
Submitted:
21 September 2023
Posted:
21 September 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Vaccine hesitancy substantially impacts global vaccination rates. During the COVID-19 pandem-ic in Germany, vaccination uptake exhibited considerable regional disparities. To assess the fac-tors contributing to this variation, we examined the influence of sociodemographic variables on COVID-19, COVID-19 booster, and influenza vaccinations within a cohort of 37,078 participants from 13 German federal states in the digital health cohort study, DigiHero. Our findings re-vealed variations in vaccination rates based on sociodemographic factors. However, these fac-tors had limited explanatory power regarding regional differences in vaccine uptake. In contrast, we found substantial correlations between regional support of specific parties during last local elections and the vaccination uptake at Landkreis-level. In conclusion, sociodemographic factors alone did not suffice to explain the regional disparities in vaccine uptake. Political stances can play a major role, but the current investigation did not assess the individual political orienta-tion, but used only ecological approach.
Keywords:
COVID-19
; influenza
; vaccine hesitancy
1. Introduction
Vaccination against SARS-CoV-2 became available in the European Union at the end of 2020. In the summer of 2021, most of the German population had received basic immunization. Subsequently, the first booster vaccination became available towards the end of 2021. The spread of the Omicron variant was observed in numerous countries across the globe, including Germany, where the Robert Koch Institute (RKI) – the federal governmental agency in Germany tasked with the control and prevention of diseases – documented 16,748 Omicron cases as of December 30th, 2021 [1]. Thus, the RKI advised individuals who had not yet received their first COVID-19 vaccine doses to get vaccinated and recommended that booster doses should be accessible to all age groups [1]. The second booster vaccination, optimized for Omicron, became available in the autumn of 2022.
However, the introduction of available vaccinations against COVID-19 in 2021 met a strong resistance from some parts of the German population [2]. This is known as vaccine hesitancy and it is characterized as “the delay in acceptance or refusal of vaccination despite availability of vaccination services” [3]. Vaccine hesitancy is not a novel phenomenon, and it did not emerge during the COVID-19 pandemic. It has been observed in the majority of countries and differs across country level income [4]. Hesitancy towards vaccinations is fueled by fears regarding vaccine adverse events or side effects [5]. Other than the COVID-19 vaccine, some vaccines that face opposition among the public include the Measles, Mumps, and Rubella (MMR), HPV (Human Papillomavirus), Hepatitis B, Influenza, and Polio vaccines [6,7]. Nevertheless, opposition towards COVID-19 became part of political ideology in some countries [8].
In Germany, vaccine hesitancy towards COVID-19 vaccines had a particularly noticeable presence in the former Eastern German states [2]. As of April 2023, the overall vaccination coverage in Germany was 77.9%, with people of all ages receiving at least one dose [9]. Furthermore, 76.4% of the total population received basic immunization, 62.6% received one or more booster doses, and 15.2% received at least two booster doses [9]. Moreover, age played a fundamental role in the uptake of vaccinations. While individuals above the age of 60 demonstrated higher rates of acquiring basic immunization (90.1%) and obtaining at least two booster vaccinations (39%), those in the 18 to 59 years age group exhibited lower rates of 83% for basic immunization and only 6.8% for two booster doses [9].
Due to respective recommendations from the STIKO (Standing Committee on Vaccination), a higher proportion of those aged 60 and above receive influenza or pneumococci vaccinations [10]. During the winter of 2021/22, 43.3% of individuals aged above 60 and 35.4% of individuals aged above 18 (with relevant underlying conditions) were vaccinated against influenza [10], with a higher vaccination coverage rate against influenza was observed in Eastern Germany than in Western Germany [11]. For other vaccinations such as Pertussis/Diphtheria/Tetanus, the vaccination coverage rates were also considerably higher in former Eastern German states than in former Western German states [12,13]. This outcome is probably attributed to distinct attitudes associated with these established immunizations [12,13].
Given this contextual background, we aimed to explore how much of the variation in vaccine coverage could be explained by differences in sociodemographic characteristics given that national reporting includes information on vaccination uptake by age and sex, but not factors such as education and income. Additionally, we compared the situation for any COVID-19 vaccination, boosters administered in the autumn of 2022, and the influenza vaccination in the same time period.
2. Materials and Methods
2.1. Study design and questionnaires
The data used in this study were collected in the population-based prospective cohort study for digital health research in Germany (DigiHero, DRKS Registration-ID: DRKS00025600) [14]. DigiHero started in the city of Halle (Saxony-Anhalt, Germany) in January 2021 and was later extended to other federal states in Germany, with a strong focus on Middle Germany. Random samples were derived from registration registries, and the selected individuals were invited through postal letters to DigiHero. The participation in the study is online, and participants are invited to various questionnaires three to four times per year. In the first questionnaire, sociodemographic information was collected. The Ethics Committee of the Martin Luther University Halle-Wittenberg (2020-076) approved the study and informed consent was obtained from all participants during online registration.
In the spring of 2023, we invited 70,538 participants from 13 federal states in Germany who had been recruited until then to answer questions regarding vaccinations against COVID-19 and influenza in the preceding autumn/winter season. Additionally, we collected information on all vaccinations against SARS-CoV-2 since the beginning of the pandemic. In our study, individuals who have received four doses or more are considered to have received a SARS-CoV-2 booster vaccination. We combined these data with sociodemographic information from the initial questionnaire. We categorized education levels based on the International Standard Classification of Education (ISCED-97) into three categories: low, medium, and high [15]. In the baseline questionnaire, we inquired about the net household income, providing seven income categories. To determine the net household equivalent income, we first computed the mean of each category and divided the mean by the sum of the household weights. Household weights were calculated using the following weights: the first adult was assigned a weight of “1”, while all other adults (individuals aged 14 and above) held a weight of “0.5”, and children were assigned a weight of “0.3”. The resulting value was then categorized using the initial seven income categories.
2.2. Statistical analysis
Descriptive statistics for this study are presented using frequencies and percentages. We employed generalized additive models (GAM) to effectively model vaccination uptake by age. We examined three outcomes: (i) receiving any vaccinations against SARS-CoV-2 versus none; (ii) receiving any booster vaccinations against SARS-CoV-2 versus none; and (iii) receiving an influenza vaccination in autumn/winter 2022/23 versus not receiving one. We examined the vaccination uptake across federal states – initially without adjustments and subsequently accounting for sociodemographic factors such as age, sex, place of residence, urban/rural place of living, migration background, net household equivalent income, and education by a stepwise approach. We used the order of importance of the adjustment factors determined for any vaccination for the other outcomes as well.
Finally, we analyzed regional variation patterns in vaccination uptake within two specific federal states, Saxony and Saxony-Anhalt, where DigiHero included participants from all administrative units (Landkreise) and correlated those with percentage of support for the political parties in the state elections.
3. Results
Out of the individuals invited for the study, 38,827 (53.7%) completed the vaccination questionnaire between March and April 2023. We removed participants with incomplete vaccination data (n=1,749), resulting in a final sample of 37,078. Those who responded to this questionnaire showed some differences in terms of sociodemographic data compared to those who did not participate, mainly a lower response rate among males, individuals in the youngest age group, and participants with low education and low income (Table 1).
Differences in the uptake of SARS-CoV-2 and influenza vaccinations were observed across various sociodemographic characteristics and regions (Table 2). The overall vaccination uptake was highest for any COVID-19 vaccination (92.8%), followed by influenza vaccine (44.1%), and booster vaccination for COVID-19 (25.6%).
The association between age and vaccination uptake displayed different patterns for the three studied vaccines (Figure 1). It is interesting to note the lower uptake in the age group of 30 to 60 for all vaccinations. Another observation is the low booster uptake below 60 years, and a nearly linear increase in uptake with age for influenza vaccination.
Vaccination uptake for SARS-CoV-2 was lowest for Saxony, followed by further federal states in the former East Germany (Table 2). In Schleswig-Holstein, the uptake of booster vaccination was much higher than in the other federal states. For influenza vaccination, the uptake was highest in the city of Hamburg, as well as the federal states of Saxony-Anhalt and Schleswig-Holstein.
In general, the differences in sociodemographic variables did not explain much of the regional variation in vaccine uptake (Figure 2). However, when city residence was included in the models for COVID-19 vaccination, the estimates for Berlin, Hamburg, and Stuttgart changed substantially. In contrast to the COVID-19 vaccines, influenza vaccination uptake was, among the studied federal states, highest in Saxony-Anhalt.
Within the federal states of Saxony and Saxony-Anhalt, similar regional patterns emerged for uptake of COVID-19 and influenza vaccines. Across the seven strongest parties, for three existed positive correlations (Figure 4, with substantial fraction of variation explained, Figure 5), for three rather minor and for one party a strong negative correlation. The latter is a right-wing party, which holds strong anti-vaccination policies.
4. Discussion
Our study aimed to investigate whether differences in sociodemographic characteristics could account for variations in uptake for COVID-19, booster, and influenza vaccines. National reporting provides data on vaccination rates based on age, but it does not include factors such as education and income. Despite considering these sociodemographic variables, the substantial differences in vaccination uptake across different federal states remained largely unchanged. The regional uptake showed a rather strong correlation with the regional proportion of first votes in the last local elections, with three parties with a positive correlation, two with no correlation and one with a strong negative correlation in the two federal states studied. These correlations explained considerable fraction of variation.
Sociodemographic factors did not explain lot of the regional variations. In fact, it appears that beliefs related to vaccination are more profound and related to personal preferences. An in-depth qualitative survey involving 33 German participants identified four primary themes that influenced the decision to receive a COVID-19 vaccine: (i) assessment of the benefits and risks of being vaccinated against COVID-19; (ii) influence of existing social and political conditions; (iii) emotional responses to the pandemic and its’ social and political impact; and (iv) trust and confidence in health authorities and the vaccines themselves [18]. Recurrent themes across multiple studies in both Germany and Europe as a whole included reasons such as low levels of trust in healthcare authorities and COVID-19 vaccines, concerns about potential side effects, and alignment with right-wing political stances [19,20,21,22,23,24]. Thus, it appears that there are fundamental concerns about vaccination that are also intertwined with political ideologies. It is not clear in which direction the influence between politics and vaccination concerns occurs.
Several other vaccines, apart from the SARS-CoV-2 vaccine, had faced resistance from the public. For example, the Hepatitis B vaccine and HPV (Human Papillomavirus) vaccine are two modern vaccines that have encountered substantial resistance from the population [7]. Many of these concerns were attributed to fears regarding claims of association with autoimmune diseases such as multiple sclerosis for Hepatitis B Vaccine, and the apprehension of promoting sexual activity for the HPV vaccine [7].
Hesitancy towards influenza vaccine was prominent even before the COVID-19 pandemic, and this hesitancy persisted when the initial COVID-19 vaccination rollout began in 2021. Less than half of the study participants were vaccinated for influenza, with the highest uptake observed in Eastern German states. This trend is consistent with previous research on influenza vaccination, which has shown higher coverage rates in Eastern Germany compared to Western Germany [11]. Vaccine hesitancy towards influenza was also seen in other countries before and during the COVID-19 pandemic. For instance, low coverage rates were observed in the United States in 2018, where 36.8% of 4,286 participants were reluctant to get vaccinated against influenza [25]. Two major factors, namely race or ethnicity and gender were found to be the predicting factors for vaccine refusal [25].
The low uptake of SARS-CoV-2 booster vaccination in the autumn/winter 2022/23 indicates that in the autumn/winter season of 2023/24 a large fraction of the population in Germany will have been vaccinated more than 12 months ago. During the winter season of 2022/23, many people still became infected [26], but the protection against a severe course of infection offered by a preceding infection is considered to last shorter than by vaccination. This situation might lead to a substantial burden of severe infections. While for influenza, the autumn vaccination campaign is sufficient to avoid a large burden of severe cases, influenza has a much lower basic reproduction number than SARS-CoV-2 and the immune protection for influenza was built over many years in the population. Since the protection against infection is only partial for the Omicron variant [27,28,29,30], its circulation hardly can be avoided and question on the proportion of severe cases will become relevant for the health care system.
Our study had several limitations. Firstly, we considered only the number of vaccinations, while particularly in the early stages of the pandemic, infections were considered to provide protection for a certain period. This approach might have led to an underestimation of willingness for vaccination. Conversely, it is possible that those who participated in the study had a more positive attitude towards vaccination, which could have resulted in higher uptake estimates in our data. In fact, when we compared our findings to national data, we found a higher vaccination uptake, suggesting that our study participants may not fully represent the general population. Additionally, relying on study participants who may be more similar to each other across federal states than the general population of these states could have led to an underestimation of differences across federal states. Moreover, our questionnaire exclusively examined sociodemographic characteristics and did not explore political viewpoints or reasons for vaccine hesitancy. In the analysis, we compared proportions of vaccinated study participants with external information on voting, this approach can be subject to ecological fallacy. On the positive side, our study included a large sample size and provided regional-level data. We systematically recruited participants using a population-based approach, which differs from typical web-based studies.
5. Conclusions
In summary, our analysis indicates that regional differences in the uptake of the studied vaccinations in Germany cannot be attributed to differences in sociodemographic factors alone. Instead, we observed different regional patterns after adjustment for sociodemographic data, and in the two federal states for which we had comprehensive regional coverage data. We also observed correlations between support of political parties and regional vaccination uptake. It appears that political stances and individual choices are rather intertwined, but the study used only ecological analysis for the assessment of this relation.
Author Contributions
Conceptualization: B.K., R.M., C.G; Data analysis: B.K., S.D.; interpretation: B.K., M.H.S., R.M., C.G., writing—original draft preparation: B.K., M.H.S., R.M., C.G.; writing—review and editing: all authors; supervision, R.M., C.G.; All authors have read and agreed to the published version of the manuscript.
Funding
There was no specific funding for the conducted survey. The DigiHero study is funded by internal resources of the Medical Faculty of the Martin Luther University Halle-Wittenberg and part of the recruitment was co-funded by the Ministry of Economy, Science and Digitalization of the Federal State of Saxony-Anhalt (Germany).
Data Availability Statement
The anonymized data reported in this study can be obtained from the corresponding author upon request. The dataset includes individual data and an additional data dictionary will be provided. The beginning of data availability starts with the date of publication and the authors will support any requests in the three following years. Data requests should include a proposal for the planned analyses. Decisions will be made according to data use by the access committee of the DigiHero study, and data transfer will require a signed data access agreement.
Acknowledgments
We thank all DigiHero participants for their efforts and contributions. Moreover, we thank Oliver Purschke, Mareike Kunze and Anja Broda for excellent technical assistance.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Attia, S.; Mausbach, K.; Klugar, M.; Howaldt, H.P.; Riad, A. Prevalence and Drivers of COVID-19 Vaccine Booster Hesitancy Among German University Students and Employees. Front Public Health. 2022, 10, 846861. [Google Scholar] [CrossRef] [PubMed]
- Jackle, S.; Timmis, J.K. Left-Right-Position, party affiliation and regional differences explain low COVID-19 vaccination rates in Germany. Microb Biotechnol. 2023, 16, 662–677. [Google Scholar] [CrossRef] [PubMed]
- Galagali, P.M.; Kinikar, A.A.; Kumar, V.S. Vaccine Hesitancy: Obstacles and Challenges. Curr Pediatr Rep. 2022, 10, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Lane, S.; MacDonald, N.E.; Marti, M.; Dumolard, L. Vaccine hesitancy around the globe: Analysis of three years of WHO/UNICEF Joint Reporting Form data-2015-2017. Vaccine. 2018, 36, 3861–3867. [Google Scholar] [CrossRef] [PubMed]
- Omer, S.B.; Salmon, D.A.; Orenstein, W.A.; deHart, M.P.; Halsey, N. Vaccine refusal, mandatory immunization, and the risks of vaccine-preventable diseases. N Engl J Med. 2009, 360, 1981–1988. [Google Scholar] [CrossRef]
- Larson, H.J.; Mnookin, S. Trust and Confidence in Vaccines: Tales of Three Vaccines, Lessons for Others. 2016, 529–540.
- Tizard, I.R. Safety and sexual promiscuity: Hepatitis B, human papilloma virus, and influenza vaccines. 2023, 281–292.
- Sorell, T.; Butler, J. The Politics of Covid Vaccine Hesitancy and Opposition. Polit Q. 2022, 93, 347–351. [Google Scholar] [CrossRef]
- Bundesministerium für Gesundheit. Current vaccination status. [Available from: https://impfdashboard.de/en/.
- Robert Koch Institute. Monitoring Des COVID-19-Impfgeschehens in Deutschland 2022 [Available from: https://www.rki.de/DE/Content/Infekt/Impfen/ImpfungenAZ/COVID-19/Monatsberichte/2022-07-07.pdf?__blob=publicationFile.
- Rieck T, Steffen A, Schmid-Küpke N, Feig M, Wichmann O, Siedler A. Impfquoten bei Erwachsenen in Deutschland–Aktuelles aus der KV-Impfsurveillance und der Onlinebefragung von Krankenhauspersonal OKaPII. 2020.
- Poethko-Muller C, Schmitz R. [Vaccination coverage in German adults: Results of the German Health Interview and Examination Survey for Adults (DEGS1)]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2013, 56, 845–857. [Google Scholar]
- Robert Koch Institut. Epidemiologisches Bulletin 2022 [Available from: https://www.rki.de/DE/Content/Infekt/EpidBull/Archiv/2022/Ausgaben/49_22.pdf?__blob=publicationFile.
- Gottschick C, Diexer S, Massag J, Klee B, Broda A, Purschke O; et al. Mental health in Germany in the first weeks of the Russo-Ukrainian war. BJPsych Open. 2023, 9, e66. [Google Scholar] [CrossRef]
- Organisation for Economic Co-operation and Development. Classifying Educational Programmes: Manual for ISCED-97 Implementation in OECD Countries. 1999.
- Sachsen, W. Waglergebnisse 2019 [Available from: https://www.wahlen.sachsen.de/landtagswahl-2019-informationen-und-downloads.html?_cp=%7B%22accordion-content-6555%22%3A%7B%220%22%3Atrue%7D%2C%22previousOpen%22%3A%7B%22group%22%3A%22accordion-content-6555%22%2C%22idx%22%3A0%7D%7D.
- Wahlergebnisse Sachsen-Anhalt. Statistisches Landesamt Sachsen-Anhalt - Wahl des 8. Landtages von Sachsen-Anhalt am 06. Juni 2021 2021 [Available from: https://wahlergebnisse.sachsen-anhalt.de/wahlen/lt21/erg/kreis/lt.15091.ergtab.php.
- Dasch, S.; Wachinger, J.; Barnighausen, T.; Chen, S.; McMahon, S.A. Deliberation, context, emotion and trust - understanding the dynamics of adults' COVID-19 vaccination decisions in Germany. BMC Public Health. 2023, 23, 136. [Google Scholar] [CrossRef]
- Lindholt, M.F.; Jorgensen, F.; Bor, A.; Petersen, M.B. Public acceptance of COVID-19 vaccines: Cross-national evidence on levels and individual-level predictors using observational data. BMJ Open. 2021, 11, e048172. [Google Scholar] [CrossRef]
- Murphy J, Vallieres F, Bentall RP, Shevlin M, McBride O, Hartman TK; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat Commun. 2021, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Desson, Z.; Kauer, L.; Otten, T.; Peters, J.W.; Paolucci, F. Finding the way forward: COVID-19 vaccination progress in Germany, Austria and Switzerland. Health Policy Technol. 2022, 11, 100584. [Google Scholar] [CrossRef] [PubMed]
- Steinert, J.I.; Sternberg, H.; Prince, H.; Fasolo, B.; Galizzi, M.M.; Buthe, T.; et al. COVID-19 vaccine hesitancy in eight European countries: Prevalence, determinants, and heterogeneity. Sci Adv. 2022, 8, eabm9825. [Google Scholar] [CrossRef] [PubMed]
- Walach, H.; Ofner, M.; Ruof, V.; Herbig, M.; Klement, R.J. Why do people consent to receiving SARS-CoV-2 vaccinations? A representative survey in Germany. BMJ Open. 2022, 12, e060555. [Google Scholar] [CrossRef] [PubMed]
- Lenart, C.; Prager, M.; Sachs, M.; Steininger, C.; Fernandes, C.; Thannesberger, J. Tackling Vaccine Hesitancy and Increasing Vaccine Willingness Among Parents of Unvaccinated Children in Austria. International Journal of Public Health. 2023, 68. [Google Scholar] [CrossRef] [PubMed]
- Srivastav, A.; Lu, P.J.; Amaya, A.; Dever, J.A.; Stanley, M.; Franks, J.L.; et al. Prevalence of influenza-specific vaccination hesitancy among adults in the United States, 2018. Vaccine. 2023, 41, 2572–2581. [Google Scholar] [CrossRef] [PubMed]
- Robert Koch Institute. Wochenberichte zu COVID-19 (bis 8.6.2023) 2023 [Available from: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Wochenbericht/Wochenberichte_Tab.html?nn=13490888&cms_gtp=16396118_list%253D2.
- Altarawneh, H.N.; Chemaitelly, H.; Hasan, M.R.; Ayoub, H.H.; Qassim, S.; AlMukdad, S.; et al. Protection against the Omicron Variant from Previous SARS-CoV-2 Infection. N Engl J Med. 2022, 386, 1288–1290. [Google Scholar] [CrossRef] [PubMed]
- Pather, S.; Madhi, S.A.; Cowling, B.J.; Moss, P.; Kamil, J.P.; Ciesek, S.; et al. SARS-CoV-2 Omicron variants: Burden of disease, impact on vaccine effectiveness and need for variant-adapted vaccines. Front Immunol. 2023, 14, 1130539. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Madewell, Z.J.; Liu, M.; Longini, I.M.; Yang, Y. Effectiveness of SARS-CoV-2 vaccines against Omicron infection and severe events: A systematic review and meta-analysis of test-negative design studies. Front Public Health. 2023, 11, 1195908. [Google Scholar] [CrossRef] [PubMed]
- Tamandjou Tchuem, C.R.; Auvigne, V.; Vaux, S.; Montagnat, C.; Paireau, J.; Monnier Besnard, S.; et al. Vaccine effectiveness and duration of protection of COVID-19 mRNA vaccines against Delta and Omicron BA.1 symptomatic and severe COVID-19 outcomes in adults aged 50 years and over in France. Vaccine. 2023, 41, 2280–2288. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Vaccine uptake by age for: (a) any SARS-CoV-2 Vaccination; (b) any SARS-CoV-2 Booster Vaccination; and (c) Influenza Vaccination; (splines model with continuous age).
Figure 1.
Vaccine uptake by age for: (a) any SARS-CoV-2 Vaccination; (b) any SARS-CoV-2 Booster Vaccination; and (c) Influenza Vaccination; (splines model with continuous age).
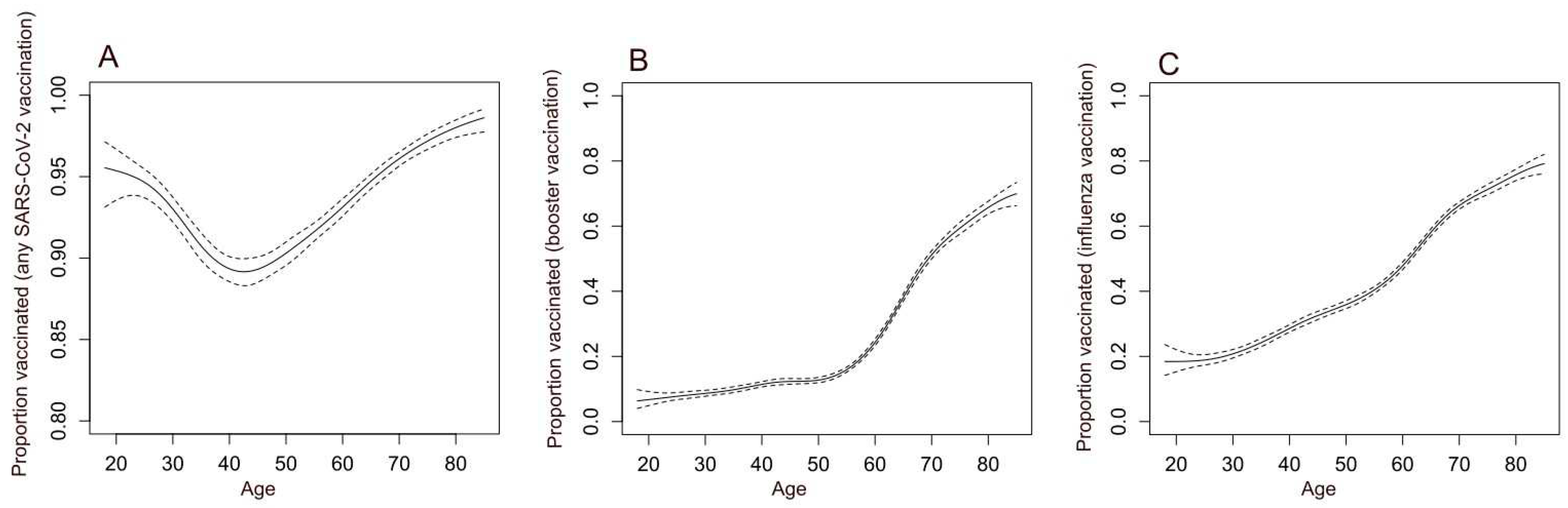
Figure 2.
Effects of adjusting for sociodemographic variables on regional variation in vaccine uptake across federal states in Germany for: (A) any SARS-CoV-2 Vaccination; (B) any SARS-CoV-2 Booster Vaccination; and (C) Influenza Vaccination (presented are odds ratios from logistic regression using Saxony-Anhalt as the reference category, with an increasing number of variables from Model 1 to 6, federal state, age (adjusted with splines), net equivalent household income, living in city (>100,000 inhabitants), education and sex.
Figure 2.
Effects of adjusting for sociodemographic variables on regional variation in vaccine uptake across federal states in Germany for: (A) any SARS-CoV-2 Vaccination; (B) any SARS-CoV-2 Booster Vaccination; and (C) Influenza Vaccination (presented are odds ratios from logistic regression using Saxony-Anhalt as the reference category, with an increasing number of variables from Model 1 to 6, federal state, age (adjusted with splines), net equivalent household income, living in city (>100,000 inhabitants), education and sex.
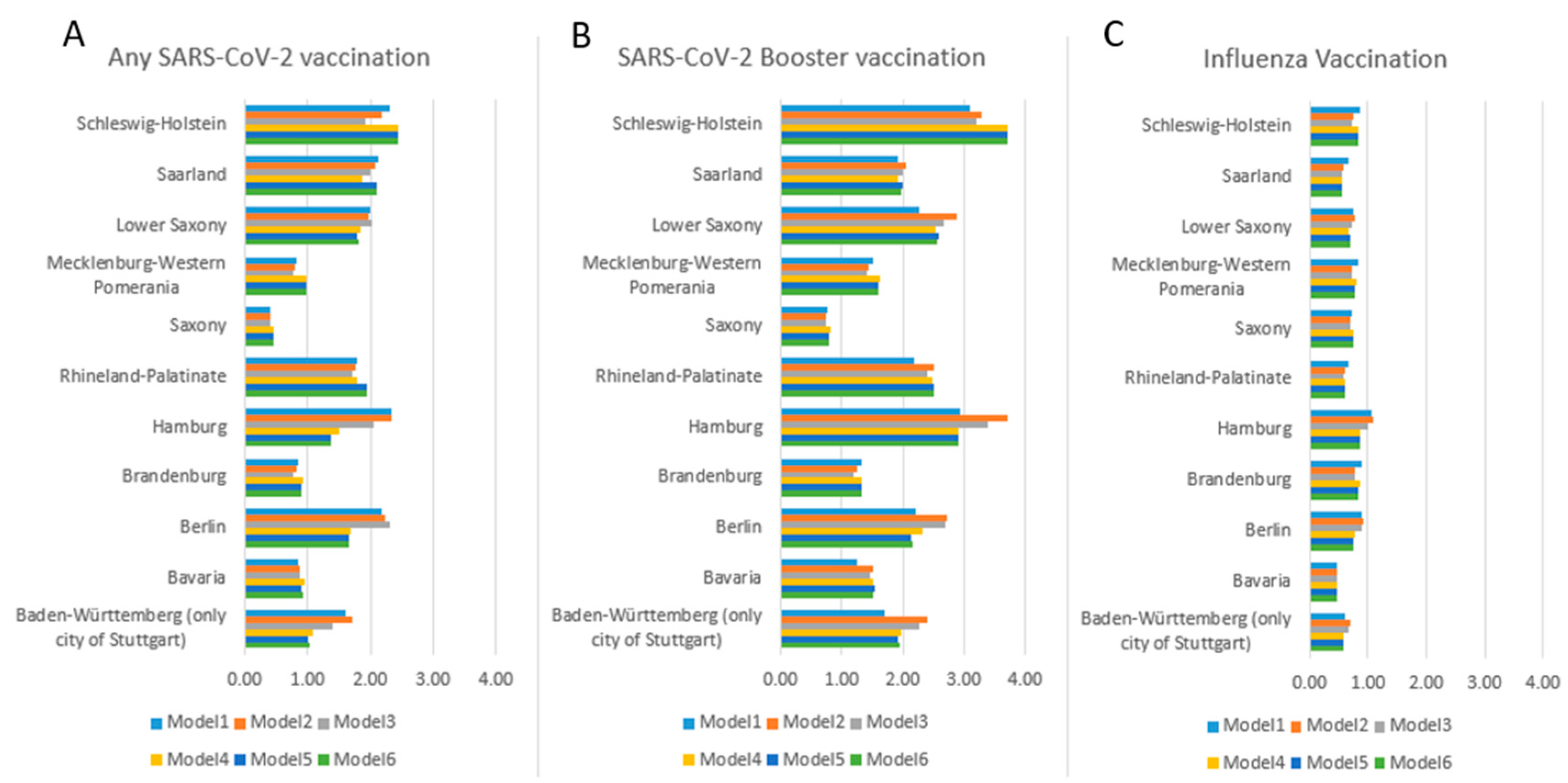
Figure 3.
Regional vaccination uptake within Saxony and Saxony-Anhalt, where participants from all administrative units (Landkreise) are included in the DigiHero study, for: (A) any SARS-CoV-2 Vaccination; (B) any SARS-CoV-2 Booster Vaccination; and (C) Influenza Vaccination (displayed is proportion vaccinated).
Figure 3.
Regional vaccination uptake within Saxony and Saxony-Anhalt, where participants from all administrative units (Landkreise) are included in the DigiHero study, for: (A) any SARS-CoV-2 Vaccination; (B) any SARS-CoV-2 Booster Vaccination; and (C) Influenza Vaccination (displayed is proportion vaccinated).
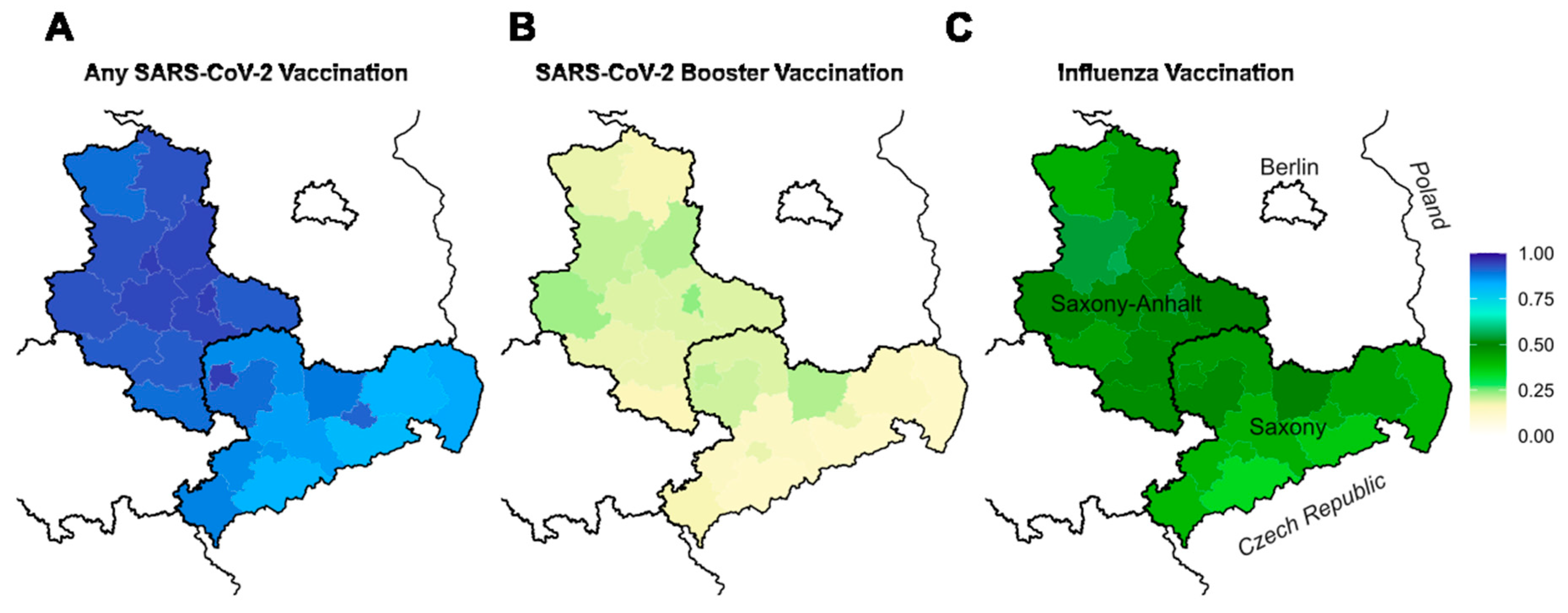
Figure 4.
Correlations between regional uptake of vaccines and political support for the seven strongest parties in Saxony and Saxony-Anhalt (SPD- Social Democratic Party of Germany; CDU- Christian Democratic Union of Germany; Freie Wähler- Free Voters; Die Grünen – The Green Party; Die Linke – The Left (Party); FDP – Democrats; SPD- Social Democratic Party of Germany).
Figure 4.
Correlations between regional uptake of vaccines and political support for the seven strongest parties in Saxony and Saxony-Anhalt (SPD- Social Democratic Party of Germany; CDU- Christian Democratic Union of Germany; Freie Wähler- Free Voters; Die Grünen – The Green Party; Die Linke – The Left (Party); FDP – Democrats; SPD- Social Democratic Party of Germany).
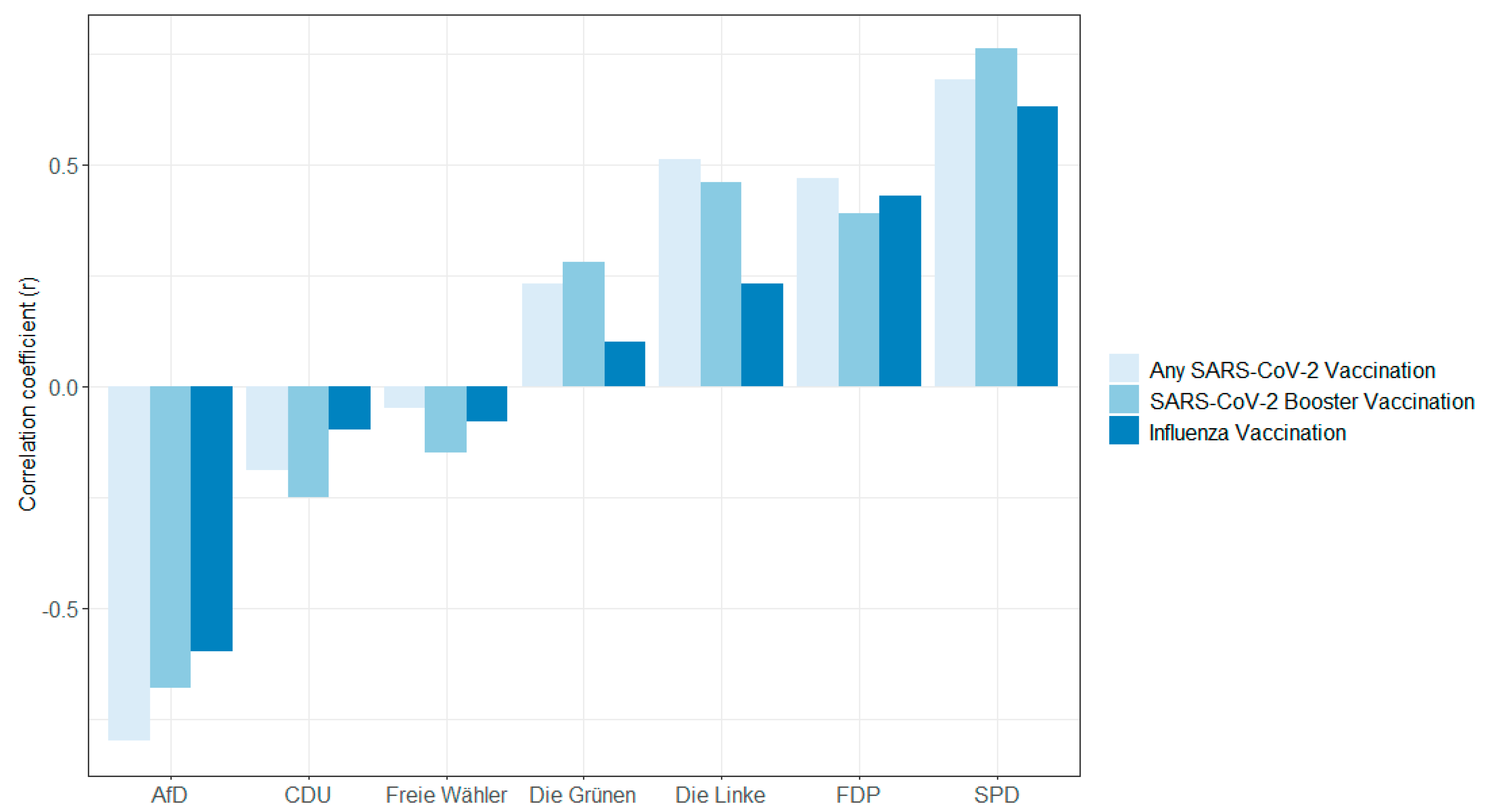
Figure 5.
Explained variance in regional uptake of vaccines by political support for the seven strongest parties in Saxony and Saxony-Anhalt (SPD- Social Democratic Party of Germany; CDU- Christian Democratic Union of Germany; Freie Wähler- Free Voters; Die Grünen – The Green Party; Die Linke – The Left (Party); FDP – Democrats; SPD- Social Democratic Party of Germany).
Figure 5.
Explained variance in regional uptake of vaccines by political support for the seven strongest parties in Saxony and Saxony-Anhalt (SPD- Social Democratic Party of Germany; CDU- Christian Democratic Union of Germany; Freie Wähler- Free Voters; Die Grünen – The Green Party; Die Linke – The Left (Party); FDP – Democrats; SPD- Social Democratic Party of Germany).
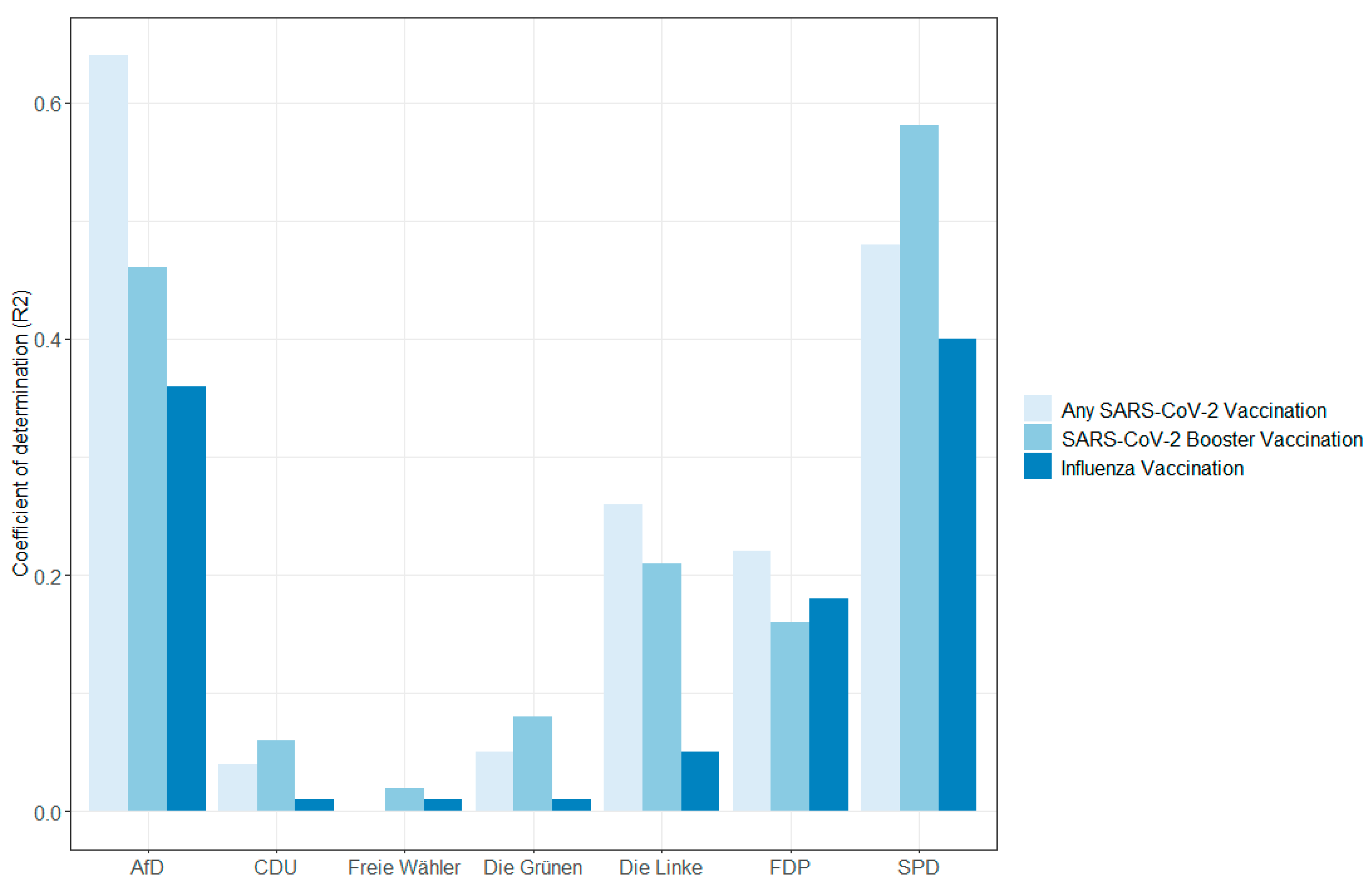

Table 1.
Sociodemographic characteristics of responders and non-responders.
| Characteristic | Value | RespondersN (n=37,078) | Responders% (95% CI) | Non-respondersN (n=33,476) | Non-responders % (95% CI) |
|---|---|---|---|---|---|
| Sex | Male | 14,216 | 38.3 (37.8-38.8) | 14,984 | 44.8 (44.2-45.3) |
| Female | 22,583 | 60.9 (60.4-61.4) | 17,308 | 51.7 (51.2-52.2) | |
| Diverse | 29 | 0.1 (0.1-0.1) | 77 | 0.2 (0.2-0.3) | |
| NA | 250 | 0.7 (0.6-0.8) | 1,107 | 3.3 (3.1-3.5) | |
| Age group | 18-29 | 2,633 | 7.1 (6.8-7.4) | 5,166 | 15.4 (15.0-15.8) |
| 30-39 | 5,079 | 13.7 (13.4-14.1) | 6,193 | 18.5 (18.1-18.9) | |
| 40-49 | 6,065 | 16.4 (15.9-16.7) | 5,499 | 16.4 (16.0-16.8) | |
| 50-59 | 9,241 | 24.9 (24.5-25.4) | 6,264 | 18.7 (18.3-19.1) | |
| 60-69 | 8,831 | 23.8 (23.3-24.3) | 5,327 | 15.9 (15.5-16.3) | |
| 70-79 | 4,023 | 10.9 (10.5-11.2) | 2,990 | 8.9 (8.6-9.2) | |
| 80+ | 890 | 2.4 (2.2-2.6) | 854 | 2.6 (2.4-2.7) | |
| NA | 316 | 0.9 (0.8-0.9) | 1,183 | 3.5 (3.3-3.7) | |
| Educationa | Low | 840 | 2.3 (2.1-2.4) | 2,177 | 6.5 (6.2-6.8) |
| Medium | 10,714 | 28.9 (28.4-29.4) | 10,223 | 30.5 (30.0-31.0) | |
| High | 23,319 | 62.9 (62.4-63.4) | 18,396 | 54.9 (54.4-55.5) | |
| NA | 2,205 | 5.9 (5.7-6.2) | 2,680 | 8.0 (7.7-8.3) | |
| Net household equivalent incomeb | Below 1250€ | 3,607 | 9.8 (9.4-10.0) | 4,958 | 14.8 (14.4-15.2) |
| 1250- <1750€ | 7,966 | 21.5 (21.1-21.9) | 7,229 | 21.6 (21.2-22.0) | |
| 1750- <2250€ | 5,061 | 13.6 (13.3-14.0) | 4,405 | 13.2 (12.8-13.5) | |
| 2250- <3000€ | 9,170 | 24.7 (24.3-25.2) | 7,115 | 21.2 (20.8-21.7) | |
| 3000- <4000€ | 7,568 | 20.4 (20.0-20.1) | 5,089 | 15.2 (14.8-15.6) | |
| 4000- <5000€ | 293 | 0.8 (0.7-0.9) | 200 | 0.6 (0.5-0.7) | |
| 5000€+ | 223 | 0.6 (0.5-0.7) | 154 | 0.5 (0.4-0.5) | |
| NA | 3,190 | 8.6 (8.3-8.9) | 4,326 | 12.9 (12.6-13.3) | |
| Born in Germany | Yes | 35,678 | 96.2 (96.0-96.4) | 30,866 | 92.2 (91.9-92.4) |
| No | 1,165 | 3.1 (2.9-3.3) | 1,507 | 4.5 (4.3-4.7) | |
| NA | 235 | 0.6 (0.6-0.7) | 1,103 | 3.3 (3.1-3.5) | |
| Living in a city > 100,000 | Yes | 13,210 | 35.6 (35.1-36.1) | 13,084 | 39.0 (38.6-39.6) |
| No | 23,322 | 62.9 (62.4-63.4) | 19,731 | 58.9 (58.4-59.5) | |
| NA | 546 | 1.5 (1.4-1.6) | 661 | 1.9 (1.8-2.1) | |
| Federal state | Saxony-Anhalt | 9,225 | 24.9 (24.4-25.3) | 10,201 | 30.5 (29.9-30.9) |
| Saxony | 7,633 | 20.6 (20.2-21.0) | 7,143 | 21.3 (20.9-21.8) | |
| Baden-Württemberg (only city of Stuttgart) | 459 | 1.2 (1.1-1.4) | 518 | 1.6 (1.4-1.7) | |
| Bavaria | 3,329 | 9.0 (8.7-9.3) | 3,675 | 10.9 (10.6-11.3) | |
| Berlin | 479 | 1.3 (1.2-1.4) | 456 | 1.4 (1.2-1.5) | |
| Brandenburg | 3,272 | 8.8 (8.5-9.1) | 2,425 | 7.2 (6.9-7.5) | |
| Hamburg | 509 | 1.4 (1.3-1.5) | 501 | 1.5 (1.4-1.6) | |
| Rhineland-Palatinate | 4,352 | 11.7 (11.4-12.1) | 3,676 | 10.9 (10.6-11.3) | |
| Mecklenburg-Western Pomerania | 2,071 | 5.6 (5.4-5.8) | 1,456 | 4.3 (4.1-4.6) | |
| Lower Saxony | 1,816 | 4.9 (4.7-5.1) | 999 | 2.9 (2.8-3.2) | |
| Saarland | 1,134 | 3.1 (2.9-3.2) | 560 | 1.7 (1.5-1.8) | |
| Schleswig-Holstein | 2,162 | 5.8 (5.6-6.1) | 1,136 | 3.4 (3.2-3.6) | |
| Other | 91 | 0.2 (0.2-0.3) | 69 | 0.2 (0.2-0.3) | |
| NA | 546 | 1.5 (1.4-1.6) | 661 | 1.9 (1.8-2.1) |
*CI – confidence interval; aWe categorized education based on the International Standard Classification of Education (ISCED-97) [15]. bIn the baseline questionnaire, we inquired about the net household income, providing seven income categories in Euro. To determine the net household equivalent income, we divided the mean of each income category by the sum of the household weights. Household weights were calculated using the following criteria: the first adult was assigned a weight of “1”, while all other adults (individuals aged 14 and above) held a weight of “0.5”, and children were assigned a weight of “0.3”. The resulting value was then categorized using the initial seven income categories.
Table 2.
Vaccination uptake for any SARS-CoV-2 vaccinations, SARS-CoV-2 booster vaccinations, and influenza vaccinations.
Table 2.
Vaccination uptake for any SARS-CoV-2 vaccinations, SARS-CoV-2 booster vaccinations, and influenza vaccinations.
| Characteristics | Value | Any SARS-CoV-2 vaccination% (95% CI) | SARS-CoV-2 booster vaccination% (95% CI) | Influenza vaccination % (95% CI) |
|---|---|---|---|---|
| Sex | Male | 93.5 (93.0-93.9) | 31.8 (31.1-32.6) | 47.8 (46.9-48.6) |
| Female | 92.5 (92.1-92.8) | 21.6 (21.1-22.2) | 41.8 (41.2-42.5) | |
| Diverse | 93.1 (75.8-98.8) | 20.7 (8.7-40.3) | 27.6 (13.4-47.5) | |
| NA | 90.4 (85.9-93.6) | 26.8 (21.5-32.8) | 41.6 (35.5-47.9) | |
| Age group | 18-29 | 94.7 (93.7-95.5) | 8.1 (7.1-9.2) | 19.6 (18.1-21.2) |
| 30-39 | 90.5 (89.7-91.2) | 10.1 (9.3-11.0) | 24.9 (23.7-26.1) | |
| 40-49 | 89.6 (88.8-90.3) | 12.1 (11.4-13.0) | 32.9 (31.8-34.2) | |
| 50-59 | 91.8 (91.2-92.3) | 16.5 (15.8-17.3) | 40.9 (39.9-41.9) | |
| 60-69 | 94.7 (94.2-95.2) | 39.7 (38.7-40.7) | 58.4 (57.3-59.4) | |
| 70-79 | 96.8 (96.2-97.3) | 57.3 (55.7-58.8) | 69.7 (68.2-71.1) | |
| 80+ | 98.5 (97.4-99.2) | 68.7 (65.5-71.7) | 77.6 (74.7-80.3) | |
| NA | 87.9 (83.7-91.2) | 21.2 (16.9-26.2) | 42.7 (37.3-48.4) | |
| Education | Low | 96.1 (94.5-97.2) | 9.4 (7.6-11.6) | 21.9 (19.1-24.9) |
| Medium | 90.7 (90.1-91.2) | 21.8 (21.0-22.6) | 38.4 (37.5-39.4) | |
| High | 93.9 (93.7-94.3) | 27.8 (27.2-28.3) | 47.8 (47.2-48.5) | |
| NA | 89.7 (88.3-90.9) | 26.7 (24.8-28.6) | ||
| Net equivalent income | Below 1250€ | 88.9 (87.7-89.9) | 17.4 (16.2-18.7) | 33.1 (31.6-34.7) |
| 1250- <1750€ | 91.5 (90.8-92.1) | 26.3 (25.3-27.3) | 45.0 (43.9-46.1) | |
| 1750- <2250€ | 91.7 (90.9-92.4) | 16.6 (15.6-17.7) | 36.6 (35.2-37.9) | |
| 2250- <3000€ | 94.2 (93.7-94.7) | 26.5 (25.6-27.5) | 46.4 (45.4-47.4) | |
| 3000- <4000€ | 95.9 (95.5-96.4) | 33.6 (32.5-34.7) | 51.0 (49.9-52.2) | |
| 4000- <5000€ | 95.9 (92.8-97.8) | 30.0 (24.9-35.7) | 50.5 (44.6-56.4) | |
| 5000€+ | 95.9 (92.2-98.0) | 33.2 (27.1-39.8) | 50.7 (43.9-57.4) | |
| NA | 90.7 (89.6-91.6) | 24.4 (22.9-25.9) | 41.9 (40.2-43.7) | |
| Born in Germany | Yes | 92.8 (92.6-93.1) | 25.3 (24.9-25.8) | 44.1 (43.6-44.6) |
| No | 94.2 (92.6-95.4) | 32.9 (30.2-35.7) | 43.2 (40.3-46.1) | |
| NA | 86.4 (81.2-90.4) | 23.4 (18.3-29.4) | 43.4 (37.0-50.0) | |
| Living in a city > 100,000 | Yes | 95.4 (95.0-95.8) | 27.5 (67.7-28.3) | 46.4 (45.5-47.2) |
| No | 91.4 (91.0-91.8) | 24.5 (23.9-25.1) | 42.8 (42.2-43.5) | |
| NA | 91.8 (89.0-93.9) | 22.9 (19.5-26.7) | 43.8 (39.6-48.1) | |
| Federal state | Saxony-Anhalt | 93.8 (93.2-94.3) | 20.1 (19.3-20.9) | 50.3 (49.3-51.4) |
| Saxony | 86.2 (85.3-86.9) | 16.3 (15.5-17.2) | 41.9 (40.8-43.0) | |
| Baden-Württemberg (only Stuttgart) | 96.1 (93.8-97.6) | 30.0 (25.9-34.5) | 38.8 (34.3-43.4) | |
| Bavaria | 92.8 (91.9-93.7) | 24.1 (22.7-25.6) | 32.5 (30.9-34.1) | |
| Berlin | 97.1 (95.0-98.3) | 35.7 (31.4-40.2) | 47.8 (43.2-52.4) | |
| Brandenburg | 92.8 (91.9-93.7) | 24.9 (23.5-26.5) | 47.4 (45.6-49.1) | |
| Hamburg | 97.2 (95.3-98.4) | 42.4 (38.1-46.9) | 52.1 (47.6-56.4) | |
| Rhineland-Palatinate | 96.4 (95.8-96.9) | 35.4 (33.9-36.9) | 40.2 (38.8-41.7) | |
| Mecklenburg-Western Pomerania | 92.6 (91.4-93.7) | 27.6 (25.7-29.6) | 45.3 (43.2-47.5) | |
| Lower Saxony | 96.9 (95.9-97.5) | 36.3 (34.1-38.6) | 43.3 (41.0-45.7) | |
| Saarland | 97.0 (95.8-97.9) | 32.4 (29.7-35.3) | 39.9 (37.1-42.9) | |
| Schleswig-Holstein | 97.2 (96.4-97.9) | 43.8 (41.7-45.9) | 46.7 (44.6-48.8) | |
| Other | 97.8 (91.5-99.6) | 25.3 (17.0-35.7) | 26.4 (17.9-36.8) | |
| NA | 91.8 (89.0-93.9) | 22.9 (19.5-26.7) | 43.8 (39.6-48.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



