
Submitted:
27 September 2023
Posted:
29 September 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The sustainable management of public hospitals is usually threatened by long-period operating deficit, especially during the pandemic of COVID-19. This study aims at quantitatively decomposing the historical changes in the annual operating costs of public hospitals in Japan to identify the main driving forces responsible for a worsening imbalance between operating costs and income over the past two decades. A dataset of the annual operating costs of public hospitals in Japan is compiled, in which influencing factors are redefined to make the data amenable to the application of a decomposition method referred to as the Logarithmic Mean Divisia Index (LMDI). Using the LMDI method, the contribution of each influencing factor to the changes in public hospital operating costs was quantitatively determined. The results indicate an overall positive effect arising out of the national reform of public hospitals that aimed to reduce the operating costs of these institutions, but the rapid increase in the prices of medicines in recent years made a major contribution to the increasing operating costs. The pandemic reveals a damage on public hospitals’ financial balance but the city-wide lockdown offset part of the increased medical expense. Both long-term and short-term pricing policies are required for the sustainable management of public hospitals.
Keywords:
factor decomposition
; operating costs
; hospital management
; COVID-19
; Japan
1. Introduction
A high quality and cost effective healthcare service is a critical target in the management of public hospitals, which represent the largest portion of total health spending in most countries. Especially during the COVID-19 pandemic, people falling sick in large numbers resulted in patients being rushed to public hospitals, immediately causing overcapacity problems with serious resource and economic costs as a consequence 1,2. To increase the cost effectiveness of public hospitals, the national governments formulated and implemented various reform plans such as developing an hierarchical medical system, incorporating public hospitals, introducing private capital and more efficient management systems, introducing a prospective payment system, implementing public reporting for price transparency, and even allowing market competition in a bid to suppress operating costs 3-8. Although various analysis tools, such as data envelope analysis, regression models, and time series analysis, have been applied to evaluate the improvements in efficiency at public hospitals after institutional reform, the results are variable and not intuitional enough to identify the key influencing factors that significantly affect the operating effectiveness of these institutions 5,9-12.
Japan’s public hospitals generally succeeded in supporting a higher quality healthcare service with lower operating costs compared to other developed countries, but they were still facing the problem of long-term financial deficits, which in turn became an additional risk factor in the national fiscal crisis 13. As Japan turns into an ageing society with a falling population, an increasing number of hospitals are facing the risks attendant on a continuously worsening financial balance brought about by an inverted population pyramid, making these hospitals vulnerable to bankruptcy in the face of socioeconomic crises or pandemic diseases. As shown in Figure 1, from 1996 to the present, the ratio of annual income to operating costs of public hospitals in Japan was always below 100%. Even though it jumped to above 92% from 2008 and remained stable for 4 years, during the other periods there was a consistent decreasing trend that remains a critical issue threatening the financial system, particularly the worst result was recorded during the pandemic of COVID-19. Despite the fact that most public hospitals carrying a deficit can continue to function for a long time due to the financial support from the government, they must implement an action plan to improve the financial balance. Meanwhile, the government has revised its guideline on hospital management to cut the amount of subsidies given to the medical system.
To suppress the financial deficit ratios, in 2007, the Japanese government formulated a guideline for the institutional reform of public hospitals and a new updated guideline was issued in 2015. The former reform plan emphasized setting numerical targets with the aim of increasing operating efficiency, restructuring and networking public hospitals including adjusting the number of doctors and beds, and resetting the operational status of public hospitals such as by privatization. In contrast, the updated 2015 reform plan emphasized flexibly setting targets to improve operating efficiency considering the quality of the healthcare service, identifying the role of public hospitals in local healthcare initiatives, adjusting hospital taxation that takes into account the actual bed occupancy rate, and strengthening financial support to restructure and network public hospitals, among other initiatives 14. According to the statistical reports on the operational status of public hospitals, both the annual operating costs and income per hospital began to increase after the introduction of the 2007 reform plan, where the driving forces for this trend appear to be the cost of salaries and other incidental costs, as shown in Figure 2 15. However, this result cannot explain how the internal and external factors had an influence on the changes in operating costs. Without a quantitative analysis to identify the driving forces from various influencing factors, it is difficult for the government and hospitals to formulate specific action plans to counter the expanding financial deficit.
Many previous studies tried to quantitatively identify the driving forces which may significantly push a hospital into either a surplus or deficit, but generally the research results are so inconsistent that a definitive conclusion cannot be reached (Table 1). For example, Taniguchi, et al. 16 applied risk factor analysis to hospitals in a management status survey during the 1990s. They identified the number of outpatients, salary costs, material costs and medical material costs as the main factors influencing whether a hospital had a surplus of funds. Similarly, Shimomura and Kubo 17 compared the cost structure of 57 hospitals that made a surplus and 44 hospitals that made a loss by regression analysis using financial statement data obtained from the National Hospital Organization. The study indicates that medical material costs, salary costs, insurance assessment, equipment-related costs, depreciation costs, etc., are much higher in the group of hospitals that made a loss than in the profitable hospital group. However, Ishikawa 18 applied a multiple linear regression analysis to cost structure changes of 569 public hospitals before/after public hospital reform. The analysis revealed that outpatients and average stay in hospital have positive effects on hospital management, while the effects from material costs and salary costs on hospital deficit were not significant. Furthermore, Ishibashi 19 also applied a multiple regression analysis to 726 municipal public hospitals in the reform plan years 2008 and 2013. He found that factors such as money transferred from other accounts, inpatient unit price, average daily number of inpatients, and outpatient unit price have a positive effect on hospital profit, while factors such as interest on revenue bonds, retirement payments, depreciation costs, and asset shrinkage have a negative effect. Other factors, such as average daily number of outpatients, average inpatient days, and average salary of regular staff do not significantly affect the income-expenditure balance. In other cases, a multiple regression analysis performed by Otsubo and Imanaka 20 indicates that outpatient number and inpatient unit price have a positive effect on hospital profit while salary costs do not have a significant effect. Meanwhile, cluster analysis by Kawaguchi 21 confirmed again that salary costs and the proportion of material costs to hospital profit are the main factors having a negative influence on hospital profit. The reasons why the results are inconsistent may be attributed to the following. First, the variables chosen in previous studies are not unified. Some decomposed the costs into more items while some considered fewer, so that the variables are not unified either in total or on average. Second, the interaction between variables is complex with both synergies and trade-offs. For example, longer inpatient stays may generate more profit but decrease the total number of inpatients hospitalized. Third, the degree to which variables have an influence may change considerably during the period of public hospital reform in response to the government’s guideline.
Although the correlation analysis referred to above can identify the main influencing factors and their relative influencing intensity on a hospital’s deficit, too many variables make it difficult to ascertain which variables interact with each other, while at the same time it cannot easily identify which factors act as the forces driving the operating costs of public hospitals. Beyond these approaches, decomposition methods, such as Logarithmic Mean Divisia Index (LMDI), make it possible to extract the driving forces from various internal and external factors to an aggregate indicator, if the indicator is defined as the product of such factors. Since the LMDI method can completely decompose the changes of an overall indicator into the contributions of influencing factors, it has become a commonly used decomposition method which is often applied to analyzing the driving forces behind carbon emissions and energy consumption of a city, region, country, or sector. For instance, in terms of energy consumption, it is usually decomposed into the contributions from population, income, energy mix, and energy intensity 22-24. In terms of carbon emissions, the indicator is usually decomposed into the contributions from economic growth, industrial structure, energy mix, energy intensity, and emission factor 25-28. In terms of the transportation sector’s carbon emissions and energy consumption, it is usually decomposed into the contributions from population, income, traffic activity intensity, modal shift, each mode’s carbon emission factor/energy intensity 24,29,30. The LMDI method is also applied to other fields in decomposition studies, but as the authors knew, this method had never formerly been used for analyzing changes in a hospital’s overall financial performance. Compared to regression analysis, the LMDI method may mask some of the complex interactions between influencing factors, but can immediately reveal the structural changes between influencing factors before and after institutional reform, and during the pandemic of COVID-19.
This study aims at quantitatively decomposing the historical changes in the annual operating costs of public hospitals in Japan to identify the main forces responsible for driving the worsening imbalance between operating costs and income over the preceding two decades. This will not only provide further evidence that can be used to evaluate the effectiveness of the recent institutional reform of the public healthcare system, but also provide an overarching perspective of the impacts arising out of the socio-economic changes to the operation of public hospitals that will in turn support further policy making. In addition, as this is the first time the LMDI method has been applied to the field of healthcare, this study also provides a reference for the academic community to broaden the scope of research in this area.
The rest of this paper is organized as follows: Section 2 describes the process of data collection and model development, Section 3 summarizes the decomposition results on operation costs of public hospitals along with some discussion, Section 4 presents the main findings from the study and their policy implications.
2. Model development
2.1. Definition of indicators
Regarding the calculation process employed in decomposition by the LMDI method, Ang 31 supported a practical guideline, while the data preparation and model development for applying the LMDI method refers back to several previous studies in the field of energy consumption and carbon emissions, as mentioned before. The basic preparation for LMDI decomposition is to establish an aggregate formula of the influencing factors contributing to the changes in the aggregate indicator. In this study, the aggregate is the total operating costs of public hospitals in Japan, and the influencing factors are defined as summarized in the Table 2:
Accordingly, the operating cost of one public hospital can be aggregated as the following equation (1):
Here, population is a kind of total indicator, while average income, consultation rate, and visit duration for a single consultation are the factors influencing the level of demand for medical consultations, the coverage of public hospitals for medical consultations means the service level of public hospitals, and each term of operating cost points to the management cost of public hospitals in providing medical consultations for the public.
2.2. Decomposition by LMDI method
According to the definition of the aggregate indicator and influencing factors mentioned above, the annual changes in the indicator (operating cost) can be calculated as the sum of the contribution of each influencing factor, as the following equation (2):

Table 3.
The contribution from each influencing factor to the total operating cost.
| Item | Definition |
|---|---|
| Annual changes in total operating cost of one public hospital (JPY) | |
| Annual contribution from population changes in Japan to the operating cost of one public hospital (JPY) | |
| Annual contribution from income level changes to the operating cost of one public hospital (JPY) | |
| Annual contribution from consultation rate changes to the operating cost of one public hospital (JPY) | |
| Annual contribution from the changes in patient visit duration to the operating cost of one public hospital (JPY) | |
| Annual contribution from the structural changes and cost-efficiency management level to the operating cost of one public hospital (JPY) |
Next, the annual contribution of each influencing factor can be calculated by the following equation (3)-(8):
The index decomposition calculation is general to any situation if the aggregate can be defined as the product of all the influencing factors.
2.3. Data preparation
To apply LMDI decomposition to the operating costs defined as above, part of the necessary data is obtained from statistics reports while the other parts are estimated from reliable statistics from other sources. In this study, the population and income data are obtained from the national annual statistics of Japan, while the overall indicators, such as consultation times of inpatients and outpatients, are obtained from the Survey of Medical Institutions issued by the Ministry of Health, Labour and Welfare 32, and the data on public hospitals are obtained from the Yearbook of Local Public Enterprises published by the Ministry of Internal Affairs and Communications 15. As summarized in the Table 4, the data of influencing factors defined in this study are prepared from the relevant statistical data.
3. Results and discussion
3.1. Historical changes in influencing factors
According to the model development mentioned above, the operating costs of a public hospital were decomposed into the product of several influencing factors, as shown in Table 5. First, it is clear that the population of Japan continued to increase to reach 128.1 million by 2010 but then began to decrease from that point on. In contrast, annual income per capita showed an overall decreasing trend up until 2009 but then began to increase after that. Second, the consultation rate by annual income per capita revealed an amazing 32% decrease from 1996 to 2021. This may be attributable to the continuous improvement in public health and the effects arising out of the implementation of an hierarchical medical system. This trend was also reflected in the changes in the coverage of one public hospital as a proportion of total medical consultations, where the coverage peaked in 2000 then began to decrease to some extent. In addition, the visit duration for a single medical consultation to a public hospital revealed an increase from 2000 that may also be caused by the hierarchical medical system where public hospitals were more focused on treating critical patients. From these factors, after 2000, the public hospital system became more concentrated on a regional scale and also became more effective in the area of critical medical care compared to other hospitals.
However, the various costs per one patient during his/her one-day stay in a public hospital showed a continuous increase in recent years, in particular, the salary cost doubled during the period from 1996-2021. Although the depreciation cost and other costs were not the largest contributors to the total operating cost, the rate of increase remained the same as that for salary cost. These changes may be caused by the reform of public hospitals whereby they became more focused on dealing with critical patients who need higher-level medical treatment. Interestingly, only the medicine cost initially kept decreasing until 2009 then began to increase so that it finally reached the same level in 2019 that it was in 1996. During this period Japan made several adjustments to the medicine price system, but clearly the exchange rate for the JPY was always a critical factor influencing the price of medicines. In fact, the changes in medicine price were in a converse relationship to the variations in the exchange rate of the JPY to the USD from 1996-2019. According to the Trade Statistics of Japan issued by the Ministry of Finance, Japan’s importation of medicines had surpassed exports for decades, particularly after the COVID-19 pandemic 33. In 2021, the value of Japan’s imported medicines reached 31 billion USD, which is 5 times the export value. In another words, the medicine price seems to play an external role by affecting changes in the total operating cost of Japan’s public hospitals.
3.2. Contribution of influencing factors based on decomposition results
The decomposition results on the annual contribution of influencing factors are summarized in Figure 3. In general, the net changes in operating cost at one public hospital consistently showed an increasing trend from 1996, but the increase declined during the period 1996-2006, but then suddenly increased again from then on. From the decomposition of each influencing factor, it is obvious that the cost for a patient during a stay in hospital made the greatest contribution to the increase in total operating cost of one public hospital. This contribution includes 2 types of effects: one was from the overall increase in each branch of operating cost, and the other was because of a worsening cost structure in which the branch with the larger proportion of the total (salary cost) increased faster than the other branches with a smaller proportion. Annually, the rising cost contributed around 45 million JPY to the total operating cost.
In contrast, the contribution from the changing consultation rate by annual income generally remained negative so that it fell annually by around 30 million JPY as a proportion of total operating cost. However, obviously, this reduction was largely offset by the contribution from the changes in annual income per capita. During the entire period, visit duration for a single consultation continued to contribute around 10 million JPY annually to the total operating cost. Additionally, the coverage of one public hospital as a proportion of total yearly medical consultations contributed to some reduction in total operating cost before 2010, but stopped after that. The smallest contribution came from the changing population in Japan, so this contribution can be ignored in the short-and-medium-term analysis. Notably, the pandemic of COVID-19 beginning from the year 2020 revealed a significant shock on public hospitals’ financial balance, where the average cost for treating a patient immediately spouted but this increase was substantially offset by unemployment and lockdown (less patients went to the hospitals). Comparing the contributions among all influencing factors, it can be concluded that the increasing cost level and worsening cost structure was the main force driving the long-term increase in total operating cost in a public hospital, while the other influencing factors are almost all yearly variables that affected total operating cost in a single fiscal year.
3.3. Discussion
- Impact from the institutional integration of public hospitals
A broad institutional reconfiguration of public hospitals in Japan arose out of the national systemic reform of public hospitals in 2007. As shown in Figure 4, the number of public hospitals in Japan reached a peak of 1000 hospitals in 2002, with this number rapidly decreasing to 753 hospitals in 2021. Even though during these two decades, annually around 5 new hospitals were established, around 15 public hospitals were disestablished, incorporated, restructured, or assigned to private owners. Particularly, the institutional reform of public hospitals in 2007 redefined the importance of public hospitals to support regional medical systems in cooperation with private hospitals and clinics. Public hospitals with serious human resource shortages were downgraded to regional clinics while some others with financial problems were transferred into local incorporated administrative agencies that enabled them to source their own funds to allow ongoing operation. Due to the budget constraints on public hospitals during the COVID-19 pandemic, this trend in unlikely to change.
The institutional reform of public hospitals had significant effects on the service level and management of public hospitals in Japan. As summarized in Figure 5, one public hospital used to perform on an annual basis 0.024% of the total number of medical consultations for all hospitals in 2000, but the coverage began to decrease during the period of institutional reform of public hospitals. This was not only caused by the decrease in the number of public hospitals, but also their increased focus on caring for critical patients, indicated by the continuous increase in the average charge income for one patient during a consultation. From 1996 to 2021, the charge income level increased by 87.6%, which is a positive outcome and evidence that shows the success of the institutional reforms. Notably, in the beginning of COVID-19 pandemic in 2020, the coverage of a public hospital recorded the lowest rate because public hospitals became locations of cluster infection that many patients tried to avoid going to, or cannot go to public hospitals due to the city-wide lockdown and temporary regulation for public hospitals. In contrast, other local and private hospitals can function more normally than public hospitals.
- 2.
- Impact of a decreasing population and an ageing society
From 2010, Japan’s population began to decline with the advent of the super-ageing society. Will this trend have an impact on the total operating cost of public hospitals? According to the decomposition result shown in Figure 6, the impact is interesting. Although overall the increase in income level made a negative contribution to the decrease in operating cost, the contribution from consultation rate by income always offset the former. It can be concluded that people increasingly went to hospitals less frequently in last two decades, perhaps as a result of a continuous improvement in public health. In general, income level seems to be an intermediate indicator, which may not have an obvious effect on the operating cost level. The situation in the year 2020 was an exception that both unemployment and lockdown happened to dramatically influence on the operation cost of a public hospital.
- 3.
- Operating cost level changes compared with charge income level
Both in terms of the overall socioeconomic situation and demand-side changes, the decomposition results indicate a positive trend in reducing the total operating cost in a public hospital, while the operating cost level increase was found to be the main force driving the increase in total operating cost. Over the last two decades, what happened to the level of operating cost? As can be seen from Table 5, salary cost represents around half of the total operating cost and has maintained a rapid and consistent increase in the preceding decades. However, by comparing the change rate of various costs to the charge income per person·day (Figure 7), it can be seen that the changes in charge income level are closely correlated with the increases in salary cost. In addition, material cost, depreciation cost, and other incidental costs were also generally following the same path of annual changes as charge income. The only mismatch was with the medicine cost, which apparently increased more slowly than the charge income level before 2010, but gradually increased more rapidly than the latter from that point on. As already mentioned, this may be caused by the monetary easing policy and the devaluation of the JPY from the year 2010. Notably, due to the pandemic of COVID-19, salary cost and material cost immediately increased while medicine cost decelerated its path of increase. It is not clear why the depreciation cost suddenly increased in year 2014, but generally it was suppressed from making a contribution to the increase in total operating cost.
4. Conclusions
The increase in operating costs against charge income is a critical problem for the financial management of public hospitals in Japan. To quantitatively identify the forces driving the increase in operating costs in recent decades, this study conducted a complete decomposition analysis of public hospital’s operating costs using the LMDI method with a corresponding definition of the influencing factors based on statistical data covering the period 1996-2021. The results indicate that the continuously increasing level of various operating costs and a worsening cost structure played key roles in increasing the total operating costs rather than the charge income. In particular, the continuous rise of medicine cost caused by monetary easing and currency devaluation was a danger signal for public hospitals’ financial status. However, the results also affirmed the positive effect of the institutional reform on the public hospital system in recent decades, through which the hierarchical medical system of public hospitals became more focused on caring for critical patients, which increased the efficiency of operating costs to charge income. The pandemic of COVID-19 revealed a short-term shock on public hospital’s financial balance in the beginning year, but the situation seems to return to normal later. Therefore, in summary, the continuous rise of medicine cost, which was not well reflected in the level of medical charges, was the main reason for the long-term operating deficit of public hospitals in Japan.
Learning from these findings, policy makers should pay more attention to medicine cost management during medical treatment. It may be difficult to reduce the amount of medicine prescribed due to the focus on critical patients, but increasing the proportion of domestic medicine production can contribute partially to stabilizing the variations in material and medicine prices arising from external factors. As experienced during the COVID-19 pandemic, the prices of masks and disinfectant increased immediately to become several times higher than they were before, which had a major impact on the financial balance of public hospitals during that time. Short-term subsidies can fill part of the gap between a hospital’s income and costs but cannot essentially solve the long-term imbalance between these factors. With the ongoing institutional reform of public hospitals, a strategic national plan on building a stable medicine supply chain is also indispensable.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, Kiyotoshi Kou and Yi Dou; methodology, Kiyotoshi Kou; software, Kiyotoshi Kou; validation, Kiyotoshi Kou; formal analysis, Kiyotoshi Kou; investigation, Kiyotoshi Kou; resources, Kiyotoshi Kou and Yi Dou; data curation, Kiyotoshi Kou and Yi Dou; writing—original draft preparation, Kiyotoshi Kou; writing—review and editing, Yi Dou; visualization, Kiyotoshi Kou; supervision, Ichiro Arai and Yi Dou; project administration, Ichiro Arai; funding acquisition, Ichiro Arai. All authors have read and agreed to the published version of the manuscript.
Funding
This work was financially supported by MEXT/JSPS KAKENHI Grant Number 21K14276.
Data Availability Statement
Data are possible to be shared if required.
Acknowledgments
This work was conducted in collaboration with Japan Kampo Inc.and PHT Inc., both of which provided great support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Cai, Y. et al. Impact of the COVID-19 pandemic on a tertiary care public hospital in Singapore: resources and economic costs. J Hosp Infect 121, 1-8 (2022). [CrossRef]
- Chen, Y. Q., Cai, M., Li, Z. P., Lin, X. J. & Wang, L. A. Impacts of the COVID-19 Pandemic on Public Hospitals of Different Levels: Six-Month Evidence from Shanghai, China. Risk Manag Healthc P 14, 3635-3651 (2021). [CrossRef]
- Barber, S. L., Borowitz, M., Bekedam, H. & Ma, J. The hospital of the future in China: China's reform of public hospitals and trends from industrialized countries. Health Policy Plann 29, 367-378 (2014). [CrossRef]
- Fidler, A. H., Haslinger, R. R., Hofmarcher, M. M., Jesse, M. & Palu, T. Incorporation of public hospitals: A "silver bullet" against overcapacity, managerial bottlenecks and resource constraints? Case studies from Austria and Estonia. Health Policy 81, 328-338 (2007). [CrossRef]
- Besstremyannaya, G. The Impact of Japanese Hospital Financing Reform on Hospital Efficiency: A Difference-in-Difference Approach. Jpn Econ Rev 64, 337-362 (2013). [CrossRef]
- Han, A., Lee, K. H. & Park, J. The impact of price transparency and competition on hospital costs: a research on all-payer claims databases. Bmc Health Serv Res 22 (2022). [CrossRef]
- Liu, P. C., Gong, X., Yao, Q. H. & Liu, Q. Impacts of the medical arms race on medical expenses: a public hospital-based study in Shenzhen, China, during 2009-2013. Cost Effect Resour A 20 (2022). [CrossRef]
- Ramamonjiarivelo, Z. et al. Public hospitals in financial distress: Is privatization a strategic choice? Health Care Manage R 40, 337-347 (2015). [CrossRef]
- Hunt, D. J. & Link, C. R. Better outcomes at lower costs? The effect of public health expenditures on hospital efficiency. Appl Econ 52, 400-414 (2020). [CrossRef]
- Fragkiadakis, G., Doumpos, M., Zopounidis, C. & Germain, C. Operational and economic efficiency analysis of public hospitals in Greece. Ann Oper Res 247, 787-806 (2016). [CrossRef]
- Kawaguchi, H., Tone, K. & Tsutsui, M. Estimation of the efficiency of Japanese hospitals using a dynamic and network data envelopment analysis model. Health Care Manag Sc 17, 101-112 (2014). [CrossRef]
- Liu, M. L., Jia, M. Y., Lin, Q., Zhu, J. W. & Wang, D. Effects of Chinese medical pricing reform on the structure of hospital revenue and healthcare expenditure in county hospital: an interrupted time series analysis. Bmc Health Serv Res 21 (2021). [CrossRef]
- Hashimoto, H. et al. Japan: Universal Health Care at 50 years 3 Cost containment and quality of care in Japan: is there a trade-off? Lancet 378, 1174-1182 (2011). [CrossRef]
- Iseki, T. Recent Municipal Hospital Policy Transition and Municipal Hospital Reform Guidelines (in Japanese). Journal of Social Security Research 1, 778-796 (2017).
- .
- Taniguchi, K., Nozawa, R., Koike, D., Ninomiya, T. & Ueda, S. Risk factors analysis of hospital management which points to extract part system. Kawasaki Journal of Medical Welfare 14, 109-123 (2004).
- Shimomura, K. & Kubo, R. Quantitative Analysis of Cost Structures in Hospital Management --Comparison between groups of surplus and deficit hospitals belonging to the National Hospital Organization--. Journal of the Japan Society for Healthcare Administration 48, 129-136 (2011). [CrossRef]
- Ishikawa, M. Factor Analyses Regarding Transition in Hospital Profit Before and After Public Hospital Reform at Public Hospitals Mainly Providing Acute Medical Services. Journal of Japanese Association for Health Care Administrators 13, 11-17 (2019). [CrossRef]
- Ishibashi, K. Factors influencing the optimization of management in the public hospital reform plan─Focusing on hospitals directly managed by local governments. Journal of the Japan Society for Healthcare Administration 53, 7-18 (2016). [CrossRef]
- Otsubo, T. & Imanaka, Y. Determinants of change in the revenue to cost ratio of municipal hospitals by scale in Japan. Nihon Koshu Eisei Zasshi(JAPANESE JOURNAL OF PUBLIC HEALTH) 55, 761-767 (2008). [CrossRef]
- Kawaguchi, H. Study for Development of a Benchmarking Method in Hospital Management Using a Multivariate Statistical Technique subtitle_in_Japanese. Iryo To Shakai 15, 2_23-22_37 (2005). [CrossRef]
- Zhang, M. & Guo, F. Y. Analysis of rural residential commercial energy consumption in China. Energy 52, 222-229 (2013). [CrossRef]
- Gonzalez, P. F., Landajo, M. & Presno, M. J. Multilevel LMDI decomposition of changes in aggregate energy consumption. A cross country analysis in the EU-27. Energ Policy 68, 576-584 (2014). [CrossRef]
- Goh, T. & Ang, B. W. Tracking economy-wide energy efficiency using LMDI: approach and practices. Energ Effic 12, 829-847 (2018). [CrossRef]
- Xu, S. C., He, Z. X. & Long, R. Y. Factors that influence carbon emissions due to energy consumption in China: Decomposition analysis using LMDI. Appl Energ 127, 182-193 (2014). [CrossRef]
- Luo, X. et al. Regional disparity analysis of Chinese freight transport CO2 emissions from 1990 to 2007: Driving forces and policy challenges. J Transp Geogr 56, 1-14 (2016). [CrossRef]
- Yu, Y. & Kong, Q. Y. Analysis on the influencing factors of carbon emissions from energy consumption in China based on LMDI method. Nat Hazards 88, 1691-1707 (2017). [CrossRef]
- Moutinho, V., Moreira, A. C. & Silva, P. M. The driving forces of change in energy-related CO2 emissions in Eastern, Western, Northern and Southern Europe: The LMDI approach to decomposition analysis. Renew Sust Energ Rev 50, 1485-1499 (2015). [CrossRef]
- Zhang, M., Li, H. A., Zhou, M. & Mu, H. L. Decomposition analysis of energy consumption in Chinese transportation sector. Appl Energ 88, 2279-2285 (2011). [CrossRef]
- Luo, X. et al. Factor decomposition analysis and causal mechanism investigation on urban transport CO2 emissions: Comparative study on Shanghai and Tokyo. Energ Policy 107, 658-668 (2017). [CrossRef]
- Ang, B. W. The LMDI approach to decomposition analysis: a practical guide. Energ Policy 33, 867-871 (2005). [CrossRef]
- MHLWJ. Survey of Medical Institutions. (The Ministry of Health, Labor, and Welfare of Japan (MHLWJ), Tokyo, Japan, 1996-2021).
- MOF. Trade Statistics of Japan. (Ministry of Finance (MOF), Tokyo, Japan, 2022).
Figure 1.
Total operating costs and income of public hospitals in Japan during 1996-2021.
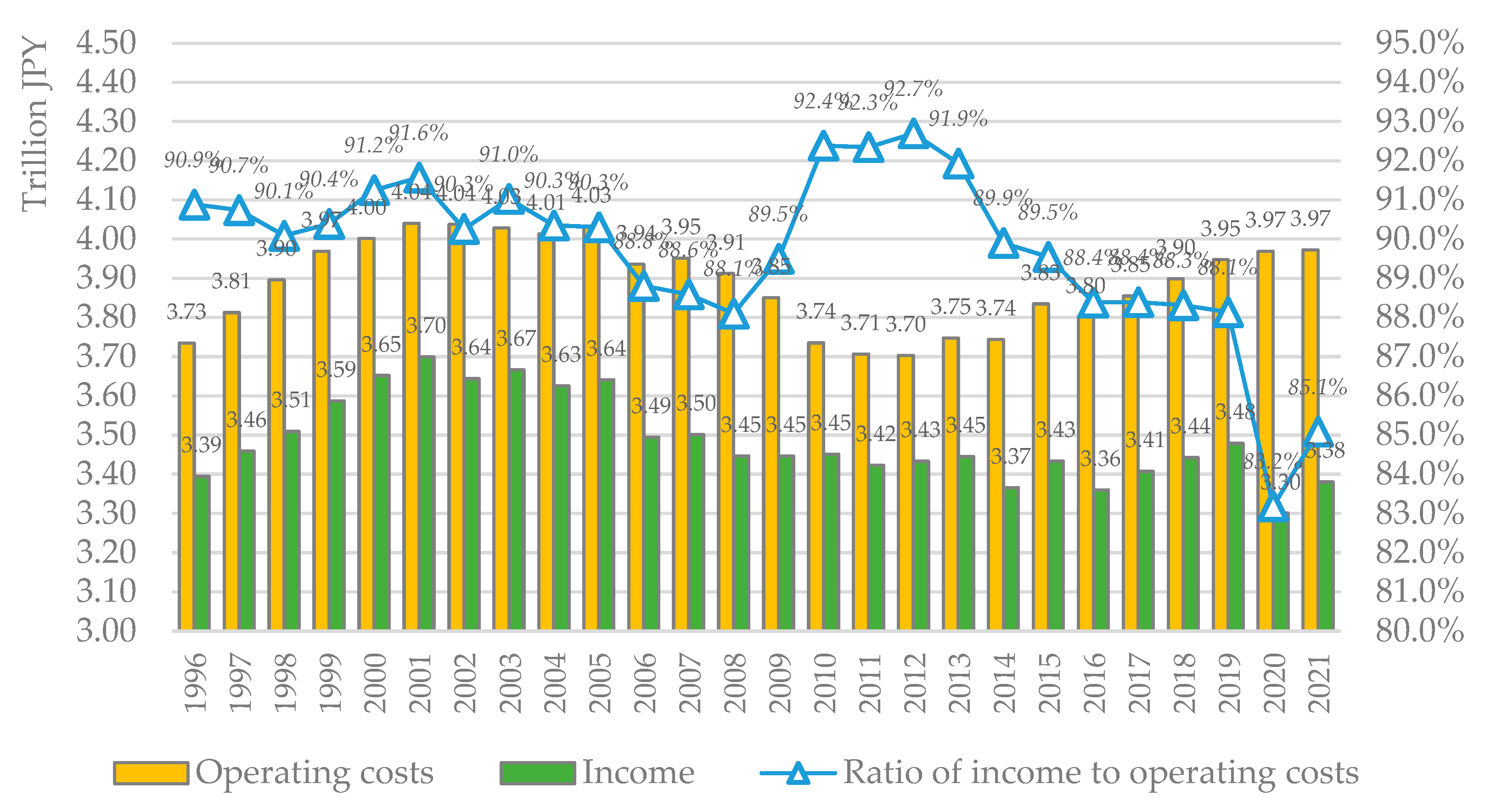
Figure 2.
Average operating costs and income of a public hospital in Japan.
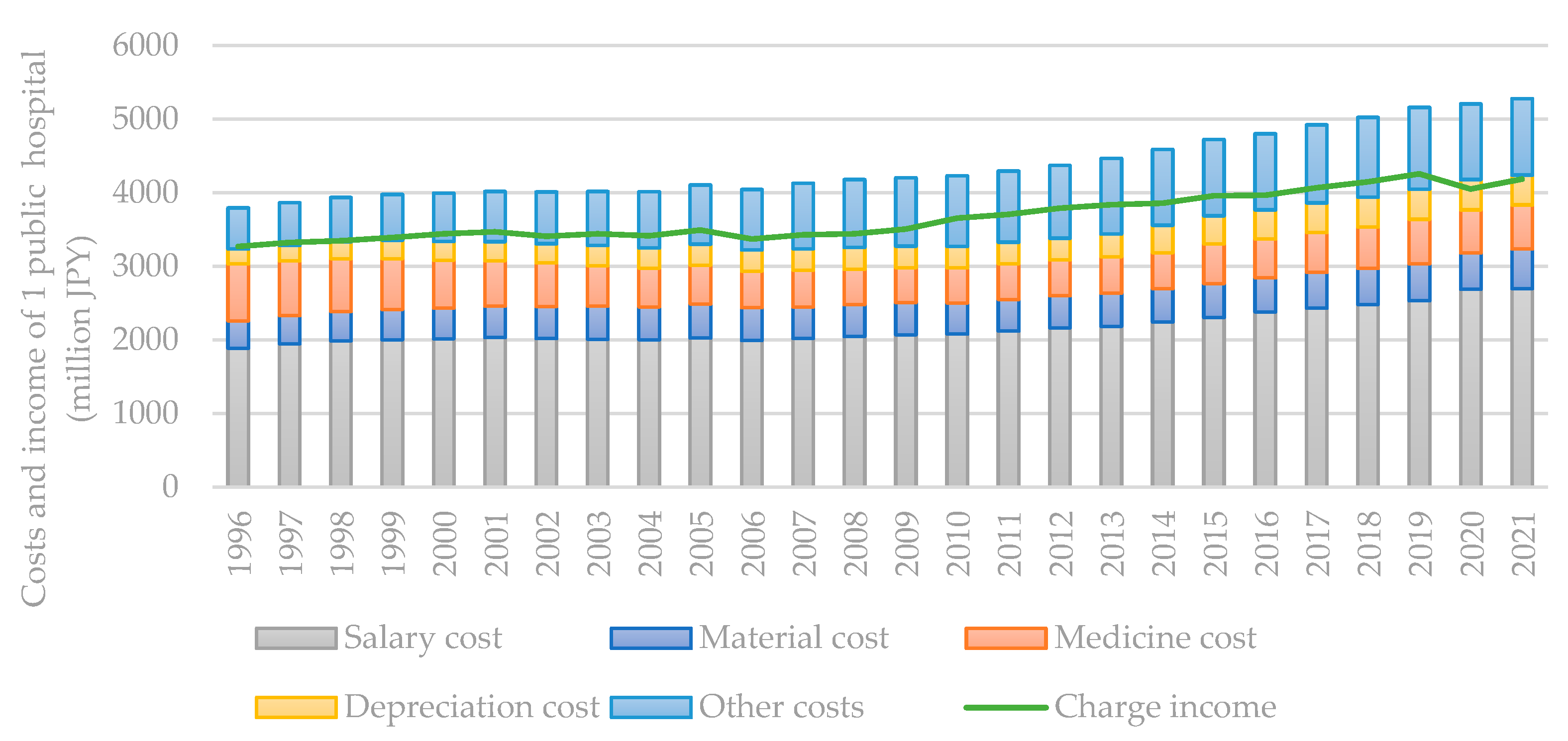
Figure 3.
Decomposition results of various factors influencing the total operating cost in a public hospital.
Figure 3.
Decomposition results of various factors influencing the total operating cost in a public hospital.
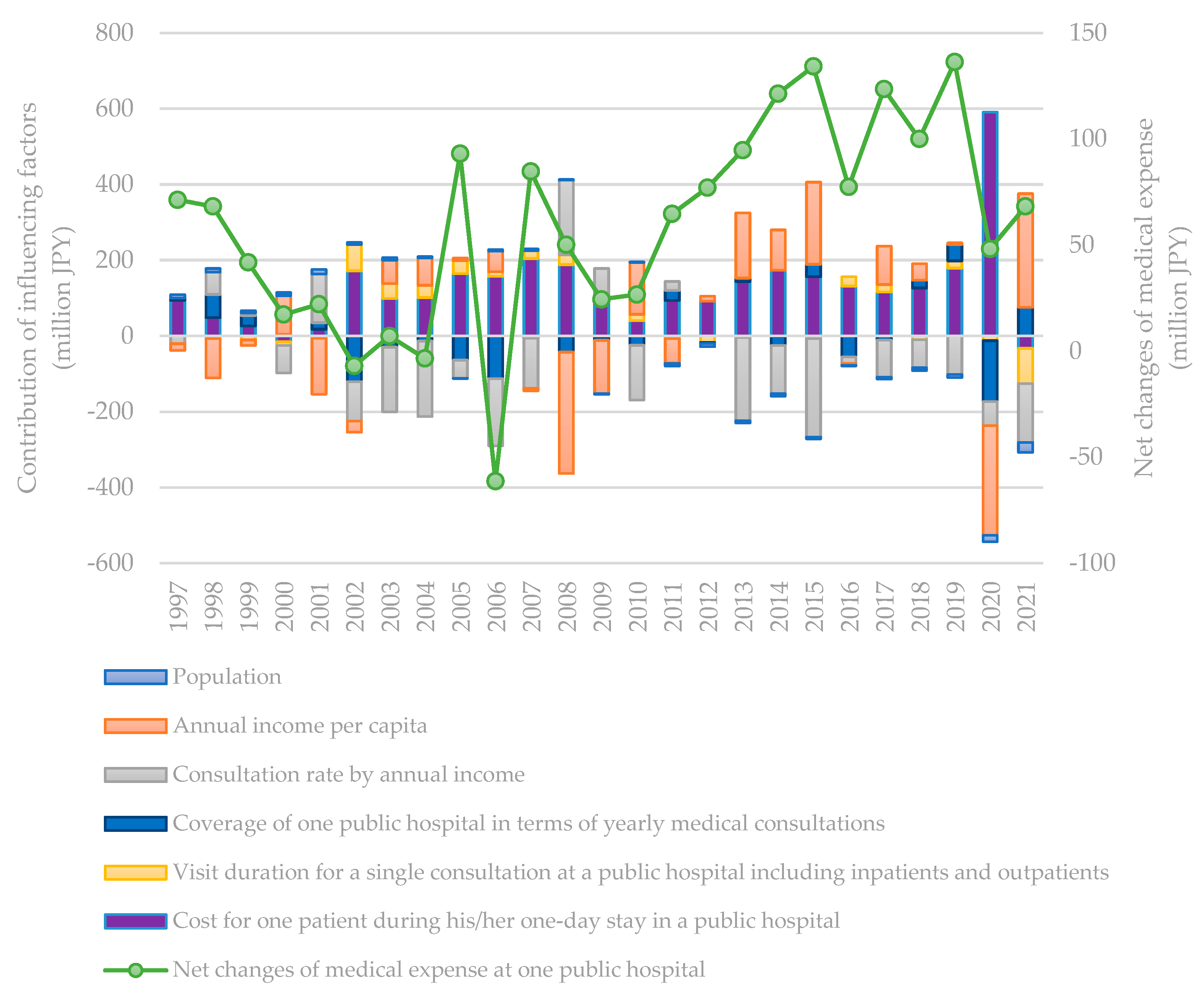
Figure 4.
Changes in the number of public hospitals in Japan (Details of the change in 2021 are currently not recorded in the statistics).
Figure 4.
Changes in the number of public hospitals in Japan (Details of the change in 2021 are currently not recorded in the statistics).
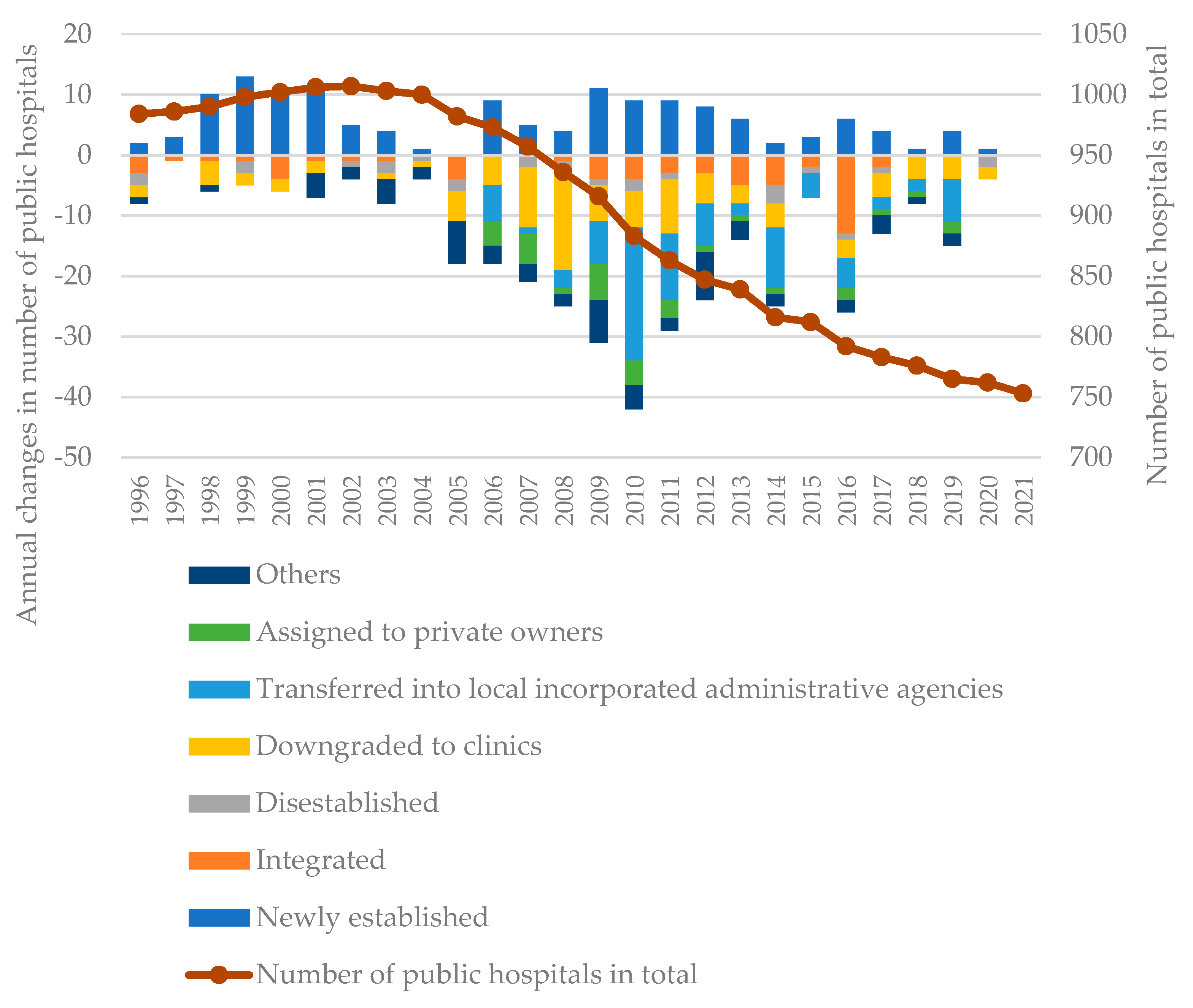
Figure 5.
Changes in service proportion of a public hospital and charge income per capita.
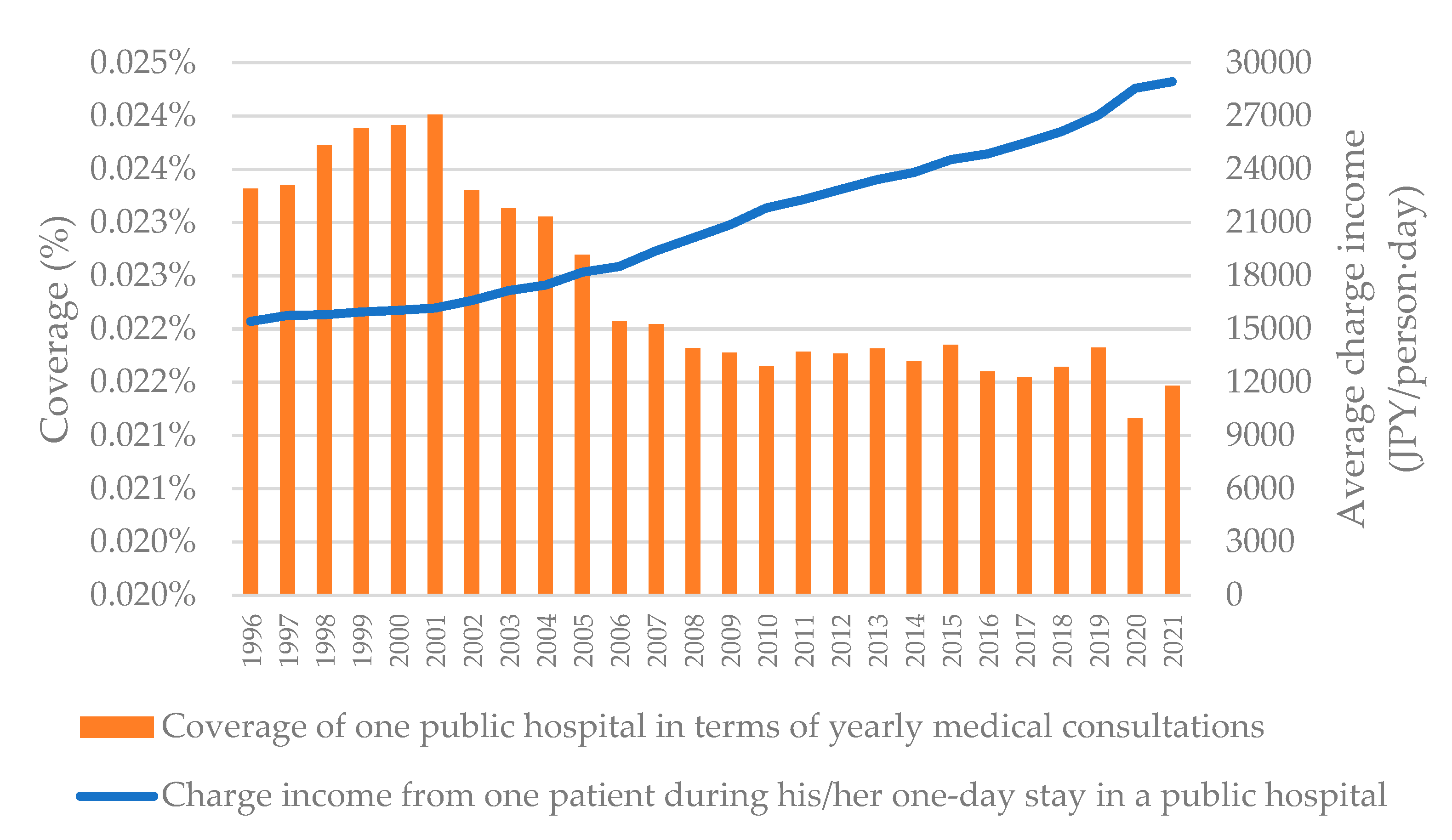
Figure 6.
Contribution of income level and consultation frequency to the operating cost of a public hospital.
Figure 6.
Contribution of income level and consultation frequency to the operating cost of a public hospital.
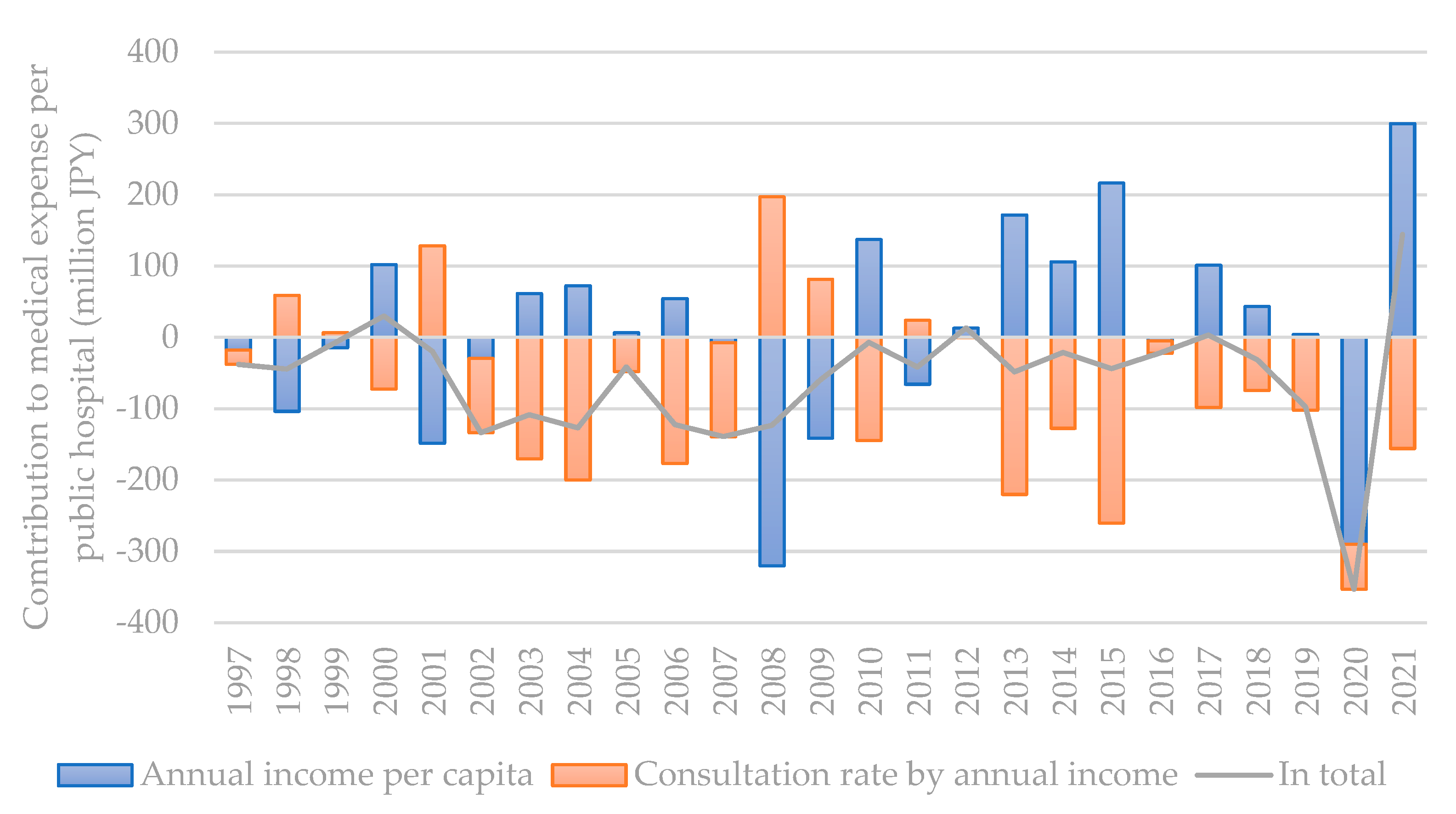
Figure 7.
Relative change rate of various costs for a patient during a one-day stay in a public hospital against the change rate of average charge income.
Figure 7.
Relative change rate of various costs for a patient during a one-day stay in a public hospital against the change rate of average charge income.
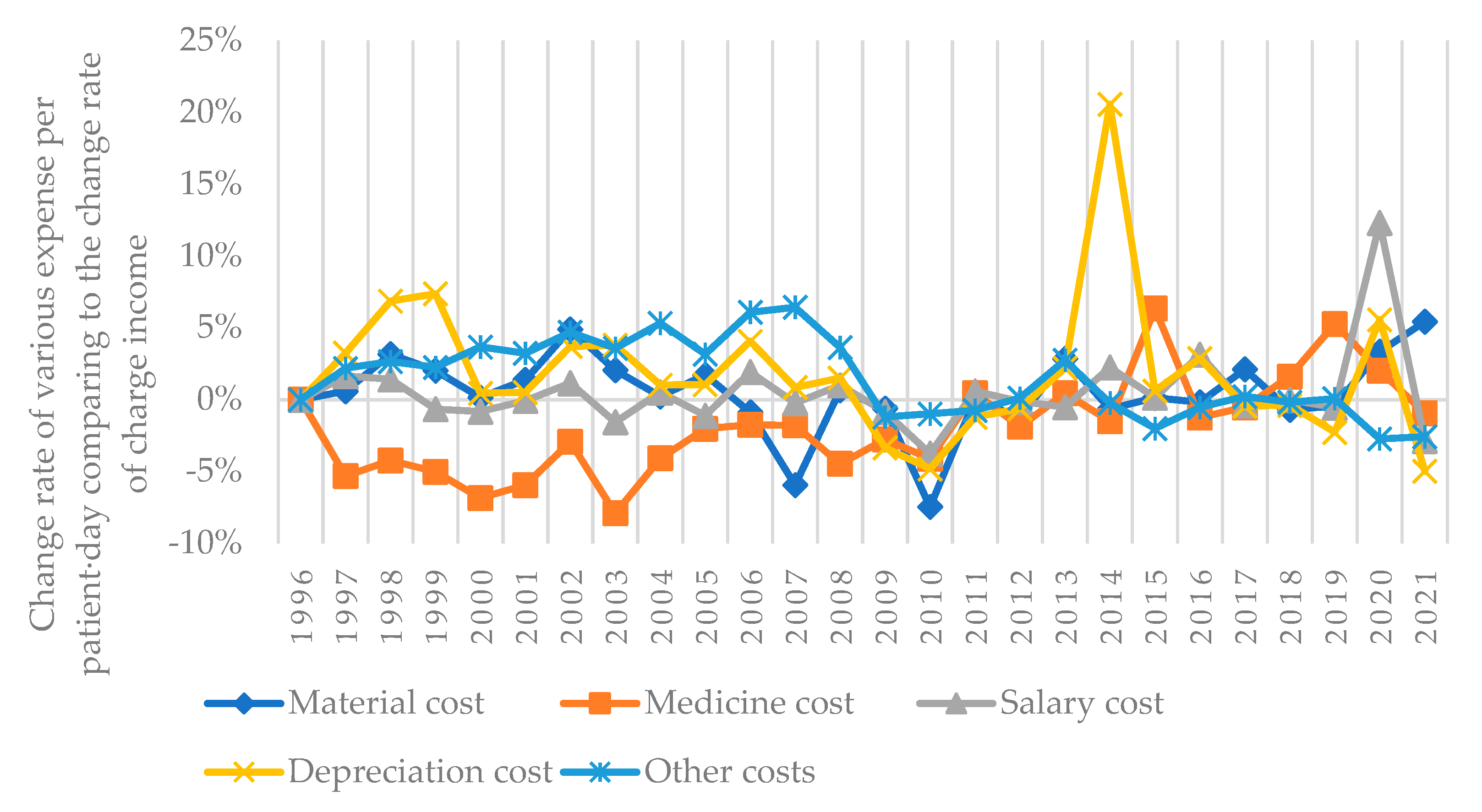
Table 1.
Representative studies focusing on correlation analysis regarding public hospital’s deficit status.
Table 1.
Representative studies focusing on correlation analysis regarding public hospital’s deficit status.
| Studies | Analysis tools | Identified key influencing factors |
| Ishikawa, 2019 | Multivariate regression analysis | Number of outpatients and average stay duration of inpatients contribute to operating profit, material cost and salary cost contribute to operating deficit |
| Ishibashi, 2016 | Multivariate regression analysis | Charge income from inpatients, number of inpatients per day, and charge income from outpatients contribute to operating profit, retirement bonus and depreciation cost contribute to operating deficit |
| Shimomura and Kubo, 2011 | t-test analysis | Insurance appraisal, salary cost, material cost, medical consumables cost, equipment-related cost, depreciation cost, etc. |
| Otsubo and Imanaka, 2008 | Multivariate multiple regression analysis | Number of outpatients and charge income from outpatients per person·day contribute to operating profit, depreciation cost contributes to operating deficit |
| Kawaguchi, 2005 | Cluster analysis | Ratio of salary cost and material cost to the total operating costs is the main factor influencing operating efficiency |
| Taniguchi et al., 2004 | Risk factor analysis | Salary cost, charge income from outpatients, material cost, depreciation cost, etc. |
Table 2.
The aggregate and influencing factors defined in this study.
| Item | Definition |
|---|---|
| Average total operating costs of one public hospital in Japan in year t (JPY) | |
| Population of Japan in year t (person) | |
| Annual income per capita in year t (JPY/person) | |
| Consultation rate by annual income in the year t (times/JPY) | |
| Coverage of one public hospital in terms of total annual medical consultations in year t (%) | |
| Visit duration for a single consultation to a public hospital including inpatients and outpatients in year t (days/time), here a single consultation of an outpatient is counted as a one-day stay in a public hospital | |
| Type i operating cost for one patient during his/her one-day stay in a public hospital in year t (JPY/day) |
Table 4.
Data preparation for LMDI decomposition from the corresponding statistical report.
| Statistics | Mark | Influencing factors | Formula |
|---|---|---|---|
| Population | ① | Population | ① |
| Number of public hospitals | ② | Annual income per capita | |
| Annual income | ③ | Consultation rate by annual income | |
| Number of outpatients per day in public hospitals | ④ | Coverage of one public hospital in terms of yearly medical consultations | |
| Number of inpatients per day in public hospitals | ⑤ | Visit duration for a single consultation at a public hospital including inpatients and outpatients | |
| Number of outpatients per day in all hospitals | ⑥ | Material cost for one patient during his/her one-day stay in a public hospital | ⑪/() |
| Number of inpatients per day in all hospitals | ⑦ | Medicine cost for one patient during his/her one-day stay in a public hospital | ⑫/() |
| Annual gross number of outpatients in public hospitals | ⑧ | Salary cost for one patient during his/her one-day stay in a public hospital | ⑬/() |
| Annual gross number of inpatients in public hospitals | ⑨ | Depreciation cost for one patient during his/her one-day stay in a public hospital | ⑭/() |
| Average visit duration of inpatients in all hospitals | ⑩ | Other costs for one patient during his/her one-day stay in a public hospital | ⑮/() |
| Material costs Medicine costs Salary costs Depreciation costs Other costs |
⑪ ⑫ ⑬ ⑭ ⑮ |
||
Table 5.
Historical changes of factors influencing a public hospital’s operating cost.
| Based on one public hospital | Year | 1996 | 1997 | 1998 | 1999 | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Population | million | 125.9 | 126.2 | 126.5 | 126.7 | 126.9 | 127.3 | 127.5 | 127.7 | 127.8 | 127.8 | 127.9 | 128.0 | 128.1 | 128.0 | 128.1 | 127.8 | 127.6 | 127.4 | 127.2 | 127.1 | 127.0 | 126.9 | 126.7 | 126.6 | 126.1 | 125.5 |
| Annual income per capita | million JPY/capita | 3.37 | 3.35 | 3.27 | 3.25 | 3.34 | 3.22 | 3.19 | 3.24 | 3.30 | 3.31 | 3.35 | 3.35 | 3.10 | 3.00 | 3.09 | 3.05 | 3.06 | 3.18 | 3.25 | 3.41 | 3.40 | 3.48 | 3.50 | 3.50 | 3.32 | 3.51 |
| Consultation rate by annual income | patient-times/million JPY | 1.43 | 1.42 | 1.45 | 1.45 | 1.42 | 1.47 | 1.43 | 1.37 | 1.31 | 1.29 | 1.24 | 1.20 | 1.25 | 1.28 | 1.24 | 1.24 | 1.24 | 1.18 | 1.15 | 1.09 | 1.08 | 1.06 | 1.05 | 1.03 | 1.01 | 0.98 |
| Coverage of one public hospital in terms of yearly medical consultations | % | 0.023 | 0.023 | 0.024 | 0.024 | 0.024 | 0.024 | 0.023 | 0.023 | 0.023 | 0.023 | 0.022 | 0.022 | 0.022 | 0.022 | 0.022 | 0.022 | 0.022 | 0.022 | 0.022 | 0.022 | 0.022 | 0.022 | 0.022 | 0.022 | 0.021 | 0.021 |
| Visit duration for a single consultation at a public hospital including inpatients and outpatients | days/time | 1.50 | 1.50 | 1.49 | 1.49 | 1.49 | 1.48 | 1.51 | 1.53 | 1.54 | 1.55 | 1.56 | 1.56 | 1.57 | 1.57 | 1.58 | 1.58 | 1.57 | 1.57 | 1.57 | 1.57 | 1.57 | 1.58 | 1.58 | 1.58 | 1.58 | 1.55 |
| Material cost for one patient during his/her one-day stay in a public hospital | JPY/patient-day | 1759 | 1808 | 1870 | 1926 | 1940 | 1981 | 2132 | 2247 | 2293 | 2426 | 2449 | 2420 | 2527 | 2603 | 2529 | 2583 | 2617 | 2756 | 2785 | 2874 | 2907 | 3040 | 3096 | 3190 | 3476 | 3712 |
| Medicine cost for one patient during his/her one-day stay in a public hospital | JPY/patient-day | 3642 | 3528 | 3388 | 3250 | 3047 | 2889 | 2882 | 2751 | 2688 | 2744 | 2746 | 2827 | 2806 | 2831 | 2845 | 2919 | 2939 | 3024 | 3030 | 3315 | 3318 | 3381 | 3522 | 3829 | 4122 | 4139 |
| Salary cost for one patient during his/her one-day stay in a public hospital | JPY/patient-day | 8912 | 9254 | 9409 | 9436 | 9416 | 9479 | 9844 | 10021 | 10253 | 10559 | 10956 | 11451 | 11992 | 12326 | 12432 | 12769 | 13081 | 13335 | 13859 | 14304 | 14941 | 15250 | 15637 | 16096 | 18981 | 18693 |
| Depreciation cost for one patient during his/her one-day stay in a public hospital | JPY/patient-day | 955 | 1007 | 1078 | 1168 | 1180 | 1195 | 1272 | 1363 | 1401 | 1473 | 1560 | 1648 | 1734 | 1739 | 1735 | 1751 | 1785 | 1869 | 2284 | 2368 | 2468 | 2517 | 2571 | 2603 | 2894 | 2790 |
| Other costs for one patient during his/her one-day stay in a public hospital | JPY/patient-day | 2642 | 2757 | 2838 | 2928 | 3053 | 3175 | 3409 | 3646 | 3906 | 4190 | 4522 | 5027 | 5397 | 5529 | 5729 | 5809 | 5964 | 6275 | 6367 | 6434 | 6484 | 6658 | 6815 | 7057 | 7262 | 7173 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



