
Submitted:
02 September 2023
Posted:
20 September 2023
You are already at the latest version
Abstract
Background: Ultrasonography (US) represents the gold standard imaging method for the assessment of testicular lesions (TL). The gray-scale (GSUS) and color-Doppler (CDUS) ultrasound examination allow sonographers to investigate size, margins, echotexture and vascular features of TL, with the effort to differentiate benign from malignant lesions. Recently, the use of contrast-enhanced US (CEUS) and sonoelastography (SE) led to further improvements in the differential diagnosis of TL. Although GSUS and CDUS are often sufficient to suggest the benign or malignant nature of TL, CEUS can be decisive in the differential diagnosis of unclear findings, while SE can help to strengthen the diagnosis. The contemporary combination of GSUS, CDUS, CEUS and SE led to a new diagnostic paradigm named multiparametric US (mp-US), able to provide a more detailed characterization of TL than the single techniques alone. This narrative and pictorial review is aimed to describe the mp-US appearance of several TL. Methods: An extensive Medline search was performed identifying studies in the English language focusing on mp-US evaluation of TL. Results: a practical mp-US “identity card” and iconographic characterization of several benign and malignant TL is provided herein. Conclusions: the mp-US characterization of TL reported herein can be useful in daily clinical practice.
Keywords:
ultrasound (US)
; multi-parametric ultrasound (mp-US)
; gray-scale ultrasound (GSUS)
; color-Doppler ultrasound (CDUS)
; contrast-enhanced ultrasound (CEUS)
; sonoelastography (SE)
; testicular lesions
; testicular tumors
; differential diagnosis
1. Introduction
Ultrasonography (US) represents the gold standard imaging method for scrotal investigation, widely used to assess a variety of scrotal diseases [1,2,3]. It is a simple, rapid and harmless diagnostic tool able to provide live images of the scrotal content and, among imaging techniques, it is the least expensive [1,2,3]. Over time, the use of the US has progressively expanded since it is useful to assess scrotal features related to reproductive health, scrotal pain, masses and trauma [1,2,3].
Currently, conventional gray scale US (GSUS), supplemented by color-Doppler US (CDUS), is considered as highly sensitive in detecting testicular lesions, however with limits in delineating their nature [3]. If performed by an expert operator, scrotal US, together with clinical history and physical examination, may suggest a differential diagnosis among benign and malignant testicular lesions [4]. However, in some cases, it is difficult to discriminate the benign or malignant origin of a testicular lesion, and in case of a “likely” malignant lesion it is challenging to suggest a possible cancer type. Hence, to date, histology remains the only certain diagnostic tool to define the nature of a testicular lesion [2].
Recently, the use of contrast-enhanced US (CEUS) and sonoelastography (SE) have led to improvements in the differential diagnosis of testicular lesions [2]. This led to a new diagnostic paradigm, the so called “multiparametric US” (mp-US) [5,6], combining conventional techniques (i.e. GSUS and CDUS) with CEUS [7] and SE [8]. Although not entirely diagnostic, mp-US is able to provide a detailed characterization of testicular lesions [4,9,10]. This is relevant in clinical practice, since an accurate mp-US evaluation of a testicular lesion, beside and along with clinical assessment, is critical to define its correct management, including testicular salvage and US follow-up or orchiectomy [11]. Of note, the clinical management of large, hard palpable lumps or nonpalpable lesions is different. On one hand, when “palpable” testicular masses are found, they can be malignant in more than 90% of cases, making radical orchiectomy the standard treatment [12]. According to the EAU guidelines [13], in this scenario, scrotal US serves to confirm the presence of a testicular mass, and to explore the contralateral testis. Anyway, every patient with a palpable testicular mass must undergo surgical exploration, with orchiectomy if malignancy is found [12]. On the other hand, when nonpalpable testicular lesions are detected, often incidentally during a scrotal US performed for different reasons (e.g. male infertility, varicocele, history of cryptorchidism, scrotal pain or trauma), the clinical management is more cautious. In fact, these lesions are small and mostly benign [14,15], so unnecessary orchiectomy must be avoided, however they can also be malignant and can grow over time. In this scenario, US is useful in the follow-up of the small lesions and in detecting testicular US-related risk factors for malignancy (e.g. cryptorchidism and microlithiasis), suggesting surgery in case of growth/modification of small nodules, especially if testicular tumor-related risk factors (e.g. age 15 to 40 years old, family history of testicular tumors, history of contralateral testicular tumor, cryptorchidism or oligo-/azoo-spermia) are present [1]. Hence, either in case of palpable testicular masses or, especially, in case of small testicular lesions, US is useful. In particular, mp-US can help in distinguishing with good accuracy benign and malignant lesions, providing a more detailed characterization than the CDUS, CEUS or SE alone.
The role of mp-US for characterizing testicular lesions has been investigated in some retrospective and prospective studies [16,17,18,19,20,21], mainly focusing on diagnostic accuracy. This review aims to summarize and update these reports, providing an “identity card” description and a wide iconographic characterization of the GSUS, CDUS, CEUS and SE appearance of several common and uncommon benign and malignant testicular lesions.
2. Methods
An extensive Medline search was performed with no restrictions regarding date of publication (i.e. from inception date until July 2023) including the following words: ("ultrasonography" [MeSH Terms] OR “ultrasound” [Text Word] OR "diagnostic imaging" [Subheading]) AND (“multiparametric” [All Fields] OR "contrast media"[MeSH Terms] OR "elasticity imaging techniques" [MeSH Terms] OR “elastography” [Text Word]) AND (“testicular” [All Fields] AND “lesions” [All Fields] OR "testicular neoplasms" [MeSH Terms] OR “testicular tumors” [Text Word]) AND ("diagnosis, differential"[MeSH Terms] OR “differential diagnosis” [Text Word]). The identification of relevant studies in the English language was performed independently by the authors. Studies focused on multiparametric US of testicular lesions without strict inclusion and exclusion criteria have been identified and reported in the present narrative review. Original pictures reporting GSUS, CDUS, CEUS and SE appearance of several benign and malignant testicular lesions have been recorded and are here provided.
3. Diagnostic steps to perform before running mp-US
Clinical history and physical examination are very important to suggest a correct diagnosis when facing a testicular lesion and should be performed before running US.
Anamnesis should investigate age (testicular cancer represent the most common malignancy in young men aged 15 to 40 years), family history of testicular tumors, history of contralateral testicular tumor, history of cryptorchidism/orchiopexy and history of infertility, which represent the main risk factors associated with testicular tumors [1,13]. In addition, previous testicular inflammation (orchitis), torsion, trauma and other relevant diseases (i.e. Klinefelter syndrome) useful to define a differential diagnosis should be assessed [1,2,3,13]. Patients should be asked to describe eventual signs (testicular mass/nodule, testicular swelling or enlargement, new onset hydrocele, sometimes revealed by self-examination by the patient) and symptoms (i.e. scrotal pain or heaviness, fever, back pain, new onset gynecomastia), together with the moment of onset and their duration [13]. Performing a physical examination before starting US is always recommended: usually palpable hard and large masses are suggestive of testicular tumors while non-palpable lesions are in most cases benign lesions, however to be assessed carefully [1,2,3,13].
4. Mp-US methodological standards
Mp-US is increasingly recognized as a valuable problem-solving technique in scrotal pathologies, and in particular in differential diagnosis of testicular lesions [9,22,23]. Mp-US combines conventional techniques (GSUS and CDUS), CEUS and SE [9,22,23], which methodological standards in evaluating scrotal organs and, in particular, testicular lesions, are relatively recent [2,24].
Scrotal/testicular color-Doppler ultrasonography (CDUS)
The standardization of the methodology used to perform scrotal color Doppler ultrasonography (CDUS) is relatively new. Practical recommendations for performing scrotal CDUS have been reported by the SIU/SIEUN collaboration in 2014 [25] and in the AIUM Practice Guideline in 2015 [25,26]. More recently, a detailed description of the Standard Operating Procedures to evaluate scrotal quantitative and qualitative parameters, and assessment of the CDUS intra- and inter-operator comparability, have been reported by the European Academy of Andrology for the entire male genital tract [24,27,28,29]. The EAA-proposed SOPs to assess scrotal CDUS and, in particular, testicular lesions, have been reported elsewhere [2,24,28] (see https://www.andrologyacademy.net/eaa-studies). In particular, testicular US should be performed with a high frequency linear transducer, with the patient in supine position. A US scan of both testicles should be performed, including longitudinal, oblique and transverse scans, with slow, continuous side-to-side movements that allow assessment of the entire parenchyma. The operator should evaluate at GSUS the volume of the testes, the echogenicity, the echotexture, the possible presence of testicular calcifications or microlithiasis, and vascularization by CDUS, comparing the two sides. Testicular lesions should be accurately evaluated in longitudinal, oblique and transverse scans. A complete evaluation should include: 1) diameters (length x height x width); 2) position and extension; 3) type (solid, cystic, mixed), homogeneity (homogeneous/inhomogeneous) and echogenicity (hypoechoic, hyperechoic, anechoic); 4) presence of intralesional calcifications; 5) shape (regular or irregular) and margins (clean-cut, smooth, multi-lobed, infiltrating) and 6) vascularization pattern (absent, peripheral, intranodular).The images must be stored to be used for comparison during follow-up. The report must also describe, beside the lesion, US characteristics of both testicles and must specify the absence of lesions in the contralateral testicle [1,2,3,24,28].
Contrast-enhanced US (CEUS)
The methodological standards for the clinical practice of contrast-enhanced US (CEUS) in non-hepatic applications, including scrotum investigation, have been reported by the EFSUMB Guidelines [30]. As a result, the assessment of some pathological conditions using CEUS has improved [7,30]. Using time-intensity curves, evaluating the wash-in and wash-out curves may help to distinguish malignant from benign tumors, although CEUS analyses still overlap between different histological types [7]. In addition, CEUS can discriminate non-viable regions in testicular trauma and can identify segmental testicular infarction [7,30].
For CEUS, a dedicated machine-setting with a low mechanical index (0.05–0.08) is needed to avoid early microbubble destruction. US contrast medium (very small-sized organic shells filled with gas with high impedance) should be injected as intravenous bolus and followed immediately by 10 mL of 0.9% saline solution. The entire examination needs to be recorded to perform qualitative and quantitative analyses [7].
Sonoelastography (SE)
The methodological standards for the clinical practice of sonoelastography (SE) in non-hepatic applications, including testicular investigation, have been reported by the EFSUMB Guidelines and Recommendations [31]. So far, strain elastography and shear wave elastography, which includes acoustic radiation force impulse based techniques, and transient elastography are available. The basic principles of SE have been extensively described in previous EFSUMB guidelines [32], while methodological standardization for different organs, including the testis, are reported in the updated EFSUMB guidelines [31]. In particular, a specifical setting should be applied, and images and cine loops should be stored for qualitative (color-coded images) and semi-quantitative evaluation of dynamic features (strain ratio on cine-loop) [6]. From a methodological point of view, the use of SE to investigate focal testicular lesions can only be recommended in conjunction with other US techniques, as there is overlap between benign and malignant neoplasms [31,33]. SE assessing overall background parenchyma has been used also to investigate infertility, testicular microlithiasis and undescended testis [31], however, currently, these specific applications are restricted to research.
5. Non-neoplastic testicular lesions
Several non-neoplastic diseases can occur within the testes, and may mimic testicular tumors. Differential diagnosis may be difficult but is imperative to avoid unnecessary surgical interventions. A summary of the clinical characteristics and mp-US features of non-neoplastic testicular lesions is provided in Table 1, and their mp-US appearance is reported in Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, Figure 6, Figure 7, Figure 8 and Figure 9.
5.1. Intratesticular cysts
Prevalence: Intratesticular cysts are rare in pediatric patients [34,35] and in young-adult men, while their prevalence in subjects aged > 40 years old has been estimated 8% to 10% [35].
Clinical history and physical examination: Simple intratesticular cysts are usually asymptomatic. They are often incidentally detected during US as they are usually not palpable [36]. However, they can even be palpable, since their size can range from 2 mm to 2 cm [37]. On palpation, they have a soft or tense-elastic consistency.
GSUS + CDUS: At GSUS examination, intratesticular cysts appear as solitary, or less commonly multiple, anechoic lesions, with a thin, clear, hyperechoic wall, and posterior acoustic enhancement [35]. They often occur near the mediastinum and can be simple or complex (if they have internal septa). Usually, they do not contain solid portions. Only when complicated by an infection or an internal hemorrhage they may appear as hypoechoic or mixed echogenicity lesions [36]. At CDUS they show absent internal vascularization.
SE: Intratesticular cysts generally appear as soft lesions showing a tricolor pattern, blu-green-red [20].
CEUS: CDUS is usually sufficient for the diagnosis of a testicular cyst and CEUS is not necessary. However, if CEUS is performed, intratesticular cysts show absent contrast enhancement [20].
Differential diagnosis: complex testicular cysts must be differentiated from cystic teratomas. Complex teratomas tend to have solid, outlying, vascularized masses, rather than fibrous strand [36]. As a corollary, besides teratomas, cystic areas can be found in embryonal carcinomas, yolk sac tumors and choriocarcinomas, but they are included in the solid lesion (see below).
5.2. Epidermoid cysts
Prevalence: Epidermoid cysts represent 1.5-2.1% of all testicular benign tumors of germ cell origin among men aged 20 to 40 years [38].
Clinical history and physical examination: At physical examination, they are palpable painless non-tender nodules (single or multiple) of size ranging 1 to 3 cm [39,40]. Some epidermoid cysts have a tendency to increase in size over time, hence at clinical history and physical examination they can be described as a firm nodule growing slowly. Very rarely, in post-pubertal subjects, they have been described as associated with/part of part of invasive testicular germ cell tumors, representing a teratoma [40].
GSUS + CDUS: At GSUS, testicular epidermoid cysts show a variable appearance depending on their maturation, compactness, and amount of keratin component. They can be classified into four categories: type 1, well circumscribed rounded lesions with “onion-ring” pattern consisting of concentric rings of hypoechogenicity and hyperechogenicity (Figure 1, Panel A); type 2, densely echogenic and calcified masses with a dark acoustic shadow; type 3, “target” appearance lesions consisting of a hypoechoic rim with a central area of increased echogenicity; type 4, mixed pattern lesions [41]. The onion-ring pattern, which corresponds to lamellar layers of keratin, is the most typical, accounting for about 60% of cases [42]. CDUS examination shows absent vascularization within the cyst (Figure 1, Panel B).
SE: Testicular epidermoid cysts demonstrate hard SE properties, showing low/absent elastic strain [41] (Figure 1, Panel C).
CEUS: No contrast enhancement is expected after contrast administration, as the lesion is avascular; occasionally it can be present a rim enhancement [41,43] (Figure 1, Panel D).
Differential diagnosis: An atypical epidermoid cyst may be mistaken for a malignant tumor, namely embryonal carcinoma with internal necrosis and calcified margins (Figure 2, Panel A), as they both can appear as avascular lesions at CDUS and CEUS (Figure 2, Panel B) and hard at SE. Serum tumor markers can be helpful in differential diagnosis, as well as the meticulous study of the margins, which are usually well demarcated in epidermoid cyst and irregular in malignant tumors. In this scenario, differential diagnosis is decisive, since while the suspicion of a malignant testicular tumor requires orchiectomy, that of an epidermoid cyst, usually benign, avoids the removal of the entire testicle. However, even if epidermoid cysts show a typical “benign” pattern at US, due to the tendency of increase in size over time both in pediatric and adult patients, and to the rare association with testicular germ cell tumor, usually they are treated with testis-sparing surgery associated with biopsies of the surrounding parenchyma [40].
5.3. Testicular Adrenal Rest Tumors (TARTs)
Prevalence: TARTs are benign lesions occurring in nearly 40% of patients with congenital adrenal hyperplasia (CAH) [44].
Clinical history and physical examination: TARTs are supposed to originate from an adrenal-like pluripotent stem cell type rising from the urogenital ridge, already present in the gonads during the embryogenesis, which undergo adrenal differentiation and increased proliferation under stimulation of high levels of adrenocorticotropic hormone (ACTH) [44]. Generally TARTs are bilateral and non-palpable due to their occurrence near or within the mediastinum, and a firm mass can be palpated only when the lesion exceeds 2 cm in diameter [44].
GSUS + CDUS: At GSUS examination TARTs usually appear as hypoechoic lesions with irregular, lobulated margins, or less frequently as hypoechoic lesions with hyperechogenic foci, and rarely as hyperechogenic lesions [44] (Figure 3, Panel A). CDUS shows markedly increased intralesional blood flow (Figure 3, Panel B).
SE: TARTs usually appear as hard lesions showing low/absent elastic strain [45] (Figure 3, Panel C).
Differential diagnosis: It is challenging to discriminate TARTs from other tumors based on their US appearance. However, TARTs are typical findings in patients with CAH. Moreover, their size might decrease with proper glucocorticoid treatment. In addition, TARTs are usually bilateral, an uncommon occurrence in malignant tumors. If small, they can be similar to Leydig cell tumors at GS [48]. Hence, the patient’s clinical history, the occurrence within the mediastinum and bilaterality of the lesions can help clinician in the management and appropriate follow-up of these lesions, often avoiding unnecessary orchiectomy [44].
5.4. Sarcoidosis
Prevalence: Sarcoidosis is a multisystem disease involving lungs, lymph nodes, kidneys, skin, liver, and spleen, characterized by noncaseating granulomas. The reported prevalence of sarcoidosis-related testicular involvement is 4-4.5%, with only 0.5% of symptomatic patients [49].
Clinical history and physical examination: Testicular sarcoidosis is usually asymptomatic, being incidentally detected during patients’ diagnostic work-up [50]. When clinically manifest, testicular sarcoidosis presents as painless or painful nodules [51].
GSUS + CDUS: At GSUS sarcoidosis appears as single or more typically multiple and bilateral small hypoechoic lesions with irregular margins [4,50] (Figure 4, Panel A). At CDUS testicular sarcoidosis granulomas can show some internal vascular spots [4,52,53] (Figure 4, Panel B).
SE: sarcoidosis granulomas appear as hard lesions showing low/absent elastic strain [4] (Figure 4, Panel C).
5.5. Segmental testicular infarction
Prevalence: Segmental testicular infarction is a rare clinical and US entity [55]. Most of the cases have been reported as idiopathic; it can also occur as a sequela of recent surgery, inflammatory and infective events, blood disorders such as sickle cell disease and polycythemia, or autoimmune diseases such as vasculitis [55,56].
Clinical history and physical examination: Segmental testicular infarction frequently presents with an acute painful, swollen scrotum, especially in men aged 20 to 40 years [57,58]. However, clinically silent cases have been described [55].
GSUS + CDUS: At GSUS evaluation segmental testicular infarction appears as a hypoechoic wedge-shaped lesion [55], usually involving the upper third of the testicle due to poor collateral vessels [59] (Figure 5, Panel A). CDUS shows absent internal vascularization, and a peripheral rim of low vascular signal may be observed [55] (Figure 5, Panel B).
SE: It appears at SE as a soft lesion showing high elastic strain [4].
CEUS: CEUS can confirm the absence of vascularization within the lesion (Figure 5, Panel C); in cases of subacute testicular infarction, a peripheral hyperenhancing rim can be detected, corresponding to histologic evidence of granulation tissue. During follow-up the peripheral hyperemic rim diminishes [60].
Differential diagnosis: In some cases, the US appearance of segmental testicular infarction can be round-shaped resembling a testicular tumor [55]. A helpful US feature to distinguish segmental infarction from a testicular tumor is markedly decreased or absent vascular flow at CDUS imaging or at CEUS. In ambiguous cases, the patient’s clinical history and lesion size reduction during follow-up can help the clinician [60].
5.6. Abscess
Prevalence: Testicular abscess is an unusual finding, complicating 3–5% of epididymitis and epididymo-orchitis [61]. It may also occur as a complication of mumps, trauma or infarction [39].
Clinical history and physical examination: Patients are usually symptomatic, presenting with acute scrotal pain and swelling and frequently with an elevated white blood cell count and fever. Patients often have comorbidities such as diabetes mellitus, human immunodeficiency virus infection or other immunosuppressive conditions [3].
GSUS + CDUS: GSUS appearance is of a focal, complex, heterogeneous low reflecting lesion with irregular margins [51]. In rare cases, focal hyperechoic spots with posterior shadowing may be present, corresponding to gas bubbles within the abscess cavity [62] (Figure 6, Panel A). At CDUS, a hypervascular rim may surround the lesion, with no internal vascular signal [4] (Figure 6, Panel B).
SE: Testicular abscess shows at SE a heterogeneous pattern of firmness [4] (Figure 6, Panel C).
CEUS: CEUS demonstrates absence of internal contrast-enhancement with some peripheral enhancement [4,63,64] (Figure 6, Panel D).
Differential diagnosis: In some cases, a testicular abscess can resemble a testicular tumor, although it never shows internal vascularization. Evidence of epididymitis/epididymo-orchitis, reactive hydrocele and scrotal skin thickening could be present in case of testicular abscess. Serial US examinations to ensure resolution should be performed.
5.7. Hematoma
Prevalence: Intratesticular hematomas are a possible sequela of a scrotal trauma, which is the third most common cause of acute scrotal pain after epididymo-orchitis and testicular torsion.
Clinical history and physical examination: A history of scrotal trauma is usually related to the detection of hematoma at US, even if not all patients report this event [65].
GSUS + CDUS: Hematomas US features change in time according to the evolving of blood products [59]. In the acute phase, hematomas appear as well-circumscribed hyperechoic lesions which subsequently liquefy over time, becoming complex lesions with septa, cystic components, and fluid levels [39,61] (Figure 7, Panel A). Typically, hematomas’ size decreases in time [Citation error]. At CDUS imaging there is no signal of internal vascularization [61] (Figure 7, Panel B). It is essential to investigate the vascularization of the residual parenchyma to assess its degree of vitality, and CEUS can be helpful in this context [61,62]. Moreover, CEUS can be useful in ambiguous cases to discriminate between intratesticular hematoma and tumor [66].
SE: Intratesticular hematomas show predominantly “soft” SE properties with intermediate/high elastic strain [67] (Figure 7, Panel C).
CEUS: CEUS confirms the absence of vascularity within the lesion. Peripheral rim and internal septa enhancement may be present [67] (Figure 7, Panel D).
Differential diagnosis: Especially when a scrotal trauma does not occur temporally close to US evaluation, hematomas may mimic testicular tumors [65]. However, performing close, serial US evaluation to assess hematomas’ size decreasing can help in the differential diagnosis.
5.8. Viral orchitis and bacterial orchitis (epididymo-orchitis)
Prevalence: The majority of orchitis originate with a previous epididymitis, later on extending to the testis (44–47% of cases). In this case, the etiology is mainly bacterial [1,2]. Conversely, primary orchitis is mainly viral in origin (mumps orchitis), occurring in 20– 30% of infected postpubertal men [1,2,37].
Clinical history and physical examination: Primary orchitis is less common than epididymo-orchitis and mostly caused by mumps during or after puberty [37]. Epididymo-orchitis is usually following epididymitis, mainly due to urinary tract infections (e.g. Escherichia coli) in young boys and sexually transmitted organisms (e.g. Naisseria gonorrhoeae and Chlamydia trachomatis) in older patients, although urine cultures are positive in only 10-25% of cases [1-3,37]. Clinically, gradual onset of pain (especially in epididymo-orchitis) or acute scrotum can occur. Both primary and secondary orchitis present with painful hemiscrotum and testis enlargement, usually bilateral in the primary form and unilateral in the secondary form, the latter often associated with epididymal enlargement or tenderness or pain [1-3]. Scrotal edema, fever and pyuria may occur.
GSUS + CDUS: The testis appears enlarged, diffusely hypoechoic and inhomogeneous at GSUS and diffusely hyperemic at CDUS [1-3,4,20].
Differential diagnosis: When an enlarged, hard, hypoechoic and diffusely hyperemic testis is detected at US, differential diagnosis should be considered with large seminomas or lymphomas. The occurrence of bilateral orchitis in postpuberal boys or of concurrent epididymitis in adult men can help to suggest primary or secondary orchitis, respectively, instead of large malignancies.
5.9. Idiopathic granulomatous orchitis
Prevalence: Idiopathic granulomatous orchitis, an inflammatory condition of the testis of unknown aetiology, is rarely encountered [68,69]. The condition tends to present in a wide age range (19–84 years), with the highest frequency between 50 and 70 years of age [70].
Clinical history and physical examination: Idiopathic granulomatous orchitis is characterized by the presence of non-specific granulomatous inflammation and admixed multinucleated giant cells [67]. Histologically, there is extensive destruction of seminiferous tubules with tubular or interstitial pattern of granulomatous inflammation and prominent collagen fibrosis. Diffuse granulomatous orchitis clinical presentation includes scrotal pain and testicular enlargement [71].
GSUS + CDUS: At GSUS, idiopathic granulomatous orchitis appears as diffusely hypoechoic testis or focal hypoechoic areas with ill-defined margins (Figure 8, Panel A) [72]. CDUS often shows hypervascularization (Figure 8, Panel B) [39].
SE: At SE, focal orchitis appears predominantly with a heterogeneous pattern of firmness (Figure 8, Panel C) [8,20].
CEUS: At CEUS, diffuse vascular hyperenhancement throughout the lesions can be observed (Figure 8, Panel D) [73].
Differential diagnosis: In case of diffuse orchitis, there is a high suspicion of testicular malignancy, and physical examination fails to differentiate benign from malignant condition [71]. In this scenario, other signs of inflammation such as scrotal wall thickening and hydrocele may help in the differential diagnosis with testicular tumor [43].
5.10. Infectious granulomatous orchitis
Prevalence: Infective granulomatous orchitis is very rare and can be caused by tuberculosis, brucellosis and actinomycosis [72]. Tuberculous orchitis usually results from contiguous extension from the epididymis. Infectious granulomatous orchitis can be acute or chronic. In the acute form, patients present with sudden onset of pain, while in the chronic form, they usually present with unilateral scrotal swelling. In some cases, granulomatous orchitis presents as a single or multiple testicular mass and can be suspicious of malignancy.
Clinical history and physical examination: Focal granulomatous orchitis clinical presentation includes acute scrotal pain, fever, and testicular enlargement [71]. Epididymal involvement is common in infectious granulomatous orchitis, especially tuberculosis, as well as concurrent septated hydrocele, scrotal wall edema and calcification of the tunica vaginalis.
GSUS + CDUS: In genitourinary tuberculosis, both the GS- and CD-US appearances of the testes can be explained by various pathologic stages of tubercular infection which include caseous necrosis, granulomas, and healing by fibrosis and calcification [39]. Generally, at GSUS, focal orchitis appears as a single or multiple hypoechoic lesion/s with variable echogenicity and blurred or well-defined margins (Figure 9, Panel A). Vascularization can be internal or peripheral (Figure 9, Panel B).
SE: At SE, focal orchitis can appear both as soft and as hard lesions [8,20], depending on the stage of infection (Figure 9, Panel C).
CEUS: In focal orchitis, CEUS can vary from uniform vascular enhancement throughout the lesions [73] to unenhanced lesions with peripheral rim, depending on the stage of the infection (Figure 9, Panel D).
Differential diagnosis: Imaging features of testicular tuberculosis are non- specific and often impossible to distinguish from other more common pathologies such as tumor, infection, inflammation, and infarction [74]. In this scenario, other signs of inflammation such as scrotal wall thickening, hydrocele and most of all epididymitis, favors the diagnosis of infection [75]. In the suspicion of a tubercular infection, it is mandatory to perform microbiological analysis (e.g. Mantoux test).
6. Neoplastic testicular lesions
Testicular cancers are rare tumors, accounting for ~1% of adult neoplasms, but represent the most common malignancies in young men aged 15 to 40 years, with increasing incidence rates in many countries in the last two decades [76,77,78].
According to the most recent World Health Organization (WHO) histological classification [79] testicular tumors can be distinguished in two main groups: 1) testicular germ cell tumors (TGCTs), which are the most common (~98% of all testicular cancers), in turn divided into two subclasses, seminomatous (s-TGCTs) and non-seminomatous (ns-TGCTs), and 2) stromal cell tumors, which are rare, even if probably underestimated. In addition, malignancies with testicular localization derived from non-testicular neoplasms (non-primary malignant tumors, i.e. hematologic tumors and metastases) must be considered.
Testicular tumors usually present as painless or paucisymptomatic (heaviness, swelling) testicular masses. In some cases, they are incidentally found during US performed for other reasons.
Serum tumor markers must be included in the diagnostic work-up, and specifically alpha fetoprotein (⍺-FP), beta subunit of human chorionic gonadotropin (β-hCG) and lactate dehydrogenase (LDH) [80,81]. Overall, serum tumor markers show low sensitivity (especially in seminoma) and, if negative, the diagnosis of testicular tumor cannot be excluded [82]. However, if positive, they allow for an almost certain diagnosis of testicular cancer and in prognosis, and they can help in differential diagnosis (for example positive ⍺-FP and β-hCG are more frequent in ns-TGCTs than in s-TGCTs, and high levels can be found in burned out tumors; see below). Of note, patients with positive β-hCG often have gynecomastia, since β-hCG is very similar to LH hormone which has a direct action in stimulating male breast tissue [83,84].
A summary of the clinical characteristics and mp-US features of neoplastic testicular lesions is provided in Table 2 and their mp-US appearance is reported in Figure 10, Figure 11, Figure 12, Figure 13, Figure 14, Figure 15, Figure 16 and Figure 17.
6.1. Seminomatous TGCTs (s-TGCTs)
Prevalence: s-TGCTs represent 55-60% of TGCTs. The median age at diagnosis is 20-40 years [85]. They are revealed as components of mixed TGCTs in 30% of cases.
Clinical history and physical examination: Patients with s-TGCTs can refer to clinicians for the detection of a testicular firm mass, testicular swelling, testicular pain, or lumbar pain when lymph node metastases are present. However, the diagnosis can be incidental during US performed for other reasons. Infertility [86,87,88] and cryptorchidism [89,90] are common risk factors for seminomas. Physical examination usually reveals a large, hard testicular mass. However, sometimes they are incidental findings at US, since small lesions (<1.5 cm) are not always palpable, especially if placed in the center of the testicle.
GSUS + CDUS: The US appearance reflects the histological characteristics which consist in a nest of large, round cells with abundant cytoplasm and distinct borders, with fibrous septa containing lymphocyte infiltration. Occasionally they can include syncytiotrophoblasts. Necrosis, intercellular edema and hemorrhage can be present, especially in larger tumors [79,91]. Therefore, at GSUS evaluation, classic seminomas usually appear as focal round homogeneous lesions, hypoechoic to the normal surrounding parenchyma [92,93,94] (Figure 10, Panel A). However, large seminomas can also appear as inhomogeneous lesions with hypo/anechoic internal areas, reflecting tumor necrosis and/or bleeding [95]. Margins can be regular, irregular, or polylobate. Microlithiasis in the affected testicle is common [96,97]. CDUS shows increased peripheral and internal vascularization [92] which is commonly characterized by arborization and branches (Figure 10, Panel B).
SE: Seminomas usually appear as hard lesions showing low/absent elastic strain [8,98,99] (Figure 10, Panel C).
CEUS: Seminomas usually shows hyperenhancement of the whole lesion after CEUS administration, apart from necrotic areas. A rapid wash-in and wash-out are distinctive characteristics of seminomas [43] (Figure 10, Panel D).
Differential diagnosis: Several neoplastic and non-neoplastic conditions may mimic testicular seminomas at imaging. Among non-neoplastic conditions, testicular inflammation, including orchitis with or without abscess formation, may mimic seminoma. In the acute phase of orchitis, diffuse testicular edema results in a hypoechoic appearance of the testis which is enlarged compared to the contralateral. Helpful imaging findings to suggest orchitis instead of seminoma include hypoechogenicity (edema) and hypervascularization of the ipsilateral epididymis, reactive hydrocele, associated scrotal edema and pain [11]. Among neoplastic conditions, non-seminomatous testicular germ cell tumors (ns-TGCTs) and lymphomas may mimic seminomas. Although seminomas, especially when large, may demonstrate cystic spaces and calcifications, these findings are more commonly encountered in ns-TGCTs. Ns-TGCTs are more likely to have ill-defined margins than seminomas, and age at the diagnosis can help (younger in ns-TGCT, older in seminomas). Lymphomas' US appearance can overlap that of seminomas, but the affected patient population is significantly older [11]. Finally, the imaging appearance of small seminomas can resemble that of Leydig cell tumors (LCTs; see below).
6.2. Non-seminomatous TGCTs (ns-TGCTs)
Prevalence: Ns-TGCTs represent 40-45% of TGCTs. They usually occur in younger patients than s-TGCTs (median age at diagnosis 25 years) [85].
Clinical history and physical examination: Similar to patients with seminomas, those with ns-TGCTs can refer to clinicians for detection of a testicular mass, testicular swelling, testicular pain, or lumbar pain when lymph node metastases are present. Due to a faster growth of ns-TGCTs, incidental diagnoses are rare, but possible [100,101].
Gynecomastia is a frequent finding [102]. Serum tumor markers, namely β-hCG and ⍺-FP, are frequently positive, especially when distant metastases are present.
Ns-TGCTs are a heterogeneous group of tumors including different malignancies, such as embryonal carcinomas, teratomas, choriocarcinomas, yolk sac tumors and mixed germ cell tumors, whose mp-US characteristics are reported below.
6.2.1. Embryonal carcinoma
Prevalence: Embryonal carcinoma accounts for about 3% of TGCTs. It represents the most frequent (80%) component in mixed TGCTs.
Clinical history and physical examination: see above (paragraphs 6 and 6.2).
GSUS + CDUS: At GSUS embryonal carcinoma often appears as an hypoechoic and/or inhomogeneous lesion, frequently with internal calcifications [73] (Figure 11, Panel A). US features may reflect histological features, which consist in significant anaplasia and necrotic areas. Sometimes these tumors may appear as hypoechoic lesions with calcified margins [103] that may mimic an epidermoid cyst. Focal areas of necrosis and hemorrhage are frequent: at US examination, they appear as anechoic areas (in case of recent hemorrhage) or hyperechoic areas (in case of organized necrosis or hemorrhage). The margins are mainly irregular and polylobulated [104]. CDUS commonly shows increased peripheral and internal chaotic vascularization, even if in a minority of cases they could be avascular if completely necrotic (Figure 11, Panel B).
SE: embryonal carcinomas usually appear as hard lesions showing low/absent elastic strain [105] (Figure 11, Panel C).
CEUS: CEUS is usually not recommended for very large lesions with positive serum tumor markers, as embryonal carcinoma usually appears, but can be useful in smaller lesions. Embryonal carcinomas show an inhomogeneous hyperenhancement [106] of the lesion after CEUS administration with rapid wash-in and rapid wash-out (Figure 11, Panel D). However, in rare cases, the lesions may also fail to pick-up the contrast medium [43,106], making it more difficult to diagnose the differential diagnosis (i.e. with atypical epidermoid cyst).
Differential diagnosis: The differential diagnosis of embryonal carcinoma is usually with other ns-TGCTs, especially mixed ones due to large size, and is not always possible. Internal calcifications, if present, are usually hallmarks. Embryonal carcinoma with internal necrosis and calcified margins can be mistaken with an atypical epidermoid cyst (see above) [3]. Serum tumor markers can be helpful, as well as the meticulous study of the margins which are usually irregular in embryonal carcinoma and well demarcated in epidermoid cyst.
6.2.2. Teratoma
Prevalence: Teratomas account for about 5-10% of TGCTs.
Clinical history and physical examination: see above (paragraphs 6 and 6.2).
GSUS + CDUS: Teratoma is composed of different somatic tissues, derived from one or more germinal layers (endoderm, mesoderm, and ectoderm). They are usually divided in mature and immature tumors according to histology and in prepubertal and postpubertal according to the age of incidence. Pre-pubertal tumors are usually benign and have a conservative treatment [107], while post-pubertal tumors (both mature and immature) can have malignant attitude and metastasize.
The US appearance varies according to the different histological features of the tumor [93]. They usually appear as well defined lesions with regular margins. Echotexture can include cystic areas (cystic teratomas), with internal septa, with different content (serous, mucoid, keratinous) [94,108,109]. A differential diagnosis with simple, complex or epidermoid cyst may sometimes be difficult. Focal calcifications are also common and are mainly due to the presence of cartilage and immature bone tissue [94]. CDUS commonly shows increased peripheral and internal vascularization in the solid portion of the lesion.
SE: As other TGCTs, teratomas usually appear as hard lesions showing low/absent elastic strain [105], but depending on the amount of liquid inside they can also have higher elastic strain [98,105].
CEUS: Teratomas show hyper-enhancement within the solid part of the lesions with rapid wash-in and rapid wash-out. Anechoic areas usually are non-enhanced.
Differential diagnosis: The differential diagnosis of teratoma is usually with other ns-TGCTs, especially mixed ones due to large size and is not always possible. Internal cysts, if present, different content, and internal septa are usually hallmarks.
6.2.3. Choriocarcinoma
Prevalence: Choriocarcinoma accounts for about 0.5-1% of TGCTs. They represent about 5-10% of mixed TGCTs.
Clinical history and physical examination: see above (paragraphs 6 and 6.2). Specifically, choriocarcinomas have a more aggressive attitude compared to other ns-TGCTs, with a higher frequency of blood rather than lymphatic metastases [110]. β-hCG levels are usually very high and therefore they are frequently associated with gynecomastia [94].
GSUS + CDUS: Choriocarcinoma can appear as a large, solid inhomogeneous mass, with calcifications and areas with different echogenicity due to necrosis and/or hemorrhages [94,95,104]. However, the GS aspect is not specific and a differentiation from other non-seminomatous tumors is not always easy. At CDUS, peripheral and internal vascularization is highly represented.
SE: choriocarcinomas usually appear as hard lesions showing low/absent elastic strain [105].
CEUS: due to the aggressiveness of the tumor and the frequent positivity of serum testicular markers, the diagnosis can be done with GS- and CD-US and it is not necessary to perform CEUS. However, at CEUS, choriocarcinomas show hyper-enhancement with rapid wash-in and rapid wash-out.
Differential diagnosis: The differential diagnosis of choriocarcinoma is usually with other ns-TGCTs and is not always possible. It could be difficult to distinguish pure forms from mixed ones.
6.2.4. Yolk sac tumor
Prevalence: Yolk sac tumor is very rare in adults (0-1%) in its pure form while it is the most common TGCT in children (60%). It represents 40% of mixed TGCTs.
Clinical history and physical examination: see above (paragraphs 6 and 6.2). Of note, serum ⍺-FP are usually high in these tumors [104].
GSUS + CDUS: Yolk sac tumors usually appear at CDUS as large, solid inhomogeneous masses, with multiple internal anechoic gaps [94,104]. At CDUS, peripheral and internal vascularization is highly represented.
SE: Yolk sac tumors usually appear as hard lesions showing low/absent elastic strain.
CEUS: diagnosis is usually performed with GS and CDUS and it is not necessary to perform CEUS.
However, at CEUS they show hyper-enhancement with rapid wash-in and rapid wash-out.
Differential diagnosis: The differential diagnosis of yolk sac tumor is usually with other ns-TGCTs and is not always possible. It could be difficult to distinguish pure forms from mixed ones.
6.2.5. Mixed germ cell tumor
Prevalence: Mixed germ cell tumors account for about 20-40% of TGCTs.
Clinical history and physical examination: see above (paragraphs 6 and 6.2). Of note, mixed germ cell tumors are the most common of ns-TGCTs and they include the various tumor types described above, including the seminomatous and non- seminomatous components, with various percentages within the tumor lesion.
GSUS, CDUS, CEUS and SE reflect the features of the different components and their representation within the lesion (Figure 12, Panel A-D).
6.3. Stromal cell tumors
Prevalence: Stromal cell tumors account for about 3-5% of testicular tumors in adults and 25% in children [107,111]. However, their prevalence is probably underestimated, and according to the recent scientific literature they represent up to 22% of nonpalpable testicular nodules [112].
Clinical history and physical examination: In adults, stromal cell tumors are usually incidental findings detected at US performed for other reasons [113]. Specifically, according to many reports, stromal cell tumors, and in particular Leydig cell tumors (LCTs), are frequent incidental findings in infertile patients [111,114,115]. However, in case of large tumors, enlargement of the scrotum is reported and can be the first reason for medical consultation.
In children and adolescents, LCTs can lead to precocious puberty, due to the excessive androgen production, or gynecomastia, caused by estrogen excess due to androgen aromatization [116]. In adults, excessive androgen secretion is exceptional even in malignant LCTs and usually is not associated with peripheral effects [117]. Conversely, Sertoli cell tumors (SCTs) usually do not show any endocrine activity. In some cases, SCTs are a part of multiple neoplasia syndromes, such as Carney Complex and Peutz-Jegers [118,119]. Serum tumor markers are always negative in case of stromal cell tumors and no specifical blood test marker exists for these tumors.
Unlike the TGCTs, the great majority of stromal cell tumors are benign, so that testis-sparing surgery is now the standard of care in these tumors [120,121]. In selected patients, a strict radiological surveillance can also be performed [120].
6.3.1. Leydig cell tumor (LCT)
Prevalence: LCTs account for about 5% of all testicular tumors.
Clinical history and physical examination: See above (paragraph 6.3). Of note, malignancy is reported for 10-15% of LCTs [97]. Histological features of malignancy are cytologic atypia, necrosis, angiolymphatic invasion, increased mitotic activity, atypical mitotic figures, infiltrative margins, extension beyond testicular parenchyma, and DNA aneuploidy [97].
GSUS + CDUS: LCTs commonly appear at GSUS as round lesions with homogeneous hypoechoic echotexture and regular well demarcated margins [43,122]. A hyperechoic halo surrounding the lesion can sometimes be found [123] (Figure 13, Panel A). Dimensions are usually small, due to a slow cells’ growth, and they usually present as single lesions. LCTs are usually unilateral even if, in rare cases, they can involve both testicles [124]. CDUS can show peripheral and, sometimes, intralesional, blood flow [43,122] (Figure 13, Panel B).
SE: LCTs usually appear as hard lesions at SE showing low/absent elastic strain [8,98,99] (Figure 13, Panel C).
CEUS: CEUS could be useful for differential diagnosis of LCTs with small seminomas (see below). After CEUS administration, LCT shows a homogeneous and intense hyperenhancement of the whole lesion [125]. A rapid wash-in and a slow wash-out are distinctive characteristics of LCTs [4,43,106] (Figure 13, Panel D). Leydig cells indeed strongly express an angiogenic mitogen, the endocrine gland–derived vascular endothelial growth factor (EG-VEGF) [126]. EG-VEGF may play a role in angiogenesis in LCTs growth and therefore in an intense vascularization [125].
Differential diagnosis: Distinguishing LCT from small seminomas may sometimes not be straightforward. Nevertheless, differential diagnosis is imperative as the two tumors have a very different clinical course and therefore therapeutic direction [11]. The clinical context is not useful, as age of onset is similar, patients could be asymptomatic in both cases and infertility could be a risk factor for both tumors. In case of small lesions, they could be undetectable with clinical examination in both cases but, if palpable, both may have a firm consistency. Serum tumor markers can be negative in both cases. Microlithiasis of the surrounding parenchyma are more frequently identified in seminomas. At GS, both seminomas and LCTs appear as hypoechoic and homogeneous lesions, margins could be well-demarcated in both lesions and CDUS usually show internal vascularization in both lesions, even if it can appear more often intralesional and arborized in seminomas and peripheral in LCTs. SE is similar in LCTs and seminomas as it shows hard lesions with low/absent elastic strain. Hence, CEUS can represent the decisive tool in the differential diagnosis between LCTs and seminomas since the contrast medium diffuses differently in the two lesions. Both seminomas and LCTs are homogeneously hyper-enhanced compared to the surrounding parenchyma [20,43,125,127,128,129], with a rapid wash-in [43], while wash-out seems to be different, being slower in LCTs and faster in seminomas [4,43,106]. In addition, according to some reports, LCTs show a greater peak enhancement than seminomas in the wash-in phase [17,105]. This data may depend on the vascular architecture of LCTs, characterized by high density of regular microvessels [106]. However, the literature does not fully agree on the results of the CEUS kinetics. This depends on very heterogeneous studies, which include different types of lesions and with small sample sizes [130].
Regarding the differential diagnosis between benign and malignant LCTs, no radiological feature can distinguish the nature of the lesion. Hence, although a strict radiological surveillance can be performed if a LCT is suspected [100], testis-sparing surgery represents the standard of care in these tumors [120,121], and orchiectomy can be performed in case of a malignancy at histology.
6.3.2. Sertoli cell tumor (SCT)
Prevalence: Sertoli cell tumors (SCTs) account for <1% of all testicular tumors, and can be found in men with a wide age range (18 to 80 years), although they are more frequent in young-adults [131]. Rarely, SCTs are also reported in pediatric patients [132].
Clinical history and physical examination: See above (paragraph 6.3). Of note, malignancy is reported for 5% of SCTs [99].
GSUS + CDUS: SCTs can appear at GSUS both as hypoechoic and hyperechoic lesions, with possible intralesional calcifications (Figure 14, Panel A). Margins are well demarcated. In some cases, there are large areas of calcification and inhomogeneous echotexture, identifying the so-called “calcifying Sertoli cell tumor”: this specific subtype is usually associated with Carney complex or Peutz-Jegers syndrome [118,119]. CDUS shows a marked internal vascularization of these lesions (Figure 14, Panel B)
SE: SCTs usually appear as hard lesions showing low/absent elastic strain (Figure 14, Panel C)
CEUS: SCTs shows an homogeneous and intense hyperenhancement of the whole lesion with rapid wash-in and a wash-out similar to the parenchyma [43,106] (Figure 14, Panel D).
Differential diagnosis: differential diagnosis includes LCTs and small seminomas and is sometimes difficult. The kinetic characteristics at CEUS can resemble both LCTs and seminomas, but relative literature is very scarce, being this histotype rare.
6.4. Non-primary malignant tumors
Among neoplasms not deriving from testicular parenchyma, primary hematologic malignancies of the testes are the most frequent, namely non-Hodgkin lymphoma or primary testicular leukemia. In very rare cases the testicle can also be the site of metastases [17].
6.4.1. Lymphoma
Prevalence: Testicular lymphomas represent the 1-9% of all testicular tumors and are frequently B-cell type [133]. They usually affect men older than 50 years.
Clinical history and physical examination: Testicular lymphomas can appear as a primary or secondary localization of the disease, and they can be unilateral or bilateral. Patients are usually asymptomatic or paucisymptomatic. Symptoms include, as for other testicular tumors, firm testicular masses, testicular swelling, or testicular heaviness. Specific lymphoma symptoms could be present: fever, weight loss, sweating at night, itching.
GSUS + CDUS: At GSUS, lymphomas usually appear as hypoechoic lesions with infiltrating margins (Figure 15, Panel A). The vascular pattern is clearly visible within the lesion and consists of well-organized vessels arranged with a linear, non-branching pattern [17] (Figure 15, Panel B).
SE: SE reveals hard lesions showing low/absent elastic strain [17] (Figure 15, Panel C).
CEUS: Usually CEUS shows hyperenhancement of the lesions, with rapid wash-in and wash-out [17], but qualitative and quantitative assessment do not add significant information to conventional CDUS (Figure 15, Panel D).
Differential diagnosis: The US differential diagnosis is usually with other testicular tumors that appear hypoechoic at GS (e.g., seminoma). The US hallmark of lymphomas are infiltrating margins and the vascular pattern, which beside the detection in men aged > 50 years old can help in suggesting the diagnosis.
6.4.2. Primary testicular leukemia
Prevalence: Primary testicular leukemia is a rare presentation of leukemia, more frequent in children and young patients. Testicular involvement is found in 1% to 2.4% of boys with acute lymphoblastic leukemia but is very rare in adult patients [134,135].
Clinical history and physical examination: Testicular localization may be simultaneous to the diagnosis of the primary disease or can occur after treatment/remission of the primary disease. Patients are usually asymptomatic. Physical examination can reveal testicular involvement by increased size, irregular swelling, and firm consistency of the testes [136].
GSUS + CDUS: GSUS appearance can include two patterns. On one hand, an infiltrating pattern with irregular hypoechoic longitudinal striae radiating peripherally from the mediastinum to the entire testicle with CDUS showing increased vascularity of non-branching linear patterns has been described. On the other hand, a focal pattern with irregular hypoechoic nodules with smooth irregular margins with increased vascularity on CDUS can be found [17,105,137,138,139] (Figure 16, Panel A). The hypoechogenicity at US reflects the infiltration and aggregation of abnormal lymphoid lesions because the density of tumor cells and vessels is greater than that of normal testicular tissue [17,105,137] (Figure 16, Panel B).
CEUS: Regarding CEUS, lesions appear hyper-enhanced due to their high vascularity [17] (Figure 16, Panel D).
Differential diagnosis: primary testicular leukemia can mimic an inflammatory process of the testis such as orchitis However, the lack of pain and normal appearance of the epididymis can guide the diagnosis [140].
6.4.3. Plasmacytoma
Prevalence: Patients with multiple myeloma can rarely present with an intratesticular plasmacytoma. So far, less than a hundred cases are reported in the literature [141].
Clinical history and physical examination: In patients with a known diagnosis of multiple myeloma, intratesticular plasmacytoma should always be suspected. Diagnosis is usually due to a rapid testicular enlargement. The lesion can be hard and elastic at physical examination [142].
GSUS + CDUS: Plasmacytoma usually involves the whole testicle, which is enlarged and hypoechoic at GSUS (Figure 17, Panel A) with markedly increased vascularization at CDUS (Figure 17, Panel B).
SE: SE reveals a hard lesion showing low/absent elastic strain (Figure 17, Panel C).
CEUS: Regarding CEUS, lesions appear hyper-enhanced due to their high vascularity [17].
Differential diagnosis: Differential diagnosis with orchitis may be difficult, even if the lack of pain and normal appearance of the epididymis can help [143].
6.4.4. Metastases
The testicle is a rare site for metastatic localization of other tumors. Some literature reports include prostate [144], lung [145], gastrointestinal tumors [146,147], melanoma [148], pancreas [149], kidneys [150], bladder [151], thyroid [152] and neuroblastoma [153].
Clinical history and physical examination: In patients with a known diagnosis of extratesticular tumor and detection at palpation of a hard testicular nodule/mass, metastases should always be suspected.
GSUS + CDUS: At GSUS, metastases show variable patterns according to the site of the primary tumor. Usually, they present as irregular hypoechoic inhomogeneous lesions vascularized at CDUS [3].
SE: SE reveals a hard lesion showing low/absent elastic strain.
CEUS: Regarding CEUS, lesions appear hyper-enhanced due to their high vascularity
Differential diagnosis: US appearance is not specific; however, metastases are generally found in the setting of widespread disease and are rarely the first reason for presentation [3].
6.5. Burned out tumor
Prevalence: The ‘burned-out’ testicular tumors are rare clinical entities which describe a spontaneously and completely regressed testicular tumor, which presents at the stage of metastases, in most cases in retroperitoneal lymph nodes, in the absence of clinical or US detection of a testicular nodule [154]. The cause of testicular mass regression is still unknown. Hypotheses of ischemia of the lesion or destruction by the immune system have been advocated [155]. Due to the rarity of burned-out tumors, no specific guidelines exist for diagnosis, clinical and therapeutic management.
Clinical history and physical examination: Symptoms are often non-specific and include nausea, vomiting and lower back pain, due to retroperitoneal lymph-node enlargement, the most common site of metastasis. Retroperitoneal, supraclavicular, cervical, and axillary lymph nodes and, less often, lung and liver localization of metastases can be the first appearance of a ‘burned-out’ testicular tumor. A few patients complain of testicular symptoms [155]. Both seminomas and non-seminomas can have “burned-out” presentations. Commonly, serum tumor markers are very high [155].
GSUS + CDUS: No primary testicular lesion is identified, and the tumor is supposed to be reduced to a fibrotic scar, represented by a linear macrocalcification (> 0.2-0.3 cm) with a rear shadow cone [156,157]. Histologically, it corresponds to psammoma bodies (smooth laminated intratubular calcifications) and haematoxyphilic bodies (non-laminated intratubular calcifications) [158,159,160,161]. Occasionally, signs of burned-out tumors are represented by hypoechoic irregular areas within the testicle with scarce vascularization [158,159,160,161]. Testicular atrophy and microlithiasis have also been reported in relation to burned-out tumors [158,159,160].
SE: In the parenchyma surrounding the scar/calcification a focal area of increased stiffness can be observed at SE.
CEUS: The fibrotic scar and surrounding areas generally do not enhance with CEUS [128].
Differential diagnosis: A burned out tumor can be confused with a simple fibrotic scar or a linear macro-calcification. When the imaging is uncertain, serum tumor markers, which show high levels in burned out tumors, must be performed to exclude distant spread of the disease.
7. Conclusions
Mp-US is a valuable diagnostic paradigm combining information derived from different US techniques (GSUS, CDUS, CEUS, and SE), which, along with clinical history and physical examination, can help in the differential diagnosis of testicular lesions. Mp-US can provide a more detailed characterization of testicular lesions than the single US techniques alone. Although GS and CDUS are often sufficient to suggest the benign or malignant nature of testicular lesions, CEUS can be decisive in the differential diagnosis of unclear findings, and SE can help to strengthen the diagnosis. The knowledge of mp-US patterns of testicular lesions, summarized in this review, is useful to the physician in daily clinical practice to discriminate benign and malignant lesions, improving the management of critical patients suggesting testicular salvage and US follow-up or orchiectomy.
Author Contributions
C.P. and F.L. conceived the study. All authors performed the literature search and collated the data. C.P., M.T. F.S and F.L. wrote the manuscript with input from all the authors. P.S.S., D.Y.H., M.B., M.M and A.M.I. provided critical feedback and helped shape the manuscript. C.P., A.M.I. and P.S.S. provided the multiparametric ultrasound pictures. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lotti, F.; Maggi, M. Ultrasound of the Male Genital Tract in Relation to Male Reproductive Health. Hum. Reprod. Update 2015, 21, 56–83. [Google Scholar] [CrossRef]
- Lotti, F.; Bertolotto, M.; Maggi, M. Historical Trends for the Standards in Scrotal Ultrasonography: What Was, What Is and What Will Be Normal. Andrology 2021, 9, 1331–1355. [Google Scholar] [CrossRef]
- Isidori, A.M.; Lenzi, A. Ultrasound of the Testis for the Andrologist: Morphological and Functional Atlas; Springer, 2018; ISBN 9783319518268.
- Huang, D.Y.; Sidhu, P.S. Focal Testicular Lesions: Colour Doppler Ultrasound, Contrast-Enhanced Ultrasound and Tissue Elastography as Adjuvants to the Diagnosis. Br. J. Radiol. 2012, 85 Spec No 1, S41–S53. [Google Scholar] [CrossRef]
- Sidhu, P.S. Multiparametric Ultrasound (MPUS) Imaging: Terminology Describing the Many Aspects of Ultrasonography. Ultraschall Med. 2015, 36, 315–317. [Google Scholar] [CrossRef]
- Shah, A.; Lung, P.F.; Clarke, J.L.; Sellars, M.E.; Sidhu, P.S. Re: New Ultrasound Techniques for Imaging of the Indeterminate Testicular Lesion May Avoid Surgery Completely. Clin. Radiol. 2010, 65, 496–497. [Google Scholar] [CrossRef]
- Tenuta, M.; Sesti, F.; Bonaventura, I.; Mazzotta, P.; Pofi, R.; Gianfrilli, D.; Pozza, C. Use of Contrast Enhanced Ultrasound in Testicular Diseases: A Comprehensive Review. Andrology 2021, 9, 1369–1382. [Google Scholar] [CrossRef]
- Pozza, C.; Gianfrilli, D.; Fattorini, G.; Giannetta, E.; Barbagallo, F.; Nicolai, E.; Cristini, C.; Di Pierro, G.B.; Franco, G.; Lenzi, A.; et al. Diagnostic Value of Qualitative and Strain Ratio Elastography in the Differential Diagnosis of Non-Palpable Testicular Lesions. Andrology 2016, 4, 1193–1203. [Google Scholar] [CrossRef]
- Cantisani, V.; Di Leo, N.; Bertolotto, M.; Fresilli, D.; Granata, A.; Polti, G.; Polito, E.; Pacini, P.; Guiban, O.; Del Gaudio, G.; et al. Role of Multiparametric Ultrasound in Testicular Focal Lesions and Diffuse Pathology Evaluation, with Particular Regard to Elastography: Review of Literature. Andrology 2021, 9, 1356–1368. [Google Scholar] [CrossRef] [PubMed]
- Dieckmann, K.-P.; Frey, U.; Lock, G. Contemporary Diagnostic Work-up of Testicular Germ Cell Tumours. Nat. Rev. Urol. 2013, 10, 703–712. [Google Scholar] [CrossRef] [PubMed]
- Marko, J.; Wolfman, D.J.; Aubin, A.L.; Sesterhenn, I.A. Testicular Seminoma and Its Mimics: From the Radiologic Pathology Archives. Radiographics 2017, 37, 1085–1098. [Google Scholar] [CrossRef] [PubMed]
- Song, G.; Xiong, G.-Y.; Fan, Y.; Huang, C.; Kang, Y.-M.; Ji, G.-J.; Chen, J.-C.; Xin, Z.-C.; Zhou, L.-Q. The Role of Tumor Size, Ultrasonographic Findings, and Serum Tumor Markers in Predicting the Likelihood of Malignant Testicular Histology. Asian J. Androl. 2019, 21, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Patrikidou, A.; Cazzaniga, W.; Berney, D.; Boormans, J.; de Angst, I.; Di Nardo, D.; Fankhauser, C.; Fischer, S.; Gravina, C.; Gremmels, H.; et al. European Association of Urology Guidelines on Testicular Cancer: 2023 Update. Eur. Urol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Carmignani, L.; Gadda, F.; Gazzano, G.; Nerva, F.; Mancini, M.; Ferruti, M.; Bulfamante, G.; Bosari, S.; Coggi, G.; Rocco, F.; et al. High Incidence of Benign Testicular Neoplasms Diagnosed by Ultrasound. J. Urol. 2003, 170, 1783–1786. [Google Scholar] [CrossRef] [PubMed]
- Rocher, L.; Ramchandani, P.; Belfield, J.; Bertolotto, M.; Derchi, L.E.; Correas, J.M.; Oyen, R.; Tsili, A.C.; Turgut, A.T.; Dogra, V.; et al. Incidentally Detected Non-Palpable Testicular Tumours in Adults at Scrotal Ultrasound: Impact of Radiological Findings on Management Radiologic Review and Recommendations of the ESUR Scrotal Imaging Subcommittee. Eur. Radiol. 2016, 26, 2268–2278. [Google Scholar] [CrossRef]
- Schröder, C.; Lock, G.; Schmidt, C.; Löning, T.; Dieckmann, K.-P. Real-Time Elastography and Contrast-Enhanced Ultrasonography in the Evaluation of Testicular Masses: A Comparative Prospective Study. Ultrasound Med. Biol. 2016, 42, 1807–1815. [Google Scholar] [CrossRef]
- Kachramanoglou, C.; Rafailidis, V.; Philippidou, M.; Bertolotto, M.; Huang, D.Y.; Deganello, A.; Sellars, M.E.; Sidhu, P.S. Multiparametric Sonography of Hematologic Malignancies of the Testis: Grayscale, Color Doppler, and Contrast-Enhanced Ultrasound and Strain Elastographic Appearances With Histologic Correlation. J. Ultrasound Med. 2017, 36, 409–420. [Google Scholar] [CrossRef]
- Lock, G.; Schröder, C.; Schmidt, C.; Anheuser, P.; Loening, T.; Dieckmann, K.P. Contrast-Enhanced Ultrasound and Real-Time Elastography for the Diagnosis of Benign Leydig Cell Tumors of the Testis - a Single Center Report on 13 Cases. Ultraschall Med. 2014, 35, 534–539. [Google Scholar] [CrossRef]
- Liu, H.; Dong, L.; Xiang, L.-H.; Xu, G.; Wan, J.; Fang, Y.; Ding, S.-S.; Jin, Y.; Sun, L.-P.; Xu, H.-X. Multiparametric Ultrasound for the Assessment of Testicular Lesions with Negative Tumoral Markers. Asian J. Androl. 2023, 25, 50–57. [Google Scholar] [CrossRef]
- Auer, T.; De Zordo, T.; Dejaco, C.; Gruber, L.; Pichler, R.; Jaschke, W.; Dogra, V.S.; Aigner, F. Value of Multiparametric US in the Assessment of Intratesticular Lesions. Radiology 2017, 285, 640–649. [Google Scholar] [CrossRef]
- Bernardo, S.; Konstantatou, E.; Huang, D.Y.; Deganello, A.; Philippidou, M.; Brown, C.; Sellars, M.E.; Sidhu, P.S. Multiparametric Sonographic Imaging of a Capillary Hemangioma of the Testis: Appearances on Gray-Scale, Color Doppler, Contrast-Enhanced Ultrasound and Strain Elastography. J. Ultrasound 2016, 19, 35–39. [Google Scholar] [CrossRef]
- Bertolotto, M.; Muça, M.; Currò, F.; Bucci, S.; Rocher, L.; Cova, M.A. Multiparametric US for Scrotal Diseases. Abdom Radiol (NY) 2018, 43, 899–917. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.Y.; Pesapane, F.; Rafailidis, V.; Deganello, A.; Sellars, M.E.; Sidhu, P.S. The Role of Multiparametric Ultrasound in the Diagnosis of Paediatric Scrotal Pathology. Br. J. Radiol. 2020, 93, 20200063. [Google Scholar] [CrossRef]
- Lotti, F.; Frizza, F.; Balercia, G.; Barbonetti, A.; Behre, H.M.; Calogero, A.E.; Cremers, J.-F.; Francavilla, F.; Isidori, A.M.; Kliesch, S.; et al. The European Academy of Andrology (EAA) Ultrasound Study on Healthy, Fertile Men: An Overview on Male Genital Tract Ultrasound Reference Ranges. Andrology 2022, 10 Suppl 2, 118–132. [Google Scholar] [CrossRef]
- Martino, P.; Galosi, A.B.; Bitelli, M.; Consonni, P.; Fiorini, F.; Granata, A.; Gunelli, R.; Liguori, G.; Palazzo, S.; Pavan, N.; et al. Practical Recommendations for Performing Ultrasound Scanning in the Urological and Andrological Fields. Arch. Ital. Urol. Androl. 2014, 86, 56–78. [Google Scholar] [CrossRef] [PubMed]
- Guideline developed in collaboration with the American College of Radiology; Society for Pediatric Radiology; Society of Radiologists in Ultrasound AIUM Practice Guideline for the Performance of Scrotal Ultrasound Examinations. J. Ultrasound Med. 2015, 34, 1–5. [CrossRef]
- Lotti, F.; Frizza, F.; Balercia, G.; Barbonetti, A.; Behre, H.M.; Calogero, A.E.; Cremers, J.-F.; Francavilla, F.; Isidori, A.M.; Kliesch, S.; et al. The European Academy of Andrology (EAA) Ultrasound Study on Healthy, Fertile Men: Prostate-Vesicular Transrectal Ultrasound Reference Ranges and Associations with Clinical, Seminal and Biochemical Characteristics. Andrology 2022, 10, 1150–1171. [Google Scholar] [CrossRef]
- Lotti, F.; Frizza, F.; Balercia, G.; Barbonetti, A.; Behre, H.M.; Calogero, A.E.; Cremers, J.F.; Francavilla, F.; Isidori, A.M.; Kliesch, S.; et al. The European Academy of Andrology (EAA) Ultrasound Study on Healthy, Fertile Men: Scrotal Ultrasound Reference Ranges and Associations with Clinical, Seminal, and Biochemical Characteristics. Andrology 2021, 9, 559–576. [Google Scholar] [CrossRef]
- Lotti, F.; Frizza, F.; Balercia, G.; Barbonetti, A.; Behre, H.M.; Calogero, A.E.; Cremers, J.-F.; Francavilla, F.; Isidori, A.M.; Kliesch, S.; et al. The European Academy of Andrology (EAA) Ultrasound Study on Healthy, Fertile Men: Clinical, Seminal and Biochemical Characteristics. Andrology 2020, 8, 1005–1020. [Google Scholar] [CrossRef]
- Sidhu, P.S.; Cantisani, V.; Dietrich, C.F.; Gilja, O.H.; Saftoiu, A.; Bartels, E.; Bertolotto, M.; Calliada, F.; Clevert, D.-A.; Cosgrove, D.; et al. The EFSUMB Guidelines and Recommendations for the Clinical Practice of Contrast-Enhanced Ultrasound (CEUS) in Non-Hepatic Applications: Update 2017 (Long Version). Ultraschall Med. 2018, 39, e2–e44. [Google Scholar] [CrossRef]
- Săftoiu, A.; Gilja, O.H.; Sidhu, P.S.; Dietrich, C.F.; Cantisani, V.; Amy, D.; Bachmann-Nielsen, M.; Bob, F.; Bojunga, J.; Brock, M.; et al. The EFSUMB Guidelines and Recommendations for the Clinical Practice of Elastography in Non-Hepatic Applications: Update 2018. Ultraschall Med. 2019, 40, 425–453. [Google Scholar] [CrossRef]
- Bamber, J.; Cosgrove, D.; Dietrich, C.F.; Fromageau, J.; Bojunga, J.; Calliada, F.; Cantisani, V.; Correas, J.-M.; D’Onofrio, M.; Drakonaki, E.E.; et al. EFSUMB Guidelines and Recommendations on the Clinical Use of Ultrasound Elastography. Part 1: Basic Principles and Technology. Ultraschall Med. 2013, 34, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Correas, J.M.; Drakonakis, E.; Isidori, A.M.; Hélénon, O.; Pozza, C.; Cantisani, V.; Di Leo, N.; Maghella, F.; Rubini, A.; Drudi, F.M.; et al. Update on Ultrasound Elastography: Miscellanea. Prostate, Testicle, Musculo-Skeletal. Eur. J. Radiol. 2013, 82, 1904–1912. [Google Scholar] [CrossRef] [PubMed]
- Hoag, N.A.; Afshar, K.; Youssef, D.; Masterson, J.S.T.; Murphy, J.; Macneily, A.E. Cystic Intratesticular Lesions in Pediatric Patients. J. Pediatr. Surg. 2013, 48, 1773–1777. [Google Scholar] [CrossRef] [PubMed]
- Gooding, G.A.; Leonhardt, W.; Stein, R. Testicular Cysts: US Findings. Radiology 1987, 163, 537–538. [Google Scholar] [CrossRef] [PubMed]
- Hamm, B.; Fobbe, F.; Loy, V. Testicular Cysts: Differentiation with US and Clinical Findings. Radiology 1988, 168, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Dogra, V.S.; Gottlieb, R.H.; Rubens, D.J.; Liao, L. Benign Intratesticular Cystic Lesions: US Features. Radiographics 2001, 21 Spec No, S273–S281. [Google Scholar] [CrossRef]
- Shah, K.H.; Maxted, W.C.; Chun, B. Epidermoid Cysts of the Testis: A Report of Three Cases and an Analysis of 141 Cases from the World Literature. Cancer 1981, 47, 577–582. [Google Scholar] [CrossRef]
- Dogra, V.S.; Gottlieb, R.H.; Oka, M.; Rubens, D.J. Sonography of the Scrotum. Radiology 2003, 227, 18–36. [Google Scholar] [CrossRef]
- Anheuser, P.; Kranz, J.; Stolle, E.; Höflmayer, D.; Büscheck, F.; Mühlstädt, S.; Lock, G.; Dieckmann, K.P. Testicular Epidermoid Cysts: A Reevaluation. BMC Urol. 2019, 19, 52. [Google Scholar] [CrossRef]
- Patel, K.; Sellars, M.E.; Clarke, J.L.; Sidhu, P.S. Features of Testicular Epidermoid Cysts on Contrast-Enhanced Sonography and Real-Time Tissue Elastography. J. Ultrasound Med. 2012, 31, 115–122. [Google Scholar] [CrossRef]
- Manning, M.A.; Woodward, P.J. Testicular Epidermoid Cysts: Sonographic Features with Clinicopathologic Correlation. J. Ultrasound Med. 2010, 29, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Isidori, A.M.; Pozza, C.; Gianfrilli, D.; Giannetta, E.; Lemma, A.; Pofi, R.; Barbagallo, F.; Manganaro, L.; Martino, G.; Lombardo, F.; et al. Differential Diagnosis of Nonpalpable Testicular Lesions: Qualitative and Quantitative Contrast-Enhanced US of Benign and Malignant Testicular Tumors. Radiology 2014, 273, 606–618. [Google Scholar] [CrossRef] [PubMed]
- Engels, M.; Span, P.N.; van Herwaarden, A.E.; Sweep, F.C.G.J.; Stikkelbroeck, N.M.M.L.; Claahsen-van der Grinten, H.L. Testicular Adrenal Rest Tumors: Current Insights on Prevalence, Characteristics, Origin, and Treatment. Endocr. Rev. 2019, 40, 973–987. [Google Scholar] [CrossRef]
- Jedrzejewski, G.; Ben-Skowronek, I.; Wozniak, M.M.; Brodzisz, A.; Budzynska, E.; Wieczorek, A.P. Testicular Adrenal Rest Tumors in Boys with Congenital Adrenal Hyperplasia: 3D US and Elastography--Do We Get More Information for Diagnosis and Monitoring? J. Pediatr. Urol. 2013, 9, 1032–1037. [Google Scholar] [CrossRef]
- Corcioni, B.; Renzulli, M.; Marasco, G.; Baronio, F.; Gambineri, A.; Ricciardi, D.; Ortolano, R.; Farina, D.; Gaudiano, C.; Cassio, A.; et al. Prevalence and Ultrasound Patterns of Testicular Adrenal Rest Tumors in Adults with Congenital Adrenal Hyperplasia. Transl. Androl. Urol. 2021, 10, 562–573. [Google Scholar] [CrossRef] [PubMed]
- Mansoor, N.M.; Huang, D.Y.; Sidhu, P.S. Multiparametric Ultrasound Imaging Characteristics of Multiple Testicular Adrenal Rest Tumours in Congenital Adrenal Hyperplasia. Ultrasound 2022, 30, 80–84. [Google Scholar] [CrossRef]
- Tresoldi, A.S.; Betella, N.; Hasenmajer, V.; Pozza, C.; Vena, W.; Fiamengo, B.; Negri, L.; Cappa, M.; Lania, A.G.A.; Lenzi, A.; et al. Bilateral Testicular Masses and Adrenal Insufficiency: Is Congenital Adrenal Hyperplasia the Only Possible Diagnosis? First Two Cases of TARTS Described in Addison-Only X-Linked Adrenoleukodystrophy and a Brief Review of Literature. J. Endocrinol. Invest. 2021, 44, 391–402. [Google Scholar] [CrossRef]
- Ricker, W.; Clark, M. Sarcoidosis; a Clinicopathologic Review of 300 Cases, Including 22 Autopsies. Am. J. Clin. Pathol. 1949, 19, 725–749. [Google Scholar] [CrossRef]
- Bhatt, S.; Jafri, S.Z.H.; Wasserman, N.; Dogra, V.S. Imaging of Non-Neoplastic Intratesticular Masses. Diagn. Interv. Radiol. 2011, 17, 52–63. [Google Scholar] [CrossRef]
- Stewart, V.R.; Sidhu, P.S. The Testis: The Unusual, the Rare and the Bizarre. Clin. Radiol. 2007, 62, 289–302. [Google Scholar] [CrossRef]
- Rafailidis, V.; Robbie, H.; Konstantatou, E.; Huang, D.Y.; Deganello, A.; Sellars, M.E.; Cantisani, V.; Isidori, A.M.; Sidhu, P.S. Sonographic Imaging of Extra-Testicular Focal Lesions: Comparison of Grey-Scale, Colour Doppler and Contrast-Enhanced Ultrasound. Ultrasound 2016, 24, 23–33. [Google Scholar] [CrossRef]
- Lung, P.F.C.; Fang, C.; Jaffer, O.S.; Deganello, A.; Shah, A.; Hedayati, V.; Obaro, A.; Yusuf, G.T.; Huang, D.Y.; Sellars, M.E.; et al. Vascularity of Intra-Testicular Lesions: Inter-Observer Variation in the Assessment of Non-Neoplastic Versus Neoplastic Abnormalities After Vascular Enhancement With Contrast-Enhanced Ultrasound. Ultrasound Med. Biol. 2020, 46, 2956–2964. [Google Scholar] [CrossRef]
- De Cinque, A.; Corcioni, B.; Rossi, M.S.; Franceschelli, A.; Colombo, F.; Golfieri, R.; Renzulli, M.; Gaudiano, C. Case Report: Testicular Sarcoidosis: The Diagnostic Role of Contrast-Enhanced Ultrasound and Review of the Literature. Front. Med. 2020, 7, 610384. [Google Scholar] [CrossRef] [PubMed]
- Gianfrilli, D.; Isidori, A.M.; Lenzi, A. Segmental Testicular Ischaemia: Presentation, Management and Follow-Up. Int. J. Androl. 2009, 32, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.V.; Huang, D.Y.; Sidhu, P.S. Metachronous Bilateral Segmental Testicular Infarction: Multi-Parametric Ultrasound Imaging with Grey-Scale Ultrasound, Doppler Ultrasound, Contrast-Enhanced Ultrasound (CEUS) and Real-Time Tissue Elastography (RTE). J. Ultrasound 2014, 17, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Bilagi, P.; Sriprasad, S.; Clarke, J.L.; Sellars, M.E.; Muir, G.H.; Sidhu, P.S. Clinical and Ultrasound Features of Segmental Testicular Infarction: Six-Year Experience from a Single Centre. Eur. Radiol. 2007, 17, 2810–2818. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Pérez, G.C.; Tardáguila, F.M.; Velasco, M.; Rivas, C.; Dos Santos, J.; Cambronero, J.; Trinidad, C.; San Miguel, P. Radiologic Findings of Segmental Testicular Infarction. AJR Am. J. Roentgenol. 2005, 184, 1587–1593. [Google Scholar] [CrossRef] [PubMed]
- Sweet, D.E.; Feldman, M.K.; Remer, E.M. Imaging of the Acute Scrotum: Keys to a Rapid Diagnosis of Acute Scrotal Disorders. Abdom Radiol (NY) 2020, 45, 2063–2081. [Google Scholar] [CrossRef] [PubMed]
- Bertolotto, M.; Derchi, L.E.; Sidhu, P.S.; Serafini, G.; Valentino, M.; Grenier, N.; Cova, M.A. Acute Segmental Testicular Infarction at Contrast-Enhanced Ultrasound: Early Features and Changes during Follow-Up. AJR Am. J. Roentgenol. 2011, 196, 834–841. [Google Scholar] [CrossRef]
- Yusuf, G.T.; Sidhu, P.S. A Review of Ultrasound Imaging in Scrotal Emergencies. J. Ultrasound 2013, 16, 171–178. [Google Scholar] [CrossRef]
- Pavlica, P.; Barozzi, L. Imaging of the Acute Scrotum. Eur. Radiol. 2001, 11, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Valentino, M.; Bertolotto, M.; Derchi, L.; Bertaccini, A.; Pavlica, P.; Martorana, G.; Barozzi, L. Role of Contrast Enhanced Ultrasound in Acute Scrotal Diseases. Eur. Radiol. 2011, 21, 1831–1840. [Google Scholar] [CrossRef] [PubMed]
- Lung, P.F.C.; Jaffer, O.S.; Sellars, M.E.; Sriprasad, S.; Kooiman, G.G.; Sidhu, P.S. Contrast-Enhanced Ultrasound in the Evaluation of Focal Testicular Complications Secondary to Epididymitis. AJR Am. J. Roentgenol. 2012, 199, W345–W354. [Google Scholar] [CrossRef] [PubMed]
- Purushothaman, H.; Sellars, M.E.K.; Clarke, J.L.; Sidhu, P.S. Intratesticular Haematoma: Differentiation from Tumour on Clinical History and Ultrasound Appearances in Two Cases. Br. J. Radiol. 2007, 80, e184–e187. [Google Scholar] [CrossRef]
- Ramanathan, S.; Bertolotto, M.; Freeman, S.; Belfield, J.; Derchi, L.E.; Huang, D.Y.; Lotti, F.; Markiet, K.; Nikolic, O.; Ramchandani, P.; et al. Imaging in Scrotal Trauma: A European Society of Urogenital Radiology Scrotal and Penile Imaging Working Group (ESUR-SPIWG) Position Statement. Eur. Radiol. 2021, 31, 4918–4928. [Google Scholar] [CrossRef]
- Yusuf, G.; Konstantatou, E.; Sellars, M.E.; Huang, D.Y.; Sidhu, P.S. Multiparametric Sonography of Testicular Hematomas: Features on Grayscale, Color Doppler, and Contrast-Enhanced Sonography and Strain Elastography. J. Ultrasound Med. 2015, 34, 1319–1328. [Google Scholar] [CrossRef]
- Öztürk, Ç.; Paşaoğlu, E.; Bölme Şavlı, T. A Lesion Mimicking Malignancy: Granulomatous Orchitis. Üroonkoloji bül. 2021, 20, 126–128. [Google Scholar] [CrossRef]
- Civelli, V.F.; Heidari, A.; Valdez, M.C.; Narang, V.K.; Johnson, R.H. A Case of Testicular Granulomatous Inflammation Mistaken for Malignancy: Tuberculosis Identified Post Orchiectomy. J Investig Med High Impact Case Rep 2020, 8, 2324709620938947. [Google Scholar] [CrossRef]
- Peyrí Rey, E.; Riverola Manzanilla, A.; Cañas Tello, M.A. [Bilateral idiopathic granulomatous orchitis]. Actas Urol. Esp. 2008, 32, 461–463. [Google Scholar] [CrossRef]
- Wegner, H.E.; Loy, V.; Dieckmann, K.P. Granulomatous Orchitis--an Analysis of Clinical Presentation, Pathological Anatomic Features and Possible Etiologic Factors. Eur. Urol. 1994, 26, 56–60. [Google Scholar] [CrossRef]
- Salmeron, I.; Ramirez-Escobar, M.A.; Puertas, F.; Marcos, R.; Garcia-Marcos, F.; Sanchez, R. Granulomatous Epididymo-Orchitis: Sonographic Features and Clinical Outcome in Brucellosis, Tuberculosis and Idiopathic Granulomatous Epididymo-Orchitis. J. Urol. 1998, 159, 1954–1957. [Google Scholar] [CrossRef] [PubMed]
- Lung, P.F.C.; Sidhu, P.S. Role of Ultrasound in the Diagnosis of Testicular Lesions. Imaging Med. 2011, 3, 587–595. [Google Scholar] [CrossRef]
- Nepal, P.; Ojili, V.; Songmen, S.; Kaur, N.; Olsavsky, T.; Nagar, A. “The Great Masquerader”: Sonographic Pictorial Review of Testicular Tuberculosis and Its Mimics. J. Clin. Imaging Sci. 2019, 9, 27. [Google Scholar] [CrossRef] [PubMed]
- Viswaroop, B.S.; Kekre, N.; Gopalakrishnan, G. Isolated Tuberculous Epididymitis: A Review of Forty Cases. J. Postgrad. Med. 2005, 51, 109–111. [Google Scholar]
- Park, J.S.; Kim, J.; Elghiaty, A.; Ham, W.S. Recent Global Trends in Testicular Cancer Incidence and Mortality. Medicine 2018, 97, e12390. [Google Scholar] [CrossRef]
- Gurney, J.K.; Florio, A.A.; Znaor, A.; Ferlay, J.; Laversanne, M.; Sarfati, D.; Bray, F.; McGlynn, K.A. International Trends in the Incidence of Testicular Cancer: Lessons from 35 Years and 41 Countries. Eur. Urol. 2019, 76, 615–623. [Google Scholar] [CrossRef]
- Znaor, A.; Skakkebaek, N.E.; Rajpert-De Meyts, E.; Kuliš, T.; Laversanne, M.; Gurney, J.; Sarfati, D.; McGlynn, K.A.; Bray, F. Global Patterns in Testicular Cancer Incidence and Mortality in 2020. Int. J. Cancer 2022, 151, 692–698. [Google Scholar] [CrossRef]
- Moch, H.; Amin, M.B.; Berney, D.M.; Compérat, E.M.; Gill, A.J.; Hartmann, A.; Menon, S.; Raspollini, M.R.; Rubin, M.A.; Srigley, J.R.; et al. The 2022 World Health Organization Classification of Tumours of the Urinary System and Male Genital Organs-Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2022, 82, 458–468. [Google Scholar] [CrossRef]
- Honecker, F.; Aparicio, J.; Berney, D.; Beyer, J.; Bokemeyer, C.; Cathomas, R.; Clarke, N.; Cohn-Cedermark, G.; Daugaard, G.; Dieckmann, K.-P.; et al. ESMO Consensus Conference on Testicular Germ Cell Cancer: Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2018, 29, 1658–1686. [Google Scholar] [CrossRef]
- Gilligan, T.D.; Seidenfeld, J.; Basch, E.M.; Einhorn, L.H.; Fancher, T.; Smith, D.C.; Stephenson, A.J.; Vaughn, D.J.; Cosby, R.; Hayes, D.F.; et al. American Society of Clinical Oncology Clinical Practice Guideline on Uses of Serum Tumor Markers in Adult Males with Germ Cell Tumors. J. Clin. Oncol. 2010, 28, 3388–3404. [Google Scholar] [CrossRef]
- Barlow, L.J.; Badalato, G.M.; McKiernan, J.M. Serum Tumor Markers in the Evaluation of Male Germ Cell Tumors. Nat. Rev. Urol. 2010, 7, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Kanakis, G.A.; Nordkap, L.; Bang, A.K.; Calogero, A.E.; Bártfai, G.; Corona, G.; Forti, G.; Toppari, J.; Goulis, D.G.; Jørgensen, N. EAA Clinical Practice Guidelines-Gynecomastia Evaluation and Management. Andrology 2019, 7, 778–793. [Google Scholar] [CrossRef] [PubMed]
- Hassan, H.C.; Cullen, I.M.; Casey, R.G.; Rogers, E. Gynaecomastia: An Endocrine Manifestation of Testicular Cancer. Andrologia 2008, 40, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Rajpert-De Meyts, E.; McGlynn, K.A.; Okamoto, K.; Jewett, M.A.S.; Bokemeyer, C. Testicular Germ Cell Tumours. Lancet 2016, 387, 1762–1774. [Google Scholar] [CrossRef] [PubMed]
- Hanson, H.A.; Anderson, R.E.; Aston, K.I.; Carrell, D.T.; Smith, K.R.; Hotaling, J.M. Subfertility Increases Risk of Testicular Cancer: Evidence from Population-Based Semen Samples. Fertil. Steril. 2016, 105, 322–328. [Google Scholar] [CrossRef]
- Skakkebaek, N.E.; Rajpert-De Meyts, E.; Buck Louis, G.M.; Toppari, J.; Andersson, A.-M.; Eisenberg, M.L.; Jensen, T.K.; Jørgensen, N.; Swan, S.H.; Sapra, K.J.; et al. Male Reproductive Disorders and Fertility Trends: Influences of Environment and Genetic Susceptibility. Physiol. Rev. 2016, 96, 55–97. [Google Scholar] [CrossRef]
- Meyts, E.R.-D. Developmental Model for the Pathogenesis of Testicular Carcinoma in Situ: Genetic and Environmental Aspects; 2006.
- Piltoft, J.S.; Larsen, S.B.; Dalton, S.O.; Johansen, C.; Baker, J.L.; Cederkvist, L.; Andersen, I. Early Life Risk Factors for Testicular Cancer: A Case-Cohort Study Based on the Copenhagen School Health Records Register. Acta Oncol. 2017, 56, 220–224. [Google Scholar] [CrossRef]
- Pettersson, A.; Richiardi, L.; Nordenskjold, A.; Kaijser, M.; Akre, O. Age at Surgery for Undescended Testis and Risk of Testicular Cancer. N. Engl. J. Med. 2007, 356, 1835–1841. [Google Scholar] [CrossRef]
- Williamson, S.R.; Delahunt, B.; Magi-Galluzzi, C.; Algaba, F.; Egevad, L.; Ulbright, T.M.; Tickoo, S.K.; Srigley, J.R.; Epstein, J.I.; Berney, D.M.; et al. The World Health Organization 2016 Classification of Testicular Germ Cell Tumours: A Review and Update from the International Society of Urological Pathology Testis Consultation Panel. Histopathology 2017, 70, 335–346. [Google Scholar] [CrossRef]
- Kawamoto, A.; Hatano, T.; Saito, K.; Inoue, R.; Nagao, T.; Sanada, S. Sonographic Classification of Testicular Tumors by Tissue Harmonic Imaging: Experience of 58 Cases. J. Med. Ultrason. 2018, 45, 103–111. [Google Scholar] [CrossRef]
- McDonald, M.W.; Reed, A.B.; Tran, P.T.; Evans, L.A. Testicular Tumor Ultrasound Characteristics and Association with Histopathology. Urol. Int. 2012, 89, 196–202. [Google Scholar] [CrossRef]
- Woodward, P.J.; Sohaey, R.; O’Donoghue, M.J.; Green, D.E. From the Archives of the AFIP: Tumors and Tumorlike Lesions of the Testis: Radiologic-Pathologic Correlation. Radiographics 2002, 22, 189–216. [Google Scholar] [CrossRef]
- Necas, M.; Muthupalaniappaan, M.; Barnard, C. Ultrasound Morphological Patterns of Testicular Tumours, Correlation with Histopathology. J Med Radiat Sci 2021, 68, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Barbonetti, A.; Martorella, A.; Minaldi, E.; D’Andrea, S.; Bardhi, D.; Castellini, C.; Francavilla, F.; Francavilla, S. Testicular Cancer in Infertile Men With and Without Testicular Microlithiasis: A Systematic Review and Meta-Analysis of Case-Control Studies. Front. Endocrinol. 2019, 10, 164. [Google Scholar] [CrossRef] [PubMed]
- Richenberg, J.; Belfield, J.; Ramchandani, P.; Rocher, L.; Freeman, S.; Tsili, A.C.; Cuthbert, F.; Studniarek, M.; Bertolotto, M.; Turgut, A.T.; et al. Testicular Microlithiasis Imaging and Follow-up: Guidelines of the ESUR Scrotal Imaging Subcommittee. Eur. Radiol. 2015, 25, 323–330. [Google Scholar] [CrossRef]
- Goddi, A.; Sacchi, A.; Magistretti, G.; Almolla, J.; Salvadore, M. Real-Time Tissue Elastography for Testicular Lesion Assessment. Eur. Radiol. 2012, 22, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Aigner, F.; De Zordo, T.; Pallwein-Prettner, L.; Junker, D.; Schäfer, G.; Pichler, R.; Leonhartsberger, N.; Pinggera, G.; Dogra, V.S.; Frauscher, F. Real-Time Sonoelastography for the Evaluation of Testicular Lesions. Radiology 2012, 263, 584–589. [Google Scholar] [CrossRef]
- Ishida, M.; Hasegawa, M.; Kanao, K.; Oyama, M.; Nakajima, Y. Non-Palpable Testicular Embryonal Carcinoma Diagnosed by Ultrasound: A Case Report. Jpn. J. Clin. Oncol. 2009, 39, 124–126. [Google Scholar] [CrossRef] [PubMed]
- Scandura, G.; Verrill, C.; Protheroe, A.; Joseph, J.; Ansell, W.; Sahdev, A.; Shamash, J.; Berney, D.M. Incidentally Detected Testicular Lesions <10 Mm in Diameter: Can Orchidectomy Be Avoided? BJU Int. 2018, 121, 575–582. [Google Scholar] [CrossRef]
- Stepanas, A.V.; Samaan, N.A.; Schultz, P.N.; Holoye, P.Y. Endocrine Studies in Testicular Tumor Patients with and without Gynecomastia: A Report of 45 Cases. Cancer 1978, 41, 369–376. [Google Scholar] [CrossRef]
- Gerber, D.; Wright, H.C.; Sussman, R.D.; Stamatakis, L. Embryonal Carcinoma Presenting as a Calcified Solitary Testicular Mass on Ultrasound. BMJ Case Rep. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Katabathina, V.S.; Vargas-Zapata, D.; Monge, R.A.; Nazarullah, A.; Ganeshan, D.; Tammisetti, V.; Prasad, S.R. Testicular Germ Cell Tumors: Classification, Pathologic Features, Imaging Findings, and Management. Radiographics 2021, 41, 1698–1716. [Google Scholar] [CrossRef] [PubMed]
- Fang, C.; Huang, D.Y.; Sidhu, P.S. Elastography of Focal Testicular Lesions: Current Concepts and Utility. Ultrasonography 2019, 38, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Xue, N.; Zhang, S.; Wang, G. The Value of Contrast-Enhanced Ultrasonography in the Diagnosis of Primary Testicular Non-Neoplastic and Neoplastic Lesions in Adults. BMC Urol. 2022, 22, 210. [Google Scholar] [CrossRef]
- Anderson, K.H.; Romao, R.L.P. Testicular Tumors in Children and Adolescents: Long-Term Endocrine and Fertility Issues. Transl. Androl. Urol. 2020, 9, 2393–2399. [Google Scholar] [CrossRef]
- Liu, P.; Phillips, M.J.; Edwards, V.D.; Ein, S.; Daneman, A. Sonographic Findings of Testicular Teratoma with Pathologic Correlation. Pediatr. Radiol. 1992, 22, 99–101. [Google Scholar] [CrossRef]
- Epifanio, M.; Baldissera, M.; Esteban, F.G.; Baldisserotto, M. Mature Testicular Teratoma in Children: Multifaceted Tumors on Ultrasound. Urology 2014, 83, 195–197. [Google Scholar] [CrossRef]
- Pagliaro, L.C. Role of High-Dose Chemotherapy With Autologous Stem-Cell Rescue in Men With Previously Treated Germ Cell Tumors. J. Clin. Oncol. 2017, 35, 1036–1040. [Google Scholar] [CrossRef]
- Lagabrielle, S.; Durand, X.; Droupy, S.; Izard, V.; Marcelli, F.; Huyghe, E.; Ferriere, J.-M.; Ferretti, L. Testicular Tumours Discovered during Infertility Workup Are Predominantly Benign and Could Initially Be Managed by Sparing Surgery. J. Surg. Oncol. 2018, 118, 630–635. [Google Scholar] [CrossRef]
- Maxwell, F.; Savignac, A.; Bekdache, O.; Calvez, S.; Lebacle, C.; Arama, E.; Garrouche, N.; Rocher, L. Leydig Cell Tumors of the Testis: An Update of the Imaging Characteristics of a Not So Rare Lesion. Cancers 2022, 14. [Google Scholar] [CrossRef]
- Leonhartsberger, N.; Ramoner, R.; Aigner, F.; Stoehr, B.; Pichler, R.; Zangerl, F.; Fritzer, A.; Steiner, H. Increased Incidence of Leydig Cell Tumours of the Testis in the Era of Improved Imaging Techniques. BJU Int. 2011, 108, 1603–1607. [Google Scholar] [CrossRef] [PubMed]
- Pozza, C.; Pofi, R.; Tenuta, M.; Tarsitano, M.G.; Sbardella, E.; Fattorini, G.; Cantisani, V.; Lenzi, A.; Isidori, A.M.; Gianfrilli, D.; et al. Clinical Presentation, Management and Follow-up of 83 Patients with Leydig Cell Tumors of the Testis: A Prospective Case-Cohort Study. Hum. Reprod. 2019, 34, 1389–1403. [Google Scholar] [CrossRef] [PubMed]
- Holm, M.; Rajpert-De Meyts, E.; Andersson, A.-M.; Skakkebaek, N.E. Leydig Cell Micronodules Are a Common Finding in Testicular Biopsies from Men with Impaired Spermatogenesis and Are Associated with Decreased testosterone/LH Ratio. J. Pathol. 2003, 199, 378–386. [Google Scholar] [CrossRef] [PubMed]
- Rajpert-De Meyts, E.; Aksglaede, L.; Bandak, M.; Toppari, J.; Jørgensen, N. Testicular Cancer: Pathogenesis, Diagnosis and Management with Focus on Endocrine Aspects. In Endotext; Feingold, K.R., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Dungan, K., Hofland, J., Kalra, S., Kaltsas, G., Kapoor, N., Koch, C., Kopp, P., Korbonits, M., Kovacs, C.S., Kuohung, W., Laferrère, B., Levy, M., McGee, E.A., McLachlan, R., New, M., Purnell, J., Sahay, R., Shah, A.S., Singer, F., Sperling, M.A., Stratakis, C.A., Trence, D.L., Wilson, D.P., Eds.; MDText.com, Inc.: South Dartmouth (MA), 2023. [Google Scholar]
- Cheville, J.C.; Sebo, T.J.; Lager, D.J.; Bostwick, D.G.; Farrow, G.M. Leydig Cell Tumor of the Testis: A Clinicopathologic, DNA Content, and MIB-1 Comparison of Nonmetastasizing and Metastasizing Tumors. Am. J. Surg. Pathol. 1998, 22, 1361–1367. [Google Scholar] [CrossRef]
- Washecka, R.; Dresner, M.I.; Honda, S.A.A. Testicular Tumors in Carney’s Complex. J. Urol. 2002, 167, 1299–1302. [Google Scholar] [CrossRef]
- Grogg, J.; Schneider, K.; Bode, P.K.; Kranzbühler, B.; Eberli, D.; Sulser, T.; Lorch, A.; Beyer, J.; Hermanns, T.; Fankhauser, C.D. Sertoli Cell Tumors of the Testes: Systematic Literature Review and Meta-Analysis of Outcomes in 435 Patients. Oncologist 2020, 25, 585–590. [Google Scholar] [CrossRef]
- Connolly, S.S.; D’Arcy, F.T.; Gough, N.; McCarthy, P.; Bredin, H.C.; Corcoran, M.O. Carefully Selected Intratesticular Lesions Can Be Safely Managed with Serial Ultrasonography. BJU Int. 2006, 98, 1005–1007. [Google Scholar] [CrossRef]
- Paffenholz, P.; Held, L.; Loosen, S.H.; Pfister, D.; Heidenreich, A. Testis Sparing Surgery for Benign Testicular Masses: Diagnostics and Therapeutic Approaches. J. Urol. 2018, 200, 353–360. [Google Scholar] [CrossRef]
- Maizlin, Z.V.; Belenky, A.; Kunichezky, M.; Sandbank, J.; Strauss, S. Leydig Cell Tumors of the Testis: Gray Scale and Color Doppler Sonographic Appearance. J. Ultrasound Med. 2004, 23, 959–964. [Google Scholar] [CrossRef]
- Grand, T.; Hermann, A.-L.; Gérard, M.; Arama, E.; Ouerd, L.; Garrouche, N.; Rocher, L. Precocious Puberty Related to Leydig Cell Testicular Tumor: The Diagnostic Imaging Keys. Eur. J. Med. Res. 2022, 27, 67. [Google Scholar] [CrossRef]
- Akman, H.; Ege, G.; Yildiz, S.; Cakiroglu, G. Incidental Bilateral Leydig Cell Tumor of the Testes. Urol. Int. 2003, 71, 316–318. [Google Scholar] [CrossRef] [PubMed]
- Drudi, F.M.; Valentino, M.; Bertolotto, M.; Malpassini, F.; Maghella, F.; Cantisani, V.; Liberatore, M.; De Felice, C.; D’Ambrosio, F. CEUS Time Intensity Curves in the Differentiation Between Leydig Cell Carcinoma and Seminoma: A Multicenter Study. Ultraschall Med. 2016, 37, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Samson, M.; Peale, F.V., Jr; Frantz, G.; Rioux-Leclercq, N.; Rajpert-De Meyts, E.; Ferrara, N. Human Endocrine Gland-Derived Vascular Endothelial Growth Factor: Expression Early in Development and in Leydig Cell Tumors Suggests Roles in Normal and Pathological Testis Angiogenesis. J. Clin. Endocrinol. Metab. 2004, 89, 4078–4088. [Google Scholar] [CrossRef] [PubMed]
- Lock, G.; Schmidt, C.; Helmich, F.; Stolle, E.; Dieckmann, K.-P. Early Experience with Contrast-Enhanced Ultrasound in the Diagnosis of Testicular Masses: A Feasibility Study. Urology 2011, 77, 1049–1053. [Google Scholar] [CrossRef]
- Luzurier, A.; Maxwell, F.; Correas, J.M.; Benoit, G.; Izard, V.; Ferlicot, S.; Teglas, J.P.; Bellin, M.F.; Rocher, L. Qualitative and Quantitative Contrast-Enhanced Ultrasonography for the Characterisation of Non-Palpable Testicular Tumours. Clin. Radiol. 2018, 73, 322–e1. [Google Scholar] [CrossRef]
- Lerchbaumer, M.H.; Auer, T.A.; Marticorena, G.S.; Stephan, C.; Hamm, B.; Jung, E.-M.; Fischer, T. Diagnostic Performance of Contrast-Enhanced Ultrasound (CEUS) in Testicular Pathologies: Single-Center Results. Clin. Hemorheol. Microcirc. 2019, 73, 347–357. [Google Scholar] [CrossRef]
- Pinto, S.P.S.; Huang, D.Y.; Dinesh, A.A.; Sidhu, P.S.; Ahmed, K. A Systematic Review on the Use of Qualitative and Quantitative Contrast-Enhanced Ultrasound in Diagnosing Testicular Abnormalities. Urology 2021, 154, 16–23. [Google Scholar] [CrossRef]
- Young, R.H.; Koelliker, D.D.; Scully, R.E. Sertoli Cell Tumors of the Testis, Not Otherwise Specified: A Clinicopathologic Analysis of 60 Cases. Am. J. Surg. Pathol. 1998, 22, 709–721. [Google Scholar] [CrossRef]
- Harms, D.; Kock, L.R. Testicular Juvenile Granulosa Cell and Sertoli Cell Tumours: A Clinicopathological Study of 29 Cases from the Kiel Paediatric Tumour Registry. Virchows Arch. 1997, 430, 301–309. [Google Scholar] [CrossRef]
- Vitolo, U.; Ferreri, A.J.M.; Zucca, E. Primary Testicular Lymphoma. Crit. Rev. Oncol. Hematol. 2008, 65, 183–189. [Google Scholar] [CrossRef]
- Nguyen, H.T.K.; Terao, M.A.; Green, D.M.; Pui, C.-H.; Inaba, H. Testicular Involvement of Acute Lymphoblastic Leukemia in Children and Adolescents: Diagnosis, Biology, and Management. Cancer 2021, 127, 3067–3081. [Google Scholar] [CrossRef] [PubMed]
- Gutjahr, P.; Humpl, T. Testicular Lymphoblastic Leukemia/lymphoma. World J. Urol. 1995, 13, 230–232. [Google Scholar] [CrossRef] [PubMed]
- de Jesus, L.E.; Dekermacher, S.; Resende, G.C.; Justiniano, R.R. Testicular Involvement in Pediatric Acute Lymphocytic Leukemia: What to Do about It? Int. Braz J Urol 2022, 48, 981–987. [Google Scholar] [CrossRef] [PubMed]
- Koh, S.Y.; Lee, S.; Lee, S.B.; Cho, Y.J.; Choi, Y.H.; Cheon, J.-E.; Kim, W.S. Shear-Wave Elastography for the Assessment of Testicular Involvement of Hematologic Malignancies in Children and Young Adults: A Feasibility Study. Ultrasonography 2022, 41, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Mazzu, D.; Jeffrey, R.B., Jr; Ralls, P.W. Lymphoma and Leukemia Involving the Testicles: Findings on Gray-Scale and Color Doppler Sonography. AJR Am. J. Roentgenol. 1995, 164, 645–647. [Google Scholar] [CrossRef]
- Arrigan, M.; Smyth, L.; Harmon, M.; Flynn, C.; Sheehy, N. Imaging Findings in Recurrent Extramedullary Leukaemias. Cancer Imaging 2013, 13, 26–35. [Google Scholar] [CrossRef]
- Hermann, A.-L.; L’Herminé-Coulomb, A.; Irtan, S.; Audry, G.; Cardoen, L.; Brisse, H.J.; Vande Perre, S.; Pointe, H.D.L. Imaging of Pediatric Testicular and Para-Testicular Tumors: A Pictural Review. Cancers 2022, 14. [Google Scholar] [CrossRef]
- Khan, M.; Rajarubendra, N.; Azer, S.; Skene, A.; Harrison, S.J.; Campbell, B.; Lawrentschuk, N. Plasmacytoma of the Testis in a Patient with Relapsed and Refractory Multiple Myeloma: Case Report and Review of the Literature. Urol. Ann. 2015, 7, 530–533. [Google Scholar] [CrossRef]
- Shimokihara, K.; Kawahara, T.; Chiba, S.; Takamoto, D.; Yao, M.; Uemura, H. Extramedullary Plasmacytoma of the Testis: A Case Report. Urol Case Rep 2018, 16, 101–103. [Google Scholar] [CrossRef]
- Schiavo, C.; Mann, S.A.; Mer, J.; Suvannasankha, A. Testicular Plasmacytoma Misdiagnosed as Orchitis. BMJ Case Rep. 2018, 2018. [Google Scholar] [CrossRef]
- McCann, C.; Doherty, A.; Flynn, C.; Mulholland, C. Prostate Cancer Metastasis to the Testis: An Unexpected Presentation of a Solitary Recurrence. BMJ Case Rep. 2021, 14. [Google Scholar] [CrossRef] [PubMed]
- Birker, I.L.; van der Zee, J.A.; Keizer, K.M. Uncommon Testicular Metastasis of a Primary Neuroendocrine Tumour of the Lung. Can. Urol. Assoc. J. 2013, 7, E614–E617. [Google Scholar] [CrossRef] [PubMed]
- Hatoum, H.A.; Abi Saad, G.S.; Otrock, Z.K.; Barada, K.A.; Shamseddine, A.I. Metastasis of Colorectal Carcinoma to the Testes: Clinical Presentation and Possible Pathways. Int. J. Clin. Oncol. 2011, 16, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Qazi, H.A.R.; Manikandan, R.; Foster, C.S.; Fordham, M.V. Testicular Metastasis from Gastric Carcinoma. Urology 2006, 68, 890–e7. [Google Scholar] [CrossRef]
- Dusaud, M.; Adjadj, L.; Debelmas, A.; Souraud, J.B.; Durand, X. Malignant Melanoma Revealed by Testicular Metastasi. Int. J. Surg. Case Rep. 2015, 12, 102–105. [Google Scholar] [CrossRef]
- Hou, G.; Jiang, Y.; Cheng, X. Testicular Metastasis of Pancreatic Carcinoma on FDG-PET/CT. Clin. Nucl. Med. 2020, 45, 85–86. [Google Scholar] [CrossRef]
- Rouvinov, K.; Neulander, E.Z.; Kan, E.; Asali, M.; Ariad, S.; Mermershtain, W. Testicular Metastasis from Renal Cell Carcinoma: A Case Report and Review of the Literature. Case Rep. Oncol. 2017, 10, 388–391. [Google Scholar] [CrossRef]
- Turo, R.; Smolski, M.; Hatimy, U.; Bromage, S.J.; Brown, S.C.W.; Brough, R.; Collins, G.N. A Rare Case of Testicular Metastasis of Bladder Transitional Cell Carcinoma. Can. Urol. Assoc. J. 2014, 8, E181–E183. [Google Scholar] [CrossRef]
- Appetecchia, M.; Barnabei, A.; Pompeo, V.; Sentinelli, S.; Baldelli, R.; Corsello, S.M.; Torino, F. Testicular and Inguinal Lymph Node Metastases of Medullary Thyroid Cancer: A Case Report and Review of the Literature. BMC Endocr. Disord. 2014, 14, 84. [Google Scholar] [CrossRef]
- Simon, T.; Hero, B.; Berthold, F. Testicular and Paratesticular Involvement by Metastatic Neuroblastoma. Cancer 2000, 88, 2636–2641. [Google Scholar] [CrossRef]
- Sidhu, P.S.; Sriprasad, S.; Bushby, L.H.; Sellars, M.E.; Muir, G.H. Impalpable Testis Cancer. BJU Int. 2004, 93, 888. [Google Scholar] [CrossRef] [PubMed]
- Iannantuono, G.M.; Strigari, L.; Roselli, M.; Torino, F. A Scoping Review on the “Burned out” or “Burnt out” Testicular Cancer: When a Rare Phenomenon Deserves More Attention. Crit. Rev. Oncol. Hematol. 2021, 165, 103452. [Google Scholar] [CrossRef] [PubMed]
- Sidhu, P.S.; Muir, G.H. Extragonadal Tumor and Testicular Microlithiasis: “Burned-out” Tumors Are Represented by Macrocalcification. J. Ultrasound Med. 2011, 30, 1604–1605. [Google Scholar] [CrossRef]
- Pedersen, M.R.; Bartlett, E.C.; Brown, C.; Rafaelsen, S.R.; Sellars, M.E.; Sidhu, P.S. Is Testicular Macrocalcification a Risk for Malignancy?: Tumor Development on Ultrasonographic Follow-up of Preexisting Intratesticular Macrocalcification. J. Ultrasound Med. 2018, 37, 2949–2953. [Google Scholar] [CrossRef] [PubMed]
- Rocher, L.; Glas, L.; Bellin, M.F.; Ferlicot, S.; Izard, V.; Benoit, G.; Albiges, L.; Fizazi, K.; Correas, J.-M. Burned-Out Testis Tumors in Asymptomatic Infertile Men: Multiparametric Sonography and MRI Findings. J. Ultrasound Med. 2017, 36, 821–831. [Google Scholar] [CrossRef]
- Comiter, C.V.; Renshaw, A.A.; Benson, C.B.; Loughlin, K.R. Burned-out Primary Testicular Cancer: Sonographic and Pathological Characteristics. J. Urol. 1996, 156, 85–88. [Google Scholar] [CrossRef]
- Tasu, J.-P.; Faye, N.; Eschwege, P.; Rocher, L.; Bléry, M. Imaging of Burned-out Testis Tumor: Five New Cases and Review of the Literature. J. Ultrasound Med. 2003, 22, 515–521. [Google Scholar] [CrossRef]
- Fabre, E.; Jira, H.; Izard, V.; Ferlicot, S.; Hammoudi, Y.; Theodore, C.; Di Palma, M.; Benoit, G.; Droupy, S. “Burned-out” Primary Testicular Cancer. BJU Int. 2004, 94, 74–78. [Google Scholar] [CrossRef]
Figure 1.
Epidermoid cyst. GSUS demonstrates a well-circumscribed, solid, mixed-reflectivity lesion with high-reflectivity “onion-skin” peripheral rims (panel A), avascular at CDUS (panel B). SE shows a mixed elasticity lesion (panel C), while contrast-enhanced US demonstrates a clear lack of enhancement within the lesion (panel D).
Figure 1.
Epidermoid cyst. GSUS demonstrates a well-circumscribed, solid, mixed-reflectivity lesion with high-reflectivity “onion-skin” peripheral rims (panel A), avascular at CDUS (panel B). SE shows a mixed elasticity lesion (panel C), while contrast-enhanced US demonstrates a clear lack of enhancement within the lesion (panel D).
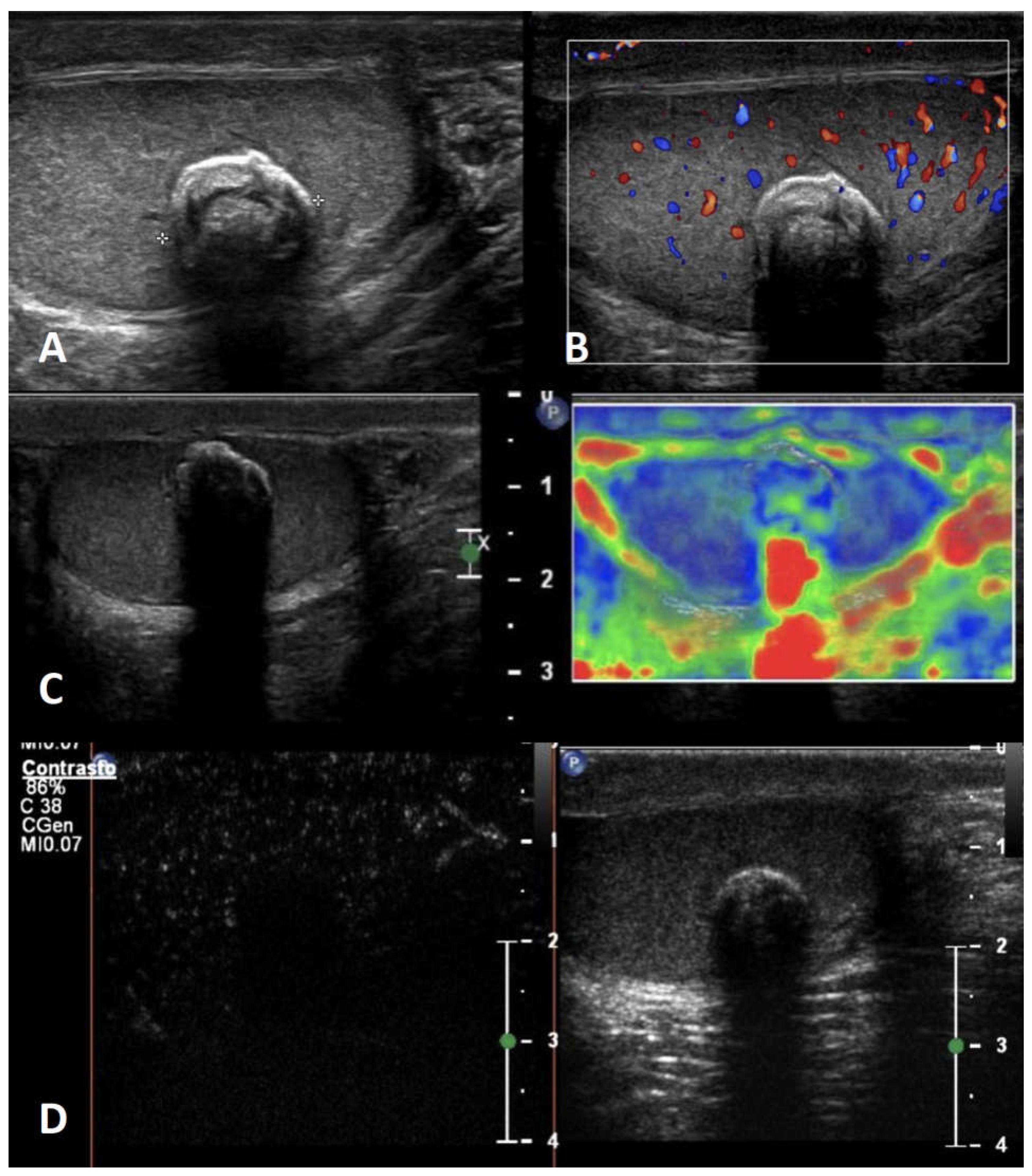
Figure 2.
Embryonal carcinoma with internal necrosis (panel A) and atypical epidermoid cyst (panel B): both demonstrate at CEUS lack of vascularity.
Figure 2.
Embryonal carcinoma with internal necrosis (panel A) and atypical epidermoid cyst (panel B): both demonstrate at CEUS lack of vascularity.
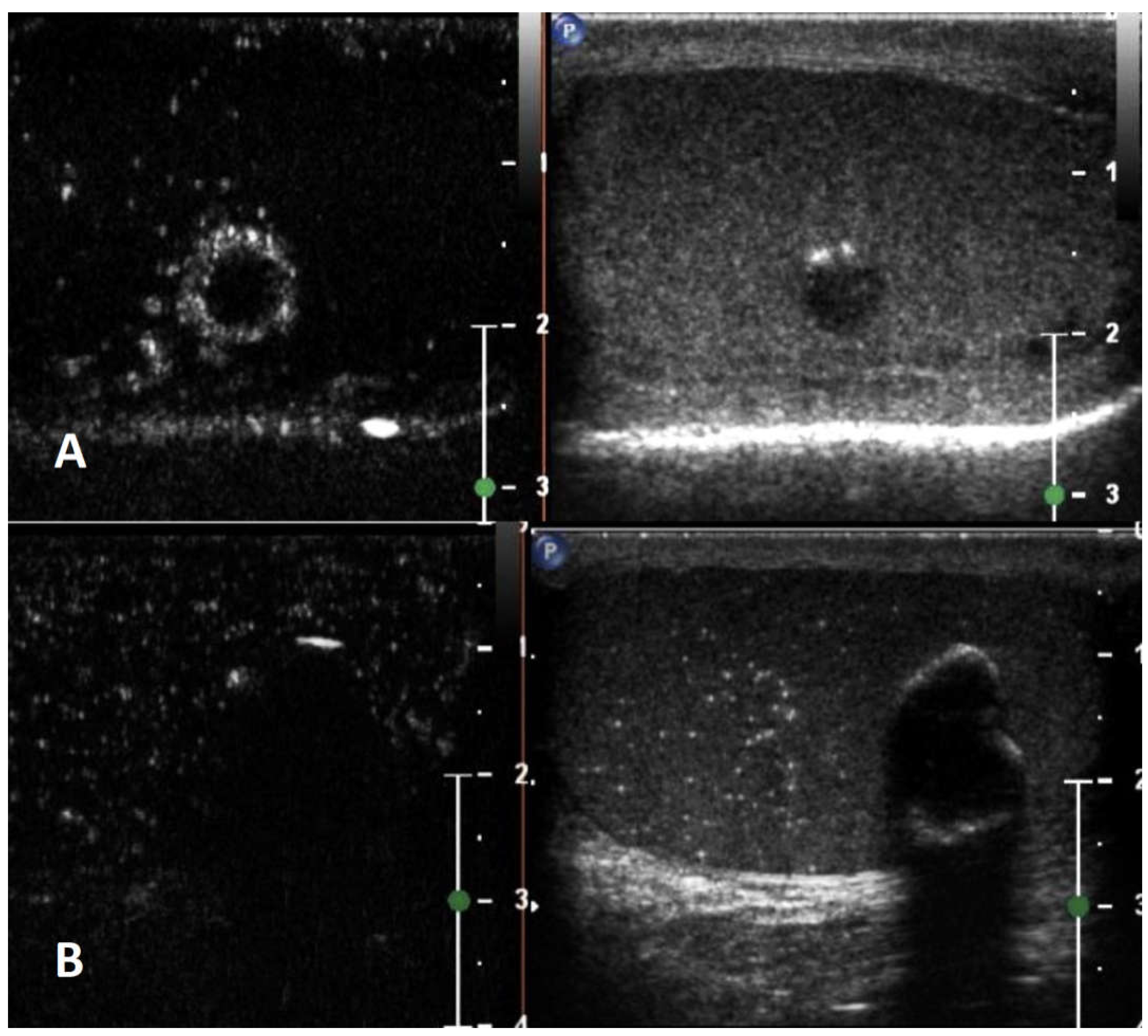
Figure 3.
Testicular adrenal rest tumor. GSUS (panel A) and CDUS (panel B) demonstrate bilateral hypoechoic lesions, highly vascularized, with irregular, lobulated margins. At SE they appear as hard lesions (panel C). TARTs show increased contrast-enhancement on CEUS (panel D).
Figure 3.
Testicular adrenal rest tumor. GSUS (panel A) and CDUS (panel B) demonstrate bilateral hypoechoic lesions, highly vascularized, with irregular, lobulated margins. At SE they appear as hard lesions (panel C). TARTs show increased contrast-enhancement on CEUS (panel D).
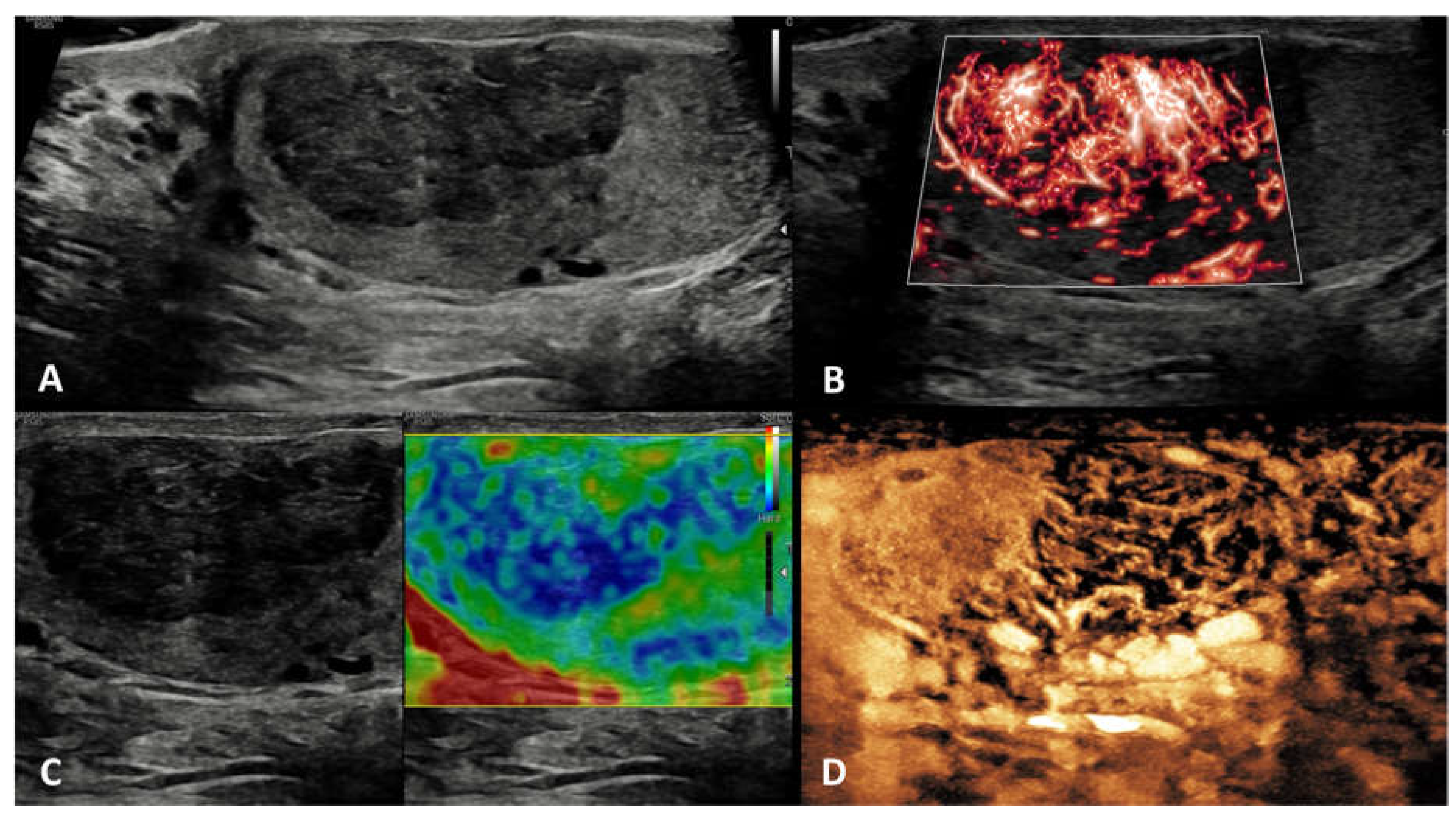
Figure 4.
Sarcoidosis. GSUS (panel A) and CDUS (panel B) demonstrate multiple small hypoechoic lesions with irregular margins and some internal vascular spots. At SE sarcoidosis granulomas appear as hard lesions (panel C). CEUS can confirm the presence of contrast-enhancement within the lesions (panel D).
Figure 4.
Sarcoidosis. GSUS (panel A) and CDUS (panel B) demonstrate multiple small hypoechoic lesions with irregular margins and some internal vascular spots. At SE sarcoidosis granulomas appear as hard lesions (panel C). CEUS can confirm the presence of contrast-enhancement within the lesions (panel D).
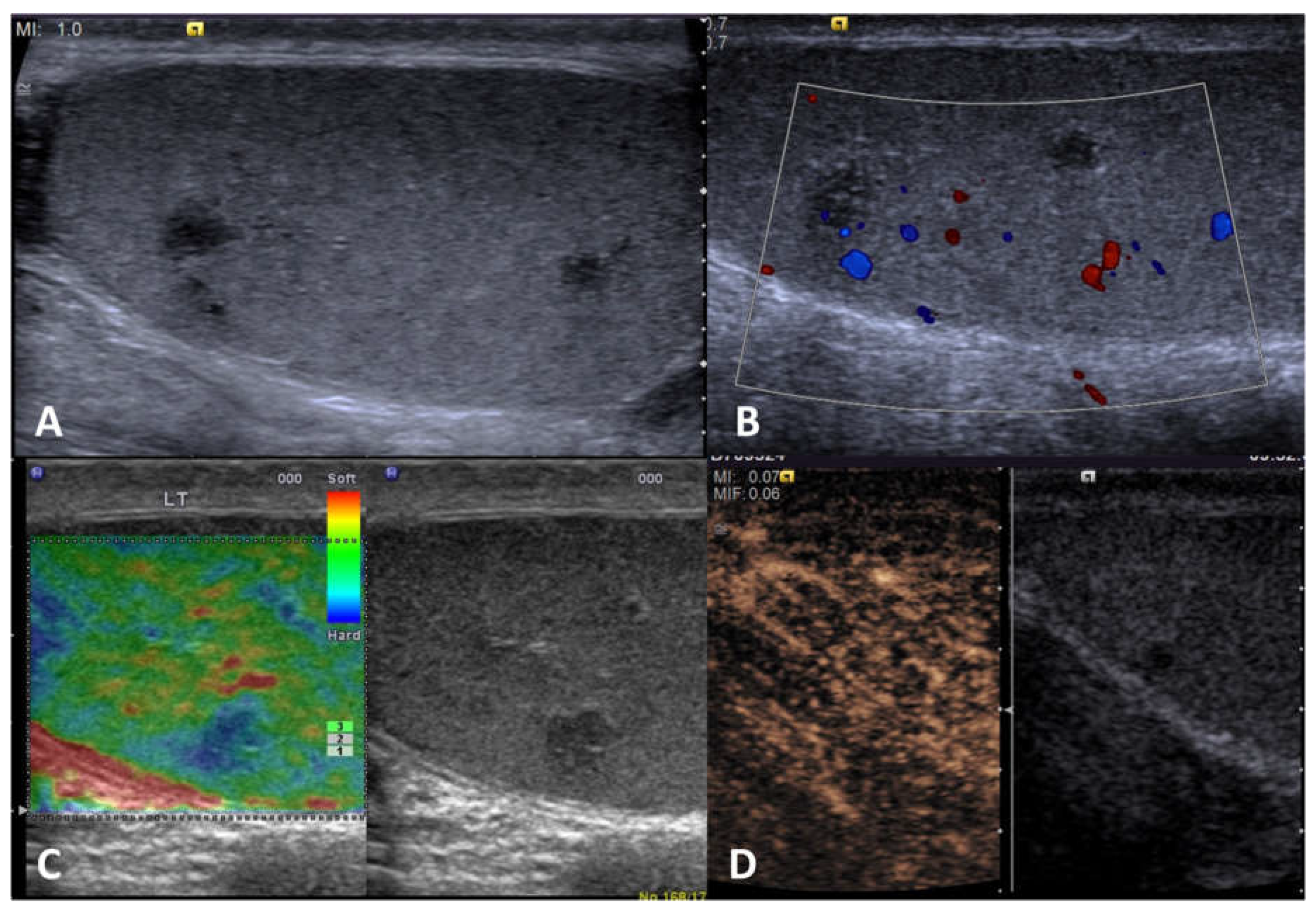
Figure 5.
Segmental testicular infarction. GSUS demonstrates hypoechoic lesions, mimicking a tumor (panel A). CDUS shows lack of internal vascularization (panel B). At SE segmental infarction shows intermediate/high elastic strain (panel C), whereas CEUS confirms the absence of vascularity within the lesion (panel D).
Figure 5.
Segmental testicular infarction. GSUS demonstrates hypoechoic lesions, mimicking a tumor (panel A). CDUS shows lack of internal vascularization (panel B). At SE segmental infarction shows intermediate/high elastic strain (panel C), whereas CEUS confirms the absence of vascularity within the lesion (panel D).

Figure 6.
Abscess. GSUS demonstrates a focal, complex, heterogeneous low reflecting lesion with irregular margins (panel A). CDUS shows a hypervascular rim surrounding the lesion, with no internal vascular signal (panel B). At SE testicular abscess shows a heterogeneous pattern of firmness (panel C). CEUS demonstrates absence of internal contrast-enhancement with some peripheral enhancement (panel D).
Figure 6.
Abscess. GSUS demonstrates a focal, complex, heterogeneous low reflecting lesion with irregular margins (panel A). CDUS shows a hypervascular rim surrounding the lesion, with no internal vascular signal (panel B). At SE testicular abscess shows a heterogeneous pattern of firmness (panel C). CEUS demonstrates absence of internal contrast-enhancement with some peripheral enhancement (panel D).
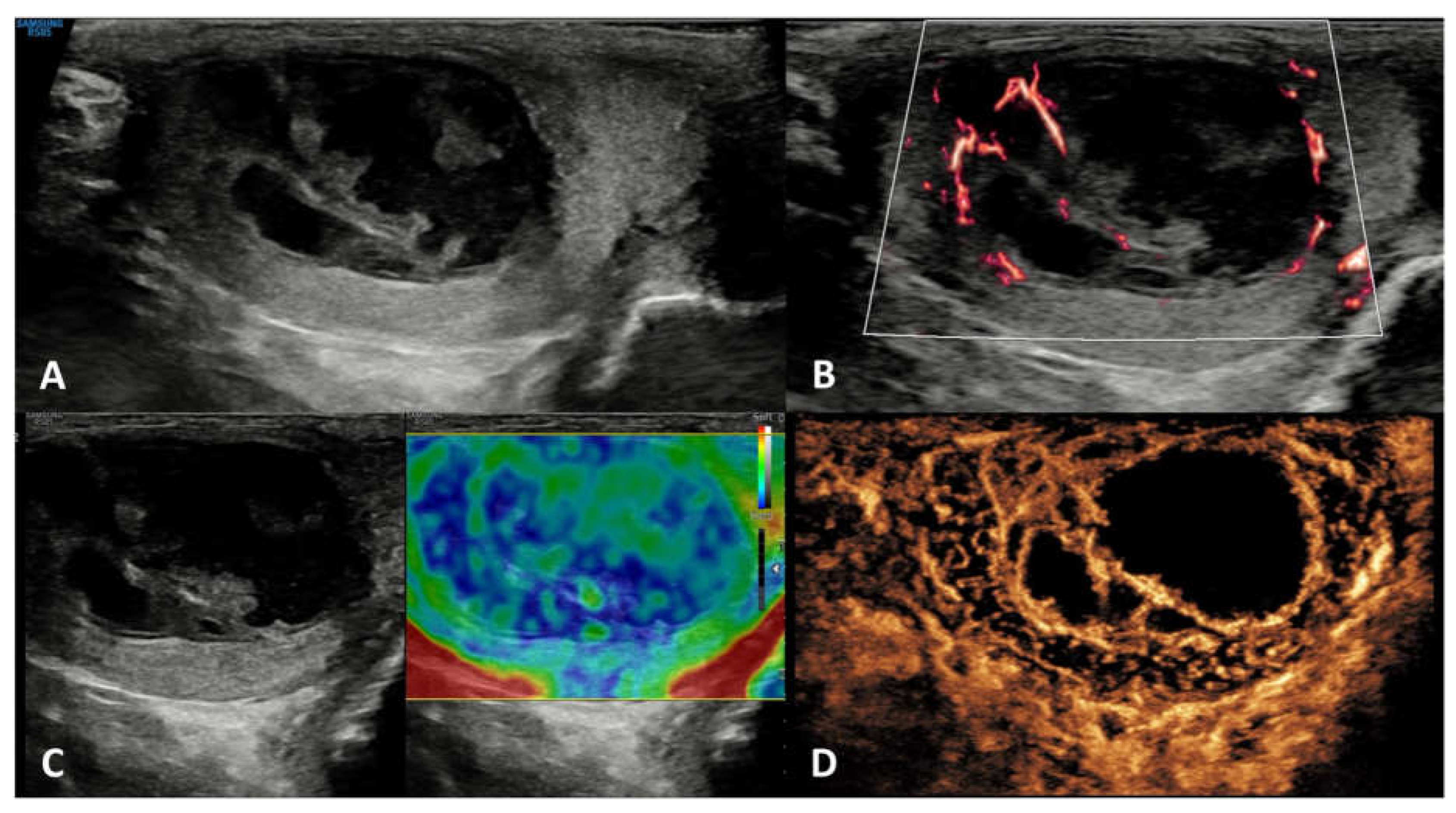
Figure 7.
Hematoma. GSUS demonstrates well-circumscribed anechoic lesions with septa and solid components (panel A). CDUS shows lack of internal vascularization (panel B). At SE hematoma shows intermediate/high elastic strain (panel C), whereas CEUS confirms the absence of vascularity within the lesion (panel D).
Figure 7.
Hematoma. GSUS demonstrates well-circumscribed anechoic lesions with septa and solid components (panel A). CDUS shows lack of internal vascularization (panel B). At SE hematoma shows intermediate/high elastic strain (panel C), whereas CEUS confirms the absence of vascularity within the lesion (panel D).
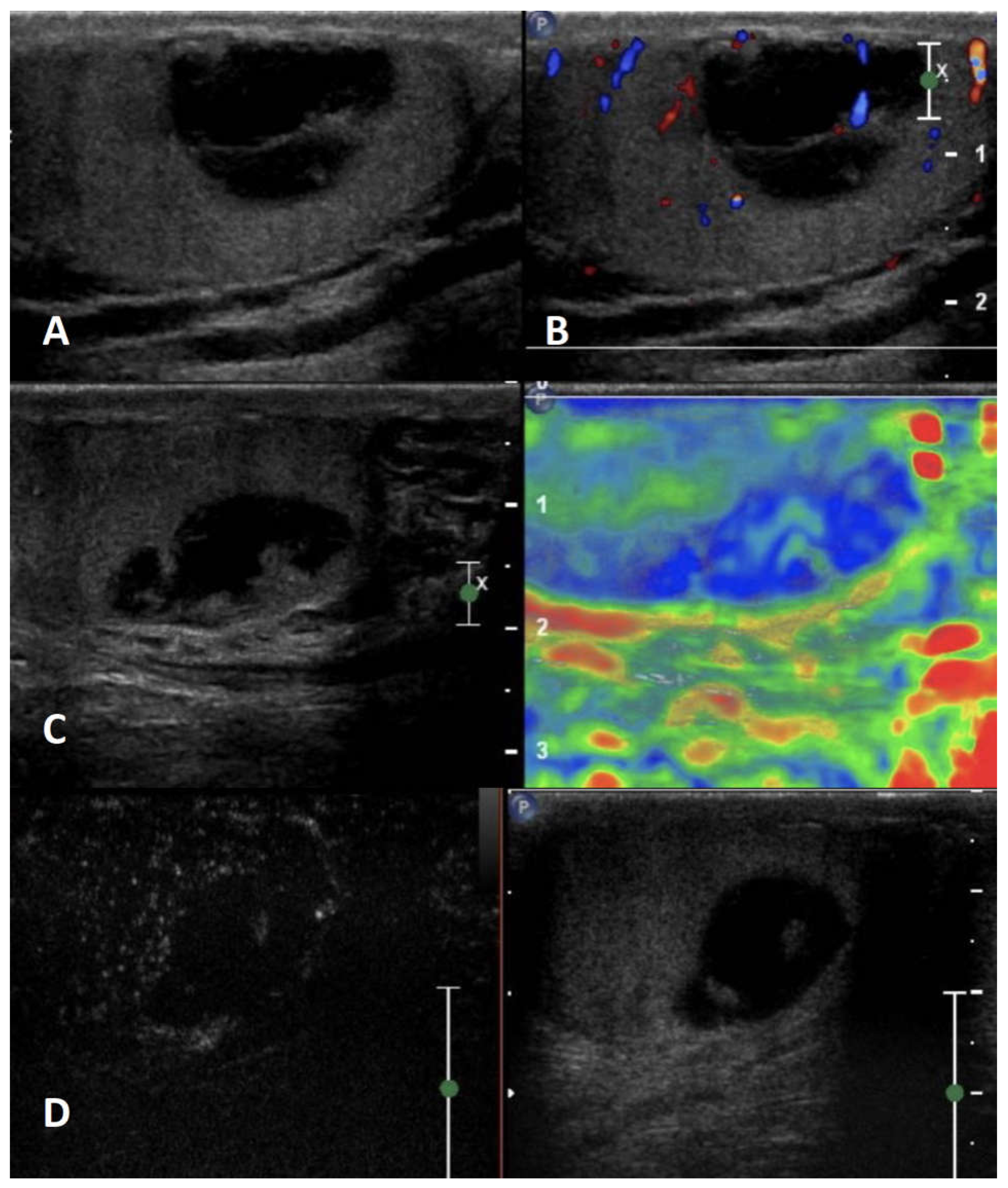
Figure 8.
Idiopathic granulomatous orchitis. GSUS demonstrates multiple ill-defined, homogeneous, hypoechoic lesions (panel A). CDUS shows increased internal vascularization (panel B). At SE the testis shows diffuse intermediate elastic strain (panel C), whereas CEUS confirms the hyperenhancement within the lesions (panel D).
Figure 8.
Idiopathic granulomatous orchitis. GSUS demonstrates multiple ill-defined, homogeneous, hypoechoic lesions (panel A). CDUS shows increased internal vascularization (panel B). At SE the testis shows diffuse intermediate elastic strain (panel C), whereas CEUS confirms the hyperenhancement within the lesions (panel D).

Figure 9.
Tuberculous granulomatous orchitis. GSUS demonstrates focal hypoechoic lesions, with blurred margins (panel A). CDUS shows only peripheric vascularization (panel B). At SE tuberculous granuloma shows intermediate elastic strain (panel C). CEUS confirms the hypoenhanced lesions with peripheral rim (panel D).
Figure 9.
Tuberculous granulomatous orchitis. GSUS demonstrates focal hypoechoic lesions, with blurred margins (panel A). CDUS shows only peripheric vascularization (panel B). At SE tuberculous granuloma shows intermediate elastic strain (panel C). CEUS confirms the hypoenhanced lesions with peripheral rim (panel D).
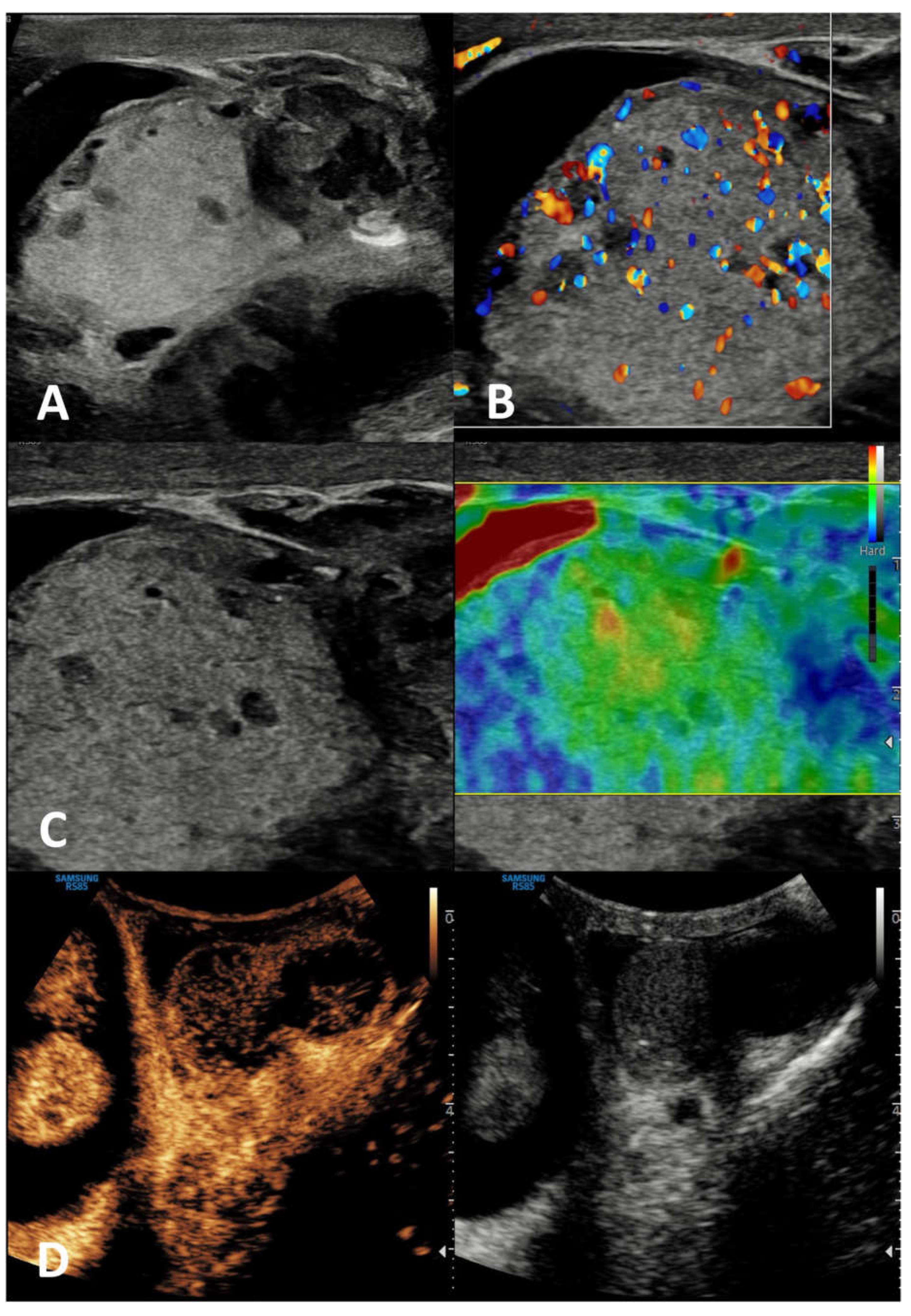
Figure 10.
Seminoma. GSUS demonstrates a well-circumscribed homogeneously hypoechoic lesion (panel A). CDUS shows increased internal vascularization (panel B). At SE seminoma shows absent elastic strain (panel C), whereas CEUS confirms the hyperenhancement within the lesion (panel D).
Figure 10.
Seminoma. GSUS demonstrates a well-circumscribed homogeneously hypoechoic lesion (panel A). CDUS shows increased internal vascularization (panel B). At SE seminoma shows absent elastic strain (panel C), whereas CEUS confirms the hyperenhancement within the lesion (panel D).
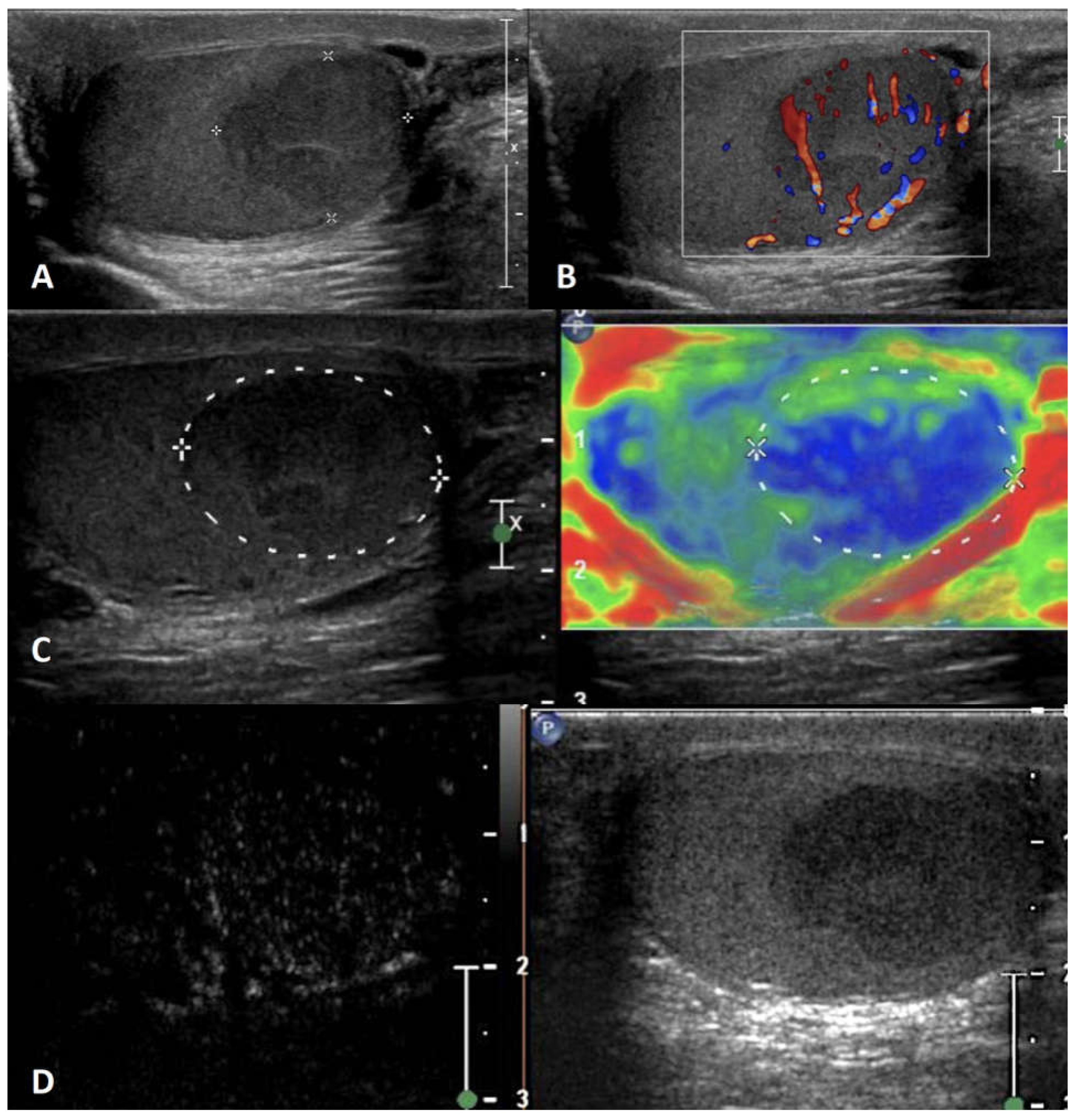
Figure 11.
Embryonal carcinoma. GSUS demonstrates a markedly hypoechoic lesion (panel A) in a testis with starry sky appearance. CDUS shows peripheral and internal vascularization (panel B). At SE the tumor shows absent elastic strain (panel C), whereas CEUS confirms the hyperenhancement within the lesion (panel D).
Figure 11.
Embryonal carcinoma. GSUS demonstrates a markedly hypoechoic lesion (panel A) in a testis with starry sky appearance. CDUS shows peripheral and internal vascularization (panel B). At SE the tumor shows absent elastic strain (panel C), whereas CEUS confirms the hyperenhancement within the lesion (panel D).
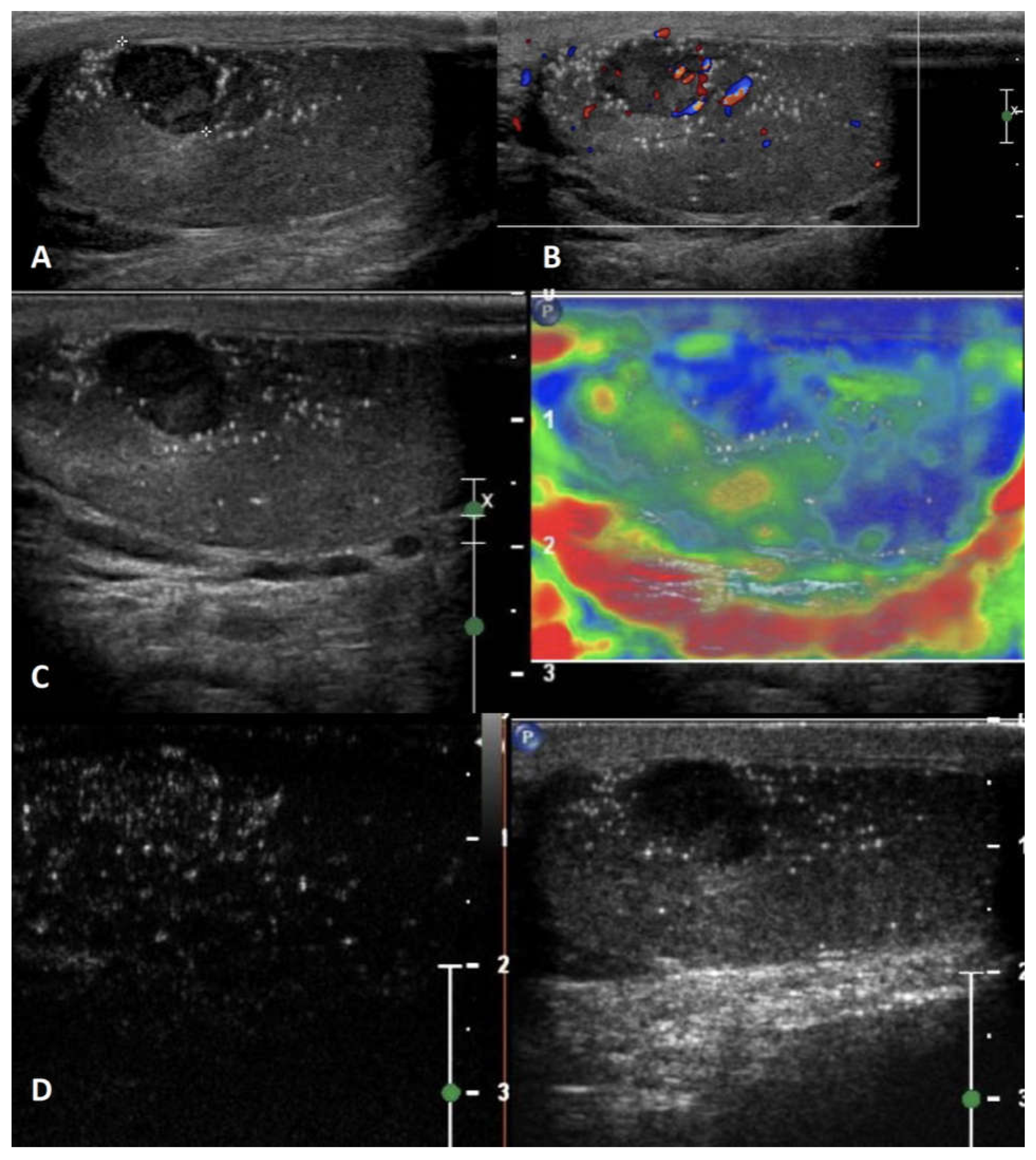
Figure 12.
Mixed germ cell tumor. GSUS demonstrates multiple markedly and mild hypoechoic lesions (panel A), occupying almost the entire testis. CDUS shows peripheral and markedly internal vascularization (panel B). At SE the tumor shows intermediate/absent elastic strain (panel C). CEUS demonstrates hyperenhancement of the entire lesion (panel D).
Figure 12.
Mixed germ cell tumor. GSUS demonstrates multiple markedly and mild hypoechoic lesions (panel A), occupying almost the entire testis. CDUS shows peripheral and markedly internal vascularization (panel B). At SE the tumor shows intermediate/absent elastic strain (panel C). CEUS demonstrates hyperenhancement of the entire lesion (panel D).
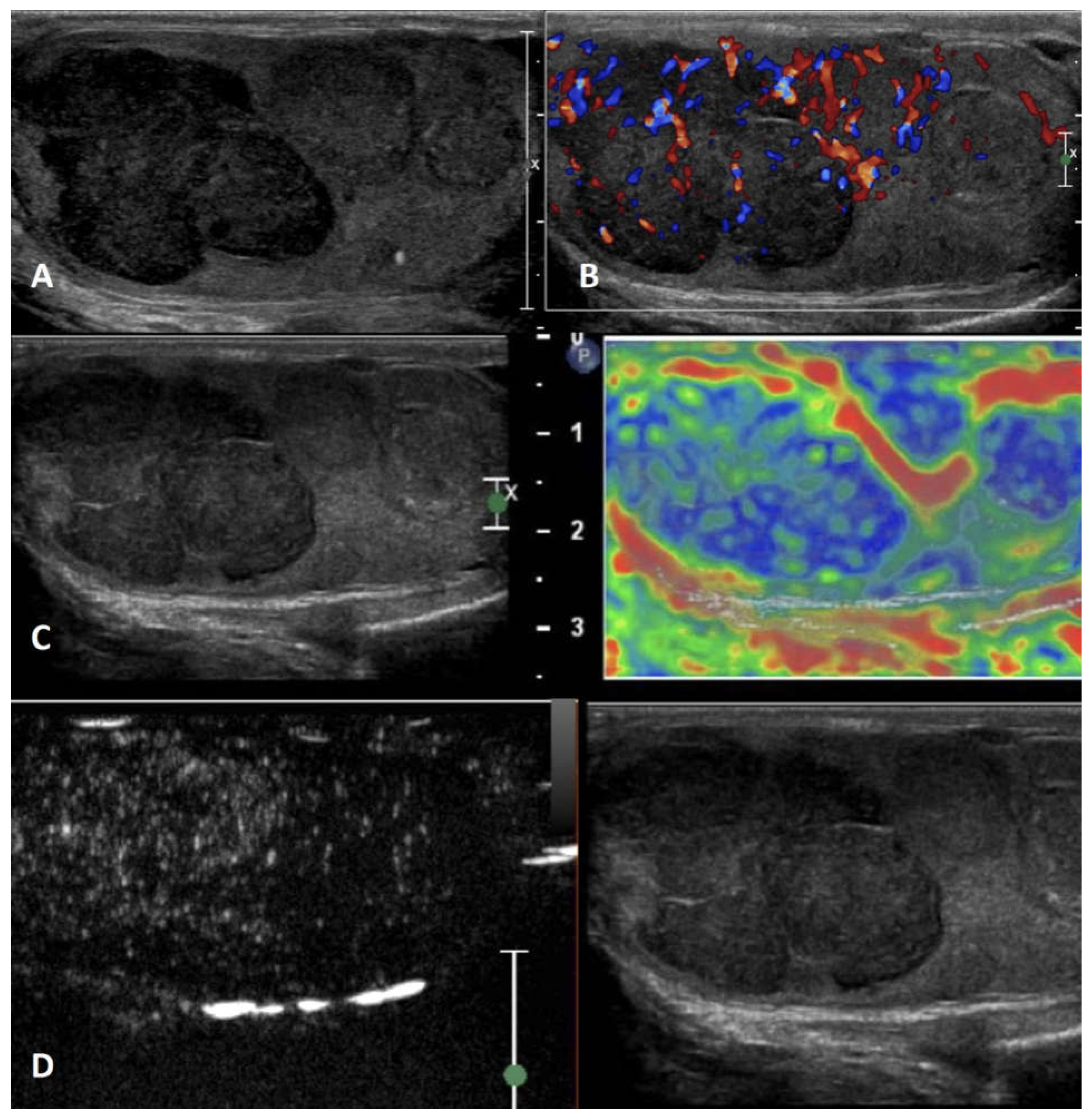
Figure 13.
Leydig cell tumor. GSUS demonstrates a well-defined hypoechoic lesion (panel A), with hyperechoic halo. CDUS shows peripheral and marked internal vascularization (panel B). At SE the tumor shows absent elastic strain (panel C). CEUS confirms the hyperenhancement within the lesion (panel D).
Figure 13.
Leydig cell tumor. GSUS demonstrates a well-defined hypoechoic lesion (panel A), with hyperechoic halo. CDUS shows peripheral and marked internal vascularization (panel B). At SE the tumor shows absent elastic strain (panel C). CEUS confirms the hyperenhancement within the lesion (panel D).
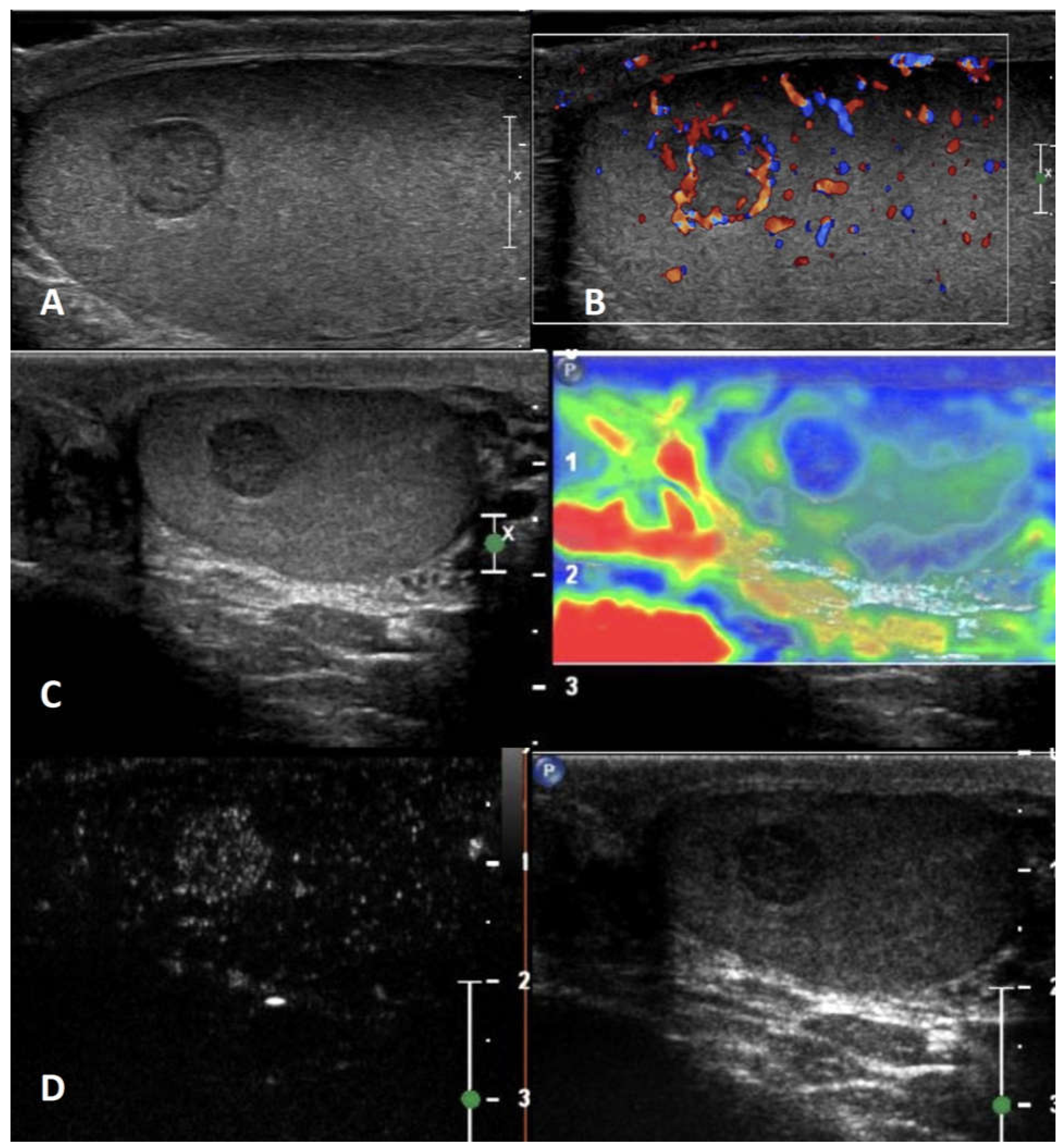
Figure 14.
Sertoli cell tumor. GSUS demonstrates a mild hypoechoic lesion (panel A), with irregular margins. CDUS shows markedly internal vascularization (panel B). At SE the tumor shows absent elastic strain (panel C). CEUS confirms the enhancement within the lesion (panel D).
Figure 14.
Sertoli cell tumor. GSUS demonstrates a mild hypoechoic lesion (panel A), with irregular margins. CDUS shows markedly internal vascularization (panel B). At SE the tumor shows absent elastic strain (panel C). CEUS confirms the enhancement within the lesion (panel D).
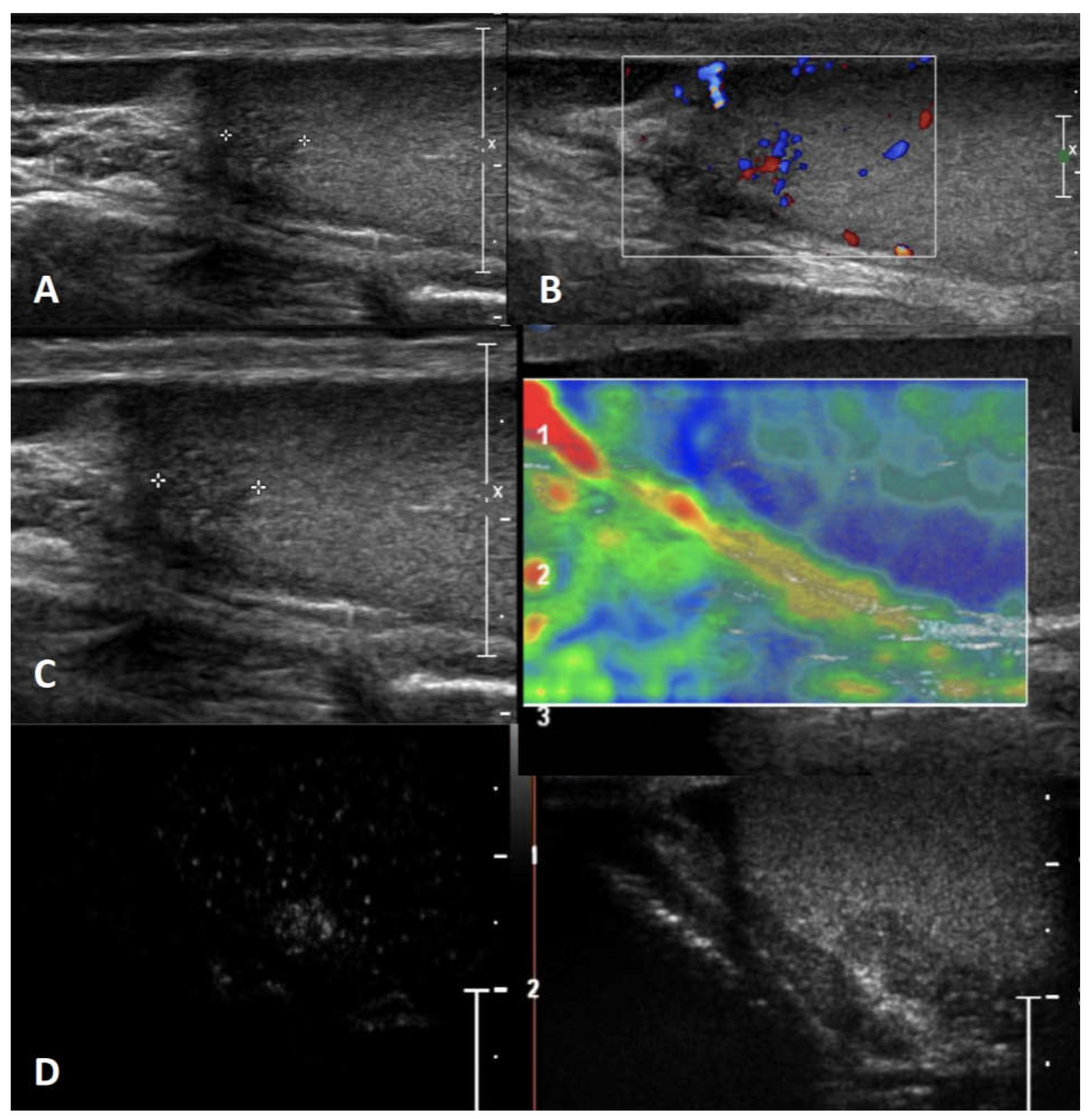
Figure 15.
Lymphoma, nodular pattern. GSUS demonstrates a markedly hypoechoic lesion, with multinodular aspect (panel A), with irregular margins, interesting the epididymis tail. CDUS shows markedly internal vascularization (panel B). At SE the tumor shows absent elastic strain (panel C). CEUS shows hyperenhancement of the lesions, with rapid wash-in and wash-out (panel D).
Figure 15.
Lymphoma, nodular pattern. GSUS demonstrates a markedly hypoechoic lesion, with multinodular aspect (panel A), with irregular margins, interesting the epididymis tail. CDUS shows markedly internal vascularization (panel B). At SE the tumor shows absent elastic strain (panel C). CEUS shows hyperenhancement of the lesions, with rapid wash-in and wash-out (panel D).
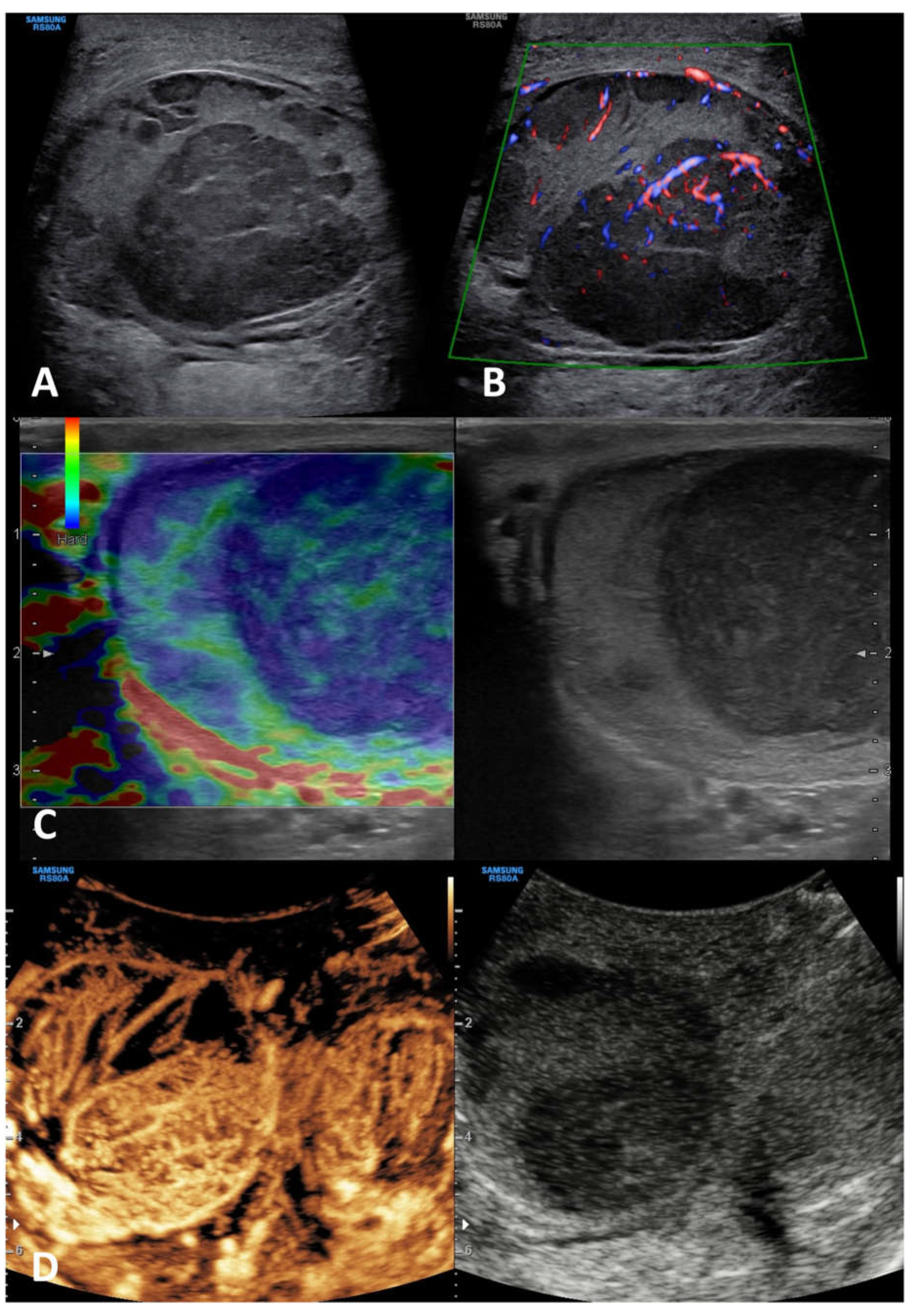
Figure 16.
Leukemia. GSUS demonstrates a hypoechoic lesion (panel A), with regular margins. CDUS shows internal vascularization of the lesion (panel B). At SE the lesion demonstrates intermediate/soft elastic strain (panel C). On CEUS lesion appears hyper-enhanced due to its high vascularity (panel D).
Figure 16.
Leukemia. GSUS demonstrates a hypoechoic lesion (panel A), with regular margins. CDUS shows internal vascularization of the lesion (panel B). At SE the lesion demonstrates intermediate/soft elastic strain (panel C). On CEUS lesion appears hyper-enhanced due to its high vascularity (panel D).
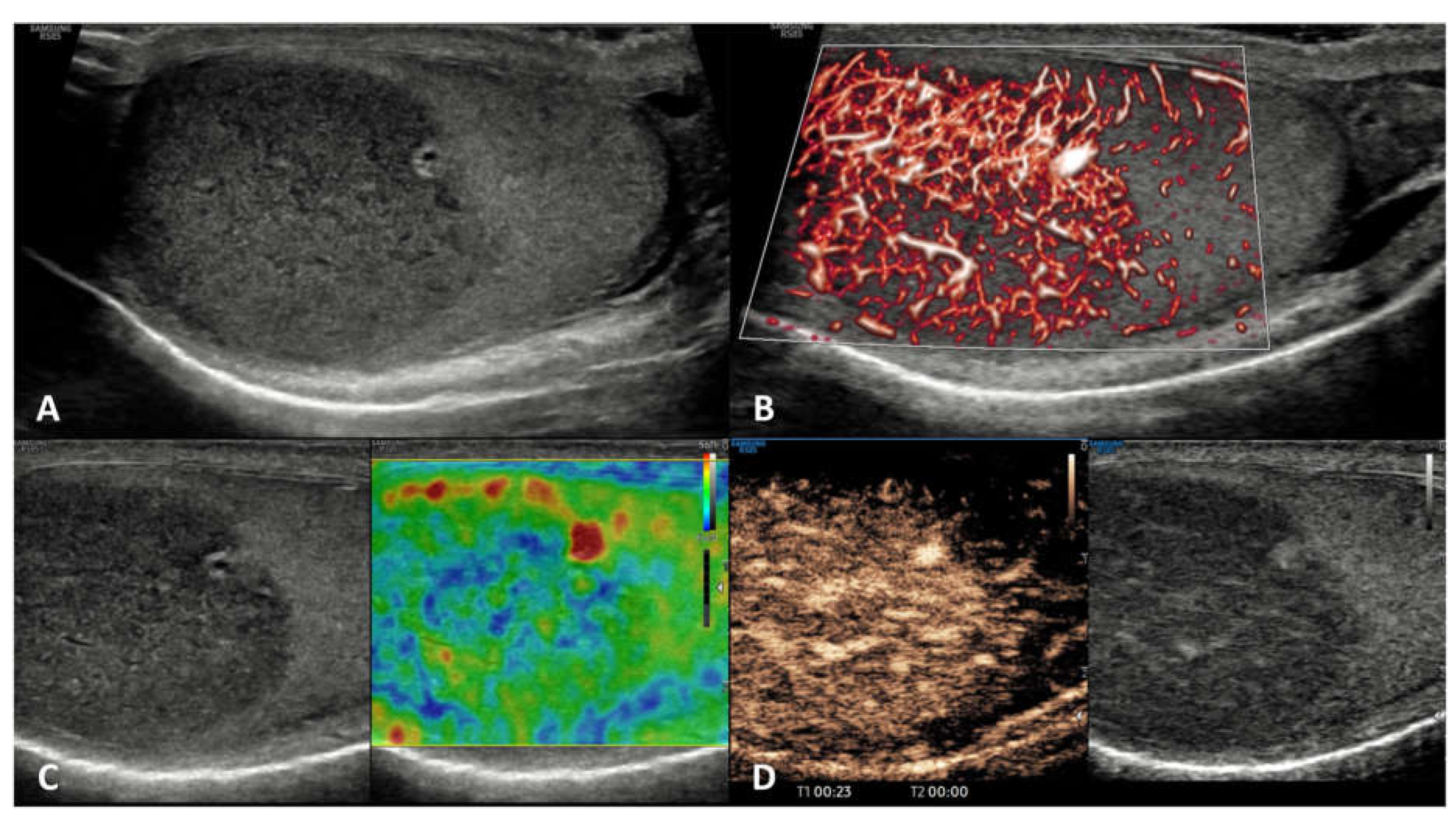
Figure 17.
Plasmacytoma. GSUS demonstrates multiple, both mild and markedly hypoechoic lesions (panel A), with smooth margins. CDUS shows internal vascularization of the lesions and hypervascularization of the entire testis (panel B). At SE the lesions demonstrate intermediate elastic strain (panel C).
Figure 17.
Plasmacytoma. GSUS demonstrates multiple, both mild and markedly hypoechoic lesions (panel A), with smooth margins. CDUS shows internal vascularization of the lesions and hypervascularization of the entire testis (panel B). At SE the lesions demonstrate intermediate elastic strain (panel C).
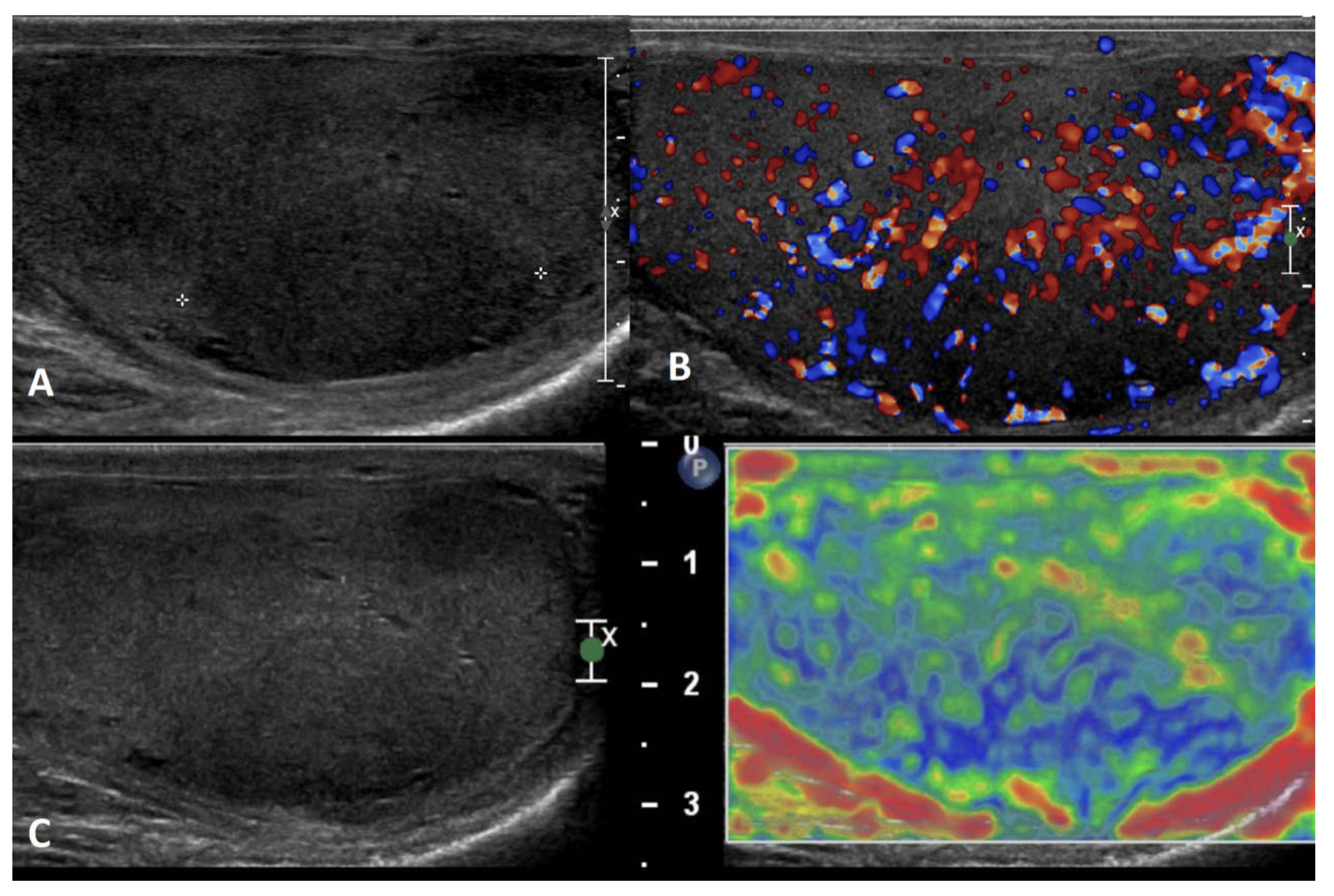

Table 1.
Clinical and multiparametric ultrasound (mp-US) characteristics of non-neoplastic lesions.
| Non-neoplastic intratesticular lesions | |||||
|---|---|---|---|---|---|
| Clinical presentation | GSUS | CDUS | CEUS | SE | |
| Simple cyst | asymptomatic/ incidental finding, usually not palpable |
rounded anechoic lesions with thin, clear, hyperechoic wall and posterior acoustic enhancement | avascular | unenhanced | soft lesion with high elastic strain |
| Epidermoid cyst | asymptomatic/ can be palpable |
well circumscribed rounded lesion with “onion ring” aspect (concentric hypo- and hyper-echoic rings) OR densely calcified mass with acoustic shadow OR cyst with hypoechoic rim and central calcification OR mixed atypical pattern | avascular | unenhanced/ perilesional rim enhancement |
hard lesion with low/absent elastic strain |
| Adrenal rest | patients with CAH; usually not palpable |
hypoechoic lesions with irregular margins, hyperechogenic foci, typically localized in the mediastinum testis, usually bilateral | markedly vascularized |
hyperenhanced | hard lesions with low/absent elastic strain |
| Sarcoidosis | in the context of a mulsystem disease; granulomas in other organs; asymptomatic OR painless/painful mass | hypoechoic lesions with irregular margins, often bilateral | possible signs of internal vascularization |
hypoenhanced | hard lesions with low/absent elastic strain |
| Segmental infarction | idiopathic or consequent to surgery, inflammatory events, blood disorders or autoimmune diseases; usually acute painful swollen scrotum (but also asymptomatic cases) | hypoechoic wedge-shaped or roundish area | Avascular or peripheral rim of low CD |
unenhanced/ perilesional rim enhancement |
soft lesions with high elastic strain |
| Abscess | acute scrotal pain and swelling/ fever/ high WBC | complex heterogeneous low reflecting lesion with irregular walls (in rare cases focal hyperechoic spots due to gas bubble) | avascular/ vascular rim |
unenhanced/ perilesional rim enhancement |
heterogeneous pattern of firmness |
| Hematoma | history of scrotal trauma | well circumscribed hyperechoic lesions which subsequently liquefy over time, becoming complex lesions with septa, cystic components, and fluid levels. Size decrease over time. | avascular | unenhanced/ perilesional rim enhancement |
soft lesion with intermediate/high elastic strain |
| Idiopathic (diffuse) granulomatous orchitis | in the context of a multisystem disease; asymptomatic OR painless/painful mass | diffusely hypoechoic testis or hypoechoic areas with ill-defined margins | markedly vascularized |
hyperenhanced | heterogeneous pattern of firmness |
| Infectious granulomatous (focal) orchitis | acute scrotal pain, testicular enlargement, and fever; possible epididymal enlargement, scrotal wall thickening and hydrocele | single or multiple variable echogenicity areas with blurred margins; appearance depends by the pathologic stages of infection, which include caseous necrosis, granulomas, and healing by fibrosis and calcification | Internal or peripheral depending on the stage |
unenhanced/ perilesional rim enhancement or hyperehnanced |
heterogeneous pattern of firmness depending on the stage |
Abbreviations: GSUS, grey scale ultrasound; CDUS, color Doppler ultrasound; CEUS, contrast-enhanced ultrasound; SE, sonoelastography; WBC = white blood count; CAH = congenital adrenal hyperplasia.
Table 2.
Clinical and multiparametric ultrasound (mp-US) characteristics of neoplastic lesions.
| Neoplastic intratesticular lesions | ||||||
|---|---|---|---|---|---|---|
| Clinical presentation | Serum tumor markers | GSUS | CDUS | CEUS | SE | |
| Leydig cell tumor | Generally asymptomatic; it can produce androgens | Negative | Hypoechoic, homogeneous well demarcated lesion (possible hyperechoic halo) |
Hypervascularized | Homogeneously hyperenhanced (rapid wash-in, delayed wash-out) |
Hard lesions with low/absent elastic strain |
| Sertoli cell tumor | Asymptomatic; they can be a part of multiple neoplasia syndromes, such as Carney Complex and Peutz-Jegers | Negative | Hypo- or hyper-echoic lesion, with possible calcifications | Hypervascularized | Homogeneously hyperenhanced |
Hard lesions with low/absent elastic strain |
| Seminoma | testicular swelling, pain, lumbar pain OR asymptomatic palpable firm testicular mass; possible gynecomastia |
Negative (possible increase of -hCG,) |
Hypoechoic homogeneous round or oval lesion, occasionally multinodular or with polycyclic lobulated margins (unfrequently inhomogeneous) |
Hypervascularized, with arborization and branches | Homogeneously hyperenhanced (rapid wash-in and wash-out) |
Hard lesions with low/absent elastic strain |
| Embryonal cell carcinoma | testicular swelling, pain, lumbar pain; palpable firm testicular mass; Possible gynecomastia |
Can be positive -FP, -hCG, LDH (not always) |
Hypoechoic heterogeneous lesions with rregular polylobate margins; can present internal cystic areas or calcific margins. |
Hypervascularized /avascular | Enhanced/unenhanced/ perilesional rim enhancement |
Hard lesions with low/absent elastic strain |
| Teratoma | testicular swelling, pain, lumbar pain; palpable firm testicular mass Possible gynecomastia |
Can be positive -FP, -hCG, LDH (not always) |
Heterogeneous lesions, well-circumscribed, with cystic areas and internal septa | Hypervascularized in the solid part | Inhomogeneously hyperenhanced |
Hard lesions with low/absent elastic strain (depending on liquid amount) |
| Choriocarcinoma | testicular swelling, pain, lumbar pain; palpable firm testicular mass Possible gynecomastia |
Can be positive -hCG, (not always) |
Heterogeneous lesions with hypo-anechoic areas (hemorrhage, necrosis) and calcifications | Hypervascularized | Hyperenhanced | Hard lesions with low/absent elastic strain |
| Yolk sac tumors | testicular swelling, pain, lumbar pain; palpable firm testicular mass |
Can be positive -FP (not always) |
Heterogeneous lesions with anechoic areas | Hypervascularized | Hyperenhanced | Hard lesions with low/absent elastic strain |
| Mixed | testicular swelling, pain, lumbar pain; palpable firm testicular mass; possible gynecomastia |
Can be positive -FP, -hCG, LDH (not always) |
Different aspect in regard to main histological component | Hypervascularized | Homogeneously/ inhomogeneously hyperenhanced |
Hard lesions with low/absent elastic strain |
| Burned-out tumor | lumbar pain, vomit; possible gynecomastia |
Can be positive -FP, -hCG, LDH (not always) |
No testicular nodule; highly echogenic foci or gross calcifications/ hypoechoic irregular areas | Hypovascularized | Unenhanced | / |
| Lymphoma | testicular swelling, pain, and specific lymphoma symptoms; affects men older than 50 years, palpable firm testicular mass |
Negative | Hypoechoic lesions with diffuse infiltration or multifocal hypoechoic lesions of various size | Hypervascularized with linear non-branching pattern | Hyperenhanced | Hard lesions with low/absent elastic strain |
| Leukaemia | More frequent in children and young patients; it can be asymptomatic | Negative | Infiltrating pattern with irregular hypoechoic longitudinal striae/ focal pattern with irregular hypoechoic nodules | Hypervascularized | Inhomogeneously hyperenhanced |
Hard lesions with low/absent elastic strain |
Abbreviations: GSUS, grey scale ultrasound; CDUS, color Doppler ultrasound; CEUS, contrast-enhanced ultrasound; SE, sonoelastography.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



