Submitted:
18 September 2023
Posted:
19 September 2023
You are already at the latest version
Abstract
Cardiovascular diseases (CVD) are prevalent and lead to high morbidity and mortality globally. Physiotherapists regularly interact with patients with or at risk of CVDs (pwCVDs). This study aimed to assess the nature of existing evidence, interventional approaches used, and the population groups included in physiotherapy-led health promotion (PLHP) for pwCVDs. The scoping review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines. Medline, PubMed, Web of Science, Cochrane Central Register of Controlled Trials, CINAHL, and PEDro databases were searched from inception until June 2023. Two reviewers independently screened the titles, abstracts, full text and conducted data extraction. All conflicts were resolved with a third reviewer. A total of 4992 records were identified, of which 20 full-text articles were included in the review. The studies had varied populations, including those with stroke, coronary artery diseases, peripheral artery diseases, hypertension, diabetes, and multiple CVD risk factors. The interventions ranged from exercise and physical activity programs, dietary interventions, education, and counselling sessions with various supplementary approaches. Most interventions were short-term, with less than 12 months of follow-up. Interventions were personalised and patientcentred to promote adherence and health behaviour change. Among the included studies, 60% employed experimental designs, with the remainder using quasi-experimental designs. Although a wide range of PLHP strategies have been used for pwCVDs, exercise and physical activity were employed in 85% of included studies. Other components of health promotion, such as sleep, smoking, and alcohol abuse, should be investigated within PLHP.
Keywords:
physiotherapy
; health promotion
; cardiovascular diseases
; risk factors
; Interventions
1. Introduction
Cardiovascular disease (CVD) includes all diseases that affect the cardiovascular system (the heart and blood vessels). CVD is the leading cause of disability and mortality globally [1] and accounts for the highest proportion (44%) of chronic non-communicable disease (CNCD) deaths annually [2] and 32% of all deaths globally [3,4]. CVDs are associated with severe social consequences, including reduced quality of life and economic growth, and consume many health service resources in developing and developed countries [5,6].
Annually, approximately 15 million people globally suffer a stroke [7], estimated to rise to 77 million by 2030 [8]. The cumulative risk of stroke recurrence at five years is 1.3%, and at ten years is 39.2% [9], with a higher death and disability rate associated with recurrent stroke [10]. CNCDs are associated with multiple risk factors, including genetics and environmental factors, metabolic factors (hypertension, diabetes, abnormal lipids, obesity) and behavioural factors (tobacco use, unhealthy diet, physical inactivity) [11]. These risk factors are drivers of the global CVD epidemic [6,12]. A global study in 52 countries identified similar risk factors for heart diseases in low- and high-income countries [12]. However, over three-quarters of the global burden of CVD is from low- and medium-income countries (LMICs) with rising incidence [13,14].
The effectiveness of lifestyle changes and physical interventions are well established in primary, secondary and tertiary prevention of CVDs [15,16]. Primary prevention aims to reduce the incidence of an index cardiovascular event, especially in at-risk people [11,17]. Secondary and tertiary prevention programmes are often provided at specialised cardiac rehabilitation (CR) centres and directed towards reducing the recurrence of cardiac events, restoring patients' quality of life, improving functional capacity, stress and self-management techniques and promoting a healthy lifestyle [18]. There is evidence that cardiovascular mortality can be reduced and signs and symptoms of established CVD improved by addressing behavioural risk factors such as unhealthy diet [19], physical inactivity [20], harmful use of alcohol [21], tobacco use [22], inadequate sleep [23] and poor stress management [3,24,25]. Adopting these preventive strategies may reduce the incidence of heart disease [26,27].
Physiotherapists play a role in reducing risk and managing patients at risk or with established CVD (pwCVDs) [28,29,30]. Despite the substantial burden of CVDs and the evidence supporting cardiac rehabilitation (CR) in preventing and managing CVDs, many LMICs do not have existing structures and programs promoting the prevention and rehabilitation of pwCVDs [18,31,32]. CR services are available in 80% of European countries but only 17% of African countries [31]. CR services are rare in LMICs for several reasons, including lack of personnel resources, competing priorities, affordability issues, and insurance coverage [32]. Physiotherapists in LMIC settings receive pwCVDs in their practice, providing an opportunity to provide CR-related interventions through health promotion. The contact time and frequent visits make them well-placed to provide physiotherapy-led health promotion (PLHP) to facilitate the adoption of healthier lifestyle choices and support patients to return to work and develop long-term self-management skills [33]. However, no evidence exists to inform or enhance PLHP practice globally. Given the rising incidence of CVDs and the lack of CR services in LMICs, it is essential that physiotherapists from these countries are able to deliver health promotion strategies effectively.
Previous reviews on PLHP are limited and focused on health education strategies for lifestyle-related conditions in general [34], promoting physical activities [28,35], entry-level training and physical activity promotion [35] and physical activity in cystic fibrosis patients [36]. There are no reviews investigating PLHP strategies for pwCVDs. Consequently, a review is warranted to systematically scope and map out the existing evidence in this area. This review summarises the available literature with the following objectives:
- To assess the characteristics of existing evidence on PLHP for pwCVDs globally.
- To identify the interventional approaches that have been used in PLHP strategies for pwCVDs
- To evaluate the type of population groups included in the PLHP research.
2. Methodology
A scoping review was used to identify and synthesise data on PHLP strategies and interventions in the literature and map existing evidence’s characteristics without critically appraising the methodological quality [37,38]. The methodological framework published by Arksey and O’Malley and the methodological advancement by Levac and colleagues was adopted for this study [39,40]. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis Extension for Scoping Reviews (PRISMA-ScR) recommendations were used for reporting this systematic scoping review [41,42]. The proposed stages in this framework are: 1) identifying the research questions, 2) identifying relevant studies, 3) study selection, 4) charting the data, and 5) collating, summarising and reporting [40]. The template for intervention description and replication (TIDieR) framework was used to extract intervention data from the included studies. The study protocol was registered on the Open Science Frame (OSF) (DOI 10.17605/OSF.IO/BFZ6Y). This review involves no direct contact with patients and healthcare professionals but reviewed and synthesised already published data, and therefore was not subject to ethical approval.
2.1. Identifying the Research Question
Scoping review questions are generally broad and aim to summarise the available evidence of interest [42]. Based on the overall project aims, the following questions were identified for the present study: 1) What are the characteristics of existing evidence of PLHP for pwCVDs globally? 2) What interventional approaches have been used in PLHP strategies for pwCVDs globally? 3) What population groups have been included in the PLHP research globally?
2.2. Identifying Relevant Studies (Database and Search Strategy)
The following electronic databases, registries and search engines were searched for eligible articles from the inception of the database to June 2023: MEDLINE, PubMed Web of Science, Cochrane Central Register of Controlled Trials, EMBASE, CINAHL, PEDro and Google Scholar, EU clinical trial register, African Index Medicus, World Physiotherapy Conference proceedings, trials registries and World Health Organisation International Clinical Trials Registry Platform portal. A search strategy that considered relevant index terms and keywords was developed with assistance from an experienced librarian from Sheffield Hallam University (Table 1). A subject librarian at Sheffield Hallam University further reviewed this. The search strategy for MEDLINE (final) was adapted for searches in other included databases. Search filters such as publication in the English language, human species, and primary studies were used in relevant databases. References of identified previous and adjacent reviews and included papers were also screened. A complete MEDLINE search strategy can be found in Appendix A.
2.3. Eligibility Criteria
Studies were included if they reported or evaluated health promotion for pwCVDs, were led by physiotherapists, and were published in English. Studies with a focus on specific clinical or therapeutic outcomes rather than health promotion were excluded. Details on inclusion and exclusion criteria are provided in Table 2.
2.4. Study Selection (Screening)
Studies identified through searches were imported to Covidence, and duplicates were removed. Two independent reviewers (ENN, CG) individually screened studies using a three-step process: first titles, then abstracts and finally, full text was screened based on the inclusion and exclusion criteria (Table 2). The full texts of selected studies were reviewed in detail against the inclusion criteria by two independent reviewers (ENN, SM). All reasons for excluding potential studies that did not meet the inclusion criteria are reported on the PRISMA flowchart. Any disagreements between the reviewers at each stage of the study selection process were resolved through discussion, and where an agreement was not met, a third reviewer (AL) was consulted.
2.5. Data Charting (Data Extraction)
Data charting is the method for extracting data for scoping reviews [39,41]. The chart included information about study participants and design. Data about the nature of the intervention(s) was extracted based on the TIDieR framework, including the theoretical framework (why), intervention type (what), intervention duration (when), intervention provider (who), delivery format (how), intervention location (where), number of intervention sessions (how much), personalised intervention (tailoring), fidelity (how well). Intervention duration of less than 12 months was described as short and more than 12 months as long. Total intervention sessions less than 15 sessions and 16 sessions and above were described as low and high volume respectively. In the cases of missing data or insufficiently described processes, the corresponding authors were contacted to clarify or provide the missing information. Screening and data extraction were completed in Covidence.
2.6. Quality Appraisal
2.7. Collating, Summarising, and Reporting
Results are synthesised narratively and presented in a table format based on elements of the TIDier framework.
3. Results
3.1. Literature Search and Included Studies
The PRISMA flow chart (Figure 1) summarises search results and the methodological steps to arrive at the included studies. The search yielded 4381 articles with the respective number for each database, as shown on the PRISMA flow chart (Figure 1). After removing the duplicates, 1716 studies remained and were screened for eligibility. After titles and abstracts screening, 227 articles were deemed potentially eligible. Following full-text screening, 20 studies were included in this review. Reasons for exclusions are documented on the PRISMA flow chart.
3.2. Characteristics of Included Studies
Table 3 summarises the characteristics of the included studies. Of the twenty included studies, 12 were Randomised Controlled Trials (RCTs) [44,45,46,47,48,49,50,51,52,53,54,55], seven were quasi-experimental studies [56,57,58,59,60,61,62], and one secondary analyses of trial data. All included studies were published between 2002 and 2022. 30% of included studies were published between 2016 and 2020 (reference these please). Studies were conducted on patients with stroke (n = 4) [52,56,57,63], risk factors for CVD (n = 4) [46,49,53,61], coronary heart diseases (n = 3) [50,62,64], peripheral arterial diseases (n = 2) [44,55], diabetes (n = 3) [47,59,65], weight/obesity (n = 2) [48,60] and hypertension (n = 2) [45,54]. The sample size of the included studies ranged from 18 to 882 participants [44,45]. The included studies were conducted in 15 countries, with England, Australia, Spain, The Netherlands, and Norway having two studies each and the remaining countries one study each (Table 4). The majority of studies were from high-income countries (HICs), with 47% from Europe alone, with only two publications [66,67] from 2 LMICs (Brazil, China). No studies were identified from the African continent.
3.3. Characteristics of the Included Interventions
All studies were either solely implemented by physiotherapists (n = 13) (reference) or in combination with other healthcare professionals (nurses, physicians, and dieticians/nutritionists), with physiotherapists leading defined components of the intervention (n = 7) (reference). Identified interventions were heterogeneous and reported according to the TIDieR framework in Table 4. 85% of studies used multimodal intervention strategies, with only 15% of studies using single intervention strategy [45,50,55]. Seven (35%) of the 20 publications employed behaviour change approaches and psychological models such as the Theory of Planned Behaviour and the Common-Sense Model of Illness Representations (n = 1) [55], Health Belief Model and Transtheoretical Model to promote participant exercise behaviours (n = 1) [49], Bandura’s Self-Efficacy Theory (n = 1) [62] and motivational interviewing (n = 4) [50,55,57,68]. The majority of interventions included exercise or physical activity (n = 18) [44,45,46,47,49,50,52,53,54,55,57,58,60,62,69,70,70], education on lifestyle (n=2)[51,58], dietary education in combination with another physiotherapists’ led intervention (n = 6) [46,49,51,54,62,69]. Seven studies employed behaviour change programs focused on physical activity uptake (n = 5) [50,55,56,60,62] and diabetes management (n = 2) [54,70]. Self-management and home programs were also identified (n = 4) [47,51,56,61]. Individualised coaching on physical activity and exercise (n = 5) [58,63,68,69,70] and use of the Health Improvement Card (HIC) (n = 1) [53] were also used by physiotherapists to enhance activity and reduce cardiovascular risks. Six studies were characterised by the provision of educational materials/resources, including brochures on healthy lifestyle practices and lifestyle behaviour change (n = 2) [44,53], written instructions and recommendations (n = 2) [46,58], workbooks (n = 1) [54] and handouts following each session (n = 1) [60]. Technology-based strategies were also used to deliver interventions for weight management (video-conferencing sessions with real-time communications and the use of remote monitoring using Fitbit) (n = 1) [68], video/television program called Sit and Be Fit during the exercise phase (n = 1) [70], videos on specific exercises and techniques (n = 1) [49]). Six studies were supplemented by telephone calls (n = 6) [47,49,50,51,55,57]. Adherence to interventions was reported in nine studies [49,55,56,57,58,62,68,69,70].
4. Discussion
This review identified the nature of the evidence and the types of interventions used and implemented by physiotherapists for pwCVDs. This is the first review explicitly exploring PLHP for pwCVDs globally, providing an opportunity for discussion and future research in this area.
This review returned 20 studies. No grey literature was found, and all included studies were published between 2002 and 2022. Given that there was no restriction in the search period, this is small volume of literature. This could be explained in two ways. Firstly, the inclusion was based on physiotherapists leading or implementing the intervention focusing on primary and secondary prevention of CVDs to heart disease risk factors. Based on this criterion, many studies were excluded as not physiotherapist-led (n = 60) (Figure 1). Secondly, earlier attention to physiotherapists' interventions was directed toward therapeutic and curative treatment rather than prevention. Over the last two decades, physiotherapy preventive roles have been increasing with the rising burden of CVDS [71,72]. This aligns with the global call for physiotherapists to contribute to preventing lifestyle-related conditions [71,72,73]. The increasing trend in research output indicates that more evidence will emerge in the coming years as physiotherapists gain skills and autonomy in leading prevention programs.
Currently, most studies emerged from Europe, with no studies from the African continent. Given the vast burden of CVDs in Africa and the lack of CR programs on the continent [31,74], it is essential to see more research investigating PLHP for pwCVDs in African countries. Only two studies (10%) from LMICs were included in this review and both were supported with research funding [66,67]. Generally, PLHP research may be difficult to realise in LMIC settings due to lack of research priorities, funding problems, lack of infrastructures and researchers with relevant skills [75,76]. Addressing funding issues by budgeting for the prevention of NCDs in LMICs, among other potential barriers, may contribute positively to data generation for pwCVDs in low-resource settings.
Many included studies were RCTs (60%), followed by different quasi-experimental designs (35%). The available data provides an opportunity for follow-up studies, such as a systematic review of effectiveness. This is necessary to determine whether PLHP are effective for wider-scale adoption. No qualitative work on PLHP was identified and there is a gap in our understanding of patient perception and experiences of PLHP approaches. More research is necessary for designing and implementing PLHP in the future.
Diverse interventional approaches have been used in PLHP for pwCVDs (Table 4). CVD PLHP interventions are likely to be complex, and therefore require a multimodal approach, due to different populations, multiple risk factors for CVD, and non-adherence to recommendations for managing these risk factors [77]. In this review included studies focused mainly on exercise and physical activity uptake, weight management and diet. Other components of health promotion for pwCVDs, such as sleep hygiene, smoking cessation, and alcohol abuse, among others, were not reported. These components are within the scope of physiotherapists, but they should receive adequate training that can enable them to confidently tackle the multiple risk factors associated with CVD. This should include counselling skills and the use of behaviour change strategies for specific populations.
Three studies employed theory-based behaviour change models supported by evidence-based behaviour change techniques such as motivational interviewing (n = 4) to inform and complement their interventions. These behaviour change theories and techniques were adopted in more recent studies published between 20xx and 20yy indicating an increased understanding of the importance of including behaviour change for effective health promotion and education.and to strengthen patients’ motivation and adherence during and beyond the active rehabilitation period. More rigorous, theoretically informed approaches to support behaviour change for pwCVDs should be included in intervention strategies that facilitate change in lifestyle risk factors. This is also necessary in clinical practice and should be integrated into physiotherapy training [72]. In delivering broad health promotion strategies for pwCVDs, physiotherapists need to receive broader training in addressing these risk factors.
4.1. Implications for Clinical Practice
It is sensible to consider PLHP strategies incorporating interventions beyond exercise and physical activity. Understanding and increasing competence in effecting behaviour change in stress management, sleep, nutrition, and weight management through appropriate strategies is necessary for effective PLHP. Dean and colleagues highlighted the need to raise the priority of lifestyle prevention strategies for NCDs [73] and competency standards, including relevant behaviour change approaches [72] to improve practice adequately. Considering the different study populations and the multiple risk factors addressed in the included studies, it is necessary that physiotherapists collaborate with other healthcare providers to optimise health promotion and prevention programmes. Digital and technological monitoring and other interventions have been used successfully in some trials and contexts [68,78]. This can be useful in other contexts while considering local challenges and possible barriers.
4.2. Research Implications
The findings of this review demonstrate that the lack of studies from Africa and other LMICs, which is concerning given the rising burden of pwCVDs in these regions. For effective interventions to be developed, it is necessary to consider increasing research output in these contexts.
PLHP interventions ought to be multimodal, theoretically informed and supported by behaviour change theories and techniques and delivered by phyiotherapists who have been adequately trained and, where necessary, optimised by appropriate health care professional who complement the physiotherapists’ skills and knowledge. These optimised interventions should also be reported in further trials following the TIDier Framework. There is no evidence to characterise the optimal intensity and critical characteristics of weight management programs for specific populations.
Findings highlight the increased use of digital technology at different levels of PLHP interventions with varied levels of adherence [68,79]. Digital or technological devices that are attractive, affordable, easy to use and sensitive to specific outcomes in different contexts for better adherence and output should be considered.
Most of the included trials reported short-term follow-up. Despite prevailing challenges, PLHP interventions are warranted to demonstrate longer-term clinical outcomes.
4.3. Strengths and Limitations
Scoping reviews provide breadth and the inclusion of all study designs and makes this realistic about a topic. This study employed the recommended guidelines for conducting a scoping review with multiple reviewers for data screening and extraction, making the findings rigorous. The broad scope provides a complete overview of PLHP, which has been trialled in primary, secondary, and tertiary health promotion in low- and high-income countries. This provides researchers with clear directions about developing the PLHP evidence based and where further research needs to be undertaken. Additionally, the results of this scoping review may apply to clinicians employing the identified strategies/approaches as CVDs and their risk factors share and pose similar risks to other CNCDs. This review considers only literature published in English. This might have limited the scope of this review to articles published or from non-English speaking countries.
5. Conclusions
Based on the literature, physiotherapists are trying to address the growing burden of CVDs through various PLHP strategies. PLHP strategies are focused on exercise and physical activity, and there is a need to tackle CVD beyond addressing sedentary behaviour, considering the multiple risk factors. Assessing the risks and needs, tailoring the interventions to individuals, and monitoring appear central and consistent with practical preventive principles and strategies. It is crucial that physiotherapists work together with other healthcare professionals to optimise relevant components of health promotion effectively. Health behaviour change theories and techniques should be commonly used to support positive health behaviour change and it may be necessary to provide comprehensive training to integrate lifestyle management approaches in physiotherapy practice. This is even more compelling for physiotherapy practice in Africa and LMICs with huge CVD burdens. Further study is needed to elucidate the effectiveness of existing PLHP interventions for pwCVDs. Avenues for future research have been highlighted.
Author Contributions
The authors E.N., S.M., and A. L. conceived the review. E.N. wrote the protocol and draft of this manuscript; initial database search, screened titles, abstracts, and full texts; and did data extraction and submitted the manuscript. C.G. screened titles, abstracts, and full text. S.M. screened full text, extracted data, and provided guidance throughout manuscript writing. A.L. resolved conflicts through the screening process and provide guidance. All authors have read and agreed to the published the final version of the manuscript.
Funding
This review received no external funding.
Institutional Review Board Statement
This review used published articles and data contained within.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data extracted and synthesised in this review were taken directly from the published articles.
Conflicts of Interest
None declared.
Appendix A
Medline Search Strings
tiab(“physical therapist*” OR “physical therapists” OR kinesiotherapist* OR physiotherapist* OR “physiotherapy assistant*” OR “physical therapy assistant*”) AND ((tiab(“angina” OR “atherosclerosis” OR “atherosclerosis” OR “blood pressure” OR “cardio vascular disease” OR “cardio vascular diseases” OR “cardiometabolic risk factors” OR “cardiomyop*” OR “cardiovascular disease” OR “cardiovascular diseases” OR “cardiovascular diseases”) OR tiab(“cerebrovascular accident” OR “cerebrovascular accidents” OR “chest pain” OR “chest pains” OR “coronary artery disease” OR “coronary artery diseases” OR “coronary heart disease” OR “coronary heart diseases” OR “diabetes mellitus” OR “diabetes mellitus, type 2” OR “diabetes”) OR tiab(“diabetic” OR “diabetics” OR “dyslipidaemia” OR “dyslipidaemic” OR “dyslipidemia” OR “dyslipidemias” OR “dyslipidemic” OR “heart attack” OR “heart attacks” OR “heart disease risk factors” OR “heart disease” OR “heart diseases” OR “heart failure” OR “heart failures”) OR tiab(“hyper tension” OR “hypertension” OR “hypertension” OR “myocardial infarction” OR “myocardial infarctions” OR “obese “ OR “obesity” OR “obesity” OR “obesity, abdominal” OR “obesity, morbid” OR “overweight” OR “overweight*” OR “peripheral artery disease” OR “peripheral artery diseases” OR “stroke” OR “strokes”)) AND (tiab(“physical therapist*” OR “physical therapists” OR kinesiotherapist* OR physiotherapist* OR “physiotherapy assistant*” OR “physical therapy assistant*”) OR (MESH.EXACT.EXPLODE(“Physical Therapists:N.02.360.790”) OR MESH.EXACT.EXPLODE(“Health Personnel:M.01.526.485”))) AND (tiab(“attitude to health” OR “attitude” OR “attitudes” OR “coping skill” OR “coping skills” OR “counselling” OR “diet therapies” OR “diet therapy” OR “diet therapy” OR “diet therapy” OR “education technologies” OR “educational model” OR “educational models” OR “educational technology” OR “exercise promotion” OR “exercise promotions”) OR tiab(“exercise therapies” OR “exercise therapy” OR “exercise therapy” OR “exercise therapies” OR “face to face” OR “goal setting” OR “group based” OR “group session*” OR “health behaviour” OR “health behaviours” OR “health behaviour” OR “health behaviours” OR “health education” OR “health education” OR “health knowledge, attitudes, practice”) OR tiab(“health promotion” OR “health promotion” OR “healthy lifestyle” OR “home based” OR “hospital based” OR “individual plan*” OR “individualised plan*” OR “individualized plan*” OR “life style” OR “lifestyle” OR “life style” OR “models, educational” OR “nutrition coach*” OR “nutrition management” OR “patient education as topic” OR “patient education handout”) OR tiab(“patient education” OR “patient handout*” OR “physical activities” OR “physical activity” OR “physical therapy modalities” OR “prevention” OR “skill training” OR “sleep health” OR “sleep management” OR “smoking cessation” OR “stress management” OR “weight management”) OR (MESH.EXACT.EXPLODE(“Health Education:I.02.233.332”) OR MESH.EXACT.EXPLODE(“Health Education:N.02.421.726.407”) OR MESH.EXACT.EXPLODE(“Education, Public Health Professional”)))).
References
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practiceThe Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J 2016, 37, 2315–2381. [Google Scholar] [CrossRef] [PubMed]
- Non communicable diseases Available online:. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 19 July 2021).
- Tulu, S.N.; Al Salmi, N.; Jones, J. Understanding cardiovascular disease in day-to-day living for African people: a qualitative metasynthesis. BMC Public Health 2021, 21, 745. [Google Scholar] [CrossRef] [PubMed]
- Cardiovascular diseases (CVDs) Available online:. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 21 November 2021).
- Gaziano, T.A. Reducing The Growing Burden Of Cardiovascular Disease In The Developing World. Health Affairs 2007, 26, 13–24. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.J.; Chin, S.L.; Rangarajan, S.; Xavier, D.; Liu, L.; Zhang, H.; Rao-Melacini, P.; Zhang, X.; Pais, P.; Agapay, S.; et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. The Lancet 2016, 388, 761–775. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Roth, G.A.; Naghavi, M.; Parmar, P.; Krishnamurthi, R.; Chugh, S.; Mensah, G.A.; Norrving, B.; Shiue, I.; Ng, M.; et al. Global burden of stroke and risk factors in 188 countries, during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet Neurology 2016, 15, 913–924. [Google Scholar] [CrossRef] [PubMed]
- Strong, K.; Mathers, C.; Bonita, R. Preventing stroke: saving lives around the world. The Lancet Neurology 2007, 6, 182–187. [Google Scholar] [CrossRef]
- Mohan, K.M.; Wolfe, C.D.A.; Rudd, A.G.; Heuschmann, P.U.; Kolominsky-Rabas, P.L.; Grieve, A.P. Risk and Cumulative Risk of Stroke Recurrence: A Systematic Review and Meta-Analysis. Stroke 2011, 42, 1489–1494. [Google Scholar] [CrossRef]
- Dhamoon, M.S.; Sciacca, R.R.; Rundek, T.; Sacco, R.L.; Elkind, M.S.V. Recurrent stroke and cardiac risks after first ischemic stroke: The Northern Manhattan Study. Neurology 2006, 66, 641–646. [Google Scholar] [CrossRef]
- Ruan, Y.; Guo, Y.; Zheng, Y.; Huang, Z.; Sun, S.; Kowal, P.; Shi, Y.; Wu, F. Cardiovascular disease (CVD) and associated risk factors among older adults in six low-and middle-income countries: results from SAGE Wave 1. BMC Public Health 2018, 18, 778. [Google Scholar] [CrossRef]
- Yusuf, S.; Hawken, S.; Ôunpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. The Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Bigna, J.J.; Noubiap, J.J. The rising burden of non-communicable diseases in sub-Saharan Africa. The Lancet Global Health 2019, 7, e1295–e1296. [Google Scholar] [CrossRef] [PubMed]
- Bowry, A.D.K.; Lewey, J.; Dugani, S.B.; Choudhry, N.K. The Burden of Cardiovascular Disease in Low- and Middle-Income Countries: Epidemiology and Management. Canadian Journal of Cardiology 2015, 31, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease - American College of Cardiology Available online:. Available online: https://www.acc.org/latest-in-cardiology/ten-points-to-remember/2019/03/07/16/00/2019-acc-aha-guideline-on-primary-prevention-gl-prevention (accessed on 15 August 2020).
- Li, D.; Jia, Y.; Yu, J.; Liu, Y.; Li, F.; Liu, Y.; Wu, Q.; Liao, X.; Zeng, Z.; Wan, Z.; et al. Adherence to a Healthy Lifestyle and the Risk of All-Cause Mortality and Cardiovascular Events in Individuals With Diabetes: The ARIC Study. Front. Nutr. 2021, 8, 698608. [Google Scholar] [CrossRef] [PubMed]
- Schuett, K.A.; Lehrke, M.; Marx, N.; Burgmaier, M. High-Risk Cardiovascular Patients: Clinical Features, Comorbidities, and Interconnecting Mechanisms. Front. Immunol. 2015, 6. [Google Scholar] [CrossRef]
- Bellmann, B.; Lin, T.; Greissinger, K.; Rottner, L.; Rillig, A.; Zimmerling, S. The Beneficial Effects of Cardiac Rehabilitation. Cardiol Ther 2020, 9, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Dietary Restrictions and Nutrition in the Prevention and Treatment of Cardiovascular Disease | Circulation Research Available online:. Available online: https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.118.313352 (accessed on 1 August 2021).
- Darden, D.; Richardson, C.; Jackson, E.A. Physical Activity and Exercise for Secondary Prevention among Patients with Cardiovascular Disease. Curr Cardiovasc Risk Rep 2013, 7, 411–416. [Google Scholar] [CrossRef]
- Smyth, A.; Teo, K.K.; Rangarajan, S.; O’Donnell, M.; Zhang, X.; Rana, P.; Leong, D.P.; Dagenais, G.; Seron, P.; Rosengren, A.; et al. Alcohol consumption and cardiovascular disease, cancer, injury, admission to hospital, and mortality: a prospective cohort study. The Lancet 2015, 386, 1945–1954. [Google Scholar] [CrossRef]
- Tobacco smoking and risk of 36 cardiovascular disease subtypes: fatal and non-fatal outcomes in a large prospective Australian study | BMC Medicine | Full Text Available online:. Available online: https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-019-1351-4 (accessed on 1 August 2021).
- Nagai, M.; Hoshide, S.; Kario, K. Sleep Duration as a Risk Factor for Cardiovascular Disease- a Review of the Recent Literature. CCR 2010, 6, 54–61. [Google Scholar] [CrossRef]
- Gomes, M.J.; Pagan, L.U.; Okoshi, M.P. Non-Pharmacological Treatment of Cardiovascular Disease | Importance of Physical Exercise. Arquivos Brasileiros de Cardiologia 2019. [Google Scholar] [CrossRef]
- How is Stress and Heart Disease Related? – Cleveland Clinic Available online:. Available online: https://health.clevelandclinic.org/how-is-stress-and-heart-disease-related/ (accessed on 1 August 2021).
- Kisling, L.A.; Das, J.M. Prevention Strategies. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2021. [Google Scholar]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease. Journal of the American College of Cardiology 2019, 74, e177–e232. [Google Scholar] [CrossRef]
- Lowe, A.; Gee, M.; McLean, S.; Littlewood, C.; Lindsay, C.; Everett, S. Physical activity promotion in physiotherapy practice: a systematic scoping review of a decade of literature. Br J Sports Med 2018, 52, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Korn, L.; Ben-Ami, N.; Azmon, M.; Einstein, O.; Lotan, M. Evaluating the Effectiveness of a Health Promotion Intervention Program Among Physiotherapy Undergraduate Students. Med Sci Monit 2017, 23, 3518–3527. [Google Scholar] [CrossRef] [PubMed]
- Maguire, A. Physiotherapy and Cardiovascular Disease: What Can It Do to Help? Available online: https://ballsbridgephysio.ie/news/physiotherapy-and-cardiovascular-disease-what-can-it-do-to-help/ (accessed on 10 August 2021).
- Turk-Adawi, K.; Supervia, M.; Lopez-Jimenez, F.; Pesah, E.; Ding, R.; Britto, R.R.; Bjarnason-Wehrens, B.; Derman, W.; Abreu, A.; Babu, A.S.; et al. Cardiac Rehabilitation Availability and Density around the Globe. EClinicalMedicine 2019, 13, 31–45. [Google Scholar] [CrossRef] [PubMed]
- Ragupathi, L.; Stribling, J.; Yakunina, Y.; Fuster, V.; McLaughlin, M.A.; Vedanthan, R. Availability, Use, and Barriers to Cardiac Rehabilitation in LMIC. gh 2017, 12, 323. [Google Scholar] [CrossRef] [PubMed]
- Bäck, M.; Öberg, B.; Krevers, B. Important aspects in relation to patients’ attendance at exercise-based cardiac rehabilitation – facilitators, barriers and physiotherapist’s role: a qualitative study. BMC Cardiovasc Disord 2017, 17, 77. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.; Bambury, E.; Mendoza, A.; Reynolds, J.; Veronneau, R.; Dean, E. Health education strategies used by physical therapists to promote behaviour change in people with lifestyle-related conditions: A systematic review. Hong Kong Physiotherapy Journal 2012, 30, 57–75. [Google Scholar] [CrossRef]
- Kunstler, B.E.; Cook, J.L.; Freene, N.; Finch, C.F.; Kemp, J.L.; O’Halloran, P.D.; Gaida, J.E. Physiotherapists use a small number of behaviour change techniques when promoting physical activity: A systematic review comparing experimental and observational studies. Journal of Science and Medicine in Sport 2018, 21, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Cox, N.S.; Alison, J.A.; Holland, A.E. Interventions for promoting physical activity in people with cystic fibrosis. Cochrane Database of Systematic Reviews 2013. [Google Scholar] [CrossRef]
- Lockwood, C.; Dos Santos, K.B.; Pap, R. Practical Guidance for Knowledge Synthesis: Scoping Review Methods. Asian Nursing Research 2019, 13, 287–294. [Google Scholar] [CrossRef]
- Munn, Z.; Stern, C.; Aromataris, E.; Lockwood, C.; Jordan, Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med Res Methodol 2018, 18, 5. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: towards a methodological framework. International Journal of Social Research Methodology 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: advancing the methodology. Implementation Sci 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Implementation 2021, 19, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef]
- Fowler, B.; Jamrozik, K.; Norman, P.; Allen, Y.; Wilkinson, E. Improving maximum walking distance in early peripheral arterial disease: randomised controlled trial. Australian Journal of Physiotherapy 2002, 48, 269–275. [Google Scholar] [CrossRef]
- Bonet, J.; Coll, R.; Rocha, E.; Romero, R. Supervised versus recommended physical exercise in hypertensive women. Is its recommendation enough? Blood pressure 2003, 12, 139–144. [Google Scholar] [CrossRef]
- Eriksson, K.M.; Westborg, C.; Eliasson, M.C.E. A randomized trial of lifestyle intervention in primary healthcare for the modification of cardiovascular risk factors. Scandinavian Journal of Public Health 2006, 34, 453–461. [Google Scholar] [CrossRef]
- Wisse, W.; Boer Rookhuizen, M.; de Kruif, M.D.; van Rossum, J.; Jordans, I.; ten Cate, H.; van Loon, L.J.C.; Meesters, E.W. Prescription of physical activity is not sufficient to change sedentary behavior and improve glycemic control in type 2 diabetes patients. Diabetes research and clinical practice 2010, 88, e10–e13. [Google Scholar] [CrossRef]
- Molenaar, E.A.; van Ameijden, E.J.C.; Vergouwe, Y.; Grobbee, D.E.; Numans, M.E. Effect of nutritional counselling and nutritional plus exercise counselling in overweight adults: a randomized trial in multidisciplinary primary care practice. Family practice 2010, 27, 143–150. [Google Scholar] [CrossRef]
- Wu, Y.-T.; Hwang, C.-L.; Chen, C.-N.; Chuang, L.-M. Home-based exercise improves exercise behavior and metabolic risk factors in middle-aged adults at diabetic risk. 2011, 97, eS523. [Google Scholar] [CrossRef]
- Reid, R.D.; Morrin, L.I.; Higginson, L.A.J.; Wielgosz, A.; Blanchard, C.; Beaton, L.J.; Nelson, C.; McDonnell, L.; Oldridge, N.; Wells, G.A.; et al. Motivational counselling for physical activity in patients with coronary artery disease not participating in cardiac rehabilitation. European journal of preventive cardiology 2012, 19, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Oerkild, B.; Frederiksen, M.; Hansen, J.F.; Prescott, E. Home-based cardiac rehabilitation is an attractive alternative to no cardiac rehabilitation for elderly patients with coronary heart disease: results from a randomised clinical trial. BMJ Open 2012, 2. [Google Scholar] [CrossRef] [PubMed]
- Takatori, K.; Matsumoto, D.; Okada, Y.; Nakamura, J.; Shomoto, K. Effect of intensive rehabilitation on physical function and arterial function in community-dwelling chronic stroke survivors. Topics in stroke rehabilitation 2012, 19, 377–383. [Google Scholar] [CrossRef]
- Bai, Y.; Wu, X.; Tsang, R.C.; Yun, R.; Lu, Y.; Dean, E.; Jones, A.Y. A Randomised Controlled Trial to Evaluate the Administration of the Health Improvement Card as a Health Promotion Tool: A Physiotherapist-Led Community-Based Initiative. International journal of environmental research and public health 2020, 17. [Google Scholar] [CrossRef]
- Gerage, A.M.; Benedetti, T.R.B.; Cavalcante, B.R.; Farah, B.Q.; Ritti-Dias, R.M. Efficacy of a behavior change program on cardiovascular parameters in patients with hypertension: a randomized controlled trial. Einstein (Sao Paulo) 2020, 18, eAO5227. [Google Scholar] [CrossRef]
- Bearne, L.M.; Volkmer, B.; Peacock, J.; Sekhon, M.; Fisher, G.; Galea Holmes, M.N.; Douiri, A.; Amirova, A.; Farran, D.; Quirke-McFarlane, S.; et al. Effect of a Home-Based, Walking Exercise Behavior Change Intervention vs Usual Care on Walking in Adults With Peripheral Artery Disease: The MOSAIC Randomized Clinical Trial. JAMA 2022, 327, 1344–1355. [Google Scholar] [CrossRef]
- Preston, E.; Dean, C.M.; Ada, L.; Stanton, R.; Brauer, S.; Kuys, S.; Waddington, G. Promoting physical activity after stroke via self-management: a feasibility study. Topics in Stroke Rehabilitation 2017, 24, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Gunnes, M.; Langhammer, B.; Aamot, I.-L.; Lydersen, S.; Ihle-Hansen, H.; Indredavik, B.; Reneflot, K.H.; Schroeter, W.; Askim, T.; group, L.C. Adherence to a Long-Term Physical Activity and Exercise Program After Stroke Applied in a Randomized Controlled Trial. Physical Therapy 2019, 99, 74–85. [Google Scholar] [CrossRef]
- Higgs, C.; Skinner, M.; Hale, L. Outcomes of a community-based lifestyle programme for adults with diabetes or pre-diabetes. J Prim Health Care 2016, 8, 130–139. [Google Scholar] [CrossRef]
- Pariser, G.; Ann Demeuro, M.; Gillette, P.; Stephen, W. Outcomes of an Education and Exercise Program for Adults with Type 2 Diabetes, and Comorbidities that Limit their Mobility: A Preliminary Project Report. Cardiopulmonary physical therapy journal 2010, 21, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Quinn, A.; Doody, C.; O’Shea, D.; Quinn, A.; Doody, C.; O’Shea, D. The effect of a physical activity education programme on physical activity, fitness, quality of life and attitudes to exercise in obese females. Journal of Science & Medicine in Sport 2008, 11, 469–472. [Google Scholar] [CrossRef]
- Batsis, J.A.; Petersen, C.L.; Clark, M.M.; Cook, S.B.; Lopez-Jimenez, F.; Al-Nimr, R.I.; Pidgeon, D.; Kotz, D.; Mackenzie, T.A.; Bartels, S.J. A Weight Loss Intervention Augmented by a Wearable Device in Rural Older Adults With Obesity: A Feasibility Study. The journals of gerontology. Series A, Biological sciences and medical sciences 2021, 76, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Deka, P.; Blesa, J.; Pathak, D.; Sempere-Rubio, N.; Iglesias, P.; Micó, L.; Soriano, J.M.; Klompstra, L.; Marques-Sule, E. Combined Dietary Education and High-Intensity Interval Resistance Training Improve Health Outcomes in Patients with Coronary Artery Disease. International journal of environmental research and public health 2022, 19. [Google Scholar] [CrossRef] [PubMed]
- Gunnes, M.; Indredavik, B.; Langhammer, B.; Lydersen, S.; Ihle-Hansen, H.; Dahl, A.E.; Askim, T. Associations Between Adherence to the Physical A ctivity and Exercise Program Applied in the LAST Study and Functional Recovery After Stroke. Archives of Physical Medicine & Rehabilitation 2019, 100, 2251–2259. [Google Scholar] [CrossRef]
- Oerkild, B.; Frederiksen, M.; Hansen, J.F.; Prescott, E. Home-based cardiac rehabilitation is an attractive alternative to no cardiac rehabilitation for elderly patients with coronary heart disease: results from a randomised clinical trial. BMJ open 2012, 2. [Google Scholar] [CrossRef] [PubMed]
- Higgs, C.; Skinner, M.; Hale, L. Outcomes of a community-based lifestyle programme for adults with diabetes or pre-diabetes. Journal of primary health care 2016, 8, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Wu, X.; Tsang, R.C.; Yun, R.; Lu, Y.; Dean, E.; Jones, A.Y. A Randomised Controlled Trial to Evaluate the Administration of the Health Improvement Card as a Health Promotion Tool: A Physiotherapist-Led Community-Based Initiative. International journal of environmental research and public health 2020, 17. [Google Scholar] [CrossRef]
- Gerage, A.M.; Benedetti, T.R.B.; Cavalcante, B.R.; Farah, B.Q.; Ritti-Dias, R.M. Efficacy of a behavior change program on cardiovascular parameters in patients with hypertension: a randomized controlled trial. Einstein (Sao Paulo, Brazil) 2020, 18, 1. [Google Scholar] [CrossRef]
- Batsis, J.A.; Petersen, C.L.; Clark, M.M.; Cook, S.B.; Lopez-Jimenez, F.; Al-Nimr, R.I.; Pidgeon, D.; Kotz, D.; Mackenzie, T.A.; Bartels, S.J. A Weight Loss Intervention Augmented by a Wearable Device in Rural Older Adults With Obesity: A Feasibility Study. Journals of Gerontology Series A: Biological Sciences & Medical Sciences 2021, 76, 95–100. [Google Scholar] [CrossRef]
- Molenaar, E.A.; van Ameijden, E.J.; Vergouwe, Y.; Grobbee, D.E.; Numans, M.E. Effect of nutritional counselling and nutritional plus exercise counselling in overweight adults: a randomized trial in multidisciplinary primary care practice. Fam Pract 2010, 27, 143–150. [Google Scholar] [CrossRef]
- Pariser, G.; Ann Demeuro, M.; Gillette, P.; Stephen, W. Outcomes of an Education and Exercise Program for Adults with Type 2 Diabetes, and Comorbidities that Limit their Mobility: A Preliminary Project Report. Cardiopulmonary physical therapy journal 2010, 21, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Dean, E. Physical therapy in the 21st century (Part I): toward practice informed by epidemiology and the crisis of lifestyle conditions. Physiotherapy theory and practice 2009, 25, 330–353. [Google Scholar] [CrossRef] [PubMed]
- Dean, E.; Skinner, M.; Myezwa, H.; Mkumbuzi, V.; Mostert, K.; Parra, D.C.; Shirley, D.; Söderlund, A.; de Andrade, A.D.; Abaraogu, U.O.; et al. Health Competency Standards in Physical Therapist Practice. Physical Therapy 2019, 99, 1242–1254. [Google Scholar] [CrossRef] [PubMed]
- Dean, E.; Creig, A.; Murphy, S.; Roots, R.; Nembhard, N.; Rankin, A.; Bainbridge, L.; Anthony, J.; Hoens, A.M.; Garland, S.J. Raising the Priority of Lifestyle-Related Noncommunicable Diseases in Physical Therapy Curricula. Physical Therapy 2016, 96, 940–948. [Google Scholar] [CrossRef]
- Dzudie, A.; Rayner, B.; Ojji, D.; Schutte, A.E.; Twagirumukiza, M.; Damasceno, A.; Ba, S.A.; Kane, A.; Kramoh, E.; Kacou, J.B.A.; et al. Roadmap to achieve 25% hypertension control in Africa by 2025. CVJA 2017, 28, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Ngeh, E.N. Research among undergraduate biomedical students in Cameroon: contextual barriers, room for improvement. Pan Afr Med J 2019, 33. [Google Scholar] [CrossRef]
- Ngeh Ngeh, E.; Chigbo, N.N.; Whitehouse, Z.; Anekwu, E.M.; Mukaruzima, L.M.; Mtsetfwa, L.; Kitur, R.; Agoriwo, M.W.; Ondogah, P.; Douryang, M.; et al. A report on the development of COVID-19 guidelines for rehabilitation professionals in African settings. Pan Afr Med J 2021, 38. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ 2008, a1655. [Google Scholar] [CrossRef]
- Bennell, K.L.; Lawford, B.J.; Keating, C.; Brown, C.; Kasza, J.; Mackenzie, D.; Metcalf, B.; Kimp, A.J.; Egerton, T.; Spiers, L.; et al. Comparing Video-Based, Telehealth-Delivered Exercise and Weight Loss Programs With Online Education on Outcomes of Knee Osteoarthritis : A Randomized Trial. Ann Intern Med 2022, 175, 198–209. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Petersen, C.L.; Clark, M.M.; Cook, S.B.; Kotz, D.; Gooding, T.L.; Roderka, M.N.; Al-Nimr, R.I.; Pidgeon, D.; Haedrich, A.; et al. Feasibility and acceptability of a technology-based, rural weight management intervention in older adults with obesity. BMC geriatrics 2021, 21, 44. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA flow chart for searches.
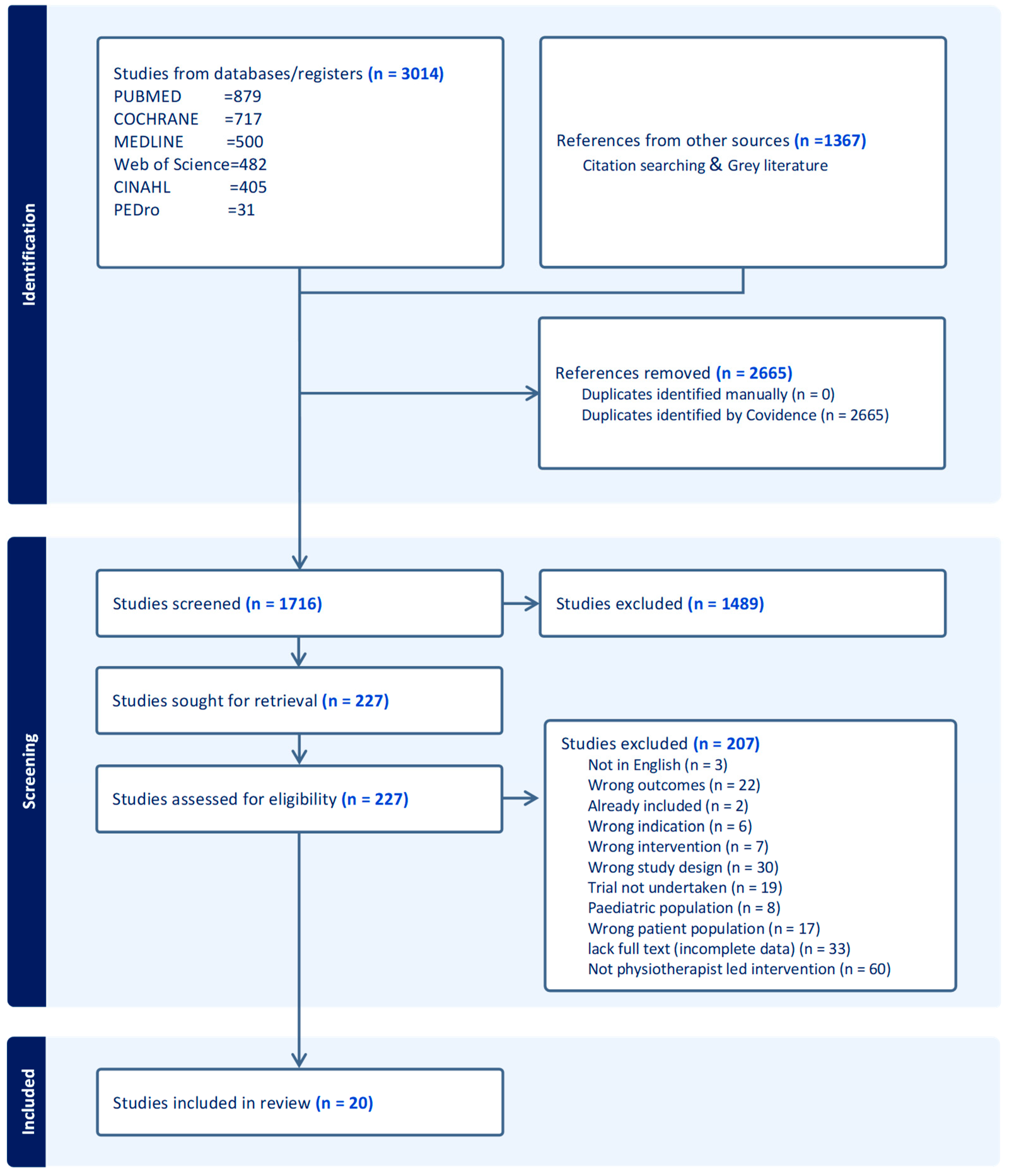

Table 1.
Search Parameters.
| Participants/population | Cardiovascular disease and risk factors block keywords, cardiovascular diseases, heart diseases, coronary artery disease, coronary heart disease, myocardial infarction, heart failure, angina, cerebrovascular disease, stroke patients, and aortic atherosclerosis patients—overweight, obesity, diabetes, blood pressure, hypertension, dyslipidaemia. |
| Concept/intervention |
Physiotherapy block keywords: Physiotherapist(s), Physiotherapy, kinesiotherapy, physical therapist(s), physiotherapy assistant. Health promotion block keywords: Patient education, health promotion, health education, health behaviour, educational technology, diet therapy, educational health promotion, group-based, individual, home and hospital-based approaches, lifestyle modification, lifestyle change recommendations, physical activity and exercise promotion, brief counselling, face to face, group sessions, skill training, visual presentation, handouts, brochures and diaries, motivational prompts, individualised plan, goal setting, nutrition and weight management, smoking cessation, sleep, stress management. |
Table 2.
Inclusion and exclusion criteria.
| Participants/Population | Concept/Intervention | Context | Study Types and Design |
|---|---|---|---|
| Inclusion criteria | |||
|
|
|
|
| Exclusion criteria | |||
| Studies on pwCVD with relevant outcomes were initiated and implemented by clinicians other than physiotherapists. |
|
|
|
Table 3.
Components and characteristics of the interventions in the included studies for pwCVDs.
| [44] | [45] | [46] | [60] | [59] | [47] | [48] | [49] | [50] | [64] | [51] | [52] | [58] | [56] | [57] | [53] | [54] | [68] | [55] | [62] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Education on lifestyle | ✓ | ✓ | ||||||||||||||||||
| Dietary education and physiotherapy | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||
| Exercise and or physical activity | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Self-management and home programs | ✓ | ✓ | ✓ | |||||||||||||||||
| Behaviour change programs on physical activity uptake | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||||
| Individualised coaching on physical activity and exercise | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||||||
| Health improvement card (HIC) | ✓ | |||||||||||||||||||
| Provision of educational materials/resources such as brochures on healthy lifestyle practices and lifestyle behaviour change | ✓ | ✓ | ||||||||||||||||||
| Workbook | ✓ | |||||||||||||||||||
| Written instructions and recommendations | ✓ | ✓ | ||||||||||||||||||
| Handouts following each session | ✓ | |||||||||||||||||||
| Technology based | ✓ | ✓ | ✓ | |||||||||||||||||
| Theory-based intervention | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||||||
| Supplemented by telephone calls | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
Table 4.
TIDIER components and the nature of PLHP interventions for pwCVDs of the included studies.
| Author Year |
Country | N | Study Design | Population | Nature of the Intervention | Intervention Duration | Theory Use | Mode of, and Delivered by | Setting(s) | Educational Component | Delivery Format | Number of Sessions | Technology | Tailoring | Fidelity |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fowler et al. 2002 [44] |
Australia | 882 | RCT | Males aged 65 to 79 years with peripheral arterial disease | Individual and community intervention for people with PAD advised participants to walk >30 minutes daily | Short (12 months) | No | Educational materials and f-t-f by PT | Combined | Yes | Combined | high | no | Yes | No |
| Bone et al. 2003 [45] |
Spain | 18 | RCT | Overweight women of 30-50 years with grade 1 hypertension | Supervised physical exercise | Short (6 months) | No | f-t-f/ supplemented by educational materials by PT | Combined | No | group | high | no | Yes | No |
| Eriksson et al. 2006 [46] |
Sweden | 151 | Randomised controlled parallel group trial | Patients diagnosed with hypertension, dyslipidaemia, type 2 diabetes, obesity, or any combination thereof are aged 18-65. | Lifestyle intervention in primary healthcare | Short (3 months) | No | f-t-f by PT and assistants, dietician and a physician | Clinical setting | Yes | group | High | no | Yes | No |
| Quinn et al. 2007[60] |
Ireland | 18 | Pre-post-test design | Obese females | Physical activity education for obese females | Short (4 months) | No | f-t-f by PT | Clinical setting | Yes | Individual | low | No | No | No |
| Pariser et al. 2010[59] |
USA | 22 | Pre-post-test design | Type 2 Diabetes patients with impaired mobility issues | Active Steps for Diabetes (Exercise and educational intervention) | Short (2months) | No | f-t-f by PT (assisted by PT student or nurse/diabetes educator) | Combined | No | Combined | High | Yes | Yes | No |
| Wisse et al. 2010 [47] |
Netherlands | 74 | RCT | Sedentary, insulin-treated type 2 diabetes | regular, structured, and personalised exercise prescription | Long (24 months) | No | f-t-f by PT supplemented with telephone calls | Combined | Yes | Individual | low | Yes | yes | No |
| Molenaar et al. 2010 [48] |
Netherlands | 203 |
RCT | Men and non-pregnant women aged 18 -65 years with a BMI of 28-35 kg/m2. | Nutritional counselling and nutritional plus exercise counselling in overweight adults. | long (13.7 months) | No | f-t-f by Dietician and PT | Clinic | Yes | Individual | low | No | yes | yes |
| Wu et al. 2011 [49] |
Taiwan | 135 | RCT | People 45 to 64 years old are at risk of developing diabetes. | Home-based exercise | Short (6 months) | Yes | f-t-f supplemented with telephone calls by PT. | Community | Yes | Individual | High | Yes | yes | Yes |
| Reid et al. 2011[50] |
Canada | 141 | RCT | Patients with acute coronary syndromes | motivational counselling intervention |
Short (12 months) | Yes | f-t-f supplemented by telephone calls. | Combined | Yes | Individual | Low | Yes | Yes | Yes |
| Oerkild et al. 2012 [64] |
Denmark | 40 | RCT | Elderly coronary heart disease above 65 years | Cardiac home program for the elderly | Short (12 months) | No | home visits in person, follow-up with telephone calls by PT | Community | Yes | Individual | Low | Yes | Yes | No |
| Takatori et al. 2012 [52] |
Japan | 44 | RCT | Chronic stroke survivors 57-89 years | Exercise therapy for post-stroke patients | Short (3monhs) | No | f-t-f by PT | Clinic | No | Individual | High | No | Yes | No |
| Higgs et al. 2016 [58] |
New Zealand | 36 | Prospective observational | Diabetic or at a high risk of developing diabetes. | Education and exercise | Short (3months) | No | f-t-f by PT, PT students and a nurse. | Clinic | Yes | Individual | High | No | Yes | Yes |
| Preston et al. 2017 [56] |
Australia | 20 | pre-post-test intervention | Patients with mild to moderate acute stroke | Self-management | Short (3months) | No | f-t-f by PT | Community | Yes | Individual | Low | No | Yes | Yes |
| Gunnes et al. 2018 [57] |
Norway | 186 | Prospective longitudinal | Adult stroke patients | Physical activity and exercise program | Long (18 months) | Yes (MI) | f-t-f and over the phone by PT | Community | Yes | Individual | High | Yes | Yes | Yes |
| Gunnes et al. 2019 [63] |
Norway | 186 | Secondary analyses of multisite RCT | Stroke patients | Individualised coaching on physical activity and exercise | Long (18 months) | Yes (MI) | F-t-f supplemented by telephone calls by PT | Clinic | Yes | Individualised | High | Yes | Yes | Yes |
| Bai et al. 2020 [53] |
China | 200 | RCT | 50-90 years | Health education based on the HIC, individualised exercise programme. Standard brochure on healthy lifestyle practices | Short (3months) | Yes (HIC) | f-t-f by PT students supervised by PT. | Community | Yes | Individualised | Low | No | Yes | No |
| Gerage et al. 2020 [67] | Brazil | 90 | RCT | Patients with primary hypertension | Behavioural change program supplemented with educational materials. | Short (3months) | Yes (VAMOS) | f-t-f by PT | Clinic | Yes | Group | Low | No | No | No |
| Batsis et al. 2021 [61] |
USA | 54 | single-arm trial | Older (65+) adults with obesity (BMI > 30 kg/m2) residing in rural New Hampshire and Vermont. | Technology-based weight management intervention | Short (6 months) | Yes (social cognitive theory, MI) | f-t-f and telemedicine (videoconferencing, remote use of Fitbit) and periodic face-to-face interaction onsite. By Dietitian and PT | Community | Yes | Combined | High | Yes | Yes | Yes |
| Bearne et al. 2022 [55] |
England | 190 | RCT | Adults with peripheral arterial disease and intermittent claudication | Walking Exercise Behaviour Change Intervention | Short (6 months) | Yes (Theory of Planned Behaviour and The Common Sense Model of Illness Representation) | face-to-face and supplemented by telephone calls by PT. | Clinic | Yes | Individualised | Low | Yes | Yes | Yes |
| Deka et al.2022 [62] | Spain | 22 | Single-arm trial | Patients with Coronary Artery Diseases | Dietary education and a high-intensity interval resistance training program (DE–HIIRT) | Short (3months) | Yes (Bandura’Self-Efficacy Theory) | f-t-f by Dietician and PT | Clinic | Yes | Combined | 22 | No | Yes | Yes |
Notes: PAD: Peripheral Arterial Diseases, f-t-f: Face-to-Face, PT: Physiotherapist, Short: <12 months, Long: >13 months, High = 16 sessions, Low = <15 sessions, HIC: Health Improvement Card, MI: Motivational Interviewing, VAMOS: Vida Ativa Melhorando a Saúde, BMI: Body Mass Index, RCT: Randomised Controlled Trial, USA: United State of America.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



