Submitted:
06 September 2023
Posted:
07 September 2023
You are already at the latest version
Abstract
Background: Gestational diabetes is a common complication during pregnancy that can lead to numerous adverse outcomes. Some studies suggest that probiotics may be used to treat gestational diabetes, however, the results remain controversial. We conducted a systematic review and meta-analysis to evaluate the effect of probiotics on blood glucose and pregnancy outcomes in women with gestational diabetes. Methods: A systematic search of PubMed, Embase, and Cochrane databases was performed (start date to August 22, 2023). Primary outcomes included fasting blood sugar (FBS), fasting serum insulin (FSI), homeostasis model assessment of insulin resistance (HOMA-IR), and quantitative insulin sensitivity check index (QUICKI). Secondary outcomes included pregnancy and neonatal outcomes. Results: 15 articles (n = 1006 women) met the inclusion criteria and were included in the analysis. Compared to a placebo, probiotics can decrease FBS (MD -2.58, 95% CI -4.38 to -0.79, p < 0.01), FSI (MD -2.29, 95% CI -3.40 to -1.18, p < 0.01), HOMA-IR (MD -0.56, 95% CI -0.81 to -0.32, p < 0.01), birthweight (MD -101.20, 95% CI -184.62 to -17.77, p = 0.02), neonatal intensive care unit (NICU) (RR 0.60, 95% CI 0.40 to 0.89, p = 0.01), and hyperbilirubinemia (RR 0.31, 95% CI 0.16 to 0.61, p < 0.01), alongside higher QUICKI (MD 0.01, 95% CI 0.00 to 0.01, p < 0.01). However, no other significant results were obtained. Conclusion: Probiotics may improve blood glucose indicators and reduce neonatal hyperbilirubinemia, NICU admissions, and birth weight in women with GDM.
Keywords:
probiotics
; pregnancy
; GDM
; gestational diabetes
; meta analysis
1. Introduction
The most common metabolic complication of pregnancy is gestational diabetes mellitus (GDM), the incidence of which has been increasing significantly in the last decade, accounting for 12-18% of all pregnant patients [1]. Studies have shown that genetic, epigenetic and environmental factors can combine to cause GDM. Poor glycemic control during pregnancy may lead to adverse maternal and infant outcomes, such as maternal preeclampsia, hypertension, neonatal macrosomia, and hypoglycemia [2].
Therefore, the cornerstone of GDM management is glycemic control. Lifestyle interventions are used as the initial treatment for GDM and include medical nutrition therapy and daily exercise. Patients are asked to check their blood glucose levels frequently at home to ensure that blood glucose goals are being met. If these measurements do not meet glycemic goals, medication should be initiated [3].
Although women with gestational diabetes still make insulin, their bodies are not sensitive to it and do not produce enough insulin to maintain blood glucose control. Insulin is often the treatment of choice for women who are unable to maintain their blood glucose treatment goals through medical nutrition therapy or other pharmacological therapies. Insulin may be an alternative for women who cannot tolerate the side effects of oral antidiabetic medications such as metformin [4]. However, some serious side effects of insulin and oral hypoglycaemic drugs, such as hypoglycaemia and gastrointestinal symptoms, limit their use, and sometimes these treatments are more dangerous for mothers and babies.
The definition of probiotics is live microorganisms that provide health benefits when consumed in sufficient quantities. For decades, it has been discovered that probiotics can treat acute gastroenteritis, Clostridium difficile-associated diarrhoea, irritable bowel syndrome, and digestive issues, among others [5]. Some studies have shown that the pathogenesis of GDM may be related to abnormalities in the composition of the gut flora of pregnant women. Dietary supplements can play a role by regulating the intestinal microbiota. Therefore, the use of dietary supplements, such as probiotics, to target the intestinal flora and regulate the disordered intestinal flora would be a potential method for the prevention and treatment of GDM [6].
However, some relevant randomized controlled trials (RCTs) have shown that probiotics have no effect on fasting blood sugar (FBS), fasting serum insulin (FSI), and neonatal weight in patients with gestational diabetes [7,8]. Some meta-analyses of GDM include RCTs involving obese or overweight pregnant women, rather than those with GDM. Therefore, considering these inconsistent effects, we conducted a novel meta-analysis of RCTs to assess the utility of probiotics on glycaemic control, maternal and infant outcomes in patients with gestational diabetes.
2. Methods
This meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) [9]. This study was registered at PROSPERO (CRD42023456637).
2.1. Literature Search
A comprehensive literature search was conducted using PubMed, Embase and the Cochrane Library. The search was limited to the English language (up to 22 August 2023). Furthermore, we conducted a search on http://www.clinicaltrials.gov/ to find information on registered RCTs in order to identify trials that were completed but had not yet published results. We primarily used the following search terms: "Gestational Diabetes Mellitus," "Probiotics," and "randomized controlled trials." We combined specific keywords and free text items with Boolean operators to create our search strategy.
2.2. Inclusion Criteria And Exclusion Criteria
The meta-analysis comprised studies that met the following criteria: fully open randomised controlled studies conducted according to English-language criteria; patients were women diagnosed with GDM in accordance with the American Diabetes Association, the World Health Organization, the Carpenter and Kushan Guidelines, and the Australian Pregnancy Association Consensus Guidelines; and interventions consisted of probiotics alone or therapies of probiotic-accessorised other substances; and the full text was available for review. The following studies were excluded: Ongoing trials whose results had not been presented or published; repetitive publications; and review articles, case reports, conference abstracts and guidelines.
2.3. Risk of Bias Assessment
Two independent investigators assessed the risk of bias in the literature. The recommended "risk of bias" tool from the Cochrane Collaboration was used.
2.4. Data Extraction
Each included study was extracted independently by two researchers. Any disagreements were discussed or negotiated with a third researcher. The main information we extracted included: first author, year of publication, country, sample size of each trial group, dose of probiotics and number of weeks of duration. We focused on three outcomes: glycaemic control, maternal outcomes and neonatal outcomes. Glycaemic outcomes included FBS, FSI, homeostasis model assessment of insulin resistance (HOMA-IR), and quantitative insulin sensitivity check index (QUICKI); maternal outcomes included pre-eclampsia, caesarean section, preterm labour, induction of labour and polyhydramnios; neonatal outcomes included birth weight, neonatal length, neonatal head circumference, neonatal intensive care unit (NICU) admission, 1-min Apgar score, 5-min Apgar score, hyperbilirubinemia, macrosomia, large for gestational age (LGA), and neonatal hypoglycaemia.
2.5. Quality Assessment
Two researchers evaluated the risk of bias of the included clinical trials independently according to the the Cochrane Collaboration Tool [10]. We use Cochrane Handbook for Systematic Reviews of Interventions version 6.3 for quality evaluation. The following quality assessments were included: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other bias. The results were classified as "low risk", "high risk" and "unclear risk". Disagreements at the time of quality assessment were resolved by discussion or referred to a third evaluator for adjudication.
2.6. Statistical Analysis
Probiotic efficacy was assessed by pooling prognostic indicators. Dichotomous data are expressed as relative risk ratios (RR) and 95% confidence intervals (CI); continuous data are expressed as mean difference (MD) and 95%CI, statistically significant differences were deemed as such when p < 0.05.
Statistical heterogeneity was assessed by chi-squared test and I2 statistic.When statistically significant heterogeneity was found (I2 > 50% or p < 0.1), a random-effects model was used [11]. If not, fixed effects models are selected. All statistical calculations were conducted with Review Manager version 5.4 (Cochrane Collaboration, Software Update, Oxford, UK). The risk of bias was assessed with the Egger statistical method using Stata software 12.0 (StataCorp, based in College Station, Texas, USA). We assessed bias only for studies included in a sample of 10 or more. For outcomes with greater heterogeneity, we conducted subgroup analyses examining the effects of both country and duration.
3. Results
3.1. Study Selection and Characteristics
A total of 221 relevant articles were retrieved from various databases and 122 studies were obtained after removing duplicates. Subsequently, 104 irrelevant articles were removed because some of them were of the review type, non-RCTs, etc. The remaining 18 articles were reviewed in full text, of which 3 had insufficient data. Therefore, a total of 15 RCT articles[8,12,13,14,15,16,17,18,19,20,21,22,23,24,25] were finally selected for meta-analysis. Figure 1 depicted the search process, and Table 1 listed the basic characteristics of eligible trials. At baseline, age, height and weight were not significantly different between the probiotic and control groups. A total of 1006 participants were included in our quantitative analyses, 503 in the probiotic group and 503 in the placebo group. All included trials were published between 2015 and 2022, and all 15 trials were conducted in 5 countries: 11 in Iran, 1 in Ireland, 1 in Israel, 1 in Thailand and 1 in Turkey. This shows that Iran was the main country studied. The findings of Egger's test for FBS, FSI, and HOMA-IR were 0.749, 0.022, and 0.020, respectively. The results suggest a possible publication bias in the probiotics' impact on the FSI and HOMA-IR variables.
3.2. Glycemic outcomes
3.2.1. FBS
Results from 12 trials with a total of 805 GDM patients included FBS (Figure 2A). In the meta-analysis, the mean difference in FBS levels (MD -2.58, 95% CI -4.38 to -0.79, p < 0.01) implies that probiotics statistically significantly improved FBS levels in pregnant women with GDM.
3.2.2. FSI
The findings from 10 studies with 661 GDM patients consistently incorporated FSI (Figure 2B). The studies indicated that the probiotic group exhibited lowered FSI levels (MD -2.29, 95% CI -3.40 to -1.18, p < 0.01).
3.2.3. HOMA-IR
HOMA-IR measurements from 661 expectant mothers with GDM across ten studies were analysed (Figure 2C). The findings indicate that the HOMA-IR levels in the intervention group were lower than those in the placebo group (MD -0.56, 95% CI -0.81 to -0.32, p < 0.01).
3.2.4. QUICKI
The QUICKI test results from seven studies including 432 pregnant women diagnosed with GDM are shown (Figure 2D). The results of the studies propose that QUICKI levels in the intervention group (MD 0.01, 95% CI 0.00 to 0.01, p < 0.01) were higher than those in the placebo group.
3.3. Maternal outcomes
3.3.1. Preeclampsia
The preeclampsia incidence was included in all 4 studies of 313 pregnant women (Figure 3A). The probiotic group did not display any statistically significant incidence of pre-eclampsia in comparison to the placebo group (RR 1.14, 95% CI 0.56 to 2.31, p = 0.71).
3.3.2. Cesarean delivery
The forest plot (Figure 3B) displays a merged analysis of the outcomes of caesarean sections in the experimental and control groups. The combined effect size estimations indicated that the differentiation between the two groups was not statistically noteworthy (RR 0.88, 95% CI 0.48 to 1.64, p = 0.70).
3.3.3. Preterm delivery
Three studies included information from 177 participants who had a caesarean section (Figure 3C). There was no statistical difference in the risk of preterm birth between the probiotic and placebo groups (RR 0.99, 95% CI 0.23 to 4.24, p = 0.99).
3.3.4. Induction of labor
Information from 212 participants who underwent a caesarean section was analysed in the two included studies (Figure 3D). The probiotic group did not show a statistically significant difference in the risk of caesarean section when compared to the placebo group (RR 0.83, 95% CI 0.34 to 2.03, p = 0.69).
3.3.5. Polyhydramnios
In addition, we found 3 publications that included a combined sample of 177 subjects with polyhydramnios during pregnancy (Figure 3E). Nevertheless, the difference between the two groups was not statistically significant (RR 0.46, 95% CI 0.13 to 1.56, p = 0.21).
3.4. Neonatal outcomes
3.4.1. Birthweight、Neonatal length and head circumference
Birth weight was compared between the two groups in seven studies. Meta-analysis (Figure 4A) showed that among all included studies, probiotic group (MD -101.20, 95% CI -184.62 to -17.77, p = 0.02) had a significant reduction in newborn weight compared to placebo group.
For neonatal length in a total of 5 studies (Figure 4B), there was no statistically significant difference between the probiotic intervention group and the placebo group for neonatal length (MD -0.44 , 95% CI -1.01 to 0.12, p = 0.12).
There were 6 studies on Neonatal head circumference (Figure 4C). There was no statistically significant difference in the results of the comparison between the probiotic and placebo groups (MD -0.02 , 95% CI -0.36 to 0.31, p = 0.89).
3.4.2. NICU
A total of six studies were included (Figure 4D), and a forest plot showed a reduced risk of NICUs compared to placebo (RR 0.60, 95% CI 0.40 to 0.89, p = 0.01).
3.4.3. Apgar score
We retrieved Apgar scores, including scores taken at one-minute and five-minute intervals (Figure 4E-F). For both the one-minute Apgar score (MD 0.03, 95% CI -0.06 to 0.11, p = 0.51) and the five-minute Apgar score (MD 0.04, 95% CI -0.03 to 0.12, p = 0.23), there was no significant difference detected between the probiotic group and the placebo group.
3.4.4. Hyperbilirubinemia
Four studies were included in the analysis (Figure 4G), revealing a significant difference between the two groups. The probiotic group exhibited a lower risk of hyperbilirubinaemia in neonates compared to the placebo group (RR 0.31 , 95% CI 0.16 to 0.61, p < 0.01).
3.4.5. Other neonatal outcomes
Furthermore, we summarised data on macrosomia, LGA and neonatal hypoglycaemia and found that none of the three outcomes were statistically significant(Figure 4H-J). For Macrosomia, we collected five papers comprising 408 individuals. These studies showed that the probiotic group did not reduce the incidence of macrosomia (RR 0.37, 95% CI 0.12 to 1.15, p = 0.08). Similarly, no reduction was observed in the incidence of LGA (RR 0.72, 95% CI 0.38 to 1.36, p = 0.31) or neonatal hypoglycaemia (RR 0.80, 95% CI 0.43 to 1.51, p = 0.49).
3.5. Subgroup Analysis
Due to FBS (I2 = 72%), FSI (I2 = 69%), HOMA-IR (I2 = 61%), QUICKI (I2 = 52%), cesarean delivery (I2 = 74%) and macrosomia (I2 = 55%), these outcomes existed with large heterogeneity and were therefore analyzed in subgroups, however, there were too few experiments on the outcome of induction of labour (I2 = 82%), so subgroup analyses were not performed. The duration and country subgroups were grouped to examine potential reasons for heterogeneity. Different groups' p-values and heterogeneity are shown in Table 2. Results suggest that country could have contributed to heterogeneity in FSI, HOMA-IR and macrosomia and did not explain heterogeneity in other outcomes; whereas duration did not explain heterogeneity in any outcomes.
3.6. Assessment of study quality
All studies provided detailed explanations of the generation of randomised sequences and were assessed to be at low risk of bias. Ten studies clearly explained the allocation concealment process, and the remaining four studies which lacked this information were categorised as being at an unclear risk of bias. One study, which was an open-label trial, was deemed to have a high risk of bias, whereas 14 studies mentioned the blinding of assessors and were thus considered to be at low risk of bias. Based on a review of the study protocols, it was observed that all studies were at low risk of bias for follow-up and other biases. This is supported by the risk of bias graph (Figure 5) and the risk of bias summary (Figure 6). Consequently, the studies met the quality criteria.
4. Discussion
The objective of this meta-analysis was to evaluate the glycaemic impact of probiotics compared to placebo among patients with gestational diabetes, along with presenting maternal and neonatal outcomes. Our meta-analysis demonstrates that regarding glycaemic outcomes, probiotics resulted in decreased levels of FBS, FSI, HOMA-IR, and increased levels of QUICKI. In relation to maternal outcomes, probiotics were found to have a significant impact on our set of preeclampsia, cesarean delivery, preterm delivery, induction of labour, and polyhydramnios indicators. However, they did not show any statistically significant results for other relevant outcomes. Concerning neonatal outcomes, probiotics were noted to result in reduced birthweight, NICU admissions and hyperbilirubinemia. Subgroup analyses indicated that the country was able to explain the heterogeneity of FSI, HOMA-IR, and macrosomia.
The most prevalent complication during pregnancy in present times is GDM. The incidence of diagnosed hyperglycaemic and even overtly diabetic young women is increasing. The primary risk factors for GDM are obesity or being overweight, a previous history of GDM, later age at childbearing, and a family history of type 2 diabetes. GDM works by altering glucose regulation during pregnancy to provide nutrients to the developing fetus[26]. Insulin sensitivity is reduced in late pregnancy compared to pre-pregnancy, while basal endogenous glucose production is increased [27,28]. In pregnant women with normal blood glucose, pancreatic β-cells produce more insulin to maintain normal glucose levels. Diagnosis is usually made using an oral glucose tolerance test (OGTT), but a non-fasting glucose provocation test is also used in some places to assess the need for a woman to undergo a complete oral glucose tolerance test, and one of the commonly used criteria includes the International Diabetes Federation (IDF), the American Diabetes Association (ADA) or the World Health Organisation (WHO). Treatment for GDM involves a healthy diet, exercise regimen, and appropriate medication. The Academy of Nutrition recommends a balanced diet for GDM, providing adequate macronutrients and micronutrients to limit blood sugar fluctuations in pregnant women and support the nutritional requirements of the foetus[29,30]. Carbohydrate intake can have an impact on blood glucose levels in pregnant women, so diets should be comprehensive and diverse, with particular attention paid to the carbohydrate content. In addition, physical activity requires energy consumption, and this energy comes from the oxidative breakdown of sugar. Therefore, appropriate exercise can consume sugar, thus reducing blood glucose levels, and can assist expecting mothers in maintaining their blood glucose levels better. Common exercises include walking, yoga, and dancing[31,32]. However, when blood glucose levels remain abnormal, treatment with insulin medication is necessary[33]. In some countries, oral hypoglycaemic agents, primarily metformin and glibenclamide, are also employed. Nevertheless, medication comes with risks and potential adverse effects. For instance, oral hypoglycaemic drugs carry the risk of hypoglycaemia to the foetus, while insulin injections may cause discomfort and skin reactions at the injection site. The pharmacological treatment entails choosing the appropriate drug, adjusting the dosage, and so on, which complicates diabetes management. Moreover, it must be used in strict compliance with the physician's advice and monitoring guidance. Medication is typically administered to manage blood glucose levels, however, gestational diabetes often resolves spontaneously postpartum. Therefore, personalized treatment is required. Hence, the necessity of pharmacotherapy must be balanced against its use throughout the entirety of pregnancy. Each pregnant woman's physical state and pancreatic function is distinctive, and their response to various drugs can vary. Thus, there is a need to find more convenient and safer treatment options.
A mounting body of research indicates a crucial connection between glucose intolerance and dysbiosis of gut microflora (GM) during pregnancy[34]. As per the analyzed data, probiotics exhibit a beneficial impact on glycaemic control and might have a role in preventing and treating GDM, thus constituting a promising strategy to lessen GDM occurrence[35,36].Evidence suggests that probiotics may reduce adverse pregnancy outcomes in GDM by modulating gut microbial composition and improving metabolism. The corresponding mechanisms are believed to involve the secretion of short-chain fatty acids, modulation of hormone secretion, and reduction of inflammatory responses[6].
One study discovered that the addition of probiotics during pregnancy did not seem to decrease the possibility of diabetes or enhance other neonatal and maternal outcomes[37]. The Shahriari et al. study aimed to investigate the impact of probiotic supplementation during pregnancy on the likelihood of GDM and other maternal and neonatal outcomes. Mothers underwent assessment for GDM presence via a 75 g OGTT between weeks 24-28 of pregnancy. The probiotic group, comprising of 507 pregnant women, were randomly assigned. Each 500 mg probiotic capsule contained a blend of Lactobacillus acidophilus LA1, Bifidobacterium longum sp54 cs, and Bifidobacterium bifidum sp9 cs, while the control group was given placebo. The study found that the incidence of GDM was similar in both the probiotic group (41.9%) and the control group (40.2%) (p = 0.780). Additionally, there were no significant differences in FBS (88.68 vs. 89.61 mg/dL; p = 0.338), OGTT-1h (163.86 vs. 166.88 mg/dL; p = 0.116), and OGTT-2h (138.39 vs. 139.27 mg/dL; p = 0.599) between the probiotic and control groups. Yet another study hints at a potential decrease in the occurrence of LGA[38]. The objective was to ascertain if probiotics (Lactobacillus rhamnosus and Bifidobacterium animalis Lactis subspecies) consumed by overweight and obese women from mid-pregnancy prevented GDM, as 411 women were randomly allocated. The frequency of GDM was 12.3% among the placebo group and 18.4% among the probiotic group (p = 0.10). For the outcomes of preeclampsia, the probiotic group had a rate of 9.2%, while the placebo group had a rate of 4.9% (p = 0.09). The incidence of LGA was 2.4% in the probiotic group and 6.5% in the placebo group (p = 0.042). Furthermore, there were no significant differences in other pregnancy and neonatal outcomes. Both studies have demonstrated that probiotics do not prevent the emergence of GDM. Nonetheless, there is a contentious debate over the results regarding maternal and infant outcomes.
In previous studies, fewer meta-analyses focused on pregnancy outcomes and neonatal outcomes, and instead mainly collected data on metrics of glycemic control, lipid metabolism and inflammation[39,40]. Unlike previous studies, we exclusively selected patients with gestational diabetes to evaluate the influence of probiotics on GDM patients. Additionally, the preceding research featured obese and overweight pregnant women, who were not diagnosed with GDM – this could have introduced biased results[7]. Due to the restricted number of outcomes, we gathered some typical glycaemic outcomes, as well as maternal and infant outcomes. Our findings revealed no significant statistical differences in maternal outcomes, however, neonatal outcomes such as birthweight, NICU, and hyperbilirubinemia were significant.
The outcome of macrosomic babies in our study showed no statistically significant difference between the probiotic group and the placebo group, contrary to a previous study[41]. Furthermore, a prior meta-analysis[42] suggested that probiotics could elevate the risk of pre-eclampsia, but this did not impact neonatal birthweight. However, our results contrasted those of our counterparts, likely due to the inclusion of additional RCTs in our study.
In our study, the subanalyses of various countries produced divergent endpoints, likely due to the majority of studies being conducted in Iran. These findings underline the possibility that women across different nations may have varying gut microbiota influenced by distinct dietary and lifestyle choices, resulting in dissimilar gut microbiota. Additionally, differences in genetic and environmental backgrounds may cause variations in the roles of relevant and metabolic pathways in vivo. In future studies, greater consideration should be given to country-specific effects when determining appropriate probiotic supplements for various nations. Furthermore, subgroup analyses were performed for duration, and none of the subgroups with an 8-week cut-off could clarify the heterogeneity of the outcomes of interest. As a result, a different duration may need to be selected for subgroup analyses in the future.
Meta-analysis has a number of strengths. Firstly, combining data from 15 articles enhances the sample size (N = 1006) and boosts the dependability of the outcomes. Second, the majority of the integrated randomised controlled trials were high-quality studies that employed randomised sequence generation and double-blind methods, thus the resulting data had a high level of reliability. Thirdly, the study collected not only glycaemic indicators but also relevant maternal and infant outcomes in women with gestational diabetes, making the results more representative. These strengths render the findings of this study of high scientific worth and practical use. However, this study has several limitations. Firstly, the number of participants in the included randomised controlled trials was relatively small, ranging from 40 to 100. Secondly, because of restricted data, only one study has reported on postprandial glycaemia. This study evaluated solely fasting glycaemia and did not examine the impact of probiotics on postprandial glycaemia. Furthermore, only one study investigated small for gestational age (SGA). Thirdly, data on maternal and infant outcomes were insufficient, as they failed to present a comprehensive range of outcomes and consider the long-term effects on mothers and offspring. Furthermore, our subgroup analyses did not group the type and dose of probiotics together appropriately, thereby obscuring the extent of heterogeneity. Therefore, more randomised controlled trials are required to achieve greater precision in the results. Overall, the data indicates a positive effect of probiotics for patients with GDM, as demonstrated by improvements in glucose-related markers and certain neonatal markers.
5. Conclusions
In conclusion, this meta-analysis, based on short-term data, indicates that probiotics have the potential to improve glycaemic control and reduce the risk of some neonatal outcomes compared with placebo. Therefore, probiotics may be a safe and effective treatment for GDM. However, due to the limited number of RCTs, further research is required to evaluate the long-term effects of probiotics on pregnant women and neonates.
Author Contributions
R.W., J.J.H., H.L., and Z.J.L. all made significant contributions to the content and structure of the study. R.W. and J.J.H. reviewed each experiment for eligibility and extracted and tabulated the relevant data. R.W. analysed the data. R.W. drafted the article. H.L. checked the format of the article.R.W., J.J.H., H.L., and Z.J.L. commented on the content of the article. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO): registration ID CRD42023456637.
Acknowledgments
We would like to thank the library of Shenyang Pharmaceutical University for their help in retrieving literature.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Szmuilowicz, E.D.; Josefson, J.L.; Metzger, B.E. Gestational Diabetes Mellitus. Endocrinol. Metab. Clin. N. Am. 2019, 48, 479–493. [Google Scholar]
- Lowe, W.L., Jr.; Scholtens, D.M.; Lowe, L.P.; Kuang, A.; Nodzenski, M.; Talbot, O.; Catalano, P.M.; Linder, B.; Brickman, W.J.; Clayton, P., et al.; et al. Association of Gestational Diabetes With Maternal Disorders of Glucose Metabolism and Childhood Adiposity. JAMA 2018, 320, 1005–1016. [Google Scholar] [PubMed]
- Alfadhli, E.M. Gestational diabetes mellitus. Saudi Med. J. 2015, 36, 399–406. [Google Scholar] [PubMed]
- Brown, J.; Grzeskowiak, L.; Williamson, K.; Downie, M.R.; Crowther, C.A. Insulin for the treatment of women with gestational diabetes. Cochrane Database Syst. Rev. 2017, 11, Cd012037. [Google Scholar]
- Suez, J.; Zmora, N.; Segal, E.; Elinav, E. The pros, cons, and many unknowns of probiotics. Nat. Med. 2019, 25, 716–729. [Google Scholar]
- Wan, J.; Ma, J. Efficacy of dietary supplements targeting gut microbiota in the prevention and treatment of gestational diabetes mellitus. Front Microbiol 2022, 13, 927883. [Google Scholar]
- Pellonperä, O.; Mokkala, K.; Houttu, N.; Vahlberg, T.; Koivuniemi, E.; Tertti, K.; Rönnemaa, T.; Laitinen, K. Efficacy of Fish Oil and/or Probiotic Intervention on the Incidence of Gestational Diabetes Mellitus in an At-Risk Group of Overweight and Obese Women: a Randomized, Placebo-Controlled, Double-Blind Clinical Trial. Diabetes Care 2019, 42, 1009–1017. [Google Scholar] [PubMed]
- Badehnoosh, B.; Karamali, M.; Zarrati, M.; Jamilian, M.; Bahmani, F.; Tajabadi-Ebrahimi, M.; Jafari, P.; Rahmani, E.; Asemi, Z. The effects of probiotic supplementation on biomarkers of inflammation, oxidative stress and pregnancy outcomes in gestational diabetes. J. Matern. Fetal Neonatal Med. 2018, 31, 1128–1136. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials revisited. Contemp. Clin. Trials 2015, 45, 139–145. [Google Scholar] [PubMed]
- Dolatkhah, N.; Hajifaraji, M.; Abbasalizadeh, F.; Aghamohammadzadeh, N.; Mehrabi, Y.; Abbasi, M.M. Is there a value for probiotic supplements in gestational diabetes mellitus? A randomized clinical trial. J. Health Popul. Nutr. 2015, 33, 25. [Google Scholar]
- Lindsay, K.L.; Brennan, L.; Kennelly, M.A.; Maguire, O.C.; Smith, T.; Curran, S.; Coffey, M.; Foley, M.E.; Hatunic, M.; Shanahan, F.; et al. Impact of probiotics in women with gestational diabetes mellitus on metabolic health: a randomized controlled trial. Am. J. Obstet. Gynecol. 2015, 212, 496.e491-411. [Google Scholar]
- Ahmadi, S.; Jamilian, M.; Tajabadi-Ebrahimi, M.; Jafari, P.; Asemi, Z. The effects of synbiotic supplementation on markers of insulin metabolism and lipid profiles in gestational diabetes: a randomised, double-blind, placebo-controlled trial. Br. J. Nutr. 2016, 116, 1394–1401. [Google Scholar] [PubMed]
- Jafarnejad, S.; Saremi, S.; Jafarnejad, F.; Arab, A. Effects of a Multispecies Probiotic Mixture on Glycemic Control and Inflammatory Status in Women with Gestational Diabetes: A Randomized Controlled Clinical Trial. J Nutr Metab 2016, 2016, 5190846. [Google Scholar]
- Karamali, M.; Dadkhah, F.; Sadrkhanlou, M.; Jamilian, M.; Ahmadi, S.; Tajabadi-Ebrahimi, M.; Jafari, P.; Asemi, Z. Effects of probiotic supplementation on glycaemic control and lipid profiles in gestational diabetes: a randomized, double-blind, placebo-controlled trial. Diabetes Metab. 2016, 42, 234–241. [Google Scholar]
- Hajifaraji, M.; Jahanjou, F.; Abbasalizadeh, F.; Aghamohammadzadeh, N.; Abbasi, M.M.; Dolatkhah, N. Effect of probiotic supplements in women with gestational diabetes mellitus on inflammation and oxidative stress biomarkers: a randomized clinical trial. Asia Pac. J. Clin. Nutr. 2018, 27, 581–591. [Google Scholar]
- Karamali, M.; Nasiri, N.; Taghavi Shavazi, N.; Jamilian, M.; Bahmani, F.; Tajabadi-Ebrahimi, M.; Asemi, Z. The Effects of Synbiotic Supplementation on Pregnancy Outcomes in Gestational Diabetes. Probiotics and antimicrobial proteins 2018, 10, 496–503. [Google Scholar]
- Nabhani, Z.; Hezaveh, S.J.G.; Razmpoosh, E.; Asghari-Jafarabadi, M.; Gargari, B.P. The effects of synbiotic supplementation on insulin resistance/sensitivity, lipid profile and total antioxidant capacity in women with gestational diabetes mellitus: a randomized double blind placebo controlled clinical trial. Diabetes Res. Clin. Pract. 2018, 138, 149–157. [Google Scholar]
- Babadi, M.; Khorshidi, A.; Aghadavood, E.; Samimi, M.; Kavossian, E.; Bahmani, F.; Mafi, A.; Shafabakhsh, R.; Satari, M.; Asemi, Z. The Effects of Probiotic Supplementation on Genetic and Metabolic Profiles in Patients with Gestational Diabetes Mellitus: a Randomized, Double-Blind, Placebo-Controlled Trial. Probiotics and antimicrobial proteins 2019, 11, 1227–1235. [Google Scholar] [PubMed]
- Jamilian, M.; Amirani, E.; Asemi, Z. The effects of vitamin D and probiotic co-supplementation on glucose homeostasis, inflammation, oxidative stress and pregnancy outcomes in gestational diabetes: a randomized, double-blind, placebo-controlled trial. Clinical nutrition (Edinburgh, Scotland) 2019, 38, 2098–2105. [Google Scholar]
- Kijmanawat, A.; Panburana, P.; Reutrakul, S.; Tangshewinsirikul, C. Effects of probiotic supplements on insulin resistance in gestational diabetes mellitus: a double-blind randomized controlled trial. Journal of diabetes investigation 2019, 10, 163–170. [Google Scholar]
- Sahhaf Ebrahimi, F.; Homayouni Rad, A.; Mosen, M.; Abbasalizadeh, F.; Tabrizi, A.; Khalili, L. Effect of L. acidophilus and B. lactis on blood glucose in women with gestational diabetes mellitus: A randomized placebo-controlled trial. Diabetol. Metab. Syndr. 2019, 11. [Google Scholar]
- Amirani, E.; Asemi, Z.; Taghizadeh, M. The effects of selenium plus probiotics supplementation on glycemic status and serum lipoproteins in patients with gestational diabetes mellitus: a randomized, double-blind, placebo-controlled trial. Clinical nutrition ESPEN 2022, 48, 56–62. [Google Scholar]
- Yefet, E.; Perlitz, Y.; Yaakov, L.S.; Magril, G.; Vitner, D.; Zipori, Y.; Weiner, E.; Alon, A.S.; Paz, Y.G.; Nezer, M.; et al. The effect of probiotics on glycemic control of women with gestational diabetes mellitus-multicenter, randomized, double blind, placebo controlled-trial. Am. J. Obstet. Gynecol. 2022, 226, S258–S259. [Google Scholar]
- McIntyre, H.D.; Catalano, P.; Zhang, C.; Desoye, G.; Mathiesen, E.R.; Damm, P. Gestational diabetes mellitus. Nat Rev Dis Primers 2019, 5, 47. [Google Scholar]
- Catalano, P.M.; Tyzbir, E.D.; Roman, N.M.; Amini, S.B.; Sims, E.A. Longitudinal changes in insulin release and insulin resistance in nonobese pregnant women. Am. J. Obstet. Gynecol. 1991, 165, 1667–1672. [Google Scholar]
- Catalano, P.M.; Tyzbir, E.D.; Wolfe, R.R.; Roman, N.M.; Amini, S.B.; Sims, E.A. Longitudinal changes in basal hepatic glucose production and suppression during insulin infusion in normal pregnant women. Am. J. Obstet. Gynecol. 1992, 167, 913–919. [Google Scholar]
- Rasmussen, L.; Poulsen, C.W.; Kampmann, U.; Smedegaard, S.B.; Ovesen, P.G.; Fuglsang, J. Diet and Healthy Lifestyle in the Management of Gestational Diabetes Mellitus. Nutrients 2020, 12. [Google Scholar]
- Hernandez, T.L.; Mande, A.; Barbour, L.A. Nutrition therapy within and beyond gestational diabetes. Diabetes Res. Clin. Pract. 2018, 145, 39–50. [Google Scholar]
- Davenport, M.H.; Ruchat, S.M.; Poitras, V.J.; Jaramillo Garcia, A.; Gray, C.E.; Barrowman, N.; Skow, R.J.; Meah, V.L.; Riske, L.; Sobierajski, F.; et al. Prenatal exercise for the prevention of gestational diabetes mellitus and hypertensive disorders of pregnancy: a systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1367–1375. [Google Scholar]
- Allman, B.R.; McDonald, S.; May, L.; Børsheim, E. Resistance Training as a Countermeasure in Women with Gestational Diabetes Mellitus: A Review of Current Literature and Future Directions. Sports Med. 2022, 52, 2871–2888. [Google Scholar] [PubMed]
- Martín-Estal, I.; Castorena-Torres, F. Gestational Diabetes Mellitus and Energy-Dense Diet: What Is the Role of the Insulin/IGF Axis? Front Endocrinol (Lausanne) 2022, 13, 916042. [Google Scholar]
- Kamińska, K.; Stenclik, D.; Błażejewska, W.; Bogdański, P.; Moszak, M. Probiotics in the Prevention and Treatment of Gestational Diabetes Mellitus (GDM): A Review. Nutrients 2022, 14. [Google Scholar]
- Davidson, S.J.; Barrett, H.L.; Price, S.A.; Callaway, L.K.; Dekker Nitert, M. Probiotics for preventing gestational diabetes. Cochrane Database Syst. Rev. 2021, 4, Cd009951. [Google Scholar]
- Okesene-Gafa, K.A.; Moore, A.E.; Jordan, V.; McCowan, L.; Crowther, C.A. Probiotic treatment for women with gestational diabetes to improve maternal and infant health and well-being. Cochrane Database Syst. Rev. 2020, 6, Cd012970. [Google Scholar] [PubMed]
- Shahriari, A.; Karimi, E.; Shahriari, M.; Aslani, N.; Khooshideh, M.; Arab, A. The effect of probiotic supplementation on the risk of gestational diabetes mellitus among high-risk pregnant women: A parallel double-blind, randomized, placebo-controlled clinical trial. Biomed. Pharmacother. 2021, 141, 111915. [Google Scholar]
- Callaway, L.K.; McIntyre, H.D.; Barrett, H.L.; Foxcroft, K.; Tremellen, A.; Lingwood, B.E.; Tobin, J.M.; Wilkinson, S.; Kothari, A.; Morrison, M.; et al. Probiotics for the Prevention of Gestational Diabetes Mellitus in Overweight and Obese Women: Findings From the SPRING Double-Blind Randomized Controlled Trial. Diabetes Care 2019, 42, 364–371. [Google Scholar]
- Yefet, E.; Bar, L.; Izhaki, I.; Iskander, R.; Massalha, M.; Younis, J.S.; Nachum, Z. Effects of Probiotics on Glycemic Control and Metabolic Parameters in Gestational Diabetes Mellitus: Systematic Review and Meta-Analysis. Nutrients 2023, 15. [Google Scholar]
- Hasain, Z.; Che Roos, N.A.; Rahmat, F.; Mustapa, M.; Raja Ali, R.A.; Mokhtar, N.M. Diet and Pre-Intervention Washout Modifies the Effects of Probiotics on Gestational Diabetes Mellitus: A Comprehensive Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2021, 13. [Google Scholar]
- Zhou, L.; Ding, C.; Wu, J.; Chen, X.; Ng, D.M.; Wang, H.; Zhang, Y.; Shi, N. Probiotics and synbiotics show clinical efficacy in treating gestational diabetes mellitus: A meta-analysis. Prim. Care Diabetes 2021, 15, 937–947. [Google Scholar] [PubMed]
- Chu, X.; Yan, P.; Zhang, N.; Feng, L.; Li, X.; Wang, Y.; Yang, K. Probiotics for preventing gestational diabetes mellitus in overweight or obese pregnant women: A systematic review and meta-analysis. Clin Nutr ESPEN 2022, 50, 84–92. [Google Scholar] [PubMed]
Figure 1.
Included in the flow chart.
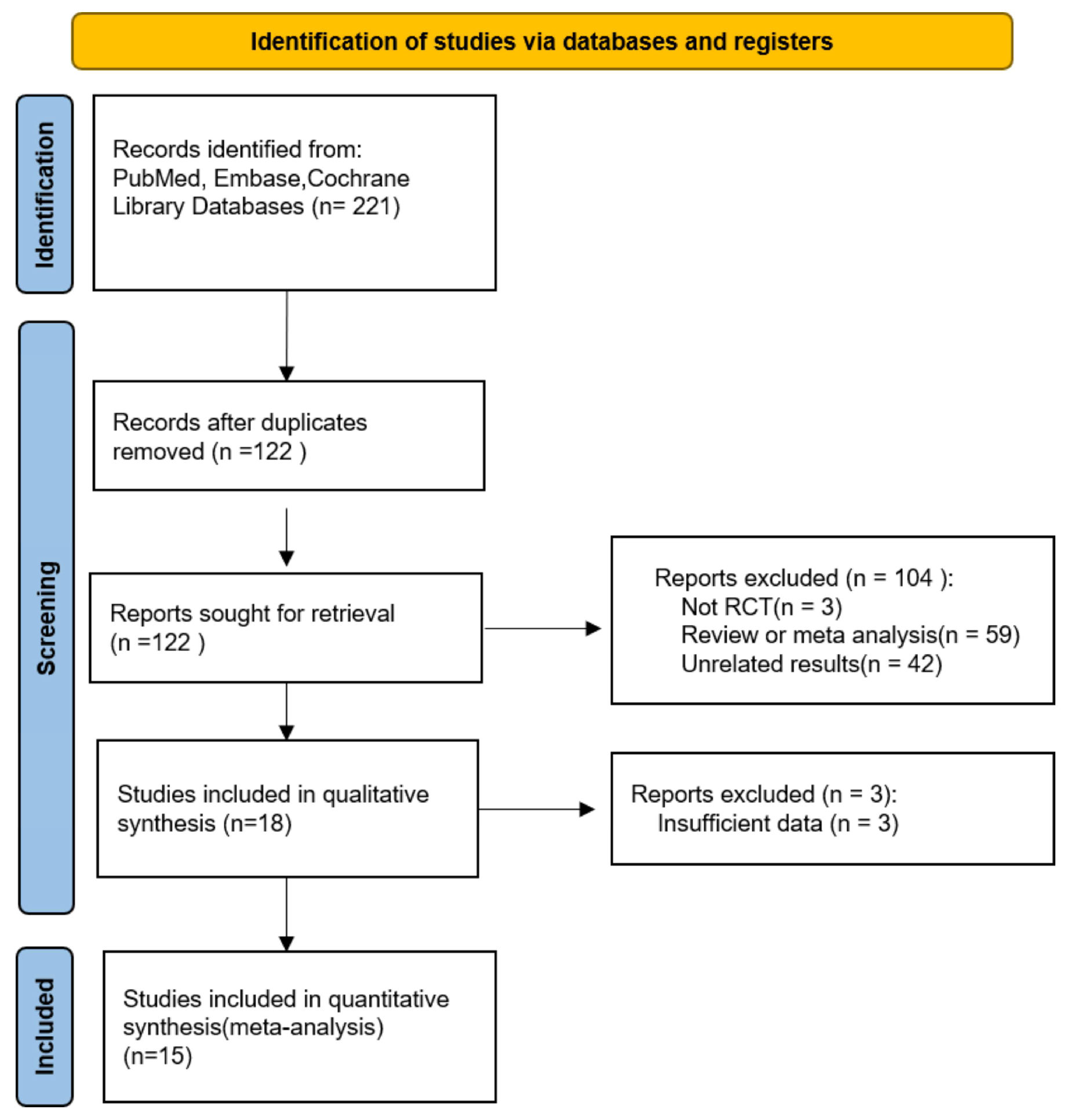
Figure 2.
Effect of probiotic on glucose control in pregnant women with GDM: (A) FBS (mg/dL), (B) FSI (mU/L), (C) HOMA-IR, and (D) QUICKI. FBS: fasting blood sugar; FSI: fasting serum insulin; HOMA-IR: the homoeostatic model assessment for insulin resistance; QUICKI: quantitative insulin sensitivity check index.
Figure 2.
Effect of probiotic on glucose control in pregnant women with GDM: (A) FBS (mg/dL), (B) FSI (mU/L), (C) HOMA-IR, and (D) QUICKI. FBS: fasting blood sugar; FSI: fasting serum insulin; HOMA-IR: the homoeostatic model assessment for insulin resistance; QUICKI: quantitative insulin sensitivity check index.
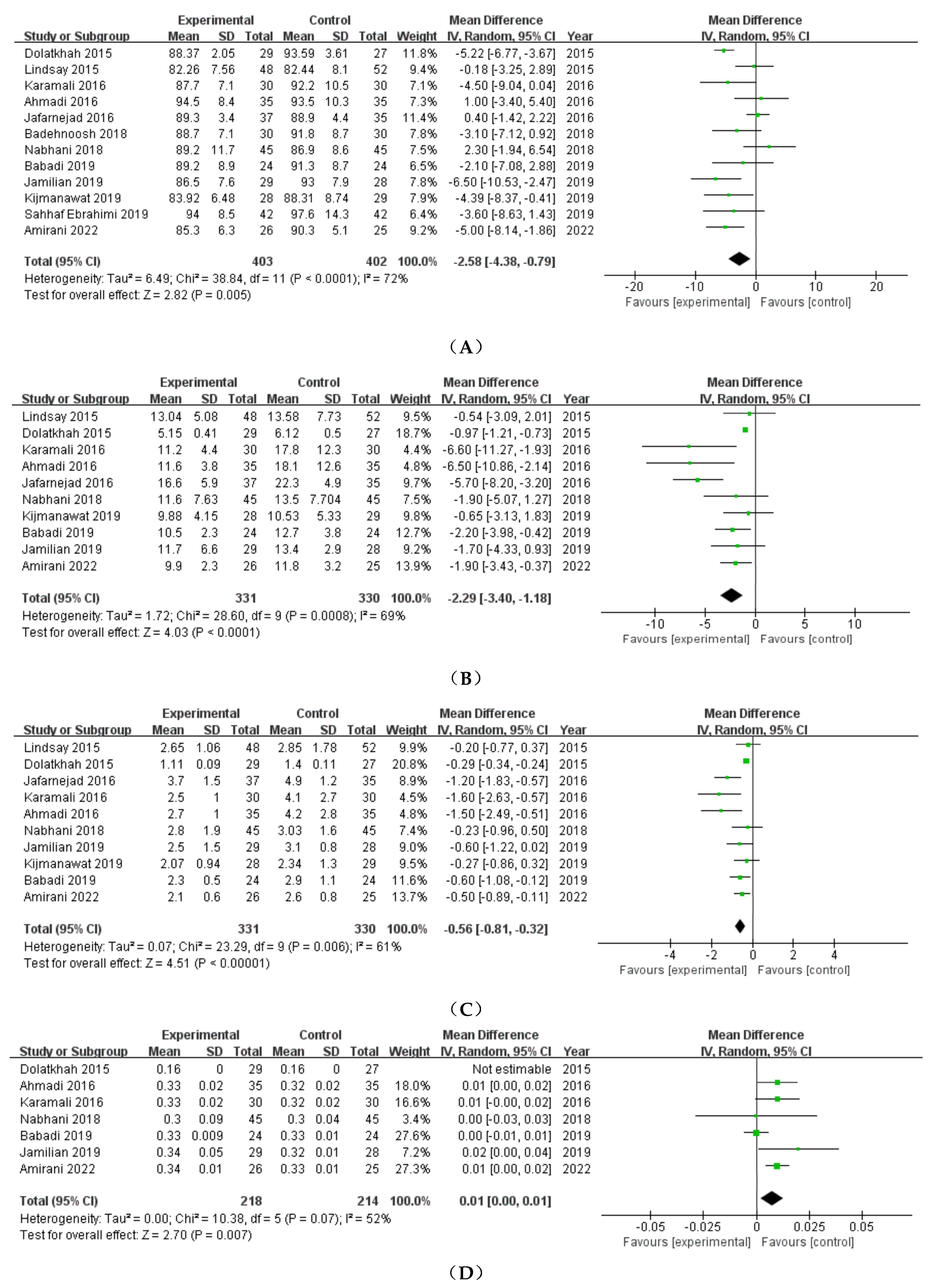
Figure 3.
Effect of probiotic on pregnancy outcomes in pregnant women with GDM: (A) Preeclampsia, (B) Cesarean delivery, (C) Preterm delivery, (D) Induction of labor, and (E) Polyhydramnios.
Figure 3.
Effect of probiotic on pregnancy outcomes in pregnant women with GDM: (A) Preeclampsia, (B) Cesarean delivery, (C) Preterm delivery, (D) Induction of labor, and (E) Polyhydramnios.
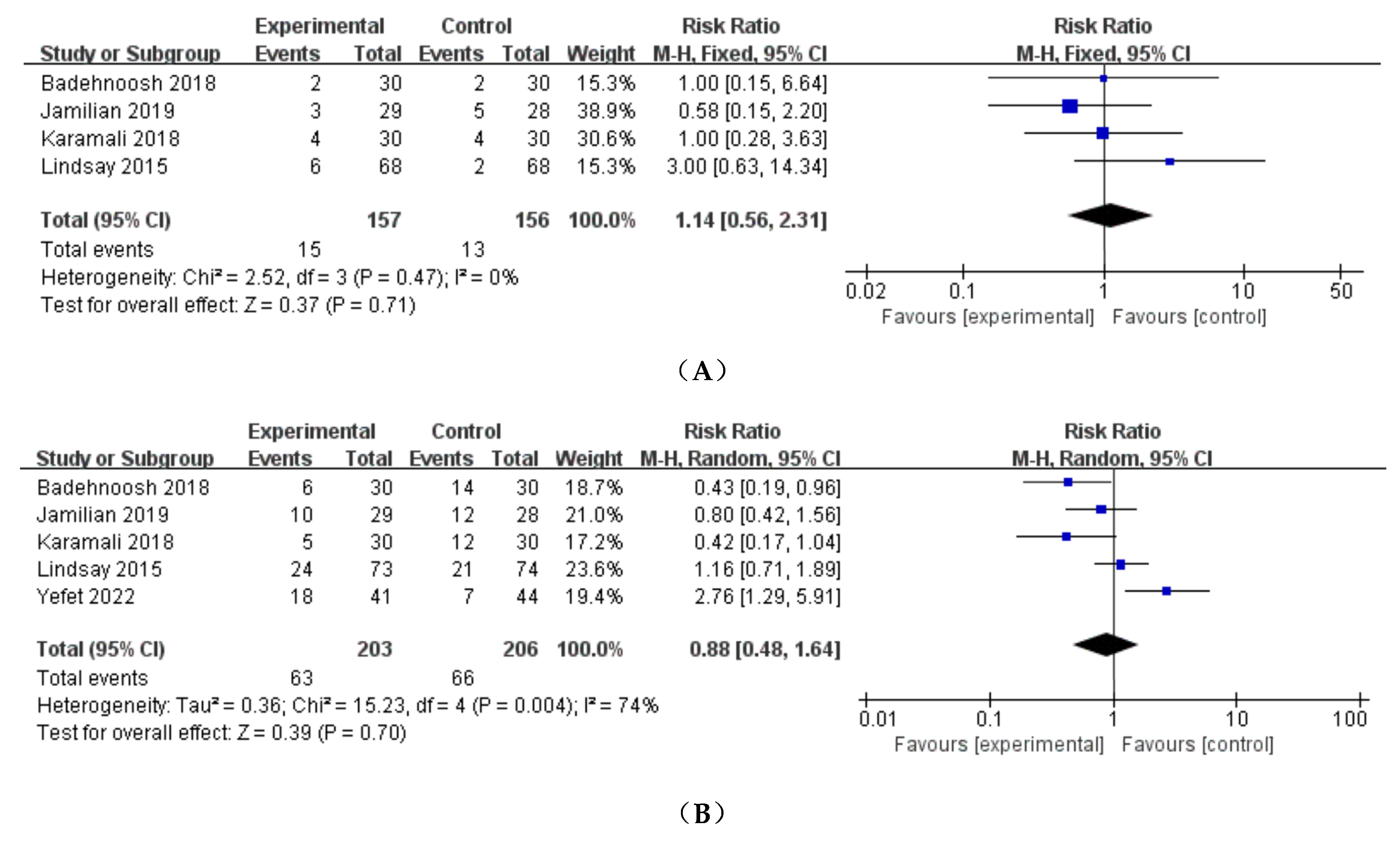
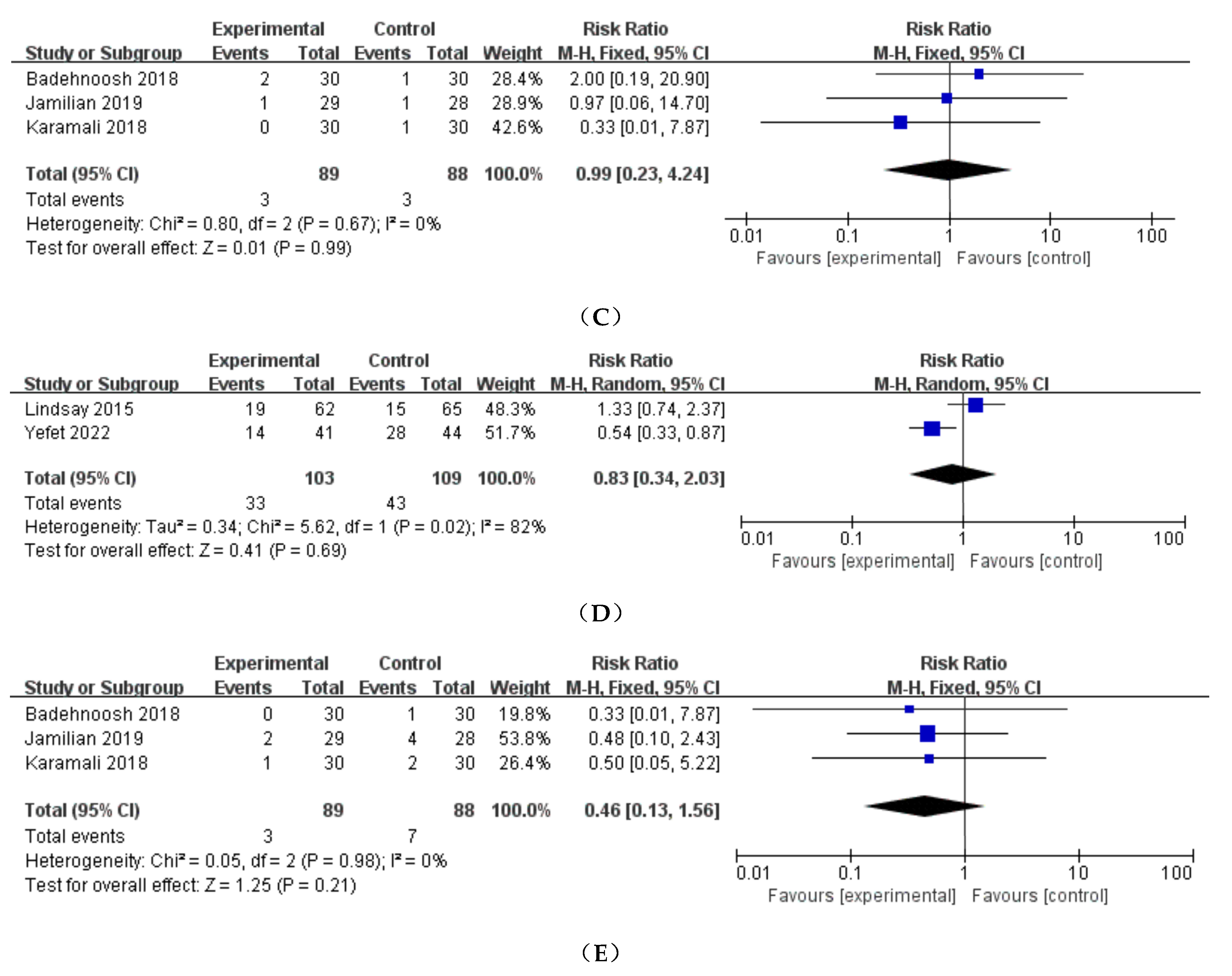
Figure 4.
Effect of probiotic on neonatal outcomes in pregnant women with GDM: (A) Birthweight (g), (B) Neonatal length (cm), (C) Neonatal head circumference (cm), (D) NICU, (E) 1-min Apgar score, (F) 5-min Apgar score, (G) Hyperbilirubinemia, (H) Macrosomia, (I) LGA, and (J) Neonatal hypoglycaemia. NICU: neonatal intensive care unit; LGA: large for gestational age.
Figure 4.
Effect of probiotic on neonatal outcomes in pregnant women with GDM: (A) Birthweight (g), (B) Neonatal length (cm), (C) Neonatal head circumference (cm), (D) NICU, (E) 1-min Apgar score, (F) 5-min Apgar score, (G) Hyperbilirubinemia, (H) Macrosomia, (I) LGA, and (J) Neonatal hypoglycaemia. NICU: neonatal intensive care unit; LGA: large for gestational age.

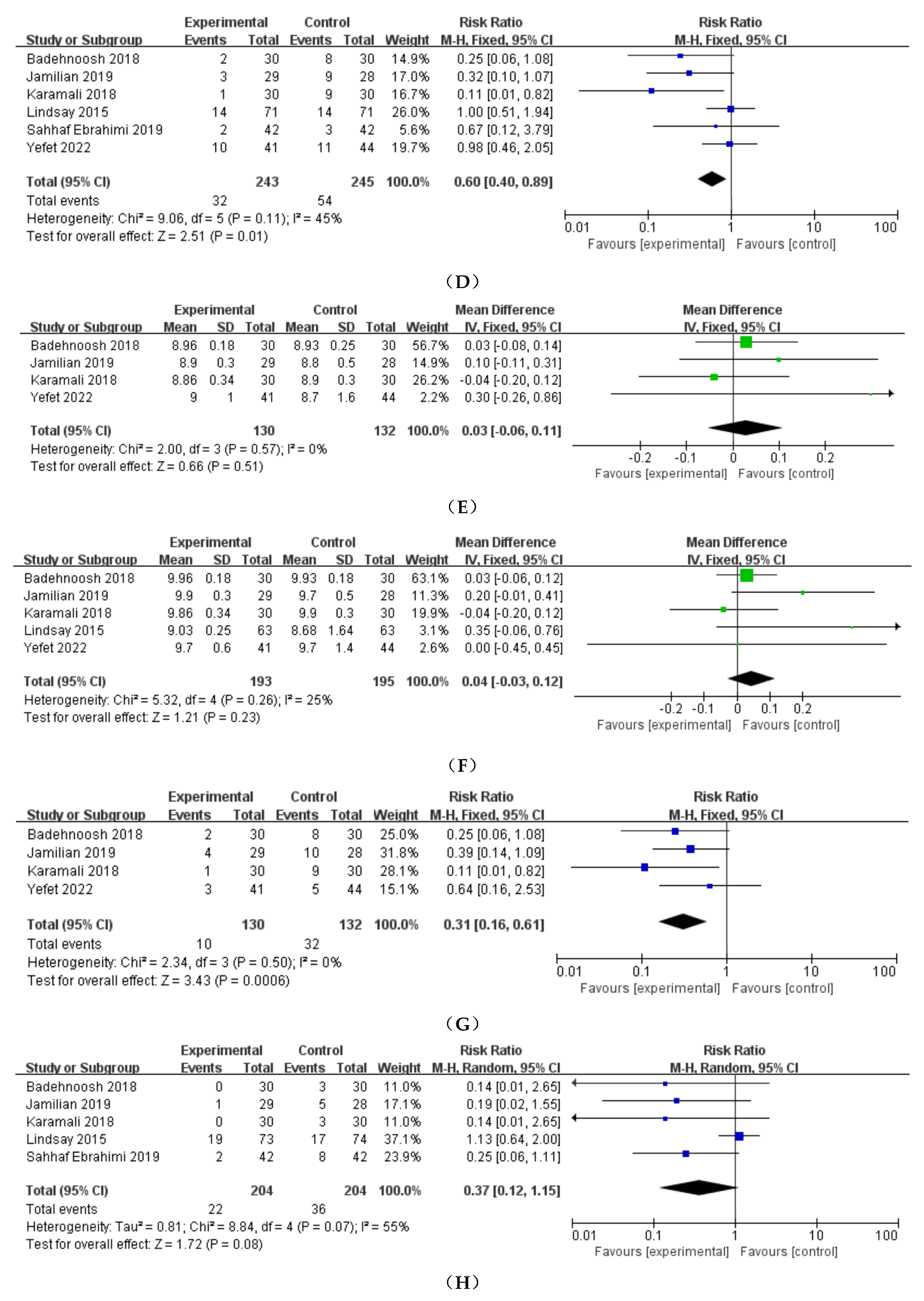
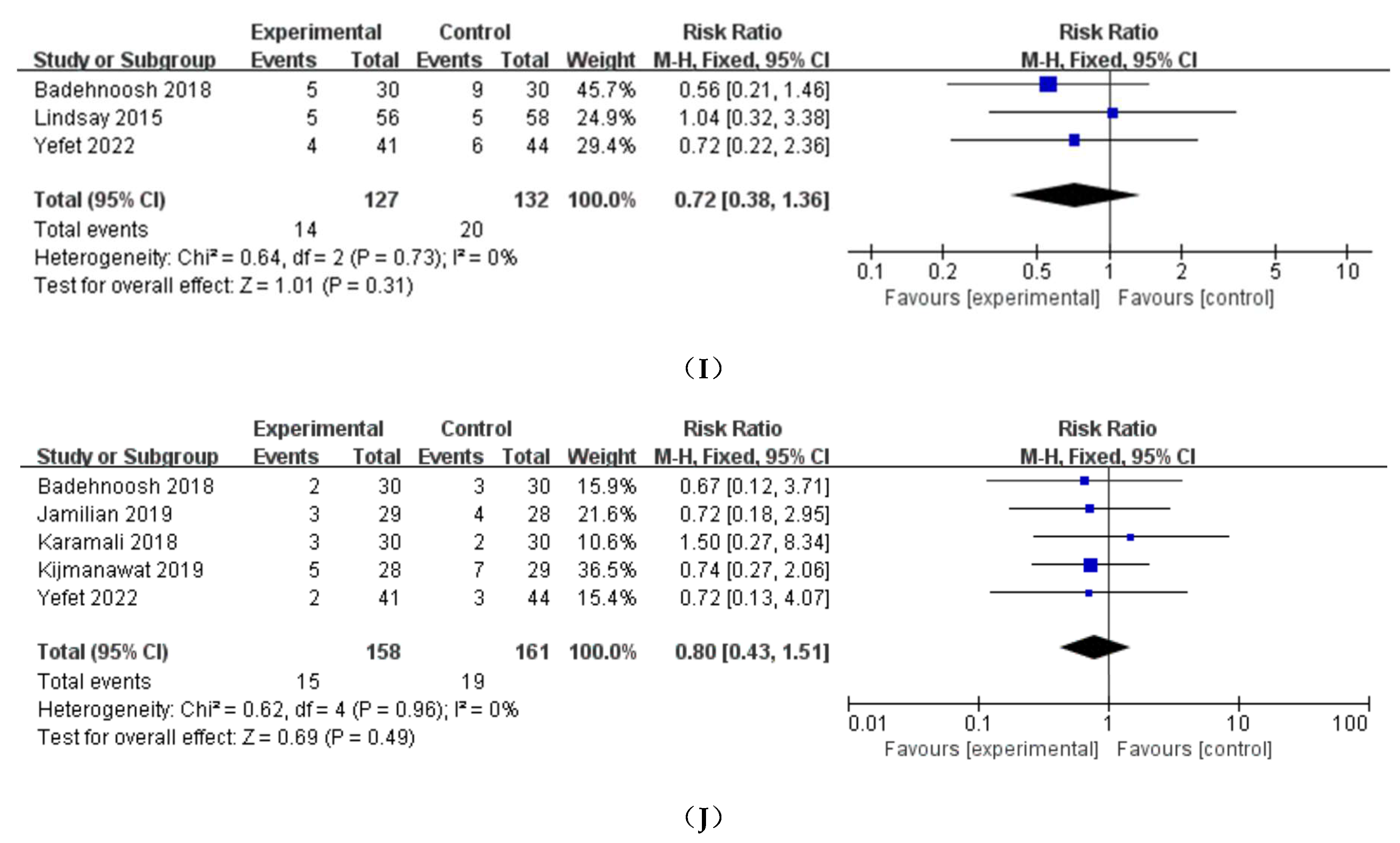
Figure 5.
The risk of bias graph.
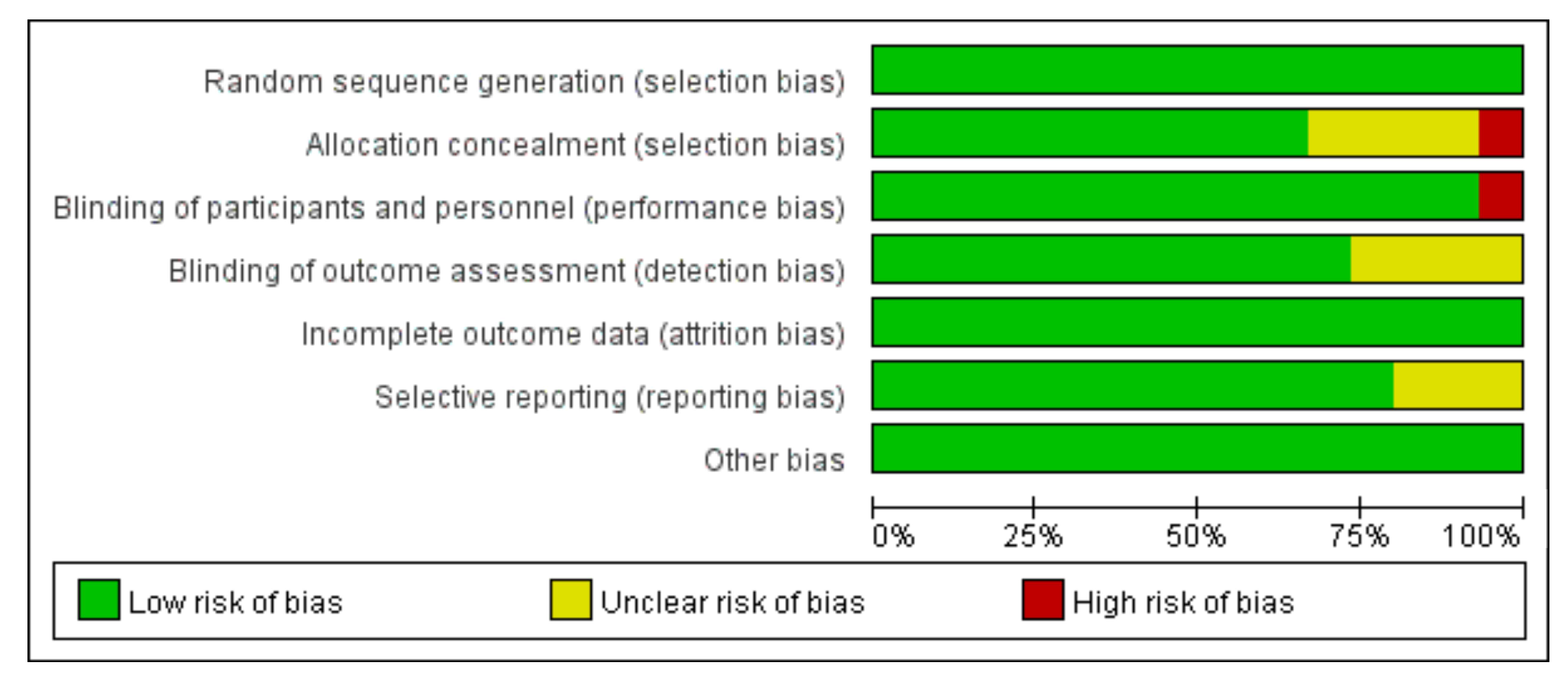
Figure 6.
The risk of bias summary.
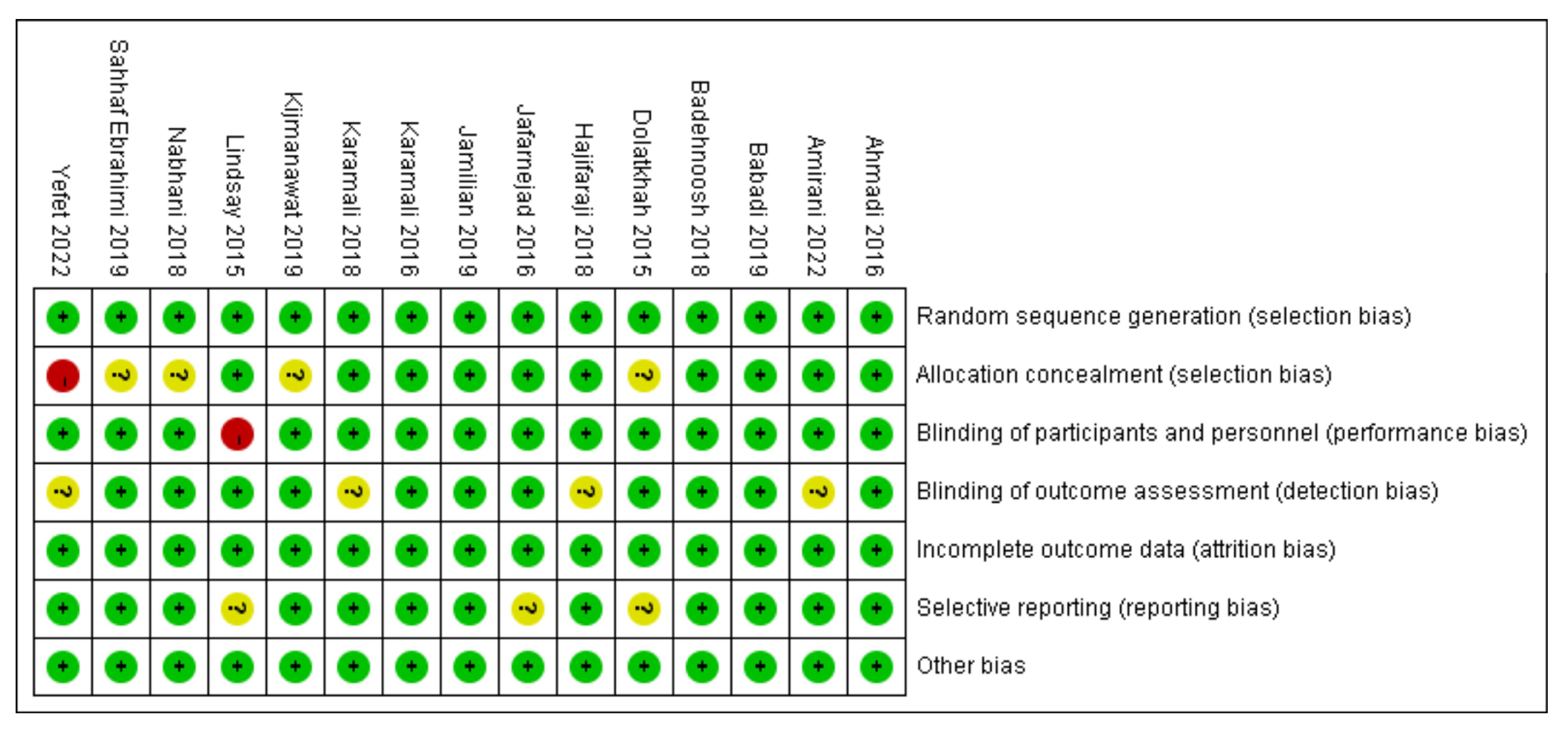

Table 1.
Basic characteristics of eligible studies.
| First authors | Year | Country | Probiotic Intervention | Control Intervention |
Probiotic Dose | Probiotic group(N) |
Control group(N) |
Duration (weeks) |
|---|---|---|---|---|---|---|---|---|
| Dolatkhah | 2015 | Turkey |
Lactobacillus acidophilus LA-5, Bifidobacterium BB-12, Streptococcus thermophilus STY-31 and Lactobacillus delbrueckii bulgaricus LBY-27 |
placebo | 4 biocap>4 × 109 CFU | 29 | 27 | 8 |
| Lindsay | 2015 | Ireland | Lactobacillus salivarius UCC118 | placebo | 1×109 CFU/g | 48 | 52 | 8 |
| Karamali | 2016 | Iran |
L. acidophilus, L. casei and B. bifidum strains |
placebo | 2 × 109 CFU/g each | 30 | 30 | 6 |
| Jafarnejad | 2016 | Iran | VSL#3 (Streptococcus thermophilus, Bifidobacterium breve, Bifidobacterium longum, Bifidobacterium infantis, Lactobacillus acidophilus, Lactobacillus plantarum, Lactobacillus paracasei, and Lactobacillus delbrueckii subsp. bulgaricus) |
placebo | 112.5 × 109 CFU | 37 | 35 | 8 |
| Ahmadi | 2016 | Iran | Lactobacillus acidophilus, Lactobacillus casei, Bifidobacterium bifidum plus 0.8 g inulin | placebo | 2 × 109 CFU/g each | 35 | 35 | 6 |
| Nabhani | 2018 | Iran |
Lactobacillus acidophilus, Lactobacillus plantarum, Lactobacillus fermentum, Lactobacillus gasseri |
placebo |
L. acidophilus(5 × 1010 CFU/g), L. plantarum (1.5 × 1010 CFU/g), L. fermentum(7 × 109 CFU/g), L. gasseri(2 × 1010 CFU/g) |
45 | 45 | 6 |
| Badehnoosh | 2018 | Iran | Lactobacillus acidophilus, Lactobacillus casei and Bifidobacterium bifidum | placebo | 2 × 109 CFU/g each | 30 | 30 | 6 |
| Karamali | 2018 | Iran | Lactobacillus acidophilus, Lactobacillus casei and Bifidobacterium bifidum strains plus 800 mg inulin | placebo | 2 × 109 CFU/g each | 30 | 30 | 6 |
| Hajifaraji | 2018 | Iran | L.acidophilus LA-5, Bifidobacterium BB-12, Streptococcus thermophilus STY-31 and Lactobacillus delbrueckii bulgaricus LBY-27 plus dextrose anhydrous filler and magnesium stearate lubricant | placebo | 4 biocap >4×109 CFU | 29 | 27 | 8 |
| Babadi | 2019 | Iran |
Lactobacillus acidophilus, Lactobacillus casei,Bifidobacterium bifidum, and Lactobacillus fermentum |
placebo | 2 × 109 CFU/g each | 24 | 24 | 6 |
| SahhafEbrahimi | 2019 | Iran | Probiotic yoghurt containing Lactobacillusacidophilus and Bifidobacterium lactis | placebo | 300 g/day of probiotic yoghurt(contained 106 CFU Lactobacillus acidophilus and Bifidobacterium lactis | 42 | 42 | 8 |
| Kijmanawat | 2019 | Thailand |
Lactobacillus acidophilus and Bifidobacterium bifidum |
placebo | 1 × 109 CFU/g each | 28 | 29 | 4 |
| Jamilian | 2019 | Iran |
Lactobacillus acidophilus, Bifidobacterium bifidum, Lactobacillus reuteri, and Lactobacillus fermentum |
placebo | 8 × 109 CFU/day | 29 | 28 | 6 |
| Amirani | 2022 | Iran |
Lactobacillus acidophilus, Bifidobacterium bifidum, Bifidobacterium lactis Bifidobacterium longum Additionally , selenium |
placebo | 2 × 109 CFU/day each | 26 | 25 | 6 |
| Yefet | 2022 | Israel |
Bifidobacterium bifidum, Bifido- bacterium lactis, Lactobacillus (L) acidophilus, L. paracasei, L.rhamnosus and Streptococcus thermophilus |
placebo | 2 capsules/day ( >6×109 CFU/capsule) |
41 | 44 | 2 |
Abbreviations: CFU, colony-forming units.
Table 2.
Results of subgroup analyses based on duration and country.
| Subgroup | Studies | Participants | MD/RR(95% CI) | Heterogeneity (I2%) | p |
|---|---|---|---|---|---|
| FBS | |||||
| Iran | 9 | 592 | -2.26 (-4.35, -0.17) | 64 | 0.03 |
| Non Iran | 3 | 213 | -3.37 (-6.64, -0.10) | 76 | 0.04 |
| Duration ≥ 8weeks | 4 | 312 | -2.56 (-3.64, -1.48) | 87 | < 0.00001 |
| Duration < 8weeks | 8 | 493 | -3.10 (-4.54, -1.66) | 52 | < 0.0001 |
| FSI | |||||
| Iran | 7 | 448 | -2.81 (-3.71, -1.91) | 55 | < 0.00001 |
| Non Iran | 3 | 213 | -0.96 (-1.20, -0.72) | 0 | < 0.00001 |
| Duration ≥ 8weeks | 3 | 228 | -1.01 (-1.25, -0.77) | 85 | < 0.00001 |
| Duration < 8weeks | 7 | 433 | -2.16 (-3.05, -1.26) | 33 | < 0.00001 |
| HOMA-IR | |||||
| Iran | 7 | 448 | -0.70 (-0.93, -0.48) | 44 | < 0.00001 |
| Non Iran | 3 | 213 | -0.29 (-0.34, -0.24) | 0 | < 0.00001 |
| Duration ≥ 8weeks | 3 | 228 | -0.30 (-0.35, -0.24) | 76 | < 0.00001 |
| Duration < 8weeks | 7 | 433 | -0.58 (-0.80, -0.36) | 35 | < 0.00001 |
| QUICKI | |||||
| Iran | 6 | 376 | 0.01 (0.00, 0.01) | 52 | 0.0001 |
| Non Iran | 1 | 56 | Not estimable | Not estimable | Not estimable |
| Duration ≥ 8weeks | 1 | 56 | Not estimable | Not estimable | Not estimable |
| Duration < 8weeks | 6 | 376 | 0.01 (0.00, 0.01) | 52 | 0.0001 |
| Cesarean delivery | |||||
| Iran | 3 | 177 | 0.57 (0.36, 0.89) | 1 | 0.01 |
| Non Iran | 2 | 232 | 1.70 (0.73, 3.97) | 72 | 0.22 |
| Duration ≥ 8weeks | 1 | 147 | 1.16 (0.71, 1.89) | Not estimable | 0.55 |
| Duration < 8weeks | 4 | 262 | 1.16 (0.71, 1.89) | 79 | 0.62 |
| Macrosomia | |||||
| Iran | 4 | 261 | 0.20 (0.07, 0.56) | 0 | 0.002 |
| Non Iran | 1 | 147 | 1.13 (0.64, 2.00) | Not estimable | 0.67 |
| Duration ≥ 8weeks | 2 | 231 | 0.85 (0.51, 1.42) | 72 | 0.53 |
| Duration < 8weeks | 3 | 177 | 0.16 (0.04, 0.71) | 0 | 0.02 |
Abbreviations: FBS, fasting blood sugar; FSI, fasting serum insulin; HOMA-IR, homeostatic model assessment for insulin resistance; QUICKI, the quantitative insulin sensitivity check index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



