
Submitted:
08 September 2023
Posted:
19 September 2023
You are already at the latest version
Abstract
Background: Galectin-3 (Gal-3) overexpression is associated with fibroblastic proliferation and the production of collagen, resulting in increased cardiac fibrosis and remodelling. Aim of the study was to investigate on the expression of Gal-3 in hypertrophic hearts. We examined 19 surgical specimens taken from interventricular septum of 8 patients with Tetralogy of Fallot, 4 patients with aortic valve stenosis, 1 cardiac explant affected from dilated cardiomyopathy, and 6 myocardial biopsies of patients submitted to heart transplantation. Methods: All the samples were routinely processed, stained with Hematoxylin-Eosin, Trichromic stain and elastic fiber stain and selected by having the morphological features of myocardial hy-pertrophy: myocytolysis, nuclear pleomorphism, interstitial fibrosis. Results: At immunohistochemistry, myocardial fibers showed cytoplasmic expression of Gal-3 in the 4 patients with aortic valve stenosis (diffuse in 3 and mild in 1), in the 1 patient with cardiac explant (mild) and in the 4/6 transplanted hearts (mild and focal in 3 and diffuse in 1). The 8 patients affected from Tetralogy of Fallot and 2 patients with transplanted hearts resulted negative. Conclusions: The results agreed with the hypothesis that Gal-3 may play a role in cardiac hyper-trophy; its expression in myocardial fibers is not related with the morphological aspects as suggested by the absence in pediatric cases. The presence in myocardial biopsies taken from transplanted hearts would suggest a possible role in predicting clinical outcome of such patients.
Keywords:
galectin-3
; cardiac hypertrophy
; immunohistochemical expression
; heart transplantation
; heart disease
; cardiorenal syndrome
Introduction
Gal3 is a member of the galectins family of carbohydrate-binding proteins [1] expressed in the cytoplasm of different cell types (epithelial and endothelial cells), mainly by activated macrophages [2].
In the human genome it is encoded by a single gene (LGALS3) located on chromosome 14, locus q21-22, composed of 6 exons and 5 introns covering about 17 kilobases [1].
Gal3 regulates basic cellular functions, namely growth, proliferation, differentiation, and inflammation; the basic expression of Gal3 is varied and unstable in different tissues and it is inducible.
Under physiological conditions in cardiac tissue, the basal expression of Gal3 is very low, but when cardiac damage occurs, it is readily induced. In fact, overexpression of Gal3 is associated with fibroblastic proliferation and collagen production, resulting in increased cardiac fibrosis and remodeling [2,3], with probable predictive role in heart failure and heart transplantation.
Furthermore, Gal3 is also present at the extracellular level and modulates the interaction between epithelial cells and extracellular matrix, playing a role in renal collecting tubule embryogenesis [4].
In several experimental studies, the serum levels of Gal3 appear to be related to the development of renal fibrosis, in an inversely proportional relationship to the eGFR in the adult population [5], with a probable predictive role in chronic renal disease and renal transplantation.
Materials and Methods
The aim of our study is to evaluate the immunohistochemical (IHC) expression of Gal3 in the hypertrophic heart secondary to different morbid states in relation to the adaptive capacity of myocardial fibers and its distribution. Importantly, such an antibody has rarely been used for this application.
The study was performed on 19 myocardial fragments from hearts of patients undergoing myocardial band resection for Tetralogy of Fallot and aortic stenosis, heart explant and biopsies taken from follow-up transplanted patients to monitor rejection reactions.
The following parameters of each patient were considered: age, sex, clinical diagnosis, evaluation of histological characteristics (cardiomyocyte hypertrophy and interstitial and subendocardial fibrosis) and immunohistochemical expression of Gal3.
We used Hematoxylin-Eosin, Trichromic stain and elastic fiber stain to select cases that have the features of hypertrophic myocardium, namely myocytolysis, nuclear pleomorphism, and interstitial fibrosis.
Results
In the 8 patients (Table 1 and Figure 1) with a clinical diagnosis of Tetralogy of Fallot, aged between 9-15 months, 5 male and 3 females, the following were highlighted: in 2 patients only cardiomyocyte hypertrophy; in 1 patient only interstitial fibrosis; in 5 patients cardiomyocyte hypertrophy and endocardial or subendocardial fibrosis.
In all cases the immunohistochemical expression of Gal3 is negative.
In other 5 patients (Table 2 and Figure 2), of which 4 with aortic stenosis and 1 with cardiac explant from dilated cardiomyopathy (CMD), aged between 48-76 years, 1 male and 4 female, we highlight: all 5 patients with cardiomyocyte hypertrophy, associated with subendocardial fibrosis in 3 patients, 1 patient with endocardial fibroelastosis, 1 patient with endocardial fibroelastosis and interstitial fibrosis.
Gal3 is positive in all cases, 2 with weak band positivity, 2 diffuse subendocardial positivity and 1 focal subendocardial positivity.
In the 6 patients (Table 3 and Figure 3) undergoing heart transplantation for various pathological conditions (dilated cardiomyopathy, acute heart failure and chronic ischemic heart disease) and in follow-up by heart biopsy for rejection, aged between 25-77 years, 4 males and 2 females, we went on to measure the peri-graft and post-graft serum Gal3 values (normal values of serum Gal3 17 ng/mL) buying them with the histological features and IHC expression of Gal3.
In this group two cases show IHC of Gal3 negative and the serum values are missing; 4 are positive to Gal3; in 3 of them that date few weeks from the transplantation, post-graft serum Gal3 is reduced as compared to peri-graft and in the remaining patient that received the heart in 2009 the serum Gal3 is not available.
Discussion
The analysis of our preliminary study allows us to make 3 considerations:
1) the hypertrophic-regressive morphological aspect does not necessarily correlate with the IIC expression of Gal3;
2) the immunohistochemical expression of Gal3 appears to be closely related to cardiac hypertrophy and remodeling;
3) in the studied cases, immunohistochemical expression and serum values of Gal3 seem to be associated with cardiomyocyte hypertrophy more than with endocardial fibrosis.
In fact, in patients with Tetralogy of Fallot, the obstruction of the ventricular-pulmonary outflow is probably the expression of a malalignment of the infundibular portion of the septum, in which the hypertrophic component has not yet had the opportunity to manifest itself; in addition, the time interval between the onset of the disease and the resection is limited due to age of patients ranging from 9 months to 15 months.
On the contrary, in patients with aortic stenosis and dilated cardiomyopathy the phenomenon of adaptation-hypertrophy of the fibers correlates with Gal3; positivity is commonly found in cardiac muscle subendocardial fibers with a progressively decreasing gradient as one moves away from the endocardial surface; moreover it is found constantly below those areas affected by a marked endocardial fibrosis, sometimes with the morphology of a real fibrous cushion and with fibroelastosis modifications of the endocardium.
In patients in follow-up for cardiac transplant rejection it is observed that the immunohistochemical expression and the serum values of Gal3 are correlated with the hypertrophic features of the cardiomyocytes.
Studies reported in the literature are conflicting whether serum Gal3 values are correlated or uncorrelated with myocardial fibrosis ; in fact, in our preliminary study, they seem to be more correlated with cardiomyocyte hypertrophy.
In most studies, clinical data correlate serum Gal-3 levels with myocardial fibrosis [6], as it is responsible for the regulation of pro-fibrotic pathways [7,8].
In other studies, no significant association was found between Gal-3 and myocardial fibrosis, suggesting that Gal-3 does not play a crucial role in the pathogenesis of fibrotic cardiomyopathy associated with pressure overload [9,10].
Furthermore, in other studies, a specific association of Gal-3 with cardiac fibrosis has not been observed and Gal-3 appears instead to be elevated due to impaired renal clearance or renal dysfunction [11], due to the involvement of the cardiac -renal axis.
Other authors believe that chronic kidney disease is a contributing cause of elevated concentrations of Gal3, since in chronic renal failure there is renal fibrosis that can be associated with cardiac fibrosis [12].
All these hypotheses suggest that Gal3 could be a potential biological marker for patients with Cardiorenal Syndrome [13] and further studies are needed.
Conclusions
Gal-3 can be considered a new promising cardiac biomarker for the evaluation of cardiac function in the follow-up of transplant patients to be associated with the study of cellular and humoral rejection alterations.
The immunohistochemical expression of Gal-3 is associated in the cases studied with cardiomyocyte hypertrophy more than with endocardial fibrosis.
There is probably a correlation with the Gal-3 values detected in the serum which, however, requires studies on larger case series and for longer time intervals.
Author Contributions
Conceptualization, A.M. and C.S.; methodology, A.M. and C.S.; investigation, G.C., L.G., G.F. and M.M.; data curation, G.C., L.G., G.F. and G.N.; writing—original draft preparation, C.S. and A.M.; writing—review and editing, A.M. and G.S.; supervision, A.M. and G.S.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bi J, Garg V, Yates AR. Galectin-3 and sST2 as Prognosticators for Heart Failure Requiring Extracorporeal Life Support: Jack n' Jill. Biomolecules. 2021 Jan 27;11:166. [CrossRef]
- Frunza O, Russo I, Saxena A, et al. Myocardial Galectin-3 Expression Is Associated with Remodeling of the Pressure-Overloaded Heart and May Delay the Hypertrophic Response without Affecting Survival, Dysfunction, and Cardiac Fibrosis. Am J Pathol. 2016;186:1114-27. [CrossRef]
- Suthahar N, Meijers WC, Silljé HHW, Ho JE, Liu FT, de Boer RA. Galectin-3 Activation and Inhibition in Heart Failure and Cardiovascular Disease: An Update. Theranostics. 2018 Jan 1;8(3):593-609. [CrossRef]
- Ochieng J, Furtak V, Lukyanov P. Extracellular functions of galectin-3. Glycoconj J. 2002;19(7-9):527-35. [CrossRef]
- Tang WH, Shrestha K, Shao Z, et al. Usefulness of plasma galectin-3 levels in systolic heart failure to predict renal insufficienc and survival. Am J Cardiol. 2011;108:385-390.
- Lin YH, Lin LY, Wu YW, et al. The relationship between serum galectin-3 and serum markers of cardiac extracellular matrix turnover in heart failure patients. Clin Chim Acta 2009;409. [CrossRef]
- Avishay Grupper, Jose Nativi-Nicolau, Joseph J. Maleszewski, Jennifer R. Geske, Walter K. Kremers, Brooks S. Edwards, Sudhir S. Kushwaha, Naveen L. Pereira, Circulating Galectin-3 Levels Are Persistently Elevated After Heart Transplantation and Are Associated With Renal Dysfunction, JACC: Heart Failure, Volume 4, Issue 11, 2016, Pages 847-856, ISSN 2213-1779. [CrossRef]
- Antoni Bayes-Genis, Marta de Antonio, Joan Vila, Judith Peñafiel, Amparo Galán, Jaume Barallat, Elisabet Zamora, Agustin Urrutia, Josep Lupón, Head-to-Head Comparison of 2 Myocardial Fibrosis Biomarkers for Long-Term Heart Failure Risk Stratification: ST2 Versus Galectin-3, Journal of the American College of Cardiology, Volume 63, Issue 2, 2014, Pages 158-166, ISSN 0735-1097. [CrossRef]
- Frunza O, Russo I, Saxena A, et al. Myocardial galectin-3 expression is associated with remodeling of the pressure-overloaded heart and may delay the hypertrophic response without affecting survival, dysfunction, and cardiac fibrosis. Am J Pathol 2016;186:1114–27. [CrossRef]
- Abou Ezzeddine OF, Haines P, Stevens S, et al. Galectin-3 in heart failure with preserved ejection fraction. A RELAX trial substudy (Phosphodiesterase-5 Inhibition to Improve Clinical Status and Exercise Capacity in Diastolic Heart Failure). J Am Coll Cardiol HF 2015;3:245–52.
- Maisel A, Kim P, Stendardi W. Galectin-3 After Heart Transplantation: Does it Get Better? JACC Heart Fail. 2016 Nov;4(11):857-859. [CrossRef] [PubMed]
- O’Seaghdha CM, Hwang SJ, Ho JE, et al. Elevated galectin-3 precedes the development of CKD. J Am Soc Nephrol 2013;24:1470-7. [CrossRef]
- Iacoviello M, Aspromonte N, Leone M, et al. Galectin-3 serum levels are independently associated with microalbuminuria in chronic heart failure outpatients. Res Cardiovasc Med 2015;5:e28952.
Figure 1.
Patient with Tetralogy of Fallot. A) HE staining which highlights cardiomyocyte hypertrophy. B) Minimal interstitial fibrosis is highlighted on trichrome staining. C) On immunohistochemistry Gal3 is negative.
Figure 1.
Patient with Tetralogy of Fallot. A) HE staining which highlights cardiomyocyte hypertrophy. B) Minimal interstitial fibrosis is highlighted on trichrome staining. C) On immunohistochemistry Gal3 is negative.
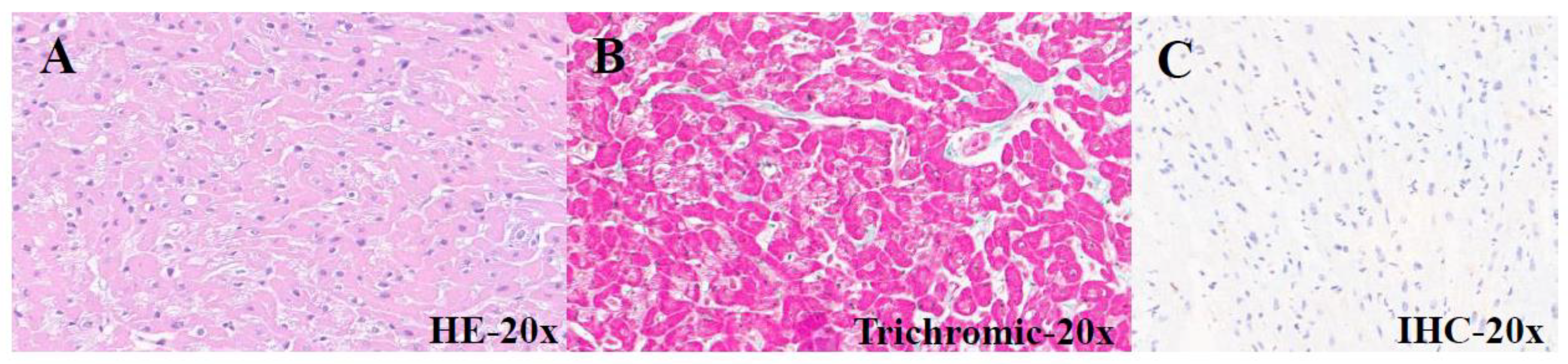
Figure 2.
Patient with aortic stenosis. A) HE staining highlights hypertrophic-regressive phenomena. B) Trichrome staining reveals subendocardial fibrosis. C) On immunohistochemistry Gal3 has diffuse subendocardial positivity.
Figure 2.
Patient with aortic stenosis. A) HE staining highlights hypertrophic-regressive phenomena. B) Trichrome staining reveals subendocardial fibrosis. C) On immunohistochemistry Gal3 has diffuse subendocardial positivity.
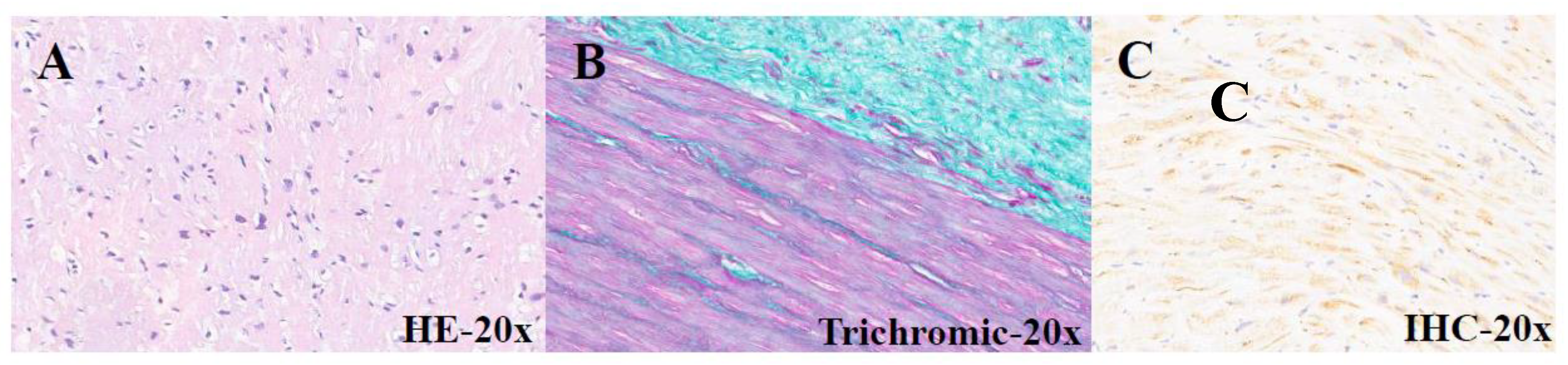
Figure 3.
Myocardial biopsy of patients submitted to heart transplantation. A) HE staining highlights hypertrophic-regressive aspects. B) Trichrome staining shows fibrosis. C) On immunohistochemistry Gal3 has diffuse positivity.
Figure 3.
Myocardial biopsy of patients submitted to heart transplantation. A) HE staining highlights hypertrophic-regressive aspects. B) Trichrome staining shows fibrosis. C) On immunohistochemistry Gal3 has diffuse positivity.
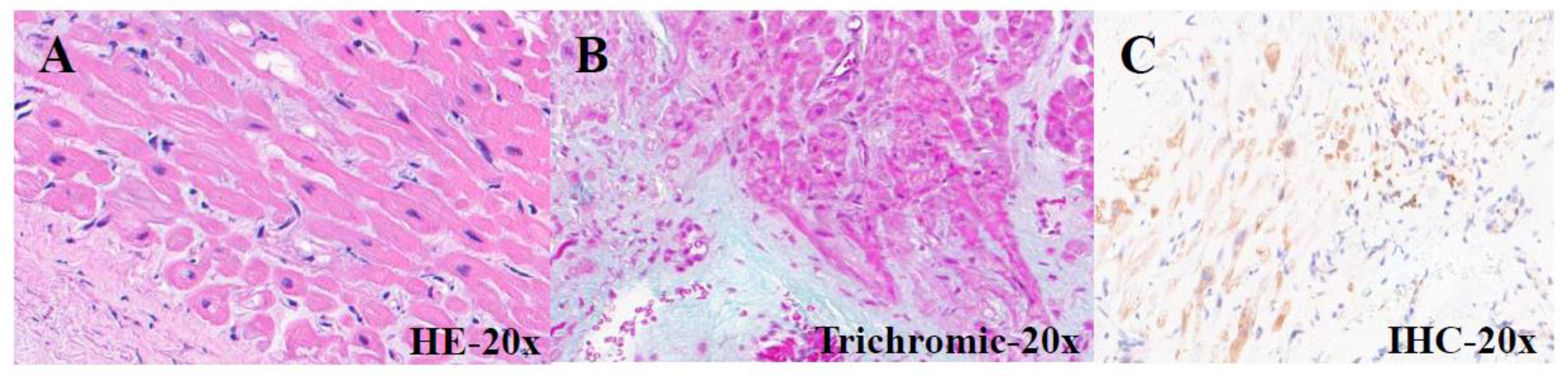

Table 1.
Patients with a Tetralogy of Fallot.
| PATIENTS | AGE (months) | GENDER | CLINICAL DIAGNOSIS |
HISTOLOGY | IHC Gal3 |
|---|---|---|---|---|---|
| 18-I-9862 A1 |
9 | M | Tetralogy of Fallot |
Cardiomyocyte hypertrophy | Negative |
| 18-I-20309 A1 | 11 | M | Tetralogy of Fallot |
Mild interstitial fibrosis | Negative |
| 18-I-20648 A1 | 14 | F | Tetralogy of Fallot |
Interstitial fibrosis and cardiomyocyte hypertrophy |
Negative |
| 18-I-21278 A1-B1 | 13 | M | Tetralogy of Fallot |
Cardiomyocyte hypertrophy | Negative |
| 19-I-2479 A1 |
15 | M | Tetralogy of Fallot |
Hypertrophic-regressive cardiomyocytes and endocardial fibrosis |
Negative |
| 19-I-3718 A1 |
12 | F | Tetralogy of Fallot |
Hypertrophic-regressive cardiomyocytes and subendocardial fibrosis |
Negative |
| 19-I-12929 A1 | 13 | F | Tetralogy of Fallot |
Hypertrophic-regressive cardiomyocytes and endocardial fibrosis |
Negative |
| 19-I-13382 A1 | 11 | M | Tetralogy of Fallot |
Hypertrophic-regressive cardiomyocytes and endocardial fibrosis |
Negative |
Table 2.
Patients with aortic stenosis and cardiac explant.
| PATIENTS | AGE (years) | GENDER | CLINICAL DIAGNOSIS |
HISTOLOGY | IHC Gal3 |
|---|---|---|---|---|---|
| 19-I-3851 A1 |
76 | F | Aortic stenosis | Hypertrophic-regressive cardiomyocytes and endocardial fibroelastosis |
Mild band positivity |
| 21-10936 A1 |
48 | F | Aortic stenosis | Hypertrophic-regressive cardiomyocytes and subendocardial fibrosis |
Diffuse subendocardial positivity |
| 21-I-10937 A1 | 48 | F | Aortic stenosis | Hypertrophic-regressive cardiomyocytes and subendocardial fibrosis |
Diffuse subendocardial positivity |
| 21-I-13205 A2 | 55 | M | Cardiac explant (CMD) |
Hypertrophic-regressive cardiomyocytes and subendocardial fibrosis |
Focal subendocardial positivity |
| 21-I-13914 A1 | 75 | F | Subaortic rim | Hypertrophic-regressive cardiomyocytes, endocardial fibroelastosis and interstitial fibrosis |
Mild band positivity |
Table 3.
Myocardial biopsies of patients submitted to heart transplantation.
| PATIENTS | AGE (years) | GENDER | CLINICAL DIAGNOSIS |
HISTOLOGY | IHC Gal3 |
Peri-graft serum Gal3 ng/mL |
Post-graft Serum Gal3 ng/mL |
|---|---|---|---|---|---|---|---|
| 21-I-12747 A1 |
71 | M | Heart transplantation (deceased) |
Hypertrophic- regressive cardiomyocytes and subendocardial fibrosis |
Negative | NN | NN |
| 21-I-14228 A1 |
51 | F | Heart transplantation (2021) |
Hypertrophic- regressive cardiomyocytes and subendocardial fibrosis |
Mild and focal positivity |
29 | 22 |
| 21-I-16007 A1 |
77 | M | Heart transplantation (2009) |
Hypertrophic- regressive cardiomyocytes and endocardial fibrosis |
Mild and focal positivity |
NN | 33 |
| 22-I-16044 A1 |
51 | M | Heart transplantation (2022) |
Hypertrophic- regressive cardiomyocytes and discrete subendocardial fibrosis |
Diffuse subendocardial positivity |
45.6 | 26 |
| 22-I-16117 A1 |
59 | M | Heart transplantation (2021) |
Hypertrophic- regressive cardiomyocytes, discrete subendocardial and interstitial fibrosis |
Mild and focal positivity |
65 | 17 |
| 22-I-17480 A1 |
25 | F | Heart transplantation (2019) |
Modest interstitial lymphocytic infiltrate and marked interstitial and subendocardial fibrosis |
Negative | NN | NN |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



