Submitted:
13 September 2023
Posted:
19 September 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The coronavirus disease 2019 (COVID-19) pandemic clearly has had a great influence on the lifestyle of the population, especially on patients with type 2 diabetes mellitus. During the COVID-19 outbreak, many countries/regions implemented social isolation measures, leading to an increase in negative behaviors and impairing the capability of diabetic patients to resist the COVID-19, ultimately causing a severe prognosis. Moreover, multiple studies have emphasized the significance of physical exercise in the management of type 2 diabetic patients infected with COVID-19 as the epidemic progressed. In our study, we selected research focusing on COVID-19-infected diabetic patients from Dec 1, 2019 to Aug 9, 2023 and sought to investigate the impact of type 2 diabetes on the immune function, inflammation factor levels, lung injury and mental disorders of patients, as well as to assess the risk of novel coronavirus pneumonia in these patients. And we also summarized the effects of high-intensity, moderate-intensity and low-intensity exercise on novel coronavirus pneumonia infection in type 2 diabetic patients and the mechanisms of their effects. Finally, diabetic patients with COVID-19 are suggested to perform low-intensity exercise to facilitate their recovery. Our study offers guidance for a proper understanding of the dangers of diabetes and the use of appropriate measures to reduce the risk of novel coronavirus pneumonia infections in type 2 diabetic patients.
Keywords:
COVID-19
; physical activity
; diabetes
; immunity
; SARS-CoV-2
1. Introduction
Coronavirus disease 2019 (COVID-19) is a type of coronavirus (COV), a virus that was first identified in the 1960s and has caused large-scale epidemics in 2002-2003 (severe acute respiratory syndrome) and 2012 (Middle East respiratory syndrome) [1]. COVID-19 was declared a pandemic by the WHO in January 2020 [2], which led to over 630 million confirmed cases and over 6.58 million deaths by 9, Nov 2022. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the causative agent of the COVID-19 pandemic, which is an enveloped virus with a great, single-stranded, positive-sense RNA genome and consists of a spike protein (S), a membrane protein (M), a nucleocapsid protein (N), and an envelope protein (E) of the genus coronaviruses [1], which can be transmitted from person to person in a state of respiratory droplet and aerosol [3]. Conventionally, cough, sneeze, droplet inhalation, and touching mucous membranes are main modes of transmission [1]. Novel coronavirus pneumonia is a very dreadful pathogen and can induce respiratory failure, pneumonia, multi-organ failure and even death [4]. Some diseases, such as hypertension, diabetes and cardiovascular disease, especially type 2 diabetes, has been continuously demonstrated as risk factors for mortality and poor prognosis in COVID-19 patients [5]. Diabetes mellitus not only contributes to high mortality and poor prognosis in patients with novel coronavirus pneumonia, but also has deleterious effects on the host immune system, lungs, mood and inflammation levels [6, 7]. In several studies comparing non-diabetic patients infected with COVID-19 to those diabetic patients with COVID-19, non-diabetic patients infected with COVID-19 exhibited higher survival rates [8]. Therefore, understanding the mechanisms of damage and negative effects of type 2 diabetes is of crucial importance for the prophylaxis of novel coronavirus pneumonia infection in the diabetic population.
Despite the development of various vaccines for the treatment of COVID-19, there will always be a need for more cost-effective ways to prevent and treat SARS-CoV-2 virus and the ensuing disease COVID-19, especially in poor countries [9]. Physical exercises, including high-intensity, moderate-intensity and low-intensity exercise, are important tools for the prophylaxis and treatment of diabetes and novel coronavirus pneumonia infection [10]. These exercises are valuable, safe and effective for the management of diabetic patients, and could be extensively used during the COVID-19 outbreak to prevent patients from being infected. The beneficial effects of exercises are reflected in improved immune function [11], suppression of lung damage and reduction of inflammation factors [12, 13], anxiety and depression [14]. In diabetic patients, exercise has been demonstrated to play a role in controlling blood glucose levels and boosting immunity [15]. As suggested by Laddu, Lavie [16], moderate-intensity physical activity can effectively protect individuals against viral respiratory infections. Sellami, Gasmi [17] also indicated that chronic exercise and high-intensity exercise can promote immunity and prevent diseases. Endurance training is a kind of exercise that can improve the aerobic system and cardio-respiratory function along with the exercised muscles, such as treadmill walking, cycling, and swimming, while resistance training, also known as strength training, consists primarily of various forms of exercise that force skeletal muscles to contract in response to some force types that resist to the movement in the presence or absence of equipment, which includes free weights, weight machines, and elastic resistance bands [15]. Considering the intensity of exercise and the needs of diabetic patients infected with COVID-19 to improve cardiorespiratory fitness, enhance muscular endurance, improve blood circulation, and reduce the risk of obesity and diabetes, non-resistance exercises with multiple benefits were included in this study.
However, what is the link between exercise intensity and COVID-19 infection in type 2 diabetics? How does each type of exercise affect the health conditions of type 2 diabetes? These questions remain unanswered. Herein, we aim to investigate the significance of different intensity non-resistance exercises in type 2 diabetes to enhance the immune function, to protect against possible infections such as COVID-19, as well as to explore the potential mechanisms of these training methods, as possible interventions that could be used in the current pandemic stage. Our findings will be of interest for choosing the optimal exercise intensity to deal with type 2 diabetes and COVID-19 infections.
2. COVID-19 infection and diabetes
Diabetes, a disease of the endocrine system characterized by abnormally high blood glucose levels, is now one of the most common and fastest growing diseases worldwide [18]. According to Lukmanto, Nugroho [19], the number of patients with diabetes had reached 415 million in 2015, and this value is expected to increase to 642 million in 2040. Diabetes could be divided into four types, including type 1, type 2, gestational diabetes mellitus and other types of diabetes [20, 21]. Numerous studies have revealed that diabetic patients are positively correlated with a higher susceptibility to certain infectious diseases, including H1N1 influenza, Staphylococcus aureus and Mycobacterium tuberculosis, which may be attributed to the disordered immune system [22, 23]. Besides, COVID-19 has been thought to result in diabetes, further worsening the control of glycemic in patients with pre-existing diabetes [24]. Therefore, the global epidemic of COVID-19 might have direct implications for the progression, treatment and prognosis of type 2 diabetes mellitus. Herein, we described the relationship between diabetes and COVID-19 infection and the proportion and prognosis of diabetic patients among those infected with COVID-19 in some studies, aiming to improve the awareness of high infection and mortality rates caused by COVID-19 in type 2 diabetic patients and ultimately strengthen the protection of frail patients.
Many factors may contribute to the progression and poor prognosis of COVID-19, such as smoking, obesity, cardiovascular diseases and diabetes [25]. Among these pathogenic factors, several researches reported that diabetes was found to have deleterious effects on host immunity and was highly associated with increased susceptibility to pulmonary infection [26, 27], suggesting that hyperglycemia may be a major contributor to the increased risk of novel coronavirus pneumonia infections and enhanced odds of death in patients with novel coronavirus pneumonia. Emerging studies indicate that COVID-19 infection is more common in diabetic patients, although the prevalence rate varied in different researches and in country-wise data. Database from Chinese Centers for Disease Control and Prevention (CDC) suggested that 5% of the COVID-19 patients was also diagnosed with diabetes, while this value was 13% and 4% for hypertension and cardiovascular disease [28]. Other studies from China also indicated that diabetes was one of the most common comorbidities, with co-occurring cases of diabetes and COVID-19 accounting for 22%, 16.2% and 12% of all cases in the studies of Yang, Yu [29], Guan, Ni [30], and Zhang, Dong [31], respectively. A research conducted by Italy scholars revealed that diabetic patients accounted for nearly 17% among the 1043 COVID-19 patients [32]. The Indian researchers similarly found that the prevalence of hypertension, diabetes and cardiovascular disease were 21%, 11% and 7% in COVID-19 cases, respectively [33]. A US study reported the highest correlation between COVID-19 and diabetes among many comorbidities, with diabetics accounting for 58% of the COVID-19 patients investigated [34]. In contrast, a Chinese study reported the lowest correlation between COVID-19 and diabetes among several comorbidities, with diabetics accounting for 5.3% of the COVID-19 patients investigated [28]. Studies from different countries and different teams have demonstrated that diabetic patients are more likely to be infected with COVID-19, and the variation in percentage of diabetics in the patients with COVID-19 might be attributed to individual differences. Furthermore, a nationwide study conducted by England reported that there were independently correlations between type 2 diabetes with higher risk of odds of in-hospital death with the novel coronavirus pneumonia [35].
In addition to being highly associated with the prevalence of diabetes, coronavirus disease 2019 is also positively correlated with a poor prognosis of diabetes. The serious adverse prognosis involves severe diabetic complications, ICU admission, and high mortality [36, 37], and long-term risks, such as fatigue, dyspnea, muscle and joint pain, and inability to concentrate [24]. In addition to this, studies have shown an higher risk of new-onset hyperglycemia in patients with COVID-19 infection, which in turn leads to worsening glycemic control in patients with pre-existing diabetes [24]. That is, COVID-19 infections are mostly found in the diabetic population, leading to poor prognosis in these patients, including diabetic complications, ICU admission, new-onset diabetes and so on. New-onset diabetes further causes elevated blood glucose, while diabetic complications may lead to a weaker immune system, thereby reducing the resistance of patient to the novel coronavirus pneumonia and further increases the risk of novel coronavirus pneumonia infection.
A review revealed that the overall symptoms of patients suffering from both diabetes and novel coronavirus pneumonia showed no significant differences compared to those with COVID-19 infection only [38]. However, a total amount of 14.5% of the subjects were diabetic patients, they exhibited poor Acute Respiratory Distress Syndrome, severe symptoms, and showed a higher death rate compared to other COVID-19 patients. Similarly, a retrospective research conducted by Roncon, Zuin [37] showed that diabetes mellitus was the second most frequent comorbidity among 1382 patients. This study also reported that the COVID-19 patients with diabetes had a higher risk of ICU admission and mortality risk with a odds ratio of 2.79 and 3.21, respectively. Analysis of individuals infected with novel coronavirus pneumonia demonstrated that diabetic patients were associated with an increased possibility of novel coronavirus pneumonia infection and death and a poorer prognosis. Although most studies support a correlation between diabetes and novel coronavirus pneumonia infection, there are also some scholars who believe that diabetes may not increase the risk of coronavirus disease 2019 infection [24]. This can be attributed to the fact that diabetics are more aware of the risk of adverse outcomes of infection and are more easily to follow non-pharmacological measures, such as wearing masks and keeping social distance. Therefore, a more in-depth study on the relationship between type 2 diabetes and novel coronavirus pneumonia is needed to offer guidance on the use of medications as well as reducing the possibility of COVID-19 infection in type 2 diabetes with COVID-19.
3. Reasons for the increased diabetic susceptibility to COVID-19 infection
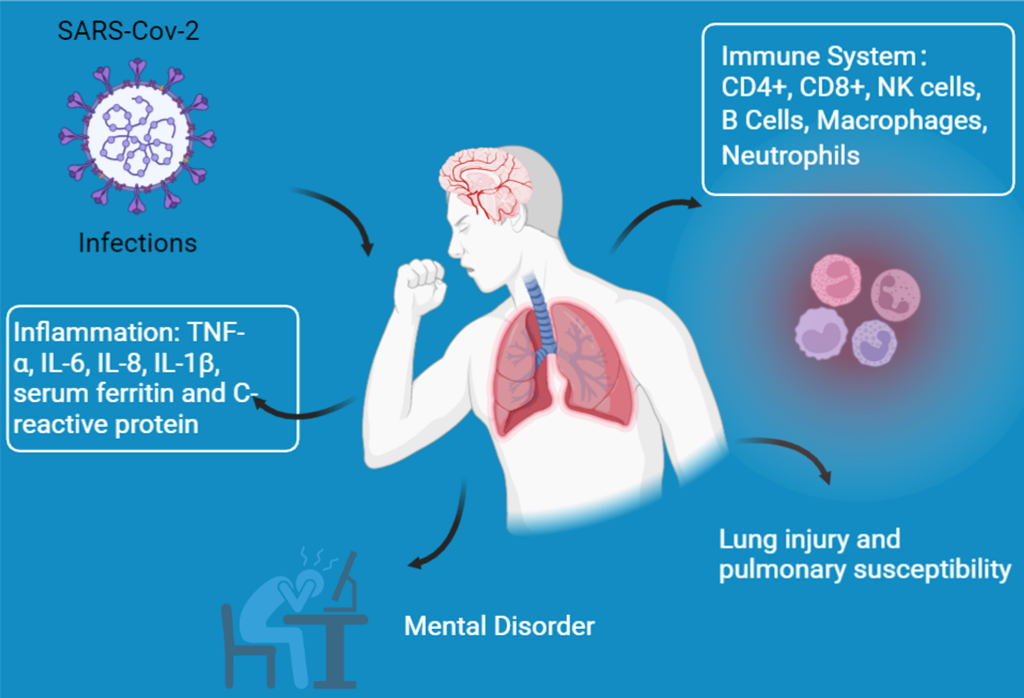
A variety of changes occur in diabetic patients that make them more susceptible to COVID-19 infection, as shown in Figure 1.
3.1. Immune system dysfunction
Generally, the human body could protect itself against the attack of toxins, parasites and microorganisms (such as bacteria, viruses and fungi) [39]. In normal conditions, the defense system of our body could prevent pathogens from penetrating this system, but the immune system may not work properly in some conditions, such as obesity, diabetes mellitus [40], hypertension, cardiovascular disease [41], and depression [42], causing the entry of bacteria, viruses and fungi into the body and finally leading to the development of a series of diseases [39]. Specially, diabetes exerts negative effects on the immune system, which includes disordered inflammation, impaired innate immunity and declining adaptive immunity [43]. According to the study of Frydrych, Bian [40], patients with type 2 diabetes are highly associated with physiologically frail and comorbidly challenging and are also recognized as the largest populations that suffer from post-infection complications and rising long-term mortality. Additionally, several scholars have reported that diabetes is highly correlated with an increased risk of viral infections, urinary tract infection, soft-tissue infections [44, 45], skin infections [43], and secondary infections [46] that may result in sepsis, renal failure and death. Among them, the respiratory infections caused by virus in patients with diabetes arouse increasing concern due to the popularity of novel coronavirus pneumonia. Fang, Karakiulakis [47] and Navand, Soltani [48] stated that the rate of influenza infection in patients with diabetes was 6 times higher than in the non-diabetic population, and the diabetes was highly correlated with an improved risk of viral respiratory diseases such as coronavirus. All of these studies have indicated that infection is a main problem in individuals with diabetes as a result of the inability of the defense system to fight off invading pathogens. Physical changes induced by diabetes that may affect COVID-19 infection are as shown in Table 1.
There is altered proliferation of T cells and macrophages and impaired function of NK cells and B cells in patients with diabetes, suggesting innate and adaptive immune abnormalities [59]. Besides, the underlying innate and adaptive immune system disorders in patients with diabetes promote infectious complications, impair sepsis recovery, and increase long-term mortality [60]. Diabetes is a complex clinical syndrome in which patients exhibit persistent hyperglycemia in the presence of reduced insulin secretion and sensitivity, causing aberrant metabolic changes, including increased accumulation of advanced glycosylation end products and flux through the polyol and hexosaine pathways as well as activation of protein kinase C isoforms [40, 61]. Finally, an upregulated NRLP3 pathway was observed in individuals with diabetes mellitus, which may also increase their susceptibility to COVID-19 infection [62]. These abnormal metabolic changes cause an increase in the production of superoxide, thereby activating inflammatory pathways, disrupting immune system, damaging lung tissues, worsening diabetes-related comorbidities, and ultimately leading to increased infectivity and virulence of SARS-CoV-2 in diabetes [3].
3.1.1. T Cells
T cells can be classified as helper (CD4+) T cells and cytotoxic (killer, CD8+) T cells and play an essential part in the development of diabetes mellitus [63]. Patients with type 2 diabetes mellitus generally exhibit over-activated and/or abnormally differentiated T cells and the activation of the inflammatory pathways [53, 55], indicating that the normal immune system is disrupted by high blood glucose content and causing the organism more susceptible to external viral infections. Among them, helper (CD4+) T cells can be further subdivided into pro-inflammatory Th1 and Th17 and anti-inflammatory Th2 and Foxp3+ regulatory T cell subsets according to different functions and types of cytokines produced [60]. Studies have shown that in peripheral blood and adipose tissue of type 2 diabetes mellitus, helper (CD4+) T cells are more easily to polarize to pro-inflammatory Th1 cells and Th17 cells, while the polarization of anti-inflammatory Th2 cells is significantly suppressed [64, 65]. The imbalance in the differentiation of helper (CD4+) T cells is also highly associated with an imbalance distribution of inflammatory factors. The study of Zhou, Chi [6] reported that in patients infected with SARS-CoV-2, the quantity of total T cells, and CD4+ and CD8+ T cell subsets were largely suppressed and functionally exhausted, while the control and clearance of pathogens were weakened in patients with diabetes mellitus, causing the inhibition of immune defences in response to the invasion of COVID-19. Asadikaram, Ram [66] and Sireesh, Dhamodharan [67] reported that Treg cells could produce CD4, CD25 and the forkhead family transcription factor Foxp3, which only account for 5-20% of the CD4+ compartment and play a crucial role in the suppression of effector T cell responses and limiting inflammation [68]. As suggested by Li, Zheng [69], patients with type 2 diabetes mellitus exhibited lower levels of Treg/Th17 and Treg/Th1 compared to normal individuals. Therefore, maintaining the balance between Treg, Th1 and Th17 cells is extremely important for the immune response in diabetic patients, which contributes to the prevention of novel coronavirus pneumonia infection in them.
CD8+ T cells also play an indispensable role in the process of adaptive immune against infections via synthesizing pro-inflammatory cytokine IL-17 and producing cytokines, including TNF-α and IFN-γ [49, 70]. Several scholars reported that increased proportions of CD8+ T cells and CD8+ T cells-derived cytokines were measured in patients with type 2 diabetes mellitus [49, 53]. These pro-inflammatory cytokines were distributed in numerous inflammatory tissues, which could aggravate inflammatory response and cause immune system imbalance. As suggested in a recent study, glucose metabolism disorder highly impaired the antiviral capacity of CD8+ T cells [71]. In detail, type 2 diabetes damaged CD8+ T cells mainly by affecting cell metabolism, memory formation, cytokine production or recall responses. Therefore, type 2 diabetic patients are more likely to be infected by novel coronavirus pneumonia due to impaired antiviral capacity of CD8+ T cells.
3.1.2. Natural Killer (NK) Cells
NK cells can be classified into two main subtypes and have shown to play an essential role in anti-tumor, hemopoietic regulation and primary control of acute viral infection, with their dysfunction thought to be highly associated with an increased risk of multiple infections [72, 73]. The activity of NK cells could be regulated by activating receptors, such as NKp30, NKp44, NKp46, NKG2C, and NKG2D. These receptors can attach to the ligands present on the surface of infected cells, finally causing the removal of invading bacteria [74]. According to previous studies, persistent hyperglycemia directly affected NK cells defects, thus damaging their function to prevent acute viral infection in the body [75]. Therefore, it can be speculated that the dysregulation of T cells and NK cells induced by diabetes, along with bacterial coinfection, are crucial causes of exacerbation of the SARS-CoV-2 infected the condition and death of patients. A study by Han, Ma [76] found that compared to non-diabetic COVID-19 patients, the counts of total T lymphocytes, CD4+ T cells, CD8+ T cells and NK cells were significantly suppressed in diabetic patients with novel coronavirus pneumonia. This finding suggests that the immune system can be highly affected by the disruption of glucose metabolism in diabetic patients, which in turn reduces the body's ability to defend itself against novel coronavirus pneumonia.
3.1.3. B Cells
B cells exert essential responsibilities in innate and adaptive immunity. It can act as antigen-presenting cells and produce cytokines in response to stimuli [77]. Besides, B cells are also emphasized to play a central role in the development of diabetes via the production of IgG antibodies, as well as the activation of T cells and macrophages [78]. Initial infection by a pathogen results in proliferation of antigen-specific T and B lymphocytes to control or kill the pathogen [79]. Finally, the immune system will develop a memory pool of antigen-specific adaptive immune cells, creating long-term protection against secondary encounters [80]. Thus, when the identical/antigenically similar pathogens attack the human body a second time, the rapid memory of the humoral and cellular arms of the adaptive immune system will be activated [80]. Several researches have also shown that reinfection with the same influenza virus strain can be inhibited or even prevented by antibody-mediated neutralization of viral particles (sterilizing immunity) in immunologically active hosts [81].
However, numerous studies have shown that type 2 diabetes impairs B-cell function and the accumulation of antibody, mainly in the form of impaired responsiveness towards viral infection, enhanced production of pro-inflammatory IL-8 and a failure to secrete anti-inflammatory IL-10, all of which are highly associated with inflammatory disease resolution [82, 83]. Moreover, Wu, Huang [83] reported that effective novel coronavirus pneumonia clearance needs both the action of CD8+ effector T cell-mediated effective killing of virally infected cells and CD4+ T cell-dependent enhancement of CD8+ T and B cell responses. As a result, impaired B-cell function affects the response of the immune system to the COVID-19 strains, impeding the interaction between B-cells and T-cells, ultimately leading to the invasion of the COVID-19 into the human body and causing positive infection, and delaying the clearance of COVID-19 virus in diabetic patients, eventually causing long-terms viral infections and ongoing symptoms [80, 84]. Besides, B-cell dysfunction caused by type 2 diabetes is also highly associated with secondary encounters of virus, and therefore it is expected that diabetic patients are more likely to have secondary infection with SARS-CoV-2 [40]. However, there is insufficient research regarding the linking between secondary COVID-19 infection and B cell dysfunctions in type 2 diabetic patients, and further studies are required to verify the results.
3.1.4. Macrophages
Macrophages are key mediators of inflammation and characterized by multiple surface markers and cytokine secretory patterns [60]. Generally, macrophages can be divided into two types, M1 or M2 cells, according to their surface phenotype [85]. The former one is triggered via several pro-inflammatory mediators, including LPS or IFN-γ, IL-6, IL-1β, and TNF-α, while the later is triggered by IL-4 and IL-13, thus secreting anti-inflammatory IL-10 and IL-1 and then blocking IL-1β and iNOS, which are important for tissue repair, angiogenesis, and resolution of inflammation [86].
Diabetes mellitus can influence the function of macrophages, thereby decreasing their capacity of bacteria recognition and phagocytosis [87, 88]. As indicated in the literature of Restrepo, Twahirwa [87], chronic hyperglycemia was greatly linked to impairment of phagocytosis, which can be reflected by drawbacks in complement and Fcγ receptors on isolated monocytes. Besides, the increased susceptibility of patients with diabetes to pathogens may be attributed to the activation of effector mechanisms for bacterial killing, which included the expression of pro-inflammatory cytokines, reactive oxygen species (ROS) and lysosomal enzymes. Pavlou, Lindsay [88] revealed that the antibacterial activity and phagocytosis of macrophages obtained from both mice bone and abdominal cavity was greatly suppressed in mice with diabetes. All these studies demonstrated that the diminished viral resistance to COVID-19 in diabetic patients may be attributed to the fact that diabetes impaired the function of macrophage.
3.1.5. Neutrophils
The presence of neutrophils is of vital importance for the containment and eradication of virus. They mainly exist in the bone marrow and exhibit antibacterial activity due to their specific proteins, including myeloperoxidase and calprotectin. According to the study of Frydrych, Bian [40], the patients with type 2 diabetes exhibit defects in almost all functions. Neutrophils migrate to the inflammation sites, release cytosolic proteases, exhibit phagocytosis and generate large amounts of ROS, thus promoting apoptosis. Furthermore, Baggiolini, Dewald [89] observed enhanced TNF-α, IL-1β, and IL-8 levels in neutrophils in patients with diabetes. The invasion of COVID-19 could impair the immune system of individuals with diabetes, especially the neutrophils, which can be reflected by their multiple function defects, such as migration to sites of inflammation, accumulation of ROS and apoptosis. These observations demonstrated that patients with diabetes had a higher possibility of neutrophil dysfunction, thereby upregulating the risk of infections.
3.2. Lung injury and pulmonary susceptibility
The novel coronavirus pneumonia attacks the human lungs, causing abnormalities in the physiology and structure of the lung tissue as well as impairing the function of the lung [90]. Meanwhile, several studies have also shown that diabetes is highly correlated with these abnormalities, suggesting that diabetes not only induces immunodeficiency, but also facilitates lung damage [6]. Zhao, Shi [91] demonstrated that type 2 diabetes mellitus was positively related to a high risk of pathogen infection, which caused inflammatory infiltration, cell apoptosis and fibrosis of lung tissues of mice, ultimately causing lung injury and increasing pulmonary susceptibility. Kruglikov, Shah [92] also stated that the invasion of the virus facilitated the interactions between ACE2 deficiency and diabetes, thus suppressing the synergistic effect between endothelial and gut barrier function, thereby inducing greater lung damage and pulmonary susceptibility in patients infected with COVID-19. Moreover, as suggested by Zheng, Wu [93] and Al-Kuraishy, Al-Gareeb [94], diabetes also induced the accumulation of ROS and pro-inflammation factors, leading to the lung injury of individuals with diabetes, including impaired respiratory system and interstitial lung injury. However, how the SARS-CoV-2 further exacerbates the lung injury and pulmonary susceptibility caused by diabetes needs to be further investigated.
3.3. Inflammation
A large body of studies also showed that diabetic patients suffered from long term low-grade chronic inflammation, which can trigger cytokine storms that may result in serve consequences of novel coronavirus pneumonia and ultimately death [6]. Several scholars have demonstrated that diabetic patients infected with COVID-19 are associated with severe inflammation and higher mortality. Besides, the inflammation markers, including serum ferritin and C-reactive protein, also largely increased in diabetes infected with SARS-CoV-2 [95]. Registry [96] found that diabetes infected with COVID-19 had higher concentrations of IL-6. Targher, Mantovani [97] reported that the concentrations of serum ferritin were greatly increased, which suggested the activation of the monocyte-macrophage system, a central part of the cytokine storms. Thus, both diabetes and novel coronavirus pneumonia may synergistically promote the inflammatory response in the human body. Moreover, the individuals with diabetes tend to have more comorbidities as a result of injured target organs. If diabetic patients then suffer from the invasion of novel coronavirus pneumonia, it may cause more severe inflammation, hypercoagulable state, and even hypoxia, ultimately resulting in a rapid progression of novel coronavirus pneumonia and higher mortality [95].
3.4. Other responses
Individuals with diabetes often suffer from two common mental health conditions: depression and anxiety [98]. Both of them will increase the risk of mortality, poor management of diabetes and diabetes-related complications, thereby worsening the disease progress. Prolonged depression and anxiety will lead to weaker immune response, which in turn increases the risk of novel coronavirus pneumonia infection [99, 100]. Furthermore, studies have also shown that the prevalence of novel coronavirus pneumonia also increases the risk of depression and anxiety, which further reduces the immunity of patients [101]. Additionaly, diabetes also influence the function of dendritic cells and γ-delta T cells [102, 103], which in turn affects the innate immunity and adaptive immunity of individuals, ultimately causing more sever novel coronavirus pneumonia infection. Nevertheless, there is not yet experimental data to confirm this view.
4. Physical activity improves the resistance of diabetics to COVID-19 infection
Exercise has been reported to exhibit well-established benefits for both healthy individuals and those with various diseases [104]. In particular, individuals with type 2 diabetes have been shown to benefit from exercise, as it can improve their immune function [105], lung function [106], the level of anti-inflammatory cytokines such as IL-4, IL-10 and lipocalin and health-related quality of life [107, 108], while reducing levels of inflammatory factors (TNF-α, IL-1β, and IL-6) and emotional burden [107, 119], thus maintaining a relatively good physical condition and a controlled glycemic status, ultimately protecting against COVID-19 virus invasion. In diabetic patients infected with COVID-19, exercise may prevent worsening of immune dysregulation and lung damage in these patients by restoring the proliferation and viability of T cells, macrophages, NK cells and B cells and reducing the accumulation of ROS, TNF-α, serum ferritin and C-reactive protein [76, 95], thus improving patient outcomes and speeding recovery. Additionally, diabetic patients participating in exercises have been shown to have acute improvements in insulin sensitivity and decreased body weight and blood glucose, blood lipids, and blood pressure levels [110, 111]. As indicated in section 3, the improved hyperglycemic and health status of diabetic patients contribute to restoring the function of the immune system, reducing lung injury and lung susceptibility, and lowering inflammatory factor levels, which eventually prevent the infection of COVID-19 and relieve the symptoms of patients after infection.
However, the emerging pandemic of novel coronavirus pneumonia induced by the SARS-CoV-2 limits people’s physical activity participation, which poses a major health, and economic burden worldwide. In many countries, a lot of restrictive measures, including quarantine, suspension of any social activities and closure of public areas, have been taken to prevent the spread of the COVID-19 virus. However, these restrictive measures decrease or even eliminate public access to physical activities, resulting in a decrease in the level of physical activity of populations during the COVID-19 pandemic [112]. The study of Amini, Isanejad [113] showed that the physical activity of the Iranian population decreased significantly and about 78% of the subjects could not meet the guidelines of physical activity during the COVID-19 pandemic. Similar observations were reported by Guthold, Stevens [114], who found that approximately 33% of the adult population of Iran did not meet the standard guidelines of physical activity during the period of COVID-19 pandemic. In addition to lack of exercise, many scholars also reported that a large number of populations exhibited higher prevalence of anxiety and depression during the COVID-19 pandemic, which may aroused from the fear of contracting the virus, the lack of effective treatment, the risk of death caused by the virus, and the uncertainty of controlling the virus [115]. A meta-analysis regarding the relationship between SARS-CoV-2 and psychological distress (anxiety and depression) conducted by Pappa, Ntella [116] suggested that the combined prevalence of anxiety was 23.2% in 12 researches, while the prevalence of depression was 22.8% in 10 studies. Elbay, Kurtulmuş [117] also conducted an online survey to evaluate psychological responses of healthcare workers and results revealed that among all the subjects (442 populations), 286 of them showed depression mood, 224 of the subjects had anxiety mood, and 182 of the cases were under stress during COVID-19 outbreak. These studies demonstrated a decrease in the number of exercise bouts and the total exercise duration and an increase in the psychological distress, including anxiety and depression during COVID-19 pandemics. Previous studies have reported that low frequency or even no exercise and psychological distress are highly associated with immune dysregulation, further causing serve immune-mediated inflammatory diseases and increasing the risk of novel coronavirus pneumonia infection [11].
Patients with diabetes generally exhibit a high incidence of novel coronavirus pneumonia infection and death, more severe infection symptoms, and a poorer prognosis [35, 37]. Some scholars have also demonstrated that among the many critical patients with novel coronavirus pneumonia, the percentage of the diabetics is higher, which is closely related to the low level of preexisting immunity, lung susceptibility and inflammation of the diabetics [118, 119]. Therefore, the lack of exercise and emotional anxiety or depression are of particular concern in the diabetic populations, which are positively correlated with low immunity, a high risk of novel coronavirus pneumonia infection, more severe infection symptoms and a poorer prognosis. Many scholars have widely studied the effects of non-resistance exercise on immunity and susceptibility to infection both before and after the COVID-19 pandemic. Herein, we collated the related information and challenges faced in high-intensity, moderate-intensity and low-intensity non-resistance exercises effectively affecting the COVID-19 infection.
4.1. High-intensity training
Performing regular exercise is beneficial for the prevention of diabetes mellitus and its complications, as well as improving immune response, susceptibility to infection, glycemic control and insulin sensitivity, ultimately increasing the resistance of patients with diabetes to COVID-19 virus [120]. However, there has been controversy about whether high-intensity exercise, mainly high-intensity interval training, contributes to improve the immunity system of diabetics and increase their resistance to novel coronavirus pneumonia infection.
High-intensity exercise was regarded as an exercise achieving a targeted heart rate equivalent to > 70% of their baseline VO2Max [17]. High-intensity interval training was defined by repeated bouts of high-intensity exercise interspersed with rest period, which is a really powerful exercise for altering body composition, reducing body weight, and improving cardiovascular, diabetes, and metabolism [121]. High-intensity interval training is a good alternative to moderate-intensity continuous training, but is more time-efficient than that exercise [122]. A number of scholars have suggested that strenuous exercise bouts or intensive training may be detrimental to the normal function of the immune system of human body, especially cellular and humoral immunity, upregulating the level of pro-inflammatory mediators and inducing apoptosis or long-term dysfunction of leukocytes, thereby possibly increasing the risk of COVID-19 infection [11, 123]. However, these claims still lack the conclusive support of direct evidence. As stated in the literature of Lancaster, Khan [124], prolonged exercise induced the frequency of leukocyte in blood increases, but this phenomenon backed to normal after exercise cessation. Moreover, exercise induced an increase in the level of cytokine production, proliferation, migration and cytotoxicity, and a decrease in the accumulation of IFN-α, which played an essential role in the upregulation of infection risk. Tuan, Hsu [123] also reported that high-intensity exercise for 3 consecutive days resulted in increased leukocyte apoptosis and TNF-α levels. These changes may result in the impaired immune function. Another study also stated that symptoms of infection were more common in athletes participating in long endurance sport events, such as marathon and ultramarathon, when compared to the control group that did not run. This may be attributed to the impairment of one or more protective mucous layers, and general host defenses (macrophage) [125]. However, all of the included studies had flaws that threaten the validity of the researches. First, although these studies suggested that prolonged exercise or endurance sports posed a threat to human health, such as increased level of cytotoxicity, and production of cytokine as well as decreased accumulation of IFN-α, a direct link between prolonged exercise and the increased risk of infection or poor prognosis caused by virus or bacteria is lacking. Second, these studies ignore the influence of other non-exercise factors, including sleep disruption, dietary changes, crowds gathering and psychological stress [11]. For example, participation in any mass participation activity increases the risk of encountering pathogens due to the crowd, regardless of whether the participants exercise or not. Therefore, based on the available studies, we can conclude that most of the studies supporting the detrimental effects of exercise on immunity has not been designed optimally to exclude the influence caused by other non-exercise factors. Secondly, other research supporting the harmful effects of exercise on COVID-19 infection is only speculative in the absence of supporting data [126]. The study of Simpson, Campbell [11] also concluded that the deleterious effects of exercise on immunity were negligible.
Other scholars have suggested that high-intensity exercise can reduce body weight, adipocytokine production, and the level of C-reactive protein, IL-6, IL-1β, TNF-α, leptin and resistin [107], increase neutrophil migration to CXCL-8 and the level of anti-inflammatory cytokines such as IL-4, IL-10 and lipocalin [130], improve oxidative stress, the ratio of Bacteroidetes-to-Firmicutes, glycemic control and insulin sensitivity to regulate immune response and improve the homeostasis of the internal environment [108, 129], thus reducing the risk of infection and diabetes [107], preventing the deterioration of inflammation, improving cardiopulmonary function and maintaining the stability of intestinal flora [108]. As indicated in the study of Robinson, Durrer [129], compared to moderate-intensity continuous training, short-term high-intensity interval training demonstrated better effect in activation of anti-inflammatory response, improving glucose control, insulin resistance-induced metabolic disorders and endothelial function and reducing the expression of Toll-like receptor (TLR) 2 (TLR2) and 4 (TLR4) on lymphocytes and monocytes in patients with type 2 diabetes. Bartlett, Slentz [127] also reported that after 10-weeks of high-intensity interval exercise training in diabetic patients, neutrophil dysfunction, glucose control and insulin sensitivity was improved, while ROS production was significantly reduced, thus decreasing the risk of infections and disease. Huang, Hsu [130] reported that diabetic patients with depression were associated with poor compliance of diabetes management and therapeutic effects, thus aggravating the symptoms of diabetes. However, high-intensity exercise could improve depression and reduce the glycemic levels of diabetics, creating a better general health condition than participants without exercise. Thus, we can conclude that high-intensity exercise can boost immune response, prevent infection, reduce inflammation and improve psychological distress (depression and anxiety), thereby improving the resistance of diabetics to COVID-19 infection. However, there were several studies suggested that high-intensity exercise was harmful to the immune system of diabetic patients, and was positively related to promoting the level of pro-inflammatory mediators and inducing apoptosis or long-term dysfunction of leukocytes, which may increase the risk of COVID-19 infection in diabetic patients [11]. Therefore, more research is needed to explore the direct effects of high-intensity exercise on the COVID-19 infection in patients with diabetes, and in-depth studies regarding the underlying mechanism of this process have also aroused the interest of many scholars.
4.2. Moderate-intensity exercise
Moderate-intensity exercise is regarded as an exercise that achieves a targeted heart rate equivalent to 40-70% of the individual’s baseline VO2Max [17]. Regarding the exercise intensity, moderate-intensity exercise is the most commonly performed exercise [131]. But whether higher-intensity exercise is more effective than moderate-intensity exercise in reducing the risk of diabetes, inflammation and mental disorders, improving the immune system and preventing COVID-19 infection? There are many controversial arguments and more research is needed to compare the respective advantages of these two types of exercise. Generally, moderate-intensity exercise can avoid over-training and overexertion, but enhance the immune response and reduce the risk of numerous diseases [132], while high-intensity exercise is positively related to increased pro-inflammatory factors and ROS accumulation [136, 134], and reduced levels of ainterferon gamma production [135]. Moreover, moderate-intensity exercise is also one of the main interventions for people with diabetes and obesity, in addition to appropriate dietary control [136]. However, there have been some studies argued that moderate-intensity exercise also has some disadvantages, such as high levels of apoptosis, poor glycemic control [137, 138], and low rates of exercise adherence [139]. Abraha, Chaves [140] also stated that the benefits of aerobic exercise seemed to be intensity-dependent, as several studies demonstrated that providing patients/populations with high-intensity aerobic exercise programs was superior to low-or moderate-intensity exercise.
However, other scholars have argued that moderate-intensity exercise could provide immuno-protective effects, such as increasing the quantity of natural killer cells, decreasing the concentrations of Tumor Necrosis Factor, and suppressing the level of inflammation, thus exhibiting its important role in preventing COVID-19 infection and improving diabetes [105]. Barrett, Hayney [141] and Dixit [105] also reported that moderate-intensity exercise can effectively prevent the incidence of acute respiratory disease and novel coronavirus pneumonia infection. These studies further revealed that moderate-intensity exercise exhibited active immune function and multiple health benefits, which can be reflected by the increased recirculation of immunoglobulins, higher levels of anti-inflammatory cytokines, neutrophils, NK cells and cytotoxic T cells [105]. Secondly, moderate-intensity exercise can positively affect the immune function of the human body, thus further improving its resistance to novel coronavirus pneumonia infection. Chamorro-Viña, Valentín [142] hold that aerobic exercise were associated with increasing levels of NK cells in human circulation, thus enhancing immune function and inhibiting susceptibility to infection. Khammassi, Ouerghi [143] indicated that moderate-intensity exercise had higher quantity of leukocyte, lymphocyte, neutrophil, and monocyte compared to high-intensity exercise, demonstrating better intervention effects in immune function. Thirdly, moderate-intensity training is also beneficial in reducing the emotional burden of patients, such as depression and anxiety mood in COVID-19 infected diabetics. As indicated in the literature of Borrega-Mouquinho, Sánchez-Gómez [109], both moderate-intensity and high-intensity exercise contributed to the reduction of anxiety, stress and depression of adults, although better effects seemed to be obtained in high-intensity exercise groups. Finally, moderate-intensity training also reduces pulmonary susceptibility, enhances pulmonary function and alleviates diabetes-related pulmonary complications in patients with diabetes, thereby improving their resistance to COVID-19 invasion. Halle, Bloch [106] reported that moderate-intensity training can effectively alleviate the pulmonary impairment of athletes caused by novel coronavirus pneumonia infection. Both high-intensity and moderate-intensity exercise could suppress excessive inflammation in the respiratory tract, thereby improving immune responses, promoting regulation of immune system and facilitating metabolic health. Therefore, we believe that both moderate-intensity exercise and high-intensity exercise have a variety of positive effects on the body, but different types of exercise are generally associated with different positive/negative effects, which in turns have different impacts on the ability of individuals to fight against virus.
4.3. Low-intensity exercise
Some scholars hold that excessive long term high-intensity exercise may lead to a down-regulation of immune function. Therefore, low-intensity exercise (<40% VO2Max) is suitable for those patients with chronic diseases and newcomers to exercise training, especially those with diabetes [17]. Hekmatikar, Shamsi [144] and Piquet, Luczak [145] recommended moderate-intensity training due to its effectiveness in increasing endorphins and decreasing stress, whereas low-intensity training was more suitable for people with COVID-19. A case study by Hekmatikar, Shamsi [144] demonstrated that low-intensity exercise accelerated the recovery from novel coronavirus pneumonia infection. Jesus, Vanhee [146] revealed that heavy exercise was highly related to immune dysfunction, increased levels of cytokines and higher risk of upper respiratory tract infections. Moreover, the activity of natural killer cells, T cells and B cells was greatly reduced. In terms of low-intensity exercises, Jesus, Vanhee [146] reported that long term adapted exercise was beneficial for the improvement of diabetes mellitus and the illness severity, viral load and anti-inflammatory effects of patients were significantly enhanced after a period of chronic exercise. Similarly, the novel coronavirus pneumonia-induced inflammation and viral respiratory infection were also suppressed in these patients. Low-intensity training is also effective in modulating immune responses and suppressing mental disorders, such as depression and anxiety, in normal individuals or diabetic patients, thus contributing to the prevention and recovery of COVID-19 infection. Rykova, Antropova [147] reported that after 8 weeks of low-intensity exercise, immunocompetent cells, such as CD3+, CD19+ and /CD56+ cells, were activated, while the degree of lymphocyte apoptosis was suppressed. Kimura [148] found that low-intensity exercise played a role in managing blood glucose levels and alleviating the progression of diabetes. As a results, the immune function and resistance to the COVID-19 might be increased in diabetes. Moreover, a study of Ji, Yang [149] indicated that low-intensity exercise can alleviate depressive symptoms, while the study conducted by Ji, Yang [149] reported that low-intensity training was effective in the treatment of raised anxiety. Tunkamnerdthai, Auvichayapat [150] demonstrated that arm swing exercise, a kind of low-intensity training, promoted the lung dysfunction in individuals with diabetes mellitus. In conclusion, the above studies prove that low-intensity exercise contributes to the reduction of anxiety and depression, prevention of lung damage, and enhancement of immune response, but the direct link between low-intensity exercise and diabetic patients infected with COVID-19 needs to be further explored.
5. Conclusion
The novel coronavirus pneumonia pandemic exhibits a negative impact on human health, especially in the diabetic population. The effects of diabetes on individuals with COVID-19 are reflected in the disruption of the immune system, disturbed inflammation levels and blood glucose levels, elevated lung susceptibility and lung damage, and the suppression of depression and anxiety. Exercise at different intensity levels, including high-intensity, moderate-intensity and low-intensity exercise, can compensate for the injury caused by COVID-19 in the type 2 diabetic population and have a positive effect on preventing infection and improving prognosis of COVID-19. We recommend low-intensity exercise for diabetic patients with COVID-19, which can accelerate their recovery from novel coronavirus pneumonia infection; for diabetic patients who wish to prevent COVID-19 infection, they are suggested to have low-intensity or moderate-intensity exercise that have a better intervention effects on immune function. High-intensity exercise is not recommended for patients with diabetes due to controversy regarding its potential harmful effects on the normal function of the immune system and and its ability to up-regulate the level of pro-inflammatory mediators and induce apoptosis. Nevertheless, more in-depth research is needed to assess which exercises are the most effective for patients with both SARS-CoV-2 and type 2 diabetes and to elucidate the underlying mechanism of exercise for the treatment of these patients.
Author Contributions
Conceptualization, L.-H.Y. and S.-N.L.; methodology, L.-H.Y.; validation, L.-H.Y., and S.-Y.G.; formal analysis, W.J.; investigation, H.-L.S.; resources, L.-H.Y.; data curation, L.-H.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This study has not received any funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The figure was created with BioRender software (https://BioRender.com).
Conflicts of Interest
All authors have no conflict of interest.
References
- Umakanthan, S.; Sahu, P.; Ranade, A.V.; Bukelo, M.M.; Rao, J.S.; Lf, A.-M.; Dahal, S.; Kumar, H.; Kv, D. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Heart 2020, 96, 753–758. [Google Scholar] [CrossRef]
- Harapan, H.; Itoh, N.; Yufika, A.; Winardi, W.; Keam, S.; Te, H.; Megawati, D.; Hayati, Z.; Wagner, A.L.; Mudatsir, M. Coronavirus disease 2019 (COVID-19): A literature review. J. Infect. Public Health 2020, 13, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Bundgaard, H.; et al. Effectiveness of adding a mask recommendation to other public health measures to prevent SARS-CoV-2 infection in Danish mask wearers: a randomized controlled trial. Annals of internal medicine 2021, 174, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Huang, I.; Lim, M.A.; Pranata, R. Diabetes mellitus is associated with increased mortality and severity of disease in COVID-19 pneumonia–a systematic review, meta-analysis, and meta-regression. Diabetes Metabolic Syndrome: Clinical Research Reviews 2020, 14, 395–403. [Google Scholar] [CrossRef]
- Umakanthan, S.; Senthil, S.; John, S.; Madhavan, M.K.; Das, J.; Patil, S.; Rameshwaram, R.; Cintham, A.; Subramaniam, V.; Yogi, M.; et al. The Effect of Statins on Clinical Outcome Among Hospitalized Patients With COVID-19: A Multi-Centric Cohort Study. Front. Pharmacol. 2022, 13, 742273. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; et al. Obesity and diabetes as high-risk factors for severe coronavirus disease 2019 (Covid-19). Diabetes/metabolism research and reviews 2021, 37, e3377. [Google Scholar] [CrossRef] [PubMed]
- Dantzer, C.; Swendsen, J.; Maurice-Tison, S.; Salamon, R. Anxiety and depression in juvenile diabetes: A critical review. Clin. Psychol. Rev. 2003, 23, 787–800. [Google Scholar] [CrossRef] [PubMed]
- Corona, G.; Pizzocaro, A.; Vena, W.; Rastrelli, G.; Semeraro, F.; Isidori, A.M.; Pivonello, R.; Salonia, A.; Sforza, A.; Maggi, M. Diabetes is most important cause for mortality in COVID-19 hospitalized patients: Systematic review and meta-analysis. Rev. Endocr. Metab. Disord. 2021, 22, 275–296. [Google Scholar] [CrossRef]
- Story, M.J. Essential sufficiency of zinc, ω-3 polyunsaturated fatty acids, vitamin D and magnesium for prevention and treatment of COVID-19, diabetes, cardiovascular diseases, lung diseases and cancer. Biochimie 2021, 187, 94–109. [Google Scholar] [CrossRef]
- Scartoni, F.R.; Sant’ana, L.d.O.; Murillo-Rodriguez, E.; Yamamoto, T.; Imperatori, C.; Budde, H.; Vianna, J.M.; Machado, S. Physical Exercise and Immune System in the Elderly: Implications and Importance in COVID-19 Pandemic Period. Front. Psychol. 2020, 11, 593903. [Google Scholar] [CrossRef]
- Simpson, R.J.; et al. Can exercise affect immune function to increase susceptibility to infection? Exercise immunology review 2020, 26, 8–22. [Google Scholar] [PubMed]
- Gleeson, M.; Bishop, N.C.; Stensel, D.J.; Lindley, M.R.; Mastana, S.S.; Nimmo, M.A. The anti-inflammatory effects of exercise: mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 2011, 11, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Golbidi, S.; Badran, M.; Laher, I. Antioxidant and Anti-Inflammatory Effects of Exercise in Diabetic Patients. Exp. Diabetes Res. 2011, 2012, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Salmon, P. Effects of physical exercise on anxiety, depression, and sensitivity to stress: A unifying theory. Clin. Psychol. Rev. 2001, 21, 33–61. [Google Scholar] [CrossRef] [PubMed]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [PubMed]
- Laddu, D.R.; Lavie, C.J.; Phillips, S.A.; Arena, R. Physical activity for immunity protection: Inoculating populations with healthy living medicine in preparation for the next pandemic. Prog. Cardiovasc. Dis. 2020, 64, 102–104. [Google Scholar] [CrossRef] [PubMed]
- Sellami, M.; et al. Effects of acute and chronic exercise on immunological parameters in the elderly aged: can physical activity counteract the effects of aging? Frontiers in immunology 2018, 9, 2187. [Google Scholar] [CrossRef]
- Zhang, Y.; et al. Regulation of NcRNA-protein binding in diabetic foot. Biomedicine Pharmacotherapy 2023, 160, 114361. [Google Scholar] [CrossRef] [PubMed]
- Lukmanto, R.B.; Suharjito; Nugroho, A. ; Akbar, H. Early Detection of Diabetes Mellitus using Feature Selection and Fuzzy Support Vector Machine. Procedia Comput. Sci. 2019, 157, 46–54. [Google Scholar] [CrossRef]
- Márquez-Valadez, B.; Valle-Bautista, R.; García-López, G.; Díaz, N.F.; Molina-Hernández, A. Maternal Diabetes and Fetal Programming Toward Neurological Diseases: Beyond Neural Tube Defects. Front. Endocrinol. 2018, 9, 664. [Google Scholar] [CrossRef]
- Wu, Y.; Lan, H.; Zhang, D.; Hu, Z.; Zhang, J.; Li, Z.; Xia, P.; Tang, X.; Cai, X.; Yu, P. Research progress on ncRNAs regulation of mitochondrial dynamics in diabetes. J. Cell. Physiol. 2022, 237, 4112–4131. [Google Scholar] [CrossRef] [PubMed]
- Allard, R.; Leclerc, P.; Tremblay, C.; Tannenbaum, T.-N. Diabetes and the Severity of Pandemic Influenza A (H1N1) Infection. Diabetes Care 2010, 33, 1491–1493. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Li, M.; Dong, Y.; Zhou, H.; Zhang, Z.; Tian, C.; Qin, R.; Wang, H.; Shen, Y.; Du, K.; et al. Diabetes is a risk factor for the progression and prognosis of COVID-19. Diabetes/Metabolism Res. Rev. 2020, 36, e3319. [Google Scholar] [CrossRef] [PubMed]
- Unnikrishnan, R.; Misra, A. Diabetes and COVID19: a bidirectional relationship. Nutr. Diabetes 2021, 11, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Framke, E.; Sørensen, J.K.; Andersen, P.K.; Svane-Petersen, A.C.; Alexanderson, K.; Bonde, J.P.; Farrants, K.; Flachs, E.M.; Hanson, L.L.M.; Nyberg, S.T.; et al. Contribution of income and job strain to the association between education and cardiovascular disease in 1.6 million Danish employees. Eur. Hear. J. 2019, 41, 1164–1178. [Google Scholar] [CrossRef] [PubMed]
- Hassan, A.O.; et al. A single-dose intranasal ChAd vaccine protects upper and lower respiratory tracts against SARS-CoV-2. Cell 2020, 183, 169–184.e13. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.; Huang, S.; Zhou, J. Perspectives of Antidiabetic Drugs in Diabetes With Coronavirus Infections. Front. Pharmacol. 2021, 11, 592439. [Google Scholar] [CrossRef]
- Team, E. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19)—China, 2020. China CDC weekly 2020, 2, 113. [Google Scholar]
- Yang, X.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. The Lancet Respiratory Medicine 2020, 8, 475–481. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. China Medical Treatment Expert Group for Covid-19. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Zhang, J.-J.; et al. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Gupta, R.; Misra, A. Comorbidities in COVID-19: Outcomes in hypertensive cohort and controversies with renin angiotensin system blockers. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Bhatraju, P.K.; Ghassemieh, B.J.; Nichols, M.; Kim, R.; Jerome, K.R.; Nalla, A.K.; Greninger, A.L.; Pipavath, S.; Wurfel, M.M.; Evans, L.; et al. Covid-19 in Critically Ill Patients in the Seattle Region—Case Series. N. Engl. J. Med. 2020, 382, 2012–2022. [Google Scholar] [CrossRef]
- Barron, E.; Bakhai, C.; Kar, P.; Weaver, A.; Bradley, D.; Ismail, H.; Knighton, P.; Holman, N.; Khunti, K.; Sattar, N.; et al. Associations of type 1 and type 2 diabetes with COVID-19-related mortality in England: a whole-population study. Lancet Diabetes Endocrinol. 2020, 8, 813–822. [Google Scholar] [CrossRef]
- Zhang, Y.; et al. Comorbid diabetes mellitus was associated with poorer prognosis in patients with COVID-19: a retrospective cohort study. MedRxiv, 2020.
- Roncon, L.; Zuin, M.; Rigatelli, G.; Zuliani, G. Diabetic patients with COVID-19 infection are at higher risk of ICU admission and poor short-term outcome. J. Clin. Virol. 2020, 127, 104354–104354. [Google Scholar] [CrossRef] [PubMed]
- Abdi, A.; Jalilian, M.; Sarbarzeh, P.A.; Vlaisavljevic, Z. Diabetes and COVID-19: A systematic review on the current evidences. Diabetes Res. Clin. Pr. 2020, 166, 108347–108347. [Google Scholar] [CrossRef] [PubMed]
- Berbudi, A.; et al. Type 2 diabetes and its impact on the immune system. Current diabetes reviews 2020, 16, 442. [Google Scholar]
- Frydrych, L.M.; Bian, G.; E O’lone, D.; A Ward, P.; Delano, M.J. Obesity and type 2 diabetes mellitus drive immune dysfunction, infection development, and sepsis mortality. J. Leukoc. Biol. 2018, 104, 525–534. [Google Scholar] [CrossRef]
- Petrie, J.; Guzik, T.J.; Touyz, R.M. Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mechanisms. Can. J. Cardiol. 2017, 34, 575–584. [Google Scholar] [CrossRef]
- Wang, J.; Zhou, D.; Dai, Z.; Li, X. Association Between Systemic Immune-Inflammation Index and Diabetic Depression. Clin. Interv. Aging 2021, 16, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Thurlow, L.R.; Stephens, A.C.; Hurley, K.E.; Richardson, A.R. Lack of nutritional immunity in diabetic skin infections promotes Staphylococcus aureus virulence. Sci. Adv. 2020, 6, eabc5569. [Google Scholar] [CrossRef]
- Prentice, B.J.; Jaffe, A.; Hameed, S.; Verge, C.F.; Waters, S.; Widger, J. Cystic fibrosis-related diabetes and lung disease: an update. Eur. Respir. Rev. 2021, 30, 200293. [Google Scholar] [CrossRef] [PubMed]
- Dryden, M.; Baguneid, M.; Eckmann, C.; Corman, S.; Stephens, J.; Solem, C.; Li, J.; Charbonneau, C.; Baillon-Plot, N.; Haider, S. Pathophysiology and burden of infection in patients with diabetes mellitus and peripheral vascular disease: focus on skin and soft-tissue infections. Clin. Microbiol. Infect. 2015, 21, S27–S32. [Google Scholar] [CrossRef] [PubMed]
- O’toole, P.; Maltenfort, M.G.; Chen, A.F.; Parvizi, J. Projected Increase in Periprosthetic Joint Infections Secondary to Rise in Diabetes and Obesity. J. Arthroplast. 2016, 31, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Fang, L.; Karakiulakis, G.; Roth, M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? The lancet respiratory medicine 2020, 8, e21. [Google Scholar] [CrossRef]
- Navand, A.H.; et al. Diabetes and coronavirus infections (SARS-CoV, MERS-CoV, and SARS-CoV-2). Journal of Acute Disease 2020, 9, 244. [Google Scholar]
- Zhao, R.; Sun, Y.; Zhang, Y.; Wang, W.; Wang, S.; Wang, C.; Liu, J.; Gao, L.; Hu, Z.; Fei, J.; et al. Distinguishable Immunologic Characteristics of COVID-19 Patients with Comorbid Type 2 Diabetes Compared with Nondiabetic Individuals. Mediat. Inflamm. 2020, 2020, 1–10. [Google Scholar] [CrossRef]
- Mobashir, M.; Helmi, N.; Alammari, D. Role of Potential COVID-19 Immune System Associated Genes and the Potential Pathways Linkage with Type-2 Diabetes. Comb. Chem. High Throughput Screen. 2022, 25, 2452–2462. [Google Scholar] [CrossRef] [PubMed]
- Alguwaihes, A.M.; Al-Sofiani, M.E.; Megdad, M.; Albader, S.S.; Alsari, M.H.; Alelayan, A.; Alzahrani, S.H.; Sabico, S.; Al-Daghri, N.M.; Jammah, A.A. Diabetes and Covid-19 among hospitalized patients in Saudi Arabia: a single-centre retrospective study. Cardiovasc. Diabetol. 2020, 19, 1–12. [Google Scholar] [CrossRef]
- Marfella, R.; D'Onofrio, N.; Sardu, C.; Scisciola, L.; Maggi, P.; Coppola, N.; Romano, C.; Messina, V.; Turriziani, F.; Siniscalchi, M.; et al. Does poor glycaemic control affect the immunogenicity of the COVID-19 vaccination in patients with type 2 diabetes: The CAVEAT study. Diabetes, Obes. Metab. 2021, 24, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Ye, S.; Wang, W.; Li, S.; Hu, Q.; Masaki, T. Clinical Features of COVID-19 Patients with Diabetes and Secondary Hyperglycemia. J. Diabetes Res. 2020, 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Nasr El-Din, A.; et al. Impact of high serum levels of MMP-7, MMP-9, TGF-β and PDGF macrophage activation markers on severity of COVID-19 in obese-diabetic patients. Infection and Drug Resistance 2021, 4015–4025. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, S.; Rankawat, G.; Singh, A.; Gupta, V.; Kakkar, S. Impact of glycemic control in diabetes mellitus on management of COVID-19 infection. Int. J. Diabetes Dev. Ctries. 2020, 40, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Yang, Y.; Wang, F.; Ren, H.; Zhang, S.; Shi, X.; Yu, X.; Dong, K. Clinical characteristics and outcomes of patients with severe covid-19 with diabetes. BMJ Open Diabetes Res. Care 2020, 8, e001343. [Google Scholar] [CrossRef]
- Al-Sofiani, M.E.; Albunyan, S.; Alguwaihes, A.M.; Kalyani, R.R.; Golden, S.H.; Alfadda, A. Determinants of mental health outcomes among people with and without diabetes during the COVID-19 outbreak in the Arab Gulf Region. J. Diabetes 2020, 13, 339–352. [Google Scholar] [CrossRef] [PubMed]
- Ajele, W.K.; Oladejo, T.A.; Akanni, A.A.; Babalola, O.B. Spiritual intelligence, mindfulness, emotional dysregulation, depression relationship with mental well-being among persons with diabetes during COVID-19 pandemic. J. Diabetes Metab. Disord. 2021, 20, 1705–1714. [Google Scholar] [CrossRef]
- Hodgson, K.; Morris, J.; Bridson, T.; Govan, B.; Rush, C.; Ketheesan, N. Immunological mechanisms contributing to the double burden of diabetes and intracellular bacterial infections. Immunology 2015, 144, 171–185. [Google Scholar] [CrossRef]
- McLaughlin, T.; Ackerman, S.E.; Shen, L.; Engleman, E. Role of innate and adaptive immunity in obesity-associated metabolic disease. J. Clin. Investig. 2017, 127, 5–13. [Google Scholar] [CrossRef]
- Brownlee, M. Biochemistry and molecular cell biology of diabetic complications. Nature 2001, 414, 813–820. [Google Scholar] [CrossRef]
- Lee, H.-M.; Kim, J.-J.; Kim, H.J.; Shong, M.; Ku, B.J.; Jo, E.-K. Upregulated NLRP3 Inflammasome Activation in Patients With Type 2 Diabetes. Diabetes 2012, 62, 194–204. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.S.; Ferreira, D.; Paige, E.; Gedye, C.; Boyle, M. Infectious Complications of Biological and Small Molecule Targeted Immunomodulatory Therapies. Clin. Microbiol. Rev. 2020, 33. [Google Scholar] [CrossRef]
- Nekoua, M.P.; et al. Modulation of immune cells and Th1/Th2 cytokines in insulin-treated type 2 diabetes mellitus. African health sciences 2016, 16, 712–724. [Google Scholar] [CrossRef]
- Sell, H.; Habich, C.; Eckel, J. Adaptive immunity in obesity and insulin resistance. Nat. Rev. Endocrinol. 2012, 8, 709–716. [Google Scholar] [CrossRef] [PubMed]
- Asadikaram, G.; et al. The study of the serum level of IL-4, TGF-β, IFN-γ, and IL-6 in overweight patients with and without diabetes mellitus and hypertension. Journal of Cellular Biochemistry 2019, 120, 4147–4157. [Google Scholar] [CrossRef] [PubMed]
- Sireesh, D.; Dhamodharan, U.; Ezhilarasi, K.; Vijay, V.; Ramkumar, K.M. Association of NF-E2 Related Factor 2 (Nrf2) and inflammatory cytokines in recent onset Type 2 Diabetes Mellitus. Sci. Rep. 2018, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Rudensky, A.Y. Foxp3 in control of the regulatory T cell lineage. Nat. Immunol. 2007, 8, 457–462. [Google Scholar] [CrossRef]
- Li, X.-Y.; et al. Treatment of foot disease in patients with type 2 diabetes mellitus using human umbilical cord blood mesenchymal stem cells: response and correction of immunological anomalies. Current Pharmaceutical Design 2013, 19, 4893–4899. [Google Scholar] [CrossRef]
- Zhao, K.; Ruan, S.; Yin, L.; Zhao, D.; Chen, C.; Pan, B.; Zeng, L.; Li, Z.; Xu, K. Dynamic regulation of effector IFN-γ-producing and IL-17-producing T cell subsets in the development of acute graft-versus-host disease. Mol. Med. Rep. 2015, 13, 1395–1403. [Google Scholar] [CrossRef]
- Kavazović, I.; Krapić, M.; Beumer-Chuwonpad, A.; Polić, B.; Wensveen, T.T.; Lemmermann, N.A.; van Gisbergen, K.P.; Wensveen, F.M. Hyperglycemia and Not Hyperinsulinemia Mediates Diabetes-Induced Memory CD8 T-Cell Dysfunction. Diabetes 2022, 71, 706–721. [Google Scholar] [CrossRef]
- Mazzoni, A.; Salvati, L.; Maggi, L.; Capone, M.; Vanni, A.; Spinicci, M.; Mencarini, J.; Caporale, R.; Peruzzi, B.; Antonelli, A.; et al. Impaired immune cell cytotoxicity in severe COVID-19 is IL-6 dependent. J. Clin. Investig. 2020, 130, 4694–4703. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Qin, C.-J.; Wu, M.-Z.; Liu, F.-F.; Liu, S.-S.; Liu, L. The Frequency of Natural Killer Cell Subsets in Patients with Acquired Immune Deficiency Syndrome with Deep Fungal Infections. Infect. Drug Resist. 2021, 14, 467–473. [Google Scholar] [CrossRef]
- Colucci, F.; Caligiuri, M.A.; Di Santo, J.P. What does it take to make a natural killer? Nature Reviews Immunology 2003, 3, 413–425. [Google Scholar] [CrossRef] [PubMed]
- Berrou, J.; Fougeray, S.; Venot, M.; Chardiny, V.; Gautier, J.-F.; Dulphy, N.; Toubert, A.; Peraldi, M.-N. Natural Killer Cell Function, an Important Target for Infection and Tumor Protection, Is Impaired in Type 2 Diabetes. PLOS ONE 2013, 8, e62418. [Google Scholar] [CrossRef] [PubMed]
- Han, M.; Ma, K.; Wang, X.; Yan, W.; Wang, H.; You, J.; Wang, Q.; Chen, H.; Guo, W.; Chen, T.; et al. Immunological Characteristics in Type 2 Diabetes Mellitus Among COVID-19 Patients. Front. Endocrinol. 2021, 12, 596518. [Google Scholar] [CrossRef]
- Shaikh, S.R.; Haas, K.M.; A Beck, M.; Teague, H. The effects of diet-induced obesity on B cell function. Clin. Exp. Immunol. 2014, 179, 90–99. [Google Scholar] [CrossRef] [PubMed]
- Winer, D.A.; Winer, S.; Shen, L.; Wadia, P.P.; Yantha, J.; Paltser, G.; Tsui, H.; Wu, P.; Davidson, M.G.; Alonso, M.N.; et al. B cells promote insulin resistance through modulation of T cells and production of pathogenic IgG antibodies. Nat. Med. 2011, 17, 610–617. [Google Scholar] [CrossRef] [PubMed]
- de Wit, J.; Souwer, Y.; Jorritsma, T.; Bos, H.K.; Brinke, A.T.; Neefjes, J.; van Ham, S.M. Antigen-Specific B Cells Reactivate an Effective Cytotoxic T Cell Response against Phagocytosed Salmonella through Cross-Presentation. PLOS ONE 2010, 5, e13016. [Google Scholar] [CrossRef]
- Pal, R.; Banerjee, M. Are people with uncontrolled diabetes mellitus at high risk of reinfections with COVID-19? Primary care diabetes 2021, 15, 18–20. [Google Scholar] [CrossRef]
- Chiu, C.; et al. B cell responses to influenza infection and vaccination. Influenza Pathogenesis and Control-Volume II, 2014: p. 381-398.
- Jagannathan, M.; McDonnell, M.; Liang, Y.; Hasturk, H.; Hetzel, J.; Rubin, D.; Kantarci, A.; Van Dyke, T.E.; Ganley-Leal, L.M.; Nikolajczyk, B.S. Toll-like receptors regulate B cell cytokine production in patients with diabetes. Diabetologia 2010, 53, 1461–1471. [Google Scholar] [CrossRef]
- Wu, Y.; Huang, X.; Sun, J.; Xie, T.; Lei, Y.; Muhammad, J.; Li, X.; Zeng, X.; Zhou, F.; Qin, H.; et al. Clinical Characteristics and Immune Injury Mechanisms in 71 Patients with COVID-19. mSphere 2020, 5, e00362–20. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; et al. Hypertension and diabetes delay the viral clearance in COVID-19 patients. MedRxiv, 2020.
- Cronstein, B.N.; Sitkovsky, M. Adenosine and adenosine receptors in the pathogenesis and treatment of rheumatic diseases. Nat. Rev. Rheumatol. 2016, 13, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Ravi, J.; Elbaz, M.; Wani, N.A.; Nasser, M.W.; Ganju, R.K. Cannabinoid receptor-2 agonist inhibits macrophage induced EMT in non-small cell lung cancer by downregulation of EGFR pathway. Mol. Carcinog. 2016, 55, 2063–2076. [Google Scholar] [CrossRef] [PubMed]
- Restrepo, B.I.; Twahirwa, M.; Rahbar, M.H.; Schlesinger, L.S. Phagocytosis via Complement or Fc-Gamma Receptors Is Compromised in Monocytes from Type 2 Diabetes Patients with Chronic Hyperglycemia. PLOS ONE 2014, 9, e92977. [Google Scholar] [CrossRef] [PubMed]
- Pavlou, S.; Lindsay, J.; Ingram, R.; Xu, H.; Chen, M. Sustained high glucose exposure sensitizes macrophage responses to cytokine stimuli but reduces their phagocytic activity. BMC Immunol. 2018, 19, 1–13. [Google Scholar] [CrossRef]
- Baggiolini, M.; Dewald, B.; Moser, B. Human Chemokines: An Update. Annu. Rev. Immunol. 1997, 15, 675–705. [Google Scholar] [CrossRef]
- Kida, K.; Utsuyama, M.; Takizawa, T.; Thurlbeck, W.M. Changes in Lung Morphologic Features and Elasticity Caused by Streptozotocin-induced Diabetes Mellitus in Growing Rats1–3. Am. Rev. Respir. Dis. 1983, 128, 125–131. [Google Scholar] [CrossRef]
- Zhao, H.; Shi, L.; Wang, X.; Yu, X.; Wang, D. Sp1 transcription factor represses transcription of phosphatase and tensin homolog to aggravate lung injury in mice with type 2 diabetes mellitus-pulmonary tuberculosis. Bioengineered 2022, 13, 9928–9944. [Google Scholar] [CrossRef]
- Kruglikov, I.L.; Shah, M.; E Scherer, P. Obesity and diabetes as comorbidities for COVID-19: Underlying mechanisms and the role of viral–bacterial interactions. eLife 2020, 9, e61330. [Google Scholar] [CrossRef]
- Zheng, H.; Wu, J.; Jin, Z.; Yan, L.-J. Potential Biochemical Mechanisms of Lung Injury in Diabetes. Aging Dis. 2017, 8, 7–16. [Google Scholar] [CrossRef]
- Al-Kuraishy, H.M.; Al-Gareeb, A.I.; Alblihed, M.; Cruz-Martins, N.; Batiha, G.E.-S. COVID-19 and Risk of Acute Ischemic Stroke and Acute Lung Injury in Patients With Type II Diabetes Mellitus: The Anti-inflammatory Role of Metformin. Front. Med. 2021, 8, 644295. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Du, Z.; Zhu, F. Glycosylated hemoglobin is associated with systemic inflammation, hypercoagulability, and prognosis of COVID-19 patients. Diabetes Res. Clin. Pr. 2020, 164, 108214–108214. [Google Scholar] [CrossRef] [PubMed]
- Registry, C.C.T., A multicenter, randomized controlled trial for the efficacy and safety of tocilizumab in the treatment of new coronavirus pneumonia (COVID-19), 2020.
- Targher, G.; Mantovani, A.; Wang, X.-B.; Yan, H.-D.; Sun, Q.-F.; Pan, K.-H.; Byrne, C.D.; Zheng, K.I.; Chen, Y.-P.; Eslam, M.; et al. Patients with diabetes are at higher risk for severe illness from COVID-19. Diabetes Metab. 2020, 46, 335–337. [Google Scholar] [CrossRef] [PubMed]
- Owens-Gary, M.D.; et al. The importance of addressing depression and diabetes distress in adults with type 2 diabetes. Journal of general internal medicine 2019, 34, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Xu, N.; Meng, H.; Liu, T.; Feng, Y.; Qi, Y.; Zhang, D.; Wang, H. Blueberry Phenolics Reduce Gastrointestinal Infection of Patients with Cerebral Venous Thrombosis by Improving Depressant-Induced Autoimmune Disorder via miR-155-Mediated Brain-Derived Neurotrophic Factor. Front. Pharmacol. 2017, 8, 853–853. [Google Scholar] [CrossRef] [PubMed]
- Jaremka, L.M.; Fagundes, C.P.; Glaser, R.; Bennett, J.M.; Malarkey, W.B.; Kiecolt-Glaser, J.K. Loneliness predicts pain, depression, and fatigue: Understanding the role of immune dysregulation. Psychoneuroendocrinology 2013, 38, 1310–1317. [Google Scholar] [CrossRef] [PubMed]
- Rudenstine, S.; et al. Depression and anxiety during the COVID-19 pandemic in an urban, low-income public university sample. Journal of Traumatic Stress 2021, 34, 12–22. [Google Scholar] [CrossRef]
- Gao, N.; Yan, C.; Lee, P.; Sun, H.; Yu, F.-S. Dendritic cell dysfunction and diabetic sensory neuropathy in the cornea. J. Clin. Investig. 2016, 126, 1998–2011. [Google Scholar] [CrossRef]
- Lu, H.; Liu, P.; Zhang, X.; Bao, T.; Wang, T.; Guo, L.; Li, Y.; Dong, X.; Li, X.; Dong, Y.; et al. Inulin and Lycium barbarum polysaccharides ameliorate diabetes by enhancing gut barrier via modulating gut microbiota and activating gut mucosal TLR2+ intraepithelial γδ T cells in rats. J. Funct. Foods 2021, 79, 104407. [Google Scholar] [CrossRef]
- Lukas, H.; Xu, C.; Yu, Y.; Gao, W. Emerging Telemedicine Tools for Remote COVID-19 Diagnosis, Monitoring, and Management. ACS Nano 2020, 14, 16180–16193. [Google Scholar] [CrossRef]
- Dixit, S. Can moderate intensity aerobic exercise be an effective and valuable therapy in preventing and controlling the pandemic of COVID-19? Medical hypotheses 2020, 143, 109854. [Google Scholar] [CrossRef] [PubMed]
- Halle, M.; et al. Exercise and sports after COVID-19—Guidance from a clinical perspective. Translational Sports Medicine 2021, 4, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Hopps, E.; Canino, B.; Caimi, G. Effects of exercise on inflammation markers in type 2 diabetic subjects. Acta Diabetol. 2011, 48, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Denou, E.; Marcinko, K.; Surette, M.G.; Steinberg, G.R.; Schertzer, J.D. High-intensity exercise training increases the diversity and metabolic capacity of the mouse distal gut microbiota during diet-induced obesity. Am. J. Physiol. Endocrinol. Metab. 2016, 310, E982–E993. [Google Scholar] [CrossRef]
- Borrega-Mouquinho, Y.; Sánchez-Gómez, J.; Fuentes-García, J.P.; Collado-Mateo, D.; Villafaina, S. Effects of High-Intensity Interval Training and Moderate-Intensity Training on Stress, Depression, Anxiety, and Resilience in Healthy Adults During Coronavirus Disease 2019 Confinement: A Randomized Controlled Trial. Front. Psychol. 2021, 12, 643069. [Google Scholar] [CrossRef]
- Stanford, K.I.; Goodyear, L.J. Exercise and type 2 diabetes: molecular mechanisms regulating glucose uptake in skeletal muscle. Adv. Physiol. Educ. 2014, 38, 308–314. [Google Scholar] [CrossRef]
- Seidu, S.; Khunti, K.; Yates, T.; Almaqhawi, A.; Davies, M.; Sargeant, J. The importance of physical activity in management of type 2 diabetes and COVID-19. Ther. Adv. Endocrinol. Metab. 2021, 12, 20420188211054686. [Google Scholar] [CrossRef] [PubMed]
- Amini, H.; Habibi, S.; Islamoglu, A.H.; Isanejad, E.; Uz, C.; Daniyari, H. COVID-19 pandemic-induced physical inactivity: the necessity of updating the Global Action Plan on Physical Activity 2018-2030. Environ. Health Prev. Med. 2021, 26, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Amini, H.; Isanejad, A.; Chamani, N.; Movahedi-Fard, F.; Salimi, F.; Moezi, M.; Habibi, S. Physical activity during COVID-19 pandemic in the Iranian population: A brief report. Heliyon 2020, 6, e05411. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- Lakhan, R.; Agrawal, A.; Sharma, M. Prevalence of depression, anxiety, and stress during COVID-19 pandemic. Journal of neurosciences in rural practice 2020, 11, 519–525. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Elbay, R.Y.; Kurtulmuş, A.; Arpacıoğlu, S.; Karadere, E. Depression, anxiety, stress levels of physicians and associated factors in Covid-19 pandemics. Psychiatry Res. 2020, 290, 113130. [Google Scholar] [CrossRef] [PubMed]
- Rohm, T.V.; et al. Inflammation in obesity, diabetes, and related disorders. Immunity 2022, 55, 31–55. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Gupta, M.; Katoch, N.; Garg, K.; Garg, B. A Systematic Review and Meta-analysis of Diabetes Associated Mortality in Patients with COVID-19. Int. J. Endocrinol. Metab. 2021, 19, e113220. [Google Scholar] [CrossRef]
- da Silva, D.E.; et al. High-intensity interval training in patients with type 2 diabetes mellitus: a systematic review. Current Atherosclerosis Reports 2019, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Guiraud, T.; Nigam, A.; Gremeaux, V.; Meyer, P.; Juneau, M.; Bosquet, L. High-Intensity Interval Training in Cardiac Rehabilitation. Sports Med. 2012, 42, 587–605. [Google Scholar] [CrossRef]
- Liu, J.; Zhu, L.; Su, Y. Comparative Effectiveness of High-Intensity Interval Training and Moderate-Intensity Continuous Training for Cardiometabolic Risk Factors and Cardiorespiratory Fitness in Childhood Obesity: A Meta-Analysis of Randomized Controlled Trials. Front. Physiol. 2020, 11, 214. [Google Scholar] [CrossRef] [PubMed]
- Tuan, T.-C.; Hsu, T.-G.; Fong, M.-C.; Hsu, C.-F.; Tsai, K.K.C.; Lee, C.-Y.; Kong, C.-W. Deleterious effects of short-term, high-intensity exercise on immune function: evidence from leucocyte mitochondrial alterations and apoptosis. Br. J. Sports Med. 2007, 42, 11–15. [Google Scholar] [CrossRef]
- Lancaster, G.I.; Khan, Q.; Drysdale, P.T.; Wallace, F.; Jeukendrup, A.E.; Drayson, M.T.; Gleeson, M. Effect of prolonged exercise and carbohydrate ingestion on type 1 and type 2 T lymphocyte distribution and intracellular cytokine production in humans. J. Appl. Physiol. 2005, 98, 565–571. [Google Scholar] [CrossRef]
- Peters, E.; Bateman, E. Ultramarathon running and upper respiratory tract infections-an epidemiological survey. South African Medical Journal 1983, 64, 582–584. [Google Scholar] [PubMed]
- Campbell, J.P.; Turner, J.E. Debunking the Myth of Exercise-Induced Immune Suppression: Redefining the Impact of Exercise on Immunological Health Across the Lifespan. Front. Immunol. 2018, 9, 648. [Google Scholar] [CrossRef]
- Bartlett, D.B.; Slentz, C.A.; Willis, L.H.; Hoselton, A.; Huebner, J.L.; Kraus, V.B.; Moss, J.; Muehlbauer, M.J.; Spielmann, G.; Muoio, D.M.; et al. Rejuvenation of Neutrophil Functions in Association With Reduced Diabetes Risk Following Ten Weeks of Low-Volume High Intensity Interval Walking in Older Adults With Prediabetes – A Pilot Study. Front. Immunol. 2020, 11, 729. [Google Scholar] [CrossRef] [PubMed]
- Von Ah Morano, A.E.; Dorneles, G.P.; Peres, A.; Lira, F.S. The role of glucose homeostasis on immune function in response to exercise: The impact of low or higher energetic conditions. J. Cell. Physiol. 2020, 235, 3169–3188. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Durrer, C.; Simtchouk, S.; Jung, M.E.; Bourne, J.E.; Voth, E.; Little, J.P. Short-term high-intensity interval and moderate-intensity continuous training reduce leukocyte TLR4 in inactive adults at elevated risk of type 2 diabetes. J. Appl. Physiol. 2015, 119, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.-C.; Hsu, C.-C.; Chiu, C.-C.; Lin, H.-J.; Wang, J.-J.; Weng, S.-F. Association between exercise and health-related quality of life and medical resource use in elderly people with diabetes: a cross-sectional population-based study. BMC Geriatr. 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Li, F. Physical activity and health in the presence of China's economic growth: meeting the public health challenges of the aging population. Journal of sport and health science 2016, 5, 258–269. [Google Scholar] [CrossRef]
- Cerqueira, É.; Marinho, D.A.; Neiva, H.P.; Lourenço, O. Inflammatory Effects of High and Moderate Intensity Exercise—A Systematic Review. Front. Physiol. 2020, 10, 1550. [Google Scholar] [CrossRef]
- Radak, Z.; Ishihara, K.; Tekus, E.; Varga, C.; Posa, A.; Balogh, L.; Boldogh, I.; Koltai, E. Exercise, oxidants, and antioxidants change the shape of the bell-shaped hormesis curve. Redox Biol. 2017, 12, 285–290. [Google Scholar] [CrossRef]
- Cobianchi, S.; Arbat-Plana, A.; Lopez-Alvarez, V.M.; Navarro, X. Neuroprotective Effects of Exercise Treatments After Injury: The Dual Role of Neurotrophic Factors. Curr. Neuropharmacol. 2017, 15, 495–518. [Google Scholar] [CrossRef] [PubMed]
- Zar, A.; Ahmadi, F.; Miri, M.; Abedi, H.A.; Salesi, M. Cytokine Pattern is Affected by Training Intensity in Women Futsal Players. Immune Netw. 2016, 16, 109–115. [Google Scholar] [CrossRef]
- Wing, R.R.; Epstein, L.H.; Paternostro-Bayles, M.; Kriska, A.; Nowalk, M.P.; Gooding, W. Exercise in a behavioural weight control programme for obese patients with Type 2 (non-insulin-dependent) diabetes. Diabetologia 1988, 31, 902–909. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Liu, J.; Yan, H. Medium-intensity acute exhaustive exercise induces neural cell apoptosis in the rat hippocampus. Neural regeneration research 2013, 8, 127–132. [CrossRef]
- Parker, L.; Shaw, C.S.; Banting, L.; Levinger, I.; Hill, K.M.; McAinch, A.J.; Stepto, N.K. Acute Low-Volume High-Intensity Interval Exercise and Continuous Moderate-Intensity Exercise Elicit a Similar Improvement in 24-h Glycemic Control in Overweight and Obese Adults. Front. Physiol. 2017, 7, 661. [Google Scholar] [CrossRef] [PubMed]
- Vickers, K.S.; Patten, C.A.; Lewis, B.A.; Clark, M.M.; Ussher, M.; Ebbert, J.O.; Croghan, I.T.; Decker, P.A.; Hathaway, J.; Marcus, B.H.; et al. Feasibility of an exercise counseling intervention for depressed women smokers. Nicotine Tob. Res. 2009, 11, 985–995. [Google Scholar] [CrossRef] [PubMed]
- Abraha, B.; Chaves, A.R.; Kelly, L.P.; Wallack, E.M.; Wadden, K.P.; McCarthy, J.; Ploughman, M. A Bout of High Intensity Interval Training Lengthened Nerve Conduction Latency to the Non-exercised Affected Limb in Chronic Stroke. Front. Physiol. 2018, 9, 827. [Google Scholar] [CrossRef] [PubMed]
- Barrett, B.; Hayney, M.S.; Muller, D.; Rakel, D.; Brown, R.; Zgierska, A.E.; Barlow, S.; Hayer, S.; Barnet, J.H.; Torres, E.R.; et al. Meditation or exercise for preventing acute respiratory infection (MEPARI-2): A randomized controlled trial. PLOS ONE 2018, 13, e0197778. [Google Scholar] [CrossRef]
- Chamorro-Viña, C.; Valentín, J.; Fernández, L.; González-Vicent, M.; Pérez-Ruiz, M.; Lucía, A.; Culos-Reed, S.N.; Díaz, M. .; Pérez-Martínez, A. Influence of a Moderate-Intensity Exercise Program on Early NK Cell Immune Recovery in Pediatric Patients After Reduced-Intensity Hematopoietic Stem Cell Transplantation. Integr. Cancer Ther. 2016, 16, 464–472. [Google Scholar] [CrossRef]
- Khammassi, M.; Ouerghi, N.; Said, M.; Feki, M.; Khammassi, Y.; Pereira, B.; Thivel, D.; Bouassida, A. Continuous Moderate-Intensity but Not High-Intensity Interval Training Improves Immune Function Biomarkers in Healthy Young Men. J. Strength Cond. Res. 2020, 34, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Hekmatikar, A.H.A.; et al. Exercise in an overweight patient with COVID-19: a case study. International Journal of Environmental Research and Public Health 2021, 18, 5882. [Google Scholar] [CrossRef] [PubMed]
- Piquet, V.; Luczak, C.; Seiler, F.; Monaury, J.; Martini, A.; Ward, A.B.; Gracies, J.-M.; Motavasseli, D.; Lépine, E.; Chambard, L.; et al. Do Patients With COVID-19 Benefit from Rehabilitation? Functional Outcomes of the First 100 Patients in a COVID-19 Rehabilitation Unit. Arch. Phys. Med. Rehabilitation 2021, 102, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Jesus, I.; Vanhee, V.; Deramaudt, T.B.; Bonay, M. Promising effects of exercise on the cardiovascular, metabolic and immune system during COVID-19 period. J. Hum. Hypertens. 2020, 35, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Rykova, M.; et al. The activation processes of the immune system during low intensity exercise without relaxation. Rossiiskii Fiziologicheskii Zhurnal Imeni IM Sechenova 2008, 94, 212–219. [Google Scholar]
- Kimura, A. IDF21-0163 The usefulness of low-intensity physical activity management for malaise in type 2 diabetic patients after ablation. Diabetes Res. Clin. Pract. 2022, 186. [Google Scholar] [CrossRef]
- Ji, C.; Yang, J.; Lin, L.; Chen, S. Physical Exercise Ameliorates Anxiety, Depression and Sleep Quality in College Students: Experimental Evidence from Exercise Intensity and Frequency. Behav. Sci. 2022, 12, 61. [Google Scholar] [CrossRef] [PubMed]
- Tunkamnerdthai, O.; Auvichayapat, P.; Donsom, M.; Leelayuwat, N. Improvement of pulmonary function with arm swing exercise in patients with type 2 diabetes. J. Phys. Ther. Sci. 2015, 27, 649–654. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Reasons for the increased diabetic susceptibility to COVID-19 infection.
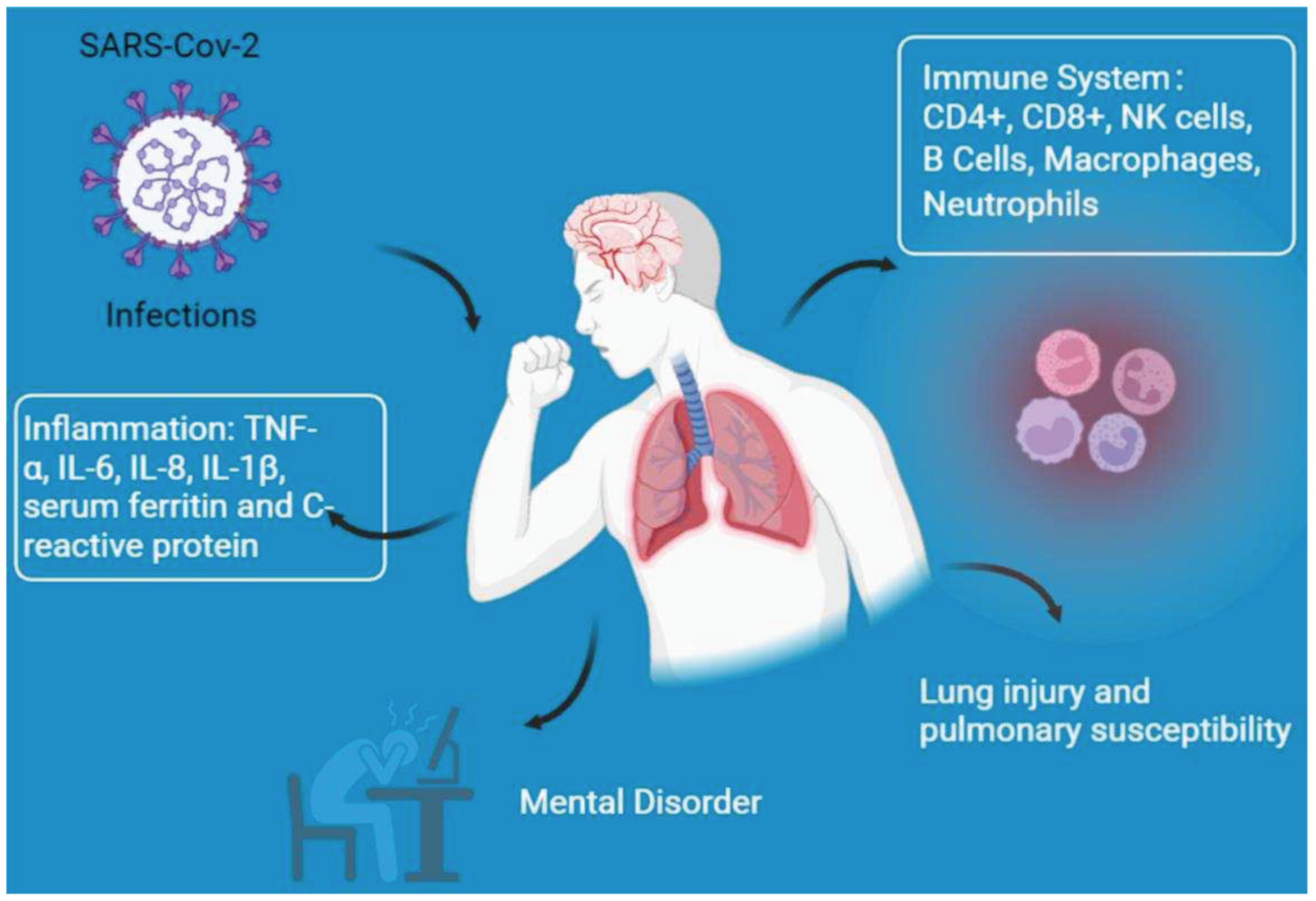

Table 1.
Physical changes induced by diabetes that affect COVID-19 infection.
| Model | Age | Research findings | Reference |
|---|---|---|---|
| HWD | NDM: 62.1 T2DP: 63.4 | Neutrophil, LS, IgE, IFN-γ, TNF-α, IL-6 ↑ T, Tc, Th, and NK cells ↓ |
[49] |
| Diabetic patients | SMARCD3, PARL, GLIPR1, STAT2, PMAIP1, GP1BA, and TOX genes and PI3K-Akt, focal adhesion, Foxo, phagosome, adrenergic, osteoclast differentiation, platelet activation, insulin, cytokine- cytokine interaction, apoptosis, ECM, JAK-STAT, and oxytocin signaling were the linkage between COVID-19 and Type-2 diabetes | [50] | |
| Diabetic patients | Median age: 55 | Creatinine, neutrophil, creatinine, alanine aminotransferase ↑ | [51] |
| HWD | Range from 18 to 60 | CD4+ T cells, CD4+/TNF-α, CD4+/IL-2, CD4+/IFN-γ ↓ | [52] |
| HWD | Median age: 47 | CD3+, CD4+, CD4+/CD8+ ↑ hs-CRP、LDH、IL-6、CD8+ ↓ |
[53] |
| HWD | MMP-7, MMP-9, PDGF and TGF-β ↑ LBP↓ |
[54] | |
| PUCD | Median age: 61.45 | uncontrolled inflammatory responses, leukocyte, neutrophil-lymphocyte ratio, IL-6, FDP, D-dimer ↑ pulmonary invasion |
[55] |
| Patients with severe covid-19 | Median age: 64 | Susceptible to receiving mechanical ventilation and admission to ICU Mortality, leukocyte, neutrophil, high-sensitivity C reaction protein, procalcitonin, ferritin, IL-2 receptor, IL-6, IL-8, TNF-α, D-dimer, fibrinogen, lactic dehydrogenase and N-terminal pro-brain natriuretic peptide ↑ |
[56] |
| HWD | Depression and anxiety ↑ | [57] | |
| HWD | Median age: 40.31 | Emotional dysregulation Depression ↑ |
[58] |
HWD: human with or without diabetes; PUCD: patients with uncontrolled and controlled diabetes; MERS-CoV: Middle East respiratory syndrome coronavirus; Tc: cytotoxic T; Th: helper T; NKT: Natural killer cells; LS: lymphocyte subpopulations; NDM: non-diabetic participants; T2DP: participants with type 2 diabetes; MMP: matrix metalloproteinase; LBP: lipopolysaccharide-binding protein; TNF-α: tumor necrosis factor; LDH: Lactate dehydrogenase.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



