Submitted:
20 September 2023
Posted:
22 September 2023
You are already at the latest version
Abstract
Here we performed a comparative experimental analysis by EPR spectroscopy of the intensity of nitric oxide (NO) production and copper content in the injured and uninjured areas of the frontal lobes and the hippocampus of the brain of male Wistar rats, after modeling of combined brain and spinal cord injury. Brain and spinal cord injury were modelled by local destruction of the left precentral region of the brain using a stylet followed by hemorrhage injury at the level of the first lumbar vertebra of the spinal cord. We found a significant decrease in NO production 7 days after injury modeling in the injured and uninjured (contralateral) brain regions, but the copper content remained unchanged one week after injury modeling. Thus, combined brain and spinal cord injury is not accompanied by a radical change in the activity of the antioxidant system in the brain, which is also confirmed by the absence of changes in NO production and copper content in the hippocampus.
Keywords:
nitric oxide
; cooper
; brain stroke
; spinal cord injury
; electron paramagnetic resonance
1. INTRODUCTION
Nitric oxide (NO) serves as a vital signaling molecule that regulates cellular metabolism and various physiological functions in the human body [1,2,3,4,5]. The discovery of NO synthesis in mammalian cells has sparked extensive research efforts aimed at understanding its role in diverse fields of biology and medicine [2,6,7,8]. Endogenous NO production has been observed in a wide range of animal groups, plants, diatoms, slime molds, and bacteria [9]. NO exhibits ubiquitous presence within the nervous system [1,2], cardiovascular system [10,11], as well as other functional systems of the body, including immunity and metabolism [5,12,13]. NO also plays a significant role in many diseases, such as diabetes, cancer, ischemia, Alzheimer's disease, diseases of the cardiovascular system [14,15,16,17,18,19]. Among its crucial functions, NO plays a pivotal role in vasodilation [20,21]. Additionally, aside from its vasodilatory, neurotransmitter, and stress-limiting properties, NO has been implicated in oxidative stress reactions, the calcium glutamate cascade, and inflammatory processes [2,6,22,23,24].
There is ample evidence pointing to the disruption of nitric oxide biosynthesis as the primary factor in the brain pathophysiological response to hypoxia-ischemia [25,26,27]. The functional role of endogenous NO in the processes occurring during nervous system damage remains controversial and inadequately explored [4,5]. This is due to the fact that NO serves as a paradigmatic example of the classical two-faced Janus [28,29,30]. Thus, an increase in the activity of neuronal NO synthase (nNOS) was found at the beginning of ischemia with a maximum in the third hour [31], as well as the onset of expression of inducible NOS (iNOS) a day after ischemia [32]. In acute hypoxia an overproduction of NO is also shown [33]. By EPR spectroscopy it was found that NO production increased after 5 minutes of ischemia and lasted for 60 minutes [34,35]. An increase in the relative concentration of free NO by 132% 15 minutes after ischemia caused by occlusion of the middle cerebral artery was found by same method using a spin trap before ischemia [13,36]. On the other hand, a number of studies which conducted on brain ischemia models have not confirmed neurotoxic role of ischemically generated NO. For example, NO-synthase inhibitors L-NNA and L-NAME have not been found to reduce the size of lesion in focal cerebral ischemia in rats [37,38], but increase focal ischemic stroke [39]. There are numerous studies on the use of NO donors as neuroprotective agents after ischemic injury [40,41,42,43,44,45]. It has been found that short-term use of NO donors before the onset of ischemia can protect function of endothelium in ischemic-reperfusion injury [46]. It was also shown that inhalation of NO or nitrite encourage brain function during perinatal hypoxic and chemical intervention [47].
Earlier, together with the team of prof. V.B. Koshelev (Moscow State University), we conducted studies aimed to study the content of NO in the focus of cerebral ischemia (left hemisphere) by EPR spectroscopy, which showed that in the ischemic part of the left hemisphere cortex, the NO content in the spin trap decreased 5 times 5 hours after an ischemic stroke, and this decrease persists for a day after the stroke [48]. In another study, the authors of this article demonstrated that 5 hours after the onset of signs of both ischemic and hemorrhagic stroke, the formation of NO in the hippocampus decreased by 2-3 times and this decrease persists for 24 and 72 hours [49]. Significantly reduced NO content was found in the olfactory bulb of the rat brain 1 and 2 days after modeling ischemia caused by carotid artery ligation [50]. The involvement of ATP-dependent K-channels in these processes has been shown [51,52].
Cerebral ischemia triggers the accumulation of excitatory amino acids in brain tissues and the activation of calcium-dependent nitric oxide synthase (NOS) isoforms, namely neuronal NOS and endothelial NOS. However, while selective inhibition of neuronal NOS demonstrates neuroprotective effects, selective inhibition of endothelial NOS yields neurotoxic outcomes [14,15,53,54,55]. Clinicians are familiar with such paradoxical effects of NO, who constantly take into account the individual reactions of each patient. The reason is the fact that the synthesis of NO by nNOS is accompanied by an overload of the ischemic neuron with calcium caused by glutamate. It is assumed that the NO generated by eNOS expressed in endothelial cells, unlike nos, has a beneficial effect [27,45]. Here, eNOS not only promotes vasodilation, but also increases the proliferation and migration of vascular smooth muscle cells and thereby enhances arteriogenesis after a stroke. nNOS inhibition protected hypoxicischemic-induced mice brain damage by the increased collateral flow. Therefore, the introduction of a 7-nitroindazole blocker can have potential utility for the treatment of ischemic-reperfusion injury in human beings [56]. Such assumptions are supported by the results of a decrease in secondary brain damage after brain damage during inhalation of NO [57,58,59].
Disruption of cerebral oxygen supply also occurs in cases where a blood vessel becomes thrombosed or an aneurysm ruptures, it often ends with the development of ischemic or hemorrhagic stroke [14,15]. In processes developing in the brain of hypoxia-ischemia, the ambivalent role of NO is again manifested, which, according to modern concepts, can exert both neurotoxic and neuroprotective functions [14,28,43,51]. In response to the development of pathological processes in the brain such as hypoxia and ischemia, the regulatory systems of the brain, including the NO system, exhibit increased activity. This naturally leads to an elevation in oxygen consumption (which exacerbates hypoxia) and the accumulation of underoxidized products in brain tissue, which, in aggregate, disrupts the integrative activity of the brain [60,61]. During reperfusion, despite the restoration of blood flow to the ischemic area, a large number of free radicals (both reactive nitrogen forms and reactive oxygen forms) are produced, which serve as important factors of ischemic reperfusion injury [55]. Thus, it is fundamentally important to take into account that the well-coordinated functioning of the NO system is disrupted with the development of hypoxia and cerebral ischemia. At the same time, cerebral ischemia is accompanied by multiple multidirectional changes in the NO content in the brain, which affects the functioning of the brain regulatory systems and the effectiveness of signal pathways to control the functions of all functional systems of the body [61,62,63]. Thus, there is increasing evidence that NO plays an important role in neuroprotection in stroke, even if NO is usually regarded as a toxic gas. Therefore, we need to be dialectical about NO, and further research, including animal studies and clinical studies, can give us a new understanding of the treatment of stroke and other diseases of the central nervous system [54].
Ischemia and trauma of the brain and spinal cord are characterized by primary injury and subsequent secondary phase of injury [58,64,65]. A critical component of secondary injury is oxidative stress and increased formation of reactive oxygen species [27,66]. Secondary injury occurs not only at the site of the initial primary injury, but also leads to the spread of the lesion to neighboring, intact tissues. Also, during reperfusion, despite the restoration of blood flow to the ischemic area, a large number of free radicals, both reactive nitrogen forms and reactive oxygen forms, are produced, which serve as important factors of ischemic reperfusion injury [55,66].
Activation of antioxidant enzymes represents a crucial defense mechanism against highly toxic oxygen radicals. The majority of these enzymes are associated with copper-containing proteins [67,68]. The most famous of them is Cu,Zn-superoxide dismutase (SOD) [68,69,70]. Various forms of SOD exist depending on the specific transition metal cofactor present in the enzyme's active site. For instance, Cu,Zn-SOD features copper as the active site cofactor and zinc as a conformation-stabilizing cofactor, as well as a number of others [71]. The primary and essential defense mechanism against free radical oxidative processes involves the neutralization of superoxide radicals (O2-) by the cytosolic enzyme Cu,Zn-SOD [72]. This enzyme plays a significant role in the antioxidant protection of virtually all cells that come into contact with oxygen. Thus, maintaining a balanced copper level in the nervous system is crucial for its proper functioning. However, imbalances in copper have been implicated in the pathogenesis of numerous neurodegenerative disorders, including Parkinson's, Alzheimer's, and Huntington's diseases, while disruptions in SOD metabolism can lead to various pathological conditions.
Brain injury following subarachnoid hemorrhage occurs in two phases: an acute ischemic stroke during the initial bleeding and subsequent secondary events, among which the most fatal the cerebral vasospasm occurring 3-7 days later [73]. Clinicians need experimental information about the patterns of development of spasm of blood vessels of the brain in order to timely correct and control the situation in clinical practice. Intracranial injury, in addition to spasm of blood vessels, can manifest as diffuse or focal damage of brain tissue and, to a certain extent, by a number of scientists and clinicians, refers to such volumetric pathologies, including but not limited to hematoma, cerebral aneurysm, tumor, and stroke [74,75]. Apart from the primary injury, secondary injuries usually accompanied in a cascade over the following hours or days [73,75,76]. NO has been shown to play a multifaceted role in the regulation of cerebral blood flow both under normal physiological conditions and in pathology, for example, after a traumatic brain injury, with subarachnoid hemorrhage, severe traumatic brain injury, ischemic stroke [15,77,78]. Several authors have highlighted the significance of NO as one of the triggers of the primary inflammatory pathway activated following hemorrhagic stroke [79].
Considering the afore mentioned literature, we aimed to investigate not only of the dynamics of nitric oxide production, but also of the copper content in both injured and non-injured regions of the frontal lobes of the brain, as well as the hippocampus, during the modeling of a combined brain and spinal cord injury.
2. RESULTS
EPR spectroscopy was employed to study the intensity of NO production and copper content (as an indicator of the 1st and 3rd subunits of superoxide dismutase) in injured and non-injured (contralateral) areas of the brain (frontal lobe), as well as in the hippocampus after combined injury of the brain and spinal cord. The EPR spectrum of a sample from the frontal lobe of the rat brain was given in Figure 1. It showed the determination of the intensity of the signals from the Cu2+-(DETC)2 and (DETC)2-Fe2+-NO complexes with amplitudes equal to their contribution to the spectrum of the sample. The details of determining these parameters were provided in the experimental procedures section.
On Figure 2 EPR spectra of the intact-control (Control rat), injured (Injured rat, injured area) and non-injured (Injured rat, non-injured area) regions (frontal lobe) of the rat brain seven days after inducing a combined injury to the brain and spinal cord was shown. The EPR signal of NO appeared as a triplet between 330-337 mT with a g-factor of 2.038 [80]. Additionally, a distinct signal was observed from the Cu2+-(DETC)2 complex, representing the interaction of copper with DETC [81,82,83]. The solid line represented the spectrum of the sample, while the dashed line corresponded to the signal of nitric oxide bound to the spin trap in the ((DETC)2-Fe2+-NO) complex spectrum (Figure 2). In the samples of biological tissues of rats that did not receive injections of spin trap components, no triplet was observed in the signal region ((DETC)2-Fe2+-NO). The frames show the signal areas ((DETC)2-Fe2+-NO) (Figure 2 and Figure 3). The relative changes in the amounts of the NO-containing complex and the Cu(DETC)2 complex were evaluated by the difference of the maximum and minimum of signal intensities from these complexes. The details of determining these parameters were given in the experimental procedures section.
Figure 4A displayed the statistical analysis of integral intensities for the (DETC)2-Fe2+-NO signal in the spectra of the investigated biological tissue samples obtained by EPR spectroscopy. This figure illustrated the spectral characteristics of both injured and non-injured (contralateral) brain areas after a combined injury of the brain and spinal cord, enabling the assessment of NO production in brain tissues. The results indicated a significant reliable decrease in NO production at 84% (P = 0.029, Mann-Whitney) in the injured brain area, as well as a significant but unreliable decrease in NO production at 66% (P = 0.38, Mann-Whitney) in the non-injured (contralateral) brain area, seven days after injury modeling. These findings demonstrated a distinct difference in NO production between the injured and contralateral brain areas (P = 0,05, Mann-Whitney). In the experimental data on the control samples, there were two data points close to 60; they were very different from the others. We carried out a processing option when excluding these two points from the statistical analysis (Figure 4B). In both variants, there is a significant difference, as in a separate comparison of the two groups ("Control rats", "Injured rats-injured area") by t-test (P = 0.021), and when comparing all three groups by ANOVA test. In this case, a posteriori tests of different types showed a significant difference between these two groups (Figure 4B).
Additionally, Figure 4C presented statistical data on the integrated signal intensities of (DETC)2-Cu. The results revealed that the copper content remains unchanged in both the injured and non-injured brain areas seven days after injury modeling. In summary, the simulation of injury led to a significant decrease in NO production in both the injured and non-injured areas of the brain, while there were no observed changes in the activity of the antioxidant system.
Figure 4.
The content of NO (A and B) and Cu (C) in the tissues from the frontal lobes of the control (Control rats) and injured (Injured rat) rats: injured (injured area) and non-injured (non-injured area) regions 7 days after the combined injury of the brain and spinal cord. The average integral intensity of the (DETC)2-Fe2+-NO and Cu(DETC)2 signal was shown in %. (*) indicates a significant difference of NO content between Control and injured groups (p<0.05).
Figure 4.
The content of NO (A and B) and Cu (C) in the tissues from the frontal lobes of the control (Control rats) and injured (Injured rat) rats: injured (injured area) and non-injured (non-injured area) regions 7 days after the combined injury of the brain and spinal cord. The average integral intensity of the (DETC)2-Fe2+-NO and Cu(DETC)2 signal was shown in %. (*) indicates a significant difference of NO content between Control and injured groups (p<0.05).
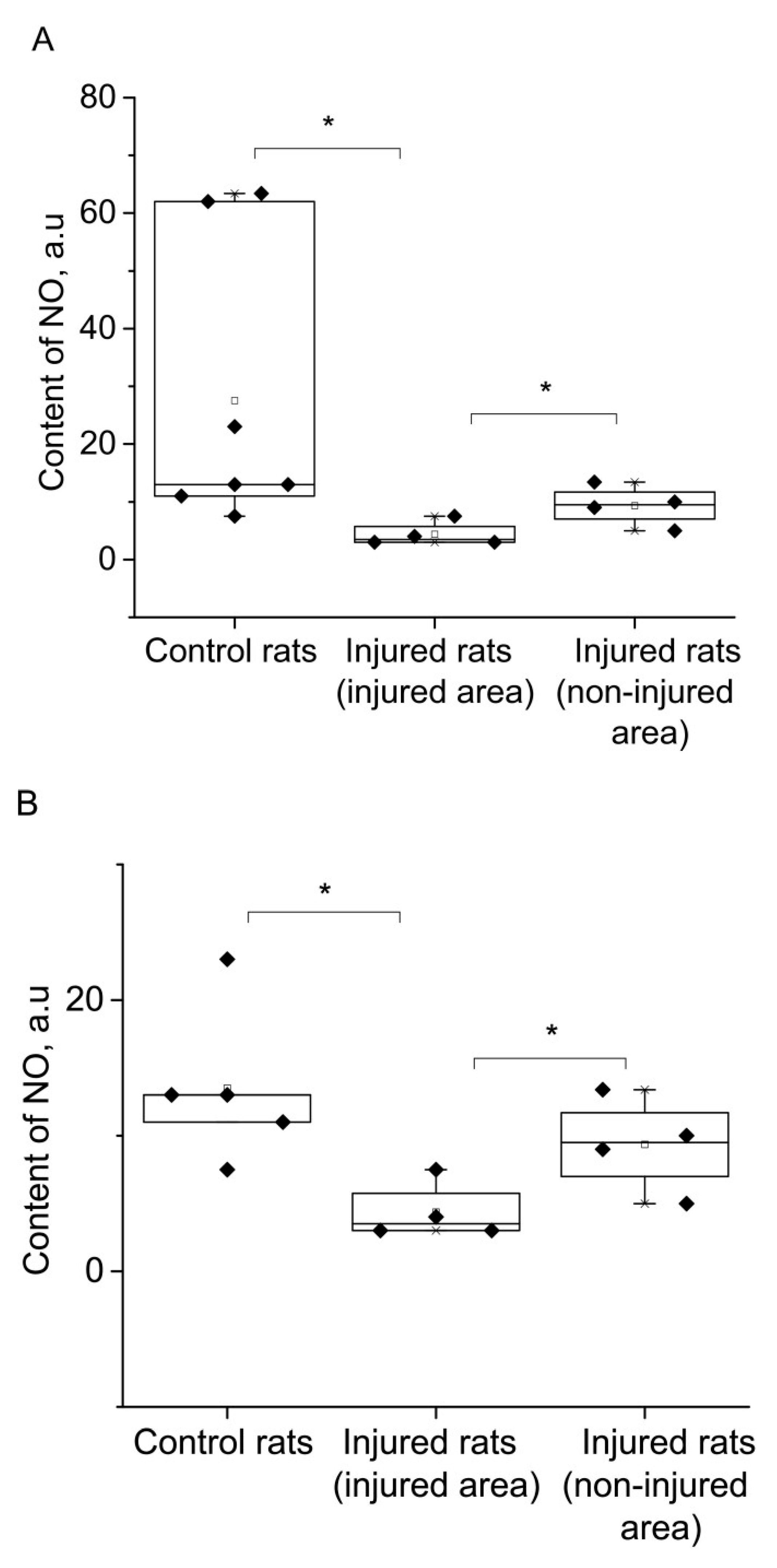
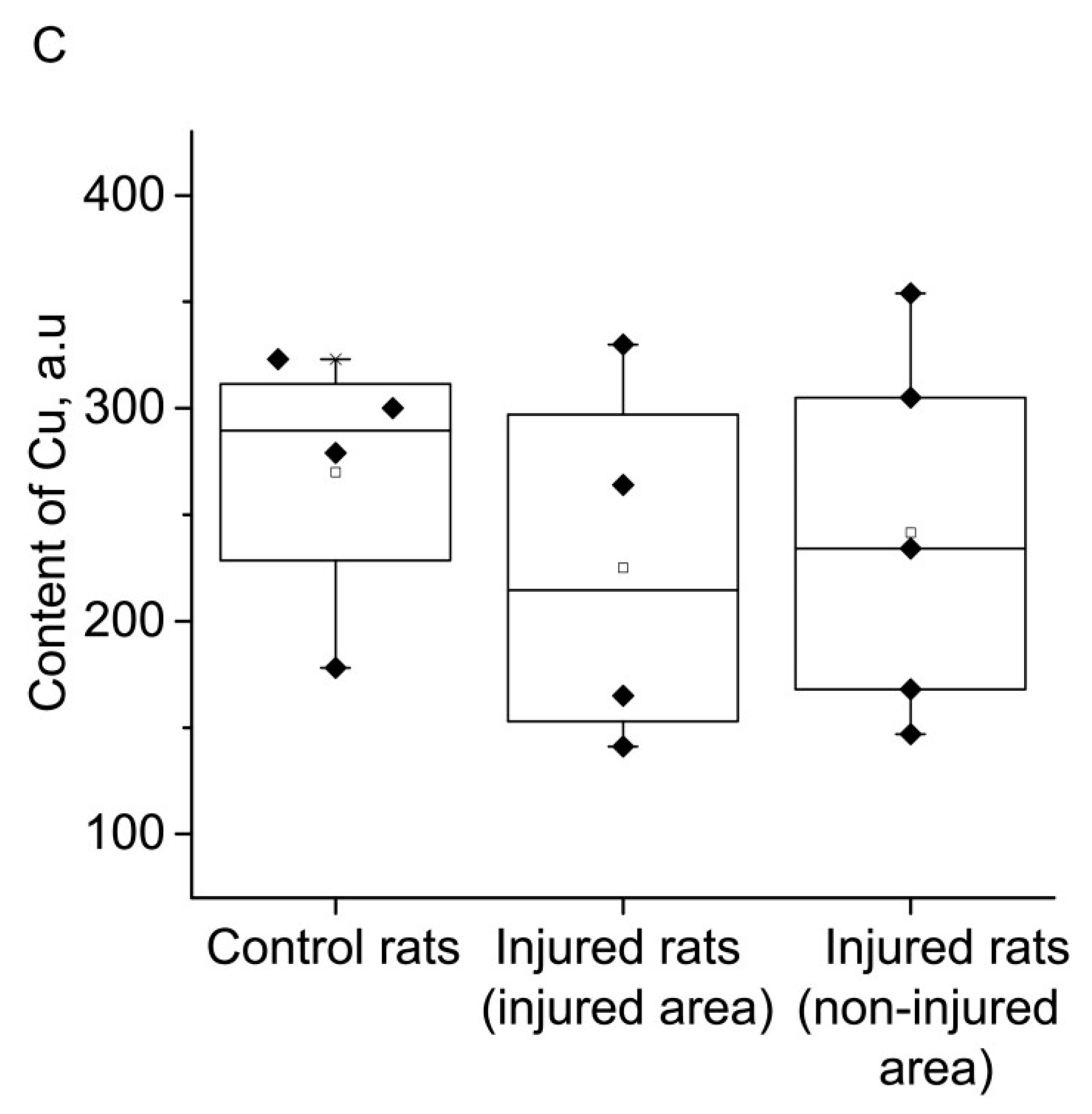
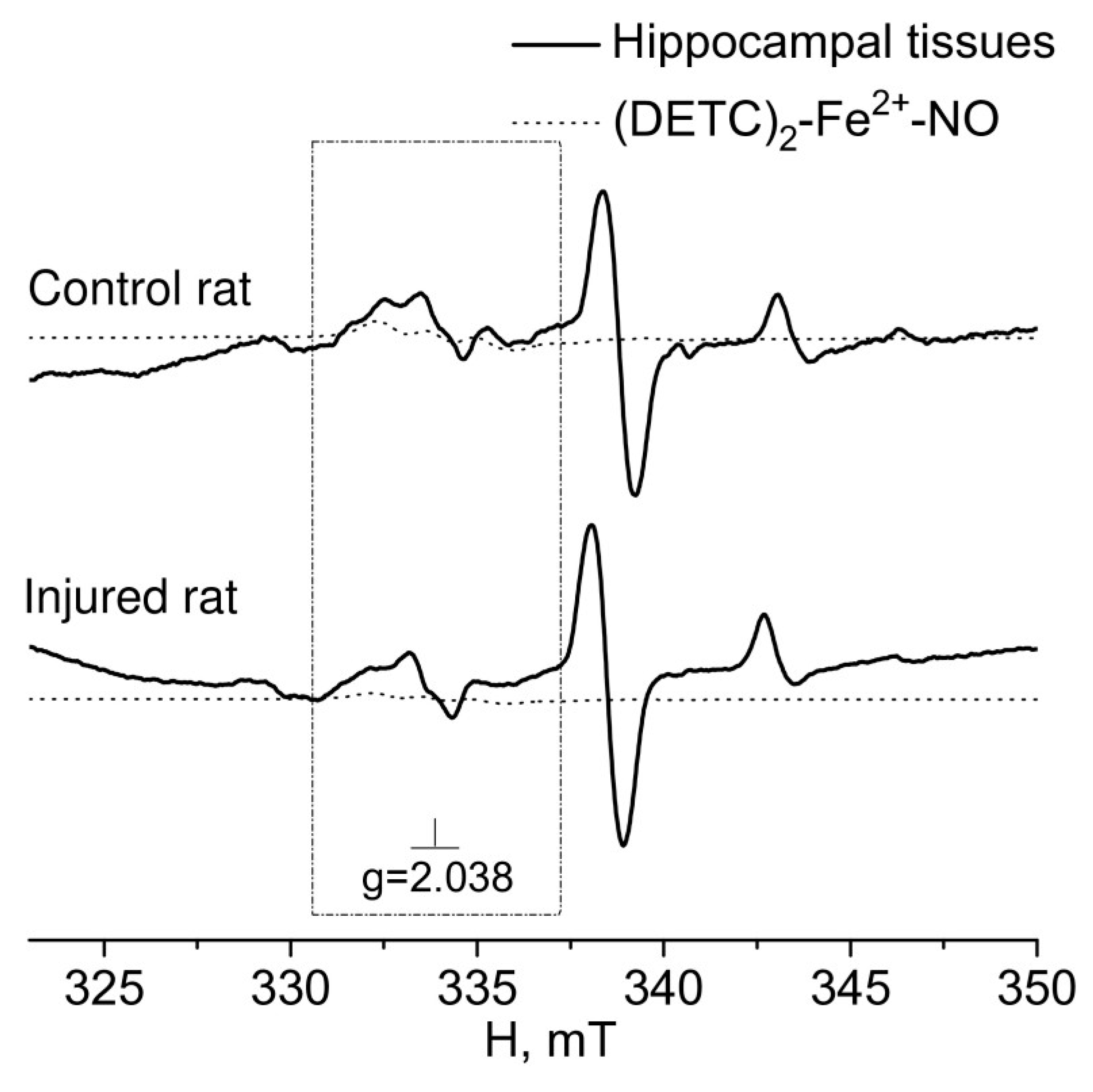
Figure 5 presented the EPR spectra of the hippocampus tissue of intact-control (Control rat) and injured ((Injured rat) rats seven days after a combined injury to the brain and spinal cord. The spectroscopic characteristics of the complexes observed in our experiments closely resembled those obtained in previous studies [80,81,82]. The g-factor was determined to be g﬩= 2.025 for Cu2+-(DETC)2 and g = 2.035 for (DETC)2-Fe2+-NO. The EPR signal for this complex exhibits a triplet hyperfine structure. Similar data were previously obtained [84].
The results of spectrum analysis, as shown in Figure 5, indicated no significant (reliable) changes in NO production in the hippocampus following the modeling of a combined injury to the brain and spinal cord (an unreliable decrease of 34%). Furthermore, there was no observed alteration in the copper content, suggesting no changes in the activity of the antioxidant system.
Figure 5.
EPR spectrum of hippocampus tissues of the control (Control rat) and injured (Injured rat) rats 7 days after a combined injury to the brain and spinal cord. The signals of the tissue sample and the calculated spectrum of the (DETC)2-Fe2+-NO complex in the observed spectrum were shown, The signals were from: a) tissue sample, b) (DETC)2-Fe2+-NO complex, and c) Cu(DETC)2 complex. The dotted line showed the contribution of NO to the observed signal. The frame showed the signal area (DETC)2-Fe2+-NO complex. Temperature is 77o K. The rats were injected with (DETC)2-Fe2+ - citrate. gср=2.038.
Figure 5.
EPR spectrum of hippocampus tissues of the control (Control rat) and injured (Injured rat) rats 7 days after a combined injury to the brain and spinal cord. The signals of the tissue sample and the calculated spectrum of the (DETC)2-Fe2+-NO complex in the observed spectrum were shown, The signals were from: a) tissue sample, b) (DETC)2-Fe2+-NO complex, and c) Cu(DETC)2 complex. The dotted line showed the contribution of NO to the observed signal. The frame showed the signal area (DETC)2-Fe2+-NO complex. Temperature is 77o K. The rats were injected with (DETC)2-Fe2+ - citrate. gср=2.038.
3. DISCUSSION
Traumatic and ischemic brain injuries remain prominent challenges in modern medicine [15,27,74,78,85]. The investigation of reparative processes in nervous tissue and the development of innovative methods to restore neuronal structures are currently focal points in physiology and medicine. These research efforts hold substantial significance for advancing novel therapeutic and rehabilitation strategies [43,52,86].
Trauma and ischemia of the brain involve various pathological mechanisms that contribute to the disruption of nerve and glial cell integrity, as well as damage to blood vessels [15,86,87]. The shared similarities in certain stages of the pathogenesis between these cerebral lesions imply that therapeutic strategies aimed at protecting nervous tissue after ischemic events may also be applicable after brain injuries [54,60,89,90]. All these processes undergo significant changes when nervous tissue is damaged due to injury or stroke, whether of ischemic or hemorrhagic nature.
Brain injuries disrupt the functioning of neural networks primarily due to mechanical damage to nervous tissue and blood vessels [54,91]. Apart from traumatic brain injury, dysfunctions of neurons and glia can develop due to compromised blood flow and the formation of hemorrhagic foci. In hemorrhagic strokes, the mechanical factor of nervous tissue compression in the cranial cavity is also present due to the formation of a hematoma. In ischemic strokes, brain tissue damage occurs due to hypoxia resulting from blood flow disturbances in the internal carotid arteries and/or vertebrobasilar region [63]. Oxygen supply disruption to brain regions also occurs during blood vessel thrombosis or aneurysm rupture, which often leads to ischemic or hemorrhagic stroke [14,15]. During reperfusion, despite the restoration of blood flow to the ischemic area, a large number of free radicals (both reactive nitrogen forms and reactive oxygen forms) are produced, which serve as important factors of ischemic reperfusion injury [55] (Wang et al., 2022).
In these processes of hypoxia-ischemia and mechanical brain damage, the role of NO appears to be contradictory, capable of both neurotoxic and neuroprotective functions [28,51]. Consequently, similarities are observed in the pathogenesis of brain injury and ischemic damage.
Using EPR spectroscopy, we investigated the intensity of NO production and the copper content in both injured and non-injured areas of the brain (frontal lobes), as well as in the hippocampus during the simulation of a combined injury to the brain and spinal cord. These molecular components have long been of interest to researchers studying the mechanisms of brain function in normal and pathological conditions. Various methodological approaches are employed for experimental analysis, with EPR spectroscopy being one of the most sensitive techniques available [92,93]. Significantly, the electron spin trap method for detecting and quantifying NO in biological tissues, developed by Prof. A.F. Vanin and colleagues, has played a crucial role in advancing the EPR spectroscopy technique [94].
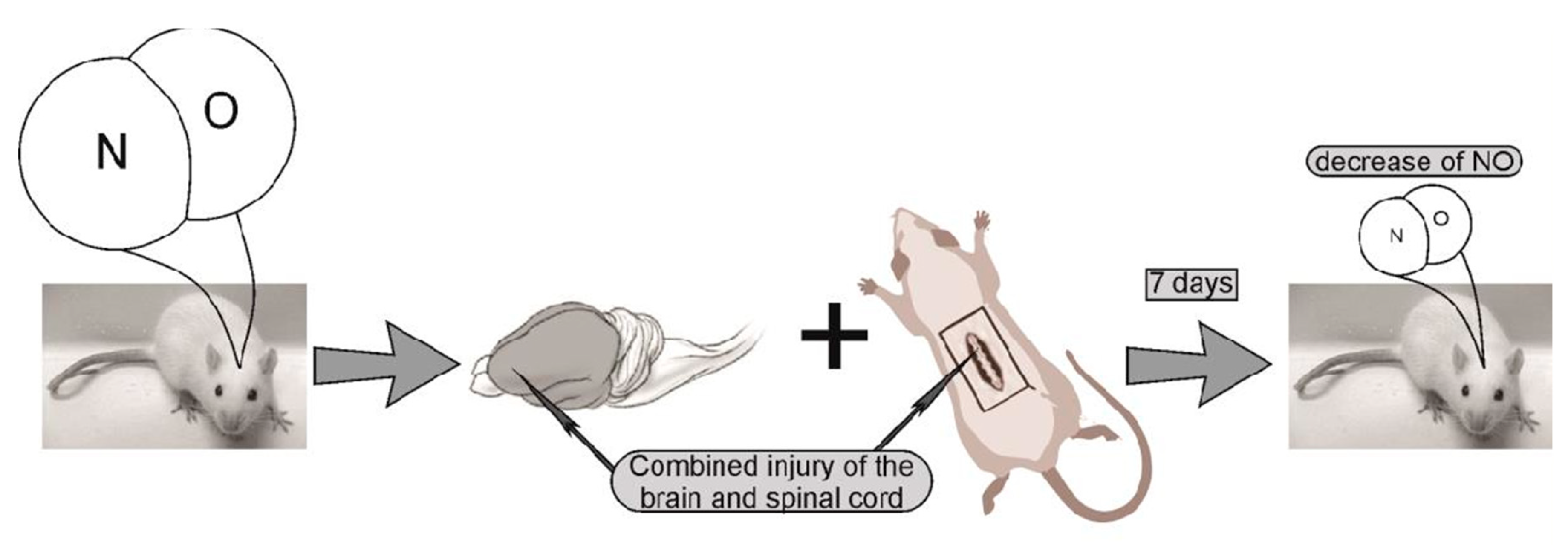
The experimental analysis of brain injuries revealed a notable reduction in NO production seven days after injury simulation, both in the injured and non-injured (contralateral) areas of the brain. These results showed a distinct difference in NO production between the damaged and contralateral regions of the brain. In the experimental data on the control samples, there were two data points close to 60; they are very different from the others. We carried out a processing option when excluding these two points from statistical analysis, in this case a significant difference was obtained, both when comparing the two groups separately ("Control rats", "Injured rats-injured area") by t-test (P = 0.021), and when comparing all three groups by ANOVA test. In this case, a posteriori tests of different types showed a significant difference between these two groups. We offered a general idea of the processes of behavioral changes and the dynamics of nitric oxide in Figure 7.
Figure 6.
The content of NO (A) and Cu (B) in the hippocampus of the control (Control rats) and injured (Injured rats) rats 7 days after the combined injury of the brain and spinal cord. The average integral intensity of the (DETC)2-Fe2+-NO and Cu(DETC)2 signals was also shown in the figure.
Figure 6.
The content of NO (A) and Cu (B) in the hippocampus of the control (Control rats) and injured (Injured rats) rats 7 days after the combined injury of the brain and spinal cord. The average integral intensity of the (DETC)2-Fe2+-NO and Cu(DETC)2 signals was also shown in the figure.
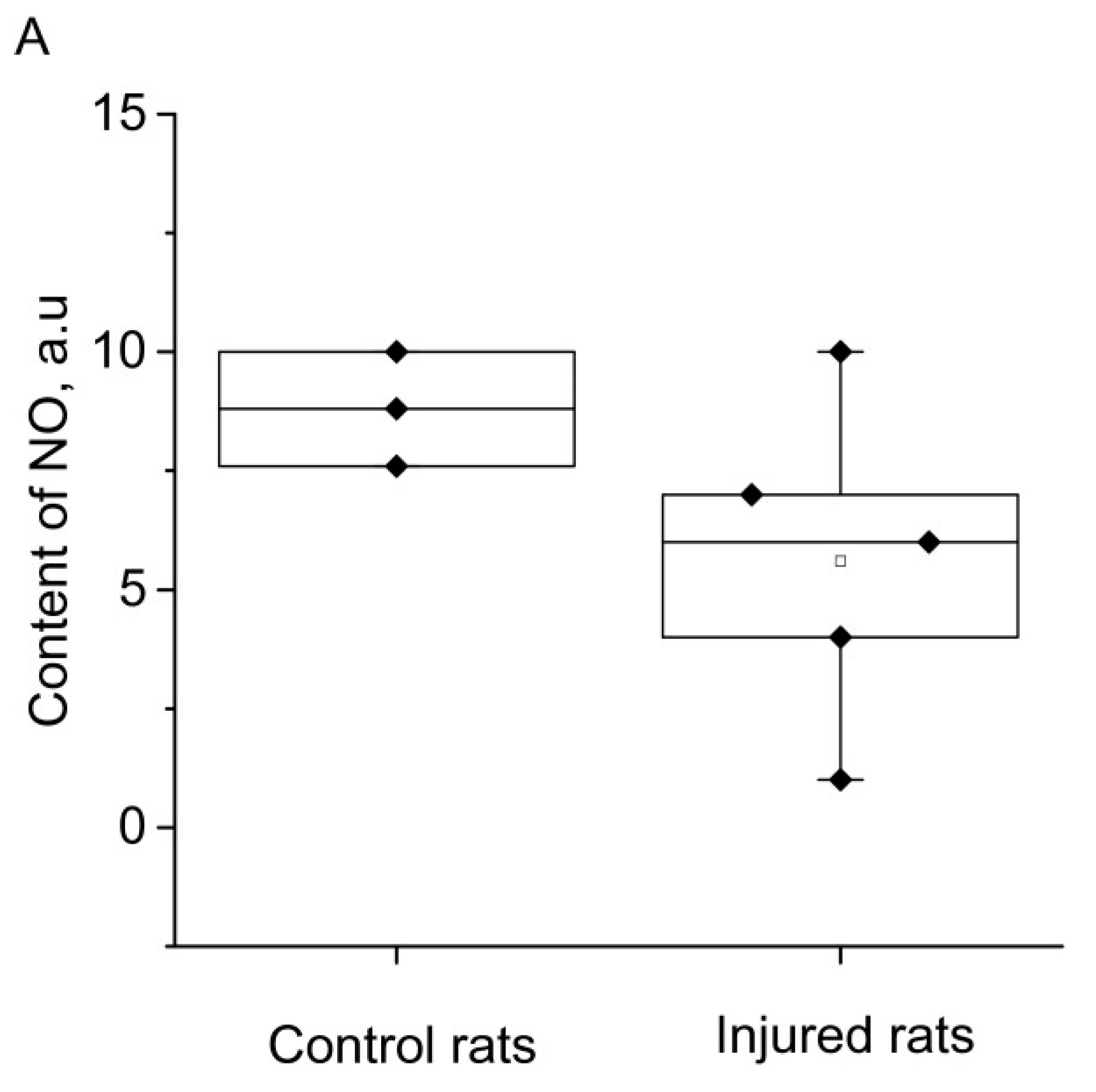
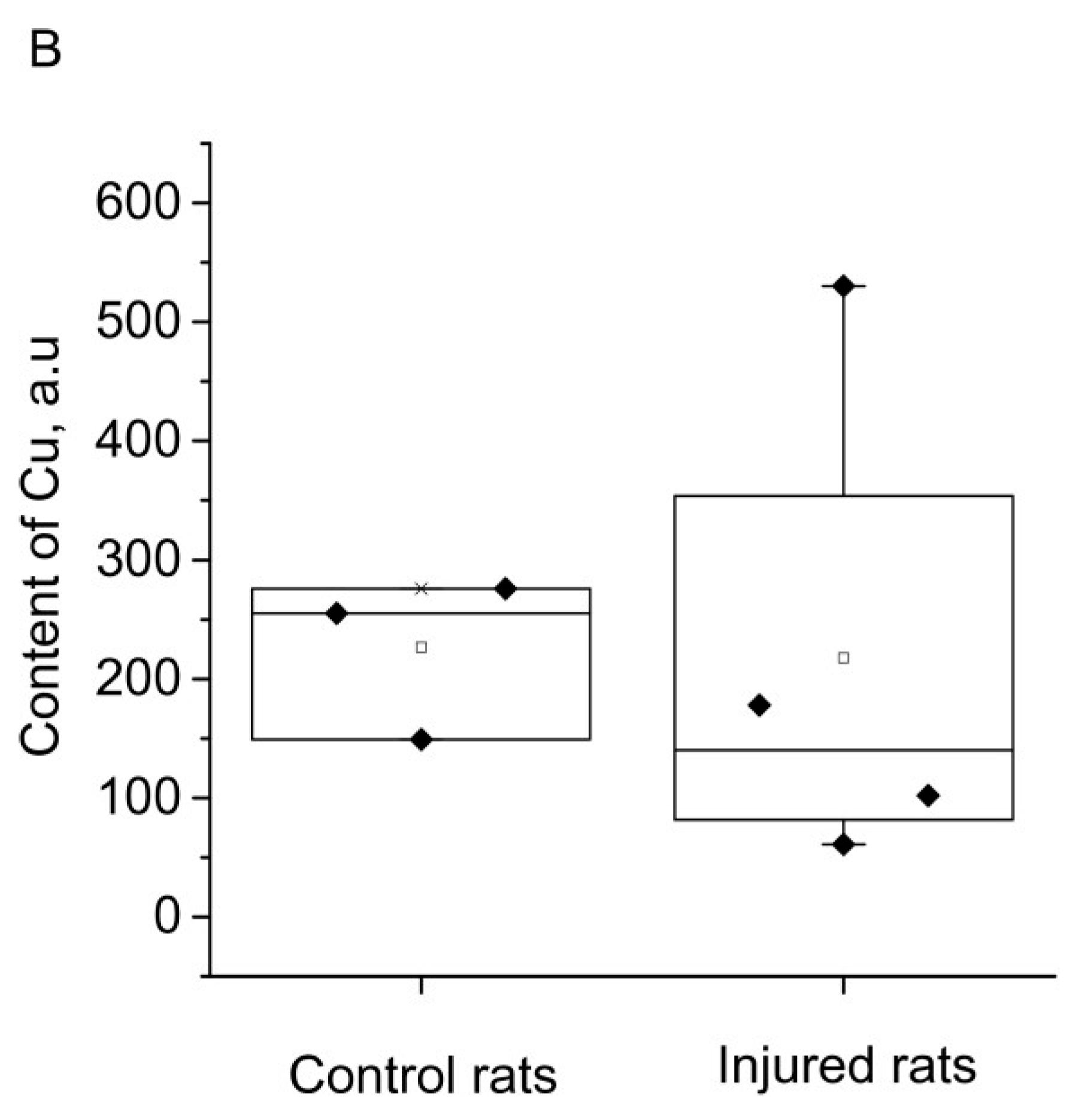
Figure 7.
An experimental scheme demonstrating the NO content in the injured and non-injured areas of the rat brain 7 days after a combined brain and spinal cord injury.
Figure 7.
An experimental scheme demonstrating the NO content in the injured and non-injured areas of the rat brain 7 days after a combined brain and spinal cord injury.
In contrast, the copper content remained unchanged after seven days of injury modeling. Consequently, the trauma led to a significant decrease in NO production in both the injured and the contralateral intact brain area, while no alterations were observed in the antioxidant system's activity. Notably, no changes in NO production and copper content were observed in the hippocampus. This finding aligned with our previous measurements, where brain injury was simulated using a different approach [78].
Considering the limited efficacy of current therapeutic approaches for brain injuries and strokes, and ongoing debates regarding the reperfusion period, it is prudent to conduct more in-depth research into the mechanisms and therapeutic potential of existing therapies. Moreover, it is essential to take into account the experimental findings presented by the authors of the article. These results highlighted notable distinctions in the dynamics of nitrosyl stress and the status of antioxidant protection between brain trauma and hemorrhagic stroke. Such differences offered an experimental foundation for the development of novel comprehensive therapeutic tactics in this field of medicine.
4. EXPERIMENTAL PROCEDURES
4.1. Animals
The study involved twenty male rats (n=10) weighing between 200 and 300 grams. The rats were housed in standard vivarium conditions with ad libitum access to food and water. The brain and spinal cord injury modeling was conducted at the Center of the Brain, Institute of Physiology, National Academy of Sciences of Belarus in Minsk. The experimental procedures followed the approved protocol of the Ethics Commission (Protocol No. 1, dated January 31, 2019; Ethic Committee Name: Ethics Commission of the Institute of Physiology, National Academy of Sciences of Belarus, Minsk; Approval Code: Approval code Е7/04/2023; Approval Date: dated January 31, 2019) of the Institute of Physiology, National Academy of Sciences of Belarus, Minsk. Tissue samples from the injured and non-injured areas of the frontal lobes of the brain, as well as the hippocampus, were collected seven days after the surgery (n=5), with ten rats in the experimental group and ten intact rats serving as the control group (n=5). These dates were chosen for two reasons: on the one hand, it is the accounting of data in previously conducted experiments with immunohistochemical staining of damaged areas of the brain [95], and, on the other hand, it is behavioral experiments [96]. Then, the biological samples were then transported from Minsk to Kazan in specialized containers. There were 20 animals left in Minsk after modeling brain and spinal cord injuries, which were continued to be observed for a month after the start of the experiment to assess the effectiveness of restoring central control of motor functions.
4.2. Experiment protocol. Modeling of combined trauma of the brain and spinal cord in rats
All surgical procedures were conducted on the anesthetized animals using a combination of ketamine (55.6 mg/kg), xylazine (5.5 mg/kg), and acepromazine (1.1 mg/kg), administered intraperitoneally [97].
Laboratory rats were anesthetized and secured in the prone position on the surgical table stretched by the limbs. The head of the animal was firmly secured, and the cranial vault area was prepared by removing hair and applying a 2% iodine solution to sterilize the skin. A midline incision of 10-12 mm was made along the cranial midline using a scalpel to access the underlying tissues. Locally, the periosteum was carefully dissected over the precentral gyrus, and a craniotomy was performed using a drill. The precentral region of the brain on the left hemisphere was then specifically targeted for localized brain tissue damage using a stylet. The procedure lasted approximately 3-4 minutes. Following the intervention, the incision was sutured, and the skin was treated again with a 2% iodine solution to minimize the risk of infection.
At the next stage, we continued to conduct a surgical procedure but already at the lumbar spinal cord level. The hair in the lumbar region was removed, and the skin was sterilized using a 2% iodine solution. A longitudinal incision was made through the skin and soft tissues, aligning with the projection of the lumbar vertebrae. With utmost care, the stylet was inserted into the spinal cord at the level of the first lumbar vertebra. When the stylet was removed, the duration of wound bleeding was observed and noted in the diary. Once the bleeding ceased, the wound was closed with two sutures, and the skin was treated again with a 2% iodine solution.
Before the operation, a day after the operation and a week (seven days) after the operation, pain thresholds (hot plate, tail-flick reflex) were determined in all animals.
After a period of one week (seven days) following the surgical procedure, tissue samples were extracted from both the injured area and the non-injured contralateral region of the brain (frontal lobe), specifically from the frontal lobe. Additionally, tissue samples were collected from the hippocampus. The control group of animals (n=5) did not undergo surgical interventions and served as a baseline for comparison.
4.3. Formation of a (DETC)2-Fe2+-NO complex with a spin trap in rats tissues
The problem of quantitative determination of NO in living systems needs an unambiguous solution, since binding of all NO produced by living organisms with iron-dithiocarbamate traps is in principle impossible, since part of the free NO molecules bypasses the traps. Nevertheless, their complete capture is theoretically possible and can be achieved through the use of ultra-high concentrations of NO traps in cells and tissues. However, this approach entails significant disturbances in cellular metabolism [98]. The major challenge in accurately determining the concentration of nitric oxide in its free form within tissues and body fluids is due to its highly reactive nature and short lifespan, resulting in low concentrations. Currently, the electron paramagnetic resonance (EPR) method is extensively employed for measuring NO production in biological systems [48,92,93]. EPR spectroscopy has emerged as one of the most reliable techniques for detecting and quantifying NO levels in biological tissues, especially when the technique of spin traps was proposed. In 1984, Vanin and colleagues proposed using a divalent iron complex with diethyldithiocarbamate (DETC) as a trap for NO in animal cells and tissues [99]. This method relies on the formation of a complex between Fe2+ and diethyldithiocarbamate (DETC) to capture NO and generate a stable ternary complex, denoted as (DETC)2-Fe2+.
In this study, this spin trap technique was utilized for measurements. To form a spin trap, DETC-Na was injected intraperitoneally at a dose of 500 mg/ kg in 2.5 ml of water. Like previous experiments, DETC-Na was administered intraperitoneally at a dose of 500 mg/kg in 2.5 ml of water. Next, a solution mixture consisting of ferrous sulfate (FeSO4 x 7 H2O, Sigma, USA) at a dose of 37.5 mg/kg and sodium citrate at a dose of 187.5 mg/kg (in a volume of 1 ml of water per 300 g of animal weight) was prepared immediately before injection [49,84]. In a mixture of iron sulfate and sodium citrate, iron citrate was formed. DETC-Na and iron citrate were delivered to the cells with blood flow. in the presence of NO, a paramagnetic complex (DETC)2-Fe2+-NO was formed (Figure 1), which was insoluble in water, was stable and could persist for a long time. The half-life of this molecule at room temperature is approximately 1.5 hours [80]. DETC-Na and iron citrate were distributed throughout the body and form a complex (DETC)2-Fe2+. Spin trap complex with NO (DETC)2-Fe2+-NO is characterized by an easily recognizable EPR spectra with a g-factor value of g=2.038 and a triplet hyperfine structure [80,82,100,101].
In the experimental group, areas of brain damage and contralateral areas in the frontal lobes, as well as hippocampal tissue, were obtained after decapitation and trepanation by few seconds. The tissue samples were then packed in an insulin syringe and placed in a container with liquid nitrogen. The inner diameter of the syringe matched the inner diameter of the finger Dewar, facilitating the measurement process of the tissue samples. Similar areas of the brain from rats weighing 100-200 mg in the control group were also collected and treated in the same manner for comparison.
4.4. Measurements of a (DETC)2-Fe2+-NO and Cu(DETC)2 complexes in rats tissues
The spectrum of the biological samples complexes were recorded using a Bruker X-band (9.5320 GHz) EMX/plus spectrometer. The sample in a Broker finger Dewar was placed in a 2-cavity of double resonator (model ER 4105DR) at a magnetic field modulation frequency of 100 kHz, modulation amplitude of 2 G, microwave radiation power of 2 mW, time constant of 327 ms and temperature of 77° K. Throughout the experiments, the modulation amplitude, gain, and microwave power settings were carefully selected to ensure that overmodulation and saturation of the electron paramagnetic resonance signal were avoided. These parameters remained consistent across all measurements. The sample weight used for the experiments was approximately 100-200 mg. The amplitude of the EPR spectra was consistently normalized to the sample weight to ensure accurate comparison and analysis [48].
The finger Dewar sample was placed in a 2-cavity of double resonator and the reference sample was placed in another cavity of the same resonator. Since each test sample was under the same conditions as the reference sample, this made it possible to quantify the intensity of the test samples and compare them in intensity with each other. Figure 1 demonstrated the EPR spectrum of the rat frontal lobe sample. Signals from different paramagnetic particles (complexes) were present in this spectrum. In the magnetic field area from 330 to 337 mT, there was an overlap of signals of the spin trap complex with NO (DETC)2-Fe2+-NO, which was characterized by an easily recognizable EPR spectra with a g-factor value of g=2.038 and a triplet hyperfine structure, as well as the second line of the Cu2+-(DETC)2 complex with a g-factor value of 2.04. As known, the spectra of this complex was represented by four lines [81,82,102,103]. This signal was present in our measurements in the field range from 335 to 343 mT.
Signal intensity from complexes (DETC)2-Fe2+-NO and Cu2+-(DETC)2 was determined sequentially. First, the intensity of the Cu2+-(DETC)2 signal was calculated along its right most line by the difference between the minimum and maximum of the line signal [71,73]. Then, the signal from the Cu2+-(DETC)2 complex was subtracted from the observed spectra with the intensity found in this way. Thus, we got rid of the contribution of the signal from the Cu2+-(DETC)2 complex in the area where the signal from the complex (DETC)2-Fe2+-NO is observed. Then the signal intensity (DETC)2-Fe2+-NO was determined by the difference between the maximum of the first line and the minimum of the third line of the triplet in the remaining spectrum. By this way the signal intensity from the Cu2+-(DETC)2 complex was calculated first, and then adjusted for this signal, the signal intensity from the complex (DETC)2-Fe2+-NO was calculated.
4.5. Statistical processing of the result.
The data are presented as mean ± standard error of the mean (M ± m). Statistical analysis was performed using Student's t-test and Mann-Whitney test. Differences were considered significant at p<0.05.
Author Contributions
KG and VK were the principal investigators, they conceived of the study, responsible for conception its design, coordination and responsible for final approval. KG, TB and VK wrote the paper. KG, VK, VA and GY participated in interpretation of results. KG, VK and MP conducted the literature search. MP handled the language and provided some comments. GY, EF, TF and AN carried out the modeling of combined injury of the brain and spinal cord. LB responsible for the operation of the EPR spectrometer. LB, ID, LM, DS and AA carried out measurements of EPR spectrum of samples. VA proposed a technique for processing EPR spectra. VA and TB carried out calculations and analysis of NO and cooper signals in EPR spectra of samples intensity. VA, ID and DS proposed a graphic abstract scheme. VA created the original figures.
Funding
The modeling of injuries to the brain and spinal cord was conducted at the Center for the Brain, Institute of Physiology, National Academy of Sciences of Belarus (Minsk, Belarus). The research was supported by the Belarusian Republican Foundation for Basic Research under grant M23RNF-067. The measurements of EPR spectra and data processing were performed at the Zavoisky Physical-Technical Institute of the Russian Academy of Sciences, this work received support from the RSF grant no. 23-45-10004.
Acknowledgments
The authors acknowledge Abdulla Chihab for his assistance in preparing the publication.
Conflict of interest
The authors declare no conflict of interest.
References
- Garthwaite, J. Concepts of neural nitric oxide-mediated transmission. Eur. J. Neurosci. 2008, 27, 2783–2802. [CrossRef]
- Steinert, J.R.; Chernova, T.; Forsythe, I.D. Nitric Oxide Signaling in Brain Function, Dysfunction, and Dementia. Neurosci. 2010, 16, 435–452. [CrossRef]
- Santos, R.M.; Lourenço, C.F.; Ledo, A.; Barbosa, R.M.; Laranjinha, J. Nitric Oxide Inactivation Mechanisms in the Brain: Role in Bioenergetics and Neurodegeneration. Int. J. Cell Biol. 2012, 2012, 1–13. [CrossRef]
- Maggio, D.M.; Singh, A.; Iorgulescu, J.B.; Bleicher, D.H.; Ghosh, M.; Lopez, M.M.; Tuesta, L.M.; Flora, G.; Dietrich, W.D.; Pearse, D.D. Identifying the Long-Term Role of Inducible Nitric Oxide Synthase after Contusive Spinal Cord Injury Using a Transgenic Mouse Model. Int. J. Mol. Sci. 2017, 18, 245. [CrossRef]
- Lundberg, J.O.; Weitzberg, E. Nitric oxide signaling in health and disease. Cell 2022, 185, 2853–2878. [CrossRef]
- Boehning, D.; Snyder, S.H. Novel neural modulators Annu. Rev. Neurosci. 2003, 26, 105-131. [CrossRef]
- Calabrese, V.; Cornelius, C.; Rizzarelli, E.; Owen, J.B.; Dinkova-Kostova, A.T.; Butterfield, D.A. Nitric Oxide in Cell Survival: A Janus Molecule. Antioxidants Redox Signal. 2009, 11, 2717–2739. [CrossRef]
- Balaban, P.M.; Roshchin, M.; Timoshenko, A.K.; Gainutdinov, K.L.; Bogodvid, T.K.; Muranova, L.N.; Zuzina, A.B.; Korshunova, T.A. Nitric oxide is necessary for labilization of a consolidated context memory during reconsolidation in terrestrial snails. Eur. J. Neurosci. 2014, 40, 2963–2970. [CrossRef]
- Moroz, L.L. Gaseous transmission across time and species. Am Zool. 2015, 41, 304-320.
- Reutov, V.P.; Okhotin, V.E.; Shuklin, A.V.; Sorokina, E.G.; Kosicin, N.S.; Gurin, Nitric oxide and the cycle in the myocardium: molecular, biochemical and physiological aspects. V.N. Uspehi fiziologicheskih nauk 2007, 38, 39-58. (in Russian).
- Andrianov, V.V.; Sitdikov, F.G.; Gainutdinov, Kh.L.; Yurtaeva, S.V.; Muranova, L.N.; Obynochnyi, A.A.; Karimov, F.K.; Chiglintsev, V.M.; Iyudin, V.S. Changes in nitric oxide in heart of intact and sympathectomized rats of different age. Russ. J. Develop. Biol. 2008, 38 (6), 352-356.
- Baider, L.M.; Reutov, V.P.; Krushinsky, A.L.; Kuzenkov, V.S.; Sorokina, E.G.; Koshelev, V.B.; Fadyukova, O.E.; Djumbaeva, T.T.; Komissarova, L.Kh.; Pinelis, V.G. et al Investigation by method of EPR of influence of hypoxia on nitric oxide (NO) production in blood of rats Krushinskii-Molodkina. Biofizika 2009, 54(5), 894-899. (in Russian).
- Tennyson, A.G.; Lippard, S.J. Generation, Translocation, and Action of Nitric Oxide in Living Systems. Chem. Biol. 2011, 18, 1211–1220. [CrossRef]
- Liu, H.; Li, J.; Zhao, F.; Wang, H.; Qu, Y.; Mu, D. Nitric oxide synthase in hypoxic or ischemic brain injury. Rev. Neurosci. 2015, 26, 105–17. [CrossRef]
- Garry, P.S.; Ezra, M.; Rowland, M.J.; Westbrook, J.; Pattinson, K.T. The role of the nitric oxide pathway in brain injury and its treatment - from bench to bedside. Exp. Neurol. 2015, 263, 235-243. [CrossRef]
- Sukmanskiy, O.I.; Reutov, V.P. Gasotransmitters: physiological role and involvement in the pathogenesis of diseases. Uspekhi fiziol. nauk 2016, 47(3), 30-58. (In Rus).
- Sobrevia, L.; Ooi, L.; Ryan, S.; Steinert, J.R. Nitric Oxide: A Regulator of Cellular Function in Health and Disease. Oxidative Med. Cell. Longev. 2015, 2016, 1–2. [CrossRef]
- Balez, R.; Ooi, L. Getting to NO Alzheimer’s Disease: Neuroprotection versus Neurotoxicity Mediated by Nitric Oxide. Oxidative Med. Cell. Longev. 2015, 2016, 1–8. [CrossRef]
- Dubey, H.; Gulati, K.; Ray, A. Effects of Nitric Oxide (NO) Modulators on Cognitive Function and Brain Oxidative Stress in Experimental Model of Alzheimers Disease in Rats. J Pharmacol Rep. 2017, 2, 2.
- Vanin, A.F. Dinitrosyl iron complexes and S-nitrosothiols are two possible forms of stabilization and transport of nitric oxide in biosystems. Biohimia 1998, 63, 924-938. (in Russian).
- Ignarro, L.J.; Cirino, G.; Casini, A.; Napoli, C. Nitric Oxide as a Signaling Molecule in the Vascular System: An Overview. J. Cardiovasc. Pharmacol. 1999, 34, 879–886. [CrossRef]
- Manukhina, E.B.; Malyshev, I.Y. Stress-limiting nitric oxide system. Rossijskii fiziologicheskii zhurnal im. I. M. Sechenova 2000, 86, 1283-1292. (in Russian).
- Luiking, Y.C.; Engelen, M.P.; Deutz, N.E. Regulation of nitric oxide production in health and disease. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 97–104. [CrossRef]
- A Heinrich, T.; da Silva, R.S.; Miranda, K.M.; Switzer, C.H.; A Wink, D.; Fukuto, J.M. Biological nitric oxide signalling: chemistry and terminology. Br. J. Pharmacol. 2013, 169, 1417–1429. [CrossRef]
- Pacher, P.; Beckman, J.S.; Liaudet, L. Nitric Oxide and Peroxynitrite in Health and Disease. Physiol. Rev. 2007, 87, 315–424. [CrossRef]
- Serrano, J.; Fernández, A.P.; Martínez-Murillo, R.; Alonso, D.; Rodrigo, J.; Salas, E.; Mourelle, M.; Martínez, A. The nitric oxide donor LA 419 decreases ischemic brain damage.. Int. J. Mol. Med. 2007, 19, 229–236. [CrossRef]
- Wierońska, J.; Cieślik, P.; Kalinowski, L. Nitric Oxide-Dependent Pathways as Critical Factors in the Consequences and Recovery after Brain Ischemic Hypoxia. Biomolecules 2021, 11, 1097. [CrossRef]
- Godecke, A.; Schrader, J. The Janus faces of NO Circ. Res. 2004, 94, e55-e57.
- Calabrese, V.; Mancuso, C.; Calvani, M.; Rizzarelli, E.; Butterfield, D.A.; Stella, A.M.G. Nitric oxide in the central nervous system: neuroprotection versus neurotoxicity. Nat. Rev. Neurosci. 2007, 8, 766–775. [CrossRef]
- Vanin, A.F. What is the Mechanism of Nitric Oxide Conversion into Nitrosonium Ions Ensuring S-Nitrosating Processes in Living Organisms. Cell Biochem. Biophys. 2019, 77, 279–292. [CrossRef]
- Samdani, A.F.; Dawson, T.M.; Dawson, V.L. Nitricoxide synthase in models of focal ischemia. Stroke 1997, 28, 1283.
- Vanin, A.F. What is the Mechanism of Nitric Oxide Conversion into Nitrosonium Ions Ensuring S-Nitrosating Processes in Living Organisms. Cell Biochem. Biophys. 1997, 77, 279–292. [CrossRef]
- Malyshev, I.Y.; Zenina, T.A.; Golubeva, L.Y.; Saltykova, V.A.; Manukhina, E.B.; Mikoyan, V.D.; Kubrina, L.N.; Vanin, A.F. NO-Dependent Mechanisms of Adaptation to Hypoxia. Nitric Oxide 1999, 3, 105–113. [CrossRef]
- Sato, S.; Tominaga, T.; Ohnishi, T.; Ohnishi, S.T. Electron paramagnetic resonance study on nitric oxide production during brain focal ischemia and reperfusion in the rat. Brain Res. 1994, 647, 91–96. [CrossRef]
- Tominaga, T.; Sato, S.; Ohnishi, T.; Ohnishi, S.T. Electron Paramagnetic Resonance (EPR) Detection of Nitric Oxide Produced during Forebrain Ischemia of the Rat. J. Cereb. Blood Flow Metab. 1994, 14, 715–722. [CrossRef]
- Chen, Y.; Irie, Y.; Keung, W.M.; Maret, W. S-Nitrosothiols React Preferentially with Zinc Thiolate Clusters of Metallothionein III through Transnitrosation. Biochemistry 2002, 41, 8360–8367. [CrossRef]
- Dawson, D.; Kusumoto, K.; Graham, D.; McCulloch, J.; Macrae, I. Inhibition of nitric oxide synthesis does not reduce infarct volume in a rat model of focal cerebral ischaemia. Neurosci. Lett. 1992, 142, 151–154. [CrossRef]
- Sancesario, G.; Iannone, M.; Morello, M.; Nisticò, G.; Bernardi, G. Nitric oxide inhibition aggravates ischemic damage of hippocampal but not of NADPH neurons in gerbils.. Stroke 1994, 25, 436–443. [CrossRef]
- Yamamoto, S.; Golanov, E.V.; Berger, S.B.; Reis, D.J. Inhibition of Nitric Oxide Synthesis Increases Focal Ischemic Infarction in Rat. J. Cereb. Blood Flow Metab. 1992, 12, 717–726. [CrossRef]
- Willmot, M.; Gray, L.; Gibson, C.; Murphy, S.; Bath, P.M. A systematic review of nitric oxide donors and l-arginine in experimental stroke; effects on infarct size and cerebral blood flow. Nitric Oxide 2005, 12, 141–149. [CrossRef]
- Jung, K.-H.; Chu, K.; Ko, S.-Y.; Lee, S.-T.; Sinn, D.-I.; Park, D.-K.; Kim, J.-M.; Song, E.-C.; Kim, M.; Roh, J.-K. Early Intravenous Infusion of Sodium Nitrite Protects Brain Against In Vivo Ischemia-Reperfusion Injury. Stroke 2006, 37, 2744–2750. [CrossRef]
- Evgenov, O.V.; Pacher, P.; Schmidt, P.M.; Haskó, G.; Schmidt, H.H.H.W.; Stasch, J.-P. NO-independent stimulators and activators of soluble guanylate cyclase: discovery and therapeutic potential. Nat. Rev. Drug Discov. 2006, 5, 755–768. [CrossRef]
- Godínez-Rubí, M.; Rojas-Mayorquín, A.E.; Ortuño-Sahagún, D. Nitric Oxide Donors as Neuroprotective Agents after an Ischemic Stroke-Related Inflammatory Reaction. Oxidative Med. Cell. Longev. 2013, 2013, 1–16. [CrossRef]
- Kuzenkov, V.S.; Krushinskiy, A.L. Protective effect of magnesium nitrate on cerebral ischemia. Vestnik Mosk.universiteta. Biologiya 2014, 4, 9-14. (In Rus).
- Yang, W.-C.; Wang, Y.-Z.; Li, T.-T.; Cao, H.-L. Recent advances in the neuroprotective effects of medical gases. Med Gas Res. 2019, 9, 80–87. [CrossRef]
- Dou, C.; Han, X.; Xie, H.; Liao, H.; Xiao, X.; Huang, Z.; Luo, G.; Zhang, X.; Yao, W. Protective role of nitric oxide donors on endothelium in ischemia-reperfusion injury: a meta-analysis of randomized controlled trials. BMC Anesthesiol. 2023, 23, 1–10. [CrossRef]
- Jung, P.; Ha, E.; Zhang, M.; Fall, C.; Hwang, M.; Taylor, E.; Stetkevich, S.; Bhanot, A.; Wilson, C.G.; Figueroa, J.D.; et al. Neuroprotective role of nitric oxide inhalation and nitrite in a Neonatal Rat Model of Hypoxic-Ischemic Injury. PLOS ONE 2022, 17, e0268282. [CrossRef]
- Gainutdinov, K.L.; Gavrilova, S.A.; Iyudin, V.S.; Golubeva, A.V.; Davydova, M.P.; Jafarova, G.G.; Andrianov, V.V.; Koshelev, V.B. EPR Study of the Intensity of the Nitric Oxide Production in Rat Brain After Ischemic Stroke. Appl. Magn. Reson. 2011, 40, 267–278. [CrossRef]
- Andrianov, V.V.; Pashkevich, S.G.; Yafarova, G.G.; Denisov, A.A.; Iyudin, V.S.; Bogodvid, T.K.; Dosina, M.O.; Kulchitsky, V.A.; Gainutdinov, K.L. Changes of Nitric Oxide Content in the Rat Hippocampus, Heart and Liver in Acute Phase of Ischemia. Appl. Magn. Reson. 2016, 47, 965–976. [CrossRef]
- Andrianov, V.V.; Yafarova, G.G.; Pashkevich, S.G.; Tokalchik, Y.P.; Dosina, M.O.; Zamaro, A.S.; Bogodvid, T.K.; Iyudin, V.S.; Bazan, L.V.; Kulchitsky, V.A.; et al. Changes of the Nitric Oxide and Copper Content in the Olfactory Bulbs of Rat Brain After Modeling of Brain Stroke and Intranasal Administration of Mesenchymal Stem Cells. Appl. Magn. Reson. 2020, 51, 375–387. [CrossRef]
- Deryagin, O.G.; Gavrilova, S.A.; Buravkov, S.V.; Andrianov, V.V.; Yafarova, G.G.; Gainutdinov, K.L.; Koshelev, V.B. The Role of ATP-Sensitive Potassium Channels and Nitric Oxide in the Protective Effect of Preconditioning of the Brain. Neurosci. Behav. Physiol. 2017, 48, 58–63. [CrossRef]
- Deryagin, O.G.; Gavrilova, S.A.; Gainutdinov, K.L.; Golubeva, A.V.; Andrianov, V.V.; Yafarova, G.G.; Buravkov, S.V.; Koshelev, V.B. Molecular Bases of Brain Preconditioning. Front. Neurosci. 2017, 11, 427–427. [CrossRef]
- Prajapati, K.D.; Devarakonda, C.B.; Joshi, A.R.; Sharma, S.S.; Roy, N. Role of nitric oxide synthases in cerebral ischemia. Current Res. and Information on Pharmaceut. Sci. 2011, 11(3), 50-56.
- Chen, Z.Q.; Mou, R.T.; Feng, D.X.; Wang, Z.; Chen, G. The role of nitric oxide in stroke. Med Gas Res. 2017, 7(3), 194-203. [CrossRef]
- Wang Y.; Hong F.; Yang S. Role of nitric oxide in brain ischemia and reperfusion. Int. J. Mol. Sci. 2022, 23, 4243. [CrossRef]
- Zhang, J.; Han, Y.; Wang, Y.; Cheng, X.; Wang, C.-J. Neuronal nitric oxide synthase inhibition reduces brain damage by promoting collateral recruitment in a cerebral hypoxia-ischemia mice model. 2018, 22, 3166–3172.
- Charriaut-Marlangue, C.; Bonnin, P.; Gharib, A.; Leger, P-L.; Villapol, S.; Pocard, M.; Gressens, P.; Renolleau, S.; Baud, Ol. Inhaled nitric oxide reduces brain dDamage by collateral recruitment in a neonatal stroke model. Stroke 2012, 43, 3078-3084.
- A Terpolilli, N.; Kim, S.-W.; Thal, S.C.; Kuebler, W.M.; Plesnila, N. Inhaled Nitric Oxide Reduces Secondary Brain Damage after Traumatic Brain Injury in Mice. J. Cereb. Blood Flow Metab. 2012, 33, 311–318. [CrossRef]
- A Terpolilli, N.; Feiler, S.; Dienel, A.; Müller, F.; Heumos, N.; Friedrich, B.; Stover, J.; Thal, S.; Schöller, K.; Plesnila, N. Nitric oxide inhalation reduces brain damage, prevents mortality, and improves neurological outcome after subarachnoid hemorrhage by resolving early pial microvasospasms. J. Cereb. Blood Flow Metab. 2016, 36, 2096–2107. [CrossRef]
- Remizova, M.I.; Kochetygov, N.I.; Gerbout, K.A.; Lakomkin, V.L.; Timoshin, A.A.; Burgova, E.N.; Vanin, A.F. Effect of dinitrosyl iron complexes with glutathione on hemorrhagic shock followed by saline treatment. Eur. J. Pharmacol. 2011, 662, 40–46. [CrossRef]
- A Terpolilli, N.; A Moskowitz, M.; Plesnila, N. Nitric Oxide: Considerations for the Treatment of Ischemic Stroke. J. Cereb. Blood Flow Metab. 2012, 32, 1332–1346. [CrossRef]
- Manukhina, E.B.; Malyshev, I.Y.; Smirin, B.V.; Mashina, S.Y.; Saltykova, V.A.; Vanin, A.F. Production and Storage of Nitric Oxide in Adaptation to Hypoxia. Nitric Oxide 1999, 3, 393–401. [CrossRef]
- Bolaños, J.P.; Almeida, A. Roles of nitric oxide in brain hypoxia-ischemia. Biochim. et Biophys. Acta (BBA) - Bioenerg. 1999, 1411, 415–436. [CrossRef]
- Capizzi, A.; Woo, J.; Verduzco-Gutierrez, M. Traumatic Brain Injury. Med Clin. North Am. 2020, 104, 213–238. [CrossRef]
- Ivanov, E.V.; Gavrilova, S.A.; Koshelev, V.B. Brain acute ischemia mechanisms: implications to experimental and clinical treatment. Reg. blood Circ. Microcirc. 2021, 20, 5-19. [CrossRef]
- Jia, Z.; Zhu, H.; Li, J.; Wang, X.; Misra, H.; Li, Y. Oxidative stress in spinal cord injury and antioxidant-based intervention. Spinal Cord 2011, 50, 264–274. [CrossRef]
- Banci, L.; Bertini, I.; Ciofi-Baffoni, S.; Kozyreva, T.; Zovo, K.; Palumaa, P. Affinity gradients drive copper to cellular destinations. Nature 2010, 465, 645–648. [CrossRef]
- Festa, R.A.; Thiele, D.J. Copper: An essential metal in biology. Curr. Biol. 2011, 21, R877–R883. [CrossRef]
- Miller, A.-F. Superoxide dismutases: Ancient enzymes and new insights. FEBS Lett. 2011, 586, 585–595. [CrossRef]
- Sheng, Y.; Abreu, I.A.; Cabelli, D.E.; Maroney, M.J.; Miller, A.-F.; Teixeira, M.; Valentine, J.S. Superoxide Dismutases and Superoxide Reductases. Chem. Rev. 2014, 114, 3854–3918. [CrossRef]
- Sheng, Y.; Capri, J.; Waring, A.; Valentine, J.S.; Whitelegge, J. Exposure of Solvent-Inaccessible Regions in the Amyloidogenic Protein Human SOD1 Determined by Hydroxyl Radical Footprinting. J. Am. Soc. Mass Spectrom. 2018, 30, 218–226. [CrossRef]
- Fukai, T.; Ushio-Fukai, M.; Kim, J.H.; Lee, M.-R.; Hong, Y.-C.; Choquet, H.; Trapani, E.; Goitre, L.; Trabalzini, L.; Akers, A.; et al. Superoxide Dismutases: Role in Redox Signaling, Vascular Function, and Diseases. Antioxidants Redox Signal. 2011, 15, 1583–1606. [CrossRef]
- Sehba, F.A.; Bederson, J.B. Mechanisms of acute brain injury after subarachnoid hemorrhage. Neurol. Res. 2006, 28, 381–398. [CrossRef]
- Cook, A.M.; Jones, G.M.; Hawryluk, G.W.J.; Mailloux, P.; McLaughlin, D.; Papangelou, A.; Samuel, S.; Tokumaru, S.; Venkatasubramanian, C.; Zacko, C.; et al. Guidelines for the Acute Treatment of Cerebral Edema in Neurocritical Care Patients. Neurocritical Care 2020, 32, 647–666. [CrossRef]
- Everitt, A.; Root, B.; Calnan, D.; Manwaring, P.; Bauer, D.; Halter, R. A bioimpedance-based monitor for real-time detection and identification of secondary brain injury. Sci. Rep. 2021, 11, 1–16. [CrossRef]
- Murthy, T.; Bhatia, P.; Sandhu, K.; Prabhakar, T.; Gogna, R. Secondary brain injury: Prevention and intensive care management. Indian J. Neurotrauma 2005, 2, 7–12. [CrossRef]
- Che, X.; Fang, Y.; Si, X.; Wang, J.; Hu, X.; Reis, C.; Chen, S. The Role of Gaseous Molecules in Traumatic Brain Injury: An Updated Review. Front. Neurosci. 2018, 12, 392. [CrossRef]
- Andrianov, V.V.; Kulchitsky, V.A.; Yafarova, G.G.; Zamaro, A.S.; Tokalchik, Y.P.; Bazan, L.V.; Bogodvid, T.K.; Iyudin, V.S.; Pashkevich, S.G.; Dosina, M.O.; et al. Comparative Study of the Intensity of Nitric Oxide Production and Copper Content in Hippocampus of Rats After Modeling of Hemorrhagic Stroke and Brain Injury. Appl. Magn. Reson. 2021, 52, 1657–1669. [CrossRef]
- Crobeddu, E.; Pilloni, G.; Tardivo, V.; Fontanella, M.M.; Panciani, P.P.; Spena, G.; Fornaro, R.; Altieri, R.; Agnoletti, A.; Ajello, M. et al Role of nitric oxide and mechanisms involved in cerebral injury after subarachnoid hemorrhage: is nitric oxide a possible answer to cerebral vasospasm? J Neurosurg Sci. 2016,60(3), 385-91. Epub 2015 Jan 20.
- Mikoyan, V.D.; Kubrina, L.N.; Serezhenkov, V.A.; Stukan, R.A.; Vanin, A.F. Complexes of Fe2+ with diethyldithiocarbamate or N-methyl-D-glucamine dithiocarbamate as traps of nitric oxide in animal tissues Biochim. Biophys. Acta 1997, 1336, 225-234.
- van Faassen, E.E.; Koeners, M.P.; Joles, J.A.; Vanin, A.F. Detection of basal NO production in rat tissues using iron–dithiocarbamate complexes. Nitric Oxide 2008, 18, 279–286. [CrossRef]
- Jakubowska, M.A.; Pyka, J.; Michalczyk-Wetula, D.; Baczyński, K.; Cieśla, M.; Susz, A.; Ferdek, P.E.; Płonka, B.K.; Fiedor, L.; Płonka, P.M. Electron paramagnetic resonance spectroscopy reveals alterations in the redox state of endogenous copper and iron complexes in photodynamic stress-induced ischemic mouse liver. Redox Biol. 2020, 34, 101566. [CrossRef]
- Gainutdinov, K.L.; Kulchitsky, V.A.; Andrianov, V.V.; Yafarova, G.G.; Tokalchik, Y.P.; Zamaro, A.S.; Bazan, L.V.; Bogodvid, T.K.; Iyudin, V.S.; Pashkevich, S.G.; et al. Application of EPR Spectroscopy to Study the Content of NO and Copper in the Frontal Lobes, Hippocampus, and Liver of Rats after Cerebral Ischemia. Tech. Phys. 2022, 67, 311–316. [CrossRef]
- Ismailova, A.I.; Gnezdilov, O.I.; Obynochny, A.A.; Muranova, L.N.; Andrianov, V.V.; Gainutdinov, K.L.; Nasyrova, A.G.; Nigmatullina, R.R.; Rakhmatullina, F.F.; Zefirov, A.L. ESR study of the nitric oxide production in tissues of animals under an external influence on the functioning of the cardiovascular and nervous systems. Appl. Magn. Reson. 2005, 28, 421–430. [CrossRef]
- AlRuwaili, R.; Al-Kuraishy, H.M.; Alruwaili, M.; Khalifa, A.K.; Alexiou, A.; Papadakis, M.; Saad, H.M.; Batiha, G.E.-S. The potential therapeutic effect of phosphodiesterase 5 inhibitors in the acute ischemic stroke (AIS). Mol. Cell. Biochem. 2023, 1–12. [CrossRef]
- Vanin, A.F. Dinitrosyl iron complexes with thiol-containing ligands as a “working form” of endogenous nitric oxide. Nitric Oxide 2016, 54, 15–29. [CrossRef]
- Maiese, K. The dynamics of cellular injury: transformation into neuronal and vascular protection. Histol. Histopathol. 2001, 16(2), 633-644. [CrossRef]
- Guo, Z.-N.; Shao, A.; Tong, L.-S.; Sun, W.; Liu, J.; Yang, Y. The Role of Nitric Oxide and Sympathetic Control in Cerebral Autoregulation in the Setting of Subarachnoid Hemorrhage and Traumatic Brain Injury. Mol. Neurobiol. 2015, 53, 3606–3615. [CrossRef]
- A Donnan, G.; Fisher, M.; Macleod, M.; Davis, S.M. Stroke. Lancet 2008, 371, 1612–1623. [CrossRef]
- Reutov, V.P.; Samosudova, N.V.; Sorokina, E.G. A Model of Glutamate Neurotoxicity and Mechanisms of the Development of the Typical Pathological Process. Biophysics 2019, 64, 233–250. [CrossRef]
- Zhang, R.L.; Zhang, Z.G.; Chopp, M. Targeting nitric oxide in the subacute restorative treatment of ischemic stroke. Expert Opin. Investig. Drugs 2013, 22, 843–851. [CrossRef]
- Vanin, A.F.; Huisman, A.; Van Faassen, E.E. Iron Dithiocarbamate as Spin Trap for Nitric Oxide Detection: Methods in Enzymology. Pitfalls and Successes 2003, 359, 27-42.
- Hogg, N. Detection of nitric oxide by electron paramagnetic resonance spectroscopy. Free. Radic. Biol. Med. 2010, 49, 122–129. [CrossRef]
- Vanin, A.F.; Mordvintcev, P.I.; Kleshchev, A.L. Appearance of nitrogen oxide in animal tissues in vivo. Studia Biophys. 1984, 102, 135-143.
- Shanko, Y.; Zamaro, A.; Takalchik, S.Y.; Koulchitsky, S.; Pashkevich, S.; Panahova, E.; Navitskaya, V.; Dosina, M.; Denisov, A.; Bushuk, S.; Kulchitsky, V. Mechanisms of neural network structures recovery in brain trauma. Biomed. J. Sci. Tech. Res. 2018, 7(5), MS.ID.001567.
- Bogodvid, T.; Pashkevich, S.; Dosina, M.; Zamaro, A.; Takalchik, Y.; Yafarova, G.; Andrianov, V.; Denisov, A.; Loiko, D.; Gainutdinov, K.; Kulchitsky, V. Effect of intranasal administration of mesenchymal stem cells on the approximate motor activity of rats after simulation of ischemic stroke. Eur. J. Clin. Investig. 2019, 49(Suppl 1, P146-T), 161. [CrossRef]
- Shanko, Y.; Navitskaya, V.; Zamaro, A.; Krivenko, S.; Zafranskaya, M.; Pashkevich, S.; Koulchitsky, S.; Takalchik–Stukach, Y.; Denisov, A.; Kulchitsky, V. Prospects of perineural administration of autologous mesenchymal stem cells of adipose tissue in patients with cerebral infarction. Biomed J Sci&Tech Res. 2018, 10(1), 1-3. [CrossRef]
- Vanin, A.; Poltorakov, A. NO spin trapping in biological systems. Front. Biosci. 2009, ume, 4427–35. [CrossRef]
- Vanin, A.F.; Mordvintcev, P.I.; Kleshchev, A.L. Appearance of nitric oxide in animal tissue in vivo. Studia Biophysica 1984, 107, 135-142.
- Plonka, P.M.; Chlopicki, S.; Wisniewska, M.; Plonka, B.K. Kinetics of increased generation of (.)NO in endotoxaemic rats as measured by EPR.. Acta Biochim. Pol. 2003, 50, 807–813. [CrossRef]
- Kleschyov, A.L.; Wenzel, P.; Munzel, T. Electron paramagnetic resonance (EPR) spin trapping of biological nitric oxide. J. Chromatogr. B 2007, 851, 12–20. [CrossRef]
- Tominaga, T.; Sato, S.; Ohnishi, T.; Ohnishi, S.T. Electron Paramagnetic Resonance (EPR) Detection of Nitric Oxide Produced during Forebrain Ischemia of the Rat. J. Cereb. Blood Flow Metab. 1994, 14, 715–722. [CrossRef]
- Suzuki, Y.; Fujii, S.; Tominaga, T.; Yoshimoto, T.; Yoshimura, T.; Kamada, H. The origin of an EPR signal observed in dithiocarmate-loaded tissues Copper (II)- dithiocarmate complexes account for the narrow hyperfine lines. Biochim. Biophys. Acta 1997, 1335, 242-245.
Figure 1.
EPR spectrum of tissue from frontal lobe of the rat (Sample - example). Determination of the signal from the Cu(DETC)2 complex and (DETC)2-Fe2+-NO complex with amplitudes equal to their contribution to the spectrum of the sample.
Figure 1.
EPR spectrum of tissue from frontal lobe of the rat (Sample - example). Determination of the signal from the Cu(DETC)2 complex and (DETC)2-Fe2+-NO complex with amplitudes equal to their contribution to the spectrum of the sample.
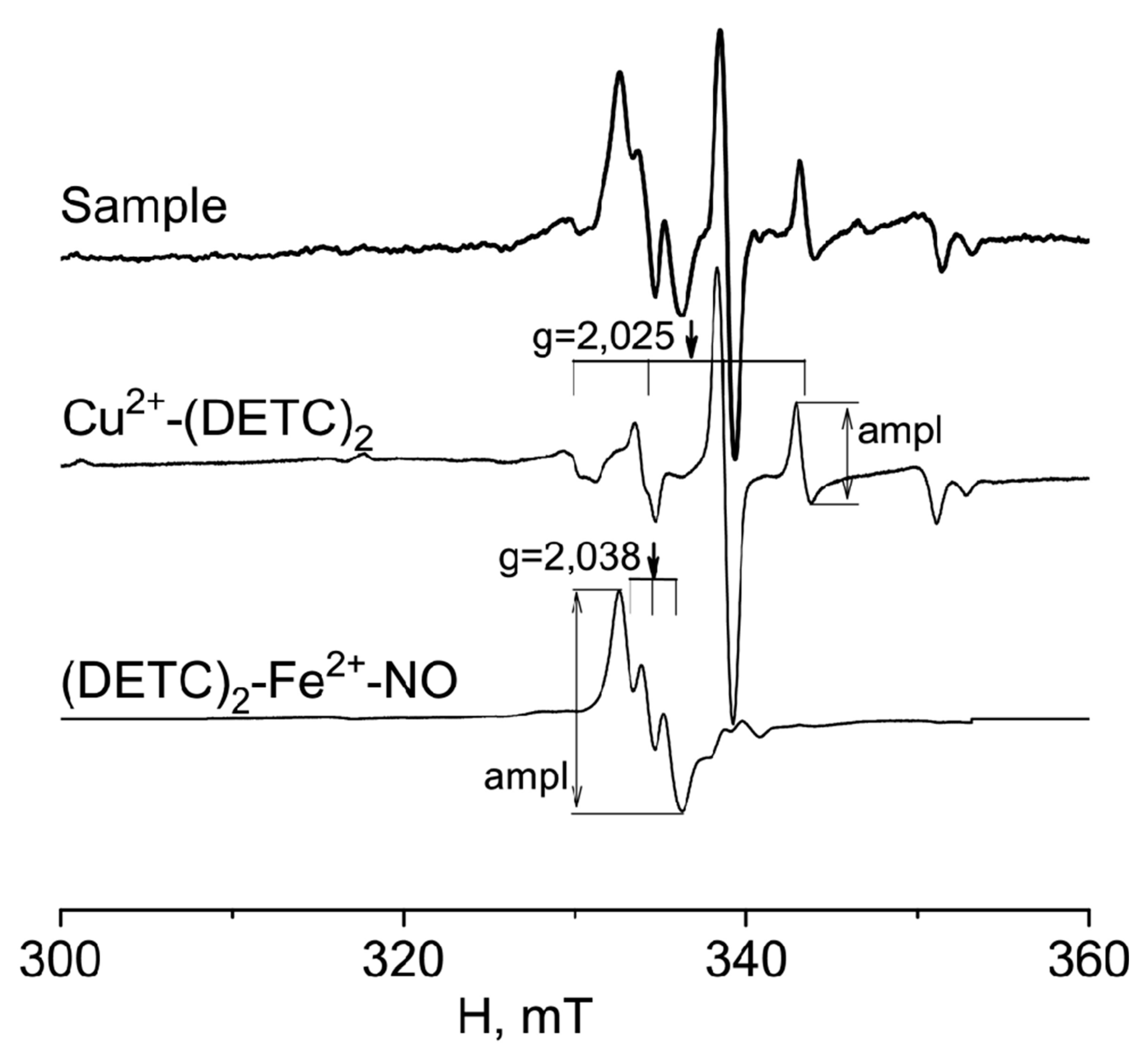
Figure 2.
EPR spectra of tissues from frontal lobe of the control-intact rat (Control rat) and two regions of frontal lobe of injured rat (Injured rat): injured area (injured area) and non-injured area (non-injured area) 7 days after modeling a combined injury of the brain and spinal cord. The spectrum displayed signals from: a) tissue sample, b) (DETC)2-Fe2+-NO complex, and c) Cu(DETC)2 complex. The calculated spectrum of the (DETC)2-Fe2+-NO complex was also depicted in the observed spectrum. The dotted line represented the NO contribution to the observed signal. The frame showed the signal area (DETC)2-Fe2+-NO complex. Temperature is 77o K. The rats were injected with (DETC)2-Fe2+ - citrate. gср=2.038.
Figure 2.
EPR spectra of tissues from frontal lobe of the control-intact rat (Control rat) and two regions of frontal lobe of injured rat (Injured rat): injured area (injured area) and non-injured area (non-injured area) 7 days after modeling a combined injury of the brain and spinal cord. The spectrum displayed signals from: a) tissue sample, b) (DETC)2-Fe2+-NO complex, and c) Cu(DETC)2 complex. The calculated spectrum of the (DETC)2-Fe2+-NO complex was also depicted in the observed spectrum. The dotted line represented the NO contribution to the observed signal. The frame showed the signal area (DETC)2-Fe2+-NO complex. Temperature is 77o K. The rats were injected with (DETC)2-Fe2+ - citrate. gср=2.038.
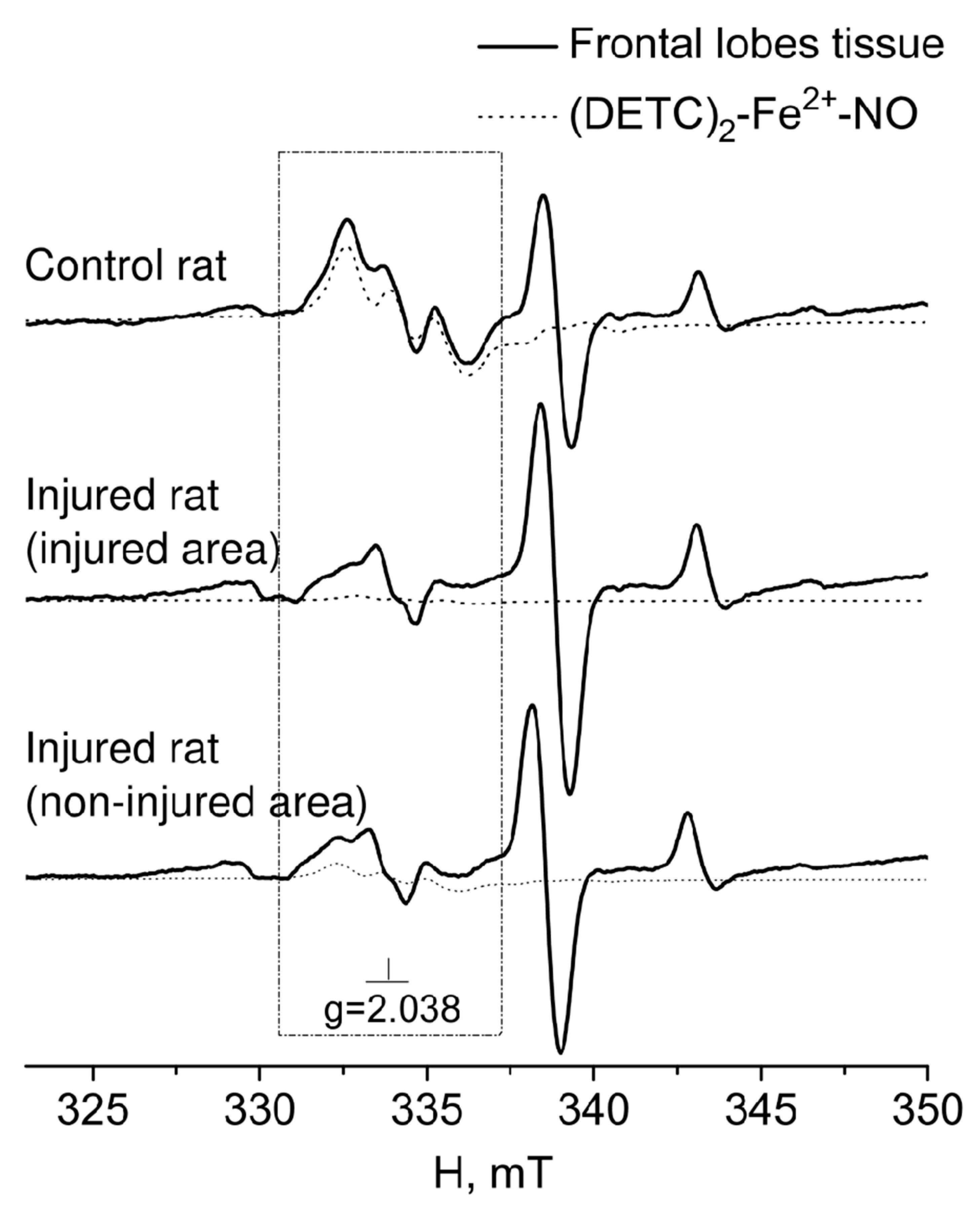
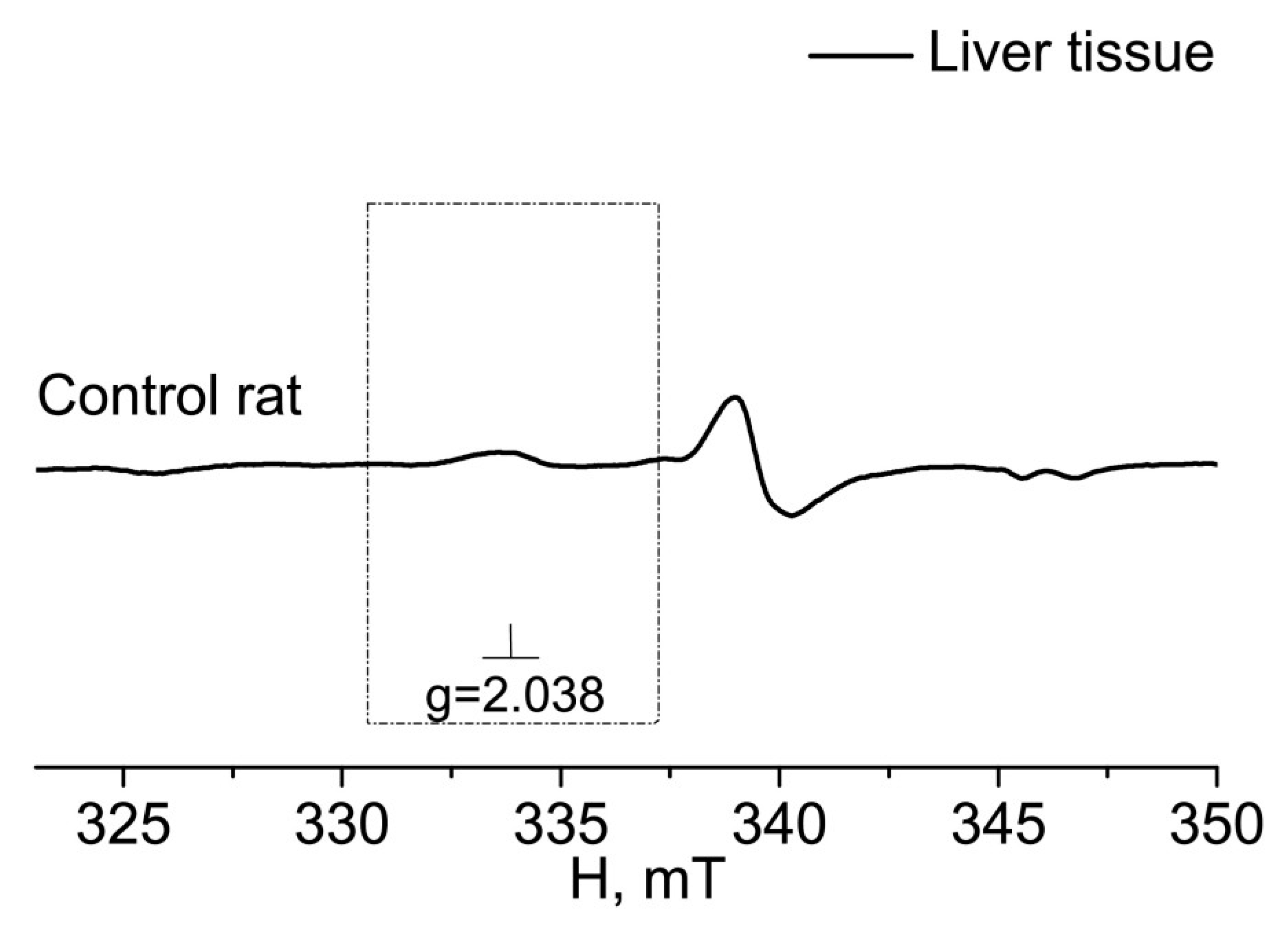
Figure 3.
EPR spectrum of liver of the control (Control rat). The dotted line represented the NO contribution to the observed signal. The frame showed the signal area (DETC)2-Fe2+-NO complex. Temperature is 77o K. The rats were injected with (DETC)2-Fe2+ - citrate. gср=2.038.
Figure 3.
EPR spectrum of liver of the control (Control rat). The dotted line represented the NO contribution to the observed signal. The frame showed the signal area (DETC)2-Fe2+-NO complex. Temperature is 77o K. The rats were injected with (DETC)2-Fe2+ - citrate. gср=2.038.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



