
Submitted:
12 September 2023
Posted:
14 September 2023
You are already at the latest version
Abstract
Fibromyalgia syndrome (FMS) is a nonarticular rheumatic syndrome which presents as chronic musculoskeletal pain, stiffness and body aches. FMS affects approximately 2.5% of the population, mostly women. FMS causes physical and psychological problems and reduces quality of life. The objective of this study is to identify qualitative evidence about experiences of women diagnosed with FMS about their sexuality. Methods: Metasynthesis of qualitative studies. The search included articles published between 2000 and June 2023 on the PubMed, WOS, CINAHL, SCOPUS, and SCIELO databases. Results: 450 articles were found through the initial search, of which, only 9 fulfilled the criteria and were included in the thematic synthesis. From this analysis, three main themes emerged: (1) “I want to, but I can’t”: FMS causes a shift in feminine sexuality. (2) Resetting sex life and intimacy. (3) Taking charge of a “new sexuality.” Conclusions: Women with FMS suffer from limitations of their sexuality that affect their partner. Pain, stiffness and a loss of desire make sexual encounters difficult. Becoming aware of this and striving not to lose their sexuality is key to coping with this problem. Women and their sexual partners can change roles and encourage communication, games, foreplay or touching. The use of lubricants, physical exercise and complementary therapies, along with social, professional and partner support, are key to coping with FMS.
Keywords:
fibromyalgia syndrome
; sexuality
; female sexual dysfunction
; qualitative research
1. Introduction
Fibromyalgia syndrome (FMS) is characterised by chronic widespread pain, fatigue, and sleep disturbances [1]. FMS is a nonarticular rheumatic syndrome that presents with chronic musculoskeletal pain and multiple points of bodily pain when pressure is applied. Prevalence of FMS in the Euro zone is estimated to be around 2.64% [2], being about 1.5% in France, 2.6% in Germany and 2.4% in Spain [3]. Differences in estimates may be due to the study population, designs, measurements and diagnostic criteria applied [4]. Prevalence rates of FMS are higher in women than in men, ranging from 3.5–5.5%, and increase with age [5,6]. FMS alters the physical and emotional health of women [7], and also affects their sexual health as it is associated with fatigue, pain and libido disorders, generating sexual dysfunction [8,9].
SFM is a chronic disease of unknown physiopathological mechanisms, with a predominantly clinical diagnosis. Prevalent symptoms include generalised musculoskeletal pain, hyperalgesia, paresthesia and joint stiffness [10], sleep disorders [11], stress and fatigue [12]. Given the difficulty in establishing a clear diagnosis, the American College of Rheumatology (ACR) established a series of diagnostic criteria such as the presence of musculoskeletal pain lasting more than 3 months, a minimum of 11 tender points to the touch (out of a total of 18), as well as the addition of a symptom intensity index measuring pain, drowsiness and fatigue [13,14]. SFM also affects the mental and emotional well-being of women by decreasing their quality of life [15,16].
FMS has been associated with major depression, mood, bipolar and panic disorders, along with coping difficulties and social stigma [17]. FMS directly affects female sexuality [11], and is associated with fatigue [18], pain [15], lubrication and pelvic floor muscle problems [10], hypoactive sexual desire and self-image disorders [19]. This situation can cause women to have decreased libido, lack of receptivity and sexual avoidance behaviours [20]; with decreased/absence of sexual intercourse and increased risk of relationship breakdown [21]. This situation is compounded by the negative side effects of pharmacological treatment [20], which greatly enhance the problems described above.
While FMS research has focused primarily on physical, psychological problems, treatment, and therapy [22,23], little is known regarding women’s own experiences of their sexuality [9,24]. Qualitative methodologies have proven useful in comprehensive FMS research, but the scientific literature on the effects of FMS on female sexuality needs to be explored. Understanding experiences of women diagnosed with FMS about their sexuality could be important for removing barriers, bringing about improvements, and developing specific protocols for care. Although several studies focus on the experiences of women with FMS [9,24,25], including review studies [26,27,28], a synthesis of aggregate data is needed to gain a deeper understanding of the phenomenon in order to guide clinical practice, raise new hypotheses, and improve quality care for these women. The research question guiding this review is: What are the experiences of women diagnosed with FMS, in terms of their sexuality? The objective of this study is to identify qualitative evidence about the experiences of women diagnosed with FSM regarding their sexuality.
2. Materials and Methods
2.1. Design
A systematic review of qualitative studies was performed. Metasynthesis involves the inductive analysis, assembly and categorisation of findings on the basis of similarity of meaning, generating a set of statements that bring together and reflect on knowledge about an area of study. This review follows the ENTREQ (Enhancing Transparency in Reporting the Synthesis of Qualitative Research) guidelines [29].
2.2. Search methods
Bibliographic searches were conducted on the PubMed, WOS, CINAHL, SCOPUS, and SCIELO databases for qualitative studies in English and Spanish, published between 2000 and June 2023. The SPIDER method was used for qualitative research (Sample, Phenomenon of Interest, Design, Evaluation, Research type) [30]. In order to perform the search, the search terms used were divided into three areas. Firstly, the terms “sexual”, “sexuality”, were joined with the Boolean operator “OR”, this search was performed with “women”, “girl”, “women’s health”, as well as “fibromyalgia”, “fibromyalgia syndrome”, “muscular rheumatism”, “chronic fatigue disorders”, “chronic fatigue syndrome”, and “qualitative research”, “qualitative design” and “metasynthesis”. After performing these searches separately, they were joined using the Boolean operator “AND”(((((((sexuality) OR sexual)) AND (((((women) OR Girl) OR Women’s Health)) AND ((((((Fibromyalgia) OR fibromyalgia syndrome) OR muscular rheumatism) OR chronic fatigue disorders) OR chronic fatigue syndrome)) AND ((qualitative research) OR qualitative design) OR Metasynthesis). This search was supplemented by a manual search of grey literature.
2.3. Inclusion and exclusion criteria
Inclusion criteria: women over 18 years of age diagnosed with FMS at least 1 year prior. Qualitative research articles (descriptive, phenomenological, ethnographic, grounded theory, etc.), or mixed methodology were included. Published full-length original research, English or Spanish language, between 2000 -2023. Exclusion criteria: non-primary articles, editorials, abstracts or opinion pieces.
2.4. Search results
A 5-stage selection process was performed: elimination of duplicates, title selection, abstract review, full paper review and reference tracking. A total of 131 studies were identified, however, only 9 articles met the inclusion criteria and were included in this review (Figure 1).
2.5. Quality assessment
Each primary study was assessed using the Joanna Briggs Institute’s Qualitative Assessment Rating Instrument (QARI) [31]. The included articles were considered to be of high quality with respect to objectives, design, analysis and results, providing useful knowledge on the topic (Table 1). No studies were excluded after quality assessment, however, 3 studies had significant methodological limitations.
2.6. Data extraction
Researchers removed all duplicate records, analysed selected studies by extracting data on author(s), year, country, design, philosophical perspective, sample, data collection, data analysis, age and research focus. The references of nine included papers were reviewed.
2.7. Data synthesis and analysis
The included studies were analysed thematically. The synthesis was undertaken by (PRA an MMJL), and verified by (JGM). Two independent reviewers with expertise in FMS and qualitative research verified the results. The thematic synthesis of qualitative data (Table 2) included line-by-line coding, developing descriptive themes and generating themes and sub-themes in three stages [32]:
2.8. Rigor
To check the validity of the review, we maintained structured summaries of all original studies, and also checked whether the findings were transferable to other research contexts. Following the thematic synthesis, we examined the studies’ contributions to the final analytical themes and intervention recommendations.

Table 3.
Characteristics of selected studies.
| Author Año | País | Muestra (FMSW) | Edad (años) | Tiempo entrevista | Data collection | Data analisys | Main Theme |
|---|---|---|---|---|---|---|---|
| Centurión N.B., et al., 2020 [33] | Brasil | 6 | 40–60 | 1 h 30 min | GDs | Content analysis | Religion and morals affect women with FMS |
| Sanabria, JP et al. (2019, a) [34] | Colombia | 15 | 23–60 | No | IDI | Organisation, segmentation and correlation | Carer roles and gender influence couple dynamics |
| Sanabria, JP et al. (2019,b) [35] | Colombia | 15 | 23–60 | No | IDI | Organisation, segmentation and correlation | Feminine viewpoint of FMS influences their erotic expression |
| Santos-Iglesias, P., et al. (2022) [36] | Canada | 16 | 21 o > | 60–90 min | SSI | Inductive Thematic Analysis | Multi-dimensional nature of sexual wellbeing in women with FMS |
| Matarin Jiménez el al., (2017) [24] | España | 13 | 22–56 | 40 min | FG, IDI | Gadamer’s phenomenological analysis | FMS affects identity and relationship with partners |
| Arnold, L.M., et al. (2008) [37] | USA | 48 | >18 | 2 h. | FG | Strauss and Corbin’s techniques | FMS has a negative impact on quality of life |
| Briones-Vozmediano et al. (2016) [38] | España | 13 | 24–61 | 60–90 min | SSI | Thematic analysis | Healthcare providers can help to improve lifestyle in women with FMS. |
| García Campayo, J. et al., 2004 [39] | España | 27 | No | 60–90 min | SSI, FG | Thematic analysis | FMS limits feminine sexuality, but is not discussed with doctors |
| Granero-Molina et al., 2018 [9] | España | 13 | 22–56 | 40 min | FG, IDI | Gadamer’s phenomenological analysis | Lack of formal support regarding fibromyalgia patient’s sexuality |
FMSWs = Fibromyalgia Syndrome Womens. IDI = in deep interview. FGs = Focus Group. GDs = Discussion Group. SSI = Semi Structures Interview.
3. Results
The nine qualitative studies comprised a total sample of 132 women diagnosed with FMS from Brazil, Colombia, Canada, Spain and the USA, aged between 18 and 61 (Table 3). Most of the studies were conducted in Spain (4). Two studies conducted in Colombia [34,35] and two studies conducted in Spain have the same data collection [9,24], although they focus on different aspects of sexuality. Thematic synthesis is an inductive process in which 3 themes and 18 sub-themes emerge (Table 4).
3.1. “I want to, but I can’t”: a shift in feminine sexuality
A common denominator in the experiences of the patients in our synthesis is the presence of debilitating pain that affects their sex life. Although the testimonies differ, this pain is accompanied by stiffness, decreased desire, irritability, altered emotional state, poor mood and decreased quality of life. Although women try to cope, there is a decrease in the frequency and quality of sexual encounters, fluctuating pleasure and fewer orgasms. Taking drug treatments can accentuate the problem, and women with FMS may avoid sexual encounters and have sex to please their partner.
3.1.1. Pain/stiffness limit pleasure and desire
Women with FMS typically experience pain and stiffness. Pain is accompanied by generalised bodily stiffness at variable periods of time, exacerbated by flare-ups. These symptoms, along with a lack of female vaginal lubrication, directly affect penetration, making it difficult and uncomfortable for the partner during intercourse.
The pain is concentrated in the vaginal area, the moment of penetration is really painful for both partners. We didn’t have these problems before, it was all because I was diagnosed with FMS. [34]
The pain is often accompanied by generalised stiffness. Women with FMS note a semi-numb, tense feeling, with a paresthetic sensation throughout their bodies. There is muscle stiffness in the legs that interferes with activities of daily life such as walking, but also negatively affects sexual desire. Women report that the pain blocks their emotions, they lose the desire to have sex and it makes orgasm difficult. After initiating intercourse they try to endure the pain, but end up exhausted and have to stop.
Sometimes you have to say, ‘Stop, stop, … you’re hurting me, I can’t do it’. Or he holds you and … ‘Ow, you’re hurting me! [24]
In this situation, changes in position do not always improve the pain; on the contrary, they can increase the discomfort during intercourse.
Changing positions during our encounters hurts a lot; I didn’t have this problem before, now it hurts anytime we do anything out of the ordinary… [35]
3.1.2. Irritability and low mood
The intensity of the pain causes irritability, discomfort and moodiness. Women suffer from headaches and general body discomfort that affects their sexual function. During flare-ups, women with FMS do not want to be touched by anyone, including their partner. They report that it hurts “down to their toes”, and sex is the last thing on their minds.
When I am in such intense pain, I get a bad temper and tell him to leave me alone, that I do not want to be with anyone, nor with myself. By the pain I get bad and insult him without him deserving it. [35]
The generalised stiffness prevents them from relaxing and enjoying sex, and they have severe difficulties in reaching orgasm. Women report that this feeling is difficult to explain, especially to their partners, as reported in a focus group:
I had a lot of discomfort doing it (coitus), some pain here (vulva) and I didn’t have one (an orgasm). I was very nervous, I couldn’t relax, I wasn’t enjoying it. How can you always explain that? It’s like … it’s a bit ridiculous. [24]
It is therefore a “hidden” pain, which affects their state of mind. They do not want to talk about it, they do not know how to explain what is happening to them, they do not want to be asked about it, so they generally keep quiet and say nothing.
Get up every day and hear that it is hurting me here or there, I know it must be exhausting. It is enough that I must deal with this daily to make another person deal with the same thing … I know it’s difficult and that’s why I always try to show a good face and avoid him knowing that it hurts me. [35]
3.1.3. Decreased frequency/difficulty reaching orgasm
Pleasure and desire are fluctuating; some women maintain their desire for sex, but most do not. They feel that they cannot enjoy it, they find it difficult to reach orgasm and want to finish as soon as possible. This increases their irritability, as their mind is not focused on sex.
My mood is directly related to the amount of pain I’m in. My irritability is directly related to the amount of pain I’m in… so, if I’m in a bad mood, feeling irritable and in pain, I’m not going to want to have sex. [36]
The frequency of sexual intercourse drops from daily to weekly, from weekly to monthly. This is very difficult for the partner to cope with, especially in young male partners.
Before I had the disease, when I was 35 years old, we were able to have sex once or twice a week. Since I was diagnosed with fibromyalgia about five years ago, the frequency has dropped to about once every two months. [39]
3.1.4. Pharmacological treatment does not help sexuality
Psychiatric comorbidity does not help to improve the sex life of women with FMS. Many are diagnosed with psychological disorders such as anxiety, depression, etc. They feel misunderstood and stigmatised by professionals. Taking antidepressants, analgesics or opiate derivatives worsens their predisposition towards sexual intercourse.
Took it, but the muscular weakness was so bad in my legs that I couldn’t get up … I told them that I wouldn’t take Tramadol® anymore or any other drug. They told me, “Well then, next time you can go to mental health. [9]
3.1.5. Having sex “for your partner”: avoiding encounters
Women with FMS avoid circumstances that could potentially lead to a sexual encounter with their partner. Sometimes they do not want it, sometimes they get angry at the lack of understanding. Excuses vary from drowsiness to headache, and women prepare their partners not to expect something (sex) that is never going to come
It’s not that I say I don’t want to, I just do everything in my power to make sure the situation doesn’t arise (...) from the afternoon on, I start telling my husband that I feel really badly and that way I can ensure that nothing sexual is going to happen between us that night. [34]
Other times they feel guilty about denying their partner something they feel they deserve and cannot give them due to their situation.
When my husband initiates sex with me (I never do), the first thing that comes to my mind is that I will have pain in my legs and hips for more than a week because of the movements and postures. This takes away all my urges, even though I might have some desire to make love. If I see that my husband is very eager, then I’ll give him that reward because the poor guy is very good to me and he deserves it. [39]
Over time, women show more direct refusal to have sex. “So one day I made the decision to tell him that I just didn’t want to have sex because I didn’t feel good and I didn’t know if that was going to change” [34]. Other times they succumb to their guilt and permit sexual intercourse to satisfy their partner’s needs, they strive to satisfy them and not lose them. This is how one woman puts it:
I do it for my husband. Yes, it’s for him, because I don’t feel like having sex at all. [36]
3.2. Resetting sex life and intimacy
Acceptance of the new situation is key to the sexuality of women with FMS. Changes in body self-image, desire, partner role or social behaviour must be addressed. Women tend to feel misunderstanding, stigma and vulnerability towards their condition. Their partner is key in the process of acceptance and change. Fear of abandonment fuels most behaviours.
3.2.1. I know it’s not mutual
FMS leads to loss of libido, therefore the partner feels that the woman is never interested in sex, has changed, or is not like she used to be. Women feel that they cannot meet their partner’s sexual demands, or are not fulfilling as wives, which generates frustration, anguish and silence.
I feel terrible for not being able to be more affectionate … but I know that this is because of the pain, because of the anguish I feel all the time. [35]
Women with FMS feel guilty, and have sex because they see the lack of affection their partner receives as unfair and want to reciprocate. Faced with frustration, they sometimes even consider going their separate ways, knowing that they no longer meet their partners’ expectations.
He (my partner) knows that I don’t do it because I feel like it, but to satisfy him, obviously. There are times when he finishes (orgasm) and you, ... mmm, … you don’t, and he also feels guilty and frustrated. [24]
3.2.2. Bearing the moral burden
Although it depends on cultural, educational or aspects of a certain country, patriarchal behaviours in the relationship undergo changes. When faced with the vulnerability and fragility of women with FMS, husbands tend to take on the role of carer.
He [my husband] takes care of me, I am the wife, so it is right for the man to take care of the woman [...] the woman takes care of the man with the housework, washing, ironing, tidying, giving [sexual] pleasure. [33]
From a religious perspective, as a partner, women equate a man’s love with sex, as if their bodies belonged to each other. They consider masculine sexual satisfaction as an obligation to be tended to as wives.
Poor him [of the husband] [...] We [the wife] have to understand that he has [sexual] needs. [33]
Social isolation is also an issue, as women observe a loss of close friends, work colleagues and the social support they once had, reducing their quality of life.
If you’re lucky enough to have someone who’ll stand by you and understands what you’re going through, or has an inkling at least, OK, but if not … each go their separate ways, that’s how it is. [38]
3.2.3. Managing misunderstandings/support
Women allude to their partner’s lack of understanding of FMS, not understanding what they are going through, not empathising with them and not being able to put themselves in their position. The partners see the situation as unreal: their wives seem older, they suddenly do not feel like having fun or being social, and get cross easily. As one woman states: You lose your sex drive, and then everybody pulls a long face [38]. The feeling of having support from their partner varies; at first the partner may feel uncomfortable, but little by little, they start accepting their fate, and mould their social lives and sexual intimacy to the woman’s current situation.
I feel like he understands me, that he makes a big effort to understand my pain. At the same time, I try to forget my pain, and put in an effort on my part so we don’t have to stop doing the things he loves. [34]
Over time the relationship strengthens, as partners understand each other better, they know what each person expects and when it is best for sexual relations to happen. “Over time we have learned to support each other mutually; all the things we’ve gone through have made us stronger.” [34] Some women even do not understand when they receive excessive support from their partners.
Since I have fibromyalgia, he has become too sensitive; if I cry, he cries with me. That makes me feel accompanied, that I think he understands my pain. Sometimes he gets so bad for my pains, that it’s my turn to console him and tell him that everything will turn out well. [35]
Along with a lack of understanding from their partners, women with FMS also note a lack of understanding from professionals. Participants express frustration upon not being understood by medical professionals [37]. Doctors and nurses usually do not know the implications of FMS on patients’ sex lives, or they minimise their concerns and attribute it to the state of their mental health. The sexual implications of FMS are not considered during examinations, as one woman states, “It’s as if you have to just figure it out on your own” [9], and these topics are never addressed:
I left the consultation feeling really down … you feel like they’re not listening to you. He told me that he was going to send me to a psychiatrist. There was no sensitivity … so I wasn’t exactly going to talk or ask about sex. [9]
3.2.4. Vulnerability … of my relationship
Women’s self-image changes with FMS, as they do not feel beautiful, attractive or desired although their partner tells them so. Treatment with steroids makes them gain weight. They feel bigger, and it is a dark time. They do not want to be seen, and want to stay hidden.
I don’t feel pretty, ... I want to hide in the dark. [36]
They feel extremely vulnerable, and worry about the repercussions of their situation on their relationship, which also becomes vulnerable.
Getting up every day and hearing that it’s hurting here or there, I know it must be draining. It’s already bad enough that I have to deal with it on a daily basis, without having to make someone else deal with it every day too. [34]
3.2.5. Faking it for fear of abandonment
Women with FMS feel frustration and vulnerability within themselves and in their relationship. Aware of the danger of being abandoned, they start to feign interest in their sex life: “He asked me if that was ok, if I was having fun, and I told him I was, even though I was actually faking it”[35]. Profound changes in a couple’s romantic life may give rise to resentment, and partners may become distant or colder, as they expect understanding rather than pity.
I wonder to myself if he would ever leave me one day, because it could happen, he might get tired of dealing with it and someone else comes along who wants to go out and have fun, who can do the things he wants to do, who has things in common with him. [34]
3.3. Taking charge of a “new sexuality”
FMS alters women and their partner’s sex lives, and facing these challenges lies in accepting the changes and adapting to a “new sexuality” by developing several different strategies.
3.3.1. Striving for my (our) sex life
Women strive to give priority to their sexuality as a first step in order to not lose it. They understand that sex is not everything, but it is part of the glue that holds the couple together. Even if they cannot perform as they wish, they make an effort.
For me, yes, obviously, it’s like before, just as important. I throw myself into it, because. I have to do things, I have to have a life, sex too. [24]
It is important to feel attractive to their partner, or for other men, feel good about their appearance and feel wanted. Wearing more beautiful clothes and wearing makeup helps them feel more desirable:
… If I can feel pretty, maybe I can feel better about myself … it will help me feel more desirable, which in turn will hopefully bring the sex back into our lives. [36]
3.3.2. Forgetting the past: taking the initiative
Women must learn how to cope with guilt, and forget the past. Increasing communication with their partner may help to recognize where there are problems and solve them.
I love you, and yes, you have fibromyalgia, but we’ll get through this together, you have to stop feeling guilty for not being able to do it [sex]. I’m fine... [36]
Women must take the initiative in their sex life and relationship. It is they who know when they are in pain or not, and when they are able to have sex: “He’ll wait until I tell him I’m ok and then we’re ready to go.” [36]. Couples must avoid comparisons with the past, look for new information and seek professional help
It would be good if they explained it to the partners, that when you have a strong chronic pain, you are physically not up to having a sexual relationship, and that if you need to rest while having sex, that’s quite normal, because physically, your bodyneeds to rest.” [9]
3.3.3. Changing habits: finding the right moment
The partner must be willing to change their sexual habits, for example, if they are accustomed to having sexual encounters at night and now their wife needs to go to bed because of fatigue, they will have to find another time. As one patient recounts:
I have to do it when I’m not tired—it’s not so much the frequency, but of finding other ways of doing it, whereby it’s not painful, not because of having sex, but of the correct position. [38]
Communication is paramount, as the partner must comprehend that it is not always the right time to have a sexual encounter. Women with FMS must show signs that “today is not the day,” and their partner must withdraw their advances and not pressure the woman, in order to avoid negative feelings.
We understood that we could not always have relationships, that we could when the pain wasbearable. [35]
Other women insist it is important to initiate, not ignore attempts by their partner to initiate, regardless of if it is cut short or ends in orgasm.
You don’t feel like it until you actually start … then you get into it and you feel like it more. [24]
3.3.4. Getting to know each other: prioritising play and touch
Women with FMS recognise the importance of making certain preparations for sex. Putting cushions on the bed, regulating foreplay or not overextending oneself due to the risk of fatigue can help. This is explained by one woman regarding penetration.
There is not much movement after penetration either, my husband knows it has to be gentle and quick. [39]
Women have moved from coitus-centred, genital sexuality to exploring, playing, caressing and getting to know each other. There are clear improvements in partner satisfaction and in the relationship. The woman feels more comfortable and enjoys her sex life more.
Sexuality for me before was from the genital, that is, from intercourse; we did not worry about what we felt … Now we explore ourselves, we talk, we laugh, we try things” [35]
3.3.5. Changing positions and using lubricants
Women with FMS do not refuse to change positions, but when it hurts or they get cramps, they are unable, so they choose to explore non-painful positions that give them pleasure. There are positions they cannot assume or must change quickly.
Sometimes, if I’m having a bad day, I may have to say, “Hey, my knee hurts, let’s not have sex in that position, let’s do it this way.” [36]
3.3.6. Exercise and therapy
After being diagnosed with FMS, women usually turn to exercise and therapy as mujeres suelen recurrir al ejercicio y la terapia como adjuvants to medical treatment. Psychotherapy can help with diagnosis and have a positive impact on pain. Regular physical exercise also seems to have a positive impact on pain and fatigue. One woman adds:
With physical exercise, yes, because you’re more active, you feel better (laughs). It helps you to get into the mood more. [24]
3.3.7. Social and professional support
Sexual problems associated with FMS are not on health professionals’ agendas. Little is discussed with doctors, nurses or physiotherapists, who also do not ask questions. This places an additional burden on patients, who are forced to raise the issue in the consultation room for treatment or referral to other specialists.
Sexual problems in fibromyalgia are never discussed with doctors. They never bring it up, it seems that it doesn’t exist or that we don’t have sexuality. We don’t bring up the problem either. [39]
Participants in the various studies emphasise the importance of patients’ organisations or groups as a primary means of support. There, women share problems with others in the same situation, and find a listening ear and understanding.
Since I’ve been coming to the association, I’ve come to understand FM. Now, being here with other people and seeing they have the same symptoms as you and everything … it’s like you understand the illness better. [9]
4. Discussion
According to our results, chronic pain limits satisfactory sexual relations and significantly influences the lives of women with FMS [35]. Women have a lower pain threshold and greater sensitivity to pressure and temperature [40]. Several studies agree that pain inhibits sexual desire and satisfaction compared to healthy women, and sexual dysfunction is essentially related to the severity of coital pain [41]. Some meta-analyses agree on the association between female sexual dysfunction and FMS [42]. Pain, stiffness, fatigue and lack of sleep especially contribute to the loss of sexual health in these women [43], which must be addressed by health professionals.
Pain appears to be associated with low mood and anxiety in women with FMS [44], and depression is common, related to problems with desire and arousal [19,45]. Women with FMS report that pain negatively influences the frequency of sexual intercourse and ability to have orgasms [19,20,45]. It is a pain they define as “hidden”, and they learn to live with it, because the treatment options for FMS are limited and focused on symptom relief [46]. Much controversy remains regarding diagnosis, treatment and assessment [47]. As in other chronic fatigue syndromes [48], women with FMS should be evaluated and treated for psychiatric conditions. Clinicians should consider how treatments could be tailored to individual symptoms, weighing the benefits and acceptability, when prescribing medications to patients with fibromyalgia [49]. In this regard, participants have said that assessing the impact of treatments on sexual activity is a critical issue [9].
Chronic pain and low moods push women towards sexual avoidance behaviours with their partner, and this emotional distance makes closeness and the ability to negotiate other forms of sexuality nearly impossible. If women with FMS perceive their partners as unsupportive or distant, they are less likely to communicate their needs or share intimate spaces, and sexual encounters are perceived as a gendered obligation [34,35]. Depressive symptoms and antidepressant medication are associated with decreased sexual desire in these women [50], which could be related to avoidance behaviours. In the case of religious women, some feel an obligation to satisfy the sexual needs of their male partner, responding as wives [33], which creates a situation of distress. Over time, avoidance behaviours develop into overt rejection and direct communication to the partner of the refusal of sexual relations [36].
FMS is often accompanied by other comorbidities. Women with FMS are three times more likely to report pelvic floor dysfunction, sometimes accompanied by urinary incontinence, mixed incontinence and flatulence [51]. FMS can also affect psychological and physiological processes in women with overactive bladder, [52]. Women have told us that their partners do not understand this situation, which leads to lack of communication, feelings of guilt and the progressive abandonment of their sex life. Self-image problems and comorbidities increase feelings of vulnerability of these women, leading to an increase in doctor visits [53]. Women do not feel beautiful, attractive or desirable, rather, they feel that their bodies have changed, they look fat, their skin condition is worse, and they do not feel like putting on make-up or dressing up to feel more attractive [24].
Evidence points to the need for support and an interdisciplinary approach to sexuality in women with FMS. Women and their partners must recognise the situation and adapt to a new type of sexuality, both taking the initiative [24]. Women are committed to forgetting their past sex life, as they are under different circumstances and currently have a new kind of sex life. It is necessary to find opportune moments for sexual intercourse; the woman must give signals and the partner must adapt [35,38]. For women suffering with FMS, owning the problem and forgiving themselves is important [54], and improving their self-image to feel attractive can also be beneficial [36]. Not refusing sexual activity from the outset may be an option, even if the activity eventually has to stop because every woman and every relationship is different [24]. Communication between partners and commitment to changing their habits is essential [35,38]. Emphasis on play, touch and preparation is key for women [39], along with lubricants and exploring less painful positions [36]. Physical exercise and complementary therapies can help [24], but women must be open to learning about them and work with qualified professionals. Although specific improvements have been reported, there is little evidence regarding the influence of these on sexuality [56,57,58]. Professional support and training, a good doctor-patient relationship and continuity of care are essential [39]. FMS is a challenge for professionals such as physiotherapists, but those specialised in treating pelvic floor problems could contribute to improving sexual problems [59]. Social support is fundamental, and patient, family and partner associations are key elements [9].
Limitations: The credibility of metasynthesis lies in finding, extracting and analysing qualitative data from studies using a systematic method of revision. Transferability may be limited because women with FMS have disparate cultural and religious backgrounds, limiting results to more specific areas. Varied definitions and the broad nature of human sexuality could lead to greater heterogeneity of findings. The authors may have influenced the process of data extraction and synthesis, but they are experienced qualitative researchers.
5. Conclusions
Women with FMS are aware of the limitations that their clinical condition imposes on their sexuality and that of their partner. Pain, stiffness or irritability translate into loss of desire, difficulty in having orgasms and fewer sexual encounters. The multimorbidity of FMS implies treatments with negative consequences on their sex life. Women do not have a fulfilling sex life, and some focus on satisfying their partner for fear of abandonment. Awareness and coping with the situation means making an effort not to lose their sexuality. FMS resets women’s sex lives, as they know they do not respond to their partner’s demands and feel a moral burden. Women feel vulnerable and guilty. Female FMS patients and their partner must take charge of their sexuality in their new situation. Changing roles and habits during sexual encounters is the responsibility of both the woman and her partner. Games, preparations, touching, lubricants, exercises and complementary therapies, along with social, professional and partner support, are considered key aspects in the process of adapting to a new type of sexuality.
Author Contributions
Conceptualization: J.G.M., P.R.A.; methodology, I.D.SS., M.C.C.; analysis, I.D.S., M.M.J.L.; resources, C.R.R., M.C.C.; writing—original draft preparation, P.R.A., M.M.J.L.; M.C.C. ; writing, review and editing, J.G.M., I.D.S.; project administration, J.G.M., C.R.R., P.R.R ; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
Authors thank To Health Science Research Group (CTS-451) and Health Research Centre (CEINSA/UAL), University of Almeria (Spain) for their support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Giorgi, V.; Sirotti, S.; Romano, M.E.; Marotto, D.; Ablin, J.N.; Salaffi, F.; Sarzi-Puttini, P. Fibromyalgia: one year in review 2022. Clin Exp Rheumatol. 2022, 40, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Heidari, F.; Afshari, M.; Moosazadeh, M. Prevalence of fibromyalgia in general population and patients, a systematic review and meta-analysis. Rheumatol Int. 2017, 37, 1527–1539. [Google Scholar] [CrossRef]
- Kocyigit, B. F.; Akyol, A. Fibromyalgia syndrome: epidemiology, diagnosis and treatment. Reumatologia. 2022, 60, 413–421. [Google Scholar] [CrossRef]
- Alzabibi, M.A.; Shibani, M.; Alsuliman, T.; Ismail, H.; Alasaad, S.; Torbey, A.; Altorkmani, A.; Sawaf, B.; Ayoub, R.; Khalayli, N.; Kudsi, M. Fibromyalgia: epidemiology and risk factors, a population-based case-control study in Damascus, Syria. BMC Rheumatol. 2022, 6, 62. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.P.; Santo, A.S.D.E.; Berssaneti, A.A. , et al. Prevalence of fibromyalgia: literature review update. Rev Bras Reumatol.
- 2017, 57, 356–363.
- Thiagarajah, A. S.; Guymer, E. K.; Leech, M.; Littlejohn, G. O. The relationship between fibromyalgia, stress and depression. Int J Clin Rheumatol. 2014, 9, 371–384. [Google Scholar] [CrossRef]
- Zielinski, R. E. Assessment of women’s sexual health using a holistic, patient centered approach. J Midwifery Womens Health. 2013, 58, 321–327. [Google Scholar] [CrossRef]
- Rico-Villademoros, F.; Calandre, E. P.; Rodríguez-López, C. M.; García-Carrillo, J.; Ballesteros, J.; Hidalgo-Tallón, J.; García-Leiva, J. M. Sexual functioning in women and men with fibromyalgia. J Sex Med 2012, 9, 542–549. [Google Scholar] [CrossRef]
- Granero-Molina, J.; Matarín, T.M.; Ramos, C.; Hernández-Padilla, J.M.; Castro-Sánchez, A.M.; Fernández-Sola, C. Social support for female sexual dysfunction in fibromyalgia. Clin Nurs Res. 2018, 27, 296–314. [Google Scholar] [CrossRef]
- Burri, A.; Lachance, G.; Williams, F. M. Prevalence and risk factors of sexual problems and sexual distress in a sample of women suffering from chronic widespread pain. J Sex Med 2014, 11, 2772–2784. [Google Scholar] [CrossRef]
- Amasyali, A.S.; Taştaban, E.; Amasyali, S.Y.; Turan, Y.; Kazan, E.; Sari, E.; Erol, B.; Cengiz, M.; Erol, H. Effects of l ow sleep quality on sexual function, in women with fibromyalgia. Int J Impot Res. 2016, 28, 46–9. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Lavín, M. Fibromyalgia in women: somatisation or stress-evoked, sex-dimorphic neuropathic pain? Clin Exp Rheumatol. 2021, 39, 422–425. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, MB. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed]
- Kumbhare, D.; Ahmed, S.; Watter, S. A narrative review on the difficulties associated with fibromyalgia diagnosis. Ther Adv Musculoskelet Dis. 2018, 10, 13–26. [Google Scholar] [CrossRef]
- Bazzichi, L.; Giacomelli, C.; Consensi, A.; Giorgi, V.; Batticciotto, A.; Di Franco, M.; Sarzi-Puttini, P. One year in review 2020: fibromyalgia. Clin Exp Rheumatol. 2020, 38 Suppl 123, 3–8. [Google Scholar]
- Altıntas, D.; Melikoglu, M.A. The frequency of fibromyalgia in familial Mediterranean fever and its impact on the quality of life. Int J Rheum Dis. 2022, 25, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Armentor, J.L. Living With a contested, stigmatized illness: experiences of managing relationships among women with fibromyalgia. Qual Health Res. 2017, 27, 462–473. [Google Scholar] [CrossRef]
- Blazquez, A. ; Ruiz. E.; Aliste, L.; Garcıa-Quintana, A.; Alegre J. The effect of fatigue and fibromyalgia on sexual dysfunction in women with chronic fatigue syndrome. J Sex Marital Ther 2015, 41, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, H.; Yilmaz, S.D.; Erkin, G. The effects of fibromyalgia syndrome on female sexual function: a controlled study. Sex Disabil. 2012, 30, 109–113. [Google Scholar] [CrossRef]
- Bazzichi, L.; Rossi, A.; Giacomelli, C.; Scarpellini, P.; Conversano, C.; Sernissi, F.; Dellosso, L.; Bombardieri, S. The influence of psychiatric comorbidity on sexual satisfaction in fibromyalgia patients. Clin Exp Rheumatol. 2013, 31, 81–85. [Google Scholar]
- Poh, L.W.; He, H.G.; Chan, W.C.; Lee, C.S.; Lahiri, M.; Mak, A.; Cheung, P.P. Experiences of patients with rheumatoid arthritis: a qualitative study. Clin Nurs Res. 2017, 26, 373–393. [Google Scholar] [CrossRef]
- Maffei, M.E. Fibromyalgia: recent advances in diagnosis, classification, pharmacotherapy and alternative remedies. Int J Mol Sci 2020, 23, 7877. [Google Scholar] [CrossRef]
- Winslow, B.T.; Vandal, C. , Dang L. Fibromyalgia: diagnosis and management. Am Fam Physician 2023, 107, 137–144. [Google Scholar]
- Matarín,T. Matarín,T.M.; Fernández-Sola, C.; Hernández-Padilla, J.M.; Correa, M.; Antequera, L.H.; Granero-Molina J. Perceptions about the sexuality of women with fibromyalgia syndrome: a phenomenological study. J Adv Nurs. 2017, 73, 1646-1656.
- Briones-Vozmediano, E.; Vives-Cases, C.; Ronda-Pérez, E.; Gil-González, D. Patients’ and professionals’ views on managing fibromyalgia. Pain Res Manag. 2013, 18, 19–24. [Google Scholar] [CrossRef]
- Mengshoel, A.M.; Sim, J.; Ahlsen, B.; Madden, S. Diagnostic experience of patients with fibromyalgia—A meta-ethnography. Chronic Illn. 2018, 14, 194–211. [Google Scholar] [CrossRef]
- Climent-Sanz, C.; Morera-Amenós, G.; Bellon, F.; Pastells-Peiró, R.; Blanco-Blanco, J.; Valenzuela-Pascual, F. , Gea-Sánchez, M. Poor sleep quality experience and self-management strategies in fibromyalgia: a qualitative metasynthesis. J Clin Med 2020, 10, 4000. [Google Scholar] [CrossRef]
- Kumbhare, D.; Ahmed, S.; Watter, S. A narrative review on the difficulties associated with fibromyalgia diagnosis. Ther Adv Musculoskelet Dis. 2018, 10, 13–26. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for 520 interviews and focus groups. Int J Qual Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Cooke, A.; Smith, D.; Booth, A. Beyond PICO: The SPIDER tool for qualitative evidence synthesis. Qual Health Res. 2012, 522, 1435–1443. [Google Scholar] [CrossRef]
- Joanna Briggs Institute. (2020). Checklist for qualitative research. Available online: https://jbi.global/critical-appraisal-tools 524 (accessed 28th June 2023).
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol 2008, 8, 45. [Google Scholar] [CrossRef]
- Centurión, N.; Sanches, R.; Ribeiro, E.J. Meanings about sexuality in women with fibromyalgia: resonances of religiosity and morality. Psicol. Estud. 2020, 25, e44849. [Google Scholar]
- Sanabria, J.P. , Gers, M. Repercussions of chronic pain on couple’s dynamics: perspectives of women with fibromyalgia. Revista Colombiana de Psicología 2019, 29, e2923. [Google Scholar]
- Sanabria, J.P. , Gers, M. Changes in erotic Expression in Women with Fibromyalgia. Paideia 2019, 28, 47–61. [Google Scholar]
- Santos-Iglesias, P.; Crump, L.; Hhenry, J.L. The sexual lives of women living with fibromyalgia: a qualitative study. Sex Disabil. 2022, 40, 669–685. [Google Scholar] [CrossRef]
- Arnold, L.M.; Crofford, L.J.; Mease, P.J.; Burgess, S.M.; Palmer, S.C.; Abetz, L.; Martin, S.A. Patient perspectives on the impact of fibromyalgia. Patient Educ Couns. 2008, 73, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Briones-Vozmediano, E.; Vives-Cases, C.; Goicolea, I. “I’m not the woman I was”: Women’s perceptions of the effects of fibromyalgia on private life. Health Care Women Int. 2016, 37, 836–854. [Google Scholar] [CrossRef]
- García, J.; Aida, M. Sexuality in patients with fibromyalgia: A qualitative study. Archivos de Psiquiatría 2004, 67, 157–167. [Google Scholar]
- Costa, L.P. , Ferreira, M.A. Fibromyalgia from the gender perspective: triggering, clinical presentation and coping. Texto Contexto Enferm 2023, 32, e20220299. [Google Scholar]
- Ricoy-Cano, A.J.; Cortés-Pérez, I.; Del Carmen Martín-Cano, M.; De La Fuente-Robles, Y.M. Impact of fibromyalgia syndrome on female sexual function: a systematic review with meta-analysis. J Clin Rheumatol 2022, 28, e574–e582. [Google Scholar] [CrossRef]
- Besiroglu, M.D.H.; Dursun, M.D.M. The association between fibromyalgia and female sexual dysfunction: a systematic review and meta-analysis of observational studies. Int J Impot Res. 2019, 31, 31,288–297. [Google Scholar] [CrossRef]
- Tristano, A.G. The impact of rheumatic diseases on sexual function. Rheumatol Int. 2009, 29, 29,853–60. [Google Scholar] [CrossRef]
- Kayhan, F.; Küçük, A.; Satan, Y.; İlgün, E.; Arslan, Ş.; İlik, F. Sexual dysfunction, mood, anxiety, and personality disorders in female patients with fibromyalgia. Neuropsychiatr Dis Treat 2016, 16, 349–55. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, L. Association between fibromyalgia and sexual dysfunction in women. Clin Rheumatol. 2009, 28, 365–699. [Google Scholar] [CrossRef] [PubMed]
- Alorfi, N.M. Pharmacological treatments of fibromyalgia in adults; overview of phase IV clinical trials. Front Pharmacol 2022, 23, 1017129. [Google Scholar] [CrossRef]
- Sarzi-Puttini, P.; Giorgi, V.; Atzeni, F.; Gorla, R.; Kosek, E.; Choy …. . A. Fibromyalgia position paper. . A. Fibromyalgia position paper. Clin Exp Rheumatol. 2021, 39 Suppl 130, 186–193. [Google Scholar] [CrossRef]
- Natelson, B.H.; Lin, J.S.; Lange, G.; Khan, S.; Stegner, A.; Unger, E.R. The effect of comorbid medical and psychiatric diagnoses on chronic fatigue syndrome. Ann Med. 2019, 51, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Farag, H.M.; Yunusa, I.; Goswami, H.; Sultan, I.; Doucette, J.A.; Eguale, T. Comparison of amitriptyline and us food and Drug Administration-Approved Treatments for Fibromyalgia: A Systematic Review and Network Meta-analysis. JAMA Netw Open 2022, 2, e2212939. [Google Scholar] [CrossRef]
- Van Overmeire, R.; Vesentini, L.; Vanclooster, S.; Muysewinkel, E.; Bilsen, J. Sexual desire, depressive symptoms and medication use among women with fibromyalgia in Flanders. Sex Med. 2022, 10, 100457. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, G.B.; Sato, T.O.; Miwa-Cerqueira, T.; Bifani, B.E.; Rocha, A.P.R.; Carvalho, C. Pelvic floor dysfunctions in women with fibromyalgia: A cross-sectional study. Eur J Obstet Gynecol Reprod Biol. 2023, 282, 1–6. [Google Scholar] [CrossRef]
- Salaffi, F. , Di Carlo, M.; Farah, S.; Giorgi, V.; Mosca, N.; Sarzi-Puttini, P. Overactive bladder syndrome and sexual dysfunction in women with fibromyalgia and their relationship with disease severity. Clin Exp Rheumatol. 2022, 40, 1091–1101. [Google Scholar] [PubMed]
- Dobkin, P.L.; De Civita, M.; Bernatsky, S.; Kang, H.; Baron, M. Does psychological vulnerability determine health-care utilization in fibromyalgia? Rheumatology (Oxford). 2003, 42, 1324–1331. [Google Scholar] [CrossRef]
- Offenbaecher, M.; Dezutter, J.; Kohls, N.; Sigl, C.; Vallejo, M.A.; Rivera, J.; Bauerdorf, F.; Schelling, J.; Vincent, A.; Hirsch, J.K.; Sirois, F.M.; Webb, J.R.; Toussaint, L.L. Struggling with adversities of life: the role of forgiveness in patients suffering from fibromyalgia. Clin J Pain. 2017, 33, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Vasileios, P.; Styliani, P.; Nifon, G.; Pavlos, S.; Aris, F.; Ioannis, P. Managing fibromyalgia with complementary and alternative medical exercise: a systematic review and meta-analysis of clinical trials. Rheumatol Int. 2022, 42, 1909–1923. [Google Scholar] [CrossRef] [PubMed]
- Mohabbat, A.B.; Mahapatra, S.; Jenkins, S.M.; Bauer, B.A.; Vincent, A.; Wahner-Roedler, D.L. Use of complementary and integrative therapies by fibromyalgia patients: a 14-year follow-up study. Mayo Clin Proc Innov Qual Outcomes. 2019, 16, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Varinen, A.; Vuorio, T.; Kosunen, E.; Koskela, T.H. Experiences of patients with fibromyalgia at a Finnish Health Centre: A qualitative study. Eur J Gen Pract. 2022, 28, 157–164. [Google Scholar] [CrossRef]
- Romero-Alcalá, P.; Hernández-Padilla, J. M.; Fernández-Sola, C.; Coín-Pérez-Carrasco, M. D. R.; Ramos-Rodríguez, C.; Ruiz-Fernández, M. D.; Granero-Molina, J. Sexuality in male partners of women with fibromyalgia syndrome: A qualitative study. PloS One 2019, 14(11), e0224990. [Google Scholar] [CrossRef]
- Roitenberg, N.; Shoshana, A. Physiotherapists’ accounts of fibromyalgia: role-uncertainty and professional shortcomings. Disabil Rehabil. 2021, 43, 545–552. [Google Scholar] [CrossRef]
Figure 1.
Flow chart.
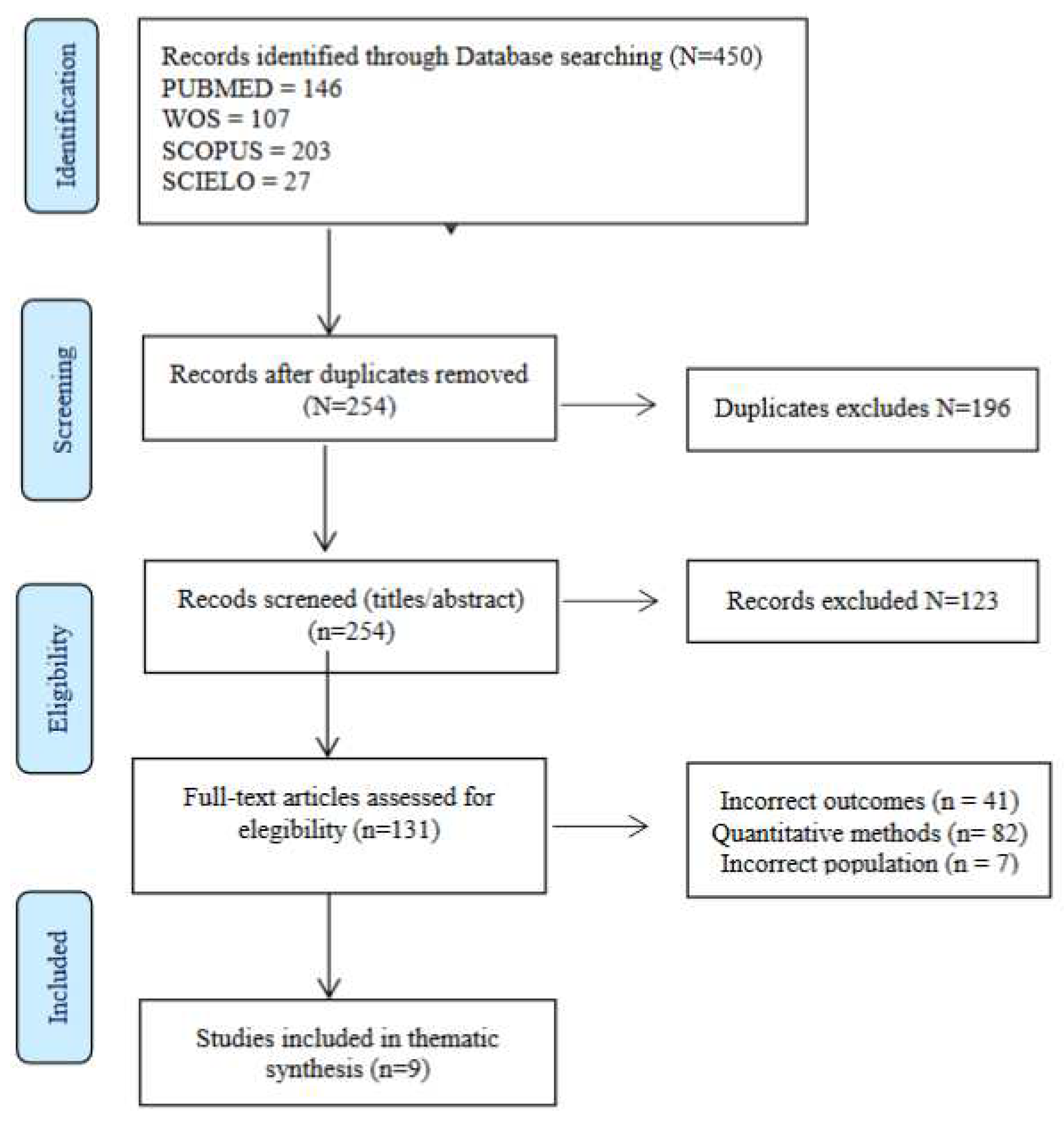
Table 1.
Quality assessment of studies [22].
Table 1.
Quality assessment of studies [22].
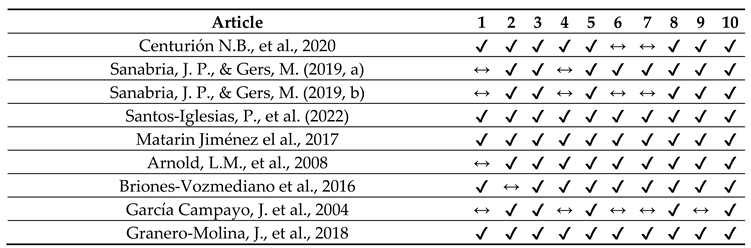
* ✔ Yes, ↔ Unclear, ✘ No. 1. Congruence of philosophical perspective/methodology 2. Congruence of methodology/objectives 3. Congruence of methodology/data collection 4. Congruence of methodology/data analysis 5. Congruence of methodology/interpretation of results 6. Cultural and theoretical context of the researcher. 7. Influence of the researcher on the research 8. Participants represented. Research Ethics Committee Approval 10. Conclusions from data analysis/interpretation.
Table 2.
Stages in the thematic synthesis process.
| Stage | Description | Steps |
|---|---|---|
| STAGE 1 | Text coding | Recall review question Read/re-read findings of the studies Line-by-line inductive coding Review of codes in relation to the text |
| STAGE 2 | Development of descriptive themes | Search for similarities/differences between codes Inductive generation of new codes Write preliminary and final report |
| STAGE 3 | Development of analytical themes | Inductive analysis of sub-themes Individual/independent analysis Pooling and group review |
Table 4.
Themes and subthemes.
| Themes | Subthemes |
|---|---|
| 3.1“I want to, but I can’t”: a shift in feminine sexuality | 3.1.1 Pain/stiffness limits pleasure and desire. 3.1.2 Irritability and low mood. 3.1.3 Decreased frequency/difficulty in having orgasm. 3.1.4 Pharmacological treatment does not help sexuality. 3.1.5 Having sex “for your partner”: avoiding sexual encounters. |
| 3.2 Resetting sex life and intimacy | 3.2.1 I know it’s not mutual. 3.2.2 Bearing the moral burden. 3.2.3 Managing misunderstanding/support. 3.2.4 Vulnerability ... of my relationship. 3.2.5 Faking it for fear of abandonment. |
| 3.3 Taking charge of a “new sexuality” | 3.3.1 Striving for my (our) sex life. 3.3.2 Forgetting the past: taking initiative. 3.3.3 Changing habits: finding the moment. 3.3.4 Getting to know each other: prioritising play and touch. 3.3.5 Changing positions and using lubricants. 3.3.6 Exercise and therapy. 3.3.7 Social and professional support. |
SRH = Sexual and reproductive Health. IMW = Irregular Migrant Women.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



