Submitted:
11 September 2023
Posted:
13 September 2023
You are already at the latest version
Abstract
Purpose: To explore parents’ perceptions of the educational intervention programme regarding their children’s postoperative pain management.
Design and Methods: A qualitative descriptive study was conducted. Thirty-two parents whose children underwent inpatient elective surgery were recruited from the two intervention groups (received an educational booklet and a video, with or without an hour of face-to-face teaching session) for this qualitative evaluation of the intervention. Participants were asked to comment on the content and delivery methods of the intervention via individual face-to-face semi-structured interviews. Thematic analysis was used to identify themes from the data.
Results: Three themes were generated from 32 participants’ interview data: current pain management practices, experiences and benefits of the educational intervention, and suggestions to improve pain management.
Conclusions: Our findings suggested that the educational intervention in children’s postoperative pain management was helpful for parents and their children. However, it is necessary to improve educational materials and equip healthcare professionals with non-pharmacological pain relief methods.
Practice Implications: Our findings reveal the current challenges in extensively adopting non-pharmacological pain relief methods. Healthcare professionals can do more to routinely integrate pharmacological and non-pharmacological pain management strategies in relieving pain effectively. Future research could develop technology-based programmes to increase ease of access.
Trial Registration Number: ISRCTN24910957.
Keywords:
child
; educational intervention
; pain management
; parents
; perception
1. Introduction
Over the past few decades, parental involvement in their children’s care in the hospital has increased [1-3], and this has been found to benefit both parents and their children [1]. However, previous studies have indicated that parents often lacked knowledge of their children’s postoperative pain management [4,5], such as available pain relief strategies, especially those regarding non-pharmacological methods of pain management [4]. This, in turn, affects their participation in their children’s care which consequently hinders their children’s pain control. Likewise, several other studies also revealed that parents have consistently expressed the need for information and guidance from nurses regarding their children’s postoperative pain management [6]. Empowering parents to be involved in their children’s pain management has been identified as an important element in delivering effective pain management [3, 7]. These studies highlight the immense need to educate parents and equip them with relevant knowledge and skills in pain management [7,8].
Parents with more knowledge and better attitudes were related to better use of pain relief and higher satisfaction with their children’s pain care [9]. Parent intervention with information about pain education has been shown to be effective in reducing parents’ misconceptions about pain medication [10] and anxiety [11], enhancing their caring behaviours (e.g., assessing pain) [10], improving their knowledge of and using more pain relief methods (e.g. positive reinforcement, distraction and relaxation) [12], and in reducing their children’s pain and anxiety [11, 12]. A systematic review and meta-analysis summarised that family-centred educational interventions probably lead to a considerable reduction of paediatric and parental anxiety and improve paediatric behaviours at induction of anaesthesia [13].
A theory-based and culturally appropriate pain management educational intervention programme was developed in addition to the routine care for parents whose children would undergo inpatient elective surgery. This programme intended to reduce the children’s postoperative pain intensity, improve parents’ knowledge and attitudes towards pain management, develop the parents’ behaviour on pain management (use of pain relief strategies), and increase the parents’ satisfaction with their children’s pain management [14]. The programme's theoretical framework was built on the modified Theory of Planned Behaviour [14, 15] (. The interventions included a booklet and a video on pain management, with (Intervention group 1) or without (Intervention group 2) one hour individual face-to-face teaching conducted by a trained research assistant approximately 3-7 days pre-surgery. The booklet contained: (i) Pain and postoperative pain; (ii) pain assessment; (iii) pharmacological pain relief methods; and (iv) non-pharmacological pain relief methods, including the five categories as defined by Pölkki et al. [16]. The video (about 10 minutes) developed based on the booklet's content demonstrated the types of pain medication and modalities available postoperatively and the application of different non-pharmacological pain relief methods for children. The research assistant went through the booklet and video with the parents and demonstrated each pain relief method in a venue preferred by the parent (e.g., an outpatient clinic consultation room at the participating hospital or home). More details about the intervention can be found in other publications [14, 15] (.
Quantitative findings have supported the effectiveness of the programme in improving the outcomes of parents whose children underwent inpatient elective surgery, with significant improvements in parents’ knowledge of pain management and increased use of non-pharmacological methods after the intervention, but not attitudes, satisfaction with pain management and children's postoperative pain [15]. Therefore, it is essential to understand how parents perceived the content and delivery methods of the programme and whether they had any suggestions for improving the intervention programme. Although more and more studies examined the effectiveness of preoperative education for parents [11, 12], limited studies have focused on pain management specifically and reported how parents perceive such pain management educational intervention. Thus, this study aimed to explore the parents’ perceptions of the educational intervention programme regarding their children’s postoperative pain management.
2. Materials and Methods
Study design
A qualitative descriptive study design was used to explore the individual experiences of parents whose children underwent inpatient elective surgery and had received the educational intervention programme on children's postoperative pain management. Semi-structured in-depth interviews were conducted with parents approximately 24 hours after their children’s surgery.
Participants
Purposive sampling was adopted when recruiting participants from a tertiary public hospital, who were allocated to one of the two intervention groups (received an educational booklet and a video, with or without an hour of face-to-face teaching session) of the main study (a three-group randomised controlled trial) in Singapore from September 2013 to January 2015. The selection criteria of children and parents who received the intervention were published in the study protocol [14], with an additional inclusion criterion for parents: only those who had received the educational intervention were eligible [14, 15]. Among the 108 parents in the intervention group [15] in the initial plan, 32 parents (16 from each intervention group) who agreed to participate in the reviews were recruited for this process evaluation. Data saturation was achieved. These parents’ children underwent either ear, nose, and throat surgery, orthopaedic surgery or general surgery in the study hospital.
Data collection
Participants’ data were collected approximately 24 hours after children’s operation in a preferred venue (e.g., a private room at the hospital, participants’ homes, or their offices). No other personnel were present during interviews conducted in the hospital. However, one more team member accompanied the main interviewer when the interviews were conducted in the participant’s home or office. Two female research assistants (one was a registered nurse and the other was a medical doctor previously) approached each parent face-to-face, who agreed to participate in the semi-structured interview. These assistants were not working in the study hospital, and although they were experienced researchers, they received additional training from the principal investigator on conducting interviews. Before the commencement of the interview, one of the two research assistants met parents during the recruitment and intervention process and asked for their interests to be interviewed. During the interviews, the parents were asked to provide their comments and opinions on the content, delivery methods, and impact of the intervention and routine care. All interviews were audio-recorded using a digital recorder. Among 32 interviews, 30 were conducted in English, while two were in Chinese using a Chinese version of the interview guide (approved by the ethical review board). A semi-structured interview guide (Supplementary file) was developed and used in this study. Field notes were taken during interviews to enhance the content of the interview data and improve clarification.
Ethical consideration
This study received ethics approval from the Institutional Review Board of the participating hospital (IRB Reference No: 2013/016/A). Voluntary participation and confidentiality of identity and data were emphasised. All parents were informed about the aim, responsibility, benefits, and risks of participating in the study. Written informed consent was also obtained before any data collection.
Data analysis
Audio-recorded data were transcribed word by word and analysed by inductive thematic analysis [17], which allowed active identification of recurrent patterns embedded in the data to build a detailed description of the data set. An inductive reasoning process enabled the researcher to derive the themes from the primary data instead of the researchers’ analytic preconceptions [18]. The two interviews conducted in Chinese were first transcribed into Chinese and then translated into English before coding. We did not send the transcripts to parents for review since the interviews were straightforward and the interviewers had already clarified any unclear information during the interviews. Transcribed data were reviewed and coded independently by two research assistants to ensure rigour [19]. Four steps were involved in the data analysis: (1) reading transcripts several times to familiarise the data; (2) identifying related words, sentences, or paragraphs representing an idea and coding the data; (3) comparing and grouping codes to generate subthemes based on the similarities of codes; (4) defining and naming themes that were grouped from similar subthemes. We also held regular group meetings to ensure consensus and accurate interpretation of the data, subthemes, and themes.
Rigour
We maintained principles of qualitative rigour to ensure the trustworthiness of findings [20]. Credibility was enhanced through prolonged engagement with the parents during data collection and investigator triangulation during data analysis. Dependability was ensured using purposive sampling, providing a thick description of the interview data, and keeping the audit trail (i.e., field notes, audio recordings, products of data analysis, and interview guides). To achieve confirmability, the interviewers maintained a reflexive attitude through critical self-reflection in the data collection and analysis process to avoid imposing personal viewpoints. Finally, transferability was established by providing detailed descriptions of the contextual information, such as interview settings.
3. Results
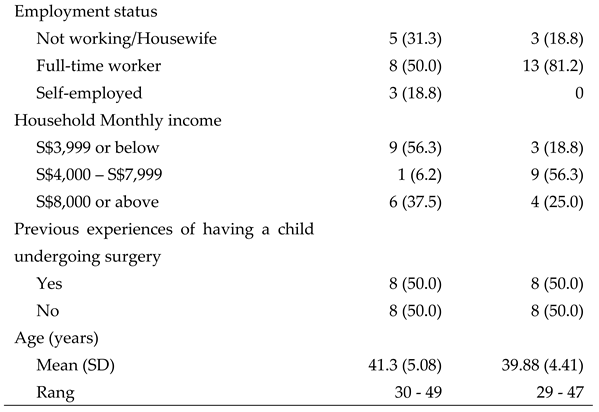
The detailed characteristics of the 32 participants are shown in Table 1. The interviews ranged from 13 to 42 minutes, with an average of 21 minutes. Three themes emerged from the data: (a) current pain management practices, (b) experiences and benefits of the educational intervention, and (c) improvement in education and intervention materials (Figure 1). Relevant quotations from the transcripts supported each theme and subtheme. All quotations were presented in their original form to retain the unique language characteristics of the Singapore participants. Behind each quotation, the participan’s group allocation, interview number and line numbers in the participant’s transcription were provided (e.g. I1 3: L87-90 means Intervention group 1, the 3rd interview, lines 87-90).
Theme 1: Current pain management practices
Parents felt hospitals frequently used pharmacological methods to relieve their children's postoperative pain. Few parents had reported considering reduced reliance on pain relief medications and adopting non-pharmacological methods to control their children’s postoperative pain.
Subtheme 1: Pharmacological approach frequently used by hospital
Many parents expressed that the hospital usually used the pharmacological approach to control their children’s postoperative pain. Besides medication, healthcare professionals did not provide other alternatives to alleviate children’s postoperative pain.
They just give pain killer. However, sometimes even after giving pain killer, some might still complain of pain. The nurse will say, “I cannot give you any more medicine because we already gave you.”(I1 3: L87-90)
They only provided pain medication, other than that, nothing else. They didn’t tell me anything, just gave her medication.(I2 13: L158-159)
Subtheme 2: Application of non-pharmacological methods
Some parents in both intervention groups put the non-pharmacological methods to good use based on what they learned from the educational intervention. A variety of non-pharmacological methods were applied to alleviate children’s postoperative pain.
We tried to let him play the game, drink some water if there is any pain, and read some storybooks. We tried to massage him, and when the position was not so good and not comfortable, (we) adjust a little bit, something like that.(I1 8: L8-10)
I taught him to do deep breathing exercises and some relaxation exercises to help him cope with the pain. I also use the imagery method, where I ask him to imagine all the things and places that he likes to distract him from the pain.(I2 1: L5-9)
When the medicines were not available and my daughter was having some pain, I was talking to her and distracting her from the pain, and putting whatever things to make her fall asleep… (I2 10: L10-13)
Subtheme 3: To reduce reliance on medication and take it only when necessary
Several parents from both intervention groups agreed that there is over-dependency on pain relief medications and were concerned about the potential side effects from long-term consumption. In addition, they acknowledged that the non-pharmacological methods were practical alternatives for managing their children’s postoperative pain.
It is not necessary to depend on pain medication. There are alternatives and other ways to relieve pain. (I1 4: L9-10)
…don’t just rely on the medication itself, which is given at time intervals. There were other ways when he was in discomfort; all the others come in non-pharmacological methods.(I1 14: L21-23)
If children’s pain were only mild and bearable, parents would prefer not to use medications to manage pain as they can lead to side effects. Parents claimed they would only give their children medications when they experienced severe pain.
…what I understand from the book is that it has some side effects if you give the medicine too much. I believe so, so I don’t give the medicine unless she really needs it, like severe pain.(I2 10: L34-36)
If my children told me that they had a bit of pain, I would not give them (Panadol) first. Later if the pain increased, and then I would give it to them. (I2 13: L74-76)
Subtheme 4: Integration of pharmacological and non-pharmacological methods
Some parents found it helpful to apply pharmacological and non-pharmacological pain management methods concurrently. As the medications could only be given during fixed time intervals, the non-pharmacological methods helped to control children’s postoperative pain in the event of pain recurring after the medicine’s effects wore off.
Medication was given, and the pain disappeared at first … That (pain) occurred a few hours after taking medication, so that is why we need to use both methods. (I18: L70-72)
Medication administration has time intervals. After taking medicine for a while, the pain started to come, so I told him to use relaxation and it helped. (I2 8: L29-29)
Theme 2: Experiences and benefits of the educational intervention
Parents who had received the educational intervention with one-hour face-to-face teaching pointed out the advantages of face-to-face teaching. Both intervention groups gave positive and negative comments regarding the video and booklet. However, regardless of the type of educational intervention, it improved parents' knowledge and attitudes towards managing their children’s postoperative pain.
Subtheme 1: Advantages of face-to-face teaching
Parents who had received the one-hour face-to-face teaching found it helpful to attain the knowledge and experience. They could ask questions and learn accurate non-pharmacological methods from trained personnel before applying them to their children.
…I gained more knowledge from face-to-face teaching because there is someone who explains it, and I also can ask questions if I have, rather than just watching TV and reading booklets. (I1 1: L13-15)
Subtheme 2: Comments on the video
Most parents found that the video had given them a clearer understanding of the non-pharmacological methods. As parents watched the demonstration of non-pharmacological methods, they better understood how to apply them. Several parents even compared the video to the booklet, commenting that the video was a better educational tool.
If you would give the booklet alone, we will not be easily understood the method. However, with the DVD, it is better because the DVD actually demonstrates the methods.(I2 15: L159-160)
However, as the video required a DVD player and time to watch, it posed inconveniences to some parents.
For DVD, you need to put it in the player, but we do not really have the time (to watch it), sometimes no time to sit down. (I21: L53-54)
Subtheme 3: Comments on the booklet
Many parents commented that the booklet was simple to understand and a good reference guide, especially with the pictures. However, the information may be too technical for a layperson and can be explained using simpler terms.
The booklet is quite good, simple enough with pictorial representation for most parents to understand. (I17: L74-75)
For the booklet, I think it is a good reference because it is pretty simplified. However, personally speaking, some of the information is too technical for a layman person. (I2 9: L7-9)
Subtheme 4: Beneficial in improving knowledge and attitudes towards pain management
Parents from both intervention groups expressed that the educational intervention benefited them by providing knowledge on managing and alleviating their children’s postoperative pain with non-pharmacological methods.
It is very useful … at least parents know what to expect and what to do when the child complains of pain. (I2 8: L52-54)
… (via the education) I do realise that actually there are a lot of ways to help him with pain management… I do realise that touching or rubbing his back is also helping him ease the pain.(I214: L8-10)
They were receptive to the non-pharmacological methods and subsequently minimised the reliance on medications to relieve their children’s pain.
If not, I just “Pain pain, take medicine, pain pain, take medicine”. But with the education that has been given to me, besides using Panadol, I used other methods like praising him or communicating more to distract him from feeling the pain.(I116: L13-16)
Theme 3: Suggestions to improve pain management
Some parents suggested enhancing post-operative pain management by refining educational materials and encouraging healthcare professionals to take more initiative in teaching non-pharmacological pain relief methods.
Subtheme 1: Refining the educational materials
Regarding the video, parents proposed including a more detailed video with specific and appropriate massage sites for patients undergoing different operations, narrating the video in different languages to benefit non-English speaking parents, and having the DVD available online for easy access.
Maybe the video can indicate specific massages for patients with different operation sites. (I2 6: L90-93)
It can be narrated in different languages… it would be good, rather than they read the subtitles to understand. (I112: L115-116)
For the DVD, you can actually make it available online, and you can actually access it. (I29: L344-346)
One parent suggested using a point-form presentation in the booklet, and another recommended having more detailed explanations on each topic.
…just go to point form, which could be done because yours is an expanded level, so it can go to the concise level to point form (I1 9: L1128-129)
I notice the booklet covers many topics, but just brief paragraphs on each (topic) so that it could be more informative (I2 1: L127-129)
Subtheme 2: More initiative in teaching non-pharmacological methods by healthcare professionals
A few parents suggested that healthcare professionals, especially nurses, be well-trained in non-pharmacological pain management. This is so that these healthcare professionals can routinely share such knowledge with parents to help manage their children’s postoperative pain.
The suggestion is that nurses should be educated on (these methods), at least give some background on what it is, pass the information on a general basis to parents. (I1 4: L97-98)
If there is a really good use of the non-pharmacological methods, the nurses can share with the patients how to use these methods other than giving the medicine only. (I2 10: L150-152)
Maybe quarterly or half-yearly, there should have this kind of courses for all the nurses. You know they should learn how to handle all these postoperative pain management, the non-medication way. (I2 11: L213-215)
4. Discussion
This study aimed to explore the perceptions of parents whose children had undergone inpatient elective surgery on a pain management educational intervention programme, which aids the researchers in understanding its strengths and weaknesses. Our findings indicated that most parents expressed how pain medications were primarily used to manage children’s postoperative pain in the hospital and that nurses rarely included non-pharmacological pain relief methods.
Notably, a previous study indicated that most parents and children felt that simple analgesia was inadequate in controlling postoperative pain of children after surgical procedures such as tonsillectomy and adenotonsillectomy [21]. As such, non-pharmacological pain management strategies may be suggested as they are known to be applicable for patients in all age groups and are effective in relieving pain, with and without additional pharmacological intervention [12, 22-25]. Our findings were congruent with a best practice implementation project in that postoperative pain management practices remain suboptimal and non-pharmacological methods were not used as there was a lack of education provided to parents [3]. Pain medications are currently the primary strategy used in the hospital setting to control children’s pain, and nurses in Singapore do not commonly apply non-pharmacological methods. The inadequacy in adopting non-pharmacological pain relief methods may be attributed to the nurses’ concerns about an anticipated increase in workload or their lack of knowledge and expertise on these strategies [3, 26] 3. Valizadeh et al. [27] also suggested that some nurses might lack sensitivity and awareness of patients' pain management needs, which diminishes their application of these non-pharmacological methods. Therefore, it is imperative to equip nurses with the skills to communicate non-pharmacological and pharmacological pain relief strategies to parents and help them develop a positive attitude towards such methods in paediatric pain management [3, 28].
Our intervention programme exposed parents to various non-pharmacological methods, including deep breathing, massage, distraction, imagery, and emotional support, to alleviate their children’s postoperative pain [15]. As a result, parents reported a reduced reliance on pharmacological medication; instead, they tried to incorporate non-pharmacological approaches to manage their children’s pain. These findings were congruent with our quantitative findings [15], which also showed that our educational programme positively influenced parents’ behaviour towards pain management and effectively increased the frequency of non-pharmacological methods used to alleviate their children’s pain. Our findings were also in line with previous studies that educational interventions effectively improved parents’ knowledge, and care behavior, and helped reduce their misconceptions about pain medications [10]. Hence, parents can become more competent in managing their children’s pain if they are educated in pain assessment and pharmacological and non-pharmacological pain management interventions [3, 29]. As reported, parents should be partners in caregiving and decision-making [5], allowing parents to play an active role in managing their children’s pain [3].
This study also showed that the pain management educational intervention was beneficial in improving parents’ knowledge and attitudes towards pain management. This finding was consistent with previous findings that educational intervention in pain management could improve nurses’ knowledge, attitudes, and behaviour related to children’s postoperative pain management [30, 31]. Our findings proved that providing parents with educational intervention programmes regarding strategies and specific techniques for their children’s postoperative pain management is valuable and necessary. Similarly, guidelines on postoperative pain management also recommended providing individually tailored education to patients and caregivers on options for postoperative pain management, appropriate pain assessment, and documenting the plan and goals for postoperative pain management [3, 32] .
The parents also commented on intervention delivery methods and the content of the educational materials in this study. They pointed out the advantages of face-to-face teaching as an effective platform for parents to ask questions, learn practical skills, and conduct return demonstrations of specific non-pharmacological methods from healthcare professionals. This implies that parents enjoy the interactive modality of the educational programme, and this may potentially enhance the programme’s effectiveness. However, adding the in-person education session requires staffing time and effort. Future study designs for similar programmes could either consider incorporating such in-person teaching methods or use mobile health to enable interaction between healthcare professionals and parents. Moreover, some parents stated that it was inconvenient having to play the video using a DVD player. Researchers could develop technology-based educational solutions for parents to extend capacity and easy access, a possible trend for pain management in the future [33]. A technology-based programme with interactivity, personalisation, tailored messages, and easy therapist contact can maximise the programme's efficacy [34]. In fact, several studies have piloted the capabilities of technology-based programmes for parents [35] or children [36, 37] in controlling children’s pain and anxiety, which could provide some ideas for future researchers to develop similar programmes.
Strengths and Limitations of this study
This study was the first to explore how parents perceived a pain management educational intervention regarding their children’s postoperative pain management. The findings provide helpful information for healthcare professionals working in pediatric settings to involve and empower parents to manage their children’s postoperative pain and for researchers to improve the intervention for future use. However, this study had several limitations. We only interviewed participants who were willing to participate in the interviews; they might have potentially higher motivations to share their experiences with the researcher or better experiences. Those who did not want to be interviewed might have had poorer experiences, which were not captured in this study. Moreover, most participants were well-educated, employed, and belonged to higher-income groups, the viewpoints of parents from the lower socio-economic group were not captured.
Implications for Nursing Practice and Recommendations for Future Studies
This research generated a comprehensive understanding of the perceptions of strengths and weaknesses among parents attending an educational intervention programme. While quantitative findings have supported the programme's effectiveness [15], constant efforts to address barriers faced by participants are valuable in informing the design of future interventions. Our findings pointed out that involving parents in caring for their children’s postoperative pain management was beneficial. It is critical for healthcare professionals to routinely advocate for educational interventions for parents with children undergoing surgery. Improving healthcare professionals’ knowledge and skills in non-pharmacological methods to teach parents about pain management is also recommended. Future studies could recruit parents of low socio-economic status, explore their needs, and develop suitable interventions for them. Moreover, incorporating technologically-based delivery of such programmes may revolutionise pain management in the future and contribute to ease of access to a broader community, enhancing their health outcomes [35].
5. Conclusions
Our findings indicated that medication was a primary approach to control children’s postoperative pain in hospitals and parents receiving the educational interventions had reduced reliance on medication through integrating pharmacological and non-pharmacological strategies for their children’s postoperative pain management. Participants felt they benefitted from the educational interventions and that the educational interventions, with or without one-hour face-to-face teaching, helped prepare parents and their children who underwent inpatient elective surgery for postoperative pain management. Healthcare professionals could use the intervention materials to support parents of children undergoing surgery. Future studies could target parents of lower socio-economic status and incorporate more sustainable and accessible technology to deliver such interventions.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org.
Author Contributions
Conceptualization, H.H.G., C.W.C.S. and C.K.F.K.; Methodology, H.H.G., C.W.C.S. and C.K.F.K.; Software, Z.L.X.; Validation, H.H.G. and Z.L.X.; Formal Analysis, H.H.G., Z.L.X. and H.C.Y.; Investigation, Z.L.X. and L.L.W.J.; Resources, H.H.G., and L.L.W.J.; Data Curation, H.H.G.; Writing – Original Draft Preparation, Z.L.X., and H.C.Y.; Writing – Review & Editing, H.H.G., C.W.C.S, N.S.X., L.L.W.J. and C.K.F.K.; Visualization, H.C.Y.; Supervision, H.H.G.; Project Administration, H.H.G.; Funding Acquisition, H.H.G., C.W.C.S. and C.K.F.K..
Funding
This study was funded by the Health Services Research Competitive Research Grant, Ministry of Health, Singapore (Award No.: HSRG/0024/2012).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the SingHealth Centralised Institutional Review Board in Singapore (CIRB Ref: 2013/016/A).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to confidentiality of the data.
Acknowledgments
We thank the Nurse Managers and Nurse Clinicians of the study venue for their great support. We thank all the parents and their children who participated in this study. We appreciate Ms Saw Sandar Ko and Ms Xiao Chunxiang for their help with the data collection.
Conflicts of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Links, A.R. , Callonb, W., Wasserman, C., Jonathan Walsha, J., Tunkela, D.E., Beachc, M.C., & Boss, E.F. Parental role in decision-making for pediatric surgery: Perceptions of involvement in consultations for tonsillectomy. Patient Educ. Couns. 2020, 103, 944–951. [Google Scholar]
- Makhlouf, M.M.; Garibay, E.R.; Jenkins, B.N.; Kain, Z.N.; A Fortier, M. Postoperative pain: factors and tools to improve pain management in children. Pain Manag. 2019, 9, 389–397. [Google Scholar] [CrossRef]
- Yang, J.; Zhang, W.; Huang, H.; Jiang, W.; Zhou, Y.; Gu, Y.; Xu, H.; Yao, W.; Zhang, F. Parental involvement in postoperative pain management among children in a urology ward: A best practice implementation project. First published: 25 December 2022, 25 December. [CrossRef]
- Dagg, W.; Forgeron, P.; Macartney, G.; Chartrand, J. Parents’ management of adolescent patients’ postoperative pain after discharge: A qualitative study. Can. J. Pain 2020, 4, 51–60. [Google Scholar] [CrossRef]
- Palomaa, A.-K.; Korhonen, A.; Pölkki, T. Factors Influencing Parental Participation in Neonatal Pain Alleviation. J. Pediatr. Nurs. 2016, 31, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, M.G.; Wakefield, C.E.; Vetsch, J.; Karpelowsky, J.S.; Darlington, A.-S.E.; Grant, D.M.; Signorelli, C. The Psychosocial Experiences and Needs of Children Undergoing Surgery and Their Parents: A Systematic Review. J. Pediatr. Heal. Care 2017, 32, 133–149. [Google Scholar] [CrossRef] [PubMed]
- Simons, J.; Carter, B.; Craske, J. Developing a Framework to Support the Delivery of Effective Pain Management for Children: An Exploratory Qualitative Study. Pain Res. Manag. 2020, 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Mackey, S.; Liam, J.L.W.; He, H. An exploration of Singaporean parental experiences in managing school-aged children’s postoperative pain: a descriptive qualitative approach. J. Clin. Nurs. 2011, 21, 860–869. [Google Scholar] [CrossRef] [PubMed]
- Chng, H. Y. , He, H. G., Chan, S. W. C., Liam, J. L. W., Zhu, L., & Cheng, K. K. F. (2015). Parents’ knowledge, attitudes, use of pain relief methods and satisfaction related to their children's postoperative pain management: a descriptive correlational study. Journal of Clinical Nursing, 24(11-12), 1630-1642.
- Huth, M.M.; Broome, M.E.; Mussatto, K.A.; Morgan, S.W. A study of the effectiveness of a pain management education booklet for parents of children having cardiac surgery. Pain Manag. Nurs. 2003, 4, 31–39. [Google Scholar] [CrossRef]
- Yadav, M. , Malar Kodi, S., & Deol, R. (2020). Effect of preoperative educational schedule on anxiety and coping mechanism among children and their parents: A randomized controlled trial. Journal of Pediatric Surgical Nursing, 9(4), 127-135.
- Chartrand, J.; Tourigny, J.; MacCormick, J. The effect of an educational pre-operative DVD on parents’ and children's outcomes after a same-day surgery: a randomized controlled trial. J. Adv. Nurs. 2016, 73, 599–611. [Google Scholar] [CrossRef]
- Martins Esteves, I. , Silva Coelho, M., Neves, H., Pestana-Santos, M., & Santos, M.R. (2022). Effectiveness of family-centred educational interventions in the anxiety, pain and behaviours of children/adolescents and their parents’ anxiety in the perioperative period: a systematic review and meta-analysis. Journal of Perioperative Nursing, 35(1), Article 1.
- He, H.; Zhu, L.; Chan, W.S.; Xiao, C.; Klainin-Yobas, P.; Wang, W.; Cheng, K.F.K.; Luo, N. A randomized controlled trial of the effectiveness of an educational intervention on outcomes of parents and their children undergoing inpatient elective surgery: study protocol. J. Adv. Nurs. 2014, 71, 665–675. [Google Scholar] [CrossRef]
- Zhu, L.; Chan, W.-C.S.; Liam, J.L.W.; Xiao, C.; Lim, E.C.C.; Luo, N.; Cheng, K.F.K.; He, H. Effects of postoperative pain management educational interventions on the outcomes of parents and their children who underwent an inpatient elective surgery: A randomized controlled trial. J. Adv. Nurs. 2018, 74, 1517–1530. [Google Scholar] [CrossRef] [PubMed]
- Pölkki, T.; Vehviläinen-Julkunen, K.; Pietilä, A.-M.; Mnsc, T.P. Nonpharmacological methods in relieving children’s postoperative pain: a survey on hospital nurses in Finland. J. Adv. Nurs. 2001, 34, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77-101. Vaismoradi, M., Turunen, H., & Bondas, T. (2013). Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nursing & Health Sciences, 15(3), 398-405. [CrossRef] [PubMed]
- Houghton, C.; Casey, D.; Shaw, D.; Murphy, K. Rigour in qualitative case-study research. Nurse Res. 2013, 20, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Noble, H. , & Smith, J. (2015). Issues of validity and reliability in qualitative research. Evidence-Based Nursing, 18(2), 34-35. [CrossRef]
- Oremule, B.; Johnson, M.; Sanderson, L.; Lutz, J.; Dodd, J.; Hans, P. Oral morphine for pain management in paediatric patients after tonsillectomy and adenotonsillectomy. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 2166–2169. [Google Scholar] [CrossRef]
- Bergomi, P.; Scudeller, L.; Pintaldi, S.; Molin, A.D. Efficacy of Non-pharmacological Methods of Pain Management in Children Undergoing Venipuncture in a Pediatric Outpatient Clinic: A Randomized Controlled Trial of Audiovisual Distraction and External Cold and Vibration. J. Pediatr. Nurs. 2018, 42, e66–e72. [Google Scholar] [CrossRef]
- Bukola, I.M.; Paula, D. The Effectiveness of Distraction as Procedural Pain Management Technique in Pediatric Oncology Patients: A Meta-analysis and Systematic Review. J. Pain Symptom Manag. 2017, 54, 589–600. [Google Scholar] [CrossRef]
- Olsen, S. W. , Rosenkilde, C., Lauridsen, J., & Hasfeldt, D. (2020). Effects of Nonpharmacologic Distraction Methods on Children's Postoperative Pain—A Nonmatched Case-Control Study. Journal of Perianesthesia Nursing, 35(2), 147-154.
- Short, S.; Pace, G.; Birnbaum, C. Nonpharmacologic Techniques to Assist in Pediatric Pain Management. Clin. Pediatr. Emerg. Med. 2017, 18, 256–260. [Google Scholar] [CrossRef]
- Ismail, A.; Forgeron, P.; Polomeno, V.; Gharaibeh, H.; Harrison, D. Pain Management Practice and Guidelines in Jordanian Pediatric Intensive Care Units. Pain Manag. Nurs. 2018, 19, 195–203. [Google Scholar] [CrossRef]
- Valizadeh, F.; Ahmadi, F.; Zarea, K. Neglect of Postoperative Pain Management in Children: A Qualitative Study Based on the Experiences of Parents. J. Pediatr. Nurs. 2016, 31, 439–448. [Google Scholar] [CrossRef]
- Islam, M.R.; Biswas, H.B.; Hossain, M.S.; Kim, H.S.; Azim, A.; Nath, P.; A Ali, M. Knowledge and Practice of Nurses on Pediatric Pain Management in Bangladesh. Mymensingh Medical Journal 2020, 29, 86–91. [Google Scholar] [PubMed]
- Chung, W. W. , Agbayani, C. J. G., Martinez, A., Le, V., Cortes, H., Har, K.,... & Fortier, M. A. (2018). Improving Children's cancer pain management in the home setting: Development and formative evaluation of a web-based program for parents. Computers in Biology and Medicine, 101, 146-152.
- He, H.-G.; Vehviläinen-Julkunen, K.; Pietilä, A.-M.; Pölkki, T. Increasing Nurses' Knowledge and Behavior Changes in Nonpharmacological Pain Management for Children in China. J. Nurs. Care Qual. 2008, 23, 170–176. [Google Scholar] [CrossRef] [PubMed]
- He, H.G. , Vehviläinen-Julkunen, K., Pölkki, T., & Pietilä, A.M. (2010). Chinese parents' perception of support received and recommendations regarding children's postoperative pain management. International Journal of Nursing Practice, 16, 254-261.
- Chou, R.; Gordon, D.B.; de Leon-Casasola, O.A.; Rosenberg, J.M.; Bickler, S.; Brennan, T.; Carter, T.; Cassidy, C.L.; Chittenden, E.H.; Degenhardt, E.; et al. Management of Postoperative Pain: A Clinical Practice Guideline From the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists' Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J. Pain 2016, 17, 131–157. [Google Scholar] [CrossRef]
- Fortier, M. A. , Yang, S., Phan, M. T., Tomaszewski, D. M., Jenkins, B. N., & Kain, Z. N. (2020). Children's cancer pain in a world of the opioid epidemic: Challenges and opportunities. Pediatric Blood and Cancer, 67(4), e28124.
- Gogovor, A.; Visca, R.; Auger, C.; Bouvrette-Leblanc, L.; Symeonidis, I.; Poissant, L.; Ware, M.A.; Shir, Y.; Viens, N.; Ahmed, S. Informing the development of an Internet-based chronic pain self-management program. Int. J. Med Informatics 2017, 97, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Kwa, Z.Y. (2020). Developing and testing the feasibility and preliminary effects of an intelligent customer-driven solution for paediatric surgery care on the improvement of outcomes of parents and their children undergoing circumcision (ICory- Circumcision): A pilot randomised controlled trial. Honour’s Thesis. Singapore: National University of Singapore.
- Fortier, M. A. , Chung, W. W., Martinez, A., Gago-Masague, S., & Sender, L. Pain buddy: A novel use of m-health in the management of children's cancer pain. Computers in Biology and Medicine, 2016, 76, 202–214. [Google Scholar]
- Wang, G.G. (2018). Preliminary effects of using mobile games to reduce perioperative anxiety and postoperative pain in children undergoing elective surgery: A pilot randomised controlled trial. Honour’s Thesis. Singapore: National University of Singapore.
Figure 1.
Themes and subthemes of the study (n = 32)
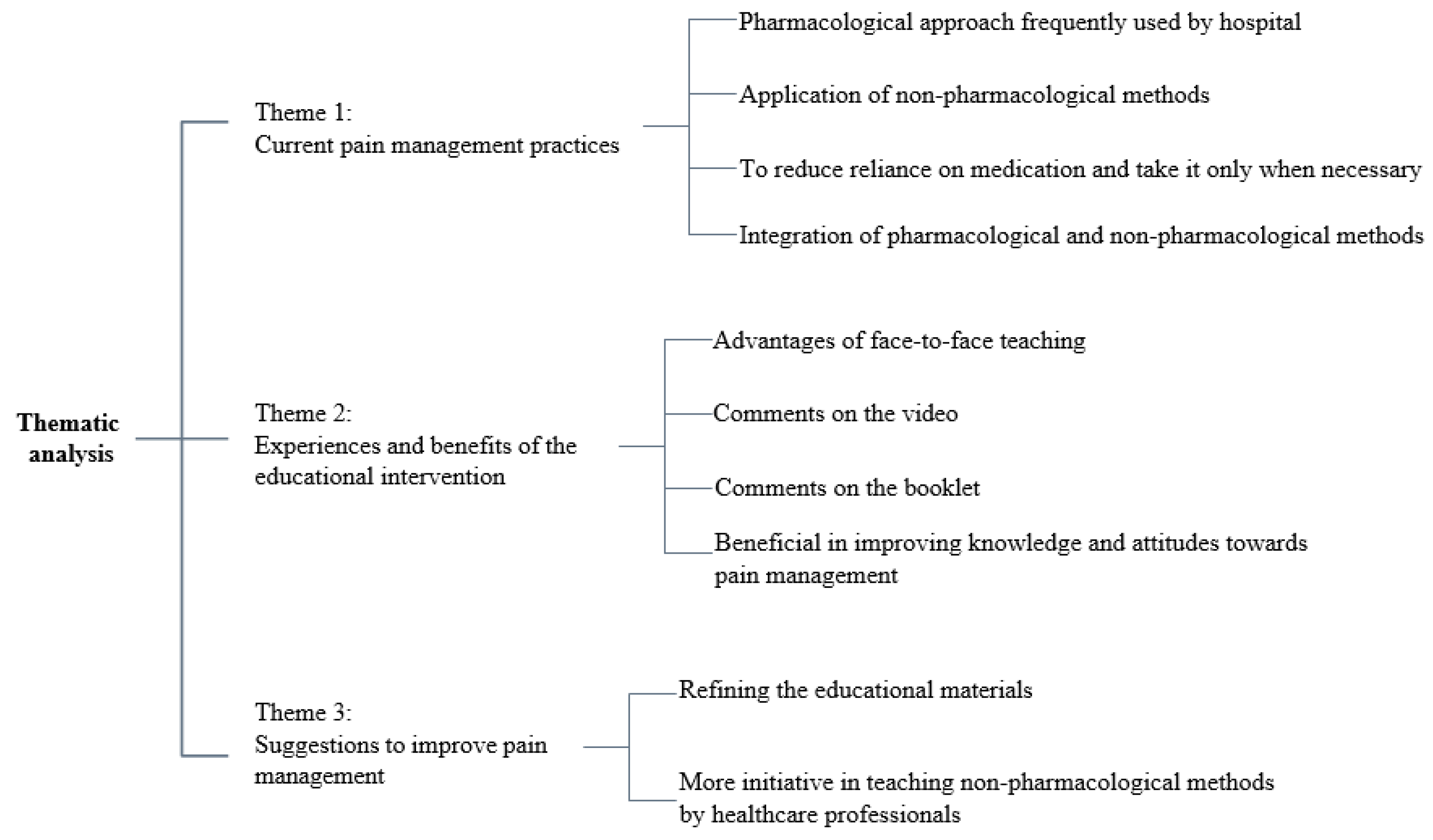

Table 1.
Demographic information of parents in this study (n = 32).
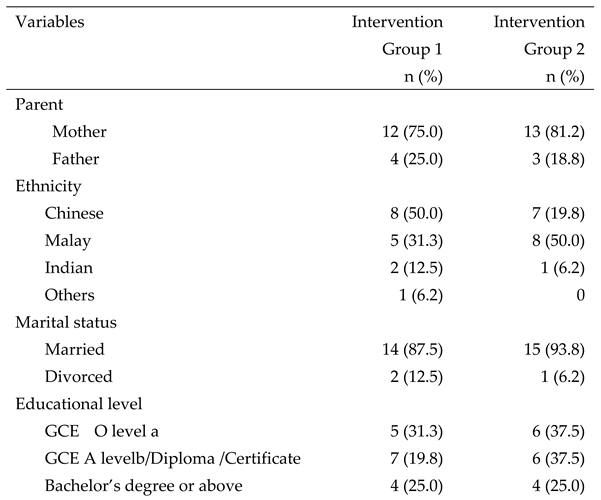

Note: a ‘O’ level: Singapore-Cambridge General Certificate of Education Ordinary Level; b ‘A’’ level: The
Singapore-Cambridge General Certificate of Education Advanced Level.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



