
Submitted:
11 September 2023
Posted:
13 September 2023
You are already at the latest version
Abstract
Type 2 diabetes mellitus (T2DM) is a common metabolic disease characterised by insulin resistance and elevated blood glucose levels, affecting millions of people worldwide. T2DM patients with dyslipidaemia have an increased risk of cardiovascular disease (CVD). A complex interplay of risk factors such as hyperglycaemia, dyslipidaemia, hypertension, obesity, inflammation and oxidative stress favour the development of atherosclerosis, a central mechanism in the pathogenesis of cardiovascular disease. Dyslipidaemia, a hallmark of T2DM, is characterised by elevated triglycerides, decreased high-density lipoprotein (HDL) cholesterol and the presence of small, dense low-density lipoprotein (LDL) particles, all of which promote atherosclerosis. In this article, we have attempted to present various treatment strategies that include pharmacological interventions such as statins, ezetimibe, PCSK9 inhibitors, fibrates and omega-3 fatty acids. We have also tried to highlight the pivotal role of lifestyle modifications, including physical activity and dietary changes, in improving lipid profiles and overall cardiovascular health in T2DM patients. We have also tried to present the latest clinical guidelines for the management of dyslipidaemia in T2DM patients. In conclusion, the treatment of dyslipidaemia in T2DM patients is of great importance as it lowers lipid particle levels, slows the progression of atherosclerosis and ultimately reduces susceptibility to cardiovascular disease.
Keywords:
Type 2 diabetes mellitus
; dyslipidaemia
; metabolic disorder
; pharmaceutical treatment
; non-pharmaceutical treatment.
1. Introduction
Type 2 diabetes mellitus (T2DM) is a chronic metabolic disorder characterised by insulin resistance and high blood glucose levels. It is estimated that 462 million people are affected by this disease, which corresponds to a prevalence rate of 6059 cases per 100,000. T2DM is more prevalent in developed regions (Europe, North America) with equal gender distribution [1]. T2DM is a significant risk factor for cardiovascular disease including coronary heart disease, heart attacks, strokes, peripheral artery disease and heart failure. Cardiovascular comorbidities in T2DM patients result in high costs for both the population and the patients. Cardiovascular expenditure accounted for between 20% and 49% of the total direct costs of treating T2DM at the population level. Compared to T2DM patients without CVD, median annual expenditures for CVD, coronary heart disease, heart failure and stroke were 112%, 107%, 59% and 322% higher, respectively. Compared with treating T2DM alone, treating patients with CVD plus T2DM resulted in an increase in costs from a median of $3418 to $9705 [2]. The increased risk of CVD in T2DM patients is influenced by a complex interplay of risk factors that include hyperglycaemia, dyslipidaemia, hypertension, obesity, inflammation and oxidative stress. These risk factors contribute to the development and progression of atherosclerosis, one of the most important underlying processes in CVD [3,4]. The aim of this review is to shed light on the management of dyslipidaemia in patients with type 2 diabetes mellitus, focusing on the underlying pathophysiology and the intricate web of interrelated metabolic disorders.
2. Pathophysiology
The pathophysiology of atherosclerosis in T2DM is a complex and multifaceted process involving a combination of metabolic abnormalities, inflammation, oxidative stress and endothelial dysfunction. The main pathophysiological mechanism is hyperglycaemia due to insulin resistance, which can damage blood vessels and increase the risk of atherosclerosis. High blood glucose levels can also contribute to inflammation and oxidative stress, both of which are factors in the development of CVD. T2DM is often associated with dyslipidaemia, characterised by increased triglyceride levels, decreased high-density lipoprotein (HDL) cholesterol levels and the presence of small, dense low-density lipoprotein (LDL) particles. These lipid abnormalities promote the development of atherosclerotic plaques. At the molecular level, chronic low grade inflammation is a hallmark of T2DM and plays an important role in atherosclerosis. Inflammatory molecules such as C-reactive protein (CRP) and interleukin-6 (IL -6) are elevated in T2DM and contribute to the development of atherosclerotic lesions [3,5,6]. In chronic inflammation, oxidative stress is the main contributor to the progression of atherosclerosis. Oxidative stress damages the endothelium and promotes inflammation, lipid oxidation and atherosclerosis. Dysfunction of the endothelium contributes to the development and progression of atherosclerosis. The endothelium, which lines the inner surface of blood vessels, plays a critical role in regulating vascular health. In T2DM, endothelial dysfunction occurs, leading to impaired vasodilation, increased vascular permeability and a proinflammatory and prothrombotic state [7,8]. The formation of atherosclerotic plaques is the beginning of the vicious cycle. Atherosclerosis begins with the accumulation of LDL cholesterol in the subendothelial space of the arteries. Inflammation and oxidative stress promote the modification of LDL particles, making them more atherogenic. Macrophages engulf modified LDL, leading to the formation of foam cells in the arterial wall. Over time, atherosclerotic plaques develop, consisting of lipid deposits, inflammatory cells, smooth muscle cells and fibrous tissue. Vulnerable atherosclerotic plaques are prone to rupture. When a plaque ruptures, the blood is exposed to prothrombotic material, leading to the formation of blood clots (thrombosis). These clots can partially or completely block blood flow and cause acute cardiovascular events such as heart attacks and strokes. As atherosclerosis progresses, the artery walls can be remodeled, leading to stenosis (narrowing) and reduced blood flow in the affected vessels [3,6,8]. The cumulative effects of atherosclerosis in people with T2DM lead to an increased risk of cardiovascular disease, including coronary heart disease, cerebrovascular disease and peripheral arterial disease. Cardiovascular disease remains the leading cause of death and disability in patients with T2DM [6].
3. Type 2 diabetes mellitus and dyslipidemia interconnection
Dyslipidaemia is one of the most common findings in patients with type 2 diabetes, affecting approximately 72-85% of patients [9]. It additionally increases cardiovascular risk, especially the risk of developing coronary heart disease. The main lipid abnormalities in diabetics are increased levels of triacylglycerols and decreased HDL cholesterol. In addition to quantitative changes in lipoproteins, there are also qualitative and kinetic changes in lipoprotein metabolism that contribute to the development of atherosclerosis [10]. Prior to the development of manifest type 2 diabetes, increased insulin resistance affects the accumulation of triglycerides and small, dense LDL particles. Starting at the chylomicron level, increased production of chylomicrons occurs in diabetics as a result of insulin resistance, leading to postprandial hyperlipidaemia. On the other hand, the clearance of chylomicrons is impaired due to decreased LPL activity, an enzyme necessary for the degradation of chylomicrons [11]. In addition, the production of large VLDL particles is increased, leading to an increase in plasma triacylglycerol levels. Studies have shown the link between VLDL production rates and fatty liver in patients with type 2 diabetes [12]. Unlike other lipids, LDL cholesterol levels are not significantly increased in diabetics compared to the general population, but increased glycation of LDL leads to severe atherosclerosis. Glycated LDL cholesterol has a lower binding affinity to LDL receptors and is taken up by macrophages, leading to the formation of foam cells [13]. In addition, oxidised LDL particles increase the formation of cytokines (TNF-α, IL -1), adhesion molecules that promote the inflammatory atherosclerotic process. Diabetics also have reduced levels of HDL cholesterol, which plays the key role in the uptake and transport of lipoproteins. Studies have shown that HDL particles are degraded more in diabetics due to the accumulation of triacylglycerol [14]. HDL plays an important role in cardiovascular prevention due to its antioxidant and vasodilator effects, so lower levels also increase overall cardiovascular risk. The most common quantitative changes in the lipid profile of diabetics are increased triglyceride levels, residual particles and decreased HDL cholesterol levels. Qualitative and kinetic changes in the metabolism of LDL cholesterol have a major atherogenic effect, so treatment of dyslipidaemia should be taken very seriously.
4. Target lipid levels in type 2 diabetes mellitus
The American Diabetes Association recently released updated guidelines for 2023 that include new recommendations for people with diabetes, including guidance on managing lipid levels. The current recommendations suggest that it is advisable for people with diabetes who are at increased risk for cardiovascular problems, particularly those with one or more risk factors for atherosclerotic cardiovascular disease (ASCVD), to be prescribed high-intensity statin treatment. The primary goal is to reduce LDL cholesterol levels by at least 50% from baseline, aiming for LDL cholesterol levels of less than 70 mg/dL (1,8 mmol/L) [15]. However, in clinical practice, it can be difficult to determine the exact baseline LDL cholesterol level before starting statin therapy. Therefore, for these individuals, it is recommended to focus on achieving a target LDL cholesterol level below 70 mg/dL (1,8 mmol/L) rather than focusing on the percentage reduction in LDL cholesterol. Where appropriate, it may also be useful to supplement maximally tolerated statin therapy with ezetimibe or a proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor to achieve the desired LDL cholesterol reduction of at least 50% and reach the recommended LDL cholesterol target of below 70 mg/dL (1,8 mmol/L). Although primary prevention trials have typically involved limited numbers of older people with diabetes, they have not shown significant differences in the relative benefits of lipid-lowering therapy between age groups. However, because older age is associated with a higher risk profile, the absolute benefit of lipid-lowering therapy is greater. Therefore, it is advisable to recommend moderate-intensity statin therapy to people with diabetes aged 75 years or older. High-intensity statin therapy is recommended for all people with diabetes who have a history of ASCVD. The goal is to achieve a significant reduction in LDL cholesterol levels of at least 50% from baseline, with a specific goal of maintaining LDL cholesterol levels below 55 mg/dL (1,42 mmol/L) [15]. If these targets are not met despite administration of the maximally tolerated statin, it is advisable to consider the additional administration of ezetimibe or a PCSK9 inhibitor. The new guidelines do not include precise target values for other lipoproteins. Therefore, it is advisable to consider the following target values: HDL cholesterol levels should be above 40 mg/dL (1.02 mmol/L) and triglyceride levels should be below 150 mg/dL (1.7 mmol/L) [16].
5. Treatment of dyslipidaemia in type 2 diabetes mellitus
The treatment of dyslipidaemia in patients with type 2 diabetes mellitus (T2DM) can be divided into two categories: non-pharmacological and pharmacological. If we talk about pharmacological therapeutic strategies with regard to elevated lipid levels in patients who have already been diagnosed DM type 2, the most important approach is treatment with statins. Other options include cholesterol absorption inhibitors, fibrates, PCSK9 inhibitors and omega-3 fatty acids [17].
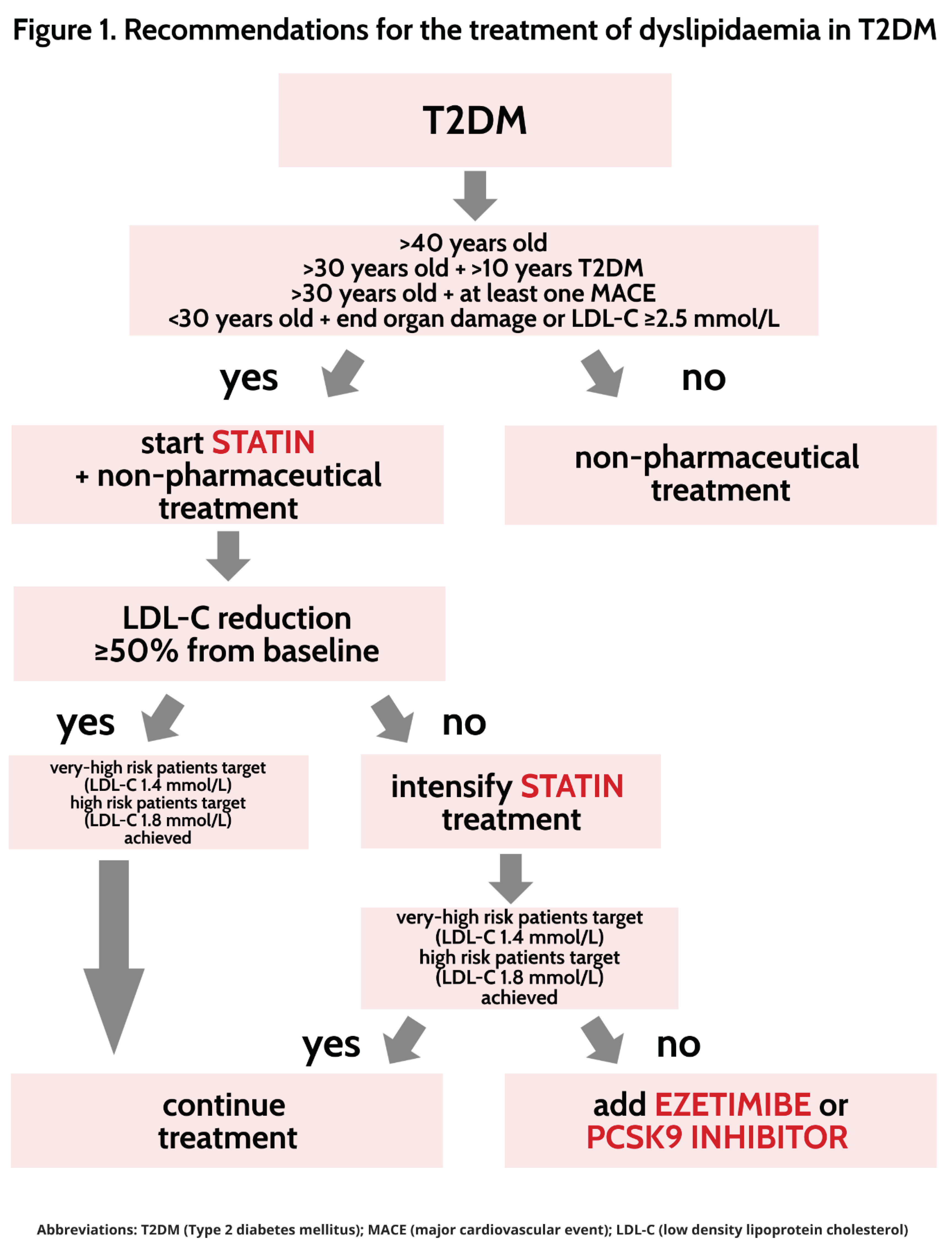
Despite significant benefits in treatment strategies that reduce CVD risk factors, CVD remains the major cause of morbidity and mortality in patients with T2DM. The risk of MACE in T2DM is strongly determined by the presence of target organ damage, with risks increasing with the number of diseases present. In light of this information, the main focus of treatment for dyslipidaemia in patients with T2DM is early initiation of treatment [17]. According to the latest guidelines, patients who have had diabetes for at least 10 years or less but have known cardiovascular disease and/or at least one target organ damage and elevated lipid levels should start statin treatment immediately [17,18]. If an early 50% reduction is achieved, further supplementation is not required but continuation of pharmacological and non-pharmacological treatment is. However, if the desired reduction is not achieved, the additional administration of ezetimibe or PCSK9 inhibitor is suggested [17,18] (Figure 1).
5.1. Statins
Statins are the first treatment option for patients with T2DM. Management of LDL cholesterol is of paramount importance in these patients. The Cholesterol Treatment Trialists (CTT) study did a comprehensive analysis of the data and uncovered 3247 serious vascular events in the diabetic cohort [19]. Strikingly, each one millimole per litre (mmol/L) reduction in LDL cholesterol was associated with a remarkable 9% proportional reduction in all-cause mortality in participants with diabetes. Remarkably, this reduction paralleled the 13% decrease observed in individuals without diabetes, underscoring the importance of LDL-C modulation in preventing mortality [19]. This positive trend was underlined by a statistically significant reduction in vascular mortality in the diabetic cohort, while no discernible effect on non-vascular mortality was observed. In addition, a substantial proportional reduction in major vascular events of 21% per mmol/L reduction in LDL cholesterol was observed in participants with diabetes, mirroring the effects in participants without diabetes [19]. The discernible effects of statin therapy also extended to specific cardiovascular outcomes in the diabetes population, including reductions in myocardial infarction or coronary death, coronary revascularisation and stroke. Of note, these results held true regardless of whether participants had a history of vascular disease [20,21]. After 5 years, statin therapy had significant clinical benefit in the diabetic cohort, as evidenced by a reduction in major vascular events among participants receiving statin therapy [19]. Overall, these results highlight the compelling efficacy of statin therapy in reducing the burden of serious vascular events in people with diabetes mellitus and support the thesis that statins are a key therapeutic intervention for LDL-C management in the context of diabetes treatment. On the other hand, recent studies have brought to light a possible increase in the incidence of diabetes mellitus (DM) in patients receiving statin therapy [22,23]. This trend has been supported by clinical trials, with the clearest effects observed in people who are already at increased risk of DM, such as those with prediabetes [24]. It is critical to emphasise that these results should not diminish our commitment to patient care, as the overarching benefits in reducing cardiovascular disease persist and far outweigh the increased incidence of DM. Conversely, a separate prospective study of T2DM patients found no statistically significant difference in glycosylated haemoglobin (HbA1c) levels between statin-treated and non-statin-treated groups [25]. The safety profile of statins is well established, with adverse effects such as muscle pain and liver damage frequently reported [26]. These adverse effects may be the most important factor in the low adherence to statin treatment. However, newer approaches such as fix-dose combination therapy with statins and other drugs such as antihypertensives or even antidiabetics are leading to better adherence and positive cardiovascular outcomes in patients [27].
5.2. Ezetimibe
Ezetimibe, a lipid-lowering agent that acts as a cholesterol absorption inhibitor, is associated with a 19% reduction in LDL-C levels [28]. Although ezetimibe alone has no positive results in risk reduction MACE, when added to statin therapy, ezetimibe has shown remarkable ability to reduce the risk of serious vascular events. It is important to note that the magnitude of relative risk reduction in MACE is directly proportional to the absolute degree of LDL-C reduction, a relationship consistent with the observed effects of statins [29]. In the study IMPROVE-IT, which included a subgroup of patients diagnosed with T2DM, it was expected that this subgroup would have a higher rate of major vascular events than patients without DM. In fact, the placebo arm of the study showed that patients with DM had a significantly increased rate of MACE, with a 7-year Kaplan–Meier rate of 46% compared to 31% in patients without DM [30]. Of particular importance is the observation that ezetimibe proved to be particularly effective in patients with DM in the IMPROVE-IT study. When ezetimibe was added to their treatment regimen, patients with DM experienced a relative risk reduction of 15% in MACE, which corresponds to a substantial absolute risk reduction of 5.5% [30]. However, it is worth noting that the IMPROVE-IT study did not demonstrate a significant reduction in MACE with single-use ezetimibe [31]. The reduction in major vascular events was most notable when ezetimibe was used in conjunction with statin therapy, highlighting the synergy between these therapies in achieving significant clinical benefits in cardiovascular risk management. Importantly, the safety profile of the combined statin-ezetimibe treatment remained consistent regardless of the presence of DM, underscoring the tolerability of this therapeutic approach [30,31]. Based on the observed results, ezetimibe is used as a second treatment option in combination with statins in patients in whom LDL-C lowering cannot be achieved with statin treatment alone [17,18].
5.3. PCSK9 inhibitors
PCSK9 monoclonal antibodies such as evolocumab and alirocumab have attracted considerable attention due to their efficacy in lowering LDL-C levels, which is around 60% [32,33]. In the FOURIER study, the relative risk reduction for MACE was consistent in all patient groups with and without diabetes mellitus. However, the baseline risk profile of patients with DM, characterised by an inherently higher cardiovascular risk, resulted in a more pronounced absolute risk reduction of 2.7% in MACE over 3 years [32]. These outstanding results are consistent with those of the ODYSSEY study, which demonstrated a consistent benefit of PCSK9 inhibitors, particularly in diabetic patients after an acute coronary syndrome [33]. These studies highlight the potent LDL-C lowering effect of PCSK9 monoclonal antibody inhibitors and their potential to reduce the risk of MACE in both diabetics and non-diabetics [32,33]. A recent study that deepened our understanding of the effects of PCSK9 inhibitor therapy examined the effect of alirocumab in patients of different glycaemic categories34. Importantly, alirocumab resulted in similar relative reductions in the incidence of primary cardiovascular endpoints in all glycaemic categories. However, in patients with diabetes, there was a greater absolute reduction of 2.3% in the incidence of primary endpoints than in patients with prediabetes (1.2%) or normoglycaemia (1.2%) [34]. Furthermore, in patients without diabetes, the risk of new-onset diabetes was not increased by alirocumab therapy. These results highlight the safety profile of alirocumab with respect to new-onset diabetes [34,35]. Similar observations were made with evolocumab in a study that included patients with and without diabetes. Evolocumab reduced cardiovascular outcomes in both patient groups [32,35]. These results suggest that the benefit of evolocumab is not dependent on diabetes status. Importantly, evolocumab did not increase the risk of new-onset diabetes in patients without diabetes. In addition, haemoglobin A1c (HbA1c) and fasting plasma glucose (FPG) levels remained constant over time in all glycaemic categories between the evolocumab and placebo groups [36]. In addition, the frequency of adverse events was comparable between the evolocumab and placebo groups, further underscoring the safety profile of this PCSK9 inhibitor therapy regardless of diabetes status [32,33]. Overall, these comprehensive results highlight the robust efficacy and safety of monoclonal antibody PCSK9 inhibitors in both diabetic and non-diabetic patients, supporting their role in controlling LDL-C levels and lowering MACE. However, the elephant in the room needs to be addressed, as the cost-benefit analysis of PCSK9 inhibitors is still ongoing. While some countries report further price reductions to increase cost-effectiveness, inclusion in T2DM treatment may justify their cost [37].
5.4. Fibrates
Fibrates are drugs used primarily to treat abnormal lipid profiles and conditions such as hypertriglyceridaemia and low levels of high-density lipoprotein cholesterol (HDL-C). These drugs work by activating peroxisome proliferator-activated receptors (PPARs), which regulate lipid metabolism [38]. The therapeutic efficacy of treating elevated triglyceride levels (TG) and low high-density lipoprotein cholesterol (HDL-C) levels, which are common in people with diabetes mellitus (DM), remains controversial. This debate arises from observations in studies such as FIELD and ACCORD, conducted in the context of T2DM cohorts, in which the effects of fenofibrate therapy on MACE did not yield positive results. In the FIELD study, fenofibrate showed a 27% reduction in CVD in individuals with elevated TG levels and elevated HDL-C levels [39]. Similarly, the ACCORD study confirmed that participants with both elevated TG and low HDL-C levels appeared to benefit from taking fenofibrate and statin at the same time [40]. The available evidence suggests that diabetics with dyslipidaemia may derive clinical benefits from TG -lowering therapy when administered concurrently with statin treatment.
5.5. Omega-3 fatty acids
Omega-3 fatty acids are essential polyunsaturated fats that provide a number of health benefits. These fats are abundant in certain fish such as salmon, mackerel and sardines, as well as in flaxseeds, chia seeds and walnuts [41]. They have the benefit of lowering triglyceride levels, improving blood vessel function and possibly reducing inflammation [42]. Omega-3 supplements are widely available in various forms such as fish oil capsules, krill oil and algae-based supplements, so it is extremely difficult to regulate them and determine the exact dosage. There are limited data on the effects of adding omega-3 fatty acids to statin therapy in patients with elevated plasma levels TG. The study REDUCE-IT sought to fill this gap by investigating the effects of icosapent ethyl at a dose of 2 grammes twice daily in high-risk HTG patients taking statins concomitantly. The results showed a 25% reduction in the composite primary outcome, which includes cardiovascular death (CV), non-fatal myocardial infarction (MI), non-fatal stroke, coronary revascularisation or unstable angina. This decrease corresponded to an absolute decrease of 4.8% [43]. Although more research is needed, omega-3 fatty acids have an excellent safety profile. The most commonly reported adverse effects are gastrointestinal discomfort, increased risk of bleeding and allergic reactions. Patients and healthcare professionals need to be aware of the potential effects of the supplements they take [44]. However, omega-3 fatty acids are quite safe and may be of benefit to T2DM patients.
5.6. Non-pharmaceutical treatment
A healthy lifestyle is a key element in the prevention of adverse cardiovascular events. A healthy lifestyle includes not only physical activity, but also improving dietary habits, reducing environmental risk factors and maintaining mental health [45]. People suffering from type 2 diabetes mellitus have a higher risk of developing serious adverse cardiovascular events. Therefore, expected lifestyle changes for these patients include improving dietary habits, increasing physical activity and even taking medication to prevent further complications [46]. Added fats, organ or processed meats, and sweetened beverages can significantly increase the risk of developing diabetes mellitus and cardiovascular disease. For example, drinking a single sweetened beverage per day can increase the risk of developing diabetes mellitus by up to 20% [47]. Physical activity and balanced dietary habits lead to weight loss in overweight patients. Weight loss has a significant impact on lipid levels as well as on the treatment of diabetes mellitus type II and thus improves overall health. The impact of increased physical activity on lowering HbA1c levels has been known for several decades and points to the importance of a healthy lifestyle on blood glucose levels and cardiovascular-related morbidity and mortality in patients with diabetes mellitus [48]. Exercise and increased physical activity have the greatest impact on HDL and triglyceride levels. In the study by Coillard and al. participants were divided into four subgroups based on baseline HDL and triglyceride levels: the first consisted of individuals with normal levels (high HDL and low triglycerides), the second consisted of patients with isolated low HDL and normal triglycerides, the third consisted of patients with isolated high triglycerides and normal HDL levels, and the fourth subgroup included patients with elevated triglycerides and low HDL. For those with a combination of initially low HDL and elevated triglycerides, increased physical activity had the most significant effect, with a 4.9% increase in HDL levels, compared with a slight increase of 0.4% for those with isolated low HDL levels [49]. In addition, some studies suggest that not only physical activity but also its intensity has an impact on lipid management. In the STRRIDE study, changes in serum lipoproteins were monitored in participants with dyslipidaemia who took part in a range of physical activities. After eight months, HDL cholesterol levels and large HDL particle concentrations were higher in those who engaged in high-intensity, high-volume physical activity than in the other groups. The study STRIDDE-PD included patients with prediabetes, and global radiolabelled efflux capacity increased significantly (6.2% ) [50,51] in the high volume/high intensity group compared to all other STRRIDE-PD groups. A combination of physical activity and healthy diet has shown a greater impact on lipid management. In a study of 22 obese men with metabolic syndrome, 3 weeks of physical activity combined with dietary changes resulted in an increase in platelet-activating factor acetylhydrolase activity [52]. Some diets tend to have a positive effect on the lipid profile in people who have diabetes mellitus. For example, a ketogenic diet with 70% fat, 20% protein and only 10% carbohydrate has shown potential to reduce body mass and lower triglycerides and increase HDL levels in patients with diabetes mellitus. In one study, no significant differences were found in the values for total cholesterol and LDL cholesterol. Another important outcome of the ketogenic diet is a reduction in waist circumference, which leads to a further reduction in the risk of complications of diabetes mellitus and the development of cardiovascular complications. In addition, the same study estimates a significant improvement in blood glucose regulation through a decrease in HbA1c [53]. Although there are studies suggesting adverse effects of the ketogenic diet on lipid levels, most studies report a reduction in weight and a resulting improvement in lipid profile [54]. The Mediterranean diet, characterised by ingredients such as olive oil, seeds, whole grains, nuts and fruits, is usually recommended as a golden model for the prevention of metabolic syndrome and its components. There are data indicating a significant impact of this diet on LDL cholesterol levels as well as triglyceride levels, especially in people suffering from type 2 diabetes mellitus. In a study by Elhayany and al. three different dietary approaches were compared during a one-year follow-up period. All participants had diabetes mellitus and were followed in a community-based setting. During this period, participants strictly followed the dietary recommendations for the low-carbohydrate Mediterranean diet, the classic Mediterranean diet or the diet recommended by the American Diabetic Association in 2003. The low-carbohydrate Mediterranean diet has been shown to be most beneficial in lowering HbA1c and has been the only one associated with an increase in HDL cholesterol. The classic Mediterranean diet and the low-carbohydrate diet resulted in greater reductions in triglyceride levels [55]. Olive oil, a major component of the Mediterranean diet, has shown positive effects on regulating lipid profiles, improving HDL functions such as cholesterol metabolism and cholesterol efflux capacity, and promoting an anti-inflammatory effect [56]. Consumption of phenol-containing olive oil increased HDL cholesterol and decreased total cholesterol and LDL cholesterol, leading to a reduction in the ratio of total cholesterol/HDL cholesterol and LDL cholesterol/HDL cholesterol [57]. The CORDIOPREV (Coronary Diet Intervention with Olive Oil and Cardiovascular Prevention) trial showed that a 1.5-year intervention with a Mediterranean diet resulted in improved flow-mediated vasodilation and endothelial function and reduced overall cardiovascular risk in participants with diabetes mellitus and dyslipidaemia[58]. The exact model of dietary habits and physical activity that would lead to adequate control of the risk of developing major adverse cardiovascular events has yet to be found, but research to date may lead to a new answer to this dilemma.
6. Conclusion
The treatment of dyslipidaemia in patients with type 2 diabetes mellitus (T2DM) is of paramount importance because of the high risk of cardiovascular disease (CVD). T2DM is a complex metabolic disorder that not only affects glucose metabolism but also strongly influences lipid profiles, contributing to the development and progression of atherosclerosis — a key process underlying CVD. The pathophysiology of atherosclerosis in T2DM involves a complex interplay of metabolic abnormalities, inflammation, oxidative stress and endothelial dysfunction. High glucose levels, a hallmark of T2DM, can damage blood vessels and lead to inflammation and oxidative stress that further increase CVD risk. Dyslipidaemia is common in T2DM. It is characterised by elevated triglycerides, reduced HDL cholesterol levels and the presence of small, dense low-density lipoprotein (LDL) particles. These lipid abnormalities contribute to the formation of atherosclerotic plaques. A comprehensive approach that includes pharmacological therapies, lifestyle modifications and individualised treatment plans can significantly improve lipid profiles and reduce the risk of major cardiovascular events, ultimately improving the overall health and well-being of people with T2DM.
References
- Khan, M. A. B.; Hashim, M. J.; King, J. K.; Govender, R. D.; Mustafa, H.; Al Kaabi, J. Epidemiology of Type 2 Diabetes – Global Burden of Disease and Forecasted Trends: J. Epidemiol. Glob. Health 2019, 10, 107. [Google Scholar] [CrossRef]
- Einarson, T. R.; Acs, A.; Ludwig, C.; Panton, U. H. Economic Burden of Cardiovascular Disease in Type 2 Diabetes: A Systematic Review. Value Health 2018, 21, 881–890. [Google Scholar] [CrossRef]
- Poznyak, A.; Grechko, A. V.; Poggio, P.; Myasoedova, V. A.; Alfieri, V.; Orekhov, A. N. The Diabetes Mellitus–Atherosclerosis Connection: The Role of Lipid and Glucose Metabolism and Chronic Inflammation. Int. J. Mol. Sci. 2020, 21 (5), 1835. B. Pathophysiology of Diabetic Dyslipidaemia: Where Are We? Int. J. Mol. Sci. 2015, 21, We. [Google Scholar] [CrossRef]
- Wang, J.; Stančáková, A.; Soininen, P.; Kangas, A. J.; Paananen, J.; Kuusisto, J.; Ala-Korpela, M.; Laakso, M. Lipoprotein Subclass Profiles in Individuals with Varying Degrees of Glucose Tolerance: A Population-Based Study of 9399 Finnish Men: Lipids and Glucose Tolerance. J. Intern. Med. 2012, 272, 562–572. [Google Scholar] [CrossRef]
- Taskinen, M.-R.; Nikkil, E. A.; Kuusi, T.; Harno, K. Lipoprotein Lipase Activity and Serum Lipoproteins in Untreated Type 2 (Insulin-Independent) Diabetes Associated with Obesity. Diabetologia 1982, 22, 46–50. [Google Scholar] [CrossRef]
- Adiels, M.; Taskinen, M.-R.; Packard, C.; Caslake, M. J.; Soro-Paavonen, A.; Westerbacka, J.; Vehkavaara, S.; Häkkinen, A.; Olofsson, S.-O.; Yki-Järvinen, H.; Borén, J. Overproduction of Large VLDL Particles Is Driven by Increased Liver Fat Content in Man. Diabetologia 2006, 49, 755–765. [Google Scholar] [CrossRef]
- Makita, T.; Tanaka, A.; Nakano, T.; Nakajima, K.; Numano, F. Importance of Glycation in the Acceleration of Low Density Lipoprotein (LDL) Uptake into Macrophages in Patients with Diabetes Mellitus. Int. Angiol. J. Int. Union Angiol. 1999, 18, 149–153. [Google Scholar]
- Duvillard, L.; Pont, F.; Florentin, E.; Gambert, P.; Vergès, B. Inefficiency of Insulin Therapy to Correct Apolipoprotein A-I Metabolic Abnormalities in Non-Insulin-Dependent Diabetes Mellitus. Atherosclerosis 2000, 152, 229–237. [Google Scholar] [CrossRef]
- Fisher, R. American Diabetes Association Releases 2023 Standards of Care in Diabetes to Guide Prevention, Diagnosis, and Treatment for People Living with Diabetes.
- Solano, M. P.; Goldberg, R. B. Lipid Management in Type 2 Diabetes. Clin. DIABETES 2006, 24. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A. L.; Koskinas, K. C.; Casula, M.; Badimon, L.; Chapman, M. J.; De Backer, G. G.; Delgado, V.; Ference, B. A.; et al. 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias: Lipid Modification to Reduce Cardiovascular Risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef]
- Mancini, G. B. J.; Hegele, R. A.; Leiter, L. A. Dyslipidemia. Can. J. Diabetes 2018, 42, S178–S185. [Google Scholar] [CrossRef] [PubMed]
- Cholesterol Treatment Trialists’ (CTT) Collaborators. Efficacy of Cholesterol-Lowering Therapy in 18 686 People with Diabetes in 14 Randomised Trials of Statins: A Meta-Analysis. The Lancet 2008, 371, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Colhoun, H. M.; Betteridge, D. J.; Durrington, P. N.; Hitman, G. A.; Neil, H. A. W.; Livingstone, S. J.; Thomason, M. J.; Mackness, M. I.; Charlton-Menys, V.; Fuller, J. H. Primary Prevention of Cardiovascular Disease with Atorvastatin in Type 2 Diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): Multicentre Randomised Placebo-Controlled Trial. The Lancet 2004, 364, 685–696. [Google Scholar] [CrossRef]
- Knopp, R. H.; d’Emden, M.; Smilde, J. G.; Pocock, S. J.; on behalf of the ASPEN Study Group. Efficacy and Safety of Atorvastatin in the Prevention of Cardiovascular End Points in Subjects With Type 2 Diabetes. Diabetes Care 2006, 29, 1478–1485. [Google Scholar] [CrossRef] [PubMed]
- Ganda, O. P. Statin-Induced Diabetes: Incidence, Mechanisms, and Implications. F1000Research 2016, 5, 1499. [Google Scholar] [CrossRef]
- Galicia-Garcia, U.; Jebari, S.; Larrea-Sebal, A.; Uribe, K. B.; Siddiqi, H.; Ostolaza, H.; Benito-Vicente, A.; Martín, C. Statin Treatment-Induced Development of Type 2 Diabetes: From Clinical Evidence to Mechanistic Insights. Int. J. Mol. Sci. 2020, 21, 4725. [Google Scholar] [CrossRef]
- Abbasi, F.; Lamendola, C.; Harris, C. S.; Harris, V.; Tsai, M.-S.; Tripathi, P.; Abbas, F.; Reaven, G. M.; Reaven, P. D.; Snyder, M. P.; Kim, S. H.; Knowles, J. W. Statins Are Associated With Increased Insulin Resistance and Secretion. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 2786–2797. [Google Scholar] [CrossRef]
- Davis, T. M. E.; Badshah, I.; Chubb, S. A. P.; Davis, W. A. Dose-Response Relationship between Statin Therapy and Glycaemia in Community-Based Patients with Type 2 Diabetes: The Fremantle Diabetes Study. Diabetes Obes. Metab. 2016, 18, 1143–1146. [Google Scholar] [CrossRef]
- Merćep, I.; Strikić, D.; Slišković, A. M.; Reiner, Ž. New Therapeutic Approaches in Treatment of Dyslipidaemia—A Narrative Review. Pharmaceuticals 2022, 15. [Google Scholar] [CrossRef]
- Castellano, J. M.; Pocock, S. J.; Bhatt, D. L.; Quesada, A. J.; Owen, R.; Fernandez-Ortiz, A.; Sanchez, P. L.; Marin Ortuño, F.; Vazquez Rodriguez, J. M.; Domingo-Fernández, A.; Lozano, I.; Roncaglioni, M. C.; Baviera, M.; Foresta, A.; Ojeda-Fernandez, L.; Colivicchi, F.; Di Fusco, S. A.; Doehner, W.; Meyer, A.; Schiele, F.; Ecarnot, F.; Linhart, A.; Lubanda, J.-C.; Barczi, G.; Merkely, B.; Ponikowski, P.; Kasprzak, M.; Fernandez Alvira, J. M.; Andres, V.; Bueno, H.; Collier, T.; Van De Werf, F.; Perel, P.; Rodriguez-Manero, M.; Alonso Garcia, A.; Proietti, M.; Schoos, M. M.; Simon, T.; Fernandez Ferro, J.; Lopez, N.; Beghi, E.; Bejot, Y.; Vivas, D.; Cordero, A.; Ibañez, B.; Fuster, V. Polypill Strategy in Secondary Cardiovascular Prevention. N. Engl. J. Med. 2022, 387, 967–977. [Google Scholar] [CrossRef]
- Pandor, A.; Ara, R. M.; Tumur, I.; Wilkinson, A. J.; Paisley, S.; Duenas, A.; Durrington, P. N.; Chilcott, J. Ezetimibe Monotherapy for Cholesterol Lowering in 2,722 People: Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Intern. Med. 2009, 265, 568–580. [Google Scholar] [CrossRef] [PubMed]
- Cannon, C. P.; Blazing, M. A.; Giugliano, R. P.; McCagg, A.; White, J. A.; Theroux, P.; Darius, H.; Lewis, B. S.; Ophuis, T. O.; Jukema, J. W.; De Ferrari, G. M.; Ruzyllo, W.; De Lucca, P.; Im, K.; Bohula, E. A.; Reist, C.; Wiviott, S. D.; Tershakovec, A. M.; Musliner, T. A.; Braunwald, E.; Califf, R. M. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. N. Engl. J. Med. 2015, 372, 2387–2397. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, R. P.; Cannon, C. P.; Blazing, M. A.; Nicolau, J. C.; Corbalán, R.; Špinar, J.; Park, J.-G.; White, J. A.; Bohula, E. A.; Braunwald, E. Benefit of Adding Ezetimibe to Statin Therapy on Cardiovascular Outcomes and Safety in Patients With Versus Without Diabetes Mellitus: Results From IMPROVE-IT (Improved Reduction of Outcomes: Vytorin Efficacy International Trial). Circulation 2018, 137, 1571–1582. [Google Scholar] [CrossRef] [PubMed]
- Kosoglou, T.; Statkevich, P.; Johnson-Levonas, A. O.; Paolini, J. F.; Bergman, A. J.; Alton, K. B. Ezetimibe: A Review of Its Metabolism, Pharmacokinetics and Drug Interactions. Clin. Pharmacokinet. 2005, 44, 467–494. [Google Scholar] [CrossRef]
- Sabatine, M. S.; Giugliano, R. P.; Keech, A. C.; Honarpour, N.; Wiviott, S. D.; Murphy, S. A.; Kuder, J. F.; Wang, H.; Liu, T.; Wasserman, S. M.; Sever, P. S.; Pedersen, T. R. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef]
- Ray, K. K.; Colhoun, H. M.; Szarek, M.; Baccara-Dinet, M.; Bhatt, D. L.; Bittner, V. A.; Budaj, A. J.; Diaz, R.; Goodman, S. G.; Hanotin, C.; et al. Effects of Alirocumab on Cardiovascular and Metabolic Outcomes after Acute Coronary Syndrome in Patients with or without Diabetes: A Prespecified Analysis of the ODYSSEY OUTCOMES Randomised Controlled Trial. Lancet Diabetes Endocrinol. 2019, 7, 618–628. [Google Scholar] [CrossRef]
- Rana, K.; Reid, J.; Rosenwasser, J. N.; Lewis, T.; Sheikh-Ali, M.; Choksi, R. R.; Goldfaden, R. F. A Spotlight on Alirocumab in High Cardiovascular Risk Patients with Type 2 Diabetes and Mixed Dyslipidemia: A Review on the Emerging Data. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, Volume 12, 1897–1911. [Google Scholar] [CrossRef]
- Carugo, S.; Sirtori, C. R.; Corsini, A.; Tokgozoglu, L.; Ruscica, M. PCSK9 Inhibition and Risk of Diabetes: Should We Worry? Curr. Atheroscler. Rep. 2022, 24, 995–1004. [Google Scholar] [CrossRef]
- Memon, R.; Malek, R.; Munir, K. M. Doubling of Hemoglobin A1c on PCSK9 Inhibitor Therapy. Am. J. Med. 2019, 132, e17–e18. [Google Scholar] [CrossRef]
- Civeira, F.; Pedro-Botet, J. Cost-Effectiveness Evaluation of the Use of PCSK9 Inhibitors. Endocrinol. Diabetes Nutr. Engl. Ed 2021, 68, 369–371. [Google Scholar] [CrossRef]
- Staels, B.; Dallongeville, J.; Auwerx, J.; Schoonjans, K.; Leitersdorf, E.; Fruchart, J.-C. Mechanism of Action of Fibrates on Lipid and Lipoprotein Metabolism. Circulation 1998, 98, 2088–2093. [Google Scholar] [CrossRef]
- Effects of Long-Term Fenofibrate Therapy on Cardiovascular Events in 9795 People with Type 2 Diabetes Mellitus (the FIELD Study): Randomised Controlled Trial. The Lancet 2005, 366, 1849–1861. [CrossRef] [PubMed]
- Effects of Combination Lipid Therapy in Type 2 Diabetes Mellitus. N. Engl. J. Med. 2010, 362, 1563–1574. [CrossRef] [PubMed]
- Willett, W. C. The Role of Dietary N-6 Fatty Acids in the Prevention of Cardiovascular Disease: J. Cardiovasc. Med. 2007, 8 (Suppl 1), S42–S45. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, M.; Origasa, H.; Matsuzaki, M.; Matsuzawa, Y.; Saito, Y.; Ishikawa, Y.; Oikawa, S.; Sasaki, J.; Hishida, H.; Itakura, H.; Kita, T.; Kitabatake, A.; Nakaya, N.; Sakata, T.; Shimada, K.; Shirato, K. Effects of Eicosapentaenoic Acid on Major Coronary Events in Hypercholesterolaemic Patients (JELIS): A Randomised Open-Label, Blinded Endpoint Analysis. The Lancet 2007, 369, 1090–1098. [Google Scholar] [CrossRef]
- Bhatt, D. L.; Steg, P. G.; Miller, M.; Brinton, E. A.; Jacobson, T. A.; Ketchum, S. B.; Doyle, R. T.; Juliano, R. A.; Jiao, L.; Granowitz, C.; Tardif, J.-C.; Ballantyne, C. M. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef]
- Backes, J.; Anzalone, D.; Hilleman, D.; Catini, J. The Clinical Relevance of Omega-3 Fatty Acids in the Management of Hypertriglyceridemia. Lipids Health Dis. 2016, 15, 118. [Google Scholar] [CrossRef]
- Gonzalez, J. S.; Tanenbaum, M. L.; Commissariat, P. V. Psychosocial Factors in Medication Adherence and Diabetes Self-Management: Implications for Research and Practice. Am. Psychol. 2016, 71, 539–551. [Google Scholar] [CrossRef]
- Arnett, D. K.; Blumenthal, R. S.; Albert, M. A.; Buroker, A. B.; Goldberger, Z. D.; Hahn, E. J.; Himmelfarb, C. D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J. W.; Michos, E. D.; Miedema, M. D.; Muñoz, D.; Smith, S. C.; Virani, S. S.; Williams, K. A.; Yeboah, J.; Ziaeian, B. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease. J. Am. Coll. Cardiol. 2019, 74, e177–e232. [Google Scholar] [CrossRef]
- Löfvenborg, J. E.; Andersson, T.; Carlsson, P.-O.; Dorkhan, M.; Groop, L.; Martinell, M.; Tuomi, T.; Wolk, A.; Carlsson, S. Sweetened Beverage Intake and Risk of Latent Autoimmune Diabetes in Adults (LADA) and Type 2 Diabetes. Eur. J. Endocrinol. 2016, 175, 605–614. [Google Scholar] [CrossRef]
- Boule, N. G.; Haddad, E.; Kenny, G. P.; Wells, G. A.; Sigal, R. J. Effects of Exercise on Glycemic Control and Body Mass in Type 2 Diabetes Mellitus: A Meta-Analysis of Controlled Clinical Trials: Sports Medicine Update. Scand. J. Med. Sci. Sports 2002, 12, 60–61. [Google Scholar] [CrossRef]
- Couillard, C.; Després, J.-P.; Lamarche, B.; Bergeron, J.; Gagnon, J.; Leon, A. S.; Rao, D. C.; Skinner, J. S.; Wilmore, J. H.; Bouchard, C. Effects of Endurance Exercise Training on Plasma HDL Cholesterol Levels Depend on Levels of Triglycerides: Evidence From Men of the Health, Risk Factors, Exercise Training and Genetics (HERITAGE) Family Study. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 1226–1232. [Google Scholar] [CrossRef]
- Kraus, W. E.; Houmard, J. A.; Duscha, B. D.; Knetzger, K. J.; Wharton, M. B.; McCartney, J. S.; Bales, C. W.; Henes, S.; Samsa, G. P.; Otvos, J. D.; Kulkarni, K. R.; Slentz, C. A. Effects of the Amount and Intensity of Exercise on Plasma Lipoproteins. N. Engl. J. Med. 2002, 347, 1483–1492. [Google Scholar] [CrossRef] [PubMed]
- Sarzynski, M. A.; Ruiz-Ramie, J. J.; Barber, J. L.; Slentz, C. A.; Apolzan, J. W.; McGarrah, R. W.; Harris, M. N.; Church, T. S.; Borja, M. S.; He, Y.; Oda, M. N.; Martin, C. K.; Kraus, W. E.; Rohatgi, A. Effects of Increasing Exercise Intensity and Dose on Multiple Measures of HDL (High-Density Lipoprotein) Function. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 943–952. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C. K.; Ng, C.; Hama, S.; Eliseo, A. J.; Barnard, R. J. Effect of a Short-Term Diet and Exercise Intervention on Inflammatory/Anti-Inflammatory Properties of HDL in Overweight/Obese Men with Cardiovascular Risk Factors. J. Appl. Physiol. 2006, 101, 1727–1732. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Wang, M.; Liang, J.; He, G.; Chen, N. Ketogenic Diet Benefits to Weight Loss, Glycemic Control, and Lipid Profiles in Overweight Patients with Type 2 Diabetes Mellitus: A Meta-Analysis of Randomized Controlled Trails. Int. J. Environ. Res. Public. Health 2022, 19, 10429. [Google Scholar] [CrossRef]
- Leow, Z. Z. X.; Guelfi, K. J.; Davis, E. A.; Jones, T. W.; Fournier, P. A. The Glycaemic Benefits of a Very-Low-Carbohydrate Ketogenic Diet in Adults with Type 1 Diabetes Mellitus May Be Opposed by Increased Hypoglycaemia Risk and Dyslipidaemia. Diabet. Med. 2018, 35, 1258–1263. [Google Scholar] [CrossRef] [PubMed]
- Elhayany, A.; Lustman, A.; Abel, R.; Attal-Singer, J.; Vinker, S. A Low Carbohydrate Mediterranean Diet Improves Cardiovascular Risk Factors and Diabetes Control among Overweight Patients with Type 2 Diabetes Mellitus: A 1-Year Prospective Randomized Intervention Study. Diabetes Obes. Metab. 2010, 12, 204–209. [Google Scholar] [CrossRef]
- Mazzocchi, A.; Leone, L.; Agostoni, C.; Pali-Schöll, I. The Secrets of the Mediterranean Diet. Does [Only] Olive Oil Matter? Nutrients 2019, 11. [Google Scholar] [CrossRef]
- Covas, M.-I.; Nyyssönen, K.; E. Poulsen, H.; Kaikkonen, J.; F. Zunft, H.-J.; Kiesewetter, H.; Gaddi, A.; Torre, R. de la; Mursu, J.; Bäumler, H.; Nascetti, S.; T. Salonen, J.; Fitó, M.; Virtanen, J.; Marrugat, J.; Group, for the E. S. The Effect of Polyphenols in Olive Oil on Heart Disease Risk Factors. Ann. Intern. Med. 2006. [Google Scholar]
- Torres-Peña, J. D.; Garcia-Rios, A.; Delgado-Casado, N.; Gomez-Luna, P.; Alcala-Diaz, J. F.; Yubero-Serrano, E. M.; Gomez-Delgado, F.; Leon-Acuña, A.; Lopez-Moreno, J.; Camargo, A.; Tinahones, F. J.; Delgado-Lista, J.; Ordovas, J. M.; Perez-Martinez, P.; Lopez-Miranda, J. Mediterranean Diet Improves Endothelial Function in Patients with Diabetes and Prediabetes: A Report from the CORDIOPREV Study. Atherosclerosis 2018, 269, 50–56. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Recommendations for the treatment of dyslipidaemia in T2DM.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



