
Submitted:
24 September 2023
Posted:
28 September 2023
You are already at the latest version
Abstract
Background and Objectives: Effective strategy to cardiopulmonary resuscitation should be based on tissue perfusion. Our primary aim was to determine the association between capillary lactate values and initial rhythm as well as probability of return of spontaneous circulation in out-of-hospital cardiac arrest patients. Materials and Methods: This prospective observational cohort study included all patients with non-traumatic out-of-hospital cardiac arrest, older than 18 years, resuscitated by a prehospital emergency medical team between April 2020 and June 2021. Capillary lactate samples were collected at the time of arrival and every 10 minutes after first measurement until the time of return of spontaneous circulation (ROSC) or if ROSC was not achieved at time of declaring death on scene. Results: 83 patients were enrolled in the study. ROSC was achieved in 28 patients (33,7%), 21 were admitted to the hospital (26,3%) and 6 (7,23%) of them were discharged from the hospital. At discharge all patients had Cerebral Performance Category Scale 1 or 2. Initial capillary lactate values were significantly higher in patients with non-shockable rhythm compared to the group with shockable rhythm (9,19 +/- 4,6 versus 6,43 +/- 3,81; p = 0.037). A significant difference persisted also in a second value taken 10 minutes after in-itial value (10,03 +/- 5,19 versus 5,18 +/- 3,47; p = 0.019). Capillary lactate values were higher in the ROSC group and non-ROSC group at the time of restored circulation (11,10 +/- 6,59 and 6,77 +/- 4,23, respectively; p = 0,047). Conclusions: Capillary lactate values are significantly lower in patients with a shockable first rhythm in OHCA. There is also a significant connection between a rise in capillary lactate level and ROSC.
Keywords:
cardiopulmonary resuscitation
; out-of-hospital cardiac arrest
; lactate
; return of spontaneous circulation
1. Introduction
Despite all the scientific research and technological advances sudden out-of-hospital cardiac arrest (OHCA) remains the leading cause of death in the world. [1,2,3] Most of them occur in the home environment. [2,3]
OHCA is a sudden malfunction of the cardiovascular system which leads to a sudden decrease in perfusion of tissues. [2] Causes of the cardiac arrest (CA) are primary or secondary. [2] Myocardial ischemia, cardiac channelopathies, myocardiopathies and other diseases cause primary cardiac arrest while secondary cardiac arrest is caused by non-cardiac causes like respiratory arrest, trauma, neurological etc. [2,4]
The underlining cause defines the pathophysiological course of cardiac arrest. [2,3,4] In primary cardiac arrest, blood circulation is usually promptly stopped and, in the beginning, presented with an initial shockable rhythm. [2,4] Ventricular tachycardia (VT) initially can produce a perfusing rhythm but left untreated progresses to a pulseless VT or into ventricular fibrillation (VF). [2] Secondary cardiac arrest is characterized by a longer course of time with worsening cardiopulmonary function, deepening of hypoxia and hypercapnia until the final cardiac arrest. [4]
Duration of reduced tissue oxygenation and tissue hypoperfusion defines the difference between primary and secondary cardiac arrest also on a cellular level. [4,5] Longer lasting tissue hypoperfusion due to a disease causes lactic acidosis [4,6] which leads compensatory tachypnea and respiratory alkalosis. [7,8,9] If homeostasis is not achieved deepening of metabolic acidosis leads to respiratory failure which results in secondary CA presented initial non-shockable rhythm, higher levels of EtCO2 (end tidal carbon dioxide) and lactate are expected. [4,8,10,11,12]
Some studies showed poor neurological outcome of patients after return of spontaneous circulation (ROSC) with high levels of lactate at hospital admission. [13,14,15] A clear association between lactate levels and prognosis of OHCA still remains to be proven. [16]
This study aimed to analyze dynamics of capillary lactate levels between patients with OHCA regarding initial shockable and non-shockable rhythm during advanced CPR.
2. Materials and Methods
Emergency medical services (EMS)
In Slovenia, a two-tiered ambulance system, consisting of advanced and basic life support for emergency patient care is organized. First team includes two paramedics and an emergency physician and the second includes two paramedics. All of the units are trained in advanced life support. In cases where a severe medical condition or a cardiac arrest is suspected a unit including a physician is dispatched. EMS protocols are designed according to the Utstein style reporting for OHCA.
Study design
This prospective observational cohort study was conducted in Maribor, Slovenia and adjacent rural areas encompassing a population of about 200.000 inhabitants. Patients enrolled in the present study were all non-traumatic OHCA patients older than 18 years resuscitated by a prehospital emergency medical team. Resuscitation procedures were performed in accordance with 2015 and updated 2021 ERC guidelines by an emergency medical team.
Patients’ underage, pregnant, with traumatic CA, in whom CPR was not initiated or blood samples were not taken were excluded.
After arrival at the scene EMS advanced CPR was initiated and an initial capillary lactate sample was obtained as soon as possible (average time was 5,8 minutes after initiation of resuscitation). After that capillary lactate samples were taken every 10 minutes during advanced CPR until the time of ROSC or if ROSC was not achieved at time of declaring death on scene.
All samples were analyzed on the scene with a strip test and a point of care BM-Lactate Cobas (Roche Diagnostics GmbH) machine. Measuring range of the blood samples is between 0,8 and 22 mmmol/L. Outside this range the machine defines the measurement low or high. If the result was defined as low, we equaled it for statistical analysis with 0,8 mmol/L and if the result was defined as high, we equaled it with 23 mmol/L. For optimal performance we did a monthly quality control with the use of BM-Control-Lactate strips.
In our study capillary lactate values during advanced CPR between OHCA patients with initial shockable (VF, VT) and non-shockable rhythm (asystole, PEA) and among patients with ROSC and non-ROSC were compared. In addition, levels of EtCO2 between both previously mentioned groups were also compared.
Statistical analysis
Statistical analysis was undertaken with IBM SPSS software, version 26.0 for Windows (SPSS, Chicago, Illinois). Normality was evaluated with the Kolmogorov-Smirnov and the Shapiro-Wilk test. Two independent groups were compared by Independent Sample t-test and Leven’s Test for Equality of variables. Correlation was assessed with Pearson Correlation. Value of p < 0.05 was considered statistically significant.
National Medical Ethics Committee of the Republic of Slovenia approved the study and waived the requirement to any informed consent (No. 0120-229/2018/12).
The study has been registrated at Clinical Trials under the number NCT04571281.
3. Results
Between April 2020 and June 2021 resuscitation was attempted in 225 patients, 83 patients were enrolled in the study. The remaining 142 patients were excluded from the study if the EMS team achieved ROSC immediately after the first defibrillation if EMS team for various reasons failed to perform serial lactate measurements or the patient was declared dead on the arrival. The median age was 67 years. ROSC was achieved in 28 patients (33,7%), 21 were admitted to the hospital (26,3%) and 6 (7,23%) of them were discharged from the hospital. At discharge all patients had Cerebral Performance Category Scale (CPC) 1 or 2. Patient characteristics are presented in Figure 1.
Comparison of capillary lactate measurements among groups based on the first monitored rhythm showed that the initial values were significantly higher in patients with non-shockable rhythm compared to the group with shockable rhythm (9,19 ± 4,6 versus 6,43 ± 3,81; p = 0.037). A significant difference persisted also in a second value taken 10 minutes after initial value (10,03 ± 5,19 versus 5,18 ± 3,47; p = 0.019). The values of capillary lactate for both groups are presented in Table 1.
We also compared values of capillary lactate among ROSC and non-ROSC group where we found a significantly higher level of the 3rd value of capillary lactate in the ROSC group (11,10 ± 6,59 and 6,77 ± 4,23, respectively; p = 0,047). The values of capillary lactate for both groups are presented in Table 2. Average duration of advanced CPR before achieving ROSC was 16,35 ± 9,53 minutes while the average duration of advanced CPR before termination of CPR was 40,13 ± 15,76 minutes.
Average capillary lactate levels and EtCO2 were compared among patients with initial shockable and non-shockable rhythm (Figure 1). In the first ten minutes interval there was a slight drop in both values in patients with initial shockable rhythm. Levels of average EtCO2 in patients with initial non-shockable rhythm (asystole, PEA) increased slightly in the first 10 minutes and progressively decreased until the termination of advanced CPR.
Comparison of capillary lactate levels among ROSC and non-ROSC groups shows at first increasing levels with a peak at 20 minutes in the ROSC group (Figure 2). Non-ROSC group had the highest average level of lactate and the lowest average levels of EtCO2 at 40 minutes after starting advanced CPR. This is also an average point in time where the advanced CPR was terminated.
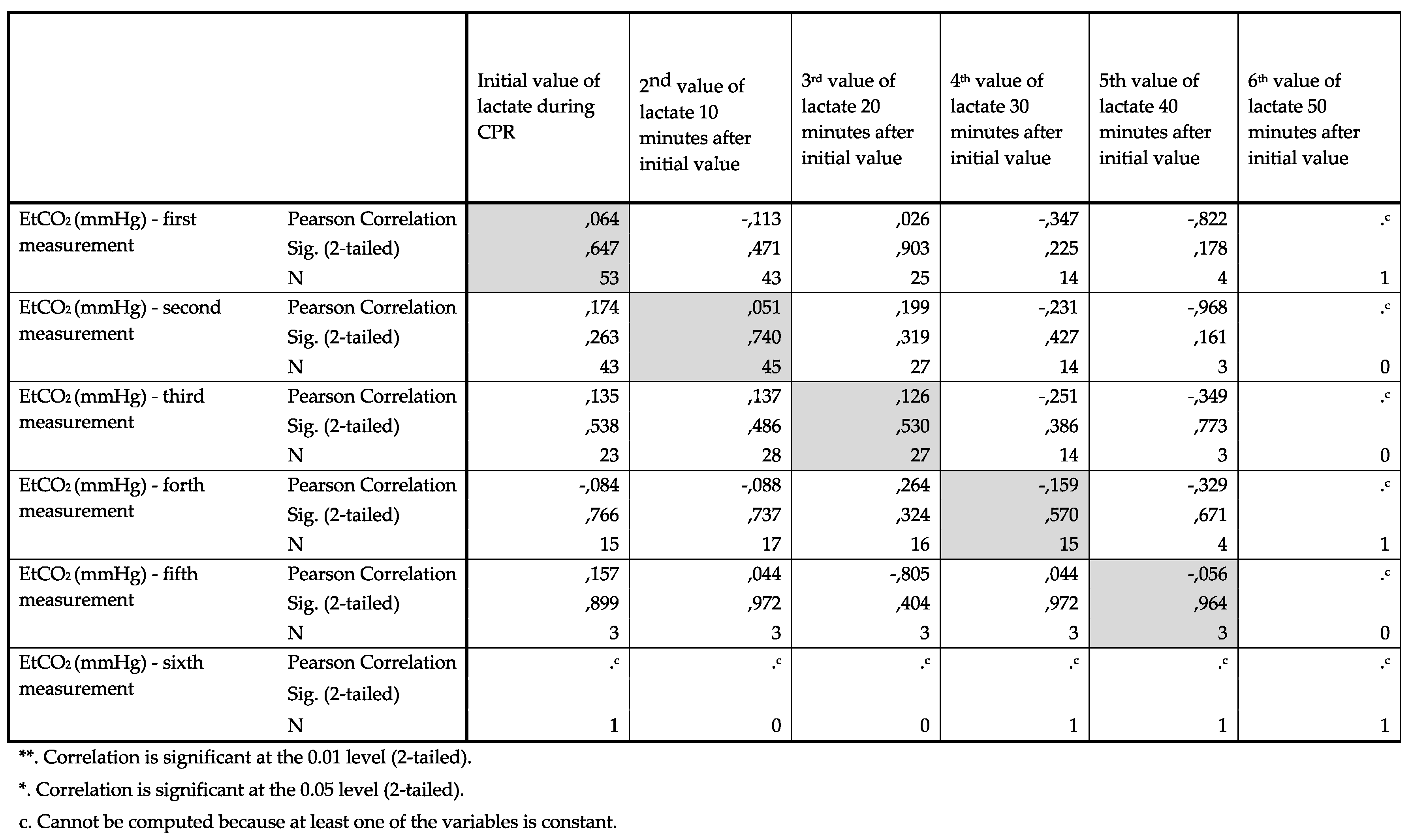
Average capillary lactate levels and EtCO2 among ROSC and non-ROSC group were analyzed and showed no correlation between EtCO2 and levels of lactate. (Appendix A)
4. Discussion
This study is to our knowledge first to report the dynamics of capillary lactate during advanced CPR in OHCA in the prehospital setting. Comparison of capillary lactate measurements among patients with OHCA showed significantly higher average initial values of capillary lactate in patients with non-shockable rhythm which persisted also in a second value taken 10 minutes after initial one. When comparing the ROSC and non-ROSC groups we found that third average capillary lactate measurement taken at 20 minutes after initial measurement was significantly higher in patients with ROSC. We found no correlation between EtCO2 and levels of capillary lactate among the same compared groups.
The role of lactate as a biomarker of mortality and predictability of ROSC has been discussed for decades now. [13,17,18,19,20] Stewart et al. published an article emphasizing the importance of correcting acidosis in the management of cardiac arrest. [21] Weil et al [20] wrote that anaerobic metabolism with lacticaemia provides quantitative measure for the extent to which the organism is deprived of oxygen and suggested that arterial lactate levels measured during the first 10 minutes of ongoing CPR and one hour after successful CPR correlate to survival. Their findings on lactate showed that arterial lactate lower than 4,5 mmol/L correlated with patient survival especially if the lactate was below that level one hour after successful CPR. [20] However if the initial arterial lactate was above 6,5 mmol/L only few patients survived. [20] There were no survivors if lactate exceeded 6,5 mmol/L after one hour. [20] Study by Wang at al [13] where the serum lactate was measured during first 10 minutes of advanced CPR in patients with in-hospital cardiac arrest (IHCA) showed a mean lactate level of 9,6 mmol/L. Their study positively associated shockable rhythm, lactate level <9 mmol/L with survival to hospital discharge. [13]
Results from our study also confirmed similar observations showing that patients with shockable first monitored rhythm had lower average initial lactate levels.
Other studies associated post-ROSC mean lactate levels in 24 hours [22] or effective lactate clearance with lower mortality [23]. Donnino at al [23] demonstrated that lactate clearance after ROSC was a better predictor of 24-h and overall, in-hospital survival. A study by Oddo et al [24] demonstrated that median initial lactate levels are lower in survivors while a study by Adrie et al [25] related initial lower lactate levels with good neurological outcome. Last two studies were done in the intensive care unit and reported median initial lactate value cut off point of 3,1 mmol/L for good neurological outcome by Adrie [25] which is much lower than median of 8,1 mmol/L reported by Oddo et al [24] who described blood lactate at addition as only other variable associated with survival beside time to ROSC and shockable rhythms.
Most of the studies done on the dynamics of lactate were done in the hospital environment after ROSC was achieved and sustained for a different time periods depending on the criteria of the study. [22,23,24,25,26,27,28,29] However a study by Miomiyama et al [16] included all OHCA admitted to the hospital and measured initial lactate and pH on the admission. They reported lower lactate levels in patients with favorable outcome (82 ± 49 vs 96 ± 41 mg/dL) but did not reach statistical significance. [16]
In our study average capillary lactate levels were analyzed mostly because it was easier to do repetitive measurements in prehospital settings while preforming CPR. The average initial capillary lactate taken on average 5,8 minutes after the arrival and was 6,43 ± 3,81mmol/L for patients with initial shockable rhythm and 9,19 ± 4,6 mmol/L for the patients with initial non-shockable rhythm.
Our findings are consistent with pathophysiological differences between primary and secondary CA. [4,5,6,30] Secondary CA is characterized by progressive and global hypoxia with incomplete ischemia. [4] Reduced whole body hypoxia and/or severe hypovolemia trigger anaerobic metabolism causing lactic acidosis and directly reflects cellular hypoxia. [6] Depletion of cellular energy results in CO2 tissue production, accumulation of CO2 in alveoli and initiates biochemical cascades that lead to cell damage and ultimately to cell death prior to cardiovascular arrest. [4,30]
Çalbay et al [31] analyzed initial blood gas samples from OHCA patients at admission to the emergency room (ER) and repeated measurements within 5 minutes after achieving ROSC and found no correlation between levels of lactate and ROSC. They reported that PCO2 was significant in ROSC estimation and could be used with EtCO2 to strengthen the estimation of ROSC. [31]
EtCO2 is used as a predictor of ROSC and as measurement to guide our management of cardiac arrest out of hospital. [11,32,33,34] Because of the known relationship between EtCO2 and lactate and its usefulness in predicting probability of ROSC and mortality. [4,7,8,9,11,12,32,33,34] We analyzed both values and found no correlation between EtCO2 and average levels of capillary lactate among same groups.
Our study found no significant difference among ROSC and non-ROSC groups of patients regarding initial capillary lactate level. A study done in pre-hospital settings by Tores et al [35] presented similar results as they also did not observe a significant statistical relationship between initial lactate and ROSC or neurological recovery but found association between base excess and outcome.
We did find a significantly higher 3rd (20 minutes after the initial capillary lactate level) average capillary lactate value in the ROSC group in comparison to non-ROSC (11,10 ± 6,59 versus 6,77 ± 4,23 mmol/L). The difference in average capillary lactate coincides with the average time of restored spontaneous circulation. When we add up average time for initial capillary lactate sample (5,8 minutes after initiation of resuscitation) and the predetermined time points we find that at the time of significantly higher 3rd average capillary lactate value coincides with ROSC (average time before achieving ROSC was 16,35 ± 9,53 minutes) for the ROSC group in comparison with non-ROSC group. These findings suggest highest average level of capillary lactate in ROSC group (Figure 2) can be associated to restored circulation.
Cardiac arrest represents the most severe shock state. [36] The degree of lactic acidosis correlates with the overall decrease in oxygen delivery, extent of tissue hypoperfusion, and severity of the disease process. [37] CRP provides an artificial state of perfusion until the physiological circulation is restored. [38] ROSC leads to improvement in tissue perfusion and clearance of lactate from tissues to blood.
In summary, this study suggests that initial capillary lactate levels and capillary lactate levels measured 10 minutes after during CRP could be associated with type of cardiac arrest. Lactate and EtCO2 values in concept with other variables could help clinicians define the cause of the cardiac arrest, the duration of resuscitation procedures, and the timing of termination of resuscitation. This however was not the aim of this study. We emphasize the value of multimodal approach in prehospital CPR decision-making.
Limitations
Study has several limitations. Study population is small and thus the conclusions need to be tested on larger studies. Another limitation is a lack of all measurements per case during advanced CPR. Thirdly, the interval of 10 minutes could have been shorter and thereby provided more information about the dynamics of lactate during advanced CPR. The COVID epidemics interrupted the conduction of the study.
5. Conclusions
Capillary lactate measurements among patients with OHCA showed significantly higher average initial values of capillary lactate in patients with non-shockable rhythm which persisted also in a second value taken 10 minutes after initial one. Findings also suggest that the highest average level of capillary lactate in ROSC group can be associated to restored circulation.
Author Contributions
V.V.: conceptualization, methodology, investigation, data curation, writing—original draft preparation, project administration, V.BL.: writing—review, editing and supervision, D.M.: validation, writing—review, editing and supervision. M.S.: conceptualization, methodology, validation, writing—review, editing and supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Republic of Slovenia (No. 0120-229/2018/12).
Informed Consent Statement
National Medical Ethics Committee of the Republic of Slovenia waived the requirement to any informed consent (No. 0120-229/2018/12).
Data Availability Statement
Study data that supports the findings of this study are available from the author upon the request.
Acknowledgments
Thank you to all members of Maribor emergency medical service for their productive work in collecting the data in these records on the scene.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
References
- Lurie, K.G.; Nemergut, E.C.; Yannopoulos, D.; Sweeney, M. The Physiology of Cardiopulmonary Resuscitation. Obstet. Anesthesia Dig. 2016, 122, 767–783. [Google Scholar] [CrossRef] [PubMed]
- Porzer M, Mrazkova E, Homza M, Janout V. Out-of-hospital cardiac arrest. 2017, 161, 348–353.
- Patil, K.D.; Halperin, H.R.; Becker, L.B.; J, C.; M, S.; T, Y.; G, N.; K, S.; J, S.; L, B.; et al. Cardiac Arrest. Circ. Res. 2015, 116, 2041–2049. [Google Scholar] [CrossRef]
- Varvarousis, D.; Varvarousi, G.; Iacovidou, N.; D'Aloja, E.; Gulati, A.; Xanthos, T. The pathophysiologies of asphyxial vs dysrhythmic cardiac arrest: implications for resuscitation and post-event management. Am. J. Emerg. Med. 2015, 33, 1297–1304. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.-S.; Huang, C.-H.; Tsai, S.-H.; Tsai, C.-Y.; Chen, H.-W.; Cheng, H.-J.; Hsu, C.-Y.; Wang, T.-D.; Chang, W.-T.; Chen, W.-J. The difference in myocardial injuries and mitochondrial damages between asphyxial and ventricular fibrillation cardiac arrests. Am. J. Emerg. Med. 2012, 30, 1540–1548. [Google Scholar] [CrossRef]
- Phypers, B.; Pierce, J.T. Lactate physiology in health and disease. Contin. Educ. Anaesth. Crit. Care Pain 2006, 6, 128–132. [Google Scholar] [CrossRef]
- Hunter, C.L.; Silvestri, S.; Dean, M.; Falk, J.L.; Papa, L. End-tidal carbon dioxide is associated with mortality and lactate in patients with suspected sepsis. Am. J. Emerg. Med. 2013, 31, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Caputo ND, Fraser RM, Paliga A, et al. Nasal cannula end-tidal CO2 correlates with serum lactate levels and odds of operative intervention in penetrating trauma patients: a prospective cohort study. J Trauma Acute Care Surg 2012, 73, 1202–1207. [CrossRef] [PubMed]
- McGillicuddy DC, Tang A, Caaldo L, et al. Evaluation of end-tidal carbon dioxide role in predicting elevated SOFA scores and lactic acidosis. Intern Emerg Med 2009, 4, 41–45. [CrossRef] [PubMed]
- Lah, K.; Vujanovic, V.; Krizmaric, M.; Grmec, S. Difference in end-tidal carbon dioxide between asphyxial cardiac arrest and ventricular fibrillation/pulseless ventricular tachycardia cardiac arrest in cardiopulmonary resuscitation—Comparison of 2000 and 2005 CPR guidelines. Resuscitation 2010, 81, S58–S58. [Google Scholar] [CrossRef]
- Grmec. ; Lah, K.; Tušek-Bunc, K. Difference in end-tidal CO2 between asphyxia cardiac arrest and ventricular fibrillation/pulseless ventricular tachycardia cardiac arrest in the prehospital setting. Crit. Care 2003, 7, R139–R144. [Google Scholar] [CrossRef]
- Hunter, C.L.; Silvestri, S.; Ralls, G.; Bright, S.; Papa, L. The sixth vital sign: prehospital end-tidal carbon dioxide predicts in-hospital mortality and metabolic disturbances. Am. J. Emerg. Med. 2014, 32, 160–165. [Google Scholar] [CrossRef]
- Wang, C.-H.; Huang, C.-H.; Chang, W.-T.; Tsai, M.-S.; Yu, P.-H.; Wu, Y.-W.; Hung, K.-Y.; Chen, W.-J. Monitoring of serum lactate level during cardiopulmonary resuscitation in adult in-hospital cardiac arrest. Crit. Care 2015, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Cocchi, M.N.; Miller, J.; Hunziker, S.; Carney, E.; Salciccioli, J.; Farris, S.; Joyce, N.; Zimetbaum, P.; Howell, M.D.; Donnino, M.W. The association of lactate and vasopressor need for mortality prediction in survivors of cardiac arrest. . 2011, 77. [Google Scholar]
- Starodub, R.; Abella, B.S.; Grossestreuer, A.V.; Shofer, F.S.; Perman, S.M.; Leary, M.; Gaieski, D.F. Association of serum lactate and survival outcomes in patients undergoing therapeutic hypothermia after cardiac arrest. Resuscitation 2013, 84, 1078–1082. [Google Scholar] [CrossRef] [PubMed]
- Momiyama, Y.; Yamada, W.; Miyata, K.; Miura, K.; Fukuda, T.; Fuse, J.; Kikuno, T. Prognostic values of blood pH and lactate levels in patients resuscitated from out-of-hospital cardiac arrest. Acute Med. Surg. 2016, 4, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Gernardin, G.; Pradier, C.; Tiger, F.; Deloffre, P.; Mattei, M. Blood pressure and arterial lactate level are early indicators of short-term survival in human septic shock. Intensiv. Care Med. 1996, 22, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Ralston, S.H.; Voorhees, W.D.; Showen, L.; Schmitz, P.; Kougias, C.; Tacker, W.A. Venous and arterial blood gases during and after cardiopulmonary resuscitation in dogs. Am. J. Emerg. Med. 1985, 3, 132–136. [Google Scholar] [CrossRef]
- Carden, D.L.; Martin, G.B.; Nowak, R.M.; Foreback, C.C.; Tomlanovich, M.C. Lactic acidosis during closed-chest CPR in dogs. Ann. Emerg. Med. 1987, 16, 1317–1320. [Google Scholar] [CrossRef]
- Weil, M.H.; Ruiz, C.E.; Michaels, S.B.; Rackow, E.C. Acid-base determinants of survival after cardiopulmonary resuscitation. Crit. Care Med. 1985, 13, 888–892. [Google Scholar] [CrossRef]
- Stewart JSS, Glasg MB,. Stewart WK, Gillies HG. Cardiac arrest and acidosis. The Lancet 1962, 280, 964–967.
- Starodub, R.; Abella, B.S.; Grossestreuer, A.V.; Shofer, F.S.; Perman, S.M.; Leary, M.; Gaieski, D.F. Association of serum lactate and survival outcomes in patients undergoing therapeutic hypothermia after cardiac arrest. Resuscitation 2013, 84, 1078–1082. [Google Scholar] [CrossRef] [PubMed]
- Donnino, M.W.; Miller, J.; Goyal, N.; Loomba, M.; Sankey, S.S.; Dolcourt, B.; Sherwin, R.; Otero, R.; Wira, C. Effective lactate clearance is associated with improved outcome in post-cardiac arrest patients. Resuscitation 2007, 75, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Oddo M, Ribordy V, Feihl F, Rossetti AO, Schaller MD, et al. Early predictors of outcome in comatose survivors of ventricular fibrillation and non-ventricular fibrillation cardiac arrest treated with hypothermia: a prospective study. Crit Care Med. 2008, 36, 2296–2301. [Google Scholar]
- Adrie C, Cariou A, Mourvillier B, Laurent I, Dabbane H, et al. Predicting survival with good neurological recovery at hospital admission after successful resuscitation of out-of-hospital cardiac arrest: the OHCA score. Eur Heart J. 2006, 27, 2840–2845. [Google Scholar] [CrossRef]
- Kliegel, A.; Losert, H.; Sterz, F.; Holzer, M.; Zeiner, A.; Havel, C.; Laggner, A.N. Serial Lactate Determinations for Prediction of Outcome After Cardiac Arrest. Medicine 2004, 83, 274–279. [Google Scholar] [CrossRef]
- Seeger, F.H.; Toenne, M.; Lehmann, R.; Ehrlich, J.R. Simplistic approach to prognosis after cardiopulmonary resuscitation—value of pH and lactate. J. Crit. Care 2013, 28, 317–e13. [Google Scholar] [CrossRef]
- Kaji, A.H.; Hanif, A.M.; Bosson, N.; Ostermayer, D.; Niemann, J.T. Predictors of Neurologic Outcome in Patients Resuscitated from Out-of-Hospital Cardiac Arrest Using Classification and Regression Tree Analysis. Am. J. Cardiol. 2014, 114, 1024–1028. [Google Scholar] [CrossRef]
- Lee, T.R.; Kang, M.J.; Cha, W.C.; Shin, T.G.; Sim, M.S.; Jo, I.J.; Song, K.J.; Jeong, Y.K.; Cho, J.H. Better lactate clearance associated with good neurologic outcome in survivors who treated with therapeutic hypothermia after out-of-hospital cardiac arrest. Crit. Care 2013, 17, R260–R260. [Google Scholar] [CrossRef]
- Wu, C.-J.; Li, C.-S.; Zhang, Y.; Yang, J.; Yin, Q.; Hang, C.-C. Differences of postresuscitation myocardial dysfunction in ventricular fibrillation versus asphyxiation. Am. J. Emerg. Med. 2013, 31, 1690–1696. [Google Scholar] [CrossRef]
- albay A, Çakir Z, Bayramoğlu A. Prognostic value of blood gas parameters and end-tidal carbon dioxide values in out-of-hospital cardiopulmonary arrest patients. Turkish J Med Sci. 2019, 49, 1298–1302. [Google Scholar] [CrossRef] [PubMed]
- Paiva EF, Paxton JH, O’Neil BJ. The use of end-tidal carbon dioxide (ETCO2) measurment to guide management of cardiac arrest: A systematic review. Resuscitation 2018, 123, 1–7. [Google Scholar]
- Asplin, B.R.; White, R.D. Prognostic Value Of End-Tidal Carbon Dioxide Pressures During Out-Of-Hospital Cardiac Arrest. Ann. Emerg. Med. 1995, 25, 756–761. [Google Scholar] [CrossRef] [PubMed]
- Grmec S, Klemen P. Does the end-tidal carbon dioxide (EtCO2) concentration have prognostic value during out-of-hospital cardiac arrest? Eur J Emerg Med 2001, 8, 263–269. [Google Scholar]
- Corral Torres E, Hernández-Tejedor A, Suárez Bustamante R, de Elías Hernández R, Casado Flórez I, San Juan Linares A. Prognostic value of venous blood analysis at the start of CPR in non-traumatic out-of-hospital cardiac arrest: association with ROSC and the neurological outcome. Crit Care. 2020, 24, 60. [Google Scholar]
- Nolan JP, Neumar RW, Adrie C, Aibiki M, Berg RA, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A Scientific Statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; the Council on Stroke. Resuscitation 2008, 79, 350–379. [Google Scholar]
- Allen, S.E. and Holm, J.L.Lactate: physiology and clinical utility. Journal of Veterinary Emergency and Critical Care 2008, 18, 123–132. [Google Scholar]
- Mohindra, RohitPatel, MatthewLin, Steve et al. A new paradigm of resuscitation: Perfusion-guided cardiopulmonary resuscitation.
Figure 1.
Characteristics of patients with Out-of-hospital cardiac arrest (OHCA). Legend: CPR, cardiopulmonary resuscitation; EMS, emergency medical service; AED, automatic external defibrillator, PEA, pulseless electrical activity; ROSC return of spontaneous circulation; VF, ventricular fibrillation; VT, pulseless ventricular tachycardia; CPC, Cerebral Performance Category Scale.
Figure 1.
Characteristics of patients with Out-of-hospital cardiac arrest (OHCA). Legend: CPR, cardiopulmonary resuscitation; EMS, emergency medical service; AED, automatic external defibrillator, PEA, pulseless electrical activity; ROSC return of spontaneous circulation; VF, ventricular fibrillation; VT, pulseless ventricular tachycardia; CPC, Cerebral Performance Category Scale.
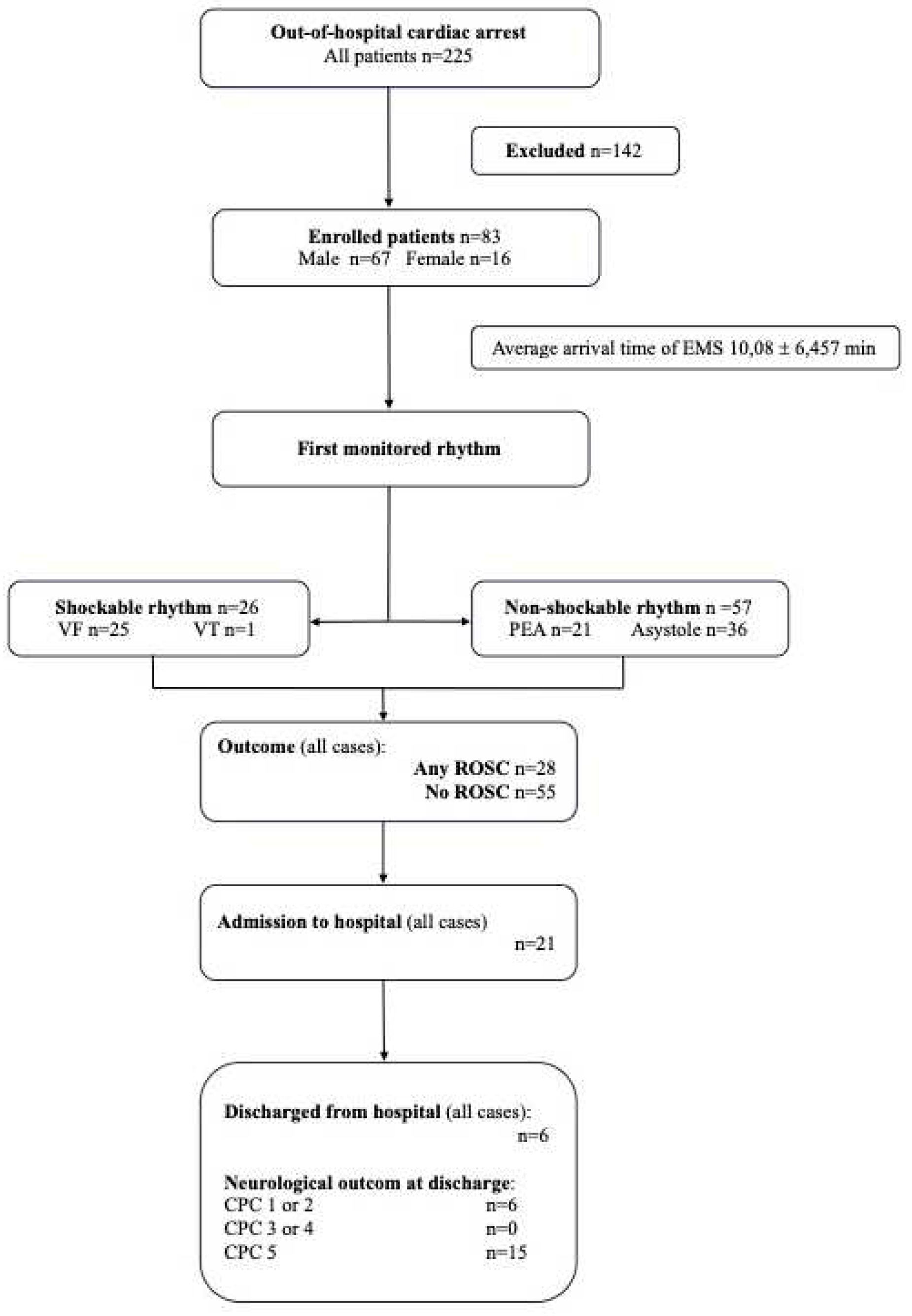
Figure 2.
Correlation between lactate and EtCO2 in group of patients with OHCA regarding initial rhythm. (for detailed values see Appendix A). Legend: *,p <0,05.
Figure 2.
Correlation between lactate and EtCO2 in group of patients with OHCA regarding initial rhythm. (for detailed values see Appendix A). Legend: *,p <0,05.
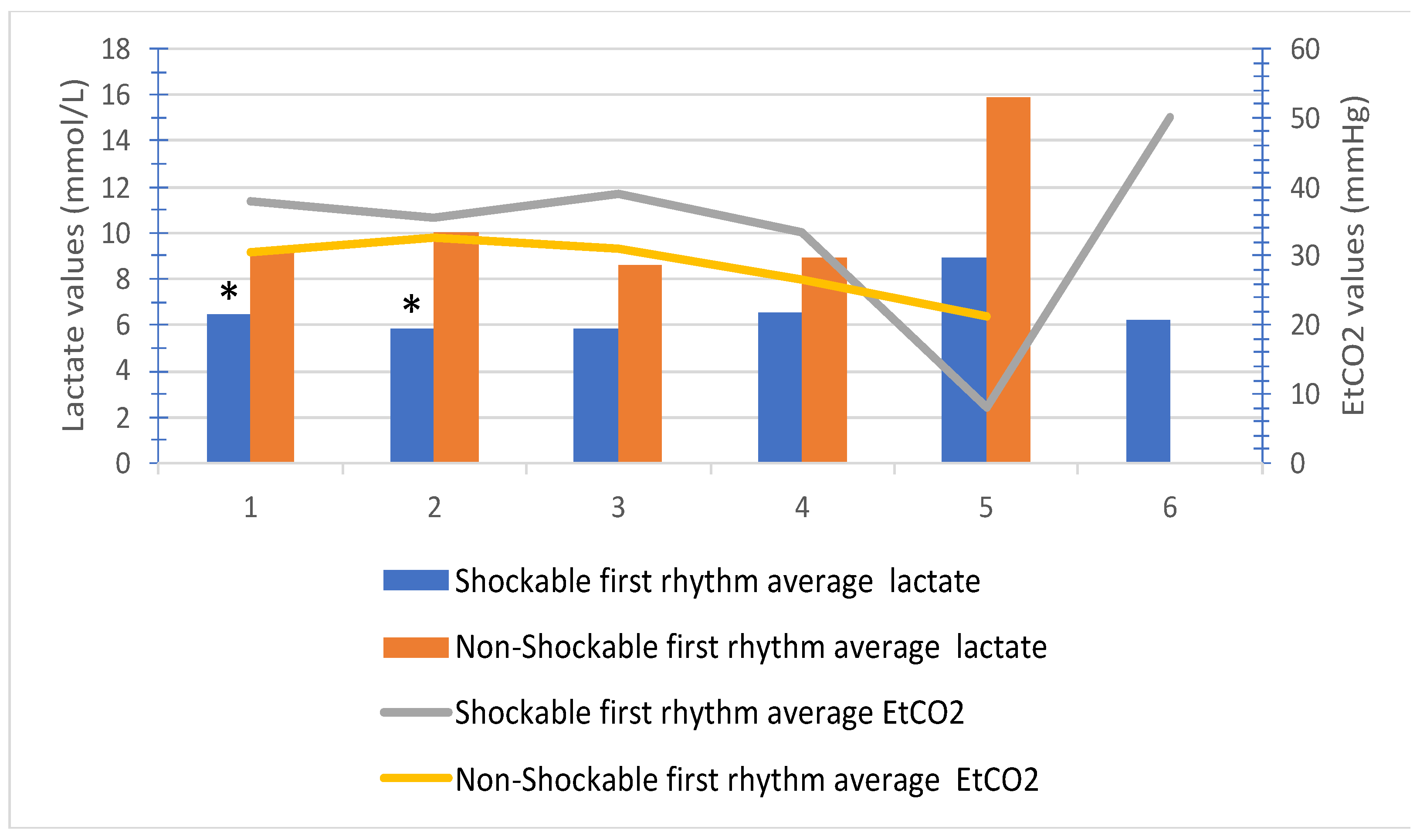
Figure 3.
Correlation between capillary lactate and EtCO2 in ROSC and non-ROSC group of patients (for detailed values see Appendix A). Legend: *,p <0,05
Figure 3.
Correlation between capillary lactate and EtCO2 in ROSC and non-ROSC group of patients (for detailed values see Appendix A). Legend: *,p <0,05
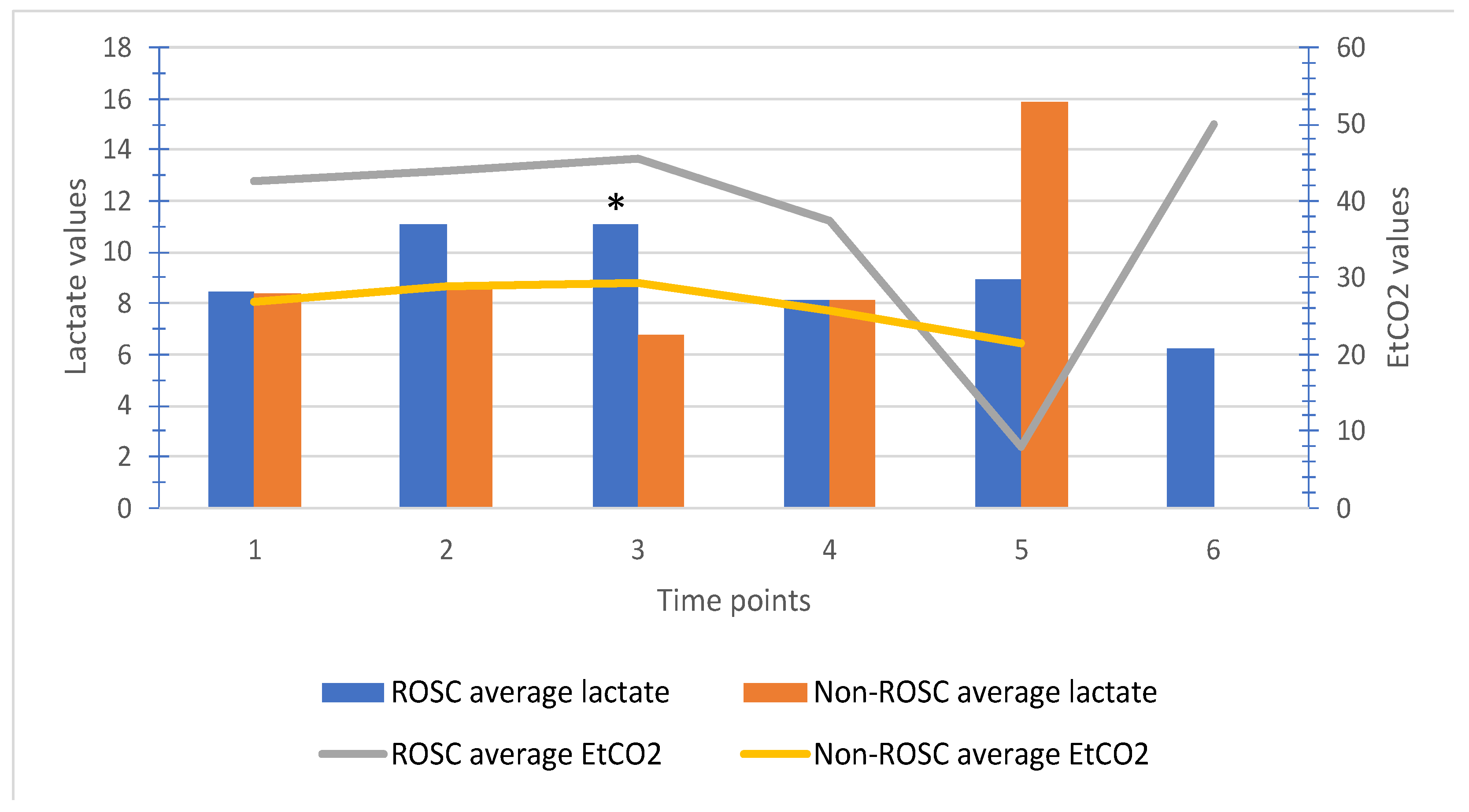

Table 1.
Initial and serial values of capillary lactate in patients depending on the first monitored (shockable or non-shockable) rhythm.
Table 1.
Initial and serial values of capillary lactate in patients depending on the first monitored (shockable or non-shockable) rhythm.
| Patients | N | Mean | Std. Deviation | p | |
| Initial value of lactate | Patients with first monitored shockable rhythm |
16 | 6,43 | 3,81 | 0,037 |
| Patients with first monitored non-shockable rhythm |
43 | 9,19 | 4,61 | ||
| Serial value of lactate after 10 minutes | Patients with first monitored shockable rhythm |
10 | 5,81 | 3,47 | 0,019 |
| Patients with first monitored non-shockable rhythm |
38 | 10,03 | 5,19 | ||
| Serial value of lactate after 20 minutes | Patients with first monitored shockable rhythm |
9 | 5,83 | 2,47 | 0,075 |
| Patients with first monitored non-shockable rhythm |
21 | 8,61 | 5,73 | ||
| Serial value of lactate after 30 minutes | Patients with first monitored shockable rhythm |
6 | 6,52 | 3,27 | 0,329 |
| Patients with first monitored non-shockable rhythm |
12 | 8,95 | 5,40 | ||
| Serial value of lactate after 40 minutes | Patients with first monitored shockable rhythm |
2 | 8,90 | 1,13 | 0,259 |
| Patients with first monitored non-shockable rhythm |
3 | 15,90 | 6,71 | ||
Legend: N, number of measurements.
Table 2.
Initial and serial values of capillary lactate in patients with ROSC or non-ROSC.
| ROSC | N | Mean | Std. Deviation | p | |
|---|---|---|---|---|---|
| Initial value of lactate during CPR | Yes | 21 | 8,48 | 4,86 | 0,959 |
| No | 38 | 8,42 | 4,43 | ||
| 2nd value of lactate after 10 min | Yes | 11 | 11,09 | 5,17 | 0,156 |
| No | 37 | 8,57 | 5,06 | ||
| 3rd value of lactate after 20 min | Yes | 7 | 11,10 | 6,59 | 0,047 |
| No | 23 | 6,77 | 4,23 | ||
| 4th value of lactate after 30 min | Yes | 3 | 8,13 | 0,95 | 0,998 |
| No | 15 | 8,14 | 5,32 | ||
| 5th value of lactate after 40 min | Yes | 2 | 8,90 | 1,13 | 0,259 |
| No | 3 | 15,90 | 6,71 | ||
| 6th value of lactate after 50 min | Yes | 1 | 6,20 | ||
| No | 0a |
Legend: CPR, cardiopulmonary resuscitation; ROSC, return of spontaneous circulation; N, number of measurements; a, t cannot be computed because at least one of the groups is empty.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



