
Submitted:
26 September 2023
Posted:
28 September 2023
You are already at the latest version
Abstract
Aims: To date, precision medicine plays a pivotal role in the clinical administration of solid tumor patients. In this scenario, a rapidly increasing number of predictive biomarkers have been approved in diagnostic practice or are currently investigated in clinical trials. A pitfall in the molecular tests is the diagnostic routine sample available to analyze predictive biomarkers; scant tissue sample often represents the only diagnostical source of nucleic acids to assess molecular analysis. At the sight of these critical issues, Next Generation Sequencing (NGS) platforms emerged as referral testing strategy for molecular analysis of predictive biomarkers in routine practice but high-skilled personnel, extensive working-time drastically impact on the widespread diffusion of this technology in diagnostic setting. Here, we technically validate a fully integrated NGS platform on diagnostic routine tissue samples previously tested with NGS based diagnostic workflow by a referral institution.
Methods: A retrospective series of n=64 samples (n=32 DNA, n=32 RNA samples), previously tested using a customized NGS assay (SiRe™ and SiRe fusion) were retrieved from internal archive of University of Naples Federico II. Each sample was tested by adopting Oncomine Precision Assay (OPA), able to detect 2769 molecular actionable alterations [hot spot mutations, copy number variations (CNV) and gene fusions on fully integrated NGS platform (Genexus, Thermofisher Scientifics. (26,27) Concordance rate between these technical approaches was carried out.
Results: Genexus system successfully carried out molecular analysis in all instances. A concordance rate of 96.9% (31 out of 32) was observed between OPA and SiRe™ panel both for DNA and RNA based analysis. A negative predictive value of 100% and a positive predictive value of 96.9% (62 out of 64) was assessed.
Conclusions: Fully automatized Genexus system combined with OPA (Thermofisher Scientifics) may be considered a technically valuable, saving time sequencing platform to test predictive biomarkers in diagnostic routine practice.
Keywords:
NGS
; predictive biomarkers
; diagnostic samples
1. Introduction
In the last decades, personalized medicine lay the basis for a novel therapeutical option for solid tumor patients. (1,2) To date, target therapy is routinely available for the clinical administration of several solid tumor patients, including metastatic colorectal cancer (mCRC), melanoma (MM), non-small cell lung cancer (NSCLC), gastrointestinal stromal tumor (GIST), breast cancer (BC) patients. (3-9) Particularly, an increasing number of predictive biomarkers was approved in clinical practice to select lung cancer patients diagnosed with NSCLC type to the best therapeutical option. (8,9) In this evolving scenario, the minimal request in terms of predictive biomarkers to clinically administrate solid tumor patients has been regulated by international societies. (10-14) The most common diagnostic sample available to approach diagnosis and molecular tests in advanced tumor stage consists in a “scant sample” with low abundance of neoplastic cells to successfully carry out mandatory gene testing. (15-17) In this scenario, cytological specimens and small biopsies represent the most common biological source to accurately perform molecular analysis. In addition, cell block (CB), a hybrid preparation where the aspirated material is processed following standardized formalin fixation and paraffin embedding (FFPE), represents an alternative source of neoplastic cells affected by lowest quality and quantity of nucleic acids adopted in molecular tests. (18-19) Despite tissue specimens is considered “gold standard” for molecular testing, a not negligible percentage of patients does not access to molecular tests due to insufficient diagnostic material. (16-17) In this scenario, liquid biopsy becomes an integrating biological source to successfully perform molecular analysis when tissue is not available. Particularly, circulating tumor DNA (ctDNA) isolated from peripheral blood withdrawn consists in a reliable source to detect target molecular alterations. (21) At the sight of these aspects, single plex technology result inadequate to successfully analyze minimum gene panel established for each solid tumor. In this heterogenous landscape of biological sources, next generation sequencing (NGS) platforms play a crucial role in the molecular analysis of predictive biomarkers. (22-24) This technology allows to simultaneously analyze very low frequency clinically relevant biomarkers from very low amount of nucleic acids in a single run. (22,23) Remarkably, NGS systems are scalable decreasing reaction cost in accordance with the number of samples processed in each run. (24) On the other hand, adequate number of samples saving technical costs may be collected in more than 30 days for a not negligible number of small-medium institutions involved in molecular tests. This aspect drastically impacts on turnaround -time (TAT) resulting in a delay for the clinical administration of tumor patients. (24,25) In this scenario, Ion Torrent™ Genexus™ Integrated Sequencer (Genexus; Thermofisher Scientifics, Waltham Massachusetts) was designed to automatically carry out entire NGS workflow (from tissue and liquid biopsy derived nucleic acids extraction to data analysis) without other manual operations. (26-28) This technology allows to successfully carry out molecular analysis of a small batch of diagnostic specimens (1- 8) without impacting on Turn-around Time (TAT) of diagnostic workflow. We aimed to evaluate the concordance rate between Genexus system and Ion Torrent S5™ plus (Thermofisher Scientifics, Waltham Massacchusetts) on a retrospective series of extracted genomic DNA (gDNA) from solid tumor patients previously tested in our diagnostic routine.
2. Study design
A retrospective series of n=64 previously extracted DNA and RNA specimens from solid tumor patients [n=16 CRC, n=13 NSCLC, n=2 BC and n=1 MM and n=32 NSCLC cases for DNA and RNA related molecular analysis, respectively) was retrieved from internal archive of Predictive molecular pathology laboratory of University of Naples Federico II. Clinical pathological data were listed in Table 1 and Table 2.
Each sample was previously tested by adopting a customized NGS assay (SiRe™ and SiRe fusion), that covers n=568 clinically relevant alterations in BRAF, EGFR, KRAS, NRAS, PIK3CA, c-KIT, PDGFRA and ALK, ROS1, RET, and NTRK gene fusions, as well as and MET exon 14 skipping alterations, routinely employed in molecular testing of solid tumor patients. (29) The Oncomine Precision Assay (OPA), able to detect 2769 molecular actionable alterations [hot spot mutations, copy number variations (CNV) and gene fusions, was combined with Genexus (Thermofisher Scientifics) platform to assess molecular profile of selected samples. (26,27) Concordance rate of OPA on Genexus system with SiRe™ on S5 plus platform was investigated. All information regarding human material will be managed using anonymous numerical codes, and all samples will be handled in compliance with the Helsinki Declaration (http://www.wma.net/ en/30publications/10policies/b3/).
3. Material and methods
3.1. Routine sample processing startegy
Nucleic acids were previously purified from n=4 representative slides of neoplastic area (>10%). Particularly, QIAamp DNA Mini Kit (Qiagen, Crawley, West Sussex, UK) was adopted following manufacturer instructions. DNA quantification was successfully carried out in all instances according to standardized procedures. Conversely, RNA volume was maximized for cDNA synthesis. Selected samples were routinely analyzed with SiRe™ and SiRe fusion panel on Ion S5™ plus (Thermofisher Scientifics) to assess mutational status in clinically relevant biomarkers for NSCLC patients. (29-31) Briefly, 15 μl of extracted DNA/cDNA was dispensed on Ion Chef system (Thermofisher Scientifics) for library preparation. A total of n= 8 samples were simultaneously processed following previously validated thermal condition. After pooling, templating procedure was carried out for n=16 libraries by using Ion 510™ & Ion 520™ & Ion 530™ Kit Chef (Thermofischer Scientifics) according to manufacturer instructions on 520 chip (Thermofisher Scientifics). Data were inspected by adopting designed bed files on proprietary Torrent Suite [v.5.0.2]. In details, variant inspection was performed with variant caller plug-in (v.5.0.2.1) able to filter variants with ⩾5X allele coverage and a quality score ⩾20, within an amplicon that covered at least 500X alleles.
3.2. Genexus analysis
A series of n=64 extracted gDNA and gRNA from solid tumor patients were retrospectively tested on Genexus (Thermofisher Scientifics) system. The platform enables entire NGS workflows (from library preparation to data interpretation) within 24 hours. OPA assay includes most clinically relevant actionable genes (EGFR, BRAF, KRAS, ALK, ROS1, NTRK, and RET) for NSCLC patients. (27,28) Briefly, samples were created on dedicated server and assigned to a new run. Genexus platform was loaded with OPA primers, strip solutions, strip reagents and supplies according to manufacturer instructions. A total of 10 ng was required by OPA assay on Genexus platform. Accordingly, each sample was diluted and immediately dispensed on 96-well plate, following manufacturer instructions. Finally, nucleic acids were sequenced on GX5TM chip that allows simultaneous processing of n=8 samples in a single line with OPA assay. Data analysis was performed on proprietary Genexus software. Particularly, detected alterations were annotated by adopting Oncomine Knowledgebase Reporter Software (Oncomine Reporter 5.0).
4. Results
4.1. Hot spot mutations
Overall, Genexus system successfully carried out molecular analysis in all DNA series. In details, a median number of total reads, mapped reads, mean read length, percent reads on target, mean depth, uniformity of amplicon coverage of 1134878.2 (ranging from 424900.0 to 1791041.0), 1074345.7 (ranging from 365139.0 to 1756414.0), 90.9 bp (ranging from 71 to 103 bp), 88.3% (ranging from 77.7 to 93.7%), 3602.9 (ranging from 994.00 to 6097.0) and 98.2% (ranging from 96.7 to 99.4%) were detected, respectively. (Table 3).
Remarkably, n=29 out of 32 (90.6%) patients [n=16 CRC, n= 10 NSCLC, n=2 BC and n=1 MM) showed molecular alterations covered by OPA reference genes. Of note, 24 out of 29 (82.7%) cases highlighted clinically relevant molecular alterations referenced by SiRe™ panel. In particular, n=3 out 29 EGFR mutations [n=1 exon 19 c.2300_2308dup p.A767_V769dup; n=1 exon 21 c.2573T>G p.L858R and a concomitant EGFR exon 20 c.2369C>T p.T790M+ exon 21 c.2573T>G p.L858R; n=13 out of 29 KRAS molecular alterations [n=3 exon 2 c.35G>A p.G12D; n=2 exon 2 c.34G>T p.G12C; n=2 exon 2 c.35G>A p.G12V; n=1 exon 2 c.38G>A p.G13D; n=1 exon 3 c.182A>T p.Q61L; n=1 exon 3 c.181C>A p.Q61K; n=1 exon 4 c.436G>A p.A146T and n=2 concomitant KRAS exon 2 c.35G>A p.G12D+ c.38G>A p.G13D; KRAS exon 2 c.38G>A p.G13D+ c.38_39delinsAA p.G13E]; n=3 out of 29 BRAF mutations [n=2 exon 15 c.1799T>A p.V600E and n=1 exon 15 c.1801A>G p.K601E]; n=4 out of 29 PIK3CA hot spot mutations [n=2 exon 9 c.1633G>A p.E545K and n=2 exon 20 c.3140A>G p.H1047R]; n=3 out 29 NRAS mutations [n=2 exon 3 c.181C>A p.Q61K and n=1 exon 3 c.182A>G p.Q61R]; n=1 out of 29 c-KIT molecular alterations [exon 11 c.1727T>C p.L576P] were detected. (Table 4).
Molecular profile detected by OPA on Genexus platform matched with Sire panel on S5 plus system in 31 out of 32 patients (96.9%). Remarkably, positive results previously identified adopting SiRe panel were confirmed in 23 out of 24 (95.8%) patients. Particularly, ID#19 showed exon 9 PIK3CA p.E545K hot spot mutation not observed by using S5 system with standardized clinical cut-off. (Figure 1)
No significant variations in accordance with histological groups, mutation type and mutant allele fraction levels between Genexus and previously tested samples on S5 platform were identified. In addition, OPA assay also identified n= 16 out of 32 (50.0%) DNA based molecular alterations in other genes not covered by SiRe panel. As regards, 12 out of 16, 1 out of 16 and 1 out of 16 highlighted TP53, CTNNB1 and MTOR hotspot molecular altercations, respectively. Moreover, a concomitant TP53 (exon 7 p.G279E plus exon 5 p.V197M) and TP53 (exon 4 p.R175H) in association with CTNNB1 (exon 3 p.S45F) hotspot mutations were identified in ID#2 and ID#16 cases. (Table 5).
4.2. Fusions rearrangements
Regarding RNA samples, Genexus platform successfully analyzed all retrieved cases. Briefly, a median number of total reads, mapped reads and mean read length of 1721491.0 (ranging from 1471817.00 to 2462555.00), 158230.4 (ranging from 37387.0 to 1029745.00), 98.8 bp (ranging from 91 to 104 bp) were identified, respectively. (Table 6).
Of note, 10 out of 32 (31.2%) patients highlighted aberrant transcripts by using Genexus platform. Among them, 5 out of 10 and 2 out of 10 patients showed ALK and RET rearrangements, respectively. Moreover, three patients were positive for ROS1, NTRK aberrant transcripts and MET Δ 14 skipping mutation, respectively. (Table 7) Interestingly, rearranged genes were identified by OPA on Genexus platform in 9 out of 10 (90.0%) retrieved cases showing a concordance rate of 96.9% (31 out of 32 cases) with SiRe panel on S5 system. Particularly, ID#1 was positive for NTRK3-KANK1 fusion transcript not previously detected with SiRe panel on S5 platform. No significant variations were observed in accordance with histological groups, rearranged genes, fusion partners, and mapped reads levels between Genexus and previously tested samples on S5 platform.
5. Discussion
In the era of personalized medicine, the rapidly increasing number of predictive biomarkers yet approved in clinical practice have revolutionized the treatment strategy for solid tumor patients. (1-2,32) Although the widespread diffusion of single-gene testing platforms in the vast majority of laboratories involved in molecular tests, low multiplexing biomarker’s analysis discouraging their implementation as pivotal diagnostic platform in clinical practice (23-24). As regards, NGS techniques allows to simultaneously cover clinically relevant molecular alterations from a plethora of diagnostic routine specimens saving technical costs and maintaining adequate TAT (33). Moreover, NGS platforms may also benefit of automatized technical procedures that allows accurate and reproducible analysis spending low bench-working time (33). Genexus system consists in a scalable, versatile and fully automatized sequencer able to carry out each technical procedure without manual operations (34). This system is built to integrate analytical procedures (nucleic acids extraction, libraries preparation, template generation, sequencing) with data analysis by adopting pre-customized pipeline analysis. Here, we have validated Genexus system in our diagnostic routine by comparing its analytical performance on a retrospective series of clinical cases previously analyzed with a custom NGS panel on S5 system. As expected, all diagnostic specimens (n=64) were successfully analyzed by using this fully automatized system. Overall, a concordance rate of 96.9% (62 out of 64) was reached by adopting Sire panel on S5 system as reference standard. Interestingly, molecular analysis unmatched with previously archived data in only two cases (DNA-ID#19 and RNA-ID#1). Of note, DNA-ID#19 sample derived from a BC patient resulted positive for PIK3CA exon 9 p.E545K hotspot alteration on Genexus system with a mutant allele fraction (MAF) of 7.2%. Following manufacturer clinical cut-off (MAF ≥5%), previous analysis did not show any clinically relevant molecular alteration. By approaching visual inspection of raw data, the same alteration at 0.9% was detected. Similarly, RNA-ID#1 showed NTRK3 (ex14) - KANK1 (ex3) aberrant transcript not previously detected with the standard reference approach. In this case NTRK3 was not covered by reference range of SiRe fusion panel.
In a not negligible percentage of cases, synchronous lesions may be observed in CRC patients. In this scenario, NGS may be considered an affordable technical strategy to comprehensively evaluate molecular assessment of CRC patients where heterogeneous specimens are clinically available (28). DNA-ID#11 and DNA-ID#2 represent synchronous lesions of a CRC elected to molecular test. Interestingly, both S5 and Genexus systems revealed KRAS exon 2 p.G12C and PIK3CA exon 20 p.H1047R hot spot mutations demonstrating a common origin of these lesions. Moreover, NGS systems overcome technical issues from the analysis of “complex” molecular alteration. DNA-ID#22 case confirmed two concomitant KRAS exon 2 hotspot mutations p.G13D+p.G13E on Genexus platform previously detected by reference technology. Although this study provides encouraging results for the implementation of Genexus system in clinical routine setting of solid tumor patients, some limitations may be identified. Firstly, this technical report aims to compare analytical parameters of two NGS-based technologies on a series of diagnostic routine specimens without any clinical considerations. Secondly, this retrospective study is based on the analysis of a small group of cases retrieved from internal archive of University of Naples Federico II. All these crucial points warrant further analysis, but this preliminary data may suggest that fully automatized Genexus system integrated with commercially available OPA (Thermofisher Scientifics) represent a technically affordable, saving time sequencing platform enable to analyze clinically relevant molecular alterations in diagnostic routine specimens.
Author Contributions
“Conceptualization, CDL, FP, GT and UM.; methodology, all the authors.; software, CDL, FP, GT and UM; validation, all the authors.; formal analysis, all the authors; data curation, CDL, FP, GT and UM.; writing—original draft preparation, CDL, FP; writing—review and editing, GT and UM.; visualization, all the authors; supervision, GT and UM.; project administration, GT and UM All authors have read and agreed to the published version of the manuscript.”
Funding
1. Monitoraggio ambientale, studio ed approfondimento della salute della popolazione residente in aree a rischio—In attuazione della D.G.R. Campanian.180/2019. 2. POR Campania FESR 2014–2020 Progetto “Sviluppo di Approcci Terapeutici Innovativi per patologie Neoplastiche resistenti ai trattamenti—SATIN”. 3. This work has been partly supported by a grant from the Italian Health Ministry’s research program (ID: NET-2016-02363853). National Center for Gene Therapy and Drugs based on RNA Technology MUR-CN3 CUP E63C22000940007 to DS.
Patient consent for publication
Not applicable
Ethics approval
Not applicable
Competing interests
Pasquale Pisapia has received personal fees as speaker bureau from Novartis for work performed outside of the current study. Umberto Malapelle has received personal fees (as consultant and/or speaker bureau) from Boehringer Ingelheim, Roche, MSD, Amgen, Thermo Fisher Scientific, Eli Lilly, Diaceutics, GSK, Merck and AstraZeneca, Janssen, Diatech, Novartis and Hedera unrelated to the current work. Giancarlo Troncone reports personal fees (as speaker bureau or advisor) from Roche, MSD, Pfizer, Boehringer Ingelheim, Eli Lilly, BMS, GSK, Menarini, AstraZeneca, Amgen and Bayer, unrelated to the current work.
References
- Yates, L.; Seoane, J.; Le Tourneau, C.; Siu, L.; Marais, R.; Michiels, S.; Soria, J.; Campbell, P.; Normanno, N.; Scarpa, A.; et al. The European Society for Medical Oncology (ESMO) Precision Medicine Glossary. Ann. Oncol. 2017, 29, 30–35. [Google Scholar] [CrossRef]
- Ciardiello, F.; Arnold, D.; Casali, P.G.; Cervantes, A.; Douillard, J.-Y.; Eggermont, A.; Eniu, A.; McGregor, K.; Peters, S.; Piccart, M.; et al. Delivering precision medicine in oncology today and in future—the promise and challenges of personalised cancer medicine: a position paper by the European Society for Medical Oncology (ESMO). Ann. Oncol. 2014, 25, 1673–1678. [Google Scholar] [CrossRef]
- Di Nicolantonio, F.; Martini, M.; Molinari, F.; Sartore-Bianchi, A.; Arena, S.; Saletti, P.; De Dosso, S.; Mazzucchelli, L.; Frattini, M.; Siena, S.; et al. Wild-Type BRAF Is Required for Response to Panitumumab or Cetuximab in Metastatic Colorectal Cancer. J. Clin. Oncol. 2008, 26, 5705–5712. [Google Scholar] [CrossRef] [PubMed]
- Lièvre, A.; Bachet, J.B.; Boige, V.; Cayre, A.; Le Corre, D.; Buc, E.; Ychou, M.; Bouché, O.; Landi, B.; Louvet, C.; André, T.; Bibeau, F.; Diebold, M.D.; Rougier, P.; Ducreux, M.; Tomasic, G.; Emile, J.F.; Penault-Llorca, F.; Laurent-Puig, P. KRAS mutations as an independent prognostic factor in patients with advanced colorectal cancer treated with cetuximab. J Clin Oncol. 2008, 26, 374–9. [Google Scholar] [CrossRef]
- Chapman, P.B.; Hauschild, A.; Robert, C.; Haanen, J.B.; Ascierto, P.; Larkin, J.; Dummer, R.; Garbe, C.; Testori, A.; Maio, M.; et al. BRIM-3 Study Group. Improved survival with vemurafenib in melanoma with BRAF V600E mutation. N Engl J Med. 2011, 364, 2507–16. [Google Scholar] [CrossRef] [PubMed]
- Antonescu, C.R. Targeted therapies in gastrointestinal stromal tumors. Semin. Diagn. Pathol. 2008, 25, 295–303. [Google Scholar] [CrossRef]
- Fusco, N.; Malapelle, U.; Fassan, M.; Marchiò, C.; Buglioni, S.; Zupo, S.; Criscitiello, C.; Vigneri, P.; Tos, A.P.D.; Maiorano, E.; et al. PIK3CA Mutations as a Molecular Target for Hormone Receptor-Positive, HER2-Negative Metastatic Breast Cancer. Front. Oncol. 2021, 11. [Google Scholar] [CrossRef]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29 (Suppl. 4), iv192–iv237. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.-R.; Schultheis, A.M.; Yu, H.; Mandelker, D.; Ladanyi, M.; Büttner, R. Precision medicine in non-small cell lung cancer: Current applications and future directions. Semin. Cancer Biol. 2020, 84, 184–198. [Google Scholar] [CrossRef]
- Lindeman, N.I.; Cagle, P.T.; Aisner, D.L.; Arcila, M.E.; Beasley, M.B.; Bernicker, E.H.; Colasacco, C.; Dacic, S.; Hirsch, F.R.; Kerr, K.; et al. Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment With Targeted Tyrosine Kinase Inhibitors: Guideline From the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology. Arch. Pathol. Lab. Med. 2018, 142, 321–346. [Google Scholar] [CrossRef]
- Kalemkerian, G.P.; Narula, N.; Kennedy, E.B.; Biermann, W.A.; Donington, J.; Leighl, N.B.; Lew, M.; Pantelas, J.; Ramalingam, S.S.; Reck, M.; et al. Molecular Testing Guideline for the Selection of Patients With Lung Cancer for Treatment With Targeted Tyrosine Kinase Inhibitors: American Society of Clinical Oncology Endorsement of the College of American Pathologists/International Association for the Study of Lung Cancer/Association for Molecular Pathology Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Jennings, L.J.; Arcila, M.E.; Corless, C.; Kamel-Reid, S.; Lubin, I.M.; Pfeifer, J.; Temple-Smolkin, R.L.; Voelkerding, K.V.; Nikiforova, M.N. Guidelines for Validation of Next-Generation Sequencing-Based Oncology Panels: A Joint Consensus Recommendation of the Association for Molecular Pathology and College of American Pathologists. J Mol Diagn. 2017, 19, 341–365. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda, A.R.; Hamilton, S.R.; Allegra, C.J.; Grody, W.; Cushman-Vokoun, A.M.; Funkhouser, W.K.; Kopetz, S.E.; Lieu, C.; Lindor, N.M.; Minsky, B.D.; et al. Molecular Biomarkers for the Evaluation of Colorectal Cancer: Guideline From the American Society for Clinical Pathology, College of American Pathologists, Association for Molecular Pathology, and the American Society of Clinical Oncology. J. Clin. Oncol. 2017, 35, 1453–1486. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Wu, Y.L.; Thongprasert, S.; Yang, C.H.; Chu, D.T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; Nishiwaki, Y.; Ohe, Y.; Yang, J.J.; Chewaskulyong, B.; Jiang, H.; Duffield, E.L.; Watkins, C.L.; Armour, A.A.; Fukuoka, M. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009, 361, 947–57. [Google Scholar] [CrossRef] [PubMed]
- Kris, M.G.; Johnson, B.E.; Berry, L.D.; Kwiatkowski, D.J.; Iafrate, A.J.; Wistuba, I.I.; Varella-Garcia, M.; Franklin, W.A.; Aronson, S.L.; Su, P.-F.; et al. Using Multiplexed Assays of Oncogenic Drivers in Lung Cancers to Select Targeted Drugs. JAMA 2014, 311, 1998–2006. [Google Scholar] [CrossRef] [PubMed]
- Meric-Bernstam, F.; Brusco, L.; Shaw, K.; Horombe, C.; Kopetz, S.; Davies, M.A.; Routbort, M.; Piha-Paul, S.A.; Janku, F.; Ueno, N.; et al. Feasibility of Large-Scale Genomic Testing to Facilitate Enrollment Onto Genomically Matched Clinical Trials. J. Clin. Oncol. 2015, 33, 2753–2762. [Google Scholar] [CrossRef]
- Sundaresan, T.K.; Sequist, L.V.; Heymach, J.V.; Riely, G.J.; Jänne, P.A.; Koch, W.H.; Sullivan, J.P.; Fox, D.B.; Maher, R.; Muzikansky, A.; Webb, A.; Tran, H.T.; Giri, U.; Fleisher, M.; Yu, H.A.; Wei, W.; Johnson, B.E.; Barber, T.A.; Walsh, J.R.; Engelman, J.A.; Stott, S.L.; Kapur, R.; Maheswaran, S.; Toner, M.; Haber, D.A. Detection of T790M, the Acquired Resistance EGFR Mutation, by Tumor Biopsy versus Noninvasive Blood-Based Analyses. Clin Cancer Res. 2016, 22, 1103–10. [Google Scholar] [CrossRef]
- Roy-Chowdhuri, S.; Chow, C.; Kane, M.K.; Yao, H.; Wistuba, I.I.; Krishnamurthy, S.; Stewart, J.; Staerkel, G. Optimizing the DNA yield for molecular analysis from cytologic preparations. Cancer Cytopathol. 2015, 124, 254–260. [Google Scholar] [CrossRef]
- Pepe, F.; De Luca, C.; Smeraglio, R.; Pisapia, P.; Sgariglia, R.; Nacchio, M.; Russo, M.; Serra, N.; Rocco, D.; Battiloro, C.; et al. Performance analysis of SiRe next-generation sequencing panel in diagnostic setting: focus on NSCLC routine samples. J. Clin. Pathol. 2018, 72, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Velizheva, N.P.; Rechsteiner, M.P.; Wong, C.E.; Zhong, Q.; Rössle, M.; Bode, B.; Moch, H.; Soltermann, A.; Wild, P.J.; Tischler, V. Cytology smears as excellent starting material for next-generation sequencing-based molecular testing of patients with adenocarcinoma of the lung. Cancer Cytopathol. 2016, 125, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Heitzer, E.; Haque, I.S.; Roberts, C.E.S.; Speicher, M.R. Current and future perspectives of liquid biopsies in genomics-driven oncology. Nat. Rev. Genet. 2019, 20, 71–88. [Google Scholar] [CrossRef]
- Pisapia, P.; Pepe, F.; Iaccarino, A.; Sgariglia, R.; Nacchio, M.; Conticelli, F.; Salatiello, M.; Tufano, R.; Russo, G.; Gragnano, G.; et al. Next Generation Sequencing in Cytopathology: Focus on Non-Small Cell Lung Cancer. Front. Med. 2021, 8. [Google Scholar] [CrossRef]
- Hayashi, H.; Tanishima, S.; Fujii, K.; Mori, R.; Okada, C.; Yanagita, E.; Shibata, Y.; Matsuoka, R.; Amano, T.; Yamada, T.; et al. Clinical impact of a cancer genomic profiling test using an in-house comprehensive targeted sequencing system. Cancer Sci. 2020, 111, 3926–3937. [Google Scholar] [CrossRef]
- Kou, T.; Kanai, M.; Yamamoto, Y.; Kamada, M.; Nakatsui, M.; Sakuma, T.; Mochizuki, H.; Hiroshima, A.; Sugiyama, A.; Nakamura, E.; et al. Clinical sequencing using a next-generation sequencing-based multiplex gene assay in patients with advanced solid tumors. Cancer Sci. 2017, 108, 1440–1446. [Google Scholar] [CrossRef]
- Pisapia, P.; Pepe, F.; Baggi, A.; Barberis, M.; Galvano, A.; Gristina, V.; Mastrilli, F.; Novello, S.; Pagni, F.; Pasini, S.; et al. Next generation diagnostic algorithm in non-small cell lung cancer predictive molecular pathology: The KWAY Italian multicenter cost evaluation study. Crit. Rev. Oncol. 2022, 169, 103525. [Google Scholar] [CrossRef]
- Low, S.-K.; Ariyasu, R.; Uchibori, K.; Hayashi, R.; Chan, H.T.; Chin, Y.M.; Akita, T.; Harutani, Y.; Kiritani, A.; Tsugitomi, R.; et al. Rapid genomic profiling of circulating tumor DNA in non-small cell lung cancer using Oncomine Precision Assay with GenexusTM integrated sequencer. Transl. Lung Cancer Res. 2022, 11, 711–721. [Google Scholar] [CrossRef]
- Ilié, M.; Hofman, V.; Bontoux, C.; Heeke, S.; Lespinet-Fabre, V.; Bordone, O.; Lassalle, S.; Lalvée, S.; Tanga, V.; Allegra, M.; et al. Setting Up an Ultra-Fast Next-Generation Sequencing Approach as Reflex Testing at Diagnosis of Non-Squamous Non-Small Cell Lung Cancer; Experience of a Single Center (LPCE, Nice, France). Cancers 2022, 14, 2258. [Google Scholar] [CrossRef]
- Sheffield, B.S.; Beharry, A.; Diep, J.; Perdrizet, K.; Iafolla, M.A.J.; Raskin, W.; Dudani, S.; Brett, M.A.; Starova, B.; Olsen, B.; et al. Point of Care Molecular Testing: Community-Based Rapid Next-Generation Sequencing to Support Cancer Care. Curr. Oncol. 2022, 29, 1326–1334. [Google Scholar] [CrossRef]
- Malapelle, U.; Mayo de-Las-Casas, C.; Rocco, D.; Garzon, M.; Pisapia, P.; Jordana-Ariza, N.; Russo, M.; Sgariglia, R.; De Luca, C.; Pepe, F.; Martinez-Bueno, A.; Morales-Espinosa, D.; González-Cao, M.; Karachaliou, N.; Viteri Ramirez, S.; Bellevicine, C.; Molina-Vila, M.A.; Rosell, R.; Troncone, G. Development of a gene panel for next-generation sequencing of clinically relevant mutations in cell-free DNA from cancer patients. Br J Cancer. 2017, 116, 802–810. [Google Scholar] [CrossRef]
- Pepe, F.; De Luca, C.; Smeraglio, R.; Pisapia, P.; Sgariglia, R.; Nacchio, M.; Russo, M.; Serra, N.; Rocco, D.; Battiloro, C.; et al. Performance analysis of SiRe next-generation sequencing panel in diagnostic setting: focus on NSCLC routine samples. J. Clin. Pathol. 2018, 72, 38–45. [Google Scholar] [CrossRef]
- Malapelle, U.; Pepe, F.; Pisapia, P.; Sgariglia, R.; Nacchio, M.; De Luca, C.; Lacalamita, R.; Tommasi, S.; Pinto, R.; Palomba, G.; et al. Harmonization of Next-Generation Sequencing Procedure in Italian Laboratories: A Multi-Institutional Evaluation of the SiRe® Panel. Front. Oncol. 2020, 10, 236. [Google Scholar] [CrossRef]
- Yang, S.R.; Schultheis, A.M.; Yu, H.; Mandelker, D.; Ladanyi, M.; Büttner, R. Precision medicine in non-small cell lung cancer: current applications and future directions. Semin. Cancer Biol. Epub ahead of print. 2020. [Google Scholar] [CrossRef]
- Mosele, F.; Remon, J.; Mateo, J.; Westphalen, C.; Barlesi, F.; Lolkema, M.; Normanno, N.; Scarpa, A.; Robson, M.; Meric-Bernstam, F.; et al. Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: a report from the ESMO Precision Medicine Working Group. Ann. Oncol. 2020, 31, 1491–1505. [Google Scholar] [CrossRef]
- Werner, R.; Connolly, A.; Bennett, M.; Hand, C.K.; Burke, L. Implementation of an ISO15189 accredited next-generation sequencing service with the fully automated Ion Torrent Genexus: the experience of a clinical diagnostic laboratory. J. Clin. Pathol. 2022. [Google Scholar] [CrossRef]
Figure 1.
PIK3CA p.E545K hotspot mutations manually inspected with Golden Helix Genome Browser v.2.0.7 (Bozeman, MT, USA) (A) and automatically annotated on on proprietary Genexus software (B).
Figure 1.
PIK3CA p.E545K hotspot mutations manually inspected with Golden Helix Genome Browser v.2.0.7 (Bozeman, MT, USA) (A) and automatically annotated on on proprietary Genexus software (B).
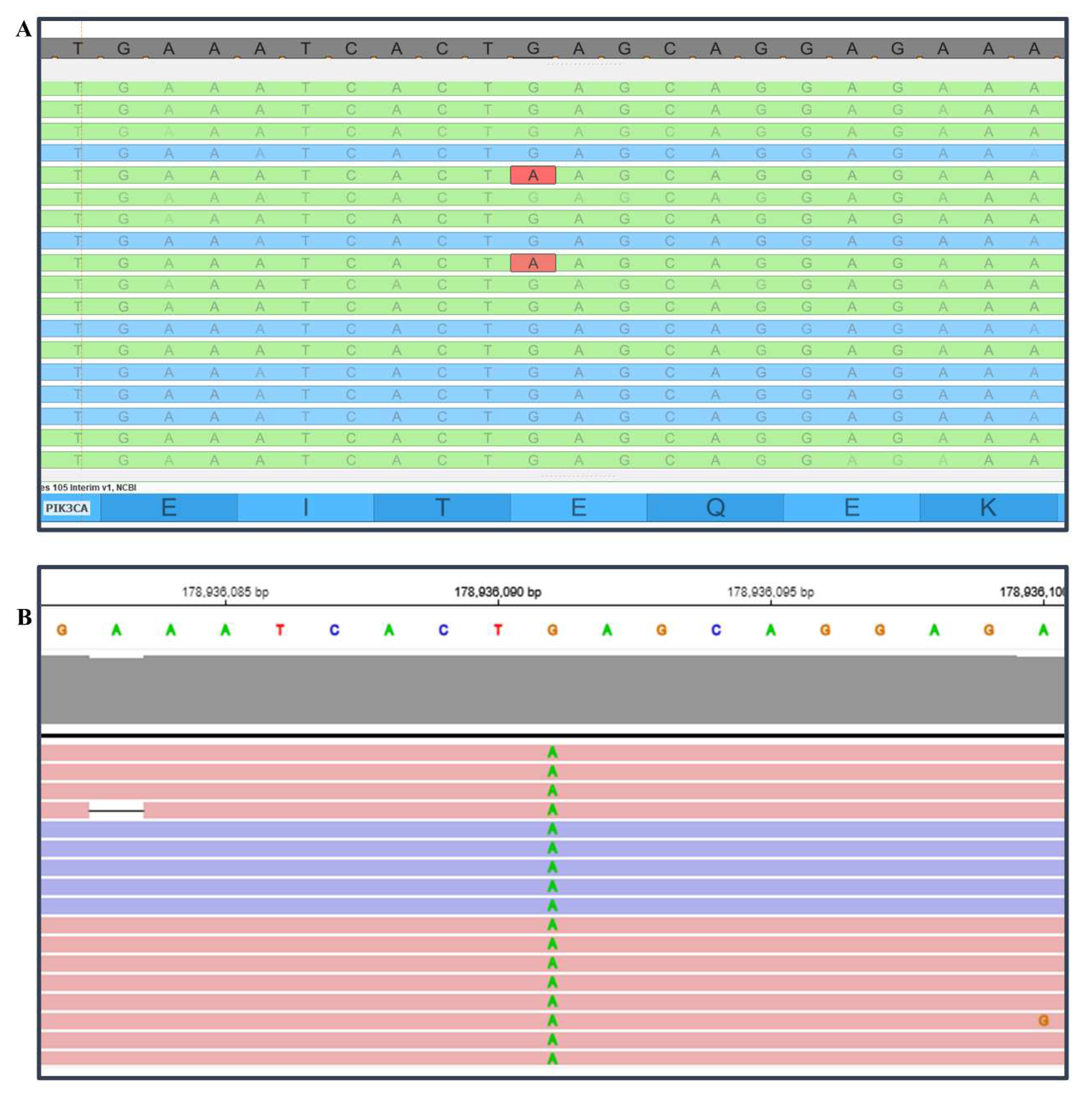

Table 1.
Clinical characteristics of archival cases and corresponding requests on DNA-based molecular alterations.
Table 1.
Clinical characteristics of archival cases and corresponding requests on DNA-based molecular alterations.
| ID | Sex | Age | Sample Type | Tumour | N.C. | Clinical Request |
|---|---|---|---|---|---|---|
| DNA 1* | M | 78 | Resection | CRC | 70.0% | RAS, BRAF |
| DNA 2* | M | 78 | Resection | CRC | 70.0% | RAS, BRAF |
| DNA 3 | M | 89 | Biopsy | CRC | 50.0% | RAS, BRAF |
| DNA 4 | F | 68 | Resection | NSCLC | 70.0% | EGFR, KRAS, BRAF |
| DNA 5 | M | 73 | Resection | CRC | 50.0% | RAS, BRAF |
| DNA 6 | M | 53 | Biopsy | NSCLC | 30.0% | EGFR, KRAS, BRAF |
| DNA 7 | M | 66 | Resection | CRC | 40.0% | RAS, BRAF |
| DNA 8 | F | 78 | Resection | CRC | 40.0% | RAS, BRAF |
| DNA 9 | F | 67 | Resection | NSCLC | 60.0% | EGFR, KRAS, BRAF |
| DNA 10 | F | 51 | Resection | CRC | 30.0% | RAS, BRAF |
| DNA 11 | M | 50 | Resection | CRC | 80.0% | c-KIT, PDGFRA |
| DNA 12 | F | 50 | Biopsy | NSCLC | 50.0% | EGFR, KRAS, BRAF |
| DNA 13 | M | 70 | Biopsy | NSCLC | 20.0% | EGFR, KRAS, BRAF |
| DNA 14 | F | 59 | Resection | NSCLC | 40.0% | EGFR, KRAS, BRAF |
| DNA 15 | M | 66 | Biopsy | NSCLC | 30.0% | EGFR, KRAS, BRAF |
| DNA 16 | M | 56 | Resection | CRC | 50.0% | RAS, BRAF |
| DNA 17 | M | 66 | Resection | NSCLC | 60.0% | EGFR, KRAS, BRAF |
| DNA 18 | F | 51 | Biopsy | CRC | 50.0% | RAS, BRAF |
| DNA 19 | F | 41 | Biopsy | BC | 30.0% | PIK3CA |
| DNA 20 | F | 82 | Biopsy | CRC | 30.0% | RAS, BRAF |
| DNA 21 | M | 67 | Biopsy | CRC | 50.0% | RAS, BRAF |
| DNA 22 | M | 82 | Resection | NSCLC | 80.0% | EGFR, KRAS, BRAF |
| DNA 23 | M | 74 | Resection | NSCLC | 70.0% | EGFR, KRAS, BRAF |
| DNA 24 | M | 74 | Resection | CRC | 40.0% | RAS, BRAF |
| DNA 25 | F | 44 | Biopsy | CRC | 40.0% | RAS, BRAF |
| DNA 26 | F | 69 | Biopsy | NSCLC | 60.0% | EGFR, KRAS, BRAF |
| DNA 27 | M | 54 | Resection | CRC | 30.0% | RAS, BRAF |
| DNA 28 | F | 74 | Resection | MM | 90.0% | BRAF, NRAS |
| DNA 29 | F | 63 | Biopsy | NSCLC | 40.0% | EGFR, KRAS, BRAF |
| DNA 30 | M | 56 | Resection | NSCLC | 50.0% | EGFR, KRAS, BRAF |
| DNA 31 | F | 52 | Resection | CRC | 60.0% | RAS, BRAF |
| DNA 32 | F | 45 | Resection | BC | 60.0% | PIK3CA |
* Same patient, different lesions. Abbreviations: BC (Breast Cancer); BRAF (Murine Sarcoma Viral Oncogene Homolog B); c-KIT (KIT Proto-Oncogene); CRC (Colorectal Cancer); DNA (Deoxyribonucleic Acid); EGFR (Epidermal Growth Factor Receptor); F (Female); ID (Identifier); KRAS (Kirsten Rat Sarcoma Virus); M (Male); MM (Malignant Melanoma); N.C. (Neoplastic Cellularity); NSCLC (Non-Small-Cell Lung Cancer); PIK3CA (Phosphatidylinositol-4,5-Bisphosphate 3-Kinase, Catalytic Subunit Alpha); RAS (Rat Sarcoma Virus).
Table 2.
Clinical characteristics of archival cases and corresponding requests on RNA-based molecular alterations.
Table 2.
Clinical characteristics of archival cases and corresponding requests on RNA-based molecular alterations.
| ID | Sex | Age | Sample Type | Tumour | N.C. | Clinical Request |
|---|---|---|---|---|---|---|
| RNA 1 | M | 56 | Resection | NSCLC | 60.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 2 | F | 58 | Biopsy | NSCLC | 70.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 3 | M | 77 | Biopsy | NSCLC | 25.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 4 | M | 79 | Resection | NSCLC | 70.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 5 | M | 79 | Biopsy | NSCLC | 30.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 6 | M | 59 | Biopsy | NSCLC | 30.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 7 | F | 70 | Biopsy | NSCLC | 50.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 8 | M | 62 | Biopsy | NSCLC | 25.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 9 | M | 61 | Biopsy | NSCLC | 40.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 10 | M | 66 | Resection | NSCLC | 60.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 11 | M | 68 | Biopsy | NSCLC | 40.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 12 | M | 64 | Biopsy | NSCLC | 50.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 13 | F | 65 | Biopsy | NSCLC | 60.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 14 | M | 58 | Biopsy | NSCLC | 20.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 15 | F | 79 | Biopsy | NSCLC | 50.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 16 | M | 52 | Biopsy | NSCLC | 50.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 17 | M | 67 | Resection | NSCLC | 60.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 18 | M | 87 | Biopsy | NSCLC | 40.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 19 | M | 25 | Biopsy | NSCLC | 60.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 20 | F | 60 | Biopsy | NSCLC | 30.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 21 | M | 60 | Resection | NSCLC | 60.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 22 | F | 36 | Biopsy | NSCLC | 30.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 23 | M | 66 | Biopsy | NSCLC | 60.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 24 | F | 47 | Biopsy | NSCLC | 50.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 25 | M | 67 | Biopsy | NSCLC | 30.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 26 | F | 64 | Biopsy | NSCLC | 10.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 27 | M | 54 | Biopsy | NSCLC | 40.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 28 | F | 37 | Biopsy | NSCLC | 50.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 29 | M | 79 | Biopsy | NSCLC | 50.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 30 | F | 71 | Biopsy | NSCLC | 30.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 31 | M | 68 | Biopsy | NSCLC | 50.0% | ALK, ROS1, RET, MET, NTRK |
| RNA 32 | F | 72 | Biopsy | NSCLC | 70.0% | ALK, ROS1, RET, MET, NTRK |
Abbreviations: ALK (Anaplastic Lymphoma Kinase); F (Female); ID (Identifier); M (Male); MET (Tyrosine-Protein Kinase Met); N.C. (Neoplastic Cellularity); NSCLC (Non-Small-Cell Lung Cancer); NTRK (Neurotrophic Tyrosine Receptor Kinase); RET (RET Proto-Oncogene); RNA (Ribonucleic Acid); ROS1 (Proto-Oncogene Tyrosine-Protein Kinase ROS).
Table 3.
Technical parameters from DNA-based analysis by using S5 plus and Genexus systems.
| DNA Analysis Technical Parameters - S5 Plus (SiRe™ Panel) vs Genexus (OPA Panel) | |||||||
|---|---|---|---|---|---|---|---|
| ID | Platform | Total Reads | Mean Read Length | Mapped Reads | On Target Reads | Mean Depth | Uniformity |
| DNA 1* | S5 Plus | 254212 | 126 | 253622 | 94.6% | 5712 | 100% |
| Genexus | 872831 | 76 | 736530 | 77.7% | 2044 | 99.1% | |
| DNA 2* | S5 Plus | 215464 | 128 | 215047 | 92.6% | 4740 | 100% |
| Genexus | 732691 | 84 | 663064 | 83.9% | 2034 | 98.8% | |
| DNA 3 | S5 Plus | 298541 | 135 | 297999 | 93.9% | 6662 | 100% |
| Genexus | 1143038 | 91 | 1076855 | 88.8% | 3528 | 98.1% | |
| DNA 4 | S5 Plus | 524926 | 155 | 523086 | 92.3% | 11489 | 100% |
| Genexus | 1419289 | 101 | 1393603 | 92.9% | 5210 | 98.1% | |
| DNA 5 | S5 Plus | 361148 | 137 | 360373 | 91.3% | 7830 | 100% |
| Genexus | 1094620 | 98 | 1064051 | 91.5% | 3810 | 98.6% | |
| DNA 6 | S5 Plus | 314176 | 128 | 313706 | 99.2% | 7406 | 100% |
| Genexus | 1090358 | 98 | 1049935 | 90.8% | 3837 | 99,0% | |
| DNA 7 | S5 Plus | 635201 | 142 | 634226 | 92.1% | 13911 | 100% |
| Genexus | 1002231 | 92 | 946318 | 88.9% | 3150 | 98.9% | |
| DNA 8 | S5 Plus | 524182 | 131 | 523608 | 93.0% | 11591 | 100% |
| Genexus | 1262760 | 95 | 1208543 | 90.9% | 4176 | 98.9% | |
| DNA 9 | S5 Plus | 942781 | 161 | 940605 | 94.6% | 21192 | 100% |
| Genexus | 1791041 | 97 | 1756414 | 93,0% | 6097 | 97.9% | |
| DNA 10 | S5 Plus | 393979 | 126 | 393371 | 89.5% | 8381 | 100% |
| Genexus | 989635 | 60 | 717385 | 64.9% | 1459 | 98.9% | |
| DNA 11 | S5 Plus | 451494 | 139 | 450779 | 94.4% | 10127 | 100% |
| Genexus | 776893 | 78 | 679358 | 80.4% | 1863 | 96.7% | |
| DNA 12 | S5 Plus | 88915 | 129 | 88784 | 98.0% | 2072 | 92.9% |
| Genexus | 1297992 | 91 | 1263558 | 92.7% | 3996 | 93.9% | |
| DNA 13 | S5 Plus | 296845 | 143 | 296434 | 96.2% | 6790 | 100% |
| Genexus | 1196122 | 99 | 1174442 | 92.7% | 4258 | 98.5% | |
| DNA 14 | S5 Plus | 37206 | 133 | 37173 | 95.2% | 842,7 | 97.6% |
| Genexus | 1125616 | 97 | 1093531 | 91.8% | 3824 | 98.6% | |
| DNA 15 | S5 Plus | 782397 | 150 | 780894 | 95.2% | 17703 | 100% |
| Genexus | 1465786 | 92 | 1423741 | 91.9% | 4574 | 95.3% | |
| DNA 16 | S5 Plus | 378978 | 140 | 378373 | 93.3% | 8402 | 100% |
| Genexus | 1084647 | 87 | 1012693 | 87.6% | 3054 | 98.2% | |
| DNA 17 | S5 Plus | 520304 | 135 | 519653 | 91.5% | 11317 | 100% |
| Genexus | 1048030 | 98 | 1016324 | 91.4% | 3617 | 98.8% | |
| DNA 18 | S5 Plus | 49127 | 138 | 49055 | 95.3% | 1113 | 97.6% |
| Genexus | 1294194 | 97 | 1256161 | 91.9% | 4435 | 98.9% | |
| DNA 19 | S5 Plus | 486407 | 147 | 485652 | 96.6% | 11165 | 97.6% |
| Genexus | 1343529 | 97 | 1311776 | 92.3% | 4658 | 99.4% | |
| DNA 20 | S5 Plus | 346019 | 131 | 345464 | 97.4% | 8010 | 97.6% |
| Genexus | 974476 | 71 | 759420 | 75.7% | 2023 | 98.8% | |
| DNA 21 | S5 Plus | 67488 | 130 | 67417 | 95.9% | 1540 | 97.6% |
| Genexus | 1150249 | 90 | 1094010 | 90.3% | 3519 | 98.8% | |
| DNA 22 | S5 Plus | 52080 | 170 | 51956 | 90.4% | 1119 | 100% |
| Genexus | 1494337 | 100 | 1470085 | 92.3% | 5451 | 97.9% | |
| DNA 23 | S5 Plus | 614960 | 141 | 613813 | 96.2% | 14059 | 97.6% |
| Genexus | 1574234 | 91 | 1510266 | 91.2% | 4865 | 97.7% | |
| DNA 24 | S5 Plus | 188967 | 136 | 188623 | 98.1% | 4407 | 97.6% |
| Genexus | 1093646 | 103 | 1071141 | 92.2% | 4072 | 99.1% | |
| DNA 25 | S5 Plus | 140163 | 145 | 139930 | 95.5% | 3183 | 97.6% |
| Genexus | 949852 | 94 | 911448 | 90,0% | 3064 | 99.4% | |
| DNA 26 | S5 Plus | 40233 | 142 | 40180 | 96.7% | 925,4 | 97.6% |
| Genexus | 1497022 | 99 | 1476425 | 93.7% | 5365 | 98.3% | |
| DNA 27 | S5 Plus | 153378 | 133 | 153236 | 96.0% | 3501 | 97.6% |
| Genexus | 1059772 | 95 | 1021186 | 90.2% | 3498 | 98.7% | |
| DNA 28 | S5 Plus | 155154 | 118 | 154695 | 96.5% | 3553 | 92.8% |
| Genexus | 424900 | 75 | 365139 | 79.3% | 994 | 97.4% | |
| DNA 29 | S5 Plus | 358001 | 160 | 356995 | 95.2% | 8095 | 100% |
| Genexus | 1165795 | 98 | 1134969 | 92.2% | 4075 | 98.4% | |
| DNA 30 | S5 Plus | 275579 | 149 | 274340 | 98.4% | 6428 | 100% |
| Genexus | 1080846 | 92 | 1034348 | 90.3% | 3392 | 98.4% | |
| DNA 31 | S5 Plus | 259364 | 130 | 258623 | 92.6% | 5702 | 100% |
| Genexus | 1109488 | 92 | 1054465 | 89.9% | 3457 | 98.9% | |
| DNA 32 | S5 Plus | 263420 | 126 | 262682 | 93.4% | 5841 | 97.6% |
| Genexus | 710181 | 82 | 631880 | 82.5% | 1893 | 96.7% | |
*Same patient with different lesions. Abbreviations: DNA (Deoxyribonucleic Acid); ID (Identifier).
Table 4.
Comparison of DNA-related molecular alterations between S5 plus and Genexus platforms.
| ID | S5Plus (SiRe™ Panel) | Genexus (OPA Panel) |
|---|---|---|
| DNA 1* |
KRAS p.G12C 27.6% PIK3CA p.H1047R 35.0% |
KRAS p.G12C 32.9% PIK3CA p.H1047R 33.2% |
| DNA 2* |
KRAS p.G12C 37.2% PIK3CA p.H1047R 42.2% |
KRAS p.G12C 32.7% PIK3CA p.H1047R 36.4% |
| DNA 3 | KRAS p.G12D 20.7% | KRAS p.G12D 18.9% |
| DNA 4 | EGFR p.L858R 27.7% | EGFR p.L858R 18.9% |
| DNA 5 | KRAS p.G12V 34.5% | KRAS p.G12V 33.0% |
| DNA 6 | WT | WT |
| DNA 7 | KRAS p.G12D 57.2% | KRAS p.G12D 60.8% |
| DNA 8 | KRAS p.Q61K 16.8% | KRAS p.Q61K 19.3% |
| DNA 9 | WT | WT |
| DNA 10 | KRAS p.G12D 50.6% | KRAS p.G12D 55.3% |
| DNA 11 | c-KIT p.L576P 68.0% | c-KIT p.L576P 63.8% |
| DNA 12 | EGFR p.A767_V769dup 67.2% | EGFR p.A767_V769dup 72.8% |
| DNA 13 | WT | WT |
| DNA 14 | WT | WT |
| DNA 15 | BRAF p.K601E 16.3% | BRAF p.K601E 16.1% |
| DNA 16 |
KRAS p.G12D 9.3% KRAS p.G13D 14.1% |
KRAS p.G12D 8.2 KRAS p.G13D 12.1% |
| DNA 17 | KRAS p.Q61L 32.7% | KRAS p.Q61L 36.3% |
| DNA 18 | NRAS p.Q61K 19.3% | NRAS p.Q61K 18.2% |
| DNA 19 | PIK3CA E545K 0.8%** | PIK3CA E545K 7.2% |
| DNA 20 | BRAF p.V600E 30.5% | BRAF p.V600E 30.0% |
| DNA 21 | NRAS p.Q61K 46.7% | NRAS p.Q61K 36.2% |
| DNA 22 |
KRAS p.G13D 47.4%*** KRAS p.G13E 47.9%*** |
KRAS p.G13D 41.9%*** KRAS p.G13E 42.0%*** |
| DNA 23 | WT | WT |
| DNA 24 | KRAS p.A146T 30.80% | KRAS p.A146T 26.4% |
| DNA 25 | WT | WT |
| DNA 26 | BRAF p.V600E 27.3% | BRAF p.V600E 30.3% |
| DNA 27 | KRAS p.G13D 14.9% | KRAS p.G13D 12.2% |
| DNA 28 | NRAS p.Q61R 34.3% | NRAS p.Q61R 28.2% |
| DNA 29 |
EGFR p.L858R 9.7% EGFR p.T790M 9.5% |
EGFR p.L858R 9.3% EGFR p.T790M 11.0% |
| DNA 30 | WT | WT |
| DNA 31 |
KRAS p.G12V 51.2% PIK3CA p.E545K 32.2% |
KRAS p.G12V 59.2% PIK3CA p.E545K 31.0% |
| DNA 32 | WT | WT |
* Different lesion of same patient. ** Below 5%; *** Concominant SNV. Abbreviations: BRAF (Murine Sarcoma Viral Oncogene Homolog B); c-KIT (KIT Proto-Oncogene); DNA (Deoxyribonucleic Acid); EGFR (Epidermal Growth Factor Receptor); ID (Identifier); KRAS (Kirsten Rat Sarcoma Virus); PIK3CA (Phosphatidylinositol-4,5-Bisphosphate 3-Kinase, Catalytic Subunit Alpha); RAS (Rat Sarcoma Virus); WT (Wild-Type).
Table 5.
Expanded list of molecular alterations covered by OPA on Genexus platform.
| ID | Other Mutations (OPA Panel) |
|---|---|
| DNA 1* | MTOR p.R2217W 4.5% |
| DNA 2* |
TP53 p.G279E 4.8% TP53 p.V197M 4.0% |
| DNA 7 | TP53 p.H179Y 75.8% |
| DNA 9 | TP53 p.R273H 35.0% |
| DNA 12 | TP53 p.V197M 77.7% |
| DNA 14 | TP53 p.R273H 10.0% |
| DNA 16 |
CTNNB1 p.S45F 41.1% TP53 p.R175H 13.2% |
| DNA 18 | TP53 p.Y220C 19.7% |
| DNA 19 | TP53 p.L194F 9.9% |
| DNA 20 | TP53 p.P151S 54.7% |
| DNA 21 | TP53 p.K132R 51.4% |
| DNA 23 | TP53 p.C238S 25.3% |
| DNA 27 | CTNNB1 p.S45F 21.8% |
| DNA 30 | TP53 p.H179Y 24.6% |
| DNA 31 | TP53 p.Y220C 56.1% |
| DNA 32 | TP53 p.E285K 4.8% |
*Same patient, different lesion. Abbreviations: CTNNB1 (Catenin Beta 1); DNA (Deoxyribonucleic Acid); ID (Identifier); MTOR (Mammalian Target Of Rapamycin); TP53 (Tumor Protein P53).
Table 6.
Technical parameters from RNA-based analysis by using S5 plus and Genexus systems.
| RNA analysis Technical Parameters - S5 Plus (SiRe Fusion Panel) vs Genexus (OPA Panel) | ||||
|---|---|---|---|---|
| ID | Platform | Total Reads | Mean Read Length | Mapped Reads |
| RNA 1 | S5 Plus | 503832 | 92 | 489474 |
| Genexus | 2355408 | 99 | 170105 | |
| RNA 2 | S5 Plus | 829380 | 124 | 823978 |
| Genexus | 1748261 | 99 | 140327 | |
| RNA 3 | S5 Plus | 641591 | 89 | 348169 |
| Genexus | 2462555 | 104 | 54529 | |
| RNA 4 | S5 Plus | 254394 | 93 | 242076 |
| Genexus | 1667488 | 100 | 37387 | |
| RNA 5 | S5 Plus | 234803 | 67 | 176276 |
| Genexus | 1755508 | 91 | 111713 | |
| RNA 6 | S5 Plus | 357284 | 89 | 319350 |
| Genexus | 1542252 | 101 | 72995 | |
| RNA 7 | S5 Plus | 1070656 | 111 | 1067615 |
| Genexus | 1571469 | 100 | 150711 | |
| RNA 8 | S5 Plus | 535701 | 103 | 526127 |
| Genexus | 1737696 | 96 | 1029745 | |
| RNA 9 | S5 Plus | 494550 | 87 | 421901 |
| Genexus | 1634624 | 103 | 72104 | |
| RNA 10 | S5 Plus | 161964 | 100 | 153003 |
| Genexus | 1815512 | 96 | 51505 | |
| RNA 11 | S5 Plus | 190170 | 98 | 187044 |
| Genexus | 1597727 | 98 | 386493 | |
| RNA 12 | S5 Plus | 677654 | 91 | 513093 |
| Genexus | 1554237 | 101 | 171919 | |
| RNA 13 | S5 Plus | 765186 | 129 | 753177 |
| Genexus | 1777747 | 100 | 178846 | |
| RNA 14 | S5 Plus | 222717 | 103 | 217972 |
| Genexus | 1503566 | 102 | 48005 | |
| RNA 15 | S5 Plus | 490208 | 125 | 483482 |
| Genexus | 1523971 | 99 | 61024 | |
| RNA 16 | S5 Plus | 20405 | 91 | 17060 |
| Genexus | 1878041 | 97 | 42572 | |
| RNA 17 | S5 Plus | 367743 | 117 | 346142 |
| Genexus | 1769313 | 97 | 80920 | |
| RNA 18 | S5 Plus | 191027 | 99 | 189336 |
| Genexus | 1513615 | 97 | 365130 | |
| RNA 19 | S5 Plus | 240954 | 126 | 239481 |
| Genexus | 1744270 | 100 | 133226 | |
| RNA 20 | S5 Plus | 203214 | 86 | 195547 |
| Genexus | 1284559 | 94 | 173554 | |
| RNA 21 | S5 Plus | 195912 | 91 | 185689 |
| Genexus | 1940917 | 96 | 60947 | |
| RNA 22 | S5 Plus | 464854 | 119 | 462638 |
| Genexus | 1715374 | 98 | 294552 | |
| RNA 23 | S5 Plus | 258734 | 93 | 251939 |
| Genexus | 1644449 | 99 | 141394 | |
| RNA 24 | S5 Plus | 287598 | 104 | 284682 |
| Genexus | 1573653 | 103 | 68184 | |
| RNA 25 | S5 Plus | 297871 | 114 | 294124 |
| Genexus | 1587686 | 99 | 111160 | |
| RNA 26 | S5 Plus | 428858 | 118 | 426903 |
| Genexus | 1682103 | 100 | 185977 | |
| RNA 27 | S5 Plus | 173120 | 98 | 171187 |
| Genexus | 1471817 | 98 | 252247 | |
| RNA 28 | S5 Plus | 187176 | 145 | 185591 |
| Genexus | 1903859 | 98 | 126388 | |
| RNA 29 | S5 Plus | 311784 | 84 | 262726 |
| Genexus | 1839064 | 102 | 45998 | |
| RNA 30 | S5 Plus | 416422 | 93 | 393110 |
| Genexus | 1727113 | 101 | 57972 | |
| RNA 31 | S5 Plus | 240891 | 112 | 239186 |
| Genexus | 1598494 | 99 | 133522 | |
| RNA 32 | S5 Plus | 156106 | 63 | 97917 |
| Genexus | 1965363 | 93 | 52222 | |
Abbreviations: ID (Identifier); RNA (Ribonucleic Acid).
Table 7.
Comparison of RNA-related molecular alterations between S5 plus and Genexus platforms.
| ID | S5Plus (SiRe Fusion Panel) | Genexus (OPA Panel) |
|---|---|---|
| RNA 1 | No Fusion | NTRK3 (ex14) - KANK1 (ex3) 1571 reads * |
| RNA 2 | No Fusion | No Fusion |
| RNA 3 | No Fusion | No Fusion |
| RNA 4 | No Fusion | No Fusion |
| RNA 5 | No Fusion | No Fusion |
| RNA 6 | No Fusion | No Fusion |
| RNA 7 | ALK (ex20) - EML4 (ex6) 601 reads | ALK (ex20) - EML4 (ex6) 353 reads |
| RNA 8 | No Fusion | No Fusion |
| RNA 9 | No Fusion | No Fusion |
| RNA 10 | No Fusion | No Fusion |
| RNA 11 | No Fusion | No Fusion |
| RNA 12 | No Fusion | No Fusion |
| RNA 13 | ALK (ex20) - unknown partner 149 reads | ALK (ex20) - DCTN1 (ex26) 2268 reads |
| RNA 14 | No Fusion | No Fusion |
| RNA 15 | No Fusion | No Fusion |
| RNA 16 | No Fusion | No Fusion |
| RNA 17 | No Fusion | No Fusion |
| RNA 18 | No Fusion | No Fusion |
| RNA 19 | ROS1 (ex34) - CD74 (ex6) 2208 reads | ROS1 (ex34) - CD74 (ex6) 1992 reads |
| RNA 20 | ALK (ex20) - EML4 (ex6) 43 reads | ALK (ex20) - EML4 (ex6) 1040 reads |
| RNA 21 | No Fusion | No Fusion |
| RNA 22 | ALK (ex20) - EML4 (ex13) 11335 reads | ALK (ex20) - EML4 (ex13) 7212 reads |
| RNA 23 | No Fusion | No Fusion |
| RNA 24 | RET (ex12) - KIF5B (ex15) 4063 reads | RET (ex12) - KIF5B (ex15) 2417 reads |
| RNA 25 | No Fusion | MET (ex13) - MET (ex15) 9638 reads |
| RNA 26 | No Fusion | No Fusion |
| RNA 27 | No Fusion | No Fusion |
| RNA 28 | ALK (ex20) - EML4 (ex20) 6293 reads | ALK (ex20) - EML4 (ex20) 1140 reads |
| RNA 29 | No Fusion | No Fusion |
| RNA 30 | No Fusion | No Fusion |
| RNA 31 | No Fusion | No Fusion |
| RNA 32 | RET (ex12) - CCDC6 (ex1) 494 reads | RET (ex12) - CCDC6 (ex1) 172 reads |
*Not covered from SiRe Fusion Panel. Abbreviations: ALK (Anaplastic Lymphoma Kinase); CCDC6 (Coiled-Coil Domain-Containing Protein 6); CD74 (HLA Class II Histocompatibility Antigen Gamma Chain); DCTN1 (Dynactin Subunit 1); EML4 (Echinoderm Microtubule-Associated Protein-Like 4); EX (Exon); ID (Identifier); KANK1 (KN Motif And Ankyrin Repeat Domains 1); KIF5B (Kinesin Family Member 5B); MET (Tyrosine-Protein Kinase Met); NTRK (Neurotrophic Tyrosine Receptor Kinase); RET (RET Proto-Oncogene); RNA (Ribonucleic Acid); ROS1 (Proto-Oncogene Tyrosine-Protein Kinase ROS).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



