitamin D and Risk of Oropharynx and Larynx Cancers in Finnish MenVitamin D and Head and Neck Cancers. Cancer epidemiology, biomarkers & prevention. 2011;20(6):1178-84.
- Skaaby T, Husemoen LLN, Thuesen BH, Pisinger C, Jørgensen T, Roswall N, et al. Prospective Population-Based Study of the Association between Serum 25-Hydroxyvitamin-D Levels and the Incidence of Specific Types of CancerVitamin D and Cancer Incidence. Cancer epidemiology, biomarkers & prevention. 2014;23(7):1220-9.
- Akutsu T, Kitamura H, Himeiwa S, Kitada S, Akasu T, Urashima M. Vitamin D and Cancer Survival: Does Vitamin D Supplementation Improve the Survival of Patients with Cancer? Current oncology reports. 2020 2020/06/04;22(6):62.
- Lathers DM, Clark JI, Achille NJ, Young MRI. Phase IB study of 25-hydroxyvitamin D3 treatment to diminish suppressor cells in head and neck cancer patients. Human immunology. 2001;62(11):1282-93. [CrossRef]
- Grimm M, Cetindis M, Biegner T, Lehman M, Munz A, Teriete P, et al. Serum vitamin D levels of patients with oral squamous cell carcinoma (OSCC) and expression of vitamin D receptor in oral precancerous lesions and OSCC. Medicina oral, patologia oral y cirugia bucal. 2015;20(2):e188. [CrossRef]
- Jolliffe DA, Holt H, Greenig M, Talaei M, Perdek N, Pfeffer P, et al. Effect of a test-and-treat approach to vitamin D supplementation on risk of all cause acute respiratory tract infection and covid-19: phase 3 randomised controlled trial (CORONAVIT). BMJ. 2022;378:e071230. [CrossRef]
- Maturana-Ramírez A, Aitken-Saavedra J, Guevara-Benítez AL, Espinoza-Santander I. Hypovitaminosis D, oral potentially malignant disorders, and oral squamous cell carcinoma: a systematic review. Med Oral Patol Oral Cir Bucal. 2022 Mar 1;27(2):e135-e41. PubMed PMID: 35218642. Pubmed Central PMCID: PMC8898584. Epub 2022/02/27. eng.
- Shukla A, Mehrotra D. Oral Potentially Malignant Disorders. Fundamentals of Oral and Maxillofacial Surgery-E-Book. 2020:313.
- Gupta J, Aggarwal A, Asadullah M, Khan MH, Agrawal N, Khwaja KJ. Vitamin D in the treatment of oral lichen planus: A pilot clinical study. Journal of Indian Academy of Oral Medicine and Radiology. 2019;31(3):222-7. [CrossRef]
- Grimm M, Cetindis M, Biegner T, Lehman M, Munz A, Teriete P, et al. Serum vitamin D levels of patients with oral squamous cell carcinoma (OSCC) and expression of vitamin D receptor in oral precancerous lesions and OSCC. Med Oral Patol Oral Cir Bucal. 2015 Mar 1;20(2):e188-95. PubMed PMID: 25662556. Pubmed Central PMCID: PMC4393981 interest exist. Epub 2015/02/11. eng. [CrossRef]
- McMahon L, Schwartz K, Yilmaz O, Brown E, Ryan LK, Diamond G. Vitamin D-mediated induction of innate immunity in gingival epithelial cells. Infection and immunity. 2011;79(6):2250-6. [CrossRef]
- Walsh JE, Clark A-M, Day TA, Gillespie MB, Young MRI. Use of α, 25-dihydroxyvitamin D3 treatment to stimulate immune infiltration into head and neck squamous cell carcinoma. Human immunology. 2010;71(7):659-65. [CrossRef]
- Sakyi SA, Owusu-Yeboah M, Obirikorang C, Dadzie Ephraim RK, Kwarteng A, Opoku S, et al. Profiling vitamin D, its mediators and pro-inflammatory cytokines in rheumatoid arthritis: A case–control study. Immunity, Inflammation and Disease. 2022;10(8):e676.
- Halim C, Mirza AF, Sari MI. The Association between TNF-α, IL-6, and Vitamin D Levels and COVID-19 Severity and Mortality: A Systematic Review and Meta-Analysis. Pathogens (Basel, Switzerland). 2022 Feb 1;11(2). PubMed PMID: 35215138. Pubmed Central PMCID: PMC8879207. Epub 2022/02/27. eng. [CrossRef]
- Bayraktar N, Turan H, Bayraktar M, Ozturk A, Erdoğdu H. Analysis of serum cytokine and protective vitamin D levels in severe cases of COVID-19. Journal of medical virology. 2022 Jan;94(1):154-60. PubMed PMID: 34427934. Pubmed Central PMCID: PMC8661791. Epub 2021/08/25. eng. [CrossRef]
- Giulietti A, van Etten E, Overbergh L, Stoffels K, Bouillon R, Mathieu C. Monocytes from type 2 diabetic patients have a pro-inflammatory profile: 1, 25-Dihydroxyvitamin D3 works as anti-inflammatory. Diabetes research and clinical practice. 2007;77(1):47-57. [CrossRef]
- Gwenzi T, Zhu A, Schrotz-King P, Schöttker B, Hoffmeister M, Brenner H. Effects of vitamin D supplementation on inflammatory response in patients with cancer and precancerous lesions: Systematic review and meta-analysis of randomized trials. Clinical nutrition (Edinburgh, Scotland). 2023 Jul;42(7):1142-50. PubMed PMID: 37244755. Epub 2023/05/28. eng. https://doi.org/10.1016/j.clnu.2023.05.009. [CrossRef]
- McLachlan CS. The angiotensin-converting enzyme 2 (ACE2) receptor in the prevention and treatment of COVID-19 are distinctly different paradigms. Clin Hypertens. 2020;26:14. PubMed PMID: 32685191. Pubmed Central PMCID: PMC7360378. https://doi.org/10.1186/s40885-020-00147-x. [CrossRef]
- Zhang YG, Lu R, Xia Y, Zhou D, Petrof E, Claud EC, et al. Lack of Vitamin D Receptor Leads to Hyperfunction of Claudin-2 in Intestinal Inflammatory Responses. Inflamm Bowel Dis. 2019 Jan 1;25(1):97-110. PubMed PMID: 30289450. Pubmed Central PMCID: PMC6290786. https://doi.org/10.1093/ibd/izy292. [CrossRef]
- Krishnan AV, Feldman D. Mechanisms of the anti-cancer and anti-inflammatory actions of vitamin D. Annual review of pharmacology and toxicology. 2011;51:311-36. PubMed PMID: 20936945. Epub 2010/10/13. eng. [CrossRef]
- Fernández-Barral A, Bustamante-Madrid P, Ferrer-Mayorga G, Barbáchano A, Larriba MJ, Muñoz A. Vitamin D Effects on Cell Differentiation and Stemness in Cancer. Cancers (Basel). 2020 Aug 25;12(9). PubMed PMID: 32854355. Pubmed Central PMCID: PMC7563562. Epub 2020/08/29. eng. [CrossRef]
- Samuel S, Sitrin MD. Vitamin D's role in cell proliferation and differentiation. Nutrition Reviews. 2008;66(suppl_2):S116-S24.
- Hendi NN, Nemer G. Epigenetic regulation of vitamin D deficiency. Future Medicine; 2023. [CrossRef]
- Snegarova V, Naydenova D. Vitamin D: a Review of its Effects on Epigenetics and Gene Regulation. Folia Med (Plovdiv). 2020 Dec 31;62(4):662-7. PubMed PMID: 33415918. Epub 2021/01/09. eng. [CrossRef]
- Fetahu IS, Höbaus J, Kállay E. Vitamin D and the epigenome. Frontiers in physiology. 2014;5:164. [CrossRef]
- Skrajnowska D, Bobrowska-Korczak B. Potential Molecular Mechanisms of the Anti-cancer Activity of Vitamin D. Anticancer Res. 2019 Jul;39(7):3353-63. PubMed PMID: 31262856. Epub 2019/07/03. eng. [CrossRef]
- Diaz L, Diaz-Munoz M, Garcia-Gaytan AC, Mendez I. Mechanistic Effects of Calcitriol in Cancer Biology. Nutrients. 2015 Jun 19;7(6):5020-50. PubMed PMID: 26102214. Pubmed Central PMCID: PMC4488829. [CrossRef]
- Vuolo L, Di Somma C, Faggiano A, Colao A. Vitamin D and cancer. Front Endocrinol (Lausanne). 2012;3:58. PubMed PMID: 22649423. Pubmed Central PMCID: PMC3355893.
- Zhang J, Yang S, Xu B, Wang T, Zheng Y, Liu F, et al. p62 functions as an oncogene in colorectal cancer through inhibiting apoptosis and promoting cell proliferation by interacting with the vitamin D receptor. Cell Prolif. 2019 May;52(3):e12585. PubMed PMID: 30793399. Pubmed Central PMCID: PMC6536406. [CrossRef]
Figure 1.
Overview of oral potentially malignant disorders. Histopathological illustration depicting various oral potentially malignant disorders and highlighting the potential sequelae of malignant transformation.
Figure 1.
Overview of oral potentially malignant disorders. Histopathological illustration depicting various oral potentially malignant disorders and highlighting the potential sequelae of malignant transformation.
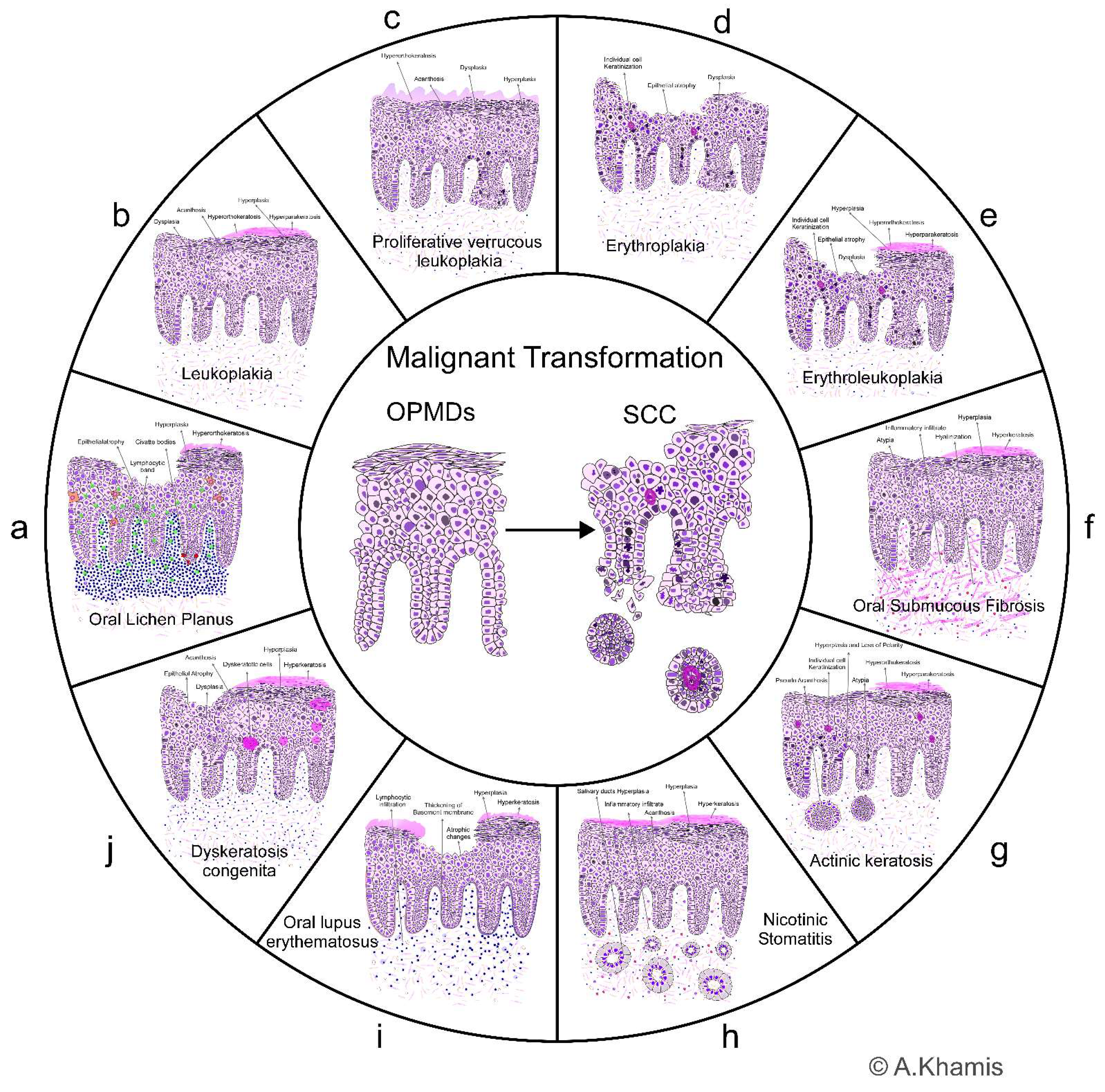
Figure 2.
Vitamin D Metabolism. Schematic illustration representing the successive stages involved in VitD production and activation within the human body, as well as the metabolic pathways responsible for VitD utilization.
Figure 2.
Vitamin D Metabolism. Schematic illustration representing the successive stages involved in VitD production and activation within the human body, as well as the metabolic pathways responsible for VitD utilization.
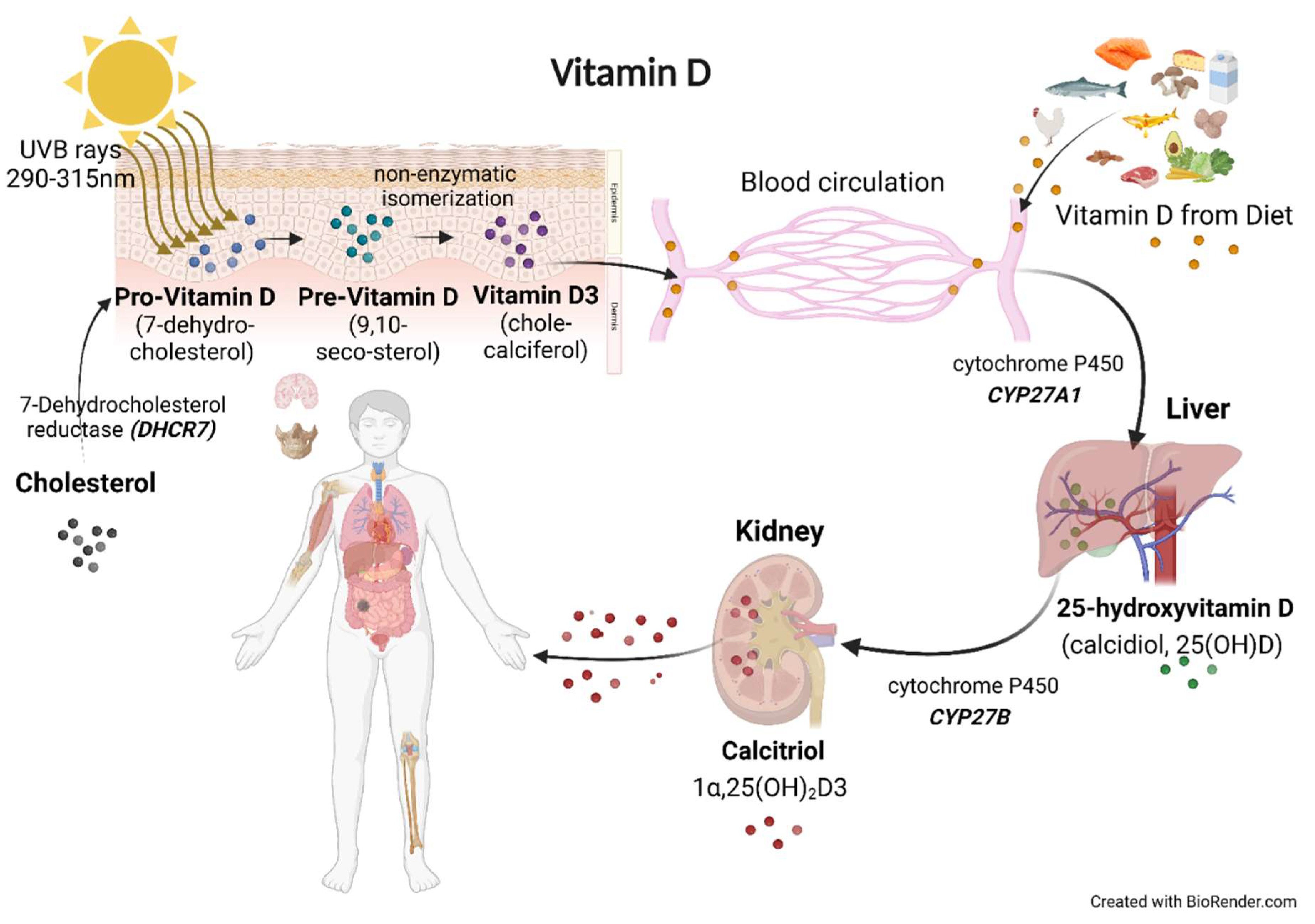
Figure 3.
Sequela of Oral Potentially Malignant Disorders (OPMDs) and the Influence of Vitamin D on Lesion Progression. Illustration depicting the potential consequences of Oral Potentially Malignant Disorders (OPMDs) and highlighting the biological functions of VitD that influence the progression of oral lesions. “+” indicates induction/enhancement, “-“ inhibition/decrease by VitD.
Figure 3.
Sequela of Oral Potentially Malignant Disorders (OPMDs) and the Influence of Vitamin D on Lesion Progression. Illustration depicting the potential consequences of Oral Potentially Malignant Disorders (OPMDs) and highlighting the biological functions of VitD that influence the progression of oral lesions. “+” indicates induction/enhancement, “-“ inhibition/decrease by VitD.
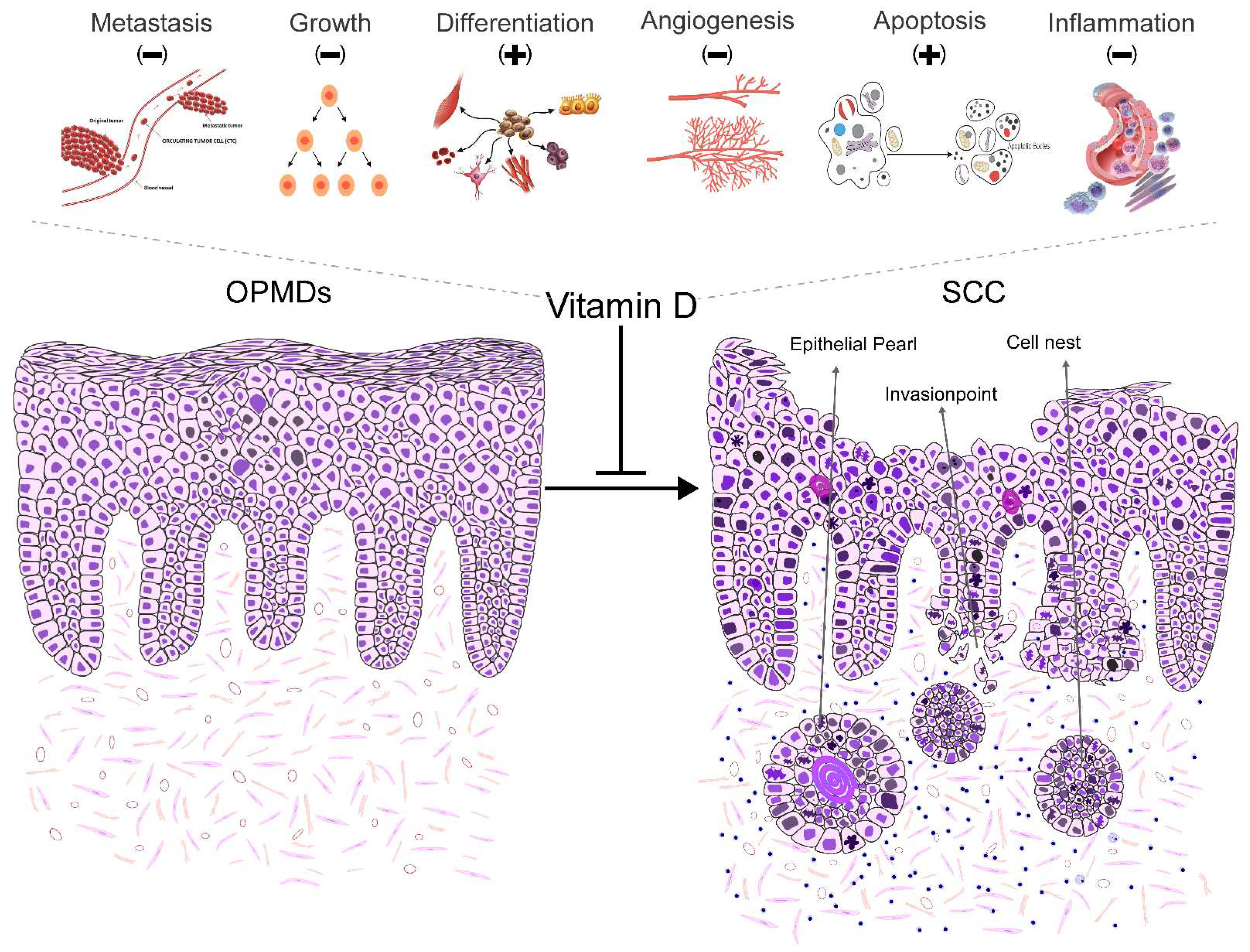
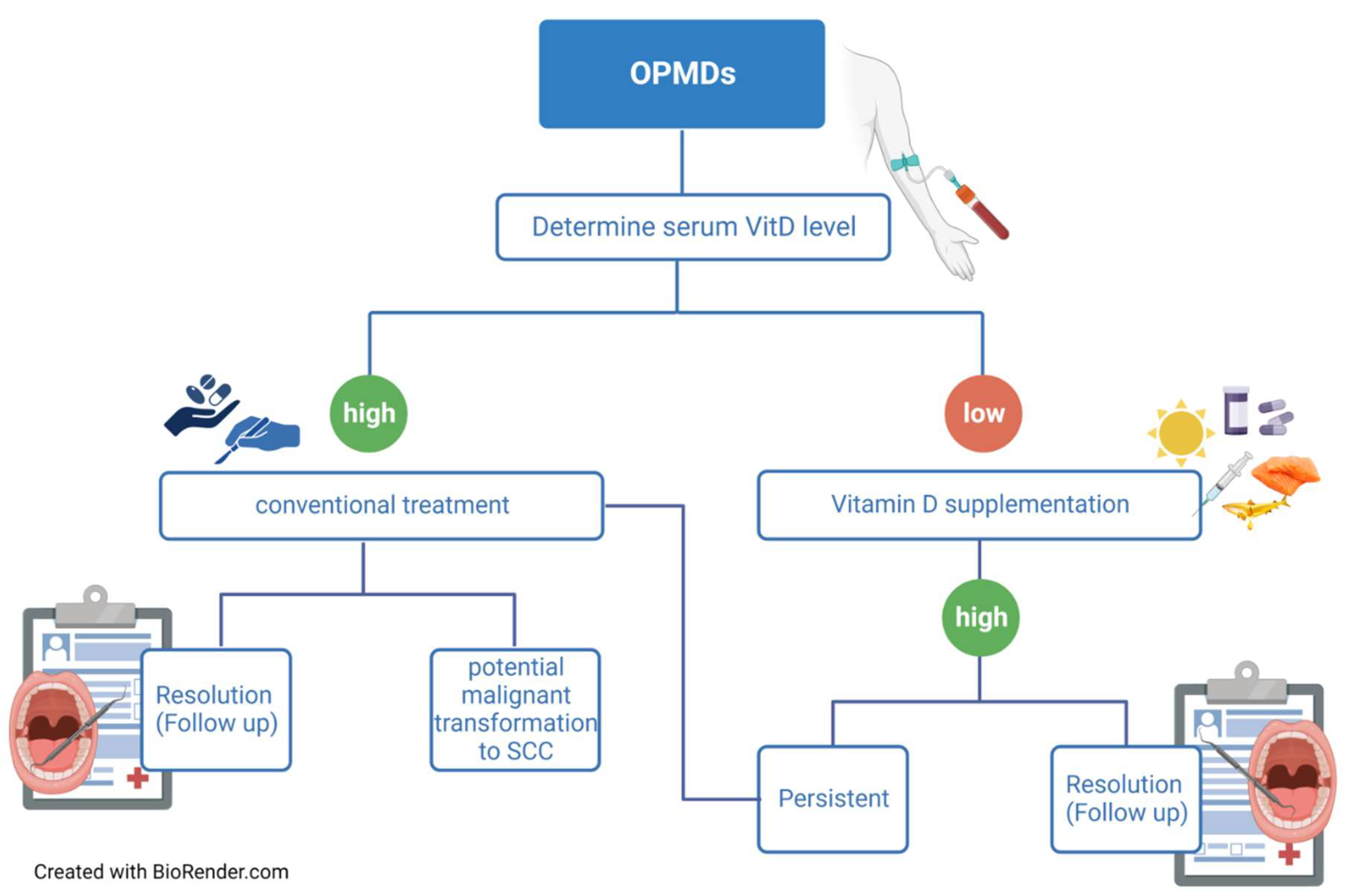
Figure 4.
Flow Chart Depicting Vitamin D Supplementation Strategies for OPMDs Treatment. Schematic representation illustrating various treatment modalities for OPMDs with respect to Vitamin D supplementation. The treatments are categorized based on serum Vitamin D levels following diagnosis. 'Low' indicates deficient or insufficient Vitamin D levels, while 'High' signifies sufficient Vitamin D status.
Figure 4.
Flow Chart Depicting Vitamin D Supplementation Strategies for OPMDs Treatment. Schematic representation illustrating various treatment modalities for OPMDs with respect to Vitamin D supplementation. The treatments are categorized based on serum Vitamin D levels following diagnosis. 'Low' indicates deficient or insufficient Vitamin D levels, while 'High' signifies sufficient Vitamin D status.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



