Submitted:
17 September 2023
Posted:
18 September 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The best form of prevention against human infection through bacteria, viruses and other parasites is ozone disinfection of wastewater and drinking water as a highly effective, well-known method. As a therapeutic measure, various preclinical studies showed promising results, which are being revisited and reconsidered in times of pandemics and led to interesting results in recent clinical trials and reports, as presented by the example of protective measures against covid-19 in particularly vulnerable clinical personnel. In patients with rheumatoid arthritis, repeated ozone treatments have led to new findings in the "immunomodulation" through ozone. The more effective immune response is discussed as the response of innate immune memory and opens interesting aspects for complementary treatment of autoimmune diseases.
Keywords:
Covid-19
; innate immune memory
; rheumatoid arthritis
; autoimmune disease
; redox bioregulation
1. Introduction
Times of pandemics are times when health maintenance, protection against infections, prevention in general and protective measures come to the fore. When at the turn of the 19th/20th century sewage and drinking water was recognized as one of the major epidemic causes of typhoid, cholera etc. and appropriate water treatment plants were built, this nightmare soon became a thing of the past, unfortunately not everywhere in the world even up to the present. Ozone as one of the most potent disinfectants is installed, to make use of its high oxidation potential for the degradation of toxic substances; its germicidal, bactericidal and antiviral properties guarantee a perfect drinking water, the most important basic food [1].
1.1. Prevention through room and surface disinfection.
To protect against germ transmission in clinics and hospitals, various surface and room disinfectants are used that must be registered and listed as disinfectants following both the national and international regulations. As a gas, ozone occupies a special position: Despite its pronounced bactericidal and virus-inactivating character, it requires a high humidity of > 80% and is therefore, and due to its high redox potential, not very compatible with materials. In addition, its toxicity to the respiratory tract requires significant measures to completely decompose the ozone before rooms can be used again [2].
In contrast, in wastewater, drinking water and industrial water, it is superior to all known disinfectants, depending on concentration and contact time -ct concept-, well documented for many decades [3].
Ozonated water can be used in the medical field for surface and equipment disinfection, of particular benefit in dentistry, since viruses such as Corona are also inactivated [4,5,6,7,8].
The underlying molecular mechanism is mainly based on a direct contact with the germs; at pH values >7 the radical mechanism dominates [9].
Of interest in medicine, this mechanism is employed in the local treatment of infected wounds for effective germ elimination and wound cleansing as a precondition for wound healing, though not in the systemic application and action of ozone where we discuss an indirect mechanism via ozone peroxides (Figure 1); this is described in detail in [10].
1.2. From empirical findings to science.
In medical applications, ozone occupies a subordinate place in prevention although, in many private practices and clinics the systemic use of ozone has shown remarkable success, especially in the secondary prevention of chronic diseases. In the 1990s, Schulz [11] transferred these reports of experience into an animal model of lethal peritonitis and used preventive intraperitoneal ozone injections to increase the survival rate of animals up to 100%, depending on their combination with antibiotics. Systematic studies using animal and cell models were in an initial phase, and the activation of cell metabolism, immunomodulation, and redox regulation were recognized as the underlying biochemical and pharmacological mechanisms. Prevention of liver and kidney intoxication by chemotherapeutic agents or radiation exposure through ozone oxidative preconditioning are well known and have been discussed earlier [12]. After two introductory historical preclinical studies providing us with a basic understanding, we here focus on very new aspects such as protection against infections including Covid-19 and secondary prevention in rheumatoid arthritis by claiming the involvement of the immune memory. Preclinical and clinical trials on the preventive effect of ozone are listed in Tables I and II, without claim to completeness.
2. Results
2.1. Preclinical trials in animal and cell models
2.1.1. Growth inhibition of plasmodium falciparum in ozone-pretreated Red Blood Cells.
Plasmodium falciparum, the single-celled parasite inducing malaria tropica, grows in RBC´s after passing most of its life cycle up to the RBC´s bursting and consequent releases the parasites into the blood plasma. The sensitivity of plasmodia to reactive oxygen species is well-known and is the basis of various drugs, such as artemisinin, an endoperoxide from the group of sesquiterpenes [13], Thus, the idea of using ozone as an oxidant in prevention and / or therapy as a drug was obvious. The therapeutic method failed completely, at least with a single ozone treatment of infected RBC´s whereas one single pretreatment with ozone prior to infection inhibited plasmodium growth by a factor of up to seven [14].
Mechanism of action
At the high concentration of 80 g/ml, ozone appears to dramatically reduce the antioxidative capacity of RBC´s by disturbing the GSH GSSG balance and shifting it to the right (GSH reduced form of glutathione, GSSG being the oxidated form). Red Blood Cells are constantly exposed to reactive oxygen compounds and therefore have a high level (90%) of the most important cellular antioxidant GSH; this is crucial for survival and growth of plasmodia. Similar effects can be seen in patients with a G-6PDH (glucose-6-phosphate dehydrogenase) deficiency, the enzyme that initiates the pentose phosphate pathway with its antioxidant ability: these patients are mostly malaria resistant, see Figure 2.
Unlike the low-dose and low concentration concept (10-40 g/ml) in systemic ozone treatment with its regulatory effects, red blood cells have no nucleus and cannot start regulation for a repair mechanism.
2.1.2. Protection against lethal peritonitis by oxidative preconditioning with ozone in animal models.
With our knowledge of the immunomodulating effect of medically used ozone (Bocci xx) and the idea of establishing protection against bacterial infections in both humans and animals through preventive ozone administration [11,16]. Schulz determined the survival rate in a suitable animal model (rats) of lethal peritonitis as a function of intraperitoneally administered ozone concentrations (10 to 100 μg/mL) and dose. Here, lethality was remarkably reduced from 95% (control) to 35%, and interestingly at the lowest concentration of 10 μg/mL (20 mL) corresponding to a dose of 200 μg, administered 1x daily for 5 consecutive days. Synergistic effects with different antibiotics in the follow-up studies increased the survival rate to 93% and 100% in the case of Tazobac/Piperacillin TZP, accompanied by a reduced amount of IL-1 and TNF- mRNA in spleen and liver [17,18]. These early preclinical studies on prevention provided us with important guidance on dosing and establishing the low-dose ozone concept (Figure 3).
Redox bioregulation through oxidative preconditioning by ozone as the basic mechanism of ozone in prevention. In addition to immunomodulation, oxidative protection mechanisms by upregulation of antioxidative enzymes, such as GSHox, GSHred, SOD, CAT and others, dominate in prevention. Healthy cells with a strong antioxidant capacity are largely protected against reactive oxygen species and free radicals generated by infection, inflammation, antibiotics or other drugs. In the late 1990´s León started a broad-based research project on ozone-oxidative preconditioning, that rapidly expanded to attain worldwide acceptance: protection through, principally against liver and kidney intoxication through xenobiotics, remedies, chemotherapy or reperfusion damage in surgery.
A variety of animal models and a few clinical trials with excellent, convincing results form the basis for our molecular and pharmacological understanding of the use of ozone in preventive medicine. By its very nature, it is difficult to convince healthy people to take preventive measures and to set up appropriate studies although a current awareness, interest and demand for prevention in clinics and hospitals is increasing.
Clinical studies and reports involving elderly patients [19] in the prevention of Covid-19, the Corona induced disease, show very promising outcomes. These are listed in Table II. We will now discuss some of the most interesting results.
2.2. Clinical trials and reports
2.2.1. Prevention from Covid-19
The best remedy for viral diseases is prevention, and the question is: can we contribute with low-dose, systemically administered ozone in the form of major auto-hemotherapy MAH or rectal insufflation RI and consequently protect particularly vulnerable individuals against Covid-19 ?
Physicians and clinical staff caring for Covid-19 patients find themselves in such a difficult situation and are more likely to be open to preventive measures. We therefore focus on clinical reports involving this group.
A. A clinical trial conducted at the Indonesian Police Central Bhayangkara Hospital and the Department of Forensic Medicine, Jakarta University, presented at the 26th Ozone World Congress of the International Ozone Association IOA in Milan, Italy, July 2023.
Procedure. 150 health care professionals, including 25 physicians and 125 nurses (exclusion G-6PDH glucose-6-phosphate dehydrogenase deficiency) received systemic ozone treatments in the form of MAH, RI or vaginal insufflation on five consecutive days before coming into contact with the Covid-19 patients in the hospital with a high risk of infection via the corona virus. Concentration and dose were chosen according to the guidelines [20].
Results. None of the 150 health care professionals were infected by corona virus, all of them remained PCR negative. Preventive ozone treatment was able to stabilize the immune status of the involved persons.
At the same time there was a nursing emergency in other hospitals due to the high sickness rate, and care of the patients collapsed [21].
B. A retrospective study at the Marmara University together with the health sciences University Sisli, Istanbul reports the very same results: Could ozone therapy be used to prevent Covid-19?
Procedure. 71 persons who completed at least 10 sessions of MAH in accordance with the low-dose ozone concept within six months participated in the retrospective study. 45% of them were medical professionals, all of them had contacts and travel history. 50,7 % were aged over of 50 years and 52 % had comorbidities: consequently their risk of developing covid-19 was higher than that of the normal population in Turkey [22].
Two of the included persons were infected, acquiring covid-19 without severe symptoms corresponding to 2,8 % of the participants.
C. The effect of systemic ozone application on the activity of B-lymphocytes and the level of antibodies in corona vaccinated persons.
A retrospective clinical trial (Goji Medical Group Ozone Therapy Institute, Miami Lakes, FL. USA) including 109 persons, mostly triple vaccinated, 57 of them receiving systemic ozone application as MAH (60%) or rectal insufflation (40%). 52 persons not treated with ozone served as controls.

Table 1.
Clinical trial in Covid-19 antibody production. Patients and treatment procedure.
| Control group, n=52 | Ozone group, n=57 |
|---|---|
| 3x vaccinated: n=33 (63,5%); 2x vaccinated: n=19 (36,5%) |
3x vaccinated: n=31 (54,4%); 2x vaccinated: n=26 (45,6%) |
| female n=33, male n=19 age 20 to 55 |
female n=24, male n=33 age 20 to 55 |
| MAH: 1x per week, 8 treatments RI: 2x per week during 2 weeks, then 1x per week; 15-16 treatments |
MAH: Major autohemotherapy, RI: Rectal insufflation.
No person in the ozone group was PCR positive compared to 48 persons in the controls who developed weak or moderate Covid (omicron).
Activated B lymphocytes (CD23) were elevated in the ozone group, probably via ozone-activated helper cells. IgG values ranged between 120-170 AU/mL compared with controls having 40 to 50 AU/mL (values below 10 AU/mL are considered as being a weak immune response [23]
Other trials are reported using intramuscularly administered minor autohemotherapy or ozonized saline; however, we here only refer to reports of pilot studies applying ozone systemically and applying the standardized methods of MAH and RI (Tables I-II).
Of course, more data need to be collected, relevant parameters on redox regulation, immune status and oxidative stress need to be measured before these promising results can be translated into a clinical concept. However, many reports from daily practice in dealing with the pandemic are confirmed.
Mechanism of action of medical ozone in preventive medicine. From the numerous preclinical studies on protection against hepatic, renal or pancreatic intoxication and others, as well as from clinical studies e.g., rheumatoid arthritis (methotrexate MTX intoxication) or aging processes, the biochemical mechanism of action and the pharmacological effect of systemic ozone in preventive medicine have been elaborated and confirmed.
For prevention, the following applies: Ozone with its polar molecule structure reacts preferably with the isolated double bonds of fatty acids as they are situated in large amounts in the cell membranes, splitting them and forming hydroxy hydro peroxides “ozone peroxides”. These small peroxides with their terminal -C(OH)OOH group are less active than ozone itself but still oxidants being immediately reduced by glutathione GSH via ionic reaction mechanisms, here initiate redox bioregulation.
Long-chain peroxides with a central peroxide group as initiators for radical chain reactions are responsible for permanent oxidative stress; as long-lived peroxides they form suitable parameters for the determination of oxidative stress in redox medicine
Here the “ozone peroxide” behaves as a second messenger and regulatory molecule transducing its information via the GSH reaction to nuclear factors, mainly NFkB responsible for immunomodulation, among other factors, and Nrf2, which is responsible for regulation of antioxidants. The first step seems to be an inflammatory response to the low and specific oxidative stress of “ozone peroxide” via NfkB and -in a second- step the anti-inflammatory response via Nrf2 regulating the enzymatic antioxidant system [24] e. g. GSHox and GSHred which are needed to recover the GSH balance.
Redox bioregulation will be blocked when using high peroxide concentrations and dosages; this is the situation in patients under high oxidative stress in chronic inflammatory diseases [10].
On this basis the low-dose ozone concept was developed; it is suitable for prevention by modulating the immune response and protecting cells from oxidative stress and free radicals through a strong antioxidant system.
D. Oxidative preconditioning in rheumatoid arthritis patients with a second cycle of ozone treatment. Procedure: Rheumatoid arthritis RA already has a history in ozone treatment. In the 1980´s we saw a complete failure; the ozone concentrations and amounts (70-80 g/mL, volume of 200 mL corresponding to 16,000 g O3 per 200 ml of blood in the form of MAH [25] were too high and therefor contributed to the oxidative stress of the chronic inflammatory process. On the basis of oxidative preconditioning in redox medicine the biochemical and pharmacological mechanisms were elaborated and our understanding of ozone as a redox bioregulatory molecule improved to a far better extent. The O3 concentration and amounts were drastically reduced in order to regulate oxidative stress instead of increasing it: consequently, RA became one of the characteristic indications for ozone application [10,20].
Once again and renewed, the treatment of rheumatoid arthritis changes and deepens our understanding of the ozone mechanism of action: a controlled clinical trial including 20 RA patients receiving rectal ozone insufflation in 2 cycles in combination with a basic treatment (MTX (methotrexate), Ibuprofen, folic acid) and an intermediate period of 3 months [26]. The protection of liver intoxication by MTX in RA patients was reported earlier [27].
Reference substances. Redox biomarkers -antioxidants being the protective ones and oxidative stress as injury parameters- are suitable parameters to follow the progression of the disease; the following are used to show a secondary prevention in a clinical trial on rheumatoid arthritis in a second treatment cycle where an innate immune memory by preventive ozone treatment is discussed, Table 2.
The second cycle with rectal ozone insufflation following the low-dose ozone concept and applying the same therapeutic plan as in the first treatment cycle: 1st week: 25 g/mL, 100 mL; 2nd week: 30 g/mL, 150 mL; 3rd week: 35 g/mL, 200 mL; 4th week: 40 g/mL, 200 mL resulted in a more effective therapeutic response compared to the end of the first cycle (interval of 3 months between end of 1st, beginning of 2nd cycle). Six of seven biomarkers returned to normal, a number of them are displayed in Figure 4. Injury biomarkers TH and MDA reached normal values at the end of the 2nd cycle, a remarkable difference to the end of the 1st one. GSH as protection marker increased when compared with the end of the 1st cycle in 15/20 patients, 4 patients showed a slight decrease, and in one patient no change was measured.
Figure 4.
Immune memory in RA (rheumatoid arthritis) patients in a 2nd cycle of systemic ozone treatment with a 3 months interval. Rectal insufflation in both cycles, treatment schedule (ozone concentration, volume): 1st week: 25 g/mL, 100 mL; 2nd week: 30 g/mL, 150 mL; 3rd week: 35 g/mL, 200 mL; 4th week: 40 g/mL, 200 mL. a. Auto antibodies measured as anti-CCP (Anti-Cyclic Citrullinate Peptides), show a remarkable decrease at the end of the second treatment cycle corresponding to the improvement of b. the clinical parameters. c. Redox protection markers GSH (reduced glutathione) and SOD (superoxide dismutase) reach normal values after the second treatment cycle (GSH normal range: 790-1100 g/mL; SOD normal range: (50-110) x10-1 U/L) d. Oxidative stress measured as MDA (malondialdehyde) and TH (total hydroperoxides) decrease according to the increase of antioxidant capacity, both are even in the reference range after the 2nd cycle (TH: 8-15 M; MDA: (1-2 ) x10-1 M). Obviously, the repeated treatment is recognized by memory cells [26].
Figure 4.
Immune memory in RA (rheumatoid arthritis) patients in a 2nd cycle of systemic ozone treatment with a 3 months interval. Rectal insufflation in both cycles, treatment schedule (ozone concentration, volume): 1st week: 25 g/mL, 100 mL; 2nd week: 30 g/mL, 150 mL; 3rd week: 35 g/mL, 200 mL; 4th week: 40 g/mL, 200 mL. a. Auto antibodies measured as anti-CCP (Anti-Cyclic Citrullinate Peptides), show a remarkable decrease at the end of the second treatment cycle corresponding to the improvement of b. the clinical parameters. c. Redox protection markers GSH (reduced glutathione) and SOD (superoxide dismutase) reach normal values after the second treatment cycle (GSH normal range: 790-1100 g/mL; SOD normal range: (50-110) x10-1 U/L) d. Oxidative stress measured as MDA (malondialdehyde) and TH (total hydroperoxides) decrease according to the increase of antioxidant capacity, both are even in the reference range after the 2nd cycle (TH: 8-15 M; MDA: (1-2 ) x10-1 M). Obviously, the repeated treatment is recognized by memory cells [26].
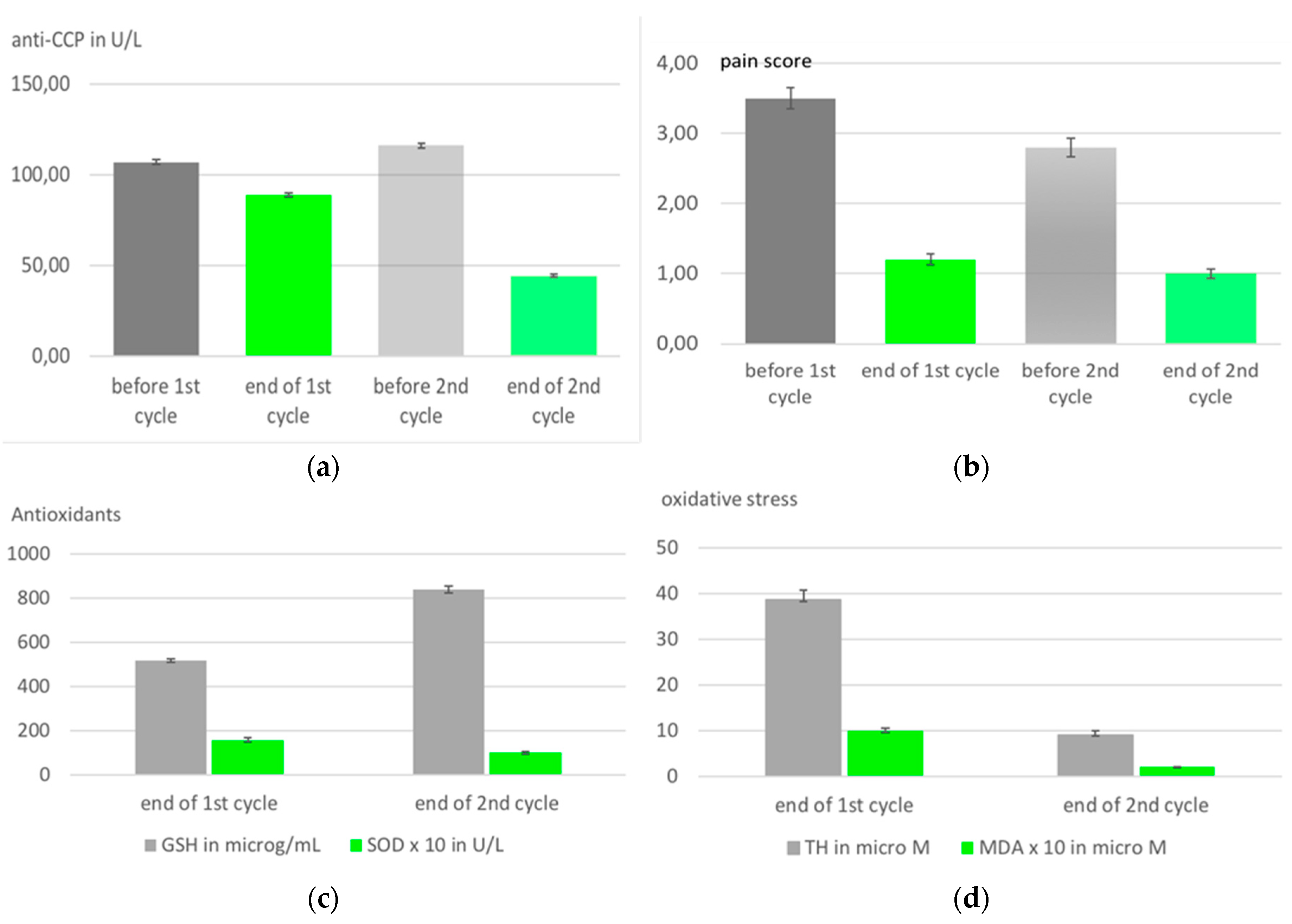
Involvement of the innate immune system. Compared with the first treatment cycle, there was a further improvement of almost all parameters at the end of the 2nd treatment cycle, which means a further enhancement of the oxidative protection mechanisms and is understandable through a possible involvement of the innate immune system. Obviously, the innate memory is stimulated by the 2nd ozone treatment after the 3-months interval, strengthening the protection of bone and cartilage against inflammatory processes as we know them from autoimmune diseases such as rheumatoid arthritis.
Auto-antibodies CCP (Anti-Cyclic Citrullinate Peptides), which specifically correlate with RA disease progression, support this assumption: Again, we find the same overall picture, namely, compared to the first treatment series, a significant decrease after the 2nd cycle, accompanied by a substantial improvement in the clinical course. This completely new aspect of the low-dose ozone concept in secondary prevention will be further pursued and should be consolidated by including other autoimmune diseases [26].
3. Discussion
While primary prevention is usually reserved for private clinics and the demand is here increasing, especially from elderly patients and those with pre-existing conditions, secondary prevention for chronic inflammatory diseases and autoimmune diseases should also be transferred to hospitals in the form of a complementary treatment concept. To strengthen the immune system and enhance the protection mechanism of the cells by means of redox bioregulation will help to protect patients from bacteria and diseases of viral origin. The specific and relevant redox parameter will have to be measured in further trials.
The well known underlying biochemical mechanisms are now being expanded through a deeper understanding of a number of processes in the immune system: a repeated treatment cycle in RA patients leads to a decrease in autoantibodies indicating the formation of memory cells in the preceding treatment cycle. After the 3-months interval in ozone/MTX treatment the second exposure to ozone apparently assumes the function of stimulating the innate immune system and bringing the memory cells onto the scene, the oxidative protection mechanisms are further strengthened and the subsequent damage is reduced. This knowledge may well open new aspects in the treatment of autoimmune diseases.
4. Material and methods
In recent decades, cellular and animal models have been developed and used to understand empirical results in the application of ozone, to clarify the underlying mechanisms and to establish guidelines, and the idea of prevention has emerged. Although there are several thousand scientific publications on the use of ozone in biology and medicine, prevention is rarely found in the corresponding medical databases. We therefore searched the extensive, relevant literature that we were aware of to meet the increasing demand for preventive measures in the post-pandemic period, presently subject to heated discussions. Tables I and II provide a good overview, and a few of them are discussed here, especially those that open and have opened new aspects.
Table I.
Prevention from general oxidative stress. Literature survey.
| Type of study | Results | Application route | References |
|---|---|---|---|
| Medical ozone promotes Nrf2 phosphorylation reducing oxidative stress and proinflammatory cytokines in multiple sclerosis patients | Secondary prevention GSH increase. |
Rectal insufflation 20mg/L | Livan Delgado-Roche, Mario Riera-Romo, Fernando Mesta, Yanet Hernández-Matos, Juan M. Barrios, Gregorio Martínez-Sánchez, Said M. Al-Dalaien. European Journal of Pharmacology, 2017, 811, 148-154 |
| Ozone influence on the RBC metabolism” (german Einfluss auf den Erythrozyten-Stoffwechsel). Clinical trial . | Metabolic activation in RBC´s: 2,3-DPG and ATP increase. See text. | Rectal insufflation | Viebahn-Hänsler, R. Washüttl. J. Wasser, G. Gutzen, U.1995 [15] |
| Medical ozone arrests oxidative damage progression and regulates vasoactive mediator levels in older patients (60-70 years) with oxidative etiology diseases. Controlled clinical study. | Positive influence on aging process. See text. | Rectal insufflation | León Fernández, O. S., Takon Oru, G., Viebahn-Hänsler, R., López Cabreja, G., Serrano Espinosa, I., García Fernández, E. 2022 [19] |
| Medical ozone increases methotrexate clinical response and improves cellular redox balance in patients with rheumatoid arthritis. Clinical trial. |
Statistical significant reduction of liver toxicity in patients with rheumatoid arthritis during MTX treatment. See text. | 10 rectal insufflations in 10 days | León, O.S., Viebahn-Haensler, R., López, C.G., Serrano, E.I., Hernández, M.Y., Delgado, R.L., Tamargo, S.B., Takon, O.G., Polo, V.J.C., 2016. [27] |
| Modulation of Oxidative Stress by Ozone Therapy in the Prevention and Treatment of Chemotherapy-Induced Toxicity: Review and Prospects. |
Prevention from toxicity, mainly in animal models | systemic applications | Bernardino Clavo, Francisco Rodríguez-Esparragó , Delvys Rodríguez-Abreu,Gregorio Martínez-Sánchez, Pedro Llontop, David Aguiar-Bujanda,Leandro Fernández-Pérez and Norberto Santana-Rodríguez Antioxidants 2019, 8, 588; doi:10.3390/antiox8120588 |
Table II.
Literature Survey.
| Type of study | Results | Application route | References |
|---|---|---|---|
| Ozone Therapy for Prevention and Treatment of COVID-19. Review. | 4 publications in prevention. | Different forms of application. | Gregorio Martínez-Sánchez1Journal of Exploratory Research in Pharmacology, April 2022. DOI: 10.14218/JERP.2022.00015 |
| Intravenous ozonized saline therapy as prophylaxis for healthcare workers (HCWs) in a dedicated COVID-19 hospital in India. A retrospective study | Less infections in the ozone group (4.6%) than in the control (14.03%). N=64 (235). | Ozonized saline. | A. Sharma, M. Shah, H. Sane, N. Gokulchandran, A. Paranjape, P. Khubchandani, J. Captain, S. Shirke, P. Kulkarni. European Review for Medical and Pharmacological Sciences, 2021; 25, 3632-3639 |
| Immunity Prophylaxis With Ozone Therapy Review Report. | 2.19 % incidence rate (n=320). | Minor autohemotherapy. | Dr. Mili Shah, Jignasha Captain and Gayatri Ganu. ejbps, 2020, 7, 86-88. |
| Could the minor autohemotherapy be a complementary therapy for healthcare professionals to prevent COVID-19 infection? | (n=73) No infection or positive test. |
Minor autohemotherapy. | Aydan Orscelik, Burak Karaaslan, Betul Agiragac, Ilker Solmaz, Murat Parpucu. Ann Med Res 2021, 28, 1863-9 DOI:10.5455/annalsmedres.2020.11.1133 |
| Could ozone therapy be used to prevent COVID-19? Clinical Trial. | 2 of 71 persons were tested positive.Retrospective, no control. 45 % medical professionals. See text. | Major autohemotherapy 10 treatments. | Kardelen Gencer-Atalay1 , Tulay Sahin-Marmara Med J 2022;35(2): 196-201. http://doi.org/10.5472/marumj.1121363. [22] |
| COVID-19 profilaxis with ozone therapy | n=9, good effect but no protection from further infection. | Rectal insufflation. | Falzoni, W.; Senvaitis, M. I.; Iwasa, S. Acupuncture and Electro-TherapeuticsResearch,2021,46,3 5-36,. |
| Comparative analysis of 2 groups of people according to age and sex, vaccinated triple versus covid-19, were subjected to quantitative analysis of antibodies and B lymphocytes after ozone therapy. Clinical trial. | See text. | Major autohemotherapy . |
Medina, José German, Journal of Ozone Therapy, 2022. 6, 11-12. [23] |
| The Role of Ozone Therapy as Adjuvant in the Management of Covid-19 in Indonesia. Clinical trial. | See text. | Major autohemotherapy, Rectal insufflation, vaginal insufflation. | Dian Chaijadi, Asep Hendradiana, Peter Djoko Tjahjono, Endang Kusumaningsih, Hariyanto, Carles Siagian, Djaja Surya Atmadja, Renate Viebahn-Hänsler. Indonesian Police Central Hospital and Faculty of Medicine, Indonesia University, Jakarta, proceedings Association IOA in Milan 2023. [21] |
5. Conclusion
Preventive measures should be integrated into health care systems. In addition to a variety of other measures, complementary medical measures certainly could have a key role to play here, as is already being provided by a number of clinics. Promising results are also now known from clinical trials in elderly patients [19] and patients suffering from rheumatoid arthritis. These must be confirmed, and the corresponding clinical and relevant redox markers have to be determined. The evidenced influence of the innate immune system should initiate a variety of clinical trials to investigate primary and secondary prevention.
References
- Schalekamp, M. Alles über Ozon, seine Vor- und Nachteile bei der Trinkwasserversorgung. (All about ozone, its advantages and disadvantages in drinking water supply)). OzoNachrichten 1983, 2, 74-82. http://ozongesellschaft.de/ozone-society.html.
- Alimohammadi, M.; Naderia, M. Effectiveness of Ozone Gas on Airborne Virus Inactivation in Enclosed Spaces: A Review Study. Ozone Sci. Eng. 2021, 43, 21–31. [CrossRef]
- Loeb. B. Ozone: Sci. & Engineering. Thirty Years of Progress. Ozone Sci. Eng. 2009, 31, 379–392. [CrossRef]
- Martins, R. B.; Castro, I. A.; Pontelli, M.; Souza, J.P.; Lima, T.M.; Rezende Melo, R.S.; Zen Siqueira, J. P.; Caetano, M.H.; Arruda, E.; Gottardo de Almeida. M.T. SARS-CoV-2 Inactivation by Ozonated Water: A Preliminary Alternative for Environmental Disinfection. Ozone Sci. Eng. 2021, 43, 108–111. [CrossRef]
- Inagaki, H. Akatsuki, S.; Sudaryatma, P.E.; Sugiyama, H.; Okabayashi, T.; Fujimoto, S. Rapid Inactivation of SARS-CoV-2 with Ozonated Water. Ozone Sci. Eng. 2021, 43, 208–212. [CrossRef]
- Tizaoui, C. Ozone: A Potential Oxidant for COVID-19 Virus (SARS-CoV-2)Ozone Sci. Eng 2020, 42, 378–385. [CrossRef]
- Hudson, J.B.; Sharma, M.; Vimalanathan, S. Development of a Practical Method for Using Ozone Gas as a Virus Decontaminating Agent Ozone Sci. Eng. 2009 31, 216–223. [CrossRef]
- Morrison, C.; Atkinson, A.; Zamyadi, A.; Kibuye, F.; McKie, M.; Hogard, S.; Mollica, P.; Jasim, S.; Wert, E.C. Critical Review and Research Needs of Ozone Applications Related to Virus Inactivation: Potential Implications for SARS-CoV-2 Ozone Sci. Eng. 2021, 43. 2–20. [CrossRef]
- Hoigne, L.; Bader.H. Ozonation of Water: Selectivity and Rate of Oxidation of Solutes. Ozone Sci. Eng. 1979, 1, 73-85. [CrossRef]
- Viebahn-Haensler, R.; León Fernández, O.S. Ozone In Medicine. The Low-Dose Ozone Concept and Its Basic Biochemical Mechanisms of Action In Chronic Inflammatory Diseases. Int. J. Mol. Sci. 2021, 22, 7890. [CrossRef]
- Schulz, S.; Rodriguez, Z.; Mutters, R.; Bette M.; Hoffmann, S. Die lethale postoperative Peritonitis im Tiermodell. Infektprophylaxe und Therapie durch Kombination von Ozon und Antibiotika. (The lethal post-operative peritonitis in an animal model. Infection prophylaxis and therapy by combination of ozone and antibiotics) in Viebahn-Hänsler, R.; Knoch, H.G. (Eds.) Ozon-Handbuch. Grundlagen-Prävention-Therapie (Ozone-Handbook, Basics-Prevention-Therapy) ecomed, Landsberg, 2000 (1995-2006).
- Viebahn-Haensler, R.; León Fernández, O.S. The low-dose ozone concept and its pharmacologyin prevention and convalescence. Babacan, C.A. (ed.). Ozone and Neural Therapy. 1st ed. Ankara: Türkiye Klinikleri; 2022, 19-29.
- Krishna, S. Bustamante, L. Haynes R.K. Staines, H.M. Artemisinins: their growing importance in medicine. Trends in Pharmacological Sciences 2008. 29, 520-527. [CrossRef]
- Lell, B.; Viebahn, R.; Kremsner, P. The activity of ozone against plasmodium falciparum. Ozone: Sci Eng 2001 23: 89-93. [CrossRef]
- Viebahn, R. Washüttl, J. Wasser, G. Gutzen, U. Influence of ozone on RBC metabolism“ referring a pilot study: „Rectal ozone insufflation in elderly“ in Viebahn-Haensler, R.; Knoch, H.G. (eds.) Ozone Handbook 1995. Ecomed, Landsberg 1995-2006.
- Schulz,S.; Rodriguez, Z.Z.; Mutters, R.; Menendez, S.; Bette, M. Repetitive pneumoperitoneum with ozonized oxygen as a preventive in lethal polymicrobial sepsis in rats. Eur Surg Res. 2003 Jan-Feb;35(1):26-34. [CrossRef]
- Zamora, Z.B.; Borrego, A.; Lopez, O. Y.; Delgado, R.; Gonzalez, R.; Menendez, S.; Hernandez, F.; Schulz, S. Effects of Ozone Oxidative Preconditioning on TNF- α Release and Antioxidant-Prooxidant Intracellular Balance in Mice During Endotoxic Shock. Mediators of Inflammation, 2005. 1–7. PII. S0962935104309257 http://mi.hindawi.com.
- Bette, M.; Nuessing, R.M.; Mutters,R.; Zamora, Z.B.; Menendez, S.; Schulz, S.; Efficiency of tazobactam/piperacillin in lethal peritonitis is enhanced after preconditioning of rats with O3/O2-pneumoperitoneum. SHOCK, 2006. 25, 23–29. [CrossRef]
- León Fernández, O. S.; Takon Oru, G.; Viebahn-Hänsler, R.; López Cabreja, L.; Serrano Espinosa, I.; García Fernández, E. Medical ozone arrests oxidative damage progression and regulates vasoactive mediator levels in older patients (60-70 years) with oxidative etiology diseases. Front. Physiol. 03 November 2022, 13. https://www.frontiersin.org/articles/10.3389/fphys.2022.1029805/full.
- Viebahn-Haensler, R.; León Fernández, O.S.; Fahmy, Z. Ozone in medicine: The low-dose ozone concept. Guidelines and treatment strategies. Ozone: Sci. Eng. 2012, 34, 408–424. [CrossRef]
- Chaijadi, D.; Hendradiana, A.; Tjahjono, P.D.; Kusumaningsih, E.; Hariyanto.; Siagian, C.; Atmadja, D.S.; Viebahn-Hänsler, R. The Role of Ozone Therapy as Adjuvant in the Management of Covid-19 in Indonesia. Proceedings 26 Ozone World Congress of the International Ozone Association IOA, 2023.
- Gencer-Aalay, K.; Sahin, T.; Could ozone therapy be used to prevent COVID-19? Marmara Med J- .2022; 35, 196-201. https://dergipark.org.tr/tr/pub/marumj.
- Medina, J. G. Journal of Ozone Therapy. 2022. 6, 11-12. [CrossRef]
- Togi, S.; Togo, M.; Nagashima, S.; Kitai, Y.; Muromoto, R.; Kashiwakura, J.; Miura, T.; Matsuda, T. Implication of NFkB Activation of Ozone-Induced HO-1 Activation. BRP Reports 2021. 4: 59-63. http://hdl.handle.net/2115/82070.
- Wolff, Hans 1979 “Das Medizinische Ozon” Verlag für Medizin vfm Heidelberg/Thieme.
- Takon Oru, G.; Viebahn-Haensler, R.; García Fernández, E.; Alvarez Almiñaque, D.; Polo Vega, J.C.; Tamargo Santos, B.; López Cabreja, G.; Serrano Espinosa, I.; Tabares Nápoles, N.; León Fernández, O.S. Medical Ozone Effects and Innate Immune Memory in Rheumatoid Arthritis Patients Treated with Methotrexate+Ozone After a Second Cycle of Ozone Exposure. Chronic Pain Manag 2019, 2, 114. [CrossRef]
- León, F.O.S.; Viebahn-Haensler, R.; López, C.G.; Serrano, E.I.; Hernández, M.Y.; Delgado,R.L.; Tamargo, S.B.; Takon, O.G.; Polo, V.J.C. Medical ozone increases methotrexate clinical response and improves cellular redox balance in patients with rheumatoid arthritis. Eur. J.Pharmacol. 2016, 789, 313–318. [CrossRef]
Figure 1.
The general mechanisms of ozone depend on pH, partial pressure, temperature, on the substrate, solvents and other factors. The ozone molecule has a polar structure, here written in its mesomeric form. Therefore, the preferred reaction is a non-radical 1,3 electrophilic addition or, at pH >7 a radical reaction in water as solvent.
Figure 1.
The general mechanisms of ozone depend on pH, partial pressure, temperature, on the substrate, solvents and other factors. The ozone molecule has a polar structure, here written in its mesomeric form. Therefore, the preferred reaction is a non-radical 1,3 electrophilic addition or, at pH >7 a radical reaction in water as solvent.

Figure 2.
a. The metabolism of RBC´s influenced by peroxides, here “ozone peroxide” (formed from ozone and unsaturated fatty acids with isolated double bonds): Hexose phosphate and pentose phosphate pathways are activated at low ozone concentrations [10], whereby 2,3 DPG (diphosphoglycerate) increases. b. As regards the pentose phosphate path and its function of peroxide detoxification by GSH; at high ozone concentrations (here 80g/ml) the GSH balance is disturbed and the antioxidant efficacy is lost [14,15]. The pentose phosphate path is induced by glucose-6-phosphate dehydrogenase providing the RBC with the antioxidant system; a deficiency is seen in patients with malaria resistance.
Figure 2.
a. The metabolism of RBC´s influenced by peroxides, here “ozone peroxide” (formed from ozone and unsaturated fatty acids with isolated double bonds): Hexose phosphate and pentose phosphate pathways are activated at low ozone concentrations [10], whereby 2,3 DPG (diphosphoglycerate) increases. b. As regards the pentose phosphate path and its function of peroxide detoxification by GSH; at high ozone concentrations (here 80g/ml) the GSH balance is disturbed and the antioxidant efficacy is lost [14,15]. The pentose phosphate path is induced by glucose-6-phosphate dehydrogenase providing the RBC with the antioxidant system; a deficiency is seen in patients with malaria resistance.
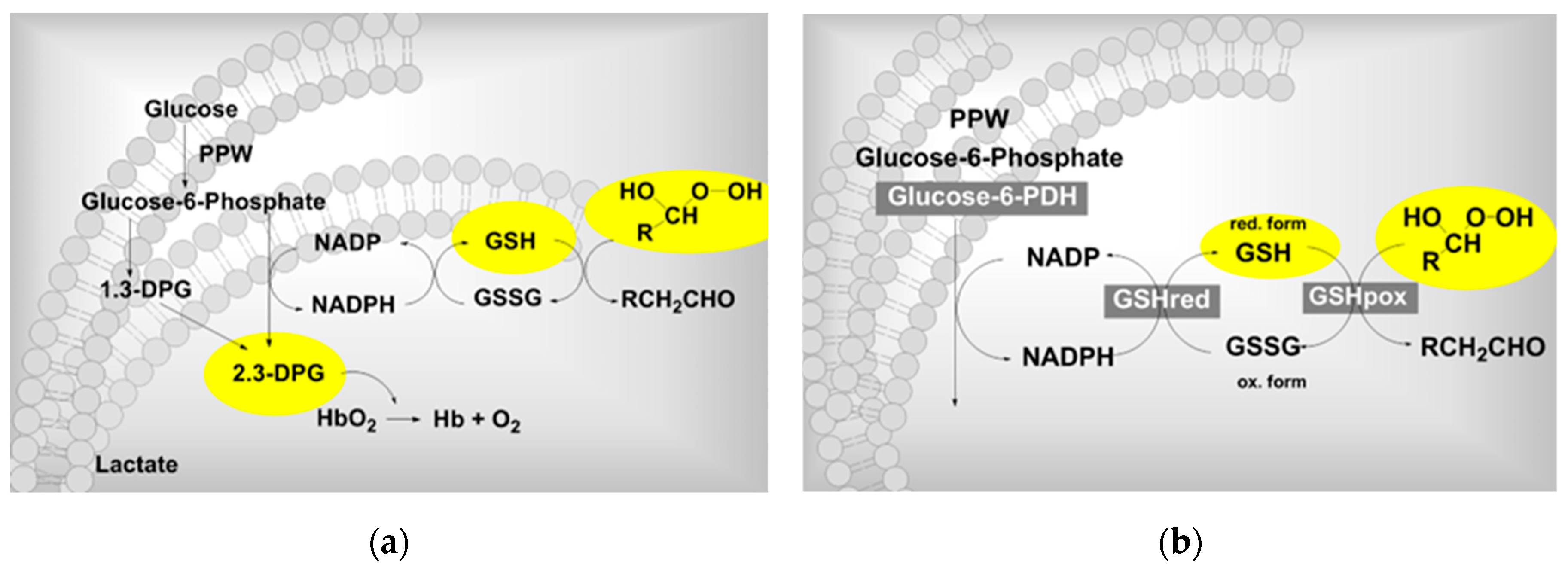
Figure 3.
Lethal peritonitis in an animal model. a. Survival rate after ozone pretreatment in dependance on ozone concentration: intraperitoneal ozone infiltration with 10 g/ml prior to the infection shows with a survival rate of 57 % the best outcome (20 mL corresponding to a dose of 200 μg, administered 1x daily for 5 consecutive days prior to infection); by applying an ozone concentration of 100 g/ml the survival rate decreases again to 23 %, even worse than with oxygen. b. Synergistic effects with antibiotics. Ozone pretreatment with a concentration of 10g/ml in all groups. Four different antibiotics were used only in one treatment, immediately after infection: Antibiotic 1: Cefodizim, antibiotic 2: Cefotaxim, antibiotic 3: Levofloxacin, antibiotic 4: Piperacillin/Tazobactam. Synergistic effects could be achieved with antibiotic 1 and 4 after one treatment only. In case of Piperacillin/Tazobactam (4) after a second treatment one hour later even a 100 % survival was counted [11], not shown here.
Figure 3.
Lethal peritonitis in an animal model. a. Survival rate after ozone pretreatment in dependance on ozone concentration: intraperitoneal ozone infiltration with 10 g/ml prior to the infection shows with a survival rate of 57 % the best outcome (20 mL corresponding to a dose of 200 μg, administered 1x daily for 5 consecutive days prior to infection); by applying an ozone concentration of 100 g/ml the survival rate decreases again to 23 %, even worse than with oxygen. b. Synergistic effects with antibiotics. Ozone pretreatment with a concentration of 10g/ml in all groups. Four different antibiotics were used only in one treatment, immediately after infection: Antibiotic 1: Cefodizim, antibiotic 2: Cefotaxim, antibiotic 3: Levofloxacin, antibiotic 4: Piperacillin/Tazobactam. Synergistic effects could be achieved with antibiotic 1 and 4 after one treatment only. In case of Piperacillin/Tazobactam (4) after a second treatment one hour later even a 100 % survival was counted [11], not shown here.
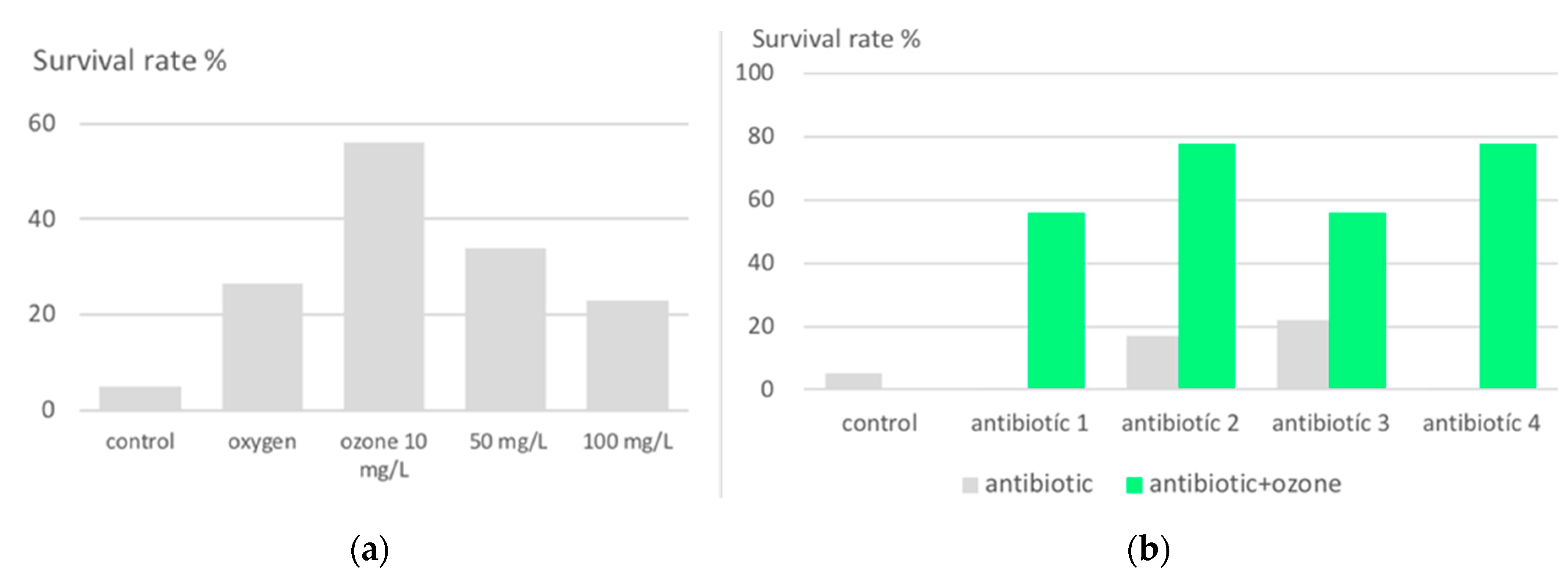
Table 2.
Characteristic injury and protective redox markers and some clinical parameters in RA patients during a two-cycle systemic ozone treatment, see Figure 4.
Table 2.
Characteristic injury and protective redox markers and some clinical parameters in RA patients during a two-cycle systemic ozone treatment, see Figure 4.
| Injury biomarkers: Oxidative stress markers | Protective markers: antioxidants | Clinical parameters |
|---|---|---|
| TH (total hydroperoxides) | total SOD (superoxide dismutase) CAT (catalase) |
DAS (disease activity score) PAIN |
| MDA (malondialdehyde) AOOP (advanced oxidation protein products) |
GSH (reduced glutathione) | HAQ: DI, (health Assessment disability questionnaire) |
| NO (nitrogen monoxide) | GGT (gamma glutamyl transferase) | Auto antibodies CCP (anti-cyclic citrullinated peptides) |
Table 3.
Ozone and prevention: treatment recommendation.
| Application | Ozone conc. | Ozone volume | Treatment frequency |
|---|---|---|---|
| Rectal ozone-insufflation | 15 - 25 µg/ml In general: 10 to max. 40 µg/ml |
150–300 ml |
2x to 3x per week, if possible prior to chemotherapy or antibiotics. At least 1x per week as adjuvant therapy or 2 to 3 series per year with 10 treatments each |
| Major autohemotherapy | 15 - 25 µg/ml In general: 10 to max. 40 µg/ml |
50 ml | 2x to 3x per week, if possible prior to chemotherapy or antibiotics. At least 1x per week as adjuvant therapy or 2 to 3 series per year with 10 treatments each |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



