
Submitted:
19 September 2023
Posted:
20 September 2023
You are already at the latest version
Abstract
This paper reviews the appearance of joint lesions during arthroscopic surgery of inter-est to the arthroscopic surgeon and their interpretation within the continuum of joint disease. It also points out the relevance of surgical findings as well as giving directions to the surgeon as to how to approach an appropriate decision-making process during an arthroscopic procedure and what therapeutic options are optimal.
Keywords:
Arthroscopy
; Joint disease
; Surgery
; Sport horses
1. Introduction
To perform arthroscopic surgery, it is essential to have an in-depth knowledge of the anatomy, physiology, pathophysiology and biomechanics of each joint and joint region. Hence, the surgeon must consider these aspects of the joint to be intervened in his intraoperative decision-making. Without this knowledge, it is normal to make errors in judgment that lead to a worse prognosis or, at least, to not maximizing recovery options. Likewise, the surgeon must have at his disposal during the arthroscopic procedure, instrumentation, and operational capacity to perform different interventions that may be decided intra-operatively. Therefore, it is not just a question of knowing how to perform the technique and having the equipment, but of having sufficient knowledge for appropriate decision-making in each situation. In the absence of such knowledge, arthroscopic surgery becomes an act of technical nature rather than a procedure based on science.
Surgeons often find joint injuries that, if not completely unexpected, at least their severity may be. This is because there are currently no reliable methods for precisely evaluating articular cartilage, despite research about its evaluation using different methods such as MRI [1]. The thin nature of the cartilage together with the lack of adequate resolution of most MRI systems used in horses, preclude such evaluation. On some occasions, the use of contrast studies can offer additional information [2], but it is not until the surgeon looks at the joint directly through the arthroscope, when a concrete evaluation of the state of the joint is made.
During joint evaluation, instant decision-making challenges may be presented to the surgeon who must know how to respond to the different degrees and types of pathology.
2. Injuries and physiology of joint healing
A joint is a complex system made up of different tissues with different functional capacities, orchestrated and tuned to facilitate movement with minimal effort [3]. Any alteration of the articular tissues may potentially lead to a reduction in performance, either due to restriction of range of motion or due to pain. When these alterations are of significant magnitude that can affect the performance of the horse, present or future, and there are no medical options that guarantee a good result, a surgical intervention is necessary to try to solve the problem and to give the horse the best opportunities for rehabilitation. Alternatively, arthroscopy may be performed in sound horses to avoid further problems, a situation that is much less tolerant to complications. During surgical intervention it is necessary to be able to respond to an unexpected lesion from a technical and equipment point of view.
Primary synovial inflammation or synovitis is routinely treated by intraarticular administration of therapeutic agents and exercise management. However, damage to the articular cartilage surface, joint instability or damage to intra-articular ligaments or menisci generally requires surgical intervention via arthroscopy.
During arthroscopic surgery the surgeon must evaluate the state of the joint in an expeditious and yet thorough manner. The decision-making process will be related to the amount, severity, and location of the pathology. Of consideration is that all joints have a percentage of articular surface impossible to assess and/or intervene and therefore pre-operative planning is critical. On some occasions, these non-accessible areas are also those of greatest interest, since they are where the greatest compressive loads are produced and that tend to present pathologies that are difficult to visualize and sometimes impossible to intervene [4]. Such is the case of almost 40% of the articular surface of the fetlock, specifically the area of the transverse ridge, where many injuries occur, especially in racehorses and which is inaccessible to the surgeon [4].
The arthroscopic approach and anatomy for most joints in the body has been detailed and as of recently even arthroscopy of the intervertebral joints of the cervical spine has been published [5,6].
When evaluating the cartilage, the surgeon must be able to assess all the possible manifestations of articular pathology. Osteoarthrosis evolves from an early inflammatory process that, if uncared for, progresses to a degenerative one through a continuum of well described pathological changes [7]. These lesions progress from an early-stage synovitis characterized by hyperplasia, hyperemia, and hypertrophy of the synovial membrane. One of the earliest changes occurring in the cartilage surface is discoloration and loss of shining (Figure 1) which heralds the initiation of degeneration. This is followed by “swelling” and softening of cartilage (Figure 2), sensed by the surgeon by using a palpator (Figure 3) which marks the initial loss of collagen network [7].
As the disease advances, the surgeon will observe surface fibrillation (Figure 4), partial thickness erosions (Figure 5), and full thickness erosions (Figure 6) in that order [7].
Osteophytes can be seen along the mid-to late-stage process, and these should have been seen on radiographs during pre-operative evaluation. Removal of osteophytes is only indicated when they are interfering with the joint range of motion or are irritating the joint capsule. In the radio-carpal, mid-carpal, temporomandibular and femorotibial joints, the surgeon will also evaluate the state of intraarticular ligaments (Figure 7) and meniscus (Figure 8).
Damage to these structures has different clinical consequences and is manifested by their fibrillation and rupture identified by loss of integrity and anatomical disruption (Figure 9).
Damage to the meniscus of the temporomandibular joint can be well tolerated while meniscal damage in the femorotibial joint has a prognosis that ranges from good to poor [8,9]. Similarly, damage to intraarticular ligaments is related to its severity and location with desmitis of the transverse carpal and meniscotibial ligaments being usually better tolerated than damage to cruciate ligaments in the femorotibial joint. As a rule, any ligament damage that produces significant instability will trigger a rapidly evolving degenerative process [10].
3. Decision making process
When faced with different pathologies the surgeon must make appropriate decisions to optimize the outcome of the horse. It is important to know that all attempts to produce cartilage regeneration have so far failed, resulting in cartilage repair of different qualities, but not regeneration at a histological level. Along these lines, healing refers to the restoration of the structural and functional integrity of tissue after injury or disease, but repair generally has a narrower meaning. Repair refers to the replacement of damaged or lost cells and matrix with new cells and matrix, a process that does not necessarily mean restoring the original structure or function of a tissue. Regeneration can be considered a special form of repair in which cells replace lost or damaged tissue with tissue identical to the original [11,12].
Articular cartilage can be damaged either traumatically or degenerative. Regardless, the surgeon must always consider that whatever the repair process, such newly formed tissue, usually fibrocartilage will be of inferior biomechanical resilience and eventually more prone to develop degeneration leading to further disruption of joint homeostasis [12]. Therefore, both mechanisms of cartilage degeneration will eventually progress to irreversible osteoarthrosis leading to exercise-related pain, inflammation, and decreased joint range of motion [13].
The surgeon must understand the cartilage repair mechanisms to modulate them to optimize the final outcome. Once damaged, articular cartilage undergoes a repair process based on three mechanisms:
- Intrinsic repair: relies on the limited mitotic capacity of chondrocytes and a somewhat ineffective increase in collagen and proteoglycan production.
- Extrinsic repair: it comes from mesenchymal elements of the subchondral bone that participate in the formation of new connective tissue that can undergo some metaplastic change to form cartilage elements. For it to exist, there must be a method by which blood reaches the subchondral bone to the articular surface, generally through a technique known as microfracture.
Generally, there is a critical size of the lesion depending on the joint (4 mm in the carpus, 9 mm in the stifle), where larger lesions cannot re-establish repair tissue in optimal conditions, so a focal zone of degeneration (osteoarthritis) remains [15,16,17]. Larger defects have been shown to be less likely to heal. A study distinguished between large (15 mm2 ) and small (5 mm2 ) full-thickness lesions in the weight-bearing and non-weight-bearing areas of the radiocarpal, intercarpal, and patellofemoral joints [15]. After 1 month, the small defects were filled with poorly organized fibrovascular repair tissue; at 4 months, the repair was limited to an increase in the amount of organization of this fibrous tissue, and at 5 months, the small radiocarpal and patellofemoral lesions were barely detectable due to combinations of matrix flow and extrinsic repair mechanisms. Large lesions showed good initial repair, but perilesional and intralesional subchondral clefts developed at 5 months [15]. This is the reason why any study or case in which an intervention is made must have a minimum of 8 months of follow-up because the initial improvement followed by a subsequent deterioration is a constant in studies and clinical documentation.
The depth of the injury also determines the cartilage's ability to heal. With partial thickness defects, a certain amount of repair is produced, characterized by an increase in the synthesizing capacity of joint tissues, translated into an increase in GAG's ( glycosaminoglycans ) and collagen. However, the repair process is never completely effective. In humans, for instance complete repair of chondromalacia of the patella has been documented if the articular surface defect is minimal [18]. However more recent work with arthroscopic debridement of partial thickness defects has questioned that any real regeneration occurs [19].
Furthermore, superficial partial thickness defects are not necessarily progressive and although they tend to not healing, they do not necessarily compromise joint function [20]. With full-thickness defects, and depending on the extent, the response of adjacent articular cartilage provides only the limited repair necessary to replace dead cells and damaged matrix at the margins of the defect. These defects are repaired mostly by an extrinsic mechanism characterized by ingrowth of subchondral fibrous tissue, which may or may not undergo metaplasia to fibrocartilage, but never to hyaline cartilage identical to the damaged one [21].
The decision that the surgeon must make is to intervene appropriately in the event of a lesion in relation not only to its size but also to its thickness and location. If the surgeon considers that an attempt to repair a partial thickness lesion is necessary, the lesion should be converted to full thickness and stimulate the body's own repair mechanisms and those mentioned above. However, when making decisions, it must be considered that a partial thickness lesion, although it is never repaired, does not evolve [15,17] if the noxious stimulus that started it is controlled. Therefore, a non-intervention decision may also be appropriate. The presence of a cartilage defect does not have to represent a clinical commitment to intervene and hence the surgeon's judgment when it comes to intervening, preserving the fundamental principle of medicine “ primum non nocere ”. For example, in the equine carpus, loss of up to 30% of the articular surface of an individual bone may not compromise a horse's successful return to racing. However, loss of 50% of the articular surface or severe loss of subchondral bone leads to a significantly worse prognosis [22]. The inadequate healing response may not necessarily apply to immature animals or to non-weight bearing defects since under these conditions the prognostic implications are very different generally being more favorable.
3.1. Decision-making process in different pathological scenarios
3.1.1. Intra-articular fragments and fractures
The presence of one or several intra-articular fragments regardless of their origin, either traumatic or, because of osteochondrosis (OC) (Figure 9), requires their surgical removal in the vast majority of cases. Although the conservative management of certain osteochondral fragments due to OC, such as in the tibiotarsal or metacarpophalangeal joints, has been described and even recommended by some authors, a careful analysis of the literature, as well as the author's opinion, leads to a decision that favors surgical removal of these in those horses where significant athletic activity occurs or will occur [23]. Additionally, and due to the equestrian market reluctancy to accept horses with presence of articular fragmentation in their transactions, the removal of fragments is also favored in young horses, although free of lameness, from 12 months of age onwards, or even younger if they present lameness or in cases with severe detachment of articular cartilage requires of reattachment techniques to preserve the articular surface. In young horses, particularly under one year of age, the surgeon must exercise extreme caution and not cause unnecessary damage during surgical debridement of the fragment, due to the fragility of the immature cartilage at that age. In those situations where the fragment has a traumatic origin, it is necessary to carefully evaluate the situation of the articular cartilage, since the surgeon will frequently find coexisting pathology such as erosions (Figure 6), wear lines (Figure 10) and degenerative changes possibly including the subchondral bone.
Osteochondral fragments of traumatic origin are commonly found in racehorses and those that by virtue of their athletic activity repeatedly load the articular edges, particularly the first phalanx and carpal bones [24].
Another type of intra-articular fragmentation of traumatic origin can also occur, for example in the sesamoids or tibial plateau. Any joint fragment that produces symptoms and/or joint instability must be removed or, in the case of fragments larger than 6 mm and accessible, osteosynthesis may be another option and, depending on the case, even better if the removal of the fragment is associated with post-surgical joint instability due to its size. This is the situation with intra-articular fractures, which require osteosynthesis (Figure 11) and intra-articular evaluation during their fixation to avoid joint incongruity, which is a great promoter of joint degeneration.
Although there is no verified information, it is considered that, like the human species, an incongruity of 2 mm is the maximum tolerated by a joint in order not to suffer a degenerative process [25]. Therefore, high precision and arthroscopic monitoring are required during these procedures. Such is the case of intra-articular condylar fractures of the metacarpal or metatarsus (Figure 12), carpal fractures, fractures of the third phalanx or of the proximal part of the tibia. The objective in these cases is to achieve 100% joint congruence and the surgeon must manipulate the fragments until this is achieved, for which arthroscopic monitoring is essential.
3.1.2. Articular surface restoration
Due to the poor results obtained through natural repair mechanisms, restoration of the articular surface by different techniques has been investigated in the past. These techniques include mosaicplasty, microfracture, use of stem cells and grafts or implants of different types [26].
When the location (in load-bearing areas), the size and depth of the cartilage lesion prevent a repair by one of the three mechanisms mentioned in preceding section, several strategies have been developed, with varying degrees of success, to assist this process. The author recommends caution regarding the extrapolation of data from the human species, because the post-operative management that a horse requires in relation to the use of the affected limb is completely opposite to that used in the human species, since the horse needs immediate support of the operated limb, this being the main obstacle to be managed by the equine surgeon, and the main reason why these techniques have not been satisfactory in horses.
- Mosaicplasty
The initial clinical experiences in horses had sub-optimal results. Subsequently, better results have been documented with this technique, but these have not been replicated by other authors [27].
Arthroscopic mosaic arthroplasty or mosaicplasty is commonly used in human surgery to repair large chondral defects by harvesting osteochondral grafts from non-weight-bearing areas and transplanting them to the affected site. This approach has been experimentally evaluated in the equine radiocarpal, metacarpophalangeal and femoropatellar joints [28]. In one study, three osteochondral grafts were harvested arthroscopically from the femoropatellar joint and transplanted to the third carpal bone. Nine months after the operation, the osteochondral grafts in the third carpal bone had less proteoglycans, leaving the cartilage softer and less resistant compared to the surrounding cartilage. Six of 18 grafts had histological evidence of cartilage degeneration and it was suggested that the discrepancy in cartilage thickness as well as chondrocyte phenotypic expression between the donor and recipient sites was a major limitation to obtaining functional osteochondral integration [28].
In another study osteochondral cylinder grafts were removed from the cranial surface of the medial femoral trochlea and implanted into defects in the bearing surface of the contralateral medial femoral condyle in five horses. After 12 months, 50% of the grafts had hyaline cartilage, while the other half had loss of glycosaminoglycans and transformation to fibrocartilage. During follow-up arthroscopy at 12 months, the transplanted areas appeared smooth and congruent, and radiologically there were no signs of osteoarthritis. Most donor sites were reconstructed with cancellous bone and covered with fibrocartilage, and 3 of 60 showed mild surface fibrillation. The discrepancy in articular surface geometry between the donor and recipient sites results in articular surface incongruity which in many cases is the major limitation to the success of this procedure [28].
- 2.
- Implantation of autologous chondrocytes implantation without (ACI) or with matrix (scaffold) support (MACI)
Although more than 100 years old, this technique, called ACI, has experienced a renaissance and represents the latest in articular surface restoration. To do this, the lesion is debrided with a synovial resector by arthroscopic approach and all the debrided articular cartilage residues are collected using an aspiration system with a filter connected to the resector. Once the process is finished, all the cartilage that has remained in the filter is mixed with a combination of platelet rich plasma and fibrin and with this mixture, of a rubbery consistency, the joint defect is filled and leveled with the rest of the articular surface [29]. The Arthrex ® company markets a ready-made kit for the said process under the name of AutoCart ™. The advantages of this technique are extensive as cell differentiation is favored, implanting activated chondrocytes with their corresponding matrix and ready to proliferate in a favorable environment [29]. The challenge, as always, is to prevent the immediate support required by the horse from destroying the construct made, generally in support areas. In the equine, autologous chondrocytes fixed with a periosteal flap and fibrin glue led to an overall improvement in histologic scores compared with nongrafted defects, but the repair tissue was not different in composition from the fibrocartilaginous repair and study had a short follow-up period of only 8 weeks when 8 months would be ideal [30]. The combination of the ACI procedure with growth factors (IGF-1) and the use of genetic overexpression of IGF-1 and BMP-7 stimulated early repair within the cartilage defect, but in the long term the results were less significant [31]. The use of MACI in horses has also been documented experimentally [32], although both histological and biomechanical results have not been as spectacular as anticipated.
- 3.
- Microfracture
Microfracture is a technique that has been routinely performed for almost two decades for full-thickness defects with an intact subchondral bone plate in horses. This process of making small entries into the subchondral bone plate through a specific instrument called a micropick (Figure 13), has as objective to facilitate the access of blood elements such as stem cells and growth factors into the defect enhancing healing mostly through the extrinsic pathway.
Three basic research studies of microfracture in the horse in the medial femoral condyle and radial carpal bone have been conducted, but only one is a long-term (12-month) study [33,34,35]. Lesions treated with microfracture showed more defect filling compared to other treatments in terms of the amount of tissue repaired. Histologically, the composition of the repair tissue, including the moderate presence of type 2 collagen, was not different between microfracture-treated and untreated (control) lesions. In none of these studies the functionality in terms of biomechanical resistance of the repaired tissue was evaluated [33,34,35]. In addition, formation of intralesional osteophytes has been observed in equine studies in which chondral defects were treated with microfracture and bone marrow concentrate [36]. Therefore, the decision to perform this technique remains at the discretion of the surgeon based on criteria such as location, thickness, and extension of the lesion. There is limited evidence that microfracture should be accepted as the gold standard for the treatment of cartilage injuries. However, the technical simplicity and low cost make microfracture a popular treatment for chondral and subchondral joint lesions not only in human but also equine patients.
- 4.
- Use of mesenchymal stem cells (MSC)
Several studies in articular cartilage defect models using different constructs and approaches have investigated the effect of MSC without proof of real cartilage regeneration. These have included use of MSC as bone marrow concentrate (BMC) with and without microfracture and suspended in different orthobiologic products and at different follow up times [37,38,39]. Due to the poor results obtained , the use of stem cells, either alone or in combination with other products, is currently not a technique that can be recommended to repair articular surface defects.
- 5.
- Grafts
Apart from mosaicplasty and the AutoCart ® technique, the use of osteochondral grafts in horses in the form of allografts, biomaterial 3D printing or biphasic grafts has been done experimentally but currently there is not enough experimental development to consider its clinical use.
3.1.3. Chondromalacia -progression and decision making process
During the arthroscopic examination, the surgeon will encounter different types of visual representations of inflammation and chondromalacia, often part of a continuous process over time. Thus, this evolution leads to the following sequence of lesions on the articular surface from more incipient to more advanced [7] :
- Proliferation (hyperplasia and hypertrophy) and hyperemia of the synovial membrane (Figure 14)
- Loss of gloss of the articular surface (Figure 1)
- Discoloration of the articular surface
- Softening of the articular surface (Figure 2)
- Thinning or hypertrophy of the cartilage
- Wear lines on the articular surface (Figure 10)
- Articular surface fibrillation (Figure 4)
- Formation of small craters ( pitting ) on the articular surface
- Chondral fissures of the articular surface
- Partial erosion of the articular surface (Figure 5)
- Complete erosion – (damage of calcified layer) on the articular surface (Figure 6)
- Eburnation - If a full thickness erosion presents a smooth polished appearance exposing porous subchondral bone. (Figure 15)
- 1.
- Thermal chondroplasty
After an optimistic start of this technique, its deleterious effects on cartilage were demonstrated [40], but more recently the development of radiofrequency probes with greater control of thermal energy seems to have given rise to this technique, which is used to debride the articular surface in cases of joint fibrillation [41]. Currently, the author suggests caution when using thermal chondroplasty.
- 2.
- Chondrectomy ( Debridement of the articular surface)
In joint surgery, less is often more. If the surgeon considers that the situation found cannot be improved, he should not proceed with any type of chondrectomy. As a rule, if the cartilage has good integration with the subchondral plate, regardless of its appearance, it should be left alone. However, if a separation and detachment of the cartilage from the subchondral plate is observed during palpation, a chondrectomy would be indicated in combination with microfacture .
- 3.
- Microfracture (see above)
- 4.
- Synovectomy and soft tissue debridement
One of the strategies to reduce the bacterial and inflammatory load is to perform a partial or total synovectomy. Synovectomy is performed with a synovial resector that must be sharp. Preferably, a tourniquet should be used because the procedure is associated with significant bleeding, making it difficult to visualize during surgery, especially in situations where there is severe inflammation. Synovectomy is not an innocuous process. It is irreversible and can take up to 120 days to restore, although the new synovial membrane will be made up of more fibrous tissue, which can lead to movement restrictions due to fibrosis [42], leading to the decision to use this procedure partially when strictly necessary and not used indiscriminately due to its side effects. The presence of soft tissues such as ligaments and menisci will be found in the carpus and stifle. The surgical approach with the menisci has not changed in the last 15 years and the recommendation is to debride the affected area after proper evaluation. In the same way, both cruciate ligament injuries and meniscotibial or intercarpal ligament injuries must be debrided with the help of a synovial resector or even biopsy forceps that tend not to damage healthy tissue as much, although their use is more tedious for the surgeon. The recommendation is to always use fresh cutting material to avoid tearing unaffected ligamentous tissue.
3.1.4. Synovial Sepsis
The invasion of the synovial environment by infectious agents produces an inflammatory reaction that irreversibly damages the joint structures if action is not taken quickly and efficiently. In the equine species we can consider that most infectious agents are bacteria, however fungal infections have been previously described [43]. The joint environment is characterized by the presence of a delicate homeostatic balance intended to produce the ideal conditions for joint function. The establishment of a synovial infection depends not only on the bacterial presence but also on the patient's immune response. The bacterial presence in a synovial structure in high numbers can overwhelm the defense capacity of the individual's immune system and produce an inflammatory response characterized by the massive influx and activation mainly of neutrophils. At the same time, the release of inflammatory mediators such as cytokines and enzymes from said neutrophils, synoviocytes, monocytes and macrophages that contribute to the degradation of the cartilage matrix and collagen and to the perpetuation of the degenerative process occurs. In the case of a joint, the components of the joint matrix, mainly glycosaminoglycans (GAG's), proteoglycans (PG's) and collagen can be rapidly destroyed. In experimental models, losses of up to 40% of GAG’s produced in the first 48 hours and up to 50% loss of collagen three weeks after the establishment of an infectious process have been documented. The magnitude of this degradation and loss of joint elements depends on the bacteria involved and the bacterial load. Given the regenerative inability of articular cartilage, the damage produced is irreversible. The inflammatory process gives rise to clinical signs within 12 hours of bacterial inoculation [44]. Infectious arthritis should be considered as an emergency in veterinary practice. As such, once diagnosed, treatment must be instituted immediately, without waiting for the results of the microbiological culture, which can take an average of 48 hours. Early and aggressive treatment of these problems undoubtedly improves the patient's chances of recovery. The elimination of the agent causing inflammation as well as the inflammatory mediators and the attenuation of the immune response are the principles on which the treatment of these infectious processes must be based. Synovial lavage aims to:
- Reduce intrasynovial bacterial load.
- Eliminate fibrin accumulations that can harbor bacteria.
- Drain the presence of inflammatory mediators and cellular waste products.
The use of the arthroscope allows observation of the interior of the synovial capsule and cartilage. In turn, it allows better access and facilitates washing of all areas inside the synovial structure. Fibrin clots can be removed by visualization and a synovectomy can be performed if indicated. This is especially true during the first synovial washout. To maximize results, use of the arthroscope is essential in infections longer than 3 to 5 days to effectively flush the joint and remove fibrin clots that cannot otherwise be drained. The volume of irrigation fluid depends on the volume of the synovial structure to be irrigated. Hence, a stifle requires more volume than a fetlock. Generally during an arthroscopic lavage to treat septic arthritis, a minimum of ten liters of fluid is used in any synovial structure. Regarding the type of fluid used, the use of Ringer's lactate is favored due to its similar characteristics to synovial fluid [45].
3.1.5. Subchondral bone cysts
There is no universal treatment for this pathology and there are several therapeutic options with similar results from a clinical viewpoint[46]. When deciding as to the optimal treatment option, the surgeon must consider the age of the horse, future athletic purpose as well as sale, chondral health, subchondral bone health, and the biomechanics of the combined bone-cartilage unit, which is mostly compressive. The principles of treatment of injuries to the articular surface apply in this situation, but bone regrowth remained a challenge until the development of the stabilization technique through the application of a screw through the cystic cavity [47]. The purpose of the screw is to stabilize the bony vault that forms the cyst, thus allowing the body to receive the appropriate signals to mineralize [47]. More recently, the use of resorbable screws of polylactic acid have given very good cosmetic and functional results without the need to remove the screw in a second surgery [48]. The healing of the chondral defect continues to be a challenge for the surgeon depending on its extension and depth. The principles of chondral treatment must be applied in each joint considering the size, depth, and location of the lesion, taking into account that the absence of a healthy subchondral plate, where the cartilage can be supported similarly to a mattress and box spring, will lead to a collapse of the articular surface and a degenerative process. The use of intra-articular medication helps with the treatment of an inflammatory process, but it lacks effects to treat the structural problem that subchondral bone disappearance entails. Therefore, the surgeon's priority must be the simultaneous reconstruction of the bone scaffold and the articular surface, as well as the treatment of the existing inflammation. In cysts of the medial femoral condyle, the biomechanical environment is transformed by the presence of a screw that crosses the cystic cavity and its optimal use is in those cysts with a greater proximal-distal dimension (as a bishop's miter). Currently, the recommendation to treat subchondral cysts if the objective is it radiographic disappearance is the implantation of a PLA (polylactic acid) resorbable screw, simultaneously with an arthroscopic exploration to observe the articular surface. If the articular cartilage is detached from its bony anchorage, the recommendation is to debride the affected cartilage. Since the interior of the cystic cavity is replete with inflammatory mediators, the debridement of the interior lining of the cyst and/or intralesional treatment with corticosteroids is recommended [49]. Other treatments can be successful in the short/medium term, especially in young horses if they eliminate the inflammatory process. The age of the horse is important and there is a higher percentage of success in horses under 3 years of age. Despite the different treatments, the percentage of success in the treatment of subchondral cysts remains between 70-80% of return to exercise [46]. Unfortunately, we do not have data with very long-term follow-up (>5 years). Radiographic disappearance of the cyst occurs more frequently when the cyst is treated with the implantation of a screw [48].
3.1.6. Large OCD lesions – reattachment of chondral flaps
In young horses suffering from osteochondrosis manifested by the formation of chondral flaps, particularly in the trochleas of the distal femur, the use of resorbable pins to re-attach the chondral flap to its underlying subchondral bone bed has been described with a good degree of success [50]. For this to occur the surgeon must evaluate the health of the subchondral bone. In the absence of a healthy subchondral bone bed, the procedure will most likely fail. The reader is referred to a previous publication for the description of the technique [51].
4. Conclusions
In short, an in-depth knowledge of the patient's characteristics as well as joint pathophysiology is necessary to make the appropriate intraoperative decisions. Joint regeneration is not yet possible, but it is possible to help our patients with the techniques that have been developed recently. Long-term follow-up of our patients is essential for a critical evaluation of the results of any surgical technique.
References
- Nelson, B.; Mäkelä, J.; Lawson, T.; Patwa, A.; Barrett, M.; McIlwraith, C.; Hurtig, M.; Snyder, B.; Moorman, V.; Grinstaff, M.; et al. Evaluation of equine articular cartilage degeneration after mechanical impact injury using cationic contrast-enhanced computed tomography. Osteoarthr. Cartil. 2019, 27, 1219–1228. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.; Carballido-Gamio, J.; Majumdar, S.; Li, X. Comparison of quantitative imaging of cartilage for osteoarthritis: T2, T1ρ, dGEMRIC and contrast-enhanced computed tomography. Magn. Reson. Imaging 2009, 27, 779–784. [Google Scholar] [CrossRef] [PubMed]
- McIlwraith, C.W.; Frisbie, D.D.; Kawcak, C.E.; van Weeren, P.R. Joint Disease in the Horse. 2016. [Google Scholar] [CrossRef]
- Brommer, H.; Rijkenhuizen, A.B.M.; Brama, P.A.J.; Barneveld, A.; Weeren, P.R. Accuracy of diagnostic arthroscopy for the assessment of cartilage damage in the equine metacarpophalangeal joint. Equine Veter- J. 2004, 36, 331–335. [Google Scholar] [CrossRef] [PubMed]
- McIlwraith, C. W. , Wright, I., & Nixon, A. J. (2014). Diagnostic and surgical arthroscopy in the horse. Elsevier Health Sciences.
- McIlwraith, C.; Frisbie, D.; Kawcak, C.; Fuller, C.; Hurtig, M.; Cruz, A. The OARSI histopathology initiative – recommendations for histological assessments of osteoarthritis in the horse. Osteoarthr. Cartil. 2010, 18, S93–S105. [Google Scholar] [CrossRef] [PubMed]
- White, S.A.; Canada, N.C.; Carmalt, J.L.; Schumacher, J.; Amitrano, F.N.; Ortved, K.; Henry, T.J.; Brounts, S.H.; Arnold, C.E. Long-Term Outcome of Horses Undergoing Unilateral Mandibular Condylectomy and Meniscectomy for Temporomandibular Joint Disease. Front. Veter- Sci. 2022, 9, 898096. [Google Scholar] [CrossRef]
- Walmsley, J.P.; Phillips, T.J.; Townsend, H.G.G. Meniscal tears in horses: an evaluation of clinical signs and arthroscopic treatment of 80 cases. Equine Veter- J. 2003, 35, 402–406. [Google Scholar] [CrossRef]
- Simmons, E.J.; Bertone, A.L.; E Weisbrode, S. Instability-induced osteoarthritis in the metacarpophalangeal joint of horses. Am. J. Veter- Res. 1999, 60, 7–13. [Google Scholar]
- Krafts, K.P. Tissue repair: the hidden drama. Organogenesis. 2010, 6, 225. [Google Scholar] [CrossRef]
- Fugazzola, M.C.; van Weeren, P.R. Surgical osteochondral defect repair in the horse—a matter of form or function? Equine Veter- J. 2020, 52, 489–499. [Google Scholar] [CrossRef]
- Alford, J.W.; Cole, B.J. Cartilage restoration, Part 1. Am J Sports Med. 2005, 33, 295–306. [Google Scholar] [CrossRef]
- McIlwraith, C.W.; Fortier, L.A.; Frisbie, D.D.; Nixon, A.J. Equine Models of Articular Cartilage Repair. CARTILAGE 2011, 2, 317–326. [Google Scholar] [CrossRef]
- Hurtig, M.B.; Fretz, P.B.; E Doige, C.; Schnurr, D.L. Effects of lesion size and location on equine articular cartilage repair. Can. J. Veter- Res. = Rev. Can. de Rech. Veter- 1988, 52, 137–46. [Google Scholar]
- Convery, F.R.; Akeson, W.H.; Keown, G.H.D. The Repair of Large Osteochondral Defects An Experimental Study in Horses. Clin. Orthop. Relat. Res. 1972, 82, 253–262. [Google Scholar] [CrossRef]
- Salonius, E.; Rieppo, L.; Nissi, M.J.; Pulkkinen, H.J.; Brommer, H.; Brünott, A.; Silvast, T.S.; Van Weeren, P.R.; Muhonen, V.; Brama, P.A.J.; et al. Critical-sized cartilage defects in the equine carpus. Connect. Tissue Res. 2019, 60, 95–106. [Google Scholar] [CrossRef] [PubMed]
- Bentley, G. Articular cartilage changes in chondromalacia patellae. J Bone Joint Surg Br. 1985, 67, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Schmid, A.; Schmid, F. Ultrastructural studies after arthroscopic cartilage shaving. Arthroscopy. 1987, 3, 137. [Google Scholar]
- Hunziker, E.B.; Rosenberg, L.C. Repair of Partial-Thickness Defects in Articular Cartilage. J. Bone Jt. Surg. 1996, 78, 721–33. [Google Scholar] [CrossRef] [PubMed]
- Hanie, E.A.; Sullins, K.E.; Powers, B.E.; Nelson, P.R. Healing of full-thickness cartilage compared with full-thickness cartilage and subchondral bone defects in the equine third carpal bone. Equine Veter- J. 1992, 24, 382–386. [Google Scholar] [CrossRef] [PubMed]
- McIlwraith, C.W.; Yovich, J.V.; Martin, G.S. Arthroscopic surgery for the treatment of osteochondral chip fractures in the equine carpus. J. Am. Veter- Med Assoc. 1987, 191, 531–540. [Google Scholar]
- McIlwraith, C.W. Surgical versus conservative management of osteochondrosis. Veter- J. 2013, 197, 19–28. [Google Scholar] [CrossRef]
- Nixon, A.J.; Fortier, L.A.; Goodrich, L.R.; Ducharme, N.G. Arthroscopic reattachment of osteochondritis dissecans lesions using resorbable polydioxanone pins. Equine Veter- J. 2004, 36, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Kawcak, C.E.; McILWRAITH, C.W.; Norrdin, R.W.; Park, R.D.; James, S.P. The role of subchondral bone in joint disease: a review. Equine Veter- J. 2010, 33, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Petsatodis, G.; Antonarakos, P.; Chalidis, B.; Papadopoulos, P.; Christoforidis, J.; Pournaras, J. Surgically treated acetabular fractures via a single posterior approach with a follow-up of 2–10 years. Injury 2007, 38, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Makris, E.A.; Gomoll, A.H.; Malizos, K.N.; Hu, J.C.; Athanasiou, K.A. Repair and tissue engineering techniques for articular cartilage. Nat. Rev. Rheumatol. 2015, 11, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Bodó, G.; Vásárhelyi, G.; Hangody, L.; Módis, L. Mosaic arthroplasty of the medial femoral condyle in horses — An experimental study. Acta Veter- Hung. 2014, 62, 155–168. [Google Scholar] [CrossRef]
- Tuska, P.; Tóth, B.; Vásárhelyi, G.; Hangody, L.; Papp, M.; Bodó, G. Evaluation of biomarkers following autologous osteochondral transplantation in the equine stifle joint — An experimental study. Acta Veter- Hung. 2016, 64, 164–178. [Google Scholar] [CrossRef]
- Christensen, B.B.; Olesen, M.L.; Hede, K.T.C.; Bergholt, N.L.; Foldager, C.B.; Lind, M. Particulated Cartilage for Chondral and Osteochondral Repair: A Review. CARTILAGE 2021, 13, 1047S–1057S. [Google Scholar] [CrossRef]
- Nixon, A.J.; Begum, L.; Mohammed, H.O.; Huibregtse, B.; O'Callaghan, M.M.; Matthews, G.L. Autologous chondrocyte implantation drives early chondrogenesis and organized repair in extensive full- and partial-thickness cartilage defects in an equine model. J. Orthop. Res. 2011, 29, 1121–1130. [Google Scholar] [CrossRef]
- Ortved, K.F.; Begum, L.; O Mohammed, H.; Nixon, A.J. Implantation of rAAV5-IGF-I Transduced Autologous Chondrocytes Improves Cartilage Repair in Full-thickness Defects in the Equine Model. Mol. Ther. 2015, 23, 363–373. [Google Scholar] [CrossRef]
- Nixon, A.J.; Sparks, H.D.; Begum, L.; McDonough, S.; Scimeca, M.S.; Moran, N.; Matthews, G.L. Matrix-Induced Autologous Chondrocyte Implantation (MACI) Using a Cell-Seeded Collagen Membrane Improves Cartilage Healing in the Equine Model. J. Bone Jt. Surg. 2017, 99, 1987–1998. [Google Scholar] [CrossRef]
- Frisbie, D.D.; Morisset, S.; Ho, C.P.; Rodkey, W.G.; Steadman, J.R.; Mcllwraith, C.W. Effects of Calcified Cartilage on Healing of Chondral Defects Treated with Microfracture in Horses. Am. J. Sports Med. 2006, 34, 1824–1831. [Google Scholar] [CrossRef] [PubMed]
- Frisbie, D.D.; Oxford, J.T.; Southwood, L.; Trotter, G.W.; Rodkey, W.G.; Steadman, J.R.; et al. Early events in cartilage repair after subchon- dral bone microfracture. Clin Orthop Relat Res. 2003, 407, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Frisbie, D.D.; Trotter, G.W.; Powers, B.E.; Rodkey, W.G.; Steadman, J.R.; Howard, R.D.; et al. Arthroscopic subchondral bone plate microfrac- ture technique augments healing of large chondral defects in the radial carpal bone and medial femoral condyle of horses. Vet Surg. 1999, 28, 242–255. [Google Scholar] [CrossRef] [PubMed]
- A Fortier, L.; Potter, H.G.; Rickey, E.J.; Schnabel, L.V.; Foo, L.F.; Chong, L.R.; Stokol, T.; Cheetham, J.; Nixon, A.J. Concentrated Bone Marrow Aspirate Improves Full-Thickness Cartilage Repair Compared with Microfracture in the Equine Model. Minerva Anestesiol. 2010, 92, 1927–1937. [Google Scholar] [CrossRef] [PubMed]
- Wilke, M.M.; Nydam, D.V.; Nixon, A.J. Enhanced early chondrogenesis in articular defects following arthroscopic mesenchymal stem cell implantation in an equine model. J. Orthop. Res. 2007, 25, 913–925. [Google Scholar] [CrossRef]
- Goodrich, L.R.; Chen, A.C.; Werpy, N.M.; Williams, A.A.; Kisiday, J.D.; Su, A.W.; et al. Addition of mesenchymal stem cells to autologous platelet-en- hanced fibrin scaffolds in chondral defects: does it enhance repair? J Bone Joint Surg Am. 2016, 98, 23–34. [Google Scholar] [CrossRef]
- Chu, C.R.; Fortier, L.A.; Williams, A.; Payne, K.A.; McCarrel, T.M.; Bowers, M.E.; et al. Minimally manipulated bone marrow concentrate com- pared with microfracture treatment of full-thickness chondral de- fects: a one-year study in an equine model. J Bone Joint Surg Am. 2018, 100, 138–146. [Google Scholar] [CrossRef]
- Edwards, R.B.; Lu, Y.; Markel, M.D. The basic science of thermally assisted chondroplasty. Clin. Sports Med. 2002, 21, 619–647. [Google Scholar] [CrossRef]
- Lin, C.; Deng, Z.; Xiong, J.; Lu, W.; Chen, K.; Zheng, Y.; Zhu, W. The Arthroscopic Application of Radiofrequency in Treatment of Articular Cartilage Lesions. Front. Bioeng. Biotechnol. 2022, 9, 822286. [Google Scholar] [CrossRef]
- Hewes, C.A.; Schneider, R.K.; Baszler, T.V.; Oaks, J.L. Septic arthritis and granulomatous synovitis caused by infection with Mycobacterium avium complex in a horse. J. Am. Veter- Med Assoc. 2005, 226, 2035–2038. [Google Scholar] [CrossRef]
- Wysocki, A.B. Evaluating and Managing Open Skin Wounds: Colonization Versus Infection. AACN Adv. Crit. Care 2002, 13, 382–397. [Google Scholar] [CrossRef] [PubMed]
- Lugo, J.; Gaughan, E.M. Septic Arthritis, Tenosynovitis, and Infections of Hoof Structures. Veter- Clin. North Am. Equine Pr. 2006, 22, 363–388. [Google Scholar] [CrossRef] [PubMed]
- Theoret, C.L.; Barber, S.M.; Moyana, T.; Townsend, H.G.; Archer, J.F. Repair and Function of Synovium After Arthroscopic Synovectomy of the Dorsal Compartment of the Equine Antebrachiocarpal Joint. Veter- Surg. 1996, 25, 142–153. [Google Scholar] [CrossRef]
- Young, N.; Barker, W.; Minshall, G.; Wright, I. Arthroscopically guided lag screw fixation of subchondral bone cysts in the medial femoral condyle in Thoroughbred racehorses: description of technique and comparative results. Veter- Surg. 2023. [Google Scholar] [CrossRef] [PubMed]
- Santschi, E.M.; Williams, J.M.; Morgan, J.W.; Johnson, C.R.; Bertone, A.L.; Juzwiak, J.S. Preliminary Investigation of the Treatment of Equine Medial Femoral Condylar Subchondral Cystic Lesions With a Transcondylar Screw. Veter- Surg. 2015, 44, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Ravanetti, P.; Lechartier, A.; Hamon, M.; Zucca, E. A composite absorbable implant used to treat subchondral bone cysts in 38 horses. Equine Veter- J. 2021, 54, 97–105. [Google Scholar] [CrossRef]
- Rechenberg, B.; Guenther, H.; McIlwraith, C.W.; Leutenegger, C.; Frisbie, D.D.; Akens, M.K.; Auer, J.A. Fibrous Tissue of Subchondral Cystic Lesions in Horses Produce Local Mediators and Neutral Metalloproteinases and Cause Bone Resorption in Vitro. Veter- Surg. 2000, 29, 420–429. [Google Scholar] [CrossRef]
- Sparks, H.D.; Nixon, A.J.; Fortier, L.A.; Mohammed, H.O. Arthroscopic reattachment of osteochondritis dissecans cartilage flaps of the femoropatellar joint: Long-term results. Equine Veter- J. 2011, 43, 650–659. [Google Scholar] [CrossRef]
- Bertuglia, A.; Pallante, M.; Pillon, G.; Valle, D.; Pagliara, E.; Riccio, B. Reattachment of Osteochondritis Dissecans Lesions in the Lateral Femoral Trochlear Ridge With Bioabsorbable Screws in 4 Yearling Standardbreds. J. Equine Veter- Sci. 2023, 123, 104242. [Google Scholar] [CrossRef]
Figure 1.
Loss of shinning seen in articular cartilage in case of carpal osteoarthritis.
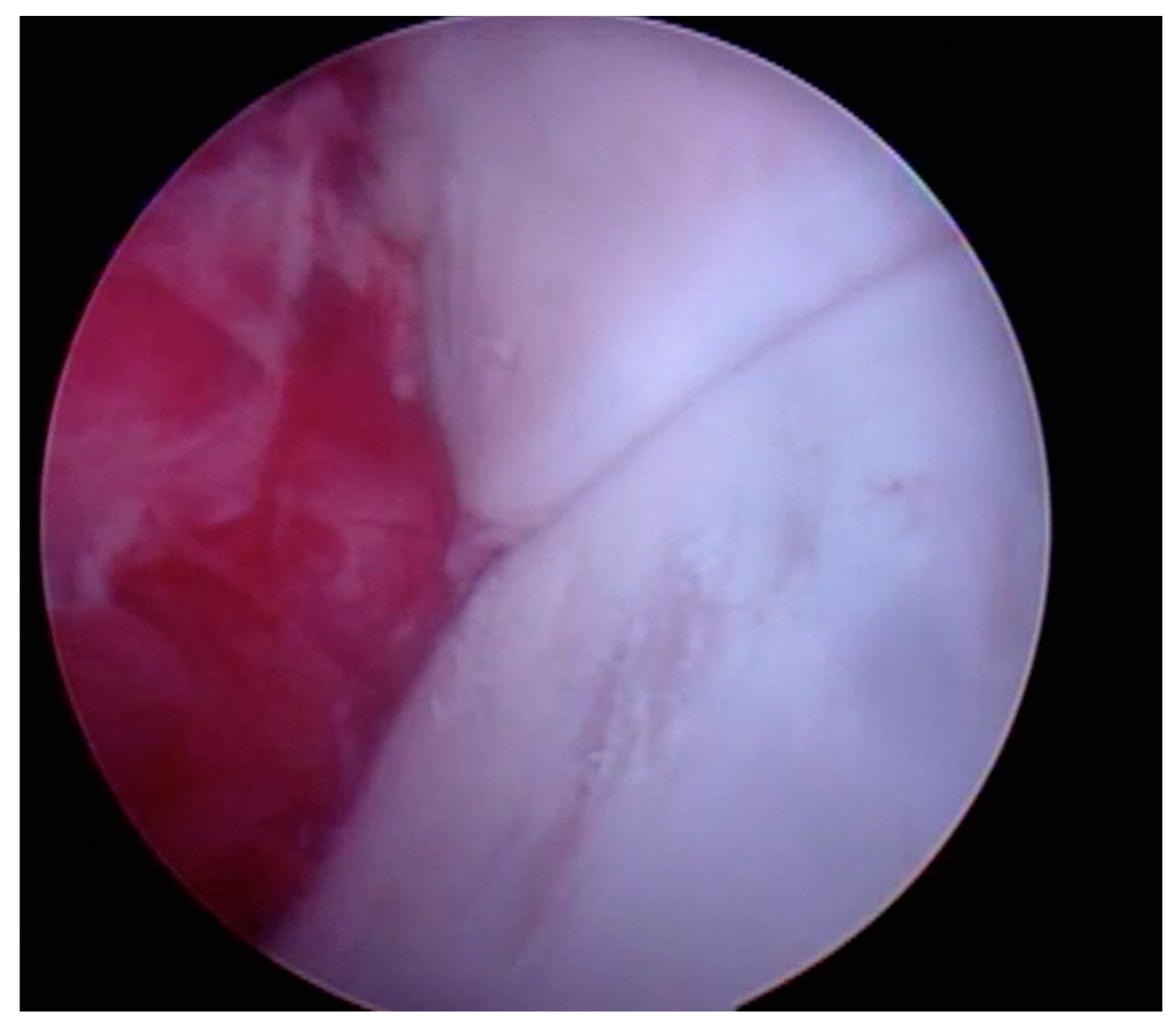
Figure 2.
Soft cartilage.

Figure 3.
Use of the palpator to assess cartilage health.

Figure 4.
Articular surface fibrillation.
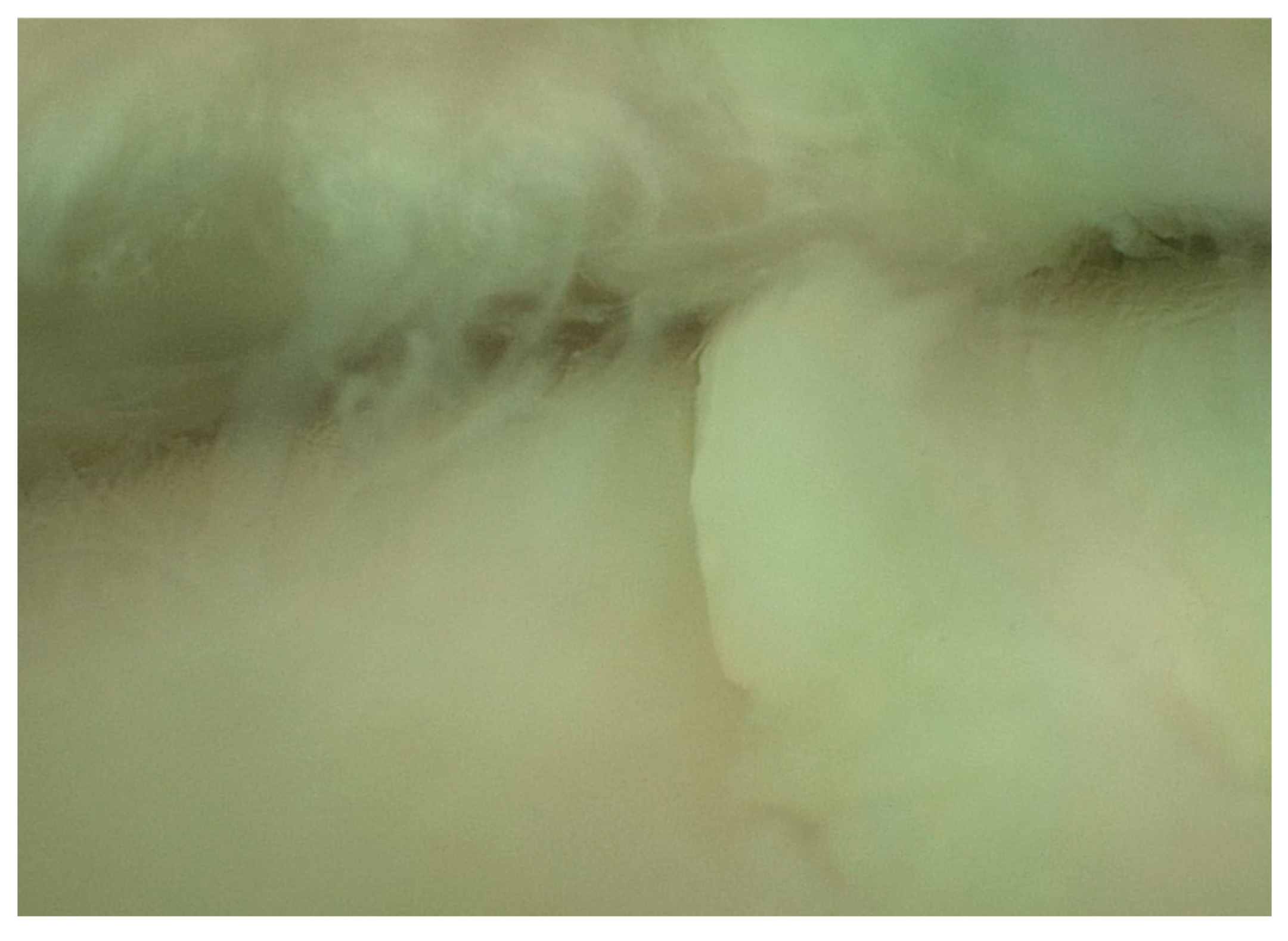
Figure 5.
Partial thickness erosion and fibrillation.

Figure 6.
Full thickness erosions where the subchondral bone plate can be seen exposed to the synovial environment.
Figure 6.
Full thickness erosions where the subchondral bone plate can be seen exposed to the synovial environment.
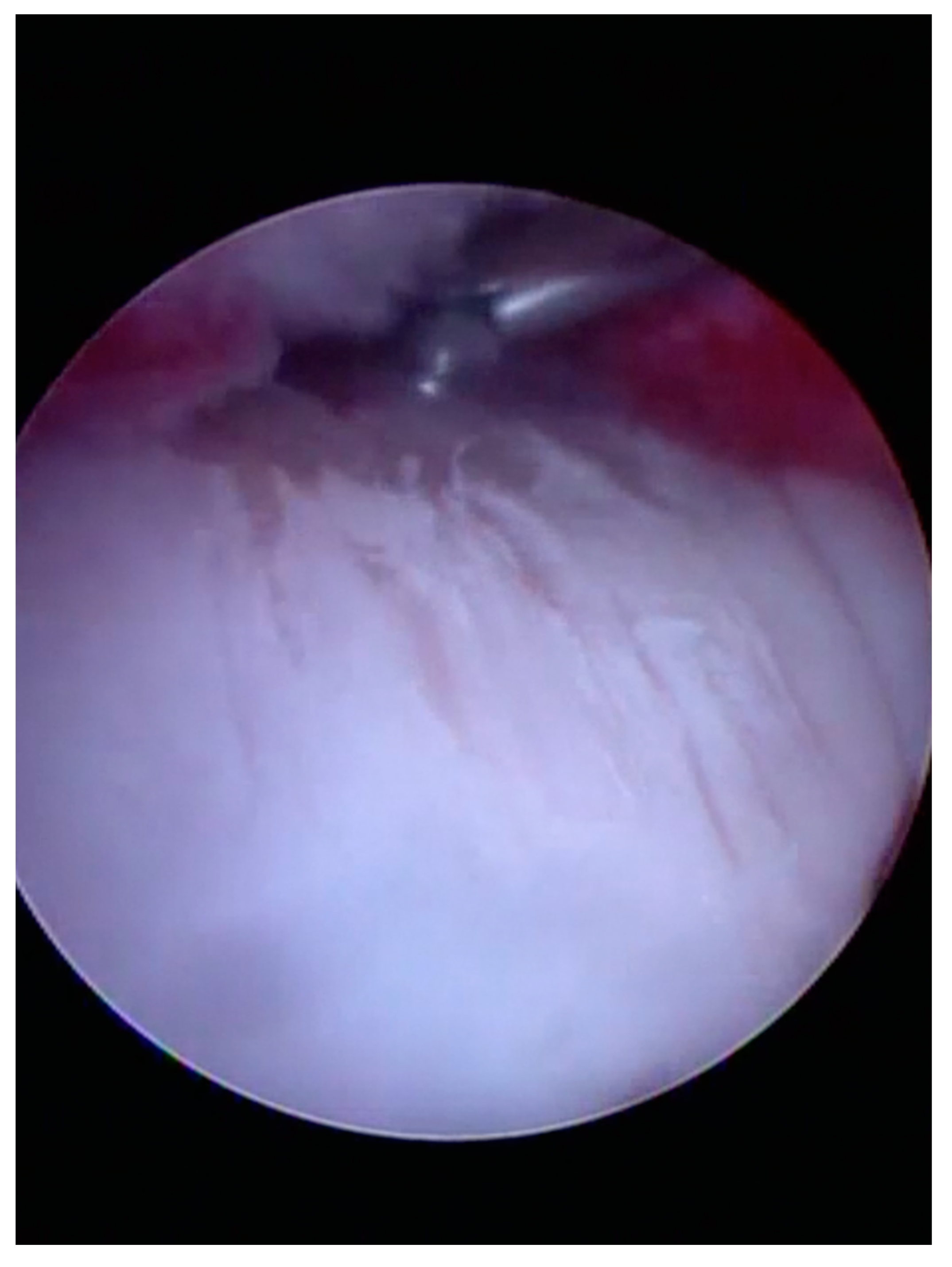
Figure 7.
Medial intercarpal ligaments.

Figure 8.
Normal meniscus.

Figure 9.
Fibrillated meniscus.
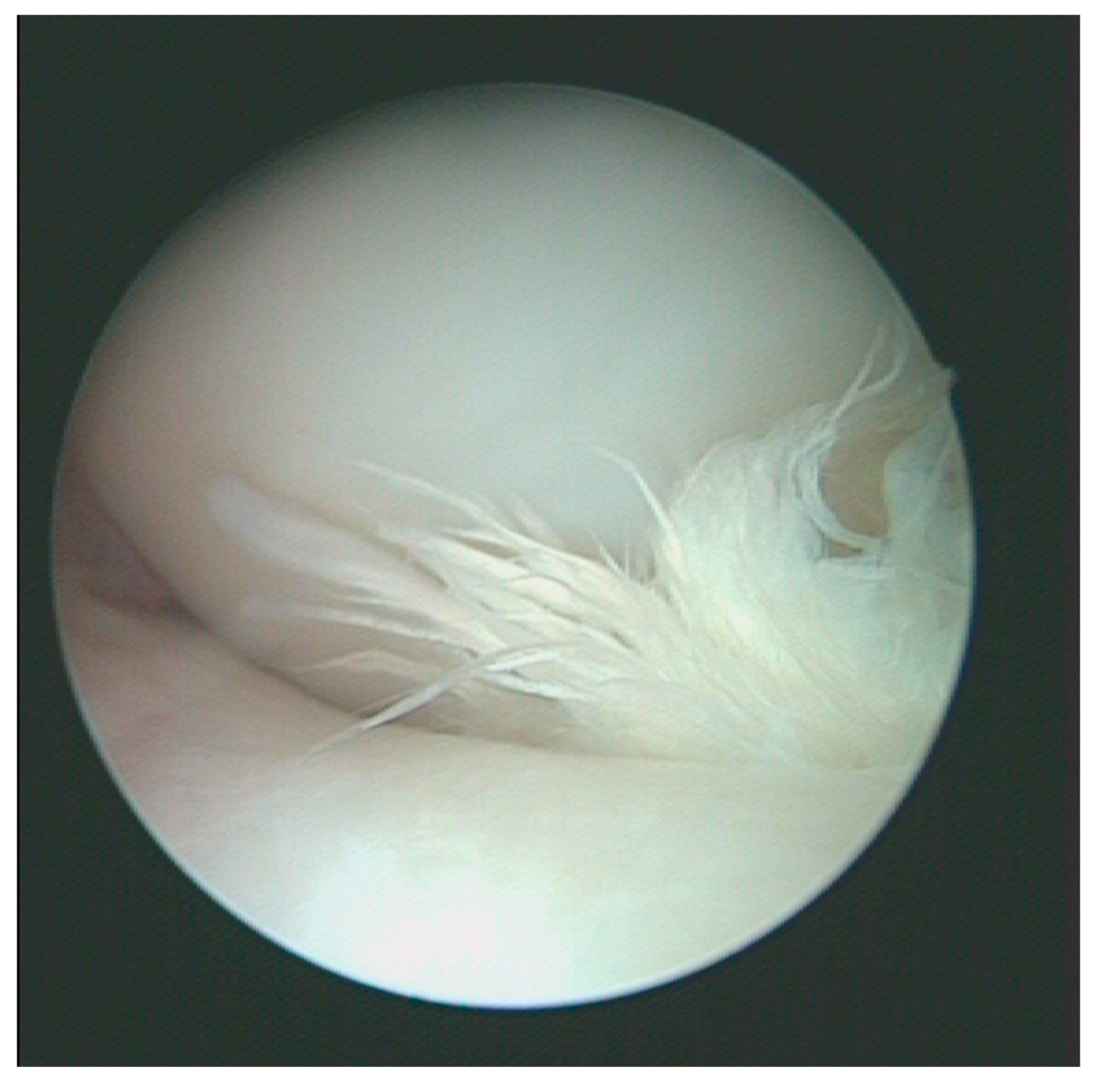
Figure 10.
Wear lines.
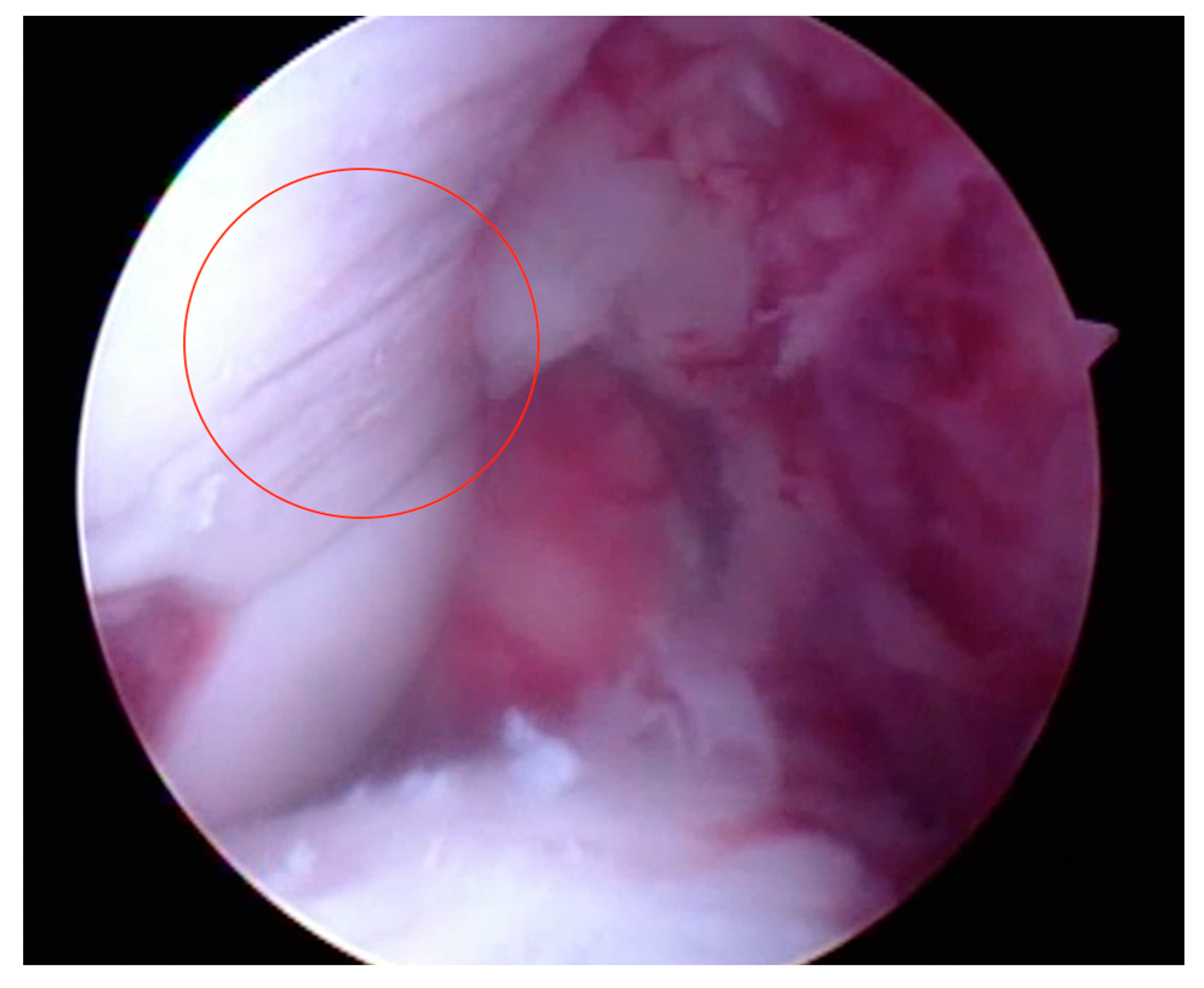
Figure 11.
Third carpal bone slab fracture requiring osteosynthesis.
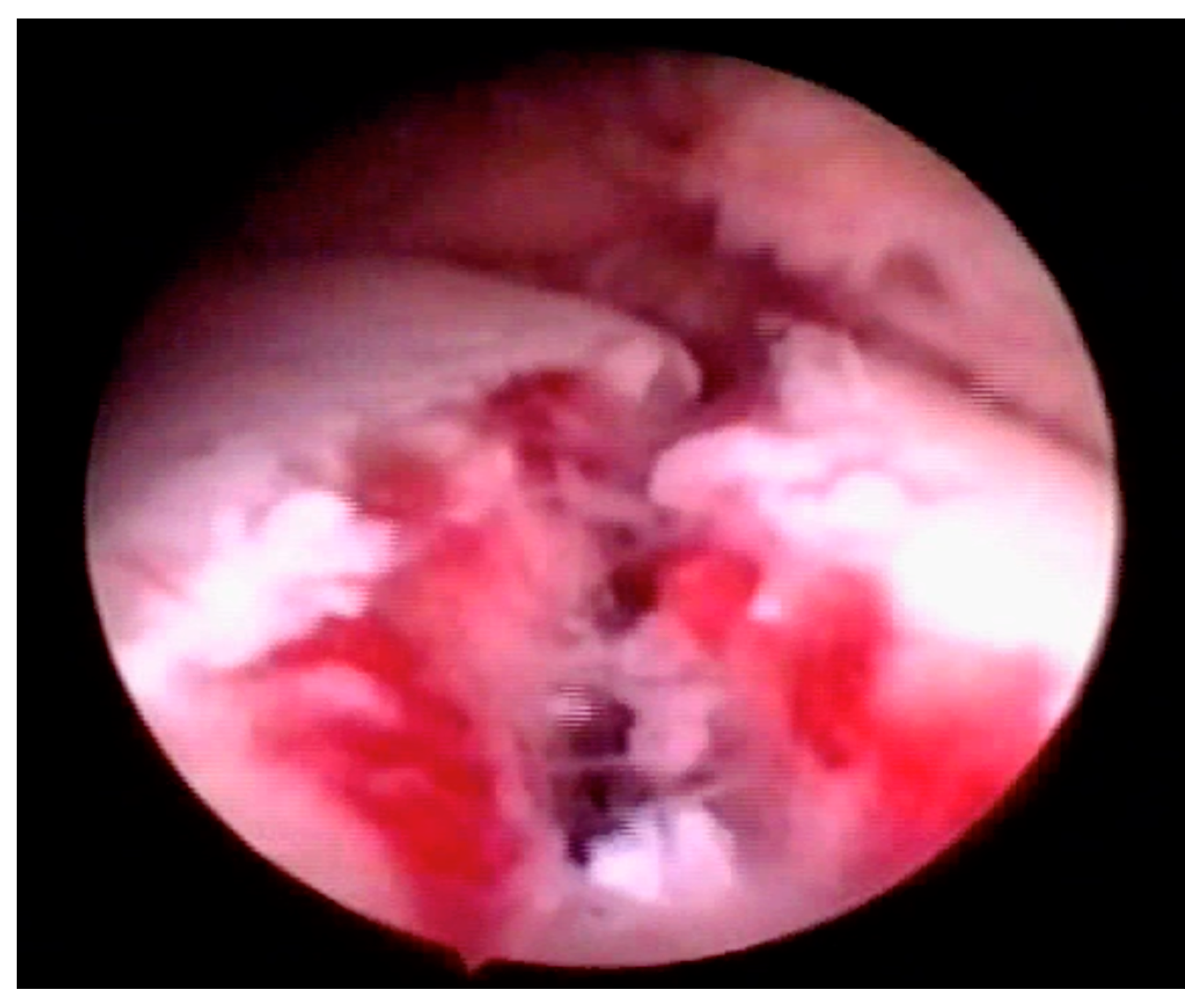
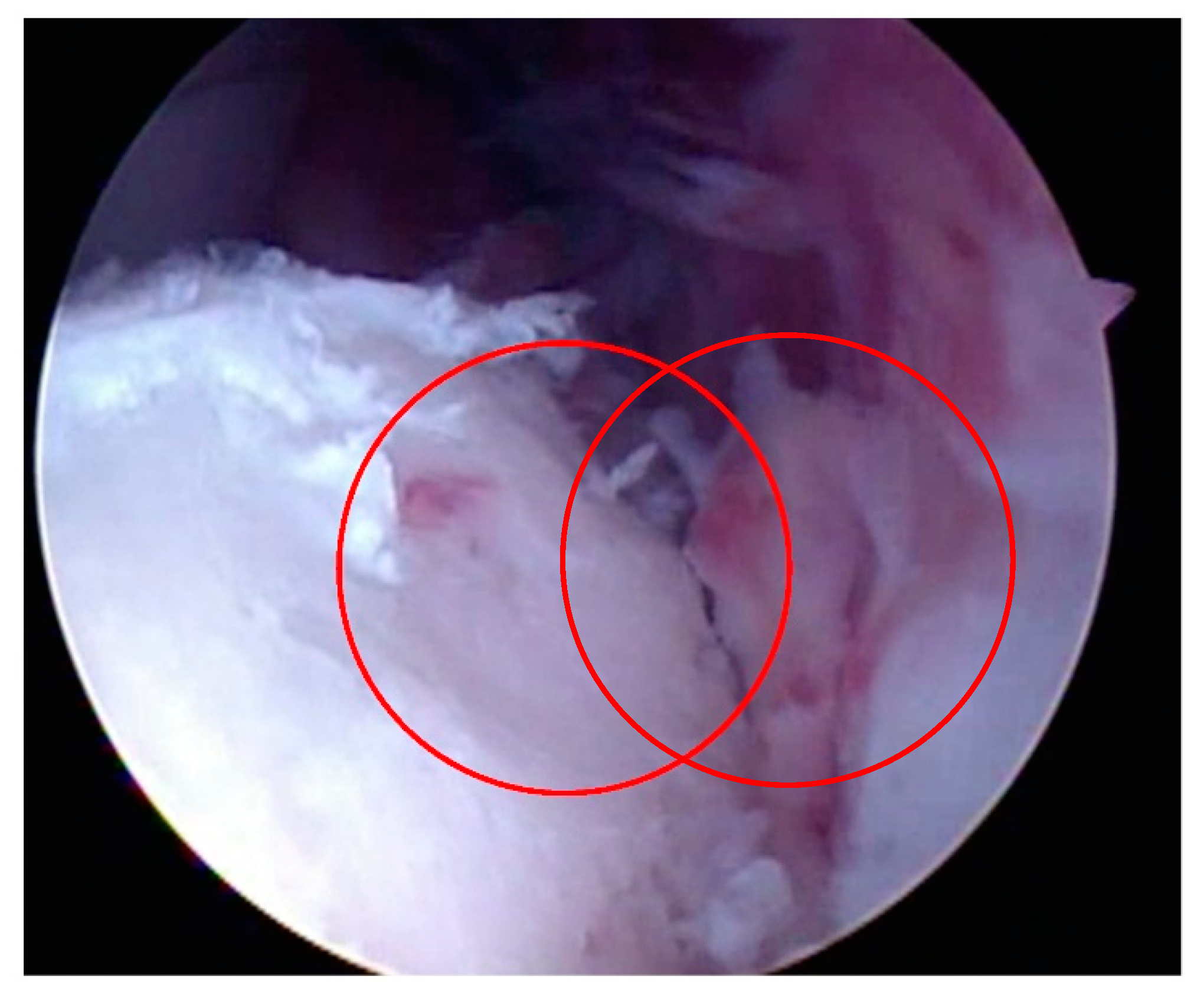
Figure 12.
Condylar fracture following inter-fragmentary compression (arrows).
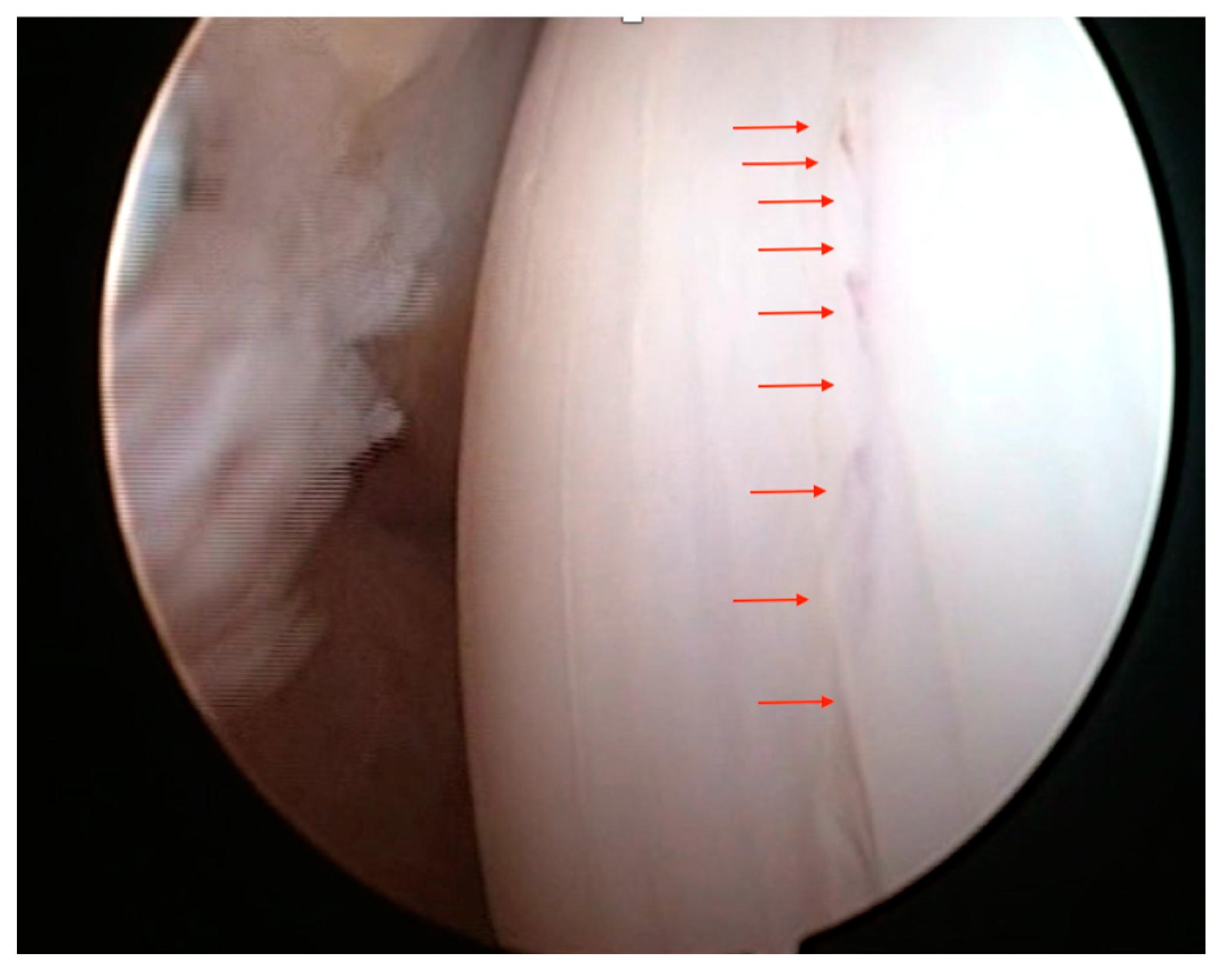
Figure 13.
Micropicking of subchondral bone plate to stimulate the pathway of extrinsic healing.
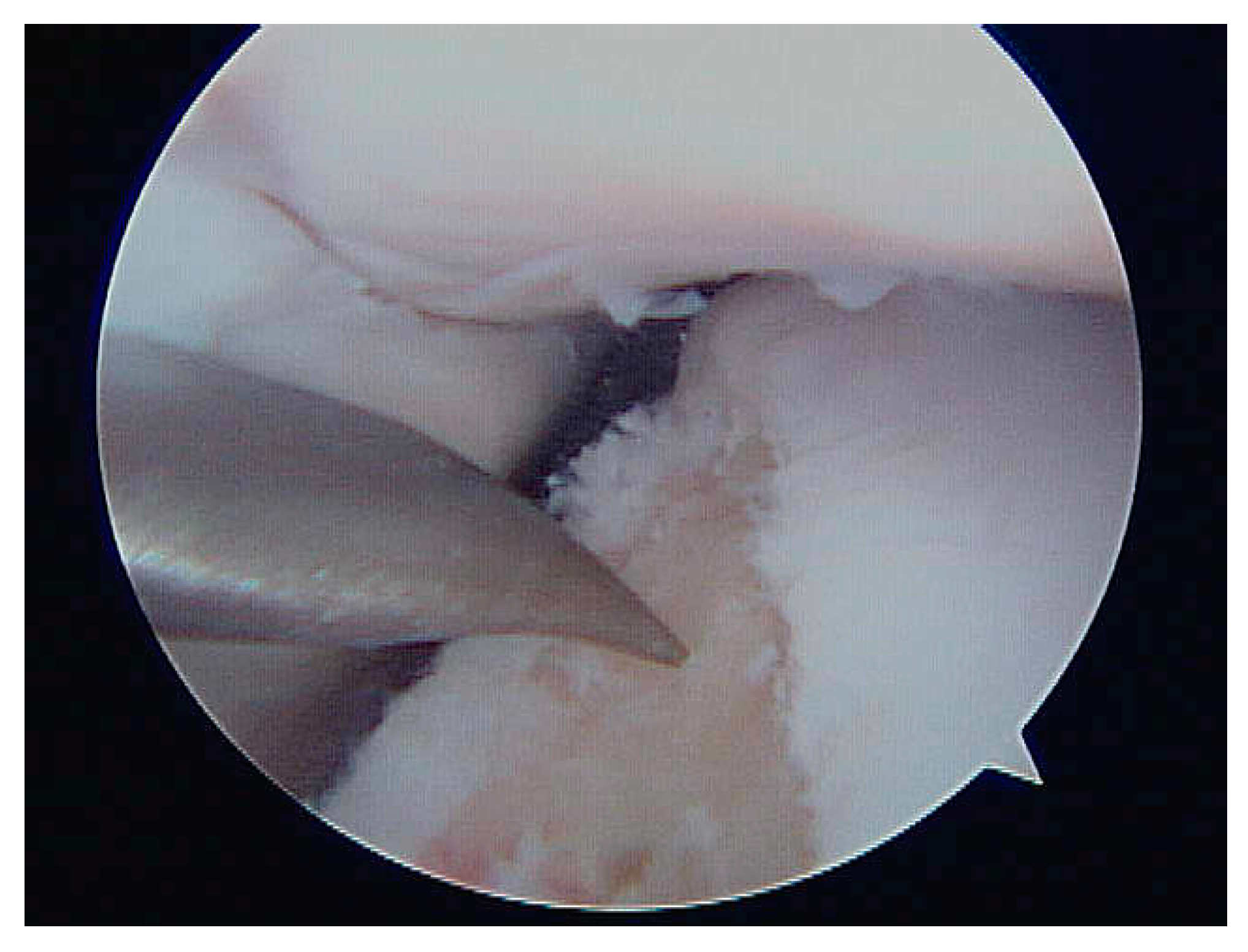
Figure 14.
Synovial hyperplasia in a case of mild (a) or severe synovitis (b).
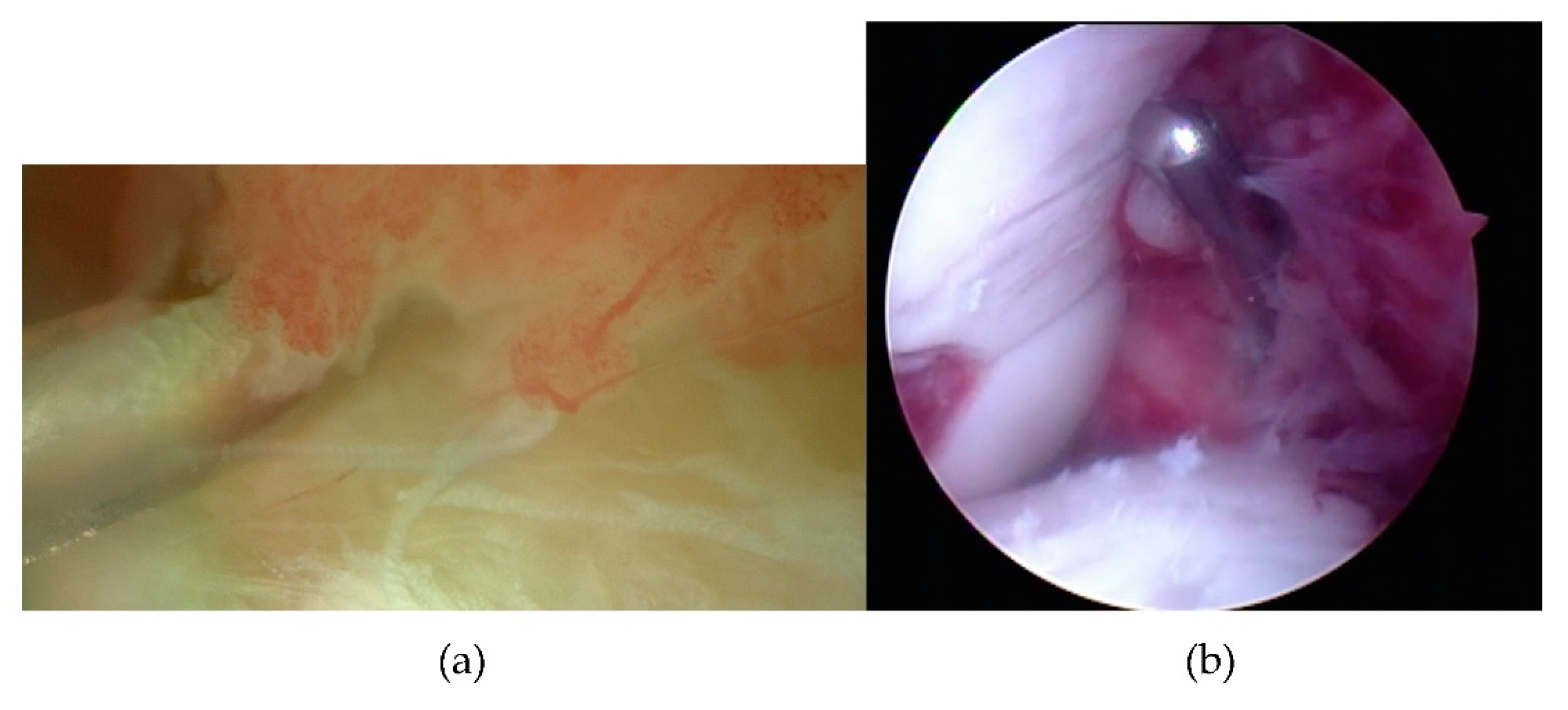
Figure 15.
Eburnation of articular cartilage.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



