
Submitted:
22 September 2023
Posted:
25 September 2023
You are already at the latest version
Abstract
Taxanes, particularly docetaxel (DTX), has been widely used for combination therapy of head and neck squamous cell carcinoma (HNSCC). For locally advanced unresectable HNSCC, DTX combined with cisplatin and 5-fluorouracil as a revolutionary treatment revealed an advantage in improvement of patient outcome. In addition. DTX plus immune check inhibitors (ICIs) showed low toxicity and increased response of patients with recurrent or metastatic HNSCC (R/M HNSCC). Accumulating data indicate that taxanes not only function as antimitotics but also impair diverse oncogenic signalings including angiogenesis, inflammatory response, ROS production, and apoptosis induction. However, despite an initial response, development of resistance remains a major obstacle to treatment response. Taxane resistance could result from intrinsic mechanisms such as enhanced DNA/RNA damage repair, increased drug efflux, and apoptosis inhibition, and extrinsic effects such as angiogenesis and interactions between tumor cells and immune cells. This review provides an overview of taxanes therapy applied in different stages of HNSCC and describe the mechanisms of taxane resistance in HNSCC. Through a detailed understanding the mechanisms of resistance may help developing the potential therapeutic methods and the effective combination strategies to overcome drug resistance.
Keywords:
head and neck squamous cell carcinoma (HNSCC)
; taxanes
; docetaxel (DTX)
; resistance
1. Introduction
Head and neck squamous cell carcinoma (HNSCC) is the sixth most common type of cancer worldwide, with an annual incidence of more than 890,000 cases [1]. HNSCC develops in the outer layer of skin and in the mucosal epithelium of the mouth, nose, and throat, and impairs important physiological functions such as breathing, swallowing, and vocalization depending on its location. Common risk factors for HNSCC are associated with human papillomavirus infection and dietary habits such as betel nut chewing, cigarette heavy smoking, and excessive alcohol consumption [2]. Due to lack of appropriate screening biomarkers and unobvious or nonspecific symptoms in the early-stage HNSCC, patients are often diagnosed in an advanced state with a poor prognosis and a 5-year overall survival (OS) rate of < 50% [3,4,5]. The multidisciplinary treatments including surgery, targeted therapy, radiotherapy, chemotherapy, and immunotherapy have been considered for HNSCC patients according to the stage of disease, anatomical site, and surgical accessibility [5]. Among these therapeutic methods, chemotherapeutic drugs remain the major regimens for systemic treatment. Currently, combination of docetaxel (DTX) with cisplatin plus 5-fluorouracil (TPF) has been the most popular therapeutic strategy for HNSCC [6]. Clinical verification revealed that complete response to TPF treatment was significantly associated with longer progression-free survival (PFS) and OS in HNSCC patients [7,8].
Taxanes with core structure of taxadiene are a class of diterpenes originally identified from plants of the genus Taxus (yews). They represent one of the most interesting categories of antineoplastic drugs, paclitaxel (PTX) and the synthetic derivatives DTX and cabazitaxel (CTX) are FDA approved taxane and currently used in the treatment of various cancers [9]. Taxanes bind with β-tubulin with high affinity via π-π interactions [10] and are characterized to promote the polymerization of microtubules and cause the formation of stable, dysfunctional microtubules thereby preventing normal cellular processes and arrest cell cycle progression [11]. Accumulating data indicate that except antimitotic function, taxanes affect diverse oncogenic signaling pathways including apoptosis, angiogenesis, inflammatory response, and ROS production [9]. However, despite an initial response, resistance to taxanes treatment can develop either at the first treatment or after multiple treatments, which could be one of the major causes responsible for relapses and poor outcomes in HNSCC patients [12]. Hence, a detailed understanding the mechanisms of resistance development may help overcoming chemoresistance to prolonged treatment response.
In this review, we provide an overview of taxanes therapy applied in different stages of HNSCC, summarize the new treatment modalities in recent clinical trials. We describe the mechanisms of taxane resistance in HNSCC and highlight the potential strategies to overcome this resistance.
2. Taxane in HNSCC clinical application
2.1. Locally advanced HNSCC
Combination chemotherapy with radiotherapy (RT) for patients with locally advanced HNSCC includes concurrent chemoradiotherapy (CRT) and induction chemotherapy (ICT) followed by RT or CRT [13,14]. The most conventional ICT regimen is a combination of cisplatin and 5-fluorouracil (PF) [15]. In order to enhance the effectiveness of ICT, a revolutionary advancement in treatment over the past decades is the integration of docetaxel into the PF ICT regimen. Extensive evidence from two phase III trials confirms that this modified regimen, known as TPF ICT, significantly improves survival rates compared to standard PF ICT [16,17]. Nevertheless, the debate about whether TPF ICT combined with CRT offers superior survival outcomes compared to the standard CRT remain continued. While two phase III trials demonstrated that TPF ICT combined with CRT did not result in a statistically significant survival advantage over CRT alone [18,19], only one phase III trial of TPF ICT has shown an overall survival benefit compared to no-induction treatment [20]. Notably, a major concern in clinical practice is the occurrence of more severe adverse events, particularly grade 3/4 neutropenia and TPF-related deaths, which can potentially compromise the efficacy of treatment [21,22]. Therefore, the modification of TPF regimens has been developed to lower toxicity and enhance compliance for the older patients and Asian population [8,23]. TPF regimen is a highly selective treatment for locally advanced HNSCC. Patients who exhibit good partial response and complete response frequently acquire clinical benefit from this treatment [8,24]
2.2. Recurrent/metastatic HNSCC
For recurrent or metastatic HNSCC (R/M HNSCC), the systemic treatments such as immune check point inhibitor, chemotherapy, and targeted therapy against EGFR are used as the primary approach to improve long-term disease control; however, their efficacy remains limited [25]. Cetuximab, a monoclonal EGFR antibody, plus cisplatin and docetaxel have been clinically evaluated for the treatment of R/M HNSCC [26]. The result revealed that the progression free survival was around 6 months in the both arms and most of patients developed resistance to treatment in 12 months. Despite less toxicity, this combination therapy was unable to achieve longer survival comparing to conventional EXTREME regimen in R/M HNSCC. The advent of immune checkpoint inhibitors targeting programmed death 1 (PD-1) creates a revolutionized HNSCC treatment. Pembrolizumab plus cisplatin and fluorouracil have been demonstrated enduring response rates and improved overall survival compared to cetuximab plus platinum chemotherapy [27], although this treatment had merely a median progression-free survival of around 5 months. Additionally, a phase IV trial, keynote B10 study, demonstrated that pembrolizumab plus paclitaxel and carboplatin had less toxicity and better compliance [28]. In general, taxane backbone treatment plus immune checkpoint inhibitors or cetuximab are a better alternative in R/M HNSCC. In the TPExtreme study, a first line chemotherapy with a taxane (TPEx) followed by second line with immunotherapy yields a 21.9 month median survival (95% CI 15.9–35.0) [29]. Further study revealed an interesting finding that immunotherapy followed by chemotherapy increased 30% of objective response rate (ORR) to chemotherapy [30]. Immune checkpoint inhibitors plus taxane have been showed a synergic effect in the phase III KEYNOTE-407 study for squamous non-small-cell lung cancer [31]. A phase I/II study shown that combination of DTX with pembrolizumab showed promising activity (median OS 21.3 months, 95% CI 6.3–31.1 months) accompanied with a manageable side effect profile in platinum resistant R/M HNSCC [32]. Collectively, these studies demonstrate an important role of taxane in chemotherapy for R/M HNSCC.
3. Molecular Mechanisms of taxane
3.1. Interfering the function of microtubules
The functional mechanism of taxanes was primarily characterized to interfere with normal functioning of microtubules, which are essential structures involved in cell division and maintenance of cell shape [11]. Taxanes, such as paclitaxel and docetaxel, bind to beta subunit of tubulin, an essential part of microtubules. This binding stabilizes the microtubules by preventing their disassembly. During cell mitosis, microtubules help separate chromosomes into two daughter cells. Taxanes interfere with the normal formation and function of the mitotic spindle, leading to errors in chromosome segregation and ultimately preventing cell division. By disrupting microtubule dynamics, taxanes induce cell cycle arrest at the G2/M phase. This arrest prevents cells from progressing through the cell cycle and undergoing mitosis, effectively inhibiting cell proliferation and inducing cell death.
3.2. Induction of apoptosis
Taxanes also triggers signaling pathways of apoptosis. Taxanes can activate several pro-apoptotic signaling pathways within cancer cells. One key pathway is involved in the activation of the c-Jun N-terminal kinase (JNK) and p38 kinase. These kinases phosphorylate and activate c-Jun and ATF-2, which induce the pro-apoptotic signaling [33]. In addition, taxanes disrupt the function of anti-apoptotic proteins, such as Bcl-2 and Bcl-xL, which normally prevent apoptosis by inhibiting the release of cytochrome c from the mitochondria [34]. Taxanes modulate the expression or activity of these anti-apoptotic proteins, promoting the release of cytochrome c and activation of the caspase cascade. Additionally, taxanes induce the generation of reactive oxygen species (ROS). Taxanes interfere the mitochondrial function, leading to an imbalance in electron transport chain activity and an increase in electron leakage. The electron leakage can result in the formation of superoxide radicals (O2·-) within the mitochondria, which then undergo enzymatic dismutation to form hydrogen peroxide (H2O2), a type of ROS [35]. Taxanes also stimulate the activity of NADPH oxidase to generate ROS. NADPH oxidase can produce superoxide radicals by transferring electrons from NADPH to molecular oxygen [36,37]. The metabolism of taxanes can result in the formation of reactive metabolites that are involving in inducing oxidative stress and contribute to ROS production. Moreover, taxanes can disrupt calcium signaling within cells. The calcium imbalance is able to activate nitric oxide synthase and xanthine oxidase thereby producing ROS [38,39], the accumulation of ROS could finally cause intracellular apoptosis.
3.3. DNA damage and DNA repair inhibition
Taxanes have been shown to suppress a set of DNA repair-related genes, whose silence is associated with cancer cell death [40]. In addition, many of these genes are overexpressed in tumors exhibiting chromosomal instability (CIN), which is associated with both poor prognosis in solid tumors and the rapid acquisition of multidrug resistance in cell culture models [41]. In the OV01 clinical trial, a high level of CIN was associated with taxane resistance, indicating that CIN may determine taxanes response in vivo [40]. A retrospective cohort study showed that the combined use of paclitaxel could benefit survival of patient with homologous recombination (HR) deficient ovarian cancers [42]. On the other hand, paclitaxel can inhibit the overexpression of nucleotide excision repair (NER)-related genes induced by doxorubicin thereby improving efficacy of the dose-dense ACT protocol for breast cancer treatment [43]. These findings suggest the functional roles of taxanes in modulating DNA repair mechanisms, including nucleotide excision repair (NER) and homologous recombination (HR).
4. Taxane resistance in HNSCC
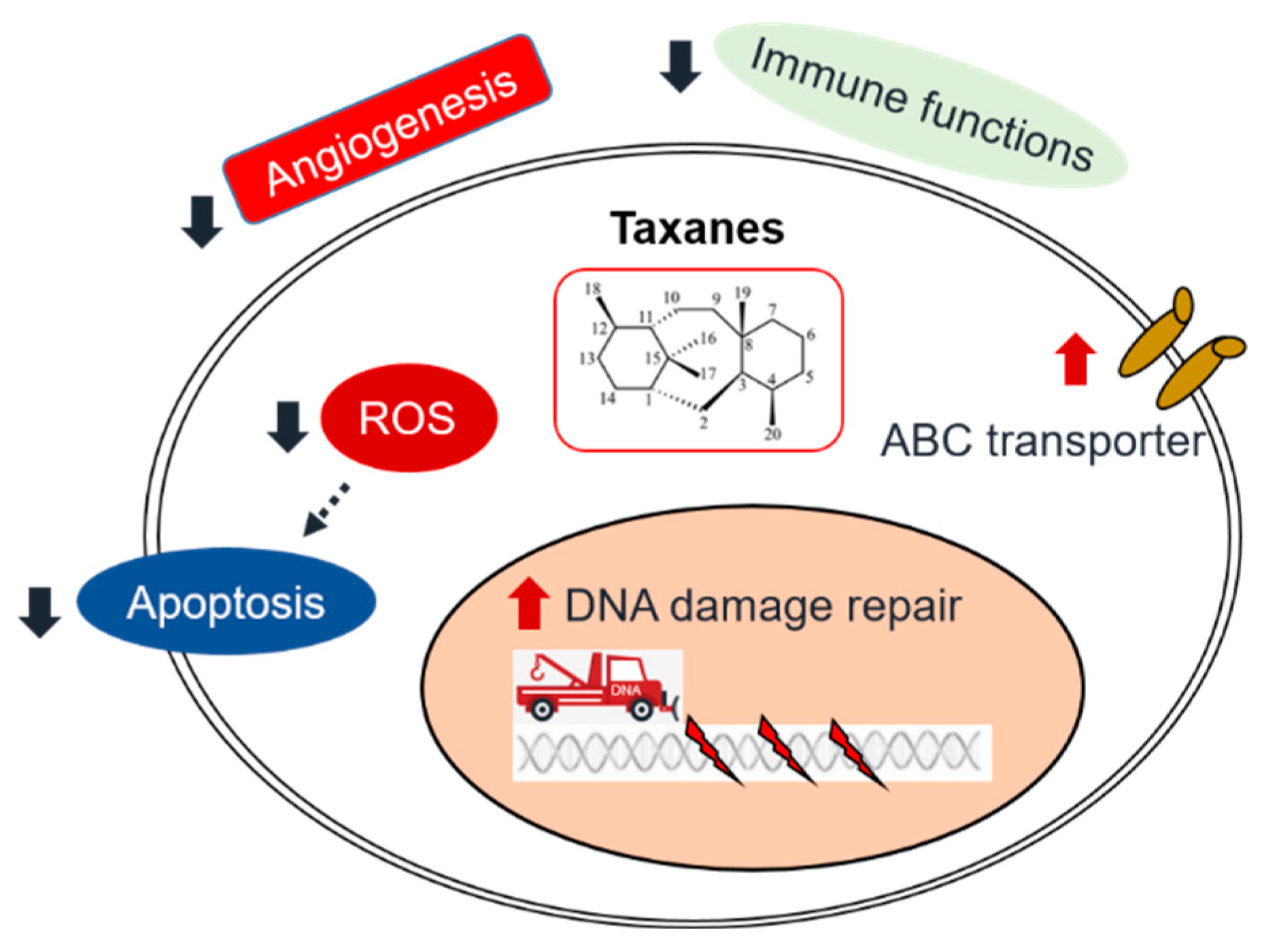
Chemotherapy is a cancer treatment modality that employs drugs to eliminate tumor cells. A typical chemotherapy protocol consists of administering several drugs in cycles of three weeks. However, there are compelling arguments supporting the use of dose-dense protocols in various cancers, including HNSCC. Pharmacodynamics and pharmacokinetics both play crucial roles in the development of taxane resistance (Figure 1). To understand the effect of drug treatment on the organism (pharmacodynamics), it is essential to consider both intrinsic characteristics and the extrinsic tumor microenvironments. There are four primary intrinsic mechanisms associated with taxane resistance: DNA/RNA damage repair, drug efflux, apoptosis inhibition, and abnormal expression of tyrosine kinase pathways. The extrinsic tumor microenvironments involve angiogenesis and interactions between immune cells and tumor cells.
4.1. Intrinsic mechanisms
4.1.1. DNA/RNA damage repair
DNA damage and aberrant repair is important in the tumorigenesis, treatment response, and prognosis of HNSCC. A retrospective study of 170 patients with HNSCC reported that among DNA damage response (DDR genes), 17.6% of patients have BRCA2 and ARID1A mutations, 13.5% have ATM mutation, followed by 10% of patients have BRCA1 mutation [44]. Another study, which employed whole-exome sequencing for 45 patients with oral and oropharyngeal cancer, revealed that FANCG, CDKN2A, and TPP germline variants were strongly associated with HNSCC risk. Furthermore, the study found that 67% of patients had at least one germline variation in DNA repair pathway genes [45]. Abnormal expression of DDR-related genes is associated with the treatment response of HNSCC. A study involving 453 HNSCC patients found that the dysregulated expression of ERCC1 and XPA was associated with inferior overall survival and chemotherapy resistance in patients with squamous cell carcinoma of oral cavity [46]. High expression of DNA repair-related genes (MRE11A, Rad50, RAD51, and XRCC2) in HNSCC patients also contributes to tumor progression and induces drug-resistant phenotypes [47]. In our laboratory, we have found that the combination of arsenic trioxide (ATO) and EGFR inhibitors exhibits a synergistic inhibitory effect on HNSCC. This combination impairs the DNA damage repair response by suppressing the BRCA1-PLK1 signaling pathway. Our single-case experience with a heavily treated HNSCC patient who had TP53 and BRCA2 mutations showed an unusual and prolonged response to ATO and osimertinib, suggesting the potential to target the DNA damage repair pathway in HNSCC patients [48].
Several novel therapeutic approaches targeting the DDR pathway in HNSCC have been developed. PARPs are a group of enzymes that use beta-nicotinamide adenine dinucleotide (β-NAD+) to covalently add poly(ADP-ribose) (PAR) chains to target proteins, a process known as PARylation [49]. PARP plays an important role in DNA damage repair and the maintenance of genome integrity. It binds to nuclear DNA single-strand breaks (SSBs) and recruits various DNA repair proteins, such as XRCC1, to facilitate DNA damage repair [50]. PARP inhibitors have been reported to provide significant clinical benefits in various solid tumors, including HNSCC [51,52]. Several clinical trials combining PARP inhibitors with taxanes are in progress [53,54,55].
In addition to PARP inhibitors, Wee1 is a serine/threonine kinase that regulates DNA damage-induced G2/M phase arrest by phosphorylating cyclin-dependent protein kinase 1 (CDK1) [56]. Suppression of Wee1 kinase activity negatively regulates the G2/M checkpoint and induces DNA damage, ultimately leading to cell death through mitotic catastrophe [57]. A study reported that the combination of the Wee1 inhibitor adavosertib with cisplatin can synergistically inhibit the proliferation and survival of cisplatin-resistant HNSCC cells by inducing DNA damage [58]. The results of a Phase I clinical trial showed that the triplet combination of adavosertib, cisplatin, and docetaxel was safe and well-tolerated, demonstrating the promising anti-tumor efficacy in patients with advanced HNSCC [55].
4.1.2. Drug efflux
Multidrug resistance 1 (MDR1)/P-glycoprotein (P-gp), a plasma membrane glycoprotein encoded by the MDR1 gene, is a member of the adenosine triphosphate-binding cassette (ABC) transporter family. Substantial evidence exists regarding the role of P-gp in mediating taxane resistance in vitro [59,60,61]. Therefore, inhibition of P-gp activity has been explored as a potential approach. For instance, pentagalloyl glucose was investigated for its inhibitory effects on P-gp and its impact on cancer stem-like cells in HNSCC [62]. Additionally, cabazitaxel is a derivative of docetaxel, which is cytotoxic to docetaxel-resistant cell lines due to P-gp overexpression. cabazitaxel has been shown to improve the survival of prostate cancer patients who experienced relapse after docetaxel treatment [63]. A phase II clinical trial was conducted to evaluate the efficacy of cabazitaxel compared to docetaxel in recurrent head and neck cancer patients. Unfortunately, cabazitaxel did not show superior disease control compared to docetaxel [64]. Further investigation is needed to determine whether cabazitaxel can provide benefits to patients who have progressed after docetaxel treatment. While most of the literature has primarily concentrated on MDR1, the absence of ABCC10, another ATP-dependent drug efflux pump, has been linked to heightened sensitivity to DTX and PTX in both in vivo and in vitro settings [65]. This implies that other ATP-dependent pumps might play compensatory roles in taxane efflux and should be taken into account in the quest for targeted therapies.
4.1.3. Apoptosis inhibition
Apoptosis inhibition has been observed in taxane-resistant HNSCC. Liu et al. indicated that HNSCC cells can upregulate survivin expression by activating the NF-κB pathway. Survivin inhibits active caspase-9, thereby preventing apoptosis induced by aberrant mitosis resulting from mitotic damage caused by paclitaxel [66]. Other inhibitors of apoptosis proteins (IAP), including XIAP (X-linked inhibitor of apoptosis), cIAP1/2 (cellular inhibitor of apoptosis 1 and 2), and SMAC (second mitochondria-derived activator of caspases), have also been found to play crucial roles as survival factors in HNSCC [67]. Currently, clinical trials are underway to investigate the use of IAP antagonists for targeting HNSCC. An exploratory trial is designed to study HNSCC patients who received xevinapant, cisplatin chemotherapy, or both treatments before surgery [68]. After xevinapant treatment, tumors exhibited higher infiltration by CD8+ T cells and NF-κB/IAP pathway mediators [68]. Further investigation is needed to explore the combined effects of taxanes and apoptosis inhibitors.
4.2. Extrinsic mechanisms
4.2.1. Angiogenesis
The proliferation of HNSCC cells results in the formation of abnormal blood vessels and lymphatic vessels, leading to the leakage and accumulation of fluid in the interstitium. This elevated tumor interstitial pressure (TIP) physically hinders the infiltration of immune cells and chemotherapy [69]. Angiogenesis is a hallmark of tumor progression, and targeting it has proven to be a successful approach in treating certain solid tumors. Bevacizumab, in combination with chemotherapy, has received approval from the US FDA for the treatment of several malignancies [70]. Because preclinical data showed promising results for bevacizumab in the treatment of HNSCC [71,72], numerous clinical trials investigated bevacizumab in combination with chemotherapy [73,74,75]. Although these studies showed promising response rates, concerns about toxicities such as perforation and hemorrhage persisted. A large Phase III trial was conducted to assess the addition of bevacizumab to chemotherapy regimens. This trial revealed a significant improvement in progression-free survival and the overall response rate. However, it did not demonstrate a statistically significant survival advantage. Notably, the addition of bevacizumab was associated with a higher incidence of grade 3–5 bleeding events (6.7% vs. 0.5%; p<0.001) and treatment-related deaths (9.3% vs. 3.5%; p=0.022) [73]. Regarding tyrosine kinase inhibitors of angiogenesis, compounds such as sorafenib, sunitinib, semaxanib, levantinib, and vandetanib have been studied to enhance the response rate to chemotherapy [76,77,78]. However, the combination of tyrosine kinase inhibitors with chemotherapy, including docetaxel and paclitaxel, showed only limited clinical significance.
4.2.2. The interaction of immune therapy and chemotherapy
HNSCC is characterized with a combination of immune escape mechanisms that suppress immune attacks. Among the immune pathways involved in this interaction, the most well-known pathway is the programmed cell death protein 1 (PD-1)/programmed cell death ligand-1 (PD-L1) axis. PD-1 is a member of the CD28/cytotoxic T-lymphocyte antigen 4 (CTLA-4) family of T cell regulators and is expressed on both immune and cancer cells. Physiologically, PD-1 promotes self-tolerance by preventing the immune system from killing cancer cells and suppressing T cell inflammatory activity [79]. Targeting T cells with PD-1/PD-L1 inhibitors in combination with chemotherapeutic drugs has been the standard of care in metastatic/recurrent HNSCC. It is still unclear whether the combination effects of PD-1/PD-L1 inhibitors and chemotherapies are synergistic or additive. Several retrospective studies have shown that exposure to immune checkpoint inhibitors improves the response to salvage chemotherapy in HNSCC, suggesting that immune checkpoint inhibitors may increase tumor sensitivity to chemotherapy [30,80].
In addition to T cells, other immune cells also play important roles in tumorigenesis and drug resistance in HNSCC. In our laboratory, we have found that tumor-associated macrophages are associated with chemotherapeutic resistance [36]. Macrophages can secrete IL-1beta to promote docetaxel resistance in HNSCC by upregulating the expression of intercellular adhesion molecule 1 (ICAM1) in tumor cells, which promotes stemness and the formation of polypoid giant cancer cells. Preclinical data have shown that ATO can reduce macrophage infiltration into the tumor microenvironment and impair IL-1β secretion by macrophages. The combinatorial use of arsenic trioxide enhances the in vivo efficacy of docetaxel in a mouse model [36]. Although targeting IL-1β or ICAM1 is a promising concept, there are no clinical trials that have assessed targeting IL-1β or ICAM1 for HNSCC treatment and more research in this area is warranted.
4.2.3. Optimizing the pharmacokinetics of chemotherapy
Dose-dense chemotherapy increases the dose intensity of the regimen by delivering standard-dose chemotherapy with shorter intervals to avoid regrowth of cancer cells. Dose-dense chemotherapy can help overcome chemotherapy resistance in some cases. By delivering chemotherapy more frequently and at higher doses, it may prevent cancer cells from developing resistance mechanisms and reduce the chances of tumor growth. This approach is particularly relevant in the treatment of certain aggressive cancers, such as breast cancer, bladder cancer, and lymphoma [81,82]. However, the associated studies in HNSCC are scarce. Our team conducted a phase II clinical trial using biweekly TPF rather than the conventional triweekly TPF regimen. The data showed that this biweekly TPF induction chemotherapy regimen had an overall response rate of 89.7% and a complete response rate of 31%. Notably, the grade 3-4 neutropenia rate is lower than that of the conventional triweekly TPF regimen [8]. A retrospective study by J. Fayette et al. in France reported a similar biweekly regimen for metastatic head and neck HNSCC and also confirmed a high response rate with tolerable toxicity [83]. A randomized phase II prospective study conducted in India showed that the biweekly regimen had better response rates with fewer toxicities compared to conventional triweekly regimens [84]. In summary, dose-dense regimens are a promising approach in HNSCC patients. Further investigation is warranted to determine the appropriateness of this concept in combination with targeted therapies or immune therapies.
5. Conclusion
Currently, taxanes, comprising PTX and its synthetic derivatives, have been broadly used for chemotherapy in diverse cancers, including HNSCC. In addition to stabilize β-tubulin polymerization to suppress microtubule dynamics and impairs mitosis, the functions of taxanes were characterized to be involved in many oncogenic signaling pathways such as angiogenesis, inflammatory response, ROS production, and apoptosis induction. However, the intrinsic and acquired resistance remains a major obstacle to prolonged treatment response. Through a detailed understanding the mechanisms of resistance may lead to emerge the development of dual targeting compounds and the effective combination strategies for surmounting drug resistance.
Funding
This study was funded by the National Science and Technology Council (NSTC, Grant No. 111-2314-B-039-033-MY3 and 112-2314-B-039-026-MY3) and China Medical University Hospital (Grant No. DMR-110-018), Taiwan.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat Rev Dis Primers. 2020, 6, 92. [Google Scholar] [CrossRef]
- Leemans, C.R.; Snijders, P.J.F.; Brakenhoff, R.H. The molecular landscape of head and neck cancer. Nat Rev Cancer. 2018, 18, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Economopoulou, P.; de Bree, R.; Kotsantis, I.; Psyrri, A. Diagnostic Tumor Markers in Head and Neck Squamous Cell Carcinoma (HNSCC) in the Clinical Setting. Front Oncol. 2019, 9, 827. [Google Scholar] [CrossRef] [PubMed]
- Chow, L.Q.M. Head and Neck Cancer. N Engl J Med. 2020, 382, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Gau, M.; Karabajakian, A.; Reverdy, T.; Neidhardt, E.M.; Fayette, J. Induction chemotherapy in head and neck cancers: Results and controversies. Oral Oncol. 2019, 95, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Wichmann, G.; Krüger, A.; Boehm, A.; Kolb, M.; Hofer, M.; Fischer, M.; Müller, S.; Purz, S.; Stumpp, P.; Sabri, O.; et al. Induction chemotherapy followed by radiotherapy for larynx preservation in advanced laryngeal and hypopharyngeal cancer: Outcome prediction after one cycle induction chemotherapy by a score based on clinical evaluation, computed tomography-based volumetry and 18F-FDG-PET/CT. Eur J Cancer. 2017, 72, 144–155. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Lein, M.Y.; Yang, S.N.; Wang, Y.C.; Lin, Y.J.; Lin, C.Y.; Hua, C.H.; Tsai, M.H.; Lin, C.C. Dose-dense TPF induction chemotherapy for locally advanced head and neck cancer: a phase II study. BMC Cancer. 2020, 20, 832. [Google Scholar] [CrossRef]
- Mosca, L.; Ilari, A.; Fazi, F.; Assaraf, Y.G.; Colotti, G. Taxanes in cancer treatment: Activity, chemoresistance and its overcoming. Drug Resist Updat. 2021, 54, 100742. [Google Scholar] [CrossRef]
- Churchill, C.D.; Klobukowski, M.; Tuszynski, J.A. Elucidating the mechanism of action of the clinically approved taxanes: a comprehensive comparison of local and allosteric effects. Chem Biol Drug Des. 2015, 86, 1253–1266. [Google Scholar] [CrossRef]
- Schiff, P.B.; Fant, J.; Horwitz, S.B. Promotion of microtubule assembly in vitro by taxol. Nature. 1979, 277, 665–667. [Google Scholar] [CrossRef] [PubMed]
- Ramos, A.; Sadeghi, S.; Tabatabaeian, H. Battling Chemoresistance in Cancer: Root Causes and Strategies to Uproot Them. Int J Mol Sci. 2021, 22, 9451. [Google Scholar] [CrossRef] [PubMed]
- Grégoire, V.; Lefebvre, J.L.; Licitra, L.; Felip, E. ; EHNS-ESMO-ESTRO Guidelines Working Group. Squamous cell carcinoma of the head and neck: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010, 21 Suppl 5, v184–v186. [Google Scholar] [CrossRef]
- Marur, S.; Forastiere, A.A. Head and Neck Squamous Cell Carcinoma: Update on Epidemiology, Diagnosis, and Treatment. Mayo Clin Proc. 2016, 91, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Pignon, J.P.; le Maître, A.; Maillard, E.; Bourhis, J.; MACH-NC Collaborative Group. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): an update on 93 randomised trials and 17,346 patients. Radiother Oncol. 2009, 92, 4–14. [Google Scholar] [CrossRef]
- Vermorken, J.B.; Remenar, E.; van Herpen, C.; Gorlia, T.; Mesia, R.; Degardin, M.; Stewart, J.S.; Jelic, S.; Betka, J.; Preiss, J.H.; et al. Cisplatin, fluorouracil, and docetaxel in unresectable head and neck cancer. N Engl J Med. 2007, 357, 1695–1704. [Google Scholar] [CrossRef]
- Posner, M.R.; Hershock, D.M.; Blajman, C.R.; Mickiewicz, E.; Winquist, E.; Gorbounova, V.; Tjulandin, S.; Shin, D.M.; Cullen, K.; Ervin, T.J.; et al. Cisplatin and fluorouracil alone or with docetaxel in head and neck cancer. N Engl J Med. 2007, 357, 1705–1715. [Google Scholar] [CrossRef]
- Hitt, R.; Grau, J.J.; López-Pousa, A.; Berrocal, A.; García-Girón, C.; Irigoyen, A.; Sastre, J.; Martínez-Trufero, J.; Brandariz Castelo, J.A.; Verger, E.; et al. A randomized phase III trial comparing induction chemotherapy followed by chemoradiotherapy versus chemoradiotherapy alone as treatment of unresectable head and neck cancer. Ann Oncol. 2014, 25, 216–225. [Google Scholar] [CrossRef]
- Cohen, E.E.; Karrison, T.G.; Kocherginsky, M.; Mueller, J.; Egan, R.; Huang, C.H.; Brockstein, B.E.; Agulnik, M.B.; Mittal, B.B.; Yunus, F.; et al. Phase III randomized trial of induction chemotherapy in patients with N2 or N3 locally advanced head and neck cancer. J Clin Oncol. 2014, 32, 2735–2743. [Google Scholar] [CrossRef]
- Ghi, M.G.; Paccagnella, A.; Ferrari, D.; Foa, P.; Alterio, D.; Codecà, C.; Nolè, F.; Verri, E.; Orecchia, R.; Morelli, F.; et al. Induction TPF followed by concomitant treatment versus concomitant treatment alone in locally advanced head and neck cancer. A phase II-III trial. Ann Oncol. 2017, 28, 2206–2212. [Google Scholar] [CrossRef]
- Haddad, R.I.; Posner, M.; Hitt, R.; Cohen, E.E.W.; Schulten, J.; Lefebvre, J.L.; Vermorken, J.B. Induction chemotherapy in locally advanced squamous cell carcinoma of the head and neck: role, controversy, and future directions. Ann Oncol. 2018, 29, 1130–1140. [Google Scholar] [CrossRef] [PubMed]
- Yano, R.; Konno, A.; Watanabe, K.; Tsukamoto, H.; Kayano, Y.; Ohnaka, H.; Goto, N.; Nakamura, T.; Masada, M. Pharmacoethnicity of docetaxel-induced severe neutropenia: integrated analysis of published phase II and III trials. Int J Clin Oncol. 2013, 18, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Okano, S.; Enokida, T.; Onoe, T.; Ota, Y.; Motegi, A.; Zenda, S.; Akimoto, T.; Tahara, M. Induction TPF chemotherapy followed by CRT with fractionated administration of cisplatin in patients with unresectable locally advanced head and neck cancer. Int J Clin Oncol. 2019, 24, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Q.; Fang, J.; Huang, Z.; Yang, Y.; Lian, M.; Liu, H.; Zhang, Y.; Ye, J.; Hui, X.; Wang, Y.; et al. A response prediction model for taxane, cisplatin, and 5-fluorouracil chemotherapy in hypopharyngeal carcinoma. Sci Rep. 2018, 8, 12675. [Google Scholar] [CrossRef] [PubMed]
- Lau, A.; Yang, W.F.; Li, K.Y.; Su, Y.X. Systemic Therapy in Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma- A Systematic Review and Meta-Analysis. Crit Rev Oncol Hematol. 2020, 153, 102984. [Google Scholar] [CrossRef]
- Guigay, J.; Aupérin, A.; Fayette, J.; Saada-Bouzid, E.; Lafond, C.; Taberna, M.; Geoffrois, L.; Martin, L.; Capitain, O.; Cupissol, D.; et al. Cetuximab, docetaxel, and cisplatin versus platinum, fluorouracil, and cetuximab as first-line treatment in patients with recurrent or metastatic head and neck squamous-cell carcinoma (GORTEC 2014-01 TPExtreme): a multicentre, open-label, randomised, phase 2 trial. Lancet Oncol. 2021, 22, 463–475. [Google Scholar] [CrossRef]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G Jr.; Psyrri, A.; Basté, N.; Neupane, P.; Bratland, Å.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): a randomised, open-label, phase 3 study. Lancet. 2019, 394, 1915–1928. [CrossRef]
- Dzienis, M.R.; Cundom, J.E.; Fuentes, C.S.; Hansen, A.R.; Nordlinger, M.J.; Pastor, A.V.; Oppelt, P.; Neki, A.; Gregg, R.W.; Lima, I.P.F.; et al. Pembrolizumab (pembro)+carboplatin (carbo)+paclitaxel (pacli) as first-line (1L) therapy in recurrent/metastatic (R/M) head and neck squamous cell carcinoma (HNSCC): Phase VI KEYNOTE-B10 study. Ann Oncol. 2022, 33 suppl 7, S295–S322. [Google Scholar] [CrossRef]
- Guigay, J.; Fayette, J.; Mesia, R.; Saada-Bouzid, E.; Lafond, C.; Geoffrois, L.; Martin, L.; Capitain, O.; Cupissol, D.; Castanie, H.; et al. TPExtreme randomized trial: Quality of Life (QoL) and survival according to second-line treatments in patients with recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC). J. Clin. Oncol. 2020, 38 Suppl 15, 6507. [Google Scholar] [CrossRef]
- Saleh, K.; Daste, A.; Martin, N.; Pons-Tostivint, E.; Auperin, A.; Herrera-Gomez, R.G.; Baste-Rotllan, N.; Bidault, F.; Guigay, J.; Le Tourneau, C.; et al. Response to salvage chemotherapy after progression on immune checkpoint inhibitors in patients with recurrent and/or metastatic squamous cell carcinoma of the head and neck. Eur J Cancer. 2019, 121, 123–129. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Çay Şenler, F.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non-Small-Cell Lung Cancer. N Engl J Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Fuereder, T.; Minichsdorfer, C.; Mittlboeck, M.; Wagner, C.; Heller, G.; Putz, E.M.; Oberndorfer, F.; Müllauer, L.; Aretin, M.B.; Czerny, C.; et al. Pembrolizumab plus docetaxel for the treatment of recurrent/metastatic head and neck cancer: A prospective phase I/II study. Oral Oncol. 2022, 124, 105634. [Google Scholar] [CrossRef] [PubMed]
- Bacus, S.S.; Gudkov, A.V.; Lowe, M.; Lyass, L.; Yung, Y.; Komarov, A.P.; Keyomarsi, K.; Yarden, Y.; Seger, R. Taxol-induced apoptosis depends on MAP kinase pathways (ERK and p38) and is independent of p53. Oncogene. 2001, 20, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Gurbi, B.; Brauswetter, D.; Varga, A.; Gyulavári, P.; Pénzes, K.; Murányi, J.; Zámbó, V.; Birtalan, E.; Krenács, T.; Becker, D.L.; et al. The Potential Impact of Connexin 43 Expression on Bcl-2 Protein Level and Taxane Sensitivity in Head and Neck Cancers-In Vitro Studies. Cancers. 2019, 11, 1848. [Google Scholar] [CrossRef] [PubMed]
- Selimovic, D.; Hassan, M.; Haikel, Y.; Hengge, U.R. Taxol-induced mitochondrial stress in melanoma cells is mediated by activation of c-Jun N-terminal kinase (JNK) and p38 pathways via uncoupling protein 2. Cell Signal. 2008, 20, 311–322. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Lin, C.C.; Huang, Y.W.; Chen, J.H.; Tsou, Y.A.; Chang, L.C.; Fan, C.C.; Lin, C.Y.; Chang, W.C. Macrophage secretory IL-1β promotes docetaxel resistance in head and neck squamous carcinoma via SOD2/CAT-ICAM1 signaling. JCI Insight. 2022, 7, e157285. [Google Scholar] [CrossRef]
- Hung, C.H.; Chan, S.H.; Chu, P.M.; Tsai, K.L. Docetaxel Facilitates Endothelial Dysfunction through Oxidative Stress via Modulation of Protein Kinase C Beta: The Protective Effects of Sotrastaurin. Toxicol Sci. 2015, 145, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Pan, Z.; Gollahon, L. Taxol directly induces endoplasmic reticulum-associated calcium changes that promote apoptosis in breast cancer cells. Breast J. 2011, 17, 56–70. [Google Scholar] [CrossRef]
- Pan, Z.; Avila, A.; Gollahon, L. Paclitaxel induces apoptosis in breast cancer cells through different calcium--regulating mechanisms depending on external calcium conditions. Int J Mol Sci. 2014, 15, 2672–2694. [Google Scholar] [CrossRef]
- Swanton, C.; Nicke, B.; Schuett, M.; Eklund, A.C.; Ng, C.; Li, Q.; Hardcastle, T.; Lee, A.; Roy, R.; East, P.; et al. Chromosomal instability determines taxane response. Proc Natl Acad Sci U S A. 2009, 106, 8671–8676. [Google Scholar] [CrossRef] [PubMed]
- Carter, S.L.; Eklund, A.C.; Kohane, I.S.; Harris, L.N.; Szallasi, Z. A signature of chromosomal instability inferred from gene expression profiles predicts clinical outcome in multiple human cancers. Nat Genet. 2006, 38, 1043–1048. [Google Scholar] [CrossRef] [PubMed]
- Jean, S.; Li, J.; Katsaros, D.; Wubbenhorst, B.; Maxwell, K.N.; Fishbein, L.; McLane, M.W.; Benedetto, C.; Canuto, E.M.; Mitra, N.; et al. Paclitaxel is necessary for improved survival in epithelial ovarian cancers with homologous recombination gene mutations. Oncotarget. 2016, 7, 48577–48585. [Google Scholar] [CrossRef] [PubMed]
- Busatto, F.F.; Viero, V.P.; Schaefer, B.T.; Saffi, J. Cell growth analysis and nucleotide excision repair modulation in breast cancer cells submitted to a protocol using doxorubicin and paclitaxel. Life Sci. 2021, 268, 118990. [Google Scholar] [CrossRef] [PubMed]
- Burcher, K.M.; Faucheux, A.T.; Lantz, J.W.; Wilson, H.L.; Abreu, A.; Salafian, K.; Patel, M.J.; Song, A.H.; Petro, R.M.; Lycan, T. Jr.; et al. Prevalence of DNA Repair Gene Mutations in Blood and Tumor Tissue and Impact on Prognosis and Treatment in HNSCC. Cancers (Basel). 2021, 13, 3118. [Google Scholar] [CrossRef]
- Cury, S.S.; Miranda, P.M.; Marchi, F.A.; Canto, L.M.D.; Chulam, T.C.; Petersen, A.H.; Aagaard, M.M.; Pinto, C.A.L.; Kowalski, L.P.; Rogatto, S.R. Germline variants in DNA repair genes are associated with young-onset head and neck cancer. Oral Oncol. 2021, 122, 105545. [Google Scholar] [CrossRef] [PubMed]
- Prochnow, S.; Wilczak, W.; Bosch, V.; Clauditz, T.S.; Muenscher, A. ERCC1, XPF and XPA-locoregional differences and prognostic value of DNA repair protein expression in patients with head and neck squamous cell carcinoma. Clin Oral Investig. 2019, 23, 3319–3329. [Google Scholar] [CrossRef]
- Psyrri, A.; Gkotzamanidou, M.; Papaxoinis, G.; Krikoni, L.; Economopoulou, P.; Kotsantis, I.; Anastasiou, M.; Souliotis, V.L. The DNA damage response network in the treatment of head and neck squamous cell carcinoma. ESMO Open. 2021, 6, 100075. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Chang, W.C.; Lin, C.C.; Chen, J.H.; Lin, C.Y.; Liu, C.H.; Lin, C.; Hung, M.C. Combination treatment of arsenic trioxide and osimertinib in recurrent and metastatic head and neck squamous cell carcinoma. Am J Cancer Res. 2022, 12, 5049–5061. [Google Scholar]
- De Vos, M.; Schreiber, V.; Dantzer, F. The diverse roles and clinical relevance of PARPs in DNA damage repair: current state of the art. Biochem Pharmacol. 2012, 84, 137–146. [Google Scholar] [CrossRef]
- Pascal, J.M. The comings and goings of PARP-1 in response to DNA damage. DNA Repair. 2018, 71, 177–182. [Google Scholar] [CrossRef]
- Moutafi, M.; Economopoulou, P.; Rimm, D.; Psyrri, A. PARP inhibitors in head and neck cancer: Molecular mechanisms, preclinical and clinical data. Oral Oncol. 2021, 117, 105292. [Google Scholar] [CrossRef] [PubMed]
- Glorieux, M.; Dok, R.; Nuyts, S. Novel DNA targeted therapies for head and neck cancers: clinical potential and biomarkers. Oncotarget. 2017, 8, 81662–81678. [Google Scholar] [CrossRef] [PubMed]
- de Haan, R.; van Werkhoven, E.; van den Heuvel, M.M.; Peulen, H.M.U.; Sonke, G.S.; Elkhuizen, P.; van den Brekel, M.W.M.; Tesselaar, M.E.T.; Vens, C.; Schellens, J.H.M.; et al. Study protocols of three parallel phase 1 trials combining radical radiotherapy with the PARP inhibitor olaparib. BMC Cancer. 2019, 19, 901. [Google Scholar] [CrossRef]
- Jelinek, M.J.; Foster, N.R.; Zoroufy, A.J.; Schwartz, G.K.; Munster, P.N.; Seiwert, T.Y.; de Souza, J.A.; Vokes, E.E. A phase I trial adding poly(ADP-ribose) polymerase inhibitor veliparib to induction carboplatin-paclitaxel in patients with head and neck squamous cell carcinoma: Alliance A091101. Oral Oncol. 2021, 114, 105171. [Google Scholar] [CrossRef]
- Méndez, E.; Rodriguez, C.P.; Kao, M.C.; Raju, S.; Diab, A.; Harbison, R.A.; Konnick, E.Q.; Mugundu, G.M.; Santana-Davila, R.; Martins, R.; et al. A Phase I Clinical Trial of AZD1775 in Combination with Neoadjuvant Weekly Docetaxel and Cisplatin before Definitive Therapy in Head and Neck Squamous Cell Carcinoma. Clin Cancer Res. 2018, 24, 2740–2748. [Google Scholar] [CrossRef] [PubMed]
- Portugal, J.; Mansilla, S.; Bataller, M. Mechanisms of drug-induced mitotic catastrophe in cancer cells. Curr Pharm Des. 2010, 16, 69–78. [Google Scholar] [CrossRef]
- Kao, M.; Green, C.; Sidorova, J.; Méndez, E. Strategies for Targeted Therapy in Head and Neck Squamous Cell Carcinoma Using WEE1 Inhibitor AZD1775. JAMA Otolaryngol Head Neck Surg. 2017, 143, 631–633. [Google Scholar] [CrossRef]
- Yang, Z.; Liao, J.; Lapidus, R.G.; Fan, X.; Mehra, R.; Cullen, K.J.; Dan, H. Targeting Wee1 kinase to suppress proliferation and survival of cisplatin-resistant head and neck squamous cell carcinoma. Cancer Chemother Pharmacol. 2022, 89, 469–478. [Google Scholar] [CrossRef]
- Li, D.W.; Gao, S.; Shen, B.; Dong, P. Effect of apoptotic and proliferative indices, P-glycoprotein and survivin expression on prognosis in laryngeal squamous cell carcinoma. Med Oncol. 2011, 28 Suppl 1, S333–S3440. [Google Scholar] [CrossRef]
- Zhigang, H.; Qi, Z.; Jugao, F.; Xiaohong, C.; Wei, Z.; Hong, W.; Hu, H.; Na, M.; Zheng, Y.; Demin, H. Reverse multidrug resistance in laryngeal cancer cells by knockdown MDR1 gene expression. J Otolaryngol Head Neck Surg. 2009, 38, 440–448. [Google Scholar]
- Li, L.; Jiang, A.C.; Dong, P.; Wan, Y.; Yu, Z.W. The characteristics of Hep-2 cell with multiple drug resistance induced by Taxol. Otolaryngol Head Neck Surg. 2007, 137, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Dechsupa, N.; Khamto, N.; Chawapun, P.; Siriphong, S.; Innuan, P.; Suwan, A.; Luangsuep, T.; Photilimthana, N.; Maita, W.; Thanacharttanatchaya, R.; et al. Pentagalloyl Glucose-Targeted Inhibition of P-Glycoprotein and Re-Sensitization of Multidrug-Resistant Leukemic Cells (K562/ADR) to Doxorubicin: In Silico and Functional Studies. Pharmaceuticals 2023, 16, 1192. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.H. Crosstalk between Microtubule Stabilizing Agents and Prostate Cancer. Cancers. 2023, 15, 3308. [Google Scholar] [CrossRef] [PubMed]
- Joshi, A.; Patil, V.; Noronha, V.; Dhumal, S.; Pande, N.; Chandrasekharan, A.; Turkar, S.; Dsouza, H.; Shrirangwar, S.; Mahajan, A.; et al. Results of a phase II randomized controlled clinical trial comparing efficacy of Cabazitaxel versus Docetaxel as second line or above therapy in recurrent head and neck cancer. Oral Oncol. 2017, 75, 54–60. [Google Scholar] [CrossRef]
- Domanitskaya, N.; Wangari-Talbot, J.; Jacobs, J.; Peiffer, E.; Mahdaviyeh, Y.; Paulose, C.; Malofeeva, E.; Foster, K.; Cai, K.Q. Zhou, Y.; et al. Abcc10 status affects mammary tumour growth, metastasis, and docetaxel treatment response. Br J Cancer. 2014, 111, 696–707. [Google Scholar] [CrossRef]
- Liu, Y.; Li, G.; Liu, C.; Tang, Y.; Zhang, S. RSF1 regulates the proliferation and paclitaxel resistance via modulating NF-κB signaling pathway in nasopharyngeal carcinoma. J Cancer. 2017, 8, 354–362. [Google Scholar] [CrossRef]
- Kansal, V.; Kinney, B.L.C.; Uppada, S.; Saba, N.F.; Stokes, W.A.; Buchwald, Z.S.; Schmitt, N.C. The expanding role of IAP antagonists for the treatment of head and neck cancer. Cancer Med. 2023, 12, 13958–13965. [Google Scholar] [CrossRef]
- Gomez-Roca, C.; Even, C.; Le Tourneau, C.; Basté, N.; Delord, J.P.; Sarini, J.; Vergez, S.; Temam, S.; Hoffmann, C.; Rochaix, P.; et al. Exploratory window-of-opportunity trial to investigate the tumor pharmacokinetics/pharmacodynamics of the IAP antagonist Debio 1143 in patients with head and neck cancer. Clin Transl Sci. 2022, 15, 55–62. [Google Scholar] [CrossRef]
- Ariffin, A.B.; Forde, P.F.; Jahangeer, S.; Soden, D.M.; Hinchion, J. Releasing pressure in tumors: what do we know so far and where do we go from here? A review. Cancer Res. 2014, 74, 2655–2662. [Google Scholar] [CrossRef]
- Lin, Z.; Zhang, Q.; Luo, W. Angiogenesis inhibitors as therapeutic agents in cancer: Challenges and future directions. Eur J Pharmacol. 2016, 793, 76–81. [Google Scholar] [CrossRef]
- Heydar, H.; Mansouri, K.; Norooznezhad, M.; Norooznezhad, F.; Mohamadnia, A.; Bahrami, N. Bevacizumab Inhibits Angiogenic Cytokines in Head and Neck Squamous Cell Carcinoma: From Gene to the Protein. Int J Hematol Oncol Stem Cell Res. 2018, 12, 136–141. [Google Scholar] [PubMed]
- Hoang, T.; Huang, S.; Armstrong, E.; Eickhoff, J.C.; Harari, P.M. Enhancement of radiation response with bevacizumab. J Exp Clin Cancer Res. 2012, 31, 37. [Google Scholar] [CrossRef] [PubMed]
- Argiris, A.; Li, S.; Savvides, P.; Ohr, J.P.; Gilbert, J.; Levine, M.A.; Chakravarti, A.; Haigentz, M Jr. ; Saba, N.F.; Ikpeazu, C.V.; et al. Phase III Randomized Trial of Chemotherapy With or Without Bevacizumab in Patients With Recurrent or Metastatic Head and Neck Cancer. J Clin Oncol. 2019, 37, 3266–3274. [Google Scholar] [CrossRef] [PubMed]
- Yao, M.; Galanopoulos, N.; Lavertu, P.; Fu, P.; Gibson, M.; Argiris, A.; Rezaee, R.; Zender, C.; Wasman, J.; Machtay, M.; et al. Phase II study of bevacizumab in combination with docetaxel and radiation in locally advanced squamous cell carcinoma of the head and neck. Head Neck. 2015, 37, 1665–1671. [Google Scholar] [CrossRef]
- Salama, J.K.; Haraf, D.J.; Stenson, K.M.; Blair, E.A.; Witt, M.E.; Williams, R.; Kunnavakkam, R.; Cohen, E.E.; Seiwert, T.; Vokes, E.E. A randomized phase II study of 5-fluorouracil, hydroxyurea, and twice-daily radiotherapy compared with bevacizumab plus 5-fluorouracil, hydroxyurea, and twice-daily radiotherapy for intermediate-stage and T4N0-1 head and neck cancers. Ann Oncol. 2011, 22, 2304–2309. [Google Scholar] [CrossRef] [PubMed]
- Elser, C.; Siu, L.L.; Winquist, E.; Agulnik, M.; Pond, G.R.; Chin, S.F.; Francis, P.; Cheiken, R.; Elting, J.; McNabola, A.; et al. Phase II trial of sorafenib in patients with recurrent or metastatic squamous cell carcinoma of the head and neck or nasopharyngeal carcinoma. J Clin Oncol. 2007, 25, 3766–3773. [Google Scholar] [CrossRef]
- Cooney, M.M.; Tserng, K.Y.; Makar, V.; McPeak, R.J.; Ingalls, S.T.; Dowlati, A.; Overmoyer, B.; McCrae, K.; Ksenich, P.; Lavertu, P.; et al. A phase IB clinical and pharmacokinetic study of the angiogenesis inhibitor SU5416 and paclitaxel in recurrent or metastatic carcinoma of the head and neck. Cancer Chemother Pharmacol. 2005, 55, 295–300. [Google Scholar] [CrossRef]
- Limaye, S.; Riley, S.; Zhao, S.; O'Neill, A.; Posner, M.; Adkins, D.; Jaffa, Z.; Clark, J.; Haddad, R. A randomized phase II study of docetaxel with or without vandetanib in recurrent or metastatic squamous cell carcinoma of head and neck (SCCHN). Oral Oncol. 2013, 49, 835–841. [Google Scholar] [CrossRef]
- Seidel, J.A.; Otsuka, A.; Kabashima, K. Anti-PD-1 and Anti-CTLA-4 Therapies in Cancer: Mechanisms of Action, Efficacy, and Limitations. Front Oncol. 2018, 8, 86. [Google Scholar] [CrossRef]
- Sakai, A.; Ebisumoto, K.; Iijima, H.; Yamauchi, M.; Teramura, T.; Yamazaki, A.; Watanabe, T.; Inagi, T.; Maki, D.; Okami, K. Chemotherapy following immune checkpoint inhibitors in recurrent or metastatic head and neck squamous cell carcinoma: clinical effectiveness and influence of inflammatory and nutritional factors. Discov Oncol. 2023, 14, 158. [Google Scholar] [CrossRef]
- Reinisch, M.; Ataseven, B.; Kümmel, S. Neoadjuvant Dose-Dense and Dose-Intensified Chemotherapy in Breast Cancer - Review of the Literature. Breast Care. 2016, 11, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Lyman, G.H.; Barron, R.L.; Natoli, J.L.; Miller, R.M. Systematic review of efficacy of dose-dense versus non-dose-dense chemotherapy in breast cancer, non-Hodgkin lymphoma, and non-small cell lung cancer. Crit Rev Oncol Hematol. 2012, 81, 296–308. [Google Scholar] [CrossRef] [PubMed]
- Fayette, J.; Fontaine-Delaruelle, C.; Ambrun, A.; Daveau, C.; Poupart, M.; Ramade, A.; Zrounba, P.; Neidhardt, E.M.; Péron, J.; Diallo, A.; et al. Neoadjuvant modified TPF (docetaxel, cisplatin, fluorouracil) for patients unfit to standard TPF in locally advanced head and neck squamous cell carcinoma: a study of 48 patients. Oncotarget. 2016, 7, 37297–37304. [Google Scholar] [CrossRef] [PubMed]
- Anantharamu, S.; Jacob, L.A.; Dasappa, L.; Babu, M.C.S.; Lokesh, K.N.; Rudresha, A.H.; Lakkavalli Krishnappa, R.; Saldanha, S.C. A prospective comparative study on biweekly docetaxel, cisplatin, 5-fluorouracil, leucovorin (TPFL) versus triweekly TPF as an induction chemotherapy in locally advanced squamous cell carcinoma of head and neck. Ann Oncol. 2022, 33, S850. [Google Scholar] [CrossRef]
Figure 1.
Resistant mechanisms of taxanes in HNSCC.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



