
Submitted:
20 September 2023
Posted:
22 September 2023
You are already at the latest version
Abstract
Polycystic ovary syndrome (PCOS) is a prevalent condition characterized by manifestations that can influence self-image and potentially result in psychological distress; however, data from literature on sexual function (SF) in PCOS women are contradictory. We aimed to evaluate sexual dysfunction (SD) in PCOS women by carrying out a systematic review and meta-analysis, using the gold-standard assessment tool SD-diagnosis (Female Sexual Function Index:FSFI). Seven databases were analyzed until August-2023; study quality was assessed by risk of bias and Newcastle Ottawa Scale. Our analysis encompassed 25 case-control studies (9933 women). PCOS group presented significantly lower scores in arousal (MD= -0.36 CI95%-0.60;-0.11), lubrication (MD= -0.52 CI95%-0.75;-0.28), orgasm (MD= -0.39 CI95%-0.57;-0.20), satisfaction (MD= -0.32 CI95%-0.50;-0.14) and pain subdomains (MD= -0.46 CI95%-0.75;-0.16), as in overall FSFI score (MD= -2.27 CI95%-3.23;-1.31). Overweight/obese (OW/O) patients exhibited significantly higher overall FSFI than OW/O controls (MD=1.98 CI95%0.68;3.27), particularly in lubrication (MD= -0.34), orgasm (MD= -0.26) and satisfaction (MD= -0.25) subdomains. These findings offer insights regarding SD in PCOS women and emphasize the need to incorporate SF assessment into multidisciplinary care. By this way, PCOS can be also considered a gateway diagnosis to other long-term consequences. Further research should focus on controlling variables, as ethnicity, culture, religion and economic disparities.
Keywords:
Stein-Leventhal Syndrome
; Polycystic Ovary Syndrome
; Sexuality
; Sexual Activity
; Sexual Dysfunction
; Female Sexual Function Index
; Sexual Function
; Sexual Disorders
; Sexual Behavior
; Meta-analysis.
1. Introduction
Polycystic ovary syndrome (PCOS) is one of the most common endocrine disorders during reproductive age, with prevalence ranging between 5 to 20%, depending on the diagnostic criteria [1, 2]. This entity is a heterogeneous disorder defined by a combination of clinical hirsutism or biochemical hyperandrogenism, chronic oligo-anovulation and polycystic ovarian morphology on ultrasound. After excluding other hyperandrogenic disorders, the diagnostic is based on expert consensuses: US National Institutes of Health (NIH) in 1990 [3], and the Rotterdam consensus, organized by the American Society for Reproductive Medicine (ASRM) and the European Society of Human Reproduction and Embryology (ESHRE), in 2003 [1, 4].
The clinical presentation of PCOS arises from hyperandrogenism, giving rise to symptoms like acne, seborrhea and hirsutism, as well as menstrual irregularities, such as oligomenorrhea or amenorrhea and infertility. This syndrome is further linked to several enduring health risks, including metabolic syndrome, insulin resistance, dyslipidemia and obesity [5]. Together, these factors collectively contribute to a detrimental effect on a woman's self-perceived body image, ultimately leading to a sense of disconnection from her feminine identity. This incongruity arises from the contrast between societal ideals of feminine body image and the physical changes experienced by PCOS women [6].
While PCOS is commonly recognized for its metabolic and cosmetic effects, its psychological repercussions are increasingly coming to light. These encompass distress, anxiety, depression, impaired self-esteem and decreased body satisfaction; and, the severity of PCOS symptoms is likely related to self-esteem, trait anxiety and the pressures of lifestyle factors [7, 8]. Given the established link between psychological well-being and sexual function (SF), it is crucial to comprehensively assess the presence of any interconnected concerns.
Sexual dysfunction (SD), a prevalent condition affecting around 40% of women, is marked by difficulties in fulfilling sexual activities [9]. It arises from a complex interplay of cultural, medical, biological, psychological and relational factors [10]. The gold-standard assessment tool SD-diagnosis is the Female Sexual Function Index (FSFI), a 19-item self-report questionnaire that evaluates six domains: desire, arousal, lubrication, orgasm, pain and satisfaction. A total score below 25 on the FSFI suggests SD [11]. The inquiry into whether SD might exhibit a higher prevalence among PCOS patients has been a subject of discussion. For PCOS patients, multiple elements could contribute to SD, including clinical manifestations of hyperandrogenism, insulin resistance, obesity, irregular menstrual cycles, infertility and even psychological factors [10]. Therefore, comprehending the intricate connections between these components and SD in PCOS is of paramount importance to enhance the well-being of these patients.
The potential correlation between hyperandrogenemia and SF has been explored. Given that androgen excess is one of the hallmarks of PCOS, understanding the relationship between them is crucial. While some studies suggest a potential protective effect [12, 13], others revealed the opposite [14-17]. However, due to controversial existing data on this topic, definitive conclusions cannot be drawn.
Controversial evidence exists when comparing the frequency of SD among PCOS patients [16, 18-22], possibly attributed to the relatively limited number of available works. Even more, a notable challenge arises from the fact that many studies used distinct assessment questionnaires to diagnose SD [16, 18-20]. The divergence in evaluation methods not only makes it arduous to achieve a standardized outcome, as also leads to divergent interpretations of scores, complicating the process of comparing outcome across different studies. The meta-analysis by Pastoor et al. (2018), that included 18 works, employed a range of questionaries with validated scales to assess SD, such as VAS, ISS, McCoy-FSQ, FSFI, CSFQ, SQ-F, FSDQ and MSQ [21]. The complete analysis showed no significant differences in SD prevalence among PCOS women; however, when FSFI scale was solely used, it showed a significant outcome [21]. In opposite, a prior meta-analysis conducted by Murgel et al. (2019), which encompassed four studies using only the FSFI scale, did not yield evidence substantiating this correlation [22].
Recognizing the paramount importance of SF in overall quality of life, there has been an increasing interest in comprehensively elucidating this matter. In this way, with the newest ample body of research in this field, the primary aim of the present study is to reexamine the critical issue of the potential association between SD and PCOS through a novel systematic review and meta-analysis, and using the well-established gold-standard diagnostic tools to assess SD and PCOS - FSFI scale and modified Rotterdam consensus, respectively [4, 8, 11]. Through these endeavors, we seek to address the aforementioned knowledge gap, thereby shedding light on an important facet of women's health and providing updates into multiprofessional care for women impacted by PCOS.
2. Materials and Methods
This study conducted a systematic review and meta-analysis to investigate the prevalence of SD in PCOS women. The systematic review was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analysis: PRISMA [23], and was registered on the PROSPERO platform (ID 456871). The meta-analysis provided a quantitative synthesis of the data, yielding a more precise estimate of the overall prevalence of SD in PCOS women. By integrating these methodologies, we obtained a robust understanding of the association between PCOS and SF, with implications for clinical practice and future researches.
2.1. Data Sources
A systematic search of all medical literature published from January 2013 to August 2023 was performed in the PubMed/Medline, Embase, Lilacs, Cinahl, PsycINFO, Google Scholar and Cochrane databases using Medical Subject Headings (Table 1).
Additionally, we also reviewed the references of the selected articles obtained from the initially database search, identifying any study that might not have been included. When the articles were not available or when the published data were insufficient, attempts were made to contact the respective authors via email to obtain the full articles and detailed data.
2.2. PICO Question and Search Strategy
Eligibility criteria using the Population-Intervention-Comparison-Outcome (PICO) framework was expressed as follows: P (patient) for PCOS patient; I (intervention) for the questionnaire to evaluate sexuality; C (comparison) for the control group; and O (outcome) for the relationship between SD and PCOS.
To be included in the analysis, studies had to fulfill the following criteria: studies that used FSFI scale for assessing sexuality in PCOS patients and diagnosis of PCOS according to the modified Rotterdam criteria [1].
2.3. Study Selection and Quality Assessment
Study selection and the assessment of titles and abstracts were conducted by the strict observation of the inclusion and exclusion criteria. Two independent reviewers selected the titles and abstracts of all identified articles. Any discrepancies were resolved by the third reviewer. In the next stage, the selected articles were critically assessed for inclusion or non-inclusion in this review.
Visual inspection of funnel plot asymmetry was performed to assess potential publication bias. The Newcastle Ottawa Scale was used to assess the quality of included case-control and cohort studies in this systematic review, classifying them as: a) good quality 7-8 points, b) fair quality 3-6 points and c) poor quality 0-2 points [24].
2.4. Data Extraction
The information extracted from the articles is presented in Table 2, organized based on author name, publication date, countries, study design, sample sizes, participant ages, BMI and outcomes.
2.5. Statistical Analysis
Meta-analyses were performed using R software version 4.0, jointly with the metapackage [50]. We applied the quantile estimation method to sample mean and to te standard deviation, that reported median and interquartile ranges [51]. The random and fixed effects models for the meta-analysis, depending on the heterogeneity among the studies, was applied. The I2 statistic was applied to quantify heterogeneity [52], and when equal or greater than 50%, indicated a large amount of heterogeneity and random-effect; otherwise, the fixed-effect model was considered.
The studies were functionally different and involved different participants and settings. Accordingly, we used a random-effects model that allowed more heterogeneity. Forest plots were created to display the meta-analysis findings. The funnel plots and Begg tests were used to explore publication bias. Also, we performed the sensitivity analysis to test the robustness of the findings. All statistical tests were two sided, and the significance level was fixed at 5% for all tests.
3. Results
3.1. Literature Search
The search strategies yielded 5919 articles. Among them, 2917 were duplicates, 548 did not meet the PICO requirements, 2417 did not use the FSFI scale and 9 were incomplete. Further, two records were added through the examination of references in the previously selected articles (Figure 1).
3.2. Risk of Bias Assessment and Overall Quality of Included Studies in this Systematic Review (n = 28)
The studies exhibited heterogeneity and were found to have a high risk of bias, as indicated by visual assessment of funnel plots (Figure 2a–h).
3.3. Study Characteristics
Twenty-five studies (10 from Iran, 6 from Turkey, 3 from Brazil, 1 from Germany, 1 from Georgia, 1 from Poland, 1 from Spain, 1 from Greece and 1 from Bulgaria) were included in this meta-analysis, comprising a total of 9933 women.
3.4. Overall FSFI and subdomains scores of Included Studies in this Systematic Review (n = 28)
Twenty-eight studies assessed SD through the overall FSFI score [5, 9, 10, 25-49]; and, among them, 12 were significantly lower in PCOS women than controls [5, 10, 25-31, 35-37]. Twenty-four studies analyzed the FSFI subdomains scores [5, 9, 10, 25-31, 35-39, 41-49]. Orgasm, lubrication, satisfaction, arousal, desire and pain subdomains were significantly lower in PCOS women than controls in 14 [9, 10, 27-31, 35-37, 44, 46, 48, 49], 15 [5, 10, 26-31, 35-37, 41, 46, 47, 49], 14 [5, 10, 27-31, 36-38, 43, 44, 46, 49], 13 [5, 26-28, 30, 31, 35-37, 41, 43, 46, 49], 7 [10, 28, 29, 35-37, 49] and 10 studies [5, 26, 28-30, 35-37, 41, 46], respectively.
3.5. Meta-analysis
Figure 3a shows the mean difference (MD) of studies that assessed SD through the overall FSFI score comparing PCOS group to controls, ranging from 15.1 to 29.9, and 17.8 to 29.9, respectively [5, 9, 10, 25-30, 35-48]. The pooled results revealed that overall FSFI score was significantly lower in PCOS women than controls (MD = -2.27 CI95% [-3.23; -1.31], p < 0.01; heterogeneity: I2 = 94%, 95%CI: 93%; 96%, p < 0.01), indicating a link between PCOS and SD.
Regarding the specific FSFI subscales, PCOS women had lower scores of arousal (MD = -0.36 CI95% [-0.60; -0.11], p < 0.01) (Figure 3b), lubrication (MD = -0.52 CI95% [-0.75; -0.28], p < 0.01) (Figure 3c), orgasm (MD = -0.39 CI95% [-0.57; -0.20], p < 0.01) (Figure 3d), satisfaction (MD = -0.32 CI95% [-0.50; -0.14], p < 0.01) (Figure 3e) and pain (MD = -0.46 CI95% [-0.75; -0.16], p < 0.01) (Figure 3f). Desire was also lower in PCOS group than controls, nevertheless it was not significantly different (MD = -0.15 CI95% [-0.35; 0.06], p = 0.16).
Figure 4 displays the MD of the studies that assessed SD through the overall FSFI scale in overweight/obese (OW/O) PCOS group and OW/O controls, ranging from 21.6 to 70.39, and 20.04 to 64.47, respectively [5, 9, 10, 14, 26-29, 31, 35-41, 43-46, 48] The combined findings indicated that overall FSFI scores were significantly higher in OW/O PCOS women than matched controls (MD = 1.98 CI95% [0.68; 3.27], p < 0.01; heterogeneity: I2 = 96%, CI95%: 95%; 97%, p < 0.01), particularly in lubrication (MD = -0.34; p < 0.01), orgasm (MD = -0.26; p = 0.01) and satisfaction (MD = -0.25; p = 0.5) domains.
4. Discussion
Since its initial description in 1935, PCOS has gained increasing recognition as a complex disorder. Beyond its long-term consequences, there's a growing awareness highlighting the interconnected psychosocial repercussions of its clinical manifestations. While some studies have indicated a higher prevalence of SD (up to 63.5%) among PCOS patients in comparison to the general population [31], others have not identified the same [19, 20]. To investigate this relationship, five meta-analyses were conducted [18-22]; however, this issue remains controversial.
This divergence in findings could arise from the fact that different questionnaires were employed to assess SD across these studies. For instance, Zhao et al. reviewed studies that applied FSFI scale, Sexual Functioning Questionnaire and Sexual Quotient-Female [20]; Thannickal et al. considered those using the VAS-sexual satisfaction scale [18], and Pastoor et al. included those that assessed SD from several scales, such as VAS, ISS, McCoy-FSQ, FSFI, CSFQ, SQ-F, FSDQ and MSQ [21]. Only the meta-analysis conducted by Loh et al. and Murgel et al. selected works that exclusively applied the FSFI scale [19, 22]. Hence, the use of different measurement questionaries could significantly complicate the process of comparing outcomes across different studies, thereby limiting the ability to reach definitive conclusions.
In this present meta-analysis involving the highest number of studies (25 case-control studies), we chose works that exclusively applied the FSFI assessment score, since it is recognized as the gold-standard assessment tool SD-diagnosis [11]. This selection not only enhanced the reliability and comparability of the results but also enabled us to achieve robustness conclusions.
Our data analysis indicated that PCOS women are more prone to experiencing SD compared to women without PCOS. When Pastoor et al. conducted a meta-analysis that evaluated SD across 18 studies that used several scales, they did not find a significant association. However, when they focused on the subset of 8 studies that assessed SD solely from FSFI scale, they found a statistically significant association [21]. The others meta-analyses did not achieve statistically significant differences between PCOS women and controls, possibly due to the limited number of studies, generally, less than 10 [18-20, 22].
In line with previous meta-analyses, our study supports the findings of reduced pain and satisfaction scores among PCOS group [19], as well as lower arousal and lubrication scores [20]; only desire domain was not significantly different. Despite experiencing reduced SF in other domains, PCOS women presented similar levels of sexual desire as women without PCOS [18-22]. While testosterone supplementation has generally been linked to increased desire and overall well-being [6], interestingly, it is not observed in PCOS patients, even among those with increased testosterone levels. Further, no improvement in sexual desire was observed even after the achievement of normal androgen levels in these patients, suggesting that disrupted endocrine function might not directly impact sexual desire [53]. In fact, the coexistence of hyperandrogenism and limited SF could suggest a "saturation" point for the influence of testosterone on libido. It seems that the impact of psychological and cognitive-emotional factors on SF in hyperandrogenic PCOS patients is more prominent than that of biological factors [6].
PCOS is driven by a vicious cycle of excessive androgens, amplifying LH-triggered androgen secretion. The insensitivity of the hypothalamic gonadotropin-releasing hormone (GnRH) pulse generator to the inhibitory effects of estrogen and progesterone, induced by androgens, leads to increased and rapid GnRH pulsing. This reduces FSH levels and subsequently inhibiting the growth of ovarian follicles [54]. This sequence can lead to estrogen deficiency and potential vaginal atrophy, which explains increased pain experienced by PCOS women, as demonstrated in this current study.
Increased androgen levels in PCOS have been recognized to induce both physical and psychological changes in affected women, rendering them more susceptible to develop depression and anxiety. These emotional factors can also exert a negative influence on their SF [34, 55, 56]. Additionally, the challenges of infertility add an additional layer of complexity to the issues faced by PCOS women, which is further exacerbated by the tendency to assign blame for infertility to the female partner within the relationship [28]. The pressures associated with the desire for parenthood also intensify feelings of frustration when the journey to conception becomes arduous. In light of this, Diamond et al. investigated the connection between PCOS and SD; through a comparison of PCOS and unexplained infertility (UI) groups, they revealed no significant disparities in total SF scores, measured by FSFI and Female Sexual Distress scales [43]. In essence, this suggests that SD in PCOS women might be a "side effect" of the frustration and emotional distress linked to their inability to conceive.
Frequently, PCOS women perceive themselves as less attractive, which could also impact their SF. This influence might be compounded by additional factors, such as obesity, since it is widely recognized as an independent risk factor for SD [57, 58]. To investigate this relationship, we compared OW/O PCOS women to similar controls (also OW/O). Contrary to common beliefs, the pooled results reveal that the OW/O PCOS group exhibited improved SF compared to their OW/O counterparts, particularly in lubrication, satisfaction and orgasm domains. We speculate that since increased weight is linked to an increase in estrogen levels, it facilitates improvement in lubrication, satisfaction and orgasm domains [6]. However, these findings should be interpreted cautiously, considering the potential bias in previous studies that suggested a negative link between SD and OW/O PCOS women thought an unmatched control group comparison [6, 59]. Thus, considering obesity as an independent risk factor for SD, the assumption that OW/O PCOS patients are inherently at a heightened risk of SD may require reconsideration.
There are limitations to consider in this research; firstly, the quality and availability of the studies included may vary, potentially leading to heterogeneity in the data. Moreover, the studies included in this analysis relied on self-report measures to assess SD, which are susceptible to recall bias and the influence of social desirability effects. Also, the majority of the included studies focused on adult women, limiting the generalizability of the findings to other age groups. However, there are strengths that should be highlighted. This meta-analysis encompasses a substantial number of studies, making it one of the largest in its field. Additionally, it is worth noting that our research aimed to standardize the selection criteria for studies inclusion; we exclusively selected studies that utilized the FSFI scale as an assessment tool for diagnosing SD and the modified Rotterdam criteria for diagnosing PCOS. These methodological refinements have contributed to achieving more robust and reliable conclusions.
In brief, our findings suggests that PCOS women are more prone to experiencing SD, particularly due to difficulties in arousal, lubrification, orgasm, satisfaction and pain subdomains. We further demonstrated that OW/O PCOS women exhibited better SF compared to controls, primarily in the lubrication, orgasm, and satisfaction subdomains. Upon diagnosis, in order to improve the quality of life, a comprehensive approach to management should encompasse aspects spanning reproductive, metabolic and psychological dimensions, as well as psychosexual therapy. Education, self-empowerment, multidisciplinary care and lifestyle interventions are given priority. By this way, PCOS can be considered a gateway diagnosis to also screen other long-term comorbidities. Future endeavors should involve higher-quality studies to shed light on distinct patient groups, while controlling for variables such as ethnicity, culture, religion, and economic disparities.
Author Contributions
Conceptualization: Bachega F.S. and Baracat E.C.; methodology: Bachega F.S., Baracat M.C., Simões R.D.S., Maciel G.A.R., Lobo R.A., Soares Júnior J.M. and Baracat E.C.; software: Simões R.D.S.; validation: Bachega F.S., Baracat M.C., Simões R.D.S., Maciel G.A.R., Lobo R.A., Soares Júnior J.M. and Baracat E.C.; formal analysis: Lobo R.A and Baracat E.C.; investigation: Bachega F.S., Baracat M.C., Simões R.D.S., Maciel G.A.R., Lobo R.A., Soares Júnior J.M. and Baracat E.C.; resources: Bachega F.S., Baracat M.C., Simões R.D.S., Maciel G.A.R., Lobo R.A., Soares Júnior J.M. and Baracat E.C.; data curation: Bachega F.S; writing—original draft preparation: Bachega F.S., Baracat M.C.; Maciel G.A.R., Soares Júnior J.M. and Baracat E.C.; writing—review and editing: Bachega F.S., Baracat M.C., Simões R.D.S., Maciel G.A.R., Lobo R.A., Soares Júnior J.M. and Baracat E.C.; visualization: Bachega F.S., Baracat M.C., Simões R.D.S., Maciel G.A.R., Lobo R.A., Soares Júnior J.M. and Baracat E.C.; supervision: Baracat M.C., Simões R.D.S., Maciel G.A.R., Lobo R.A., Soares Júnior J.M. and Baracat E.C.; project administration: Baracat E.C.
Funding
This research received no external funding.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to Vinicius Fernando Calsavara for statistical analysis support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rotterdam, E.A.-S.P.C.W.G. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril 2004, 81, 19–25. [Google Scholar]
- Baracat, E.C.; Baracat, M.C.P.; Jose, M.S., Jr. Are there new insights for the definition of PCOS? Gynecol Endocrinol 2022, 38, 703–704. [Google Scholar] [CrossRef]
- Hsu, M.-I.; Liou, T.-H.; Chou, S.-Y.; Chang, C.-Y.; Hsu, C.-S. Diagnostic criteria for polycystic ovary syndrome in Taiwanese Chinese women: comparison between Rotterdam 2003 and NIH 1990. Fertil. Steril. 2007, 88, 727–729. [Google Scholar] [CrossRef]
- Teede, H.J.; Tay, C.T.; E Laven, J.J.; Dokras, A.; Moran, L.J.; Piltonen, T.T.; Costello, M.F.; Boivin, J.; Redman, L.M.; A Boyle, J.; et al. Recommendations from the 2023 international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Eur. J. Endocrinol. 2023, 189, G43–G64. [Google Scholar] [CrossRef]
- Benetti-Pinto, C.L.; Ferreira, S.R.; Antunes, A., Jr.; Yela, D.A. The influence of body weight on sexual function and quality of life in women with polycystic ovary syndrome. Arch Gynecol Obstet 2015, 291, 451–455. [Google Scholar] [CrossRef]
- Daescu, A.C.; et al. Effects of Hormonal Profile, Weight, and Body Image on Sexual Function in Women with Polycystic Ovary Syndrome. Healthcare (Basel) 2023, 11. [Google Scholar] [CrossRef]
- Lobo, R.A.; Granger, L.R.; Paul, W.L.; Goebelsmann, U.; Mishell, D.R. Psychological stress and increases in urinary norepinephrine metabolites, platelet serotonin, and adrenal androgens in women with polycystic ovary syndrome. Am. J. Obstet. Gynecol. 1983, 145, 496–503. [Google Scholar] [CrossRef]
- Kogure, G.S.; Ribeiro, V.B.; Lopes, I.P.; Furtado, C.L.M.; Kodato, S.; de Sá, M.F.S.; Ferriani, R.A.; Lara, L.A.d.S.; dos Reis, R.M. Body image and its relationships with sexual functioning, anxiety, and depression in women with polycystic ovary syndrome. J. Affect. Disord. 2019, 253, 385–393. [Google Scholar] [CrossRef]
- Sene, A.A.; Tahmasbi, B.; Keypour, F.; Zamanian, H.; Golbabaei, F.; Amini-Tehrani, M. Differences in and Correlates of Sexual Function in Infertile Women with and without Polycystic Ovary Syndrome. International Journal of Fertility & Sterility 2021, 15, 65–72. [Google Scholar] [CrossRef]
- Tian, X.; Ruan, X.; Du, J.; Cheng, J.; Ju, R.; Mueck, A.O. Sexual function in Chinese women with different clinical phenotypes of polycystic ovary syndrome. Gynecol. Endocrinol. 2023, 39, 2221736. [Google Scholar] [CrossRef]
- Giraldi, A.; Rellini, A.; Pfaus, J.G.; Bitzer, J.; Laan, E.; Jannini, E.A.; Fugl-Meyer, A.R. Questionnaires for Assessment of Female Sexual Dysfunction: A Review and Proposal for a Standardized Screener. J. Sex. Med. 2011, 8, 2681–2706. [Google Scholar] [CrossRef]
- Veras, A.B.; Bruno, R.V.; de Avila, M.A.P.; Nardi, A.E. Sexual dysfunction in patients with polycystic ovary syndrome: clinical and hormonal correlations. Compr. Psychiatry 2011, 52, 486–489. [Google Scholar] [CrossRef]
- Månsson, M.; Norström, K.; Holte, J.; Landin-Wilhelmsen, K.; Dahlgren, E.; Landén, M. Sexuality and psychological wellbeing in women with polycystic ovary syndrome compared with healthy controls. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 155, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Elsenbruch, S.; Hahn, S.; Kowalsky, D.; Öffner, A.H.; Schedlowski, M.; Mann, K.; Janssen, O.E. Quality of Life, Psychosocial Well-Being, and Sexual Satisfaction in Women with Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2003, 88, 5801–5807. [Google Scholar] [CrossRef]
- Rellini, A.; Stratton, N.; Tonani, S.; Santamaria, V.; Brambilla, E.; Nappi, R. Differences in sexual desire between women with clinical versus biochemical signs of hyperandrogenism in polycystic ovarian syndrome. Horm. Behav. 2013, 63, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Castelo-Branco, C.; Naumova, I. Quality of life and sexual function in women with polycystic ovary syndrome: a comprehensive review. Gynecol. Endocrinol. 2020, 36, 96–103. [Google Scholar] [CrossRef]
- Fliegner, M.; Richter-Appelt, H.; Krupp, K.; Brunner, F. Sexual Function and Socio-Sexual Difficulties in Women with Polycystic Ovary Syndrome (PCOS). Geburtshilfe und Frauenheilkd. 2019, 79, 498–509. [Google Scholar] [CrossRef] [PubMed]
- Thannickal, A.; Brutocao, C.; Alsawas, M.; Morrow, A.; Zaiem, F.; Murad, M.H.; Chattha, A.J. Eating, sleeping and sexual function disorders in women with polycystic ovary syndrome (PCOS): A systematic review and meta-analysis. Clin. Endocrinol. 2020, 92, 338–349. [Google Scholar] [CrossRef]
- Yee, A.; Loh, H.S.; Kanagasundram, S.; Francis, B.; Lim, L.-L. Sexual dysfunction in polycystic ovary syndrome: a systematic review and meta-analysis. Hormones 2020, 19, 413–423. [Google Scholar] [CrossRef]
- Zhao, S.; Wang, J.; Xie, Q.; Luo, L.; Zhu, Z.; Liu, Y.; Luo, J.; Zhao, Z. Is polycystic ovary syndrome associated with risk of female sexual dysfunction? A systematic review and meta-analysis. Reprod. Biomed. Online 2019, 38, 979–989. [Google Scholar] [CrossRef] [PubMed]
- Pastoor, H.; Timman, R.; de Klerk, C.; Bramer, W.M.; Laan, E.T.; Laven, J.S. Sexual function in women with polycystic ovary syndrome: a systematic review and meta-analysis. Reprod. Biomed. Online 2018, 37, 750–760. [Google Scholar] [CrossRef]
- Murgel, A.C.F.; Simões, R.S.; Maciel, G.A.R.; Soares, J.M.; Baracat, E.C. Sexual Dysfunction in Women With Polycystic Ovary Syndrome: Systematic Review and Meta-Analysis. J. Sex. Med. 2019, 16, 542–550. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiology 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Basirat, Z.; Faramarzi, M.; Esmaelzadeh, S.; Firoozjai, S.A.; Mahouti, T.; Geraili, Z. Stress, Depression, Sexual Function, and Alexithymia in Infertile Females with and without Polycystic Ovary Syndrome: A Case-Control Study. Int J Fertil Steril 2019, 13, 203–208. [Google Scholar] [CrossRef]
- Bahadori, F.; Sadatmahalleh, S.J.; Montazeri, A.; Nasiri, M. Sexuality and psychological well-being in different polycystic ovary syndrome phenotypes compared with healthy controls: a cross-sectional study. BMC Women's Heal. 2022, 22, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mantzou, D.; Stamou, M.I.; Armeni, A.K.; Roupas, N.D.; Assimakopoulos, K.; Adonakis, G.; Georgopoulos, N.A.; Markantes, G.K. Impaired Sexual Function in Young Women with PCOS: The Detrimental Effect of Anovulation. J. Sex. Med. 2021, 18, 1872–1879. [Google Scholar] [CrossRef]
- Ashrafi, M.; Jahangiri, N.; Sadatmahalleh, S.J.; Mirzaei, N.; Hesari, N.G.; Rostami, F.; Mousavi, S.S.; Zeinaloo, M. Does prevalence of sexual dysfunction differ among the most common causes of infertility? A cross-sectional study. BMC Women's Heal. 2022, 22, 1–8. [Google Scholar] [CrossRef]
- Deniz, A.; Kehribar, D. Evaluation of sexual functions in infertile Women with Polycystic Ovary Syndrome. Niger. J. Clin. Pr. 2020, 23, 1548–1554. [Google Scholar] [CrossRef]
- Mojahed, B.S.; Ghajarzadeh, M.; Khammar, R.; Shahraki, Z. Depression, sexual function and sexual quality of life in women with polycystic ovary syndrome (PCOS) and healthy subjects. J. Ovarian Res. 2023, 16, 105. [Google Scholar] [CrossRef]
- Hashemi, S.; Tehrani, F.R.; Farahmand, M.; Khomami, M.B. Association of PCOS and Its Clinical Signs with Sexual Function among Iranian Women Affected by PCOS. J. Sex. Med. 2014, 11, 2508–2514. [Google Scholar] [CrossRef]
- Anger, J.T.; Brown, A.J.; Amundsen, C.L. Sexual Dysfunction in Women With Polycystic Ovary Syndrome: The Effects of Testosterone, Obesity, and Depression. J. Pelvic Med. Surg. 2007, 13, 119–124. [Google Scholar] [CrossRef]
- Eftekhar, T.; Sohrabvand, F.; Zabandan, N.; Shariat, M.; Haghollahi, F.; Ghahghaei-Nezamabadi, A. Sexual dysfunction in patients with polycystic ovary syndrome and its affected domains. Iran J Reprod Med 2014, 12, 539–546. [Google Scholar]
- Dashti, S.; A Latiff, L.; Hamid, H.A.; Sani, S.M.; Akhtari-Zavare, M.; Abu Bakar, A.S.; Sabri, N.A.I.B.; Ismail, M.; Esfehani, A.J. Sexual Dysfunction in Patients with Polycystic Ovary Syndrome in Malaysia. Asian Pac J Cancer Prev. 2016, 17, 3747–51. [Google Scholar]
- Aba, Y.A.; Şik, B.A. Body image and sexual function in women with polycystic ovary syndrome: a case-control study. Rev Assoc Med Bras (1992) 2022, 68, 1264–1269. [Google Scholar] [CrossRef]
- Daneshfar, Z.; Sadatmahalleh, S.J.; Jahangiri, N. Comparison of sexual function in infertile women with polycystic ovary syndrome and endometriosis: A cross-sectional study. Int. J. Reprod. Biomed. (IJRM) 2022, 20, 761–768. [Google Scholar] [CrossRef]
- Taghavi, S.-A.; Aramesh, S.; Azizi-Kutenaee, M.; Allan, H.; Safarzadeh, T.; Taheri, M.; Salari, S.; Khashavi, Z.; Bazarganipour, F. The influence of infertility on sexual and marital satisfaction in Iranian women with polycystic ovary syndrome: a case-control study. Middle East Fertil. Soc. J. 2021, 26, 1–7. [Google Scholar] [CrossRef]
- Kępczyńska-Nyk, A.; Kuryłowicz, A.; Nowak, A.; Bednarczuk, T.; Ambroziak, U. Sexual function in women with androgen excess disorders: classic forms of congenital adrenal hyperplasia and polycystic ovary syndrome. J. Endocrinol. Investig. 2021, 44, 505–513. [Google Scholar] [CrossRef]
- Ercan, C.M.; Coksuer, H.; Aydogan, U.; Alanbay, I.; Keskin, U.; E Karasahin, K.; Baser, I. Sexual dysfunction assessment and hormonal correlations in patients with polycystic ovary syndrome. Int. J. Impot. Res. 2013, 25, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Ferraresi, S.R.; Lara, L.A.d.S.; Reis, R.M.; Silva, A.C.J.d.S.R.e. Changes in Sexual Function among Women with Polycystic Ovary Syndrome: A Pilot Study. J. Sex. Med. 2013, 10, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Lara, L.A.S.; Ramos, F.K.P.; Kogure, G.S.; Costa, R.S.; de Sá, M.F.S.; Ferriani, R.A.; dos Reis, R.M. Impact of Physical Resistance Training on the Sexual Function of Women with Polycystic Ovary Syndrome. J. Sex. Med. 2015, 12, 1584–1590. [Google Scholar] [CrossRef] [PubMed]
- Shafti, V.; Shahbazi, S. Comparing Sexual Function and Quality of Life in Polycystic Ovary Syndrome and Healthy Women. J Family Reprod Health 2016, 10, 92–98. [Google Scholar] [PubMed]
- Diamond, M.P.; Legro, R.S.; Coutifaris, C.; Alvero, R.; Robinson, R.D.; Casson, P.A.; Christman, G.M.; Huang, H.; Hansen, K.R.; Baker, V.; et al. Sexual function in infertile women with polycystic ovary syndrome and unexplained infertility. Am. J. Obstet. Gynecol. 2017, 217, 191–e1. [Google Scholar] [CrossRef] [PubMed]
- Noroozzadeh, M.; Tehrani, F.R.; Mobarakabadi, S.S.; Farahmand, M.; Dovom, M.R. Sexual function and hormonal profiles in women with and without polycystic ovary syndrome: a population-based study. Int. J. Impot. Res. 2017, 29, 1–6. [Google Scholar] [CrossRef]
- Altuntaş, S. .; Çelik,.; Özer,.; Çolak, S. Depression, anxiety, body image scores, and sexual dysfunction in patients with polycystic ovary syndrome according to phenotypes. Gynecol. Endocrinol. 2022, 38, 849–855. [Google Scholar] [CrossRef]
- Gateva, A. and Z. Kamenov. Sexual function in bulgarian patients with PCOS and/or obesity before and after metformin treatment. in JOURNAL OF SEXUAL MEDICINE. 2011. WILEY-BLACKWELL COMMERCE PLACE, 350 MAIN ST, MALDEN 02148, MA USA.
- Aydogan Kirmizi, D.; et al. Sexual function and depression in polycystic ovary syndrome: Is it associated with inflammation and neuromodulators? Neuropeptides 2020, 84, 102099. [Google Scholar] [CrossRef] [PubMed]
- Yıldız, A.; Dogan, O. Sexual dysfunction in women with polycystic ovary syndrome. Kocaeli Medical Journal 2017, 6, 17–23. [Google Scholar]
- Naumova, I.; Castelo-Branco, C.; Casals, G. Psychological Issues and Sexual Function in Women with Different Infertility Causes: Focus on Polycystic Ovary Syndrome. Reprod. Sci. 2021, 28, 2830–2838. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, G.; Antes, G.; Schumacher, M. A test for publication bias in meta-analysis with sparse binary data. Stat. Med. 2007, 26, 721–733. [Google Scholar] [CrossRef] [PubMed]
- McGrath, S.; Zhao, X.; Steele, R.; Thombs, B.D.; Benedetti, A.; Levis, B.; Riehm, K.E.; Saadat, N.; Levis, A.W.; Azar, M.; et al. Estimating the sample mean and standard deviation from commonly reported quantiles in meta-analysis. Stat. Methods Med Res. 2020, 29, 2520–2537. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Weiss, M.S.; Roe, A.H.; Allison, K.C.; Dodson, W.C.; Kris-Etherton, P.M.; Kunselman, A.R.; Stetter, C.M.; Williams, N.I.; Gnatuk, C.L.; Estes, S.J.; et al. Lifestyle modifications alone or combined with hormonal contraceptives improve sexual dysfunction in women with polycystic ovary syndrome. Fertil. Steril. 2021, 115, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Dokras, A.; Stener-Victorin, E.; Yildiz, B.O.; Li, R.; Ottey, S.; Shah, D.; Epperson, N.; Teede, H. Androgen Excess- Polycystic Ovary Syndrome Society: position statement on depression, anxiety, quality of life, and eating disorders in polycystic ovary syndrome. Fertil. Steril. 2018, 109, 888–899. [Google Scholar] [CrossRef] [PubMed]
- Shakeel, M.; Ashraf, F.; Wajid, A. Sexual functioning as predictor of depressive symptoms and life satisfaction in females with Polycystic Ovary Syndrome (PCOS). Pak. J. Med Sci. 2020, 36, 1500–1504. [Google Scholar] [CrossRef] [PubMed]
- Yin, X.; Ji, Y.; Chan, C.L.W.; Chan, C.H.Y. The mental health of women with polycystic ovary syndrome: a systematic review and meta-analysis. Arch Womens Ment Health 2021, 24, 11–27. [Google Scholar] [CrossRef]
- Dokras, A. Mood and anxiety disorders in women with PCOS. Steroids 2012, 77, 338–341. [Google Scholar] [CrossRef]
- Fereidooni, B.; Jenabi, E.; Khazaei, S.; Abdoli, S. The Effective Factors on The Sexual Function of Polycystic Ovary Syndrome Women: A Cross-Sectional Study. Int J Fertil Steril 2022, 16, 220–223. [Google Scholar] [CrossRef]
- Carmina, E.; Lobo, R.A. Comparing Lean and Obese PCOS in Different PCOS Phenotypes: Evidence That the Body Weight Is More Important than the Rotterdam Phenotype in Influencing the Metabolic Status. Diagnostics 2022, 12, 2313. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of Article Selection; FSFI: female sexual function index.
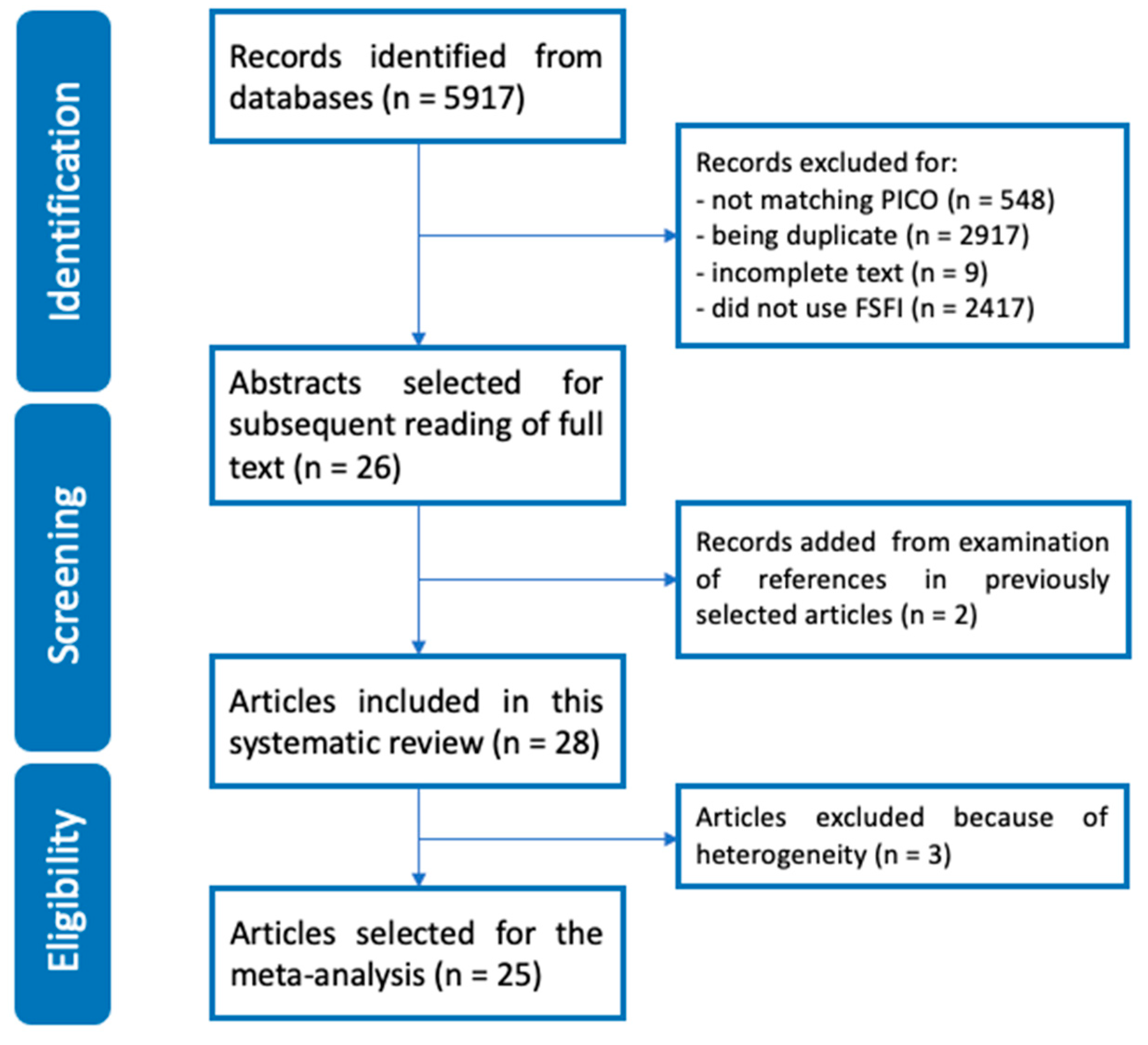
Figure 2.
Funnel plots showing elevated risk of bias concerning Body Mass Index (2a), Overall Female Sexual Function Index (2b), Desire (2c), Arousal (2d), Lubrication (2e), Orgasm (2f), Satisfaction (2g) and Pain (2h) subdomains between PCOS women and controls.
Figure 2.
Funnel plots showing elevated risk of bias concerning Body Mass Index (2a), Overall Female Sexual Function Index (2b), Desire (2c), Arousal (2d), Lubrication (2e), Orgasm (2f), Satisfaction (2g) and Pain (2h) subdomains between PCOS women and controls.
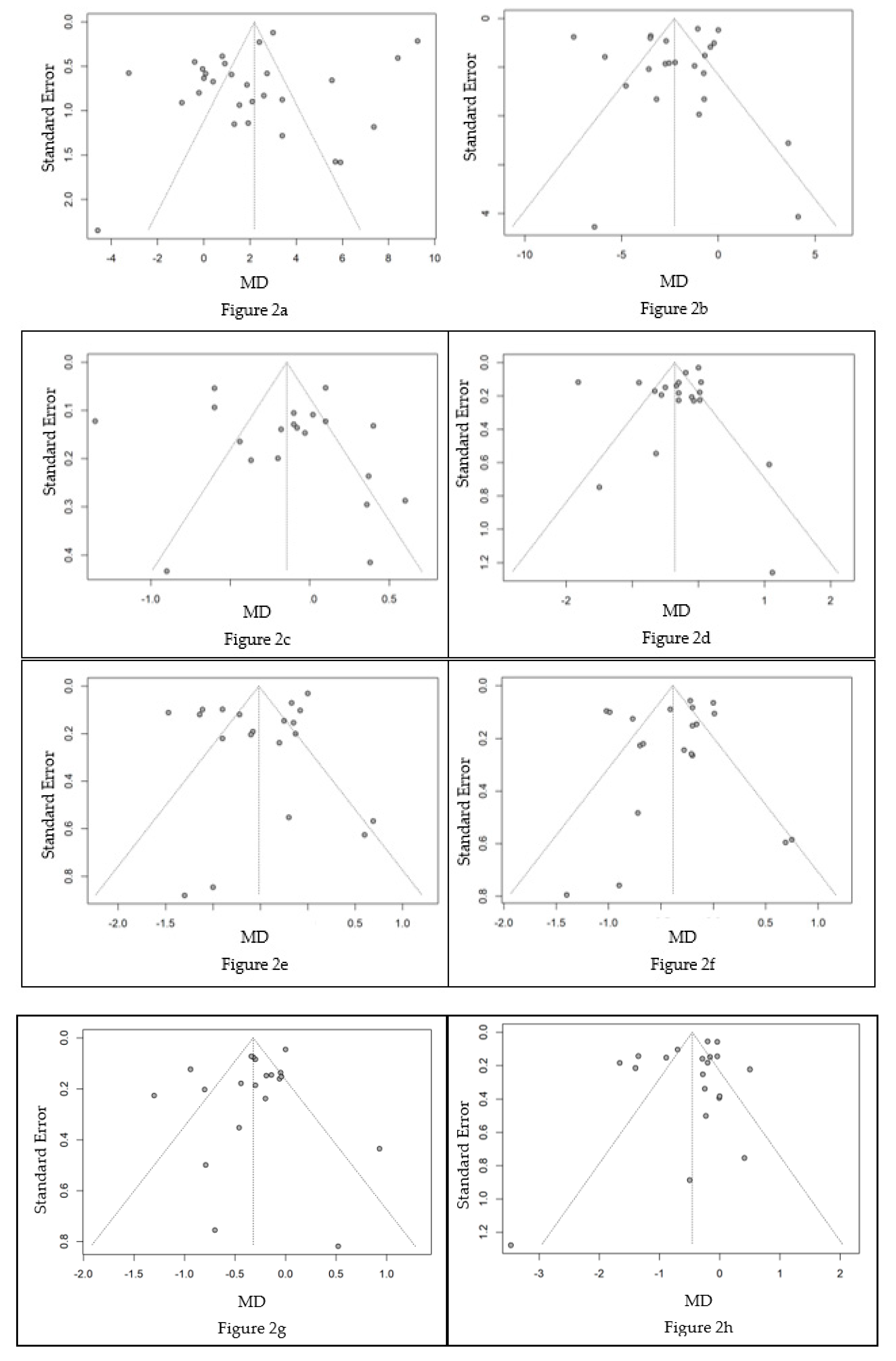
Figure 3.
Forest Plots of Meta-analysis showing Overall FSFI score (3a), Arousal (3b), Lubrication (3c), Orgasm (3d), Satisfaction (3e) and Pain (3f) subdomains, representing significantly lower overall FSFI score in PCOS women than controls, especially due to arousal, lubrication, orgasm, satisfaction and pain subdomains. FSFI: Female Sexual Function Index; PCOS: Polycystic Ovary Syndrome; SD: standard deviation; MD: mean difference; CI: confidence interval.
Figure 3.
Forest Plots of Meta-analysis showing Overall FSFI score (3a), Arousal (3b), Lubrication (3c), Orgasm (3d), Satisfaction (3e) and Pain (3f) subdomains, representing significantly lower overall FSFI score in PCOS women than controls, especially due to arousal, lubrication, orgasm, satisfaction and pain subdomains. FSFI: Female Sexual Function Index; PCOS: Polycystic Ovary Syndrome; SD: standard deviation; MD: mean difference; CI: confidence interval.
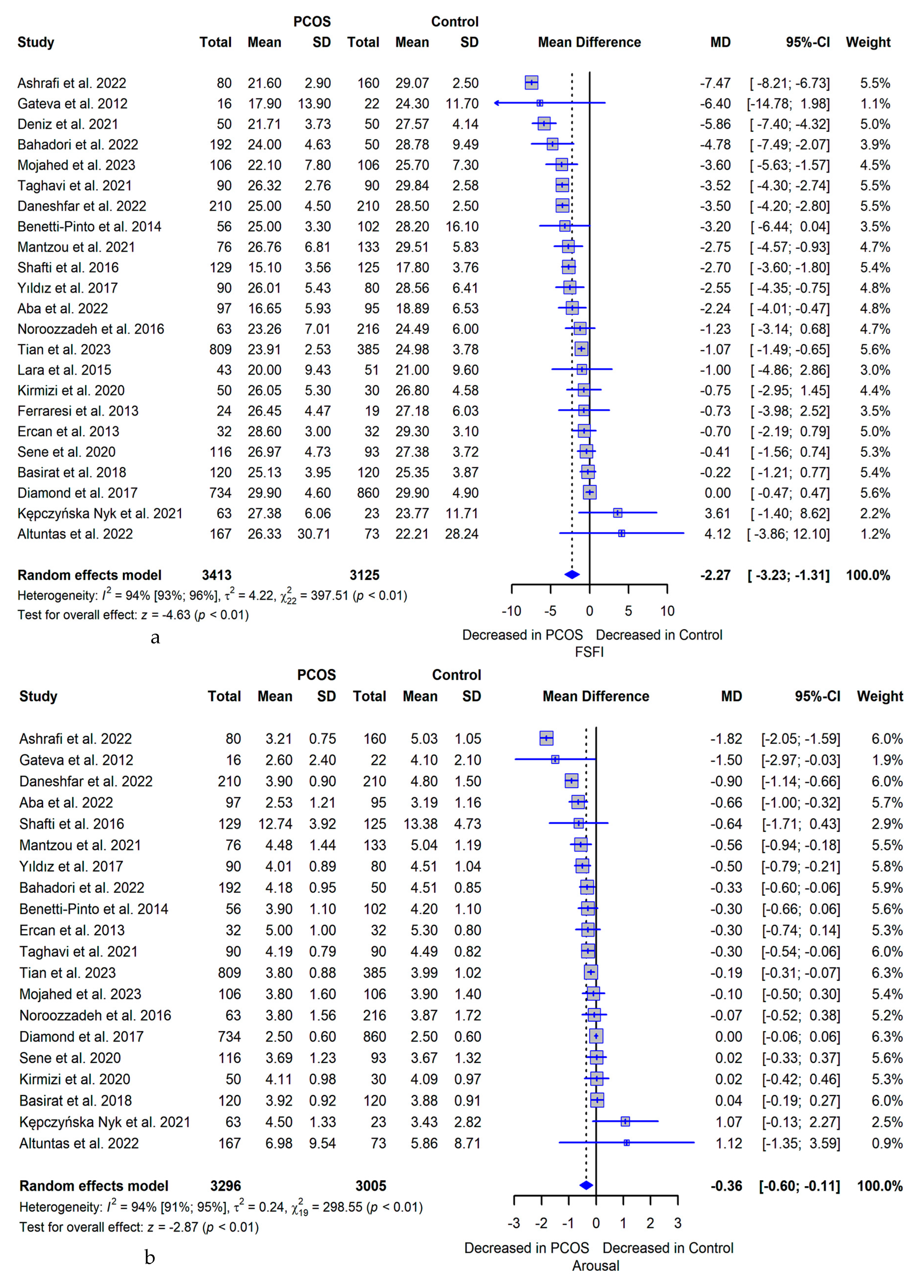
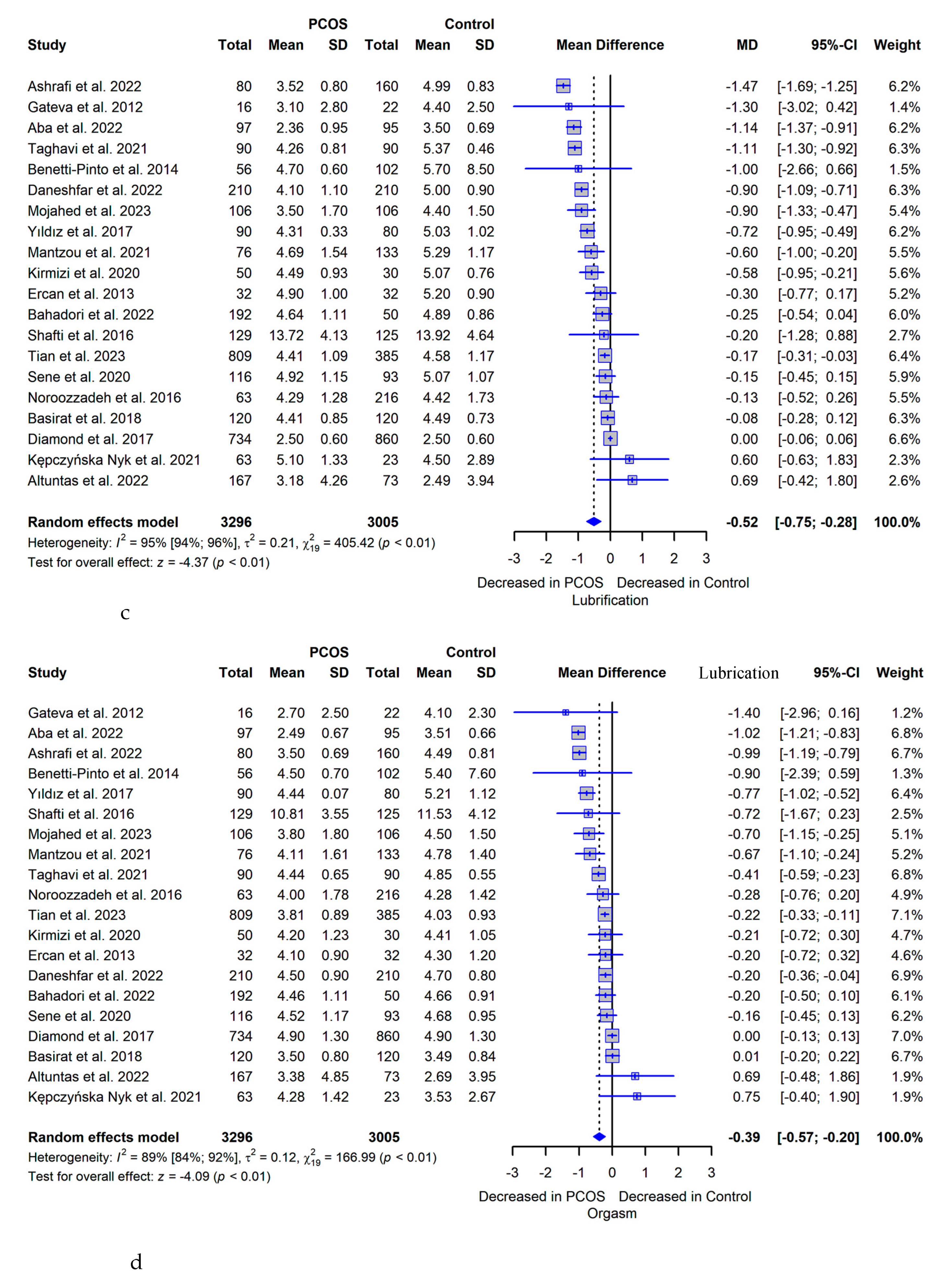
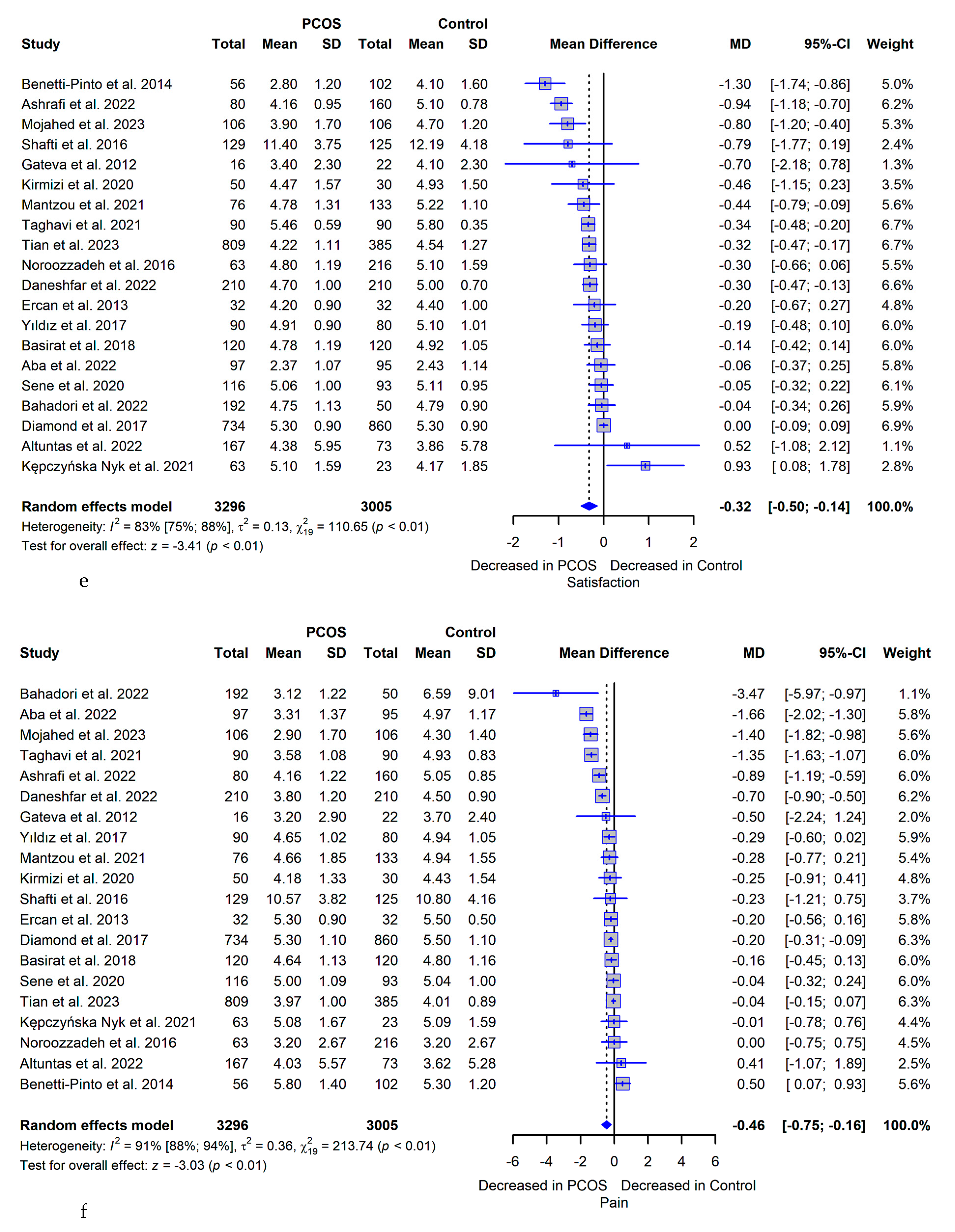
Figure 4.
Forest Plots of Meta-analysis Based on the Overall FSFI score Between OW/O PCOS Women and OW/O Controls, showing significantly higher overall FSFI score in OW/O PCOS group; BMI: body mass index; OW/O: overweight/ obese; PCOS: Polycystic Ovary Syndrome; SD: standard deviation; MD: mean difference; CI: confidence interval.
Figure 4.
Forest Plots of Meta-analysis Based on the Overall FSFI score Between OW/O PCOS Women and OW/O Controls, showing significantly higher overall FSFI score in OW/O PCOS group; BMI: body mass index; OW/O: overweight/ obese; PCOS: Polycystic Ovary Syndrome; SD: standard deviation; MD: mean difference; CI: confidence interval.
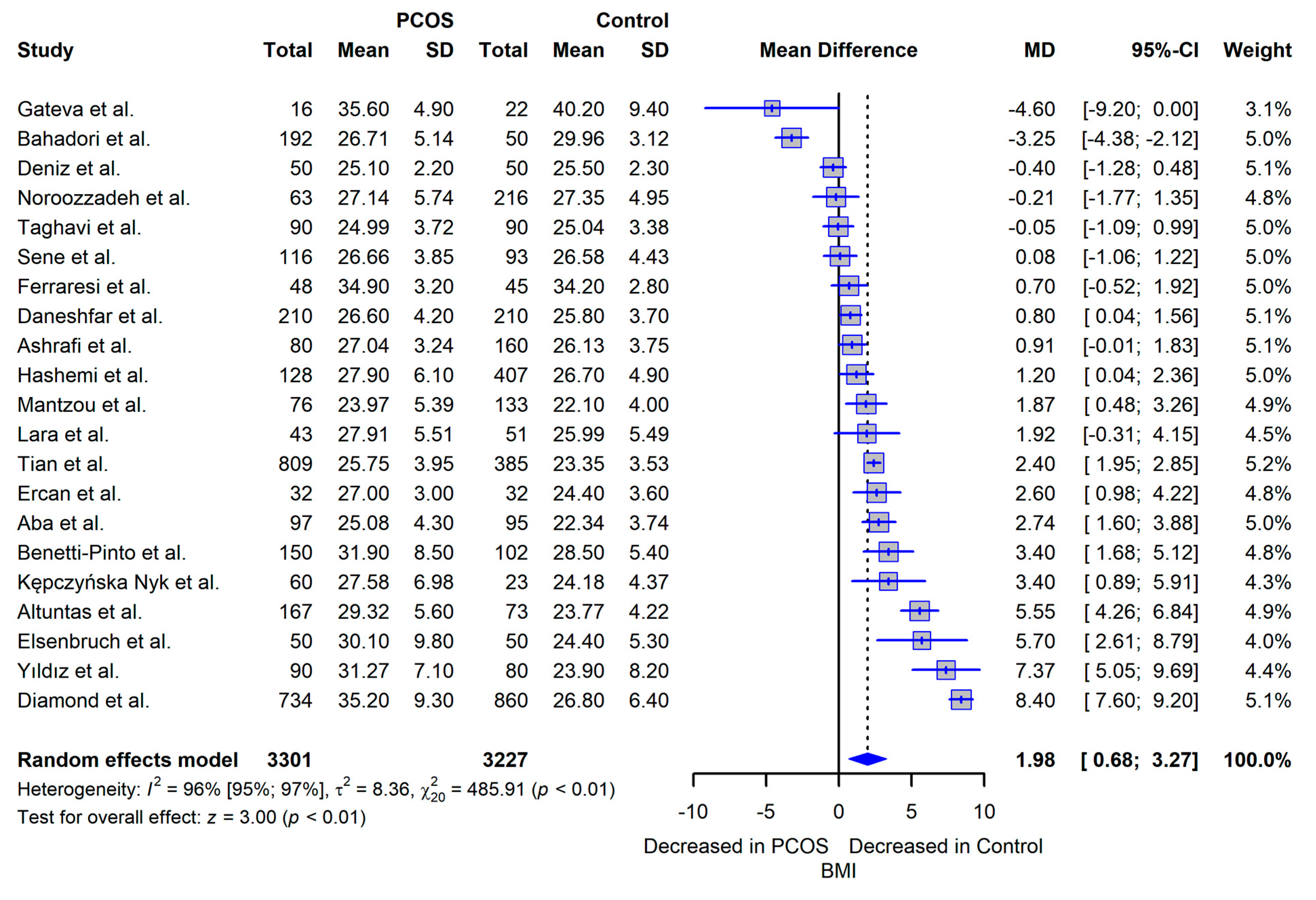

Table 1.
Databases and Medical Subject Headings.
| Database | Medical Subject Headings |
|---|---|
| Pubmed/ Medline | (Ovary Syndrome, Polycystic OR Syndrome, Polycystic Ovary OR Stein-Leventhal Syndrome OR Sclerocystic Ovarian Degeneration OR Ovarian Degeneration, Sclerocystic OR Ovarian Degeneration, Sclerocystic OR Polycystic Ovary Syndrome OR Sclerocystic Ovary Syndrome OR Sclerocystic Ovaries) AND (Behavior, Sexual OR Sexual Activities OR Sexual Activity OR Sex Behavior OR Physiological Sexual Dysfunction OR Physiological Sexual Dysfunctions OR Sex Disorders OR Physiological Sexual Disorders) |
| Embase | (Polycystic ovary syndrome OR polycystic ovary disease) AND (sexuality OR sexual behavior) |
| Lilacs | [tw:(polycystic ovary syndrome)] AND [tw:(sexuality)] |
| Cinahl | (Polycystic ovary syndrome AND Sexual Dysfunction) OR (Polycystic ovary syndrome AND Sexual Function) |
| PsycINFO | Polycystic Ovary Syndrome AND (Behavior, Sexual OR Sexual Activities OR Sexual Activity OR Sex Behavior OR Physiological Sexual Dysfunction OR Physiological Sexual Dysfunctions OR Sex Disorders OR Physiological Sexual Disorders) |
| Google Scholar | (Polycystic ovary syndrome AND Sexual Dysfunction) OR (Polycystic ovary syndrome AND Sexual Function) |
| Cochrane | Polycystic Ovary Syndrome AND Sex Behavior |
Table 2.
Comparison of PCOS and Control Groups: Demographic Data, Study Characteristics and Sexual Function Results
Table 2.
Comparison of PCOS and Control Groups: Demographic Data, Study Characteristics and Sexual Function Results
| Author/ Year/ Country | Study Design | Sample size per group (n) | Mean age ± SD | BMI ± SD | Total FSFI Comparison: PCOS Group vs. Control | Total FSFI p-value | Affected FSFI Domains |
|---|---|---|---|---|---|---|---|
| Benetti-Pinto et al 2014 Brazil [5] |
Case control | PCOS: 150 Control: 102 |
PCOS: 26.9 ± 4.9 Control: 35.6 ± 7.3 |
PCOS: 31.9 ± 8.5 Control: 28.5 ± 5.4 |
Lower in PCOS | p = 0.005 | Arousal, lubrication, satisfaction and pain |
| Basirat et al 2019 Iran [25] |
Case control | PCOS: 120 Control: 120 |
PCOS: 29.55 ± 5.17 Control: 29.33 ± 6.23 |
PCOS: 39.5 ± 15.81 Control: 45.5 ± 5.48 |
Lower in PCOS | p < 0.05 | None |
| Bahadori et al 2022 Iran [26] |
Cross sectional | PCOS: 192 Control: 50 |
PCOS: 31.17 ± 6.57 Control: 34.18 ± 4.13 |
PCOS: 26.71 ± 5.14 Control: 26.96 ± 3.12 |
Lower in PCOS | p < 0.05 | Arousal, lubrication and pain |
| Mantzou et al 2021 Greece [27] |
Case control | PCOS: 76 Control: 133 |
PCOS: 22.17 ± 2.51 Control: 21.62 ± 1.93 |
PCOS: 23.97 ± 5.39 Control: 22.1 ± 4 |
Lower in PCOS | p < 0.001 | Arousal, lubrication, orgasm and satisfaction |
| Ashrafi et al 2022 Iran [28] |
Cross sectional | PCOS: 80 Control: 160 |
PCOS: 31.94 ± 4.44 Control: 31.66 ± 1.89 |
PCOS: 27.04 ± 3.24 Control: 26.13 ± 3.75 |
Lower in PCOS | p < 0.001 | Desire, arousal, pain, lubrication, orgasm and satisfaction |
| Deniz et al 2020 Turkey [29] |
Case control | PCOS: 50 Control: 50 |
PCOS: 32 ± 4 Control: 31 ± 4 |
PCOS: 25.1 ± 2.2 Control: 25.5 ± 2.3 |
Lower in PCOS | p = 0.001 | Desire, lubrication, orgasm, satisfaction and pain |
| Tian et al 2023 Germania [10] |
Cross sectional | PCOS: 809 Control: 385 |
PCOS: 27.25 ± 3.98 Control: 27.56 ± 3.83 |
PCOS: 25.75 ± 3.95 Control: 23.35 ± 3.53 |
Lower in PCOS | p < 0.05 | Desire, orgasm, lubrication and satisfaction |
| Mojahed et al 2023 Iran [30] |
Case control | PCOS: 106 Control: 106 |
PCOS: 26.9 ± 5.2 Control: 27.8 ± 6.8 |
N.A. | Lower in PCOS | p < 0.001 | Arousal, pain, lubrication, orgasm and satisfaction |
| Hashemi et al 2014 Iran [31] |
Case control | PCOS: 128 Control: 407 |
PCOS: 30.6 ± 5.01 Control: 29.4 ± 5.8 |
PCOS: 26.7 ± 4.9 Control: 27.9 ± 6.1 |
Lower in PCOS | p < 0.05 | Satisfaction, orgasm, lubrication and arousal |
| Anger et al 2007 USA [32] | Case control | PCOS: 33 | PCOS: 36 ± N.A. | N.A. | Lower in PCOS | p < 0.05 | Arousal and lubrication |
| Eftekhar et al 2014 Iran [33] | Case control | PCOS: 130 | PCOS: 27.02 ± 4.27 | N.A. | Lower in PCOS | p < 0.05 | None |
| Dashti et al 2016 Malasya[34] | Cross sectional | PCOS: 16 | PCOS: 33.44 ± 5.88 | PCOS: 28.04 ± 3.34 | Lower in PCOS | p < 0.05 | Arousal and lubrication |
| Aba et al 2022 Turkey [35] |
Case control | PCOS: 97 Control: 95 |
PCOS: 28.23 ± 4.56 Control: 29.33 ± 5.61 |
PCOS: 25.08 ± 4.3 Control: 22.34 ± 3.74 |
Lower in PCOS | p < 0.05 | Desire, arousal, pain, lubrication and orgasm |
| Daneshfar et al 2022 Iran [36] |
Cross sectional | PCOS: 210 Control: 210 |
PCOS: 30 ± 5.3 Control: 31.4 ± 2.7 |
PCOS: 26.6 ± 4.2 Control: 25.8 ± 3.7 |
Lower in PCOS | p < 0.001 | Desire, arousal, pain, lubrication, orgasm and satisfaction |
| Taghavi et al 2021 Iran [37] |
Case control | PCOS: 90 Control: 90 |
PCOS: 28.8 ± 4.39 Control: 30 ± 4.83 |
PCOS: 24.99 ± 3.72 Control: 25.04 ± 3.38 |
Lower in PCOS | p < 0.05 | Desire, arousal, pain, lubrication, orgasm and satisfaction |
| Kępczyńska-Nyk et al 2021 Poland [38] | Case control | PCOS: 60 Control: 23 |
PCOS: 26.56 ± 5.45 Control: 30.85 ± 6.73 |
PCOS: 27.58 ± 6.98 Control: 24.18 ± 4.37 |
Higher in PCOS | p > 0.05 | Satisfaction |
| Ercan et al 2013 Turkey [39] |
Case control | PCOS: 32 Control: 32 |
PCOS: 27.4 ± 3.3 Control: 27 ± 3 |
PCOS: 24.4 ± 3.6 Control: 27 ± 3 |
PCOS similar to controls | p > 0.05 | None |
| Ferraresi et al 2013 Brazil [40] |
Case control | PCOS: 48 Control: 45 |
PCOS: 26.1 ± 1.05 Control: 31.1 ± 1.02 |
PCOS: 34.2 ± 2.8 Control: 34.9 ± 3.2 |
Lower in PCOS | p > 0.05 | N.A. |
| Lara et al 2015 Brazil [41] |
Case control | PCOS: 43 Control: 51 |
PCOS: 27.8 ± 5.34 Control: 29.74 ± 5.26 |
PCOS: 27.91 ± 5.51 Control: 25.99 ± 5.49 |
Lower in PCOS | p > 0.05 | Pain, lubrication and arousal |
| Shafti et al 2016 Iran [42] |
Casual comparative study | PCOS: 129 Control: 125 |
PCOS: 30.10 ± N.A. Control: 32.79 ± N.A. |
N.A. | PCOS similar to controls | p > 0.05 | None |
| Diamond et al 2017 Georgia [43] |
Cross sectional | PCOS: 734 Control: 860 |
PCOS: 95.1 ± 26.3 Control: 72.4 ± 18.5 |
PCOS: 35.2 ± 9.3 Control: 26.8 ± 6.4 |
PCOS similar to controls | p > 0.05 | Arousal and satisfaction |
| Noroozzadeh et al 2017 Iran [44] |
Case control | PCOS: 63 Control: 216 |
PCOS: 33.6 ± 7.2 Control: 36.3 ± 6.9 |
PCOS: 27.14 ± 5.74 Control: 27.35 ± 4.95 |
Lower in PCOS | p > 0.05 | Orgasm and satisfaction |
| Sene et al 2021 Iran [9] |
Case control | PCOS: 116 Control: 93 |
PCOS: 32 ± 5 Control: 34 ± 6 |
PCOS: 26.66 ± 3.85 Control: 26.58 ± 4.43 |
Lower in PCOS | p > 0.05 | Orgasm |
| Altuntas et al 2022 Turkey [45] |
Cross sectional | PCOS: 167 Control: 73 |
PCOS: 25.87 ± 5.64 Control: 27.25 ± 5.85 |
PCOS: 29.32 ± 5.6 Control: 23.77 ± 4.22 |
Higher in PCOS | p > 0.05 | None |
| Gateva et al 2012 Bulgaria [46] |
Case control | PCOS: 16 Control: 22 |
PCOS: 32.5 ± 8.5 Control: 32.5 ± 8.5 |
PCOS: 35.6 ± 4.9 Control: 40.2 ± 9.4 |
Lower in lean PCOS than obese PCOS |
p > 0.05 | Arousal, lubrication, orgasm, satisfaction and pain |
| Kirmizi et al 2020 Turkey [47] |
Case control | PCOS: 50 Control: 30 |
PCOS: 25.1 ± 4.4 Control: 31.9 ± 4.73 |
PCOS: 26.4 ± 5.22 Control: 25.08 ± 4.84 |
Lower in PCOS | p > 0.05 | Lubrication |
| Yıldız et al 2017 Turkey [48] |
Cross sectional | PCOS: 90 Control: 80 |
PCOS: 28.3 ± 2.12 Control: 29.1 ± 4.8 |
PCOS: 31.27 ± 7.1 Control: 23.9 ± 8.2 |
Lower in PCOS | p > 0.05 | Orgasm |
| Naumova et al 2021 Spain [49] |
Case control | PCOS: 37 Control: 67 |
N.A. | N.A. | Lower in PCOS | p > 0.05 | Desire, arousal, lubrication, orgasm and satisfaction |
3 N.A.: not available; FSFI: Female Sexual Function Index; PCOS: Polycystic Ovary Syndrome; SD: standard deviation; BMI: body mass index; Affected domains: p ≤ 0.05 between patients and controls.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



