
Submitted:
06 September 2023
Posted:
07 September 2023
You are already at the latest version
Abstract
Background: The mental state is important in the health/illness process. Including stress, depression and anxiety. Nature immersion therapies have been implemented as a valid method for reducing these disorders. The aim will evaluate the effect of forest intervention therapies on levels of stress, depression, and anxiety. Methods: We searched for randomized clinical trials related to stress, anxiety and depression levels. Risk of bias was assessed according to the guidelines of the Cochrane Handbook for International Systematic Reviews. Results: We identified and synthesized eight publications. Two studies for cortisol showed significant differences between the pre-test and post-test levels in the intervention groups. One study including Natural killer cells, that reported a significant decrease in the intervention group compared to the control group. Two studies used the Stress Response Inventory, indicated a significant reduction in stress levels in the intervention group compared to the control group. Regarding Restorative Out-come Scale, no significant differences were found. Three studies were selected for the evaluation of anxiety and depression levels according to the Positive and Negative Affect Schedule. Four studies used The Profile of Mood States scale; no significant difference was observed. Conclusions: There is limited evidence to recommend forest bathing for reducing these disorders.
Keywords:
Forests
; cortisol
; natural killer
; blood pressure
; intervention.
1. Introduction
Psychological factors play an important role in the natural history of the development of diseases [1]. Some of those factors, which are referred to as emotional or psychological disorders, include stress, depression, and anxiety [2]; they are among the current major global mental health issues and can affect the outcome of chronic diseases such as diabetes, cardiovascular diseases, cancer, and obesity, among others [3].
Stress is the body’s reaction to feeling threatened or pressured, and it increases susceptibility to inflammatory disorders, including those of infectious aetiology. In this sense, stress may influence different systems, including the immune system and its response [4]. Some authors have proposed that the reaction to stress depends on the stressful condition that is triggered by the individual’s relationship in a social environment [5]. The hormones associated with stress (i.e., cortisol, catecholamines, and gonadotropins) promote adaptation and protect the body in the short term; however, in the long term, the physiological response to stress causes changes in the body, especially in the brain, which can lead to the development of diseases [6].
Anxiety is a condition in which an individual experiences excessive fear, tension, and nervousness over the possibility of something frightful occurring [7]. It can be adaptive or pathological, the latter being characterized by persistent or extensive degrees of anxiety that are associated with distress or psychological impairment [8,9]. Studies have identified that the development of anxiety disorders around the world has ranged from 1.2% to 47% in both young-old and old-old populations [10].
On the other hand, depression is a disabling and life-threatening mental illness that is increasingly affecting large parts of society at an alarming rate worldwide [11]. The World Health Organization (WHO) has reported that depression is one of the most common disorders found among the world population; it is estimated that 5% of adults suffer from depression and that it is one of the main contributors to the global burden of disease [11].
In recent years, nature immersion therapies have been implemented as an alternative method for reducing stress levels, depression, and anxiety [12,13,14]. Authors have proposed that, through exposure to natural environmental stimuli, a state of physiological relaxation can be generated, which may contribute to improving immune functions, thereby aiding in disease prevention [15,16]. Various methodologies of nature immersion therapy have been developed, including Shinrin-Yoku, mindfulness, yoga, physical activity, and Tai-Chi in nature [17,18,19]. “Shinrin-Yoku” can be translated as “assimilating the forest atmosphere through all senses”, also known as forest bathing. This mode of therapy is associated with a plethora of positive health benefits for the human physiological and psychological systems [20,21].
Investigators of Shinrin-Yoku have proposed that the main effects of this treatment include enhancements to the immune system (specifically, increased natural killer-NK cells, reduced allergies) to the cardiovascular system (reduced blood pressure), and also include a decrease in depression and anxiety (control of mood disorders and stress), an increase in mental relaxation (attention deficit hyperactivity disorder), and other beneficial effects [22,23,24].
Although there is evidence that demonstrates the potential for immersion therapies in nature to reduce levels of stress, anxiety, and depression, there have been conflicting results and great methodological variability between studies. Therefore, the present systematic review aims to evaluate the effect of forest intervention therapies on levels of stress, depression, and anxiety.
2. Materials and Methods
This systematic review was designed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [25]. The protocol for the review was registered on the international prospective register for systematic reviews, PROSPERO (CRD42021279423).
2.1. Selection criteria
Randomized clinical trials with healthy participants aged 18 years or older were included in this review. We included studies that performed interventions in natural areas, such as forests, natural parks, urban parks, urban green areas, cultivated fields or gardens, and included walking, observing, performing relaxation exercises, or simply resting and breathing air for a given amount of time. All studies were included regardless of the type of comparison/control group. Finally, we included articles with both physiological outcomes, such as cortisol levels, natural killer cell levels, and blood pressure readings, and psychological outcomes, such as stress, depression, and anxiety levels. Trials that included patients with diseases and clinical studies that performed the intervention using virtual photographs or simulations were excluded.
2.2. Information resources and search strategy
A structured literature search was conducted using PubMed, Scopus, and Lilacs between August and September 2021, and it included all articles published up to the search date in English and Spanish. A search for the following terms was performed: Forests, Relaxation Therapy, Nature, Humans, Walking, Psychological Stress, Physiological Stress, Anxiety, Cortisol, and Blood pressure (Figure S1).
2.3. Study selection and data collection process
The researchers built various search algorithms. The algorithms were tested to determine which one showed the most accurate results for each database. Once the algorithm was selected, the researchers used the Rayyan® web applications to select the articles. At least two independent researchers reviewed each title and abstract. In case of disagreement, a third evaluator settled the differences between the researchers. Later, the full text was read by three of the researchers to extract the relevant information for the study.
Data items were extracted from the included studies, including general characteristics of the study population, such as sex, age, and diseases, a description of the intervention and location of the natural area used for research purposes. In the case of dichotomous outcomes, the number of participants who experienced the event and the total number of participants were extracted. For continuous results, the total number of participants, means, and standard deviations were extracted. Additionally, when cortisol was measured, the matrix in which the determination was made was extracted.
Respecto a los instrumentos psicológicos se incluyeron estudios que midieron alguna de las siguientes escalas: Profile of Mood States questionnaire (POMS); Positive and Negative Affect Schedule (PANAS); restorative Outcome Scale (ROS); Stress Response Inventory (SRI-MF); Perceived Stress Scale - 10 items (PSS10); las cuales han sido las principales reportadas para la medición de estos trastornos psicológicos. POMS, allows a multidimensional evaluation of mood states throughout the transient emotional states: tension/anxiety, depression/rejection, anger/hostility, vigour/activity, fatigue/inertia, and confusion/bewilderment. A total mood disturbance (TMD) score may be calculated by adding the five subscales (tension/anxiety, depression/rejection, anger/hostility, fatigue/inertia, and confusion/bewilderment) and subtracting the subscale vigour [26].
2.4. Risk of bias
The risk of bias was evaluated according to the guidelines of the Cochrane Manual for International Systematic Reviews [27]. The evaluation was performed by three researchers via discussion and consensus. The risk of bias parameters included the type of randomization method (selection bias), allocation concealment (selection bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), and selective reporting (reporting bias). In all cases, a positive answer (+) indicated a low risk of bias, and a negative answer (-) indicated a high risk of bias.
2.5. Strategy for data synthesis and quality of evidence assessment
The analysis of dichotomous and continuous outcomes was performed in Review Manager® software (RevMan, version 5.3., Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) [28]. All pooled analyses were based on the random-effects model. In case of discrepancies, other researchers reviewed the data, checked the differences, and selected the best option.
Identification of heterogeneity: I2 was used for the evaluation of heterogeneity using percentage values of 25, 50, and 75 (low, moderate, and high, respectively) [29].
Sensitivity analysis: The sensitivity analysis was performed using the methodology reported by Sonia et al. [30], and was complemented by funnel plots.
3. Results
3.1. Search results
In total, eighth randomized controlled clinical trials were included (Table 1, Figure 1 and Figure S1). The articles aimed to evaluate two main targets: physiological parameters and psychological outcomes. For the physiological parameters, it was possible to identify two studies where cortisol levels were measured (Jia et al. [31]; Razani et al. [32]), one study focused on evaluating blood pressure (Bang et al. [26]) and one study measuring the effects on NK cells.
Regarding the use of psychological instruments, five articles were included: four studies that performed a stress assessment (Bielinis et al. [33]; Janeczko et al. [34]; Kim et al. [35] and Kim et al. [36]), five studies that focused on evaluating depression levels (Bang et al. [26]; Bielinis et al. [33]; Janeczko et al. [34]; Kim et al. [35,36], and five studies that focused on anxiety levels (Bielinis et al., 2018 [33]; Choe et al. [37]; Janeczko et al. [34]; Kim et al. [35,36]. Table S1 shows the definition and main characteristics that the studies included in this review used in each psychological outcome.
The number of participants varied across studies, ranging from 18 to 99 (median = 64; IQ = 37) (Table 1). The duration of the intervention (forest bathing) varied across studies, ranging from 15 min to two hours. According to the Kappa statistic obtained, there was a substantial agreement for selection by title and abstract (0.62 and 0.67, respectively).
3.2. Risk of bias
Figure 2 shows the results of the quality assessment of the included reviews. The details of the risk of bias according to the Cochrane criteria are shown in Figures S1 and S2. None of the studies met the criteria of the guidelines of the Cochrane Manual for Systematic Reviews (explanation of the selection of study designs) (see Figure S3). In the sensitivity analysis, it was found that all of the studies have a stable estimator.
3.3. Physiological parameters
Two studies identified cortisol as a physiological biomarker of stress parameters. However, the data obtained between the studies could not be analysed statistically because the samples were collected from different matrices. Razani et al. [32] assessed cortisol concentrations in saliva, while Jia et al. [31] assessed cortisol concentrations in blood. Nevertheless, in both studies, they concluded that there was a significant difference in cortisol levels between the pre-test and post-tests in the intervention group (Table S2).
One study (Bang et al. [26] including blood pressure measurements met the criteria for inclusion, and it involved the comparison of a forest intervention group with a control group without any type of intervention. No significant difference (p>0.05) in blood pressure levels were observed between the intervention group and the control group in the Pre-test data for systolic and diastolic pressure; while a significant difference were obtained in Post-test values for systolic pressure (p=0.001). The delta between the pre- and post-intervention systolic blood pressure was 0.4 mmHg (pre-test = 111.55 mmHg, and post-test = 112.02 mmHg), and the delta between the pre- and post-intervention diastolic blood pressure was 0.82 mmHg (pre-test = 68.47 mmHg, and post-test = 69.29 mmHg).
The only study involving NK that was included in the review (Jia et al. [31]) reported a significant decrease in the proportion of NK cells in the forest group after a forest bathing intervention (Pre-test = 93.72; Post-test = 55.07; p<0.001), compared to no change in the proportion of NK cells in the urban group (Pre-test = 87.93; Post-test = 70.05; p>0.05).
3.4. Psychological parameters
3.4.1. Scales used to evaluate stress
Four studies attempting to evaluate stress as an outcome measure [33,34,35,36] were identified. Among those studies, two different scales were used to measure stress response levels (Figure 3). Kim et al. (2020 [35] and 2021 [36]) used the Stress Response Inventory (SRI-MF), which utilizes a total of 22 items, The SRI-MF results indicated a significant reduction in stress levels for a nature immersion therapy intervention group compared to a control group (MD= −7.87 [95% CI: −9.44, −6.30]; I2 = 0%) (Figure 3a).
3.4.2. Scales used to evaluate anxiety and depression
The Positive and Negative Affect Schedule (PANAS) is a questionnaire used to measure two types of emotional affect that are either positively or negatively related to anxiety and depression disorders. The PANAS consists of 20 items that include adjectives associated with common feelings and emotions for the two aforementioned emotional affects.
Three studies were selected for the evaluation of anxiety and depression levels ac-cording to the PANAS scale, however only two studies were used to perform the Forest plot (Figure 4), because the study conducted by Choe et al. [37], used different criteria to obtain the results of this scale, and therefore, the data obtained were not comparable with the other studies (Table S1). Choe et al. [37] interpreted the scale using a mean of 25 (minimum value = 10 and maximum value = 50). The mental health and well-being outcomes were higher when they were performed in a natural outdoor environment than when they were performed in indoor or built environments (positive aspects with a mean = 33.70, 95% CI: 30.84; 36.55, p= 0.049; and negative aspects with a mean = 20.12, 95% CI: 17.69; 22.55, p< 0.001). Moreover, the natural outdoor environment group showed sustained improvements one month after the completion of the intervention.
Specifications related to the possible variation in temperature, humidity, and noise throughout the intervention were not quantified; in summary, the authors reported a single measurement of those variables. However, that variation could represent a significant effect on participants [38]. Notably, there has not been evidence from previous systematic reviews that critically evaluated the effect of forest baths on mental health by using the PANAS scale [39,40,41,42]. Therefore, it is considered relevant to deepen the evaluation of the sensitivity and specificity of this type of intervention through longitudinal studies that implement a more robust study design and allow for later evaluation of those results by meta-analysis.
The Profile of Mood States (POMS), consists of 65 items. Four eligible studies that used the POMS scale were identified, and their results are shown in the Figure 5. Nevertheless, it was evident that, there were variations in the criteria used to evaluate the scales between the studies, which represented a limitation for a comparison between the four studies [33,34,35,36]. Therefore, the analysis by subgroup was performed as follows: the first subgroup contained the Bielinis et al. [33] and Janeczko et al. [34] studies; while the second subgroup contained the Kim et al. [35,36] studies. No significant difference was observed among the studies using the POMS scale (I2 = 96%; Figure 5a) (Kim et al. [35,36]). The intervention groups showed a significant benefit compared to the control groups (I2 = 0%; Figure 5b).
4. Discussion
Our review summarizes the evidence from previous systematic reviews that assess the health effects of forest-based interventions. We identified and synthesized a total of eight publications, mostly from Asian countries, however, the results of this review were inconclusive, and therefore do not allow defining the effect of these therapies on levels of stress, anxiety or pressure; the above as a possible result of variations in the types of intervention change, variations in the sample sizes, changes in the methodology used to obtain the results of each of the scales, lack of clarifications in the way participants allotolize, among others.
In the selected studies, a diverse methodology was presented regarding the development of the intervention. For example, Kim et al. [35] implemented eight sessions (one per week for six weeks) with a duration of 1 to 2 hours, and Kim et al. [36] showed the development of a routine (exercises, meditation, walking and breathing) that was executed in one of the eight sessions. Bielinis et al. [33] implemented a 15-minute intervention that consisted of walking in a forest area (intervention group) and walking for 15 minutes in an urban area (control group). That walk was only implemented once, yet Janeczko et al. [34] developed an intervention that included four different scenarios (apartments, green spaces in the suburbs, coniferous forest, and deciduous forest), for which we selected the apartment setting (control group) and the coniferous forest setting (intervention group) for the analysis. However, that study does not specify the duration of the intervention.
Upon waking, the levels of cortisol should increase by 50-60%, then begin a rapid decay in the following hours, followed by a slow decay at nightfall [43]; however, a flat cortisol rhythm is associated with depression; in this review only one of the studies met the inclusion criteria (Jia et al. [31]); in which a decrease in cortisol concentration in the forest group was observed after the intervention compared to the initial measurement; whereas in the control group no differences were found between both measurements. Nevertheless, it is important to highlight that, this study does not specify in its methodology details as the sample collection, thus making it difficult to analyse and compare the studies. Additionally, one of the selected studies measured cortisol in saliva and the other measured cortisol in the blood, causing the scales of the results to be incomparable to each other, thus representing a limitation in this study.
Forest therapies have been shown to result in an increase in the activity of NK [44,45,46] and a reduction in blood pressure [47,48]. However, NK does not always show significant responses to the intervention, possibly due to the short intervention time (1 week). Bang et al. [26] did not report significant differences between the control and experimental groups in the post-tests analysis for blood pressure.
Regarding mental health, several reviews showed positive effects on stress, depression, and anxiety in healthy people after forest-based interventions. This is consistent with the results of studies showing a reduction in psychological stress after forest viewing and forest walking [40,41,42]. The scores for the ROS scale for the Bielinis et al. [33] and Janeczko et al. [34] studies showed a significant increase after forest-based interventions when compared to pre-intervention. Some review studies have shown that scores on the ROS scale increase as a result of recreation and relaxation in the forest areas [24,41]. In those two studies, an increase in ROS scores was observed after walking and watching in forest areas when compared to pre-intervention scores. However, Bielinis et al. [33] noticed a decrease in ROS scores after walking and watching in urban areas when compared to pre-intervention scores.
The PANAS scale is the most widely and frequently used scale to assess positive affect and negative affect [49]. The results reported in the selected studies were controversial. In one study, positive affect was significantly higher in the forest environment, which contributed to the mental health of participants [33]. However, Chloe et al. [37] did not report significant differences between environments for negative or positive affect; likewise, in the second study included in this review, no significant differences were found for the positive affect, but significantly decreased results were obtained in the post-tests for the negative affect [34].
The application of the POMS scale in the selected articles is varied. In the studies of Kim et al. [35,36], the methodology of the application of the instrument is not clear [35,36]. Bielinis et al. [33] administered the POMS scale 15 minutes before and 15 minutes after therapy. Janeczko et al. [34] presented their results based on three stratifications: by time, by site, and site*time; however, they do not attempt to explain those stratifications in their methodology section. Additionally, two studies did not report the total mood disturbance, causing the need for us to calculate those data, which could have introduced bias in the analysis.
In addition, we found that the studies reported a statistically significant reduction in the levels of anxiety and depression as measured by the POMS scale. However, when comparing studies, we found that the methodologies for immersion in nature are diverse in duration, periodicity, and evaluation (I2 > 75).
This review presented certain limitations; after carrying out the analysis of the findings, a lack of concordance between the results was evident, which may be due to the lack of rigor in the design of these studies. For example, none of the three included studies that reported PANAS results specified the program or methodology used to perform population randomization in the two study groups. One of these three studies did not specify the duration of the intervention. On the other hand, there was a lack of control of biases in studies focused on forest bathing interventions, which directly affects the results obtained and increases heterogeneity between studies. Based on the above, it is evident that it is necessary to generate research with a rigorous study design that allows obtaining reliable data.
5. Conclusions
There is only limited evidence to recommend forest bathing for reducing stress, blood pressure, anxiety and other physiological outcomes. Further studies should be carried out in different locations, as well as include a cost efficacy analysis. Formulating an of-ficial research protocol will enable the design of better future RCT studies.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org., Figure S1: Search algorithms, Figure S2: Summary of methodological quality: reviewers’ judgements about each item of methodological quality for each included study, and Figure S3: Funnel plots for a visual assessment of publication bias. Description: funnel plot: a) Restorative Outcome Scale (ROS); b) Stress Response Inventory; c) Positive and Negative Affect Schedule (positive affect); d) Positive and Negative Affect Schedule (negative affect); and e) Profile of Mood States. Table S1. Definition of psychological outcomes. Table S2: Cortisol study results, Jia et al. [31] (blood cortisol) and Razani et al. [32] (salivary cortisol), ng/mL.
Author Contributions
Conceptualization, D.M.P, N.V, J. MR; methodology, D.M.P, A.PL, E.T, C.P, L.B, C.G, J. C, J. MR, Y.T and N.V.; software, D.M.P, A.PL, E.T, C.P, L.B, C.G, J.C, J.MR, Y.T, and N.V; validation, D.MP, A.PL, Y.T, N.V, and J. MR; formal analysis, D.M.P, A.LP, Y.T, N.V, and J.MR; investigation, D.M.P, A.PL, Y.T, N.V, and J.MR.; resources, J.MR.; data curation, J.MR.; writing—original draft preparation, D.M.P, A.PL, Y.T, N.V, and J.MR.; writing—review and editing, D.M.P, A.PL, Y.T, N.V, and J.MR; visualization, D.M.P, A.PL, Y.T, N.V, and J.MR; supervision, J.MR.; project administration, J.MR.; funding acquisition, J.MR.
Funding
this research was funded by the Instituto Nacional de Salud of Colombia (INS-CPS-025-2022, INS-CPS-119-2022).
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
We thank researcher Diana Pinzon for her support in decision making for the selection of the articles described in this review. Likewise, we thank the entire research team of the Environmental and Occupational Health Group of the Instituto Nacional de Salud of Colombia, for the support presented during different stages of writing this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Vigo, D.; Thornicroft, G.; Atun, R. Estimating the True Global Burden of Mental Illness. The Lancet Psychiatry 2016, 3, 171–178. [CrossRef]
- Vujcic, M.; Tomicevic-Dubljevic, J.; Grbic, M.; Lecic-Tosevski, D.; Vukovic, O.; Toskovic, O. Nature Based Solution for Improving Mental Health and Well-Being in Urban Areas. Environmental Research 2017, 158, 385–392. [CrossRef]
- Yeshaw, Y.; Mossie, A. Depression, Anxiety, Stress, and Their Associated Factors among Jimma University Staff, Jimma, Southwest Ethiopia, 2016: A Cross-Sectional Study. NDT 2017, Volume 13, 2803–2812. [CrossRef]
- Dhabhar, F.S. Effects of Stress on Immune Function: The Good, the Bad, and the Beautiful. Immunol Res 2014, 58, 193–210. [CrossRef]
- Melchior, M; Caspi, A; Milne, B.J; Danese, A; Poulton, R; Moffitt, T.E. Work Stress Precipitates Depression and Anxiety in Young, Working Women and Men. Psychological Medicine 2007, 37, 1119–1129. [CrossRef]
- Eppelmann, E; Parzer, P; Salize, H; Voss, E; Resch, F; Kaess, M. Stress, Mental and Physical Health and the Costs of Health Care in German High School Students. Eur Child Adolesc Psychiatry 2020, 29, 1277–1287. [CrossRef]
- Mutepfa, M; Motsamai, T; Wright, T; Tapera, R; Kenosi, L. Anxiety and Somatization: Prevalence and Correlates of Mental Health in Older People (60+ Years) in Botswana. Aging Ment Health 2021, 5, 2320–2329. [CrossRef]
- Kroenke, K; Spitzer, R.L; Williams, J.B; Monahan, P.O.L.B. Anxiety Disorders in Primary Care: Prevalence, Impairment, Comorbidity, and Detection. Ann. Intern. Med. 2007, 146, 317–325. [CrossRef]
- Testa, A; Giannuzzi, R; Sollazzo, F; Petrongolo, L; Bernardini, L.D.S. Psychiatric Emergencies (Part I): Psychiatric Disorders Causing Organic Symptoms. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 55–64.
- Canuto, A; Weber, K; Baertschi, M; Andreas, S; Volkert, J; Dehoust, M. Anxiety Disorders in Old Age: Psychiatric Comorbidities, Quality of Life, and Prevalence According to Age, Gender, and Country. Am J Geriatr Psychiatry 2018, 26, 174–185. [CrossRef]
- Morres, I; Hatzigeorgiadis, A; Stathi, A; Comoutos, N; Arpin-Cribbie, C; Krommidas, C; Theodorakis, Y. Aerobic Exercise for Adult Patients with Major Depressive Disorder in Mental Health Services: A Systematic Review and Meta-Analysis. Depress Anxiety 2019, 36, 39–53. [CrossRef]
- Lim, P.Y.; Dillon, D.; Chew, P.K.H. A Guide to Nature Immersion: Psychological and Physiological Benefits. IJERPH 2020, 17, 5989. [CrossRef]
- Hunter, M.R.; Gillespie, B.W.; Chen, S.Y.-P. Urban Nature Experiences Reduce Stress in the Context of Daily Life Based on Salivary Biomarkers. Front. Psychol. 2019, 10, 722. [CrossRef]
- Choi, H.; Jeon, Y.-H.; Han, J.-W.; Moon, J.; Kim, S.-Y.; Woo, J.-M. The Effects of a Forest Therapy on Work-Related Stress for Employees in the Manufacturing Industry: Randomized Control Study. Glob Adv Health Med 2022, 11, 2164957X2211004. [CrossRef]
- Miyazaki, Y; Song, C; Ikei, H. Preventive Medical Effects of Nature Therapy and Their Individual Differences. J. Physiol. Anthropol 2015, 20, 19-32.
- Lee, J; Li, Q; Tyrvainen, L; Tsunetsugu, Y; Park, B.J; Kagawa, T; Miyazaki, Y. Nature Therapy and Preventive Medicine. Social and Behavioral Health 2012, 325–350.
- Smyth, N.; Rossi, E.; Wood, C. Effectiveness of Stress-Relieving Strategies in Regulating Patterns of Cortisol Secretion and Promoting Brain Health. Int Rev Neurobiol 2020, 150, 219–246. [CrossRef]
- Ibes, D.; Hirama, I.; Schuyler, C. Greenspace Ecotherapy Interventions: The Stress-Reduction Potential of Green Micro-Breaks Integrating Nature Connection and Mind-Body Skills. Ecopsychology 2018, 10. [CrossRef]
- Clarke, F.;Kotera, Y.; McEwan, K. A Qualitative Study Comparing Mindfulness and Shinrin-Yoku (Forest Bathing): Practitioners’ Perspectives. Sustainability 2021, 13. [CrossRef]
- Selhub, E.M; Logan, A.C. Your Brain on Nature: The Science of Nature’s Influence on Your Health, Happiness and Vitality; 2012;
- Craig, J.M; Logan, A.C; Prescott, S.L. Natural Environments, Nature Relatedness and the Ecological Theater: Connecting Satellites and Sequencing to Shinrin-Yoku. J. Physiol. Anthropol. 2016, 35. [CrossRef]
- Loureiro, G; Rabaça, MA; Blanco, B; Andrade, S; Chieira, C.P.C. Urban versus Rural Environment--Any Differences in Aeroallergens Sensitization in an Allergic Population of Cova Da Beira, Portugal? Eur Ann Allergy Clin Immunol 2005, 37, 187–193.
- LI, Q. Effect of Forest Bathing Trips on Human Immune Function. Environ Health Prev Med 2010, 15, 9–17. [CrossRef]
- Wen, Y; Yan, Q; Pan, Y; Gu, X.L.Y. Medical Empirical Research on Forest Bathing (Shinrin-Yoku): A Systematic Review. Environ Health Prev Med 2019, 24, 70. [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700–b2700. [CrossRef]
- Bang, K.-S.; Lee, I.; Kim, S.; Lim, C.S.; Joh, H.-K.; Park, B.-J.; Song, M.K. The Effects of a Campus Forest-Walking Program on Undergraduate and Graduate Students’ Physical and Psychological Health. IJERPH 2017, 14, 728. [CrossRef]
- Higgins, J; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; 2014; [CrossRef]
- RevMan Available online: https://training.cochrane.org/online-learning/core-software/revman (accessed on 7 September 2022).
- Catalá-López, F. Metaanálisis de ensayos clínicos aleatorizados, heterogeneidad e intervalos de predicción. 5.
- Pértega, S.; Pita, S. Guía: Revisiones Sistemáticas y Metaanálisis (II) - Fisterra Available online: https://www.fisterra.com/formacion/metodologia-investigacion/revisiones-sistematicas-metaanalisis-ii/ (accessed on 7 September 2022).
- Jia, B.; Yang, Z.; Mao, G.; Lyu, Y.; Wen, X.; Xu, W.; Lyu, X.; Cao, Y.; Wang, G. Health Effect of Forest Bathing Trip on Elderly Patients with Chronic Obstructive Pulmonary Disease. Biomed Environ Sci 2016, 29, 212–218. [CrossRef]
- Razani, N.; Morshed, S.; Kohn, M.A.; Wells, N.M.; Thompson, D.; Alqassari, M.; Agodi, A.; Rutherford, G.W. Effect of Park Prescriptions with and without Group Visits to Parks on Stress Reduction in Low-Income Parents: SHINE Randomized Trial. PLoS ONE 2018, 13, e0192921. [CrossRef]
- Bielinis, E.; Takayama, N.; Boiko, S.; Omelan, A.; Bielinis, L. The effect of winter forest bathing on psychological relaxation of young Polish adults. Urban Forestry & Urban Greening 2018, 29, 276–283. [CrossRef]
- Janeczko, E.; Bielinis, E.; Wójcik, R.; Woźnicka, M.; Kędziora, W.; Łukowski, A.; Elsadek, M.; Szyc, K.; Janeczko, K. When Urban Environment Is Restorative: The Effect of Walking in Suburbs and Forests on Psychological and Physiological Relaxation of Young Polish Adults. Forests 2020, 11, 591. [CrossRef]
- Kim, J.G.; Khil, T.G.; Lim, Y.; Park, K.; Shin, M.; Shin, W.S. The Psychological Effects of a Campus Forest Therapy Program. IJERPH 2020, 17, 3409. [CrossRef]
- Kim, J.G.; Jeon, J.; Shin, W.S. The Influence of Forest Activities in a University Campus Forest on Student’s Psychological Effects. IJERPH 2021, 18, 2457. [CrossRef]
- Choe, E.Y.; Jorgensen, A.; Sheffield, D. Does a Natural Environment Enhance the Effectiveness of Mindfulness-Based Stress Reduction (MBSR)? Examining the Mental Health and Wellbeing, and Nature Connectedness Benefits. Landscape and Urban Planning 2020, 202, 103886. [CrossRef]
- Zhu, S.; Hu, F.; He, S.; Qiu, Q.; Su, Y.; He, Q.; Li, J. Comprehensive Evaluation of Healthcare Benefits of Different Forest Types: A Case Study in Shimen National Forest Park, China. Forests 2021, 12, 207. [CrossRef]
- Kotera, Y.; Richardson, M.; Sheffield, D. Effects of Shinrin-Yoku (Forest Bathing) and Nature Therapy on Mental Health: A Systematic Review and Meta-Analysis. Int J Ment Health Addiction 2022, 20, 337–361. [CrossRef]
- Oh, B.; Lee, K.J.; Zaslawski, C.; Yeung, A.; Rosenthal, D.; Larkey, L.; Back, M. Health and Well-Being Benefits of Spending Time in Forests: Systematic Review. Environ Health Prev Med 2017, 22, 71. [CrossRef]
- Rajoo, K.S.; Karam, D.S.; Abdullah, M.Z. The Physiological and Psychosocial Effects of Forest Therapy: A Systematic Review. Urban Forestry & Urban Greening 2020, 54, 126744. [CrossRef]
- Stier-Jarmer, M.; Throner, V.; Kirschneck, M.; Immich, G.; Frisch, D.; Schuh, A. The Psychological and Physical Effects of Forests on Human Health: A Systematic Review of Systematic Reviews and Meta-Analyses. IJERPH 2021, 18, 1770. [CrossRef]
- Contreras, C.M.; Gutierrez-Garcia, A.G. Cortisol Awakening Response: An Ancient Adaptive Feature. J Psychiatry Psychiatric Disord 2018, 02, 29–40. [CrossRef]
- Morita, E.; Fukuda, S.; Nagano, J.; Hamajima, N.; Yamamoto, H.; Iwai, Y.; Nakashima, T.; Ohira, H.; Shirakawa, T. Psychological Effects of Forest Environments on Healthy Adults: Shinrin-Yoku (Forest-Air Bathing, Walking) as a Possible Method of Stress Reduction. Public Health 2007, 121, 54–63. [CrossRef]
- Song, C.; Ikei, H.; Park, B.-J.; Lee, J.; Kagawa, T.; Miyazaki, Y. Association between the Psychological Effects of Viewing Forest Landscapes and Trait Anxiety Level. IJERPH 2020, 17, 5479. [CrossRef]
- Antonelli, M.; Barbieri, G.; Donelli, D. Effects of Forest Bathing (Shinrin-Yoku) on Levels of Cortisol as a Stress Biomarker: A Systematic Review and Meta-Analysis. Int J Biometeorol 2019, 18. [CrossRef]
- Maund; Irvine; Reeves; Strong; Cromie; Dallimer; Davies Wetlands for Wellbeing: Piloting a Nature-Based Health Intervention for the Management of Anxiety and Depression. IJERPH 2019, 16, 4413. [CrossRef]
- Ideno, Y.; Hayashi, K.; Abe, Y.; Ueda, K.; Iso, H.; Noda, M.; Lee, J.-S.; Suzuki, S. Blood Pressure-Lowering Effect of Shinrin-Yoku (Forest Bathing): A Systematic Review and Meta-Analysis. BMC Complement Altern Med 2017, 17, 409. [CrossRef]
- Díaz-García, A.; González-Robles, A.; Mor, S.; Mira, A.; Quero, S.; García-Palacios, A.; Baños, R.M.; Botella, C. Positive and Negative Affect Schedule (PANAS): Psychometric Properties of the Online Spanish Version in a Clinical Sample with Emotional Disorders. BMC Psychiatry 2020, 20, 56. [CrossRef]
Figure 1.
PRISMA diagram of articles selected for review.
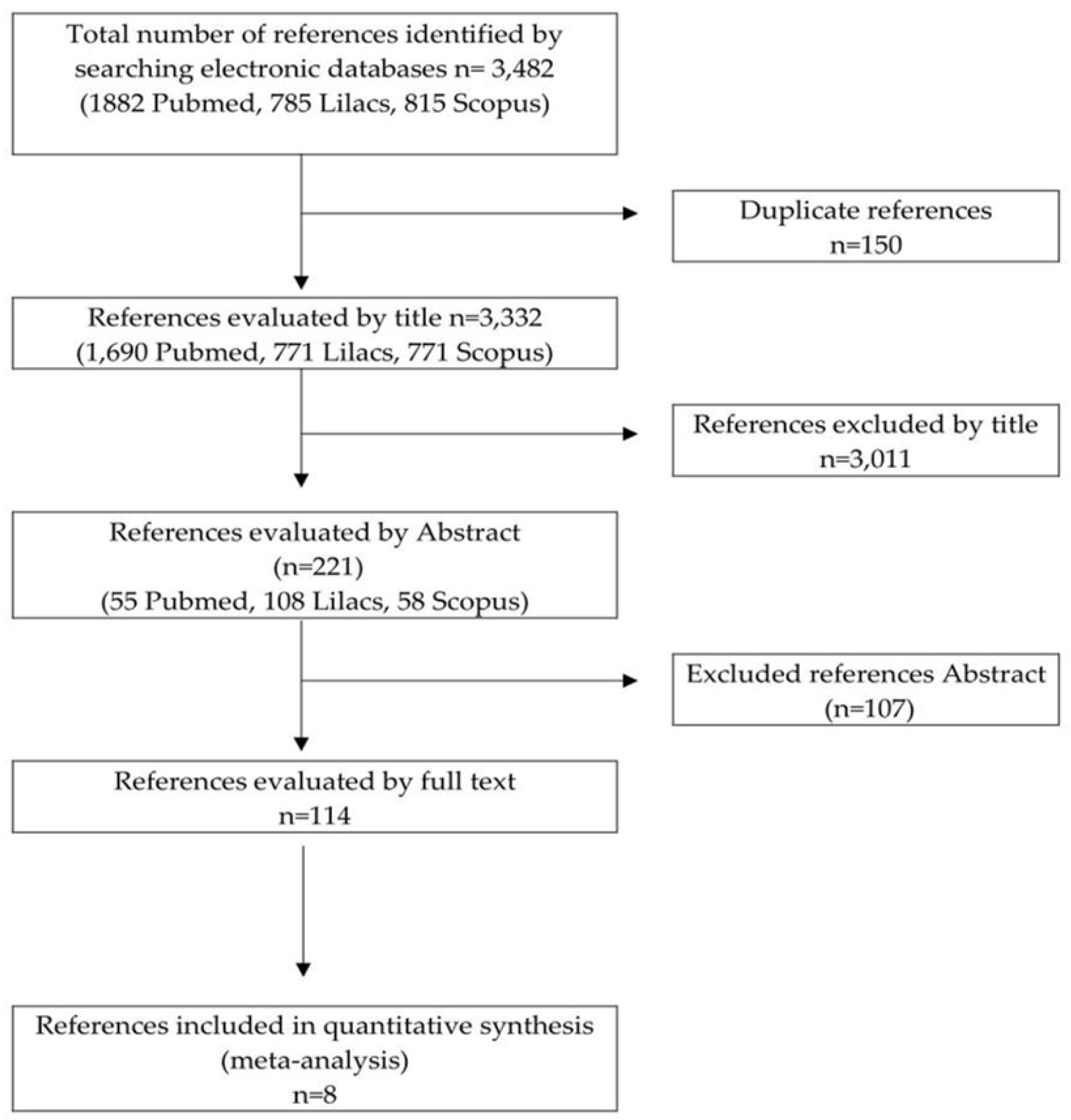
Figure 2.
Graph of methodological quality: Reviewers’ evaluations on each item of methodological quality are presented as percentages for all included studies.
Figure 2.
Graph of methodological quality: Reviewers’ evaluations on each item of methodological quality are presented as percentages for all included studies.
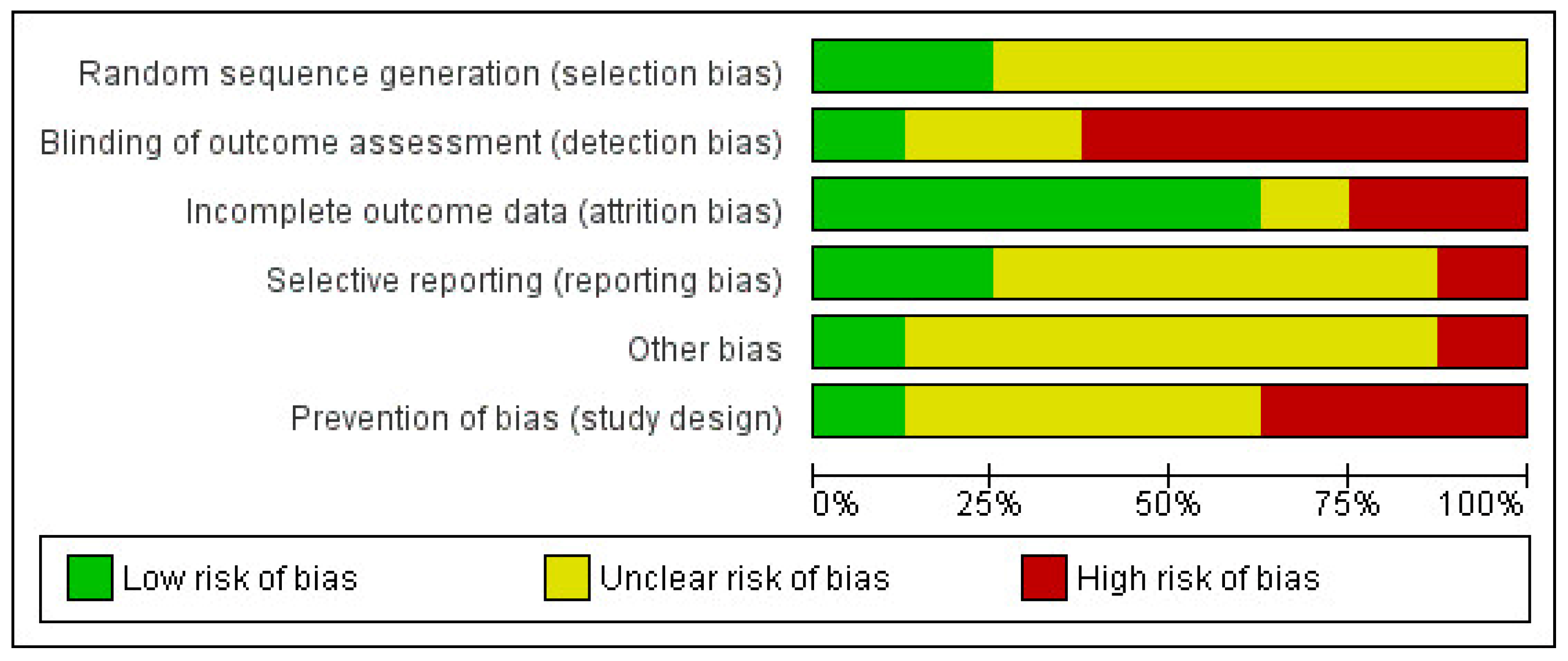
Figure 3.
A forest plot of two scales was used to measure stress pretest and posttest with a comparison between forest interventions (experimental group) and urban interventions (control group). a) SRF-MF and b) ROS. The figure summarizes the mean difference with inverse variance (IV), 95% confidence interval (95% CI), and the risk of bias. A random-effect model was adopted to estimate subgroup and overall size effects.
Figure 3.
A forest plot of two scales was used to measure stress pretest and posttest with a comparison between forest interventions (experimental group) and urban interventions (control group). a) SRF-MF and b) ROS. The figure summarizes the mean difference with inverse variance (IV), 95% confidence interval (95% CI), and the risk of bias. A random-effect model was adopted to estimate subgroup and overall size effects.
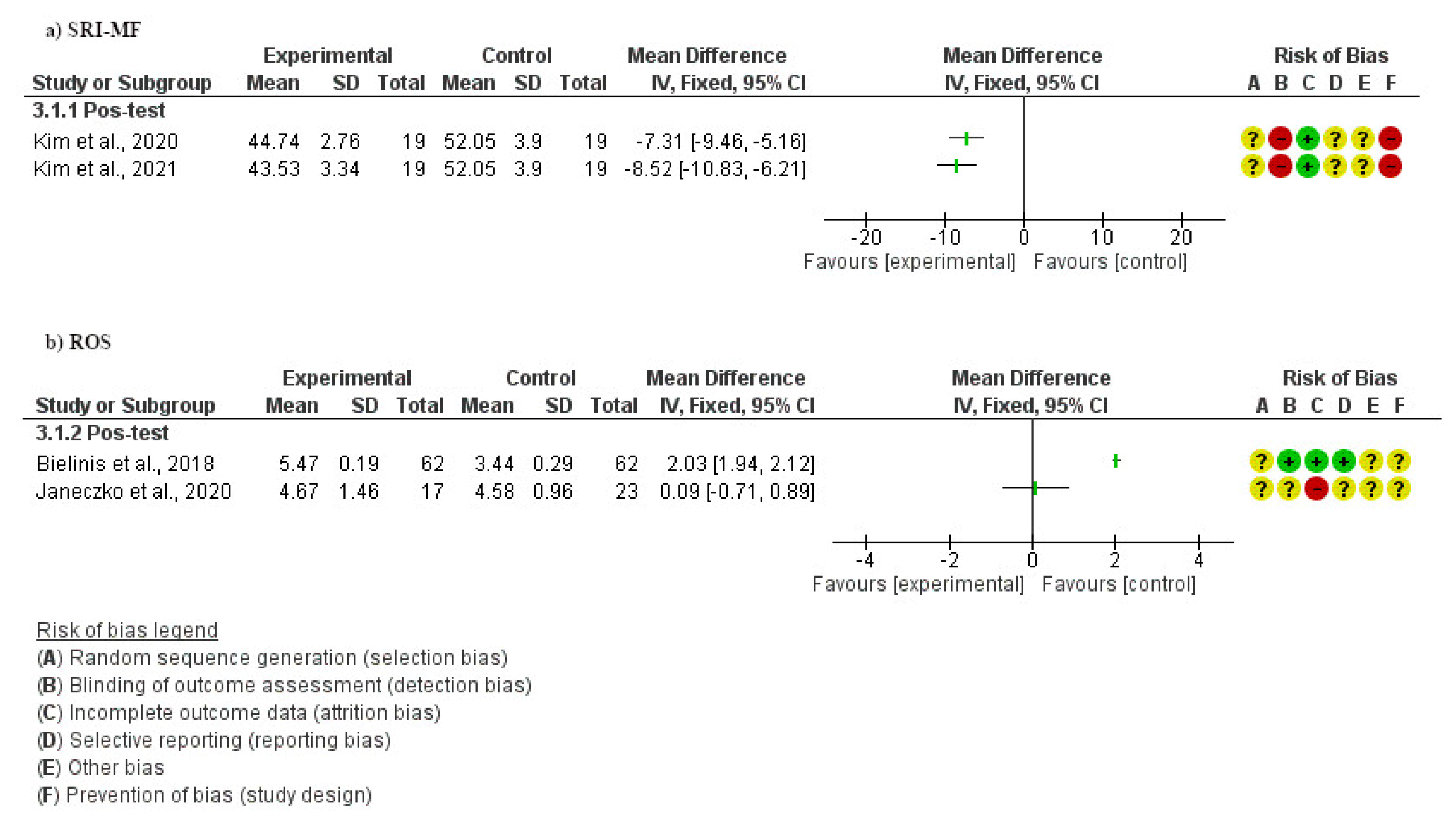
Figure 4.
Forest plot of a) positive aspects and b) negative aspects of PANAS pre-test and post-test with a comparison between forest intervention (experimental group) and urban intervention (control group). The figure summarizes the mean difference with inverse variance (IV), 95% confidence intervals (CI), and the risk of bias, and a random-effect model was adopted to estimate subgroup and overall size effects.
Figure 4.
Forest plot of a) positive aspects and b) negative aspects of PANAS pre-test and post-test with a comparison between forest intervention (experimental group) and urban intervention (control group). The figure summarizes the mean difference with inverse variance (IV), 95% confidence intervals (CI), and the risk of bias, and a random-effect model was adopted to estimate subgroup and overall size effects.
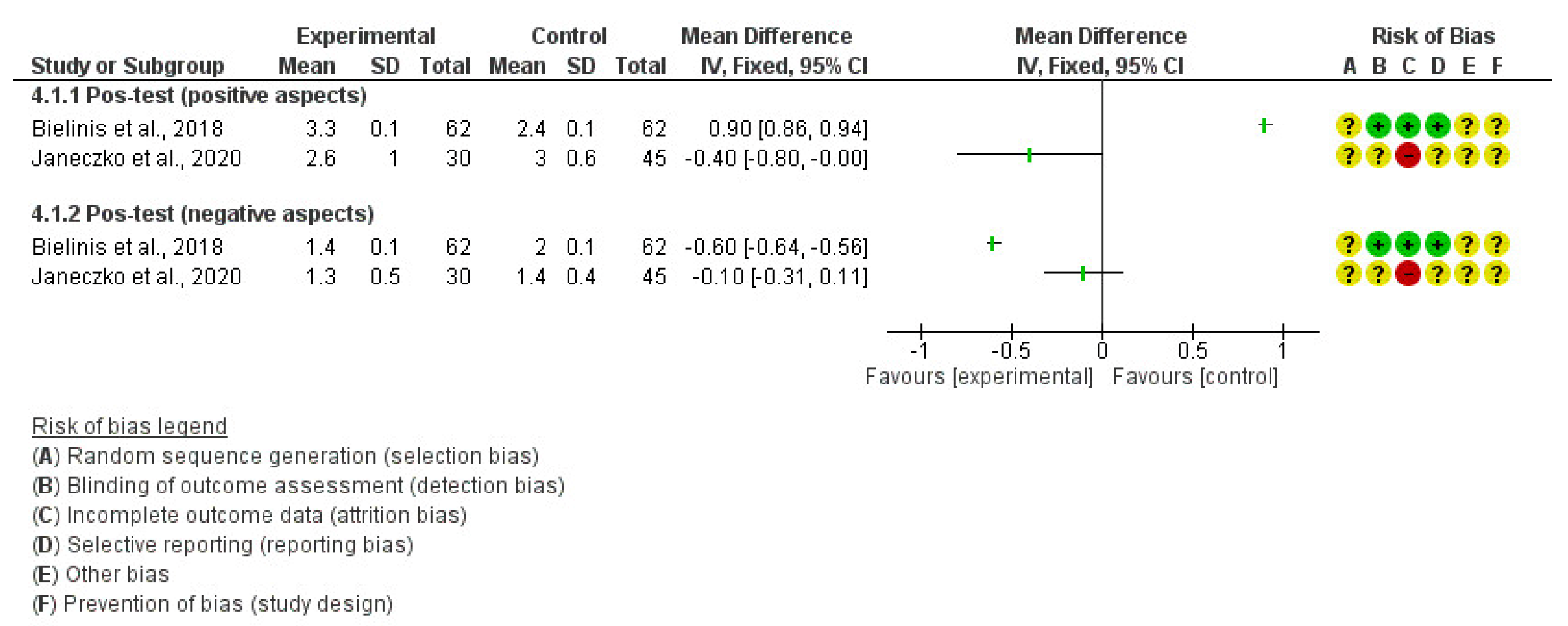
Figure 5.
Forest plot of the profile of mood states (POMS), pretest and posttest with a comparison between forest intervention (experimental group) and urban intervention (control group). The figure summarizes the mean difference with inverse variance (IV), 95% confidence interval (CI), and the risk of bias, and a random-effect model was adopted to estimate subgroup and overall size effects.
Figure 5.
Forest plot of the profile of mood states (POMS), pretest and posttest with a comparison between forest intervention (experimental group) and urban intervention (control group). The figure summarizes the mean difference with inverse variance (IV), 95% confidence interval (CI), and the risk of bias, and a random-effect model was adopted to estimate subgroup and overall size effects.
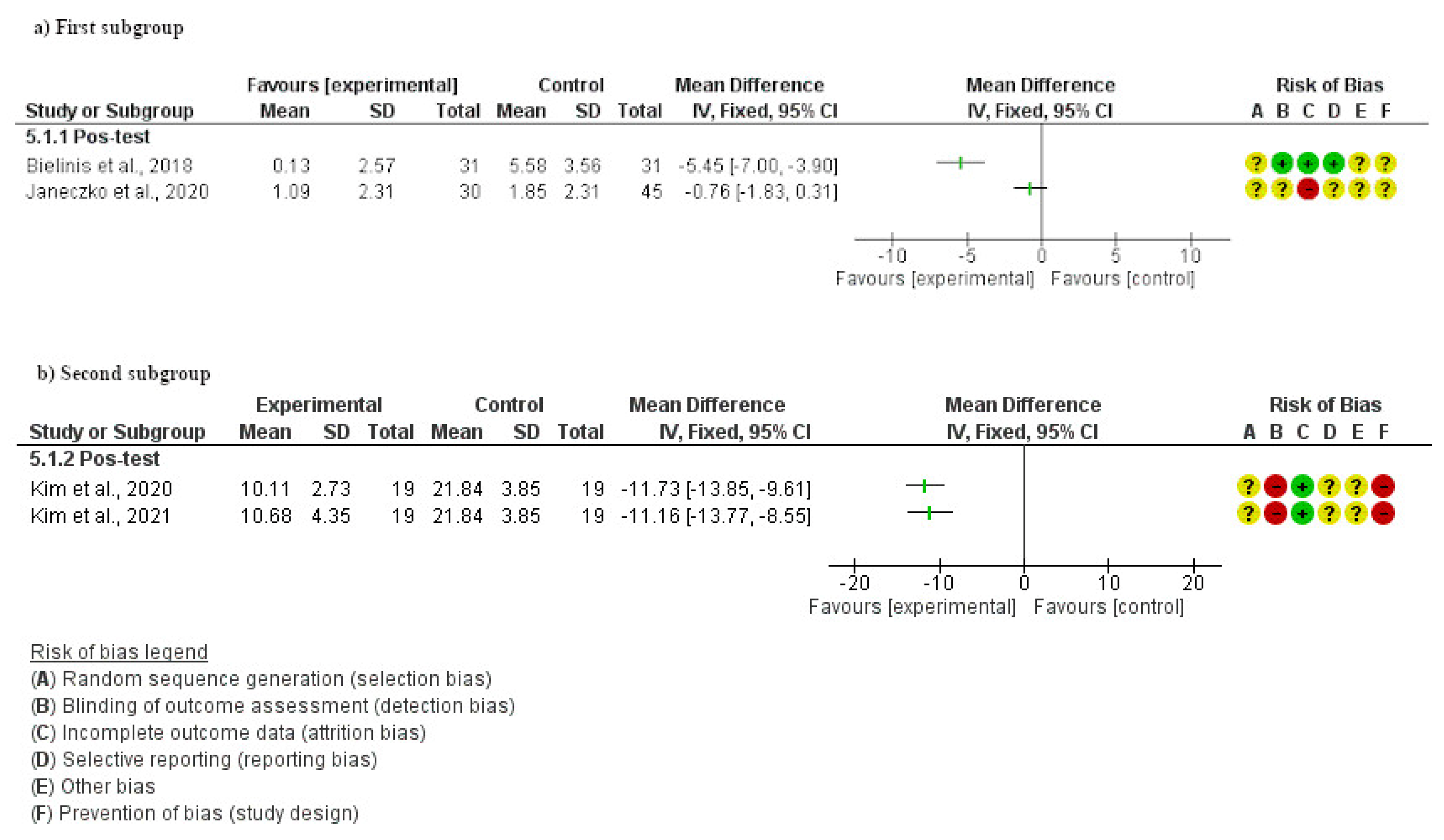

Table 1.
Data from the included studies.
| Reference (Country) | N | Age | Control group | Intervention group | Outcomes (unit) | Duration of the intervention | Full description of the intervention |
|---|---|---|---|---|---|---|---|
| Mean ±SD | |||||||
| Bang et al. [26] (South Korea) | 99 | 24.3 ± 4.19 | No intervention | Forest therapy | Physiological: | 6 weeks | The campus forest-walking program was conducted once per week during lunch. The university campus has many different trees, and there are nearby forest roads and trails. |
| M = 21 | M = 26 | Blood pressure (mm Hg) | |||||
| F = 27 | F = 25 | ||||||
| Bielinis et al. [33] (Poland) | 62 | 21.5 ± 0.18 | City intervention | Forest therapy | Psychological: POMS, PANAS and ROS. | 1 day | The field experiment was winter season. Two locations were selected: the urban and the forest environment (deciduous, broad-leaved urban forest situated near the city centre). |
| M = 18 | M = 18 | ||||||
| F = 13 | F = 13 | ||||||
| Jia et al. [31] (China) |
18 | 61-79 | City intervention | Forest therapy | Physiological: Cortisol (ng/mL) | 7 days | The study was performed at two different sites (forest and city). On the day before the study, the blood samples were taken from the participants in the morning before breakfast. |
| M/F = 8 | M/F = 10 | Natural Killer (%) | |||||
| Choe et al. [37] (United Kingdom) | 66 | 16-62 | Indoor environment | Natural environment | Psychological: PANAS | 6 weeks | The study consisted of an experiment of three different environments: natural outdoor, built outdoor and indoor environments. The intervention was in groups of between 6 and 10 participants. Each weekly session lasted one hour and included mindfulness meditation/exercises and group discussion. |
| M/F = 33 | M/F = 33 | ||||||
| Janeczko et al. [34] (Poland) | 75 | 19-24 | Urban area | Forest therapy | Psychological: POMS, PANAS and ROS. | 1 day | The outdoor experiment was conducted in four different settings: 1) an urban environment with a noticeably higher level of noise, 2) the scenery of urban housing, 3) the Sobieski Forest, and 4) a coniferous forest. |
| M/F = 45 | M/F = 30 | Physiological: Blood pressure (mmHg). | |||||
| Kim et al. [35] (South Korea) |
38 | 22 | No intervention M/F = 19 | Forest | Psychological: POMS and SRI-MF | 2 months | An eight-session forest therapy program was performed once per week, and each session lasted for 1.5 hours. Participants were involved in many activities, such as forest dance, forest meditation, forest exercise, walking, and others. The main purpose of the program was to reduce stress and improve the self-esteem of the participants. |
| M/F = 19 | |||||||
| Kim et al. [36] (Korea) | 38 | 22.1 ± 1.6 | No intervention | Forest therapy | Psychological: POMS and SRI-MF. | 8 weeks | The participants were instructed to perform individualized, voluntary forest activities for one hour-long session per week. The activities included stretching, breathing, walking, meditation, and exercise. |
| M/F = 19 | M/F = 19 | ||||||
| Razani et al. [32] (United States) | 75 | >18 | Independent park prescription | Supported park prescription | Psychological: PSS10 | 3 weeks | The outdoor experiment was conducted in three different sceneries: a bayfront park with a beach, a lake with woodlands, and a redwood forest. Outings concluded with quiet reflection and an opportunity to share experiences. |
POMS: Profile of Mood States questionnaire; PANAS: Positive and Negative Affect Schedule; ROS: Restorative Outcome Scale; SRI-MF: Stress Response Inventory; PSS10: Perceived Stress Scale - 10 items; M: male; F: female; SD: standard deviation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



