
Submitted:
25 September 2023
Posted:
26 September 2023
You are already at the latest version
Abstract
Fibrodysplasia Ossificans Progressiva (FOP) is an enigmatic, ultra-rare genetic disorder characterized by progressive heterotopic ossification, wherein soft connective tissues undergo pathological transformation into bone structures. This incapacitating process severely limits patient mobility and poses formidable challenges for therapeutic intervention. Predominantly caused by missense mutations in the ACVR1 gene, the disorder has hitherto defied comprehensive mechanistic understanding and effective treatment paradigms. This write-up offers a comprehensive overview of the contemporary understanding of FOP's complex pathobiology, underscored by advances in molecular genetics and proteomic studies. We shed light on targeted therapy, spanning genetic therapeutics, enzymatic and transcriptional modulation, stem cell therapies, and innovative immunotherapies. We also focused on the intricate complexities surrounding clinical trial design for ultra-rare disorders like FOP, addressing fundamental statistical limitations, ethical conundrums, and methodological advancements essential for the success of interventional studies. We advocate for the adoption of a multi-disciplinary approach that converges bench-to-bedside research, clinical expertise, and ethical considerations to tackle the challenges of ultra-rare diseases like FOP and comparable ultra-rare diseases. Overall, this article serves a dual role: as a definitive scientific resource for ongoing and future FOP research and as a call to action for innovative solutions to address methodological and ethical challenges that impede progress in the broader field of medical research for ultra-rare conditions.
Keywords:
Fibrodysplasia ossificans progressiva (FOP)
; heterotopic ossification
; bone morphogenetic proteins (BMPs)
; ACVR1
; antisense therapy
1. Introduction
Fibrodysplasia Ossificans Progressiva (FOP, OMIM #135100), also known colloquially as Stoneman Syndrome or Woodman Syndrome, is a rare and debilitating genetic disorder that has long perplexed the medical community [1,2,3]. As the name suggests, FOP encapsulates fibrous dysplasia and the inexorable progression of heterotopic ossification (HO). This disease is a paradigmatic model for understanding the dysregulation of cellular fate commitment and tissue homeostasis [2]. It transforms soft connective tissues, i.e., muscles, tendons, and ligaments, into bone via a process termed endochondral ossification [2]. In fact, it is the first known medical condition where one organ system changes into another [3]. Affecting roughly one in two million people worldwide, FOP is considered an ultra-rare disease [1,4,5]. A diagnostic hallmark of this condition is the congenital malformation of the big toes, commonly known as bilateral hallux valgus deformities [2,3].
At its molecular core, FOP is primarily driven by activating mutations in the gene encoding Activin Receptor A Type I (ACVR1), also referred to as ALK2 [6]. This receptor is pivotal to the bone morphogenetic protein (BMP) signaling pathways [7,8,9,10,11]. In individuals with FOP, mutations in ACVR1 lead to aberrant BMP signaling and render the receptor hyper-responsive to another ligand—Activin A [12]. This altered signaling serves as the catalyst for heterotopic ossification, the defining feature of FOP [2,6,13].
Clinically, the progression of FOP severely deteriorates the quality of life for patients. The disorder manifests in an episodic yet predictable manner; flare-ups frequently serve as precursors to localized HO [14,15,16,17,18]. Interestingly, the musculoskeletal transformation initially targets areas near the axial skeleton before spreading to the appendicular structure [19]. This spatiotemporal pattern suggests that other unidentified regulatory factors contribute to the localized susceptibility to HO. Complications of FOP are not limited to skeletal issues but extend to difficulties in speech, swallowing, and respiratory function, often leading to premature mortality [20].
Therapeutically, targeting ACVR1 presents a double-edged sword due to its ubiquitous role in skeletogenesis, raising significant concerns about potential undesirable effects [21]. Nevertheless, several therapeutic approaches, including genetic therapies, small molecules inhibitors, and stem cell therapies, are currently under stringent clinical evaluation [22,23,24]. These therapies aim to attenuate Activin A binding or inhibit the kinase activity of ALK2. Additional therapeutic avenues, e.g., modulation of mTOR (mechanistic target of rapamycin) signaling and activation of retinoic acid receptor gamma (RARγ), offer alternative strategies to inhibit the early stages of chondrogenesis and endochondral ossification [23,24,25].
This write-up aims to encapsulate our current understanding of FOP, assess the merits and limitations of emerging therapies, and identify gaps in our knowledge that could inform future research. It will delve into the molecular mechanisms underpinning the disorder, discuss current clinical management options, and critically evaluate the latest pharmaceutical advancements aimed at targeting this elusive condition.
2. A Brief Overview of the Disease FOP
The medical world's awareness of FOP can be traced back to the 17th century [26]. Early records by Parisian physicians like Guy Patin and André Falconet documented peculiar cases of progressive bone formation in muscles. Patin, then Dean of the Faculty of Medicine at the University of Paris, detailed a case involving progressive ossification of musculature along the spinal column—a seminal example of ectopic bone formation. Falconet expanded upon this understanding with his account of a woman whose body had turned "hard as wood," which likely represented an early observation of heterotopic ossification (HO).
Over the years, the condition accrued various nomenclatures including myositis ossificans progressiva, woodman syndrome, stone man syndrome, and Münchmeyer's disease. Reports from 1938 introduced additional perspectives, detailing peculiar bone growths, e.g., "shoemaker femur" and "rifle shoulders," which represented another form of ectopic bone formation [27]. It wasn't until the 1970s, however, that the name "Fibrodysplasia Ossificans Progressiva" gained official acceptance. Dr. Victor McKusick of Johns Hopkins University School of Medicine, considered the father of medical genetics, introduced this term to encompass the range of soft tissues more accurately—like tendons and ligaments—that could ossify [28]. Currently, FOP is estimated to affect approximately 0.88 individuals per million worldwide [1,4,5].
FOP's epidemiology presents marked regional variations [5,27,29,30,31,32]. The estimated global prevalence is roughly one case per two million people, with a striking 93% of affected individuals manifesting symptoms by age 15 [14,15,30]. Epidemiological data varies across nations: the United Kingdom reports 0.61 cases per million, Spain 0.36, and France 1.36 [5,27,29,30,31,33]. The United States leads in registered FOP cases, accounting for 25.6%, followed by China at 10.8% and Brazil at 8.4% [5,27,29,30,31]. Notably, significant data gaps exist in parts of Africa, the Mediterranean region, and South Asia, revealing disparities in healthcare access and awareness. Interestingly, based on our current knowledge, diagnoses in Asia often occur at younger ages [31].
Clinically, FOP manifests in a distinct yet systematic manner [14,15,16,17,18]. Individuals commonly display bilateral hallux valgus at birth and subsequently suffer from painful soft tissue flare-ups leading to HO [13]. These flare-ups can be triggered by a range of factors, including immunizations and surgeries. The pathophysiology of the diseases involves a complex interplay of events, starting with aberrant inflammation and culminating in misplaced bone formation. Secondary symptoms often include limb abnormalities, scoliosis, developmental hip dysplasia, and conductive hearing loss. FOP generally progresses in a cranial-to-caudal and axial-to-appendicular sequence, particularly in adolescents and young adults. Cardiopulmonary complications, e.g., thoracic insufficiency, are common and often lead to mortality [34]. Moreover, over one-third of patients experience deteriorating pulmonary function, usually worsening in late adolescence [14,15,30,31].
A significant challenge arises in diagnosing FOP [35]. Patients misdiagnosed as other conditions, including cancer, undergo unnecessary and even detrimental medical procedures. On average, accurate diagnosis lags four years behind the initial symptom presentation [35]. Despite advancements in both traditional and modern medicine, effective treatment options for FOP remain elusive.
3. The Complex Molecular Tapestry of FOP
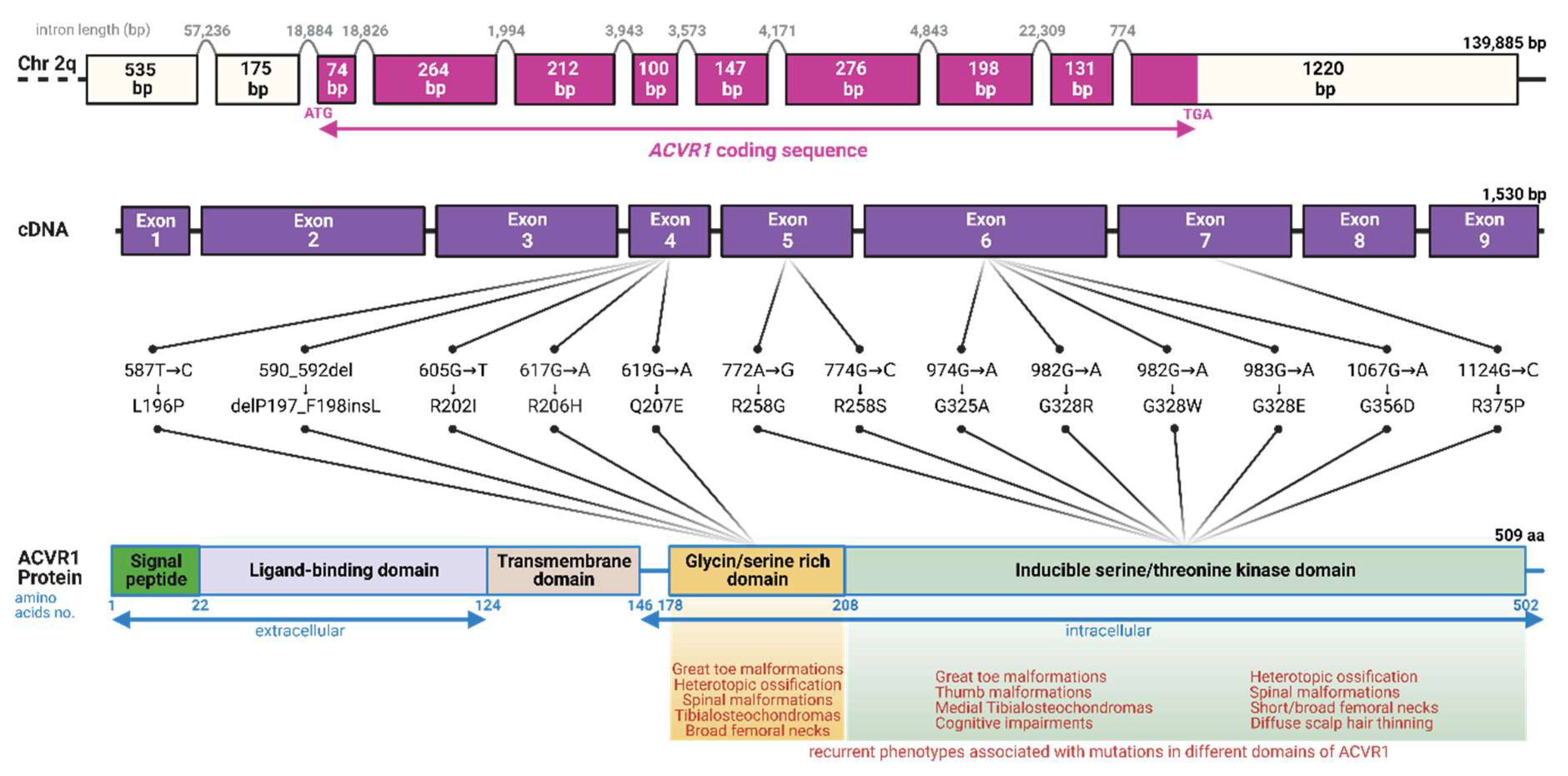
Historically, the medical community's understanding of FOP has been hindered by multiple technical and clinical obstacles [36]. These range from the challenge of obtaining viable tissue samples without exacerbating flare-ups to the absence of systematic data on early pathophysiology, which often leads to misdiagnoses. Moreover, prior to seminal discoveries in the genetic underpinnings of FOP less than two decades ago, the lack of reliable cellular and animal models further impeded progress [2,6]. In a groundbreaking effort in FOP research, the collaborative work of Eileen M. Shore and Frederick Kaplan at the University of Pennsylvania in 2006 identified a heterozygous missense mutation—ACVR1: 617G > A; R206H—in the ACVR1 gene [6]. This discovery was instrumental in FOP research, as 80–97% of all reported cases with FOP harbor this particular mutation [13,31,37,38,39]. Later studies have identified additional pathologically relevant variants within the ACVR1 gene, particularly in regions which code for the intracellular domains of the protein, including but not limited to G328E, R258S, and G356D (Figure 1) [18,40,41]. Most of these mutations arise spontaneously or de novo; however, a small subset of multi-generational FOP patients displaying an autosomal dominant inheritance pattern has been reported [42].
Figure 1.
Schematic overview of the human ACVR1 gene, its molecular architecture, and mutational landscape in FOP. This diagram depicts the structural components of the human ACVR1 gene, localized on chromosome 2q24.1, which comprises 9 coding exons spanning 1,530 base pairs (bp). The resulting encoded protein, ACVR1/ALK2, consists of 509 amino acids. Mutations linked to FOP predominantly affect the glycine/serine-rich and inducible serine/threonine kinase domains of the protein. Notably, the ACVR1R206H mutation is associated with >80% of reported FOP cases. Phenotypes commonly associated with mutations affecting different domains of ACVR1/ALK2 have been shown [13,29,31,37,38,39]. While the mutations displayed in the figure are recurrent, they are not exhaustive. Lengths of the exons at the genomic level have been shown inside each box (Created with BioRender: JQ25VJZ0R1).
Figure 1.
Schematic overview of the human ACVR1 gene, its molecular architecture, and mutational landscape in FOP. This diagram depicts the structural components of the human ACVR1 gene, localized on chromosome 2q24.1, which comprises 9 coding exons spanning 1,530 base pairs (bp). The resulting encoded protein, ACVR1/ALK2, consists of 509 amino acids. Mutations linked to FOP predominantly affect the glycine/serine-rich and inducible serine/threonine kinase domains of the protein. Notably, the ACVR1R206H mutation is associated with >80% of reported FOP cases. Phenotypes commonly associated with mutations affecting different domains of ACVR1/ALK2 have been shown [13,29,31,37,38,39]. While the mutations displayed in the figure are recurrent, they are not exhaustive. Lengths of the exons at the genomic level have been shown inside each box (Created with BioRender: JQ25VJZ0R1).
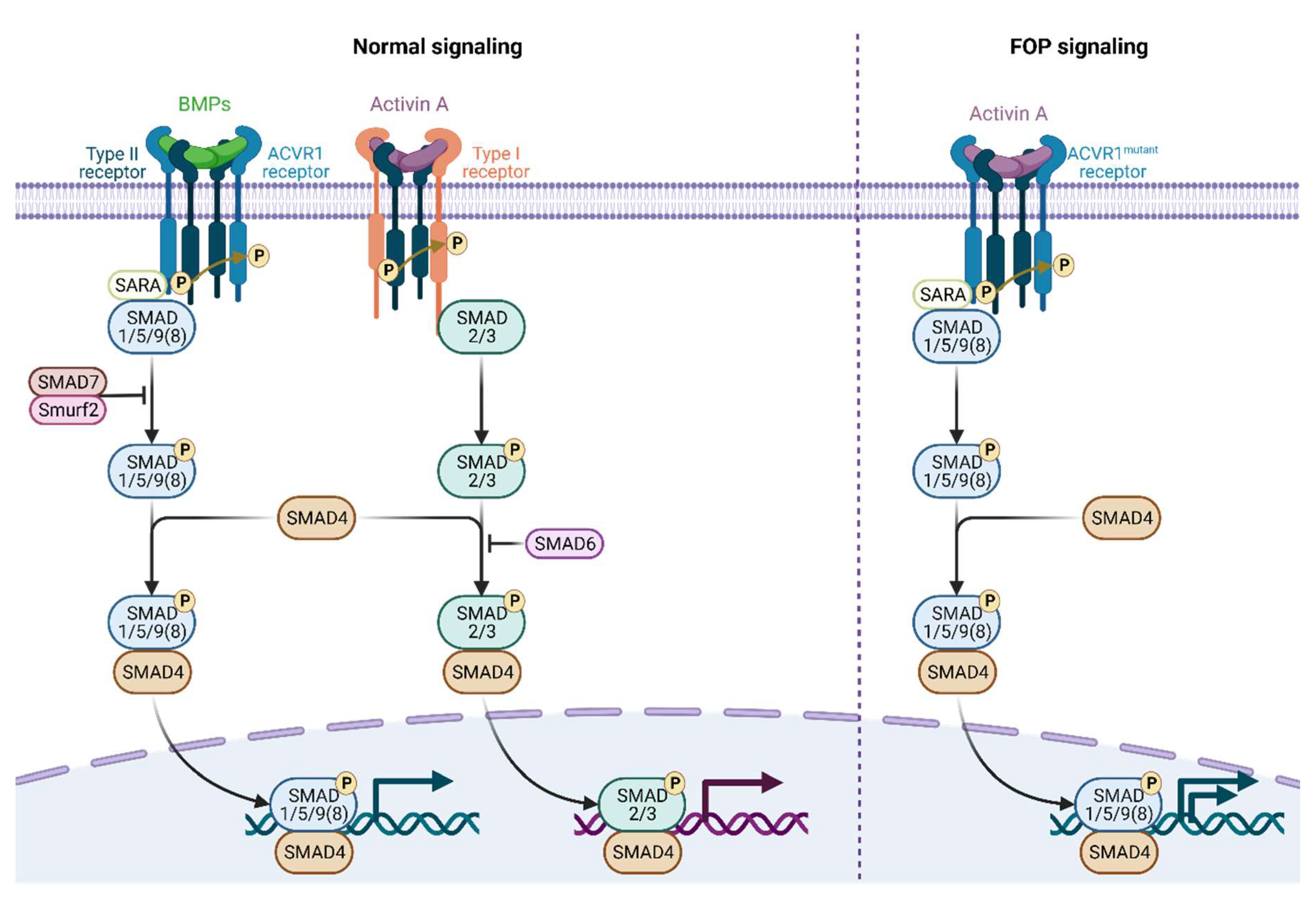
From a genomic standpoint, the ACVR1 gene, which encodes the Activin A receptor type I or activin receptor-like kinase-2 (ACVR1/ALK2), is located on the long arm of chromosome 2 [43]. This receptor plays a key role in the bone morphogenetic protein (BMP) signaling pathway, essential for developmental processes, notably bone and cartilage formation [44]. Under normal circumstances, secreted BMPs bind to complexes of type I and type II serine/threonine kinase BMP receptors on the cell surface, e.g., ACVR1 for BMP and ALK4/7 for activin A, setting off an intracellular signaling cascade [Figure 2] [12,21]. In the absence of BMP ligands, a regulatory protein called FKBP1A (FK506 binding protein 1A) binds to ACVR1, inhibiting its ability to bind effector molecules [18,41,45,46]. When BMP ligands are present, the type II receptor phosphorylates the type I receptor within its glycine/serine-rich domain [2,7,8,9,10,11,47,48,49,50]. This results in FKBP1A’s release, allowing ACVR1 to bind and phosphorylate intracellular BMP-responsive transcription factors known as receptor-regulated SMADs (R-SMADs), specifically SMAD1/5/9(8) [12]. The phosphorylated R-SMADs then form a complex with the co-mediator SMAD4. This complex then associates with co-activators or co-repressors to regulate transcription related to endochondral ossification. While SMAD1 and SMAD5 activate transcription in this context, SMAD9 serves as a transcriptional repressor.
Figure 2.
Canonical and aberrant BMP signaling and FOP. The canonical and aberrant activin A-mediated BMP signaling observed in FOP via mutant ALK2 receptors has been shown. Under physiological conditions, BMP or activin A ligands orchestrate the formation of a heterotetramaric receptor complex, comprising a homodimer of type II receptors in conjunction with a homodimer of type I receptors (e.g., ALK2 for BMP, ALK4/7 for activin A). This complex serves as a substrate for intramolecular phosphorylation events: the type II receptor phosphorylates the type I receptor, thereby activating it. Upon activation, the type I receptor in turn phosphorylates intracellular SMAD proteins—specifically SMAD1/5/9(8) in the context of BMP signaling and SMAD2/3 in the context of activin A signaling. This series of phosphorylation events, at the presence of SMAD4, culminates in the effective transduction of canonical BMP and TGF-β signaling pathways, respectively. The pathological landscape of FOP is characterized by aberrant activin A signaling, which anomalously cross-activates BMP signaling via mutated ALK2 receptors. This deviation from the canonical pathway represents a critical molecular mechanism underlying the pathological manifestations of FOP. This mutant ALK2 receptor also renders the overall signaling hyperactive (Created with BioRender: BM25VJZ5RH).
Figure 2.
Canonical and aberrant BMP signaling and FOP. The canonical and aberrant activin A-mediated BMP signaling observed in FOP via mutant ALK2 receptors has been shown. Under physiological conditions, BMP or activin A ligands orchestrate the formation of a heterotetramaric receptor complex, comprising a homodimer of type II receptors in conjunction with a homodimer of type I receptors (e.g., ALK2 for BMP, ALK4/7 for activin A). This complex serves as a substrate for intramolecular phosphorylation events: the type II receptor phosphorylates the type I receptor, thereby activating it. Upon activation, the type I receptor in turn phosphorylates intracellular SMAD proteins—specifically SMAD1/5/9(8) in the context of BMP signaling and SMAD2/3 in the context of activin A signaling. This series of phosphorylation events, at the presence of SMAD4, culminates in the effective transduction of canonical BMP and TGF-β signaling pathways, respectively. The pathological landscape of FOP is characterized by aberrant activin A signaling, which anomalously cross-activates BMP signaling via mutated ALK2 receptors. This deviation from the canonical pathway represents a critical molecular mechanism underlying the pathological manifestations of FOP. This mutant ALK2 receptor also renders the overall signaling hyperactive (Created with BioRender: BM25VJZ5RH).
In FOP, mutations, like ACVR1R206H, cause the receptor to become hyperactive, even when it should be in an inactive state [Figure 2] [2,51]. Initially, mutations in the ACVR1 gene were believed to enhance BMP signaling through ACVR1/ALK2 complexes, thereby triggering heterotopic ossification in FOP. However, subsequent research has revealed a more complex molecular landscape [2]. The transforming growth factor-β (TGF-β) superfamily has emerged as a crucial player in the molecular etiology of both FOP and trauma-induced HO. Key ligands in this superfamily, e.g., TGF-β1 and BMP, activate R-SMADs and also participate in non-canonical pathways involving molecules like mitogen-activated protein kinases (MAPKs), phosphoinositide 3-kinases (PI3K), protein kinase B (PKB/AKT), mechanistic target of rapamycin (mTOR), and TGF-β activated kinase 1 (TAK1) [11,12,52,53]. Mutation in ACVR1 causes ACVR1 to remain active without ligands, disrupting cellular homeostasis and causing pathological ossification of connective and muscle tissues [54]. The mutated receptor also shows altered affinity toward its regulatory protein FKBP1A, impairing proper receptor regulation and leading to abnormal bone and cartilage growth, ultimately resulting in joint fusion [2,11,12]. Furthermore, ACVR1R206H makes ALK2 hypersensitive to Activin A, a phenomenon referred to as neo-receptorization [55]. Under normal homeostatic conditions, ACVR1 modulates BMP signaling to maintain cellular stability. However, the ACVR1R206H mutation disrupts this equilibrium, causing the receptor to advocate for increased BMP signaling, leading to pathological outcomes.
While our understanding of FOP's pathobiology has significantly advanced, several key questions remain unanswered, particularly concerning the role of ACVR1 receptor complexes in normal cellular homeostasis and the pathways influencing fibro-adipogenic progenitors (FAPs) toward osteogenic phenotypes under traumatic or inflammatory conditions [36,56]. Additionally, there is a compelling need to elucidate the unique structural perturbations brought about by ACVR1R206H, including its propensity for ACVR1 homodimerization.
Targeting this complex etiological framework has proved therapeutically elusive. Antibodies against Activin A have demonstrated some efficacy in mitigating HO in animal models; however, counterintuitively, anti-ACVR1 antibodies designed to neutralize receptor function have exacerbated HO, thereby complicating treatment paradigms [11,22,23,24]. Current avenues of investigation include Activin A antibodies, mTOR inhibitors like rapamycin, and retinoic acid receptor-gamma (RARγ) agonists, which are collectively poised to revolutionize our understanding of FOP and potentially provide clinically viable interventions. Also, genetic therapeutic approaches, e.g., gene therapy, and allele-specific gene knockdown, are being explored [57,58,59,60,61].
Thanks to the extraordinary research in the past two decades, the understanding of FOP has transitioned from a simplistic, reductionist model to a complex interplay of signaling cascades and regulatory molecules [36,54]. Navigating this complex terrain remains a daunting task, necessitating sustained, multidisciplinary research efforts to develop targeted, effective therapies for this debilitating condition.
4. Clinical Presentation, Diagnosis, and Management of FOP
Accurate and timely identification of FOP is crucial [30,62]. Pediatricians are often the first medical professionals to encounter children with FOP, making their awareness of the disease essential for early diagnosis and appropriate management. Diagnostic suspicion is vital since a lack of it can lead to delays and potentially harmful misdiagnoses, which may result in invasive and counterproductive testing like biopsies [62,63]. These procedures could exacerbate the condition by inducing flare-ups and promoting HO.
Clinically, FOP is often initially suspected based on the presence of hallmark congenital deformities, predominantly malformations of the great toes, e.g., hallux valgus and macrodactyly [35,64]. The onset of episodic flare-ups, marked by painful and warm soft tissue swellings, usually begins in the first decade of life [16]. Triggered by a range of pro-inflammatory factors, these flare-ups result from underlying inflammation in the tendons, ligaments, or muscles. Moreover, a subset of patients may manifest non-standard features, referred to as FOP-plus (FOP+), which can include a range of anomalies from tibial osteochondromas to cognitive impairment [65]. These features are often associated with specific ACVR1 mutations, e.g., R206H and Q207E. Frequently, FOP manifests its effects on the cervical spine at an early stage [66]. This involvement begins with localized flare-ups and neck stiffness, which may progress to bony ankylosis, severely restricting neck movement. FOP can affect various body joints in an unpredictable manner, often leaving patients wheelchair-bound by their late teens or early twenties. Additional complications can include hearing loss, malnourishment due to jaw involvement, and life-threatening thoracic insufficiency syndrome. Although clinical presentation is significant, the gold standard for diagnosing FOP remains DNA sequencing to identify underlying mutations in the ACVR1 gene. Biopsy and other invasive procedures should be avoided, as they risk exacerbating the condition by promoting HO.
Current clinical management of FOP is primarily aimed at controlling inflammation, as it triggers the cascade of events leading to HO [24,25,29]. However, managing triggering events remains challenging, as they can range from significant physical trauma to seemingly trivial incidents. The pharmacological landscape is evolving, categorized into three classes: Class I medications like high-dose corticosteroids, non-steroidal anti-inflammatory drugs (NSAIDs), cyclooxygenase 2 (COX2) inhibitors, mast cell inhibitors, aminobisphosphonates, and muscle relaxants are used to manage flare-ups; Class II medications have theoretical but unproven applications in FOP; and Class III medications are under clinical investigation [29,51,67,68,69,70,71,72,73,74].
Flare-ups are usually managed by a 3–5-day course of high-dose corticosteroids, e.g., prednisone, to alleviate inflammation and tissue edema; however, the applicability of corticosteroids to relieve inflammation is not body-wide, and its frequent use to manage swelling in the trunk and neck is not recommended due to difficulties in assessing the onset of flare-ups [75]. After discontinuing corticosteroids, mast cell inhibitors, aminobisphosphonates, NSAIDs, and COX-2 inhibitors can be used to manage subsequent flare-ups [24,51,75,76,77]. A small dose of a muscle relaxant may help relieve muscle spasms [51,75,76].
Palovarotene, a selective retinoic acid receptor gamma agonist initially developed by researchers led by Maurizio Pacifici at the Children’s Hospital of Philadelphia and later licensed to Ipsen Biopharmaceuticals, is a promising medication strategy for FOP [78,79]. It received approval for medical use in FOP by Health Canada and the U.S. Food and Drug Administration (FDA) in 2022 and 2023, respectively [80,81]. Palovarotene aims to inhibit aberrant BMP signaling to reduce HO risk [61]. However, the drug failed a futility test in clinical trials, raising safety concerns [82,83]. Its inability to distinguish between wild-type and mutant ACVR1 is a significant limitation, posing significant risks, e.g., paronychia and decubitus ulcers. In addition, palovarotene and its metabolites are assumed to have embryotoxic and teratogenic effects. Consequently, it is contraindicated for a substantial subset of the FOP population [81].
Experimental approaches for FOP, including allele-selective nucleic acid-based RNA knockdown strategies, BMP receptor kinase inhibitors, gene therapy, stem cell therapies, and immuno-therapies, hold promise for both managing symptoms and modifying the course of FOP [23,24,84]. Overall, the pharmacological landscape for FOP is evolving, with the goal of achieving a balance between symptom management and disease modification. In the subsequent sections of this write-up, we will focus on these experimental approaches that are currently being investigated to treat FOP effectively.
5. Experimental and Prospective Therapeutic Approaches for FOP
In the evolving landscape of FOP research, many experimental and prospective approaches are advancing toward translational medicine, numerous approaches transcending the limitations of traditional pharmacotherapies are emerging, each with its own set of promises and challenges. These can be grouped into four main categories: genetic approaches, enzymatic and transcriptional target modulators, stem cell therapies, and immunotherapies [23,24,84]. In addition, there have been some continuous works going on to repurpose drugs for FOP [85].
CRISPR-Cas (Clustered Regularly Interspaced Short Palindromic Repeats and CRISPR-associated proteins) technology has captured significant attention for its precise ability to alter mutant ACVR1 gene [23]. This precision is a marked departure from small-molecule inhibitors, which, while effective, often carry systemic side effects like skin and metabolic issues. Another promising avenue is RNA-based therapies designed to specifically silence the mutant ACVR1 gene [59,60,61]. This could halt the abnormal bone formation characteristic of FOP, offering a targeted therapeutic approach. In parallel, researchers are investigating crucial enzymatic pathways, e.g., glycogen synthase kinase-3 (GSK-3β) and transcription factors like peroxisome proliferator-activated receptor-γ (PPARγ). Both play significant roles in bone formation and inflammation[23,24,67,78]. Small molecule inhibitors targeting these proteins offer an alternative that could avoid some of the risks associated with gene therapies. Besides, innovative strategies using mesenchymal stem cells (MSCs) and induced pluripotent stem cells (iPSCs) hold great promise for tissue regeneration [23]. However, questions remain about how these cells behave in the body and their potential to worsen FOP symptoms. In an era when immunotherapy continues to revolutionize cancer treatment, its application to FOP is intriguing [23]. Using tools like monoclonal antibodies and immune checkpoint inhibitors could represent a significant shift in FOP treatment, potentially moderating the heightened immune responses often seen in patients with this condition.
Despite these advances, challenges remain. These include a lack of suitable animal models for testing, the risk of disease flare-ups post-treatment, and the disease's variable manifestations. Each of these hurdles necessitates rigorous preclinical and clinical evaluations. The emerging therapies are expanding the treatment landscape for FOP and enhancing our understanding of both bone biology and immune responses.
5.1. Genetic Therapeutics for FOP
The advent of genetic therapies presents a promising frontier in FOP therapeutic research. These therapeutic strategies primarily focus on the genetic root of the condition, typically mutations in the ACVR1 gene. Approaches such as gene editing, gene addition, gene silencing, and gene replacement are currently being explored [Table 1] [84]. Each approach offers a unique set of advantages and challenges; however, collectively, they aim to rectify or modulate the expression of the mutated gene, thereby alleviating the clinical outcome. These genetic therapies could mark a paradigm shift in the treatment of FOP, offering not just symptomatic relief but potentially a long-term solution.
5.1.1. CRISPR-Cas gene editing therapies
CRISPR-Cas is a genome-editing tool that allows for precise targeting and modification of DNA sequences [86,87]. The realm of CRISPR-Cas9 has captivated the scientific community with its groundbreaking capabilities in gene editing [88]. In the context of FOP, CRISPR can be bioengineered to target the mutant ACVR1 allele and modify or correct the mutation [89]. The delivery of the CRISPR-Cas9 complex is generally facilitated through viral vectors, e.g., adeno-associated virus (AAV), or lipid nanoparticles (LNPs), with tissue specificity ensured through vector selection [90,91]. A carefully chosen vector, specific to the tissue of interest, ensures that the gene editing occurs only in targeted cells. Although the technology is admired for its unparalleled precision and resultant genomic permanence, significant issues, including off-target mutations, ethical considerations, and the complex process of regulatory approvals, pose challenges to the clinical adoption of CRISPR-Cas gene editing therapies for FOP.
5.1.2. RNA-based therapies
RNA-based therapies employ antisense oligonucleotides (ASOs), e.g., small interfering RNAs (siRNA), gapmers, aptamers, agomirs and antagomirs, and steric-blocking oligonucleotides—these ASOs temper gene expression post-transcriptionally with high specificity through a wide array of mechanisms [92]. An allele-specific silencing strategy is particularly appealing for FOP as it could attenuate the hyperactivity of the mutant ACVR1 without compromising the wild-type activity [93]. Studies by Kaplan et al. and Takahashi et al. demonstrated the development of allele-specific siRNAs, while Maruyama et al. have recently explored locked nucleic acid (LNA) gapmers for targeted suppression [59,60,61]. These gapmers preferentially lowered ACVR1R206H expression and the level of the protein encoded while leaving most of the normal products intact, leading to suppression of osteogenic differentiation in vitro. Despite their high specificity and reversible action, RNA-based therapies may necessitate frequent administration. In addition, in vivo delivery of these RNA-based therapies poses significant challenges for their widespread clinical use.
5.1.3. Gene therapies
Drawing parallels from the therapeutic success in monogenic disorders, e.g., lipoprotein lipase deficiency, inherited retinal dystrophy, and spinal muscular atrophy, it is conceivable that extant gene therapies could be efficacious for FOP, as it is also caused by a monogenic gain-of-function mutation in the ACVR1 gene [23,84,94,95]. In general, gene addition aims to introduce genes encoding missing proteins or encoding corrective proteins if a genetic mutation produces defective proteins. A landmark study by Yang et al. has exemplified the potential of gene replacement therapy [58]. Using an AAV vector, the researchers simultaneously silence the mutated gene (ACVR1R206H) and reintroduce its wild-type variant. This rescued the aberrant BMP signaling pathways and effectively prevented and treated trauma-induced HO in a murine model of FOP. These findings were substantiated by a prior proof-of-concept study by the same researchers, wherein a recombinant AAV vector carrying a healthy ACVR1 gene, coupled with artificial microRNA to silence the mutant gene, to suppress ectopic bone formation in mice [57]. While the prospective benefits of gene therapies are considerable, the challenges are non-trivial. Notably, the looming risks of insertional mutagenesis and immunological responses against viral vectors warrant caution.
5.1.4. Future prospects for genetic approaches for FOP
When comparing these therapeutic approaches, the intricate technical variables, such as the choice between in vivo and ex vivo interventions, as well as the accessibility of targeted tissues, must be taken into consideration [22]. From an ethical and regulatory standpoint, all these approaches encounter difficulties. Nevertheless, advancements in nanoparticle delivery systems, enhancements in CRISPR specificity, and innovations in RNA formulations offer a promising outlook for the future of FOP therapeutics.
5.2. Enzymatic and Transcriptional Target Modulators
The treatment landscape for FOP is gradually being reshaped by enzymatic and transcriptional target modulators, which aim to attenuate or reverse the pathology by selectively targeting key signaling pathways and gene expression mechanisms [23,96]. This section elucidates the principal types of modulators under investigation and their therapeutic potential, supported by preclinical studies and ongoing research.
5.2.1. Targeting BMP signaling: antagonists and allosteric modulators
The BMP signaling cascade is central to the pathogenesis of FOP. Transcriptional modulators, including BMP receptor antagonists, operate by preventing the ligand-induced conformational change requisite for intracellular signaling [96]. Allosteric inhibitors such as dorsomorphin target BMP type I receptors, particularly ACVR1, and have shown efficacy in abrogating ectopic ossification in animal models. Ligand traps, synthesized as chimeric proteins comprising the extracellular domain of ACVR2B or ACVR2A fused to the Fc region of IgG1, have also demonstrated their efficacy in sequestering BMP ligands [97,98]. Palovarotene, the only FDA-approved therapy for FOP, indirectly abrogates BMP signaling, making it a leading candidate for further investigation [45, 46]. Other proposed approaches include BMP receptor kinase inhibitors, e.g., dorsomorphin, downstream BMP signaling inhibitors, e.g., fendiline and perhexiline, and fungal metabolite osteoblast differentiation inhibitors, e.g., NG-391, NG-393 and trichocyalide A/B [51,99,100,101,102].
5.2.2. Dual-targeting via mTOR pathway inhibition
The mTOR signaling pathway plays a multifaceted role in FOP, particularly in osteogenic and chondrogenic differentiation [103]. Rapamycin, a well-known immunosuppressive drug, exerts its effects through inhibition of mTORC1, thereby thwarting activin A-induced chondrogenesis and osteogenesis. Inhibition of mTORC1 using rapamycin, in turn, mitigates activin A-induced chondrogenesis and osteogenesis, presenting a compelling avenue for FOP intervention [25]. Besides rapamycin, another promising avenue in FOP treatment revolves around PI3Kα inhibitors, notably BYL719 [104]. These inhibitors have exhibited considerable potential in preclinical models, especially in cells harboring ACVR1 mutations associated with FOP. Their mechanism of action encompasses the simultaneous inhibition of key signaling pathways, including SMAD, AKT, aside from mTOR pathway [25,96]. This multifaceted approach underscores their promise to effectively manage FOP.
5.2.3. Neutralizing hyperactivated Activin A signaling via antibody modulation
Activin A signaling, pathologically upregulated in cells with the ACVR1R206H mutation, has been efficaciously modulated using neutralizing antibodies. Such antibodies act to inhibit the ligand-receptor interaction, thereby subverting downstream signaling and ultimately reducing heterotopic ossification. Clinical trials involving REGN2477 are in progress, aimed at establishing both the long-term safety and therapeutic efficacy of this approach [54,105].
5.2.4. Other approaches: GSK-3β Inhibition and PPARγ Activation
Emerging candidates include GSK-3β inhibitors, acting as downstream effectors in BMP signaling, and PPARγ agonists, which preferentially induce adipogenesis over osteogenesis [23,101]. The former aims to block the osteogenic differentiation of pluripotent stem cells, while the latter counteracts osteogenesis through upregulation of adipogenic genes.
5.2.5. Challenges and future directions
While these pharmacological interventions offer promising avenues for FOP treatment, inherent complexities, e.g., off-target effects and the specter of therapeutic resistance, must be judiciously considered [23,56,106]. The likely synergistic benefits of multi-targeted approaches may present enhanced therapeutic efficacy, though this requires thorough combinatorial analysis to ascertain potential antagonistic interactions. Enzymatic and transcriptional modulators are increasingly positioning themselves at the cutting edge of therapeutic innovation for FOP [24,96,98]. However, a more comprehensive understanding of their long-term safety profiles, pharmacokinetics, and pharmacodynamics is imperative for translating these therapeutic modalities from bench to bedside.
5.3. Stem cell therapies for FOP
The emergence of stem cell technologies, particularly MSCs and iPSCs, has offered new vistas of therapeutic possibilities [23,107]. MSCs, derived from tissues like bone marrow and adipose tissue, can differentiate into multiple cell types and have shown the potential to inhibit abnormal bone growth in FOP models. On the other hand, iPSCs, reprogrammed from adult cells, provide an even more tailored approach by allowing for disease-specific cellular models [107,108,109]. While both technologies are in the experimental stage, their ability to potentially replace malfunctioning cells and offer insights into the disease's mechanisms holds significant promise for the future management of FOP.
5.3.1. MSCs
MSCs are versatile cells that can be extracted from different sources like bone marrow and adipose tissue [23,107]. These cells can transform into various tissue types, including bone and cartilage, making them an excellent candidate for replacing the malfunctioning cells in FOP. Researchers are also exploring genetically modifying these MSCs to improve their effectiveness, targeting specific genes or cellular pathways contributing to the disease. However, the use of MSCs has its challenges. Early studies have shown inconsistent results in their effectiveness for treating FOP. There is also a slight but essential risk of these cells contributing to tumor formation. Furthermore, since MSCs come from external sources, the body's immune system might react against them.
5.3.2. iPSCs
Much like MSCs, iPSCs can also transform into any cell type, but they come with the added advantage of being tailored to the individual patient. iPSCs are created by reprogramming cells from an adult, avoiding the ethical concerns that come with using embryonic cells [23,108,109]. These reprogrammed cells can theoretically replace the dysfunctional bone-forming cells in FOP patients. The potential to develop patient-specific or disease-specific cells makes iPSCs incredibly useful for not just treatment but also for research into FOP. Yet iPSCs come with their own set of challenges. The process of reprogramming these cells is technically complex and expensive. Like MSCs, iPSCs also carry a small but significant risk of forming tumors.
5.3.3. Challenges and future directions
Both MSCs and iPSCs offer promising new pathways for treating FOP [23,107,108,109]. Each has unique benefits but also comes with its own set of limitations. The next crucial steps involve refining these promising technologies and testing their safety and effectiveness in large, rigorous clinical trials. In this ongoing journey to find a definitive treatment for FOP, MSCs and iPSCs stand out as particularly promising, holding the potential to significantly change how this devastating disease is managed in the future.
5.4. Immunotherapy
Emerging research is reconceptualizing FOP through an immunological lens, pointing toward an ensemble of immunological actors, including monocytes, macrophages, mast cells, and various cytokines that orchestrate pathological ossification [23,96,110].
5.4.1. Targeting specific antigens using monoclonal antibodies
Monoclonal antibodies (mAbs) have emerged as biological pharmaceuticals with unparalleled specificity, demonstrating potential as a therapeutic strategy for FOP [96,98,106]. These are immunoglobulins meticulously engineered to bind to specific antigens expressed on the surface of errant cells, thereby marking them for immune-mediated destruction. The conjugation of monoclonal antibodies with cytotoxic agents, such as toxins or radioisotopes, offers an additional mechanism to selectively target and annihilate cells responsible for HO. Monoclonal antibodies can be designed to target the complex signaling pathways that contribute to FOP, including aberrant BMP signaling and heightened cytokine production (IL-3, IL-7, IL-8, and IL-10) [23,111,112].
5.4.2. Modulating immune responses using immune checkpoint inhibitors
Concurrent with the mAbs paradigm, immune checkpoint inhibitors (ICIs) stand as another modality under rigorous investigation for the treatment of FOP [23,113]. ICIs act by negating the downregulatory signals that often shield pathological cells from immune detection. In the context of FOP, where aberrant immune signaling contributes to pathogenesis, ICIs can modulate the immunological landscape, allowing for more effective targeting of cells contributing to HO. Their ability to silence the immune system's signaling pathways has implications for reducing the activation of key players like TGF-beta, NF-κB, and MAPK signaling.
5.4.3. Cellular infiltrates
Inflammatory lesions in FOP often exhibit an accumulation of monocytes, macrophages, and mast cells, which seem to play a pivotal role in enhancing the inflammatory immune response [22,53]. These cellular infiltrates are responsible for the increased production of cytokines and chemokines, e.g., IL-3, IL-7, IL-8, IL-10, CCL5, CCR7, and CXCL10 [22,53,96]. Studies utilizing mouse models have illustrated that the depletion of macrophages and mast cells significantly mitigates heterotopic ossification, offering another potential avenue for treatment.
5.4.4. Prospective immunotherapeutic strategies for FOP
Immunotherapy offers a groundbreaking approach to FOP by capitalizing on the immunological peculiarities that drive its pathogenesis [22,23]. The specificity and targeted action of monoclonal antibodies, coupled with the immune modulation offered by checkpoint inhibitors, signify a potential therapeutic renaissance for this complex disease. Further research is warranted to investigate combination therapies and to ascertain long-term safety and efficacy. In a disease state as devastating and complex as FOP, the advent of immunotherapy may represent an incremental advance and a quantum leap in our therapeutic armamentarium.
5.5. Repurposed drugs for FOP: a glimpse of promise
Developing new medications for ultra-rare conditions like FOP is highly challenging for many reasons [36,114]. An alternative is to use existing drugs, known to be safe, for new purposes. This strategy, called drug repurposing, is faster, more cost-effective, and less risky [115]. It's especially useful for rare diseases like FOP, which face unique challenges in drug development [85,114]. Historically, many drugs, such as sildenafil and thalidomide, have found new uses through repurposing [114]. Currently, drugs like corticosteroids, celecoxib, and inhibitors targeting hypoxia-inducible factor 1α (HIF1α) and PI3Kα pathways show potential to treat FOP by addressing its key pathways in FOP pathology, e.g., inflammation and BMP signaling, and have the potential to inhibit HO [85]. Saracatinib, initially developed for cancers, has exhibited selective inhibition of ALK2, the key receptor in FOP [116]. In preclinical models, it effectively prevented HO, thereby emerging as a promising candidate for further clinical trials.
While findings from initial and/or preliminary clinical studies on repurposed drugs for FOP seems encouraging, thorough clinical trials are essential [117]. Modern tools like computational biology and cell models from patients can help speed up this process. Collaborations among researchers, patient groups, and regulators can further streamline drug approval. Repurposing drugs presents an efficient and promising path to better understand and treat FOP.
6. Impediments and Innovations for Clinical trials for FOP
The structural and epistemological complexities in executing clinical trials for FOP, or any ultra-rare disease, are enormous [36,118]. These obstacles include a dearth of standardized natural history data to inform trial designs, scarcity of validated and surrogate outcome measures, and diminutive patient populations, rendering traditional large-scale randomized control trials (RCTs) infeasible [36,118,119]. RCTs serve as the acme of empirical efficacy assessment in clinical research, primarily due to its capacity for minimizing selection bias and distributing potential confounders evenly across study groups. Nevertheless, the paucity of large cohorts in ultra-rare conditions like FOP disrupts the statistical robustness of RCTs. When samples are small, the stochastic noise associated with inter-individual differences amplifies, effectively attenuating the trial's statistical power and thereby increasing the risk of Type II errors.
Conversely, uncontrolled trials, which juxtapose interventional outcomes against the known natural history of a disease, offer a somewhat more practical design for conditions like FOP. However, this utility is circumscribed by the still-evolving understanding of FOP’s natural history and its marked inter-individual heterogeneity. Furthermore, subjects in natural history studies may under-report adverse events, engendering a bias that can discredit the risk-benefit profile of a new therapeutic agent.
Future FOP trials should incorporate adaptive designs and Bayesian statistical methods to rectify these pitfalls. Adaptive designs, often employed in early-phase clinical trials, allow modifications to trial procedures (e.g., dose adjustments) based on interim results. These designs are invaluable in maximizing the data utility from a small sample size without compromising the trial's integrity. Bayesian methods, conversely, can leverage prior data to inform current analysis, enhancing the interpretative power of trials with smaller cohorts.
A multitude of drugs targeting Activin A and BMP signaling pathways are currently in various phases of clinical trials, ranging from Phase 1 to Phase 3 [Table 2]. Each trial, while conforming to a randomized, double-blind, placebo-controlled design, features its unique arm configuration and primary endpoint measures, primarily focused on the volume of new HO lesions. However, these trials are not without limitations. Issues, e.g., patient recruitment, disease heterogeneity, lack of reliable biomarkers, and ethical concerns regarding placebo controls constitute formidable challenges.
Of note are the ethical implications surrounding using placebo groups in a disease as debilitating as FOP. The ethical aspects become particularly challenging when one considers the lifelong morbidity associated with each ossification event, thus raising the question of whether a placebo-controlled design can ever be ethically justifiable in this context [119]. The daunting obstacles inherent to FOP clinical trials epitomize the methodological and ethical complexities plaguing ultra-rare disease research. While no panacea exists to surmount these challenges in their entirety, innovative trial designs, sophisticated statistical methods, and a conscientious approach to ethical considerations can ameliorate these issues. FOP trials serve as a crucible, testing the adaptability and ingenuity of clinical research methods for ultra-rare diseases [23,31,118]. They force a reconceptualization of traditional paradigms, mandating a fusion of scientific rigor and ethical sensibility, all while maintaining an unwavering focus on the exigencies of patient welfare.
7. Conclusions
In summary, our manuscript offers a comprehensive investigation into the evolving landscape of FOP research and therapy. We embark on a journey through the traditional therapeutic models, pharmacological interventions, and culminate with the advent of immunotherapy as a potential game-changer for FOP treatment. As we highlight, the disease's complex pathophysiology poses both challenges and opportunities for targeted therapies, with immunotherapy emerging as a particularly promising approach. However, while the scientific frontier appears expansive, our exploration of clinical trial methodologies elucidates numerous hurdles that need overcoming—these range from statistical challenges posed by small sample sizes to the ethical implications of placebo-controlled trials in a disease as debilitating as FOP.
This article serves not just as a summary of current research but as an urgent call to action. It underscores the need for methodological innovation in trial design and the adoption of advanced statistical approaches that can accommodate the unique constraints of ultra-rare disease research. By intertwining rigorous scientific scrutiny with ethical considerations, we can hopefully move closer to therapies that not only alleviate symptoms but genuinely improve the lives of FOP patients.
It is imperative to maintain an unwavering commitment to ethical clinical research practices, balancing both the exigencies of patient welfare and scientific rigor. In the endeavor to transform the lives of individuals affected by FOP, this manuscript aims to catalyze a concerted effort among clinicians, researchers, and bioethicists to navigate the challenges ahead. The road to efficacious FOP treatment is steep and fraught with obstacles, but it is a path that tests the resilience, innovation, and adaptability of the scientific community at large. We conclude that FOP serves as both a crucible and a beacon, guiding the evolution of research methodologies and ethical frameworks for ultra-rare diseases. The pursuit of a cure for FOP, thus, holds the potential to revolutionize not just the field of rare disease research but the broader landscape of medical science.
Author Contributions
Conception and design, S.A. and T.Y.; Literature review and writing—original draft preparation, S.A.; writing—review and editing, S.A. and T.Y.; supervision and funding acquisition, T.Y. All authors have read and agree to the published version of the manuscript.
Funding
T.Y. is supported by the Muscular Dystrophy Canada, the Friends of Garrett Cumming Research Fund, the HM Toupin Neurological Science Research Fund, Canadian Institutes of Health Research (CIHR), Alberta Innovates: Health Solutions (AIHS), Jesse’s Journey, and the Women and Children’s Health Research Institute (WCHRI). S.A. is supported by scholarships from the Maternal and Child Health (MatCH) Program, the Alberta Innovates Graduate Student Scholarship (AIGSS), the Women and Children’s Health Research Institute (WCHRI), and the Andrew Stewart Memorial Graduate Prizes.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to acknowledge Jarin Taslem Mourosi (Bacteriophage Medical Research Centre, the Catholic University of America, Washington, D.C.) for assisting in preparing the figure created using the BioRender.com web platform.
Conflicts of Interest
T.Y. is a co-founder and shareholder of OligomicsTx Inc., which aims to commercialize antisense technology. S.A. declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Kaplan, F.S.; Glaser, D.L.; Shore, E.M.; Deirmengian, G.K.; Gupta, R.; Delai, P.; Morhart, R.; Smith, R.; Le Merrer, M.; Rogers, J.G.; et al. The Phenotype of Fibrodysplasia Ossificans Progressiva. Clin. Rev. Bone Miner. Metab. 2005, 3, 183–188. [Google Scholar] [CrossRef]
- Kaplan, F.S.; Chakkalakal, S.A.; Shore, E.M. Fibrodysplasia Ossificans Progressiva: Mechanisms and Models of Skeletal Metamorphosis. Dis. Model. Mech. 2012, 5, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, F.S.; Shen, Q.; Lounev, V.; Seemann, P.; Groppe, J.; Katagiri, T.; Pignolo, R.J.; Shore, E.M. Skeletal Metamorphosis in Fibrodysplasia Ossificans Progressiva (FOP). J. Bone Miner. Metab. 2008, 26, 521–530. [Google Scholar] [CrossRef]
- Pignolo, R.J.; Shore, E.M.; Kaplan, F.S. Fibrodysplasia Ossificans Progressiva: Clinical and Genetic Aspects. Orphanet J. Rare Dis. 2011, 6, 80. [Google Scholar] [CrossRef]
- Baujat, G.; Choquet, R.; Bouée, S.; Jeanbat, V.; Courouve, L.; Ruel, A.; Michot, C.; Le Quan Sang, K.H.; Lapidus, D.; Messiaen, C.; et al. Prevalence of Fibrodysplasia Ossificans Progressiva (FOP) in France: An Estimate Based on a Record Linkage of Two National Databases. Orphanet J. Rare Dis. 2017, 12. [Google Scholar] [CrossRef]
- Shore, E.M.; Xu, M.; Feldman, G.J.; Fenstermacher, D.A.; Cho, T.-J.; Choi, I.H.; Connor, J.M.; Delai, P.; Glaser, D.L.; LeMerrer, M.; et al. A Recurrent Mutation in the BMP Type I Receptor ACVR1 Causes Inherited and Sporadic Fibrodysplasia Ossificans Progressiva. Nat. Genet. 2006, 38, 525–527. [Google Scholar] [CrossRef] [PubMed]
- Shafritz, A.B.; Shore, E.M.; Gannon, F.H.; Zasloff, M.A.; Taub, R.; Muenke, M.; Kaplan, F.S. Overexpression of an Osteogenic Morphogen in Fibrodysplasia Ossificans Progressiva. N. Engl. J. Med. 1996, 335, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.; Serrano De La Peña, L.; Shore, E.M.; Kaplan, F.S. Paresis of a Bone Morphogenetic Protein-Antagonist Response in a Genetic Disorder of Heterotopic Skeletogenesis. J. Bone Jt. Surg. 2003, 85, 667–674. [Google Scholar] [CrossRef]
- Serrano De La Peña, L.; Billings, P.C.; Fiori, J.L.; Ahn, J.; Kaplan, F.S.; Shore, E.M. Fibrodysplasia Ossificans Progressiva (FOP), a Disorder of Ectopic Osteogenesis, Misregulates Cell Surface Expression and Trafficking of BMPRIA. J. Bone Miner. Res. 2005, 20, 1168–1176. [Google Scholar] [CrossRef]
- Fiori, J.L.; Billings, P.C.; Serrano De La Peña, L.; Kaplan, F.S.; Shore, E.M. Dysregulation of the BMP-P38 MAPK Signaling Pathway in Cells from Patients with Fibrodysplasia Ossificans Progressiva (FOP). J. Bone Miner. Res. 2006, 21, 902–909. [Google Scholar] [CrossRef]
- Billings, P.C.; Fiori, J.L.; Bentwood, J.L.; O’Connell, M.P.; Jiao, X.; Nussbaum, B.; Caron, R.J.; Shore, E.M.; Kaplan, F.S. Dysregulated BMP Signaling and Enhanced Osteogenic Differentiation of Connective Tissue Progenitor Cells from Patients with Fibrodysplasia Ossificans Progressiva (FOP). J. Bone Miner. Res. 2008, 23, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Shore, E.M.; Kaplan, F.S. BMP Signaling in Fibrodysplasia Ossificans Progressiva, a Rare Genetic Disorder of Heterotopic Ossification. In Bone Morphogenetic Proteins: Systems Biology Regulators; Springer International Publishing: Cham, 2017; pp. 327–343. [Google Scholar] [CrossRef]
- Kaplan, F.S.; Xu, M.; Seemann, P.; Connor, J.M.; Glaser, D.L.; Carroll, L.; Delai, P.; Fastnacht-Urban, E.; Forman, S.J.; Gillessen-Kaesbach, G.; et al. Classic and Atypical Fibrodysplasia Ossificans Progressiva (FOP) Phenotypes Are Caused by Mutations in the Bone Morphogenetic Protein (BMP) Type I Receptor ACVR1. Hum. Mutat. 2009, 30, 379–390. [Google Scholar] [CrossRef] [PubMed]
- Connor, J.; Evans, D. Fibrodysplasia Ossificans Progressiva. The Clinical Features and Natural History of 34 Patients. J. Bone Joint Surg. Br. 1982, 64-B, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Hahn, G.; Tabas, J.; Peeper, J.; Levitz, C.; Sando, A.; Sando, N.; Zasloff, M.; Kaplan, F. The Natural History of Heterotopic Ossification in Patients Who Have Fibrodysplasia Ossificans Progressiva. J Bone Jt. Surg Am. 1993, 75, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, F.S.; Le Merrer, M.; Glaser, D.L.; Pignolo, R.J.; Goldsby, R.E.; Kitterman, J.A.; Groppe, J.; Shore, E.M. Fibrodysplasia Ossificans Progressiva. Best Pract. Res. Clin. Rheumatol. 2008, 22, 191–205. [Google Scholar] [CrossRef]
- Rocke, D.M.; Zasloff, M.; Peeper, J.; Cohen, R.B.; Kaplan, F.S. Age- and Joint-Specific Risk of Initial Heterotopic Ossification in Patients Who Have Fibrodysplasia Ossificans Progressiva. Clin. Orthop. Relat. Res. 1994, 301, 243–248. [Google Scholar] [CrossRef]
- Petrie, K.A.; Lee, W.H.; Bullock, A.N.; Pointon, J.J.; Smith, R.; Russell, R.G.G.; Brown, M.A.; Wordsworth, B.P.; Triffitt, J.T. Novel Mutations in ACVR1 Result in Atypical Features in Two Fibrodysplasia Ossificans Progressiva Patients. PLoS One 2009, 4. [Google Scholar] [CrossRef]
- Shah, Z.A.; Rausch, S.; Arif, U.; El Yafawi, B. Fibrodysplasia Ossificans Progressiva (Stone Man Syndrome): A Case Report. J. Med. Case Rep. 2019, 13, 364. [Google Scholar] [CrossRef]
- Verma, A.K.; Aga, P.; Singh, S.K.; Singh, R. The Stone Man Disease: Fibrodysplasia Ossificans Progressiva: Imaging Revisited. Case Reports 2012, 2012, bcr2012006422–bcr2012006422. [Google Scholar] [CrossRef]
- Lin, S.; Svoboda, K.K.H.; Feng, J.Q.; Jiang, X. The Biological Function of Type I Receptors of Bone Morphogenetic Protein in Bone. Bone Res. 2016, 4, 16005. [Google Scholar] [CrossRef]
- Rauner, M.; Seefried, L.; Shore, E. Genetics and Future Therapy Prospects of Fibrodysplasia Ossificans Progressiva. Medizinische Genet. 2020, 31, 391–396. [Google Scholar] [CrossRef]
- Shaikh, U.; Khan, A.; Kumari, P.; Ishfaq, A.; Ekhator, C.; Yousuf, P.; Halappa Nagaraj, R.; Raza, H.; Ur Rehman, U.; Zaman, M.U.; et al. Novel Therapeutic Targets for Fibrodysplasia Ossificans Progressiva: Emerging Strategies and Future Directions. Cureus 2023. [Google Scholar] [CrossRef]
- Kitoh, H. Clinical Aspects and Current Therapeutic Approaches for FOP. Biomedicines 2020, 8. [Google Scholar] [CrossRef]
- Wentworth, K.L.; Masharani, U.; Hsiao, E.C. Therapeutic Advances for Blocking Heterotopic Ossification in Fibrodysplasia Ossificans Progressiva. Br. J. Clin. Pharmacol. 2019, 85, 1180–1187. [Google Scholar] [CrossRef]
- Goldman, A.B. Heritable Diseases of Connective Tissue, Epiphyseal Dysplasias, and Related Conditions. In Diagnosis of bone and joint disorders; D Resnick, Ed.; Saunders: Philadelphia, 2002; pp. 4409–4415. [Google Scholar]
- Araújo Júnior, C.R. de; Carvalho, T.N.; Costa, M.A.B.; Lobo, L.V.; Fonseca, C.R.; Teixeira, K.-I.-S.S. Fibrodisplasia Ossificante Progressiva: Relato de Caso e Achados Radiográficos. Radiol. Bras. 2005, 38, 69–73. [Google Scholar] [CrossRef]
- Antol, R. The Differential, Phoenix November 2015.
- Qi, Z.; Luan, J.; Zhou, X.; Cui, Y.; Han, J. Fibrodysplasia Ossificans Progressiva: Basic Understanding and Experimental Models. Intractable Rare Dis. Res. 2017, 6, 242–248. [Google Scholar] [CrossRef]
- Pignolo, R.J.; Bedford-Gay, C.; Liljesthröm, M.; Durbin-Johnson, B.P.; Shore, E.M.; Rocke, D.M.; Kaplan, F.S. The Natural History of Flare-Ups in Fibrodysplasia Ossificans Progressiva (FOP): A Comprehensive Global Assessment. J. Bone Miner. Res. 2016, 31, 650–656. [Google Scholar] [CrossRef]
- Zhang, W.; Zhang, K.; Song, L.; Pang, J.; Ma, H.; Shore, E.M.; Kaplan, F.S.; Wang, P. The Phenotype and Genotype of Fibrodysplasia Ossificans Progressiva in China: A Report of 72 Cases. Bone 2013, 57, 386–391. [Google Scholar] [CrossRef]
- Liljesthröm, M.; Pignolo, R.; Kaplan, F. Epidemiology of the Global Fibrodysplasia Ossificans Progressiva (FOP) Community. J. Rare Dis. Res. Treat. 2020, 5, 31–36. [Google Scholar] [CrossRef]
- Morales-Piga, A.; Bachiller-Corral, J.; Trujillo-Tiebas, M.J.; Villaverde-Hueso, A.; Gamir-Gamir, M.L.; Alonso-Ferreira, V.; Vázquez-Díaz, M.; Posada de la Paz, M.; Ayuso-García, C. Fibrodysplasia Ossificans Progressiva in Spain: Epidemiological, Clinical, and Genetic Aspects. Bone 2012, 51, 748–755. [Google Scholar] [CrossRef]
- Kaplan, F.S.; Zasloff, M.A.; Kitterman, J.A.; Shore, E.M.; Hong, C.C.; Rocke, D.M. Early Mortality and Cardiorespiratory Failure in Patients with Fibrodysplasia Ossificans Progressiva. J. Bone Jt. Surgery-American Vol. 2010, 92, 686–691. [Google Scholar] [CrossRef]
- Kitterman, J. A.; Kantanie, S.; Rocke, D. M.; Kaplan, F. S. Iatrogenic Harm Caused by Diagnostic Errors in Fibrodysplasia Ossificans Progressiva. Pediatrics 2005, 116, e654–e661. [Google Scholar] [CrossRef] [PubMed]
- de Ruiter, R.D.; Smilde, B.J.; Pals, G.; Bravenboer, N.; Knaus, P.; Schoenmaker, T.; Botman, E.; Sánchez-Duffhues, G.; Pacifici, M.; Pignolo, R.J.; et al. Fibrodysplasia Ossificans Progressiva: What Have We Achieved and Where Are We Now? Follow-up to the 2015 Lorentz Workshop. Front. Endocrinol. (Lausanne). 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Miao, J.; Zhang, C.; Wu, S.; Peng, Z.; Tania, M. Genetic Abnormalities in Fibrodysplasia Ossificans Progressiva. Genes Genet. Syst. 2012, 87, 213–219. [Google Scholar] [CrossRef]
- Whyte, M.P.; Wenkert, D.; Demertzis, J.L.; Dicarlo, E.F.; Westenberg, E.; Mumm, S. Fibrodysplasia Ossificans Progressiva: Middle-Age Onset of Heterotopic Ossification from a Unique Missense Mutation (c.974G > C, p.G325A) in ACVR1. J. Bone Miner. Res. 2012, 27, 729–737. [Google Scholar] [CrossRef]
- Ratbi, I.; Borcciadi, R.; Regragui, A.; Ravazzolo, R.; Sefiani, A. Rarely Occurring Mutation of ACVR1 Gene in Moroccan Patient with Fibrodysplasia Ossificans Progressiva. Clin. Rheumatol. 2010, 29, 119–121. [Google Scholar] [CrossRef]
- Furuya, H.; Ikezoe, K.; Wang, L.; Ohyagi, Y.; Motomura, K.; Fujii, N.; Kira, J.I.; Fukumaki, Y. A Unique Case of Fihrodysplasia Ossificans Progressiva with an ACVR1 Mutation, G356D, Other than the Common Mutation (R206H). Am. J. Med. Genet. Part A 2008, 146, 459–463. [Google Scholar] [CrossRef]
- Bocciardi, R.; Bordo, D.; Di Duca, M.; Di Rocco, M.; Ravazzolo, R. Mutational Analysis of the ACVR1 Gene in Italian Patients Affected with Fibrodysplasia Ossificans Progressiva: Confirmations and Advancements. Eur. J. Hum. Genet. 2009, 17, 311–318. [Google Scholar] [CrossRef]
- Connor, J.M.; Skirton, H.; Lunt, P.W. A Three Generation Family with Fibrodysplasia Ossificans Progressiva. J. Med. Genet. 1993, 30, 687–689. [Google Scholar] [CrossRef]
- Shore, E.M.; Xu, M.; Feldman, G.J.; Fenstermacher, D.A.; Brown, M.A.; Kaplan, F.S. A Recurrent Mutation in the BMP Type I Receptor ACVR1 Causes Inherited and Sporadic Fibrodysplasia Ossificans Progressiva. Nat. Genet. 2006, 38, 525–527. [Google Scholar] [CrossRef]
- Agarwal, S.; Loder, S.J.; Brownley, C.; Eboda, O.; Peterson, J.R.; Hayano, S.; Wu, B.; Zhao, B.; Kaartinen, V.; Wong, V.C.; et al. BMP Signaling Mediated by Constitutively Active Activin Type 1 Receptor (ACVR1) Results in Ectopic Bone Formation Localized to Distal Extremity Joints. Dev. Biol. 2015, 400, 202–209. [Google Scholar] [CrossRef]
- Tuffery-Giraud, S.; Béroud, C.; Leturcq, F.; Yaou, R. Ben; Hamroun, D.; Michel-Calemard, L.; Moizard, M.P.; Bernard, R.; Cossée, M.; Boisseau, P.; et al. Genotype-Phenotype Analysis in 2,405 Patients with a Dystrophinopathy Using the UMD-DMD Database: A Model of Nationwide Knowledgebase. Hum. Mutat. 2009, 30, 934–945. [Google Scholar] [CrossRef]
- Groppe, J.C.; Shore, E.M.; Kaplan, F.S. Functional Modeling of the ACVR1 (R206H) Mutation in FOP. Clin. Orthop. Relat. Res. 2007, 462, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Shen, Q.; Little, S.C.; Xu, M.; Haupt, J.; Ast, C.; Katagiri, T.; Mundlos, S.; Seemann, P.; Kaplan, F.S.; Mullins, M.C.; et al. The Fibrodysplasia Ossificans Progressiva R206H ACVR1 Mutation Activates BMP-Independent Chondrogenesis and Zebrafish Embryo Ventralization. J. Clin. Invest. 2009, 119, 3462–3471. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, T.; Kohda, M.; Kanomata, K.; Nojima, J.; Nakamura, A.; Kamizono, J.; Noguchi, Y.; Iwakiri, K.; Kondo, T.; Kurose, J.; et al. Constitutively Activated ALK2 and Increased SMAD1/5 Cooperatively Induce Bone Morphogenetic Protein Signaling in Fibrodysplasia Ossificans Progressiva. J. Biol. Chem. 2009, 284, 7149–7156. [Google Scholar] [CrossRef] [PubMed]
- Van Dinther, M.; Visser, N.; De Gorter, D.J.J.; Doorn, J.; Goumans, M.J.; De Boer, J.; Ten Dijke, P. ALK2 R206H Mutation Linked to Fibrodysplasia Ossificans Progressiva Confers Constitutive Activity to the BMP Type I Receptor and Sensitizes Mesenchymal Cells to BMP-Induced Osteoblast Differentiation and Bone Formation. J. Bone Miner. Res. 2010, 25, 1208–1215. [Google Scholar] [CrossRef]
- Song, G.A.; Kim, H.J.; Woo, K.M.; Baek, J.H.; Kim, G.S.; Choi, J.Y.; Ryoo, H.M. Molecular Consequences of the ACVR1R206H Mutation of Fibrodysplasia Ossificans Progressiva. J. Biol. Chem. 2010, 285, 22542–22553. [Google Scholar] [CrossRef] [PubMed]
- Kaliya-Perumal, A.-K.; Carney, T.J.; Ingham, P.W. Fibrodysplasia Ossificans Progressiva: Current Concepts from Bench to Bedside. Dis. Model. Mech. 2020, 13. [Google Scholar] [CrossRef]
- Kaplan, F.S.; Chakkalakal, S.A.; Shore, E.M. Fibrodysplasia Ossificans Progressiva: Mechanisms and Models of Skeletal Metamorphosis. DMM Dis. Model. Mech. 2012, 5, 756–762. [Google Scholar] [CrossRef]
- Barruet, E.; Morales, B.M.; Cain, C.J.; Ton, A.N.; Wentworth, K.L.; Chan, T.V.; Moody, T.A.; Haks, M.C.; Ottenhoff, T.H.M.; Hellman, J.; et al. NF-ΚB/MAPK Activation Underlies ACVR1-Mediated Inflammation in Human Heterotopic Ossification. JCI Insight 2018, 3. [Google Scholar] [CrossRef]
- Hatsell, S.J.; Idone, V.; Wolken, D.M.A.; Huang, L.; Kim, H.J.; Wang, L.; Wen, X.; Nannuru, K.C.; Jimenez, J.; Xie, L.; et al. ACVR1 R206H Receptor Mutation Causes Fibrodysplasia Ossificans Progressiva by Imparting Responsiveness to Activin A. Sci. Transl. Med. 2015, 7. [Google Scholar] [CrossRef] [PubMed]
- Hino, K.; Ikeya, M.; Horigome, K.; Matsumoto, Y.; Ebise, H.; Nishio, M.; Sekiguchi, K.; Shibata, M.; Nagata, S.; Matsuda, S.; et al. Neofunction of ACVR1 in Fibrodysplasia Ossificans Progressiva. Proc. Natl. Acad. Sci. 2015, 112, 15438–15443. [Google Scholar] [CrossRef] [PubMed]
- Lees-Shepard, J.B.; Yamamoto, M.; Biswas, A.A.; Stoessel, S.J.; Nicholas, S.-A.E.; Cogswell, C.A.; Devarakonda, P.M.; Schneider, M.J.; Cummins, S.M.; Legendre, N.P.; et al. Activin-Dependent Signaling in Fibro/Adipogenic Progenitors Causes Fibrodysplasia Ossificans Progressiva. Nat. Commun. 2018, 9, 471. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.-S.; Kim, J.-M.; Xie, J.; Chaugule, S.; Lin, C.; Ma, H.; Hsiao, E.; Hong, J.; Chun, H.; Shore, E.M.; et al. Suppression of Heterotopic Ossification in Fibrodysplasia Ossificans Progressiva Using AAV Gene Delivery. Nat. Commun. 2022, 13, 6175. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.-S.; Lin, C.; Ma, H.; Xie, J.; Kaplan, F.S.; Gao, G.; Shim, J.-H. AAV-Mediated Targeting of the Activin A-ACVR1R206H Signaling in Fibrodysplasia Ossificans Progressiva. Biomolecules 2023, 13, 1364. [Google Scholar] [CrossRef]
- Maruyama, R.; Nguyen, Q.; Roshmi, R.R.; Touznik, A.; Yokota, T. Allele-Selective LNA Gapmers for the Treatment of Fibrodysplasia Ossificans Progressiva Knock Down the Pathogenic ACVR1 R206H Transcript and Inhibit Osteogenic Differentiation. Nucleic Acid Ther. 2022, 32, 185–193. [Google Scholar] [CrossRef]
- Takahashi, M.; Katagiri, T.; Furuya, H.; Hohjoh, H. Disease-Causing Allele-Specific Silencing against the ALK2 Mutants, R206H and G356D, in Fibrodysplasia Ossificans Progressiva. Gene Ther. 2012, 19, 781–785. [Google Scholar] [CrossRef]
- Kaplan, J.; Kaplan, F.S.; Shore, E.M. Restoration of Normal BMP Signaling Levels and Osteogenic Differentiation in FOP Mesenchymal Progenitor Cells by Mutant Allele-Specific Targeting. Gene Ther. 2012, 19, 786–790. [Google Scholar] [CrossRef]
- De Brasi, D.; Orlando, F.; Gaeta, V.; De Liso, M.; Acquaviva, F.; Martemucci, L.; Mastrominico, A.; Di Rocco, M. Fibrodysplasia Ossificans Progressiva: A Challenging Diagnosis. Genes (Basel). 2021, 12, 1187. [Google Scholar] [CrossRef]
- Kaplan, F.S.; Xu, M.; Glaser, D.L.; Collins, F.; Connor, M.; Kitterman, J.; Sillence, D.; Zackai, E.; Ravitsky, V.; Zasloff, M.; et al. Early Diagnosis of Fibrodysplasia Ossificans Progressiva. Pediatrics 2008, 121. [Google Scholar] [CrossRef]
- Maftei, C.; Rypens, F.; Thiffault, I.; Dubé, J.; Laberge, A.-M.; Lemyre, E. Fibrodysplasia Ossificans Progressiva: Bilateral Hallux Valgus on Ultrasound a Clue for the First Prenatal Diagnosis for This Condition-Clinical Report and Review of the Literature. Prenat. Diagn. 2015, 35, 305–307. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, F.S.; Xu, M.; Seemann, P.; Connor, J.M.; Glaser, D.L.; Carroll, L.; Delai, P.; Fastnacht-Urban, E.; Forman, S.J.; Gillessen-Kaesbach, G.; et al. Classic and Atypical Fibrodysplasia Ossificans Progressiva (FOP) Phenotypes Are Caused by Mutations in the Bone Morphogenetic Protein (BMP) Type I Receptor ACVR1. Hum. Mutat. 2009, 30, 379–390. [Google Scholar] [CrossRef] [PubMed]
- Schaffer, A.A.; Kaplan, F.S.; Tracy, M.R.; O’Brien, M.L.; Dormans, J.P.; Shore, E.M.; Harland, R.M.; Kusumi, K. Developmental Anomalies of the Cervical Spine in Patients with Fibrodysplasia Ossificans Progressiva Are Distinctly Different from Those in Patients with Klippel-Feil Syndrome: Clues from the BMP Signaling Pathway. Spine (Phila. Pa. 1976). 2005, 30, 1379–1385. [Google Scholar] [CrossRef] [PubMed]
- Pignolo, R.J.; Shore, E.M.; Kaplan, F.S. Fibrodysplasia Ossificans Progressiva: Clinical and Genetic Aspects. Orphanet J. Rare Dis. 2011, 6. [Google Scholar] [CrossRef] [PubMed]
- Schäper, C.; Noga, O.; Koch, B.; Ewert, R.; Felix, S.B.; Gläser, S.; Kunkel, G.; Gustavus, B. Anti-Inflammatory Properties of Montelukast, a Leukotriene Receptor Antagonist in Patients with Asthma and Nasal Polyposis. J. Investig. Allergol. Clin. Immunol. 2011, 21, 51–58. [Google Scholar]
- Convente, M.R.; Chakkalakal, S.A.; Yang, E.J.; Caron, R.J.; Zhang, D.; Kambayashi, T.; Kaplan, F.S.; Shore, E.M. Depletion of Mast Cells and Macrophages Impairs Heterotopic Ossification in an Acvr1R206H Mouse Model of Fibrodysplasia Ossificans Progressiva. J. Bone Miner. Res. 2018, 33, 269–282. [Google Scholar] [CrossRef]
- Werner, C.M.L.; Zimmermann, S.M.; Würgler-Hauri, C.C.; Lane, J.M.; Wanner, G.A.; Simmen, H.P. Use of Imatinib in the Prevention of Heterotopic Ossification. HSS J. 2013, 9, 166–170. [Google Scholar] [CrossRef]
- Brantus, J.F.; Meunier, P.J. Effects of Intravenous Etidronate and Oral Corticosteroids in Fibrodysplasia Ossificans Progressiva. Clin. Orthop. Relat. Res. 1998, 346, 117–120. [Google Scholar] [CrossRef]
- Pennanen, N.; Lapinjoki, S.; Urtti, A.; Mönkkönen, J. Effect of Liposomal and Free Bisphosphonates on the IL-1β, IL-6 and TNFα Secretion from RAW 264 Cells in Vitro. Pharm. Res. An Off. J. Am. Assoc. Pharm. Sci. 1995, 12, 916–922. [Google Scholar] [CrossRef]
- Pabst, A.M.; Ziebart, T.; Ackermann, M.; Konerding, M.A.; Walter, C. Bisphosphonates’ Antiangiogenic Potency in the Development of Bisphosphonate-Associated Osteonecrosis of the Jaws: Influence on Microvessel Sprouting in an in Vivo 3D Matrigel Assay. Clin. Oral Investig. 2014, 18, 1015–1022. [Google Scholar] [CrossRef]
- Wiklander, O.P.B.; Brennan, M.Á.; Lötvall, J.; Breakefield, X.O.; EL Andaloussi, S. Advances in Therapeutic Applications of Extracellular Vesicles. Sci. Transl. Med. 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, F.; Shore, E. The Medical Management of Fibrodysplasia Ossificans Progressiva: Current Treatment Considerations. Clin Proc intl clin … 2005, 1–100. [Google Scholar]
- Simmons, D.L.; Botting, R.M.; Hla, T. Cyclooxygenase Isozymes: The Biology of Prostaglandin Synthesis and Inhibition. Pharmacol. Rev. 2004, 56, 387–437. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Kingman, J.; Sundberg, J.P.; Levine, M.A.; Uitto, J. Dual Effects of Bisphosphonates on Ectopic Skin and Vascular Soft Tissue Mineralization versus Bone Microarchitecture in a Mouse Model of Generalized Arterial Calcification of Infancy. J. Invest. Dermatol. 2016, 136, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Shimono, K.; Tung, W.; Macolino, C.; Chi, A.H.-T.; Didizian, J.H.; Mundy, C.; Chandraratna, R.A.; Mishina, Y.; Enomoto-Iwamoto, M.; Pacifici, M.; et al. Potent Inhibition of Heterotopic Ossification by Nuclear Retinoic Acid Receptor-γ Agonists. Nat. Med. 2011, 17, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Chakkalakal, S.A.; Uchibe, K.; Convente, M.R.; Zhang, D.; Economides, A.N.; Kaplan, F.S.; Pacifici, M.; Iwamoto, M.; Shore, E.M. Palovarotene Inhibits Heterotopic Ossification and Maintains Limb Mobility and Growth in Mice With the Human ACVR1 R206H Fibrodysplasia Ossificans Progressiva (FOP) Mutation. J. Bone Miner. Res. 2016, 31, 1666–1675. [Google Scholar] [CrossRef] [PubMed]
- Hoy, S.M. Palovarotene: First Approval. Drugs 2022, 82, 711–716. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration (FDA) FDA Approves First Treatment for Fibrodysplasia Ossificans Progressiva. Available online: https://www.fda.gov/drugs/news-events-human-drugs/fda-approves-first-treatment-fibrodysplasia-ossificans-progressiva (accessed on 18 September 2023).
- Pignolo, R.J.; Hsiao, E.C.; Al Mukaddam, M.; Baujat, G.; Berglund, S.K.; Brown, M.A.; Cheung, A.M.; De Cunto, C.; Delai, P.; Haga, N.; et al. Reduction of New Heterotopic Ossification ( <scp>HO</Scp> ) in the <scp>Open-Label</Scp>, Phase 3 <scp>MOVE</Scp> Trial of Palovarotene for Fibrodysplasia Ossificans Progressiva ( <scp>FOP</Scp> ). J. Bone Miner. Res. 2023, 38, 381–394. [Google Scholar] [CrossRef]
- Pignolo, R.J.; Baujat, G.; Hsiao, E.C.; Keen, R.; Wilson, A.; Packman, J.; Strahs, A.L.; Grogan, D.R.; Kaplan, F.S. Palovarotene for Fibrodysplasia Ossificans Progressiva ( <scp>FOP</Scp> ): Results of a Randomized, Placebo-Controlled, Double-Blind Phase 2 Trial. J. Bone Miner. Res. 2022, 37, 1891–1902. [Google Scholar] [CrossRef]
- Eekhoff, E.M.W.; de Ruiter, R.D.; Smilde, B.J.; Schoenmaker, T.; de Vries, T.J.; Netelenbos, C.; Hsiao, E.C.; Scott, C.; Haga, N.; Grunwald, Z.; et al. Gene Therapy for Fibrodysplasia Ossificans Progressiva: Feasibility and Obstacles. Hum. Gene Ther. 2022, 33, 782–788. [Google Scholar] [CrossRef]
- Ventura, F.; Williams, E.; Ikeya, M.; Bullock, A.N.; ten Dijke, P.; Goumans, M.-J.; Sanchez-Duffhues, G. Challenges and Opportunities for Drug Repositioning in Fibrodysplasia Ossificans Progressiva. Biomedicines 2021, 9, 213. [Google Scholar] [CrossRef]
- Moineau, S.; Barrangou, R.; Boyaval, P.; Deveau, H.; Romero, D.A.; Horvath, P.; Richards, M.; Fremaux, C. CRISPR Provides Acquired Resistance Against Viruses in Prokaryotes. Science (80-. ). 2007, 315, 1709–1712. [Google Scholar] [CrossRef]
- Makarova, K.S.; Wolf, Y.I.; Iranzo, J.; Shmakov, S.A.; Alkhnbashi, O.S.; Brouns, S.J.J.; Charpentier, E.; Cheng, D.; Haft, D.H.; Horvath, P.; et al. Evolutionary Classification of CRISPR–Cas Systems: A Burst of Class 2 and Derived Variants. Nat. Rev. Microbiol. 2020, 18, 67–83. [Google Scholar] [CrossRef] [PubMed]
- Jia, C.; Huai, C.; Ding, J.; Hu, L.; Su, B.; Chen, H.; Lu, D. New Applications of CRISPR/Cas9 System on Mutant DNA Detection. Gene 2018, 641, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Kawamata, M.; Suzuki, H.I.; Kimura, R.; Suzuki, A. Optimization of Cas9 Activity through the Addition of Cytosine Extensions to Single-Guide RNAs. Nat. Biomed. Eng. 2023, 7, 672–691. [Google Scholar] [CrossRef]
- Mengstie, M.A.; Wondimu, B.Z. Mechanism and Applications of CRISPR/Cas-9-Mediated Genome Editing. Biol. Targets Ther. 2021, Volume 15, 353–361. [Google Scholar] [CrossRef]
- Lino, C.A.; Harper, J.C.; Carney, J.P.; Timlin, J.A. Delivering CRISPR: A Review of the Challenges and Approaches. Drug Deliv. 2018, 25, 1234–1257. [Google Scholar] [CrossRef]
- Anwar, S.; Mir, F.; Yokota, T. Enhancing the Effectiveness of Oligonucleotide Therapeutics Using Cell-Penetrating Peptide Conjugation, Chemical Modification, and Carrier-Based Delivery Strategies. Pharmaceutics 2023, 15, 1130. [Google Scholar] [CrossRef]
- Lowery, J.W.; Rosen, V. Silencing the FOP Gene. Gene Ther. 2012, 19, 701–702. [Google Scholar] [CrossRef]
- Li, C.; Samulski, R.J. Engineering Adeno-Associated Virus Vectors for Gene Therapy. Nat. Rev. Genet. 2020, 21, 255–272. [Google Scholar] [CrossRef]
- Cullis, P.R.; Hope, M.J. Lipid Nanoparticle Systems for Enabling Gene Therapies. Mol. Ther. 2017, 25. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Wang, H.; Hao, J. Recent Progress in Drug Development for Fibrodysplasia Ossificans Progressiva. Mol. Cell. Biochem. 2022, 477, 2327–2334. [Google Scholar] [CrossRef]
- Pang, J.; Zuo, Y.; Chen, Y.; Song, L.; Zhu, Q.; Yu, J.; Shan, C.; Cai, Z.; Hao, J.; Kaplan, F.S.; et al. ACVR1-Fc Suppresses BMP Signaling and Chondro-Osseous Differentiation in an in Vitro Model of Fibrodysplasia Ossificans Progressiva. Bone 2016, 92, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Aykul, S.; Huang, L.; Wang, L.; Das, N.M.; Reisman, S.; Ray, Y.; Zhang, Q.; Rothman, N.; Nannuru, K.C.; Kamat, V.; et al. Anti-ACVR1 Antibodies Exacerbate Heterotopic Ossification in Fibrodysplasia Ossificans Progressiva (FOP) by Activating FOP-Mutant ACVR1. J. Clin. Invest. 2022, 132. [Google Scholar] [CrossRef]
- Katagiri, T.; Tsukamoto, S.; Kuratani, M. Heterotopic Bone Induction via BMP Signaling: Potential Therapeutic Targets for Fibrodysplasia Ossificans Progressiva. Bone 2018, 109, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, R.; Matsushita, M.; Kitoh, H.; Masuda, A.; Ito, M.; Katagiri, T.; Kawai, T.; Ishiguro, N.; Ohno, K. Clinically Applicable Antianginal Agents Suppress Osteoblastic Transformation of Myogenic Cells and Heterotopic Ossifications in Mice. J. Bone Miner. Metab. 2013, 31, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Sanvitale, C.E.; Kerr, G.; Chaikuad, A.; Ramel, M.C.; Mohedas, A.H.; Reichert, S.; Wang, Y.; Triffitt, J.T.; Cuny, G.D.; Yu, P.B.; et al. A New Class of Small Molecule Inhibitor of BMP Signaling. PLoS One 2013, 8. [Google Scholar] [CrossRef]
- Cappato, S.; Giacopelli, F.; Ravazzolo, R.; Bocciardi, R. The Horizon of a Therapy for Rare Genetic Diseases: A “Druggable” Future for Fibrodysplasia Ossificans Progressiva. Int. J. Mol. Sci. 2018, 19. [Google Scholar] [CrossRef]
- Hino, K.; Horigome, K.; Nishio, M.; Komura, S.; Nagata, S.; Zhao, C.; Jin, Y.; Kawakami, K.; Yamada, Y.; Ohta, A.; et al. Activin-A Enhances MTOR Signaling to Promote Aberrant Chondrogenesis in Fibrodysplasia Ossificans Progressiva. J. Clin. Invest. 2017, 127, 3339–3352. [Google Scholar] [CrossRef]
- Valer, J.A.; Sánchez-de-Diego, C.; Gámez, B.; Mishina, Y.; Rosa, J.L.; Ventura, F. Inhibition of Phosphatidylinositol 3-kinase α ( <scp>PI</Scp> 3Kα) Prevents Heterotopic Ossification. EMBO Mol. Med. 2019, 11. [Google Scholar] [CrossRef]
- Vanhoutte, F.; Liang, S.; Ruddy, M.; Zhao, A.; Drewery, T.; Wang, Y.; DelGizzi, R.; Forleo-Neto, E.; Rajadhyaksha, M.; Herman, G.; et al. Pharmacokinetics and Pharmacodynamics of Garetosmab (Anti-Activin A): Results From a First-in-Human Phase 1 Study. J. Clin. Pharmacol. 2020, 60, 1424–1431. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Shore, E.M.; Pignolo, R.J.; Kaplan, F.S. Activin A Amplifies Dysregulated BMP Signaling and Induces Chondro-Osseous Differentiation of Primary Connective Tissue Progenitor Cells in Patients with Fibrodysplasia Ossificans Progressiva (FOP). Bone 2018, 109, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.-Z.; Lee, J.H. Mesenchymal Stem Cell Therapy for Bone Regeneration. Clin. Orthop. Surg. 2018, 10, 271. [Google Scholar] [CrossRef] [PubMed]
- Hamasaki, M.; Hashizume, Y.; Yamada, Y.; Katayama, T.; Hohjoh, H.; Fusaki, N.; Nakashima, Y.; Furuya, H.; Haga, N.; Takami, Y.; et al. Pathogenic Mutation of ALK2 Inhibits Induced Pluripotent Stem Cell Reprogramming and Maintenance: Mechanisms of Reprogramming and Strategy for Drug Identification. Stem Cells 2012, 30, 2437–2449. [Google Scholar] [CrossRef]
- Kim, B.Y.; Jeong, S.K.; Lee, S.Y.; Lee, S.M.; Gweon, E.J.; Ahn, H.; Kim, J.; Chung, S.K. Concurrent Progress of Reprogramming and Gene Correction to Overcome Therapeutic Limitation of Mutant ALK2-IPSC. Exp. Mol. Med. 2016, 48. [Google Scholar] [CrossRef]
- Brennan, T.A.; Lindborg, C.M.; Bergbauer, C.R.; Wang, H.; Kaplan, F.S.; Pignolo, R.J. Mast Cell Inhibition as a Therapeutic Approach in Fibrodysplasia Ossificans Progressiva (FOP). Bone 2018, 109, 259–266. [Google Scholar] [CrossRef]
- Nikishina, I.P.; Arsenyeva, S.V.; Matkava, V.G.; Arefieva, A.N.; Kaleda, M.I.; Smirnov, A.V.; Blank, L.M.; Kostik, M.M. Successful Experience of Tofacitinib Treatment in Patients with Fibrodysplasia Ossificans Progressiva. Pediatr. Rheumatol. 2023, 21, 92. [Google Scholar] [CrossRef]
- Huang, Y.; Wang, X.; Zhou, D.; Zhou, W.; Dai, F.; Lin, H. Macrophages in Heterotopic Ossification: From Mechanisms to Therapy. npj Regen. Med. 2021, 6, 70. [Google Scholar] [CrossRef]
- Kan, C.; Yang, J.; Na, D.; Xu, Y.; Yang, B.; Zhao, H.; Lu, H.; Li, Y.; Zhang, K.; McGuire, T.L.; et al. Inhibition of Immune Checkpoints Prevents Injury-Induced Heterotopic Ossification. Bone Res. 2019, 7, 33. [Google Scholar] [CrossRef]
- Dhir, N.; Jain, A.; Mahendru, D.; Prakash, A.; Medhi, B. Drug Repurposing and Orphan Disease Therapeutics. In Drug Repurposing - Hypothesis, Molecular Aspects and Therapeutic Applications; IntechOpen, 2020. [Google Scholar]
- Jourdan, J.-P.; Bureau, R.; Rochais, C.; Dallemagne, P. Drug Repositioning: A Brief Overview. J. Pharm. Pharmacol. 2020, 72, 1145–1151. [Google Scholar] [CrossRef]
- Williams, E.; Bagarova, J.; Kerr, G.; Xia, D.-D.; Place, E.S.; Dey, D.; Shen, Y.; Bocobo, G.A.; Mohedas, A.H.; Huang, X.; et al. Saracatinib Is an Efficacious Clinical Candidate for Fibrodysplasia Ossificans Progressiva. JCI Insight 2021, 6. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Gilbert, L.A.; Cimini, B.A.; Schnitzbauer, J.; Zhang, W.; Li, G.W.; Park, J.; Blackburn, E.H.; Weissman, J.S.; Qi, L.S.; et al. Dynamic Imaging of Genomic Loci in Living Human Cells by an Optimized CRISPR/Cas System. Cell 2013, 155, 1479–1491. [Google Scholar] [CrossRef] [PubMed]
- Pignolo, R.J.; Bedford-Gay, C.; Cali, A.; Davis, M.; Delai, P.L.R.; Gonzales, K.; Hixson, C.; Kent, A.; Newport, H.; Robert, M.; et al. Current Challenges and Opportunities in the Care of Patients with Fibrodysplasia Ossificans Progressiva (FOP): An International, Multi-Stakeholder Perspective. Orphanet J. Rare Dis. 2022, 17, 168. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, F.S.; Pignolo, R.J.; Shore, E.M. From Mysteries to Medicines: Drug Development for Fibrodysplasia Ossificans Progressiva. Expert Opin. Orphan Drugs 2013, 1, 637–649. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Overview of genetic approaches for treating FOP. Gene editing focuses on directly correcting the ACVR1/ALK2 gene mutations at the DNA level using gene editing tools like CRISPR-Cas9, while gene addition aims to introduce healthy copies of the ACVR1 gene into the cells. Gene silencing explores either the full inactivation of the ACVR1 gene or selective suppression of only the mutated allele. Gene replacement approach integrates gene addition and gene silencing techniques for a multi-faceted therapeutic solution.
Table 1.
Overview of genetic approaches for treating FOP. Gene editing focuses on directly correcting the ACVR1/ALK2 gene mutations at the DNA level using gene editing tools like CRISPR-Cas9, while gene addition aims to introduce healthy copies of the ACVR1 gene into the cells. Gene silencing explores either the full inactivation of the ACVR1 gene or selective suppression of only the mutated allele. Gene replacement approach integrates gene addition and gene silencing techniques for a multi-faceted therapeutic solution.
| Therapeutic Strategy | Objective | Molecular Target | Anticipated Outcome |
|---|---|---|---|
| Gene editing | Rectification of mutations in the ACVR1 Gene using strategies like CRISPR-Cas9 | DNA | Exclusive expression of the corrected ACVR1/ALK2 protein |
| Gene addition | Introduction of healthy, functional ACVR1 gene copies | DNA, mRNA | Competition between newly added functional ACVR1/ALK2 and existing mutant forms |
| Gene silencing | Full inactivation or allele-specific suppression of ACVR1 | mRNA | Full inactivation may lead to unintended physiological ramifications; allele-specific suppression selectively diminishes expression of the mutant ACVR1 gene |
| Gene replacement | Synchronizing gene addition and gene silencing | mRNA | Allele-specific suppression reduces mutant ACVR1 expression, while the addition of functional ACVR1 compensates for the deficiency in functional ACVR1/ALK2 |
Table 2.
Ongoing interventional clinical trials for FOP. A brief summary of ongoing interventional clinical trials focused on therapeutic interventions for FOP (as of 18 Sep, 2023).
Table 2.
Ongoing interventional clinical trials for FOP. A brief summary of ongoing interventional clinical trials focused on therapeutic interventions for FOP (as of 18 Sep, 2023).
| ClinicalTrials.gov Identifier | Study Title/Sponsoring Entity | Intervention | Participants | Primary outcome |
|---|---|---|---|---|
| NCT05394116 | OPTIMA: A study to assess safety, tolerability, and efficacy of garetosmab versus placebo administered intravenously (IV) in adult participants with Fibrodysplasia ossificans progressiva (FOP)/Regeneron Pharmaceuticals | Garetosmab | Adults, both sexes | Quantification of newly developed HO lesions via adjudicated CT scans; occurrence and gradation of special-interest treatment-emergent adverse events (AESIs) |
| NCT05039515 | FALKON: Study to assess the effectiveness and safety of 2 dosage regimens of oral fidrisertib (IPN60130) for the treatment of Fibrodysplasia ossificans progressiva (FOP)/Clementia Pharmaceuticals Inc. | Fidrisertib | Ages 5 and above, both sexes | Yearly alteration in HO volume, measured through low-dose WBCT (head excluded); incidence of Adverse Events/Serious Adverse Events (AEs/SAEs); baseline deviation in critical laboratory parameters (hematology, biochemistry, urinalysis); baseline changes in physical examinations; alterations in vital signs and ECG readings from baseline |
| NCT04307953 | STOPFOP: Saracatinib trial to prevent FOP/Amsterdam UMC | Saracatinib | Ages 18 to 65, both sexes | Objective variance in heterotopic bone volume, assessed via low-dose whole-body CT, across both study arms during initial 6-month RCT period |
| NCT05090891 | PROGRESS: To assess the efficacy, safety, and tolerability of INCB000928 in participants with Fibrodysplasia ossificans progressiva/Incyte Corporation | INCB000928 | Ages 12 to 99, both sexes | Comprehensive assessment of new HO volume |
| NCT05027802 | PIVOINE: A rollover study to further evaluate the safety and efficacy of palovarotene capsules in male and female participants aged ≥14 years with Fibrodysplasia ossificans progressiva (FOP) who have completed the relevant parent studies/Ipsen Biopharmaceuticles | Palovarotene | Ages 14 and above, both sexes | Incidence and categorical elucidation of all serious and non-serious treatment-emergent adverse events (TEAEs), irrespective of their causal relation to the study intervention |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



