
Submitted:
06 September 2023
Posted:
08 September 2023
You are already at the latest version
Abstract
Oral pyogenic granuloma (PG) is generally a solitary benign connective tissue proliferation of unknown etiology. It is the most common type of oral inflammatory hyperplasia histologically characterized by proliferation of granulation tissue with inflammatory infiltrates and high angiogenic capacity. Vascular neoformations of different diameters are usually present. Due to their structural characteristics, tendency to bleed, and rapid and alarming growth rate, these neoformations may have serious consequences. Sometimes, it is complex to make an accurate diagnosis. Therefore, adequate management and treatment are based on the characteristics and systemic conditions of each patient. This review was carried out to provide an overview of the factors involved in, or attributed to the etiopathogenesis of oral PG. It describes the different forms of presentation and clinical evolution, as well as the most frequent signs and symptoms that characterize this disease, while incorporating recent radiographic and microscopic findings. In addition, it describes the different modalities for the management of oral pyogenic granuloma depending on the particular characteristics of each patient.
Keywords:
Pyogenic granuloma
; Hyperplastic lesion
; Lobulated capillary hemangioma.
1. Introduction
Pyogenic granuloma (PG) is a benign connective tissue proliferation that is predominantly characterized by granulation tissue hyperplasia, and it occurs frequently in the skin or mucous membranes [1,2,3,4]. It is considered as one of the most common lesions responsible for soft tissue enlargements, due to its rapid and alarming growth rate [1,5,6,7].
Pyogenic granuloma (PG) was first described in 1897 by Poncet and Dor, who reported four patients with “vascular tumors” on the fingers which they named “Botrichomycosis hominis” [8]. The term “pyogenic granuloma” was introduced in 1904 by Hartzell. However, the name is considered inappropriate as it is neither related to pus formation, nor is it histologically a true granuloma [2,8,10]. Due to the controversy regarding its true pathological nature, this lesion has been given several names such as granuloma pediculatum benignum, benign vascular tumor, septic granuloma, hemangiomatous granuloma, vascular epulis, fibroangioma, polypoid capillary hemangioma, eruption capillary hemangioma, non-lobular capillary hemangioma, and Crocker and Hartzell’s disease [2]. In pregnant women, GP is identified as pregnancy granuloma, pyogenic granuloma of pregnancy, or granuloma gravidarum [11]. In the dermatological literature, Cawson et al. (1998) have described this disease as “granuloma telangiectacticum” due to the presence of numerous blood vessels observed in histological sections. Some pyogenic granulomas (also known as lobular capillary hemangiomas) are categorized as vascular tumors, according to the classification of the International Society for the Study of Vascular Anomalies (ISSVA, 2022).
Given that PG is a common lesion in the oral cavity, this article was aimed at reviewing its prevalence, etiopathogenesis, clinical picture, radiographical and histopathological features, as well as its differential diagnosis and treatment.
2. Epidemiology
There are some discrepancies in the epidemiological pattern of this pathology. Oral PG manifests within the range of 4.5 to 93 years, and it shows a preeminent incidence in the second and fifth decades, with the female gender often being more affected than the male gender [3,4]. On the other hand, some researchers have suggested that this disease manifests mostly in males younger than 18 years and in females aged 18–39 years, with equal gender distribution in older patients [10]. With regard to its prevalence, in a retrospective study conducted at the Oral and Maxillofacial Pathology Department, Faculty of Dentistry, Shiraz University of Medical Sciences in Iran, analysis was done on 1000 biopsies of gingival lesions, out of which 92.4% of the cases were found to be non-neoplastic lesions. The most common reports were related to reactive lesions (71.8%), with the highest PG-associated prevalence of 24.6% [12,13]. In their descriptive study of 427 patients, PG accounted for 50.35% of all reactive oral cavity lesions reported at Dharwad Dental Institute in Karnataka, India. Shammin et al. (2008) analyzed 244 cases of gingival lesions at the Department of Oral Pathology, Government Dental College, Calicut, India, and reported that non-neoplastic lesions comprised 75.5% of the cases, out of which PG accounted for 52.7%. A descriptive study of 923 Iranian pregnant women revealed that only 2 of them (0.22%) presented with PG [15]. On the other hand, a 4.2% PG prevalence has been reported in this group of patients in a medical center in Kerman/Iran [16]. These discrepancies in prevalence could be attributed to the differences in diagnostic methods applied. The diagnosis in [16] was based only on the clinical picture of the lesion, while Tabatabaei et al. (2014) implemented confirmation through histopathological studies.
3. Etiopathogenesis
Some factors are implicated in the etiopathogenesis of PG. However, the exact cause is unknown. Historically, some researchers consider it to be a pathology attributable to an infectious agent, hence the term “pyogenic” [3,18]. Kerr in 1951 was of the view that the factors that influence the progression of PG were bebotryomycosis, staphylococci, foreign particles, and the accumulation of infection in the endothelium of blood vessels. In a study by Bhaskar & Jacoway, Gram-positive and Gram-negative bacilli were identified in GP. However, these microorganisms could be members of the oral microbiota, since they were more frequent in ulcerated lesions than in non-ulcerated lesions [20]. On the other hand, in 2001, Lee & Lynde pioneered the establishment of statistically significant association between Bartonella seropositivity and PG, which has important therapeutic implications. This association suggested the possibility of non-surgical treatment with an antibiotic such as erythromycin. In addition, they suggested that such treatment may also decrease recurrence and satellitosis of PG.
Several researchers define the PG as a “reactive” or “reparative” process. Regezi et al. consider PG a reactive or repairing process in which a certain stimulus generates an exuberant proliferation of connective tissue [2,3]. The etiological factors considered as stimuli that trigger this reactive process are trauma, dental calculus, dental biofilm, chronic irritation, pre-existing vascular lesions, chronic irritation due to exfoliation of primary teeth, injury of a primary tooth, eruption of permanent teeth, defective restorations in the area of the lesion, occlusal interference, food impaction, periodontitis, and trauma from toothbrushing [2,3,7]. These factors are summarized in Figure 1.
Pyogenic granuloma (PG) may manifest after a hypersensitivity reaction associated with the use of drugs such as calcineurin inhibitors (cyclosporine and tacrolimus), carbamazepine, phenytoin, nifedipine, levothyroxine and ramucirumab [21,22,23,24,25,26,27,28,29]. Additionally, PG is associated with retinoid, antineoplastic and antiretroviral agents [21]. The mechanism involved in the presence of PG following hematopoietic cell transplant (HCT) is unknown. Cheney & Lund described 5 cases of pediatric patients who developed oral PG after HCT, under treatment with the calcineurin inhibitors cyclosporine A or tacrolimus. It has been suggested that the side effect of cyclosporine, which is less common in tacrolimus, is the proliferation of fibroblasts, thereby generating increased collagen synthesis in the oral mucosa, resulting in triggering of a critical gingival hyperplasia that leads to PG. Moreover, there is an increase in the level of connective tissue growth factor [23,29]. Cyclosporine decreases the productions of collagenase and matrix metalloproteinases, and also up-regulates the expressions of the inhibitors of these metalloproteinases, thereby playing a crucial role in tissue growth. These hyperplastic effects on the gums may be implicated in the development of PG associated with calcineurin inhibitors [22]. Cheney et al. (2016) described a case series in which they included 5 pediatric/adolescent patients who developed oral PG after HCT for acute lymphoblastic leukemia, Fanconi anemia, nodular sclerosis Hodgkin’s lymphoma, or junctional epidermolysis bullosa. It was suggested that calcineurin inhibitors which are used for graft versus host disease, play a crucial role due to irritation and chronic inflammatory changes in the oral cavity, leading to tissue proliferation, and eventually to PG formation. Regarding carbamazepine, the release of angiogenic factors stimulated by the inflammatory process and the impairment of liver functions contribute to the development of PG [24]. Levothyroxine has been considered a possible etiological factor in PG through its pro-angiogenic and proliferative effects [25]. Piraccini et al. (2010) reported that a side effect in psoriasis or acne patients treated with retinoids (systemic isotretinoin, systemic etretinate, systemic acitretin, topical retinoic acid, and topical tazarotene) is the appearance of periungual PGs. Retinoids decrease the attachments amongst keratinocytes, exert angiogenic properties, and inhibit the activities of collagenases and gelatinases in vitro [21,30]. Antiretrovirals, particularly indinavir and lamivudine, are associated with the presence of PG in the nail folds, and the time of appearance varies from 2 months to 1 year from the initiation of therapy [21,26]. It has been suggested that protease inhibitors may have a retinoid-like effect by virtue of homologies between the amino acid sequences of cellular retinoic acid binding protein 1 (CRABP1) and the catalytic site of HIV-1 protease. Thus, the specific retinoid receptor may be occupied and activated by the antiretroviral agent, thereby increasing the activity of vitamin A and its analogues [31]. Multiple PGs have been described in metastatic carcinoma patients treated with antineoplastic drugs (epidermal growth factor receptor inhibitors, capecitabine, cyclosporin, docetaxel, and mitoxantrone) [21]. Aragaki et al. (2021) described 2 clinical cases with the presence of oral PG during administration of ramucirumab for gastric cancer. Ramucirumab, an entirely human IgG1 monoclonal antibody, favors the appearance of this pathology (PG) by generating systemic deterioration of the angiogenic balance and local deterioration of the oral environment.
Hormonal changes, especially in estrogen and progesterone during puberty and pregnancy, may promote the development of PG or pregnancy granuloma. Increased levels of these hormones during puberty deteriorate already established gingival inflammation by increasing the dilation and proliferation of blood vessels and releasing vasoactive mediators from damaged mast cells [2,32]. In pregnancy in particular, these hormonal changes have been associated with vascular, microbiological, cellular and immunological modifications which generate a favorable environment for the initiation and development of PG [11,32,33,34]. The hormones estrogen, progesterone and chorionic gonadotropin induce certain alterations in the microcirculatory system, including swelling of endothelial cells, increased adhesion of platelets and eukocyte to vessel walls, formation of microthrombi, disruption of perivascular mast cells, increased vascular permeability, and vascular proliferation [32,33] (Figure 2). The oral microbiota may present changes characterized by an increase in the proportion of anaerobic and aerobic bacteria such as Bacteroides melaninogenicus, Prevotella intermedia, and Porphyromonas gingivalis. Thus, high levels of Fusobacterium nucleatum and Aggregatibacter actinomycetemcomitans have also been observed, particularly in the second and third trimesters of pregnancy [11,32,33,35,36]. The cellular changes comprise a decrease in the keratinization of the gingival epithelium, an increase in epithelial glycogen, proliferation of fibroblasts, and a blockage in collagen degradation, leading to changes in the epithelial barrier that result in an increased response against irritating factors, especially dental biofilm [33]. Progesterone may act as an immunosuppressant in the periodontal tissues of pregnant women, thereby preventing the appearance of an acute inflammatory response to an irritant stimulus. However, it allows an increase in chronic tissue reactions which clinically results in an exaggerated appearance of inflammation [37]. Additionally, there is a decrease in the antimicrobial activity of peripheral neutrophils which constitute essential components of the innate immune defenses of periodontal tissues. All these changes result in the exacerbation of the prevalence and/or severity of some pathologies in the oral cavity during pregnancy, particularly in the tissues, especially from the second month onwards, because it is exactly at this point that elevations in plasma estrogen and progesterone levels occur [32,34].
The imbalance between angiogenesis enhancers and inhibitors is one of the hypotheses for the etiopathogenesis of PG. It highlights the important role of certain factors such as basic fibroblast growth factor (bFGF), vascular endothelial growth factor (VEGF), tyrosine kinase with immunoglobulin-like, EGF-like domains-2 (Tie-2), angiopoietin-1 (Ang-1), angiopoietin-2 (Ang-2), ephrin-B2 and Eph-B4 in the processes involved in adult inflammatory neovascularization [38,39]. On the other hand, Shetty et al. (2020) reported that PG is triggered by the presence of local and/or systemic factors that generate the release of various endogenous substances (tumor cell angiogenic factors and vascular morphogenic factors), leading to alterations in the vascular system of the affected area [40]. Decorin is an integral component of new capillaries in in vivo angiogenesis, especially angiogenesis associated with severe inflammation. Nelimarkka et al. (2001) have demonstrated that decorin is present in the endothelial cells of capillary neovessels in PGs and in the granulation tissue of healing dermal wounds.
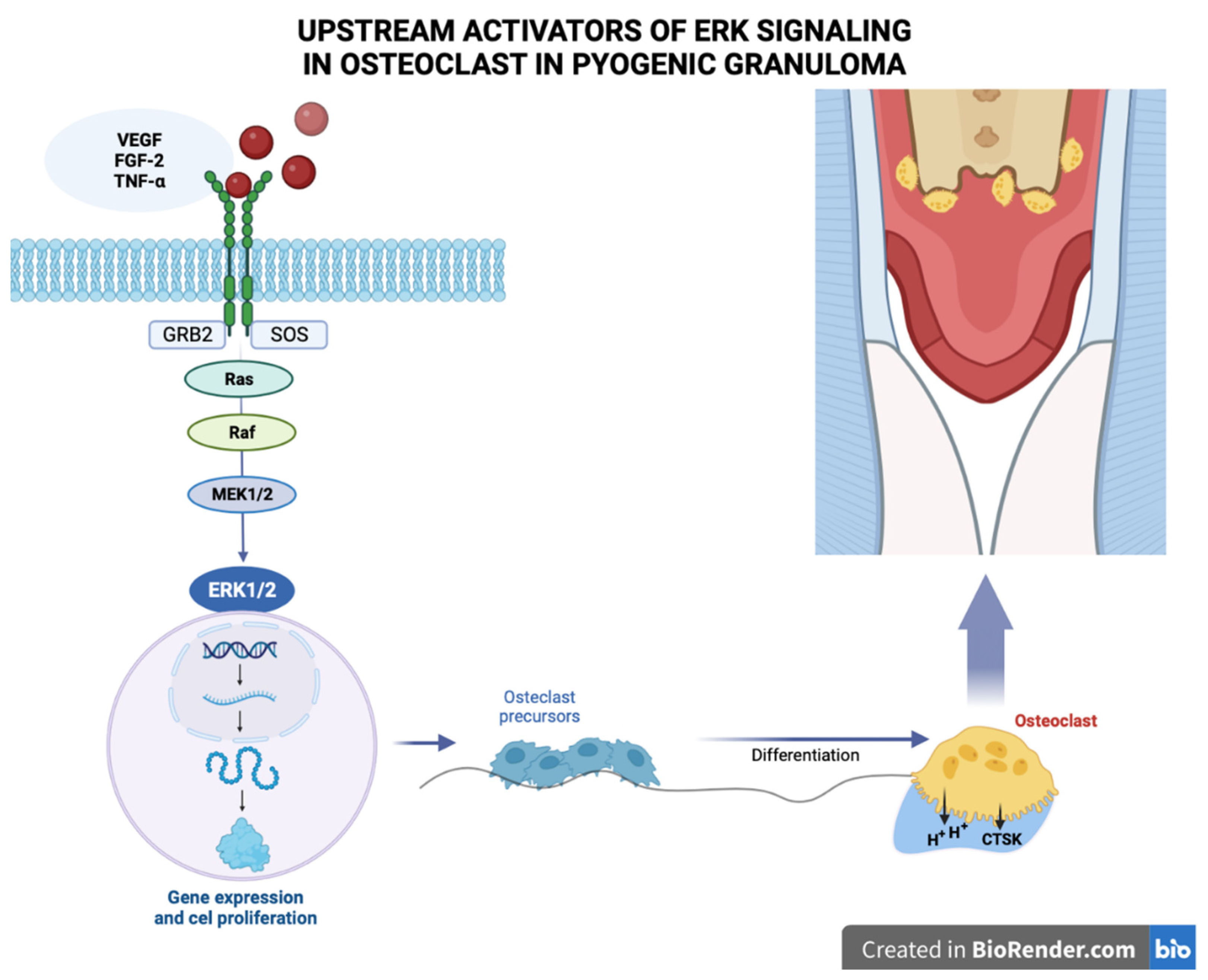
Pyogenic granuloma (PG) is considered a neovascular hyperplastic response in which inducible nitric oxide synthase expression, increased VEGF expression, and low apoptotic rate expression of Bax/Bcl-2 proteins have been reported [40]. In this regard, Blackwell et al. [2016] demonstrated the expressions of embryonic stem cell markers, i.e., OCT4, SOX2, pSTAT3 and NANOG, suggesting that the endothelium of PG shows a primitive phenotype. Chen et al. (2008) found over-expressions of phosphorylated (p)-activating transcription factor-2 (p-ATF2) and phosphorylated (p)-signal transducer and activator of transcription-3 (p-STAT3) in cutaneous angiosarcoma and PG. Additionally, activation of the MAPK/ERK pathway demonstrated by immunohistochemical evidence for phospho-ERK1/2 positivity, has been identified in oral PG endothelial cells (Figure 3). However, further studies are needed to elucidate the mechanism involved [43].
4. Clinical features
Pyogenic granuloma (PG) occurs most often in the skin or in the oral cavity, but rarely in the gastrointestinal tract, trachea, urinary bladder, and central nervous system [27,44]. In the oral cavity, the gingiva accounts for 75% of the sites of predilection of this pathology. However, PG may occur in other areas such as the lips, tongue, buccal mucosa, hard plate and peri-implant mucosa, and it affects the maxilla more than the mandible, the anterior region more than the posterior region, with the buccal surfaces more affected than the lingual surfaces [2,3,45]. In the literature, the floor of the mouth is not considered as a site of occurrence of PG. This is perhaps due to the fact that in addition to the absence of sufficient amount of connective tissue in the mucosa of the floor of the mouth, the tongue protects this region from traumatic injury [46].
Oral PG is a pathology that manifests as a raised, smooth or exophytic growth on a sessile or pedunculated broad base with a smooth and lobulated surface covered with red hemorrhagic and erythematous compressible papules which appear lobulated and warty, complete with ulcerations and covered by a yellow brackish membrane [2,10,27,45]. The surface of the pathology is frequently ulcerated in areas subjected to trauma, and due to its pronounced vascularity, occasional bleeding may occur, especially during mastication. The clinical course of PG is generally slow, asymptomatic and painless [2,27]. The growth of PG is slow, and it takes from weeks to months to reach optimal size [10,27]. As shown in Table 1, the size of PG may vary in diameter from a few millimeters to several centimeters [2,10,27]. The color of this pathology depends on its age: younger PGs tend to be reddish due to the large number of blood vessels, while older ones appear pink in color. The consistency of the oral PG depends on the age of the lesion: as the lesion matures, collagen fibers increase in number, and the lesion becomes firm [27,47].
5. Radiographic features
Oral PG generally does not present radiographic findings: some authors make a presumptive diagnosis with the clinical features. Thus, most of the clinical cases described in the literature do not present radiographic analysis and/or description. However, some authors have reported bone loss or erosion of the alveolar ridge associated with the area where the PG is located [48,57,58,60,61,62,63,64,65,66] (Table 1).
The molecular mechanisms leading to bone loss or erosion associated with oral PG are unclear. However, PG is a benign inflammatory lesion that expresses significantly more VEGFs and basic fibroblast growth factors than healthy gingiva and periodontitis [38]. Growth factors such as fibroblast growth factor-2, growth arrest-specific gene 6, and TNF-α, among other molecules, stimulate mature osteoclast function and survival through activation of extracellular signal-regulated kinase (ERK), resulting in degradation or resorption of organic and inorganic bone components [18]. The ERK signaling pathway has been associated with the regulation of osteoclasts with respect to survival, proliferation, apoptosis, formation, polarity, podosome disassembly, and differentiation [18].
This signaling cascade constitutes the core of three serially-phosphorylated protein kinases. Activation of Raf isoforms through the Ras-Raf interaction stimulates MAPKK, MEK1 and MEK2, and then activates ERK1 and ERK2 via dual phosphorylation at the conserved Thr-Glu-Tyr (TEY) motif, leading to phosphorylation of various downstream substrates [18,67,68]. Among the latter are c-Fos, NFATc1, MITF, TFE3, Hedgehog-Gli, Egr2, RSK2 and MMp-9, which ultimately activate the ERK signaling pathway [18]. Pereira et al. (2019) reported MAPK/ERK pathway activation, as demonstrated by the immunohistochemical positivity of phospho-ERK1/2 in oral PG endothelial cells. Future research should focus on elucidating the molecular mechanisms that trigger PG-associated bone loss or erosion, particularly the role of the MAPK/ERK pathway in this process (Figure 3).
6. Microscopic features
Most PGs are constituted by a lobular mass of hyperplastic granulation tissue representing a non-neoplastic proliferation formed by abundant vascular spaces, young fibroblasts, and infiltration of acute and/or chronic inflammatory cells with lymphocytes, plasma cells, histiocytes, and polymorphonuclear cells in a collagen matrix. This entity is partially or totally covered by parakeratotic or non-keratinized stratified squamous epithelium. Ulcerated lesions exhibit an extensive fibrin layer in the epithelium [2,27].
7. Differential diagnosis of oral PG
The features used for differential diagnosis of oral PG include red or reddish-blue growths such as gingival hyperplasia, peripheral giant cell granuloma, hemangiomas, conventional granulation tissue, peripheral ossifying fibroma, peripheral odontogenic fibroma, metastatic cancer, Kaposi’s sarcoma, bacillary angiomatosis, angiosarcoma, and non-Hodgkin’s lymphoma [2,3,4,10,27].

Table 1.
Reviewed articles.
| Year | Author | Country | Age (Years) |
Gender | Location | Consistency | Comorbidity | Radiographic | Lesion size | Diagnosis | Treatment |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Features | |||||||||||
| 2001 | Akyol et al., 2001 [46] | Turkey | 4 m | B | Tongue | Soft | No | NA | 1 x 0.8 x 0.8 cm | H | Surgical excision |
| 2002 | Aguilo L. 2002 [56] | Spain | 19 m | B | Gingiva | Soft | No | Fracture of the crown of 61 | NA | H | Surgical excision |
| 2006 | Parisi E et al., (2006) [73] | USA | 33 | F | Gingiva | NA | NA | NA | 0.5 x 0.5 cm | H | Intralesional corticosteroids |
| 2006 | Patil et al., 2006 [84] | India | 50 | F | Lower Lip | NA | No | NA | 1 x 0.5 cm | H | Surgical excision |
| 2006 | Shenoy S. 2006 [64] | India | 8 | G | Gingiva | NA | NA | loss of alveolar crestal bone | 2.0 x 1.0 x 1.0 cm | H | Surgical excision |
| 2008 | Amirchaghmaghi et al., 2008 [85] | Iran | 16 | M | Hard palate | Firm | No | NA | 0.7 cm | H | Surgical excision |
| 2009 | Goncalves 2009 [101] | Brazil | 12 | F | Upper lip | NA | NA | NA | 1.0 cm | H | Surgical excision |
| 2009 | Olmedo D et al., (2009) [86] | Argentina | 75 | F | Peri-implant mucosa | NA | No | No abnormalities | 1.0 x 1.0 x 0.6 cm | H | Surgical excision |
| Argentina | 64 | F | Peri-implant mucosa | Firm | No | Bone loss | 0.6 x 0.5 x 0.4 cm | H | Surgical excision | ||
| 2010 | Gondivkar et al., 2010 [61] | India | 25 | F | Gingiva | Soft | Pregnancy | Alveolar bone loss | 3 x 7 cm | H | Surgical excision |
| 2010 | Rizwanulla et al., 2010 [87] | Nepal | 13 | F | Gingiva | Firm | No | NA | 2.0 x 1.0 x 1.0 cm | H | Surgical excision |
| 2011 | Behl et al., 2011 [60] | India | 60 | F | Gingiva | Firm | No | Vertical bone loss | 3.2 x 3.4 cm | H | Surgical excision |
| 2011 | Mubben et al., 2011 [102] | India | 63 | F | Gingiva | Soft | No | NA | 5.0 x 3.5 cm | H | Surgical excision |
| 2011 | Penseriya et al. 2011 [88] | India | 30 | M | Gingiva | NA | No | Interdental bone loss | 2.0 x 1.5 cm | H | Surgical excision |
| 2011 | Shivaswamy et al., 2011 [65] | India | 19 | M | Gingiva and palate | Soft | NA | Horizontal bone loss | 4.0 x 5.0 mm | H | Surgical excision |
| 2012 | Chandrashekar 2012 [69] | India | 28 | F | Gingiva | Soft | No | NA | NA | H | Surgical excision |
| 2012 | Panjwani et al., 2012 [50] | India | 69 | M | Tongue | Firm | No | NA | 2.0 x 3.0 cm | H | Surgical excision |
| 2012 | Ravi et al., 2012 [89] | India | 33 | M | Lower lip | Firm | NA | NA | 3.0 x 2.0 cm | H | Surgical excision |
| 2012 | Piscoya et al., 2012 [90] | Brazil | 44 | M | Lower lip | NA | NA | NA | NA | H | Surgical excision |
| 2012 | Verma et al., 2012 [62] | India | 30 | F | Gingiva | NA | No | Alveolar bone loss | 1.5 x 1.0 cm | H | Surgical excision |
| 2013 | Adusumilli et al., 2013 [91] | India | 24 | F | Gingiva | Firm | NA | NA | 2 x 3.5 cm | H | Surgical excision |
| 27 | F | Gingiva | Firm | NA | NA | 2 x 3.5 cm | Surgical excision | ||||
| 27 32 |
F F |
Gingiva Gingiva |
Firm Firm |
NA NA |
NA NA |
2 x 3.5 cm 1.5 x 2.5 cm |
H | Surgical excision Surgical excision |
|||
| H | |||||||||||
| 23 | F | Gingiva | Soft | NA | NA | 1.5 x 1.75 cm | H | Surgical excision | |||
| 26 | F | Gingiva | Soft | NA | NA | 2.0 x 2.5 cm | H | Surgical excision | |||
| 28 | F | Gingiva | Soft | NA | NA | 0.5 x 0.8 cm | H | Surgical excision | |||
| 2013 | Deshmukh et al., 2013 [58] | India | 9 | M | Gingiva and mucogingival junction | Soft | No | Horizontal bone loss | NA | H | Surgical excision |
| 2013 | Gomes et al., 2013 [2] | India | 22 | M | Gingiva | NA | NA | No bone loss | 2.1 x 4.4 cm | H | Surgical excision |
| 2013 | Kamala 2013 [3] | India | 30 | F | Upper lip | Firm | No | NA | 0.8 cm | H | Surgical excision |
| 2013 | Mahabob et al., 2013 [92] | India | 22 | F | Palate | Firm | Pregnancy | NA | 2 x 2 cm | H | Surgical excision |
| 2013 | Moraes, et al., 2013 [93] | Brazil | 65 | M | Gingiva | NA | Diabetes and high blood pressure | No abnormalities | NA | H | Surgical excision |
| 2013 | Sangamesh et al., 2013 [94] | India | 40 | F | Buccal mucosa | Firm | NA | NA | 1.5 x 1.5 cm | H | Surgical excision |
| 2014 | Asha et al., 2014 [59] | India | 54 | M | Lower lip | Firm | No | NA | 3.0 x 3.0 cm | H | Surgical excision |
| 2014 | Fekrazad R et al., (2014) [54] | Iran | 24 | F | Gingiva | Soft | NA | No abnormalities | 1.4 x 0.8 mm | H | Laser excision |
| 2014 | Ghalayani et al., 2014 [83] | Iran | 45 | M | Tongue | NA | Epilepsy beginning | NA | 4.0 x 3.0 x 1.0 cm | H | Surgical excision |
| 2014 | Kejriwal et al., 2014 [81] | India | 59 | M | Gingiva | Firm | No | No abnormalities | 1.5 x 2.0 x 1.0 cm | H | Surgical excision |
| 2014 | Mastammanavar et al., 2014 [52] | India | 44 | F | Gingiva | Soft | NA | NA | 1.5 x 3.0 cm | H | Surgical excision |
| 2014 | Sun et al., 2014 [78] | China | 22 | F | Gingiva | NA | Pregnancy | NA | 3 cm | C | No |
| 2015 | Asnaashari M et al., (2015) [70] | Iran | 6 | M | Gingiva | Soft | No | No abnormalities | 1.1 x 1.3 cm | H | Laser excision |
| 2015 | Bugshan a., et al., (2015) [74] | USA | 51 | F | Gingiva and palatal | NA | NA | NA | 0.9x0.6 cm buccal and 0.8x0.7 cm palatal. | H | Intralesional inyections |
| 2015 | De Carvalho et al., 2015 [95] | Brazil | 11 | B | Upper Lip | NA | No | NA | 4.5 cm | H | Surgical |
| 2015 | Ganesan A. 2015 [55] | India | 49 | F | Gingiva | Firm | No | No bone loss | 4.0 x 3.0 cm | H | Surgical excision |
| 2015 | Sachdeva 2015 [96] | India | 45 | F | Buccal mucosa | Firm | No | NA | 2 x 1 cm | H | Surgical excision |
| 2015 | Tripathi et al., 2015 [63] | India | 55 | M | Gingiva | NA | No | Alveolar bone loss | 3 x 3 cm | H | Surgical excision |
| 2016 | Agarwal N et al., 2016 [97] | India | 8 d | B | Gingiva | Soft | No | NA | 0.5 x 0.8 cm | H | Surgical excision |
| 2016 | Al-Mohaya et al., 2016 [23] | Saudí arabia | 51 | F | Gingiva | Firm | Uncontrolled type II diabetes mellitus | NA | 2.0 x 1.5 cm | H | Laser excision |
| 2016 | Marla et al., 2016 [98] | Nepal | 40 | F | Gingiva | NA | NA | NA | 1.0 – 2.0 cm | H | Surgical excision |
| Nepal | 40 | F | Buccal mucosa | NA | NA | NA | 1.0 – 2.0 cm | H | Surgical excision | ||
| Nepal | 9 | M | Buccal mucosa | NA | NA | NA | <1.0 cm | H | Surgical excision | ||
| Nepal | 23 | F | Gingiva | NA | NA | NA | 1.0 – 2.0 cm | H | Surgical excision | ||
| 2016 | Cheney et al., 2016 [22] | USA | 16 | M | Tongue, Buccal mucosa, | Soft | Acute lymphoblastic leukemia | N/A | N/A | Surgical excision | |
| USA | 14 | G | Tongue | N/A | Fanconi anemia | No | 0.5 x 0.2cm 1.0 x 0.3 cm 0.3 x 0.2 |
H | Surgical excision | ||
| USA | 11 | G | Tongue | N/A | Fanconi anemia | No | 2.0 x 2.5 cm | H | Surgical excision | ||
| USA | 15 | Buccal mucosa | Stage IIIB nodular sclerosing Hodgkin lymphoma. | No | 1 cm 2.0 x 4.0 cm | H | CO2 laser | ||||
| USA | 6 | B | Tongue | N/A | Junctional epidermolysis bullosa | No | 1.0 x 0.5 cm | H | Surgical excision | ||
| 2017 | Rosa et al., 2017 [48] | México | 34 | F | Gingiva | Firm | No | Absence of interproximal contact | 1.5 x 0.9 cm | H | Surgical excision |
| 2018 | Canivell et al [77] | Spain | 32 | F | Lower lip | NA | Pregnancy | NA | 0.5 x 1.0 cm | H | Surgical excision |
| 2018 | Parajuli et al., 2018 [49] | Nepal | 26 | F | Tongue | Soft | No | NA | 2.5 x 2.0 cm | H | Surgical excision |
| Nepal | 15 | G | Upper lip | NA | NA | NA | 0.5 x 0.5 cm | C | Surgical excision | ||
| 2019 | Poudel et al., 2019 [99] | Nepal | 49 | M | Upper lip | Firm | NA | NA | 0.6 x 0.8 cm | H | Surgical excision |
| 2020 | Gutierrez 2020 [25] | Perú | 51 | F | Alveolar ridge | NA | Hypothyroidism erythrodermic psoriasis | Alveolar bone loss | 2.5 x 2.5 cm | H | Surgical excision |
| 2020 | Banjar et al., 2020 [100] | Saudí arabia | 15 | B | Lower lip | Soft | No | NA | 1.2 × 0.8 × 0.6 cm | H | Surgical excision |
| 2021 | Aragaki et al 2021 [28] | Japan | 55 | M | Tongue | Soft | Gastric Cancer | No abnormalities | 0.6cm | H | Surgical excision |
| 67 | M | Upper lip | Soft | Gastric Cancer | No abnormalities | 0.5 mm | H | Surgical excision | |||
| 2021 | Pisano et al., 2021 [72] | Italy | 11 | G | Lower lip | Soft | No | N/A | 1.5 cm | H | Diode Laser |
| 2023 | Lomelí et al., | México | 32 | F | Hard palate | Soft | No | Alveolar bone loss | 25 x 12 mm | H | Surgical excision |
| 2023 | [66] | México | 42 | F | Gingiva | Soft | No | Alveolar bone loss | 16 x 10 mm | H | Surgical excision |
| 38 | F | Gingiva | 20 x 15 | ||||||||
Note: (m): mounths. (d): Day. (F): Female. (M): Male. (B): Boy. (G): Girl. (NA): data not available. (H): Histopathological. (C): Clinical.
8. Treatment of oral PG
The treatment or the management of oral PG depends on the particular characteristics presented by each patient. However, the treatment of choice is conventional surgical excision. Other minimally-invasive treatment modalities have been suggested, including laser, corticosteroid injections, cryosurgery and sclerotherapy [2,4,27] (Table 1).
Surgical excision consists of the complete removal of the lesion and the extension of the cut to the periosteum, including a 2-mm margin to the adjacent soft tissues. If the PG is located near adjacent teeth, it is important that after removal of the lesion, debridement is performed both supra- and sub-gingivally to the biofilm and/or dental calculus. Additionally, it is important to remove all irritating agents (foreign materials, sources of trauma, overhang crowns, etc.) that are present in the area of the lesion. These suggested measures, both in the surgical technique and in the removal of irritants, are aimed at avoiding recurrence of PG [2,7,48,66].
Chandrashekar (2012) implemented a minimally-invasive approach as a treatment strategy for oral PG. This protocol consists of performing scaling and root planning in the area where the lesion is located. In addition, it is crucial to maintain complete oral hygiene by brushing twice a day and using a 0.12% chlorhexidine rinse twice a day. It is necessary to monitor the evolution of the lesion every week. If the lesion persists, scaling and root planning should be implemented every week for 4 consecutive weeks in order to continue with the non-invasive approach. At the same time, it is recommended that patients should maintain adequate brushing and flossing twice a day. This minimally invasive treatment may be considered when the PG is small in size, painless, and without bleeding.
Recently, a laser-assisted removal treatment was used for oral PG [54,70,71,72]. Asnaashari et al. (2015) implemented the Er:YAG Laser therapy using the Diode Laser Gallium-Aluminum-Arsenide (GA-LA-AS). Moreover, Al-Mohaya et al. [2016] used the 940nm diode laser in a diabetic patient uncontrolled, without observing recurrences and/or postoperative complications. The advantages of applying the laser is that by sealing the blood vessels and nerve bundles, there is no bleeding during surgery, thereby ensuring better visualization of the surgery site, sterile conditions, cutting precision, reduced number of instruments used, and sutureless procedure with minimal postoperative pain [70,71,72]. In addition, the laser instantly disinfects the surgical wound, resulting in lower possibility of postoperative infection, minimal inflammation and better healing of surgical wound. In oral cavity lesions, the use of laser reduces intraoperative and postoperative complications, when compared to surgical excision [70,71].
A proposed therapeutic alternative is corticosteroid injection into the oral PG, an option which was identified in two studies in this review (Table 1). Parisi et al. (2006) were the pioneers in implementing, for the first time, the use of a series of corticosteroid injections into lesions for the management of multiple intraoral PG nodules as a new conservative treatment option for this pathology. However, Bugshan et al. (2015) suggested a series of injections in 5 different sites of the lesion with 0.1 ml of 10 mg/ml triamcinolone acetonide, without exceeding a total of 0.5ml, in addition to local application of 0.05% clobetasol propionate for 2 weeks. The latter protocol is appropriate and effective, particularly in patients with high PG recurrences due to poor surgical excisions. The exact mechanism of action of corticosteroid therapy is still unknown. However, these drugs may improve the response of the lesion in the vascular bed to vasoconstrictor agents. A corticosteroid such as dexamethasone stops vascular proliferation by downregulating proangiogenic factors such as VEGF-A, MMP1, and IL-6 [9].
Cryotherapy is a simple, easy-to-execute, inexpensive, and safe treatment that has become one of the therapeutic options used for PG patients. Its implementation is simpler than that of surgical excision, and it is cheaper than laser. It allows resolution of the pathology without leaving significant scarring. Endothelial cells may be more vulnerable to cryotherapy than collagen fibers [75].
Sodium tetradecyl sulfate sclerotherapy is among the alternative therapies that have been implemented. This technique offers a better alternative to excision due to its simplicity and the absence of scarring, although multiple treatment sessions are required. The therapeutic effects of this treatment may be mediated through a mechanism involving the specific and non-specific actions of sodium tetradecyl sulfate, which specifically causes damage to endothelial cells and obliterates the lumen of vessels. Additionally, in stromal tissues, it may cause non-specific necrotic changes. The adverse effects of treatment with sodium tetradecyl sulfate include allergic reactions, skin necrosis, and hyperpigmentation. Sodium tetradecyl sulfate Injection is usually painless. Therefore, extravasation may develop asymptomatically. To avoid skin necrosis, slow and careful injection with some pressure is necessary [76].
During pregnancy, choosing the treatment modality for oral PG is challenging, and it depends on the severity of the symptoms. Gondivkar et al. (2020) and Canivell et al. (2018) have proposed surgical excision of the granuloma during pregnancy. On the other hand, Su et al., (2014) suggest that for patients without hemorrhagic or painless lesions, oral hygiene instructions, clinical monitoring of development of PG, follow-up, and oral self-care at home should be implemented. Regardless of the treatment implemented for PG in pregnant women, we suggest, particularly in this group of patients, a strict control of oral hygiene, the continuous removal of biofilm and/or dental calculus, the use of soft toothbrushes, as well as flossing in order to avoid recurrence.
The formation of a reactive lesion (for example, PG) around dental implants is a complication that has received attention. These lesions may lead to marginal bone loss and, consequently, implant failure. Therefore, several treatments for implant-associated PG have been considered, with the treatment of choice being conservative surgical excision with total removal of the base of the lesion and bone curettage [79]. Additionally, it is recommended that the implant surface should be polished so as to eliminate any irritating factor that may be causing or favoring the appearance of PG [79]. Photodynamic therapy is a simple, non-invasive adjunctive treatment for peri-implant diseases. It allows for control of disease progression through de-contamination of infected surfaces. However, further studies are needed to establish its efficacy in cases of reactive lesions around dental implants [79,80].
Regarding postoperative management for arresting recurrence of PG after treatment, some authors have suggested implementation of oral hygiene measures, among which are the use of a soft toothbrush, keeping the lesion area clean, use of mouth rinses, and antibiotic therapy [48,60,65,70]. The suggested rinses entail the use of 0.2% chlorhexidine [54,65,81] and 0.12% chlorhexidine [48]; use of gluconate twice daily, and saline rinse [65]. The antibiotic of choice frequently used for adequate intervention is amoxicillin at a dose of 500 mg every 8 hours for 5 days [50,51,52]. In pediatric patients, good oral hygiene is recommended for keeping the lesion area clean, and neither analgesics nor antibiotics are prescribed [70,72].
The recurrence rate of PG is 15%, and this is associated with incomplete lesion removal and failure to eliminate etiological factors [13,82]. Frumkin et al. (2015) proposed a conservative protocol for preventing recurrence. This entails removal of irritants with debridement under local anesthesia, along with ancillary measures such as chlorhexidine rinse and oral hygiene instructions. In addition, the protocol suggests a follow-up schedule that involves visits every 2 weeks during the first 2 months, followed by maintenance visits once every 2 months. However, recurrence is uncommon in extra-gingival locations after surgical excision [83].
9. Conclusion
Pyogenic granuloma (PG) is a benign tumor of the blood vessels that forms as a result of an exaggerated reaction of the connective tissue to a minor localized lesion or any underlying irritation. Treatment for the management of PG depends on the particular characteristics of each patient. It is essential to implement a continuous comprehensive dental evaluation which allows for preventive measures consisting of elimination of local irritating agents (dental biofilm, calculus, and overhanging restorations) and meticulous oral hygiene care (brushing after eating, at least twice daily, using fluoridated toothpaste on a soft-bristled toothbrush, and daily flossing). This is in order to decrease the possibility of appearance and development of PG.
References
- Sarwal P, Lapumnuaypol K. Pyogenic Granuloma. 2021 Nov 21. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 32310537.
- Gomes SR, Shakir QJ, Thaker PV, Tavadia JK. Pyogenic granuloma of the gingiva: A misnomer?—A case report and review of literature. J Indian Soc Periodontol. 2013 Jul;17(4):514-9. PMID: 24174735; PMCID: PMC3800418. [CrossRef]
- Kamal R, Dahiya P, Puri A. Oral pyogenic granuloma: Various concepts of etiopathogenesis. J Oral Maxillofac Pathol. 2012 Jan;16(1):79-82. PMID: 22434943; PMCID: PMC3303528. [CrossRef]
- Sharma S, Chandra S, Gupta S, Srivastava S. Heterogeneous conceptualization of etiopathogenesis: Oral pyogenic granulo-ma. Natl J Maxillofac Surg. 2019 Jan-Jun;10(1):3-7. PMID: 31205381; PMCID: PMC6563641. [CrossRef]
- Ghalayani P, Hajisadeghi S, Babadi F. Extragingival pyogenic granuloma associated with medication: Report of an unusual case. Dent Res J (Isfahan). 2014 May;11(3):400-4. PMID: 25097653; PMCID: PMC4119376.
- Parisi E, Glick PH, Glick M. Recurrent intraoral pyogenic granuloma with satellitosis treated with corticosteroids. Oral Dis. 2006 Jan;12(1):70-2. PMID: 16390473. [CrossRef]
- Al-Noaman AS. Pyogenic granuloma: Clinicopathological and treatment scenario. J Indian Soc Periodontol. 2020 May-Jun;24(3):233-236. Epub 2020 May 4. PMID: 32773973; PMCID: PMC7307466. [CrossRef]
- Poncet A, Dor L (1897) Botyromycose humaine. Rev Chir 18: 996.
- Greenberger S, Boscolo E, Adini I, Mulliken JB, Bischoff J: Corticosteroid suppression of VEGF-A in infantile hemangio-ma-derived stem cells. N Engl J Med 2010;362:1005–1013. [CrossRef]
- Jafarzadeh H, Sanatkhani M, Mohtasham N. Oral pyogenic granuloma: A review. J Oral Sci. 2006 Dec;48(4):167-75. PMID: 17220613. [CrossRef]
- Wiener RC, Wiener-Pla R. Literacy, pregnancy and potential oral health changes: The Internet and readability levels. Matern Child Health J. 2014 Apr;18(3):657-62. PMID: 23784613; PMCID: PMC4919661. [CrossRef]
- Montazer Lotf-Elahi MS, Farzinnia G, Jaafari-Ashkavandi Z. Clinicopathological study of 1000 biopsied gingival lesions among dental outpatients: A 22-year retrospective study. BMC Oral Health. 2022 Apr 29;22(1):154. PMID: 35488268; PMCID: PMC9052626. [CrossRef]
- Krishnapillai, R., Punnoose, K., Angadi, P. V., & Koneru, A. (2012). Oral pyogenic granuloma—A review of 215 cases in a South Indian Teaching Hospital, Karnataka, over a period of 20 years. Oral and Maxillofacial Surgery, 16(3), 305–309. [CrossRef]
- Shamim T, Varghese VI, Shameena PM, Sudha S. A retrospective analysis of gingival biopsied lesions in South Indian pop-ulation: 2001-2006. Med Oral Patol Oral Cir Bucal. 2008 Jul 1;13(7):E414-8. PMID: 18587304.
- Nejad ES, BigomTaheri J, Azimi S. Frequency of gingival pregnancy tumor in iran (confirmed by biopsy). J Int Oral Health. 2014 Nov-Dec;6(6):72-6. PMID: 25628488; PMCID: PMC4295460.
- Chamani G,NavvabiN,AbdollahzadehSH.Thefrequency of pregancny tumor in pregnant mothers. Dent J Shiraz Med Sci Univ 2009;10:79-82. [CrossRef]
- Tabatabaei et al., (2014) Frequency of Gingival Pregnancy Tumor in Iran (confirmed by biopsy) Journal of international Oral Health, 6(6):72-76.
- Lee J, Lynde C. Pyogenic granuloma: Pyogenic again? Association between pyogenic granuloma and Bartonella. J Cutan Med Surg. 2001 Nov-Dec;5(6):467-70. PMID: 11907853. [CrossRef]
- KERR DA. Granuloma pyogenicum. Oral Surg Oral Med Oral Pathol. 1951 Feb;4(2):158-76. PMID: 14807485. [CrossRef]
- Bhaskar SN, Jacoway JR. Pyogenic granuloma – Clinical features, incidence, histology, and result of treatment: Report of 242 cases. J Oral Surg 1966;24:391-8.
- Piraccini BM, Bellavista S, Misciali C, Tosti A, de Berker D, Richert B. Periungual and subungual pyogenic granuloma. Br J Dermatol. 2010 Nov;163(5):941-53. PMID: 20545691. [CrossRef]
- Cheney-Peters D, Lund TC. Oral Pyogenic Granuloma After Bone Marrow Transplant in the Pediatric/Adolescent Population: Report of 5 Cases. J Pediatr Hematol Oncol. 2016 Oct;38(7):570-3. PMID: 27271813. [CrossRef]
- Al-Mohaya M, Treister N, Al-Khadra O; et al. Calcineurin inhibitor-associated oral inflammatory polyps after trans- planta-tion. J Oral Pathol Med. 2007;36:570–574. [CrossRef]
- Palmero ML, Pope E. Eruptive pyogenic granulomas developing after drug hypersensitivity reaction. J Am Acad Dermatol. 2009 May;60(5):855-7. Epub 2009 Feb 10. PMID: 19211171. [CrossRef]
- Gutierrez PA. An unusual case of multiple oral pyogenic granuloma, ¿associated with treatment with levothyroxin?. Rev Estomatol Herediana 2020 Oct-Dic;30(4):294-301.
- Tosti A, Piraccini BM, D’Antuono A, Marzaduri S, Bettoli V. Paronychia associated with antiretroviral therapy. Br J Derma-tol. 1999 Jun;140(6):1165-8. PMID: 10354091. [CrossRef]
- Leung AKC, Barankin B, Hon KL (2014) Pyogenic Granuloma. Clinics Mother Child Health 11: e106. [CrossRef]
- Aragaki T, Tomomatsu N, Michi Y, Hosaka H, Fukai Y, Iijima M, Yoda T. Ramucirumab-related Oral Pyogenic Granuloma: A Report of Two Cases. Intern Med. 2021 Aug 15;60(16):2601-2605. Epub 2021 Mar 8. PMID: 33678742; PMCID: PMC8429295. [CrossRef]
- Uzel MI, Kantarci A, Hong HH; et al. Connective tissue growth factor in drug-induced gingival overgrowth. J Perio- dontol. 2001;72:921–931. [CrossRef]
- Baran R. Etretinate and the nails (study of 130 cases) possible mechanisms of some side-effects. Clin Exp Dermatol 1986; 11:148– 52. [CrossRef]
- Williams LH, Fleckman P. Painless periungual pyogenic granulo- mata associated with reverse transcriptase inhibitor therapy in a patient with human immunodeficiency virus infection. Br J Dermatol 2007; 156:163–4. [CrossRef]
- Silva de Araujo Figueiredo C, Gonçalves Carvalho Rosalem C, Costa Cantanhede AL, Abreu Fonseca Thomaz ÉB, Fontoura Nogueira da Cruz MC. Systemic alterations and their oral manifestations in pregnant women. J Obstet Gynaecol Res. 2017 Jan;43(1):16-22. PMID: 28074549. [CrossRef]
- Figuero-Ruiz E, Prieto Prieto I, Bascones-Martínez A. Cambios hormonales asociados al embarazo. ón gin-givo-periodontal. Av Periodon Implantol. 2006; 18, 2: 101-113. First Published: 09 June 2006. Cryotherapy in the treatment of pyogenic granuloma.
- Cardoso JA, Spanemberg JC, Cherubini K, Figueiredo MA, Salum FG. Oral granuloma gravidarum: A retrospective study of 41 cases in Southern Brazil. J Appl Oral Sci. 2013;21(3):215-8. PMID: 23857656; PMCID: PMC3881906. [CrossRef]
- Jang H, Patoine A, Wu TT, Castillo DA, Xiao J. Oral microflora and pregnancy: A systematic review and meta-analysis. Sci Rep. 2021 Aug 19;11(1):16870. PMID: 34413437; PMCID: PMC8377136. [CrossRef]
- Borgo PV, Rodrigues VA, Feitosa AC, Xavier KC, Avila-Campos MJ. Association between periodontal condition and sub-gingival microbiota in women during pregnancy: A longitudinal study. J Appl Oral Sci. 2014 Nov-Dec;22(6):528-33. PMID: 25591021; PMCID: PMC4307767. [CrossRef]
- Ojanotko-Harri AO, Harri MP, Hurttia HM, Sewon LA. Altered tissue metabolism of progesterone in pregnancy gingivitis and granuloma. J Clin Periodontol 1991;18:262-6. [CrossRef]
- Yuan K, Jin YT, Lin MT. Expression of Tie-2, angiopoietin-1, angiopoietin-2, ephrinB2 and EphB4 in pyogenic granuloma of human gingiva implicates their roles in inflammatory angiogenesis. J Periodontal Res. 2000 Jun;35(3):165-71. PMID: 10929871. [CrossRef]
- Yuan K, Jin YT, Lin MT. The detection and comparison of angiogenesis-associated factors in pyogenic granuloma by im-munohistochemistry. J Periodontol. 2000 May;71(5):701-9. PMID: 10872949.Author 1, A.B. Title of Thesis. Level of Thesis, Degree-Granting University, Location of University, Date of Completion. [CrossRef]
- Shetty SJ, Hallikeri K, Anehosur V, Desai A. An aggressive pyogenic granuloma masquerading as a vascular neoplasm. J Indian Soc Periodontol. 2020 May-Jun;24(3):276-279. Epub 2020 Jan 27. PMID: 32773980; PMCID: PMC7307463. [CrossRef]
- Nelimarkka L, Salminen H, Kuopio T, Nikkari S, Ekfors T, Laine J, Pelliniemi L, Järveläinen H. Decorin is produced by capillary endothelial cells in inflammation-associated angiogenesis. Am J Pathol. 2001 Feb;158(2):345-53. PMID: 11159170; PMCID: PMC1850307. [CrossRef]
- Blackwell MG, Itinteang T, Chibnall AM, Davis PF, Tan ST. Expression of embryonic stem cell markers in pyogenic granu-loma. J Cutan Pathol. 2016 Dec;43(12):1096-1101. Epub 2016 Sep 15. PMID: 27509392. [CrossRef]
- Pereira TDSF, de Amorim LSD, Pereira NB, Vitório JG, Duarte-Andrade FF, Guimarães LM, Diniz MG, Gomes CC, Gomez RS. Oral pyogenic granulomas show MAPK/ERK signaling pathway activation, which occurs independently of BRAF, KRAS, HRAS, NRAS, GNA11, and GNA14 mutations. J Oral Pathol Med. 2019 Nov;48(10):906-910. Epub 2019 Aug 4. PMID: 31310691. [CrossRef]
- Yao T, Nagai E, Utsunomiya T, Tsuneyoshi M. An intestinal.
- Sharma, S., Chandra, S., Gupta, S., & Srivastava, S. (2019). Heterogeneous conceptualization of etiopathogenesis: Oral pyo-genic granuloma. National journal of maxillofacial surgery, 10(1), 3–7. [CrossRef]
- Akyol MU, Yalçiner EG, Doğan AI. Pyogenic granuloma (lobular capillary hemangioma) of the tongue. Int J Pediatr Otorhinolaryngol. 2001 May 11;58(3):239-41. PMID: 11335013. [CrossRef]
- Nejad ES, BigomTaheri J, Azimi S. Frequency of gingival pregnancy tumor in Iran (confirmed by biopsy). J Int Oral Health. 2014 Nov-Dec;6(6):72-6.
- Rosa G., Cartagena C., Andrea L, & La Torre C.,(2017). Oral pyogenic granuloma diagnosis and treatment: A series of cases. Revista odontológica mexicana, 21(4), 253-261. Recuperado en 04 de septiembre de 2023, de http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S1870-199X2017000400253&lng=es&tlng=en.
- Parajuli R, Maharjan S. Unusual presentation of oral pyogenic granulomas: A review of two cases. Clin Case Rep. 2018 Feb 27;6(4):690-693. PMID: 29636941; PMCID: PMC5889261. [CrossRef]
- Panjwani S., Issrani R., Keluskar V., Naik Z. (2012). An unusual presentation of pyogenic granuloma, Indian Journal of Dentistry, Volume 3, Number 3; pp. 178e181. [CrossRef]
- Mubeen K., Vijayalakshmi K. R. and Abhishek R. P., (2011). Oral pyogenic granuloma with mandible involvement: An unusual presentation, Journal of Dentistry and Oral Hygiene Vol. 3(1), pp.6- 9, 2141-2472.
- Mastammanavar, D., Hunasgi, S., Koneru, A., Vanishree, M.R., Surekha, R., & Vardendra, M. (2014). Aggressive Pyogenic Granuloma: A Case Report. International Journal of Oral and Maxillofacial Pathology, 5, 29-32.
- Gonçales ES, Damante JH, Fischer Rubira CM, Taveira LA. Pyogenic granuloma on the upper lip: An unusual location. J Appl Oral Sci. 2010 Sep-Oct;18(5):538-41. PMID: 21085814; PMCID: PMC4246389. [CrossRef]
- Fekrazad R, Nokhbatolfoghahaei H, Khoei F, Kalhori KA. Pyogenic Granuloma: Surgical Treatment with Er:YAG Laser. J Lasers Med Sci. 2014 Fall;5(4):199-205. PMID: 25653822; PMCID: PMC4281984.
- Ganesan A, Kumar N G, Azariah E, Asokan G S. Oral pyogenic granuloma: A case report and a comprehensive review. SRM J Res Dent Sci [serial online] 2015 [cited 2023 Sep 3];6:257-60. Available from: https://www.srmjrds.in/text.asp?2015/6/4/257/170284.
- Aguilo L. Pyogenic granuloma subsequent to injury of a primary tooth. A case report. Int J Paediatr Dent. 2002 Nov;12(6):438-41. PMID: 12452987. [CrossRef]
- Panseriya BJ, Hungund S. Pyogenic granuloma associated with periodontal abscess and bone loss—A rare case report. Contemp Clin Dent. 2011 Jul;2(3):240-4. PMID: 22090773; PMCID: PMC3214537. [CrossRef]
- Deshmukh J. Kulkarni VK., Katti G., Deshpande S. (2013). Pyogenic Granuloma, An Unusual Presentation In Pediatric Patient—A Case Report.. Indian Journal of Dental Sciences. 5. 90-93.
- Asha V, Dhanya M, Patil BA, Revanna G. An unusual presentation of pyogenic granuloma of the lower lip. Contemp Clin Dent. 2014 Oct;5(4):524-6. PMID: 25395771; PMCID: PMC4229764. [CrossRef]
- Behl AB., Bali V., Bali R. Pyogenic Granuloma—A case report and review of literature, international journal of stomatology & occlusion medicine, 2011. 4:166–170. [CrossRef]
- Gondivkar SM, Gadbail A, Chole R. Oral pregnancy tumor. Contemp Clin Dent. 2010 Jul;1(3):190-2. PMID: 22114415; PMCID: PMC3220110. [CrossRef]
- Verma PK, Srivastava R, Baranwal HC, Chaturvedi TP, Gautam A, Singh A. “Pyogenic granuloma–Hyperplastic lesion of the gingiva: Case reports”. Open Dent J. 2012;6:153-6. Epub 2012 Oct 5. Erratum in: Open Dent J. 2012;6:188. PMID: 23091574; PMCID: PMC3474946. [CrossRef]
- Tripathi AK, Upadhaya V, Kumar V, Saimbi CS. Hyperactive lesions of gingiva associated with severe alveolar bone loss: A rare finding. Contemp Clin Dent. 2015 Apr-Jun;6(2):223-5. PMID: 26097359; PMCID: PMC4456746. [CrossRef]
- Shenoy SS, Dinkar AD. Pyogenic granuloma associated with bone loss in an eight year old child: A case report. J Indian Soc Pedod Prev Dent. 2006 Dec;24(4):201-3. PMID: 17183185. [CrossRef]
- Shivaswamy S, Siddiqui N, Jain SA, Koshy A, Tambwekar S, Shankar A. A rare case of generalized pyogenic granuloma: A case report. Quintessence Int. 2011 Jun;42(6):493-9. PMID: 21519587.
- Lomelí Martínez SM, Bocanegra Morando D, Mercado González AE, Gómez Sandoval JR. Unusual clinical presentation of oral pyogenic granuloma with severe alveolar bone loss: A case report and review of literature. World J Clin Cases. 2023 Jun 6;11(16):3907-3914. PMID: 37383141; PMCID: PMC10294161. [CrossRef]
- Ma Y, Nicolet J. Specificity models in MAPK cascade signaling. FEBS Open Bio. 2023 Jul;13(7):1177-1192. Epub 2023 Jun 11. PMID: 37157227; PMCID: PMC10315774. [CrossRef]
- Rodríguez-Carballo E, Gámez B, Ventura F. p38 MAPK Signaling in Osteoblast Differentiation. Front Cell Dev Biol. 2016 May 6;4:40. PMID: 27200351; PMCID: PMC4858538. [CrossRef]
- Chandrashekar B. Minimally invasive approach to eliminate pyogenic granuloma: A case report. Case Rep Dent. 2012;2012:909780. Epub 2012 Jan 26. PMID: 22567459; PMCID: PMC3335552. [CrossRef]
- Asnaashari M, Mehdipour M, MoradiAbbasabadi F, Azari-Marhabi S. Expedited removal of pyogenic granuloma by diode laser in a pediatric patient. J Lasers Med Sci. 2015 Winter;6(1):40-4. PMID: 25699167; PMCID: PMC4329141.
- Al-Mohaya MA, Al-Malik AM. Excision of oral pyogenic granuloma in a diabetic patient with 940nm diode laser. Saudi Med J. 2016 Dec;37(12):1395-1400. PMID: 27874157; PMCID: PMC5303780. [CrossRef]
- Pisano M, Sammartino P, Di Vittorio L, Iandolo A, Caggiano M, Roghi M, Bizzoca ME, Lo Muzio L. Use of Diode Laser for Surgical Removal of Pyogenic Granuloma of the Lower Lip in a Pediatric Patient: A Case Report. Am J Case Rep. 2021 Jun 19;22:e929690. PMID: 34146391; PMCID: PMC8218884. [CrossRef]
- Parisi E, Glick PH, Glick M: Recurrent intraoral pyogenic granuloma with satellitosis treated with corticosteroids. Oral Dis 2006;12:70–72. [CrossRef]
- Bugshan A, Patel H, Garber K, Meiller TF. Alternative Therapeutic Approach in the Treatment of Oral Pyogenic Granuloma. Case Rep Oncol. 2015 Nov 14;8(3):493-7. PMID: 26668570; PMCID: PMC4677718. [CrossRef]
- Mirshams M, Daneshpazhooh M, Mirshekari A, Taheri A, Mansoori P, Hekmat S. Cryotherapy in the treatment of pyogen-ic granuloma. J Eur Acad Dermatol Venereol. 2006 Aug;20(7):788-90. PMID: 16898898. [CrossRef]
- Moon SE, Hwang EJ, Cho KH. Treatment of pyogenic granuloma by sodium tetradecyl sulfate sclerotherapy. Arch Derma-tol. 2005 May;141(5):644-6. PMID: 15897398. [CrossRef]
- Canivell-Zabaleta M, Martin-Lozano G, Olmos-Juarez E, Fontillon-Alberdi M, Infante-Cossio P. Extragingival Pregnancy Pyogenic Granuloma on the Lip. J Craniofac Surg. 2018 Jan;29(1):e49-e50. PMID: 29040143. [CrossRef]
- Sun WL., Lei L., Zhong L., Yu S., Zhou JW., Multiple gingival pregnancy tumors with rapid growth, Journal of Dental Sciences. 2013, 9 (3), 289-293, ISSN 1991-7902. [CrossRef]
- Román-Quesada, N., González-Navarro, B., Izquierdo-Gómez, K. et al. An analysis of the prevalence of peripheral giant cell granuloma and pyogenic granuloma in relation to a dental implant. BMC Oral Health 21, 204 (2021). [CrossRef]
- Baesso RCP, de Lima Jacy Monteiro Barki MC, de Souza Azevedo R, da Costa Fontes KBF, Pereira DL, Tucci R, Pires FR, Picciani BLS. Peripheral giant cell granuloma associated with a dental implant. BMC Oral Health. 2019;19:283. [CrossRef]
- Kejriwal S, Bhandary R, Thomas B. Oral pyogenic granuloma: A case report, Nitte University Journal of Health Science, Vol. 4, No.1, March 2014, ISSN 2249-7110.
- Ghalayani P, Hajisadeghi S, Babadi F. Extragingival pyogenic granuloma associated with medication: Report of an unusual case. Dent Res J 2014; 11(3): 400e404.
- Frumkin N, Nashef R, Shapira L, Wilensky A. Nonsurgical treatment of recurrent gingival pyogenic granuloma: A case report. Quintessence Int 2015; 46(6): 539e544. [CrossRef]
- Patil K, Mahima VG, Lahari K. Extragingival pyogenic granuloma. Indian J Dent Res. 2006 Oct-Dec;17(4):199-202. Erratum in: Indian J Dent Res. 2007 Jan-Mar;18(1):45. Ambika, L [corrected to Lahari, K]. PMID: 17217217. [CrossRef]
- Amirchaghmaghi M, Falaki F, Mohtasham N, Mozafari PM. Extragingival pyogenic granuloma: A case report. Cases J. 2008 Dec 3;1(1):371. PMID: 19055747; PMCID: PMC2614954. [CrossRef]
- Olmedo DG, Paparella ML, Brandizzi D, Cabrini RL. Reactive lesions of peri-implant mucosa associated with titanium dental implants: A report of 2 cases. Int J Oral Maxillofac Surg. 2010 May;39(5):503-7. Epub 2009 Dec 11. PMID: 20005076. [CrossRef]
- Rizwanulla MD, Koirala B., Sharma S., Adhikari L., Pradhan A. (2011). Pyogenic Granuloma: A Case Report. Health Renaissance. 8. [CrossRef]
- Penseriya et al. (2011). Pyogenic granuloma associated with periodontal abscess and bone loss—A rare case report, Con-temporary Clinical Dentistry, 2(3): 240–244. [CrossRef]
- Ravi V, Jacob M, Sivakumar A, Saravanan S, Priya K. Pyogenic granuloma of labial mucosa: A misnomer in an anomolous site. J Pharm Bioallied Sci. 2012 Aug;4(Suppl 2):S194-6. PMID: 23066251; PMCID: PMC3467924. [CrossRef]
- Piscoya MDB de V., Ximenes, RA de A., Silva GM., Jamelli SR., Coutinho SB. (2012). Periodontitis-associated risk factors in pregnant women. Clinics, 67(1), 27–33. [CrossRef]
- Adusumilli S, Yalamanchili PS, Manthena S. Pyogenic granuloma near the midline of the oral cavity: A series of case reports. J Indian Soc Periodontol. 2014 Mar;18(2):236-9. PMID: 24872636; PMCID: PMC4033894. [CrossRef]
- Mahabob N, Kumar S, Raja S. Palatal pyogenic granulomaa. J Pharm Bioallied Sci. 2013 Jul;5(Suppl 2):S179-81. PMID: 23956603; PMCID: PMC3740672. [CrossRef]
- Moraes SH., Moraes GF., Durski J., Viero FL., Da Silva Meira DD. And Caron ME. (2013) GRANULOMA PIOGÊNICO: RELATO DE CASO CLÍNICO. Revista Gestão & Saúde, Curitiba, v. 9, n. 2, p.12-19.
- Sangamesh NC., Poornima B., Vidya KCh., Sakri SB. (2013). Extragingival pyogenic granuloma: A rare case report. J Sci Soc, 2013;40:49-51. [CrossRef]
- de Carvalho FK, Pinheiro TN, Arid J, de Queiroz AM, de Rossi A, Nelson-Filho P. Trauma-Induced Giant Pyogenic Granuloma in the Upper Lip. J Dent Child (Chic). 2015 Sep-Dec;82(3):168-70. PMID: 26731254.
- Sachdeva SK. Extragingival Pyogenic Granuloma: An Unusual Clinical Presentation. J Dent (Shiraz). 2015 Sep;16(3 Suppl):282-5. PMID: 26535410; PMCID: PMC4623838.
- Agarwal N, Kumar D, Vaish A, Anand A. A Rare Case of Pyogenic Granuloma with a Natal Tooth. J Clin Diagn Res. 2016 Oct;10(10):ZD28-ZD29. Epub 2016 Oct 1. PMID: 27891487; PMCID: PMC5121825. [CrossRef]
- Marla V, Shrestha A, Goel K, Shrestha S. The Histopathological Spectrum of Pyogenic Granuloma: A Case Series. Case Rep Dent. 2016;2016:1323798. Epub 2016 Jun 12. PMID: 27382492; PMCID: PMC4921146. [CrossRef]
- Poudel P, Chaurasia N, Marla V, Srii R. Pyogenic granuloma of the upper lip: A common lesion in an uncommon location. J Taibah Univ Med Sci. 2018 Dec 4;14(1):95-98. PMCID: PMC6694911. PMID: 31435396. [CrossRef]
- Banjar A, Abdrabuh A, Al-Habshi M, Parambil M, Bastos P, Abed H. Labial pyogenic granuloma related to trauma: A case report and mini-review. Dent Traumatol. 2020 Aug;36(4):446-451. Epub 2020 Jan 9. PMID: 31869498. [CrossRef]
- Gonçales ES, Damante JH, Fischer Rubira CM, Taveira LA. Pyogenic granuloma on the upper lip: An unusual location. J Appl Oral Sci. 2010 Sep-Oct;18(5):538-41. PMID: 21085814; PMCID: PMC4246389. [CrossRef]
- Mubeen K., Vijayalakshmi K. R. and Abhishek R. P. (2011). Oral pyogenic granuloma with mandible involvement: An unusual presentation, Journal of Dentistry and Oral Hygiene Vol. 3(1), pp.6- 9, 2141-2472.
Figure 1.
The etiopathogenesis and risk factors of the GP are observed.
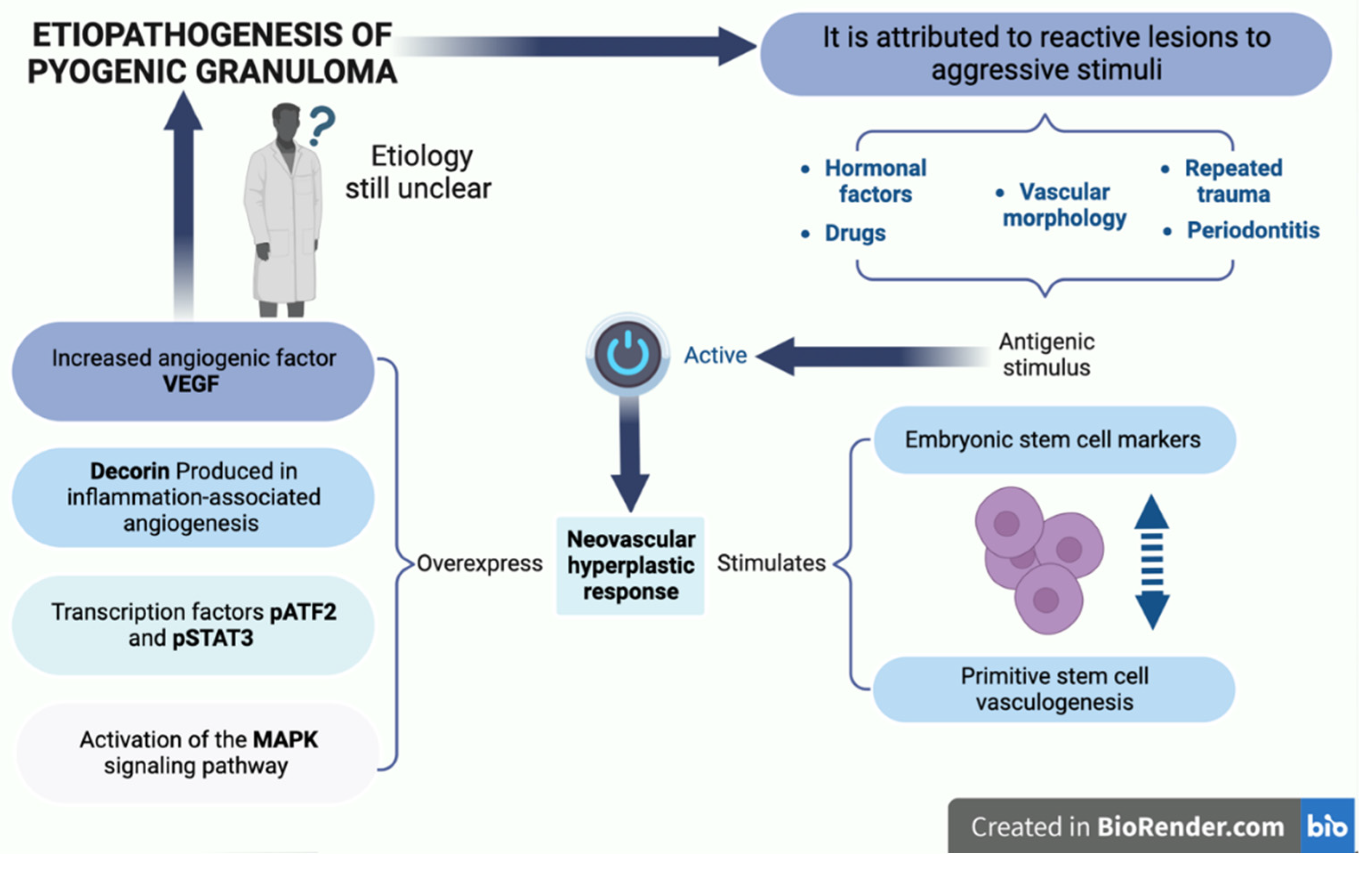
Figure 2.
A lobular mass of hyperplastic granulation tissue is observed, formed by abundant vascular spaces, young fibroblasts, infiltration of acute and/or chronic inflammatory cells with macrophages, neutrophils, lymphocytes, and polymorphonuclear cells. NOS: nitric oxide synthase, VEGF: vascular endothelium-derived grow.
Figure 2.
A lobular mass of hyperplastic granulation tissue is observed, formed by abundant vascular spaces, young fibroblasts, infiltration of acute and/or chronic inflammatory cells with macrophages, neutrophils, lymphocytes, and polymorphonuclear cells. NOS: nitric oxide synthase, VEGF: vascular endothelium-derived grow.
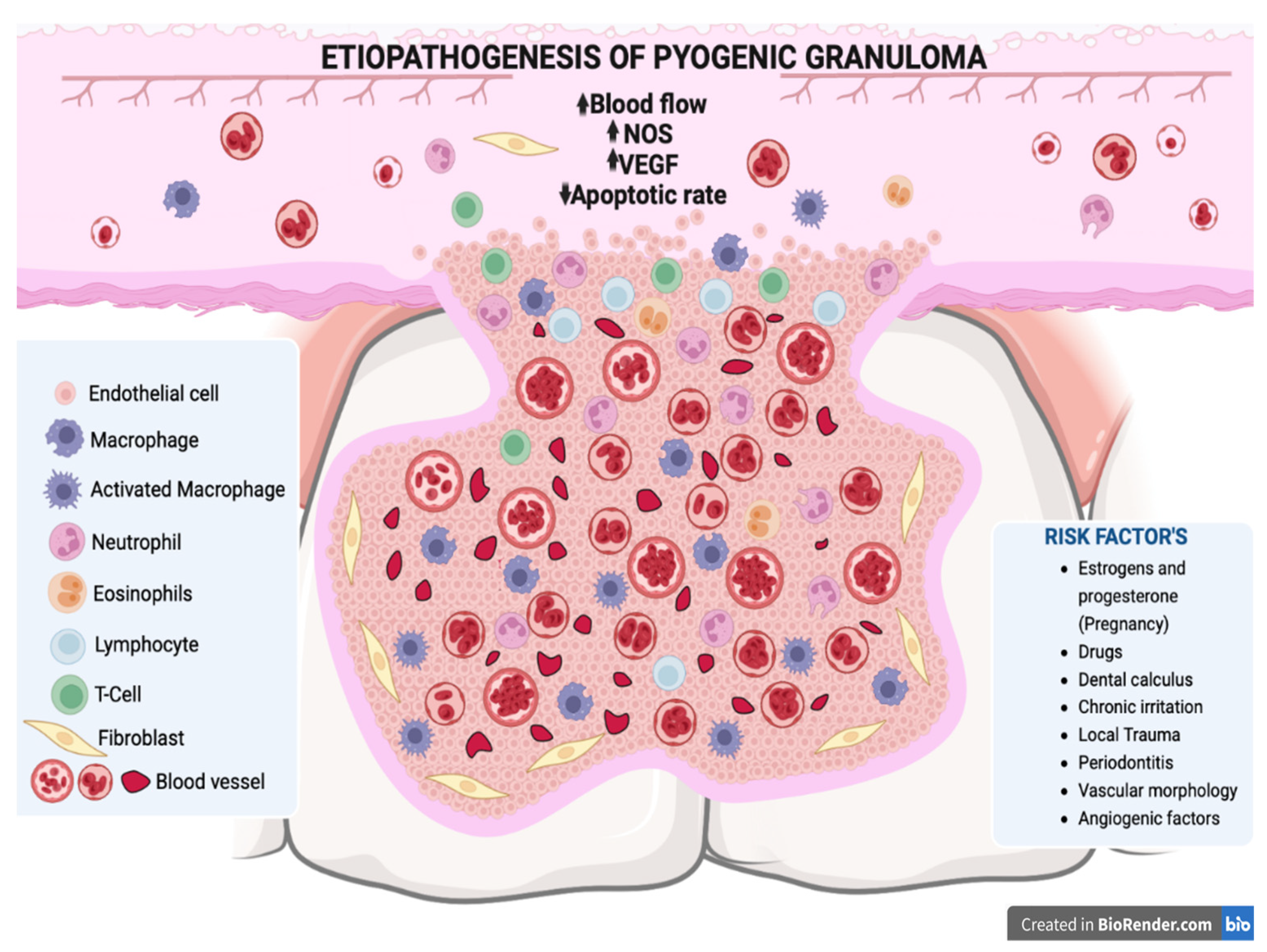
Figure 3.
Growth factors such as vascular endothelium-derived growth factor (VEGF), fibroblast growth factor-2 (FGF-2), tumor necrosis factor α (TNF-α) among other molecules, bind to the extracellular domain of a receptor tyrosine kinase that acts with docking sites for GRB2 adapter proteins that also binds to a guanine nucleotide exchange factor SOS, for a protein called Ras, which activates another signaling protein called Raf, acting on the MEK substrate 1/2, which phosphorylates and activates ERK 1/2, which enters the nucleus where it activates specific transcription factors and genes involved in the proliferation of osteoclast precursors that differentiate into mature osteoclasts that will resorb the bon crest in the Pyogenic Granuloma area.
Figure 3.
Growth factors such as vascular endothelium-derived growth factor (VEGF), fibroblast growth factor-2 (FGF-2), tumor necrosis factor α (TNF-α) among other molecules, bind to the extracellular domain of a receptor tyrosine kinase that acts with docking sites for GRB2 adapter proteins that also binds to a guanine nucleotide exchange factor SOS, for a protein called Ras, which activates another signaling protein called Raf, acting on the MEK substrate 1/2, which phosphorylates and activates ERK 1/2, which enters the nucleus where it activates specific transcription factors and genes involved in the proliferation of osteoclast precursors that differentiate into mature osteoclasts that will resorb the bon crest in the Pyogenic Granuloma area.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



