
Submitted:
17 September 2023
Posted:
19 September 2023
You are already at the latest version
Abstract
The risk of developing cardiovascular diseases (CVD) in patients suffering from rheumatoid arthritis (RA) is 1.5 times higher compared to the general population. The objective of this retrospective study was to determine the type of cardiovascular complications that can appear in patients with rheumatoid arthritis. Reducing the cardiovascular risk, through an aggressive management of the traditional and non-traditional risk factors, is another objective of this study. Early diagnosis and initiation of therapeutic measures to reduce the progression rate of rheumatoid arthritis, while also maintaining an active lifestyle, are the most important problems in young patients.
We included a number of 200 patients with rheumatoid arthritis, presenting various stages of disease, concomitant with cardiovascular complications. The incidence by gender was higher in women, while men presented a higher incidence of traditional and non-traditional cardiovascular risk factors. All the patients presented an atherogenic coefficient over 2, indicating a significant risk of atherogenesis. An increased incidence of coronary artery disease was found in men. The patients presented cardiac arrhythmias, especially in the active stage of the condition, while the incidence of atrial fibrillation was higher in women. The active stage of the disease was evaluated using inflammatory biomarkers (ESR, PCR). ESR is not a specific tool for diagnosing the disease, but its important role in monitoring the activity of RA should not be ignored. Moreover, ESR has a significant role in monitoring the evolution and determining the prognostic of congestive heart failure.
A target treatment prescribed a target treatment to reduce inflammation and prevent exacerbations was prescribed for all patients.
However, in daily clinical practice, the screening for RA is poorly done. Thus, patients are often undiagnosed, while the risk factors are not assessed. In conclusion, even nowadays, RA patients continue to present an increased risk of developing CVD.
Keywords:
rheumatoid arthritis
; cardiovascular complications
; atherogenesis
; cardiac arrhythmias
; inflammation
; disease
1. Introduction
Rheumatoid arthritis (RA) is the most prevalent chronic inflammatory joint disease, with a prevalence of 460 per 100,000 people. [1] It is known that CVD is a common comorbidity in RA patients, resulting in a more severe disease burden. [2] Several meta-analyses have indicated an increased risk of CV death by 50–60%. [3,4] This could be explained by the contribution of systemic inflammation in the development of atherogenesis, while the “traditional” CV risk factors are also attributed to nearly 50% of the total CVD risk. [5]
Patients with active RA have significantly lower high- and low-density lipoprotein cholesterol (HDL-c/LDL-c) levels compared to the healthy population. [6] Smoking is also significantly associated with a higher disease activity score, leading to worse clinical outcomes. [7]
Suppressing the inflammatory process reduces CVD morbidity and mortality in patients with severe RA, according to recent data. Even modest, but clinically relevant, efficacy of atorvastatin in the treatment of RA highlights the significant anti-inflammatory properties of statins. The need for structured preventive strategies to reduce the risk of CVD in patients with rheumatic disease is widely recognized. Such strategies should target the mechanisms involved in the occurrence of atherosclerosis in patients with RA, as well as optimal management of lifestyle related risk factors is needed. [8]
The aim of this study was to determine the cardiovascular complications that can appear in patients with rheumatoid arthritis, while also preventing their appearance through better control strategies of the “traditional” and “non-traditional” CV risk factors. Patient education regarding the cardiovascular complications associated with RA represents the first step for a more effective preventive strategy, while a good collaboration between specialists in rheumatology and cardiology is important in the establishment of optimal therapeutic decisions.
2. Materials and method
In this retrospective, observational and descriptive study were included 200 patients diagnosed with rheumatoid arthritis and treated in the Rheumatology Department, in collaboration with the Cardiology Department, of the Bihor County Clinical and Emergency Hospital, between March 2020 and March 2023. The inclusion criteria were the diagnosis of rheumatoid arthritis and the presence of cardiovascular complications. No patient was excluded from the study. At admission, it were collected data regarding the main symptoms which have led to admission in the hospital, complete medical history, history of family disease, harmful behaviors, home medication, and environment of origin, The general clinical examination was done for each patient. Moreover, we determined the blood pressure of all patients and conducted concurrent electrocardiograms in conjunction with echocardiographic examinations and laboratory tests. This data was statistically analyzed according to the intended purpose of this study. Detailed quantitative data on the amount of tobacco used and body mass index was not available.
Data analysis
All the data from the study was analyzed using IBM SPSS Statistics 25 and illustrated using Microsoft Office Excel/Word 2021. Quantitative variables were tested for normal distribution using the Shapiro-Wilk Test and were written as averages with standard deviations or medians with interquartile ranges. Quantitative independent variables with non-parametric distribution were tested between groups using Mann-Whitney U tests.
Qualitative variables were written as counts or percentages and differences between groups were tested using Fisher’s Exact test/Pearson Chi-Square Test. Z-tests with Bonferroni corrections were used to further detail the results obtained in the contingency tables.
Logistic regression univariable and multivariable models were used to predict the odds of cardiac complications and arterial fibrillation. The measure of prediction was cuantified as odds ratios with 95% confidence intervals. The validity and significance of models were tested along with the goodness-of-fit tests and validation of linearity assumption. In the case of atrial fibrillation, a multivariable model was constructed using the forward stepwise selection based on the Wald criterium.
Results
This clinical study included 200 patients, 124 women and 76 men, with a higher incidence observed in females. (Table 1)
The highest prevalence of the disease was observed in patients aged between 50 to 69 years old. The existence of 25 cases in the 40-49 age category could be suggestive for early onset of rheumatoid arthritis and cardiovascular complications. (Table 1)
Most of the patients were diagnosed with stage III of the disease; 13% of patients were diagnosed during stage I, 19% of patients were diagnosed with stage II, 42.5 % in stage III and quite a high percentage of 25.5% were diagnosed in stage IV. It was observed a correlation between the chronic evolution of RA , and the presence of cardiovascular complications in patients with advanced rheumatoid arthritis. (Table 2)
The “traditional” CV risk factors were identified to nearly 50% of the total CVD risk. [9] Smoking was more frequently observed in RA patients, since this behavior was associated with a higher incidence of RA. [10,11,12]
Smoking was also significantly associated with a higher disease activity score, leading to worse clinical outcomes. [13]
Hypertension and diabetes were also more prevalent in RA patients compared to healthy control groups. [14]
While arterial hypertension was established as a risk factor for cardiovascular disease, there was consistent evidence that systemic inflammation, present in patients with RA, played a central role in maintaining high blood pressure values. [15]
In addition to the traditional risk factors, patients with RA were more likely to suffer from metabolic syndrome. [16] Metabolic syndrome was highly correlated with traditional risk factors such as hyperlipidemia, hypertension and diabetes mellitus, and resulted in a relative risk for cardiovascular disease of 1.93. [17]
As displayed in the table above, there was a higher incidence in men regarding traditional and non-traditional CV risk factors. (Table 3)
In addition to traditional risk factors, novel “non-traditional” risk factors involved in acceleration of atherosclerosis were emphasized in recent years. In this study, non-traditional risk factors were identified and distributed by gender.
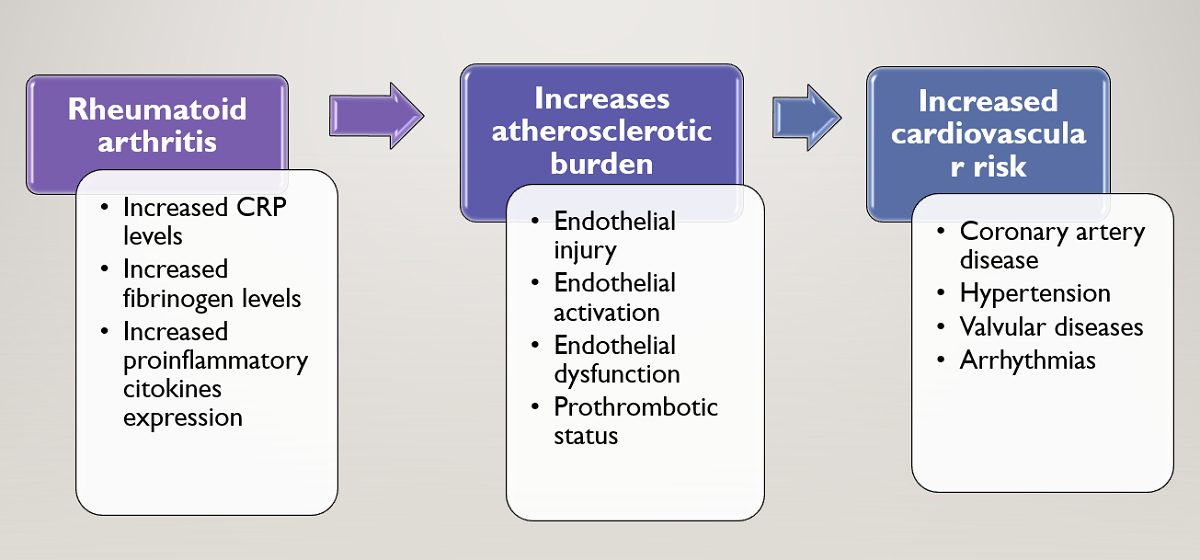
The inflammatory mechanisms involved in the pathophysiology of RA enhance atherogenesis in several ways. C-reactive protein, a useful marker of disease activity, is elevated in RA and has significant prognostic value. [18] It also causes endothelial injury directly through the activation of endothelial cells due to T-cell mediated cytotoxicity. [19] Circulating cytokines in RA, such as TNF-α, result in endothelial activation and up-regulation of adhesion molecules. [20] Endothelial dysfunction is frequently present in RA patients, even in the absence of identifiable CV risk factors, and improves with anti-TNF-α therapy. [21,22]
In recent years, new cardiovascular risk factors, suggested to be useful in cardiovascular risk stratification, were described: C-reactive protein, interleukin 6, TNF- α, endothelial dysfunction,homocysteine, prothrombotic status, rheumatoid factor. The presence of “traditional” and “non-traditional” risk factors in rheumatoid arthritis increases the risk of atherosclerosis and cardiovascular comorbidities.
Based on collected data, we determined the atherogenic coefficient, men scoring an average value of 4,52 +/- 0,27 (median = 4.60, IQR = 4-5) and women scoring 3,13 +/- 0,20 (median = 2.75, IQR = 2.37-4.10), the Mann-Whitney U Test showing higher values in men versus women (p<0.001). In conclusion, both groups scored an atherogenic coefficient over 2, indicating a higher risk of atherogenesis, more frequently in men (100%) than women (93.5%) (Fisher’s Exact Test – p=0.025). (Figure 1)
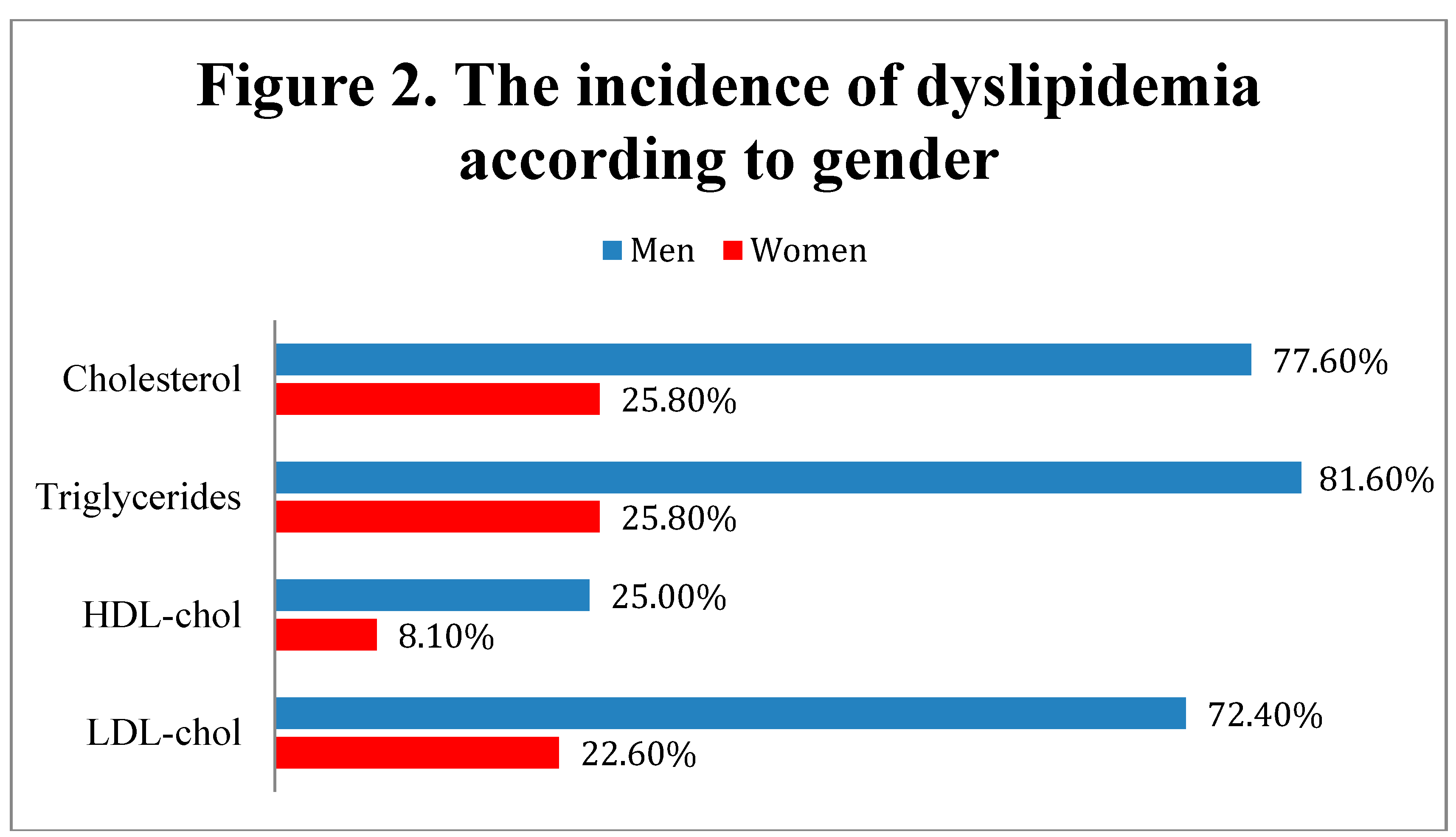
According to the data presented in Figure 2, men were significantly more associated with dyslipidemia criteria, having more frequently elevated levels of total cholesterol (≥ 200 mg/dL) (77.6% - men vs. 25.8% - women, Fisher’s Exact Test – p<0.001), LDL-cholesterol (≥ 140 mg/dL) (72.4% - men vs. 22.6% - women, Fisher’s Exact Test – p<0.001), triglycerides (≥ 150 mg/dL) (81.6% - men vs. 25.8% - women, Fisher’s Exact Test – p<0.001) and lower concentrations of HDL-cholesterol (< 40 mg/dL) (25% - men vs. 8.1% - women, Fisher’s Exact Test – p=0.002),
As displayed in the table above, men presented a higher incidence of coronary disease compared to women (Fisher’s Exact Test with Bonferroni corrected Z-tests – p<0.001). 42.1% of men presented monovascular coronary artery disease, 19.7% bivascular coronary artery disease, and 11.8% trivascular coronary artery disease. Women exhibited monovascular coronary artery disease in 24.1% of cases, bivascularcoronary artery disease in 9.6% of cases, and trivascular coronary artery disease in 4% of cases. (Table 4)
Electrocardiogram examinations was recorded for every patient enrolled in the study. Left ventricular hypertrophy was significantly more frequent in men (51.3%) than women (27.4%), p=0.001. Secondary ST-T appeared in 39.5% of men and 26.6% of women (showing a tendency towards statistical significance in the direction of higher frequencies in men than women, p=0.062), while atrial fibrillation was more frequently in women (32.3%) than men (17.1%) (p=0.021). Thus, a higher incidence of ECG abnormalities could be observed in men. The examination of the ECGs highlighted the presence of arrhythmias and conduction disorders (supraventricular extrasystoles, left anterior fascicular block, left bundle branch block, premature ventricular contractions, atrial fibrillation). (Table 5)
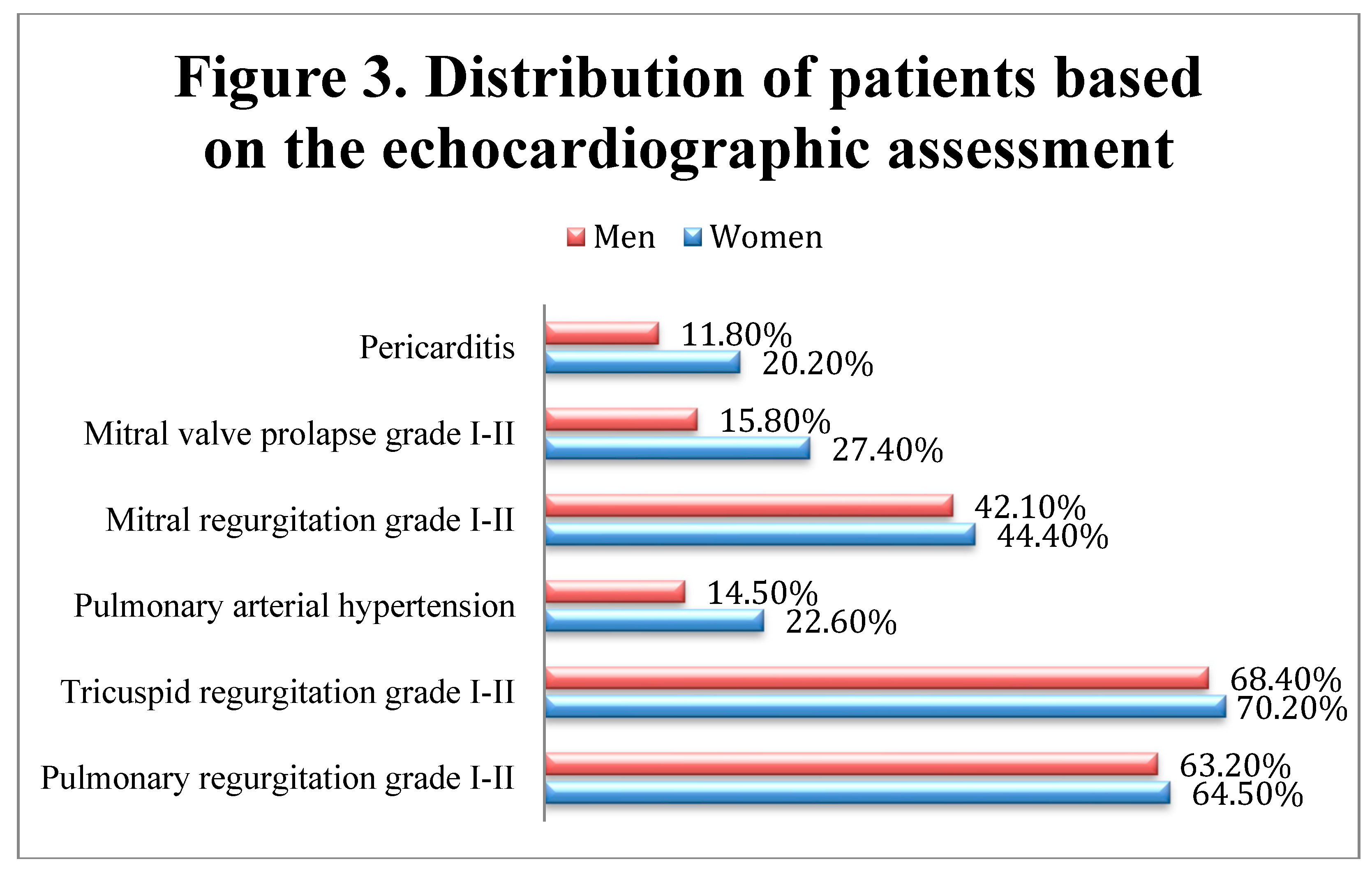
The echocardiography confirmed the presence of ventricular hypertrophy, previously reported on the ECGs. Moreover, pericarditis, pulmonary arterial hypertension, and mitral valve prolapse appeared to have a higher incidence in women compared to men, although significant differences between genders were not observed (Fisher’s Exact Tests – pericarditis (p=0.174), mitral Valve Prolapse (p=0.083), mitral Regurgitation (p=0.771), pulmonary arterial hypertension (p=0.199), tricuspid regurgitation (p=0.874), pulmonary regurgitation (p=0.880)), while wall motion abnormalities (hypokinesia and akinesia) were present in 31 patients (17 men and 14 women), possibly due to past myocardial infarctions. (Figure 3)
The etiology of congestive heart failure is complex and varies according to geographical and socio-economic factors. During the initial clinical evaluation, numerous patients complained about heart failure symptomes, which were correlated with echocardiography findings. As result, 19 patients (9.5%) were diagnosed with congestive heart failure.
Coronary artery disease and high blood pressure were the most common causes of congestive heart failure. The main cause for heart failure was arterial hypertension (44.5%) , while coronary artery disease was responsible for 17.5%, valvular heart disease for 14% of cases, and arrhythmias and conduction disorders for 7.5% of cases. (Table 6)
The comparision of analyzed parameters between patients according to the existence of cardiac complications showed that in patients with pericarditis, only HDL-cholesterol and atrial fibrillation were significantly different between groups. Patients with pericarditis had significantly higher values of HDL-cholesterol (median = 42, IQR = 40-45) in comparison to patients without pericarditis (median = 40, IQR = 40-43) (p=0.039). Also,atrial fibrillation were sig nificantly more frequently associated with pericarditis (41.2% vs. 23.5%, (p=0.033).
Data from Table no 7 show the logistic regression models used for the prediction of cardiac complications In patients with mitral valve prolapse, only frequency of LVH was significantly different between groups, patients with LVH were significantly less associated with mitral valve prolapse (40.9% vs. 21.7%) than patients without LVH (78.3% vs. 59.1%) (p=0.023). CRP, tryglicerides, HDL-cholesterol and secondary ST-T changes were significantly different between groups in patients with mitral regurgitation. This patients had a higher CRP values (median = 121, IQR = 4-150 vs. median = 105, IQR = 2-132.5, p=0.012), lower values of HDL-cholesterol (median = 40, IQR = 40-42 vs. median = 42, IQR = 40-44, p=0.018), higher frequencies of triglycerides dyslipidemia (55.2% vs. 40.7%, p=0.047) and lower frequencies of secondary ST-T changes (38.1% vs. 23%, p=0.031) than patients without mitral regurgitation.
In case of pulmonary arterial hypertension, only rheumatoid factor and HDL-cholesterol were significantly different between groups, patients with pulmonary arterial hypertension had significantly higher values of rheumatoid factor (median = 206, IQR = 137-216 vs. median = 202, IQR = 123-211, p=0.036) and higher values of HDL-cholesterol (median = 42, IQR = 40-45 vs. median = 40, IQR = 40-43, p=0.045) in comparison to patients without pulmonary arterial hypertension. In case of tricuspid regurgitation, none of the parameters were significantly different between groups (p>0.05).
LVH was a significant predictor for mitral valve prolapse (p=0.020). Patients without LVH have increased odds of having mitral valve prolapse by 2.493 times (95% C.I.: 1.153-5.376); In case of mitral regurgitation, in univariate models, HDL-cholesterol was not a significant predictor (p=0.055), while CRP (p=0.019), triglycerides dyslipidemia (p=0.043) and secondary ST-T changes (p=0.024) were significant predictors. Each increase of 1 unit of CRP was associated with increased odds of having mitral regurgitation by 1.005 times (95% C.I.:1.001-1.009); Patients with dyslipidemia had increased odds of having mitral regurgitation by 1.793 times (95% C.I.:1.019-3.154);. Patients without secondary ST-T changes had increased odds of having mitral regurgitation by 2.057 times (95% C.I.:1.098-3.861);
In case of pulmonary arterial hypertension, none of the variables were significant predictors (p>0.05). For pulmonary regurgitation, left bundle branch block was a significant predictor (p=0.009), patients with this condition had increased odds of having pulmonary regurgitation by 7.264 times (95% C.I.: 1.656-31.869).

Table 8.
Comparison of analyzed parameters between patients according to the existence of atrial fibrillation (*Fisher’s Exact Test, **Mann-Whitney U Test, ***Pearson Chi-Square Test, ****Fisher’s Exact Test with Bonferroni corrected Z-tests).
Table 8.
Comparison of analyzed parameters between patients according to the existence of atrial fibrillation (*Fisher’s Exact Test, **Mann-Whitney U Test, ***Pearson Chi-Square Test, ****Fisher’s Exact Test with Bonferroni corrected Z-tests).
| Parameter / Group | Atrial fibrillation | p | |
| Absent (N=147) | Present (N=53) | ||
| Gender (Male) (Nr., %) | 63 (42.9%) | 13 (24.5%) | 0.021* |
| Age (Median (IQR)) | 63 (55-73) | 61 (55-70.5) | 0.642** |
| Stages of RA disease (Nr., %) | 0.890* | ||
| Stage I | 20 (13.6%) | 6 (11.3%) | |
| Stage II | 28 (19%) | 10 (18.9%) | |
| Stage III | 60 (40.8%) | 25 (47.2%) | |
| Stage IV | 39 (26.5%) | 12 (22.6%) | |
| Smoking (Nr., %) | 59 (40.1%) | 11 (20.8%) | 0.012* |
| Alcohol consumption (Nr., %) | 37 (25.2%) | 10 (18.9%) | 0.450* |
| Hypertension (Nr., %) | 85 (57.8%) | 21 (39.6%) | 0.025* |
| Hypercholesterolemia (Nr., %) | 72 (49%) | 19 (35.8%) | 0.110* |
| Diabetes mellitus (Nr., %) | 24 (16.3%) | 4 (7.5%) | 0.165* |
| CRP (Median (IQR)) | 110 (2-135) | 114 (3-147) | 0.505** |
| Fibrinogen (Median (IQR)) | 4.7 (4.5-5.1) | 4.6 (4.5-4.85) | 0.022** |
| ESR (Median (IQR)) | 98 (14-106) | 98 (15.5-110.5) | 0.535** |
| Rheumatoid factor (Median (IQR)) | 201 (121-213) | 206 (168.5-213.5) | 0.047** |
| Atherogenic coefficient (Median (IQR)) | 3.375 (2.75-4.75) | 2.90 (2.29-4.67) | 0.016** |
| Total cholesterol (Median (IQR)) | 180 (157-230) | 160 (145-222.5) | 0.003** |
| Dyslipidemia – Total cholesterol (Nr., %) | 72 (49%) | 19 (35.8%) | 0.110* |
| Triglycerides (Median (IQR)) | 150 (100-170) | 110 (85-157.5) | 0.028** |
| Dyslipidemia – Triglycerides (Nr., %) | 74 (50.3%) | 20 (37.7%) | 0.148* |
| HDL-cholesterol (Median (IQR)) | 40 (40-44) | 40 (40-44.5) | 0.460** |
| Dyslipidemia – HDL-cholesterol (Nr., %) | 24 (16.3%) | 5 (9.4%) | 0.262* |
| LDL-cholesterol (Median (IQR)) | 116 (95-154) | 100 (83.5-149) | 0.008** |
| Dyslipidemia – LDL-cholesterol (Nr., %) | 65 (44.2%) | 18 (34%) | 0.255* |
| Coronary artery disease (Nr., %) | 0.030**** | ||
| Absent | 64 (43.5%) | 33 (62.3%) | |
| Monovascular artery disease | 46 (31.3%) | 16 (30.2%) | |
| Bivascular artery disease | 24 (16.3%) | 3 (5.7%) | |
| Trivascular artery disease | 13 (8.8%) | 1 (1.9%) | |
| Pericarditis (Nr., %) | 20 (13.6%) | 14 (26.4%) | 0.033*** |
| Mitral valve prolapse (Nr., %) | 33 (22.4%) | 13 (24.5%) | 0.849* |
| Mitral regurgitation (Nr., %) | 63 (42.9%) | 24 (45.3%) | 0.872* |
| Pulmonary arterial hypertension (Nr., %) | 24 (16.3%) | 15 (28.3%) | 0.070* |
| Tricuspid regurgitation (Nr., %) | 102 (69.4%) | 37 (69.8%) | 1.000* |
| Pulmonary regurgitation (Nr., %) | 90 (61.2%) | 38 (71.7%) | 0.186* |
| CHF etiology | |||
| Hypertension (Nr., %) | 69 (46.9%) | 20 (37.7%) | 0.264* |
| Coronary artery disease (Nr., %) | 30 (20.4%) | 5 (9.4%) | 0.091* |
| Valvular heart disease (Nr., %) | 18 (12.2%) | 10 (18.9%) | 0.252* |
| Arrhythmias (Nr., %) | 1 (0.7%) | 14 (26.4%) | <0.001* |
Data from Table no.8 show the comparison of analyzed parameters between patients according to the existence of atrial fibrillation. Men were significantly less associated with atrial fibrillation (42.9% vs. 24.5%) than women (75.5% vs. 57.1%) (p=0.021) Patients with arterial hypertension were significantly less associated with atrial fibrillation (57.8% vs. 39.6%) than patients without arterial hypertension (60.4% vs. 42.2%) (p=0.025). Fibrinogen levels were significantly lower in patients with atrial fibrillation (median = 4.6, IQR = 4.5-4.85) than in patients without atrial fibrillation (median = 4.7, IQR = 4.5-5.1) (p=0.022). Rheumatoid factor levels were significantly higher in patients with atrial fibrillation (median = 206, IQR = 168.5-213.5) than in patients without atrial fibrillation (median = 201, IQR = 121-213) (p=0.047);
Patients without coronary artery disease were significantly more associated with atrial fibrillation (62.3% vs. 43.5%) (p=0.030);
Data from Table 9 show the logistic regression models used for the prediction of atrial fibrillation. In univariate models, each of the analyzed parameters were significant predictors (p<0.05). Female patients had increased odds of atrial fibrillation by 2.308 times (95% C.I.:1.139-4.674) (p=0.020), Non-smokers had increased odds of atrial fibrillation by 2.557 times (95% C.I.:1.219-5.376) (p=0.013) and non-hypertensive patients had increased odds of atrial fibrillation by 2.087 times (95% C.I.:1.101-3.968) (p=0.024). Each decrease of 1 unit of fibrinogen had increased odds of atrial fibrillation by 3.322 times (95% C.I.:1.183-9.345) (p=0.023), each increase of 1 unit of rheumatoid factor had increased odds of atrial fibrillation by 1.009 times (95% C.I.: 1.001-1.017) (p=0.020). Also, patients without coronary artery disease had increased odds of atrial fibrillation by 1.972 times (95% C.I.:1.008-3.861) (p=0.047); Each decrease of 1 unit of atherogenic coefficient had increased odds of atrial fibrillation by 1.388 times (95% C.I.:1.055-1.828) (p=0.019) and each decrease of 1 unit of total cholesterol had increased odds of atrial fibrillation by 1.010 times (95% C.I.:1.002-1.018) (p=0.011);
The multivariable model was selected using the forward step-wise selection, as such only total cholesterol, coronary artery disease and pericarditis were the selected variables in the prediction, all of them being independent significant predictors
The progression of rheumatoid arthritis is characterized by flare episodes, alternating with periods of remission. Assessing the active stage of the disease relies on evaluating inflammatory joints signs, functional status, and various immunological activity tests, including erythrocyte sedimentation rate (ESR) and C-reactive protein. While ESR alone cannot diagnose a specific disease, it plays a crucial role in monitoring the activity of inflammatory conditions like rheumatoid arthritis and gauging their response to therapy. Additionally, ESR is essential for tracking the progression and establishing prognostics in congestive heart failure.
In certain diseases, such as rheumatoid arthritis, serial measurements of C-reactive protein hold prognostic value. [23]
As displayed in Table 10, 70% of patients (140 individuals) presented an ESR exceeding the upper limits, while the remaining cases presented values within the normal range. Additionally, C-reactive protein levels were within the normal range for 34.5% of patients (69 cases), while 65.5% (132 patients) displaying elevated C-reactive protein values.
These results provide new evidence suggesting that inflammatory factors present in rheumatoid arthritis patients may contribute to both the onset and prognosis of congestive heart failure. ESR, along with other specific inflammatory markers, may play a potential role in assessing congestive heart failure in patients with rheumatoid arthritis.
Rheumatoid arthritis (RA) is asociated with an increased mortality, primarily due to accelerated coronary artery and cerebrovascular atherosclerosis, which occurs in both early and established RA. The QUEST-RA study demonstrates that the prolonged use of medications such as methotrexate, sulfasalazine, glucocorticoids, leflunomide, and TNF-α blockers reduces the risk of cardiovascular events. [24]
All patients received DMARDs, with 40 (20%) of them also taking NSAIDs. Remissive treatment was administered as follows: triple therapy (methotrexate, hydroxychloroquine, and sulfasalazine) to 50 patients (25%), DMARDs inmonotherapy to 93 patients (46.5%), and DMARDs in dual therapy to 57 patients (28.5%). Corticosteroids were included in the remissive treatment of 86 patients (43%). (Table 11)
Ninety-seven patients in the study were on statin treatment (Atorvastatin), consisting of 51 men (67.10%) and 46 women (37%), men being more frequently associated with statin treatment than women ( p<0.001). Among these patients, improvements were observed in lipid profiles, along with visible clinical improvements and reductions in inflammatory markers such as ESR and CRP.
Statins, by reducing LDL-C levels, significantly lower the risk of major cardiovascular events in both high and low-risk patients for CVD. [25,26] In addition to their lipid-lowering effects, statins possess properties like stabilizing and regressing atherosclerotic plaques and limiting LDL-C oxidation, theoretically contributing to the prevention of primary atherosclerosis in RA. [27,28] These pleiotropic effects consist in anti-inflammatory, antiproliferative, antithrombotic, antioxidative, and immunomodulatory properties. [29]
3. Discussions
This study aimed to identify cardiovascular complications in patients with rheumatoid arthritis (RA) and reduce their cardiovascular risk through comprehensive management of traditional and non-traditional risk factors. An important concern arises in younger patients, emphasizing the need for early RA diagnosis and optimal therapeutic measures to maintain an active lifestyle.
In our retrospective study that included 200 patients, the most of them were women and the highest prevalence of the disease was observed in patients aged between 50 to 69 years old. Several cases in younger patients suggested an early onset of RA and potential cardiovascular complications. As expected, advanced RA stages correlated with cardiovascular complications, with a higher incidence of traditional and non-traditional risk factors in men. Both groups showed elevated atherogenic coefficients, indicating increased atherogenesis risk. Men also exhibited higher LDL-cholesterol, total cholesterol and triglyceride levels and lower levels of HDL-cholesterol and coronary artery disease incidence. Among statin-treated patients, it was observed an improved lipidic profiles and reduced inflammatory markers (ESR, CRP), especially in men.
ECG findings included left ventricular hypertrophy, secondary ST-T changes, left bundle branch block, atrial fibrillation, premature ventricular contraction, sinus tachycardia, and supraventricular extrasystole, particularly during active disease periods. Atrial fibrillation incidence was higher in women. The echocardiography assessment revealed pericarditis, pulmonary arterial hypertension, mitral valve prolapse, mitral and tricuspid regurgitation, and pulmonary regurgitation. We observed no significant differences between genders regarding cardiac valvulopathies. Common causes of congestive heart failure included coronary artery disease and arterial hypertension.
RA progression involves alternating exacerbation and remission episodes, assessed by inflammatory markers (ESR, PCR). ESR aids in monitoring disease activity and prognostics for congestive heart failure. Moreover, the prescribed treatment in this study aimed to reduce inflammation and prevent exacerbation.
Rheumatoid arthritis is a systemic autoimmune disease characterized by increased morbidity and mortality associated with cardiovascular disease [30].
The exact etiology of RA remains incompletely understood; however, both genetic and environmental factors contribute to its development. Several genetic and epigenetic components have been linked to RA, in addition to various environmental factors like cigarette smoke, dust exposure, and the microbiome. Hormonal influences may also explain the higher risk observed in women. Disease progression often begins years before symptom onset, with the development of specific autoantibodies, including rheumatoid factor (RF) and anti-citrullinated protein antibodies (ACPA). ACPA-positive RA patients typically experience more severe disease activity and an elevated risk of cardiovascular mortality. The presence of these antibodies may also contribute to the atherosclerotic process. Interestingly, ACPA has been identified in non-RA patients with cardiovascular disease, correlating with worse cardiovascular outcomes. [31]
The JAK/STAT signaling pathway, regulated by cytokines like IL-6, plays a role in RA pathogenesis, increasing systemic inflammation and extra-articular comorbidities such as atherosclerosis. [32,33,34] The European Society of Cardiology (ESC) recognizes the heightened risk of RA but provides fewer specific recommendations. It suggests a thorough evaluation of total CVD risk in adult patients with a lower threshold and considers multiplying the calculated risk by 1.5 based on disease activity [35]. Additionally, the ESC recommends similar interventions for managing CVD risk as applied to the general high-risk population.
Atherosclerotic plaques, the main CVD mechanism in RA, result from vascular, metabolic, and inflammatory factors. Dyslipidemia, hypertension, smoking, and inflammation contribute to arterial endothelial damage, causing atherosclerosis. Plaques may grow gradually or become unstable, leading to acute cardiovascular events. [33] Pro-inflammatory cytokines like TNF-α from RA increase endothelial dysfunction, while IL-6 promotes fatty streak development and IL-1 regulates macrophages and T-helper 17 cells.
According to numerous studies, physical activity significantly reduces inflammation, relieves arthritis pain, and improves mobility, making it a recommended treatment by the American College of Rheumatology. [34]
Glucocorticoids, like prednisolone, may elevate cardiovascular risk among RA patients in a dose- and duration-dependent manner. In an extensive retrospective registry study by Ocon et al., RA patients who used <5 mg daily or had a cumulative dose of <750 mg in total did not experience an increased CV risk [35]. However, patients with higher daily doses, greater cumulative doses, or longer treatment durations did face an elevated CV risk. In the recent GLORIA trial, where patients received low-dose glucocorticoids (5 mg prednisolone) for 24 months, there was a 35% increase in the incidence of CV events (2.4 cases per 100 patient years in the prednisolone group vs. 1.7 in the placebo group). [36]
Selective COX-2 inhibitors are known to increase the CV risk in the general population by approximately 35–40%. [37,38] This increase is comparable to that of traditional NSAIDs such as ibuprofen or diclofenac. [39]
Regarding atrial fibrillation (AF), the systemic inflammatory state in chronic inflammatory conditions like RA may increase the risk. Studies suggest a significantly increased incidence of AF in RA compared to the general population [40]. A Danish nationwide cohort study by Lindhardsen et al. reported an overall 40% higher incidence of AF in RA patients. [41] Using data from a large US commercial insurance plan, Kim et al. found that hospitalization for AF in RA patients was 1.4 times higher than in non-RA patients. [42]
The prevalence of coronary artery disease (CAD) in RA patients is notably higher than in the general population. Although the relationship between RA and CAD is not fully understood, RA accelerates atherosclerosis and worsens cardiovascular outcomes. Recent meta-analyses have shown higher cardiovascular disease mortality in RA patients compared to the general population. [43]
Rheumatoid arthritis-associated pulmonary hypertension can be attributed to interstitial lung disease, vascular issues, and chronic thromboembolic disease. Chronic inflammation reduces patients' functional capacity and conceals early cardiovascular and pulmonary hypertension symptoms. [44]
4. Conclusions
Rheumatoid arthritis is a chronic inflammatory disease associated with an increased cardiovascular death compared to the general population. This presence of cardiovascular disease (CVD) in patients with rheumatoid arthritis could be explained by a higher prevalence of traditional CV risk factors and systemic inflammation in this patients. Traditional risk factors are often underdiagnosed, particularly in younger patients, leading to increased cardiovascular morbidity and mortality. Regular cardiovascular risk assessments are crucial for rheumatoid arthritis patients. To reduce this additional risk, aggressive control of inflammatory activity is necessary. Anti-inflammatory drugs could decrease this risk by reducing inflammation. The glucocorticoids and cyclooxygenase-2 inhibitors should be used with caution, at the lowest effective dose, to minimize side effects. An effective preventive strategy requires close collaboration between rheumatologists and general practitioners, with an emphasis on patient education. It is recommended that the choice of therapeutic strategies be made by common agreement between rheumatologists and cardiologists, prioritizing the safety and efficacy of therapeutic decisions.
References
- Almutairi K, Nossent J, Preen D, Keen H, Inderjeeth C. The global prevalence of rheumatoid arthritis: A meta-analysis based on a systematic review. Rheumatology International. 2020; 41(5):863–877. [CrossRef]
- Logstrup, B.B.; Ellingsen, T.; Pedersen, A.B.; Darvalics, B.; Olesen, K.K.W.; Botker, H.E.; Maeng, M. Cardiovascular risk and mortality in rheumatoid arthritis compared with diabetes mellitus and the general population. Rheumatology 2021, 60, 1400–1409. [CrossRef]
- Avina-Zubieta, J.A.; Choi, H.K.; Sadatsafavi, M.; Etminan, M.; Esdaile, J.M.; Lacaille, D. Risk of cardiovascular mortality in patients with rheumatoid arthritis: A meta-analysis of observational studies. Arthr. Rheum. 2008, 59, 1690–1697. [CrossRef]
- Meune, C.; Touze, E.; Trinquart, L.; Allanore, Y. Trends in cardiovascular mortality in patients with rheumatoid arthritis over 50 years: A systematic review and meta-analysis of cohort studies. Rheumatology 2009, 48, 1309–1313. [CrossRef]
- Crowson, C.S.; Rollefstad, S.; Ikdahl, E.; Kitas, G.D.; van Riel, P.; Gabriel, S.E.; Matteson, E.L.; Kvien, T.K.; Douglas, K.; Sandoo, A.; et al. Impact of risk factors associated with cardiovascular outcomes in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2018, 77, 48–54. [CrossRef]
- Boyer, J.-F.; Gourraud, P.-A.; Cantagrel, A.; Davignon, J.-L.; Constantin, A. Traditional cardiovascular risk factors in rheumatoid arthritis: A meta-analysis. Jt. Bone Spine 2011, 78, 179–183. [CrossRef]
- Gianfrancesco, M.A.; Trupin, L.; Shiboski, S.; van der Laan, M.; Graf, J.; Imboden, J.; Yazdany, J.; Schmajuk, G. Smoking Is Associated with Higher Disease Activity in Rheumatoid Arthritis: A Longitudinal Study Controlling for Time-varying Covariates. J. Rheumatol. 2019, 46, 370–375. [CrossRef]
- Toms TE, Panoulas VF, Douglas KM, Griffiths H, Sattar N, Smith JP, Symmons DP, Nightingale P, Metsios GS, Kitas GD. Statin use in rheumatoid arthritis in relation to actual cardiovascular risk: evidence for substantial undertreatment of lipid-associated cardiovascular risk? Ann Rheum Dis. 2010 Apr; 69(4):683-8.
- Crowson C.S., Rollefstad S., Ikdahl E., Kitas G.D., van Riel P., Gabriel S.E., Matteson E.L., Kvien T.K., Douglas K., Sandoo A., et al. Impact of risk factors associated with cardiovascular outcomes in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2018; 77:48–54. [CrossRef]
- Di Giuseppe D., Discacciati A., Orsini N., Wolk A. Cigarette smoking and risk of rheumatoid arthritis: A dose-response meta-analysis. Arthritis Res. 2014; 16:R61. [CrossRef]
- Sugiyama D., Nishimura K., Tamaki K., Tsuji G., Nakazawa T., Morinobu A., Kumagai S. Impact of smoking as a risk factor for developing rheumatoid arthritis: A meta-analysis of observational studies. Ann. Rheum. Dis. 2010; 69:70–81. [CrossRef]
- Gianfrancesco M.A., Trupin L., Shiboski S., van der Laan M., Graf J., Imboden J., Yazdany J., Schmajuk G. Smoking Is Associated with Higher Disease Activity in Rheumatoid Arthritis: A Longitudinal Study Controlling for Time-varying Covariates. J. Rheumatol. 2019; 46:370–375. [CrossRef]
- Boyer J.-F., Gourraud P.-A., Cantagrel A., Davignon J.-L., Constantin A. Traditional cardiovascular risk factors in rheumatoid arthritis: A meta-analysis. Jt. Bone Spine. 2011; 78:179–183. [CrossRef]
- Hallajzadeh J., Safiri S., Mansournia M.A., Khoramdad M., Izadi N., Almasi-Hashiani A., Pakzad R., Ayubi E., Sullman M.J., Karamzad N. Metabolic syndrome and its components among rheumatoid arthritis patients: A comprehensive updated systematic review and meta-analysis. PLoS ONE. 2017; 12:e0170361. [CrossRef]
- Ford E.S. Risks for all-cause mortality, cardiovascular disease, and diabetes associated with the metabolic syndrome: A summary of the evidence. Diabetes Care. 2005; 28:1769–1778.
- Otterness IG. The value of C-reactive protein measurement in rheumatoid arthritis. Semin Arthritis Rheum. 1994; 24:91–104. [CrossRef]
- Nakajima T, Schulte S, Warrington KJ, Kopecky SL, Frye RL, Goronzy JJ, Weyand CM. T-cell-mediated lysis of endothelial cells in acute coronary syndromes. Circulation. 2002; 105:570–575. [CrossRef]
- Abbot SE, Whish WJ, Jennison C, Blake DR, Stevens CR. Tumour necrosis factor alpha stimulated rheumatoid synovial microvascular endothelial cells exhibit increased shear rate dependent leucocyte adhesion in vitro. Ann Rheum Dis. 1999;58:573–581. [CrossRef]
- Vaudo G, Marchesi S, Gerli R, Allegrucci R, Giordano A, Siepi D, Pirro M, Shoenfeld Y, Schillaci G, Mannarino E. Endothelial dysfunction in young patients with rheumatoid arthritis and low disease activity. Ann Rheum Dis. 2004; 63:31–35. [CrossRef]
- Hurlimann D, Forster A, Noll G, Enseleit F, Chenevard R, Distler O, Bechir M, Spieker LE, Neidhart M, Michel BA, et al. Anti-tumor necrosis factor-alpha treatment improves endothelial function in patients with rheumatoid arthritis. Circulation. 2002; 106: 2184–2187. [CrossRef]
- Van Leeuwen MA, van der Heijde DMFM, van Rijswijk MH, et al. Interrelationship of outcome measures and process variables in early rheumatoid arthritis: a comparison of radiologic damage, physical disability, joint counts, and acute phase reactants. J Rheumatol 1994;21:425-429.
- Naranjo A, Sokka T, Descalzo MA, Calvo-Alén J, Hørslev-Petersen K, Luukkainen RK, Combe B, Burmester GR, Devlin J, Ferraccioli G, Morelli A, Hoekstra M, Majdan M, Sadkiewicz S, Belmonte M, et al. Cardiovascular disease in patients with rheumatoid arthritis: Results from the quest-ra study. Arthritis Research; Therapy. 2008;10(2). [CrossRef]
- Mihaylova B, Emberson J, Blackwell L, Keech A, Simes J, Barnes EH, et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet (2012) 380:581–90.
- Minder CM, Blumenthal RS, Blaha MJ. Statins for primary prevention of cardiovascular disease. CurrOpinCardiol (2013) 28:554–60.
- Banach M, Serban C, Sahebkar A, Mikhailidis DP, Ursoniu S, Ray KK, et al. Impact of statin therapy on coronary plaque composition: a systematic review and meta-analysis of virtual histology intravascular ultrasound studies. BMC Med (2015) 13:229. [CrossRef]
- Rosenson RS. Statins in atherosclerosis: lipid-lowering agents with antioxidant capabilities. Atherosclerosis (2004) 173:1–12.
- Bedi O, Dhawan V, Sharma PL, Kumar P. Pleiotropic effects of statins: new therapeutic targets in drug design. NaunynSchmiedebergs Arch Pharmacol (2016) 389:695–712. [CrossRef]
- England BR, Thiele GM, Anderson DR, Mikuls TR. Increased cardiovascular risk in rheumatoid arthritis: Mechanisms and implications. BMJ. 2018. [CrossRef]
- Hermans, M.P.J.; van der Velden, D.; MonteroCabezas, J.M.; Putter, H.; Huizinga, T.W.J.; Kuiper, J.; Toes, R.E.M.; Schalij, M.J.; WouterJukema, J.; van der Woude, D. Long-term mortality in patients with ST-segment elevation myocardial infarction is associated with anti-citrullinated protein antibodies. Int. J. Cardiol. 2017, 240, 20–24. [CrossRef]
- Ciobanu D.A., Poenariu I.S., Crînguș L.-I., Vreju F.A., Turcu-Stiolica A., Tica A.A., Padureanu V., Dumitrascu R.M., Banicioiu-Covei S., Dinescu S.C., et al. JAK/STAT pathway in pathology of rheumatoid arthritis (Review) Exp. Ther. Med. 2020;20:3498–3503.
- Malemud C.J. The role of the JAK/STAT signal pathway in rheumatoid arthritis. Ther. Adv. Musculoskelet. Dis. 2018; 10:117–127. [CrossRef]
- Cojocaru M., Cojocaru I.M., Silosi I., Vrabie C.D., Tanasescu R. Extra-articular Manifestations in Rheumatoid Arthritis. Maedica. 2010;5:286–291.
- Visseren F.L.J., Mach F., Smulders Y.M., Carballo D., Koskinas K.C., Bäck M., Benetos A., Biffi A., Boavida J.-M., Capodanno D., et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies with the special contribution of the European Association of Preventive Cardiology (EAPC) Eur. Heart J. 2021;42:3227–3337. 3: 2021;42.
- Hansson G.K., Libby P., Tabas I. Inflammation and plaque vulnerability. J. Intern. Med. 2015; 278: 483–493. [CrossRef]
- Ocon, A.J.; Reed, G.; Pappas, D.A.; Curtis, J.R.; Kremer, J.M. Short-term dose and duration-dependent glucocorticoid risk for cardiovascular events in glucocorticoid-naive patients with rheumatoid arthritis. Ann. Rheum. Dis. 2021, 80, 1522. [CrossRef]
- Boers, M.; Hartman, L.; Opris-Belinski, D.; Bos, R.; Kok, M.; Pereira da Silva, J.; Griep, E.; Klaasen, R.A.C.; Baudoin, P.; Raterman, H.; et al. Favorable Balance of Benefit and Harm of Long-Term, Low Dose Prednisolone Added to Standard Treatment in Rheumatoid Arthritis Patients Aged 65+: The Pragmatic, Multicenter, Placebo-Controlled GLORIA Trial. Arthr. Rheumatol. 2021, 73.
- Bhala, N.; Emberson, J.; Merhi, A.; Abramson, S.; Arber, N.; Baron, J.A.; Bombardier, C.; Cannon, C.; Farkouh, M.E.; FitzGerald, G.A.; et al. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: Meta-analyses of individual participant data from randomised trials. Lancet 2013, 382, 769–779. [CrossRef]
- Kearney, P.M.; Baigent, C.; Godwin, J.; Halls, H.; Emberson, J.R.; Patrono, C. Do selective cyclo-oxygenase-2 inhibitors and traditional non-steroidal anti-inflammatory drugs increase the risk of atherothrombosis? Meta-analysis of randomised trials. BMJ 2006, 332, 1302–1308. [CrossRef]
- Nissen, S.E.; Yeomans, N.D.; Solomon, D.H.; Lüscher, T.F.; Libby, P.; Husni, M.E.; Graham, D.Y.; Borer, J.S.; Wisniewski, L.M.; Wolski, K.E.; et al. Cardiovascular Safety of Celecoxib, Naproxen, or Ibuprofen for Arthritis. N. Engl. J. Med. 2016, 375, 2519–2529. [CrossRef]
- Ungprasert P, Srivali N. Risk of incident atrial fibrillation in patients with rheumatoid arthritis: a systematic review and meta-analysis. Int J Rheum Dis. 2017;20(4):434–441. [CrossRef]
- Lindhardsen J, Ahlehoff O, Gislason GH, et al. Risk of atrial fibrillation and stroke in rheumatoid arthritis: Danish nationwide cohort study. BMJ. 2012; 8:344. [CrossRef]
- Kim SC, Liu J, Solomon DH. The risk of atrial fibrillation in patients with rheumatoid arthritis. Ann Rheum Dis. 2014;73(6):1091–1095. [CrossRef]
- Avina-Zubieta JA, Thomas J, Sadatsafavi M, Lehman AJ, Lacaille D. Risk of incident cardiovascular events in patients with rheumatoid arthritis: a meta-analysis of observational studies. Ann Rheum Dis. 2012; 71:1524–9. [CrossRef]
- C.M. Kahler, D. Colleselli Pulmonary arterial hypertension (PAH) in connective tissue diseases Rheumatology, 45 (2006), pp. 11-13.
Figure 1.
Comparison of atherogenic coefficient according to gender.

Table 1.
Gender and age distribution.
| Gender/Age group | Number of cases | Percentage |
|---|---|---|
| Female | 124 | 62% |
| Male | 76 | 38% |
| 40-49 years | 25 | 12.5% |
| 50-69 years | 112 | 56% |
| >70 years | 63 | 31.5% |
Table 2.
Distribution by stages of the disease.
| Stages of disease | Number of cases | Percentage |
|---|---|---|
| Stage I | 26 | 13% |
| Stage II | 38 | 19% |
| Stage III | 85 | 42.5% |
| Stage IV | 51 | 25.5% |
Table 3.
Distribution of patients depending on traditional CV risk factors and non-traditional risk factors.*Fisher’s Exact Test, **Mann-Whitney U Test.
Table 3.
Distribution of patients depending on traditional CV risk factors and non-traditional risk factors.*Fisher’s Exact Test, **Mann-Whitney U Test.
| Traditional CV risk factors | Men | Women | p |
|---|---|---|---|
| Smokers | 65.8% | 16.1% | <0.001* |
| Consumption of alcohol | 42.1% | 12.1% | <0.001* |
| High blood pressure | 89.4% | 30.6% | <0.001* |
| Hypercholesterolemia | 77.6% | 25.8% | <0.001* |
| Diabetes mellitus | 19.7% | 10.4% | 0.054* |
| Non-traditional risk factors | Men | Women | |
| CRP mg/l (Median (IQR)) | 123 (2-153.75) | 105.5 (3-116.5) | 0.006** |
| Fibrinogen g/l | 5.2 (5.1-5.2) | 4.6 (4.5-4.6) | <0.001** |
| Rheumatoid factor (RF) UI | 210 (205-216.75) | 119 (111-132) | <0.001** |
Table 4.
Distribution of patients by coronary artery disease.
| Monovascular coronary a. disease | Bivascular coronary a. disease | Trivascular coronary a. disease | |
|---|---|---|---|
| Men | 32 (42.1%) | 15 (19.7%) | 9 (11.8%) |
| Women | 30 (24.2%) | 12 (9.7%) | 5 (4%) |
Table 5.
Distribution of patients based on ECG changes, *Fisher’s Exact Test.
| ECG changes | Men | Women | p* |
|---|---|---|---|
| Sinus tachycardia | 19.7% | 20.2% | 1.000 |
| Left ventricular hypertrophy | 51.3% | 27.4% | 0.001 |
| Secondary ST-T changes | 39.5% | 26.6% | 0.062 |
| Atrial fibrillation | 17.1% | 32.3% | 0.021 |
| Supraventricular extrasystole | 26.3% | 17.7% | 0.210 |
| Left anterior fascicular block | 18.4% | 14.5% | 0.552 |
| Premature ventricular contraction | 15.8% | 11.3% | 0.391 |
| Left bundle branch block | 13.2% | 11.3% | 0.823 |
Table 6.
Distribution of patients based on the etiology of congestive heart failure.
| Etiological factors | Number of cases | Percentage |
|---|---|---|
| High blood pressure | 89 | 44.5% |
| Coronary artery disease | 35 | 17.5% |
| Valvular heart disease | 28 | 14% |
| Arrhythmias and conduction disorders | 15 | 7.5% |
Table 7.
Logistic regression models used for the prediction of cardiac complications.
| Pericarditis | ||||
| Parameter | Univariable | Multivariable | ||
| OR (95% C.I.) | p* | OR (95% C.I.) | p* | |
| HDL-cholesterol | 1.138 (0.996-1.301) | 0.057 | - | - |
| Atrial fibrillation | 2.279 (1.054-4.931) | 0.036 | - | - |
| Mitral valve prolapse | ||||
| LVH | 0.401 (0.186-0.867) | 0.020 | - | - |
| Mitral regurgitation | ||||
| CRP | 1.005 (1.001-1.009) | 0.019 | 1.005 (1.001-1.009) | 0.025 |
| Dyslipidemia – Triglycerides | 1.793 (1.019-3.154) | 0.043 | 1.760 (0.985-3.145) | 0.056 |
| HDL-cholesterol | 0.895 (0.800-1.002) | 0.055 | - | - |
| Secondary ST-T changes | 0.486 (0.259-0.910) | 0.024 | 0.522 (0.275-0.989) | 0.046 |
| Pulmonary arterial hypertension | ||||
| Rheumatoid factor | 1.008 (1.000-1.016) | 0.063 | - | - |
| HDL-cholesterol | 1.113 (0.979-1.264) | 0.102 | - | - |
| Pulmonary regurgitation | ||||
| Left bundle branch block | 7.264 (1.656-31.869) | 0.009 | - | - |
Table 9.
Logistic regression models used for the prediction of atrial fibrillation (*Multivariable model selected based on the Forward stepwise selection).
Table 9.
Logistic regression models used for the prediction of atrial fibrillation (*Multivariable model selected based on the Forward stepwise selection).
| Parameter | Univariable | Multivariable* | ||
| OR (95% C.I.) | p* | OR (95% C.I.) | p* | |
| Gender (Female) | 2.308 (1.139-4.674) | 0.020 | - | - |
| Smoking | 0.391 (0.186-0.820) | 0.013 | - | - |
| Hypertension | 0.479 (0.252-0.908) | 0.024 | - | - |
| Fibrinogen | 0.301 (0.107-0.845) | 0.023 | - | - |
| Rheumatoid factor | 1.009 (1.001-1.017) | 0.020 | - | - |
| Atherogenic coefficient | 0.720 (0.547-0.947) | 0.019 | - | - |
| Total cholesterol | 0.990 (0.982-0.998) | 0.011 | 0.991 (0.983-0.999) | 0.034 |
| Triglycerides | 0.991 (0.983-0.999) | 0.029 | - | - |
| LDL-cholesterol | 0.988 (0.979-0.997) | 0.012 | - | - |
| Coronary artery disease | 0.467 (0.245-0.890) | 0.021 | 0.507 (0.259-0.992) | 0.047 |
| Pericarditis | 2.279 (1.054-4.931) | 0.036 | 2.401 (1.078-5.350) | 0.032 |
Table 10.
Inflammation biomarkers in patients with rheumatoid arthritis.
| Inflammation biomarkers | Number of cases | Percentage |
|---|---|---|
| ESR | 140 | 70% |
| CRP | 131 | 65.5% |
Table 11.
Distribution of patients according to treatment.
| Therapy | Number of cases | Percentage |
|---|---|---|
| DMARDs | 200 | 100% |
| DMARDs +NSAIDs | 40 | 20% |
| DMARDs in monotherapy | 93 | 46.5% |
| DMARDs in dual therapy | 57 | 28.5% |
| MTX+HCQ+SSZ | 50 | 25% |
| Corticosteroids | 86 | 43% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



