
Submitted:
13 September 2023
Posted:
19 September 2023
You are already at the latest version
Abstract
The amino acids (AAs) and vitamins imbalances are observed in celiac disease (CD). This study evaluated the plasma profile of vitamin A and AAs and the expression level of IL-2, IL-4, IL-10, IL-12 and TGFβ in CD patients. A total of 60 children and adults with CD and 40 healthy controls (HCs) were included. Plasma profile of Vitamin A and AAs and the mRNA expression levels of target genes were assessed. Active adult patients exhibited a decrease in Vitamin A levels (p=0.04) and an increase in IL-2 (p=0.008) and IL-12 (p=0.007) mRNA expression compared to HCs. Treated adult patients showed elevated Serine (p=0.003) and Glycin (p=0.04) levels, as well as increased IL-12 (P<0.0001) mRNA expression, and a decrease in Tryptophan (p=0.04) levels relative to the controls. Additionally, treated adult patients had higher plasma levels of Threonine compared to both active (p=0.04) and control (p=0.02) subjects, and increased mRNA expression of IL-4 (p=0.01) in comparison to active patients. In active children with CD, IL-2 mRNA level was found to be higher than in controls (P<0.0001) and in treated children (p=0.005). Treated children with CD exhibited decreased plasma levels of Tryptophan (p=0.01) and Isoleucine (p=0.01) relative to the controls, and increased mRNA expression of TGFβ (p=0.04) relative to active patients. Managing Retinoic acid levels is crucial to alleviate intestinal inflammation of CD patients. Threonine, tryptophan, and Isoleucine are potential therapeutic options for treating CD, and targeting serine, histidine, tyrosine, and aspartate may hold promise as therapeutic targets for CD patients.
Keywords:
celiac disease
; gluten free diet
; amino acids
; vitamin A
; treatment
1. Introduction
Celiac disease (CD) is a chronic intestinal inflammatory disorder caused by intolerance to gluten protein in genetically susceptible individuals [1]. According to the screening studies, the prevalence of CD is about 0.5 to 1 percent worldwide [2]. It is widely accepted that human leukocyte antigen (HLA)-DQ2 and HLA-DQ8 are the main predisposing factors for CD development [3]. This disorder can present with intestinal (like bloating, chronic diarrhea, dyspepsia) and extra-intestinal (like chronic anemia, fatigue, osteoporosis, infertility) symptoms and some CD patients do not exhibit any of the classical manifestations [4]. As gluten proteins are the primary cause of this enteropathy, adherence to a lifelong gluten-free diet (GFD) is considered as the only available treatment for CD patients [5]. Abnormal T-cell mediated immune responses to dietary gluten leads to the massive production pro-inflammatory cytokines including [6]. There is also endogenous immunoregulatory mechanisms, although not sufficient, involving the negative feedback mechanisms like the secretion of anti-inflammatory cytokines attempt to counterbalance these abnormal immune responses [7]. The inflammation caused by immune responses to ingested gluten leads to villous atrophy and crypt hyperplasia in the small intestine [8]. Villous atrophy is accompanied by decreased surface area of the small bowel available for nutrient absorption [9]. It is well documented that celiac disease is often accompanied by imbalances in amino acids (AAs) and vitamins [10,11,12].
Vitamin A (VA), as a lipid-soluble organic compound, is one of the most studied nutrients in context of its effect on the immune system [13]. In fact, Retinoic acid (RA), the vitamin A metabolite, affects both adaptive and innate immune responses and plays an important role in inducing effector CD4+ T cell responses during infection [14,15]. RA through binding to its receptors can drive Th1/Th2 differentiation towards Th2 and also induces the TGF-β-dependent conversion of naïve T cells into Foxp3+ regulatory T cells and mediates the immune homeostasis [15,16,17,18]. It can also affect the expression of both pro-inflammatory (like IFN-γ and IL-12) and anti-inflammatory (like IL-10 and IL-4) production [18,19]. Vitamin A deficiency (VAD) is reported to be associated with dysregulated immune responses [20]. Overall, RA exhibits significant anti-inflammatory effects in alleviating intestinal inflammation, what is observed in CD. However, a recent study has revealed that RA may also collaborate with elevated levels of IL-15 to stimulate a proinflammatory T-cell reaction against dietary antigens. As such, further research is required to gain a deeper understanding of RA’s role in inflammatory pathways [21,22,23].
Amino acids, which are divided into essential and non-essential amino acids, stand as important regulators of natural killer cells, B lymphocytes, T lymphocytes, and macrophages and participate to the regulation of innate and adaptive immune responses [24,25]. Indoleamine 2,3-dioxygenase (IDO), as an enzyme with high expression in the intestinal biopsy samples of CD patients, can metabolize tryptophan (TRP) to kynurenine that has anti-inflammatory properties [26,27,28]. Moreover, increased histidine (HIS), glycine (GLY), arginine (ARG) could enhance the vulnerability to intestinal inflammation in potential CD patients [29]. The roles of Metionin (MET), threonine (THR), His, and several other amino acids in improving intestinal villus morphology, intestinal barrier integrity and regulating immune responses have also been demonstrated so far [30]. Additionally, ameliorating gut inflammation by serine (SER), glutamine (GLN) and glutamate (GLU) has been discussed [31,32,33]. Recent studies indicates that amino acids play a crucial role in regulating inflammatory responses and can modulate the expression of pro- and anti-inflammatory cytokines [34].
Gluten containing grains are essential part of a healthy diet and considered as a good source of complex carbohydrates, some important vitamins, minerals and amino acids and eliminating them from the diet may cause health problems [35,36]. Therefore, monitoring the changes in essential micronutrient levels that occur during CD pathogenesis and assessing the impact of GFD on these changes is of great importance. Among essential micronutrients, vitamin A and amino acids play important roles in regulating immune responses and maintaining intestinal homeostasis. Therefore, in the present study, we evaluated the changes in plasma levels of vitamin A and AAs of adults and children patients with CD relative to the healthy controls and evaluate the effects of these changes on the expression level of IL-2, IL-4, IL-10, IL-12 and TGFβ.
2. Materials and Methods
Recruitment of Participants and Peripheral Blood Sample Collection
We studied 30 newly diagnosed (active) CD patients: 15 children (mean age 9.20±3.27 years) and 15 adults (mean age 31.8 ± 12.71 years); 30 treated CD subjects: 15 children (mean age 10.60±2.92 years) and 15 adults (mean age 39.0 ± 8.87 years). CD patients were recruited between February 2021 and Jun 2022 from Celiac Disease and Gluten Related Disorders Research Center, Shahid Beheshti University of Medical Sciences. The inclusion criteria were confirmed CD according to the European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) criteria in children [37] and according to the American Gastroenterological Association (AGA) recommendations in adults [38]. Moreover, 40 healthy subjects including 20 children (mean age 10.9±3.97 years) and 20 adults (mean age 35.25 ± 10.7 years) with no clinical and serological evidences of CD and any other immune-related diseases up to their first-degree relatives that were willing to participate in the study, recruited as a control group. Pregnant and lactating women, subjects with other autoimmune and inflammatory conditions, acute or chronic diseases, cancer, gastrointestinal infections were excluded from the study.
Venous peripheral blood samples (10 ml) were carefully obtained from study participants between 8:00 and 8:30 a.m. after an overnight fasting of at least 12 hr. Demographic data, clinical symptoms, and self-reported dietary habits were recorded earlier than blood sampling. In fact, the self-reported amount of meat, fish, eggs, pulses, dairy products, fats, vegetables, fruits, sweets, and nuts consumption during 1 month prior to the study were inquired by a questionnaire and categorized as sufficient or insufficient consumptions (according to the Asian food pyramid) [39].
The study was admitted by the ethical committee of the Research Institute for Gastroenterology and Liver Diseases (RIGLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran (IR.SBMU.MSP. REC.1397.564) and written informed consent was provided from all included subjects before participation.
Metabolite Analysis
Whole blood samples were centrifuged at 3500 rpm for 15 min, and the resulting plasma fraction was immediately stored at -80℃ until used for HPLC analysis of Vitamin A and total amino acids profiles. An HPLC series system (ACME 9000 system, Younglin, Anyang, Korea) with a UV detector (for Vitamin A levels) and a fluorescence detector (for amino acids levels) was used in the present study. Plasma samples were deproteinized by adding a methanolic solution. After vortexing for 30 sec and centrifugation for 7 min at 5000 rpm, the clear supernatant was used for further analysis. For Vitamin A analysis, 100 λ of the supernatant was injected into the C18 column (250 mm × 4.6 mm, 5 µm) along with methanol- ethanol (3:1 V/V) as the mobile phase, and the UV signals were recorded at 295nm. Moreover, the chromatographic separation of AAs was achieved by adding 100 λ of the clear supernatant to the GL Sciences column (250 mm × 3.0 mm, 3 μm) using methanol- Tetrahydrofuran (4:1 V/V) as the mobile phase and the fluorescence signals were recorded at the optimal excitation and emission wavelength (ex:340 nm, em:450 nm).
RNA Extraction and cDNA Synthesis
Total ribonucleic acid (RNA) was isolated from whole blood samples of all participants a YTA Total RNA Purification Mini kit for Blood/Cultured Cell/Tissue (Yekta Tajhiz Azma, Iran) according to manufacture instruction. RNA concentration and quality were evaluated by NanoDrop 1000 spectrophotometer (NanoDrop Fisher Thermo, Wilmington, DE, USA). After adjusting the RNA concentrations, cDNA synthesis was performed using the 2 Step 2X RTPCR Premix (Taq) kit (BioFact™, South Korea) and was stored at -20°C for quantitative real-time PCR.
Primer Designing and Quantitative Real-Time PCR (RT-qPCR)
The specific primers used for amplification of IL-2, IL-4, IL-10, IL-12, TGFβ and Beta- 2-microglobulin (B2M), as a housekeeping gene, were designed using the Gene Runner (version 3.05) software. These sequences were analyzed by PrimerBlast in the NCBI database (http://blast.ncbi.nlm. nih.gov/) and their properties are shown in supplementary Table 1. The mRNA expression levels of target genes were assessed by SYBR Premix Ex Taq (RealQ Plus 2x Master Mix Green-Amplicon, Japan using Rotor-Gene® Q (Qiagen, Germany) real-time PCR system. All qPCR reactions were performed in duplicates and the mRNA expression level of each gene was calculated according to delta-Ct (ΔCt = ΔCt target − ΔCt endogenous), and was presented in graphs using the comparative Ct method (2-ΔΔCt).
Statistical Analysis
All data were assessed using Statistical Package for the Social Sciences (SPSS) version 25.0, SPSS Inc., Chicago, IL, USA. Figures were drawn using GRAPHPAD Prism 8.4.0 (GraphPad Software, Inc, San Diego, CA). All the data were expressed as the mean ± standard deviation (SD). The one-way analysis of variance (ANOVA) was used to analyze the difference between groups. The correlation between variables was assessed using the Pearson’s and Spearman’s correlation tests and P-value < 0.05 was considered significant.
3. Results
Demographic and Clinical Characteristics
Demographic characteristics of study subjects were reported in Table 1. Briefly, 60 confirmed CD patients, including 30 treated subjects (15 children and 15 adults) and 30 active patients (15 children and 15 adults), and 40 healthy controls were included. The case and control participants in both the pediatrics and adults groups were matched for age, BMI and gender and there was no significant difference in this regard between the studied groups (P>0.05) (Table 1).
HLA-DQ2 haplotype was observed in 60% of active CD adults, 80% of treated CD adults, 80% of active CD children, 73.3% of treated CD children (Supplementary Figure 1). According to the Marsh classification, most of the patients in treated adults, active adults, and treated pediatrics groups were in the Marsh III stage (80%, 80% and 40% respectively). (Supplementary Figure 1 and Figure 2).
Weight loss was reported as the most prevalent gastrointestinal symptom among all groups of patients with CD, with rates of 60% in active and treated adults and treated pediatrics, and 100% in active pediatrics. Meanwhile, fatigue emerged as the most common non-gastrointestinal symptom, with percentages of 66.7% in treated adults, 80% in active adults, 53.3% in treated children, and 100% in active children. Among active CD adults, both fatigue and anemia were the most frequently reported symptoms, with rates of 80% (Figure 1).
Vitamin A Levels
Our data demonstrated a significant decrease in plasma level of Vitamin A in active CD adult patients in comparison to the control adults (p=0.04). There was not any significant difference in plasma level of Vitamin A between pediatric groups (p˃0.05) (Figure 2).
Amino Acids Profiles
Our results revealed that in the comparison between the adult groups, plasma levels of SER (p=0.003) and GLY (p=0.04) were significantly higher in treated CD patients than in controls. THR level was also increased in treated CD patients than in active CD (p=0.04) and control (p=0.02) subjects. In contrast, treated CD patients showed a lower concentration of TRP than controls (p=0.04) (Figure 3A).
TRP and ILE levels have been shown to be significantly lower in treated pediatric CD patients relative to the controls (p=0.01 for both of them) (Figure 3B).
mRNA Expression Analysis
IL-2 mRNA expression was higher in active adult CD patients compared to healthy adult controls (P=0.008). Active CD children also exhibited higher IL-2 expression compared to treated (P=0.005) and control children groups (P<0.0001). Adult CD patients, both active and treated, displayed higher IL-12 mRNA levels than adult control subjects (P=0.007 and P<0.0001, respectively). Although this pattern was also observed in pediatric groups the differences were not statistically significant (P>0.05). IL-4 mRNA expression was increased in adult treated CD patients compared to those with active CD (P =0.01). IL-4 expression in pediatric groups resembled that of the adult groups, but no significant difference was found (P>0.05). Children with treated CD had higher TGFβ expression than those with the active form of the disease (P=0.04). Similar observations were made in adult groups, but the difference was not found to be statistically significant (P>0.05). The levels of IL-10 did not significantly differ between children and adult groups (P>0.05) (Figure 4).
Dietary Habits
According to the data presented in Figure 5, adults with active CD had a reduced intake of fish. Similarly, both treated adults and children had a considerably lower consumption of dairy products.
Correlation Analysis
IL-4 mRNA level had positive correlations with ILE (P=0.04, r=0.31), PHE (P=0.02, r=0.52), and TYR (P=0.02, r=0.52) concentrations in adults. TGF-β mRNA expression showed positive correlations with ILE (P=0.04, r=0.43), VAL (P=0.04, r=0.57), MET (P=0.007, r=0.7), TRP (P=0.04, r=0.49), ALA (P=0.03, r=0.6), and CIT (P=0.03, r=0.59) in adults, as well as with PHE (P=0.04, r=0.46) and TYR (P=0.01, r=0.55) in children. IL-10 mRNA levels had a positive correlation with THR (P=0.03, r=0.48) plasma levels in adults (Figure 6).
4. Discussion
Our results showed that adult patients with CD had significantly lower levels of plasma vitamin A compared to adult controls, but there was not any significant difference between pediatrics in this regard. This finding is consistent with previous reports. For instance, Wierdsma et al. evaluated the nutritional and vitamin/mineral status of early diagnosed adult CD-patients in comparing to healthy individuals. According to their results, 7.5% of patients revealed deficiency of vitamin A [36]. Weintraub et al. in a study on active children with CD, did not observe an association between CD and vitamin A deficiency [40]. It should be noted that lower consumption of fish by our participated adults with active CD may had a negative effect on their vitamin A levels. Due to the importance of RA as a vitamin A metabolite in alleviating intestinal inflammation and affecting adaptive and innate immune responses, controlling its level in CD patients is of great importance [14,15].
Previous research has indicated that AAs possess the ability to serve as biomarkers for diagnosing CD in a noninvasive manner. Furthermore, there is potential for utilizing AAs as targets for therapy in CD treatment [41,42]. For instance, Khalkhal et al. showed that changes in metabolic pathways like glutamine and glutamate metabolism; valine, leucine, and isoleucine biosynthesis and degradation can be used in distinguishing CD patients from HCs [41]. Fathi et al. [42] also suggested that valine is an important AA that can be used as potential target for CD therapy. Through examination of plasma amino acid levels, we observed significantly elevated levels of SER and GLY in treated adult patients with CD compared to control subjects. Additionally, level of THR was also higher in treated CD patients compared to both active CD patients and control subjects. SER, GLY, and THR are known as amino acids involved in maintaining intestinal barrier integrity and possess anti-inflammatory properties [43,44,45]. The elevation of these amino acids in treated patients may contribute to the improvement of intestinal damage. Crucially, THR plays a significant role in the composition of intestinal mucins and IgA. These substances are produced in large quantities during inflammation, aiding in the restoration of intestinal balance and regulating the body’s pro- and anti-inflammatory reactions [46,47,48]. In the current study, the THR concentration showed a positive correlation with IL-10 mRNA level, a cytokine that plays a critical role in preventing inflammatory responses. It may suggest that THR could potentially be used as a therapeutic option for treating CD [49].
Importantly, plasma concentration of TRP was reduced in our treated CD adults and pediatrics. The decreased levels of TRP in our treated CD patients may be attributed to a lower consumption of dairy products, which are the primary source of this essential amino acid [50]. In fact, lactose intolerance can be caused by the impaired intestinal mucosa in individuals with CD. Many individuals adhering to a gluten-free diet often report lactose intolerance and subsequently refrain from consuming milk and dairy items [51]. A potential hindrance to intestinal healing may occur as a result of decreased TRP intake, since TRP catabolism plays a role in regulating intestinal inflammation [28]. Additionally, CD patients exhibited reduced bacterial metabolism of tryptophan and their gut microbiota failed to adequately activate the aryl hydrocarbon receptor (AhR) pathway, which is responsible for controlling inflammation and safeguarding the gut barrier [52]. According to reports, the high tryptophan diet was found to increase the production of AhR ligands and decrease gluten immunopathology in mice expressing the DQ8 gene [53]. As a result, there is a hypothesis suggesting that supplementing with TRP could potentially serve as a new treatment for CD patients. TRP also showed to promote the production of TGF-β cytokines and activate the TGF-β signaling pathway [54]. In the current study, a positive correlation was observed between TGF-β and TRP. Pediatrics with GFD-treated CD had increased expression of TGFβ than active subjects. This change was also observed in adult groups but was insignificant. Since TGFβ is an anti-inflammatory cytokine with a regulatory effect on immune homeostasis, impairment in TGFβ signaling may be associated with intestinal inflammation [55] and the decrease in TGFβ gene expression observed in active CD subjects is justified. New experimental studies are needed to approve this potential of TRP for controlling CD patients’ manifestations. The level of TGF-β showed positive correlation with ILE, VAL, MET, ALA, PHE, TYR and CIT too.
ILE (p=0.01) level was also significantly lower in treated pediatric CD patients relative to the controls. ILE is a crucial amino acid acknowledged for its role in controlling immune function, particularly in the production of substances important for immune response [56]. Mao et al. demonstrated that the administration of l-isoleucine could alleviate rotavirus infection by impacting the immune response in weaned piglets. Specifically, they observed changes in the mRNA expression and concentration of inflammation-related cytokines in the ileal mucosa (13). Actually, the administration of l-isoleucine can effectively manage and treat colitis induced by dextran sulfate sodium (DSS) in rats [56,57]. A notable outcome of this treatment is its ability to boost the levels of IL-4 in the rats’ colon [56]. In the current study treated adults with CD had higher levels of IL-4 mRNA than active CD adult subjects and there was a significant positive correlation between the level of this cytokine and ILE level. Due to the potential protective role of IL4 toward the inflammatory processes occurring in the gut mucosa of CD patients, evaluating the potential of ILE to be used as another amino acid supplement for alleviating CD patients’ inflammation is of great importance. Furthermore, the presence of IL-4 had been shown to negatively impact the activity of IDO, an enzyme responsible for breaking down tryptophan [58]. Therefore, the increased levels of IL-4 observed in adults with CD who were treated with a GFD could be attributed to the prevention of total TRP loss in this group (as previously mentioned, the level of TRP had decreased in GFD-treated adult CD patients). On the other hand, since vitamin A is a positive regulator of IL-4, the low level of this cytokine in active CD adults may be related to the low level of vitamin A in this group [59]. This cytokine also showed positive correlations with PHE, and TYR.
IL-2 mRNA expression was higher in our studied adult patients with active CD than in healthy adult controls and in children with active CD than in treated and control children groups. In this regard, Manavalan et al. demonstrated a significant elevation in IL-2 levels in active CD patients relative to the controls and also in patients who were on GFD for less than 1 year in comparison to the patients on GFD for more than 1 year. Actually, IL-2 is among the important mediators of the Th-1 immune response, and its role in CD is well documented [60]. Its level increases after one-off gluten ingestion and it is considered as a potential diagnostic biomarker for CD [61,62]. Active and treated adult CD patients also had higher IL-12 mRNA levels in comparison to the control subjects. Since IL-12 is effective in the expansion of naive CD4+ T cells to Th1 cells, the important cells in CD pathogenesis, the increase of this cytokine in active CD groups is not unexpected [63]. On the other hand, the regulatory effects of this cytokine on immune responses and its positive effect on the expansion and increase of regulatory T cells have also been reported in studies that justify its increase in the treated groups [64]. According to Björck et al., the serum level of IL-12 was significantly increased in children with CD and decreased following GFD adherence [65]. The mucosal increase of IL-12 during intestinal inflammation has also been observed [66]. It has been shown that SER, HIS and TYR are required for IL-2 binding and biological activity, and ASP, THR, and TRP are among the important amino acids for the interaction of IL-12 with its receptor [67]. So might controlling these residues have the potential to be considered as therapeutic targets for CD patients, which needs to be approved in further studies [68].
5. Conclusions
In summary, the points discussed underscore the importance of managing RA levels in CD patients due to its role in alleviating intestinal inflammation and modulating immune responses. THR, TRP, and ILE have been suggested as potential therapeutic options for treating CD. Additionally, targeting specific amino acids such as SER, HIS, TYR, and ASP may hold promise as therapeutic targets for CD patients, although further research is needed to confirm this hypothesis.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org., Figure S1: HLA status of studied patients; Figure S2. Histological classification of studied patients; Table S1: Sequence of primers used in real-time PCR.
Author Contributions
Conceptualization, M.R.N. and K.R.; methodology, S.F., and N.A.; software, S.F., and N.A.; validation, M.R.N. and A.N.; formal analysis, N.A., S.F., S. A.; investigation, S.F.; Data curation, M.R.N.; writing—original draft preparation, S.F., N.A.; writing—review and editing, M.R.N, K.R., A.S., S.A.; visualization, N.A.; supervision, M.R.N., K.R.; project administration, S.F.; All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Gastroenterology and Liver Diseases Research Center, Research Institute for Gastroenterology and Liver Diseases, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Institutional Review Board Statement
The study was admitted by the ethical committee of the Research Institute for Gas-troenterology and Liver Diseases (RIGLD), Shahid Beheshti University of Medical Scienc-es, Tehran, Iran (IR.SBMU.MSP. REC.1397.564) and written informed consent was pro-vided from all included subjects before participation.
Informed Consent Statement
Written informed consent has been obtained from the patients.
Data Availability Statement
The data presented in this study are available on request from the corresponding author
Acknowledgments
The Research Institute for Gastroenterology and Liver Diseases (RIGLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran is gratefully acknowledged.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ferretti, G.; Bacchetti, T.; Masciangelo, S.; Saturni, L. Celiac disease, inflammation and oxidative damage: A nutrigenetic approach. Nutrients 2012, 4, 243–257. [Google Scholar] [CrossRef] [PubMed]
- Gujral, N.; Freeman, H.J.; Thomson, A.B. Celiac disease: Prevalence, diagnosis, pathogenesis and treatment. World J. Gastroenterol. 2012, 18, 6036–6059. [Google Scholar] [CrossRef]
- Mashayekhi, K.; Rostami-Nejad, M.; Amani, D.; Rezaei-Tavirani, M.; Mohaghegh-Shalmani, H.; Zali, M.R. A rapid and sensitive assay to identify HLA-DQ2/8 risk alleles for celiac disease using real-time PCR method. Gastroenterol. Hepatol. Bed Bench 2018, 11, 250–258. [Google Scholar] [PubMed]
- Parzanese, I.; Qehajaj, D.; Patrinicola, F.; Aralica, M.; Chiriva-Internati, M.; Stifter, S.; Elli, L.; Grizzi, F. Celiac disease: From pathophysiology to treatment. World J. Gastrointest. Pathophysiol. 2017, 8, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Itzlinger, A.; Branchi, F.; Elli, L.; Schumann, M. Gluten-Free Diet. in Celiac Disease-Forever and for All? Nutrients 2018, 10, 1796. [Google Scholar] [CrossRef]
- Barone, M.V.; Auricchio, R.; Nanayakkara, M.; Greco, L.; Troncone, R.; Auricchio, S. Pivotal Role of Inflammation in Celiac Disease. Int. J. Mol. Sci. 2022, 23, 7177. [Google Scholar] [CrossRef]
- Mazzarella, G.; Aufiero, V. Immunoregulation in celiac disease. Gastroenterol. Hepatol. Endosc. 2016, 1, 13–17. [Google Scholar] [CrossRef]
- Uhde, M.; Ajamian, M.; Caio, G.; De Giorgio, R.; Indart, A.; Green, P.H.; Verna, E.C.; Volta, U.; Alaedini, A. Intestinal cell damage and systemic immune activation in individuals reporting sensitivity to wheat in the absence of coeliac disease. Gut 2016, 65, 1930–1937. [Google Scholar] [CrossRef]
- Tran, T.H.; Smith, C.; Mangione, R.A. Drug absorption in celiac disease. Am. J. Health-Syst. Pharm. 2013, 70, 2199–2206. [Google Scholar] [CrossRef]
- Unalp-Arida, A.; Liu, R.; Ruhl, C.E. Nutrient intake differs among persons with celiac disease and gluten-related disorders in the United States. Sci. Rep. 2022, 12, 5566. [Google Scholar] [CrossRef]
- McGrogan, L.; Mackinder, M.; Stefanowicz, F.; Aroutiounova, M.; Catchpole, A.; Wadsworth, J.; Buchanan, E.; Cardigan, T.; Duncan, H.; Hansen, R.; et al. Micronutrient deficiencies in children with coeliac disease; a double-edged sword of both untreated disease and treatment with gluten-free diet. Clin. Nutr. 2021, 40, 2784–2790. [Google Scholar] [CrossRef] [PubMed]
- Drabińska, N.; Krupa-Kozak, U.; Ciska, E.; Jarocka-Cyrta, E. Plasma profile and urine excretion of amino acids in children with celiac disease on gluten-free diet after oligofructose-enriched inulin intervention: Results of a randomised placebo-controlled pilot study. Amino Acids 2018, 50. [Google Scholar] [CrossRef] [PubMed]
- Chea, E.P.; Lopez, M.J.; Milstein, H.; Vitamin, A. In StatPearls; Treasure Island, FL, USA, 2022.
- Dzopalic, T.; Bozic-Nedeljkovic, B.; Jurisic, V. The role of vitamin A and vitamin D in modulation of the immune response with a focus on innate lymphoid cells. Cent. Eur. J. Immunol. 2021, 46, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.A.; Cannons, J.L.; Grainger, J.R.; Dos Santos, L.M.; Hand, T.W.; Naik, S.; Wohlfert, E.A.; Chou, D.B.; Oldenhove, G.; Robinson, M.; et al. Essential role for retinoic acid in the promotion of CD4(+) T cell effector responses via retinoic acid receptor alpha. Immunity 2011, 34, 435–447. [Google Scholar] [CrossRef] [PubMed]
- Raverdeau, M.; Mills, K.H. Modulation of T cell and innate immune responses by retinoic Acid. J. Immunol. 2014, 192, 2953–2958. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Awasthi, A. Vitamin A and the Immune System; 2019; pp. 53–73.
- Cassani, B.; Villablanca, E.J.; De Calisto, J.; Wang, S.; Mora, J.R. Vitamin A and immune regulation: Role of retinoic acid in gut-associated dendritic cell education, immune protection and tolerance. Mol. Asp. Med. 2012, 33, 63–76. [Google Scholar] [CrossRef]
- Stephensen, C.B.; Rasooly, R.; Jiang, X.; Ceddia, M.A.; Weaver, C.T.; Chandraratna, R.A.; Bucy, R.P. Vitamin A enhances in vitro Th2 development via retinoid X receptor pathway. J. Immunol. 2002, 168, 4495–4503. [Google Scholar] [CrossRef]
- Stephensen, C.B. Vitamin A, infection, and immune function. Annu. Rev. Nutr. 2001, 21, 167–192. [Google Scholar] [CrossRef]
- DePaolo, R.W.; Abadie, V.; Tang, F.; Fehlner-Peach, H.; Hall, J.A.; Wang, W.; Marietta, E.V.; Kasarda, D.D.; Waldmann, T.A.; Murray, J.A.; et al. Co-adjuvant effects of retinoic acid and IL-15 induce inflammatory immunity to dietary antigens. Nature 2011, 471, 220–224. [Google Scholar] [CrossRef]
- Hall, Jason, A. ; Grainger, John, R.; Spencer, Sean, P.; Belkaid, Y. The Role of Retinoic Acid in Tolerance and Immunity. Immunity 2011, 35, 13–22. [Google Scholar] [CrossRef]
- Oliveira, L.d.M.; Teixeira, F.M.E.; Sato, M.N. Impact of Retinoic Acid on Immune Cells and Inflammatory Diseases. Mediat. Inflamm. 2018, 2018, 3067126. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Wu, G. Important roles of amino acids in immune responses. Br. J. Nutr. 2022, 127, 398–402. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Yin, Y.L.; Li, D.; Kim, S.W.; Wu, G. Amino acids and immune function. Br. J. Nutr. 2007, 98, 237–252. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Xu, K.; Liu, H.; Liu, G.; Bai, M.; Peng, C.; Li, T.; Yin, Y. Impact of the Gut Microbiota on Intestinal Immunity Mediated by Tryptophan Metabolism. Front. Cell Infect. Microbiol. 2018, 8, 13. [Google Scholar] [CrossRef]
- Mellor, A.L.; Munn, D.H. Tryptophan catabolism and T-cell tolerance: Immunosuppression by starvation? Immunol. Today 1999, 20, 469–473. [Google Scholar] [CrossRef]
- Torres, M.I.; López-Casado, M.A.; Lorite, P.; Ríos, A. Tryptophan metabolism and indoleamine 2,3-dioxygenase expression in coeliac disease. Clin. Exp. Immunol. 2007, 148, 419–424. [Google Scholar] [CrossRef]
- Upadhyay, D.; Das, P.; Dattagupta, S.; Makharia, G.K.; Jagannathan, N.R.; Sharma, U. NMR based metabolic profiling of patients with potential celiac disease elucidating early biochemical changes of gluten-sensitivity: A pilot study. Clin. Chim. Acta Int. J. Clin. Chem. 2022, 531, 291–301. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, X.; Hu, C.A. Therapeutic Potential of Amino Acids in Inflammatory Bowel Disease. Nutrients 2017, 9, 920. [Google Scholar] [CrossRef]
- Sugihara, K.; Morhardt, T.L.; Kamada, N. The Role of Dietary Nutrients in Inflammatory Bowel Disease. Front. Immunol. 2018, 9, 3183. [Google Scholar] [CrossRef]
- Xu, L.; Sun, J.; Lu, R.; Ji, Q.; Xu, J.G. Effect of glutamate on inflammatory responses of intestine and brain after focal cerebral ischemia. World J. Gastroenterol. 2005, 11, 733–736. [Google Scholar] [CrossRef]
- Kim, M.H.; Kim, H. The Roles of Glutamine in the Intestine and Its Implication in Intestinal Diseases. Int. J. Mol. Sci. 2017, 18. [Google Scholar] [CrossRef] [PubMed]
- Qian, B.; Zhao, X.; Yang, Y.; Tian, C. Antioxidant and anti-inflammatory peptide fraction from oyster soft tissue by enzymatic hydrolysis. Food Sci. Nutr. 2020, 8, 3947–3956. [Google Scholar] [CrossRef]
- van Hees, N.J.; Giltay, E.J.; Tielemans, S.M.; Geleijnse, J.M.; Puvill, T.; Janssen, N.; van der Does, W. Essential amino acids in the gluten-free diet and serum in relation to depression in patients with celiac disease. PLoS ONE 2015, 10, e0122619. [Google Scholar] [CrossRef]
- Wierdsma, N.J.; van Bokhorst-de van der Schueren, M.A.; Berkenpas, M.; Mulder, C.J.; van Bodegraven, A.A. Vitamin and mineral deficiencies are highly prevalent in newly diagnosed celiac disease patients. Nutrients 2013, 5, 3975–3992. [Google Scholar] [CrossRef] [PubMed]
- Revised criteria for diagnosis of coeliac disease. Report of Working Group of European Society of Paediatric Gastroenterology and Nutrition. Arch. Dis. Child. 1990, 65, 909–911. [Google Scholar] [CrossRef]
- AGA Institute Medical Position Statement on the Diagnosis and Management of Celiac Disease. Gastroenterology 2006, 131, 1977–1980. [CrossRef]
- Marcus, J.B. Chapter 12—Global Food and Nutrition: World Food, Health and the Environment: Practical Applications for Nutrition, Food Science and Culinary Professionals. In Culinary Nutrition; Marcus, J.B., Ed.; Academic Press: San Diego, CA, USA, 2013; pp. 545–605. [Google Scholar]
- Weintraub, Y.; Ben-Tov, A.; Dotan, G.; Yerushalmy-Feler, A.; Weiner, D.; Levy, D.; Lubetzky, R.; Cohen, S. Vitamin A levels are comparable between children with newly diagnosed coeliac disease and non-coeliac controls. Acta Paediatr. 2019, 108, 2095–2099. [Google Scholar] [CrossRef] [PubMed]
- Khalkhal, E.; Rezaei-Tavirani, M.; Fathi, F.; Nobakht, M.G.B.F.; Taherkhani, A.; Rostami-Nejad, M.; Asri, N.; Haidari, M.H. Screening of Altered Metabolites and Metabolic Pathways in Celiac Disease Using NMR Spectroscopy. Biomed. Res. Int. 2021, 2021, 1798783. [Google Scholar] [CrossRef] [PubMed]
- Fathi, F.; Ektefa, F.; Arefi Oskouie, A.; Rostami, K.; Rezaei-Tavirani, M.; Mohammad Alizadeh, A.H.; Tafazzoli, M.; Rostami Nejad, M. NMR based metabonomics study on celiac disease in the blood serum. Gastroenterol. Hepatol. Bed Bench 2013, 6, 190–194. [Google Scholar]
- Rémond, D.; Buffière, C.; Godin, J.P.; Mirand, P.P.; Obled, C.; Papet, I.; Dardevet, D.; Williamson, G.; Breuillé, D.; Faure, M. Intestinal inflammation increases gastrointestinal threonine uptake and mucin synthesis in enterally fed minipigs. J. Nutr. 2009, 139, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Zheng, Y.; Ma, J.; Yin, J.; Chen, S. The Effects of Dietary Glycine on the Acetic Acid-Induced Mouse Model of Colitis. Mediat. Inflamm. 2020, 2020, 5867627. [Google Scholar] [CrossRef] [PubMed]
- Sugihara, K.; Kamada, N. 10 the Role of Dietary L-Serine in the Regulation of Intestinal Mucus Barrier during Inflammation. Gastroenterology 2020, 158, S70. [Google Scholar] [CrossRef]
- Zhang, Q.; Chen, X.; Eicher, S.D.; Ajuwon, K.M.; Applegate, T.J. Effect of threonine on secretory immune system using a chicken intestinal ex vivo model with lipopolysaccharide challenge. Poult. Sci. 2017, 96, 3043–3051. [Google Scholar] [CrossRef]
- Gaifem, J.; Gonçalves, L.G.; Dinis-Oliveira, R.J.; Cunha, C.; Carvalho, A.; Torrado, E.; Rodrigues, F.; Saraiva, M.; Castro, A.G.; Silvestre, R. L-Threonine Supplementation During Colitis Onset Delays Disease Recovery. Front. Physiol. 2018, 9, 1247. [Google Scholar] [CrossRef] [PubMed]
- Park, H.-B.; Choi, B.-C.; Baek, K.-H. PGK1 modulates balance between pro- and anti-inflammatory cytokines by interacting with ITI-H4. Biomed. Pharmacother. 2023, 161, 114437. [Google Scholar] [CrossRef]
- Iyer, S.S.; Cheng, G. Role of interleukin 10 transcriptional regulation in inflammation and autoimmune disease. Crit. Rev. Immunol. 2012, 32, 23–63. [Google Scholar] [CrossRef] [PubMed]
- Bertazzo, A.; Ragazzi, E.; Visioli, F. Evolution of tryptophan and its foremost metabolites’ concentrations in milk and fermented dairy products. PharmaNutrition 2016, 4, 62–67. [Google Scholar] [CrossRef]
- Zingone, F.; Iovino, P.; Bucci, C.; Ciacci, C. Coeliac disease: No difference in milk and dairy products consumption in comparison with controls. BMJ Nutr. Prev. Health 2019, 2, 39–42. [Google Scholar] [CrossRef]
- Lamas, B.; Hernandez-Galan, L.; Galipeau, H.J.; Constante, M.; Clarizio, A.; Jury, J.; Breyner, N.M.; Caminero, A.; Rueda, G.; Hayes, C.L.; et al. Aryl hydrocarbon receptor ligand production by the gut microbiota is decreased in celiac disease leading to intestinal inflammation. Sci. Transl. Med. 2020, 12. [Google Scholar] [CrossRef]
- Ray, K. Connecting coeliac disease to the AhR pathway. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 6–6. [Google Scholar] [CrossRef]
- Wang, C.; Wang, F.; Wang, Y.; Fu, L. D-tryptophan triggered epithelial-mesenchymal transition by activating TGF-β signaling pathway. Food Sci. Hum. Wellness 2022, 11, 1215–1221. [Google Scholar] [CrossRef]
- Del Zotto, B.; Mumolo, G.; Pronio, A.M.; Montesani, C.; Tersigni, R.; Boirivant, M. TGF-beta1 production in inflammatory bowel disease: Differing production patterns in Crohn’s disease and ulcerative colitis. Clin. Exp. Immunol. 2003, 134, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Mao, X.; Sun, R.; Wang, Q.; Chen, D.; Yu, B.; He, J.; Yu, J.; Luo, J.; Luo, Y.; Yan, H.; et al. l-Isoleucine Administration Alleviates DSS-Induced Colitis by Regulating TLR4/MyD88/NF-κB Pathway in Rats. Front. Immunol. 2021, 12, 817583. [Google Scholar] [CrossRef] [PubMed]
- Mao, X.; Gu, C.; Ren, M.; Chen, D.; Yu, B.; He, J.; Yu, J.; Zheng, P.; Luo, J.; Luo, Y.; et al. l-Isoleucine Administration Alleviates Rotavirus Infection and Immune Response in the Weaned Piglet Model. Front. Immunol. 2018, 9, 1654. [Google Scholar] [CrossRef] [PubMed]
- Wichers, M.C.; Maes, M. The role of indoleamine 2,3-dioxygenase (IDO) in the pathophysiology of interferon-alpha-induced depression. J. Psychiatry Neurosci. Jpn. 2004, 29, 11–17. [Google Scholar] [PubMed]
- Meysam, Z.; Mina, A.; Ali Akbar Saboor, Y.; Sama, B.; Fariba, K.; Mohammad Hossein, H.; Mohammad Ali, S.; Niaz Mohammadzadeh, H. Does vitamin A supplementation affect GATA3 and IL-4 genes expression in TCD4+ cell culture? A double blind randomized clinical trial on MS patients. J. Nutr. Sci. Diet. 2018, 4, 8–14. [Google Scholar]
- Manavalan, J.S.; Hernandez, L.; Shah, J.G.; Konikkara, J.; Naiyer, A.J.; Lee, A.R.; Ciaccio, E.; Minaya, M.T.; Green, P.H.; Bhagat, G. Serum cytokine elevations in celiac disease: Association with disease presentation. Hum. Immunol. 2010, 71, 50–57. [Google Scholar] [CrossRef]
- Tye-Din, J.A.; Skodje, G.I.; Sarna, V.K.; Dzuris, J.L.; Russell, A.K.; Goel, G.; Wang, S.; Goldstein, K.E.; Williams, L.J.; Sollid, L.M.; et al. Cytokine release after gluten ingestion differentiates coeliac disease from self-reported gluten sensitivity. United Eur. Gastroenterol. J. 2020, 8, 108–118. [Google Scholar] [CrossRef]
- Tye-Din, J.A.; Daveson, A.J.M.; Ee, H.C.; Goel, G.; MacDougall, J.; Acaster, S.; Goldstein, K.E.; Dzuris, J.L.; Neff, K.M.; Truitt, K.E.; et al. Elevated serum interleukin-2 after gluten correlates with symptoms and is a potential diagnostic biomarker for coeliac disease. Aliment. Pharmacol. Ther. 2019, 50, 901–910. [Google Scholar] [CrossRef]
- Hamza, T.; Barnett, J.B.; Li, B. Interleukin 12 a key immunoregulatory cytokine in infection applications. Int. J. Mol. Sci. 2010, 11, 789–806. [Google Scholar] [CrossRef]
- Balasubbramanian, D.; Goodlett, B.L.; Mitchell, B.M. Is IL-12 pro-inflammatory or anti-inflammatory? Depends on the blood pressure. Cardiovasc. Res. 2019, 115, 998–999. [Google Scholar] [CrossRef] [PubMed]
- Björck, S.; Lindehammer, S.R.; Fex, M.; Agardh, D. Serum cytokine pattern in young children with screening detected coeliac disease. Clin. Exp. Immunol. 2015, 179, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Hisamatsu, T.; Erben, U.; Kühl, A.A. The Role of T-Cell Subsets in Chronic Inflammation in Celiac Disease and Inflammatory Bowel Disease Patients: More Common Mechanisms or More Differences? Inflamm Intest. Dis. 2016, 1, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Georgy, J.; Arlt, Y.; Moll, J.; Ouzin, M.; Weitz, H.; Gremer, L.; Willbold, D.; Grötzinger, J.; Thives-Kurenbach, F.; Scheller, J.; et al. Tryptophan (W) at position 37 of murine IL-12/IL-23 p40 is mandatory for binding to IL-12Rβ1 and subsequent signal transduction. J. Biol. Chem. 2021, 297, 101295. [Google Scholar] [CrossRef] [PubMed]
- Imler, J.L.; Miyajima, A.; Zurawski, G. Identification of three adjacent amino acids of interleukin-2 receptor beta chain which control the affinity and the specificity of the interaction with interleukin-2. EMBO J. 1992, 11, 2047–2053. [Google Scholar] [CrossRef]
Figure 1.
(A) GI and (B) non-GI symptoms of studied CD patients.
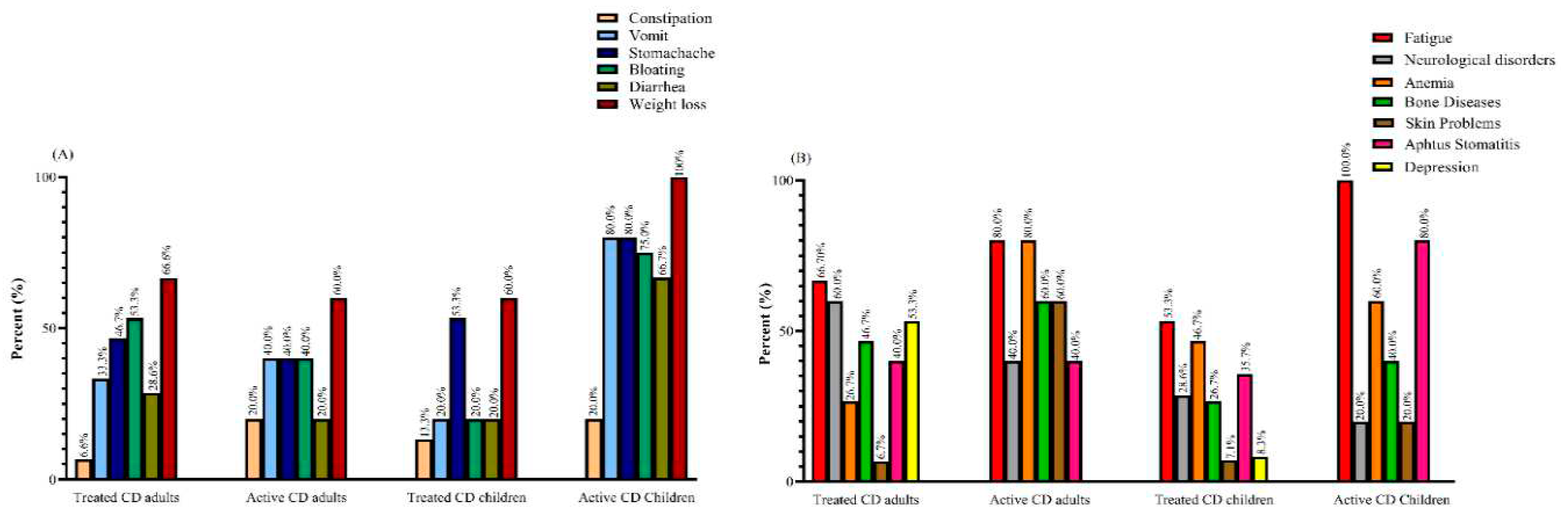
Figure 2.
Plasma vitamin A levels in patients and controls.
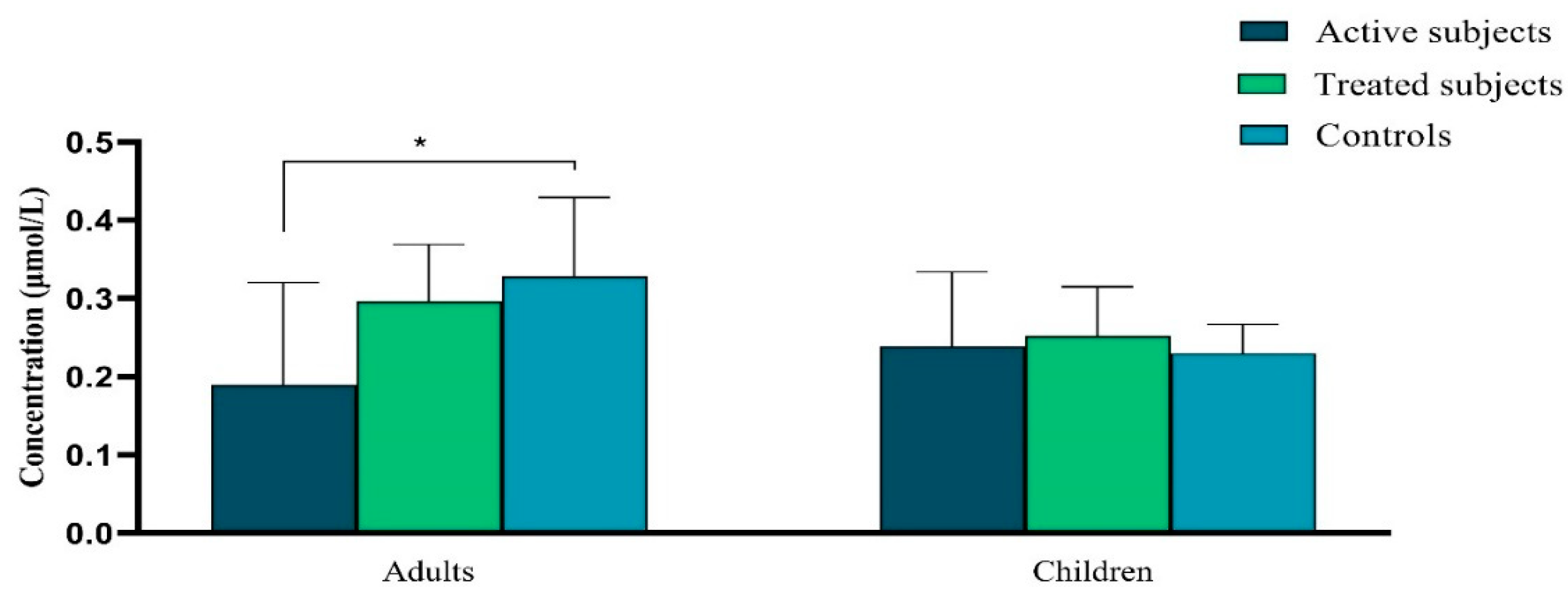
Figure 3.
Amino acids profile of (A) adults and (B) pediatric subjects.
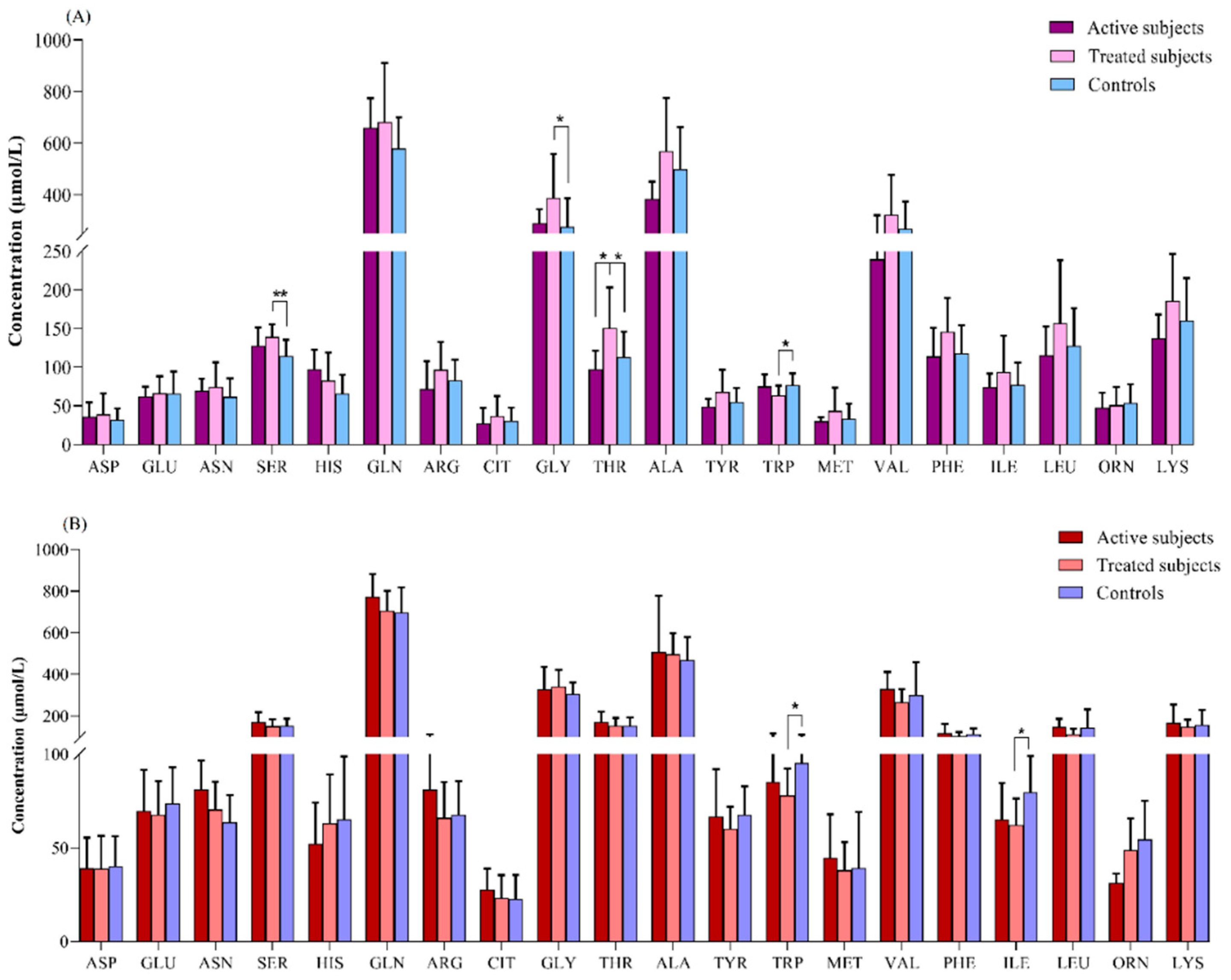
Figure 4.
Analysis of (A) IL-2, (B) IL-12, (C) IL-4, (D) IL-10 and TGF-β relative expression levels in studied groups using real-time PCR assay.
Figure 4.
Analysis of (A) IL-2, (B) IL-12, (C) IL-4, (D) IL-10 and TGF-β relative expression levels in studied groups using real-time PCR assay.
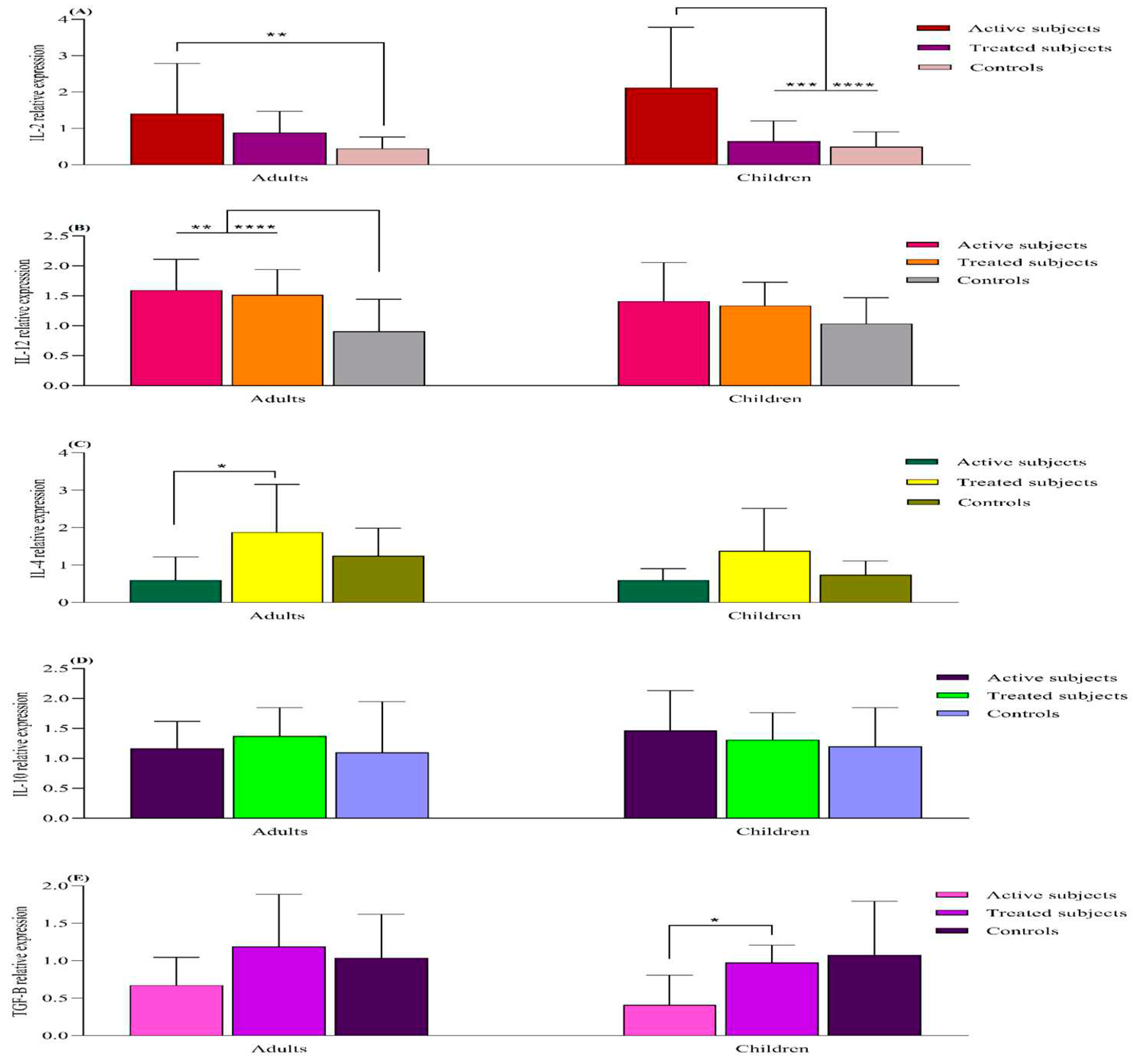
Figure 5.
Food consumption pattern of studied participants.
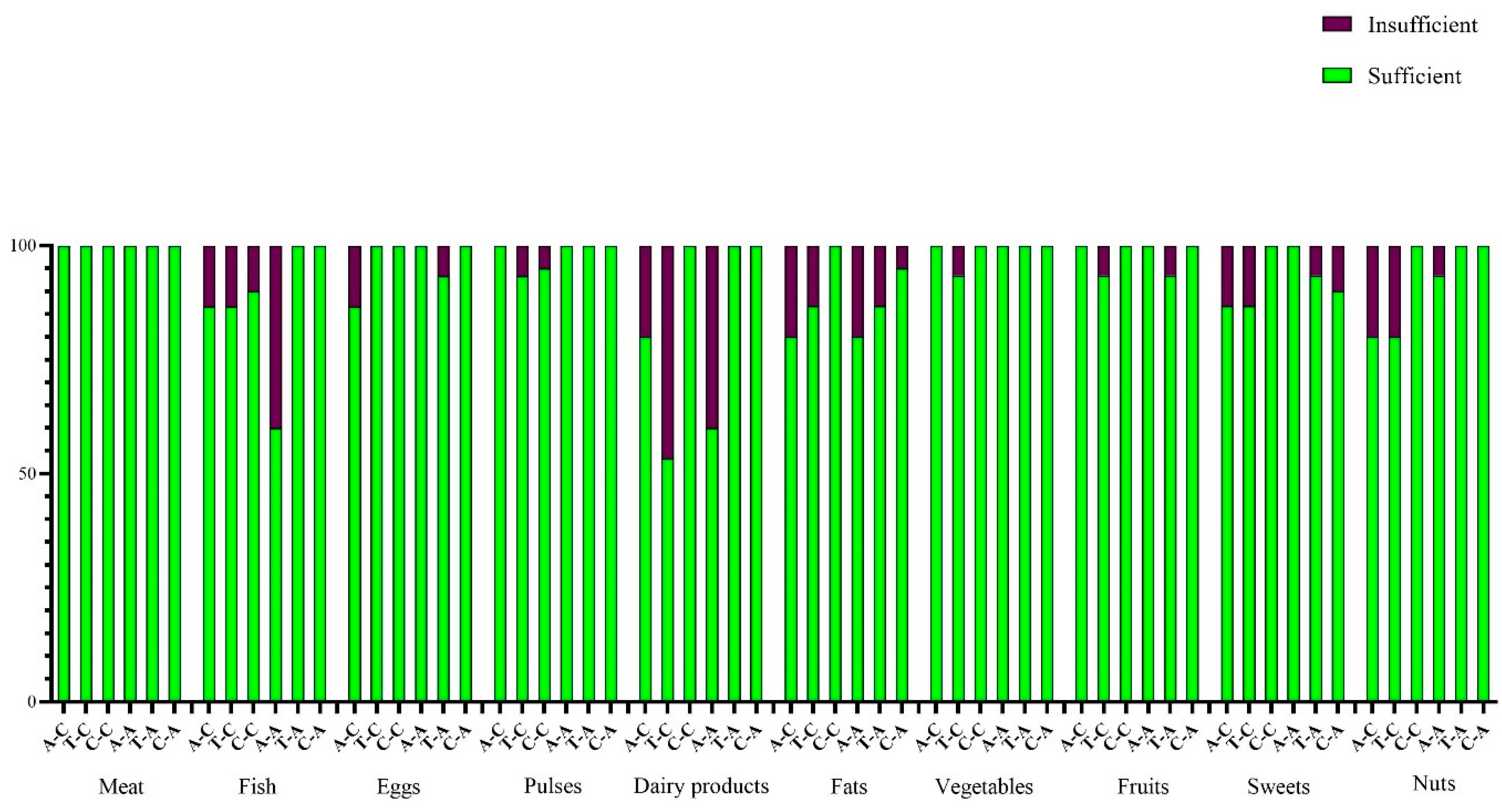
Figure 6.
a Heat map of correlations between (A) vitamin A and amino acid levels and genes expression in adults, (B) vitamin A and amino acid levels and genes expression in pediatric patients. *p < 0.05, **p < 0.01.
Figure 6.
a Heat map of correlations between (A) vitamin A and amino acid levels and genes expression in adults, (B) vitamin A and amino acid levels and genes expression in pediatric patients. *p < 0.05, **p < 0.01.
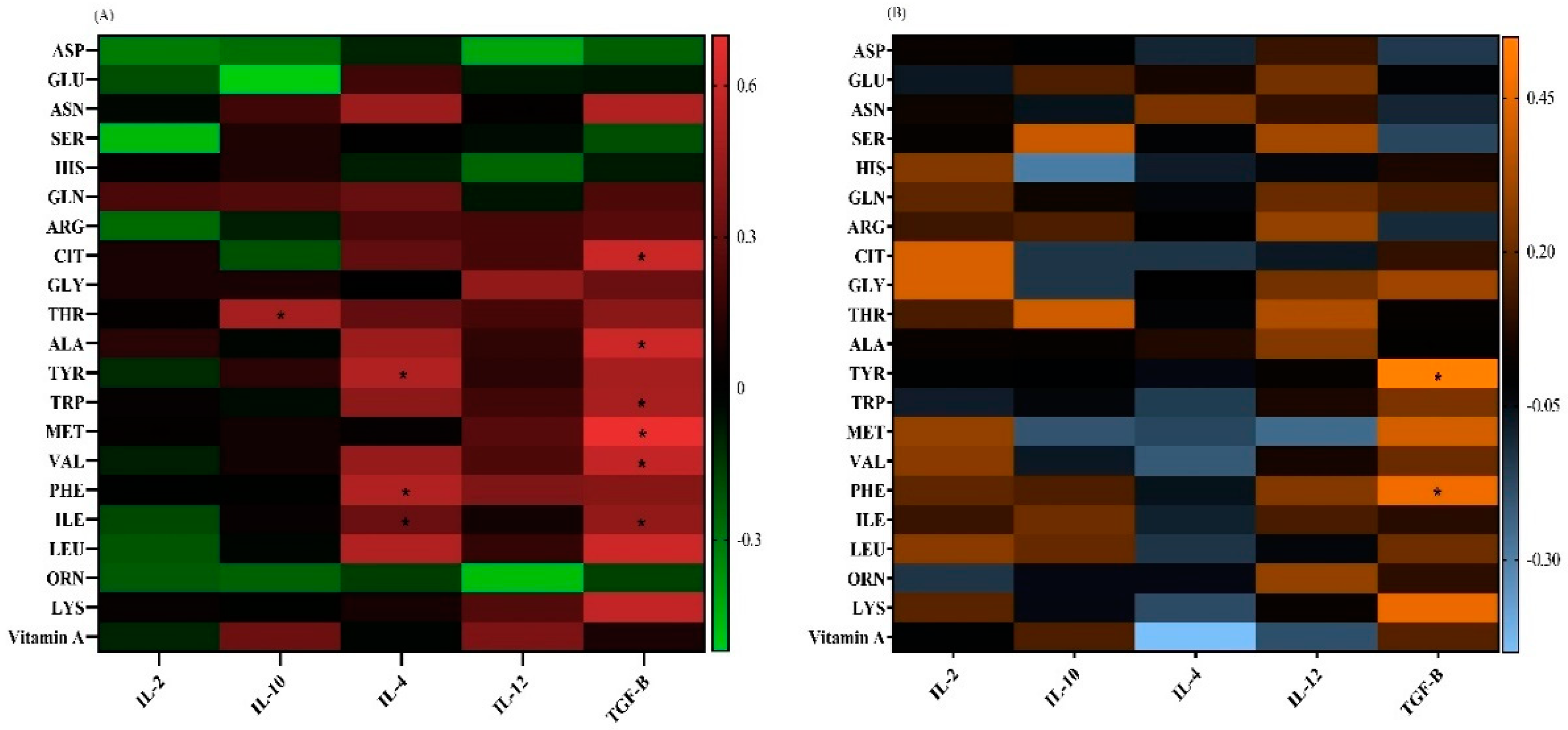

Table 1.
Demographic characteristics of study groups.
| Adults | ||||||
|---|---|---|---|---|---|---|
|
Variables Groups |
Number | Gender | Age | BMI | ||
| Female | Male | |||||
| Controls | 20 | 10 (50%) | 10 (50%) | 35.25 ± 10.7 | 22.06 ± 8.33 | |
| Treated | 15 | 8 (53.3%) | 7 (46.7%) | 39.0 ± 8.87 | 26.28 ± 4.57 | |
| Active | 15 | 10 (66.6%) | 5 (33.3%) | 31.8 ± 12.71 | 21.68 ± 4.54 | |
| P-value | 0.49 | 0.34 | 0.12 | |||
| Children | ||||||
|
Variables Groups |
Number | Gender | Age | BMI | ||
| Girl | Boy | |||||
| controls | 20 | 10 (50%) | 10 (50%) | 10.9±3.97 | 19.69±4.45 | |
| Treated | 15 | 8 (53.3%) | 7 (46.7%) | 10.60±2.92 | 133.77±12.63 | |
| Active | 15 | 9 (60%) | 6 (40%) | 9.20±3.27 | 14.75±3.81 | |
| P-value | 0.92 | 0.63 | 0.16 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



