
Submitted:
19 September 2023
Posted:
21 September 2023
You are already at the latest version
Abstract
The violence against women is a theme that extrapolates health issues, since after a victim seek for a health care, there is the notification of the act [1]. In Brazil, many times, these women are first assisted by mobile urgency services (SAMU/SIATE) and, as far as we have concern, there are no other studies with specific data about these assistance. The present paper aimed to analyze SAMU/SIATE assistance to abused women. Qualitative and retrospective epidemiological study of assistance to assaulted women carried out by SIATE and SAMU Maringá/Norte Novo between 2011 and 2020. Women between 20 and 39 years old, non-pregnant, were the main victims, and 19,52% of them have used some kind of drug. The (ex)partner figured as the perpetrator in 17,35%, but there were no information about this variable in 73,75% of the records. The Qui-square test shows a mortality rate superior to 70% among the severe traumatized victims. This is one of the first studies to analyze this kind of care provided by SAMU/SIATE, and reveals some gaps in its “modus-operandi” that can limitate an extrapolation of the results to bigger spheres. More researches in mobile urgency care services, in other provinces also, are needed to propose strategies to fight against this epidemic.
Keywords:
Violence against women
; Feminicide
; Pre-Hospital Emergency Care
1. Introduction
The violence against the woman is a health menace that can be considered as a silent global epidemics, in which one in three women all around the world suffers violence, affecting 641 million of them [2]. It´s called gender based violence (GBV) any act of violence against a woman causing physical, psychological and sexual affliction, as well as threats or deprivation of liberty, and encompasses a series of forms of violence that affects women and girls, including child abuse, sexual violence, domestic violence, in addition to its most serious and extreme form, the feminicide. The aggression or violence by intimate partner (IPV) is the most common form of GBV [3].
Several studies indicate that the most common modality of violence suffered by women around the world is psychological, followed by physical and sexual violence [4,5,6,7].
In the Americas and Caribbean, prevalences range from 1% in Canada to 27% in Bolivia [8], corroborating the prevalence estimate of 29,8% made by the World Health Organization [2].
In Brazil, approximately 43% of women do not feel completely respected by their partners [9]. Brazil is one of the countries where women are most killed. According to data from the United Nations Economic Commission for Latin America and Caribbean [10], 40% of all female homicide in both regions occur in Brazil, which ranks the country in 5th place for femicides among 84 countries in the world [11].
Despite the existence of mechanisms that aims to curb gender violence, the overall incidence of crimes against women and femicides, increases every year in Brazil [12]. Since 2003 the violence against women became an item of compulsory notification (Act n° 10.778/2003), other important measures to fight against and prevent this crime are the Maria da Penha Act (Act n° 11.340/2006) and the Act nº 13.104/2015, also known as the Feminicide Act, which toughened the penalty for this crime [13].
The World Health Organization established as “One of the Millennium Goals” within the 2030 Agenda, to end with all kinds of discrimination over all women and girls in the world. However, efforts are still needed around the world to implement actions that intensify non-discrimination in employment, gender equality in public life, gender equality in marriage and in family, stricter laws and elimination of all forms of violence in public and private spheres, including trafficking and sexual exploitation [14].
The theme of violence against women is gaining greater relevance, which is revealed in increasingly frequent discussions to understand their circumstances, whether through journalistic, legal and/or political discourse, or even in the domestic sphere in conversations between relatives and friends [15,16,17]. To understand the numbers of violence in a given region can facilitate the insertion of new public policies and actions that will curb acts of violence, thus reducing the disastrous incidence of feminicides.
Violence against women is a problem that goes beyond the health sphere, since after the victim seeks care at a health service, the act is reported [18]. In Brazil, these services are often provided by mobile emergency services (SAMU/SIATE) and, as far as we know, there are no studies with specific data on the assistances provided to women victims of aggression, carried out by these mobile services. In view of the above, this study aimed to analyze cases of aggression suffered by women, treated in mobile emergency services (SAMU/SIATE).
2. Materials and Methods
Qualitative, observational and retrospective epidemiological study of cases of aggression against women, carried out by the Emergency Care Service (SIATE and SAMU Maringá and Norte Novo), between 2011 and 2020. The study was developed in the municipality of Maringá, located in the southern region of Brazil, it is the third most populous city in the State of Paraná, with an estimated population of 436,472 inhabitants [19], which is constituted mainly of whites (71% of the population), followed by mixed races (22%), asians (4%), blacks (3%) and less than 1% indigenous [20].
2.1. Data Source
Data collection was carried out from September 2020 to August 2021, at the SAMU Norte Novo regulation center, directly from physical files of the Medical Care Records and Nursing Care Records (Portuguese Acronyms: RAM/RAE) of the Advanced Mobile Support Unities and the Basic Mobile Support Unities registries of assistance.
All incidents identified as aggression and female victims were included, and the information was compiled using Microsoft Excel® spreadsheets. To homogenize the information and minimize bias, all records were integrally read and analyzed individually by the researcher.
2.2. Variables
We analysed the following: age of the victims, aggressor, pregnancy, trauma severity, drug use and death. Each of these independent variables were then correlated with the common variable: Aggression.
2.3. Data Evaluation and Statistical Analysis
The individual analysis of the variables was subjected to descriptive statistics and represented graphically. Based on the indicators of the locations where the attacks occurred, grouped by neighborhood and municipality, heat graphs were generated, pointing to the regions with the highest records of violence. All the analysis were performed with the aid of the statistical environment R (R Development Core Team), version 3.5 [21], adopting a 5% level of significance (p value < 0.05).
The types of aggression were characterized according to the International Classification of Diseases (ICD-10), using the codes Y09 (Unspecified Aggression), X93 (Assault by Handgun Discharge), X99 (Assault by Sharp Object), and T74.2 (Sexual Abuse). Due to the low number of observations within each category, the results generated by the regression were not significant, and therefore these variables were regrouped in a dichotomous way, creating an indicator variable named "Nature of aggression" that includes:
Nature of aggression: "Non Specified" (n= 332);
Nature of aggression: “Specified" (n= 129).
Assaults of a specified nature included codes X93, X99 and T74.2. The other categories of physical aggression, as they did not have specific coding (ICD-10), were considered of an unspecified nature (code Y09). With that, it was possible to make use of the Binomial family logistic regression model, increasing its predictive capacity.
The equation for the applied logistic regression model is written as:
where are the regression coefficients and are the explanatory variables.
2.4. Ethical Aspects
The State University of Maringá Ethics Committee Involving Human Beings, protocol No. 3.071.844, approved this project.
3. Results
Data on violence, whether regional, municipal, national or international, must be analyzed in order to understand its causes, the risks associated to the act, the victim, and the aggressor. Urgengy and emergency services are qualified to do this type of assistance. Between 2011 and December 31, 2020, SIATE and SAMU Norte Novo recorded 461 incidents of aggression against women.
3.1. Sample characteristics
The age group with the highest occurrence ranged between 20 and 39 years old, with a median of 31 years old, gradually decreasing from then on, until reaching a maximum age of 87 years old. It was found that 5.21% of the victims were pregnant, 78.52% were not pregnant, and 16.27% of the records did not contain information on this issue
Regarding drug use, 19.52% of women used some type of drug, with alcohol being the most common, the other 80.48% did not declare this information. Records with information on the use of illicit drugs or a combination of alcohol + illicit drugs were grouped into the use of “illicit drugs” with 2.6% of use of other drugs, without mentioning alcohol.
Physical aggression covers all (100%) of the events, being the only variable common to all records. In correlating the nature of physical aggression (dichotomous distribution) with the other variables, the most common was the “Non Specified” (NS Aggression), with 72.02% of cases. Among the Specified attacks, 11.5% were stab wounds (SW), 10.2% were firearm injuries (FAI) and 4.56% were victims of sexual violence (SV) (Table 1).
In the association of the severity of trauma with the outcome “Death” among victims who suffered trauma considered severe measured by the GCS (Glasgow Coma Scale), 71.0% died. The application of the chi-square test indicates the dependence between this variables, which means that the severity of the injury caused by the aggressor impacts directly on a woman’s death (Table 2). We observed that 10.24% of victims refused referral after assistance from SAMU professionals and 4.52% of records do not mention referrals. The chi-square test (p = 0) demonstrated dependence between severities and types of referral (Table 3).
In 73.75% of the records there is no information about the aggressor. In 17.35% of cases, the partner (husband/boyfriend) appears as the aggressor, and in lower percentages, other perpetrators appear, such as parents or stepfathers, children, siblings, other family members and acquainteds (Table 4).
The variable day of the week and time of aggression presented a percentage of 58.14% of aggressions occurring between Monday and Friday (n = 268), with a higher prevalence at night (39.7%). Then, the dawn and afternoon periods presented a very similar distribution of occurrences, around 23.4% each. In the morning there were fewer cases attended, comprising 13.45% of records, but there is still a high incidence (n = 62).
We observed that the type of aggressor, severity of the injury and death have a statistically significant association with the nature of the aggression. The aggressors are mostly (ex)partners and family members, and committed violence by unspecified means, which resulted in less severe injuries. The most serious injuries, including those resulting in death, resulted from injuries caused by firearms and bladed weapons. In this study there was no significant correlation between the variables pregnancy and drug use, and the nature of the attacks.
In the correlation regression model between the found nature of the attacks (dichotomous distribution) and their incidence in different locations and different age groups, we did not find significant values. Geographic location also did not influence the nature of the attacks.
The severity of the aggression was measured using the Glasgow Coma Scale (GCS) found on the care forms. Mild traumas (GCS between 13 and 15) were the vast majority (91.11%) and severe traumas (GCS between 3 and 8) accounted for 6.72% of cases. Traumas considered moderate (ECG between 9 and 12) correspond to 0.43%, and 1.74% (n= 8) of records do not have information on severity, according to the GCS.
3.2. Spatial distribution
Heat maps were generated in order to facilitate visual understanding of the geographic points of occurrences. For its construction, the addresses contained in the RAS and RAM/RAE were used, which originated the coordinates from the neighborhood where the aggression was recorded.
The first heat map illustrates all cases in the period analyzed in Maringá and region:
Map 1.
Aggressions against women between 2011 and 2020. Maringá, Pr, 2022.
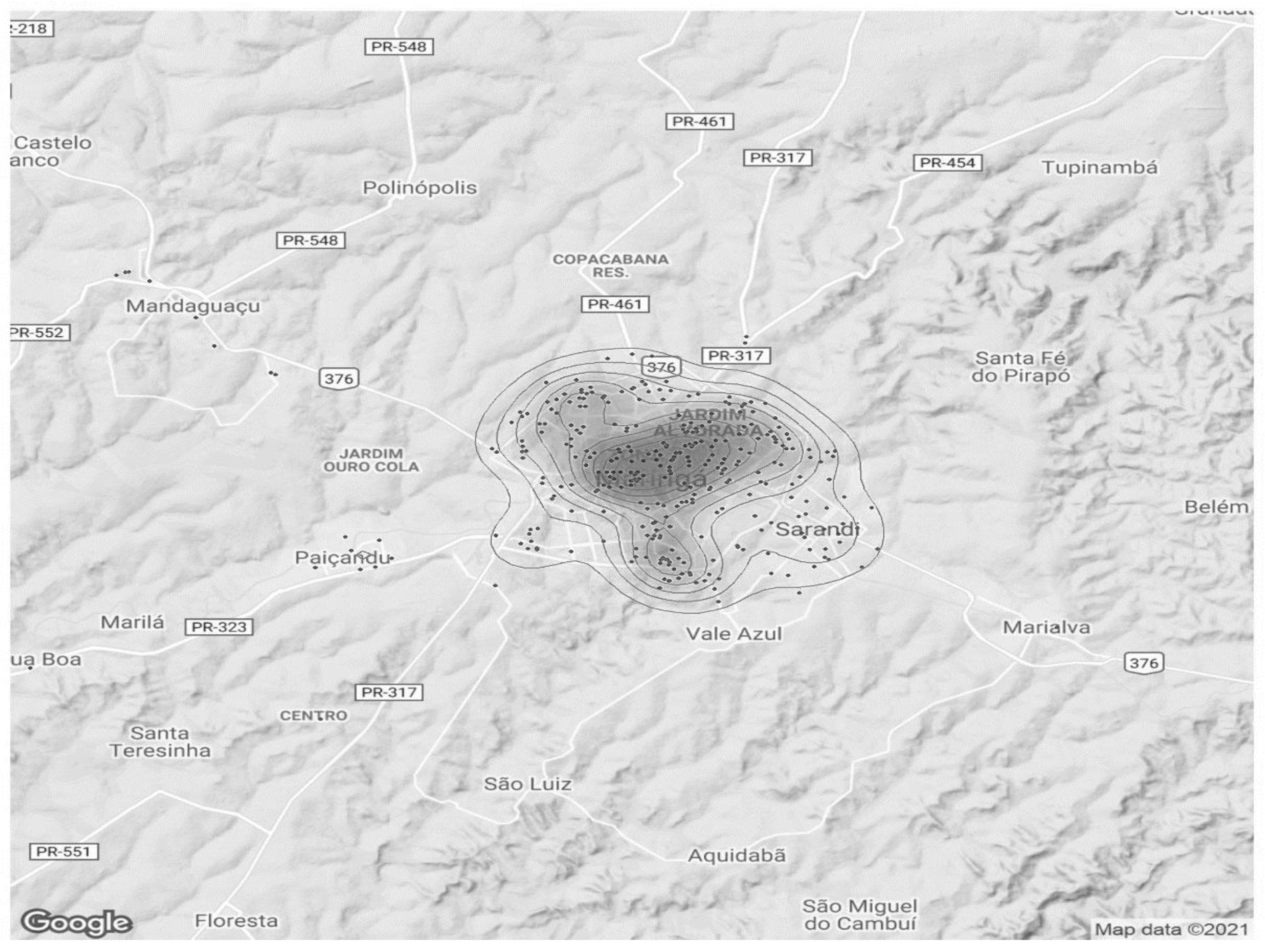
Hot spots are observed located in the central region of the city of Maringá, and some hot spots occurring in neighboring regions.
The second map shows, in more detail, only the Maringá occurrences during the entire study period. There is a large accumulation of cases occurring in central regions of the city and extending across Zone 07 neighborhood, including Av. Morangueira and Jardim Alvorada neighborhood. Some other foci of lesser intensity were found northwest and south of Maringá.
Map 2.
Aggressions against women by neighborhood from 2011 to 2020. Maringá, Pr, 2022.
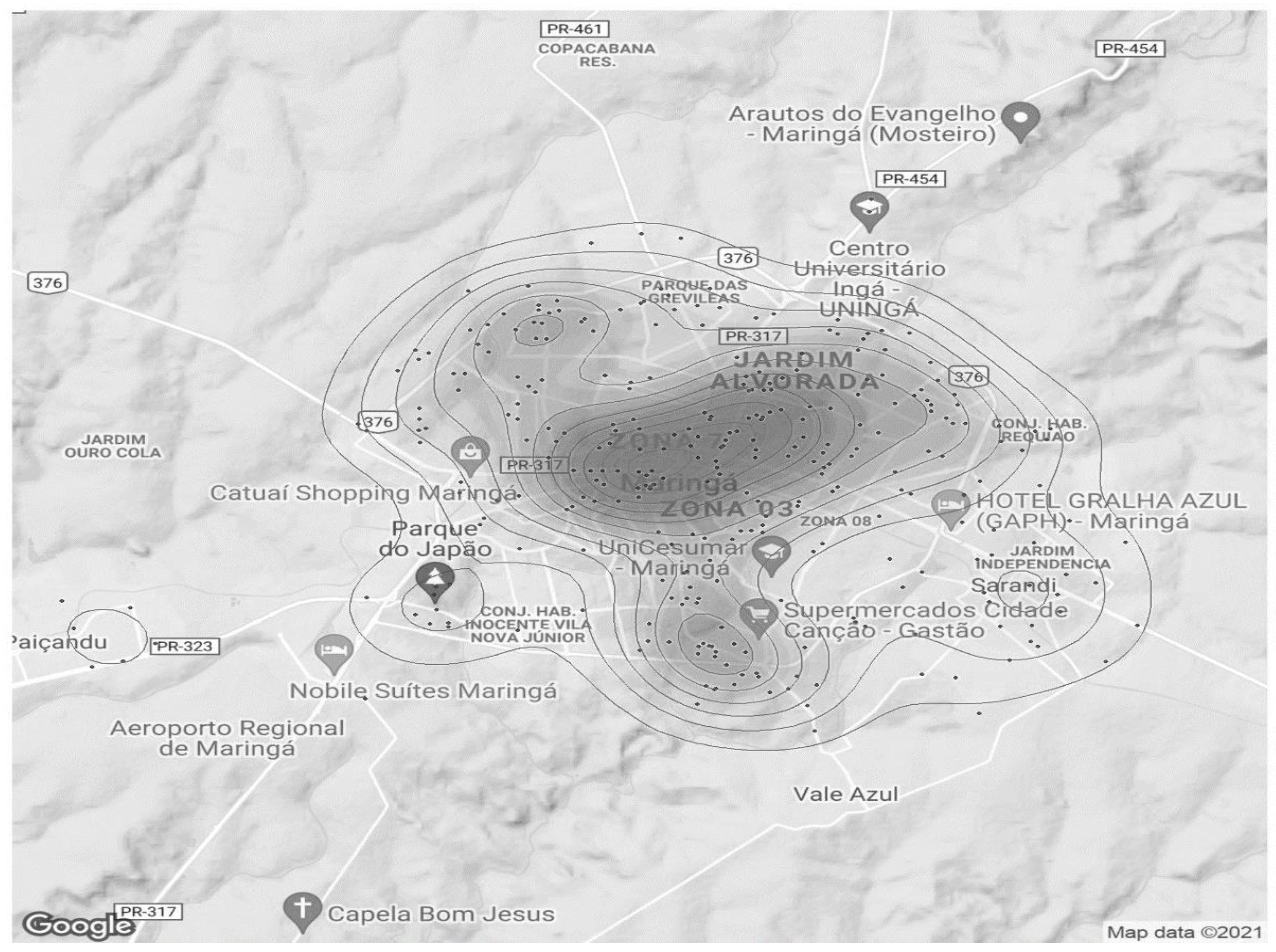
The distribution of incidents of aggression against women proved to be quite heterogeneous, with records in all regions of the municipality. However, throughout the period studied, it is consistently observed that there is a higher prevalence of violent actions against women in the central region, Zone 07 and Jardim Alvorada neighborhoods.
4. Discussion
This is one of the first studies to analyze cases of aggression suffered by women treated in mobile emergency services (SAMU/SIATE). A study carried out in Italy, with data from an Emergency Service during 2017 to 2020, the authors observed an increase in the rate of domestic violence in the first wave of the pandemic [22]. We observed a non significant decrease in records, however, violence is often underreported. Evidences suggests that the COVID-19 outbreak has also reduced the access as well as help-seeking by victims [23,24]. People who needed SAMU’s care are satisfied with its resolutivity, demonstrating the importance of this service for immediate assistance in urgency and emergency cases [25].
Research has demonstrated the importance of investigating variables associated with violence since data from mobile care services, in order to demonstrate epidemiological data as well as enable professionals to carry out good practices and improve access to health services [1]. Professionals who work in the emergency services often face the unpredictability of the act, since in the case of violence there is the woman, the aggressor and the police force, whose training generally does not consider this particularities. A study with health teams in pre-hospital services recognizes that, if these professionals are faced with a case of violence against a woman, they must, first of all, think about physical safety, provide medical care and treatment, demonstrate a sensitive and supportive attitude, keep the records of the findings and report the case [26].
The main reason for assistance was physical and/or sexual aggression. Despite being a silent epidemic, physical violence has several particularities that contribute to its occurrence, such as lack of paid work, abuse of legal and illicit drugs and low education [27]. Despite much discussion, the issue of gender and race are main conditions associated with violence. Black women aged between 20 and 39 are the most affected [28,29]. This study brought important information about women who suffered aggression and whose data are not a part of the system's statistics, since continuity of care does not always occur.
The results show that women aged between 20 and 39 are more exposed to physical aggression. This group represented more than half of the women attacked throughout the period, however, there is no data on the races of the victims. Recently, a study found an even higher prevalence of facial trauma in women victims of GBV in this age group [30].
Concerning the women victims of sexual violence (SV), the majority did not identify the aggressor. Data from DATASUS, however, indicate that the vast majority of perpetrators of sexual crimes are known people or family members, strangers are responsible for approximately 22% of these crimes [31]. This omission may be associated with the fear on delate someone close, reprisal and submission.
Among the abused women who sought care from the mobile service, and who deserve greater attention due to their particularities, are the pregnants. Although this study identified a small percentage, it deserves to be investigated, since its statistics should be zero. Several researchers, however, report prevalence rates of assaulted pregnant women ranging from 1.2% to up to 27.6% in some countries [32]. Violence against pregnant women is an act that not only affects the health of the abused woman, but also the fetus in her womb, which may not be born at all, be born prematurely, and/or have a low birth weight [33].
Among the findings of this study, the use of some type of drug was verified, but there was no correlation between this variable and the severity or nature of the attacks. It is known, however, that the use/abuse of legal and/or illicit drugs, whether by the victim or the aggressor, is another factor that appears associated with the occurrence of violent acts [34,35].
The majority of women were victims of assault by means of physical force/beating (ICD-10: Y09), followed by injuries by means of a cutting or penetrating weapon (ICD-10: X99), firearm shooting (ICD-10 :X93) and sexual violence (ICD-10: T74.2). Women who were victims of burglery were included in the group of assaults involving physical force. The observation of violent acts associated with being a woman is increasingly frequent in our society, a fact that is directly linked to patriarchal cultural aspects. A study comparing the description of intimate partner violence, from the perspective of men and women, shows that men justify their acts of aggression through vague speeches, with euphemisms, often blaming a third part for the inflicted act [36].
An analysis of the profile of IPV cases treated in urgency and emergency services in 25 Brazilian capitals revealed very similar numbers regarding drug use (21.98%), and the prevalence of means of aggression, with 70.9% per means of bodily force/beating and 14.5% for injuries caused by a sharp or penetrating weapon [28]. In this study, however, the prevalence of victims due to firearm shooting was much lower than that found in the Maringá region. Part of this difference can perhaps be explained by the environment analyzed, since in the study of those authors, hospital care was evaluated and, in our study, we evaluated pre-hospital care. We found 47 records of aggression by fire arms, and 33 were referred to a hospital service, the other victims were either sent directly to the Forensic Medicine Institute (FMI), or refused referral.
Considering the severity of the injuries, few women were classified as severe, according to the Glasgow Coma Scale. Tragically, however, a high rate of death was observed among these cases. There were 22 deaths among 31 victims with severe trauma, which represents almost 71% fatality. This percentage surpasses the lethality rate of severe or congestive heart failure, which is 50% in 5 years [37] and, in Brazil, the cardiovascular diseases are the main cause of death [38].
IPV is the most common form of violence against women [2]. The database utilized in this study contains little information about the perpetrators of the attacks and, when present, it was handwritten in the body of the anamnesis text. This lack of information is possibly associated with the health professional approach to the assaulted woman, who did not even ask the victim and/or witnesses this important information. Some factors in the context of emergency care are considered to facilitate failure to register, such as in-depth care of cases, rapid intervention, flow of care, disarticulation with the reference service, frustration in resolving the problem and lack of preparation to approach and deal with the problem [1].
Another relevant variable concerns the period in which the violence occurred. This aggression can occur at any time and in any place. Studies indicate higher prevalence at night and on weekdays [30,39], while others points to weekends as the highest risk days for women [40,41]. In our study, women suffered more aggression at night and less on weekends, yet a considerable number of women suffered physical violence at all times of the day.
The domestic environment, her home, should be a woman's refuge. But IPV in their own home remains the most common form of aggression suffered by women [29,42]. Factors such as low income, low level of education, and living in rural areas are associated with higher prevalence of violence against women [43]. In the present study, the contained information does not detail the locations of the occurrences. But what was noticed through the heat maps was a predominance of services in the urban area, and mainly in the most central regions of the city of Maringá.
Maringá is a city in the southern region of Brazil, with a predominantly urban population (>98%), and with a Human Development Index (HDI) considered very high (0.808) [19]. The database does not include sociodemographic aspects, with evidence of higher prevalence in the most populous and demographically dense regions of the city (central region, Zone 07 and Jardim Alvorada) [19], perhaps it can be considered just a reflection of what occurs in areas with greater population concentration, inserted in an environment whose socioeconomic panorama is relatively homogeneous.
A limitation of the study was the origin of the data, which comes from a secondary database, in which the form of registration in the service records (RAS, RAM/RAE) is subjective. Specifically for cases of aggression against women, we found many gaps of filling the records, basic and essential data to the approach of this type of victim by a health professional were missing, such as the specific location of the incident, the identification of the perpetrator and also the race of the victim, revealing a lack of training for this assistance. However, studies have demonstrated the importance of using official databases as a source of research, change of paradigms and new policies proposal. Further research into mobile care services in other states is suggested in order to propose strategies to combat this epidemic.
5. Conclusions
Society and governments can no longer tolerate acts of violence against women. The consequences of this crime add up to an endless number of evils, with negative repercussions on health, education and the economy, representing an important brake on the evolution of nations, and a cursed inheritance passed down from generation to generation.
Aiming to protect precisely the most exposed population, it is argued that prevention measures against GBV should begin before the first marriage and before the age of 19 [44].
In Brazil, despite the existence of measures and laws to curb and strictly punish this crime, there is a progressive increase in cases. Which portrays a structural problem, rooted in the culture and habits of a patriarchal society. Therefore, the fight against this evil, like many diseases, must focus on prevention, which will involve access to information and changing customs and paradigms since childhood. The seeds of tolerance and the notion of equality, including gender equality, must be planted in elementary education, becoming a formal part of the curriculum.
It was found that the service provided by mobile services (SAMU/SIATE) is insufficient with regards to the capture of data that allows the profile of the victims to be traced, much less the aggressors. This may limit the use of this data as a source of information, especially if the objective is to plan measures, whether prevention or combat.
Therefore, in view of what was observed in this study and, considering not only the importance of mobile assistance services as a damage control instrument, but also their potential in the secondary prevention of these crimes, we propose that SAMU/SIATE adopt adequate training, and the use of a specific assistance form for incidents of aggression against women, with data that allows the identification of risk factors and also the aggressors.
Author Contributions
Conceptualization, Investigation, Methodology, Validation, Writing-original draft, D.M.S. and S.M.P.; Formal analysis, Project administration, Supervision, Writing-review and editing, D.M.S., M.D.B.C and S.M.P.; Resources, Data curation, D.M.S., M.P.S., M.D.B.C and S.M.P.; Funding acquisition, D.M.S. and S.M.P.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this review. Data sharing does not apply to this article
Acknowledgments
This work was carried out with the support of the Coordination for the Improvement of Higher Education Personnel - Brazil (Capes) – Financing Code – 00.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Avanci, J.Q.; Pinto, L.W.; de Assis, S.G. Atendimento dos casos de violência em serviços de urgência e emergência Brasileiros com foco nas relações intrafamiliares e nos ciclos de vida. Cienc e Saude Coletiva. 2017, 22, 2825–40. [Google Scholar] [CrossRef] [PubMed]
- WHO Violence Against Women [Internet]. March, 9. 2021 [cited 2021 Nov 28]. Available from: https://www.who.int/news-room/fact-sheets/detail/violence-against-women.
- OMS 2013. Global and regional estimates of violence against women: prevalence and health effects of intimate partner violence and non-partner sexual violence. OMS. 2013.
- Thompson RS, Bonomi AE, Anderson M, Reid RJ, Dimer JA, Carrell D, et al. Intimate Partner Violence. Prevalence, Types, and Chronicity in Adult Women. Am J Prev Med. 2006, 30, 447–57. [Google Scholar] [CrossRef]
- Breiding, M.J.; Smith, S.G.; Basile, K.C.; Walters, M.L.; Chen, J.; Merrick, M.T. Prevalence and characteristics of sexual violence, stalking, and intimate partner violence victimization - national intimate partner and sexual violence survey, united states, 2011. MMWR Surveill Summ. 2014, 63, 1–18. [Google Scholar] [PubMed]
- Marabotti, F.; Leite, C.; Helena, M.; Amorim, C.; Iii, F.C.W. Violence against women , Espírito Santo , Brazil. 2017, 1–12.
- Kwaramba T, Ye JJ, Elahi C, Lunyera J, Oliveira AC, Calvo PRS, et al. Lifetime prevalence of intimate partner violence against women in an urban Brazilian city: A cross-sectional survey. PLoS One. 2019, 14, 1–13. [Google Scholar]
- Bott, S.; Guedes, A.; Ruiz-Celis, A.P.; Mendoza, J.A. Intimate partner violence in the Americas: a systematic review and reanalysis of national prevalence estimates. Rev Panam Salud Publica/Pan Am J Public Heal. 2021, 45, 1–12. [Google Scholar]
- Souza MB, Silva S, Abreu GS De. Artigo de Revisão Violência Doméstica entre Parceiros Íntimos : Questões Culturais e Sociais acerca dos Homens Autores de Violência Domestic Violence among Intimate Partners : Cultural and Social Issues About Men Who Commit Violence. 2016, 388–407.
- ECLAC. ECLAC: At least 4.091 Women Were Victims of Femicide in 2020 in Latin America and the Caribbean, Despite Greater Visibility and Social Condemnation [Internet]. cepal.org. 2021 [cited 2021 Nov 29]. Available from: https://www.cepal.org/en/pressreleases/eclac-least-4091-women-were-victims-femicide-2020-latin-america-and-caribbean-despite.
- Waiselfisz, J.J. Mapa Da Violência 2015 - Preliminar. MAPA DA VIOLÊNCIA 2015 Adolesc 16 e 17 anos do Bras. 2015, 1, 72. [Google Scholar]
- Cerqueira, D.; Lima RSDe Silva, E.R.A.; Pimentel, A.; Marques, D. ATLAS DA VIOLÊNCIA 2020. 2020.
- Messias, E.R.; do Carmo, V.M.; de Almeida, V.M. Femicide: An Analysis from the Perspective of The Human Person’s Dignity. Rev Estud Fem. 2020, 28, 1–14. [Google Scholar]
- ONU The sustainable development goals report 2019. United Nations Publ issued by Dep Econ Soc Aff [Internet]. 2019, 64. Available from: https://unstats.un.org/sdgs/report/2019/The-Sustainable-Development-Goals-Report-2019_Spanish.pdf%0Ahttps://undocs.org/E/2019/68. 2019.
- Meneghel, S.N.; Portella, A.P. Feminicídios: Conceitos, tipos e cenários. Cienc e Saude Coletiva. 2017, 22, 3077–86. [Google Scholar]
- ROSAM da, F.L.O.R.E.S.I.G. A double-smashed body : ( in ) visibility of femicide victims in newspaper headlines. 2020, (September):147–68.
- Martins-Filho PRS, Mendes MLT, Reinheimer DM, do Nascimento-Júnior EM, Vaez AC, Santos VS, et al. Femicide trends in Brazil: relationship between public interest and mortality rates. Arch Womens Ment Health. 2018, 21, 579–82. [Google Scholar] [CrossRef]
- Chisholm CA, Bullock L, Ferguson JE (Jef. Intimate partner violence and pregnancy: epidemiology and impact. Am J Obstet Gynecol [Internet]. 2017, 217, 141–4. [Google Scholar] [CrossRef]
- IBGE No Title [Internet]. 2021 [cited 2021 Nov 29]. Available from: https://cidades.ibge.gov.br/brasil/pr/maringa/panorama.
- IBGE Censo Brasileiro de 2010. 2012. 2012.
- R Development Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing. 2015.
- Delaidelli, G.; Georgiu, A. Domestic violence in Val Camonica: survey on the accesses to the emergency deparment in the period post Covid-19. Assist Inferm e Ric. 2021, 40, 87–91. [Google Scholar]
- Fraser, E. Impact of Covid-19 Pandemic on Violence Against Women and Girls [Internet]. VAWG Helpdesk Research Report No 284. 2020. Available from: http://www.sddirect.org.uk/media/1881/vawg-helpdesk-284-covid-19-and-vawg.pdf.
- Kaukinen, C. When Stay-at-Home Orders Leave Victims Unsafe at Home: Exploring the Risk and Consequences of Intimate Partner Violence during the COVID-19 Pandemic. Am J Crim Justice. 2020, 45, 668–79. [Google Scholar] [CrossRef]
- Battisti, G.R.; Branco, A.; Caregnato, R.C.A.; De Oliveira, M.M.C. Profile of service and satisfaction of users of the Mobile Emergency Care Service (SAMU). Rev Gauch Enferm. 2019, 40, 1–8. [Google Scholar]
- Gümüşsoy, S.; Dönmez, S.; Ekşi, A.; Dal, N.A. Relationship of knowledge about and attitudes towards violence with recognition of violence against women among health staff in pre-hospital emergency medical services. Int Emerg Nurs. 2021; 56. [Google Scholar]
- Leite, F.M.C.; Luis, M.A.; Amorim, M.H.C.; Maciel, E.L.N.; Gigante, D.P. Violence against women and its association with the intimate partner’s profile: A study with primary care users. Rev Bras Epidemiol. 2019, 22. [Google Scholar]
- Garcia, L.P.; da Silva, G.D.M. Violência por parceiro íntimo: Perfil dos atendimentos em serviços de urgência e emergência nas capitais dos estados brasileiros, 2014. Cad Saude Publica. 2018, 34. [Google Scholar]
- Mascarenhas, M.D.M.; Tomaz, G.R.; de Meneses, G.M.S.; Rodrigues, M.T.P.; Pereira VO de, M.; Corassa, R.B. Analysis of notifications of intimate partner violence against women, Brazil, 2011-2017. Rev Bras Epidemiol. 2020, 23, 1–13. [Google Scholar]
- Mayrink G, Araújo S, Kindely L, Marano R, Filho AB de M, de Assis TV, et al. Factors Associated With Violence Against Women and Facial Trauma of a Representative Sample of the Brazilian Population: Results of a Retrospective Study. Craniomaxillofac Trauma Reconstr. 2021, 14, 119–25. [Google Scholar]
- Onça, J.S.; Silva, D.A. Violência Sexual No Brasil : Perfil Epidemiológico ( 2009-2017 ). 2017,.
- Cavalin C, Garcia-Moreno C, Jansen HAFM, Ellsberg M, Heise L, Watts C. WHO Multi-country Study on Women’s Health and Domestic Violence against Women. Initial Results on Prevalence, Health Outcomes and Women’s Responses. 2010, (May 2014).
- Hill, A.; Pallitto, C.; McCleary-Sills, J.; Garcia-Moreno, C. A systematic review and meta-analysis of intimate partner violence during pregnancy and selected birth outcomes. Int J Gynecol Obstet. 2016, 133, 269–76. [Google Scholar] [CrossRef]
- Xavier Hall, C.D.; Evans, D.P. Social comorbidities? A qualitative study mapping syndemic theory onto gender-based violence and co-occurring social phenomena among Brazilian women. BMC Public Health. 2020, 20, 1–12. [Google Scholar]
- Ally EZ, Laranjeira R, Viana MC, Pinsky I, Caetano R, Mitsuhiro S, et al. Intimate partner violence trends in Brazil: Data from two waves of the Brazilian National Alcohol and Drugs Survey. Rev Bras Psiquiatr. 2016, 38, 98–105. [Google Scholar]
- Rodriguez, J.; Burge, S.K.; Becho, J.; Katerndahl, D.A.; Wood, R.C.; Ferrer, R.L. He Said, She Said_ Comparing Men’s and Women’s Descriptions of Men’s Partner Violence. J Interpers Violence. 2021, 36, NP11695–716. [Google Scholar] [CrossRef] [PubMed]
- Rohde LEP, Montera MW, Bocchi EA, Clausell NO, de Albuquerque DC, Rassi S, et al. Diretriz brasileira de insuficiência cardíaca crônica e aguda. Arq Bras Cardiol. 2018, 111, 436–539. [Google Scholar]
- Silva Jr. JB da, Ramalho WM. Cenário epidemiológico do Brasil em 2033: uma prospecção sobre as próximas duas décadas. Brasil Saúde Amanhã: dimensões para o planejamento da atenção à saúde. 2017. 31–62 p.
- Orellana, J.D.Y.; Da Cunha, G.M.; Marrero, L.; Horta, B.L.; Da Costa Leite, I. Urban violence and risk factors for femicide in the Brazilian Amazon. Cad Saude Publica. 2019, 35, 1–13. [Google Scholar]
- DAVIDLMV; MINAMISAVAR; VITORINOPV de, O.; ROCHAMJP; CARNEIROVSM; VIEIRAMA da, S. Perfil dos óbitos femininos por homicídios no município de Goiânia. 2020, 73(Suppl 4), 1–7.
- Garcia, L.P.; Freitas LRS de Höfelmann, D.A. Avaliação do impacto da Lei Maria da Penha sobre a mortalidade de mulheres por agressões no Brasil, 2001-2011. Epidemiol e Serviços Saúde. 2013, 22, 383–94. [Google Scholar] [CrossRef]
- Costa MS, Serafim MLF, Nascimento ARS do. Violência contra a mulher: descrição das denúncias em um Centro de Referência de Atendimento à Mulher de Cajazeiras, Paraíba, 2010 a 2012. Epidemiol e Serviços Saúde. 2015, 24, 558–551. [Google Scholar] [CrossRef]
- HENRICAAF; GARDNERJ; JUBEROM; LIANGM; DIOUFT Prevalence Rates , Trends and Disparities in Intimate Partner Violence : POWER OF DATA IN THE. 2021.
- Peterman, A.; Bleck, J.; Palermo, T. Age and intimate partner violence: An analysis of global trends among women experiencing victimization in 30 developing countries. J Adolesc Heal. 2015, 57, 624–30. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Characterization and description of victims treated by the Mobile Emergency Service. Maringá, PR, 2022.
Table 1.
Characterization and description of victims treated by the Mobile Emergency Service. Maringá, PR, 2022.
| Nature of Aggression | ||||||
| Non Specified (N = 332) | Specified (N = 129) | |||||
| Variable | n | % | n | % | p-value(X²) | Odds Ratio |
| Agressor | ||||||
| Partner | 75 | 22,59% | 5 | 3,88% | <0,0001 | 7,24 |
| Acquainted | 6 | 1,81% | 0 | 0,00% | Inf | |
| Ex-Partner | 4 | 1,20% | 1 | 0,78% | 1,56 | |
| Family Member | 27 | 8,13% | 3 | 2,33% | 3,72 | |
| Uninformed | 220 | 66,27% | 120 | 93,01% | 0,15 | |
| Pregnancy | ||||||
| No | 255 | 76,81% | 107 | 82,95% | 0,077 | 0,68 |
| Uninformed | 55 | 16,57% | 20 | 15,50% | 1,08 | |
| Yes | 22 | 6,63% | 2 | 1,55% | 4,51 | |
| Severity | ||||||
| Severe | 7 | 2,1% | 24 | 18,6% | <0,0001 | 0,09 |
| Mild | 319 | 96,09% | 101 | 78,3% | 8,42 | |
| Moderate | 2 | 0,61% | 0 | 0,00% | Inf | |
| Uninformed | 4 | 1,2% | 4 | 3,1% | Inf | |
| Age | ||||||
| <20 | 46 | 13,86% | 26 | 20,15% | 0,26 | 0,63 |
| >60 | 19 | 5,72% | 4 | 3,1% | 1,87 | |
| 20 a 39 | 178 | 53,61% | 67 | 51,94% | 1,06 | |
| 40 a 59 | 89 | 26,81% | 32 | 24,81% | 1,14 | |
| Death | ||||||
| No | 329 | 99,10% | 110 | 85,27% | <0,0001 | 18,94 |
| Yes | 3 | 0,90% | 19 | 14,73% | 0,05 | |
| Drug Use | ||||||
| Ilicit drugs | 9 | 2,71% | 5 | 3,88% | 0,074 | 0,69 |
| Licit drugs | 54 | 16,27% | 10 | 7,75% | 2,31 | |
| Uninformed | 259 | 78,01% | 112 | 86,82% | 0,54 | |
| Others | 10 | 3,01% | 2 | 1,55% | 1,97 | |
Table 2.
Deaths based on the severity of the injury.
| Severity | Death | Amount | Percentual |
| Severe | No | 9 | 29.03% |
| Severe | Yes | 22 | 70.97% |
| Mild | No | 420 | 100% |
| Moderate | No | 2 | 100% |
Table 3.
Referral based on the severity of the injury.
| Severity | Referral | Amount | Percentual |
| Severe | Medical referral | 9 | 29.03% |
| Severe | Forensic Medicine Institute (FMI) | 22 | 70.97% |
| Mild | Medical referral | 358 | 85.24% |
| Mild | Uninformed | 19 | 4.52% |
| Mild | Refused referral | 43 | 10.24% |
| Moderate | Medical referral | 2 | 100% |
Table 4.
Aggressor identity.
| Amount | Percentual | ||
| Partner | 80 | 17.35% | |
| Acquainted | 6 | 1.3% | |
| Ex-Partner | 5 | 1.08% | |
| Family member | 30 | 6.51% | |
| Uninformed | 340 | 73.75% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



