
Submitted:
13 September 2023
Posted:
14 September 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Tixagevimab–cilgavimab are effective for treatment of early COVID-19 among outpatients with risk factors for progression to severe illness, as well as for primary prevention and post-exposure prophylaxis. We aimed to retrospectively evaluate the hospital stay (expressed in days), prognosis, and negativity rate for COVID-19 after treatment with tixagevimab–cilgavimab.
We enrolled 42 patients who were nasal swab positive for SARS-CoV-2 (antigenic and molecular), both vaccinated and not vaccinated for COVID-19, hospitalized at the first division of the Cotugno Hospital in Naples and who received intramuscular single dose of tixagevimab-cilgavimab (300 mg / 300 mg). All patients candidates for tixagevimab-cilgavimab had immunocompromised immune system either for chronic degenerative disorders (Group A: 27 patients) or onco-hematological diseases (Group B: 15patients). Patients enrolled in group A came to our observation after 10 days from the detection of positivity to COVID-19 unlike the other types of patients enrolled in this study. The mean stay in hospital of patients in Group A was 21±5 days vs 25±5 days in Group B. Twenty patients resulted negative after a median of hospitalization stay of 16 days (IQR: 18-15.25), of them 5 (25%) patients belonged to group B. Therefore, patients with active hematological malignancy had the lower negativization rate.
Keywords:
COVID19
; Tixagevimab–cilgavimab
; Remdesivir
1. Introduction
Antiviral therapies alone are not sufficient to change the course of the COronaVIrus Disease 2019 (COVID-19) [1], especially in frail patients. Therefore, identifying new therapeutic options to prevent or fight this disease is essential [2].
Tixagevimab–cilgavimab is a long acting monoclonal antibody combination of two Fc-modified human monoclonal antibodies obtained from patients who recovered from COVID-19. Tixagevimab and cilgavimab bind non-overlapping sites of the spike (S) glycoprotein of the Severe Acute Respiratory Syndrome COronaVirus-2 (SARS-CoV-2), the causative agent of COVID-19 [3]. The Fc region was modified to extend their half-life (about 90 days) and reduce the binding to the Fc receptor and C1q complement minimizing the risk of increasing disease inflammation [4,5]. This extended half-life could also offer the advantage of a long-term protection against symptomatic COVID-19 compared to shorter half-lives of other anti-SARS-CoV-2 monoclonal antibodies (approximately 18–32 days) [6,7,8]. Tixagevimab-cilgavimab by binding different sites of the S protein may also help to overcome the immune escape and maintain susceptibility to SARS-CoV-2 variants [9]. Based on this beneficial properties, this combination was authorized in Europe for the treatment of early COVID-19 among outpatients (aged ≥12 years and weighed at least 40 Kg) who do not require oxygen supplement therapy and have risk factors for progression to severe illness, as well as for pre-exposure prophylaxis to SARS-CoV-2 [10].
After the marketing authorization, a randomized, phase 3, clinical trial was published. This trial compared tixagevimab–cilgavimab with placebo in hospitalized COVID-19 patients receiving remdesivir and standard care, finding no improvement in the primary outcome (time to sustained recovery) but a good safety profile and a low mortality rate in the tixagevimab–cilgavimab group [11]. Moreover, few evidence described the use of tixagevimab–cilgavimab in patients affected by hematological malignancies or impaired immune system [12,13].
Although tixagevimab-cilgavimab seems to be an important therapeutic strategy for protecting people who cannot be vaccinated or respond poorly to COVID-19 vaccines and to treat early COVID-19, based on the few real-world evidence available in frail patients, further researches are needed to better define the place in therapy of this medicine. Therefore, we decided to conduct a retrospective observational chart review to describe the use of tixagevimab-cilgavimab in patients affected by COVID-19 and other comorbidities.
2. Materials and Methods
In this observational retrospective chart review study, we enrolled patients who were nasal swab positive for SARS-CoV-2 (Antigenic and molecular), vaccinated or not for COVID-19, hospitalized at the first division of the Cotugno Hospital in Naples (UOC of Emerging and Highly Contagious Infectious Diseases) and who received a therapeutic dose of tixagevimab-cilgavimab from July 8, 2022 to January 10, 2023. Patients received an intramuscular single dose of tixagevimab-cilgavimab at 300 mg/300 mg.
Patients were divided into two groups: those affected by chronic disorders (group A) and those affected by oncohaematological diseases (group B). The two groups were evaluated for the length of stay in hospital (expressed in days) and negativity for COVID-19 at follow-up. Patients’ venous blood sampling was analyzed for immunoglobulins A (IgA), M (IgM), and G (IgG), C-reactive protein (CRP), procalcitonin, interleukine-6 (IL6), D-dimer, and fibrinogen. High resolution CT scan of the chest (HR chest CT) at hospital admission was also performed. Antigen research for SARS-CoV2 was carried out on the nasal swab (Methodical: Chemiluminescence Enzyme ImmunoAssay), also the search for viral RNA was carried out with the Real time PCR.
Positivity for antispike antibodies did not exclude treatment with intramuscular tixagevimab-cilgavimab.
3. Results
Forty-two patients were enrolled and received tixagevimab-cilgavimab. All patients were affected by omicron SARS-CoV-2 variants and were hospitalized for causes other than COVID-19. No patient complained for side effects related to the administration of tixagevimab-cilgavimab.
Of the 42 enrolled patients, 21 were females and 21 were males, with a median age of 71 years (Interquartile range, IQR: 78.5-59.0). Fifteen patients had onco-hematological diseases (Group B); specifically, 11 patients were affected by active non-Hodgkin lymphoma (NHL), and 4 patients by chronic lymphocytic leukemia (CLL). A total of 27 patients were affected by chronic disorders (Group A), including cardiovascular disorders (n=8), degenerative diseases (n=7), solid tumors (n=5), infections (n=4), and autoimmune diseases (n=3). Ten (37%) patients of group A were affected by more than one chronic disorder. Basal characteristics of these patients are shown in table 1, while the underlying pathologies in table 2. Eleven (40.7%) patients of group A and 12 (80.0%) patients of group B were treated with remdesivir (Table 1). One patient of group B did not receive remdesivir treatment because she was discharged against the advice of the health care workers in oxygen therapy with a Venturi mask (during the short hospitalization the patient presented a rapid worsening of respiratory function). Patients with NHL and CLL also had immunoglobulins deficiency. Two patients presented sepsis upon admission to the hospital. One patient had legionella pneumonia. The enrolled patients presented a variegated pulmonary CT picture (Table 3).
Of the 42 enrolled patients, 16 patients were unvaccinated (12 patients for group A and 4 patients in group B). IL-6 levels were similar between groups. CRP at admission was higher in Group A compared to Group B (Table 1). Moreover, in stratifying CRP levels for remdesivir treatment we found an higher median levels for remdesivir 5 mg (Median: 20.5; IQR: 27.06-9.70, Figure 1).
The mean stay in hospital of patients in Group A was 21±5 days vs 25±5 days in Group B. Twenty patients resulted negative after a median of hospitalization stay of 16 days (IQR: 18-15.25), of them 5 (25%) patients belonged to group B. Eight patients died from COVID-related respiratory failure: 4 for each group. 2 patients in Group B presented respiratory distress syndrome . Patients enrolled in our study and affected by CLL and NHL came to our observation after 10 days from the detection of positivity to COVID-19 unlike the other types of patients enrolled in this study.
4. Discussion
Treatments are needed for patients with COVID-19 at high risk of being hospitalized or death, such as older adults, those with multiple comorbidities, or patients immunocompromised [14,15,16,17]. Specifically, patients with an impaired immune system are at higher risk of prolonged or unresolved SARS-CoV-2 infection, which might also facilitate the development of new variants [18]. In fact, the presence of active malignancy as well as the type of hematological malignancy, altogether with age, presence of comorbidities, stay in the Intensive Care Unit, and need of mechanical ventilation are recognized risk factors for adverse outcomes in patients with COVID-19 and hematological malignancies [19].
In this study, we observed a mean stay in hospital similar between patients treated with tixagevimab-cilgavimab affected by onco-hematological tumor or those affected by chronic disorders in spite of a higher negativization rate for those affected by chronic disorders (75%). Indeed, patients with hematologic malignancy are characterized by a more compromised immune response to SARS-CoV-2 and high mortality rate (about 34%) [19]. Moreover, hematologic patients can have an impaired response to COVID-19 vaccines by failing in the production of anti-S antibodies after a full vaccination cycle [20]. This poor response is common in patients with B cell tumors, such as the CLL [21]. Our hematologic patients mostly had a 3-dose schedule of COVID-19 vaccines (n= 10; 66.7%). In the literature, the administration of tixagevimab-cilgavimab did not show to change the response to COVID-19 vaccines [22], but rather to potentiate the pre-existing protection against SARS-CoV-2 infection, also in immunocompromised patients receiving a full vaccination [23,24].
Moreover, the low negativization rate observed in patients with hematological tumors may also be due to the delayed start of treatment with tixagevimab-cilgavimab, since patients came to our observation only after 10 days from the positivity to COVID-19. This may suggest the importance of starting early the treatment with tixagevimab-cilgavimab to have a higher probability of a good and effective clinical response to the therapy.
Generally, the effectiveness and safety of tixagevimab-cilgavimab as pre-exposure prophylaxis against COVID-19 was widely evaluated. A meta-analysis found that tixagevimab-cilgavimab prophylaxis may reduce the rate of SARS-CoV-2 infection (OR: 0.24; 95% CI: 0.15-0.40) and COVID-19 hospitalization (OR: 0.13; 95% CI: 0.07-0.24), and decrease the severity (OR: 0.13; 95% CI: 0.07-0.24), and mortality (OR: 0.17; 95% CI: 0.03-0.99) associated with COVID-19 [25]. Another meta-analysis evaluated the effectiveness of tixagevimab-cilgavimab prophylaxis in immunocompromised participants, including patients with hematological malignancies, confirming an overall clinical effectiveness of tixagevimab/cilgavimab in terms of hospitalisation, intensive care admission and mortality [26]. Both meta-analyses showed the efficacy and safety of tixagevimab-cilgavimab for preventing COVID-19. However, its efficacy as post-exposure treatment has been more conflicting. A randomised, double-blind, phase 3, placebo-controlled trial (ACTIVE-3 study) investigating the efficacy of tixagevimab-cilgavimab compared to placebo in patients treated with remdesivir and other standard therapy found no improvement in the primary outcome of time to sustained recovery with tixagevimab–cilgavimab but it was safe and with low mortality [11]. Another phase 3 study (STORMCHASER study) evaluated the treatment with tixagevimab/cilgavimab as post-exposure prophylaxis against symptomatic COVID-19, finding no difference in the incidence of post-dose positive symptomatic COVID-19 compared to placebo [27]. On the contrary, the phase 3, randomized, double-blind, placebo-controlled trial (TACKLE study) demonstrated that tixagevimab/cilgavimab can prevent the development of severe COVID-19 by reducing the risk of severe COVID-19 or death of 50.5% (95%CI 14.6–71.3; p=0.0096) and 66.9% (95%CI 31.1–84.1; 0.0017) in patients with mild or moderate COVID-19 overall and symptomatic for less than 5 days, respectively [8]. In particular, this study suggested the efficacy of tixagevimab/cilgavimab in reducing COVID-19 progression and death in high risk patients [8]. However, it should be highlighted that the most representative risk factors (>10%) were obesity, smoking, hypertension, diabetes, and lung diseases, while the immunocompromised state was underrepresented [8].
We observed a good safety profile for tixagevimab/cilgavimab in accordance with results of aforementioned clinical trials, in which most event were found mild and moderate in severity, with an incidence similar between the tixagevimab–cilgavimab and placebo groups [8,11,27].
In our study, all patients were affected by omicron variants. In this regards, in-vitro studies have shown the efficacy of tixagevimab/cilgavimab in neutralizing the BA.1, BA.1.1, BA.2, BA.2.12.1, BA.3, BA.4, and BA.5 omicron subvariants with a potency within the half maximal inhibitory concentration (IC50) range of 4.0–806.0 ng/mL [28,29,30,31].
The main limitation of our study was the small number of patients enrolled and treated with tixagevimab-cilgavimab, which also hindered the execution of an adequate statistical analysis. Even so, we described our experience on the use of tixagevimab-cilgavimab in patients with chronic and onco-hematological disorders, thus providing new data on the safety and efficacy of this therapy in frail patients.
5. Conclusion
In conclusion, patients with active hematological malignancy are those with the worst prognosis for COVID-19, despite the therapy with tixagevimab-cilgavimab and remdesivir. These results, according to the new COVID19 wave currently interesting Europe and USA [32], could be considered to early intercept frail patients to be treated as soon as possible with current antiviral and monoclonal antibodies. Therefore, it could be useful to sensitize hematologists and patients with active hematological malignancies to early start the pharmacological treatment (within 10 days from the detection of COVID-19 positivity). Further studies with an adequate sample size are needed to better elucidate the efficacy and safety of tixagevimab-cilgavimab in patients with COVID-19 and affected by chronic comorbidities or an impaired immune response.
Conflicts of Interest
The authors declare no conflict of interest
References
- Hammond, J.; Leister-Tebbe, H.; Gardner, A.; Abreu, P.; Bao, W.; Wisemandle, W.; Baniecki, M.; Hendrick, V.M.; Damle, B.; Simón-Campos, A.; et al. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with Covid-19. N. Engl. J. Med. 2022, 386, 1397–1408. [Google Scholar] [CrossRef]
- UK NERVTAG: Antiviral Drug Resistance and the Use of Directly Acting Antiviral Drugs (DAAs) for COVID-19, 8 December 2021 - GOV.UK. Available online: https://www.gov.uk/government/publications/nervtag-antiviral-drug-resistance-and-the-use-of-directly-acting-antiviral-drugs-daas-for-covid-19-8-december-2021/nervtag-antiviral-drug-resistance-and-the-use-of-directly-acting-antiviral-drugs-daas-for-covid-19-8-december-2021 (accessed on 3 May 2023).
- Dong, J.; Zost, S.J.; Greaney, A.J.; Starr, T.N.; Dingens, A.S.; Chen, E.C.; Chen, R.E.; Case, J.B.; Sutton, R.E.; Gilchuk, P.; et al. Genetic and Structural Basis for SARS-CoV-2 Variant Neutralization by a Two-Antibody Cocktail. Nat. Microbiol. 2021, 6, 1233–1244. [Google Scholar] [CrossRef]
- Loo, Y.M.; McTamney, P.M.; Arends, R.H.; Abram, M.E.; Aksyuk, A.A.; Diallo, S.; Flores, D.J.; Kelly, E.J.; Ren, K.; Roque, R.; et al. The SARS-CoV-2 Monoclonal Antibody Combination, AZD7442, Is Protective in Nonhuman Primates and Has an Extended Half-Life in Humans. Sci. Transl. Med. 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Oganesyan, V.; Damschroder, M.M.; Woods, R.M.; Cook, K.E.; Wu, H.; Dall’Acqua, W.F. Structural Characterization of a Human Fc Fragment Engineered for Extended Serum Half-Life. Mol. Immunol. 2009, 46, 1750–1755. [Google Scholar] [CrossRef]
- O’Brien, M.P.; Forleo-Neto, E.; Musser, B.J.; Isa, F.; Chan, K.-C.; Sarkar, N.; Bar, K.J.; Barnabas, R. V.; Barouch, D.H.; Cohen, M.S.; et al. Subcutaneous REGEN-COV Antibody Combination to Prevent Covid-19. N. Engl. J. Med. 2021, 385, 1184–1195. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration FACT SHEET FOR HEALTH CARE PROVIDERS EMERGENCY USE AUTHORIZATION (EUA) OF BAMLANIVIMAB AND ETESEVIMAB. Available online: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.fda.gov/media/145802/download (accessed on 3 May 2023).
- Montgomery, H.; Hobbs, F.D.R.; Padilla, F.; Arbetter, D.; Templeton, A.; Seegobin, S.; Kim, K.; Campos, J.A.S.; Arends, R.H.; Brodek, B.H.; et al. Efficacy and Safety of Intramuscular Administration of Tixagevimab–Cilgavimab for Early Outpatient Treatment of COVID-19 (TACKLE): A Phase 3, Randomised, Double-Blind, Placebo-Controlled Trial. Lancet Respir. Med. 2022, 10, 985–996. [Google Scholar] [CrossRef] [PubMed]
- Keam, S.J. Tixagevimab + Cilgavimab: First Approval. Drugs 2022, 82, 1001. [Google Scholar] [CrossRef] [PubMed]
- Europea Medicine Agency Evusheld: EPAR - Product Information. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/evusheld (accessed on 13 April 2023).
- Ginde, A.A.; Paredes, R.; Murray, T.A.; Engen, N.; Grandits, G.; Vekstein, A.; Ivey, N.; Mourad, A.; Sandkovsky, U.; Gottlieb, R.L.; et al. Tixagevimab-Cilgavimab for Treatment of Patients Hospitalised with COVID-19: A Randomised, Double-Blind, Phase 3 Trial. Lancet. Respir. Med. 2022, 10, 972–984. [Google Scholar] [CrossRef]
- Wang, Y.; Zheng, J.; Zhu, K.; Xu, C.; Wang, D.; Hou, M. The Effect of Tixagevimab-Cilgavimab on Clinical Outcomes in Patients with COVID-19: A Systematic Review with Meta-Analysis. J. Infect. 2023, 86, e15–e17. [Google Scholar] [CrossRef]
- Lafont, E.; Pere, H.; Lebeaux, D.; Cheminet, G.; Thervet, E.; Guillemain, R.; Flahault, A. Targeted SARS-CoV-2 Treatment Is Associated with Decreased Mortality in Immunocompromised Patients with COVID-19. J. Antimicrob. Chemother. 2022, 77, 2688–2692. [Google Scholar] [CrossRef] [PubMed]
- Dougan, M.; Nirula, A.; Azizad, M.; Mocherla, B.; Gottlieb, R.L.; Chen, P.; Hebert, C.; Perry, R.; Boscia, J.; Heller, B.; et al. Bamlanivimab plus Etesevimab in Mild or Moderate Covid-19. N. Engl. J. Med. 2021, 385, 1382–1392. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Coupland, C.A.C.; Mehta, N.; Keogh, R.H.; Diaz-Ordaz, K.; Khunti, K.; Lyons, R.A.; Kee, F.; Sheikh, A.; Rahman, S.; et al. Risk Prediction of Covid-19 Related Death and Hospital Admission in Adults after Covid-19 Vaccination: National Prospective Cohort Study. BMJ 2021, 374. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, U.; Katikireddi, S.V.; McCowan, C.; Mulholland, R.H.; Azcoaga-Lorenzo, A.; Amele, S.; Fagbamigbe, A.F.; Vasileiou, E.; Grange, Z.; Shi, T.; et al. COVID-19 Hospital Admissions and Deaths after BNT162b2 and ChAdOx1 NCoV-19 Vaccinations in 2·57 Million People in Scotland (EAVE II): A Prospective Cohort Study. Lancet. Respir. Med. 2021, 9, 1439–1449. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, M.; Penfold, R.S.; Merino, J.; Sudre, C.H.; Molteni, E.; Berry, S.; Canas, L.S.; Graham, M.S.; Klaser, K.; Modat, M.; et al. Risk Factors and Disease Profile of Post-Vaccination SARS-CoV-2 Infection in UK Users of the COVID Symptom Study App: A Prospective, Community-Based, Nested, Case-Control Study. Lancet. Infect. Dis. 2022, 22, 43–55. [Google Scholar] [CrossRef]
- Kemp, S.A.; Collier, D.A.; Datir, R.P.; Ferreira, I.A.T.M.; Gayed, S.; Jahun, A.; Hosmillo, M.; Rees-Spear, C.; Mlcochova, P.; Lumb, I.U.; et al. SARS-CoV-2 Evolution during Treatment of Chronic Infection. Nature 2021, 592, 277–282. [Google Scholar] [CrossRef]
- Langerbeins, P.; Hallek, M. COVID-19 in Patients with Hematologic Malignancy. Blood 2022, 140, 236–252. [Google Scholar] [CrossRef]
- Griffiths, E.A.; Segal, B.H. Immune Responses to COVID-19 Vaccines in Patients with Cancer: Promising Results and a Note of Caution. Cancer Cell 2021, 39, 1045–1047. [Google Scholar] [CrossRef]
- Greenberger, L.M.; Saltzman, L.A.; Senefeld, J.W.; Johnson, P.W.; DeGennaro, L.J.; Nichols, G.L. Antibody Response to SARS-CoV-2 Vaccines in Patients with Hematologic Malignancies. Cancer Cell 2021, 39, 1031–1033. [Google Scholar] [CrossRef]
- Nkolola, J.P.; Yu, J.; Wan, H.; Chang, A.; McMahan, K.; Anioke, T.; Jacob-Dolan, C.; Powers, O.; Ye, T.; Chandrashekar, A.; et al. A Bivalent SARS-CoV-2 Monoclonal Antibody Combination Does Not Affect the Immunogenicity of a Vector-Based COVID-19 Vaccine in Macaques. Sci. Transl. Med. 2022, 14. [Google Scholar] [CrossRef]
- Bar, D.Z.; Atkatsh, K.; Tavarez, U.; Erdos, M.R.; Gruenbaum, Y.; Collins, F.S. Biotinylation by Antibody Recognition—a Method for Proximity Labeling. Nat. Methods 2017 152 2017, 15, 127–133. [Google Scholar] [CrossRef]
- Conte, W.L.; Golzarri-Arroyo, L. Tixagevimab and Cilgavimab (Evusheld) Boosts Antibody Levels to SARS-CoV-2 in Patients with Multiple Sclerosis on b-Cell Depleters. Mult. Scler. Relat. Disord. 2022, 63. [Google Scholar] [CrossRef]
- Soeroto, A.Y.; Yanto, T.A.; Kurniawan, A.; Hariyanto, T.I. Efficacy and Safety of Tixagevimab-Cilgavimab as Pre-Exposure Prophylaxis for COVID-19: A Systematic Review and Meta-Analysis. Rev. Med. Virol. 2023, 33. [Google Scholar] [CrossRef] [PubMed]
- Suribhatla, R.; Starkey, T.; Ionescu, M.C.; Pagliuca, A.; Richter, A.; Lee, L.Y.W. Systematic Review and Meta-Analysis of the Clinical Effectiveness of Tixagevimab/Cilgavimab for Prophylaxis of COVID-19 in Immunocompromised Patients. Br. J. Haematol. 2023, 00, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.J.; Ustianowski, A.; Thomas, S.; Templeton, A.; Yuan, Y.; Seegobin, S.; Houlihan, C.F.; Menendez-Perez, I.; Pollett, S.; Arends, R.H.; et al. AZD7442 (Tixagevimab/Cilgavimab) for Post-Exposure Prophylaxis of Symptomatic Coronavirus Disease 2019. Clin. Infect. Dis. 2023, 76. [Google Scholar] [CrossRef]
- Iketani, S.; Liu, L.; Guo, Y.; Liu, L.; Chan, J.F.W.; Huang, Y.; Wang, M.; Luo, Y.; Yu, J.; Chu, H.; et al. Antibody Evasion Properties of SARS-CoV-2 Omicron Sublineages. Nat. 2022 6047906 2022, 604, 553–556. [Google Scholar] [CrossRef]
- VanBlargan, L.A.; Errico, J.M.; Halfmann, P.J.; Zost, S.J.; Crowe, J.E.; Purcell, L.A.; Kawaoka, Y.; Corti, D.; Fremont, D.H.; Diamond, M.S. An Infectious SARS-CoV-2 B.1.1.529 Omicron Virus Escapes Neutralization by Therapeutic Monoclonal Antibodies. Nat. Med. 2022 283 2022, 28, 490–495. [Google Scholar] [CrossRef]
- Zhou, T.; Wang, L.; Misasi, J.; Pegu, A.; Zhang, Y.; Harris, D.R.; Olia, A.S.; Talana, C.A.; Yang, E.S.; Chen, M.; et al. Structural Basis for Potent Antibody Neutralization of SARS-CoV-2 Variants Including B.1.1.529. Science 2022, 376. [Google Scholar] [CrossRef]
- Tuekprakhon, A.; Nutalai, R.; Dijokaite-Guraliuc, A.; Zhou, D.; Ginn, H.M.; Selvaraj, M.; Liu, C.; Mentzer, A.J.; Supasa, P.; Duyvesteyn, H.M.E.; et al. Antibody Escape of SARS-CoV-2 Omicron BA.4 and BA.5 from Vaccine and BA.1 Serum. Cell 2022, 185, 2422–2433. [Google Scholar] [CrossRef]
- https://www.ecdc.europa.eu/en/news-events/epidemiological-update-covid-19-transmission-eueea-sars-cov-2-variants-and-public.
Figure 1.
PCR levels according to remdesivir treatment (10 mg, 5 mg, or no treatment).
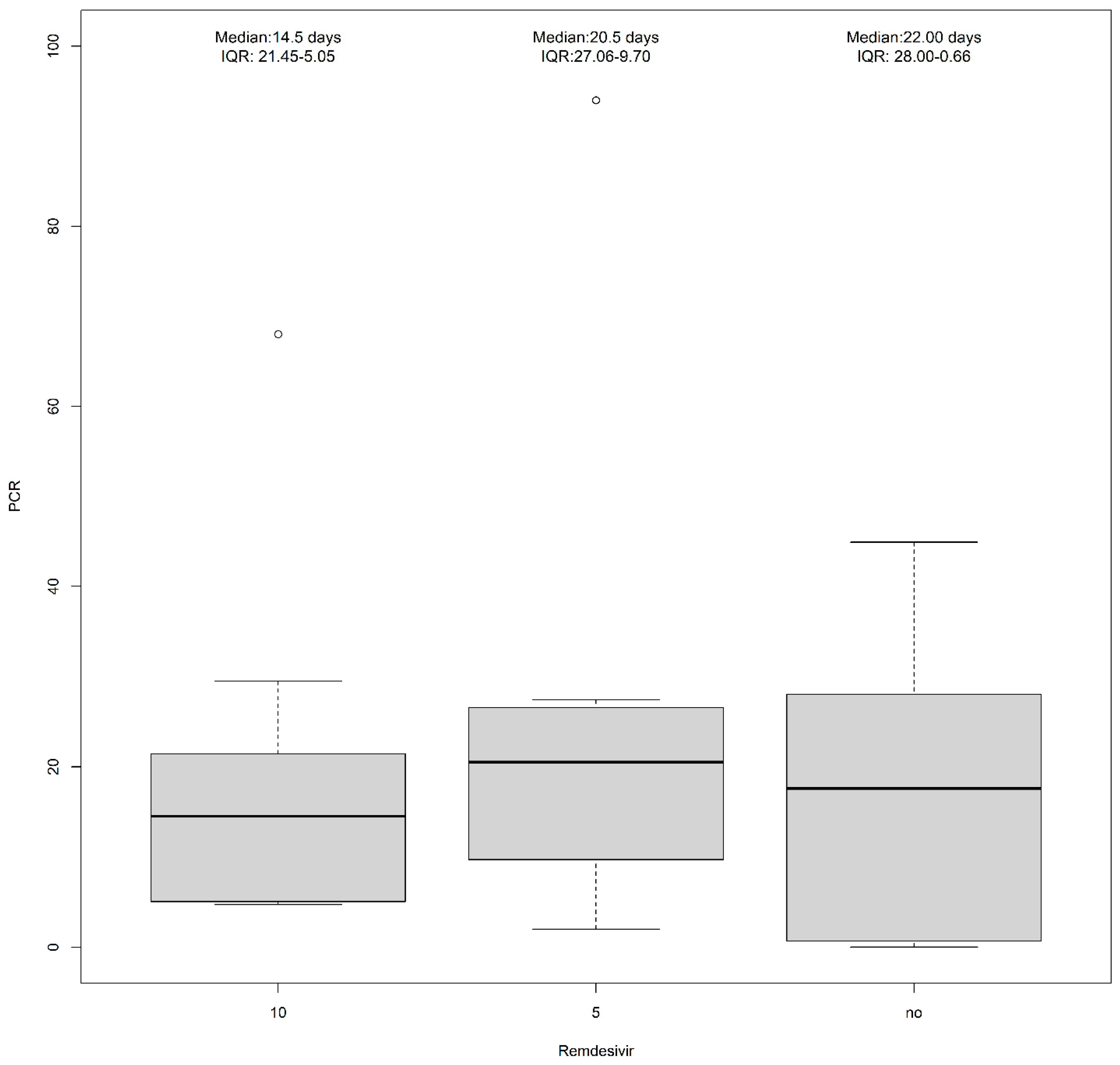

Table 1.
The demographic, laboratory and clinical characteristics of the 42 patients with COVID-19 receiving tixagevimab-cilgavimab. Group A: patients affected by chronic disorders; Group B: patients affected by oncohematological disorders.
Table 1.
The demographic, laboratory and clinical characteristics of the 42 patients with COVID-19 receiving tixagevimab-cilgavimab. Group A: patients affected by chronic disorders; Group B: patients affected by oncohematological disorders.
| A (N=27) |
B (N=15) |
Overall (N=42) |
|
|---|---|---|---|
| Age | |||
| Mean (SD) | 66.8 (18.2) | 69.9 (10.1) | 68.0 (15.6) |
| Median [Min, Max] | 71.0 [35.0, 98.0] | 73.0 [49.0, 88.0] | 71.0 [35.0, 98.0] |
| Missing | 2 (7.4%) | 0 (0%) | 2 (4.8%) |
| Gender | |||
| F | 15 (55.6%) | 6 (40.0%) | 21 (50.0%) |
| M | 12 (44.4%) | 9 (60.0%) | 21 (50.0%) |
| CRP | |||
| Mean (SD) | 16.3 (12.6) | 25.3 (30.9) | 19.3 (20.5) |
| Median [Min, Max] | 16.1 [0.0200, 44.9] | 13.2 [4.70, 94.0] | 14.8 [0.0200, 94.0] |
| Missing | 7 (25.9%) | 5 (33.3%) | 12 (28.6%) |
| IL6 | |||
| Mean (SD) | 176 (509) | 36.6 (28.6) | 116 (387) |
| Median [Min, Max] | 19.0 [3.20, 2030] | 27.7 [3.10, 96.3] | 22.9 [3.10, 2030] |
| Missing | 11 (40.7%) | 3 (20.0%) | 14 (33.3%) |
| D-Dimer | |||
| Mean (SD) | 1880 (1910) | 521 (477) | 1400 (1680) |
| Median [Min, Max] | 1030 [220, 6890] | 290 [103, 1470] | 776 [103, 6890] |
| Missing | 5 (18.5%) | 3 (20.0%) | 8 (19.0%) |
| Fibrinogen | |||
| Mean (SD) | 539 (254) | 493 (107) | 527 (221) |
| Median [Min, Max] | 554 [179, 1140] | 451 [387, 666] | 519 [179, 1140] |
| Missing | 14 (51.9%) | 10 (66.7%) | 24 (57.1%) |
| Procalcitonin | |||
| Mean (SD) | 2.57 (5.82) | 0.788 (2.54) | 1.92 (4.91) |
| Median [Min, Max] | 0.940 [0.0200, 26.6] | 0.0500 [0.0200, 8.86] | 0.140 [0.0200, 26.6] |
| Missing | 6 (22.2%) | 3 (20.0%) | 9 (21.4%) |
| IgA | |||
| Mean (SD) | 247 (124) | 124 (135) | 196 (140) |
| Median [Min, Max] | 235 [35.0, 519] | 78.5 [11.0, 495] | 156 [11.0, 519] |
| Missing | 10 (37.0%) | 3 (20.0%) | 13 (31.0%) |
| IgM | |||
| Mean (SD) | 125 (133) | 29.4 (11.5) | 95.5 (119) |
| Median [Min, Max] | 73.0 [29.0, 580] | 25.5 [21.0, 53.0] | 62.5 [21.0, 580] |
| Missing | 9 (33.3%) | 7 (46.7%) | 16 (38.1%) |
| IgG | |||
| Mean (SD) | 953 (413) | 631 (315) | 822 (404) |
| Median [Min, Max] | 991 [245, 1780] | 662 [149, 1290] | 771 [149, 1780] |
| Missing | 8 (29.6%) | 2 (13.3%) | 10 (23.8%) |
| Antiviral therapy | |||
| Remdesivir (10 mg) | 4 (14.8%) | 9 (60.0%) | 13 (31.0%) |
| Remdesivir (5 mg) | 7 (25.9%) | 3 (20.0%) | 10 (23.8%) |
| No treatment | 11 (40.7%) | 1 (6.7%) | 12 (28.6%) |
| Molnupiravir | 1 (3.7%) | 0 (0%) | 1 (2.4%) |
| Missing | 4 (14.8%) | 2 (13.3%) | 6 (14.3%) |
| COVID-19 vaccine | |||
| Not vaccinated | 12 (44.4%) | 4 (26.7%) | 16 (38.1%) |
| 2 dose | 5 (18.5%) | 1 (3.7%) | 6 (14.3%) |
| 3 dose | 8 (29.6%) | 10 (66.7%) | 18 (42.8%) |
| 4 dose | 2 (7.4%) | - | 2 (4.8%) |
C-reactive protein (CRP); Interleukin-6 (IL6); Standard deviation (SD).
Table 2.
Pathologies of COVID-19 patients treated with tixagevimab-cilgavimab.
| Diseases | Group A | Group B |
|---|---|---|
| Cardiovascular disorders (n=8) | ||
| Hypertensive cardiopathy | 3 | - |
| Atrial fibrillation | 2 | - |
| Arterial hypertension | 1 | - |
| Ischemic cardiopathy | 1 | - |
| Stroke | 1 | - |
| Degenerative diseases (n=7) | ||
| Wagner syndrome | 1 | - |
| Alzheimer’s disease | 4 | - |
| Multiple sclerosis | 1 | - |
| Creutzfeldt-Jakob disease | 1 | - |
| Solid tumors (n=5) | ||
| Lung carcinoma | 4 | - |
| Breast carcinoma | 1 | - |
| Infections (n=4) | ||
| Cirrhosis HBV related | 1 | - |
| Cryptococcal meningitis | 1 | - |
| HIV | 2 | - |
| Autoimmune disorders (n=3) | ||
| Autoimmune gastritis | 1 | - |
| Rheumatoid arthritis | 1 | - |
| Magic Syndrome | 1 | - |
| Other (n=5) | ||
| Iatrogenic marrow aplasia | 1 | - |
| Chronic kidney disease | 4 | - |
| Oncohematological diseases (n=15) | ||
| Chronic lymphocytic leukemia | - | 4 |
| Non-Hodgkin lynfoma | - | 11 |
Table 3.
HR chest CT scan of 42 patients with SARS-CoV-2 infection before treatment with tixagevimab-cilgavimab.
Table 3.
HR chest CT scan of 42 patients with SARS-CoV-2 infection before treatment with tixagevimab-cilgavimab.
|
Group A Patient 2: GGO + consolidation Patient 3: 7/20 + acinetobacter multi-drug resistant Patient 4: 15/20 Patient 7: 5/20 Patient 14: GGO Patient 15: GGO + effusion Patient 16: 9/20 Patient 18: GGO + thickening Patient 19: GGO + effusion Patient 20: Not available Patient 21: GGO + thickening Patient 23: no pneumonia Patient 24: GGO Patient 27: GGO + thickening Patient 28: GGO Patient 29: 13/20 Patient 30: Not available Patient 31: 7/20 Patient 32: GGO + thickening Patient 33: GGO Patient 34: no pneumonia Patient 35: Not available Patients 36: Not available Patient 37: GGO + thickening + effusion Patient 38: Not available Patient 39: GGO + thickening + effusion Patient 40: GGO + thickening |
|
Group B Patient 1: GGO + Legionella infection Patient 5: 13/20 Patient 6: areoles Patient 8: Not available Patient 9: GGO Patient 10: 18/25 Patient 11: 12/20 Patient 12: GGO Patient 13: GGO + consolidation + effusion Patient 17: GGO + thickening Patient 22: cerebral edema, no pneumonia Patient 25: GGO Patient 26: GGO + consolidation Patient 41: 4/20 + thickening Patient 42: bilateral GGO |
Ground-glass opacity (GGO).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



